11- Peripheral nerve injuries.pdf - KSUMSC
13
Objectives: ● Brachial plexus injuries. ● Peripheral nerve injuries: Axillary, Musculocutaneous, Median and Radial nerves. Resources: ● Davidson’s ● Doctor’s notes Done by: Samar AlOtaibi Sub-leader: Omar Alotaibi Leaders: Abdulrahman Alsayyari & Monerah Alsalouli [ Color index | Important | Notes | Extra ] [ Editing file ]
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of 11- Peripheral nerve injuries.pdf - KSUMSC
Objectives:
● Brachial plexus injuries. ● Peripheral nerve injuries: Axillary, Musculocutaneous, Median and Radial nerves.
Resources: ● Davidson’s
● Doctor’s notes
Done by: Samar AlOtaibi Sub-leader: Omar Alotaibi Leaders: Abdulrahman Alsayyari & Monerah Alsalouli
[ Color index | Important | Notes | Extra ] [ Editing file ]

Introduction: PERIPHERAL NERVE LESIONS: Classified as: “TOM GAIN”
Traumatic cOmpressive Metabolic Genetic Autoimmune Inflammatory Neoplastic
Sunderland Classification of Peripheral Nerve Injury: ● Type 1: Conduction block (neuropraxia) Spared Myelin sheath. ● Type 2: Axonal injury (axonotmesis). ● Type 3: Type 2 + Endoneurium injury. ● Type 4: Type 3 + Perineurium injury. ● Type 5: Type 4 + Epineurium injury (neurotmesis).
The common compressive neuropathies are carpal tunnel syndrome, ulnar nerve compression at the elbow and meralgia paresthetica.
Brachial Plexus Injury: When examining the brachial plexus you don’t examine the nerve, you examine the root (dermatome and myotome)
Anatomy: - Brachial Plexus is formed by the union of anterior rami of 5th,6th,7th,8th cervical and 1st thoracic nerves. - It is divided into Roots, Trunks, Divisions, Cords, and terminal Branches. - Roots are examined by examining dermatomes (sensation) and myotomes (movements).
Root Myotomes (Motor Function) Dermatomes (Sensory Function)
C5 Shoulder abduction + External Rotation Shoulder tip + Lateral arm
C6 Elbow Flexion (biceps muscle) Lateral forearm + Thumb and index finger.
C7 Wrist extension Middle fingers
C8 Making a fist Ring and little finger + Lower medial forearm
T1 Finger crossing intrinsic muscles of the hand (hase 3 groups): 1
1. Thenar >> thumb adduction + opposition (Froment's sign if affected)
2. Hypothenar >> little finger abduction + opposition 3. Interossei: fingers abduction + adduction. 4. Lumbricals: ” لما تأشر “تعال >> MCP flexion +
interphalangeal extension (Claw hand if both 3&4 are affected)
Upper medial forearm + Entire medial arm
1 Intrinsic muscles of the hand are the muscles that originate and insert within the hand, unlike the tendons.
1

Classification of Brachial Plexus Injuries: Open injuries (stab wounds or
gunshot wounds): Closed injuries:
➢ Can be at any evel (roots, trunks, divisions, etc.).
Classified into: ● Supraclavicular (roots, trunks,
divisions). ● Infraclavicular (divisions, cords,
terminal branches).
➢ More common than open injuries. ➢ Injury is most commonly at the
roots level. ➢ Caused by car accidents, outstretching
of the shoulder like when playing sports or during difficult deliveries where the baby is pulled in emergency situations.
Types of closed brachial of plexus injury:
Upper Brachial Plexus Lesion Lower Brachial Plexus Lesion Total Palsy
“Erb-Duchenne Palsy” “Klumpke’s palsy”
Root injured C5, C6, +/- C7
C8 & T1 All roots C5, C6, C7, C8, T1
Sensory exam
(Dermatome)
Loss of sensation over: C5: Shoulder tip + lateral arm. C6: lateral forearm, thumb, index. C7: middle finger.
Loss of sensation over: C8: Ring and little finger + lower medial forearm. T1: Upper medial forearm + medial arm.
Loss of all arm, forearm and
hand sensation
Motor exam (Myotome)
➢ C5: shoulder adduction + internal rotation.
➢ C6: Elbow extension. ➢ C7: Wrist flexion.
➢ C8: cannot make a fist. ➢ T1: cannot cross fingers.
