Slide 1 Integrating The Cardiopulmonary System Into Physical ...
128
Slide 1 Integrating The Cardiopulmonary System Into Physical Therapy Practice ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 2 Integrating The Cardiopulmonary System Into Physical Therapy Practice Jamie Dyson Kathy Swanick ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 3 Objectives At the conclusion of this continuing education course the participant shall be able to: • Describe cardiopulmonary anatomy • Discuss cardiopulmonary pathophysiology • Demonstrate chest physical therapy techniques • Discuss results of pulmonary function tests • Demonstrate appropriate manual and mechanical airway clearance techniques • Discuss modes of mechanical ventilation and invasive monitoring • Perform Basic interpretation of EKG • Discuss phases of cardiac rehab and energy conservation • Discuss role in a medical emergency. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Slide 1 Integrating The Cardiopulmonary System Into Physical ...

Slide 1
Integrating The
Cardiopulmonary System Into
Physical Therapy Practice
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 2
Integrating The
Cardiopulmonary System Into
Physical Therapy Practice
Jamie Dyson
Kathy Swanick
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 3
Objectives
At the conclusion of this continuing education course the participant
shall be able to:
• Describe cardiopulmonary anatomy
• Discuss cardiopulmonary pathophysiology
• Demonstrate chest physical therapy techniques
• Discuss results of pulmonary function tests
• Demonstrate appropriate manual and mechanical airway clearance
techniques
• Discuss modes of mechanical ventilation and invasive monitoring
• Perform Basic interpretation of EKG
• Discuss phases of cardiac rehab and energy conservation
• Discuss role in a medical emergency.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 4
Introduction-
Why
Cardiopulmonary
Physical Therapy?
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 5
LIFE=
VENTILATION +
PERFUSION
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 6
Vital Signs
• Heart Rate
• Pulse Oximetry
• NBP/ ABP
• MAP
• Temperature
• End Tidal CO2
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 7
Vital Signs
Heart Rate
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 8
Pulse Palpation
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 9
Pulse Oximetry
An infrared light is used to measure
the percentage of hemoglobin
converted to oxyhemoglobin
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 10
NBP/ ABP
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 11
MAP
Mean Arterial Pressure
Its all about perfusion
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 12
Temperature
Normal Oral
Temperature 98.6
degrees F or 37.0
degrees Celsius
Rectal or Core
temperatures will be
slightly higher.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 13
End Tidal CO2
The level of carbon dioxide in
the air exhaled from the body,
the normal values of which are
4% to 6%; that is equivalent to
35 to 45 mm Hg
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 14
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 15
The Human Movement System
Our Vision-
Transforming society by optimizing
movement to improve the human
experience
IDENTITY
FOUNDATION
The Core Of Physical Therapist Practice,
Education, And Research
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 16
The human movement system comprises the
anatomic structures and physiologic functions that interact to move the body
or its component parts.
American Physical Therapy Association (2015).
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 17
PRACTICE AND THE HUMAN MOVEMENT SYSTEM
Human movement is a complex behavior within a
specific context.
Provide a unique perspective on purposeful, precise, and efficient movement across
the lifespan based upon the synthesis of their distinctive knowledge of the movement
system and expertise in mobility and locomotion.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 18
PHYSICAL THERAPIST PRACTICE AND THE HUMAN MOVEMENT SYSTEM
Physical therapists examine and evaluate the movement system (including diagnosis and prognosis)to provide a customized and integrated plan of care to achieve the individual’s goal-directed
outcomes.
American Physical Therapy Association (2015).
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 19
PRACTICE AND THE HUMAN MOVEMENT SYSTEM
Maximize an individual’s ability to engage with
and respond to his or her environment using movement-related
interventions to optimize functional capacity and
performance.American Physical Therapy Association (2015).
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 20
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 21
http://www.wilkes.med.ucla.edu/inex.htm
Auscultation
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 22
Auscultation
Breath Sounds
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 23
AuscultationContinuous Breath Sounds
Wheezes- a high-pitched whistling sound
made on exhaling.
Rhonchi- a rattling or rumbling sound, kind
of like a garden hose when the water has
just been turned on
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 24
Auscultation
Discontinuous Breath Sounds
Crackles- (Rales)– a crackling sound, like when paper is crinkled
Pleural Rubs- a soft brushing sound, like when sandpaper goes on wood.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 25
Review of
Pulmonary Anatomy
and Breathing
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 26
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 27
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 28
Surface Anatomy
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 29
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 30
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 31
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 32
Oxygen entering an alveolus
dissolves in the film of water
on its wall
Oxygen is in higher
concentration inside the
alveolus than in the blood.
Oxygen moves from a higher
concentration to a lower
concentration by the process
of diffusion.
Carbon dioxide is higher in the
blood than in the alveoli.
Carbon dioxide also moves
from a high concentration to a
lower concentration by the
process of diffusion.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 33
The (VRG) and the (DRG) within the medullary rhythmicity
area cooperate to establish the pattern for spontaneous
ventilation and basal rate of ventilation which may be adjusted
by impulses from related respiratory control centers in the
pons
The (VRG) has both inspiratory and expiratory neurons;
• The autorythmic inspiratory neurons stimulate the
