Intraradicular and intradural lumbar disc herniation: Experiences with nine cases
8
ELSEVIER SDine INTRARADIC~LAR AND INTRADURAL LUMBAR DISC HERNIATION: EXPERIENCES WITH NINE CASES Ciuseppe Schisano, M.D.; Antonio France, M.D.; and Pierpaolo Nina, M.D. Department of Neurosurgery, Nuouo PelLegrini Hospital, Napoli, Italy Schisano Ci, France A, Nina P. lntraradicular and intradural lum- bar disc herniation: experiences with nine cases. Surg Neural 1995;44:536-43. BACKGROUND lntraradicular or intradural disc herniation is a very rare complication of spinal degenerative processes. The aim of our study is to analyze the clinical spectrum, the mech- anism, and the treatment of this acute spinal pathology. METHODS Retrospective clinical examination was performed in nine personal cases of intradural disc herniation: among these, six were associated with lateral perforation, the remaining three with intradural herniation and ventral perforation. A review of the literature concerning mainly the frequency pathogenesis and diagnosis of intradural disc herniation has also been done. RESULTS Nine cases of intradural herniations comprise 1.51% of the 593 cases of ruptured lumbar disc that underwent surgery from 1980to 1992.The site most frequently in- volved is at level L4-L5, and 30% of patients have previ- ously undergone surgery for lumbar disc herniation. Most patients reported in literature and in our present series have been complaining of a chronic history of sciatica, complicated later by bilateral neurologic signs. In the present series,diagnosiswas obtained by means of myelography and computerized tomography; magnetic resonance imaging was performed in one case. All pa- tients underwent surgery, reporting excellent results in five cases and good results in the other four. Surgery was performed either with an interlaminar approach or with a bilateral laminectomy in casesof ventral perforation. CONCLUSIONS There is no typical neuroradiologic picture of intraradicu- lar herniation, while a total or subtotal block is frequently observed in intradural ventral perforations. Dural perfo- ration is often an unexpected intraoperative finding. Sur- gical treatment is always necessary. Favorable results are obtained if surgical treatment is carried out before the neurologic deficit becomestoo pronounced. Presented at the Scandinavian Congress of Neurosurgery, UppsaIa, Sweden, June 9-12, 1993. Address reprint requests to: Giuseppe Schisano, M.D., Discesa Coroglio, 22, 80123 Napoli, Italy. Received November 22, 1994; accepted March 22, 1995. 0090-3019/95/$15.00 SSDI 0090-3019(95)002483 KEY WORDS Lumbar disc, intradural disc rupture, intraradicular disc rup ture, cauda equina syndrome, X-ray diagnosis. I n the natural history of disc pathology, intradural lumbar disc herniation is a rare event; this con- dition was first described by Dandy [9] in 1942. Since that time until 1988, only 70 [ 171 cases were reported. In this paper the most important literature has been revised and 18 other cases have been added to the ones published by Kataoka [17] (up to 1988), and others published subsequently (from 1988 to 1991). Most cases refer to patients with ventral dural herniation; dural perforation at the radicular sheath level caused by fragments of lumbar intervertebral disc was first documented in 1984 [2]. In the current report, nine cases of lumbar disc herniation with intradural perfora- tion are presented; all patients were operated on in the Department of Neurosurgery of Nuovo Pel- legrini Hospital, Naples. They represent 1.51% of the 593 cases of disc herniation operated on be- tween 1980 and 1992. CASE MATERIAL Out of a series retrospectively studied of 593 patients suffering from lumbar disc herniation, nine cases of intradural perforation were selected and, in relation to the localization of dural lesion, ventral or lateral near the root’s axilla, they were divided into two groups. Lateral dural perforation was observed in six cases (Table l), three females and three males ranging in age from 45 to 72 years. As to the length of neurologic symptoms, it must be said that two patients were affected for several years by pain, whereas three other pa- 0 1995 by EIsevIer Science Inc. 655 Avenue of the Americas, New York, NY 10010
Transcript of Intraradicular and intradural lumbar disc herniation: Experiences with nine cases
ELSEVIER
SDine
INTRARADIC~LAR AND INTRADURAL LUMBAR DISC HERNIATION: EXPERIENCES WITH NINE CASES Ciuseppe Schisano, M.D.; Antonio France, M.D.; and Pierpaolo Nina, M.D. Department of Neurosurgery, Nuouo PelLegrini Hospital, Napoli, Italy
Schisano Ci, France A, Nina P. lntraradicular and intradural lum- bar disc herniation: experiences with nine cases. Surg Neural 1995;44:536-43.
BACKGROUND lntraradicular or intradural disc herniation is a very rare complication of spinal degenerative processes. The aim of our study is to analyze the clinical spectrum, the mech- anism, and the treatment of this acute spinal pathology.
