
Excision of an asymptomatic cervical intradural neurenteric cyst through the anterior approach: a...
8
Excision of an asymptomatic cervical intradural neurenteric cyst through the anterior approach: a study of two cases and a review of the literature Mehdi Sasani, MD a, * , A. Fahir Ozer, MD a , B. Tunc Oktenoglu, MD a , Kamil Peker, MD b , M. Hakan Bozkus, MD a , Ali Cetin Sarioglu, MD a a Department of Neurosurgery, American Hospital, Guzelbahce Sk. No: 20, 34365 Istanbul, Turkey b Istanbul Pathology Center, Valikonagi Cd. No: 125/2 Nisantasi, 34365 Istanbul, Turkey Received 4 November 2006; accepted 18 December 2006 Abstract BACKGROUND: Spinal neurenteric cysts are very rare lesions, especially after the second decade of life. They account for 0.3% to 0.5% of all spinal tumors and occur most commonly in ventral locations. The cysts are usually removed via a posterior approach. PURPOSE: To present the clinical and radiologic results of patients with spinal neurenteric cysts who were treated via anterior approach procedures. STUDY DESIGN: This report is composed of two cervical neurenteric cyst cases that are com- pared with published studies. METHODS: We present two patients, 41- and 39-year-old women, each with a cervical intradural neurenteric cyst. Both of these patients had apparent neck pain without neurological deficit. MRI revealed neurenteric cysts located at C7 and C7–T1 levels. After anterior corpectomy, the intradural cysts were removed, and then fusion was performed. RESULTS: The postoperative period went well. The follow-up cervical MRI studies were per- formed at 3, 6, and 18 months postoperatively, and there were no abnormalities found. CONCLUSIONS: This study has led to the conclusion that although neurenteric cysts are rare in adults, they can still be present with only persistent neck pain and without neurological deficits. This may lead to misdiagnosis. The importance of MRI is not controversial in the early diagnosis. An anterior approach may be considered the first preference for surgical technique in patients with ventrally located neurenteric cysts. Ó 2007 Elsevier Inc. All rights reserved. Keywords: Neurenteric cyst; Cervical intradural extramedullary mass; Anterior cervical corpectomy; Cervical intradural cyst; Cervical anterior approach; Anterior cervical fusion Introduction Spinal neurenteric cysts are very rare lesions. They represent approximately 0.7% of tumors and 16% of cysts in the central nervous system and 0.3% to 0.5% of spinal tumors [1,2]. Most of these lesions have an extramedullary intradural location and rarely arise intramedullarily [3–9]. The pathogenesis of neurenteric cysts of the spinal cord is unclear, although the neurenteric cysts pathogenesis has been suggested to be congenital in origin [10–12]. Neuren- teric cysts may occur as a result of the failure of notochord formation. [13,14]. These lesions are derived from dis- placed endodermal tissue. Neurenteric cysts are occasion- ally symptomatic, with neck pain and constriction of head movement being prominent symptoms. They are usually di- agnosed in childhood and puberty [15]. Although the pos- terior approach is the usual surgical technique for the treatment of this disease, the anterior approach and lateral approach have been described by some authors [16–19]. In this study, we present a report of two adult patients with asymptomatic neurenteric cysts that were removed via an anterior approach with a favorable outcome. FDA device/drug status: approved for this indication (cervical anterior plate and screw, Totoplast Crista iliaca allograft bone). Nothing of value received from a commercial entity related to this manuscript. * Corresponding author. Department of Neurosurgery, American Hos- pital, Guzelbahce Sk. No: 20, 34365 Nisantasi, _ Istanbul, Turkey. E-mail address: [email protected] (M. Sasani) 1529-9430/07/$ – see front matter Ó 2007 Elsevier Inc. All rights reserved. doi:10.1016/j.spinee.2006.12.010 The Spine Journal 7 (2007) 720–727
Transcript of Excision of an asymptomatic cervical intradural neurenteric cyst through the anterior approach: a...

The Spine Journal 7 (2007) 720–727
Excision of an asymptomatic cervical intraduralneurenteric cyst through the anterior approach: a study
of two cases and a review of the literature
Mehdi Sasani, MDa,*, A. Fahir Ozer, MDa, B. Tunc Oktenoglu, MDa,Kamil Peker, MDb, M. Hakan Bozkus, MDa, Ali Cetin Sarioglu, MDa
aDepartment of Neurosurgery, American Hospital, Guzelbahce Sk. No: 20, 34365 Istanbul, TurkeybIstanbul Pathology Center, Valikonagi Cd. No: 125/2 Nisantasi, 34365 Istanbul, Turkey
Received 4 November 2006; accepted 18 December 2006
Abstract BACKGROUND: Spinal neurenteric cysts are very rare lesions, especially after the second decadeof life. They account for 0.3% to 0.5% of all spinal tumors and occur most commonly in ventrallocations. The cysts are usually removed via a posterior approach.PURPOSE: To present the clinical and radiologic results of patients with spinal neurenteric cystswho were treated via anterior approach procedures.STUDY DESIGN: This report is composed of two cervical neurenteric cyst cases that are com-pared with published studies.METHODS: We present two patients, 41- and 39-year-old women, each with a cervical intraduralneurenteric cyst. Both of these patients had apparent neck pain without neurological deficit. MRIrevealed neurenteric cysts located at C7 and C7–T1 levels. After anterior corpectomy, the intraduralcysts were removed, and then fusion was performed.RESULTS: The postoperative period went well. The follow-up cervical MRI studies were per-formed at 3, 6, and 18 months postoperatively, and there were no abnormalities found.CONCLUSIONS: This study has led to the conclusion that although neurenteric cysts are rare inadults, they can still be present with only persistent neck pain and without neurological deficits.This may lead to misdiagnosis. The importance of MRI is not controversial in the early diagnosis.An anterior approach may be considered the first preference for surgical technique in patients withventrally located neurenteric cysts. � 2007 Elsevier Inc. All rights reserved.
