
Extracorporeal photopheresis: From solid organs to face transplantation
12
Review Extracorporeal photopheresis: From solid organs to face transplantation Mikaël Hivelin a,b, ⁎, Maria Siemionow b , Philippe Grimbert c , Laurent Lantieri a a Plastic Surgery Department, Henri Mondor Hospital, University Paris 12, Creteil, France b Plastic Surgery Department, Cleveland Clinic, Ohio, USA c Department of Nephrology, Henri Mondor Hospital, University Paris 12, Creteil, France abstract article info Article history: Received 9 February 2009 Received in revised form 19 April 2009 Accepted 24 April 2009 Keywords: Early apoptotic Composite tissue allotransplantation Face transplantation Tolerance Photopheresis Photochemotherapy Composite tissue allotransplantations (CTA), were introduced with the first successful hand transplantation and are now a part of reconstructive surgery armamentarium. These reconstructive procedures for non life- threatening indications remain rare due to adverse effects of the associated lifelong immunosuppressive therapy. Indeed, despite recent progress, immunosuppressive therapies remain non-specific to the type of donor and still bear significant risks of serious side effects. Extracorporeal photopheresis (ECP), also called photochemotherapy, has been introduced in the composite tissue allotransplantation field as a part of acute rejection treatment in face transplantations. ECP has been performed after solid organ transplantations as a supportive therapy for acute rejection episodes. It has also been used to treat graft versus host diseases, which can occur after bone marrow or stem cell transplantations. ECP is also used to treat dermatologic diseases, such as cutaneous T-cell lymphoma, or autoimmune diseases, such as scleroderma or pemphigus vulgaris. The principle of ECP is to induce leucocyte apoptosis with UVA radiation after their presentation by psoralens. These leucocytes are immediately re-infused into the patient, where they undergo early apoptosis. Following apoptosis, the leucocytes are engulfed by macrophage or other antigen-presenting cells, such as immature dendritic cells, in an anti-inflammatory cytokine environment. The anti-inflammatory cytokine secretion pattern, with a switch from TH1 to TH2 for CD4+ lymphocytes, and the engulfment by immature cells without co-stimulatory molecules induces anergy, by deleting effector T-cells that responded to the presented antigens. An increase in regulatory T-cells (T-regs) is also induced after ECP and may contribute to allograft acceptance by the recipient. ECP has already been used for the great majority of solid organ transplantations to cure acute rejection episodes or in an attempt to prevent or cure chronic rejections, such as bronchitis obliterans, which occurs after lung transplantation. Considering composite tissue allotransplantations, ECP was used in two face transplantations after the occurrence of second rejection episodes triggered by viral infections. ECP therapy, associated with maintenance immunosuppressive therapy and doses of methylprednisolone, and the control of viral infection, succeeded to reverse the rejection process without the development of other side effects. Despite the fact that the mechanism of action of ECP has not been fully elucidated, this therapy could be a useful supportive therapy during the treatment of acute rejection episodes in composite tissue allotransplantations. In this review, we introduce the interest of ECP implementation in CTA in face allotransplantations. © 2009 Elsevier B.V. All rights reserved. Contents 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118 2. UV-induced apoptosis, modification of cytokine secretion patterns, and T-regs induction after ECP . . . . . . . . . . . . . . . . . . . . . 118 2.1. Definition of extracorporeal photopheresis (ECP) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118 2.2. Donor apoptotic cells injections as experimental models to study ECP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119 2.3. Different steps in cell apoptosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119 2.4. Apoptosis induced during ECP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119 2.5. Different delays in apoptosis occurrence after UV radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119 2.6. Characteristics of these apoptotic cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119 Transplant Immunology 21 (2009) 117–128 ⁎ Corresponding author. Department of Plastic Surgery, Henri Mondor Hospital, 51, av Mal de Lattre de Tassigny, 94010 Créteil Cedex, France. Tel.: +33149812533. E-mail address: [email protected] (M. Hivelin). 0966-3274/$ – see front matter © 2009 Elsevier B.V. All rights reserved. doi:10.1016/j.trim.2009.04.005 Contents lists available at ScienceDirect Transplant Immunology journal homepage: www.elsevier.com/locate/trim
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Extracorporeal photopheresis: From solid organs to face transplantation

Transplant Immunology 21 (2009) 117–128
Contents lists available at ScienceDirect
Transplant Immunology
j ourna l homepage: www.e lsev ie r.com/ locate / t r im
Review
Extracorporeal photopheresis: From solid organs to face transplantation
Mikaël Hivelin a,b,⁎, Maria Siemionow b, Philippe Grimbert c, Laurent Lantieri a
a Plastic Surgery Department, Henri Mondor Hospital, University Paris 12, Creteil, Franceb Plastic Surgery Department, Cleveland Clinic, Ohio, USAc Department of Nephrology, Henri Mondor Hospital, University Paris 12, Creteil, France
⁎ Corresponding author. Department of Plastic SurgerE-mail address: [email protected] (M. Hiv
0966-3274/$ – see front matter © 2009 Elsevier B.V. Adoi:10.1016/j.trim.2009.04.005
a b s t r a c t
a r t i c l e i n f oArticle history:Received 9 February 2009Received in revised form 19 April 2009Accepted 24 April 2009
Keywords:Early apoptoticComposite tissue allotransplantationFace transplantationTolerancePhotopheresisPhotochemotherapy
Composite tissue allotransplantations (CTA), were introduced with the first successful hand transplantationand are now a part of reconstructive surgery armamentarium. These reconstructive procedures for non life-threatening indications remain rare due to adverse effects of the associated lifelong immunosuppressivetherapy. Indeed, despite recent progress, immunosuppressive therapies remain non-specific to the type ofdonor and still bear significant risks of serious side effects.Extracorporeal photopheresis (ECP), also called photochemotherapy, has been introduced in the compositetissue allotransplantation field as a part of acute rejection treatment in face transplantations.ECP has been performed after solid organ transplantations as a supportive therapy for acute rejectionepisodes. It has also been used to treat graft versus host diseases, which can occur after bone marrow or stemcell transplantations. ECP is also used to treat dermatologic diseases, such as cutaneous T-cell lymphoma, orautoimmune diseases, such as scleroderma or pemphigus vulgaris.The principle of ECP is to induce leucocyte apoptosis with UVA radiation after their presentation bypsoralens. These leucocytes are immediately re-infused into the patient, where they undergo early apoptosis.Following apoptosis, the leucocytes are engulfed by macrophage or other antigen-presenting cells, such asimmature dendritic cells, in an anti-inflammatory cytokine environment. The anti-inflammatory cytokinesecretion pattern, with a switch from TH1 to TH2 for CD4+ lymphocytes, and the engulfment by immaturecells without co-stimulatory molecules induces anergy, by deleting effector T-cells that responded to thepresented antigens. An increase in regulatory T-cells (T-regs) is also induced after ECP and may contribute toallograft acceptance by the recipient.ECP has already beenused for the greatmajority of solid organ transplantations to cure acute rejection episodes orin an attempt to prevent or cure chronic rejections, such as bronchitis obliterans, which occurs after lungtransplantation.Considering composite tissue allotransplantations, ECPwasused in two face transplantations after the occurrenceof second rejection episodes triggered by viral infections. ECP therapy, associated with maintenanceimmunosuppressive therapy and doses of methylprednisolone, and the control of viral infection, succeeded toreverse the rejection process without the development of other side effects.Despite the fact that the mechanism of action of ECP has not been fully elucidated, this therapy could be a usefulsupportive therapy during the treatment of acute rejection episodes in composite tissue allotransplantations.In this review, we introduce the interest of ECP implementation in CTA in face allotransplantations.
© 2009 Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1182. UV-induced apoptosis, modification of cytokine secretion patterns, and T-regs induction after ECP . . . . . . . . . . . . . . . . . . . . . 118
2.1. Definition of extracorporeal photopheresis (ECP) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1182.2. Donor apoptotic cells injections as experimental models to study ECP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1192.3. Different steps in cell apoptosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1192.4. Apoptosis induced during ECP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1192.5. Different delays in apoptosis occurrence after UV radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1192.6. Characteristics of these apoptotic cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119
y, Henri Mondor Hospital, 51, av Mal de Lattre de Tassigny, 94010 Créteil Cedex, France. Tel.: +33 149812533.elin).
ll rights reserved.

118 M. Hivelin et al. / Transplant Immunology 21 (2009) 117–128
2.7. Differences between early or late apoptotic cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1192.8. The need for early apoptotic cells to induce anti-inflammatory effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1192.9. Engulfment by monocytes, macrophages, and immature dendritic cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1202.10. Interactions between the early apoptotic cells and immature dendritic cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 121
2.10.1. A total and rapid clearance of early apoptotic cells is required . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1212.10.2. Apoptotic lymphocytes induce changes in cytokine secretion patterns . . . . . . . . . . . . . . . . . . . . . . . . . . . 121
2.11. Replacement of the “suppressor” T-cell concept by the regulatory T-cell (T-Regs) idea . . . . . . . . . . . . . . . . . . . . . . . . 1222.12. Donor-specific or non-specific immunomodulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 122
3. Indications for photopheresis in solid organ transplantations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1223.1. ECP in experimental organ transplantations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1223.2. Clinical implementation in transplantations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 122
3.2.1. Kidney transplantation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1223.2.2. Heart transplantation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1233.2.3. Lung transplantation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1233.2.4. Pancreas transplantations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1233.2.5. Liver transplantations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1233.2.6. Intestinal transplantations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1233.2.7. Phototherapy and bone marrow allografts. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 123
3.3. ECP sessions schedule . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1243.4. Adverse effects of extracorporeal photopheresis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 124
4. Introduction and relevance of ECP for composite . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1244.1. Composite tissue allotransplantations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1244.2. Rejection and immunosuppressive therapy in CTA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1244.3. Opportunistic infections management and immunosuppressive therapy modulation . . . . . . . . . . . . . . . . . . . . . . . . . 1244.4. GVHD in CTA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1254.5. ECP in CTA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 125
5. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 126Conflict of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 126
Acknowledgement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 126References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 126
Conflict of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
tissue allotransplantations
1. Introduction
Composite tissue allotransplantations (CTA), such as hand, face, orabdominal wall transplantations are new promising options inreconstructive surgery. Despite encouraging functional results ofthese procedures, indications remain limited by adverse effectsrelated to a lifelong immunosuppression.
Mono or polyclonal antibodies, steroids, cyclosporine A, FK506,rapamycin, or mycophenolate mophetil are current immunosuppres-sive protocols used for induction and maintenance therapy. Co-stimulation blockade by monoclonal antibodies is a new promisingoption that seems to reduce the risks for diabetes and opportunisticinfections, but it can increase the incidence of hyperlipidemia [1].
Major adverse effects such as hypertension, diabetes, lipidmetabolismdisorders, opportunistic infections, andmalignancies result from thenon-specific modes of action of immunosuppressive protocols. More selectiveand safer therapies for induction, maintenance, or rejection treatmentcould be obtained through donor-specific tolerance inducing strategies.
