
Cardiopulmonary Effects of Hypercapnia during Controlled ...
Upload
independentCategory
view
0download
0
Cardiopulmonary responses to treadmill and cycleergometry exercise in patients with peripheralvascular diseaseStephen L. Tuner, MBChB, MRCS,a Chris Easton, PhD,a John Wilson,a Dominique S. Byrne, MBChB,FRCS,b Paul Rogers, MBChB, FRCS,b Liam P. Kilduff, PhD,c David B. Kingsmore, MBChB, FRCS,b
and Yannis P. Pitsiladis, PhD,a Glasgow and Swansea, United Kingdom
Background: Peripheral arterial disease (PAD) presenting as intermittent claudication (IC) is routinely assessed as thedistance or time walked to the onset of pain, which often occurs before significant cardiopulmonary stress and is subjectto confounding factors such as increased body mass and altered gait. Thus, where exercise-induced cardiovascular stressis desirable, such as in cardiac stress testing or clinical trials, an alternative modality of exercise is required. Cycling willcircumvent several of the associated problems of treadmill walking and may provide an alternative preferable method ofexercise, although there is limited information on the physiologic response of patients with PAD to cycling. This studycompared the peak cardiorespiratory responses and the repeatability of cycling and treadmill exercise in patients withPAD.Methods: Ten men (mean age, 54 � 10 years) with stable IC completed two incremental exercise tests to the limit oftolerance on a treadmill and a cycle ergometer after familiarization with the outcome measures of exercise duration, workperformed, respiratory gas exchange variables using continuous breath-by-breath measurement, heart rate, and ratings ofperceived pain.Results: Both methods of exercise assessment revealed high reproducibility in terms of absolute claudication time(treadmill, r � 0.95; cycle, r � 0.91), time to volitional fatigue (treadmill, r � 0.96; cycle, r � 0.91), andcardiopulmonary exercise responses such as the lactate threshold (treadmill, r � 0.95; cycle, r � 0.94), peak heart rate(treadmill, r � 0.94; cycle, r � 0.96), and peak oxygen uptake (treadmill, r � 0.98; cycle, r � 0.87). Cycling inducedsignificantly higher cardiopulmonary responses (peak heart rate, peak carbon dioxide output, peak minute ventilation,and respiratory exchange ratio) than treadmill exercise. There was no difference in time to volitional fatigue or in absoluteclaudication time between exercise modalities.Conclusion: These results demonstrate that exercise testing using cycling offers an alternative method of cardiopulmonarytesting for patients with IC that is equally reliable and reproducible to treadmill walking. Cycling may be preferable totreadmill exercise because it induces greater cardiopulmonary and metabolic responses and is better tolerated by patients.
(J Vasc Surg 2008;47:123-30.)Intermittent claudication (IC) is the most commonpresentation of peripheral arterial disease (PAD). It is thesymptom of cramping muscle pain brought on by walkingthat is felt in the lower limb(s), with subsequent exerciseintolerance, and is relieved by rest. The prevalence in themiddle-aged population in the United Kingdom is 5% andis expected to rise dramatically due to an increasingly agedpopulation.1 IC represents the local manifestation of sys-temic arterial disease that is reflected in a poor life expect-ancy, with a mortality rate of 20% to 30% at 5 years and 40%to 72% at 10 years.2 Although IC is the presenting symp-tom, assessment and treatment of a patient with PAD must
From the Institute of Diet, Exercise and Lifestyle (IDEAL), Faculty ofBiomedical and Life Sciences, University of Glasgow, the Department ofSurgery, Gartnavel General Hospital, and the Department of SportsScience, University of Wales.
Competition of interest: none.This research was supported by an unconditional grant from Iovate Health
Sciences Research Inc, Canada.Reprint requests: Dr Yannis P. Pitsiladis, Institute of Diet, Exercise and
Lifestyle (IDEAL), Faculty of Biomedical and Life Sciences, University ofGlasgow, Glasgow G12 8QQ, UK(e-mail: [email protected]).
0741-5214/$34.00Copyright © 2008 by The Society for Vascular Surgery.
doi:10.1016/j.jvs.2007.09.001also incorporate evaluation of cardiopulmonary function tounmask any latent cardiac ischemia. Cardiac stress testing inthis patient population is difficult, however, because walk-ing exercise tests are limited by peripheral pain rather thancardiopulmonary function.
Assessment of severity of IC is usually based on patientself-reporting and quantified by means of ankle-brachialindices. Treatment for IC most commonly focuses onconservative therapy, although the number of percutane-ous transluminal angioplasty procedures has increased ex-ponentially in recent years despite associated risks andlimited success.3 Initial treatment consisting of a programof regular dynamic exercise for at least 2 months has limitedfinancial outlay and has been shown to be as equally effec-tive as percutaneous transluminal angioplasty.4
Despite several clinical trials reporting that structuredexercise programs result in an improvement in walkingdistance in patients with PAD,5,6 the exact mechanismbehind the improvement is unknown. One possibility isthat the improvement in walking distance may reflect directeffects on the peripheral circulation, but it more likelyrepresents other cardiopulmonary adaptations to the car-
diopulmonary system.7123

JOURNAL OF VASCULAR SURGERYJanuary 2008124 Turner et al
Clinical trials designed to quantify the success of thesevarious treatments consistently use treadmill walking as themodality of outcome analysis.8 As discussed previously,however, treadmill-walking performance will be limited byperipheral pain, and thus, any change in cardiopulmonaryfunction resulting from a treatment program may be missedby this modality of testing. The overwhelming use oftreadmill walking as the preferred method of assessmentmay be due to the assumption that treadmill walking sim-ulates the activities of daily living, but it may also be due toa lack of research on the physiologic responses of patientswith PAD to other methods of exercise. Treadmill walkingmay be subject to confounding factors such as musculoskel-etal disease and joint problems, cardiopulmonary disease,gait abnormalities, and increased body mass in addition todaily changes in the subjective assessment of pain. Indeed,Barletta et al9 found a poor correlation between treadmillperformance and quality-of-life scores measured using theMcMaster Health Index.