METHODS Retrospective clinical examination was performed in nine personal cases of intradural disc herniation: among these, six were associated with lateral perforation, the remaining three with intradural herniation and ventral perforation. A review of the literature concerning mainly the frequency pathogenesis and diagnosis of intradural disc herniation has also been done. RESULTS Nine cases of intradural herniations comprise 1.51% of the 593 cases of ruptured lumbar disc that underwent surgery from 1980 to 1992. The site most frequently in- volved is at level L4-L5, and 30% of patients have previ- ously undergone surgery for lumbar disc herniation. Most patients reported in literature and in our present series have been complaining of a chronic history of sciatica, complicated later by bilateral neurologic signs. In the present series, diagnosis was obtained by means of myelography and computerized tomography; magnetic resonance imaging was performed in one case. All pa- tients underwent surgery, reporting excellent results in five cases and good results in the other four. Surgery was performed either with an interlaminar approach or with a bilateral laminectomy in cases of ventral perforation. CONCLUSIONS There is no typical neuroradiologic picture of intraradicu- lar herniation, while a total or subtotal block is frequently observed in intradural ventral perforations. Dural perfo- ration is often an unexpected intraoperative finding. Sur- gical treatment is always necessary. Favorable results are obtained if surgical treatment is carried out before the neurologic deficit becomes too pronounced.
Presented at the Scandinavian Congress of Neurosurgery, UppsaIa, Sweden, June 9-12, 1993.
Address reprint requests to: Giuseppe Schisano, M.D., Discesa Coroglio, 22, 80123 Napoli, Italy.
Received November 22, 1994; accepted March 22, 1995.
0090-3019/95/$15.00 SSDI 0090-3019(95)002483
KEY WORDS Lumbar disc, intradural disc rupture, intraradicular disc rup ture, cauda equina syndrome, X-ray diagnosis.
I n the natural history of disc pathology, intradural lumbar disc herniation is a rare event; this con-
dition was first described by Dandy [9] in 1942. Since that time until 1988, only 70 [ 171 cases were reported.
In this paper the most important literature has been revised and 18 other cases have been added to the ones published by Kataoka [17] (up to 1988), and others published subsequently (from 1988 to 1991). Most cases refer to patients with ventral dural herniation; dural perforation at the radicular sheath level caused by fragments of lumbar intervertebral disc was first documented in 1984 [2]. In the current report, nine cases of lumbar disc herniation with intradural perfora- tion are presented; all patients were operated on in the Department of Neurosurgery of Nuovo Pel- legrini Hospital, Naples. They represent 1.51% of the 593 cases of disc herniation operated on be- tween 1980 and 1992.
CASE MATERIAL Out of a series retrospectively studied of 593 patients suffering from lumbar disc herniation, nine cases of intradural perforation were selected and, in relation to the localization of dural lesion, ventral or lateral near the root’s axilla, they were divided into two groups. Lateral dural perforation was observed in six cases (Table l), three females and three males ranging in age from 45 to 72 years. As to the length of neurologic symptoms, it must be said that two patients were affected for several years by pain, whereas three other pa-