Extracorporeal photopheresis (ECP) has already been used formore than 30 years for solid organ transplantations and can serve asan additional therapy during acute rejection episodes.
ECP has been recently implemented in the CTA field to treat acuterejection episodes in face allotransplantation [2,3].
In this review,wedescribe themechanismsof action for ECP, includingthe induction of peripheral lymphocyte apoptosis, the modification ofcytokine patterns, and the activation of regulatory T-cells. Then, wepresent the indications of ECP in transplantation, with emphasis on itsimplementation to composite tissue allotransplantations.
2. UV-induced apoptosis, modification of cytokine secretionpatterns, and T-regs induction after ECP
Ultraviolet (UV) light is the primary cause of non melanoma skincancer, the most prevalent form of human cancer [4,5]. Within
ultraviolet light, 3 subtypes are distinguished based on theirwavelengths: UVA (400 nm–315 nm) and a subset called UVA1(400–340 nm), UVB (315 nm–280 nm), or UVC (280 nm–100 nm).UVA radiation contributes to skin cancer via indirect DNA damagedue to highly reactive chemical intermediates, such as hydroxyl andoxygen radicals. UVA radiation penetrates deeply but does not causesunburn. UVA1 radiation has to be used in conjunctionwith psoralens(PUVA therapy) to induce direct DNA lesions.
UVB light can cause direct DNA damage. UVB radiation excites DNAmolecules in skin cells, causing aberrant covalent bonds to formbetween adjacent cytosine bases, producing a dimer. UVB radiationcan cause sunburn and induce skin tumors through direct effects onDNA, leading to gene mutations [6,7] and to indirect effects onthe immune system [4]. UVA and UVB are both used in clinicalapplications.
UVC radiation has a shorter wavelength and is not used clinically,except for its germicidal properties. Little attention is usually given toUVC rays since they are filtered out by the atmosphere.
The tolerogenic effect on tumor cells induced by UVB radiation hasbeen described since 1974 [8], when UVB-induced skin tumors inmicewere not rejected when the recipient was exposed to the sameradiation. These immunosuppressive properties were also transferredby adoptive therapy, thanks to T-cells called “suppressive” T-cellsfound in UVB exposed mice.
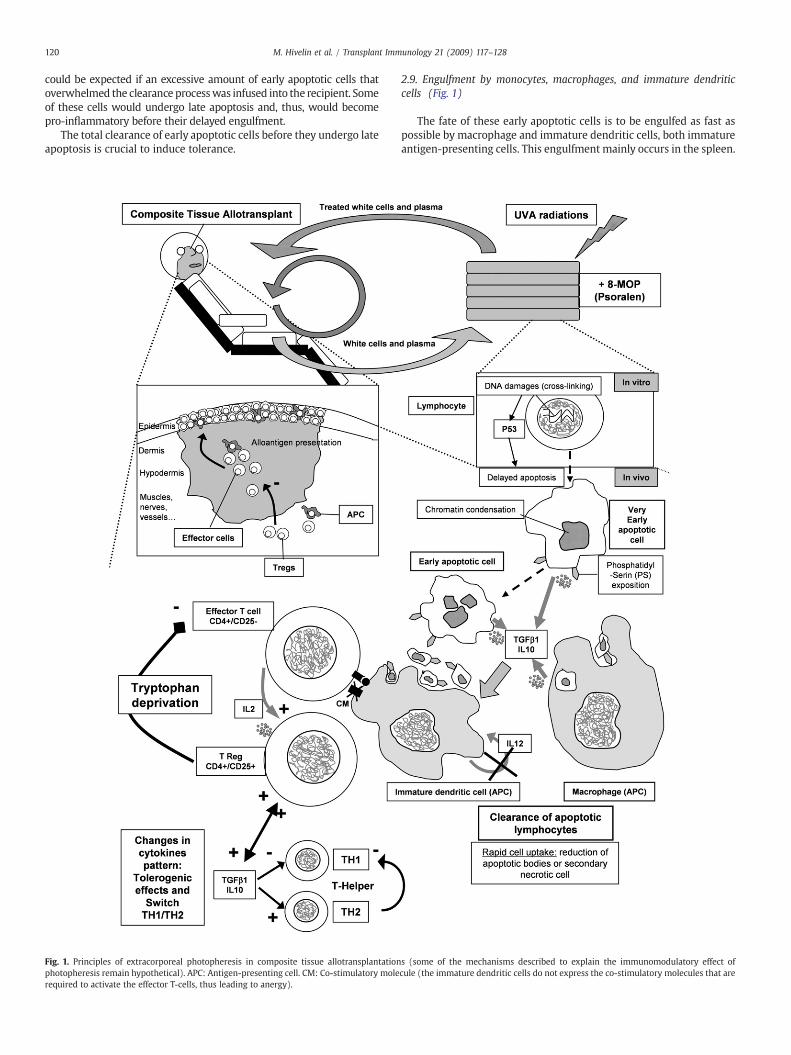
2.1. Definition of extracorporeal photopheresis (ECP) (Fig. 1)
ECP, or photochemotherapy [9], consists of re-infusion of 8-methylpsoralen-sensitized and UVA-radiated blood mononuclear cells.Plasma and leukocyte-rich fractions from the patient's peripheral bloodare separated by centrifugation. A thin buff layer is then wedgedbetween a clear layer (theplasma) anda red layer containingmostof thered blood cells. This 1% of the total blood volume contains most of thewhite blood cells and platelets.

119M. Hivelin et al. / Transplant Immunology 21 (2009) 117–128
The 8-methoxypsoralen (200–300 ng/mL) can be given systemi-cally or can be infused ex vivo, into the plasma, after its extraction byapheresis. This latter method allows increased drug levels during theradiation treatment and limits adverse effects, such as nausea.
The leukocyte-rich fraction is then passed through a 1mmdiameterplastic channel and is exposed to UVA1 light (wavelength: 340–400 nm,energy: 2 J/m2). The photoexposed white cells are then infused backinto the patient, and the total procedure lasts from 4 to 5 h.
During one ECP session, about 10 to 15% of all the peripherallymphocytes are treated and re-infused into the patient [10], with theexpectation that amajority of the cellswill undergo apoptosiswithin 48 h.
The number of ECP sessions depends on the indications, type oftransplant, type and intensity of rejection, and also on ECP's efficacy.
ECPproperties have beenused since the 1970s for all diseases that canbe mediated by unregulated T-cell populations, such as cutaneous T-celllymphoma; graft versus host disease (GVHD) [11]; autoimmune diseaseslike systemic lupus erythematosus, rheumatoid arthritis, scleroderma,and pemphigus vulgaris [12,13]; and also many types of allotransplanta-tions [2,14–21] so as to control acute or chronic rejection episodes.
2.2. Donor apoptotic cells injections as experimental models to study ECP
The apheresis process used for ECP is difficult to implement in smallanimalmodels, such as rodents.Most small animal experimental studiesthat can be directly compared with ECP used apoptotic cells created exvivo that were then injected into recipients. These studies described thesame effects on the rejection process.
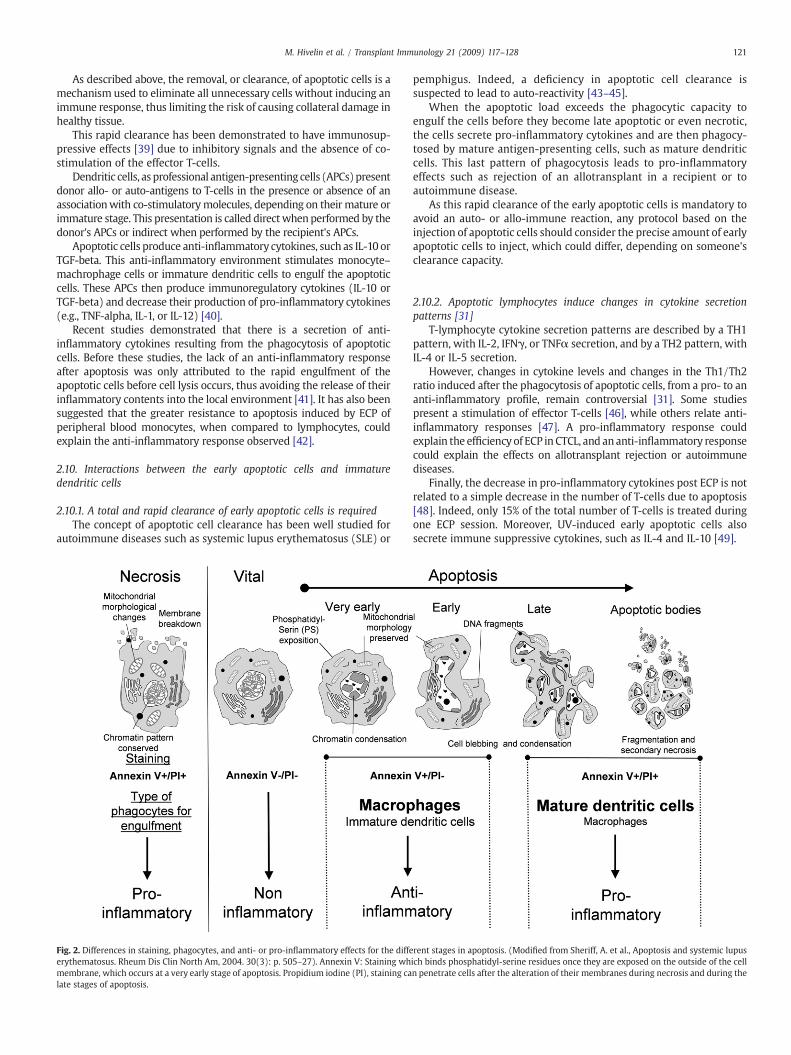
2.3. Different steps in cell apoptosis (Fig. 2)
Apoptotis or Programmed Cell Death (PCD) allows the suppressionof all damaged or dangerous cells without initiation of theinflammatory cascade. This physiological process controls cell num-bers during growth or healing, with lower risks of collateral damage tothe surrounding tissues.
Fig. 2 illustrates different steps of cellular apoptosis with acomparison to the process of cellular necrosis.
2.4. Apoptosis induced during ECP
Exposure of cells treated with 8-MOP to UVA radiation inducesDNA monoadducts and covalent crosslink formation [10] (Fig. 1).Photo-activated 8-MOP covalently binds to DNA pyrimidine bases, cellsurface molecules, and cytoplasmic components of the exposed whitecells [22]. These covalent links result in cellular lethal effects, andleukocytes are re-infused when entering the apoptotic phase. Thegreat majority of blood lymphocytes undergo apoptosis within 48 hafter ECP [23].
2.5. Different delays in apoptosis occurrence after UV radiation
UV radiation can induce two types of cell apoptosis, immediateapoptosis or pre-programmed cell death (Pre-PCD) versus delayedapoptosis (or PCD) [24,25], depending on the wavelength (UVA orUVB), the radiation energy, and the presence or absence of aphotosensitizer [24,26,27].
Pre-PCD can be induced by UVA1 without psoralens through adirect membrane rupture by the oxygen-singlet oxidative process[27]. This Pre-PCD appears immediately after the radiation.