diaphragm and external intercostals (2 seconds) to cause
inspirations
• Antagonistic expiratory neurons fire ( 3 seconds) to permit
expiration
The (DRG) neurons are involved in altering the pattern for
ventilation in response to the physiological needs of the body
Control of Breathing
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 34
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 35
Primary Muscles of Inhalation
Muscle Action Nerve Spine
DiaphragmElongates
the pleuraPhrenic C3,4,5
External
Intercostals
(11)
Elevates the
ribsIntercostal T1-11
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 36
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 37
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 38
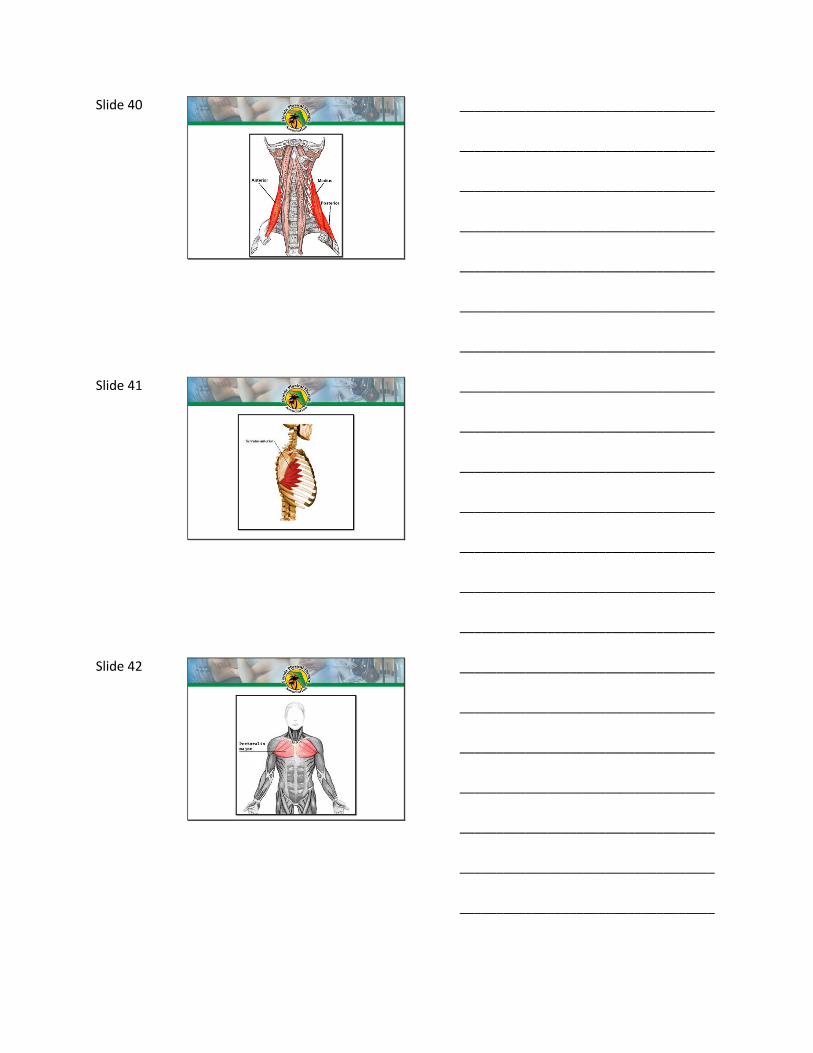
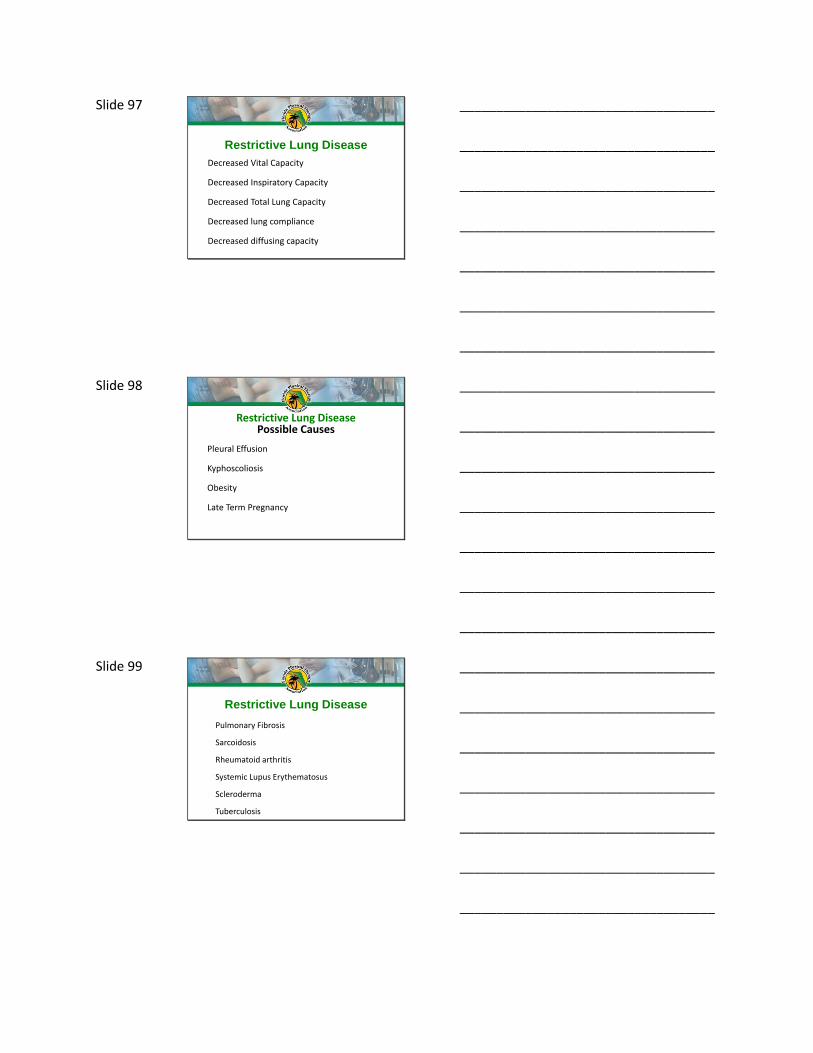
Accessory Muscles of Respiration
Muscle Action Nerve Spine
Sternocleidom
astoidElevates the sternum Accessory C2
Scalenes Elevate 1st 2 ribs Cervical Nerves C3-8
Serratus
AnteriorElevates 1st 8 ribs Long thoracic nerve C5-7
Pectoralis
Major
Increases thoracic
diameter
Lateral and medial
pectoral nervesC5-T1
Pectoralis
minorElevates ribs 3-5 Medial Pectoral nerve C8-T1
TrapeziusStabilizes the
scapula Accessory nerve C3-4
Erector Spinae Extends the trunkPosterior branch
spinal nervesAll
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 39
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 40
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 41
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 42
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 43
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 44
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 45
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 46
Primary Muscles of Exhalation
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 47
Forced ExhalationMuscle Action Nerve Spine
Rectus
Abdominis
Increase
intrathoracic
pressure
Thoraco-abdominal
nerveT7-12
Obliquus
Externus
Abdominis
Increase
intrathoracic
pressure
thoraco-abdominal
nervesT7-12
Obliquus
Internus
Abdominis
Increase
intrathoracic
pressure
thoracico-abdominal
nervesT6-L1
Transverse
Abdominis
Increase
intrathoracic
pressure
thoraco-abdominal
nerveT9-T12
Internal
Intercostals
Depresses
ribsIntercostal Nerve T1-T11
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 48
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 49
Pathophysiology Of
The Pulmonary System
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 50
Atelectasis
Atelectasis is defined as a state in which the
lung, in whole or in part, is collapsed or without
air.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 51
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 52
Atelectasis
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 53
Atelectasis
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 54
Obstructive Lung Disease
Decrease exhalatory airflow
Restrictive Lung Disease
Decreased inspiratory capacity
Pulmonary Disease
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 55
Obstructive Lung Disease
Chronic Obstructive Pulmonary Disease (COPD)
Chronic Obstructive Lung Disease (COLD)
Chronic Obstructive Airway Disease (COAD)
Chronic Airway Obstruction (COA)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 56
Obstructive Lung Disease
Emphysema- permanent enlargement of air-spaces distal to the terminal bronchiole with destruction of their walls.
Leading cause is SMOKING
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 57
Emphysema
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 58
EmphysemaTwo Types
Centriloblular Emphysema
Panlobular Emphysema
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 59
EmphysemaCentriloblular Emphysema
Inflammation, edema, thickened bronchiolar walls
Destruction of the bronchioles
Common in upper lobes and superior
segments of the lower lobes
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 60
EmphysemaPanlobular Emphysema
Rare
Destructive enlargement of the alveoli
Alpha 1 antitripsen deficiency
Loss of recoil in the alveoli
Primarily lower lobes
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 61
Develop Bullea- enlarged alveoli caused by decreased ability to exhale caused by increased lung compliance = decreased elastic recoil
Emphysema
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 62
EmphysemaClinical Presentation
Dyspnea- with exertion
Accessory muscle
breathing
Pursed Lip breathing
Forward Posture
Barreled Chest
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 63
EmphysemaClinical Presentation
Pink Puffers
Increased Respiratory Work
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 64
Pink Puffer
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 65
EmphysemaClinical Presentation
Reduced breath sounds in all lung fields
Wheezes
Increased Total Lung Capacity
Increased Residual Volumes
Increased dead Space
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 66
EmphysemaClinical Presentation
Chest X-ray
Over inflated
Lungs
Flattened
Diaphragm
Elongated
Heart
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 67
TreatmentNon PT
Iv Fluids
Antibiotics
Low Flow O2
Bronchodilators
Corticosteriods
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 68
TreatmentNote
Hypercapnia commonly occurs in severe
Emphysema Oxygen given to patients with
emphysema may reduce their ability to breath,
resulting in hypercapnia. This is why exact
doses of oxygen are usually figured out for
those with emphysema so that they receive
neither too little nor too much oxygen. Note: if a
patient is actively short of breath, never
withhold oxygen from them.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 69
TreatmentPT
Energy Conservation
Exercise Program to decrease muscle wasting
Treatment of tight accessory muscles
Quit Smoking!!!!!!!!!!!
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 70
Smoking Is The Leading
Cause Of Emphysema
All physical therapy practitioners will
have to discuss cessation of smoking
with their patients.
Lets get the facts
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 71
Quit Now
20 minutes after quitting your heart rate and blood pressure drops
12 hours after quitting carbon monoxide levels in your blood drop to normal2 weeks to 3 months after quitting circulation improves and lung function increases
1 to 9 months after quitting coughing and shortness of breath decrease; cilia regain normal function, increasing the ability to handle mucus.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 72
1 year after quitting the excess risk of coronary heart disease is half that of a smoker5 years after quitting your stroke risk decreases to that of a nonsmoker 5 to 15 years after quitting.
