
Unique CD8� T cell-rich lymphoid aggregates in human uterine endometrium
Upload
independentCategory
view
5download
0
B Cell Survival in Intragraft Tertiary Lymphoid OrgansAfter Rituximab Therapy
Olivier Thaunat,1,2,11 Natacha Patey,3 Chantal Gautreau,4 Sophie Lechaton,5 Veronique Fremeaux-Bacchi,6
Marie-Caroline Dieu-Nosjean,2 Elisabeth Cassuto-Viguier,7 Christophe Legendre,5 Michel Delahousse,8
Philippe Lang,9 Jean-Baptiste Michel,10 and Antonino Nicoletti2,10
Background. Rituximab is emerging as a potent therapeutic option in chronic inflammatory diseases associated with aprominent humoral component. Recent studies have demonstrated that chronic inflammatory infiltrate organizeprogressively themselves into ectopic lymphoid tissues (tertiary lymphoid organs; TLOs) supporting a local humoralimmune response. In the present study, we evaluated the impact of rituximab therapy on TLOs associated with chronicactive antibody-mediated rejection, a prototypic humoral chronic inflammatory condition.Methods. Renal allografts removed for terminal chronic rejection were prospectively collected in four transplantationcenters over 4 years. Among 38 grafts collected, two were explanted after rituximab therapy for chronic active antibody-mediated rejection. Clinical characteristics and circulating B cell count were recorded for these two patients. Thecomposition and the microarchitecture of the inflammatory infiltrate were analyzed by flow cytometry and immuno-histochemistry. Organotypic cultures were performed to evaluate the intragraft production of alloantibody. Levels ofexpression of BAFF (Blys, CD257) were evaluated by quantitative reverse transcriptase-polymerase chain reaction.Results. Despite the complete depletion of circulating B cells in peripheral blood, TLOs were evidenced in the inter-stitium of both explanted grafts. Their functionality was assessed by the demonstration of a persistent local productionof alloantibody. BAFF, a potent survival factor for B cells, was found to be overexpressed (both at the gene and theprotein levels) in chronically rejected grafts when compared with normal kidneys and lymph nodes.Conclusions. In certain patients, inflammatory microenvironment provides BAFF-dependent paracrine survival signalto B-cells in TLOs, allowing them to escape rituximab-induced apoptosis, thereby thwarting therapeutic efficiency.
Keywords: Rituximab, Lymphoid neogenesis, Tertiary lymphoid organs, Chronic rejection, Inflammation.
(Transplantation 2008;85: 1648–1653)
R ituximab, an engineered monoclonal antibody directedagainst the B cell specific CD20 molecule, has recently
emerged as a potent therapeutic option for chronic inflam-matory diseases with a prominent humoral component, suchas rheumatoid arthritis (1), lupus (2), and antibody-mediatedallograft rejection (3). In these indications, rituximab admin-
istration is currently guided on the peripheral B cell countthat should decrease below 5/mm3 (2). However, focusing thefollow-up of rituximab therapy on circulating B cells could beinappropriate because this parameter may not provide reli-able information regarding the impact of the treatment ontertiary lymphoid organs. Indeed, chronic inflammatory in-filtrates progressively organize into ectopic lymphoid tissuesnamed “tertiary lymphoid organs” (TLOs) (4). Recurrent ob-servations of these fully functional ectopic germinal centerswithin inflamed tissues suggest that the local humoral im-mune response participates in the pathological process (5).
The aim of the present study was to investigate the ef-fect of rituximab therapy on the TLOs located within chron-ically rejected renal allografts.
MATERIALS AND METHODS
Origin of Human Samples
Renal allografts removed because of terminal chronic rejec-tion have been collected in four transplantation centersover a period of 4 years. Among a total of 38 consecutivegrafts, two were harvested after rituximab therapy forchronic active antibody-mediated rejection (CAAMR).The individual characteristics of these two patients are pre-sented in Table 1.Fresh normal renal tissue was obtained from the intact por-tion of six kidneys removed for renal cancer.Frozen lymphoid tissues were obtained from lymph nodesharvested during surgery (for colorectal cancer [n�6], orduring a coronary artery bypass procedure [n�2]) andwere found normal after histological examination.
This work was supported by the research grants from INSERM, the Fonda-tion pour la Recherche Medicale, and the Fondation du Rein (O.T.).
Disclosures: The authors reported no financial conflict.1 Renal Transplantation and Clinical Immunology Department, Edouard
Herriot Hospital, HCL; Universite Claude Bernard Lyon I; INSERMU851, Lyon, France.