Immediate apoptosis induced by UVA1 is caused by membranealterations and requires a significantly higher energy level than thatused to activate psoralens [24].
On the contrary, both UVA1 radiation associated with psoralensand UVB radiation induce direct DNA damage of the lymphocyteswithout direct membrane alterations, leading to PCD. This PCD canalso be divided into intermediate and delayed apoptosis.
Intermediate apoptosis, imputed to direct DNA lesions, is due to adepolarization of the inner mitochondrial membrane [25], withcessation of ATP production, and inversion in the ratio of themitochondrial pro-apoptotic protein Bcl-2 to the anti-apoptoticprotein Bax [28]. The level of the pro-apoptotic protein p53 increases,shifting the p53 to Bcl-2 ratio, which activates the caspase apoptoticpathway. The scramblase protein is also activated and provokes thephosphatidyl-serine flip-flop described above.
Delayed apoptosis is observed 20 h after UV radiation and isimputable to the Fas (CD95)–Fas ligand interaction through thecaspase pathway [25,29,30].
2.6. Characteristics of these apoptotic cells [31]
During the first stages of apoptosis, phosphatidyl-serine residues(PS), which are present on the inner leaf of the cell membrane underbasal conditions, “flip-flop” to the outer leaf, allowing for theirphagocytosis by antigen-presenting cells (APCs) [32,33] (Fig. 1). Thesephosphatidyl-serine residues can be identified by annexin V staining[34,35]. From 0 to 1 h after ECP, the number of annexin V-positivelymphocytes rises to 15% and remains quite stable for the first 20 h.After 20 h, however, the number of annexin V-positive cells increases,as does the number of necrotic cells [29].
Indeed, annexin V can also detect necrotic cells, which alsoundergo a loss of membrane integrity [36]. Propidium iodine (PI)specifically stains necrotic cells, thanks to their membrane alterations,and it enables the differentiation of necrotic from apoptotic cells.
2.7. Differences between early or late apoptotic cells (Fig. 2)
Two apoptotic stages can be determined with the use of annexinand propidium iodine (PI) staining. During the first, or early, stage ofapoptosis, cells will stain positively for annexin V, thanks to the PSflip-flop that occurs early; but cells will stain negatively for PI, as thereis nomodification in theirmembrane permeability. During the second,or late, stage of apoptosis, cells will stain positively for annexin V andfor PI since this dye can penetrate the damaged membranes. The lateapoptotic cells progressively flake into apoptotic bodies (Fig. 2).
Thus, cells can be divided into three groups; intact (Annexin V−/PI−), early apoptotic (Annexin V+/PI−), and late apoptotic ornecrotic (Annexin V+/PI+) cells [37] (Fig. 2).
In conclusion, we emphasize the different types of apoptosis,immediate, intermediate or delayed, as well as the early and late stagesin the apoptotic process that should be considered when analyzingapoptosis.
2.8. The need for early apoptotic cells to induce anti-inflammatory effects
As illustrated in Fig. 2, the pro- or anti-inflammatory reactionstriggered by antigen-presenting cells (APCs) are dependent on theapoptotic stage of the lymphocytes during their engulfment by APCs.
Early apoptotic cells are the only ones to provide immunomodu-latory effects. On the contrary, normal, late apoptotic, or necrotisedcells can stimulate the recipient's lymphocytes.
A recent study describes an absence of tolerogenic effects afterinfusion of donor apoptotic cells [38]. Donor lymphocyteswere renderedapoptotic by gamma radiation or UVA radiation after sensitization bypsoralens, and their infusion reduced the engraftment of donor bonemarrow when compared to living cells. Interestingly, this study wasperformed with the co-stimulation blockade using anti-CD 154antibodies, which can interfere with the tolerogenic process initiatedby apoptotic cells. Moreover, the assessment method of the apoptoticstagewas performedwith annexin V and actinomycinD staining, but thepercentage of early or late apoptotic cells infused was not described.Indeed, a high proportion of injected cells in a late apoptotic stage couldinduce an inflammation that could explain these results. The same result
120 M. Hivelin et al. / Transplant Immunology 21 (2009) 117–128
could be expected if an excessive amount of early apoptotic cells thatoverwhelmed the clearance processwas infused into the recipient. Someof these cells would undergo late apoptosis and, thus, would becomepro-inflammatory before their delayed engulfment.
The total clearance of early apoptotic cells before they undergo lateapoptosis is crucial to induce tolerance.
Fig. 1. Principles of extracorporeal photopheresis in composite tissue allotransplantationphotopheresis remain hypothetical). APC: Antigen-presenting cell. CM: Co-stimulatory molerequired to activate the effector T-cells, thus leading to anergy).
2.9. Engulfment by monocytes, macrophages, and immature dendriticcells (Fig. 1)
The fate of these early apoptotic cells is to be engulfed as fast aspossible by macrophage and immature dendritic cells, both immatureantigen-presenting cells. This engulfment mainly occurs in the spleen.
s (some of the mechanisms described to explain the immunomodulatory effect ofcule (the immature dendritic cells do not express the co-stimulatory molecules that are
121M. Hivelin et al. / Transplant Immunology 21 (2009) 117–128
As described above, the removal, or clearance, of apoptotic cells is amechanism used to eliminate all unnecessary cells without inducing animmune response, thus limiting the risk of causing collateral damage inhealthy tissue.
This rapid clearance has been demonstrated to have immunosup-pressive effects [39] due to inhibitory signals and the absence of co-stimulation of the effector T-cells.
Dendritic cells, as professional antigen-presenting cells (APCs)presentdonor allo- or auto-antigens to T-cells in the presence or absence of anassociationwith co-stimulatorymolecules, depending on their mature orimmature stage. This presentation is called direct whenperformed by thedonor's APCs or indirect when performed by the recipient's APCs.
Apoptotic cells produce anti-inflammatory cytokines, such as IL-10 orTGF-beta. This anti-inflammatory environment stimulates monocyte–machrophage cells or immature dendritic cells to engulf the apoptoticcells. These APCs then produce immunoregulatory cytokines (IL-10 orTGF-beta) and decrease their production of pro-inflammatory cytokines(e.g., TNF-alpha, IL-1, or IL-12) [40].
Recent studies demonstrated that there is a secretion of anti-inflammatory cytokines resulting from the phagocytosis of apoptoticcells. Before these studies, the lack of an anti-inflammatory responseafter apoptosis was only attributed to the rapid engulfment of theapoptotic cells before cell lysis occurs, thus avoiding the release of theirinflammatory contents into the local environment [41]. It has also beensuggested that the greater resistance to apoptosis induced by ECP ofperipheral blood monocytes, when compared to lymphocytes, couldexplain the anti-inflammatory response observed [42].
2.10. Interactions between the early apoptotic cells and immaturedendritic cells
2.10.1. A total and rapid clearance of early apoptotic cells is requiredThe concept of apoptotic cell clearance has been well studied for
autoimmune diseases such as systemic lupus erythematosus (SLE) or
Fig. 2. Differences in staining, phagocytes, and anti- or pro-inflammatory effects for the diffeerythematosus. Rheum Dis Clin North Am, 2004. 30(3): p. 505–27). Annexin V: Staining whmembrane, which occurs at a very early stage of apoptosis. Propidium iodine (PI), staining calate stages of apoptosis.
pemphigus. Indeed, a deficiency in apoptotic cell clearance issuspected to lead to auto-reactivity [43–45].
When the apoptotic load exceeds the phagocytic capacity toengulf the cells before they become late apoptotic or even necrotic,the cells secrete pro-inflammatory cytokines and are then phagocy-tosed by mature antigen-presenting cells, such as mature dendriticcells. This last pattern of phagocytosis leads to pro-inflammatoryeffects such as rejection of an allotransplant in a recipient or toautoimmune disease.
As this rapid clearance of the early apoptotic cells is mandatory toavoid an auto- or allo-immune reaction, any protocol based on theinjection of apoptotic cells should consider the precise amount of earlyapoptotic cells to inject, which could differ, depending on someone'sclearance capacity.
2.10.2. Apoptotic lymphocytes induce changes in cytokine secretionpatterns [31]
T-lymphocyte cytokine secretion patterns are described by a TH1pattern, with IL-2, IFNγ, or TNFα secretion, and by a TH2 pattern, withIL-4 or IL-5 secretion.
However, changes in cytokine levels and changes in the Th1/Th2ratio induced after the phagocytosis of apoptotic cells, from a pro- to ananti-inflammatory profile, remain controversial [31]. Some studiespresent a stimulation of effector T-cells [46], while others relate anti-inflammatory responses [47]. A pro-inflammatory response couldexplain the efficiency of ECP in CTCL, and ananti-inflammatory responsecould explain the effects on allotransplant rejection or autoimmunediseases.
Finally, the decrease in pro-inflammatory cytokines post ECP is notrelated to a simple decrease in the number of T-cells due to apoptosis[48]. Indeed, only 15% of the total number of T-cells is treated duringone ECP session. Moreover, UV-induced early apoptotic cells alsosecrete immune suppressive cytokines, such as IL-4 and IL-10 [49].
rent stages in apoptosis. (Modified from Sheriff, A. et al., Apoptosis and systemic lupusich binds phosphatidyl-serine residues once they are exposed on the outside of the celln penetrate cells after the alteration of their membranes during necrosis and during the

122 M. Hivelin et al. / Transplant Immunology 21 (2009) 117–128
2.11. Replacement of the “suppressor” T-cell concept by the regulatory T-cell(T-Regs) idea
The benefits of ECP on autoimmune diseases and transplantrejection as well as the T-cell phenotypes responsible for inhibition ofthe immune response remain unclear, and two main theories areconsidered from a historical perspective.
The first is based on an anticlonal immunity theory, which involvessuppressor T-cells that act by a “vaccine-like” process [50], as firstintroduced by Kripke's studies [51].
The second is based on tolerance induction by anergy or peripheraldeletion and by regulatory T-cell activation.
Early descriptions of antigen-specific suppressor T-cells generatedafter UV radiationwere observed after UVB radiation [8,51]. This T-cellsubset was supposed to inactivate alloreactive T-cells. In the samestudy, immunosuppressive properties were transferred by adoptivetherapy of suppressive T-cells found in previously UVB-radiated mice.
Other studies used adoptive therapy between UVB-radiated miceto search for lymphocyte subsets supporting the alloreactive T-celldeletion concept [52,53]. The existence of suppressor cells, to explainimmunomodulatory effects following UV radiation, was demonstratedin the 1970s [54] when donor-specific immunosuppression wasobtained in mice and when the host was UVB radiated beforesensitization with allogenic spleen cells [55]. Interestingly, the sameeffect was obtained by the direct radiation of the donor skin [56].
The second theory to explain the immunomodulativeproperties relieson the induction of regulatory T-cells [5,57–63]. CD4+CD25+Foxp3+cells are known todown-regulate the immune response. This last conceptwas first introduced by Rivas and Ulrich [64], with immunomodulatoryeffects explained by IL-4 and IL-10 regulatory cytokines, provided byregulatory T-cells CD4+CD8−.