Cycling could potentially circumvent several of theseconfounding factors, because unlike treadmill walking, thesaddle bears most the subject’s weight, which minimizesthe impact of increased body mass and altered gate onexercise performance. Furthermore, the risk of falling dur-ing cycling exercise is reduced in patients who are extremelyfrail. Clinical trials investigating other cardiovascular dis-eases such as ischemic heart disease have used cycling as themainstay of assessing exercise tolerance where walking isnot well tolerated or desirable.10
To date, only one study has compared the cardiopul-monary responses of patients with IC to cycling and walk-ing,11 reflecting the difficulties in recruiting a stable ho-mogenous population of patients with IC in isolation ofother major disease. This study suggested that cycling andwalking exercise induce a similar level of metabolic andcardiovascular strain. Given the likely unfamiliarity withcycling exercise, however, it is unknown whether cyclingcould provide an appropriate modality of exercise for car-diac stress testing or indeed a repeatable and quantitative
Table I. Exercise-limiting symptoms, ankle-brachialindex, and preferred mode of exercise by subject
Subjects ABI
Primary exercise-limitingsymptom
PreferenceTreadmill Cycle
1 0.75 Left calf/foot Left calf Cycle2 0.80 Right calf Right calf Treadmill3 0.54 Left calf Left calf Cycle4 0.69 Right calf Right calf Cycle5 0.64 Left calf Left calf Cycle6 0.67 Left calf Left calf Cycle7 0.75 Right calf Right knee Cycle8 0.80 Left calf Left calf Cycle9 0.85 Right calf Right calf Treadmill
10 0.71 Right calf Right calf Cycle
ABI, Ankle-brachial index at rest.
measure of success for any particular clinical treatment
where walking assessment is not possible. The aim of thisstudy, therefore, was to compare the repeatability of exer-cise tolerance and maximal cardiopulmonary responses oftreadmill-based exercise with cycle ergometry exercise byusing continuous breath-by-breath measurement for en-hanced discriminating potential.
METHODS
Subjects. Ten men with IC from whom written in-formed consent had been obtained were recruited from thevascular outpatient clinics at Gartnavel General Hospital,Glasgow, Scotland, to participate in the study. The studywas approved by the North Glasgow NHS Trust EthicsCommittee, and all research was performed in accordancewith the Declaration of Helsinki. Each subject had beenseen several times by a consultant vascular surgeon, had ahistory that was in keeping with IC, and had undergone aclinical examination that supported this. Each had a satis-factory full medical examination, including an exercise elec-trocardiogram (ECG), and symptoms that were unchangedfor at least 1 year. In addition, results of static and ambu-latory ankle-brachial index (ABI) measurements of �0.9indicated the presence of occlusive arterial disease. Clinicalhistory and examination indicated that the location ofdisease in all subjects was predominately in the superficialfemoral artery division. Their mean age was 52 � 6 years,and their mean body mass was 74.6 � 13.2 kg.
From 20 subjects initially recruited, 4 were excludedbecause of other exercise-limiting diseases, 3 had ECGchanges on exercising, and 3 had other uncontrolled dis-ease. Patients with diabetes mellitus were not included atthe request of the Ethics Committee as a precaution due totheir relatively poorer outlooks compared with nondiabeticpatients.8 The remaining 10 men in the study cohort hadstable claudication. Their medications included antihyper-tensives in 3, antiplatelet agents in 10, lipid-loweringagents in 9, and �-blockers in 2. All were receiving maximalmedical therapy for atherosclerosis. Eight of the 10 subjectswere ex-cigarette smokers and had ceased smoking �6months before the study, one continued to smoke, and onehad never smoked.
Experimental design. Subjects were familiarized withthe laboratory procedures and testing methodology on atleast two occasions. After familiarization, each patient com-pleted two incremental exercise tests to the limit of toler-ance on a treadmill (T1 and T2) and a cycle (C1 and C2)ergometer, with at least 6 days separating each test. Theorder of initial testing was randomized using computer-generated allocation, and alternated each week thereafter.Subjects fasted for 3 hours before all tests and refrainedfrom alcohol and strenuous exercise for 24 hours beforeexercise testing. The ambient temperature of the laboratorywas maintained at 20°C for all exercise tests.
Exercise protocols. Cycling tests were performed us-ing a ramp-incremental protocol on an electronicallybraked computer-controlled cycle ergometer (ExcaliburSport, Lode, The Netherlands) to limit of tolerance. After 3
minutes of unloaded cycling (actual work rate equal to 10
T2 an
JOURNAL OF VASCULAR SURGERYVolume 47, Number 1 Turner et al 125
W), an incrementation rate of 10 W/min was used until legpain limited further exercise.12 Symptom-limited time tovolitional fatigue was defined as the point at which thepatient could no longer maintain the pedal cadence above40 rpm. This time was withheld from the patient until allexercise tests had been completed.
Treadmill-walking tests were performed on a wide-bodied motorized treadmill (Woodway PPS55 Med, Weilam Rhein, Germany) at a speed of 2 km/h at 0% gradientfor 2 minutes, followed by a speed of 3.2 km/h with anincrease in gradient of 0.5% every 30 seconds. Symptom-limited time to volitional fatigue during treadmill walkingwas defined as the point at which subjects could no longermaintain the preset walking pace.