Keywords: Neurenteric cyst; Cervical intradural extramedullary mass; Anterior cervical corpectomy; Cervical intradural
cyst; Cervical anterior approach; Anterior cervical fusion
Introduction
Spinal neurenteric cysts are very rare lesions. Theyrepresent approximately 0.7% of tumors and 16% of cystsin the central nervous system and 0.3% to 0.5% of spinaltumors [1,2]. Most of these lesions have an extramedullaryintradural location and rarely arise intramedullarily [3–9].
FDA device/drug status: approved for this indication (cervical anterior
plate and screw, Totoplast Crista iliaca allograft bone).
Nothing of value received from a commercial entity related to this
manuscript.
* Corresponding author. Department of Neurosurgery, American Hos-
pital, Guzelbahce Sk. No: 20, 34365 Nisantasi, _Istanbul, Turkey.
E-mail address: [email protected] (M. Sasani)
1529-9430/07/$ – see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.spinee.2006.12.010
The pathogenesis of neurenteric cysts of the spinal cordis unclear, although the neurenteric cysts pathogenesis hasbeen suggested to be congenital in origin [10–12]. Neuren-teric cysts may occur as a result of the failure of notochordformation. [13,14]. These lesions are derived from dis-placed endodermal tissue. Neurenteric cysts are occasion-ally symptomatic, with neck pain and constriction of headmovement being prominent symptoms. They are usually di-agnosed in childhood and puberty [15]. Although the pos-terior approach is the usual surgical technique for thetreatment of this disease, the anterior approach and lateralapproach have been described by some authors [16–19].In this study, we present a report of two adult patients withasymptomatic neurenteric cysts that were removed via ananterior approach with a favorable outcome.
721M. Sasani et al. / The Spine Journal 7 (2007) 720–727
Case reports
Case 1
A 41-year-old female patient was admitted with the com-plaint of slight neck pain for 9 months. Her past medical
history revealed that she had been treated for cervical degen-erative disc disease for 6 months and had been referred to thepsychiatric department with a diagnosis of psychosomaticdisorder. She had been given antidepressants for 3 months(amitriptiline 1�10 mg and a specific serotonin reuptakeinhibitor, paroxetine 1�40 mg).
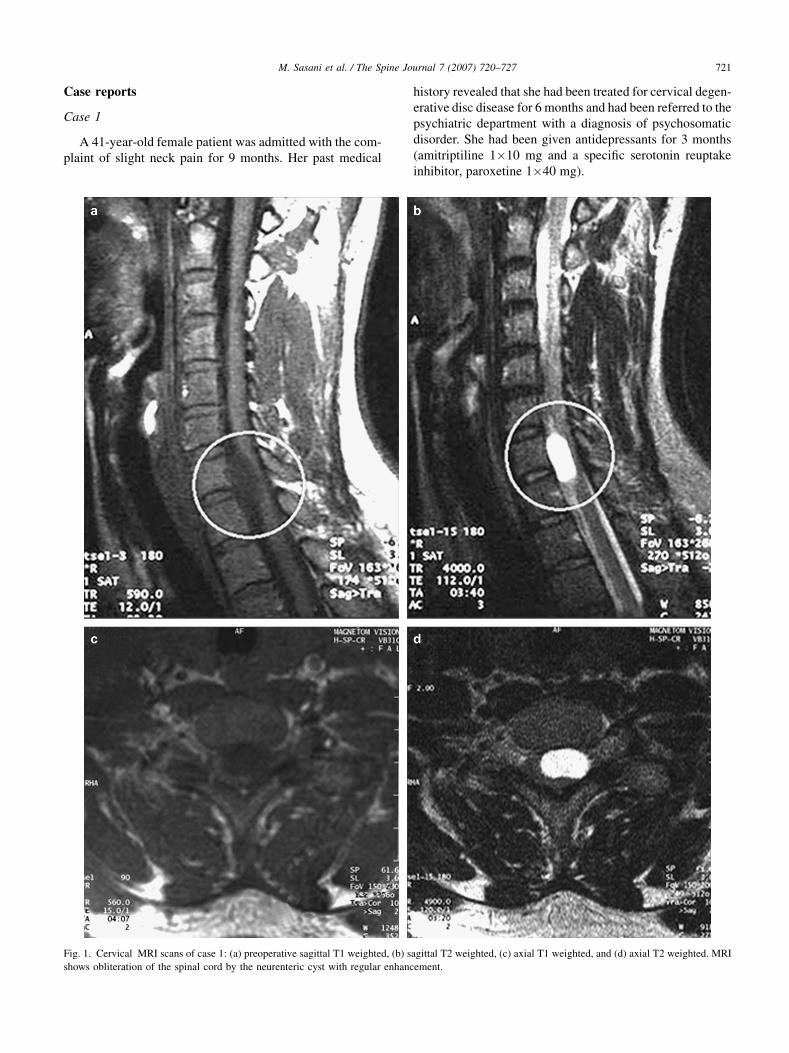
Fig. 1. Cervical MRI scans of case 1: (a) preoperative sagittal T1 weighted, (b) sagittal T2 weighted, (c) axial T1 weighted, and (d) axial T2 weighted. MRI
shows obliteration of the spinal cord by the neurenteric cyst with regular enhancement.