This theory is compatible with the induction of effector T-cellanergy after ECP. Anergy is the peripheral inactivation of alloreactiveT-cells after antigen presentation by APCs without co-stimulationmolecules in an anti-inflammatory cytokine environment.
ECP seemed to enhance the immune tolerance instead of inducingan immunosuppression [65].
2.12. Donor-specific or non-specific immunomodulation
The first studies on suppressor T-lymphocytes induced by UVradiation promoting tolerance for tumor engraftment in micedescribed this suppression to be cell-mediated, adoptively transferred,and specific [53,54,66]. It is still unclear whether the effects are donorspecific or whether the immunomodulation is non-specific and onlylinked to the secretion of immunoregulatory interleukins, such as IL-4,IL-10, or TGF-beta.
If the immunomodulation through apoptotic cells injections is donorspecific, ECP could be performed on the donor lymphocytes after theircollection before organ harvesting, and these donor-origin leukocyteswould be injected during the immunosuppressive induction protocol.
This description of apoptosis stages after ECP is helpful tounderstand the molecular principles, but some of the mechanismsdescribed to explain the immunomodulatory effect of photopheresisremain hypothetical. It even remains controversial as to whether cellapoptosis is relevant for immunomodulation.
3. Indications for photopheresis in solid organ transplantations
All UV-mediated therapies such as UVA with or without psoralensensitization, and UVB radiation are efficient therapies in immunologicdisorders via their immunomodulating effects [67–69].
ECP has been used in dermatology for cutaneous T-cell lymphoma[9,70,71] and in autoimmune diseases, such as systemic sclerosis,systemic lupus, pemphigus, ulcerative colitis, or atopic dermatitis[5,72]. Other autoimmune diseases, such as inflammatory bowel
disease or rheumatoid arthritis, can also benefit from this therapy[72,73].
Indications in hematology include graft versus host diseasetreatment and after bone marrow or stem cell allotransplantation,particularly for steroid refractory transplantations [74–80].
ECP indications in solid organ transplantation can be divided intoacute [15,20,81–84] and chronic [85] rejection episodes treatments.
3.1. ECP in experimental organ transplantations
The use of ECP implementation to prevent or treat rejectionepisodes can be traced back to 1985, when the first transplantation ofa UVA-radiated rat kidney after administration of 8-methylpsoralenwas reported [86]. In 1989, the first ECP implementation in a primatemodel was performed for heterotrophic heart xenotransplantation(from cynomolgus monkey to baboon) and for allotransplantation(baboon to baboon) [87,88]. Animals were submitted to ECP twice aweek, starting 3 days after transplantation; controls only receivedcyclosporine and steroids. In this study, an absence of hyperacuterejection, an increased graft survival, and a suppression of response inmixed lymphocyte reaction (MLR) were observed in recipientspresensitized by donor blood. In two animals, biopsy-proven rejectionepisodes were reversed in the photochemotherapy groups, whereascontrols suffered from progressive rejection.
This study demonstrated how ECP could specifically suppressrecipient immune responses to donor xenoantigens, while maintainingthe capacity to respond to other unrelated antigens.
Thus, the suppression induced by photochemotherapy seemsspecific for the immunoreactive cell type [12].
For small bowel transplantation, ECP was only introduced inexperimental models [89]. In this study, small bowel transplantationswere performed from ACI rat donors to LEW rat recipients. These ratsreceived either donor splenocytes (radiated or not) or FK506, or boththerapies combined.
The non-radiated splenocytes did not delay the rejection, whichoccurred in one week. The donor splenocytes submitted to radiationslightly improved the survival, as did the FK506 cells alone. Whenradiated splenocytes and FK506 were combined, the small bowelsurvival was dramatically increased: 86 days on average (Pb0.005),and up to 100 days for 7 animals out of 24.
Using this last example, we want to insist that there are numerouscommon points between tolerance induction through apoptoticlymphocyte injections and extracorporeal phototherapy.
The main difference between these two types of treatments is theorigin of the apoptotic cells: from donor origin in the studies withapoptotic cell injections and from the recipient (collected byapheresis) in ECP. The second main difference is the timing withregard to the transplantation procedure: before or during thetransplantation for the tolerance inductions with apoptotic cells, andduring or after transplantation for ECP.
3.2. Clinical implementation in transplantations
Since thefirst clinical applications of ECP, its potential as an additionaltherapy to treat the rejection of all kinds of allografts or autoimmunediseases was sensed, leading to many experimental protocols [12] andclinical implementations in solid organ transplantation (Table 1).
3.2.1. Kidney transplantationThe first clinical application of UV radiation in transplantationwas
the treatment of kidney allograft acute rejection [90]. This firstclinical attempt was performed using PUVA therapy (UVA radiationand 8-methylpsoralen), on the donor-kidney before its transplanta-tion. Thirty-three PUVA-pretreated kidneys were compared totwenty-six non-pretreated kidney allografts. The results wereencouraging, as significantly fewer rejection episodes were reported

Table 1Implementation of extracorporeal photopheresis (ECP) in solid organ transplantationsfor the treatment of acute rejection episodes.
Type of solid organ allotransplant Year of introduction (andreference)
Kidney 1987 [88]Heart 1992 [12]Lung 1995 [99]Pancreas 1995 [90]a
Liver 2000 [103]Composite tissue allotransplantation (partial facetransplantation)
2006 [2]
Small bowel –
a The third patient presented among the case reports had received a combinedkidney and pancreas transplantation and is cited as the first implementation of ECP forpancreas transplantation, even if the function of the pancreas is not described after theECP therapy.
123M. Hivelin et al. / Transplant Immunology 21 (2009) 117–128
at 3 months, even if the difference considering the allograft survivalitself was not significant. The number of patients in the studies onkidney rejection treated by extracorporeal photopheresis is relativelylow, when compared to studies involving other solid organs. Twoarticles presenting the same protocols and number of patients forkidney allotransplant rejection, presented contradictory results[91,92].
The extracorporeal photopheresis, also called photochemotherapy,was then used to treat recurrent acute rejection episodes [16] andsteroid refractory acute rejection episodes in kidney transplantation[82,84,92–94].
3.2.2. Heart transplantationCostanzo-Nordin et al. first described the efficiency of ECP as a
complementary treatment for acute rejection in a heart allotrans-plantation [14,95,96] and even described a single cycle of ECP able toreverse moderate acute rejection. After 25 days, the inflammatoryinfiltrate disappeared from the transplants. The recurrent acuterejection of heart allotransplant [15] also became another indicationfor this therapy. A study on the effect of ECP on recurrent or refractorycardiac allograft rejection was performed on 11 patients (with goodresponses for 7), with sessions scheduled as described for heartallograft rejection therapy and a follow up from two to five years [18].The B lymphocytes and the macrophages were also lowered moresignificantly by ECP compared to steroids alone [14]. Because ECP wasworking on the levels of B lymphocytes and cytotoxic antibodies, itwas also indicated for hypersensitized patients [97]. Finally, thebenefits of ECP have even clearly been demonstrated on patientsurvival and allograft function during multiple and or refractoryrejection [98,99].
3.2.3. Lung transplantationLung transplantation is the standard therapy for end-stage lung
deficiency resulting from chronic obstructive pulmonary disease andan increasing number of pulmonary fibrosis cases. Despite potentimmunosuppressive maintenance treatments incorporating tacroli-mus, mycophenolate mofetil, and corticosteroids [100], the develop-ment of chronic allograft rejection, with bronchiolitis obliteranssyndrome (BOS), continues to decrease the long-term survival oflung transplant recipients.
The first introduction of ECP in human lung transplantation wasperformed for an acute rejection episode occurring in a severelyinfected patient [101], who improved clinically after 3 weeks andhistologically after 4 weeks. The same year, ECP was used for lungchronic rejection refractory to steroid doses in 3 patients, allowingstabilization of the degradation of their pulmonary function [102]. ECPfor lung transplantation was then implemented for refractory BOS[103], and the stabilization of pulmonary function and the improve-ment of survival was related tomonthly ECP treatments performed on
2 consecutive days [104]. Patients were receiving a range of 3 to 13ECP, with a median number of 6 [17].
It is interesting to notice that after ECP for lung transplantation,levels of T-Regs did not correlate with the number of photopheresis,but rather, with the lung function itself [58].
There are no studies addressing the prophylactic effect of ECP forlung transplantation.
3.2.4. Pancreas transplantationsAmong the three cases reported in 1995 by Sunder-Plassman about
the use of ECP for acute kidney rejection [92], the third patient hadreceived both a kidney and a pancreas transplant, and was treated byECP for acute rejection. The function of the pancreas allotransplant isunfortunately not reported before or after the ECP therapy. There is noother study on ECP for pancreas transplantation or for Langerhansislets in humans. This case can be considered to be the first onereported about ECP after pancreas transplantation (Table 1).
3.2.5. Liver transplantationsThe implementation of ECP among treatments for liver allograft
rejection was introduced later [105], which could be explained by itssuspected tolerogenic properties, with fewer rejection episodescompared to other solid organ transplantations [106–108].
The studies on ECP for liver transplantation suggested that ECPwould be an alternative to treat recalcitrant graft rejection in somepatient subsets. Rejections occurring with HCV recurrence, steroid-resistant acute rejection, or acute rejection in a major ABO-mismatched liver graft were particularly considered as electiveindications for ECP [20]. ECP was then studied for rejectionprophylaxis. First, ECP was used to delay the calcineurin inhibitorintroduction in high-risk liver allograft recipients (18 patients), so asto decrease the calcineurin inhibitor toxicity without an increase inthe rejection risk in the immediate post-operative time [21].
Then, ECP was applied to ABO-incompatible liver transplantationto prevent antibody-mediated rejection (AMR) and cell-mediatedrejection. The study consisted of 19 patients receiving ABO-incompa-tible allografts, 11, treated by therapeutic plasma exchange (TPE), and8 treated by TPE but also by ECP and receiving immunoglobulin IV. Allpatients also received an immunosuppression regimen, includingsteroids, mycophenolate mofetil, and tacrolimus. The graft survival at6, 12, and 18 months was significantly higher in the second group,treated by ECP and anti-CD25monoclonal antibodies (basiliximab) IV,and no case of acute rejection was noticed after up to 568 days offollow up. The main drawback that can be outlined in the design ofthis study is the introduction of IV immunoglobulin in addition to ECP,which makes it difficult to draw any conclusion about ECP efficiencyon the control of rejection in these ABO-incompatible patients.
Finally, the last implementation of ECP for liver transplantation hasbeen performed in HCV RNA-positive patients receiving livers fromdonors older than 40 years (median age: 66 years). The objective of thisstudy was to reduce the immunosuppressive regimen so as to begin(69.2% of 78 patients could receive the antiviral prophylaxis) to improvethe efficacy of antiviral treatment (interferon and ribavirin) [109].
3.2.6. Intestinal transplantationsTo our knowledge, there is still no description of the use of ECP for
small bowel transplant rejection except for an experimental protocolof an induction therapy with apoptotic splenocytes in a rat smallbowel transplantation model [89].
