
Chapter 22. Genetic diseases reveal DNA nucleotide excision ...
Upload
independentCategory
view
0download
0
CLINICAL ARTICLE
Surgical planning for microsurgical excision of cerebralarterio-venous malformations using virtualreality technology
Ivan Ng & Peter Y. K. Hwang & Dinesh Kumar &
Cheng Kiang Lee & Ralf A. Kockro & Y. Y. Sitoh
Received: 20 March 2008 /Accepted: 13 October 2008 /Published online: 25 March 2009# Springer-Verlag 2009
AbstractBackground To evaluate the feasibility of surgical planningusing a virtual reality platform workstation in the treatmentof cerebral arterio-venous malformations (AVMs)Methods Patient- specific data of multiple imaging modal-ities were co-registered, fused and displayed as a 3Dstereoscopic object on the Dextroscope, a virtual realitysurgical planning platform. This system allows for manipu-lation of 3D data and for the user to evaluate and appreciatethe angio-architecture of the nidus with regards to position andspatial relationships of critical feeders and draining veins. Weevaluated the ability of the Dextroscope to influence surgicalplanning by providing a better understanding of the angio-architecture as well as its impact on the surgeon’s pre- andintra-operative confidence and ability to tackle these lesions.
Findings Twenty four patients were studied. The mean agewas 29.65 years. Following pre-surgical planning on theDextroscope, 23 patients underwent microsurgical resectionafter pre-surgical virtual reality planning, during which all haddocumented complete resection of the AVM. Planning on thevirtual reality platform allowed for identification of criticalfeeders and draining vessels in all patients. The appreciationof the complex patient specific angio-architecture to establisha surgical plan was found to be invaluable in the conduct ofthe procedure and was found to enhance the surgeon’sconfidence significantly.Conclusion Surgical planning of resection of an AVM witha virtual reality system allowed detailed and comprehensiveanalysis of 3D multi-modality imaging data and, in ourexperience, proved very helpful in establishing a good sur-gical strategy, enhancing intra-operative spatial orientationand increasing surgeon’s confidence.
Keywords Cerebral arterio-venous malformation .
Virtual reality . Simulation . Surgical planning
Introduction
While different modalities such as endovascular embolisationand radiosurgery have emerged as options in addition tomicrosurgery in the treatment of cerebral arterio-venousmalformations (AVMs), microsurgical resection remains animportant treatment modality for these lesions [9]. However,the surgical excision of a symptomatic cerebral arterio-venousmalformation can represent one of the most technicallychallenging procedures for the neurovascular surgeon. An
Acta Neurochir (2009) 151:453–463DOI 10.1007/s00701-009-0278-5
I. Ng (*) : P. Y. K. Hwang :D. Kumar : C. K. LeeDepartment of Neurosurgery, National Neuroscience Institute,11 Jalan Tan Tock Seng,Singapore 308433, Singaporee-mail: [email protected]
Y. Y. SitohDepartment of Neuroradiology, National Neuroscience Institute,11 Jalan Tan Tock Seng,Singapore 308433, Singapore
I. NgDuke-NUS Graduate Medical School,Singapore, Singapore
R. A. KockroVolume Interactions Pte Ltd Singapore,1 Kim Seng Promenade, #12-01, Great World City East Tower,Singapore 237994, Singapore

important key to surgical success in this endeavour is thecapability of the surgical team to mentally conceptualise a pre-surgical plan based on careful analysis of pre-operativeconventional angiography, magnetic resonance imaging(MRI) and angiography (MRA) and where necessaryancillary imaging such as functional MRI [2], diffusiontensor imaging [10], positron emission tomography andmagneto-encephalography. The ability to assimilate thisinformation with the objective to mentally visualise andunderstand the pathological-anatomy of the specific locationand. the unique AVM angio-architecture, including spatialrelationship to feeding arteries and draining veins, contributesa significant part towards the steep learning curve associatedwith treating these lesions. Contemporary planning with theabove-mentioned images is usually carried out with two-dimensional (2D) imaging series with each technique provid-ing specific information which the neurosurgeon has tointegrate mentally. AlthoughMRA andCTAmay be displayedin 3D, comprehensive surgical planning is limited by the rathersimple manipulation tools provided by the radiologicalviewing stations. The difficulty of surgical planning increaseswith increasing complexity of specific spatial geometricrelationships of critical structures in 3 D space. A stereoscopicdisplay which indicates all the complexities in 3D space wouldconceivably be helpful in the surgical planning of theselesions. The benefits of surgical planning would augment theprocess of optimisation of operative exposure, shortening ofoperative time, minimisation of blood loss and potentiallyreduce complications and improve overall outcomes of AVMsurgery [19]. In this regard, we utilised a virtual realityworkstation previously published [11] to integrate therelevant information derived from multiple imaging modal-ities in order to three-dimensionally reconstruct the uniqueangio-architecture of each AVM for pre-surgical planning.We evaluated the system’s usefulness for the understandingof the individual spatial vascular complexity and theformulation of a strategy for surgical AVM excision. In ad-dition, we assessed the system’s overall clinical benefits.