0 1995 by EIsevIer Science Inc. 655 Avenue of the Americas, New York, NY 10010
lntraradicular and Intradural Lumbar Disc Herniation
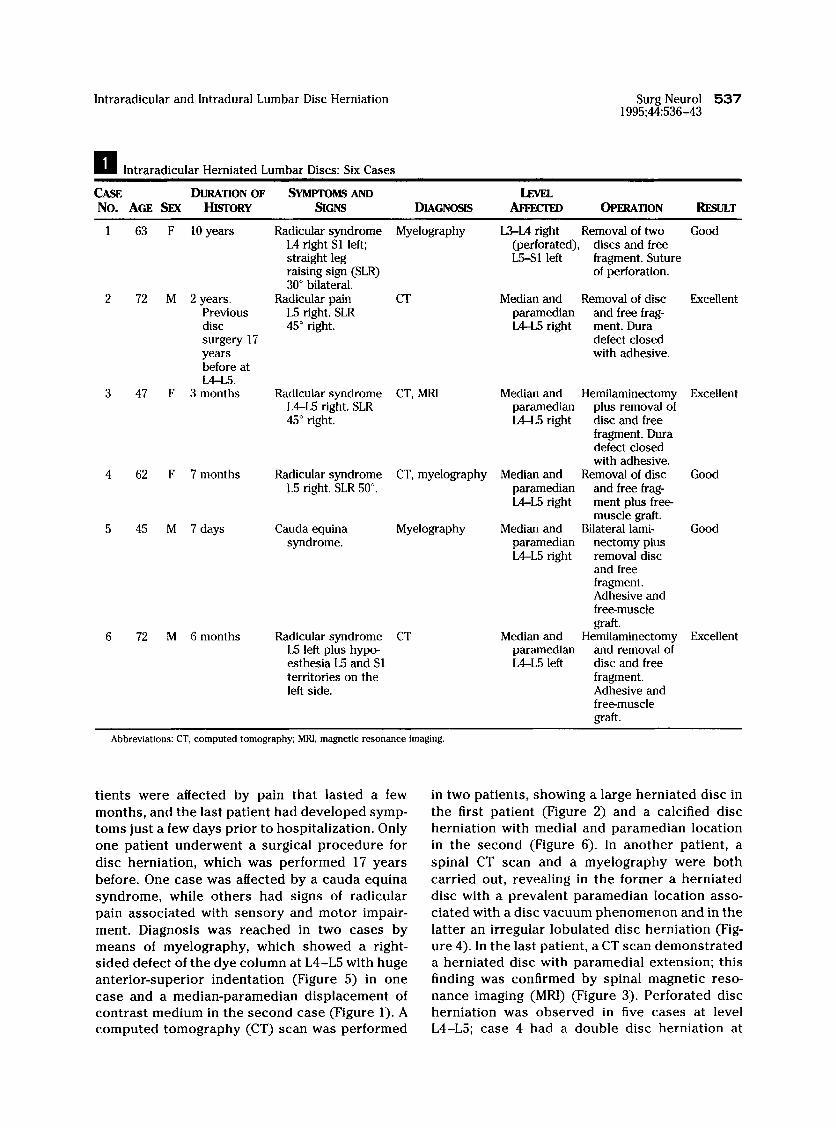
II lntraradicular Herniated Lumbar Discs: Six Cases
Surg Neurol 537 1995;44:536-43
CASE DURATION OF SYMPTOMS AND No. AGE Snr I-hSORY !3cNs DIAGNOSIS AFFECTED OPERATION RJ!SlJlT
63 F 10 years Radicular syndrome L4 right Sl left; straight leg raising sign (SLR) 30” bilateral.
72 M 2 years. Radicular pain Previous L5 right. SLR disc 45” right. surgery 17 years before at L4-L5.
47 F 3 months Radicular syndrome L4-L5 right. SLR 45” right
62 F 7 months
45 M 7 days
72 M 6 months
Radicular syndrome L5 right. SLR 50”.
Cauda equina syndrome.
Radicular syndrome L5 left plus hype esthesia L5 and Sl territories on the left side.
Myelography L3-L4 right Removal of two Good (perforated), discs and free L5-Sl left fragment. Suture
of perforation.
CT Median and Removal of disc Excellent paramedian and free frag- LPL5 right ment. Dura
defect closed with adhesive.
CT, MRf Median and Hemilaminectomy Excellent paramedian plus removal of L4-L5 right disc and free
fragment. Dura defect closed with adhesive.
CT, myelography Median and Removal of disc Good paramedian and free frag- LPL5 right ment plus free-
muscle grak Myelography Median and Bilateral lami- Good
paramedian nectomy plus LPL5 right removal disc
and free fragment. Adhesive and freemuscle graft.
CT Median and Hemilaminectomy Excellent paramedian and removal of LPL5 left disc and free
fragment. Adhesive and freemuscle graft.
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging.
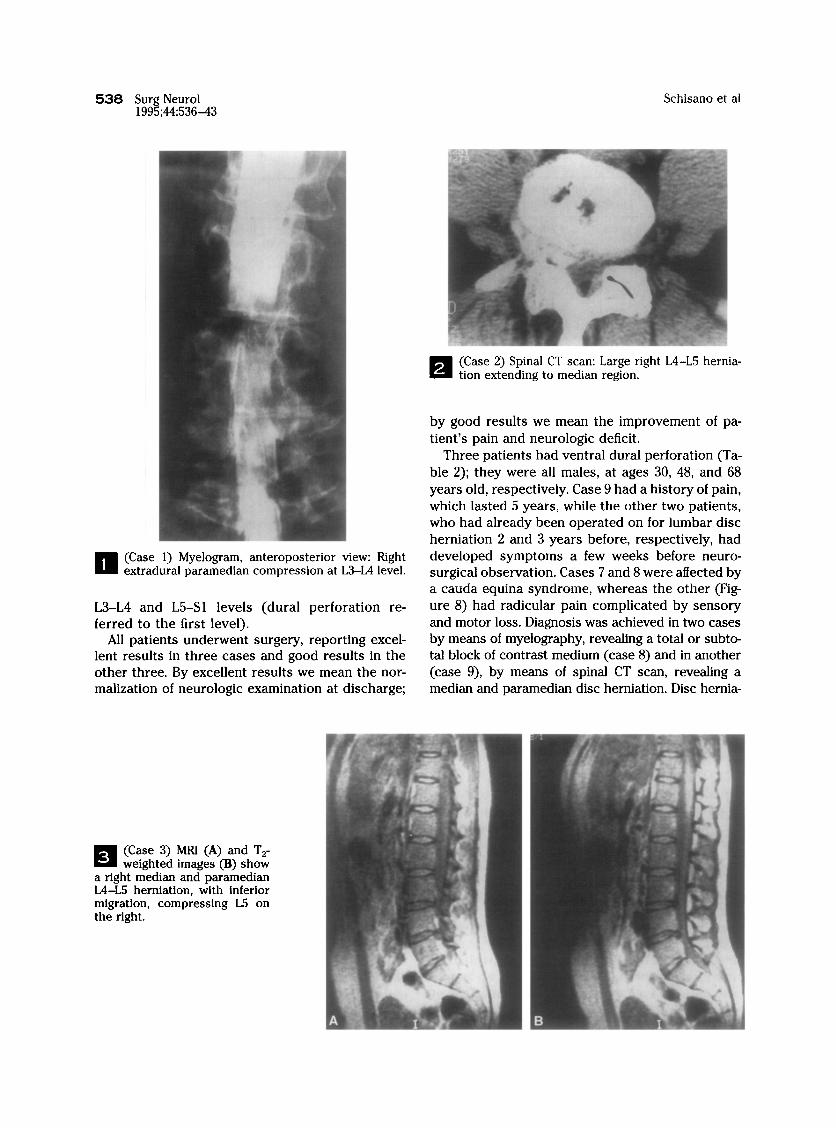
tients were affected by pain that lasted a few in two patients, showing a large herniated disc in months, and the last patient had developed symp- the first patient (Figure 2). and a calcified disc toms just a few days prior to hospitalization. Only herniation with medial and paramedian location one patient underwent a surgical procedure for in the second (Figure 6). In another patient, a disc herniation, which was performed 17 years spinal CT scan and a myelography were both before. One case was affected by a cauda equina carried out, revealing in the former a herniated syndrome, while others had signs of radicular disc with a prevalent paramedian location asso- pain associated with sensory and motor impair- ciated with a disc vacuum phenomenon and in the ment. Diagnosis was reached in two cases by latter an irregular lobulated disc herniation (Fig- means of myelography, which showed a right- ure 4). In the last patient, a CT scan demonstrated sided defect of the dye column at L4-L5 with huge a herniated disc with paramedial extension; this anterior-superior indentation (Figure 5) in one finding was confirmed by spinal magnetic reso- case and a median-paramedian displacement of nance imaging (MRI) (Figure 3). Perforated disc contrast medium in the second case (Figure 1). A herniation was observed in five cases at level computed tomography (CT) scan was performed L4-L5; case 4 had a double disc herniation at
538 Surg Neurol 1995;44:536-43
Schisano et al
II (Case 1) Myelogram, anteroposterior view: Right extradural paramedian compression at L3-L4 level.