The patient is unable to move entire limb; flail
limb 2
Special sign Waiter’s tip posture. Ape’s Hand (No hands intrinsic muscles > MCP
hyperextension + interphalangeal flexion > Clawing of all fingers)
*for fingers to go into claw both lumbricals and interossei are affected
-
2 Medical Term refers to an extremity in which the primary nerve has been severed, resulting in complete lack of mobility and sensation.
2

Associated injuries
Phrenic nerve injury (C4): Which arises from the 3rd, 4th, and 5th cervical roots, so half of the diaphragm will be paralyzed.
- Adult X-ray: it will show elevated hemidiaphragm.
- In children the intercostals are not strong enough to compensate,so the baby will have breathing problems (obstetric palsy).
Horner Syndrome (T1): Sympathetic nerves come to the face from a branch of the 1st thoracic nerve T1. If T1 is injured a loss of sympathetic supply to the face on one side ”Ipsilateral” lead to Horner’s syndrome:
1. Ptosis (drooping of upper eyelid) 2. Miosis (Constricted pupil). 3. Anhidrosis (inability to sweat).
-
In a pt with Erb’s palsy will he have sensation in his little finger? Yes (C8 intact) How about the index finger? No (C6 injured) Can this pt make a fist? Yes (C8 intact) Will he have a claw hand? No (T1 intact) Shoulder, elbow and wrist are affected Can he develop phrenic nerve injury? Yes (C4 is next to C5) Can he develop horner's syndrome? No T1 النه بعید من
In a pt with Klumpke’s palsy will he have sensation in his thumb? Yes (C6 intact) Can the pt make a fist? No ( no lumbricals nor interossei) Shoulder, elbow and wrist are normal. Can he develop phrenic nerve injury? No Can he develop horner's syndrome? Yes
Can he develop phrenic nerve injury? Yes Can he develop horner's syndrome? Yes
Examples
-
Peripheral nerve Injury: For any nerve injury you have to know 4 things: the cause of injury, sensory, motor loss and special sign
1. Upper limbs:
Axillary nerve injury 3
Course It passes inferiorly and laterally along the posterior wall of the axilla. Then, it passes posteriorly (through a quadrangular space) and passes around the surgical neck of the humerus. ➔ It Supplies: the Deltoid (shoulder abduction) and Teres minor muscle (external rotation) and the skin over it
Cause Shoulder Surgery, shoulder dislocation, trauma.
Sensory exam Loss of sensation over the deltoid and the lateral upper arm.
3 No special sign
3
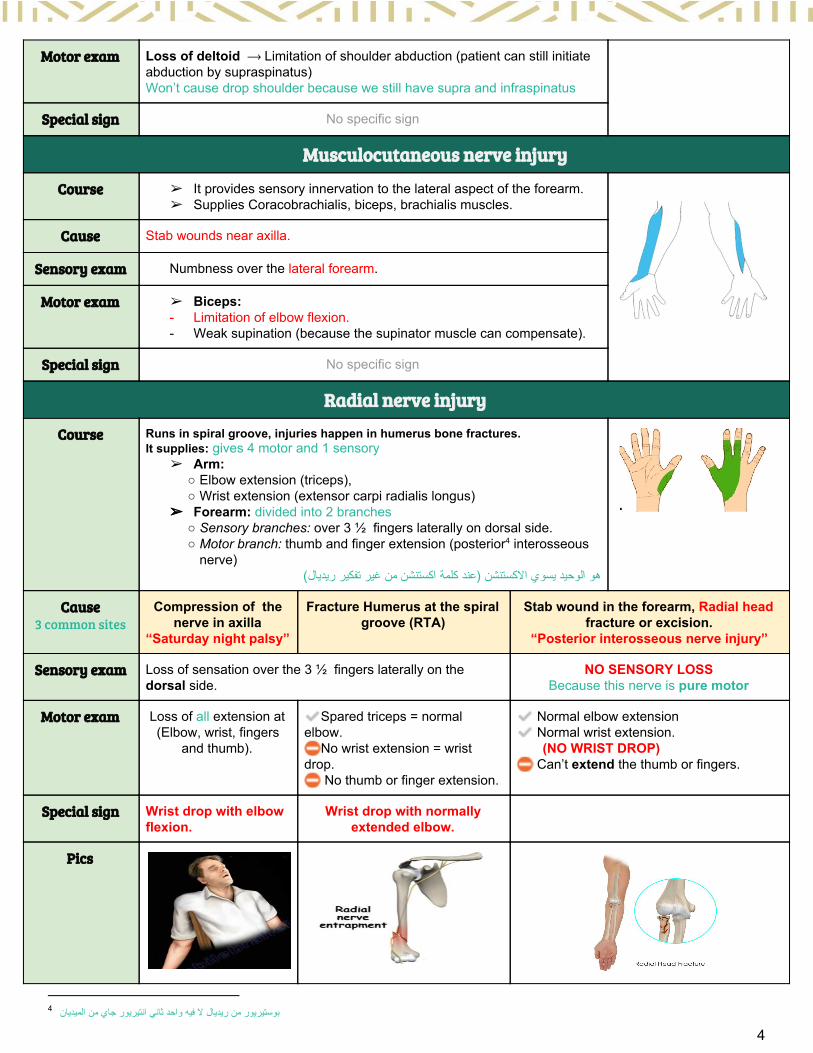
Motor exam Loss of deltoid ⟶ Limitation of shoulder abduction (patient can still initiate abduction by supraspinatus) Won’t cause drop shoulder because we still have supra and infraspinatus