722 M. Sasani et al. / The Spine Journal 7 (2007) 720–727
The neurological examination revealed no motor deficitor sensorial disorders, and there was only moderately con-striction of head movement in flexion and extension.Magnetic resonance imaging (MRI) of the cervical spinerevealed the presence of an anterior intradural extramedul-lary cystic lesion behind the C7 vertebral body. The cystwas hyperintense compared with cerebrospinal fluid onT1-weighted MRI and slightly hypointense on proton den-sity and T2-weighted sequences (Fig. 1). Cranial, thoracic,and lumbar MRI showed no pathological evidence.
Discectomies and C7 corpectomy were performed withvisualization via a surgical microscope. The dura was tight,expulsed, and without pulsation. A vertical small incisionwas made on the dura mater. The cystic lesion was ob-served to be attached to the ventral aspect of the spinalcord. Total resection was performed without tearing ofthe cyst membrane. The dura was stitched with a single su-ture (4-0 absorbable vicryl). The dural surface was rein-forced with artificial dura mater (duragen) and a piece offree fat tissue. Finally, artificial bone graft and anterior in-strumentation were performed. The cyst measured 25 mmin length and 10 mm in width (Fig. 2). The cystic contentwas mucoid in nature.
The histologic sections of the cyst wall showed a cysticlesion lined by a cuboidal to columnar epithelium contain-ing mucus resembling intestinal epithelium. No epithelialatypia was noted. The wall of the cyst was thin and edem-atous (Fig. 3).
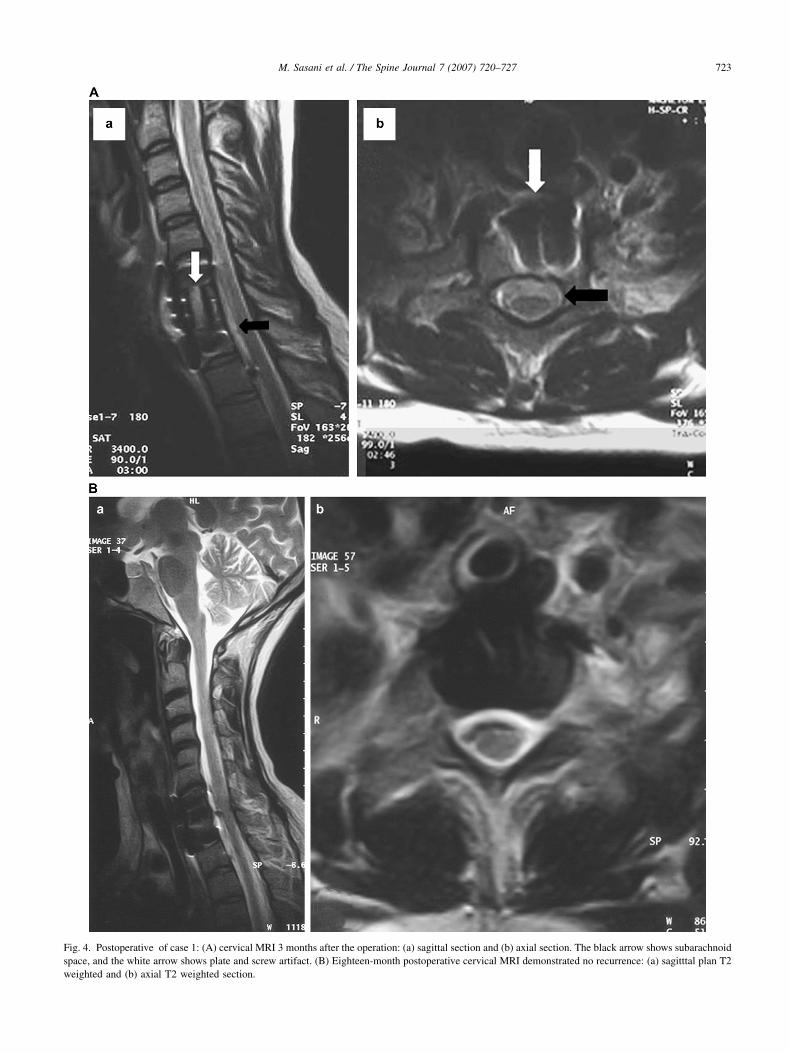
The patient’s neck pain disappeared postoperatively. Shewas discharged in good condition on the third postoperativeday. The follow-up MRI studies were performed in postop-erative months 3, 6, and 18. No residual lesion or recur-rence of the lesion was observed (Fig. 4).
