
Herders of Indian and European Cattle Share Their Predominant Allele for Lactase Persistence
Upload
independentCategory
view
0download
0
doi:10.1182/blood-2002-08-2644Prepublished online February 13, 2003;
Yasodha Natkunam, Nancy L Bartlett and Sandra J HorningBradley C Ekstrand, Jennifer B Lucas, Steven M Horwitz, Zhen Fan, Sheila Breslin, Richard T Hoppe, Phase II TrialRituximab in Lymphocyte Predominant Hodgkin's Disease: Results of a
(4217 articles)Neoplasia � (577 articles)Immunotherapy �
(3716 articles)Clinical Trials and Observations �Articles on similar topics can be found in the following Blood collections
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
digital object identifier (DOIs) and date of initial publication. theindexed by PubMed from initial publication. Citations to Advance online articles must include
final publication). Advance online articles are citable and establish publication priority; they areappeared in the paper journal (edited, typeset versions may be posted when available prior to Advance online articles have been peer reviewed and accepted for publication but have not yet
Copyright 2011 by The American Society of Hematology; all rights reserved.20036.the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

0
RITUXIMAB IN LYMPHOCYTE PREDOMINANT HODGKIN’S DISEASE: RESULTS OF A PHASE II TRIAL
Bradley C. Ekstrand1, Jennifer B. Lucas1, Steven M. Horwitz1, Zhen Fan2, Sheila Breslin1, Richard T. Hoppe3, Yasodha Natkunam2,
Nancy L. Bartlett4, and Sandra J. Horning1
Departments of Medicine (Oncology)1, Pathology2, and Radiation Oncology3, Stanford University School of Medicine, Stanford, CA; and
Department of Medicine (Oncology)4, Washington University, St. Louis, MO.
Scientific heading: Clinical observations, interventions, and therapeutic trials
Running Title: Rituximab in LPHD
Word Counts: Abstract: 239 words; Article: 3052 words
Financial Support: supported by a grant from Genentech and by National Institutes of Health grant R01-CA56060
Correspondence: Sandra J. Horning, MDDivision of OncologyStanford University1000 Welch Road, Suite 202Palo Alto, CA 94304Tel: 650-725-6456Fax: [email protected]
Copyright (c) 2003 American Society of Hematology
Blood First Edition Paper, prepublished online February 13, 2003; DOI 10.1182/blood-2002-08-2644 For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom
1
ABSTRACT
Lymphocyte predominant Hodgkin’s disease (LPHD) is a unique clinical entity characterized
by indolent nodal disease that tends to relapse after standard radiotherapy or chemotherapy. The
malignant cells of LPHD are CD20+ and therefore rituximab may have activity with fewer late
effects than standard therapy. In this phase II trial, 22 patients with CD20+ LPHD received four
weekly doses of rituximab at 375 mg/m2. Ten patients had previously been treated for HD while
12 patients had untreated disease. All 22 patients responded to rituximab (OR 100%) with CR in
9 (41%), CRu in 1 (5%) and PR in 12 (54%). Acute treatment-related adverse events were
minimal. With a median follow-up of 13 months, 9 patients had relapsed, and estimated median
freedom from progression was 10.2 months. Progressive disease was biopsied in 5 patients: 3
had recurrent LPHD while 2 patients had transformation to large cell non-Hodgkin’s lymphoma
(LCL). All 3 patients with recurrent LPHD were retreated with rituximab, with a second CR
seen in 1 patient and stable disease in 2. Rituximab induced prompt tumor reduction in each of
22 LPHD patients with minimal acute toxicity; however, based on the relatively short response
duration seen in our trial and the concerns about transformation, rituximab should be considered
investigational treatment for LPHD. Further clinical trials are warranted to determine the
optimal dosing schedule of rituximab, the potential for combination treatment, and the possible
relationship of rituximab treatment to the development of LCL.
Email: [email protected]
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