10 years after quitting the lung cancer death rate is about half that of someone who continues to smoke. Quitting lowers the risk of cancers of the mouth, throat, esophagus, bladder, cervix and pancreas15 years after quitting the risk of coronary heart disease is lowered to that of a nonsmoker.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 73
Chronic Bronchitis
Chronic swelling and inflammation of the bronchi
and bronchioles
Diagnosis is based on a report of a productive
cough for 3 months during 2 consecutive years.
Obstructive Lung Disease
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 74
Decreased number of cilia
Increased mucus
Bronchiolitis
Bronchiolar narrowing
Chronic Bronchitis
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 75
• Caused by long term irritation of the
tracheobronchial tree
• Most common cause of irritation= smoking
• Cigarette smoke causes inflammation of the
epithelium = increased production of mucus from
goblet cells and mucus glands
• Smoking inhibits ciliary action and destroys cilia
• Can also be caused by allergens and air pollution
Chronic Bronchitis
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 76
Hypersucretion of mucus + impairment of cilia =
chronic productive cough
Increased mucus = Increased risk of respiratory
infection
Chronic Bronchitis
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 77
Chronic Bronchitis
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 78
Blue Bloater
StockyAppear blue
due to
hypoxemia
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 79
Chronic Bronchitis
Blue Bloater
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 80
Chronic BronchitisTreatment
Non PTIv Fluids
Antibiotics
Low Flow O2
Bronchodilators
Corticosteriods
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 81
Chronic Bronchitis
Treatment PT
Energy Conservation
Exercise Program to decrease muscle wasting
Treatment of tight accessory muscles
Quit Smoking!!!!!!!!!!!
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 82
Asthma- chronic condition involving in which the
airways occasionally constrict, become inflamed, and
are lined with excessive amounts of mucus, often in
response to triggers
Triggered by exposure to an environmental stimulant
such as an allergen, environmental tobacco smoke,
cold or warm air, perfume, pet dander, moist air,
exercise or exertion, or emotional stress.
Obstructive Lung Disease
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 83
Bronchial smooth muscle spasm
Inflammation of the mucosa
Overproduction of mucus
Asthma
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 84
Asthma
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 85
Asthma
Affects 5-10% of the US
Prevalent in people under 25- usually allergic
Appox 80% of children with asthma do not
have asthma after 10 years of age
Can have an adult onset- intrinsic asthma
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 86
AsthmaClinical Signs
Tachypnea
Cough
Dyspnea
Wheezing
Chest Tightness
Diminished Breath Sounds
Prolonged Exhalation
Hyperinflated Lungs
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 87
AsthmaTreatment- Non PT
Iv Fluids
Supplemental O2
Bronchodilators
Corticosteriods
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 88
AsthmaTreatment- PT
Stop activities as symptoms arise
Take a good history prior to prescribing an
exercise program
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 89
Bronchiectasis is a disease that causes localized
irreversible dilation of part of the bronchial tree.
Involved bronchi are dilated, inflamed and easily
collapsible resulting in airflow obstruction and
impaired clearance of secretions
Generally associated with a chronic necrotizing infection
within these airways
Obstructive Lung Disease
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 90
Usually localized to a few segments or entire
lobe of one lung.
40-50% of cases are bilateral
Can cause varicese which can cause
hemoptysis
Bronchiectasis
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 91
BronchiectasisCystic Fibrosis
Hereditary disease affecting the exocrine (mucus)
glands of the lungs, liver, pancreas, and intestines,
causing progressive disability due to multisystem
failure. Thick mucus production results in frequent
lung infections
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 92
Cystic Fibrosis
Decreased pancreatic enzymes lead to poor
growth
Many die young in their 20s and 30s
Can be confirmed by high levels of salt found
during a sweat test.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 93
Cystic Fibrosis
Affects Multiple
Organs
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 94
Bronchiectasis
Treatment
Non PT
Antibiotics
Oxygen
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 95
BronchiectasisTreatment
PT
Chest Physical Therapy- percussion
Segmental breathing
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 96
Restrictive Lung Disease
Environmental factors play a major role in
etiology
Characterized by stiffening of the parenchyma-
prevents lungs from expanding fully
Increased recoil of lung tissue
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 97
Restrictive Lung Disease
Decreased Vital Capacity
Decreased Inspiratory Capacity
Decreased Total Lung Capacity
Decreased lung compliance
Decreased diffusing capacity
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 98
Restrictive Lung DiseasePossible Causes
Pleural Effusion
Kyphoscoliosis
Obesity
Late Term Pregnancy
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 99
Restrictive Lung Disease
Pulmonary Fibrosis
Sarcoidosis
Rheumatoid arthritis
Systemic Lupus Erythematosus
Scleroderma
Tuberculosis
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 100
Restrictive Lung DiseasePulmonary Fibrosis
Causes
Inhaled environmental and occupational pollutants
Smoking!!!!!!!!!
Certain medications
Therapeutic radiation
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 101
Restrictive Lung DiseasePulmonary Fibrosis
The current thinking is that pulmonary
fibrosis begins with repeated injury to the
lining of the alveoli. The damage eventually
leads to scarring (fibrosis), which stiffens
your lungs and makes breathing difficult.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 102
Pulmonary Fibrosis
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 103
Restrictive Lung DiseaseSarcoidosis
Disorder where one develops small inflammatory nodules and can affect multiple organs.
Affects African Americans> Caucasians.
Women > Men
Most cases can spontaneously regress.
Most common treatment is corticosteroids
Physical therapy interventions involve working on general conditioning and endurance.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 104
Restrictive Lung DiseaseRheumatoid Arthritis
Pleural disease can be a manifestation of RA
Causes fibrous tissue on outside of lung causing restriction.
In severe cases treated with decortication
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 105
Restrictive Lung DiseaseSystemic Lupus Erthematosus
• Lupus can cause polyserositis around the lung tissue causing pleural effusion.
• Pneumonitis can also develop.• Patients will complain of dyspnea on
exertion pleural pain or discomfort and productive cough
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 106
Restrictive Lung DiseaseScleroderma
• Scleroderma causes thickening and fibrosis of the connective tissue.
• Two thirds of patients can have pulmonary involvement.
• Chest x-ray will show fibrosis of middle and lower lung fields.
• Treatment is corticosteroids.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 107
Restrictive Lung DiseaseTuberculosis
Tuberculosis (TB) is a common and often
deadly infectious disease caused by
mycobacteria
The typical symptoms of tuberculosis are a
chronic cough with blood-tinged sputum, fever,
night sweats and weight loss.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 108
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 109
Restrictive Lung DiseaseLung Cancer
Leading cause of death due to cancer
Smoking is leading cause
Can be primary or metastatic
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 110
Other Pathologies
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 111
Pneumonia• Inflammatory illness of the lung
• Alveoli fill with fluid
• Infection can be bacteria, viruses, fungi or parasites.
• Can be caused by chemical or physical injury to the lungs.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 112
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 113
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 114
Ventilator Associated Pneumonia
Refers specifically to nosocomial bacterial
pneumonia that has developed in patients who
are receiving mechanical ventilation. Ventilator-
associated pneumonia that occurs within 48 to
72 hours after tracheal intubation is usually
termed early-onset pneumonia; it often results
from aspiration
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 115
Ventilator Associated Pneumonia
Prevention
Good hand washing
Head of bed 30 degrees at all times.
Control of GERD
Change circuits frequently
Oral hygiene
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 116
Aspiration Pneumonia
Foreign material enters
the bronchial tree
Usually in the right
lower lobe.
Early identification of
dysphagia
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 117
Collapsed lung caused by
air in the pleural space.
Can be caused
spontaneously or by
disease or injury.
Air can come from within
the lung or from
atmosphere.
Pneumothorax
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 118
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 119
Blood accumulating in the pleural cavity
Usually caused by trauma
Blood from the serous membrane lining the thorax and covering the lungs.
Hemothorax
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 120
Empyema
A collection of pus in an existing cavity.
Can arise from pneumonia.