Fig. 2. The neurenteric cyst was totally removed and measures 25 mm in
length and 10 mm in width.
Case 2
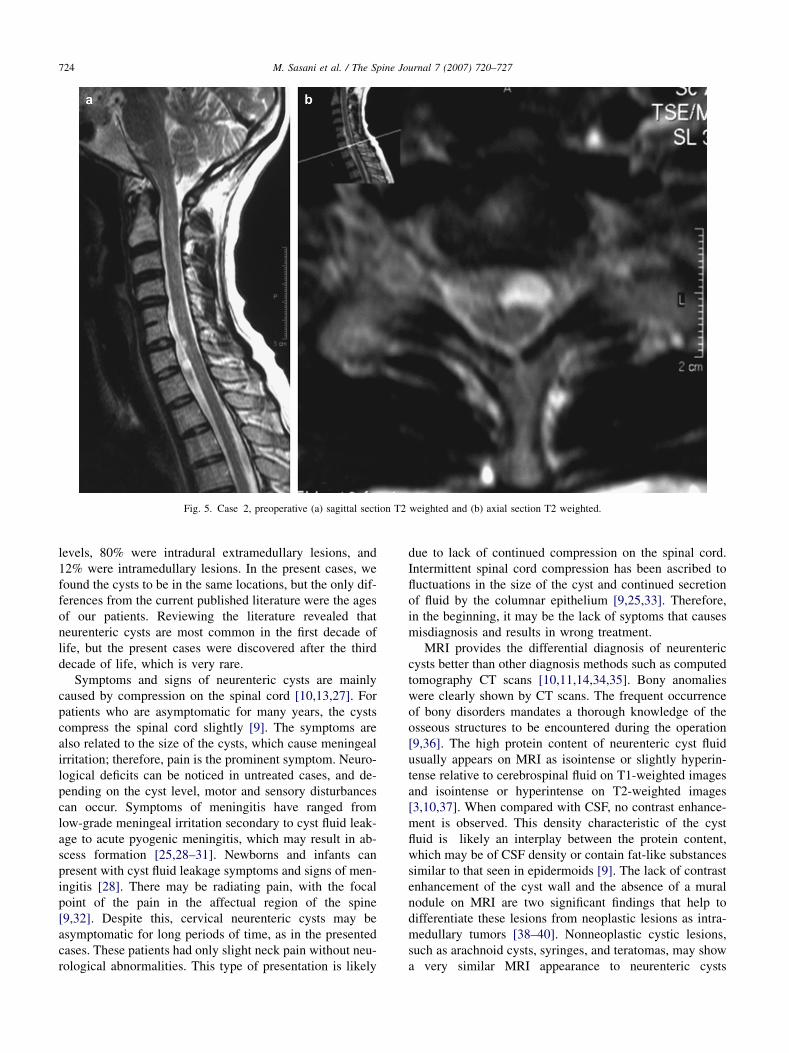
A 39-year-old woman complained of neck pain for 1year. The medical treatment, including a painkiller (diclofe-nac Na), a muscle relaxant (dizanidine hydrochlorur), andphysical therapy, was not helpful. Neurological examina-tion determined no neurological deficit. The MRI studiesof the cervical spine showed anterior intradural extramedul-lary cyst (hypointense on T1 and hyperintense on T2) at theC7–T1 disc level (Fig. 5). First, anterior discectomy wasperformed at the C7–T1 level in addition to partial corpec-tomies of the lower part of the C7 and the upper part of theT1 vertebrae. As in the first case, a vertical small incisionwas made through the dura mater to expose the lesion.The cyst was mucoid lesions attached to the ventral aspectof the spinal cord. After total removal of the neurentericcyst, the dura was closed with 4-0 absorbable sutures andsupported with artificial dura mater and fat grafts. Fusionwas then performed with allograft crista iliaca bone, andanterocervical plates were applied.