Special sign No specific sign
Musculocutaneous nerve injury
Course ➢ It provides sensory innervation to the lateral aspect of the forearm. ➢ Supplies Coracobrachialis, biceps, brachialis muscles.
Cause Stab wounds near axilla.
Sensory exam Numbness over the lateral forearm.
Motor exam ➢ Biceps: - Limitation of elbow exion. - Weak supination (because the supinator muscle can compensate).
Special sign No specific sign
Radial nerve injury
Course Runs in spiral groove, injuries happen in humerus bone fractures. It supplies: gives 4 motor and 1 sensory
➢ Arm: ○ Elbow extension (triceps), ○ Wrist extension (extensor carpi radialis longus)
➢ Forearm: divided into 2 branches ○ Sensory branches: over 3 ½ ngers laterally on dorsal side. ○ Motor branch: thumb and nger extension (posterior interosseous 4
nerve) هو الوحید یسوي االكستنشن (عند كلمة اكستنشن من غیر تفكیر ریدیال)
Cause 3 common sites
Compression of the nerve in axilla
“Saturday night palsy”
Fracture Humerus at the spiral groove (RTA)
Stab wound in the forearm, Radial head fracture or excision.
“Posterior interosseous nerve injury”
Sensory exam Loss of sensation over the 3 ½ ngers laterally on the dorsal side.
NO SENSORY LOSS Because this nerve is pure motor
Motor exam Loss of all extension at (Elbow, wrist, fingers
and thumb).
ÊSpared triceps = normal elbow. »No wrist extension = wrist drop. » No thumb or nger extension.
Ê Normal elbow extension Ê Normal wrist extension. (NO WRIST DROP) » Can’t extend the thumb or ngers.
Special sign Wrist drop with elbow flexion.
Wrist drop with normally extended elbow.
Pics
بوستیریور من ریدیال ال فیه واحد ثاني انتیریور جاي من المیدیان 4
4

❖Anatomy: Muscle Nerve
Fingers Metacarpophalangeal (MP) joints: ● Extension is by the radial nerve. ● Flexion is by the ulnar nerve by the “Interossei and
Lumbrical” Interphalangeal (IP) joints:
● Extension is by the ulnar nerve by the “Interossei and Lumbrical”
● Flexion is by the long flexors of the forearm.
Hands ● Hypothenar: little finger abduction, opposition.
● Thenar: opposition of thumb + adduction of the thumb (adductor pollicis)
● Interossei: abduction and adduction of the fingers(except for little finger abduction) + MP flexion + IP extension
● Lumbricals: MP flexion+IP extension(anticlaw).
The hand has 20 muscles. ● 15 supplied by the ulnar nerve:
(3 hypothenar + 8 interossei (dorsal and palmar) + 2 lumbricals + adductor pollicis + Palmaris brevis).
● 5 by the median nerve: (3 thenar + 2 lumbricals (1st and 2nd) Basically: All the actions are from the ulnar nerve Except one and half are from the median nerve:
● Opposition of the thumb. ● Index and middle radial lumbricals.