2
INTRODUCTION
Lymphocyte predominant Hodgkin’s disease (LPHD) has long been recognized as the
subtype of Hodgkin’s disease (HD) with the most favorable prognosis. Typical patients are
males in the third or fourth decade of life who present with asymptomatic lymphadenopathy,
usually limited to cervical, axillary, or inguinal regions. The disease is generally indolent, with
slowly progressive lymphadenopathy that is often present for years prior to diagnosis.1
Pathologically, LPHD is characterized by the presence of atypical large cells known as
lymphocytic and/or histiocytic (L&H) cells or “popcorn” cells due to the unique appearance of
their nuclei.2 L&H cells reside within a characteristic cellular background composed mostly of
small B-lymphocytes with fewer numbers of T cells. Recent advances in immunophenotyping
and molecular genetics have confirmed that LPHD represents a B-cell neoplasm likely derived
from a germinal center precursor cell.3 L&H cells express the B-cell marker CD20 and lack
expression of CD15 and CD30, the markers characteristic of classical HD.1 This unique
immunophenotype constitutes an integral component of the definition of LPHD in the current
WHO classification.4
On average, fewer than 400 patients are diagnosed with LPHD each year in the United
States.5 Therefore, our understanding of the clinical features of this subtype has generally
evolved from retrospective reviews of cases seen at single institutions.6 Unfortunately, these
studies differ in patient populations, pathological criteria for the diagnosis of LPHD, and
approaches to treatment. The European Task Force on Lymphoma (ETFL) project on LPHD
sought to address this problem by retrospectively evaluating a large group of patients previously
diagnosed with LPHD using the pathological requirements of the WHO classification. The
results of this study form the basis of our current knowledge of the pathologic and clinical
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

3
features of LPHD and its response to standard Hodgkin’s disease treatment.7,8 The ETFL found
that treatment of LPHD with radiotherapy and/or chemotherapy using standard Hodgkin’s
disease protocols can lead to a complete response (CR) in greater than 95% of patients.8
However, two observations suggest that this approach may not represent the optimal
treatment for patients with LPHD. First, both radiotherapy and chemotherapy are associated
with significant late toxic effects, including secondary malignancies.9 In the ETFL study at least
as many patients died of secondary malignancies as did from LPHD itself.8 Second, despite the
high initial CR rate, these patients tend to relapse continuously over time, with relapses often
occurring greater than 10 years after initial therapy. A plateau in the failure-free survival (FFS)
curve at 10-20 years has only been observed in retrospective single institution studies that have
remarkably long follow-up.10,11 Fortunately, most relapses are not life threatening, and overall
survival is excellent, exceeding 90 percent at 10 years in most published studies.6
Therefore, current LPHD research aims to identify alternative treatment approaches that
possess significant activity but less toxicity. Because L&H cells express CD20, the anti-CD20
antibody rituximab has naturally emerged as a potential treatment option for patients with LPHD.
Two individual case reports have documented complete remission of advanced, recurrent and
chemotherapy-refractory LPHD after 4 weekly doses of rituximab.12,13 In order to formally
define the overall response rate and response duration of this approach, we performed a phase II
trial of rituximab in patients with either newly-diagnosed or recurrent LPHD. Here, we describe
the results of rituximab treatment in 22 patients.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom
4
METHODS
Patients
In 1999 we opened a phase II trial for LPHD patients at Stanford University and Washington
University. The diagnosis was confirmed by institutional pathologists according to morphologic
features and immunohistochemistry with the CD20+, CD15-, CD30- profile. We included
patients with either untreated or previously treated LPHD. Patients were eligible if they were
between the ages of 3 and 70 and had an ECOG performance status of 0-2. Patients were
required to have measurable disease, with at least one lymph node mass measuring ≥ 1.0 cm in
largest dimension, or quantifiable extranodal disease. Adequate end-organ function was required
as follows: absolute neutrophil count of > 1500, platelet count > 50,000, serum creatinine of <
1.5 times the upper limit of normal, and alkaline phophatase, bilirubin, AST, and ALT all less
than 2 times the upper limit of normal. All patients gave written informed consent. The protocol
was approved by the human subjects review board at each of the participating institutions.
Patients were excluded if they had any of the following: radiotherapy or chemotherapy
within the previous 4 weeks, prior monoclonal antibody treatment, major surgery within the
previous 4 weeks, current use of systemic glucocorticoids, or any other previous malignancy
other than cured carcinoma in situ of the cervix or basal cell carcinoma of the skin. Women had
to be of non-childbearing potential or using adequate contraception with a negative pregnancy
test at study entry. We also excluded patients with serious non-malignant disease, such as
congestive heart failure or active, uncontrolled bacterial, viral, or fungal infections.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