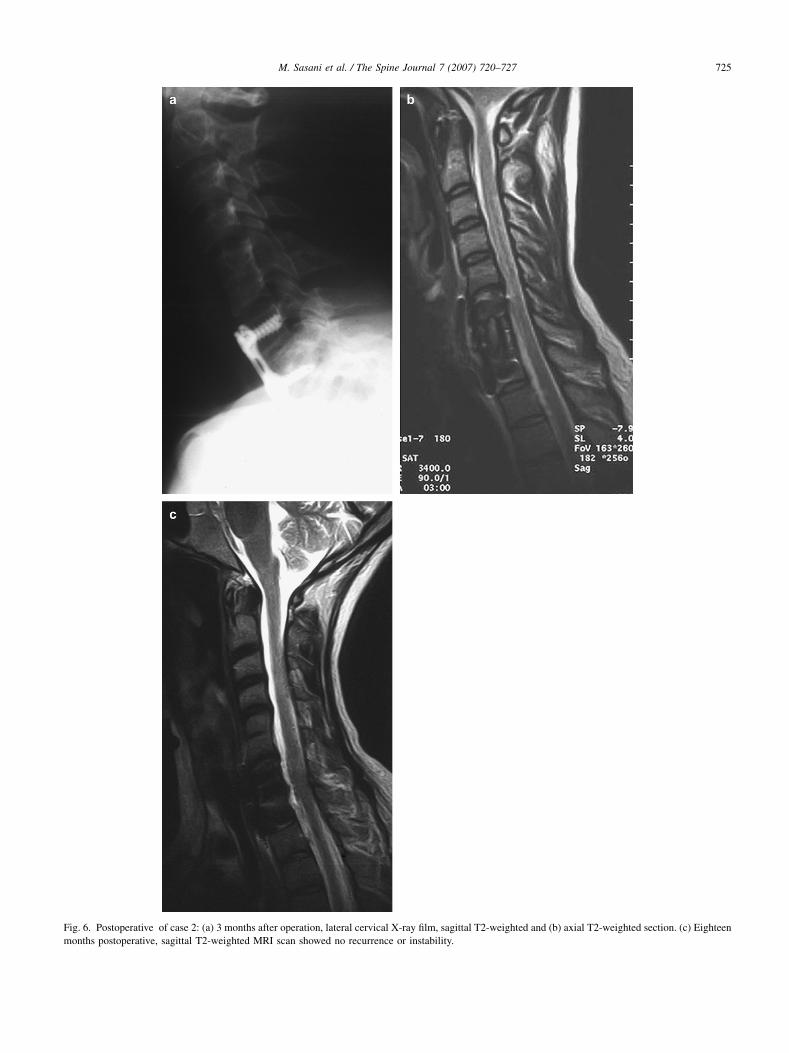
The histologic sections of the cyst wall determined thatthe lesions were neurenteric cyst. The postoperative periodwas uneventful. The patient was discharged in goodcondition on the third postoperative day. The 3-, 6-, and18-month postoperative MRI showed resolution of theselesions and no recurrence (Fig. 6).
Discussion
Spinal cord neurenteric cysts are rare. They are mostcommonly found during the first decade of life[1,2,10,20–25]. The male:female ratio for development ofthese cysts is 2:1 [26]. The cervical canal and the cervico-thoracic junction are the most common locations. Anteriorcysts are always localized ventral or anterolateral to thespinal cord in both children and adults [9]. Agnoli et al.[2] reviewed 33 histologically verified neurenteric intraspi-nal cysts. The study’s findings showed that 18 cases werelocated in the cervicodorsal spine between C3 and T7
Fig. 3. Histopathological examination showed a cystic lesion resembling
intestinal epithelium.
723M. Sasani et al. / The Spine Journal 7 (2007) 720–727
Fig. 4. Postoperative of case 1: (A) cervical MRI 3 months after the operation: (a) sagittal section and (b) axial section. The black arrow shows subarachnoid
space, and the white arrow shows plate and screw artifact. (B) Eighteen-month postoperative cervical MRI demonstrated no recurrence: (a) sagitttal plan T2
weighted and (b) axial T2 weighted section.
724 M. Sasani et al. / The Spine Journal 7 (2007) 720–727
Fig. 5. Case 2, preoperative (a) sagittal section T2 weighted and (b) axial section T2 weighted.
levels, 80% were intradural extramedullary lesions, and12% were intramedullary lesions. In the present cases, wefound the cysts to be in the same locations, but the only dif-ferences from the current published literature were the agesof our patients. Reviewing the literature revealed thatneurenteric cysts are most common in the first decade oflife, but the present cases were discovered after the thirddecade of life, which is very rare.
Symptoms and signs of neurenteric cysts are mainlycaused by compression on the spinal cord [10,13,27]. Forpatients who are asymptomatic for many years, the cystscompress the spinal cord slightly [9]. The symptoms arealso related to the size of the cysts, which cause meningealirritation; therefore, pain is the prominent symptom. Neuro-logical deficits can be noticed in untreated cases, and de-pending on the cyst level, motor and sensory disturbancescan occur. Symptoms of meningitis have ranged fromlow-grade meningeal irritation secondary to cyst fluid leak-age to acute pyogenic meningitis, which may result in ab-scess formation [25,28–31]. Newborns and infants canpresent with cyst fluid leakage symptoms and signs of men-ingitis [28]. There may be radiating pain, with the focalpoint of the pain in the affectual region of the spine[9,32]. Despite this, cervical neurenteric cysts may beasymptomatic for long periods of time, as in the presentedcases. These patients had only slight neck pain without neu-rological abnormalities. This type of presentation is likely
due to lack of continued compression on the spinal cord.Intermittent spinal cord compression has been ascribed tofluctuations in the size of the cyst and continued secretionof fluid by the columnar epithelium [9,25,33]. Therefore,in the beginning, it may be the lack of syptoms that causesmisdiagnosis and results in wrong treatment.