Perceptual responses. Three time periods were used:the onset of calf pain (initial claudication time, ICT), thetime to maximal pain (absolute claudication time, ACT),and time to volitional fatigue (TF). Previously demon-strated hand signals were used to indicate ICT and ACT.During the recovery period, subjects were asked to describethe primary and secondary exercise-limiting symptoms.Subjects were also required to grade the comparative easeof cycle compared with treadmill exercise at the end of allthe tests.
Cardiopulmonary gas exchange measures. Gas ex-change variables were determined breath-by-breath usingalgorithms.13 Respiratory volumes were measured with abidirectional VMM turbine transducer (Alpha Technolo-gies, Laguna Niguel, Calif), calibrated with a 3-L syringe,using a range of different flow profiles (Hans Rudolph,Kansas City, Mo). Respiratory gas concentrations weremeasured every 20 milliseconds by a QP9000 quadruplemass spectrometer (Morgan Medical, Gillingham, Kent,UK), which was calibrated against precision-analyzed gasmixtures. Peak oxygen uptake (V̇O2 peak) was calculated asthe average of the last 15 seconds of the test.
The lactate threshold (�L) was estimated noninvasivelyas the V̇O2 at which (1) the break-point in the relationshipbetween carbon dioxide (CO2) output (V̇CO2) and V̇O2
Table II. Exercise tolerance and cardiopulmonary respons
Variables
Treadmill test
1
TF (min) 10.0 � 4.7ACT (min) 9.1 � 5.3ICT (min) 3.4 � 0.8V̇O2 peak (L/min) 1.27 � 0.44V̇O2 at �L (L/min)* 1.03 � 0.20V̇CO2 peak (L/min) 1.08 � 0.41V̇E peak (L/min) 41.6 � 18.2HR peak (beats/min) 128 � 29RER peak 0.84 � 0.09
TF, Time to volitional fatigue; ACT, absolute claudication time; ICT, initialoutput; V̇E, minute ventilation; HR, heart rate; RER, respiratory exchange*N � 9 because �L was impossible to identify.†Represents a significant difference between the two modes of exercise (ie,
(“V-slope” technique) occurred and (2) the ventilatory
equivalent for O2 (V̇E/V̇O2) and end-tidal PO2 started toincrease systematically without a concomitant increase inthe ventilatory equivalent for CO2 (V̇E/V̇CO2) and a fallin the end-tidal PCO2 .
14 Heart rate was derived beat-to-beat from the R-R interval of a 12-lead ECG (QuintonMedical, Manchester, UK).
Data analysis. Mean and standard deviation (SD)were calculated for each variable. The Pearson productmoment correlation coefficient (r) was used to compareexercise tests. The limits of agreement (LOA) between thefirst and second exercise tests were investigated by plottingthe individual between-day differences against their respec-tive means (Bland-Altman plots).15 Heteroscedasticity wasexamined by plotting the absolute (positive) differencesagainst the individual means and calculating the correlationcoefficient.16 If the heteroscedasticity correlation was closeto zero and the differences were normally distributed(Shapiro-Wilks test), the mean bias and 95% LOA werecalculated as mean � 1.96 SD of the between methoddifference.17 Paired t tests were used to compare the mea-surements obtained from treadmill and cycle tests. All datawere analyzed using SPSS 11.0 software (SPSS Inc, Chi-cago, Ill). Significance was set a priori at P � .05.
RESULTS
Exercise tolerance. All subjects were primarily limitedby calf pain (Table I). Several subjects reported secondarylimiting symptoms of pain in other areas. A summary of thecardiopulmonary responses for treadmill and cycling exer-cise is presented in Table II for group responses and in Figs1 and 2 for individual responses. No significant differenceswere found in TF within or between modes of exercise(Table II, Fig 1). TF on the two treadmill tests (r � 0.96;P � .001) and the two cycle tests (r � 0.91; P � .001) werehighly correlated. TF was also significantly correlated be-tween modes of exercise but only on the second test (T1 vsC1, r � 0.53, P � .115 and T2 vs C2, r � 0.65, P � .042).Bland-Altman plots for TF for within and between modes
ring treadmill and cycling exercise.
Cycle test
2 1 2
� 5.0 9.3 � 2.4 9.5 � 2.5� 5.4 8.7 � 2.3 8.9 � 2.6� 1.5 5.1 � 2.1 4.7 � 1� 0.36 1.35 � 0.29 1.39 � 0.30� 0.23 0.92 � 0.13 0.92 � 0.12� 0.35† 1.31 � 0.32 1.35 � 0.31†
� 16.5† 54.2 � 16.5 55.2 � 16.1†
� 31† 140 � 30 140 � 25†
� 0.08† 0.96 � 0.1 0.96 � 0.07†
cation time; V̇O2, oxygen uptake; �L, lactate threshold; V̇CO2, carbon dioxide
d C2).
es du
10.610.2
4.31.281.031.0941.81260.84
claudiratio.
of exercise are shown in Fig 3.