Materials & methods
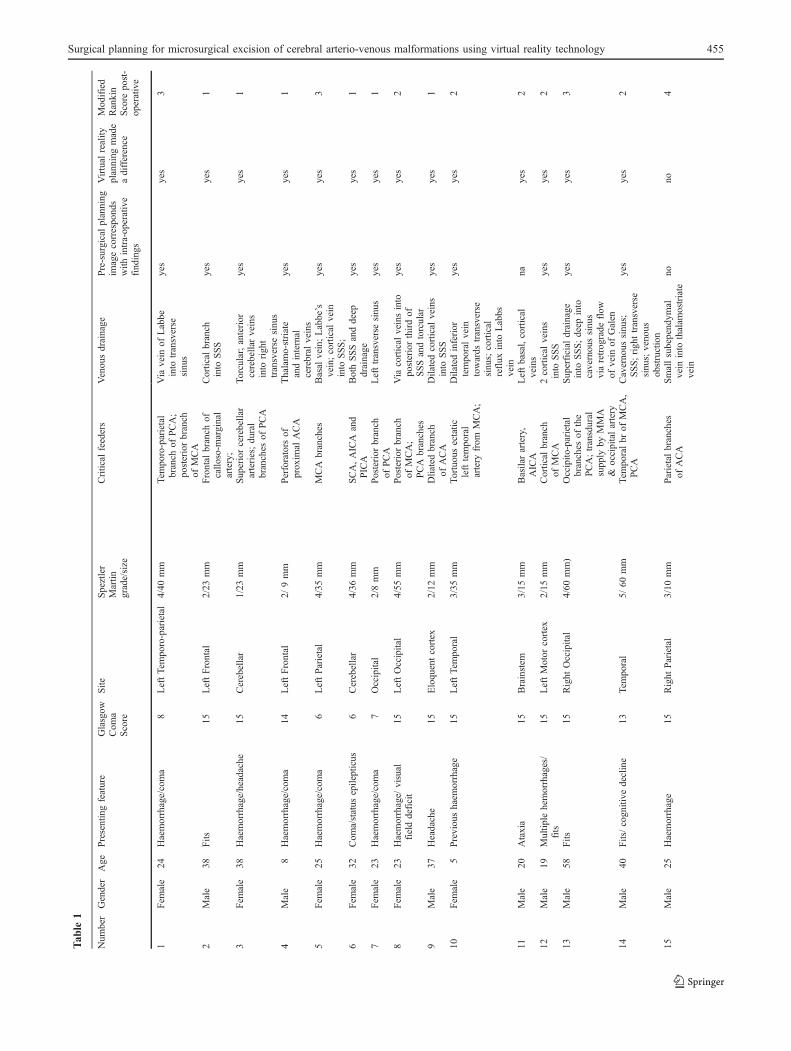
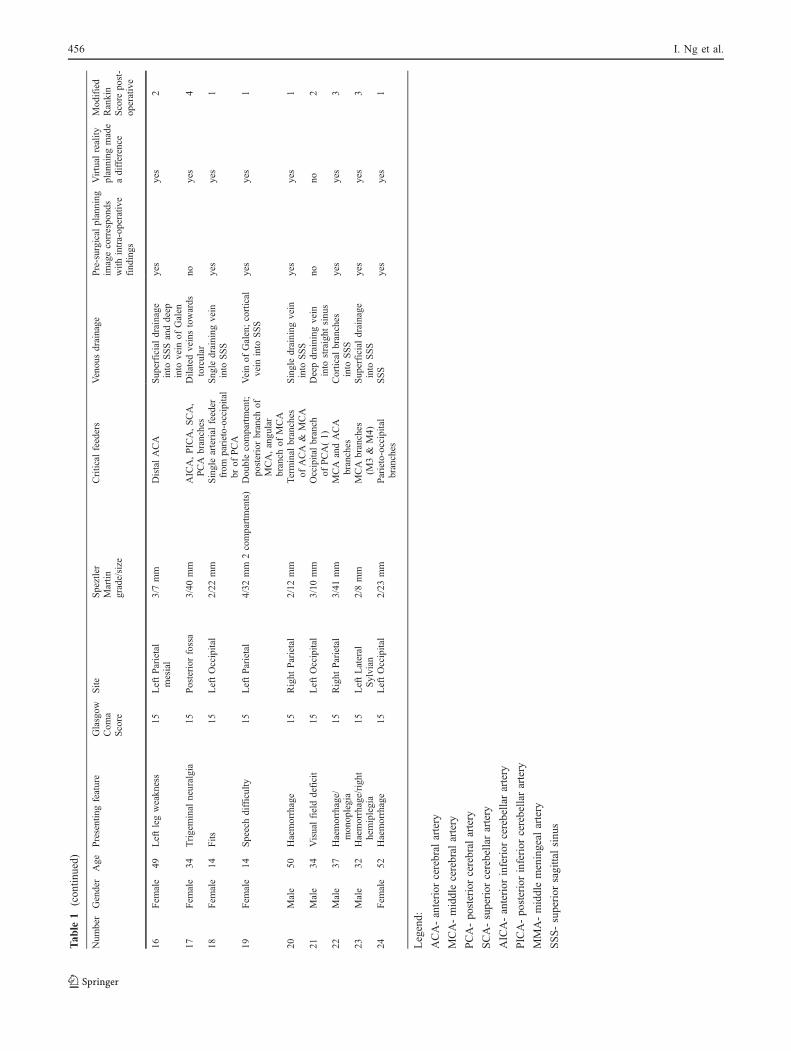
This prospective clinical study comprised 24 patients whounderwent microsurgical resection of cerebral AVMs at ourinstitute between May 2005 to May 2007 (Table 1). All thepatients underwent pre-operative magnetic resonance im-aging (MRI), magnetic resonance angiography (MRA),contrast catheter angiography and where necessary compu-terised tomographic angiography (CTA) as part of thesurgical work-up.
MRI imaging was performed on a GE 1.5 T scanner or aPhilips 3 Tscanner. MRAwas obtained in a 3D Time of Flight(TOF) mode (General Electric: TR 36 ms, TE 6.9 ms, flip
angle 25, FOV 24 cm, matrix 512×512, 1.2 mm thicknesswith 0.6 mm overlap )
The information was transferred to a virtual reality work-station (Dextroscope; Volume Interactions Pte Ltd, Singapore)via data from the respective modalities using a DICOM formaton a CD. The data from these images were registered into thecomputer of the Dextroscope. A three dimensional multi-coloured interactive virtual reconstruct of the patient’s headshowing the AVM including feeding arteries, draining veins,other intra-cranial arteries, venous sinuses, cortex and skull wasthen produced using the Dextroscope software.
Dextroscope hardware
The Dextroscope consists of two combined workspaces for2D and 3D image processing, visualisation and surgicalplanning. Inside the Dextroscope’s virtual workspace the userworks with both hands inside a stereoscopic environmentcontaining the patient’s specific 3D imaging data as well asvarious image processing and surgical planning tools. This isachieved by reflecting a computer generated 3D scenario via amirror into the user’s eyes. Wearing liquid display shutterglasses synchronised with the time split display, the userreaches with both hands behind the mirror into the “floating”3D data. Electromagnetic sensors in both hands convey theinteraction and allow 3D data manipulation in real time. Onehand holds an ergonomically shaped handle to move the 3Ddata freely as if it were an object held in real space. The otherhand holds a pen-shaped instrument, which appears inside thevirtual reality workspace as a computer generated instrumentand which can be used to perform detailed data manipulations.The Dextroscope’s hardware and software concept has beendescribed by Kockro et al in 2000 [11]. However, theunderlying hardware implementation has been changed froma Silicon Graphics Onyx2 workstation to a PC and thestructural design of the Dextroscope has been adapted toergonomic requirements. The graphics engine relies onhardware assisted texture mapping.
Dextroscope software
The virtual workspace inside the Dextroscope provides allthe tools necessary for 3D data exploration and surgicalplanning. By lowering the hand-held pen onto the physicalbottom of the workspace inside the Dextroscope, a virtualtool rack automatically appears consisting of virtual buttonsand sliders, which can be activated with the virtualinstrument [11]. Software tools for colour and transparencycoding, manual and semi-automatic segmentation, imagefusion, curved, linear and volumetric measurements, crop-ping and cutting in any angle, virtual tissue removal (virtual“drilling” or “suctioning”) and reconstruction as well assnapshot and video reporting tools are available.