2 Centre de Recherche des Cordeliers; Universite Pierre et Marie Curie -Paris6; Universite Rene Descartes Paris5; UMR S 872, Paris, France.
3 Pathology Department, Necker Hospital AP-HP, Paris, France.4 Immunology and Histocompatibility Laboratory, Saint-Louis Hospital
AP-HP, Paris, France.5 Renal Transplantation Department, Necker Hospital, APHP; Universite
Rene Descartes, Paris, France.6 Immunology Department, Georges Pompidou Hospital AP-HP, Paris,
France.7 Nephrology Department, Pasteur Hospital, Nice, France.8 Nephrology Department, Foch Hospital, Suresnes, France.9 Nephrology and Transplantation Department, Henri Mondor Hospital
AP-HP; Universite Paris 12, Creteil, France.10 INSERM U698; Universite Denis Diderot- Paris 7; CHU Xavier Bichat,
Paris, France.11 Address Correspondence to: Olivier Thaunat, M.D., Renal Transplanta-
tion and Clinical Immunology Department, Edouard Herriot Hospital, 5place d’Arsonval, 69437 Lyon Cedex 03, France.
E-mail: [email protected] 17 December 2007. Revision requested 7 January 2008.Accepted 4 March 2008.Copyright © 2008 by Lippincott Williams & WilkinsISSN 0041-1337/08/8511-1648DOI: 10.1097/TP.0b013e3181735723
1648 Transplantation • Volume 85, Number 11, June 15, 2008

All the patients gave informed consent for the usage of thesamples for research purpose.
Renal Allograft Pathology
Paraffin-embedded renal tissues were cut into 4 �m-thicksections and underwent routine examination.Indirect immunoperoxidase staining was performed on 4�m-thick paraffin-embedded sections with a mouse anti-human CD20 antibody (1:50; clone L26; Zymed Laborato-ries) to detect B cells; with an antiperipheral lymph nodeaddressin ([PNAd]; 1:100; clone MECA79; Pharmingen) todetect high endothelial venules; or with rat anti-humanBAFF (BLyS, CD257; 1:300; clone buffy-2; Abcam) as pre-viously described (6).Detection of C4d was performed on 4 �m-thick frozensections, with a mouse anti-human C4d (1:50; Quidel) andan FITC-labeled secondary antibody (1:20; rabbit anti-mouse IgG; DAKO).
Flow Cytometry AnalysisFragments of renal grafts were incubated in a solution
of 1 mg/mL collagenase A and 0.1 mg/mL DNAse I (Roche).The cell suspension was filtered and mononuclear cells wereisolated on a Ficoll gradient. Cells (0.1 million) were incu-bated with two fluorescent monoclonal antibodies (BD Bio-sciences) directed against human CD3 (PE-TxRed), andCD19 (AmCyan). Analysis was performed with an LSRII flowcytometer and the DIVA software (BD Biosciences).
In Vitro Production of AlloantibodiesOrganocultures were performed as previously de-
scribed (7). After 5 days, concentrations of IgG, IgA, and IgMwere measured using nephelometry (Beckman Instruments)in the supernatants.
Luminex assays were used to detect the presence ofanti-human leukocyte antigen alloantibodies in the super-natants (LifeScreen®, Tepnel Lifecodes Corporation) andsubsequently to determine their specificity (LABScreen®single antigen human leukocyte antigen class I and class IIdetection tests, One Lambda). The results are expressed asthe difference between the mean fluorescence intensitymeasured after incubation of the beads with the supernatantsand the background mean fluorescence intensity (determinedfor this particular single antigen bead after incubation with anegative control serum).
Semiquantitative Reverse Transcriptase-Polymerase Chain Reaction Analysis
Total RNA was isolated from the 38 explanted grafts, sixcontrol kidneys, and eight lymph nodes using the RNeasy MiniKit (Qiagen). cDNAs were generated from 1 �g of total RNAusing SuperScript II reverse transcriptase (Invitrogen) and randomdecamers (ABgene). The primers for GAPDH (5�-GTGAAGG-TC GGAGTCAAC-3�; 5�-GGTGAAGACGCCAGTGGACTC-3�)and B-cell activating factor (BAFF; 5�-CCTCACGGTGGT-GTCTTTCT-3�; 5�-AAAGCTGAGAAGCCATGGAA-3�) weredesigned using Primer3 software and obtained from Euro-gentec. Real-time quantitative polymerase chain reaction(PCR) was performed on an ABI Prism 7300 sequence detec-tion system (Applied Biosystems) with SYBR Green MasterMix (Qiagen). Results were expressed as threshold cycle (Ct)values corresponding to the cycle at which PCR enters theexponential phase.