Drained with thoracentesis.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 121
Rib Fractures
Pain with breathing and/or movement.
Suppressed cough secondary to pain.
Grating sound with breathing or movement.
A portion of the chest wall moving separately from the rest of the chest- flail chest.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 122
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 123
Chest Tube
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 124
Chest Tube
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 125
Obstructive Sleep Apnea
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 126
Obstructive Sleep Apnea
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 127
Pulmonary Function
Testing
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 128
Tidal Volume (TV) The volume of air breathed in and out
without conscious effort
Inspiratory Reserve Volume (IRV) The additional volume of air that can be
inhaled with maximum effort after a
normal inspiration.
Expiratory Reserve Volume (ERV) The additional volume of air that can be
forcibly exhaled after normal exhalation.
Vital Capacity (VC) The total volume of air that can be
exhaled after a maximum inhalation:
VC=TV+IRV+ERV
Residual Volume (RV) The volume of air remaining in the lungs
after maximum exhalation. The lungs are
never completely emptied.
Total Lung Capacity (TLC) Vital Capacity+Residual Volume
Minute Ventilation The volume of air breathed in 1 minute
(TV) * breaths/minute
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 129
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 130
Pulmonary Function TestingHow much air volume can be moved into and out of the lungs?
How fast the air in the lungs can be moved in and out?
How is the compliance of the lungs?
How do the lungs respond to chest physical therapy and medications?
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 131
Pulmonary Function TestingUses
Screening for presence of obstructive or restrictive diseases.
Evaluating a patient prior to surgery.
Evaluate the patient’s condition for weaning from a ventilator.
Documenting the progression of pulmonary disease
Documenting the effectiveness of interventions
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 132
Pulmonary Function Testing
Age- As a person ages the natural elasticity of the lungs
decreases which means smaller and smaller lung volumes as one
age.
Gender- Lung volumes for males are larger than those of
females even if they are matched for height and weight.
Body height and size- A small man will have a smaller
PFT result than a man of the same age who is much larger
Race- Environmental Factors and Altitude may have an affect
on PFT results.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 133
Pulmonary Function TestingTerminology
• FVC- Forced Vital Capacity
• FEV1- Forced Expiratory Volume in 1 second
• FEV1/FVC- FEV1%- what percent of FVC is expelled in 1st second
• FEV3- Forced Expiratory Volume in 3 seconds
• FEV3/FVC- FEV3%- should be close to 100%
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 134
Pulmonary Function TestingFVC
• Obstructive lung disease- FVC will be decreased due to obstruction and airway collapse during forced exhalation.
• Restrictive lung disease FVC will be smaller due to the lungs being smaller to start with because of the disease.
• Bronchodilators will improve FVC 10-15% with obstructive lung disease.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 135
Pulmonary Function TestingSVC
Slow vital capacity (SVC) test- Have the patient
slowly and completely blow out all of the air from
their lungs. Eliminates the strong
bronchoconstriction that come with a forced
exhalation. The VC may be larger with a SVC test
leading to an obstructive diagnosis.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 136
Pulmonary Function Testing
FEV1
• In healthy individuals it is common the exhale 75-80% of vital capacity in first second of FVC test.
• If FEV1 is low compared to predicted values the patient may have an obstructive or restrictive lung disease.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 137
Pulmonary Function TestingFEV1%
• Both FVC and FEV1 will be low in both obstructive
and resistive lung disease.
• If FEV1% is low (<70%) it is consistent with an
obstructive disease.
• If FEV1% is 85%-100% it is consistent with a
restrictive disease.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 138
Pulmonary Function Testing
Lets Give It A Try
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 139
Pulmonary Function TestingCase 1
Predicted Values Measured Values % Predicted
FVC 6.00 liters 4.00 liters 67%
FEV1 5.00 liters 2.00 liters 40%
FEV1/FVC 83% 50% 60%
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 140
Pulmonary Function TestingCase 1
Predicted Values Measured Values % Predicted
FVC 6.00 liters 4.00 liters 67%
FEV1 5.00 liters 2.00 liters 40%
FEV1/FVC 83% 50% 60%
Obstructed Lung Disease
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 141
Pulmonary Function Testing
Case 2
Predicted Values Measured Values % Predicted
FVC 5.68 liters 4.43 liters 78%
FEV1 4.90 liters 3.52 liters 72%
FEV1/FVC 84% 79% 94%
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 142
Pulmonary Function TestingCase 2
Predicted Values Measured
Values
% Predicted
FVC 5.68 liters 4.43 liters 78%
FEV1 4.90 liters 3.52 liters 72%
FEV1/FVC 84% 79% 94%
Restricted Lung Disease
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 143
Pulmonary Function TestingCase 3
Predicted Values Measured Values % Predicted
FVC 5.04 liters 5.98 liters 119%
FEV1 4.11 liters 4.58 liters 111%
FEV1/FVC 82% 77% 94%
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 144
Pulmonary Function TestingCase 3
Predicted
Values
Measured
Values
% Predicted
FVC 5.04 liters 5.98 liters 119%
FEV1 4.11 liters 4.58 liters 111%
FEV1/FVC 82% 77% 94%
Normal
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 145
Pulmonary Physical
Therapy Lab
Including Vitals And
Breath Sounds
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 146
Vents and Invasive
Monitors
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 147
Modes of Mechanical Ventilation
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 148
Modes of Mechanical VentilationTerms
Trigger- variable that causes a breath to be delivered- pressure, volume, flow
Flowrate- The speed at which a breath is delivered- liters/min
Frequency- breaths /time- breaths/minute
Spontaneous Breaths- Breathing through vent circuit without assistance
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 149
Modes of Mechanical Ventilation
Controlled Mechanical Ventilation (CMV)
Requires patient to be sedated and chemically
paralyzed. The vent delivers all breaths at a preset
frequency, volume and flow rate.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 150
Modes of Mechanical Ventilation
Assist Control (AC)
The patient receives a preset volume, flow rate
and frequency. The patient can trigger the
machine to deliver a breath at the preset
parameters. All breaths are machine delivered.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 151
Modes of Mechanical Ventilation
Assisted Mechanical Ventilation (AMV)
Similar to AC without a set frequency. The
patient triggers the vent to deliver a preset
volume at a set flow rate.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 152
Modes of Mechanical Ventilation
Intermittent Mandatory Ventilation (IMV)
The vent delivers a set frequency and volume. The patient is allowed to take spontaneous
breaths. The machine may cycle a breath before the patient can exhale a spontaneous breath
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 153
Modes of Mechanical Ventilation
Synchronized Intermittent Mandatory Ventilation (SIMV)
Synchronizes the machine delivered breaths with the patients spontaneous breaths. If no inspiratory effort the
machine delivers a mandatory breath.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 154
Modes of Mechanical Ventilation
Continuous Positive Airway Pressure (CPAP)
The patient spontaneously breaths and a preset level of pressure is constantly maintained. Can be used with both an artificial airway or with a
tight fitting mask.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 155
Modes of Mechanical Ventilation
Bilevel Positive Airway Pressure (BIPAP)
Noninvasive form of mechanical ventilation-uses a tight fitting nasal or face
mask. There are different pressures for inhalation and exhalation but both above
atmospheric pressure.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 156
Modes of Mechanical Ventilation
Airway Pressure Release Ventilation (APRV)
The patient spontaneously breaths with a set amount of CPAP. If additional ventilation is
needed the CPAP can be dropped allowing the patient to exhale. CPAP is restored once
exhalation is complete. Allows more patient control then traditional CPAP.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 157
Modes of Mechanical Ventilation
Pressure Support Ventilation (PSV)
Patient is allowed to breath spontaneously with a preset inspiratory support until the flow rate reaches a minimal level. Patient controls the rate, TV and inspiratory time.