5
All patients were evaluated at most 4 weeks prior to initiating treatment with routine medical
history, physical examination, baseline laboratory tests, and baseline computed tomography (CT)
scans of the neck, chest, abdomen, and pelvis to identify all sites of measurable disease.
Treatment and evaluation
Treatment consisted of rituximab (Rituxan, IDEC pharmaceuticals) given as an intravenous
infusion of 375 mg/m2 weekly for four consecutive weeks. Patients were premedicated 30
minutes prior to treatment with oral doses of acetaminophen 650 mg and diphenhydramine 25
mg. Premedication with glucocorticoids was prohibited. Patients were seen in follow up at 1
month after the fourth dose of antibody and then again at 3, 6, 12, 15, 18, and 24 months. At
each of these visits history, physical exam, and determination of CBC and serum chemistries
were obtained. Repeat CT scans of the neck, chest, abdomen, and pelvis were required at 3, 6,
12, 18, and 24 months after the fourth dose of rituximab. Patients with bone marrow
involvement prior to rituximab were required to have a bone marrow biopsy to confirm a
complete response.
Data management and statistics
The primary outcome measure was overall response rate. Response to treatment was
determined on post-treatment CT scans using the criteria of the National Cancer Institute (NCI)
Workshop.14 Freedom from progression (FFP) was calculated starting with the date of the first
rituximab treatment. FFP estimations were performed with the Kaplan-Meier method using
Statview 5.0 (SAS Institute, Carey, North Carolina). Toxicity was measured using the NCI
Common Toxicity Criteria.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

6
A Simon 2-stage optimal trial design was employed.15 It was assumed that rituximab would
be of no further interest if the true overall response rate is 20% or lower, and of interest if the
true response rate is 40% or greater. For rejection of the null hypothesis, 12 responses were
required among a total of 43 patients targeted for enrollment. We terminated the study after 22
patients because the response rate was 100%, indicating that rituximab was of sufficient interest
for further study.
RESULTS
Patient characteristics
From March 1999 to April 2002, 22 patients with either recurrent or untreated LPHD met the
enrollment criteria and agreed to participate. Nineteen patients were treated at Stanford
University and 3 were treated at Washington University. The characteristics of the cohort are
summarized in Table 1. Generally, involved regions were characterized by the presence of
several distinctly abnormal lymph nodes that individually had little bulk. The largest lymph
node in each patient ranged from 1.5 to 5.5 cm. Only two patients had nodes greater than 5 cm
in maximum diameter.
Ten patients had been previously treated for Hodgkin’s disease as outlined in Table 1. The
median time from original diagnosis of Hodgkin’s disease in the relapsed patients was 11.9 years
(range 1 – 33), and the median length of the most recent remission was 9 years (range 0.4 – 27).
Twelve patients had untreated disease, with staging shown in Table 1. The median time from
diagnosis to the start of treatment in these patients was 3 months (range 1.8 – 7.5).
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