The relative quantification of BAFF mRNA was deter-mined using the 2(���Ct) formula (8), in which GAPDH wasused as house keeping gene, and normal kidneys were consid-ered as control tissues (level of expression arbitrarily fixed to 1).
TABLE 1. Characteristics of the patients and timing of rituximab therapy
Patient 1 Patient 2
Age (yr) 42 41
Gender Male Female
Ethnicity Caucasian Caucasian
Cause of end stage renal failure Henoch-Schonlein purpura Membranous glomerulopathy
Rank of the transplantation 2 1
Type of donor Living donation Cadaveric
Age of donor (yr) 38 45
Baseline immunosuppressive regimen Anti-IL2R/MMF/FK506/CS OKT3/Aza/Csa/CS
Time from transplantation to diagnosis of CAAMR (mos) 12 166
Treatment of antibody-mediated rejection IVIg IVIg
Plasmapheresis Rituximab (1 course)
Rituximab (2 courses)
At the time of explantation
Time from transplantation to explantation (mos) 26 174
Time from last course of rituximab (mos) 10.3 3.8
CD19 count in peripheral blood 5/mm3 3/mm3
Anti-IL2R, anti-interleukine 2 receptor antibody; MMF, mycophenolate mofetil; FK506, tacrolimus; CS, corticosteroid; Aza, azathioprine; Csa, cyclospor-ine; IVIg, intravenous immunoglobulin.
© 2008 Lippincott Williams & Wilkins 1649Thaunat et al.
RESULTS
C4d Deposition and Tertiary Lymphoid Organsin Chronic Active Antibody-Mediated Rejection
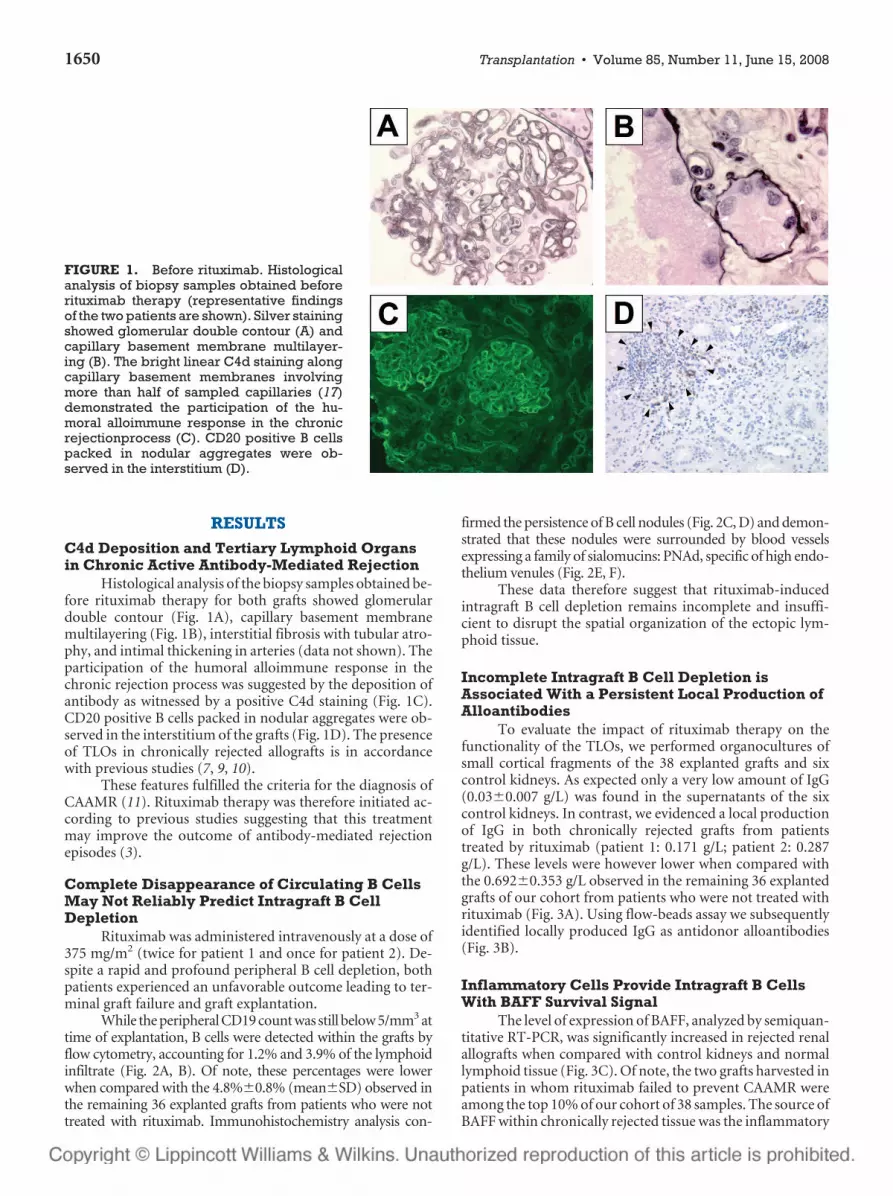
Histological analysis of the biopsy samples obtained be-fore rituximab therapy for both grafts showed glomerulardouble contour (Fig. 1A), capillary basement membranemultilayering (Fig. 1B), interstitial fibrosis with tubular atro-phy, and intimal thickening in arteries (data not shown). Theparticipation of the humoral alloimmune response in thechronic rejection process was suggested by the deposition ofantibody as witnessed by a positive C4d staining (Fig. 1C).CD20 positive B cells packed in nodular aggregates were ob-served in the interstitium of the grafts (Fig. 1D). The presenceof TLOs in chronically rejected allografts is in accordancewith previous studies (7, 9, 10).