3.2.7. Phototherapy and bone marrow allograftsThe main indication of ECP after bone marrow transplantation is
for the treatment of graft versus host disease (GVHD), which can alsooccur after stem cell allotransplantation or even after solid organtransplantations. We will not describe the principle and interests ofECP for the treatment of GVHD.

124 M. Hivelin et al. / Transplant Immunology 21 (2009) 117–128
Nevertheless, a better donor bone marrow engraftment has beendescribed inmanyexperimentalmodels after injections of donor-derivedearly apoptotic cells.
In experimental mouse models, injecting UVB-induced apoptoticleukocytes intravenously can facilitate allogenic bone marrow engraft-ment [110].
3.3. ECP sessions schedule
There is no exact number of ECP sessions required to treat acuterejection after organ transplantation, as it is used as an additionaltherapy. ECP used as a treatment for CTCL involved treatment on twosuccessive days every four weeks. This number of session implied thatless than 5% of total body lymphocytes were irradiated each month [9].
Considering the average number of sessions of ECP per patient,after a transplantation, themedian number of ECP sessions per patientwas 20 in a liver transplantation study reported in 2004 [20].
For transplanted patients, the therapy can begin with one to twosessions a week for four weeks and are then tapered, depending onthe effect on the rejection episode.
3.4. Adverse effects of extracorporeal photopheresis
No significant or major side effects are generally observed duringand after the ECP therapy for GVHD treatment, as for the treatment ofrejection episodes in transplantations, in adults or children[17,20,111,112]. However, some adverse effects are reported, such asmalaise, low-grade fever, and gastrointestinal troubles [113].
Some side effects are not specific but linked to repeated and long-term vascular access with large catheters used for apheresis [114]. Theuse of large catheters and the risk of hemostasis troubles withformation of massive thrombosis [115] need to be carefully weighedagainst the benefits.
The number of opportunistic infections is not increased by ECPtreatment, confirming that the immunoregulation induced is specific[16,116]. The reported episodes of sepsis [103] seem to be more likelyrelated to the increased vascular access of the procedure inconjunction with the generally poor health status of the patient.
Minor side effects observed for patients receiving photopheresisinclude hypotension and syncope resulting from volume shifts duringthe leukapheresis phase of treatment.
Although many studies describe ECP as helpful to control allograftrejection [85,95,96,117], there is a lack of prospective randomized trialsand no sufficient evidence to demonstrate an advantage of photopher-esis over othermethods used to treat rejection exists. Thus, ECP remainsan additional therapy in transplantation, rather than a standard therapy.
4. Introduction and relevance of ECP for compositetissue allotransplantations
Composite tissue allotransplantation indications will remain excep-tional until the lifelong immunosuppressive therapy and its adverseeffects are reduced. The immunosuppression currently used in CTA iscomparable with that used for solid organ transplantation. Althoughsome attempts at tolerance induction protocols have been performed inthe clinic, for kidney [118], liver [119], pancreatic islets [120], andcomposite tissue allotransplantations [2,121], tolerance has not beenroutinely achieved, and themost encouraging results obtained in kidneytransplantation were obtained with family-related living donors [118].
4.1. Composite tissue allotransplantations
The first successful hand transplantation was performed in 1999,thanks to amore efficient immunosuppressive treatment than the oneused for the first attempt in 1964 [122,123].
The donor and recipient had the same blood group (O+), but 6human leukocyte antigen (HLA) group mismatches [124]. Therecipient did not observe a continuous immunosuppressive therapy,and signs of cutaneous rejection appeared at 15 months post-transplantation and were partially reversed after reintroduction ofanti-CD25 antibodies and steroids. However, the patient did notpursue the immunosuppressive protocol for a second time, and thus,the transplanted hand was re-amputated after 29 months post-transplantation. No rejections have been reported to lead to a handloss when the immunosuppressive therapy has been well observed.
Despite 19 unilateral and 11 bilateral hand transplantations, 3 facetransplantations, and 38 other subtypes of CTA performed throughoutthe world [125,126] with mainly fair or good functional results and norejection justifying the removal of these allografts when theimmunosuppressive treatment was not interrupted [127], the justi-fication for such procedures is still debated.
For face transplantation, themajority (78.4%) of a panel of 162NorthAmerican plastic surgeons agreed about the limitations of autologousreconstructions for severe facial injuries, but only 27% were in favor ofsuch a procedure under the current immunosuppressive protocols. Theothers would prefer to wait for 10 years of hindsight (16%), for animprovement in immunosuppression (23.8%), or for the clinicalapplication of tolerance induction protocols (28%) [128].
Considering these last two positions, one canwonder what preciselevel of improvement in the immunosuppressive protocols wouldmake the CTA as acceptable as another type of transplantation.
4.2. Rejection and immunosuppressive therapy in CTA
The clinical and histological assessments of the allograft arenecessary and sufficient to detect and prove the rejection in compositetissue allotransplantation because the skin is visible and is the firstcomponent to suffer from rejection.
It is interesting that, contrary to primate models, acute rejectionepisodes in human hand allotransplantation have been completelyreversedwith intravenousmethylprednisolone, provided that thepatientshad a good observance of the immunosuppressive therapy [129]. Somecases also benefited from topical applications of steroid cream.
Considering the face transplantation rejections, this one can bemonitored clinically as a hand allograft. Mild or moderate rejectionepisodes led to methylprednisolone doses but also to antibodyinjections, when the steroid doses were inefficient [2].
In contrast with rejection episodes occurring in hand transplanta-tion which could be controlled by an increase in the dose ofprednisone and local application of tacrolimus and corticosteroidcream, intravenous doses of corticosteroids were necessary to reverseacute rejection in face transplantation.
The numbers of hand and face transplantations remain too small toperform prospective and randomized studies, but different teams arealready using the same patterns for induction and maintenancetherapies. Nevertheless, considering the indication of the varioustreatments for acute rejection, and even maintenance therapy, there isno consensus on the grade of rejection and time to wait for its responseafter methylprednisolone doses before beginning the antibody treat-ment. The same statement can be made for the topical therapy.
4.3. Opportunistic infections management and immunosuppressivetherapy modulation
Risk of opportunistic infection is related to the deepness ofimmunosuppression after the transplantation. For viral infections, thelevel of serology matching between the donor and the recipient alsohas to be considered.
CMV infection is one of the most frequent opportunistic infectionsand is the most frequent systemic viral infection complicating solidorgan transplantation [130–133].

Fig. 3. a. Chronology of the acute rejection episodes and of the introduction of extracorporeal photopheresis after the face transplantations performed in Lyon (legend in b).b. Chronology of the acute rejection episodes and of the introduction of extracorporeal photopheresis after the face transplantations performed in Paris.
125M. Hivelin et al. / Transplant Immunology 21 (2009) 117–128
CMV infection can result in direct effects or CMV disease, related tothe presence of high rates of viral replication, and to indirect effectscaused by virus interactions with the host immune response which canincrease the risk of rejection and graft dysfunction, acceleratedatherosclerosis, opportunistic infections, malignancies, post-transplantdiabetes mellitus, and Guillain–Barré syndrome.
The prophylaxis of CMV infection is based on gancyclovir orvalgancyclovir and on the control of the immunosuppressive protocol.
CMV-related complications in composite tissue allotransplantationshave been described for hand [134], and face transplantations. Amongthe 18 patients who received uni or bilateral hand transplantationsbefore 2005,17 were tested for CMV infection. Three CMV-seronegativerecipients (Lyon-France, Louisville, USA and Insbruck, Austria) receivedCMV-positive hands andwere, thus, exposed to an important viral load.
Considering the increased risk of rejection caused by a CMVinfection, which is also suspected in CTA [134], transplantationsbetween CMV-matched donors and recipients appear mandatory.
ECP is already used to treat acute rejection episodes occurring afterliver transplantation in HCV-positive patients [20]. As CMV alsoincreases the risk of rejection [130–133], ECP would be a valuableadditional treatment for the acute rejection episode, without increas-ing in the level of immunosuppression.
Barr et al. performed a prospective randomized study on the effects ofECPoncardiac allograft acute rejection that showed that cytomegalovirusDNA was detected significantly less frequently in patients receivingphotopheresis than in those receiving the standard therapy [116].
4.4. GVHD in CTA
Another indication of ECP in composite tissue allotransplantationwould be the graft versus host therapy. Nevertheless, as inductionprotocols in CTA or in solid organ transplantation are non myeloa-blative, there is a reduced risk for GVHD, and it has not been reportedfor hand or face transplantation. The experimental models, includingvascularized and unvascularized bone marrow, highlighted this needfor myeloablation to obtain a GVHD in CTA [135,136].
4.5. ECP in CTA (Figs. 1, 3a and 3b)
Two human face transplantations were the first reported clinicalimplementations of extracorporeal photopheresis in composite tissueallotransplantations [2,3].

126 M. Hivelin et al. / Transplant Immunology 21 (2009) 117–128
In both cases ECP was used after the second acute rejectionepisode, to prevent both acute and chronic rejection withoutintensifying the immunosuppressive regimen.
In thefirst case, theauthors suspected aherpes virus infection tohavetriggered the second episode of rejection. On day 185, a Herpes SimplexVirus Type 1 (HSV1) infection of the patient's lip was documented andwas treated by valacyclovir systematically and acyclovir topically.
TheCMVstatuses of both thedonorand the recipient are not indicatedin the early report [137], nor in the 18 month follow up report [2].
ECP was started 2 months after the second rejection episode, thus10 months post-transplantation, in order to reduce the risk of furtheracute rejectionwithout intensifying the immunosuppressive regimen.ECP was performed twice a week for 4 weeks or once a week for8 weeks and was described as well tolerated (Fig. 3a). It was notdetermined whether the HSV1 infection, suspected to have triggeredthe second rejection, was already cured when this rejection began, orwhen the ECP was started.
The second patient who received face transplantation alsobenefited from ECP during the second rejection episode. This secondepisode of rejection was associated with a CMV viremia [3] (Fig. 3b)and required steroid boluses and anti-thymocyte globulin for 7 days.ECP was also started to control the rejection process withoutintensifying the immunosuppressive regimen, as the patient sufferedfrom valgancyclovir-resistant CMV viremia. ECP was performed twiceweekly for 2 weeks, thenwas reduced to one course every 2 weeks for3 months to control subclinical rejection, which persisted on mucosalbiopsies.
ECP has proven to be valuable to treat rejection in liver transplanta-tions challenged by HCV recurrences, and it has been used in facetransplantation for a rejection thatmay have been triggered by a herpesvirus infection.
As ECP has been demonstrated to be a powerful additional therapy toprevent and treat acute, recurrent, and refractory rejection in trans-plantation, the next step was to use it in the anti-rejection therapy forcomposite tissue allotransplantations (CTA), as most of them includeskin, which is considered a strong immunogenic component [138].
It is not clear why ECP was first implemented in face transplanta-tion rather than in hand or abdominal wall transplantations. ECPseems to be an interesting option as an additional therapy for acuterejection episodes, as it does not have the adverse effects ofimmunosuppressive treatment, such as steroid doses, which stillseem to be required for grade 2 rejection episodes.