7
Toxicity
All 22 patients received the planned treatment on schedule and without dose modification.
Rituximab treatment was well tolerated, and toxicity was limited to mild infusion related
reactions that were expected. No grade III or IV toxicity was seen, and no patient required
hospitalization. Hematologic toxicity was limited to one instance each of leukopenia,
thrombocytopenia, and anemia, all grade 1.
Initial response to treatment
All 22 patients were evaluable for response. As demonstrated in Table 2, the overall
response rate to rituximab was 100 percent. Nine patients (41%) achieved a CR, 1 patient (5%)
achieved an unconfirmed complete response (CRu), and 12 patients (54%) achieved a partial
response (PR). Each patient’s best response was seen within 3 months after treatment. Patients
with relapsed disease had responses similar to untreated patients. We noted that patients with
larger lymph nodes, transdiaphragmatic disease, and > 2 nodal regions involved were generally
less likely to achieve a CR (Table 2). However, these associations were not statistically
significant (all p > 0.1 by Chi squared test), likely due to the limited number of patients in our
study.
Response duration
The responses we observed were in general short-lived. With a median follow up of 13
months (range 3 – 32), 9 patients have relapsed a median of 9 months after start of treatment
(range 6 – 14). The characteristics of these patients are shown in Table 3. Eight patients
relapsed exclusively at sites previously involved with LPHD. We found that the quality of the
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

8
response to rituximab correlated with relapse. At the time of the analysis, only 2 of 10 patients
who attained a CR or CRu had relapsed compared with 7 of 12 patients who had a PR (p =
0.0686 by Chi-squared test).
Figure 1 shows the estimated freedom from progression (FFP) in all 22 patients. No relapses
were seen before 6 months. The estimated probability of progressive disease at 10.2 months was
52% (± standard error of 13%). While the number of patients enrolled makes subgroup analysis
hazardous, patient age, sex, disease extent, and previous treatment did not appear to correlate
with the probability of relapse. However, the quality of response to rituximab (CR/CRu vs. PR)
was a significant predictor of relapse (p = 0.0027 by log-rank test). There have been no deaths,
yielding an overall survival of 100%.
Pathological analysis of relapsed disease
Of the 9 patients who relapsed, 5 underwent re-biopsy to assess the status of their disease.
The characteristics of relapsed patients and the results of these biopsies are summarized in Table
3. Three patients were found to have recurrent LPHD. However, specimens from two other
patients demonstrated evidence of transformation to large cell non-Hodgkin’s lymphomas
(LCL). The subtypes were found to be T-cell rich B-cell lymphoma (TCR-BCL) in patient 1 and
diffuse large B-cell lymphoma (DLBCL) in patient 9.
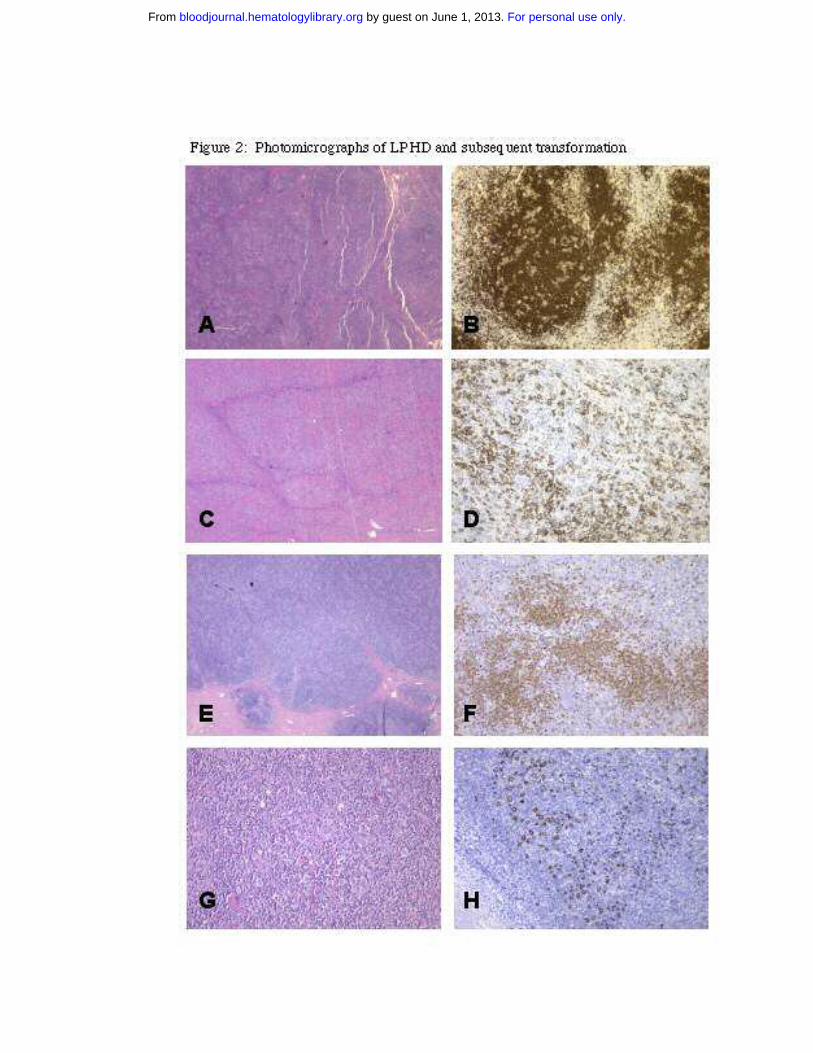
To better understand the potential effect of rituximab treatment on the transformation
process, we performed a dedicated pathological review of the initial biopsy and subsequent LCL
in these two cases. The initial biopsies of both patient 1 and patient 9 showed features typical of
LPHD characterized by a nodular lymphocytic proliferation containing scattered large atypical
CD20+ cells against a small lymphocytic background (Figure 2, A, B, E, F). The biopsy of
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