454 I. Ng et al.
Tab
le1
Num
ber
Gender
Age
Presentingfeature
Glasgow
Com
aScore
Site
Speztler
Martin
grade/size
Critical
feeders
Venousdrainage
Pre-surgicalplanning
imagecorresponds
with
intra-operative
findings
Virtual
reality
planning
made
adifference
Modified
Rankin
Score
post-
operative
1Fem
ale
24Haemorrhage/coma
8LeftTemporo-parietal
4/40
mm
Tem
poro-parietal
branch
ofPCA;
posteriorbranch
ofMCA
Via
vein
ofLabbe
into
transverse
sinus
yes
yes
3
2Male
38Fits
15LeftFrontal
2/23
mm
Frontal
branch
ofcallo
so-m
arginal
artery;
Cortical
branch
into
SSS
yes
yes
1
3Fem
ale
38Haemorrhage/headache
15Cerebellar
1/23
mm
Superiorcerebellar
arteries;dural
branches
ofPCA
Torcular;anterior
cerebellarveins
into
right
transverse
sinus
yes
yes
1
4Male
8Haemorrhage/coma
14LeftFrontal
2/9mm
Perforators
ofproxim
alACA
Thalamo-striate
andinternal
cerebral
veins
yes
yes
1
5Fem
ale
25Haemorrhage/coma
6LeftParietal
4/35
mm
MCA
branches
Basal
vein;Labbe’s
vein;cortical
vein
into
SSS;
yes
yes
3
6Fem
ale
32Com
a/status
epilepticus
6Cerebellar
4/36
mm
SCA,AICA
and
PICA
BothSSSanddeep
drainage
yes
yes
1
7Fem
ale
23Haemorrhage/coma
7Occipital
2/8mm
Posterior
branch
ofPCA
Lefttransverse
sinus
yes
yes
1
8Fem
ale
23Haemorrhage/
visual
fielddeficit
15LeftOccipital
4/55
mm
Posterior
branch
ofMCA;
PCA
branches
Via
cortical
veinsinto
posteriorthirdof
SSSandtorcular
yes
yes
2
9Male
37Headache
15Eloquentcortex
2/12
mm
Dliatedbranch
ofACA
Dilatedcortical
veins
into
SSS
yes
yes
1
10Fem
ale
5Previoushaem
orrhage
15LeftTemporal
3/35
mm
Tortuousectatic
lefttemporal
artery
from
MCA;
Dilatedinferior
temporalvein
towards
transverse
sinus;cortical
reflux
into
Labbs
vein
yes
yes
2
11Male
20Ataxia
15Brainstem
3/15
mm
Basilarartery,
AICA
Leftbasal,cortical
veins
nayes
2
12Male
19Multip
lehemorrhages/
fits
15LeftMotor
cortex
2/15
mm
Cortical
branch
ofMCA
2cortical
veins
into
SSS
yes
yes
2
13Male
58Fits
15Right
Occipital
4/60
mm)
Occipito
-parietal
branches
ofthe
PCA;transdural
supply
byMMA
&occipitalartery
Superficial
drainage
into
SSS;deep
into
cavernoussinus
viaretrograde
flow
ofvein
ofGalen
yes
yes
3
14Male
40Fits/cognitive
decline
13Temporal
5/60
mm
Tem
poralbr
ofMCA,
PCA
Cavernous
sinus;
SSS;righttransverse
sinus;venous
obstruction
yes
yes
2
15Male
25Haemorrhage
15Right
Parietal
3/10
mm
Parietalbranches
ofACA
Smallsubependym
alvein
into
thalam
ostriate
vein
nono
4
Surgical planning for microsurgical excision of cerebral arterio-venous malformations using virtual reality technology 455
Tab
le1
(con
tinued)
Num
ber
Gender
Age
Presentingfeature
Glasgow
Com
aScore
Site
Speztler
Martin
grade/size
Critical
feeders
Venousdrainage
Pre-surgicalplanning
imagecorresponds
with
intra-operative
findings
Virtual
reality
planning
made
adifference
Modified
Rankin
Score
post-
operative
16Fem
ale
49Leftlegweakness
15LeftParietal
mesial
3/7mm
DistalACA
Superficial
drainage
into
SSSanddeep
into
vein
ofGalen
yes
yes
2
17Fem
ale
34Trigeminal
neuralgia
15Posterior
fossa
3/40
mm
AICA,PICA,SCA,
PCA
branches
Dilatedveinstowards
torcular
noyes
4
18Fem
ale
14Fits
15LeftOccipital
2/22
mm
Singlearterial
feeder
from
parieto-occipital
brof
PCA
Sngle
draining
vein
into
SSS
yes
yes
1
19Fem
ale
14Speechdifficulty
15LeftParietal
4/32
mm
2compartments)
Doublecompartment;
posteriorbranch
ofMCA,angular
branch
ofMCA
Veinof
Galen;cortical
vein
into
SSS
yes
yes
1
20Male
50Haemorrhage
15Right
Parietal
2/12
mm
Terminal
branches
ofACA
&MCA
Singledraining
vein
into
SSS
yes
yes
1
21Male
34Visualfielddeficit
15LeftOccipital
3/10
mm
Occipitalbranch
ofPCA(1)
Deepdraining
vein
into
straight
sinus
nono
2
22Male
37Haemorrhage/
monoplegia
15Right
Parietal
3/41
mm
MCA
andACA
branches
Cortical
branches
into
SSS
yes
yes
3
23Male
32Haemorrhage/right
hemiplegia
15LeftLateral
Sylvian
2/8mm
MCA
branches
(M3&
M4)
Superficial
drainage
into
SSS
yes
yes
3
24Fem
ale
52Haemorrhage
15LeftOccipital
2/23
mm
Parieto-occipital
branches
SSS
yes
yes
1
Legend:
ACA-anterior
cerebral
artery
MCA-middlecerebral
artery
PCA-po
steriorcerebral
artery
SCA-superior
cerebellarartery
AICA-anterior
inferior
cerebellarartery
PICA-po
steriorinferior
cerebellarartery
MMA-middlemeningeal
artery
SSS-superior
sagittalsinu
s
456 I. Ng et al.

Pre-surgical planning with analysis of conventionalimaging
For the purposes of this study, we analysed conventionalpre-operative angiography to understand flow dynamics aswell as contribution of the flow to the AVM by criticalarterial feeders, nidus geometry and draining veins. Local-isation of the nidus site is complemented by studying theMRI source images and its relationship with eloquentcortex, varices and haematoma cavity.
Data analysis and surgical planning with the Dextroscope
Individual patient specific datasets from multiple imagingtechniques, including magnetic resonance imaging (MRI),magnetic resonance angiography (MRA), magnetic resonancevenography (MRV), computed tomography (CT), etc, wereco-registered, fused, and displayed as a stereoscopic three-dimensional (3D) object within the Dextroscope.
This 3D stereoscopic virtual image of the AVM wascarefully studied and analysed with respect to geometry ofnidus, spatial relationship of main critical arterial feeders,draining veins and varices in relation to the nidus andhaematoma cavity if present. Nidal location was also notedwith regard to its anatomical relation with the haematomacavity or eloquent brain where appropriate. From this, weconceptualised a surgical strategy with regards to optimalpatient positioning, size and location of the craniotomy,avoidance of eloquent brain areas, and concentrating on firstlyobliterating arterial feeders followed by the draining veins.
The surgical approach was then “rehearsed” by simulatingthe approach to the individual arterial feeders and drainingveins. By using the Dextroscope’s 3D tools such as virtualcutting, tissue removal and alteration of transparency, wechecked the feasibility of a variety of approaches. If necessary,this pre-surgical simulationwas repeated until wewere satisfiedthat the best approach and excision strategy was obtained.