Themechanisms bywhich ECPworks to prevent allograft rejections,like pathways for apoptosis induction or regulatory T-cells inductionbegin to be understood. Nevertheless, many unknowns remain such asthe precise modification of the cytokines secretion patterns, andwhether the apparent tolerance induction that occurs with ECPtreatment is donor specific or not.
5. Conclusions
Tolerance induction protocols that include apoptotic cell injectionsor extracorporeal photopheresis for the treatment of acute or chronicrejections have effects on apoptotic cells/monocyte–macrophages thepro/anti-inflammatory cytokine profile, and the induction of regulatoryT-cells.
There is still no evidence that these processes are donor specificsince the donor antigens presented after donor apoptotic cellinjections and the recipient antigens presented during photopheresisinduce the same results.
The efficiencyand safety of extracorporeal photopheresis has alreadyproven in solid organ transplantation and in bone marrow transplanta-tionwhen it is used post-operatively during acute rejection episodes oreven in chronic rejection states. Additionally, ECP appears to be atreatment of choice for treating rejections triggered by infections.
Face transplantation was the first implementation of extracorporealphotopheresis for composite tissue allotransplantations.
ECP on the donor and/or recipient blood or tolerance inductionprotocols based on donor early apoptotic cell injections can also be usedbefore the transplantation or during or after the immunosuppressiveinduction, even when there are not any signs of rejection.
Conflict of interest
None of the authors has a financial interest in any of the products,devices, or drugs mentioned in this article.
Acknowledgement
Mikael Hivelin was supported by an additional grant from thePhilippe Foundation, Inc.
References
[1] Vincenti F, Larsen C, Durrbach A, Wekerle T, Nashan B, Blancho G, et al.Costimulation blockade with belatacept in renal transplantation. N Engl J MedAug 25 2005;353(8):770–81.
[2] Dubernard JM, Lengele B, Morelon E, Testelin S, Badet L, Moure C, et al. Outcomes18 months after the first human partial face transplantation. N Engl J Med Dec 132007;357(24):2451–60.
[3] Lantieri L, Meningaud JP, Grimbert P, Bellivier F, Lefaucheur JP, Ortonne N, et al.Repair of the lower and middle parts of the face by composite tissueallotransplantation in a patient with massive plexiform neurofibroma: a 1-yearfollow-up study. Lancet Aug 23 2008;372(9639):639–45.
[4] Ullrich SE. Photoimmune suppression and photocarcinogenesis. Front Biosci Mar1 2002;7:d684–703.
[5] Aubin F, Mousson C. Ultraviolet light-induced regulatory (suppressor) T cells: anapproach for promoting induction of operational allograft tolerance? Transplan-tation Jan 15 2004;77(1 Suppl):S29–31.
[6] Ziegler A, Jonason A, Simon J, Leffell D, Brash DE. Tumor suppressor genemutations and photocarcinogenesis. Photochem Photobiol Apr 1996;63(4):432–5.
[7] Brash DE, Ziegler A, Jonason AS, Simon JA, Kunala S, Leffell DJ. Sunlight andsunburn in human skin cancer: p53, apoptosis, and tumor promotion. J InvestigDermatol Symp Proc Apr 1996;1(2):136–42.
[8] Kripke ML. Antigenicity of murine skin tumors induced by ultraviolet light. J NatlCancer Inst Nov 1974;53(5):1333–6.
[9] Edelson R, Berger C, Gasparro F, Jegasothy B, Heald P, Wintroub B, et al. Treatmentof cutaneous T-cell lymphoma by extracorporeal photochemotherapy. Prelimin-ary results. N Engl J Med Feb 5 1987;316(6):297–303.
[10] Yoo EK, Rook AH, Elenitsas R, Gasparro FP, Vowels BR. Apoptosis induction ofultraviolet light A and photochemotherapy in cutaneous T-cell Lymphoma:relevance to mechanism of therapeutic action. J Invest Dermatol Aug 1996;107(2):235–42.
[11] Greinix HT, Volc-Platzer B, Knobler RM. Extracorporeal photochemotherapy inthe treatment of severe graft-versus-host disease. Leuk Lymphoma Feb 2000;36(5-6):425–34.
[12] Berger CL. Experimental murine and primate models for dissection of theimmunosuppressive potential of photochemotherapy in autoimmune diseaseand transplantation. Yale J Biol Med Nov-Dec 1989;62(6):611–20.
[13] Richter HI, Krutmann J, Goerz G. [Extracorporeal photopheresis in therapy-refractory disseminated discoid lupus erythematosus]. Hautarzt Jun 1998;49(6):487–91.
[14] Costanzo-Nordin MR, Hubbell EA, O'Sullivan EJ, Johnson MR, Mullen GM, HerouxAL, et al. Successful treatment of heart transplant rejection with photopheresis.Transplantation Apr 1992;53(4):808–15.
[15] Dall'Amico R, Livi U, Milano A, Montini G, Andreetta B, Murer L, et al.Extracorporeal photochemotherapy as adjuvant treatment of heart transplantrecipients with recurrent rejection. Transplantation Jul 15 1995;60(1):45–9.
[16] Dall'Amico R, Murer L, Montini G, Andreetta B, Zanon GF, Zacchello G, et al.Successful treatment of recurrent rejection in renal transplant patients withphotopheresis. J Am Soc Nephrol Jan 1998;9(1):121–7.
[17] Salerno CT, Park SJ, Kreykes NS, Kulick DM, Savik K, Hertz MI, et al. Adjuvanttreatment of refractory lung transplant rejection with extracorporeal photopher-esis. J Thorac Cardiovasc Surg Jun 1999;117(6):1063–9.
[18] Dall'Amico R, Montini G, Murer L, Andreetta B, Zacchello G, Gambino A, et al.Extracorporeal photochemotherapy after cardiac transplantation: a new ther-apeutic approach to allograft rejection. Int J Artif Organs Jan 2000;23(1):49–54.
[19] Wise BV, King KE, Rook AH, Mogayzel Jr PJ. Extracorporeal photopheresis in thetreatment of persistent rejection in a pediatric lung transplant recipient. ProgTransplant Mar 2003;13(1):61–4.
[20] Urbani L, Mazzoni A, Catalano G, De Simone P, Vanacore R, Pardi C, et al. The use ofextracorporeal photopheresis for allograft rejection in liver transplant recipients.Transplant Proc Dec 2004;36(10):3068–70.
[21] Urbani L, Mazzoni A, De Simone P, Catalano G, Coletti L, Petruccelli S, et al.Avoiding calcineurin inhibitors in the early post-operative course in high-risk

127M. Hivelin et al. / Transplant Immunology 21 (2009) 117–128
liver transplant recipients: The role of extracorporeal photopheresis. J ClinApheresis 2007;22(4):187–94.
[22] Barr ML. Photopheresis in transplantation: future research and directions.Transplant Proc Aug 1998;30(5):2248–50.
[23] Bladon J, Taylor PC. Extracorporeal photopheresis induces apoptosis in thelymphocytes of cutaneous T-cell lymphoma and graft-versus-host diseasepatients. Br J Haematol Dec 1999;107(4):707–11.
[24] Godar DE. UVA1 radiation triggers two different final apoptotic pathways. J InvestDermatol Jan 1999;112(1):3–12.
[25] Bladon J, Taylor PC. Extracorporeal photopheresis in cutaneous T-cell lymphomaand graft-versus-host disease induces both immediate and progressive apoptoticprocesses. Br J Dermatol Jan 2002;146(1):59–68.
[26] Godar DE. Light and death: photons and apoptosis. J Investig Dermatol Symp ProcSep 1999;4(1):17–23.
[27] Godar DE, Miller SA, Thomas DP. Immediate and delayed apoptotic cell deathmechanisms: UVA versus UVB and UVC radiation. Cell Death Differ Jul 1994;1(1):59–66.
[28] Bladon J, Taylor PC. Lymphocytes treated by extracorporeal photopheresisdemonstrate a drop in the Bcl-2/Bax ratio: a possible mechanism involved inextracorporeal-photopheresis-induced apoptosis. Dermatology2002;204(2):104–7.
[29] Gerber A, Bohne M, Rasch J, Struy H, Ansorge S, Gollnick H. Investigation ofannexin V binding to lymphocytes after extracorporeal photoimmunotherapy asan early marker of apoptosis. Dermatology 2000;201(2):111–7.
[30] Tambur AR, Ortegel JW, Morales A, Klingemann H, Gebel HM, Tharp MD.Extracorporeal photopheresis induces lymphocyte but not monocyte apoptosis.Transplant Proc Jun 2000;32(4):747–8.
[31] Bladon J, Taylor PC. Extracorporeal photopheresis: a focus on apoptosis andcytokines. J Dermatol Sci Aug 2006;43(2):85–94.
[32] Fadok VA, Chimini G. The phagocytosis of apoptotic cells. Semin Immunol Dec2001;13(6):365–72.
[33] Henson PM, Bratton DL, Fadok VA. Apoptotic cell removal. Curr Biol Oct 2 2001;11(19):R795–805.
[34] HoffmannPR, deCathelineau AM,Ogden CA, Leverrier Y, BrattonDL, Daleke DL, et al.Phosphatidylserine (PS) induces PS receptor-mediated macropinocytosis andpromotes clearance of apoptotic cells. J Cell Biol Nov 12 2001;155(4):649–59.
[35] Fadok VA, de Cathelineau A, Daleke DL, Henson PM, Bratton DL. Loss ofphospholipid asymmetry and surface exposure of phosphatidylserine is requiredfor phagocytosis of apoptotic cells by macrophages and fibroblasts. J Biol ChemJan 12 2001;276(2):1071–7.
[36] Vermes I, Haanen C, Steffens-Nakken H, Reutelingsperger C. A novel assay forapoptosis. Flow cytometric detection of phosphatidylserine expression on earlyapoptotic cells using fluorescein labelled Annexin V. J Immunol Methods Jul 171995;184(1):39–51.
[37] Breuckmann F, von Kobyletzki G, Avermaete A, Radenhausen M, Hoxtermann S,Pieck C, et al. Mechanisms of apoptosis: UVA1-induced immediate and UVB-induced delayed apoptosis in human Tcells in vitro. J Eur Acad Dermatol VenereolJul 2003;17(4):418–29.
[38] Li JM, Gorechlad J, Larsen CP, Waller EK. Apoptotic donor leukocytes limit mixed-chimerism induced by CD40-CD154 blockade in allogeneic bone marrowtransplantation. Biol Blood Marrow Transplant Dec 2006;12(12):1239–49.
[39] Voll RE, Herrmann M, Roth EA, Stach C, Kalden JR, Girkontaite I. Immunosup-pressive effects of apoptotic cells. Nature Nov 27 1997;390(6658):350–1.
[40] Saas P, Bonnefoy F, Kury-Paulin S, Kleinclauss F, Perruche S. Mediators involved inthe immunomodulatory effects of apoptotic cells. Transplantation Jul 15 2007;84(1 Suppl):S31–4.