9
progressive disease in patient 9 demonstrated sheets of CD20+ large atypical cells without
significant nodularity, a typical finding in DLBCL (Figure 2, C). Areas rich in T cells (Figure 2,
D) were rare and did not warrant the diagnosis of TCR-BCL. The LCL that developed in patient
1 contained numerous small T-cells in the background of scattered large neoplastic B-cells, a
pattern typical of TCR-BCL (Figure 2, G&H).
Management of progressive disease
The management of disease progression depended largely on the results of rebiopsy, if
performed (see Table 3). The three patients with recurrent LPHD were re-treated with rituximab.
One patient had a CR one month after retreatment. A second patient had stable disease 4.5
months after treatment. The third patient had stable disease for 16.5 months but then progressed.
A total of 4 patients have been observed for periods ranging from 2 –19 months. These patients
remain asymptomatic from their disease and are doing well.
The patient with diffuse large B-cell lymphoma (patient 9) received 4 weekly infusions of
rituximab followed by CHOP. Interestingly, a positron emission tomography scan that was
positive at relapse became negative after rituximab was given but prior to beginning CHOP. The
patient achieved a complete remission and is currently free of both LPHD and large cell
lymphoma. The patient with TCR-BCL (patient 1) had advanced disease involving the bone
marrow and was started on CHOP chemotherapy. At of the time of this analysis he had received
4 cycles and was in complete remission, including a negative bone marrow biopsy.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

10
DISCUSSION
We report here the results of a phase II trial of rituximab in patients with either untreated or
recurrent LPHD. We have found that rituximab has high initial activity, with an overall response
rate of 100 percent. Patients who had relapsed after standard chemo- or radiotherapy had
responses similar to those who had not been previously treated. Rituximab appeared to be less
effective in patients with greater disease bulk or more widespread disease at baseline. However,
despite the high initial response rate, we found the duration of response to be relatively short.
With a median follow up of 13 months, a total of 9 patients had relapsed. The estimated
probability of relapse reached 50 percent by ten months after the start of treatment. Not
surprisingly, we found that patients who achieved a PR were at significantly higher risk for
relapse than those who attained a CR. Treatment with rituximab was well tolerated, with toxicity
limited to transient infusion reactions.
The initial response rate we observed is essentially identical to that seen in a phase II trial
performed by the German Hodgkin’s Lymphoma Study Group (GHSG)16. These investigators
studied a heterogeneous group of patients with recurrent CD20+ disease, consisting of 10 patients
with LPHD, 2 patients with lymphocyte-rich classical HD, and 2 patients with HD that had
transformed to TCR-BCL. At the time of their most recent analysis, OR was 100% with 7 CR
and 5 PR in 12 assessable patients; 9 of 12 patients were in remission 10 to 26 months after
treatment.16 Differences in eligibility criteria and other patient characteristics may underlie the
variable response durations seen in the two trials. The GHSG study was limited to patients with
relapsed disease and included 4 patients who were not classified as LPHD. The patients in our
study, particularly untreated patients, tended to have more advanced disease than typical LPHD.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