The surgical plan was then implemented on the patientand the AVM excised according to the plan, with intra-operative guidance from a Stealth neuronavigation appara-tus (Medtronics, Sofamor Danek, USA ). Following theresection, intra-operative angiography was performed toconfirm complete removal.
Analysis of data
We collected data with regards to the following
a. Ability of the Dextroscope to visualise critical arterialfeeders and their specific geometric association withthe nidus as identified from conventional catheterangiography.
b. Visualisation of general orientation of nidus and AVMarchitecture
c. Whether the pre-surgically established operative strate-gy was altered intra-operatively
d. Surgeon’s overall confidence and opinions about whetherthe Dextroscope planning added significant value to thewhole process
Results
This study included all patients with AVMs who underwentevaluation for surgery by the author (Ivan Ng) from March2005 to March 2007 (24 months). There were 24 with anequal sex distribution. The mean age was 29.65 years(range 5–61 years). The clinical characteristics and presen-tation as well as the site of the AVM and the Spetzler &Martin grade are presented in Table 1. One patient with abrainstem AVM (patient 11) was treated with radiosurgeryafter pre-surgical planning revealed that surgery would bedeemed too hazardous, given the position of the nidus andits relationship with the critical feeders. Four patients (18%)had pre-operative embolisation before definitive surgery(patients 7, 12,14, 15). One patient had an AVM incom-pletely resected 10 years ago and presented with ahaemorrhage (patient 24). All patients who underwentsurgery (23 of 24; 95%) had complete resection asconfirmed by intra-operative angiography.
As compared to visualisation on catheter angiography,virtual reality surgical planning allowed for identification ofcritical arterial feeders and venous drainage in all AVMs.This appreciation of AVM angio- architecture and the pre-conception of the surgical plan were found to be valuableduring intra-operative execution in 21 of 23 excisions(91%). Practically, this meant that the course of the actualsurgery did not veer significantly off the pre-operative plan.In patients 16 and 22, the pre-operative Dextroscopeplanning was not found to add significantly to conventionalangiography analysis, since the vascular anatomy was quiteclear. Patient 16 had 2 feeders supplying a small nidus andpatient 22 had a direct fistula with a single feeder.
Additionally, clear pre-operative identification of thevenous pouch within the nidus and its intra-operativeverification allowed for intra-operative orientation of itsspatial relationships with the critical arterial feeders givingus the capability to rationalise a strategy to locate andcoagulate or clip major feeders during the dissection of thenidus. The relationship of venous pouches in relation to thenidus allowed for the surgeon to modify his dissection planof the nidus with due consideration to the exact geometry ofthe angio-architecture. All draining veins were similarlyidentified with no intra-operative ‘surprises’. Dextroscope
Surgical planning for microsurgical excision of cerebral arterio-venous malformations using virtual reality technology 457
planning also allowed us to visualise and appreciate spatialrelationships of the AVM nidus to the previous haematomacavity in 14 of 24 or 58% patients [1, 4–8, 12, 15, 18, 20–24]which was extremely useful in determining the best approachto the nidus and its critical feeders and in minimisingcollateral injury to vital areas.
Twenty two of the 23 patients awoke from anaesthesiawithout added neurological deficits (95.7%). Patient 17(cerebellar AVM) had a posterior fossa haematoma post-surgery which required emergency evacuation and ventri-culostomy for hydrocephalus. Her post-operative recoverywas complicated by multi-resistant acinetobacter baumaniiinfection which required intra- ventricular polymyxin. Thepatient survived but is severely disabled.
Pre-surgical planning with the VR system was associatedwith increased confidence and a perceived impression fromthe surgeons that it made a significant difference withrespect to intra-operative spatial orientation and hencefacilitation of decision making during the dissection in 21of 23 excisions (91%).
Representative clinical illustration (patient 13)
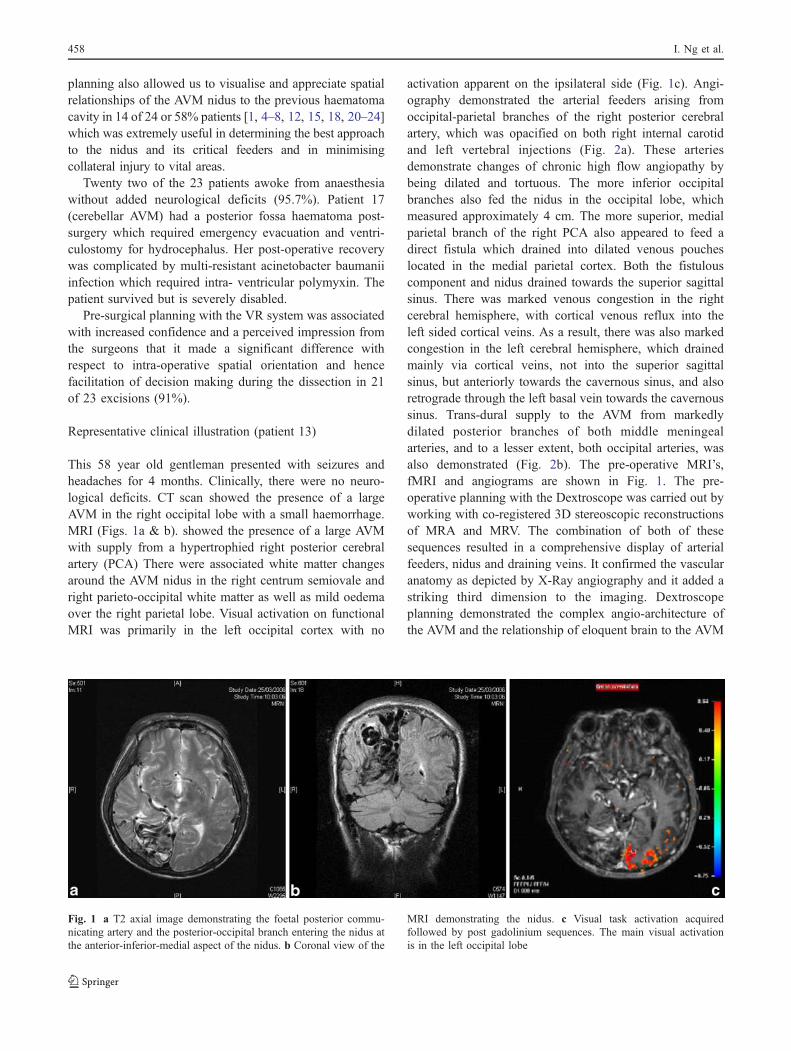
This 58 year old gentleman presented with seizures andheadaches for 4 months. Clinically, there were no neuro-logical deficits. CT scan showed the presence of a largeAVM in the right occipital lobe with a small haemorrhage.MRI (Figs. 1a & b). showed the presence of a large AVMwith supply from a hypertrophied right posterior cerebralartery (PCA) There were associated white matter changesaround the AVM nidus in the right centrum semiovale andright parieto-occipital white matter as well as mild oedemaover the right parietal lobe. Visual activation on functionalMRI was primarily in the left occipital cortex with no
activation apparent on the ipsilateral side (Fig. 1c). Angi-ography demonstrated the arterial feeders arising fromoccipital-parietal branches of the right posterior cerebralartery, which was opacified on both right internal carotidand left vertebral injections (Fig. 2a). These arteriesdemonstrate changes of chronic high flow angiopathy bybeing dilated and tortuous. The more inferior occipitalbranches also fed the nidus in the occipital lobe, whichmeasured approximately 4 cm. The more superior, medialparietal branch of the right PCA also appeared to feed adirect fistula which drained into dilated venous poucheslocated in the medial parietal cortex. Both the fistulouscomponent and nidus drained towards the superior sagittalsinus. There was marked venous congestion in the rightcerebral hemisphere, with cortical venous reflux into theleft sided cortical veins. As a result, there was also markedcongestion in the left cerebral hemisphere, which drainedmainly via cortical veins, not into the superior sagittalsinus, but anteriorly towards the cavernous sinus, and alsoretrograde through the left basal vein towards the cavernoussinus. Trans-dural supply to the AVM from markedlydilated posterior branches of both middle meningealarteries, and to a lesser extent, both occipital arteries, wasalso demonstrated (Fig. 2b). The pre-operative MRI’s,fMRI and angiograms are shown in Fig. 1. The pre-operative planning with the Dextroscope was carried out byworking with co-registered 3D stereoscopic reconstructionsof MRA and MRV. The combination of both of thesesequences resulted in a comprehensive display of arterialfeeders, nidus and draining veins. It confirmed the vascularanatomy as depicted by X-Ray angiography and it added astriking third dimension to the imaging. Dextroscopeplanning demonstrated the complex angio-architecture ofthe AVM and the relationship of eloquent brain to the AVM
Fig. 1 a T2 axial image demonstrating the foetal posterior commu-nicating artery and the posterior-occipital branch entering the nidus atthe anterior-inferior-medial aspect of the nidus. b Coronal view of the
MRI demonstrating the nidus. c Visual task activation acquiredfollowed by post gadolinium sequences. The main visual activationis in the left occipital lobe