JOURNAL OF VASCULAR SURGERYJanuary 2008126 Turner et al
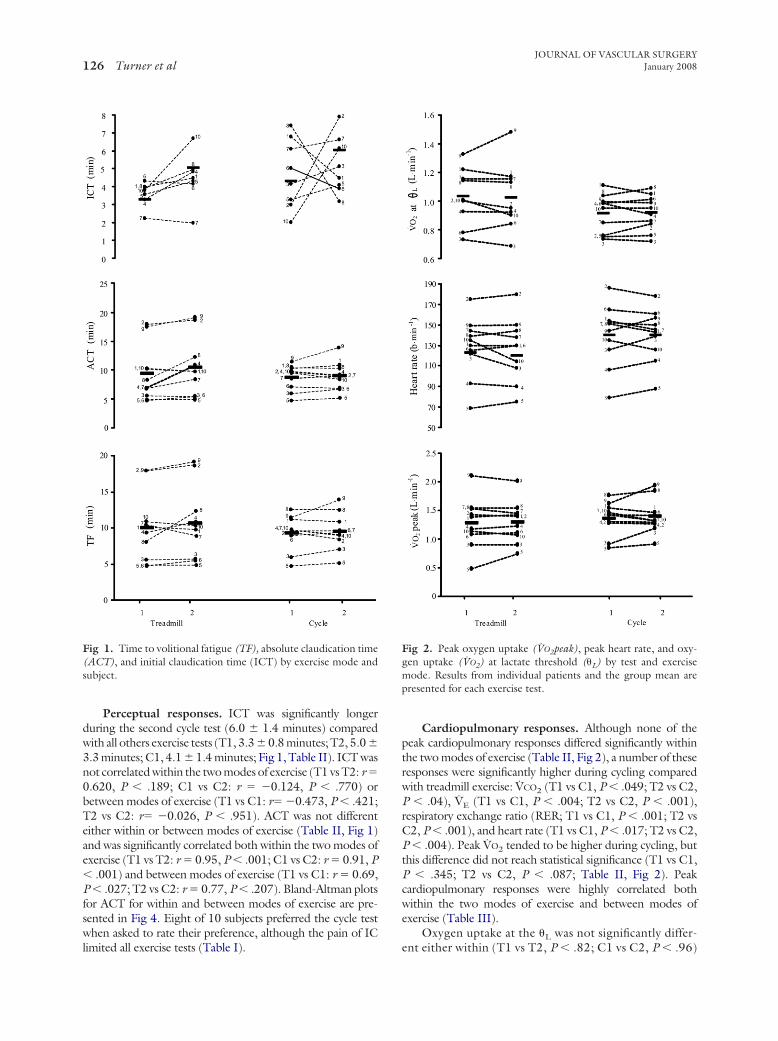
Perceptual responses. ICT was significantly longerduring the second cycle test (6.0 � 1.4 minutes) comparedwith all others exercise tests (T1, 3.3 � 0.8 minutes; T2, 5.0 �3.3 minutes; C1, 4.1 � 1.4 minutes; Fig 1, Table II). ICT wasnot correlated within the two modes of exercise (T1 vs T2: r �0.620, P � .189; C1 vs C2: r � �0.124, P � .770) orbetween modes of exercise (T1 vs C1: r� �0.473, P � .421;T2 vs C2: r� �0.026, P � .951). ACT was not differenteither within or between modes of exercise (Table II, Fig 1)and was significantly correlated both within the two modes ofexercise (T1 vs T2: r � 0.95, P � .001; C1 vs C2: r � 0.91, P� .001) and between modes of exercise (T1 vs C1: r � 0.69,P � .027; T2 vs C2: r � 0.77, P � .207). Bland-Altman plotsfor ACT for within and between modes of exercise are pre-sented in Fig 4. Eight of 10 subjects preferred the cycle testwhen asked to rate their preference, although the pain of IC
Fig 1. Time to volitional fatigue (TF), absolute claudication time(ACT), and initial claudication time (ICT) by exercise mode andsubject.
limited all exercise tests (Table I).
Cardiopulmonary responses. Although none of thepeak cardiopulmonary responses differed significantly withinthe two modes of exercise (Table II, Fig 2), a number of theseresponses were significantly higher during cycling comparedwith treadmill exercise: V̇CO2 (T1 vs C1, P � .049; T2 vs C2,P � .04), V̇E (T1 vs C1, P � .004; T2 vs C2, P � .001),respiratory exchange ratio (RER; T1 vs C1, P � .001; T2 vsC2, P � .001), and heart rate (T1 vs C1, P � .017; T2 vs C2,P � .004). Peak V̇O2 tended to be higher during cycling, butthis difference did not reach statistical significance (T1 vs C1,P � .345; T2 vs C2, P � .087; Table II, Fig 2). Peakcardiopulmonary responses were highly correlated bothwithin the two modes of exercise and between modes ofexercise (Table III).
Oxygen uptake at the �L was not significantly differ-
Fig 2. Peak oxygen uptake (V̇O2peak), peak heart rate, and oxy-gen uptake (V̇O2) at lactate threshold (�L) by test and exercisemode. Results from individual patients and the group mean arepresented for each exercise test.
ent either within (T1 vs T2, P � .82; C1 vs C2, P � .96)

Fig 3. Bland-Altman plot of time to volitional fatigue (TF).
Fig 4. Bland-Altman plot of absolute claudication time (ACT).
JOURNAL OF VASCULAR SURGERYVolume 47, Number 1 Turner et al 127
or between (T1 vs C1, P � .215; T2 vs C2, P � .207) thetwo modes of exercise (Table II, Fig 3). The V̇ O2 at the�L for the two treadmill tests and the two cycle tests werehighly correlated and did not correlate between the twomodes of exercise (Table III). Bland-Altman plots forV̇ O2 PEAK, peak heart rate, and V̇ O 2 at the �L for bothwithin and between modes of exercise are presented inFigs 5 to 7, respectively.