11
Nearly half of the untreated patients were stage III, and overall 10 patients had three or more
nodal sites of disease. Of note, in the ETFL only 20% of patients were stage III or IV.8
In our study, two of the patients with recurrent disease after rituximab treatment were found
on rebiopsy to have transformed to a large cell lymphoma. The occurrence of these 2 cases
within a cohort of 22 patients, when compared to the 2.9% incidence of NHL in the ETFL
study,1 raises concern that rituximab might facilitate transformation. Our cases showed
morphologic and immunophenotypic patterns similar to those of transformed LCL in the absence
of rituximab therapy.17 We found that in both cases the initial LPHD lesions showed an
increased number of extranodular L&H cells, the presence of which has been observed to
correlate with recurrence as well as progression to LCL (Fan et al., manuscript in preparation).
This observation suggested a high risk for transformation in these patients, before rituximab was
given. It is also possible that rituximab created a pathological artifact by depleting the
background B-cell population, leaving a predominance of T-cells and histiocytes. In support of
this view, rituximab treatment has been shown to increase the ratio of T cells to B cells in lymph
nodes affected by low-grade NHL.18
The optimal treatment for patients with LPHD remains uncertain. Radiotherapy for early
stage patients and chemotherapy or combined modality treatment for advanced stage patients
continue to represent the standard of care. Based on the relatively short response duration seen
in our trial and the concerns about transformation, rituximab should be considered an
investigational agent in LPHD. The high initial activity seen in our trial, along with the observed
benefit of re-treatment for relapsed patients, suggests that perhaps alternative dosing schedules or
combination therapy with other treatment modalities might increase response duration. With a
disease as rare as LPHD, the optimal treatment approach can only be defined by cooperative
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

12
efforts between community and academic physicians in prospective clinical trials. We therefore
gratefully acknowledge referrals to our current study.
ACKNOWLEDGEMENTS
The authors would like to thank the following physicians for referral of patients for this
study: James Heckman, Alan Yuen, Peter Sayre, Joseph Szumawski, Tony Reid, Carol Portlock,
Daniel Wong, Brian Lewis, Beverly McLeod, Lawrence Strieff, James Wong, Barbara Beach,
Peter Wong, Thierry Jahan, Charlotte Kim, George Selby, Sidney Crain, Richard Robinson, Alex
Denes, and Shabir Safdar.
REFERENCES
1. Diehl V, Franklin J, Sextro M, Mauch PM. Clinical presentation and treatment of
lymphocyte predominance Hodgkin’s disease. In: Mauch PM, Armitage JO, Diehl V et al.
Hodgkin’s Disease. Philadelphia, PA: Lippincott Williams & Williams; 1999:563-582.
2. Harris NL. Hodgkin’s lymphomas: classification, diagnosis, and grading. Semin Hematol.
1999;36:220-232.
3. Chan WC. Cellular origin of nodular lymphocyte-predominant Hodgkin’s lymphoma:
immunophenotypic and molecular studies. Semin Hematol. 1999;36:242-252.
4. Harris NL, Jaffe ES, Diebold J, et al. World Health Organization classification of
neoplastic diseases of the hematopoietic and lymphoid tissues: report of the clinical
advisory committee meeting—Airlie House, Virginia, November 1997. J Clin Oncol.
1999;17:3835-3849.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