These features fulfilled the criteria for the diagnosis ofCAAMR (11). Rituximab therapy was therefore initiated ac-cording to previous studies suggesting that this treatmentmay improve the outcome of antibody-mediated rejectionepisodes (3).
Complete Disappearance of Circulating B CellsMay Not Reliably Predict Intragraft B CellDepletion
Rituximab was administered intravenously at a dose of375 mg/m2 (twice for patient 1 and once for patient 2). De-spite a rapid and profound peripheral B cell depletion, bothpatients experienced an unfavorable outcome leading to ter-minal graft failure and graft explantation.
While the peripheral CD19 count was still below 5/mm3 attime of explantation, B cells were detected within the grafts byflow cytometry, accounting for 1.2% and 3.9% of the lymphoidinfiltrate (Fig. 2A, B). Of note, these percentages were lowerwhen compared with the 4.8%�0.8% (mean�SD) observed inthe remaining 36 explanted grafts from patients who were nottreated with rituximab. Immunohistochemistry analysis con-
firmed the persistence of B cell nodules (Fig. 2C, D) and demon-strated that these nodules were surrounded by blood vesselsexpressing a family of sialomucins: PNAd, specific of high endo-thelium venules (Fig. 2E, F).
These data therefore suggest that rituximab-inducedintragraft B cell depletion remains incomplete and insuffi-cient to disrupt the spatial organization of the ectopic lym-phoid tissue.
Incomplete Intragraft B Cell Depletion isAssociated With a Persistent Local Production ofAlloantibodies
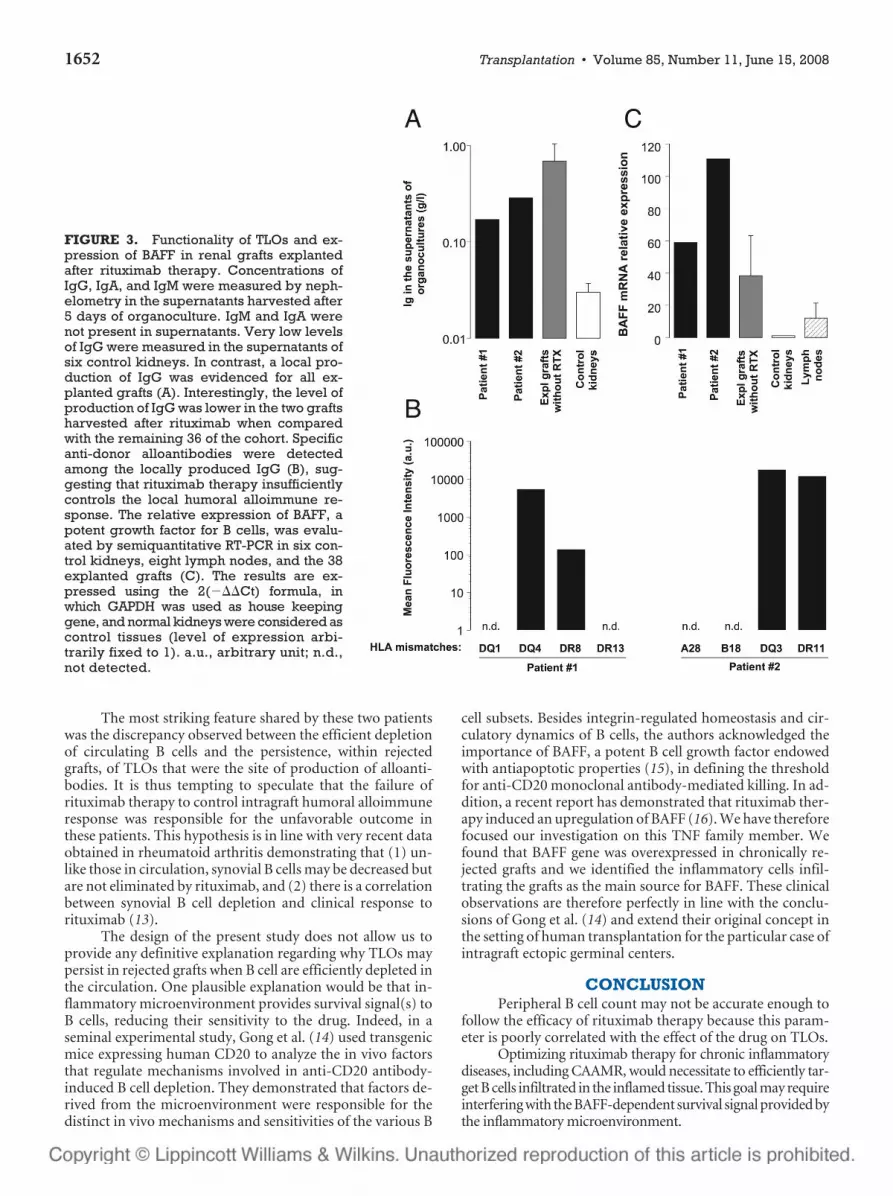