[41] Savill J, Fadok V, Henson P, Haslett C. Phagocyte recognition of cells undergoingapoptosis. Immunol Today Mar 1993;14(3):131–6.
[42] Rook AH, Suchin KR, Kao DM, Yoo EK, Macey WH, DeNardo BJ, et al.Photopheresis: clinical applications andmechanism of action. J Investig DermatolSymp Proc Sep 1999;4(1):85–90.
[43] Wolf R, Matz H, Ruocco E, Ruocco V. The putative role of apoptosis in theinduction of pemphigus. Med Hypotheses 2005;64(1):44–5.
[44] Kuhn A, Bijl M. Pathogenesis of cutaneous lupus erythematosus. Lupus 2008;17(5):389–93.
[45] Munoz LE, van Bavel C, Franz S, Berden J, HerrmannM, van der Vlag J. Apoptosis inthe pathogenesis of systemic lupus erythematosus. Lupus 2008;17(5):371–5.
[46] Tokura Y, Seo N, Yagi H, Wakita H, Moriwaki S, Furukawa F, et al. Treatment ofT lymphocytes with 8-methoxypsoralen plus ultraviolet A induces transient butbiologically active Th1-skewing cytokine production. J Invest Dermatol Aug1999;113(2):202–8.
[47] Bladon J, Taylor PC. Lymphocytes treated by extracorporeal photopheresis candown-regulate cytokine production in untreated monocytes. PhotodermatolPhotoimmunol Photomed Dec 2005;21(6):293–302.
[48] Bladon J, Taylor PC. Early reduction in number of T cells producing proin-flammatory cytokines, observed after extracorporeal photopheresis, is not linkedto apoptosis induction. Transplant Proc Jun 2003;35(4):1328–32.
[49] Tomimori Y, Ikawa Y, Oyaizu N. Ultraviolet-irradiated apoptotic lymphocytesproduce interleukin-10 by themselves. Immunol Lett Jan 10 2000;71(1):49–54.
[50] Perez MI, Edelson RL, John L, Laroche L, Berger CL. Inhibition of antiskin allograftimmunity induced by infusions with photoinactivated effector T lymphocytes(PET cells). Yale J Biol Med Nov-Dec 1989;62(6):595–609.
[51] Kripke ML, Fisher MS. Immunologic parameters of ultraviolet carcinogenesis.J Natl Cancer Inst Jul 1976;57(1):211–5.
[52] Daynes RA, Spellman CW, Woodward JG, Stewart DA. Studies into thetransplantation biology of ultraviolet light-induced tumors. TransplantationApr 1977;23(4):343–8.
[53] Spellman CW, Daynes RA. Modification of immunological potential by ultravioletradiation. II. Generation of suppressor cells in short-term UV-irradiated mice.Transplantation Aug 1977;24(2):120–6.
[54] Daynes RA, Spellman CW. Evidence for the generation of suppressor cells byultraviolet radiation. Cell Immunol Jun 1 1977;31(1):182–7.
[55] Ullrich SE, Magee M. Specific suppression of allograft rejection after treatment ofrecipient mice with ultraviolet radiation and allogeneic spleen cells. Transplanta-tion Jul 1988;46(1):115–9.
[56] Vermeer BJ, Santerse B, Van De Kerckhove BA, Schothorst AA, Claas FH.Differential immune response of congenic mice to ultraviolet-treated majorhistocompatibility complex class II-incompatible skin grafts. TransplantationMar1988;45(3):607–10.
[57] George JF, Gooden CW, Guo WH, Kirklin JK. Role for CD4(+)CD25(+) T cells ininhibition of graft rejection by extracorporeal photopheresis. J Heart LungTransplant Jun 2008;27(6):616–22.
[58] Meloni F, Cascina A, Miserere S, Perotti C, Vitulo P, Fietta AM. Peripheral CD4(+)CD25(+) TREG cell counts and the response to extracorporeal photopheresis inlung transplant recipients. Transplant Proc Jan-Feb 2007;39(1):213–7.
[59] Lamioni A, Carsetti R, Legato A, Landolfo A, Isacchi G, Emma F, et al. Induction ofregulatory T cells after prophylactic treatment with photopheresis in renaltransplant recipients. Transplantation May 27 2007;83(10):1393–6.
[60] Biagi E, Di Biaso I, Leoni V, Gaipa G, Rossi V, Bugarin C, et al. Extracorporealphotochemotherapy is accompanied by increasing levels of circulating CD4+CD25+GITR+Foxp3+CD62L+ functional regulatory T-cells in patients withgraft-versus-host disease. Transplantation Jul 15 2007;84(1):31–9.
[61] Maeda A, Schwarz A, Kernebeck K, Gross N, Aragane Y, Peritt D, et al. Intravenousinfusion of syngeneic apoptotic cells by photopheresis induces antigen-specificregulatory T cells. J Immunol May 15 2005;174(10):5968–76.
[62] Lamioni A, Parisi F, Isacchi G, Giorda E, Di Cesare S, Landolfo A, et al. Theimmunological effects of extracorporeal photopheresis unraveled: induction oftolerogenic dendritic cells in vitro and regulatory T cells in vivo. TransplantationApr 15 2005;79(7):846–50.
[63] Schwarz T. Regulatory T cells induced by ultraviolet radiation. Int Arch AllergyImmunol Jul 2005;137(3):187–93.
[64] Rivas JM, Ullrich SE. The role of IL-4, IL-10, and TNF-alpha in the immunesuppression induced by ultraviolet radiation. J Leukoc Biol Dec 1994;56(6):769–75.
[65] Peritt D. Potential mechanisms of photopheresis in hematopoietic stem celltransplantation. Biol Blood Marrow Transplant Jan 2006;12(1 Suppl 2):7–12.
[66] Spellman CW, Woodward JG, Daynes RA. Modification of immunologicalpotential by ultraviolet radiation. I. Immune status of short-term UV-irradiatedmice. Transplantation Aug 1977;24(2):112–9.
[67] Barr ML. Immunomodulation in transplantationwith photopheresis. Artif OrgansAug 1996;20(8):971–3.
[68] Wolfe JT, Lessin SR, Singh AH, Rook AH. Review of immunomodulation byphotopheresis: treatment of cutaneous T-cell lymphoma, autoimmune disease,and allograft rejection. Artif Organs Dec 1994;18(12):888–97.
[69] Maccherini M, Diciolla F, Laghi Pasini F, Lisi G, Tanganelli P, D'Ascenzo G, et al.Photopheresis immunomodulation after heart transplantation. Transplant ProcFeb-Mar 2001;33(1-2):1591–4.
[70] Heald P, Rook A, Perez M, Wintroub B, Knobler R, Jegasothy B, et al. Treatment oferythrodermic cutaneous T-cell lymphoma with extracorporeal photoche-motherapy. J Am Acad Dermatol Sep 1992;27(3):427–33.
[71] Whittaker SJ, Marsden JR, Spittle M, Russell Jones R. Joint British Association ofDermatologists and U.K. Cutaneous Lymphoma Group guidelines for themanagement of primary cutaneous T-cell lymphomas. Br J Dermatol Dec2003;149(6):1095–107.
[72] Oliven A, Shechter Y. Extracorporeal photopheresis: a review. Blood Rev Jun2001;15(2):103–8.
[73] Knobler R. Extracorporeal photochemotherapy–present and future. Vox Sang2000;78(Suppl 2):197–201.
[74] Schooneman F, Claise C. Treatment of graft versus host disease (GVHD) byphotopheresis? Transfus Sci Dec 1996;17(4):527–36.
[75] Vural F, Donmez A, Doganavsargil B, Cagyrgan S, Alper H, Tombuloglu M. Severeintestinal graft versus host disease after donor lymphocyte infusion; response toextracorporeal photochemotherapy. Transfus Apheresis Sci Oct 2005;33(2):129–33.
[76] Dall'Amico R, Messina C. Extracorporeal photochemotherapy for the treatment ofgraft-versus-host disease. Ther Apher Aug 2002;6(4):296–304.
[77] Imanguli MM, Pavletic SZ, Guadagnini JP, Brahim JS, Atkinson JC. Chronic graftversus host disease of oral mucosa: review of available therapies. Oral Surg OralMed Oral Pathol Oral Radiol Endod Feb 2006;101(2):175–83.
[78] Plumas J, Manches O, Chaperot L. Mechanisms of action of extracorporealphotochemotherapy in the control of GVHD: involvement of dendritic cells.Leukemia Nov 2003;17(11):2061–2.
[79] Berger M, Pessolano R, Albiani R, Asaftei S, Barat V, Carraro F, et al. Extracorporealphotopheresis for steroid resistant graft versus host disease in pediatric patients:a pilot single institution report. J Pediatr Hematol Oncol Oct 2007;29(10):678–87.
[80] D'Incan M, Kanold J, Halle P, De Lumley L, Souteyrand P, Demeocq F.[Extracorporeal photopheresis as an alternative therapy for drug-resistant graftversus host disease: three cases]. Ann Dermatol Venereol Feb 2000;127(2):166–70.
[81] Meiser BM, Kur F, Reichenspurner H, Wagner F, Boos KS, Vielhauer S, et al.Reduction of the incidence of rejection by adjunct immunosuppression withphotochemotherapy after heart transplantation. Transplantation Feb 27 1994;57(4):563–8.

128 M. Hivelin et al. / Transplant Immunology 21 (2009) 117–128
[82] Kumlien G, Genberg H, Shanwell A, Tyden G. Photopheresis for the treatment ofrefractory renal graft rejection. Transplantation Jan 15 2005;79(1):123–5.
[83] Giunti G, Schurfeld K, Maccherini M, Tanganelli P, Rubegni P, Alfani D, et al.Photopheresis for recurrent acute rejection in cardiac transplantation. TransplantProc Feb-Mar 1999;31(1-2):128–9.
[84] Genberg H, Kumlien G, Shanwell A, Tyden G. Refractory acute renal allograftrejection successfully treated with photopheresis. Transplant Proc Oct 2005;37(8):3288–9.
[85] Barr ML, Baker CJ, Schenkel FA, McLaughlin SN, Stouch BC, Starnes VA, et al.Prophylactic photopheresis and chronic rejection: effects on graft intimalhyperplasia in cardiac transplantation. Clin Transplant Apr 2000;14(2):162–6.
[86] Oesterwitz H, Scholz D, Kaden J, Mebel M. Prolongation of rat renal allograftsurvival time by donor pretreatment with 8-methoxypsoralen and longwaveultraviolet irradiation of the graft (PUVA therapy). Urol Res 1985;13(2):95–8.
[87] Fuzesi L, Pepino P, Berger CL, Panza A, Chiang YC, Marboe CC, et al.Immunomanipulation of the response to cardiac allo and xenoreactiveleukocytes. Transplant Proc Feb 1989;21(1 Pt 1):537–9.
[88] Pepino P, Berger CL, Fuzesi L, Panza A, Pierson RN, Gutierrez C, et al. Primatecardiac allo-and xenotransplantation: modulation of the immune response withphotochemotherapy. Eur Surg Res 1989;21(2):105–13.