458 I. Ng et al.

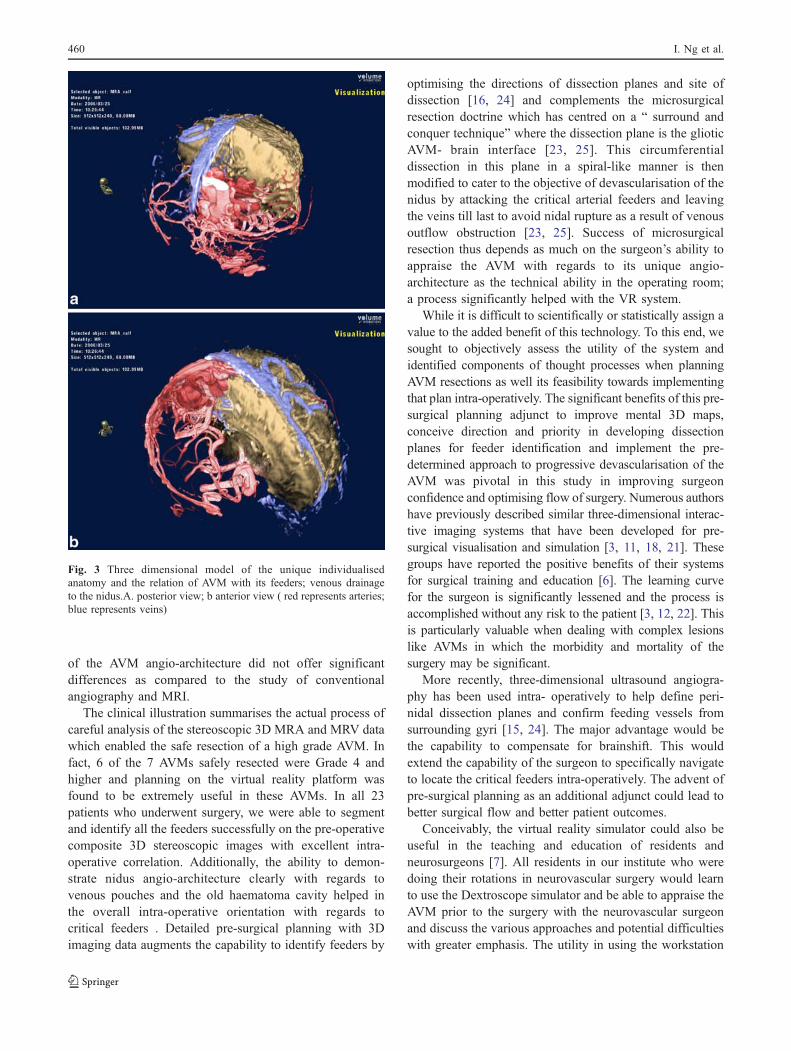
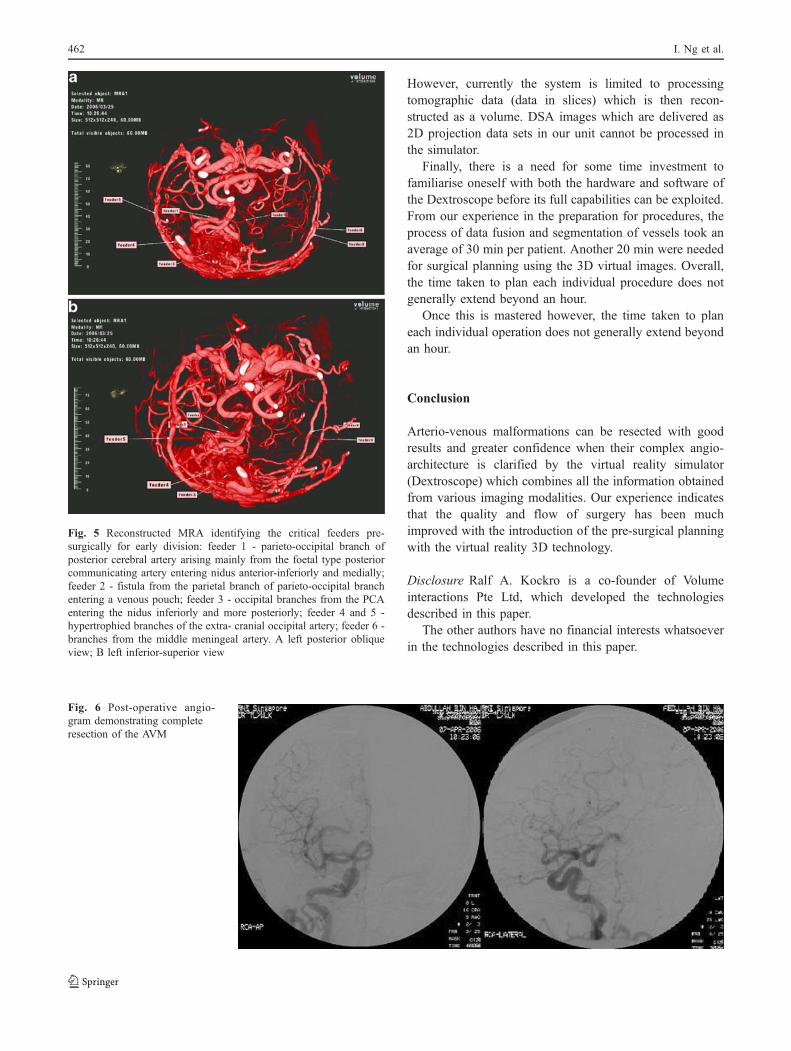
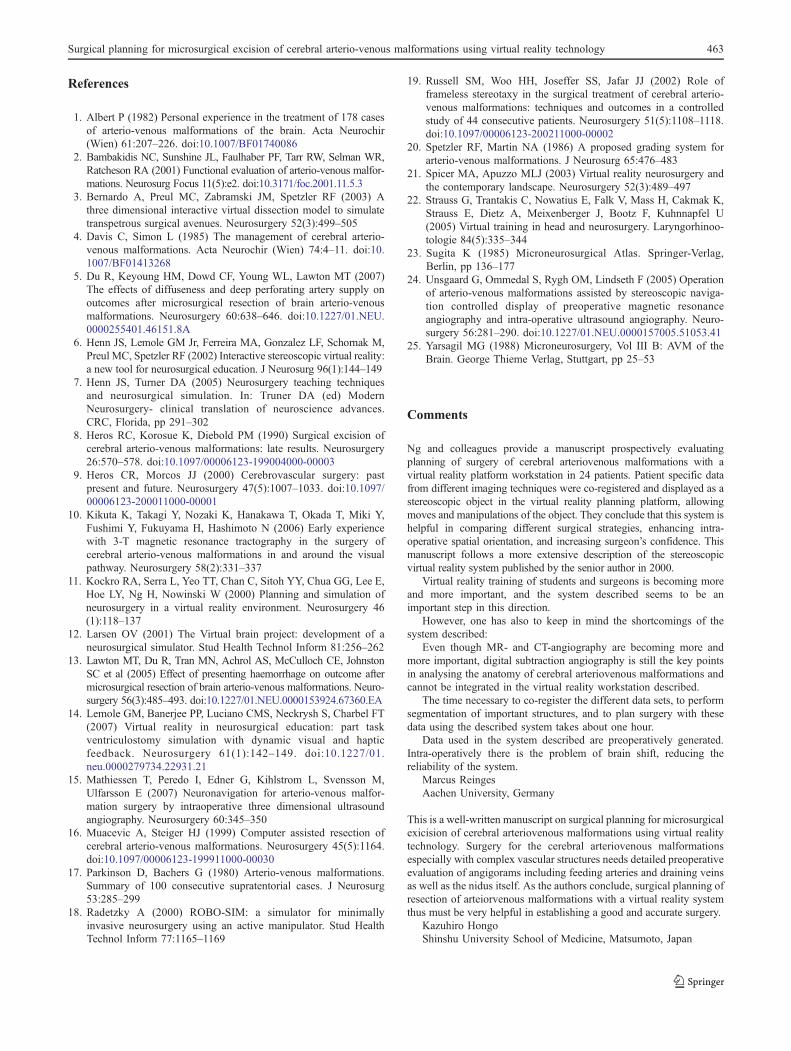
as well as the spatial relationships of the main feeders inrelation to the nidus (Figs. 3 and 4). Specifically, we wereable to formulate a surgical attack focused on securing themajor arterial feeders (Fig. 5); first from the occipital artery(feeders 4 and 5) by clipping these vessels early and thendrilling off the bone and cauterising them as they enter thedura to supply the nidus; branches of the middle meningealartery were cauterised as they enter the nidus superficially.The nidus was then dissected circumferentially and earlyidentification of the hypertrophied PCA feeder (feeder 1)was possible at the anterior-inferior-lateral aspect of thenidus arising from the hypertrophied posterior cerebralarterial feeder. The medially situated fistula (feeder 2) waslocated by referencing it with the medially situated venouspouch (Fig. 3b) before skeletonising the arterial supply ofthe occipital branches (feeder 3); this technique has alreadybeen described in detail by several authors [15, 16, 24]. Theprocedure was completed by creating a pedicle attachingthe nidus to the draining veins that enters the sagittal sinus.We followed this surgical strategy intra-operatively aidedby surgical navigation. The patient recovered from theoperation with no added neurological deficits and the post-operative angiograms are shown in Fig. 6.
Discussion
The morbidity and mortality rates for AVM microsurgicalresection in the reported literature vary from 7.8–30 % and0 to 12.5% respectively [1, 4, 8, 17]. Factors that affectsurgical outcome include the Spetzler —Martin grade [20],diffuseness of nidus, presence of deep perforating vesselsand presentation with haemorrhage [5, 13].