Discussion
The primary finding of this comparative study of stablemen with IC is that using cycling for exercise testing yieldsinformation comparable with treadmill exercise, whethermeasured by traditional subjective measures of pain-limitedexercise tolerance or other more objective physiologic perfor-mance outcome measures such as V̇ O2, V̇ CO2, V̇
E, RER, heartrate, and �L. To our knowledge, however, this study is the firstto show that exercise testing using cycle ergometry incurred asignificantly higher cardiovascular and metabolic responsethan treadmill walking and, paradoxically, was better toleratedby subjects. This may be particularly relevant where the aim isto stress the cardiopulmonary system in patients with ICrather than peripheral musculature, such as during a cardiacstress test or when cardiopulmonary function is assessed be-fore and after a treatment program.
Previous studies of claudication have used a number ofsubjective outcome measures, for example, ICT, ACT, andTF. However, many factors can influence the subjectiveassessment of pain and physical performance with conse-quent potential increased variability and unreliability. Thisis reflected in some studies of treadmill-based exercisetesting that report coefficients of variation of 15% to 40%for claudication distance and maximal walking dis-tance.12,16-18 ICT would appear to be a less reliable mea-sure of walking ability than ACT.19-21 The results of thepresent study support this and suggest that ACT and TF are
Table III. Predicted* maximum oxygen consumption vsmeasured peak oxygen consumption on treadmill andcycle.
Subject Predicted* Treadmill Cycle
1 2.32 1.42 1.462 2.30 1.40 1.263 2.38 0.89 1.184 2.06 1.22 1.295 1.92 0.74 0.916 2.40 1.10 1.417 2.20 1.45 1.328 2.38 1.54 1.849 2.36 2.01 1.94
10 1.92 1.07 1.32Mean (SD) 2.22 1.28† 1.39†
(0.19) (0.36) (0.30)
*Maximum oxygen consumption predicted on basis of age, sex, height, andweight.†Represents a significant difference from predicted maximum oxygen con-sumption,
Treadmill
Cycle
TF (Test 1 + Test 2)/2 (min)
-8
-4
0
4
8
12
200 5 10 15
TF
(T1
- C
1) (
min
)
TF (T1 + C1)/2 (min)
-8
-4
0
4
8
12
200 5 10 15
Mean
Upper
Lower
TF
(T2
- C
2) (
min
)
TF (T2 + C2)/2 (min)
-8
-4
0
4
8
12
200 5 10 15
Mean
Upper
Lower
Mean CycleUpper Cycle
Lower CycleMean Treadmill
Upper Treadmill
Lower Treadmill
TF
(Tes
t 2 -
Tes
t 1)
(min
)
ACT
(Te
st 2
- T
est
1) (
min
)
ACT (Test 1 + Test 2)/2 (min)
-10
-8
-6
-4
-2
0
2
4
6
8
10
4 6 8 10 12 14 16 18 20
AC
T (T
1 - C
1) (
mi n
)
ACT (T1 + C1)/2 (min)
-10
-8
-6
-4
-2
0
2
4
6
8
10
4 6 8 10 12 14 16 18 20
AC
T (T
2 -
C2)
(m
i n)
ACT (T2 + C2)/2 (min)
-10
-8
-6
-4
-2
0
2
4
6
8
10
4 6 8 10 12 14 16 18 20
Treadmill
Cycle
the preferred end points to measure.
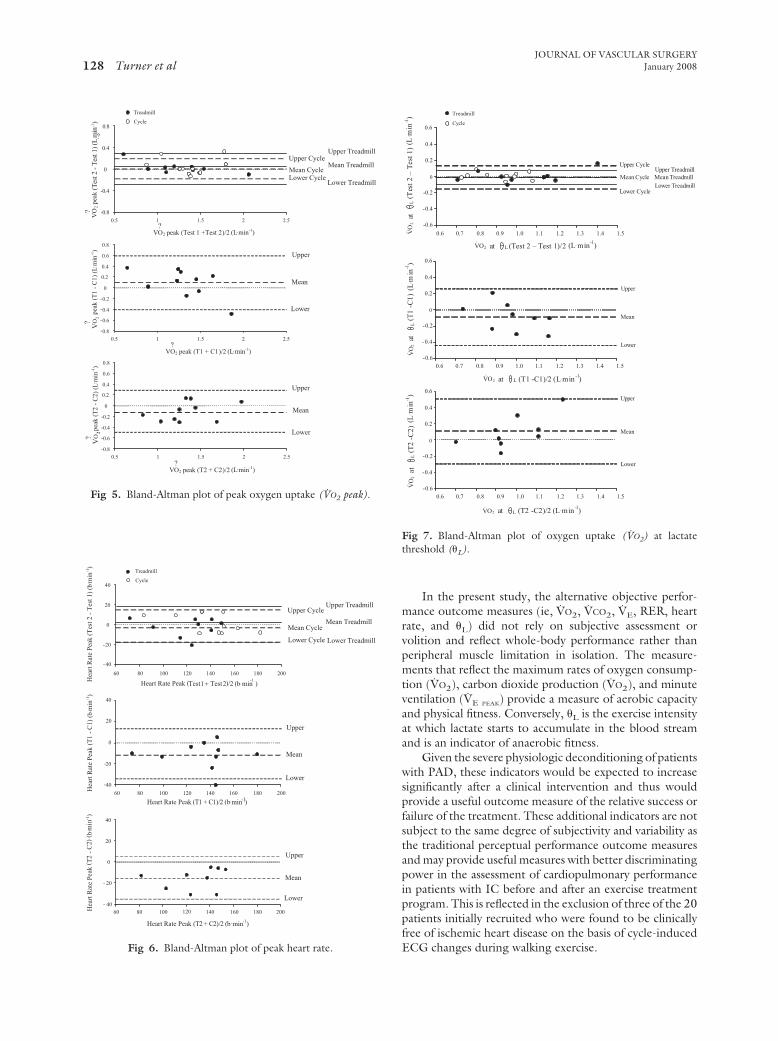
Fig 5. Bland-Altman plot of peak oxygen uptake (V̇O2 peak).