MRI provides the differential diagnosis of neurentericcysts better than other diagnosis methods such as computedtomography CT scans [10,11,14,34,35]. Bony anomalieswere clearly shown by CT scans. The frequent occurrenceof bony disorders mandates a thorough knowledge of theosseous structures to be encountered during the operation[9,36]. The high protein content of neurenteric cyst fluidusually appears on MRI as isointense or slightly hyperin-tense relative to cerebrospinal fluid on T1-weighted imagesand isointense or hyperintense on T2-weighted images[3,10,37]. When compared with CSF, no contrast enhance-ment is observed. This density characteristic of the cystfluid is likely an interplay between the protein content,which may be of CSF density or contain fat-like substancessimilar to that seen in epidermoids [9]. The lack of contrastenhancement of the cyst wall and the absence of a muralnodule on MRI are two significant findings that help todifferentiate these lesions from neoplastic lesions as intra-medullary tumors [38–40]. Nonneoplastic cystic lesions,such as arachnoid cysts, syringes, and teratomas, may showa very similar MRI appearance to neurenteric cysts
725M. Sasani et al. / The Spine Journal 7 (2007) 720–727
Fig. 6. Postoperative of case 2: (a) 3 months after operation, lateral cervical X-ray film, sagittal T2-weighted and (b) axial T2-weighted section. (c) Eighteen
months postoperative, sagittal T2-weighted MRI scan showed no recurrence or instability.

726 M. Sasani et al. / The Spine Journal 7 (2007) 720–727
[38,41,42]. The diagnostic marker of an arachnoid cyst isthat the cerebrospinal fluid of patients with arachnoid cystsdoes not have a high protein content like that of patientswith neurenteric cysts. MRI usually shows increased signalon T2-weighted images with no cyst wall postcontrast en-hancement [43]. Intramedullarily located neurenteric cystsin the literature are reported to be very rare [7,8,9,44,45].
Neurenteric cysts are benign lesions; this criterion is thereason for the increased importance in achieving a success-ful outcome during the surgical procedure. The basic aim oftreatment is excision of the lesion to avoid neurologicaldeficits. A review of the literature shows that mostly sur-gery via the posterior approach has been performed, despitethe ventral location of the neurenteric cyst [46]. Althoughthe anterior cervical approach carries risks, such as theinjury of nearby structures, failure of fusion and graft dis-placement, and delayed formation of hematoma and cere-brospinal fluid leakage, the posterior approach has riskswith different, severe side effects from the anterior ap-proach. Complications associated with posterior proceduresare related to the degree of exposure, the neural element ex-posed, and the use of instrumentation and vascular elementinjuries [47,48]. The primary risks of cervical laminectomyinclude cord, dura, and root injuries. The vascular compli-cations, including vertebral artery injury and venous bleed-ing, may result in hematoma. Lateral mass screws requireprecise localization to avoid injury to the vertebral artery.Although the cyst is often ventral to the cord, a posteriorlateral approach usually provides the most direct avenueto resection. The cord is often displaced from the massand may be dissected free from the cord after sectioningof the dentate ligaments and aspiration of the cyst contents.Because of the viscous, mucinous contents, this proceduremay provide only partial collapse of the cystic mass. In ad-dition, total resection may be accomplished with tearing ofthe cyst membrane. Leakage of the cyst contents may resultin meningeal irritation in the posterior approach, whereasdirect exposure of the cyst in the anterior approach maycause total resection without rupturing of the cyst.
Obviously, the anterior approach to remove neurentericcysts that are ventrally localized and completely extrame-dullary in position is more satisfactory than the posteriorapproach [9]. In 1990, Koksal et al. [18] described an ante-rior approach to the craniocervical neurenteric cyst. Fouryears later, Devkota et al. [15] reported a case of an intra-dural neurenteric cyst of the cervical spine approachedthrough a central corpectomy. It is important to identifythe vascular anatomy of ventrally located lesions becausea posterior approach may compromise the abnormal vascu-lature [9,30,31]. In the posterior approach, the retraction ofthe spinal cord to reach the ventral location may causepermanent damages.
The other underlying point is surgery for the recurrenceof neurenteric cysts. Menezes and Traynelis [9] andMenezes and Ryken [29] described that there is no correla-tion between age, sex, and size and level of neurenteric cyst
recurrence. Partial resection is the major cause leading torecurrence of a neurenteric cyst. We believe that only a bi-opsy or aspiration of the cyst is not an adequate procedure;total resection of the cyst is the main goal, and it can beeasily performed via an anterior approach, without tearingof the cyst membrane to avoid meningeal irritation thatmay result in meningitis. The anterior approach does notcarry the risks of artery injury related to instrumentationlike posterior approach.