Practically, the process of surgery for AVMs can beconceptualised in three phases; 1) careful examination ofthe pre-operative images with a mental 3D reconstruction(planning phase), 2) execution of a suitable approach to theAVM (approach phase) and 3) meticulous dissection of thenidus including identification and clipping of arterialfeeders and draining veins (assault phase). We found VRplanning with the ability to manipulate the imagesstereoscopically to be a useful adjunct in all these threeaspects and noted that it improved the surgical flow andconfidence. We also felt it made a difference in the surgicaldecision making intra-operatively (in over 90% of AVMoperations). In the two procedures that we felt it was notuseful, the number of arterial feeders were few (2 in patient16 and 1 feeder in patient 22) and the Virtual Reality study
Fig. 2 a Catheter Angiogram(internal carotid artery injec-tion) of the AVM demonstratingthe filling of the nidus by thefilling of 2 major arterial feedersfrom the parieto-occipitalbranches of the posterior cere-bral artery from a foetal poste-rior communicating artery. Thearterial feeders are relatedanterior-inferiorly to the nidus.The more inferior occipitalfeeders are related to the nidusinferio-posteriorly. There is afistulous connection between thesuperior-medial parietal branchthat feeds the nidus and drainsdirectly into the superior sagittalsinus via dilated venouspouches. b Catheter angiogra-phy (external carotid arteryinjection demonstrating trans-dural supply from the occipitalarteries bilaterally and bothmiddle meningeal arteries
Surgical planning for microsurgical excision of cerebral arterio-venous malformations using virtual reality technology 459
of the AVM angio-architecture did not offer significantdifferences as compared to the study of conventionalangiography and MRI.