L3-L4 and L5-Sl levels (dural perforation re- ferred to the first level).
All patients underwent surgery, reporting excel- lent results in three cases and good results in the other three. By excellent results we mean the nor- malization of neurologic examination at discharge;
q (Case 2) Spinal CT scan: Large right L4-L5 hernia- tion extending to median region.
by good results we mean the improvement of pa- tient’s pain and neurologic deficit.
Three patients had ventral dural perforation (Ta- ble 2); they were all males, at ages 30, 48, and 68 years old, respectively, Case 9 had a history of pain, which lasted 5 years, while the other two patients, who had already been operated on for lumbar disc herniation 2 and 3 years before, respectively, had developed symptoms a few weeks before neuro- surgical observation. Cases 7 and 8 were affected by a cauda equina syndrome, whereas the other (Fig- ure 8) had radicular pain complicated by sensory and motor loss. Diagnosis was achieved in two cases by means of myelography, revealing a total or subto- tal block of contrast medium (case 8) and in another (case 9), by means of spinal CT scan, revealing a median and paramedian disc herniation. Disc hernia-
(Case 3) MRl (A) and T,- weighted images (B) show
a right median and paramedian L4-L5 herniation, with inferior migration, compressing L5 on the right.
lntraradicular and Intradural Lumbar Disc Herniation Surg Neurol 539 1995;44:536-43
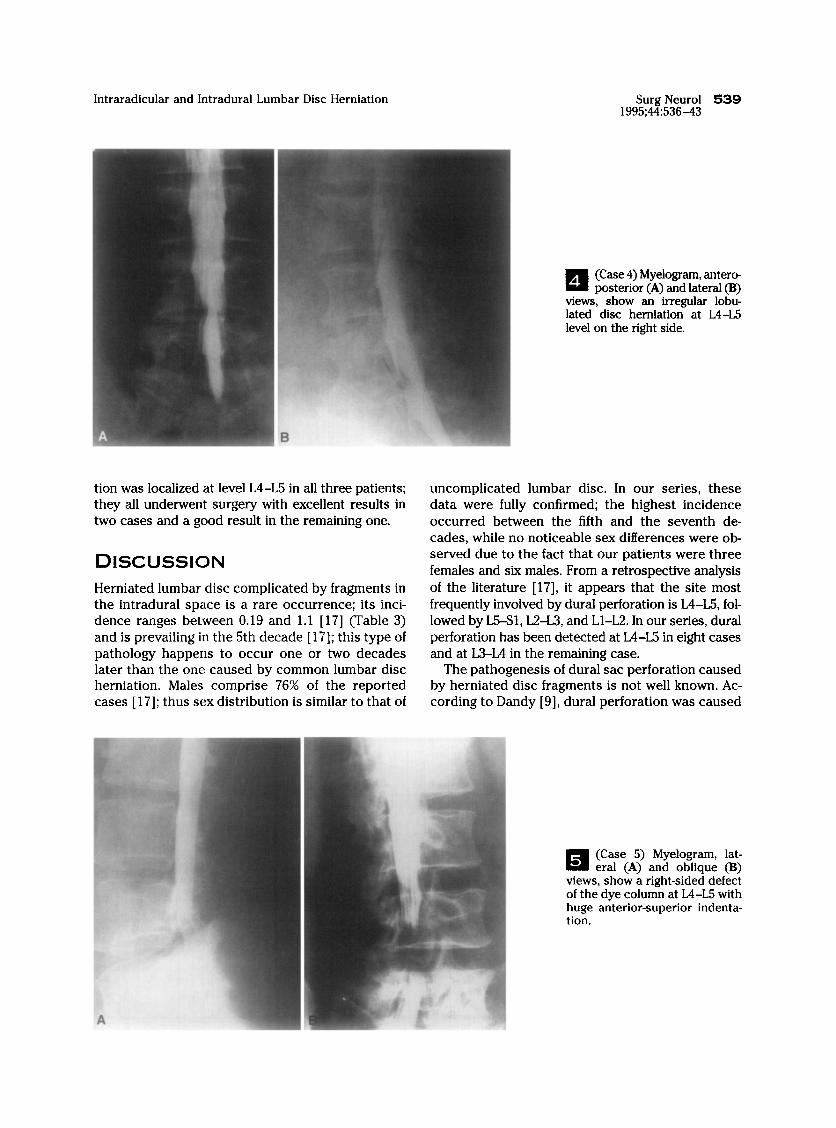
q A view: lated level
(Case 4) Myelogram, antero posterior (A) and lateral (B)
5, show an irregular lobu- disc hemiation at L4-L5
on the right side.
tion was localized at level L4-L5 in all three patients; they all underwent surgery with excellent results in two cases and a good result in the remaining one.