13
5. Jemal A, Thomas A, Murray T, Thun M. Cancer statistics, 2002. CA Cancer J Clin.
2002;52:23-47.
6. Ekstrand BC, Horning SJ. Lymphocyte predominant Hodgkin’s disease. Curr Oncol Rep.
2002;4:424-433.
7. Anagnostopoulos I, Hansmann ML, Franssila K, et al. European Task Force on
Lymphoma project on lymphocyte-predominance Hodgkin’s disease: histologic and
immunohistologic analysis of submitted cases reveals 2 types of Hodgkin disease with a
nodular growth pattern and abundant lymphocytes. Blood. 2000;96:1889-1899.
8. Diehl V, Sextro M, Franklin J, et al. Clinical presentation, course, and prognostic factors in
lymphocyte-predominant Hodgkin’s disease and lymphocyte-rich classical Hodgkin’s
disease: report from the European Task Force on Lymphoma project on lymphocyte-
predominant Hodgkin’s disease. J Clin Oncol. 1999;17:776-783.
9. Dores GM, Metayer C, Curtis RE, et al. Second malignant neoplasms among long-term
survivors of Hodgkin’s disease: a population-based evaluation over 25 years. J Clin Oncol.
2002;20:3484-3494.
10. Regula DP, Hoppe RT, Weiss LM: Nodular and diffuse types of lymphocyte
predominance Hodgkin’s disease. N Engl J Med. 1988;318:214-219.
11. Bodis S, Kraus MD, Pinkus G, et al. Clinical presentation and outcome in lymphocyte-
predominant Hodgkin’s disease. J Clin Oncol. 1997;15:3060-3066.
12. Kielholz U, Szelenya H, Siehl J, et al. Rapid regression of chemotherapy refractory
lymphocyte predominant Hodgkin’s disease after administration of rituximab (anti CD20
monoclonal antibody) and interleukin-2. Leuk Lymphoma. 1999;35:641-642.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

14
13. Lush RJ, Jones SG, Haynes AP. Advanced-stage, chemorefractory lymphocyte-
predominant Hodgkin’s disease: long-term follow-up of allografting and monoclonal
antibody therapy. Br J Haematol. 2001;114:734-735.
14. Cheson BD, Horning SJ, Coiffier B, et al. Report of an international workshop to
standardize response criteria for non-Hodgkin’s lymphomas. J Clin Oncol. 1999;17:1244-
1253.
15. Simon R. Design and analysis of clinical trials. In: DeVita VT, Hellman S, Rosenberg SA,
eds. Cancer: Principles and Practice of Oncology. Philadelphia, PA: Lippincott Williams
& Williams; 2001:521-538.
16. Schulz H, Rehwald U, Reiser M, Diehl V, Engert A. The monoclonal antibody rituximab
is well tolerated and extremely effective in the treatment of relapsed CD20-positive
Hodgkin’s lymphoma—an update [abstract]. Ann Oncol. 2002;13(Suppl 2):63a.
17. Natkunam Y, Stanton TS, Warnke RA, Horning SJ. Durable remission in recurent T-cell-
rich B-cell lymphoma with the anti-CD20 antibody rituximab. Clin Lymphoma. 2001;2:1-
3.
18. Maloney DG, Liles TM, Czerwinski DK, et al. Phase I clinical trial using escalating
single-dose infusion of chimeric anti-CD20 monoclonal antibody (IDEC-C2B8) in patients
with recurrent B-cell lymphoma. Blood. 1994;84:2457-2466.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

15
Table 1: Characteristics of 22 patients with LPHD
CharacteristicRelapsedn = 10
Untreatedn = 12
Male:female 8:2 8:4
Median Age (range) 44 (29 – 61) 45 (18 – 63)
Stage/Relapse StageIIIIII
343
435
B symptoms 0 2
Number of lymph node regions involved
1-2 3-4 > 4
532
741
Relapse history1st relapse2nd relapse4th relapse
631
n.a.
Prior treatmentRadiotherapy
IFRegional*STLI
ChemotherapyMOPPABVDMOPP/ABVDCHOP
232
3221
n.a.
*Mantle (1 pt), Mini-mantle (1 pt), Inverted-Y (1 pt)Abbreviations: IF, involved field; STLI, subtotal lymphoid irradiation; MOPP, mechlorethamine, vincristine, procarbazine, prednisone; ABVD, doxorubicin, bleomycin, vinblastine, dacarbazine; CHOP, cyclophosphamide, doxorubicin, vincristine, prednisone; n.a., not applicable.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