Fig 6. Bland-Altman plot of peak heart rate.
JOURNAL OF VASCULAR SURGERYJanuary 2008128 Turner et al
In the present study, the alternative objective perfor-mance outcome measures (ie, V̇O2, V̇CO2, V̇E, RER, heartrate, and �L) did not rely on subjective assessment orvolition and reflect whole-body performance rather thanperipheral muscle limitation in isolation. The measure-ments that reflect the maximum rates of oxygen consump-tion (V̇O2), carbon dioxide production (V̇O2), and minuteventilation (V̇E PEAK) provide a measure of aerobic capacityand physical fitness. Conversely, �L is the exercise intensityat which lactate starts to accumulate in the blood streamand is an indicator of anaerobic fitness.
Given the severe physiologic deconditioning of patientswith PAD, these indicators would be expected to increasesignificantly after a clinical intervention and thus wouldprovide a useful outcome measure of the relative success orfailure of the treatment. These additional indicators are notsubject to the same degree of subjectivity and variability asthe traditional perceptual performance outcome measuresand may provide useful measures with better discriminatingpower in the assessment of cardiopulmonary performancein patients with IC before and after an exercise treatmentprogram. This is reflected in the exclusion of three of the 20patients initially recruited who were found to be clinicallyfree of ischemic heart disease on the basis of cycle-induced
0
0.2
0.4
0.6
0.6 0.7 0.8 0.9 1.0 1.1 1.2 1.3 1.4 1.5
Treadmill
Cycle
Lat
VO
2
.
(Tes
t2 –
Tes
t1)
(L. m
in-1)
-0.2
-0.4
-0.6
0
0.2
0.4
0.6
-0.2
-0.4
-0.6
0
0.2
0.4
0.6
-0.2
-0.4
-0.6
0.6 0.7 0.8 0.9 1.0 1.1 1.2 1.3 1.4 1.5
0.6 0.7 0.8 0.9 1.0 1.1 1.2 1.3 1.4 1.5
Lat
VO
2
.
(T1
-C1)
(L. m
in-1)
Lat
VO
2
.
(T2
-C2)
(L. m
in-1
)
LatVO2
.
(T2 -C2)/2 (L.min-1)
LatVO2
.
(T1 -C1)/2 (L.min-1)
LatVO2
.
(Test 2 – Test 1)/2 (L.min-1)
Fig 7. Bland-Altman plot of oxygen uptake (V̇O2) at lactatethreshold (�L).
V
0.5 1 1.5 2 2.5
0.8
0.4
0
0.4
0.8
0.5 1 1.5 2 2.5
peak
(T1
-C
1)(L
min
-1)
-0.8
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
0.8
0.5 1 1.5 2 2.5
peak
(T2
-C
2)(L
min
-1)
-0.8
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
0.8
Mean
Upper
Lower
Mean
Upper
Lower
Treadmill
Cycle
Mean Cycle
Upper Cycle
Lower Cycle
Mean Treadmill
Upper Treadmill
Lower Treadmill
?2
O?2
OV
.
.
-
-(Tes
t2-T
est1
)(L
min
)
(Test 1 +Test 2)/2 (L min-1).
?
?VO2 peak
?V
O2
peak
(T1 + C1)/2 (L min-1).
?VO2 peak
(T2 + C2)/2 (L min-1).
?VO2 peak
-1
Treadmill
Cycle
Heart Rate Peak (Test1+ Test 2)/2 (b.min-1
)
60 80 100 120 140 160 180 200
-40
-20
0
20
40
Mean Cycle
Upper Cycle
Lower Cycle
Mean Treadmill
Upper Treadmill
Lower Treadmill
Hea
rtR
ate
Peak
(Tes
t2-
Tes
t1)
(b. m
in-1
)H
eart
Rat
ePe
ak(T
1-
C1)
(b. m
in-1
)
Heart Rate Peak (T1 + C1)/2 (b.min-1)
Mean
Upper
Lower
Hea
rtR
a te
Peak
( T2
-C
2)( b
min
- 1)
Heart Rate Peak (T2 + C2)/2 (b.min-1)
60 80 100 120 140 160 180 200- 40
- 20
0
20
40
Mean
Upper
Lower
-40
-20
0
20
40
60 80 100 120 140 160 180 200
.
ECG changes during walking exercise.

JOURNAL OF VASCULAR SURGERYVolume 47, Number 1 Turner et al 129
A major finding of this study was the successful deter-mination of the �L in all but one patient (Table II). It is wellacknowledged that the determination of the �L is difficult,even by experienced investigators, when the exercise dura-tion is short, as is the case in this patient group. Rates ofV̇O2 at the �L were not different either within or betweenthe two modes of exercise and were highly correlatedwithin modes of exercise but not between modes of exer-cise (Table II, Fig 3). The �L as a measure of musclebioenergetics has been applied with considerable success ina variety of conditions characteristic of moderate to severeexercise intolerance such as chronic obstructive pulmonarydisease (COPD)22,23 and heart failure.24 It also has practi-cal applications and has been used to stratify preoperativecardiac risk.25 In the population of patients with PAD inwhom operative treatment is required, �L ascertained usingcycling exercise testing might provide a valuable method ofoperative risk stratification.