DISCUSSION Herniated lumbar disc complicated by fragments in the intradural space is a rare occurrence; its inci- dence ranges between 0.19 and 1.1 [ 171 (Table 3) and is prevailing in the 5th decade [ 171; this type of pathology happens to occur one or two decades later than the one caused by common lumbar disc herniation. Males comprise 76% of the reported cases [ 171; thus sex distribution is similar to that of
uncomplicated lumbar disc. In our series, these data were fully confirmed; the highest incidence occurred between the fifth and the seventh de- cades, while no noticeable sex differences were ob- served due to the fact that our patients were three females and six males. From a retrospective analysis of the literature [17], it appears that the site most frequently involved by dural perforation is L4-L5, fol- lowed by L5S1, L2-L3, and Ll-L2. In our series, dural perforation has been detected at L4-L5 in eight cases and at L3-L4 in the remaining case.
The pathogenesis of dural sac perforation caused by herniated disc fragments is not well known. Ac- cording to Dandy [9], dural perforation was caused
(Case 5) Myelogram, lat- eral (A) and oblique (B)
views, show a right-sided defect of the dye column at L4-L5 with huge anterior-superior indenta- tion.
540 Surg Neurol 1995;44:536-43
Schisano et al
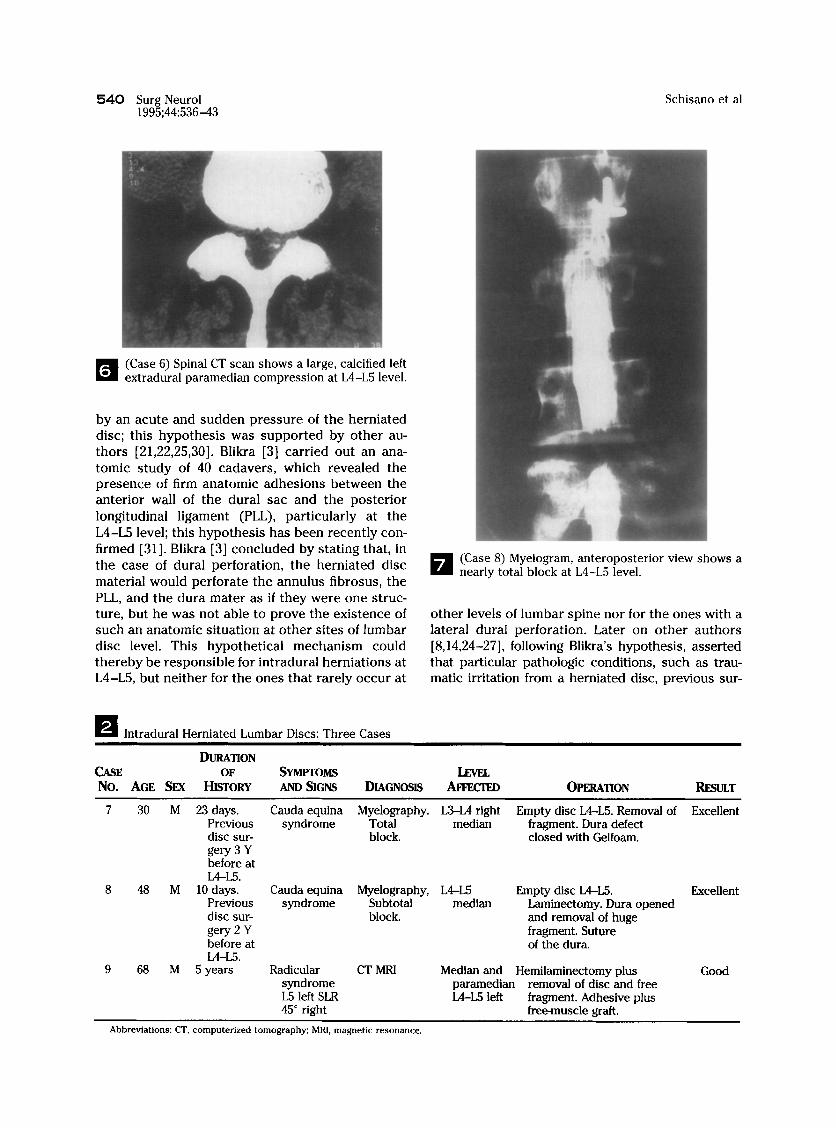
H - (Case 6) Spinal CT scan shows a large, calcified left extradural paramedian compression at L4-L5 level.