To evaluate the impact of rituximab therapy on thefunctionality of the TLOs, we performed organocultures ofsmall cortical fragments of the 38 explanted grafts and sixcontrol kidneys. As expected only a very low amount of IgG(0.03�0.007 g/L) was found in the supernatants of the sixcontrol kidneys. In contrast, we evidenced a local productionof IgG in both chronically rejected grafts from patientstreated by rituximab (patient 1: 0.171 g/L; patient 2: 0.287g/L). These levels were however lower when compared withthe 0.692�0.353 g/L observed in the remaining 36 explantedgrafts of our cohort from patients who were not treated withrituximab (Fig. 3A). Using flow-beads assay we subsequentlyidentified locally produced IgG as antidonor alloantibodies(Fig. 3B).
Inflammatory Cells Provide Intragraft B CellsWith BAFF Survival Signal
The level of expression of BAFF, analyzed by semiquan-titative RT-PCR, was significantly increased in rejected renalallografts when compared with control kidneys and normallymphoid tissue (Fig. 3C). Of note, the two grafts harvested inpatients in whom rituximab failed to prevent CAAMR wereamong the top 10% of our cohort of 38 samples. The source ofBAFF within chronically rejected tissue was the inflammatory
FIGURE 1. Before rituximab. Histologicalanalysis of biopsy samples obtained beforerituximab therapy (representative findingsof the two patients are shown). Silver stainingshowed glomerular double contour (A) andcapillary basement membrane multilayer-ing (B). The bright linear C4d staining alongcapillary basement membranes involvingmore than half of sampled capillaries (17)demonstrated the participation of the hu-moral alloimmune response in the chronicrejectionprocess (C). CD20 positive B cellspacked in nodular aggregates were ob-served in the interstitium (D).