From this study, it can be concluded that although neu-renteric cysts are rare in adults, they can still be presentwith only persistent neck pain and without neurologicaldeficits. This may lead to misdiagnosis. The importanceof MRI is not controversial in the early diagnosis. Theanterior approach may be considered the first preferencefor surgical technique in patients with ventrally locatedneurenteric cysts.
References
[1] Adams RD, Wegner W. Congenital cyst of the spinal meningies as
cause of intermittent compression of spinal cord. Arch Neurol
Psychiatry 1974;58:57–69.
[2] Agnoli AL, Laun A, Schhonmar R. Entregenous intraspinal cyst.
J Neurosurgery 1984;61:834–40.
[3] Paolini S, Ciapetta P, Domenicucci M, Guiducci A. Intramedullary
neurenteric cyst with a false mural nodule: case report. Neurosurgery
2003;52:243–6.
[4] Kwok DM, Jeffreys RV. Intramedullary enterogenouscyst of the
spinal cord: case report. J Neurosurg 1982;56:270–4.
[5] Lippman CR, Arginteanu M, Purohit D, Naidich TP, Camins MB.
Intramedullary neurenteric cysts of the spine. J Neurosurg 2001;
94:305–9.
[6] Mizuno J, Fiandaca MS, Nishio S, O’Brien MS. Recurrent intrame-
dullary entergenous cyst of the cervical spinal cord. Child Nerv Syst
1988;4:47–9.
[7] Rivierez M, Buisson G, Kujas M, et al. Intramedullary neurenteric
cyst without any associated malformation: one case evaluated by
RMI and dectron microscopic study. Acta Neurochir (Wien)
1997;139:887–90.
[8] Silvernail W, Brown R. Intramedullary entergenous cyst: case report.
J Neurosurg 1972;36:235–8.
[9] Menezes AH, Traynelis VC. Spinal neurenteric cyst in the magnetic
resonance imaging era. Neurosurgery 2006;58:97–105.
[10] Brooks BS, Duvall ER, Gammal TE, Garcia JH, Gupta KI, Kapila A.
Neuroimaging features of neurenteric cysts: analysis of nine cases
and review of literature. AJNR Am J Neuroradiol 1993;14:735–46.
[11] Fernandes ET, Custer MD, Burton EM, et al. Neurenteric cyst:
surgery and diagnostic imaging. J Pediatr Surg 1991;26:108–10.
[12] Paleologos TS, Thom M, Thomas DG. Spinal neurenteric cysts with-
out associated malformations. Are they the same as those presenting
in spinal dysraphism? Br J Neurosurg 2000;14:185–94.
[13] Alrabeeah A, Gillis DA, Giacomantoniom M, Lau H. Neurenteric
cysts. A spectrum. J Pediatr Surg 1988;23:752–4.
[14] Kantrowitz LR, Pais MJ, Burnett K, Choi B, Pritz MB. Intraspinal
neurenteric cyst containing gastric mucosa. CT and MRI findings.
Pediatr Radiol 1986;16:324–7.
[15] Devkota UP, Lam JM, Ng H, Poon WS. An anterior intradural neu-
renteric cyst of the cervical spine: complete excision through central
corpectomy approach. Case report. Neurosurgery 1994;35:1150–3.
[16] Takase T, Ishikawa M, Nishi S, et al. A recurrent intradural cervical
neurenteric cyst operated on using an anterior approach: a case
report. Surg Neurol 2003;59:34–9.
727M. Sasani et al. / The Spine Journal 7 (2007) 720–727
[17] Miyoshi K, Nakamura K, Hoshin OY, Kuribayashi Y, Saita K,
Kurokawa T. Removal of enterogenous cyst of the cervical spine
through anterior approach. J. Spinal Disord 1998;11:84–8.
[18] Koksal T, Revesz T, Crockard HA. Craniospinal neurenteric cyst. Br J
Neurosurg 1990;4:425–8.
[19] Song JK, Burkey BB, Konrad PE. Lateral approach to neurenteric
cyst of the cervical spine. Case presentation and review of surgical
technique. Spine 2003;28:E81–5.
[20] Aoki S, Machide T, Sasaki Y, et al. Entrogenous cyst of cervical
spine: clinical and radiological aspect (including CT and MRI).
Neuroradiology 1987;29:291–3.
[21] Fallon M, Gordon AR, Lendrom AC. Mediastinal cysts of fore-gut
origin associated with vertebral abnormalities. Br J Surg 1954;41:
520–33.
[22] Fortuna A, Mercuri S. Intradural spinal cysts. Acta Neurochir
1983;68:289–314.
[23] Holmes GL, Trader S, Iangatidis P. Intraspinal entrogenous cysts.
Am J Dischild 1978;132:906–8.
[24] Lach B, Russell N, Atack D, Benoit B. Intraparanchymal epithelial
(entrogenous) cyst of the medulla oblongata. Can J Neurol Sci
1989;16:206–10.