by an acute and sudden pressure of the herniated disc; this hypothesis was supported by other au- thors [21,22,25,30]. Blikra [3] carried out an ana- tomic study of 40 cadavers, which revealed the presence of firm anatomic adhesions between the anterior wall of the dural sac and the posterior longitudinal ligament (PLL), particularly at the L4-L5 level; this hypothesis has been recently con- firmed [31]. Blikra [3] concluded by stating that, in the case of dural perforation, the herniated disc material would perforate the annulus fibrosus, the PLL, and the dura mater as if they were one struc- ture, but he was not able to prove the existence of such an anatomic situation at other sites of lumbar disc level. This hypothetical mechanism could thereby be responsible for intradural herniations at L4-L5, but neither for the ones that rarely occur at
(Case 8) Myelogram, anteroposterior view shows a nearly total block at L4-L5 level.
other levels of lumbar spine nor for the ones with a lateral dural perforation. Later on other authors [8,14,24-271, following Blikra’s hypothesis, asserted that particular pathologic conditions, such as trau- matic irritation from a herniated disc, previous sur-
q lntradural Herniated Lumbar Discs: Three Cases
DURATION CASE OF SYMPTOMS No. AGE SEX HISTORY AND SIGNS DIAGNOSIS AFFECTED OPER4TION RESULT
7 30 M 23 days. Cauda equina Myelography. L3-L4 right Empty disc L4-L5. Removal of Excellent Previous syndrome Total median fragment. Dura defect disc sur- block. closed with Gelfoam. gery3Y before at LPL5.
8 48 M 10 days. Cauda equina Myelography, L4-L5 Empty disc L4-L5. Excellent Previous syndrome Subtotal median Laminectomy. Dura opened disc sur- block. and removal of huge gery2Y fragment. Suture before at of the dura. L4-L5.
9 68 M 5 years Radicular CT MRf Median and Hemilaminectomy plus Good syndrome paramedian removal of disc and free L5 left SLR L4-L5 left fragment. Adhesive plus 45” right free-muscle graft.
Abbreviations: CT, computerized tomography; MRI, magnetic resonance.

Intraradicular and Intradural Lumbar Disc Herniation Surg Neurol 54 1 1995;44:536-43
q ’ (Case 9) Spinal CT scan shows a large left L4-L5 herniation extending to the medial region.
gery, and local inflammation [ 13,14,21,26,29] could have been potential causes of firm adhesions between the anterior part of the dura and the PLL, forming a very hard tissue similar to the one observed by Blikra [3] at L4-L5. Lesoin et al [20] indicated the possible existence of a posterior osteophytosis, which pre vented lateral disc herniation but indirectly could cause the medial herniation through the dura mater.
As far as the pathogenesis of disc herniation with lateral perforation was concerned, Barbera et al [ 21 supported the idea of a congenital weakness of the radicular sheath.
Seventy-nine percent of cases reported in litera- ture [ 171 had been suffering from low-back pain or sciatica for more than a year. Frequently a clinical history could last for several years. One case was reported with long-lasting symptoms for 34 years [12]. Only in five cases [4,6,16,21,28], an acute onset of clinical symptoms was observed; in the current series, we report three cases with a pain history that lasted 7, 10, and 23 days respectively. The 28% of cases described in literature [ 17,231 had been previously operated on for disc herniation, while in our current series three patients out of nine had already been operated on in the lumbar spine. Most patients in literature had thereby a history of low- back pain or chronic sciatica suddenly complicated by neurologic deficit causing often a cauda equina syndrome [23] or, in mild cases, neurologic signs often bilateral involving lumbar roots. In summary, it can then be said that the clinical syndrome of patients suffering from intradural perforated herni- ated disc is more severe than the one of patients suffering from uncomplicated lumbar disc hernia- tion. In the nine cases in our series, neurologic examination showed a cauda equina syndrome in three patients, while in six others, a severe radicu- lar syndrome with frequent motor and sensitive signs. As far as the localization of dural lesion is
El - Surgical specimen removed from the radicular sheath.
concerned, we must underline that no typical clin- ical syndrome has been observed, since the cauda equina syndrome was found in two cases (cases 7 and 8) with ventral dural lesion, and in another, with lateral dural perforation (case 5).
Preoperative diagnosis of dural perforation from disc herniation is rarely obtained. Myelography generally shows a total or subtotal block of contrast medium [ 191. Fardoun et al [ 121 studied a series of 21 patients from literature and found that in 90.5% there was a block; instead, in Kataoka’s review [ 171 a total block was observed in 71% and partial de- fects were noted in 11.5%. Therefore, in these two series published by Fardoun [ 121 and Kataoka [ 171 patients were likely to have herniations with ventral dural perforation. Hodge et al [ 141 pointed out that the presence of an irregular filling defect might have been indicative of an intradural disc herniation; they also emphasized the importance of utilizing metrizamide. Esposito et al [ 1 l] described one case (among the two they published) in which preoper- ative diagnosis was suspected because myelogra- phy showed an irregular dural mass. According to Graves et al [ 131, this method had better diagnostic accuracy in showing lobulate or irregular masses, suggestive of intradural lumbar disc herniation.