Forearms 5 Superficial muscles: ● Pronator teres → pronation of the
forearm. ● Flexor carpi radialis → wrist flexion. ● Palmaris longus → wrist flexion. ● Flexor carpi ulnaris → wrist flexion. ● Flexor digitorum superficialis → flexion
of the proximal Interphalangeal joints (PIP) so flexes the middle phalynx.
The median nerve has 2 branches.
1) Superficial which supplies all the superficial group muscles EXCEPT Flexor carpi ulnaris (supplied by ulnar nerve)
3 deep muscles: ● Flexor digitorum profundus. ● Flexor pollicis longus. ● Pronator quadratus.
2) Deep (anterior interosseous nerve) which supplies the deep 2 and a half muscles (PURE MOTOR) EXCEPT Half of flexor digitorum profundus to the little and ring finger (supplied by ulnar nerve)
5

The radial nerve supplies the extrinsics (extension), the median & ulnar the flexors (flexion) Always remember: Median nerve is the master of the forearm which supplies all the forearm muscles (superficial and deep) except one and a half (flexor carpi ulnaris & FDP for the little finger) Ulnar nerve is the master of the hand which supplies all the hand muscles except one and a half.
Median nerve injury
Course Motor supply for: Forearm:
➢ Superficial except flexor carpi ulnaris. ➢ Deep flexors except half of flexor digitorum profundus to little and ring finger.
Hand: ➢ Thenar muscles. ➢ Index and middle lumbricals.
Sensory supply for: ➢ Lateral 3 and half fingers on the palmar side.
Injury: Injury to the median nerve Anterior interosseous nerve injury 5
Cause At the wrist level: laceration, carpal tunnel syndrome, suicide.
At the elbow region: Supracondylar fracture of the humerus.
Sensory exam Loss collateral 3½ fingers on the palmar side. NO SENSORY LOSS pure motor
Motor exam - Only loss of thumb opposition and abduction. - The loss of radial 2 lumbricals won’t cause
clawing because interosseous muscles are intact.
Affects the deep 2 and half muscles: ➢ Half of Flexor digitorum profundus of the index. ➢ Flexor pollicis longus of the Thumb. ➢ Pronator quadratus (pronation is not lost
because of pronator teres)
Specific sign No specific sign.
“Can not make a perfect “O” sign” The “O” sign the thumb, index and middle and fingers because he can’t flex the tips of the three fingers (DIP joint: this is the action of the flexor digitorum profundus ms. Of Index)
Ulnar nerve injury
Course Motor Supply For: Forearm:
➢ Flexor carpi ulnaris (superficial) ➢ Medial half of flexor digitorum profundus. (deep)
Hand: ➢ Lumbricals +interossei + hypothenar +adductor pollicis
Sensory supply for: medial 1 and a half fingers front and back of the hand.
5 posterior interosseous comes from the radial (radial nerve supplies the posterior aspect)
6
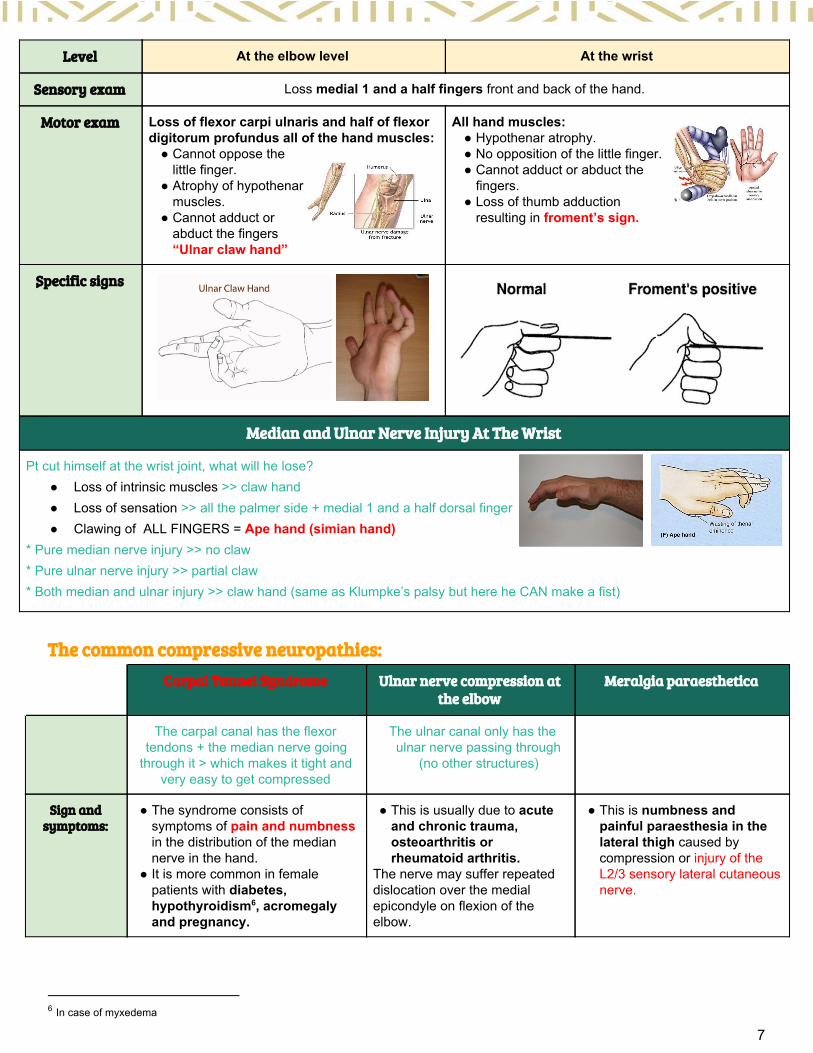
Level At the elbow level At the wrist
Sensory exam Loss medial 1 and a half fingers front and back of the hand.
Motor exam Loss of flexor carpi ulnaris and half of flexor digitorum profundus all of the hand muscles:
● Cannot oppose the little finger.
● Atrophy of hypothenar muscles.
● Cannot adduct or abduct the fingers “Ulnar claw hand”
All hand muscles: ● Hypothenar atrophy. ● No opposition of the little finger. ● Cannot adduct or abduct the
fingers. ● Loss of thumb adduction
resulting in froment’s sign.
Sٍpecific signs
Median and Ulnar Nerve Injury At The Wrist
Pt cut himself at the wrist joint, what will he lose? ● Loss of intrinsic muscles >> claw hand ● Loss of sensation >> all the palmer side + medial 1 and a half dorsal finger ● Clawing of ALL FINGERS = Ape hand (simian hand)
* Pure median nerve injury >> no claw * Pure ulnar nerve injury >> partial claw * Both median and ulnar injury >> claw hand (same as Klumpke’s palsy but here he CAN make a fist)
The common compressive neuropathies:
Carpal Tunnel Syndrome Ulnar nerve compression at the elbow
Meralgia paraesthetica
The carpal canal has the flexor tendons + the median nerve going
through it > which makes it tight and very easy to get compressed
The ulnar canal only has the ulnar nerve passing through
(no other structures)
Sign and symptoms:
● The syndrome consists of symptoms of pain and numbness in the distribution of the median nerve in the hand.
● It is more common in female patients with diabetes, hypothyroidism , acromegaly 6
and pregnancy.
● This is usually due to acute and chronic trauma, osteoarthritis or rheumatoid arthritis.
The nerve may suffer repeated dislocation over the medial epicondyle on flexion of the elbow.
● This is numbness and painful paraesthesia in the lateral thigh caused by compression or injury of the L2/3 sensory lateral cutaneous nerve.
6 In case of myxedema
7

● Symptoms may be intermittent, are usually worse at night , and may 7
be relieved by shaking the hand. ● The symptoms are often provoked
by wrist flexion. On examination, there are usually no signs. Occasionally, there may be wasting of the thenar eminence, weakness of the abductor pollicis brevis, and diminished or altered sensation in the median nerve distribution. ➢ (Tinel’s Sign): Tapping over the nerve
in the carpal tunnel may elicit paraesthesia in the median nerve distribution.
➢ (Phalen’s test): involves acutely flexing the wrist and holding it in this position. This may precipitate paraesthesia or numbness, and this is abnormal if it occurs within 1 minute.
Sometimes, the nerve may be compressed by the aponeurosis between the two heads of flexor carpi ulnaris. ● There is pain in the forearm
and wasting of the small muscles of the hand, leading in the worst cases to an ulnar ‘claw’ hand.
● There may be reduced sensation in the ulnar distribution of the hand.
The nerve emerges from the lateral border of the psoas muscle just above the iliac crest and crosses the iliacus to pass beneath or through the inguinal ligament, 1 cm medial to the anterior superior iliac spine, to pass into the thigh. ● Seat belts, pregnancy, trauma
and postsurgical scar tissue, to name but a few, can cause mechanical compression.