1650 Transplantation • Volume 85, Number 11, June 15, 2008
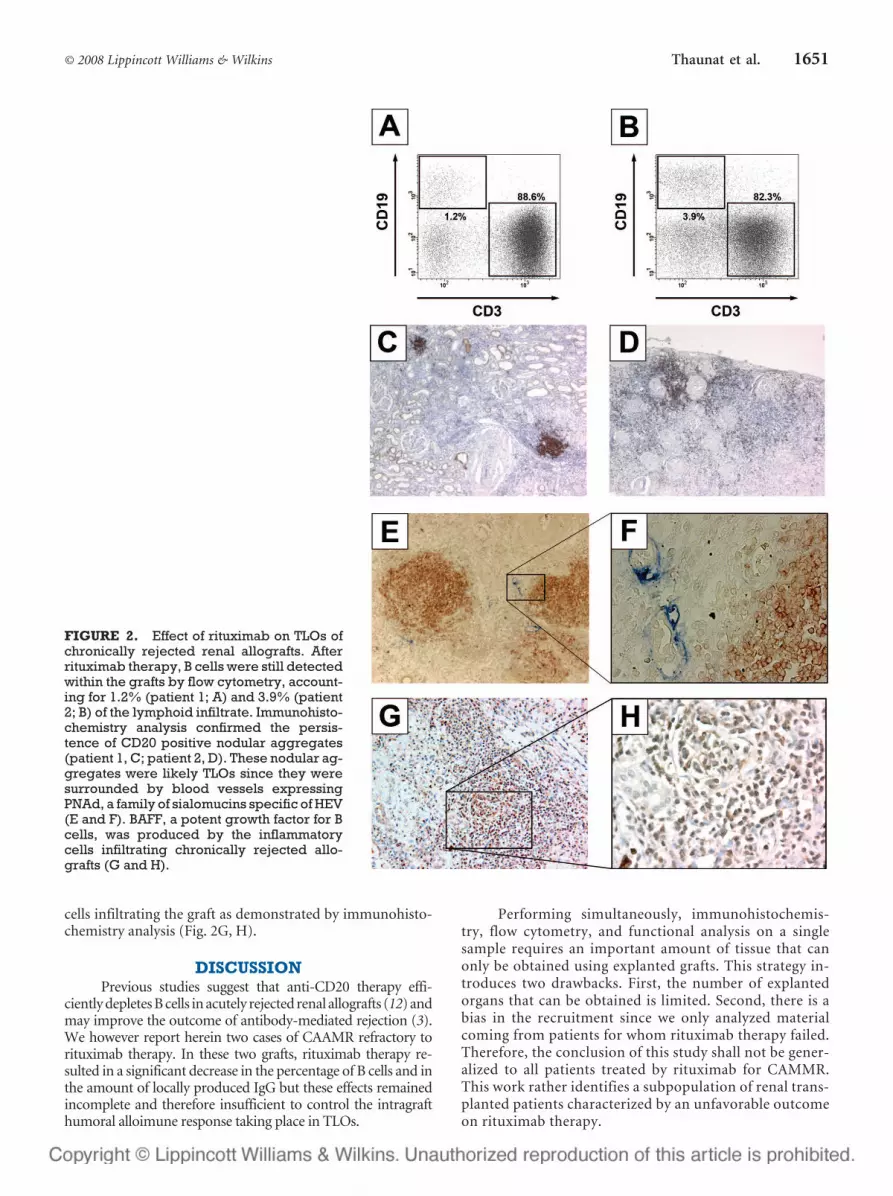
cells infiltrating the graft as demonstrated by immunohisto-chemistry analysis (Fig. 2G, H).
DISCUSSIONPrevious studies suggest that anti-CD20 therapy effi-
ciently depletes B cells in acutely rejected renal allografts (12) andmay improve the outcome of antibody-mediated rejection (3).We however report herein two cases of CAAMR refractory torituximab therapy. In these two grafts, rituximab therapy re-sulted in a significant decrease in the percentage of B cells and inthe amount of locally produced IgG but these effects remainedincomplete and therefore insufficient to control the intragrafthumoral alloimune response taking place in TLOs.
Performing simultaneously, immunohistochemis-try, flow cytometry, and functional analysis on a singlesample requires an important amount of tissue that canonly be obtained using explanted grafts. This strategy in-troduces two drawbacks. First, the number of explantedorgans that can be obtained is limited. Second, there is abias in the recruitment since we only analyzed materialcoming from patients for whom rituximab therapy failed.Therefore, the conclusion of this study shall not be gener-alized to all patients treated by rituximab for CAMMR.This work rather identifies a subpopulation of renal trans-planted patients characterized by an unfavorable outcomeon rituximab therapy.