Incidence of Reported Intradural and Intraradicular Disc Herniation
AUTHOR(S) YEAR PERCENT
Dandy Slater et al Peyser and Harari Carcavilla et al Lee and Fairholm Lesoin et al Schisano et al
1942 0.33 1965 0.20 1977 0.28 1982 0.27 1983 1984 1993

542 Surg Neural Schisano et al 1995;44:536-43
Anda et al [l] stated that the presence of gas in intradiscal space (vacuum phenomenon) might be indicative of intradural perforation, even if this con- dition is unfrequent and often aspecific. Recently Holtas et al [15] have compared MRI and myelog- raphy in a case of lumbar intradural disc herniation and have concluded that MIU is superior to myelog- raphy in visualizing all components of the hernia- tion, including adhesions and inflammatory tissue. Smith [26] stressed the importance of analyzing liquor macrophages containing fibrocartilaginous material from the perforated disc tissue in subdural space. In five patients of the current series, myelog- raphy showed a total block in one case (case 7) and a subtotal one in case 8 (Figure 7). The filling defect with the characteristics of irregularity described by Hodge [14] was found in two cases (Figures 4 and 5). In three patients a spinal CT scan without con- trast demonstrated aspecific signs of disc hernia- tion, while in one patient diagnosis was obtained by spinal CT, as well as by myelography (Figure 4). In case 3, both a CT scan and a spinal MIZI (Figure 3) were carried out, the former showing aspecific signs of a paramedian disc herniation, the latter confirming CT findings.
more evident from a clinical point of view. The presence of a tense dura and palpation of an intra- dural mass associated with observation of an empty intervertebral disc is indicative of the existence of a fragment within the dural sac. In literature [ 71 it has been suggested the necessity of a dural sac opening in order to reduce the pressure in intradural space, as well as to visualize and remove all herniated fragments. In two out of three patients in our series, a laminectomy was performed; the dural sac was widely opened only in one of them (case 7) fol- lowed by the suturing of the dura mater. In the other two cases, however, the defect was covered by a free-muscle graft or an adhesive. According to Koivukangas et al [ 181, surgical treatment could be facilitated by the usage of intraoperative ultrasound imaging, indicating the precise location and number of the disc’s fragments within the intradural space.
Surgical treatment of perforated lumbar disc her- niation is an absolute requirement. In case of lateral perforation, the dural lesion is often an unexpected surgical event. A discal fragment is found inside the sheath or in the dura nearby the radicular sheath. After removing the fragment the leakage of cerebro- spinal fluid from the sheath or from the dura lateral wall is observed, indicating the perforation’s site. In literature, it has been mentioned that the radicular sheath should not be opened routinely; however, this procedure should be undertaken in cases where, after the removal of the intradural fragment, a tense or dilated radicular sheath is found, prob- ably indicating the existence of another fragment [20]. In five out of six patients with lateral dural per- foration (Table 1) the surgical approach was inter- laminar, whereas in the remaining case a bilateral laminectomy was performed, owing to a cauda equina syndrome. In the present series no opening of the radicular sheath was performed, due to the fact that the sequestrated fragments were always removed ex- tradurally (Figure 9); moreover, after the removal and the complete disc evacuation, the dural defect was closed with a free-muscle graft and/or Aron adhesive (Eff ekappa Medica, Trieste, Italy).
After an accurate analysis of the literature and our own cases, it appears that the prognosis of this pathology is quite satisfactory and is closely related with preoperative duration and degree of neuro- logic symptoms. It may be worthwhile to emphasize that a prompt surgical intervention [5,19] facilitates the disappearance of the radicular pain and the improvement of neurologic deficits.
We are grateeful to Mercedes Gobbo for preparing the manu- script.
REFERENCES 1.
2.
3.
4.
5.
6.
7.
Generally, patients with ventral dural perforation have more severe clinical signs accompanied by a very distinctive neuroradiologic picture (total or subtotal block); hence, a laminectomy or hemilam- inectomy is often performed on the side that is
8.
9.
10.
Anda S, Dale LG, Vassal J. Intradural disc herniation with vacuum phenomenon: CT diagnosis. Neuroradi- ology 1987;29:407. Barbera J, Gonzalez-Darder J, Garcia-Vazquez F. In- traradicular herniated lumbar disc: case report. J Neurosurg 1984;60:858-60. Blikra G. Intradural herniated lumbar disc. J Neuro- surg 1969;31:676-9. Cambria S, Moraci A, Cardia E. Ernia discale lombare sottodurale (presentazione di un case). Chirurgia Triveneta 1974;14:211-4. Cantini R, Ravelli V. Ernia de1 discolombare intra- durale: contribute clinico. (In Italian). J Orthop Trau- matol 1986;281-4. Chowdhary V, Greenavar S. Intradural lumbar disc protrusion: a case report. Acta Orthop Stand 1987; 58:431-3. Ciappetta P, Delfini R, Cantore GP. lntradural lumbar disc hernia: description of three cases. Neurosurgery 1981;8:104-7. Coppola AR. Pseudoneurilemmoma of the spinal ca- nal. South Med J 1979;72:1925-6. Dandy WE. Serious complications of ruptured inter- vertebral disc. JAMA 1942;119:474-7. Ergungor MF, Kars ZH. Intraradicular herniation of a lumbar disc: a case report. Neurosurgery 1987;21: 909-11.