Can be used in conjunction with SIMV
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 158
Modes of Mechanical Ventilation
Mandatory Minute Ventilation (MMV)
The patient breaths spontaneously but a minimal level of minute ventilation will be achieved with ventilator
support. Usually used with PSV.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 159
Modes of Mechanical Ventilation
Volume Assured Pressure Support (VAPS)
The patient breaths spontaneously in the PSV mode. The ventilator monitors each tidal volume. If the
patient is not going to achieve the set volume the vent will keep a constant flow rate and increase
pressure until volume is reached
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 160
Modes of Mechanical Ventilation
High Frequency Oscillatory Ventilation (HFOV)
High respiratory rates delivered- up to 900 breaths per minute at a very small tidal volume. Gas is pushed into
the lung during inhalation and pulled out during exhalation. Used in severe cases of pulmonary disease that do not respond to normal mechanical ventilation.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 161
When Can You Pull This Thing?
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 162
Why are folks intubated?
Airway
Breathing
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 163
Airway Issues
• Mechanical
Obstruction-
surgical or non
surgical
• Edema
• Inability to mobilize
secretions
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 164
Breathing Issues
Obstructive Pulmonary Disease
Restrictive Pulmonary Disease
Respiratory Failure
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 165
CPAP Trial
Intubated patient placed on CPAP of
5mmHg
ABGs drawn
Patient closely monitored.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 166
Leak Test
• Endotrachial balloon is deflated
• Looking for at least a 50% leak from
tidal volume
• Decreased leak= increased edema
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 167
Before It Can Be Pulled
Wean pressure Support
Wean PEEP
Trach Collar trials
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 168
Arterial Line
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 169
Arterial Line
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 170
Central Venous Pressure2-6 mm Hg
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 171
Pulmonary Artery Catheter-Swan-Ganz
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 172
Pulmonary
Left VentricleRight Ventricle
Systemic
PAP PAOP
CVP ABP
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 173
Intra Cranial Pressure Monitor
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 174
ICP Monitor
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 175
Intra Aortic Balloon Pump
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 176
Dialysis
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 177
Continuous Renal Replacement Therapy
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 178
Pulmonary Case
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 179
History of Present Illness
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 180
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 181
PT Exam
• Pt received supine in bed on vent (desaturated over
night- orally intubated
• Mode SIMV rate of 2, PSV 10, PEEP 5, FiO2 40%,
• HR 98, BP 126/51, and O2 SAT 97%.
• Patient alert, pleasant, able to communicate by head
nodding and writing, and able to follow commands.
• Hemoglobin 8.5
• Trending Down
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 182
Bed Mobility/Transfers
• Roll to Left Mod Assist
• Roll to Right Mod Assist
• Supine to Sit Deferred due to Hb
• Sit to Supine Deferred due to Hb
• Sit to Stand Deferred due to Hb
• Stand to Sit Deferred due to Hb
• Bed to Chair Deferred due to Hb
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 183
Day 2
• Pt was received supine in bed on vent mode SIMV, rate 2, PSV 12, PEEP 10, FiO2 55%
• Hb stable at 8.4
• HR 100, BP 148/63, and O2 SAT 92.
• Pt family was present in room for TherEx.
• Pt transferred from supine to sit EOB Min A-performed deep breathing, diaphragmatic breathing and segmental breathing exercises. bed to chair min assist.
• Pt with BP to 173/70 HR 120- gait deferred at this time
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 184
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 185
Day 3
• Oxygen Device: Ventilator
• O2 (%): 75
• Mode: SIMV + PS
• Total breaths/minute: 14
• Set breaths/minute: 14
• Set VT (mL): 700
• PS (cmH2O): 16
• Mean Airway Pressure (cmH2O): 23
• PEEP (cmH20): 18
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 186
Day 3
• Oxygen Device: Ventilator
• O2 (%): 75
• Mode: SIMV + PS
• Total breaths/minute: 14
• Set breaths/minute: 14
• Set VT (mL): 700
• PS (cmH2O): 16
• Mean Airway Pressure (cmH2O): 23
• PEEP (cmH20): 18
Pt on Propofol
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 187
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 188
Day 5
• Oxygen Device: Ventilator
• O2 (%): 100
• Mode: PC/SIMV + PS
• Total breaths/minute: 20
• Set breaths/minute: 20
• PS (cmH2O): 12
• Mean Airway Pressure (cmH2O): 34
• PEEP (cmH20): 26.
Pt now on Rocuronium
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 189
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 190
• Required placement of bilateral chest tubes
yesterday
• Also started on NO for significant hypoxia
• Responded well and his sats have improved
significantly to mid-high 90s
• Cont PCV and wean peep and FiO2 as tolerated
• Neuro GCS 3, sedated paralyzed
• Resp on 26 PEEP, 70% FiO2
Nitrous Oxide- local vaso-dilation
Day 7
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 191
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 192
• The patient remains intubated .
• He continues to require high levels of PEEP and FiO2
and to have low saturations and continues to be
febrile.
• He was started on cooling blanket to help lower his
temperature.
• He remains sedated and paralyzed.
• Yesterday he developed acute renal failure, hydration
was attempted and nephrology was consulted for
possible HD or CRRT.
Day 10
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 193
• O2 (%): 100
• Mode: PC/SIMV + PS
• Total breaths/minute: 30
• Set breaths/minute: 30
• PS (cmH2O): 10
• PEEP (cmH20): 32
ABGs:
• Ph 7.15 PCO2 68 mmHg (35-45) PO2 71(80-100) mmHg. HCO3 23.1 22-26 mmol/l
Day 10
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 194
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 195
Day 11
Emergent laparotomy,
application of negative
pressure wound
therapy dressing
(ABThera placement) >
50 cm2
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 196
Day 14
• Pt off paralytics/NO
• Vent- SIMV with PS rate of 8, 12 PS, 10 PEEP
and 60% FiO2
• PT resumed pt OOB to chair with max assist
• Extremity strength grossly 2/5
• Pt to have tracheostomy in am.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 197
Day 15
• Trached this am- - vent SIMV rate of 2, 12
PS, 10 PEEP 50% FiO2.
• PT- Ther- ex- OOB- chair max assist
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 198
Day 16
• Off propofol
• Vent- SIMV rate of 2, 8 PS, 6 PEEP, 40%
Fio2.
• Trach Collar begun when OOB
• Began deep breathing and segmental
breathing exercises
• Pt to OR in pm for abdominal closure.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 199
Day 17
• Pt with 3/5 strength
• Tolerating 2 hours on trach collar
• Vent SIMV rate of 2, 6 PS, 5 PEEP, 40%
FiO2
• Gait trained 20 feet with PT
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 200
Day 17
• Pt with 3/5 strength
• Tolerating 2 hours on trach collar
• Vent SIMV rate of 2, 6 PS, 5 PEEP, 40%
FiO2
• Gait trained 20 feet with PT
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 201
• Transfer to Step-Down Unit
• Chest tubes out
• Foley Out
• Increased trach collar times to 24 hours-
• Rehab referral
• Progressing Mobility
• Speaking valve/Eating
Day 18-Day 20
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 202
Day 21
• Trach red capped
• Gait trained 150 feet with rolling walker on
room air with supervision
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 203
Day 22
• Discharge Home with parents and siblings
• Home Health PT/Nursing/RT
• Day 25 Trach Out.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 204
Airway Clearance Lab
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 205
Review of Cardiac
Anatomy
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 206
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 207
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 208
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 209
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 210
Innervation Of The Heart
Intrinsic
• SA node is the pacemaker of the heart-
impulse formation 100 bpm
• SA node under parasympathetic control
which decreases the normal rate to 60-
90 BPM
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 211
Innervation Of The Heart
Extrinsic
• Autonomic Nervous System
• Parasympathetic- Vagus Nerve
• Sympathetic- Upper Thoracic Nerves
• Cardiac plexus located near the tracheal bifurcation
• Supply the SA and AV nodes
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 212
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 213
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 214
Pathophysiology of
the Cardiac System
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 215
Cardiac Pathophysiology
• Coronary Artery Disease
• Congestive Heart Failure
• Valvular Heart Disease
• Athletic Heart Syndrome
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 216
Coronary Artery Disease (CAD)
• Arteries on the walls of the heart are vital to the heart muscle’s survival, providing oxygen and necessary nutrients
• The disease process begins when atherosclerotic plaque begins to build up in the arteries
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 217
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 218
Coronary Artery Disease
• Atherosclerosis
• Begins with trauma to the intima of the arterial wall
• Trauma related to list of risk factors
• Media (consists of smooth muscle is exposed to circulation
• Thought to be the origin of lesion.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 219
Atherosclerosis
• Platelet agitation at lesion site induce smooth muscle and endothelial replication
• Fatty streaks –low density lipoproteins (LDL) develop in smooth muscle of media
• Fibrous Plaque then develop impinging lumen
• Plaque – consists of connective scar like tissue, smooth muscle, and fat.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 220
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 221
CADOvertime, build-up of plaque can lead to arterial
occlusion, which can cause a devastating blockage
which will decrease or cut off oxygen to the myocardium
Major risk factors for CAD:
• Smoking
• High blood pressure
• Diabetes
• > 45 years old (men) > 55 years old (women)
• Family history
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 222
Angina Pectoris
• Chest pain related to myocardial ischemia
• May be referred to left shoulder, neck, jaw, or between scapula.