FIGURE 2. Effect of rituximab on TLOs ofchronically rejected renal allografts. Afterrituximab therapy, B cells were still detectedwithin the grafts by flow cytometry, account-ing for 1.2% (patient 1; A) and 3.9% (patient2; B) of the lymphoid infiltrate. Immunohisto-chemistry analysis confirmed the persis-tence of CD20 positive nodular aggregates(patient 1, C; patient 2, D). These nodular ag-gregates were likely TLOs since they weresurrounded by blood vessels expressingPNAd, a family of sialomucins specific of HEV(E and F). BAFF, a potent growth factor for Bcells, was produced by the inflammatorycells infiltrating chronically rejected allo-grafts (G and H).
© 2008 Lippincott Williams & Wilkins 1651Thaunat et al.
The most striking feature shared by these two patientswas the discrepancy observed between the efficient depletionof circulating B cells and the persistence, within rejectedgrafts, of TLOs that were the site of production of alloanti-bodies. It is thus tempting to speculate that the failure ofrituximab therapy to control intragraft humoral alloimmuneresponse was responsible for the unfavorable outcome inthese patients. This hypothesis is in line with very recent dataobtained in rheumatoid arthritis demonstrating that (1) un-like those in circulation, synovial B cells may be decreased butare not eliminated by rituximab, and (2) there is a correlationbetween synovial B cell depletion and clinical response torituximab (13).
The design of the present study does not allow us toprovide any definitive explanation regarding why TLOs maypersist in rejected grafts when B cell are efficiently depleted inthe circulation. One plausible explanation would be that in-flammatory microenvironment provides survival signal(s) toB cells, reducing their sensitivity to the drug. Indeed, in aseminal experimental study, Gong et al. (14) used transgenicmice expressing human CD20 to analyze the in vivo factorsthat regulate mechanisms involved in anti-CD20 antibody-induced B cell depletion. They demonstrated that factors de-rived from the microenvironment were responsible for thedistinct in vivo mechanisms and sensitivities of the various B
cell subsets. Besides integrin-regulated homeostasis and cir-culatory dynamics of B cells, the authors acknowledged theimportance of BAFF, a potent B cell growth factor endowedwith antiapoptotic properties (15), in defining the thresholdfor anti-CD20 monoclonal antibody-mediated killing. In ad-dition, a recent report has demonstrated that rituximab ther-apy induced an upregulation of BAFF (16). We have thereforefocused our investigation on this TNF family member. Wefound that BAFF gene was overexpressed in chronically re-jected grafts and we identified the inflammatory cells infil-trating the grafts as the main source for BAFF. These clinicalobservations are therefore perfectly in line with the conclu-sions of Gong et al. (14) and extend their original concept inthe setting of human transplantation for the particular case ofintragraft ectopic germinal centers.
CONCLUSIONPeripheral B cell count may not be accurate enough to
follow the efficacy of rituximab therapy because this param-eter is poorly correlated with the effect of the drug on TLOs.
Optimizing rituximab therapy for chronic inflammatorydiseases, including CAAMR, would necessitate to efficiently tar-get B cells infiltrated in the inflamed tissue. This goal may requireinterfering with the BAFF-dependent survival signal provided bythe inflammatory microenvironment.
FIGURE 3. Functionality of TLOs and ex-pression of BAFF in renal grafts explantedafter rituximab therapy. Concentrations ofIgG, IgA, and IgM were measured by neph-elometry in the supernatants harvested after5 days of organoculture. IgM and IgA werenot present in supernatants. Very low levelsof IgG were measured in the supernatants ofsix control kidneys. In contrast, a local pro-duction of IgG was evidenced for all ex-planted grafts (A). Interestingly, the level ofproduction of IgG was lower in the two graftsharvested after rituximab when comparedwith the remaining 36 of the cohort. Specificanti-donor alloantibodies were detectedamong the locally produced IgG (B), sug-gesting that rituximab therapy insufficientlycontrols the local humoral alloimmune re-sponse. The relative expression of BAFF, apotent growth factor for B cells, was evalu-ated by semiquantitative RT-PCR in six con-trol kidneys, eight lymph nodes, and the 38explanted grafts (C). The results are ex-pressed using the 2(���Ct) formula, inwhich GAPDH was used as house keepinggene, and normal kidneys were considered ascontrol tissues (level of expression arbi-trarily fixed to 1). a.u., arbitrary unit; n.d.,not detected.
1652 Transplantation • Volume 85, Number 11, June 15, 2008

ACKNOWLEDGMENTSThe authors are grateful to the physicians from the De-
partments of Nephrology, Pathology and Urology of Foch, HenriMondor, Necker and Pasteur Hospitals for their help during thecollection of tissue samples.