11. Esposito S, Canova A, Massari L, Pirozzi L, Kropp F.

Intraradicular and Intradural Lumbar Disc Herniation
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
Le ernie discali Iombari intradurali: considerazioni su due casi. Riv Neurobiol 1980;26(2):213-8. Fardoun R, Finn S, Boasson M. Hernie discale lom- baire intradurale: a propos dune observation. Ar- chives Medicales de 1’Ovest 1980;12:439-46. Graves VB, Finney HL, Mailander J. Intradural lumbar disk herniation. AJNR 1986;7:495-7. Hodge CJ, Binet EF, Kiffer SA. Intradural herniation of lumbar intervertebral discs. Spine 1978;3:346-50. Holtas S, Nordstrijm CH, Larsson EM, Petterson H. MR imaging of intradural disk herniation. J Comput Assist Tomogr 1987;11:353-6. Isobe K, Yamacla H, Tsuji H. Intradural lumbar disc hernia: report of three cases. (In Japanese). Clin Or- thop Surg 1979;14:185-7. Kataoka 0, Nishibayashi Y, Sho T. Intradural lumbar disc herniation: report of three cases with a review of the literature. Spine 1988;529-33. Koivukangas J, Tervonen 0. Intraoperative ultra- sound imaging in lumbar disc herniation surgery. Acta Neurochir (Wien) 1989;98:47-54. Lee ST, Fairholm D. Intradural rupture of lumbar in- tervertebral disc. Can J Neurol Sci 1983;10:192-4. Lesoin F, Duquennoy B, Rousseaux M, Servato R, Jomin M. Intradural rupture of lumbar intervertebral disc: report of three cases with review of the Iitera- ture. Neurosurgery 1984;14:728-31. Lyons AE, Wise BL. Subarachnoid rupture of interver- tebral disc fragments. J Neurosurg 1961;18:242-4. Marega T. Due casi di ernia de1 disco lombare espulsa nel sacco durale. Arch Putti Chir Organi Mov 1968;23: 467-74. Mikula F von, Zapletal B, Fiser Z. Intradurale prolapse der lenderbandscheibe. ZBL Neurochir 1960;20:326- 34. Peyser E, Harari A. Intradural rupture of lumbar in- tervertebral disc: report of two cases with review of the literature. Surg Neurol 1977;8:95-6. Slater RA, Pineda A, Porter RW. Intradural herniation of lumbar intervertebral discs. Arch Surg 1965;90: 266-9. Smith RV. Intradural disc rupture. J Neurosurg 1981; 55:117-20. Teng P, Papatheodorou C. Intradural dislocation of lumbar disc. Neurochirurgia (Stuttg) 1964;7:57-63. Thomalske G, Hohr G. Intradurale sequesterierung lumbaler diskus hernien unter besonderer beriick- sichtigung der achondroplasie. Nervenartz 1974;45: 376-9. Vas W, Holt MJ, Murray JK. Intrathecal herniation of a lumbar disc. J Can Assoc Radio1 1981;31:64-5. Wilson PJE. Cauda equina compression due to in- trathecal herniation of an intervertebral disk: a case report. Br J Surg 1962;49:423-6. Yildizhan A, Pasaoglu A, Okten T, Ekinci N, Aycan R, Aral 0. Intradural disc herniations: pathogenesis, clinical picture, diagnosis, and treatment. Acta Neu- rochir (Wien) 1991;110:160-5.
COMMENTARY
The paper by Schisano et al serves to remind us that intradural disc herniations do occur and gen- erally respond quite well to surgical management. As reported in this paper, the management is fairly
Surg Neurol 543 1995;44:536-43
straightforward. I have found it useful to open the dura posteriorly and to effect a repair of the area of perforation from the interior-usually using a fas- cial graft. Intradural disc herniations, which involve the root or penetrate the dura at the level of the medial margin of the root, represent a bit more of a management problem and, at least in one case, have been associated with a chronic pain state. We have also avoided the use of nonbiologic adhesives.
Harry 0. Cole, M.D. Chesterfield, Missouri
The authors have carried out a very thorough bib- liographic review of all the existing cases in the literature, and completed it with their personal con- tribution of nine cases. All patients, with one excep- tion, are over 45 years old. In the majority of cases, the affected level is L4-L5, with an exception in two cases (1 and 7), which correspond to L3-L4. It is very difficult to formulate a theory from the ethio- pathogenic point of view. These may be congenital malformations, although the embryology of the epi- dural space is not very detailed in the literature. The fact that the greatest number of cases in this and other series corresponds to the final decades of life does not indicate that it is an important congen- ital malformation, but it does indicate that it is a circumstantial anatomic variation which, on being subjected to the forces that produce the disc her- niation, tear the pachymeninx, and penetrate into the intradural space. This can also occur in osteo- ligament degenerative processes, producing adher- ence between the content of the elements of the epidural space and the dura mater, dural ischemia, and weakening of the walls of the dura mater ad- hering to the posterior longitudinal ligament. The action of bending, stretching, or vibratory forces tears the debilitated meninx, with fragments of the prolapsed disc penetrating into its interior. Neither the clinical symptomatology nor radiologic studies allow a preoperative diagnosis of the topography of the prolapsed disc. The surgical technique used is worthy of some comments. In some cases [2-5,7,9), the author uses a graft of free muscle, in others, a graft of muscle with adhesives and Gelfoam gauze. We understand that the free-muscle graft can act later as a fragment of disc, in the same way as the Gelfoam gauze. When these are used with adhesive, the frequency of fibrosis is much greater. I think the technique used in cases 1 and 8 is more suitable.
Vicente D. Calatayud Maldonado, M.D. Zaragoza, Spain