To our knowledge, this study is the first to show thatdespite both modes of exercise inducing similar and predict-able exercise intolerance—the subjective assessment of pain,the work performed and, more important, the determinationof the �L were very closely matched between modes of exer-cise—several peak cardiopulmonary responses other than V̇O2
were higher during cycling compared with treadmill exercise(ie, V̇CO2, V̇E, heart rate, and RER). This observation differsfrom previous studies of healthy adults, athletes, and othersubject groups who report a higher metabolic response duringtreadmill exercise26,27 and a V̇ O2MAX up to 7% higher thancycle exercise.28
The finding of a greater cardiopulmonary and metabolicresponse during cycling exercise in patients with IC in thepresent study is in agreement with an analogous study com-paring cycle and treadmill exercise in patients with severeCOPD.23 These authors found that although peak V̇ O2 didnot differ between the two forms of exercise, postexerciseblood lactate levels were substantially higher after cycle exer-cise than after treadmill exercise (ie, 2.5 vs 1.22 mmol/L).This was attributed to differences in the rates of lactate forma-tion and clearance due to “unfamiliarity” of cycling exercise inpatients with COPD.23 These results suggest that cycle exer-cise may be a more appropriate method of exercise testing inpatients with PAD where the aim is to stress the cardiovascularsystem, such as in cardiac stress testing to unmask any latentcardiac ischemia or when testing the efficacy of a particulartreatment program.
The peak cardiopulmonary responses during both tread-mill walking and cycling in the present group of patients withIC were significantly lower than predicted for patients’ ageand sex, likely due to severe physiologic deconditioning (Ta-ble III). This reduced exercise tolerance is in agreement withprevious studies that found lower peak responses in patientswith PAD compared with healthy controls29 and most likelyreflects the fact that exercise tolerance in this patient group islimited primarily by peripheral rather than central factors. 30
The greater cardiopulmonary and metabolic strain in theabsence of a significantly higher V̇O2 during cycling exercise
may reflect an increased and more localized recruitment ofmore proximal and better-perfused muscles during cycling.Although both modalities were equally well tolerated in termsof similar exercise duration and intensity, they appear to betesting the cardiopulmonary systems to differing degrees.
Eight of the 10 patients preferred the cycle ergometer test(Table I) even though the pain felt and the work performedwas similar between the two methods of testing. One of thetwo patients who preferred the treadmill test reported thighand knee pain in addition to calf pain during cycling, whereaship and back pain were more prevalent during treadmill walk-ing. Cycling may therefore be the preferred mode of exercisewhen greater systemic responses are desired either as a thera-peutic measure (exercise training) or as a method of revealingunderlying cardiopulmonary compromise that would other-wise be latent.
The present study is not without its limitations. A selectgroup of patients were studied; therefore, extrapolating thesefindings to a more generalized population with IC may not bepossible. Although ischemic pain from claudication may man-ifest in the thigh and buttocks, exercise performance in thepresent study was primarily limited by calf pain (Table I).Patients with ischemic pain in different locations may notnecessarily respond in the same manner to the different exer-cise modalities as those in the present study. Strict entrycriteria were chosen to create a homogenous population interms of symptoms and cardiopulmonary and metabolic re-sponses without other disease that could confound the resultsand thus ensure a greater power to detect differences incardiopulmonary responses. This study would require verifi-cation in a larger number of patients with greater severity of ICbefore its practical application to either replace treadmill test-ing or perhaps more interestingly, compare the relative bene-fits of different modes of exercise training.
Conclusion
This study has shown that cardiopulmonary exercisetesting involving cycling exercise offers an alternative modeof testing for patients with IC that is equally reliable andreproducible to treadmill exercise. Of greater interest is thenovel finding of this study that cycling exercise can inducegreater cardiopulmonary and metabolic responses and ingeneral is more acceptable to these patients compared withtreadmill exercise. Cycle exercise may therefore be thepreferred mode of exercise for testing before and after atreatment program in a clinical trial or during a cardiacstress test when the aim is to stress the general cardiovas-cular system. In addition, clinicians and researchers mayprefer the use of cycling as the modality of exercise testingin patients with IC because it is non-weight-bearing andminimizes the risk of falling in frail patients. The potentialbenefits of using cycle exercise as a method of treatment forpatients with IC is out with the remit of the present study.
The cooperation of all patients is greatly appreciated.
AUTHOR CONTRIBUTIONS
Conception and design: ST, CE, JW, DB, PR, DK, YP
Analysis and interpretation: ST, CE, LK, DK, YP
JOURNAL OF VASCULAR SURGERYJanuary 2008130 Turner et al
Data collection: ST, CE, JWWriting the article: ST, CE, DK, YPCritical revision of the article: ST, CE, DB, PR, DK, YPFinal approval of the article: ST, CE, JW, DB, PR, LK, DK,
YPStatistical analysis: ST, CE, LK, YPObtained funding: ST, DB, PR, DK, YPOverall responsibility: YP
REFERENCES
1. Fowkes FG, Housle E, Cawood EH, Macintyre CC, Ruckley CV,Prescott RJ. Edinburgh Artery Study: prevalence of asymptomatic andsymptomatic peripheral arterial disease in the general population. Int JEpidemiol 1991;20:384-92.
2. Taylor LM Jr, Porter JM. Natural history and nonoperative treatment ofchronic lower extremity ischemia. In: Rutherford RB, editor. Vascularsurgery. Vol 1. Philadelphia, PA: WB Saunders Co; 1995. p 751-66.
3. Tunis SR, Bass EB, Steinberg EP. The use of angioplasty, bypasssurgery, and amputation in the management of peripheral vasculardisease. N Engl J Med 1991;325:556-62.
4. Perkins JMT, Collin J, Creasy TS, Fletcher EWL, Morris PJ. Exercisetraining versus angioplasty for stable claudication. Long term andmedium term results of a prospective, randomised trial. Eur J VascEndovasc Surg 1996;11:409-13.