The clinical illustration summarises the actual process ofcareful analysis of the stereoscopic 3D MRA and MRV datawhich enabled the safe resection of a high grade AVM. Infact, 6 of the 7 AVMs safely resected were Grade 4 andhigher and planning on the virtual reality platform wasfound to be extremely useful in these AVMs. In all 23patients who underwent surgery, we were able to segmentand identify all the feeders successfully on the pre-operativecomposite 3D stereoscopic images with excellent intra-operative correlation. Additionally, the ability to demon-strate nidus angio-architecture clearly with regards tovenous pouches and the old haematoma cavity helped inthe overall intra-operative orientation with regards tocritical feeders . Detailed pre-surgical planning with 3Dimaging data augments the capability to identify feeders by
optimising the directions of dissection planes and site ofdissection [16, 24] and complements the microsurgicalresection doctrine which has centred on a “ surround andconquer technique” where the dissection plane is the glioticAVM- brain interface [23, 25]. This circumferentialdissection in this plane in a spiral-like manner is thenmodified to cater to the objective of devascularisation of thenidus by attacking the critical arterial feeders and leavingthe veins till last to avoid nidal rupture as a result of venousoutflow obstruction [23, 25]. Success of microsurgicalresection thus depends as much on the surgeon’s ability toappraise the AVM with regards to its unique angio-architecture as the technical ability in the operating room;a process significantly helped with the VR system.
While it is difficult to scientifically or statistically assign avalue to the added benefit of this technology. To this end, wesought to objectively assess the utility of the system andidentified components of thought processes when planningAVM resections as well its feasibility towards implementingthat plan intra-operatively. The significant benefits of this pre-surgical planning adjunct to improve mental 3D maps,conceive direction and priority in developing dissectionplanes for feeder identification and implement the pre-determined approach to progressive devascularisation of theAVM was pivotal in this study in improving surgeonconfidence and optimising flow of surgery. Numerous authorshave previously described similar three-dimensional interac-tive imaging systems that have been developed for pre-surgical visualisation and simulation [3, 11, 18, 21]. Thesegroups have reported the positive benefits of their systemsfor surgical training and education [6]. The learning curvefor the surgeon is significantly lessened and the process isaccomplished without any risk to the patient [3, 12, 22]. Thisis particularly valuable when dealing with complex lesionslike AVMs in which the morbidity and mortality of thesurgery may be significant.
More recently, three-dimensional ultrasound angiogra-phy has been used intra- operatively to help define peri-nidal dissection planes and confirm feeding vessels fromsurrounding gyri [15, 24]. The major advantage would bethe capability to compensate for brainshift. This wouldextend the capability of the surgeon to specifically navigateto locate the critical feeders intra-operatively. The advent ofpre-surgical planning as an additional adjunct could lead tobetter surgical flow and better patient outcomes.
Conceivably, the virtual reality simulator could also beuseful in the teaching and education of residents andneurosurgeons [7]. All residents in our institute who weredoing their rotations in neurovascular surgery would learnto use the Dextroscope simulator and be able to appraise theAVM prior to the surgery with the neurovascular surgeonand discuss the various approaches and potential difficultieswith greater emphasis. The utility in using the workstation
Fig. 3 Three dimensional model of the unique individualisedanatomy and the relation of AVM with its feeders; venous drainageto the nidus.A. posterior view; b anterior view ( red represents arteries;blue represents veins)
460 I. Ng et al.

to understand pathology and surgical concepts was clearlyfelt to supplement and augment the learning process.
There are certain drawbacks of the VR simulator in itscapability to provide a full immersive experience. In fact,current systems such as the one we have described, is anaugmented virtual reality platform rather than a fullyimmersive one; valuable elements that are lacking wouldbe the lack of tactile feedback. This could be achieved bythe use of haptics and there are already software andhardware algorithms that provide rudimentary componentsof such feedback [14].
Another drawback would be the inability of thesimulator to model brain shift. The planning with pre-operatively obtained data worked best for small andsuperficial lesions which required little brain retraction. Inthe advanced stages of most operations, brain shift made itincreasingly difficult to correlate the pre-operatively
obtained surgical plan with the actual surgical site. How-ever, we were still able to identify major vascular land-marks. Re-establishment of the surgical plan using freshdata sets from intra-operative CT and MR imaging wouldbe a major improvement.
The final quality of the 3D image on the simulator isvery much dependant on the quality of the source images/scans fed into it, i.e. if a particular feeder or draining vein isnot clearly visualised on the source images on MRangiography or MR venography, visualisation may not bepossible on the simulator.
In three patients [15, 17, 21] the smaller draining veinswere not clearly visualised on the source images (MRA,MRV) thus resulting in the final 3D image after segmen-tation not corresponding to the intra-operative findings.Incorporation of Digital Subtraction Angiography (DSA)images in the simulator would overcome this problem.
Fig. 4 Stereoscopic visualisation of the above images (to use red-blueglasses). a posterior; b anterior view, c close up view from rightlateral, showing the feeding PCA and right middle meningeal artery as
well as mixed arterio —venous flow signal in the area of the nidus. dCropping the MRV from the top reveals the main PCA feeder (thevirtual instrument is pointing at it)
Surgical planning for microsurgical excision of cerebral arterio-venous malformations using virtual reality technology 461
However, currently the system is limited to processingtomographic data (data in slices) which is then recon-structed as a volume. DSA images which are delivered as2D projection data sets in our unit cannot be processed inthe simulator.
Finally, there is a need for some time investment tofamiliarise oneself with both the hardware and software ofthe Dextroscope before its full capabilities can be exploited.From our experience in the preparation for procedures, theprocess of data fusion and segmentation of vessels took anaverage of 30 min per patient. Another 20 min were neededfor surgical planning using the 3D virtual images. Overall,the time taken to plan each individual procedure does notgenerally extend beyond an hour.
Once this is mastered however, the time taken to planeach individual operation does not generally extend beyondan hour.
Conclusion
Arterio-venous malformations can be resected with goodresults and greater confidence when their complex angio-architecture is clarified by the virtual reality simulator(Dextroscope) which combines all the information obtainedfrom various imaging modalities. Our experience indicatesthat the quality and flow of surgery has been muchimproved with the introduction of the pre-surgical planningwith the virtual reality 3D technology.
Disclosure Ralf A. Kockro is a co-founder of Volumeinteractions Pte Ltd, which developed the technologiesdescribed in this paper.
The other authors have no financial interests whatsoeverin the technologies described in this paper.
Fig. 5 Reconstructed MRA identifying the critical feeders pre-surgically for early division: feeder 1 - parieto-occipital branch ofposterior cerebral artery arising mainly from the foetal type posteriorcommunicating artery entering nidus anterior-inferiorly and medially;feeder 2 - fistula from the parietal branch of parieto-occipital branchentering a venous pouch; feeder 3 - occipital branches from the PCAentering the nidus inferiorly and more posteriorly; feeder 4 and 5 -hypertrophied branches of the extra- cranial occipital artery; feeder 6 -branches from the middle meningeal artery. A left posterior obliqueview; B left inferior-superior view