[89] Toyama Y, Murase N, Galvao FH, SakamotoT, NomotoM, Starzl TE, et al. Prolongedsmall bowel graft survival using photochemotherapy and low-dose FK 506.Transplant Proc Oct 1996;28(5):2506–7.
[90] Oesterwitz H, Scholz D, Kaden J, May G, MebelM, Schirrow R, et al. Photochemicaldonor pretreatment in clinical kidney transplantation–preliminary report. UrolRes 1987;15(4):211–3.
[91] Horina JH, Mullegger RR, Horn S, Holzer H, Halwachs G, Kerl H, et al.Photopheresis for renal allograft rejection. Lancet Jul 1 1995;346(8966):61.
[92] Sunder-Plassman G, Druml W, Steininger R, Honigsmann H, Knobler R. Renalallograft rejection controlled by photopheresis. Lancet Aug 19 1995;346(8973):506.
[93] Baron C, Lang P. [Extracorporeal photochemotherapy: a new approach toimmunosuppression in transplantation]. Presse Med Jan 24 1998;27(3):122–5.
[94] Baron C, Norol F, Dahmane D, Desvaux D, Chopin D, Weil B, et al.Photochemotherapy in kidney transplantation: preliminary results. TransplantProc Oct 1996;28(5):2823.
[95] Costanzo-Nordin MR, Hubbell EA, O'Sullivan EJ, Johnson MR, Mullen GM, HerouxAL, et al. Photopheresis versus corticosteroids in the therapy of heart transplantrejection. Preliminary clinical report. Circulation Nov 1992;86(5 Suppl):II242–50.
[96] Costanzo-Nordin MR, McManus BM, Wilson JE, O'Sullivan EJ, Hubbell EA,Robinson JA. Efficacy of photopheresis in the rescue therapy of acute cellularrejection in human heart allografts: a preliminary clinical and immunopathologicreport. Transplant Proc Feb 1993;25(1 Pt 2):881–3.
[97] Rose EA, Barr ML, Xu H, Pepino P, Murphy MP, McGovern MA, et al.Photochemotherapy in human heart transplant recipients at high risk for fatalrejection. J Heart Lung Transplant Jul-Aug 1992;11(4 Pt 1):746–50.
[98] Dall'Amico R, Montini G, Murer L, Andreetta B, Tursi V, Feltrin G, et al. Benefits ofphotopheresis in the treatment of heart transplant patients with multiple/refractory rejection. Transplant Proc Feb-Mar 1997;29(1-2):609–11.
[99] Kirklin JK, Brown RN, Huang ST, Naftel DC, Hubbard SM, Rayburn BK, et al.Rejection with hemodynamic compromise: objective evidence for efficacy ofphotopheresis. J Heart Lung Transplant Mar 2006;25(3):283–8.
[100] Snell GI, Westall GP. Immunosuppression for lung transplantation: evidence todate. Drugs 2007;67(11):1531–9.
[101] Andreu G, Achkar A, Couetil JP, Guillemain R, Heshmati F, Amrein C, et al.Extracorporeal photochemotherapy treatment for acute lung rejection episode.J Heart Lung Transplant Jul-Aug 1995;14(4):793–6.
[102] Slovis BS, Loyd JE, King Jr LE. Photopheresis for chronic rejection of lung allografts.N Engl J Med Apr 6 1995;332(14):962.
[103] O'Hagan AR, Stillwell PC, Arroliga A, Koo A. Photopheresis in the treatment ofrefractory bronchiolitis obliterans complicating lung transplantation. Chest May1999;115(5):1459–62.
[104] Villanueva J, Bhorade SM, Robinson JA, Husain AN, Garrity Jr ER. Extracorporealphotopheresis for the treatment of lung allograft rejection. Ann Transplant2000;5(3):44–7.
[105] Lehrer MS, Ruchelli E, Olthoff KM, French LE, Rook AH. Successful reversal ofrecalcitrant hepatic allograft rejection by photopheresis. Liver Transpl Sep 2000;6(5):644–7.
[106] Starzl TE, Murase N, Thomson A, Demetris AJ. Liver transplants contribute to theirown success. Nat Med Feb 1996;2(2):163–5.
[107] Starzl TE, Murase N, Demetris A, Trucco M, Fung J. The mystique of hepatictolerogenicity. Semin Liver Dis 2000;20(4):497–510.
[108] Starzl TE. The qprivilegedq liver and hepatic tolerogenicity. Liver Transpl Oct2001;7(10):918–20.
[109] Urbani L, Mazzoni A, Colombatto P, Biancofiore G, Bindi L, Tascini C, et al. Potentialapplications of extracorporeal photopheresis in liver transplantation. TransplantProc May 2008;40(4):1175–8.
[110] Bittencourt MC, Perruche S, Contassot E, Fresnay S, Baron MH, Angonin R, et al.Intravenous injection of apoptotic leukocytes enhances bone marrow engraft-ment across major histocompatibility barriers. Blood Jul 1 2001;98(1):224–30.
[111] Perotti C, Torretta L, Viarengo G, Roveda L, Bernuzzi S, Carbone S, et al. Feasibilityand safety of a new technique of extracorporeal photochemotherapy: experienceof 240 procedures. Haematologica Mar 1999;84(3):237–41.
[112] TalpurR,WardS,ApisarnthanaraxN, Breuer-MchamJ,DuvicM.Optimizingbexarotenetherapy for cutaneous T-cell lymphoma. J AmAcad Dermatol Nov 2002;47(5):672–84.
[113] Zackheim HS. Cutaneous T cell lymphoma: update of treatment. Dermatology1999;199(2):102–5.
[114] Bambauer R, Schneidewind-Muller JM, Schiel R, Latza R. Side-effects andcomplications in large-bore catheters for apheresis. Ther Apher Dial Apr 2003;7(2):221–4.
[115] Edelson BT, Donnelly JK, Cox-Potter TS, Shah KS, Dynis MS, Lublin DM. Heparinlow . . . photo no! Transfusion May 2006;46(5):683–4.
[116] Barr ML, Meiser BM, Eisen HJ, Roberts RF, Livi U, Dall'Amico R, et al. Photopheresisfor the prevention of rejection in cardiac transplantation. PhotopheresisTransplantation Study Group. N Engl J Med Dec 10 1998;339(24):1744–51.
[117] Bisaccia E, Klainer AS, Gonzalez J, Schwartz J, Randazzo D, Antonucci LC, et al.Feasibility of photopheresis to reduce the occurrence of restenosis afterpercutaneous transluminal coronary angioplasty: a clinical pilot study. AmHeart J Sep 2001;142(3):461–5.
[118] Kawai T, Cosimi AB, Spitzer TR, Tolkoff-Rubin N, SuthanthiranM, Saidman SL, et al.HLA-mismatched renal transplantation without maintenance immunosuppres-sion. N Engl J Med Jan 24 2008;358(4):353–61.
[119] Alexander SI, Smith N, Hu M, Verran D, Shun A, Dorney S, et al. Chimerism andtolerance in a recipient of a deceased-donor liver transplant. N Engl J Med Jan 242008;358(4):369–74.
[120] Mineo D, Ricordi C, Xu X, Pileggi A, Garcia-Morales R, Khan A, et al. Combinedislet and hematopoietic stem cell allotransplantation: a clinical pilot trial toinduce chimerism and graft tolerance. Am J Transplant Jun 2008;8(6):1262–74.
[121] Levi DM, Tzakis AG, Kato T, Madariaga J, Mittal NK, Nery J, et al. Transplantation ofthe abdominal wall. Lancet Jun 28 2003;361(9376):2173–6.
[122] Gilbert R. Hand transplanted from cadaver is reamputated. Med Trib Med News1964;5(23).
[123] Gilbert R. Transplant is successful with a cadaver forearm. Med Trib Med News1964;5(20).
[124] Kanitakis J, Jullien D, Petruzzo P, Hakim N, Claudy A, Revillard JP, et al.Clinicopathologic features of graft rejection of the first human hand allograft.Transplantation Aug 27 2003;76(4):688–93.
[125] http://www.handregistry.com.[126] LanzettaM, Petruzzo P,Margreiter R,Dubernard JM, Schuind F, BreidenbachW, et al.
The International Registry on Hand and Composite Tissue Transplantation.Transplantation May 15 2005;79(9):1210–4.
[127] LanzettaM, Petruzzo P, Dubernard JM,Margreiter R, Schuind F, BreidenbachW, et al.Second report (1998-2006) of the International Registry of Hand and CompositeTissue Transplantation. Transpl Immunol Jul 2007;18(1):1–6.
[128] Mathes DW, Ploplys E. Survey on current attitudes towards composite tissuetransplantation in north america among burn and plastic surgeons. PlastReconstr Surg June 2008;121(6S):90.
[129] Petruzzo P, Revillard JP, Kanitakis J, Lanzetta M, Hakim NS, Lefrancois N, et al. Firsthuman double hand transplantation: efficacy of a conventional immunosup-pressive protocol. Clin Transplant Oct 2003;17(5):455–60.
[130] Perez-Sola MJ, Caston JJ, Solana R, Rivero A, Torre-Cisneros J. Indirect effects ofcytomegalovirus infection in solid organ transplant recipients. Enferm InfeccMicrobiol Clin Jan 2008;26(1):38–47.
[131] Rubin RH. The indirect effects of cytomegalovirus infection on the outcome oforgan transplantation. Jama Jun 23-30 1989;261(24):3607–9.
[132] Streblow DN, Orloff SL, Nelson JA. Acceleration of allograft failure bycytomegalovirus. Curr Opin Immunol Oct 2007;19(5):577–82.
[133] Toupance O, Bouedjoro-CamusMC, Carquin J, Novella JL, Lavaud S,Wynckel A, et al.Cytomegalovirus-related disease and risk of acute rejection in renal transplantrecipients: a cohort studywith case-control analyses. Transpl Int 2000;13(6):413–9.
[134] Schneeberger S, Lucchina S, LanzettaM, Brandacher G, Bosmuller C, SteurerW, et al.Cytomegalovirus-related complications in human hand transplantation. Transplan-tation Aug 27 2005;80(4):441–7.
[135] Gorantla VS, Prabhune KA, Perez-Abadia G, Ildstad ST, Maldonado C, Orhun HI, et al.Composite tissue allotransplantation in chimeric hosts: part I. Prevention of graft-versus-host disease. Transplantation Apr 15 2003;75(7):922–32.
[136] Tai CY, Strande LF, Eydelman R, Sheng X, VanTran JL, Matthews MS, et al. Absenceof graft-versus-host disease in the isolated vascularized bone marrow transplant.Transplantation Jan 27 2004;77(2):316–9.
[137] Devauchelle B, Badet L, Lengele B, Morelon E, Testelin S, Michallet M, et al. Firsthuman face allograft: early report. Lancet Jul 15 2006;368(9531):203–9.
[138] Lee WP, Yaremchuk MJ, Pan YC, Randolph MA, Tan CM, Weiland AJ. Relativeantigenicity of components of a vascularized limb allograft. Plast Reconstr SurgMar 1991;87(3):401–11.




