5. Gardner AW, Poehlman ET. Exercise rehabilitation programs for thetreatment of claudication pain. A meta-analysis. JAMA;1995:274:975-80.
6. Robeer GG, Brandsma JW, van den Heuvel SP, Smit B, OostendorpRAB, Wittens CHA. Exercise therapy for intermittent claudication: areview of the quality of randomised clinical trials and evaluation ofpredictive factors. Eur J Vasc Endovasc Surg 1998;15:36-43.
7. Hiatt WR, Wolfel EE, Meier RH, Regensteiner JG. Superiority oftreadmill exercise testing versus strength training for patients withperipheral arterial disease. Implications for the mechanism of the train-ing response. Circulation 1994;90:1866-74.
8. Tan KH, de Cossart L, Edwards PR. Exercise training and peripheralvascular disease. Br J Surg 2000;87:553-62.
9. Barletta G, Perna S. Sabba C, Catalano A, O’Boyle C, Brevetti G.Quality of life in patients with intermittent claudication: relationshipwith laboratory exercise performance. Vasc Med 1996;1:3-7.
10. Hartung GH, Rangel R. Exercise training in post-myocardial infarctionpatients: comparison of results with high risk coronary and post-bypasspatients. Arch Phys Med Rehabil 1981;62:147-50.
11. Askew CD, Green S, Hou XY, Walker PJ. Physiological and symptom-atic responses to cycling and walking in intermittent claudication. ClinPhysiol Funct Imaging 2002;22:348-55.
12. Gardner AW. Peripheral Arterial Disease. In: Exercise Management forPersons with Chronic Diseases and Disabilities. Champaign, IL: Hu-man Kinetics; 1997. p. 64-8.
13. Beaver WL, Wasserman K, Whipp BJ. On-line computer analysis andbreath-by-breath graphical display of exercise function tests. J Appl
Physiol 1973;34:128-32.14. Whipp BJ, Ward SA, Wasserman K. Respiratory markers of the anaero-bic threshold. Adv Cardiol 1986;35:47-64.
15. Bland JM, Altman DG. Statistical methods for assessing agreementbetween two methods of clinical measurement. Lancet 1986;1:307-10.
16. Labs KH, Roessner M, Aschwanden M, Jeanneret C, Gehrig A, JaegerKA. Reproducibility of fixed load treadmill testing. J Vasc Invest 1998;4:55-60.
17. Labs KH, Nehler MR, Roessner M, Jaeger KA, Hiatt WR. Reliabilityof treadmill testing in peripheral arterial disease: a comparison of aconstant load with a graded load treadmill protocol. Vasc Med1999;4:239-46.
18. Perakyla T, Tikkanen H, von Knorring J, Lepantalo M. Poor reproduc-ibility of exercise test in assessment of claudication. Clin Physiol 1998;18:187-93.
19. Gardner AW, Skinner JS, Smith LK. Effects of handrail support onclaudication and haemodynamic responses to single-stage and progres-sive treadmill protocols in peripheral vascular occlusive disease. Am JCardiol 1991;68:99-105.
20. Gardner AW, Skinner JS, Cantwell BW, Smith LK. Progressive vssingle-stage treadmill tests for evaluation of claudication. Med SciSports Exerc 1991;23:402-8.
21. Hiatt WR, Hirsch AT, Regensteiner JG, Brass EP. Clinical trials forclaudication: assessment of exercise performance, functional status,and clinical end points: vascular clinical trialists. Circulation 1995;92:614-21.
22. Cockcroft A, Beaumont A, Adams L, Guz A. Arterial oxygen desatura-tion during treadmill and bicycle exercise in patients with chronicobstructive airways disease. Clin Sci 1985;68:327-32.
23. Mathur RS, Revill SM, Vara DD, Walton R, Morgan MD. Comparisonof peak oxygen consumption during cycle and treadmill exercise insevere chronic obstructive pulmonary disease. Thorax 1995;50:829-33.
24. Van Laethem C, Bartunek J, Goethals M, Nellens P, Andries E, Vander-heyden, M. Oxygen uptake efficiency slope, a new submaximal param-eter in evaluating exercise capacity in chronic heart failure patients. AmHeart J 2005;149:175-80.
25. Older P, Hall A, Hader R. Cardiopulmonary exercise testing as ascreening test for perioperative management of major surgery in theelderly. Chest 1999;116:355-62.
26. Shepherd RJ. Standard tests of aerobic power. In: Frontiers in fitness.Springfiled, IL: Charles C Thomas; 1971. p 319-45.
27. Withers RT, Sherman WM, Miller JM, Costello DL. Specificity ofanaerobic threshold in endurance trained cyclists and runners. EurJ Appl Physiol 1981;47:93-101.
28. Shuey CB Jnr, Pierce AK, Johnson RL Jr. An evaluation of exercise testsin chronic obstructive lung disease. J Appl Physiol 1969;27:256-61.
29. Regensteiner JG, Wolfel EE, Brass EP, Carry MR, Ringel SP, HargartenM, et al. Chronic changes in skeletal muscle histology and function inperipheral arterial disease. Circulation 1993;87:413-21.
30. Pernow B, Saltin B, Wahren R, Cronestrand R, Ekestroom S. Leg bloodflow and muscle metabolism in occlusive arterial disease of the legbefore and after reconstructive surgery. Clinical Science and MolecularMedicine 1975;49:265-75.
Submitted Apr 24, 2007; accepted Sep 3, 2007.
Copyright © 2022 FDOKUMEN




