• Anywhere above umbilicus could be anginalpain
• Three types
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 223
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 224
Stable Angina
• Brought on by physical effort or stress
• Usually substernal nonradiating pain
• Last 5 to 15 minutes after stopping stressor
• Subsides completely with treatment
• Sublingual nitrate (nitro)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 225
Unstable Angina• Brought on by same triggers as stable angina
• Occurs more frequently
• Duration greater than 15 mins
• Intensity of pain more severe
• Indication of progression of CAD
• Increased risk for MI
• Less responsive to treatment can require hospitalization with IV nitrates.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 226
Variant Angina
• Occurs at rest- during waking hours
• Not influenced by exertion
• Dysrhythmias occur
• Caused by stenosis and coronary artery spasm
• Treated with Ca Channel Blockers
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 227
Myocardial Infarction (MI)
• Necrosis of a portion of the myocardium
• Characterized by location, size and degree of involvement
• Location-anterior, posterior, lateral, inferior
• Size- large, small
• Transmural (full wall), subepicardial, subendocardial.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 228
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 229
Myocardial Infarction
• Uncomplicated- small infarction, inferior portion of heart partial wall thickness = full recovery
• Complicated MI- one or combination of dysrhythmia, heart failure, thrombosis, damage to heart structure.
• Prognosis is dependent on extent of damage to the ventricles
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 230
Congestive Heart Failure
The inability of the heart to produce adequate cardiac output due to a structural
or functional problem-impairing the ability of the
heart to fill and pump blood adequately
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 231
Risk FactorsCoronary artery disease
• It affects the heart by restricting or blocking the flow of blood
• Strongest risk factor in both men and womenSmoking Hypertension• Preexisting hypertension is present in 75% of heart
failure cases in the United StatesPrevious MIsDiabetes• More in women; associated with a 2-5 fold increase in
heart failureObesityValvular disease
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 232
Other Risk Factors
• Anemia
• Thyroid
• Toxic agents: cocaine, alcohol, nonsteroidal agents
• Albuminuria
• Viruses/Infections
• Allergic reactions
• Blood clots in the lungs
• Dyslipidemia
• Chronic kidney disease
• Sleep-disordered breathing
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 233
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 234
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 235
Valvular Heart Disease
• Congenital or Acquired
• Acquired- bacterial or viral infection of the heart valves
• Common over age of 65
• Some do not require treatment
• Mitral Valve prolapse – common in women vs men
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 236
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 237
Athletic Heart Syndrome
• Cardiovascular adaptation to intense exercise can mimic disease process
• Sudden cardiac death in athletes usually caused by hypertrophy, dysrhythmia or both.
• Can be manifestation of congenital abnormalities in electrical or mechanical function of the heart.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 238
Percutaneous Transluminal Coronary
Angioplasty (PTCA)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 239
• Checks for the presence of
heart disease (such as
coronary artery disease,
valve disease or disease of
the aorta)
• Evaluates the heart muscle
function
• Determines the need for
further treatment
(angioplasty, stent or
bypass surgery)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 240
Cardiac Stents
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 241
Balloon Angioplasty
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 242
Balloon Angioplasty
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 243
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 244
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 245
Sternotomy
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 246
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 247
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 248
Vein Harvest
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 249
Bioprosthetic – These valves come from animals and in order to avoid rejection, they are specially treated with chemicals.
Mechanical – These are valves made of materials such as metal, carbon or synthetics. To prevent blood clots when these types of valves are used, anticoagulation is required.
Biologic – These are valves taken from the human heart of deceased donors. Once the valves are removed from the donor, they are frozen for use at a later date.
Valve
Replacement
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 250
Heart Transplant
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 251
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 252
Ventricular Assistive Devices
• Bridge to Transplant
• Bridge to Recovery
• Destination Device
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 253
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 254
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 255
EKG
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 256
Cardiac Action Potential
• Phase 0- depolarization- Na+ channels open
• Phase 1-prolonged action potential due to slow and extended opening of Ca channels -repolarization begins.
• Phase 2-outward flow of K+ and prolonged opening of Ca lead to a plateau phase
• Phase 3- closure of Ca channels and opening of K channels completes repolarization.
• Phase 4- resting phase Na and Ca are pumper out K is pumped in.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 257
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 258
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 259
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 260
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 261
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 262
EKG
• 12 Lead (view) of the heart
• Six Leads record frontal plane
• Six Leads record transverse plane
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 263
Frontal Plane Leads
• 3 Bipolar limb leads I, II, III
– Single positive and single negative electrode
• 3 augmented unipolar limb leads
– aVR (right arm)
– aVL (left arm)
– aVF (left leg)
Have single positive lead derive negative from a
combination of other electrodes.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 264
Einthoven’s Triangle
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 265
Bipolar Leads
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 266
Augmented Leads
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 267
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 268
Axis Deviation
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 269
Axis Deviation
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 270
Precordial (transverse plane) Leads
• V 1-6
• V1 and V2 look at R
Ventricle
• V3 and V4 look at the
intraventricular septum
• V5 and V6 look at L
Ventricle
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 271
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 272
EKG Evaluation
• What is the rate and pattern (regularity) is R-R
interval equal for each beat?
• Is the a P wave before each QRS? = atrial
• Is the a QRS after every P wave?= conduction
of atria to the ventricles
• P-R interval? Normal= 0.12-0.2 seconds > 0.2
seconds= conduction delay or block
• QRS normal duration (0.1 sec) and shape?
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 273
Calculating Rate
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 274
Calculating Rate
• Count the number of small boxes between
two R waves and divide into 1500.