Fig. 6 Post-operative angio-gram demonstrating completeresection of the AVM
462 I. Ng et al.
References
1. Albert P (1982) Personal experience in the treatment of 178 casesof arterio-venous malformations of the brain. Acta Neurochir(Wien) 61:207–226. doi:10.1007/BF01740086
2. Bambakidis NC, Sunshine JL, Faulhaber PF, Tarr RW, Selman WR,Ratcheson RA (2001) Functional evaluation of arterio-venous malfor-mations. Neurosurg Focus 11(5):e2. doi:10.3171/foc.2001.11.5.3
3. Bernardo A, Preul MC, Zabramski JM, Spetzler RF (2003) Athree dimensional interactive virtual dissection model to simulatetranspetrous surgical avenues. Neurosurgery 52(3):499–505
4. Davis C, Simon L (1985) The management of cerebral arterio-venous malformations. Acta Neurochir (Wien) 74:4–11. doi:10.1007/BF01413268
5. Du R, Keyoung HM, Dowd CF, Young WL, Lawton MT (2007)The effects of diffuseness and deep perforating artery supply onoutcomes after microsurgical resection of brain arterio-venousmalformations. Neurosurgery 60:638–646. doi:10.1227/01.NEU.0000255401.46151.8A
6. Henn JS, Lemole GM Jr, Ferreira MA, Gonzalez LF, Schornak M,Preul MC, Spetzler RF (2002) Interactive stereoscopic virtual reality:a new tool for neurosurgical education. J Neurosurg 96(1):144–149
7. Henn JS, Turner DA (2005) Neurosurgery teaching techniquesand neurosurgical simulation. In: Truner DA (ed) ModernNeurosurgery- clinical translation of neuroscience advances.CRC, Florida, pp 291–302
8. Heros RC, Korosue K, Diebold PM (1990) Surgical excision ofcerebral arterio-venous malformations: late results. Neurosurgery26:570–578. doi:10.1097/00006123-199004000-00003
9. Heros CR, Morcos JJ (2000) Cerebrovascular surgery: pastpresent and future. Neurosurgery 47(5):1007–1033. doi:10.1097/00006123-200011000-00001
10. Kikuta K, Takagi Y, Nozaki K, Hanakawa T, Okada T, Miki Y,Fushimi Y, Fukuyama H, Hashimoto N (2006) Early experiencewith 3-T magnetic resonance tractography in the surgery ofcerebral arterio-venous malformations in and around the visualpathway. Neurosurgery 58(2):331–337
11. Kockro RA, Serra L, Yeo TT, Chan C, Sitoh YY, Chua GG, Lee E,Hoe LY, Ng H, Nowinski W (2000) Planning and simulation ofneurosurgery in a virtual reality environment. Neurosurgery 46(1):118–137
12. Larsen OV (2001) The Virtual brain project: development of aneurosurgical simulator. Stud Health Technol Inform 81:256–262
13. Lawton MT, Du R, Tran MN, Achrol AS, McCulloch CE, JohnstonSC et al (2005) Effect of presenting haemorrhage on outcome aftermicrosurgical resection of brain arterio-venous malformations. Neuro-surgery 56(3):485–493. doi:10.1227/01.NEU.0000153924.67360.EA
14. Lemole GM, Banerjee PP, Luciano CMS, Neckrysh S, Charbel FT(2007) Virtual reality in neurosurgical education: part taskventriculostomy simulation with dynamic visual and hapticfeedback. Neurosurgery 61(1):142–149. doi:10.1227/01.neu.0000279734.22931.21
15. Mathiessen T, Peredo I, Edner G, Kihlstrom L, Svensson M,Ulfarsson E (2007) Neuronavigation for arterio-venous malfor-mation surgery by intraoperative three dimensional ultrasoundangiography. Neurosurgery 60:345–350
16. Muacevic A, Steiger HJ (1999) Computer assisted resection ofcerebral arterio-venous malformations. Neurosurgery 45(5):1164.doi:10.1097/00006123-199911000-00030
17. Parkinson D, Bachers G (1980) Arterio-venous malformations.Summary of 100 consecutive supratentorial cases. J Neurosurg53:285–299
18. Radetzky A (2000) ROBO-SIM: a simulator for minimallyinvasive neurosurgery using an active manipulator. Stud HealthTechnol Inform 77:1165–1169
19. Russell SM, Woo HH, Joseffer SS, Jafar JJ (2002) Role offrameless stereotaxy in the surgical treatment of cerebral arterio-venous malformations: techniques and outcomes in a controlledstudy of 44 consecutive patients. Neurosurgery 51(5):1108–1118.doi:10.1097/00006123-200211000-00002
20. Spetzler RF, Martin NA (1986) A proposed grading system forarterio-venous malformations. J Neurosurg 65:476–483
21. Spicer MA, Apuzzo MLJ (2003) Virtual reality neurosurgery andthe contemporary landscape. Neurosurgery 52(3):489–497
22. Strauss G, Trantakis C, Nowatius E, Falk V, Mass H, Cakmak K,Strauss E, Dietz A, Meixenberger J, Bootz F, Kuhnnapfel U(2005) Virtual training in head and neurosurgery. Laryngorhinoo-tologie 84(5):335–344
23. Sugita K (1985) Microneurosurgical Atlas. Springer-Verlag,Berlin, pp 136–177
24. Unsgaard G, Ommedal S, Rygh OM, Lindseth F (2005) Operationof arterio-venous malformations assisted by stereoscopic naviga-tion controlled display of preoperative magnetic resonanceangiography and intra-operative ultrasound angiography. Neuro-surgery 56:281–290. doi:10.1227/01.NEU.0000157005.51053.41
25. Yarsagil MG (1988) Microneurosurgery, Vol III B: AVM of theBrain. George Thieme Verlag, Stuttgart, pp 25–53
Comments
Ng and colleagues provide a manuscript prospectively evaluatingplanning of surgery of cerebral arteriovenous malformations with avirtual reality platform workstation in 24 patients. Patient specific datafrom different imaging techniques were co-registered and displayed as astereoscopic object in the virtual reality planning platform, allowingmoves and manipulations of the object. They conclude that this system ishelpful in comparing different surgical strategies, enhancing intra-operative spatial orientation, and increasing surgeon’s confidence. Thismanuscript follows a more extensive description of the stereoscopicvirtual reality system published by the senior author in 2000.
Virtual reality training of students and surgeons is becoming moreand more important, and the system described seems to be animportant step in this direction.
However, one has also to keep in mind the shortcomings of thesystem described:
Even though MR- and CT-angiography are becoming more andmore important, digital subtraction angiography is still the key pointsin analysing the anatomy of cerebral arteriovenous malformations andcannot be integrated in the virtual reality workstation described.
The time necessary to co-register the different data sets, to performsegmentation of important structures, and to plan surgery with thesedata using the described system takes about one hour.
Data used in the system described are preoperatively generated.Intra-operatively there is the problem of brain shift, reducing thereliability of the system.
Marcus ReingesAachen University, Germany
This is a well-written manuscript on surgical planning for microsurgicalexicision of cerebral arteriovenous malformations using virtual realitytechnology. Surgery for the cerebral arteriovenous malformationsespecially with complex vascular structures needs detailed preoperativeevaluation of angigorams including feeding arteries and draining veinsas well as the nidus itself. As the authors conclude, surgical planning ofresection of arteiorvenous malformations with a virtual reality systemthus must be very helpful in establishing a good and accurate surgery.
Kazuhiro HongoShinshu University School of Medicine, Matsumoto, Japan
Surgical planning for microsurgical excision of cerebral arterio-venous malformations using virtual reality technology 463
Copyright © 2022 FDOKUMEN




