● Diabetes is present in up to 10% of cases.
Diagnosis Electrophysiology to measure nerve conduction velocity and distal motor latency.
Can be made clinically but we need Electrophysiology to confirm it.
Injecting local anaesthetic into the inguinal region 1 cm medial to the anterior superior iliac spine.
Treatment Depends on the severity of the symptoms.
- Splinting the wrist or injections of steroid into the carpal tunnel provide relief in a third of cases.
- If this fails, the transverse carpal ligament can be divided surgically, and in many cases this can be performed as a day case under local anaesthetic.
Treatment consists of surgically releasing and decompressing the nerve.
Treatment includes weight loss, the removal of constricting clothes and belts, NSAIDS, ice packs and injections of corticosteroid. Most cases will settle within 2 years.
- Surgical decompression is reserved for those that do not.
7in fetal position (flexed knee, back. Elbow and wrist) which will increase the pressure یشكي المریض انه یصحى من نومه بالم بیده وتنمیل,لیش؟ الن المریض وهو نایم یكون phalen's test كانه یسوي
8

2. Lower limbs: Lower limb has 2 main nerves:
● Anterior femoral nerve which supplies the quadriceps >> knee extension ● Sciatic nerve which supply the hamstring >> knee flexions, then branches to 2 nerves:
○ Common peroneal >> dorsiflexion (ankle and toe extension) ○ Posterior tibial >> plantar flexion (ankle and toe flexion)
Femoral nerve injury (Front)
Nerve roots L1 - L4
Course - Descends lateral to psoas major enters the thigh behind the inguinal ligament Passes lateral to femoral artery and divides into terminal branches.
- The first cutaneous branches of the femoral nerve are the anterior cutaneous branches that arise in the femoral triangle. They supply the skin on the anteromedial thigh.
- The last cutaneous branch of the femoral nerve is the saphenous nerve which supplied the skin on the medial side of the leg and the foot.
Sensory exam Sensation of anterior thigh and inner thigh.
Motor exam It supplies the quadriceps muscles "knee extension"
Notes If injured: he can't extend his knee and when can't extend it, he cannott walk. (More important than knee flexion, we need to extend our knee to be able to stand and walk.
● Femoral nerve injury is related to psoas muscle, so in case of psoas abscess, we may cut the nerve while draining the pus.
Sciatic nerve injury (Back)
Nerve roots L4 - S3
Motor exam Supplying hamstrings “Knee flexion”
Notes It is very commonly injured in two cases: 1. Hip arthroplasty. 2. Injections (When we are injecting we should direct the needle away from
sciatic nerve, in upper outer part of the ) If injured: the hamstring will be affected, so there will not be knee flexion. مصیبه إذا انجرح ما یقدر المریض یمشيAfter supplying the hamstring, it will be divided into two parts:
➢ Posterior tibial nerve. ➢ Common peroneal nerve.
Branches: Posterior tibial nerve injury Common fibular (Peroneal) nerve injury
Nerve roots L4 - S3
Course Descends through popliteal fossa to posterior compartment of leg, accompanied with posterior tibial vessels Passes deep to exor
Leaves the popliteal fossa & turn around the lateral aspect of the neck of fibula. Then divides into:
9

retinaculum to reach the sole of foot where it divides into 2 terminal branches.
● Superficial perotneal: descends into lateral compartment of the leg.
● Deep perotneal: descends into anterior compartment of the leg.
Sensory exam Sensation of the sole of the foot. Sensation of the dorsum of the foot.
Motor exam Innervate the posterior leg compartment, which it is responsible for ankle flexion (plantar flexion), toe flexion.
It supplies the anterior and the lateral compartment of the legs. Which is responsible for ankle extension and toe extension.
Notes Laceration in the popliteal fossa will only injure the posterior tibial nerve. “Rarely injured” causing loss of foot flexion.
● The lateral leg compartment: causes foot to Evert. ● Anterior compartment: is responsible for ankle
extension and toe extension (Dorsiflexion) ● It is the most common injury of the nerve in the
lower limb. Why? It is very superficial at the fibular head. So, any injury there, will affect the nerve, including sitting in abnormal position when you do this you stretch the nerve. If injured: Drop foot, no ankle extension and no toe extension and also loss of dorsum sensation.