[25] Le Doux MS, Faye Peterson O, Aronin PA, Vaid YN, Pitts RM. Lum-
bosacral neurenteric cyst in an infant: case report. J Neurosurg
1993;78:821–5.
[26] Singhel BS, Parekh HN, Ursekar M, Depujari CE, Manghani DK.
Intramedullary neurenteric cyst in mid thoracic spine in an adult:
a case report. Neurol India 2001;49:302–4.
[27] De Olivera RS, Cinalli G, Roujeau T, Sainte-Rose C, Pierre-Kahn A,
Zerah M. Neurenteric cyst in children: 16 consecutive cases and
review of the literature. J Neurosurg 2005;103:512–23.
[28] Jackson FE. Report of a case of neurenteric cyst with associated
chronic meningitis and hydrocephalus. J Neurosurg 1961;18:678–82.
[29] Menezes AH, Ryken TC. Craniocervical intradural neurenteric cysts.
Pediatr Neurosurg 1995;22:88–95.
[30] Millis RR, Holmes AE. Entrogenous cysts of the spinal cord with
associated interstinal reduplication, vertebral anomalies and a dorsal
dermal sinus: case report. J Neurosurg 1973;38:73–7.
[31] Schmidbauer M, Rein Perecht A, Schuster H, Wimberger D,
Kolleger H. Atypical vertebral artery in a patient with an intra and
extraspinal cervical neurenteric cyst. Acta Neurochir 1991;109:
150–3.
[32] Wilkins RH, Rossitch E Jr. Inraspinal cysts. In: Pang D, editor. Disor-
ders of the Pediatric Spine. New York, NY: Raven Press, 1995:445–60.
[33] Breunberg JA, Dipietro MA, Vnes JL, et al. Intramedullary lesions of
the pediatric spinal cord. Correlation of findings from MR imaging,
intraoperative sonography, surgery and histology study. Radiology
1991;181:573–9.
[34] Pierot L, Dormont D, Queslati S, Cornu P, Rivierez M, Bories J. Ga-
dolinium DTPA enhanced MR imaging of intradural neurenteric
cysts. J Comput Assist Tomogr 1998;12:762–4.
[35] Neuhauser EBD, Harris GB, Berrett A. Roentgenographic feature of
neurenteric cysts. AJNR Am J Roentgenol 1958;79:235–40.
[36] Ellis AM, Taylor TK. Intravertebral spinal neurenteric cysts: a unique
radiographic sign: ‘‘the hole-in one vertebrae’’. J Pediatr Orthop
1997;17:766–8.
[37] Germia GK, Russell EJ, Clasen RA. MR imaging characteristics of
a neurenteric cyst. AJNR Am J Neuroradiol 1998;9:978–80.
[38] Lippman CR, Arginteanu M, Purhoit D, Naidich TP, Camins MB. In-
tramedullary neurenteric cysts of the spine case report and review of
the literature. J Neurosurg 2001;94:305–9.
[39] Gao P, Osborn A, Smirniotopoulos J, Palmer CA, Boyer RS. Neuren-
teric cysts: pathology, imaging spectrum and differential diagnosis.
Int J Neuroradiol 1995;1:17–27.
[40] Osborn A. Diagnostic Neuroradiology. St Louis, NO: Mosby, 1994:
813–5.
[41] Kazan S, Ozdemir O, Akyuz M, Tuncer R. Spinal intradural
arachnoid cysts located anterior to the cervical spinal cord. Report
of two cases and review of the literature. J Neurosurg 1999;9:
211–5.
[42] Sharma A, Soyal P, Bodhe P, Pardey A, Diyora B, Ingale H. Spinal
intramedullary arachnoid cyst. Indian J Pediatr 2004;71:e65–7.
[43] Safriel YI, Sanchez G, Jhaveri HS. Giant anterior cervicothoracic
arachnoid cyst. Spine 2002;1(27):366–8.
[44] Kwor DM, Jeffreys RV. Intramedullary entrogenous cyst of the spinal
cord. Case report. J Neurosurg 1982;56:270–1.
[45] Mizuno J, Fiandaca MS, Nishio S, O’Brien MS. Recurrent intrame-
dullary entrogenous cyst of the cervical spinal cord. Child Nerv Syst
1988;4:47–9.
[46] Guilband JN, Arieh YB, Peyser E. Spinal intradural entragenous cyst.
A case report. Surg Neural 1980;14:359–61.
[47] Schold S, Wasserstorm W, Fleisher M, Schwartz MK, Posner JB.
Cerebrospinal fluid biomechanical markers of central nervous system
metastase. Ann Neurol 1980;85:597–604.
[48] Jenkins AL III, Deutch H, Patel NP, Post KD. Complication
avoidance in neurosurgery. In: Winn HR, editor. ed. 5, Youmans Neu-
rological Surgery, Vol 1. Philedelphia, PA: Saunders, 2004:561–93.




