• Count the number of R waves in a six
second strip and multiply by 10.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 275
Lets try it
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 276
Sinus Rhythms
• Sinus Rhythm- 60-100 bpm
• Sinus Bradycardia- < 60 bpm
• Sinus Tachycardia- > 100 bpm
• These rhythms have normal P waves, PR
int and QRS int
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 277
Supraventricular Dysrhythmias
• Atrial and junctional Mechanisms
– SVT
– Atrial tachycardia
– Atrial Flutter
– Atrial Fibulation
– Junctional Rhythm
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 278
SVT
• Rate- 150-250- regular rhythm- no visible P waves-PR not measurable- QRS .12 or less
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 279
Atrial Tachycardia
• Rate 150-250- regular- 1 P per QRS- PR
may be shorter, QRS .12 or less
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 280
Atrial Flutter
• Atrial rate 250-450- ventricular varies- Atrial is
regular- ventricular can be irregular- P wave-
saw tooth- PR not measurable- QRS <.12.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 281
Atrial Fibrillation• Rate can vary- Irregularly Irregular- P waves chaotic- PR
not measured- QRS <.12.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 282
Junctional Rhythm• Rate- 40-60- regular- P waves inverted-before or after
QRS or absent- PR if present <.12- QRS .12 or less.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 283
Ventricular Dysrhythmias
• Premature Ventricular Contraction (PVC)
– Bigiminy
– Ventricular couplet
– Multifocal PVC (>1 etopic focus)
Ventricular Tachycardia
Ventricular Fibrillation
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 284
PVC
• Rate varies- Can be regular or irregular- P wave
will be absent- unmeasurable PRI- QRS >.12.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 285
Bigiminy
• 1 PVC every other beat- regular-irregular rhythm
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 286
Ventricular Couplet
• PVC occurs twice
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 287
Multi-Focal PVC
• Can be both positive and negative since there
are different etopic origins
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 288
Ventricular Tachycardia
• 3 or more PVC with rate >100 bpm- patient can be
asymptomatic- symptomatic or unconscious and
pulseless.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 289
Ventricular Fibrillation• No organized rhythm- needs immediate defibrillation
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 290
Atrioventricular Blocks
First Degree AV Block
Second Degree AV Block• Mobitz Type 1- Wenckebach
• Mobitz Type 2
Third Degree AV Block
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 291
First Degree Heart Block
• PR interval > .20
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 292
Mobitz Type 1• PR interval progressively get longer than QRS drops
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 293
Mobitz Type 2• Regular dropped QRS every 2nd third or 4th P wave- consistent
PR interval
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 294
Third Degree Heart Block
• No conduction between A and V- both will have regular
rates- Ps can be hidden in QRS
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 295
Story of the AV block Family
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 296
Bundle Branch Blocks• Right Bundle Branch Block RBBB
• Left Bundle Branch Block LBBB
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 297
Left Bundle Branch Block
• Increased QRS >.10s
• Once a widened QRS > 0.10s is identified, we look at leads closest to the LV to identify a LBBB.Leads V5,V6, I, and aVL are in close proximity to the left ventricle, and as such, are the best location to identify a LBBB.
• Characterized by an RSR segment or notched QRS
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 298
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 299 Right Bundle Branch Block
• Look at Right chest Leads V1 and V2
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 300
Myocardial Infarction
• ST segment elevation
• ST segment depression
• Inverted T wave
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 301 ST segment elevation
• Transmural MI
• Use precordial leads to localize
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 302 ST segment depression
• Myocardial ischemia- can be diagnostic
during exercise
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 303 Inverted T wave
• Myocardial ischemia (can be old)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 304
EKG Lab
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 305 1
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 306 2
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 307 3
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 308 4
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 309 5
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 310 6
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 311 7
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 312 8
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 313 9
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 314 10
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 315 11
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 316 12
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 317
Answers• 1- Normal Sinus
Rhythm
• 2- Sinus Bradycardia
• 3-Sinus Tachycardia
• 4- SVT
• 5-A-fib
• 6-Junctional Rhythm
• 7-RBBB
• 8- Mobitz 1 HB
• 9- 3rd deg HB
• 10- STEMI
• 11- LBBB
• 12- V-fib
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 318
Cardiac Rehab
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 319
Cardiac Rehabilitation
Angina
Coronary Artery Disease
Myocardial Infarction
Heart Failure
Coronary Artery Bypass Grafting
Stent or Angioplasty
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 320
Cardiac Rehabilitation
Team Members
Cardiologist
Physical Therapist
Registered Nurse
Dietician
Exercise Physiologist
Psychologist
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 321
Cardiac Rehabilitation
Team Members
Patient
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 322
Cardiac Rehabilitation
Phases
Phase 1- inpatient
Phase 2- Outpatient- Monitored (3
months)
Phase 3 and 4- Outpatient- Unmonitored
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 323
Cardiac Rehabilitation
Phase 1Dietary Guidelines
Smoking Cessation
Activity Instructions
Self Monitoring and warning signs of MI
Medications
Get appointments for phase 2
Stress Management
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 324
Cardiac Rehabilitation
Phase 1
Do not lift pull or push greater than 10 pounds
Avoid overhead reaching
Do not reach behind your back
Avoid Valsalva
Use a rolling walker
Recommended for 6-8 weeks after sternotomy
Sternal Precautions
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 325
Cardiac Rehabilitation
Phase 1
Physical Therapy Evaluation
Early Mobility
Patient Education
Exercise Program
Walking Program
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 326
Cardiac Rehabilitation
Phase 1
Lifting- Limit to 10 pounds
Stair Climbing- Gradually resume- Limit trips at first.
Social Activities- Gradually return as you feel ready.
Walking or Stationary Bike- 7 days/wk- work up to
30 mins- Do not exceed 20 BPM over resting heart
rate.
Activity at Discharge
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 327
Cardiac Rehabilitation
Phase 1
Household Duties- Meal preparation, washing dishes,
light laundry and hobbies such as crafts or modeling
Sexual Activity- Wait 1-2 weeks and resume gradually
Return to Work- depends on type of work- MD must
release you to return to work.
Driving- MD must release the patient to drive.
Activity at Discharge
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 328
Cardiac Rehabilitation
Phase 1
Household/ Yard Duties- shoveling dirt or
snow, mowing the lawn- (even with rider),
vacuuming
Sports and Recreational Activities- No
bowling, golfing, fishing, jogging, swimming or
outdoor biking.
Activity at DischargeDo Not
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 329
Cardiac Rehabilitation
Phase 2
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 330
Cardiac Rehabilitation
Phase 2
Education
Risk Factor Modification
Exercise
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 331
Cardiac Rehabilitation
Phase 2
Meets 1-2 times per week for 1 hour
Heart rhythm, BP and pulse are monitored
Initial exercise prescription is 20-30 BPM above resting HR
progressing to 80% of Max HR.
Patients encouraged to do 30 mins of aerobic exercise on off days.
Resistance activity begins once MD clears sternotomy.
Supervised by Nurse, Exercise Physiologist or Physical Therapist.
Exercise
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 332
Cardiac Rehabilitation
Phase 3 and 4
Some hospitals offer in cardiac rehab
gym or wellness center
Programs at local fitness center
Progress monitored by MD
Patient responsibility
Education in phase 1 and 2 important
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 333
Cardiac Stress Test
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 334
Cardiac Stress Test
The stress test is used to evaluate the heart and
vascular system during exercise.
Is there underlying heart disease that only
becomes apparent when the heart is stressed by
exercise?
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 335
Cardiac Stress Test
The patient is attached to a EKG machine and
BP cuff
Baseline EKG taken
Patient begins low level exercise either walking
on treadmill or stationary bike.
Graded increase every three minutes
At each stage vitals are recorded as well as
patient symptoms
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 336
Cardiac Stress Test
• Maximal Stress Test- activity increased until
the patient cannot keep up any longer
because of fatigue, symptoms occur
(dyspnea, chest pain) or there are EKG
changes.
• Submaximal Stress Test- the patient
exercises only to a pre-determined level.
Usually used with patients with known CAD.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 337
Chemical Stress Test
Combines intravenous medication with an
echocardiogram to evaluate the left ventricle. the
medication takes the place of exercise and the echo
shows decreased movement of an affected wall
Adenosine most common drug
used.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 338
Echocardiogram
Sonography of the
heart- uses
standard ultrasound
to get a two
dimensional view of
the heart.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 339
Transesophageal Echocardiogram
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 340
Ejection Fraction (EF)
Stroke volume = end diastolic
volume - end systolic volume
EF = stroke volume / end
diastolic volume
Normal Left Ventricle EF
values are 50-70%
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 341
Ejection Fraction (EF)
Echocardiogram
Cardiac catheterization
MRI
CT scan
Nuclear Medicine Scan
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 342
Ejection Fraction (EF)
What does this mean the Physical Therapists?
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 343
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 344
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 345
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 346
Cardiac Tamponade
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 347
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 348
Pericardial Effusion
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 349
Cardiac Case
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 350
History
• Patient is a 68 y/o male who presented to ED
complaining of severe shortness of breath and
dyspnea on exertion.