REFERENCES1. Edwards JC, Szczepanski L, Szechinski J, et al. Efficacy of B-cell-targeted ther-
apy with rituximab in patients with rheumatoid arthritis. N Engl J Med 2004;350: 2572.
2. Looney RJ, Anolik JH, Campbell D, et al. B cell depletion as a novel treatmentfor systemic lupus erythematosus: A phase I/II dose-escalation trial of ritux-imab. Arthritis Rheum 2004; 50: 2580.
3. Becker YT, Becker BN, Pirsch JD, et al. Rituximab as treatment forrefractory kidney transplant rejection. Am J Transplant 2004; 4: 996.
4. Kratz A, Campos-Neto A, Hanson MS, et al. Chronic inflammationcaused by lymphotoxin is lymphoid neogenesis. J Exp Med 1996; 183:1461.
5. Aloisi F, Pujol-Borrell R. Lymphoid neogenesis in chronic inflamma-tory diseases. Nat Rev Immunol 2006; 6: 205.
6. Groom J, Kalled SL, Cutler AH, et al. Association of BAFF/BLyS over-expression and altered B cell differentiation with Sjogren’s syndrome.J Clin Invest 2002; 109: 59.
7. Thaunat O, Field AC, Dai J, et al. Lymphoid neogenesis in chronicrejection: Evidence for a local humoral alloimmune response. Proc NatlAcad Sci USA 2005; 102: 14723.
8. Livak KJ, Schmittgen TD. Analysis of relative gene expression datausing real-time quantitative PCR and the 2(-Delta Delta C(T)) method.Methods 2001; 25: 402.
9. Kerjaschki D, Regele HM, Moosberger I, et al. Lymphatic neoangiogen-esis in human kidney transplants is associated with immunologicallyactive lymphocytic infiltrates. J Am Soc Nephrol 2004; 15: 603.
10. Thaunat O, Patey N, Morelon E, et al. Lymphoid neogenesis in chronicrejection: The murderer is in the house. Curr Opin Immunol 2006; 18:576.
11. Solez K, Colvin RB, Racusen LC, et al. Banff ’05 meeting report: Differ-ential diagnosis of chronic allograft injury and elimination of chronicallograft nephropathy (“CAN”). Am J Transplant 2007; 7: 518.
12. Genberg H, Hansson A, Wernerson A, et al. Pharmacodynamics ofrituximab in kidney allotransplantation. Am J Transplant 2006; 6: 2418.
13. Kavanaugh A, Rosengren S, Lee SJ, et al. Assessment of rituximab’simmunomodulatory synovial effects (the ARISE trial). I. Clinical andsynovial biomarker results. Ann Rheum Dis 2007; 67: 402.
14. Gong Q, Ou Q, Ye S, et al. Importance of cellular microenvironmentand circulatory dynamics in B cell immunotherapy. J Immunol 2005;174: 817.
15. Batten M, Groom J, Cachero TG, et al. BAFF mediates survival of pe-ripheral immature B lymphocytes. J Exp Med 2000; 192: 1453.
16. Lavie F, Miceli-Richard C, Ittah M, et al. Increase of B cell-activatingfactor of the TNF family (BAFF) after rituximab treatment: Insightsinto a new regulating system of BAFF production. Ann Rheum Dis2007; 66: 700.
17. Racusen LC, Colvin RB, Solez K, et al. Antibody-mediated rejectioncriteria - An addition to the Banff 97 classification of renal allograftrejection. Am J Transplant 2003; 3: 708.
Instructions for Authors—Key Guidelines
Financial Disclosure and Products Page Authors must disclose any financial relationship with any entity or product described in the manuscript (including grant support, employment, honoraria, gifts, fees, etc.) Manuscripts are subject to peer review and revision may be required as a condition of acceptance. These instructions apply to all submissions.
Manuscript Review and Publication
Using an electronic on-line submission and peer review tracking system, Transplantation is committed to rapid review and publication. The average time to first decision is now less than 21 days. Time to publication of accepted manuscripts continues to be shortened, with the Editorial team committed to a goal of 3 months from acceptance to publication. Submit your manuscript to Transplantation® today. The Manuscript Central submission website (http://mc.manuscriptcentral.com/transplant) helps make the submission process easier, more efficient, and less expensive for authors, and makes the review process quicker, more accessible, and less expensive for reviewers.
© 2008 Lippincott Williams & Wilkins 1653Thaunat et al.
Copyright © 2022 FDOKUMEN




