16
Table 2: Results of treatment
Characteristic CR CRu PR
All Patients 9 1 12
Untreated patients 4 0 8
Relapsed patients 5 1 4
Stage/RestageIIIIII
522
010
246
Number of lymph node regions involved
1-2 3-4 > 4
630
100
543
Largest lymph node size 1.5 – 2.0 cm2.1 – 4.0 cm 4.1 – 5.5 cm
360
001
075
Abbreviations: CR, complete response; CRu, unconfirmed complete response; PR, partial response
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

17
Table 3: Summary of the 9 patients who relapsed after rituximab treatment
Patient Age SexStage/
Restage
Initial response to rituximab
FFP(mos)
Histology at progression Treatment Response
Not previously treated
1 60 M IIIA PR 10 TCR-BCL CHOP responding
2 23 M IIIA PR 9 LPHD Rituximab SD (4.5 mos.)
3 38 F IA PR 6 n.d. Observation n.a.
4 45 M IA PR 10 n.d. Observation n.a.
5 32 M IIIA PR 7.5 LPHD Rituximab SD (16.5 mos.)†
6 46 F IIIA CR 14 n.d. Observation n.a.
Previously treated
7 51 M IIIA CR 12 n.d. Observation n.a.
8 25 M IIA PR 7.5 LPHD Rituximab CR (11 mos.)
9 29 M IIA PR 8.5 DLBCL Rituximab followed by
CHOP
CR (12 mos.)
† progressive disease at 16.5 months
Abbreviations: FFP, freedom from progression; n.d., not done; n.a., not applicable; LPHD, lymphocyte predominant Hodgkin’s disease; TCR-BCL, T cell- rich B cell lymphoma; DLBCL, diffuse large B cell lymphoma; CHOP, cyclophosphamide, doxorubicin, vincristine, prednisone; SD, stable disease; CR, complete response
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

18
Figure 1: Freedom from progression
0
.2
.4
.6
.8
1
estim
ated
sur
viva
l
0 5 10 15 20 25 30 35
months
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom
19
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom

20
FIGURE LEGENDS
Figure 1: Freedom from progression in the entire cohort.
Figure 2: Photomicrographs of LPHD and subsequent transformation.
Shown are representative H&E stains (A, C, E, G) and CD20 immunohistochemistry (B, D, F,
H) from patient 9 (A-D) and patient 1 (E-H). A. H&E of initial biopsy of patient 9 showing
nodular proliferation of lymphocytes. B. CD20 stain of initial biopsy highlights large nodules of
B-cells containing scattered large B-cells, characteristic of NLPHD. C. H&E stain of post-
rituximab biopsy at low power showing sheets of large atypical lymphocytes, diagnostic of
DLBCL. D. CD20 stain from C highlights a focal area in which the large CD20+ B cells are
surrounded by negatively stained T cells. E. H&E stain of initial biopsy from patient 1 showing
LPHD with vague nodularity. F. Anti-CD20 antibody stain from highlights loose nodular
aggregates of B-lymphocytes. Scattered large CD20 positive cells (L&H cells) are present
within and outside the B-cell nodules. G. H&E section of post-rituximab transformation to
TCR-BCL showing diffuse proliferation of lymphocytes. CD20 stain of DLBCL (H)
demonstrates scattered CD20 positive large cells with loss of nodularity. The large neoplastic
cells are set against a background of T-cells.
For personal use only. by guest on June 1, 2013. bloodjournal.hematologylibrary.orgFrom
Copyright © 2022 FDOKUMEN




