Treatment: غیر مطالبین فیه If the nerve is compressed (e.g. carpal tunnel syndrome) >> relief the compression. If the nerve is cut first 3 weeks >> repair it.
and any یبي له على ما یوصل للدلتوید 6 شهور ولالصابع كامله سنتین Brachial Plexusالمشكله النرف یطول 1مل بالیوم, مثال لو صلحنا ال Brachialفحتى لو صلحنا ال muscle stays denervated for a year and a half will get atrophied and won't work again
Plexus لالصابع ما بتتحرك بس االحساس بیرجع!If the nerve is cut more than 3 weeks >> we cut the endings to make a new cut and reattach it واذا كان النرف قصیر ناخذ عصب من اي مكان ونوصله
10

Summary:
Nerve Lesion
Upper brachial plexus “Erb’s Duchenne” Waiter's tip + Phrenic nerve injury
Lower brachial plexus “Klumpke’s palsy” Ape’s hand + Horner syndrome
Axillary Loss of deltoid
Mucocutaneous No elbow flexion
Radial (Saturday night) Wrist drop + elbow flexion
Radial (Humerus fracture) Wrist drop + Normal elbow extension
Median (Ant. Interosseous) Can't make O sign
Ulnar (at elbow) Claw hand
Ulnar (at wrist) Froment's sign
Median + Ulnar (At wrist) Ape’s hand
Femoral Can't extend knees
Sciatic Can't flex knees
Common peroneal Foot drop
Recall :
How can the flexor digitorum profundus (FDP) apparatus be tested? Check isolated flexion of the middle finger DIP joint. How can the flexor digitorum superficialis (FDS) apparatus be tested? Check isolated flexion of the finger at the MP joint. What are the “intrinsic” hand muscles? Lumbricals, interosseous muscle. What is ADDuction and ABDuction of the fingers? ADDuction is to midline and ABDuction is separation from midline. What will common peroneal nerve injury cause? Drop foot, no ankle extension and no toe extension and also loss of dorsum sensa on. What is the problem of femoral nerve injury? Loss of knee extension and loss of sensa on of anterior and inner thigh. Sciatic nerve injury cause? Loss of Knee flexion (hamstring) and both nerves common peroneal and posterior bia. What is the problem with posterior tibial nerve injury? Loss of ankle flexion (plantar flexion), toe flexion and also loss of sensa on of sole of the foot. Drop wrist (radial nerve), and drop foot (common peroneal).
11

1) pt with Supracondylar fracture upon examination:Sensory of the upper limb was completely normal, motor examination was also normal except lack of tip of the thumb flexion and DIP joint of the middle and index finger, which of the following nerve is affected? سؤال الدكتور بالمحاضرة
A. Anterior interosseous B. Posterior interosseous C. Axillary D. Musculocutaneous
2) pt with stab wound near the axilla, examination showed completely normal upper limb except for lack of elbow flexion and numbness of the lateral forearm, which of the following nerve is affected? سؤال الدكتور بالمحاضرة
A. Anterior interosseous B. Posterior interosseous C. Axillary D. Musculocutaneous
3) pt hand a shoulder dislocation, after relocating it examination of the upper limb showed completely normal exam except limitation of shoulder abduction and numbness over the upper lateral arm, which of the following nerve is affected? سؤال الدكتور بالمحاضرة
A. Anterior interosseous B. Posterior interosseous C. Axillary D. Musculocutaneous
4) A woman fell down the stairs and broke her radial head presented with numbness on hand and motor deficits. Which of the following movements is lost?
A. Wrist flexion B. Wrist extension C. Thumb flexion D. Thumb extension
5) A 23 y/o with glass injury of the wrist which caused transection of the medial nerve. on hand examination which movement will be affected?
A. Inability to flex middle finger, index and thumb B. Clawing of index and middle finger C. Inability to adduct the thumb D. Inability to abduct the thumb
6) Which of the following is a clinical feature of carpal tunnel syndrome?
A. Weak wrist flexion B. Numbness of the radial 1.5 fingers C. Numbness of the dorsal 3.5 radial fingers D. Numbness of the volar 3.5 radial fingers
7) What is the dermatome of root C7?
A. Thumb B. Index C. Middle finger D. Ring finger
8) Patient with positive froment’s sign, lesion is in:
A. Ulnar B. Median C. Radial
Answers: 1- A 2- D 3- C 4- D 5- D 6- D 7- C 8- A
12