• In ED, patient found to be diaphoretic, in severe
respiratory distress, in atrial fibrillation with rapid
ventricular response, with ventricular rate 140s
bpm, oxygen saturation 78% on room air.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 351
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 352
History Continued
• Left heart catheterization showed severe 3
vessel coronary artery disease
• Coronary Artery Bypass Grafting (CABG) x 5,
• Mitral Valve Repair
• CryoMaze Ablation
• Patient sent to CVICU for recovery, extubated
POD #1, reintubated and sedated soon after for
respiratory distress
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 353
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 354
Typical Open Heart Surgery
• Length of Stay in ICU/Cardiovascular Recovery
~1 day
• Extubated within 4 hours of surgery
• Total Hospital Length of Stay 4-6 days
• Ambulating 4-6 times a day once out of ICU
• Follow up with Surgeon 3-4 weeks as out-patient
• Begin Cardiac Rehab 2-3 weeks
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 355
Open Heart Surgery
Medial Sternotomy
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 356
Open Heart Surgery
CABG MVR
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 357
PT Examination• Performed POD #2
• PLOF – Independent with all functional mobility and ADLs
• On 5 Liters O2, telemetry
• Bed Mobility – Max A for rolling and supine to sit transfer
• Transfers – Min A for sit to stand transfer and Mod A for bed to chair transfer with shuffling gait
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 358
PT 2nd SessionPOD #2- during PT
treatment
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 359
PT 2nd Session
• No specific complaints other than fatigue
• Sternal chest pain
• Increased HR 100 BPM
• No A-fib appreciated
• Diaphoretic
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 360
PT 2nd Session
POD #2- during PT treatment
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 361
As A Result
• Returned for Re-Do of angioplasty
• Extended Length of Stay
• Patient able to return home
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 362
Medical Emergencies
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 363
Medical Emergencies
A
B
C
D
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 364
Medical Emergencies
Airway
Breathing
Circulation
Disability
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 365
Airway Issues
D
O
P
E
Artificial Airway
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 366
Dislodged
Obstruction
Pneumothorax/ Pulmonary Emboli
Equipment Failure
Artificial Airway
Airway Issues
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 367
Less than 8 intubate
Laryngeal edema
Bronchospasm
Anaphylactic Shock
Airway Issues
Non Intubated Patient
Call for Help
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 368
Airway Issues
Non Intubated Patient
Ambu-bag
100% non-rebreather
Nasal Cannula
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 369
Breathing Issues
Tachypnea- pattern- rate
Auscultation
Pain
Chest x-ray
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 370
Circulation Issues
EKG changes
Symptomatic versus Asymptomatic (BP)
Asystole, V-fib, 3rd degree heart block=
CPR
Arrythmias
Sinus Tachycardia/ Sinus Bradycardia
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 371
Circulation Issues
Loss of Peripheral Pulses
PVD
Compartment Syndrome
EKG changes
Check Orthosis
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 372
Circulation Issues
Tachycardia
Environmental
Tone
Autonomic Dysreflexia (hyperreflexia)
Anxiety
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 373
Circulation Issues
Chest Pain
New Onset
Rib/ sternum fractures
Recent CPR
If any doubt get 12 lead
Stop activity!!!!!
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 374
Circulation Issues
Bradycardia
Blood Pressure Stable
Supine to Trendelenburg Position
Level of Consciousness
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 375
Medical Emergencies
Treat the Patient Not the
Monitor
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 376
Physical Therapy Through the
Continuum
Intensive Care
Acute Care
In patient Care- rehab, SNF, ventilator unit.
Outpatient
Home Health
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 377
End of Life Issues
DNR
Health Care Proxy
Living Will
Organ Donation
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 378
Any Questions???
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 379
References
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 380
• Adler, J., & Malone, D. (2012, March). Early Mobilization in the Intensive Care Unit: A Systematic Review. Cardiopulmonary Physical Therapy Journal, 23(1), 5-13.
• Alfirevic, M. A., & Svensson, L. (2012). Transcatheter Aortic Valve Replacement. Anesthesiology Clinics, 355-381.
• American Physical Therapy Association. (2001). Guide to Physical Therapist Practice (2nd ed.). Alexandria: American Physical Therapy Association.
• Anderson, C. M., Overend, T. J., Godwin, J., Sealy, C., & Sunderji, A. (2009). Ambulation after deep vein thrombosis: A systematic review. Physiotherapy Canada, 133-140. doi:10.3138/physio.61.3.133
• Arabi, Y., Haddad, S., Shirawi, N., & Al Shimemeri, A. (2004). Early tracheostomy in intensive care trauma patients improves resource utilization: a cohort study and literature review. Critical Care, 8(5), 347-352.
• Brahmbhatt, N., Murugan, R., & Milbrandt, E. B. (2010). Early Mobilization Improves Functional Outcomes in Critically Ill Patients. Critical Care, 14, 321-323.
• Carrougher, G. J. (1998). Burn Care and Therapy. St. Louis: Mosby.
References
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 381
• Carta, A., Parmigiani, F., Roversi, A., Rossato, R., Milini, C., Parrinello, G., . . .
Porru, S. (2010). Training in safer and healthier patient handling techniques.
British Journal of Nursing, 19(9), 576-582.
• Clark, D. E., Lowman, J. D., Griffin, R. L., Matthews, H. M., & Reiff, D. A. (2013).
Effectiveness of an Early Mobilization Protocol in a Trauma and Burns Intensive
Care Unit: A Retrospective Study. Physical Therapy, 93(2), 186-196.
• Coplin, W. M., Pierson, D. J., Cooley, K. D., Newell, D. W., & Rubenfeld, G. D.
(2000). Implications of extubation delay in brain-injured patients meeting
standard weaning criteria. American Journal of Respiratory and Critical Care
Medicine, 161, 1530-1536.
• Frownfelter, D., & Dean, E. (2012). Cardiovascular and Pulmonary Physical
Therapy Evidence to Practice (5th ed.). St. Louis: Elsevier Mosby.
• Husson, E. C., Ribbers, G. M., Willemse-van Son, A. H., Verhagan, A. P., &
Starn, H. J. (2010). Prognosis of six-month functioning after moderate to severe
traumatic brain injury: a systematic review of prospective cohort studies. Journal
of Rehabilitation Medicine, 42, 425-436. doi:10.2340/16501977-0566
References
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 382
• Jewell, D. V. (2011). Guide to Evidence-Based Physical Therapy Practice
(2nd ed.). Sudbury, Massachusetts: Jones & Bartlett Learning.
• Lang, E. F. (2002). Acute Care Handbook for Physical Therapists. (J. C.
Paz, & M. P. West, Eds.) Boston: Butterworth-Heinemann Publishing
Company.
• Leonard , M. (2010). Patient safety and quality improvement: medical errors
and adverse events. Pediatrics in Review, 31(4), 151-158.
• Lippincott, Williams & Wilkins. (2013). Lippincott's Nursing Procedures (6
ed.). Philadelphia: Lippincott, Williams & Wilkins.
• Malone, D. J. (2006). Physical Therapy in Acute Care: A clinicians guide.
Thorofare, NJ.: SLACK Corporation.
• Manske, B. B. (2011). Clinical Orthopedic Rehabilitation: An Evidence
Based Approach. Philadelphia: Mosby.
• Norton, S. (2004). Complete Decongestive Therapy Course Manual. Norton
School of Lymphatic Therapy.
References
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 383
• Paz, J. C., & West, M. P. (2002). Acute Care Handbook for Physical Therapists (2nd ed.). Boston: Butterworth-Heinemann.
• Ranchos Los Amigos National Rehabilitation Center. (2012). The rancho levels of cognitive functioning. Retrieved from rancho.org: http://www.rancho.org/research/bi_cognitive.pdf
• Rothstein, J. M., Roy, S. H., & Wolf, S. L. (1991). The Rehabilitation Clinical Specialists Handbook. Philadelphia: F.A. Davis Company.
• Stowers , R. (2008). A case study approach to professional development in physical therapy. Corpus Christi: Texas A&M University.
• U.S. Department of Health and Human Services. (2012). Guidelines summery-conditions requiring intracranial pressure monitoring/ extraventricular ventricular or lumbar drainage. Retrieved from National Guideline Clearing House: http://www.guideline.gov
• Watchie, J. (2010). Cardiovascular and Pulmonary Physical Therapy. Philadelphia: Saunders Elsevier.
References
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 384
Thank You
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________