
Bendamustine with or without rituximab for the treatment of heavily pretreated non-Hodgkin’s...
10
ORIGINAL ARTICLE Bendamustine with or without rituximab for the treatment of heavily pretreated non-Hodgkin’ s lymphoma patients A multicenter retrospective study on behalf of the Italian Lymphoma Foundation (FIL) Luigi Rigacci & Benedetta Puccini & Sergio Cortelazzo & Gianluca Gaidano & Andrea Piccin & Alfonso D’Arco & Roberto Freilone & Sergio Storti & Enrico Orciuolo & Pier Luigi Zinzani & Francesco Zaja & Velia Bongarzoni & Monica Balzarotti & Delia Rota-Scalabrini & Caterina Patti & Marco Gobbi & Andrea Carpaneto & Anna Marina Liberati & Alberto Bosi & Emilio Iannitto Received: 10 May 2011 / Accepted: 31 January 2012 / Published online: 15 February 2012 # Springer-Verlag 2012 Abstract Bendamustine is an alkylating agent with a nitro- gen mustard group and a purine-like benzimidazole group. The aim of this study was to collect all the Italian experi- ences with this drug in order to evaluate the results in term of response to therapy and toxicities. We analyzed lymphoma patients treated in 24 Italian haematological centres with bendamustine alone or in combination with anti-CD20 anti- body. One hundred seventy-five relapsed or refractory lym- phoma patients were enrolled. The median age was 69 years (range 26–87). Seventy-nine patients were relapsed, 35 were L. Rigacci : B. Puccini : A. Bosi SOD Ematologia, Azienda Ospedaliero Universitaria Careggi, Florence, Italy S. Cortelazzo : A. Piccin UO Ematologia e TMO, Ospedale Regionale San Maurizio, Bolzano, Italy G. Gaidano Division of Hematology, Department of Clinical and Experimental Medicine, Università del Piemonte Orientale Amedeo Avogadro, Novara, Italy A. D’Arco UO Ematologia, Nocera Inferiore, Italy R. Freilone SC Medicina Trasfusionale ed Ematologia ASLTO4 Ciriè, Torino, Italy S. Storti U.O OncoEmatologia, Università Cattolica del Sacro Cuore, Campobasso, Italy E. Orciuolo UO Ematologia, Azienda Ospedaliero Universitaria Pisana, Pisa, Italy P. L. Zinzani Istituto di Ematologia “Seràgnoli”, Università e Ospedale S. Orsola, Bologna, Italy F. Zaja Clinica Ematologica, Centro Trapianti e Terapia Cellulari “Carlo Melzi”, Azienda Ospedaliero Universitaria S. M. Misericordia, Udine, Italy V. Bongarzoni UO Ematologia, Azienda Ospedaliera “S. Giovanni Addolorata”, Rome, Italy M. Balzarotti Hematology Unit, Humanitas Cancer Center Rozzano, Milan, Italy D. Rota-Scalabrini IRCC FPO, Candiolo, Italy C. Patti U.O. Ematologia, A.O. Villa Sofia-Cervello, Palermo, Italy M. Gobbi Clinica Ematologica, Dipartimento di Ematologia e Oncologia, Ospedale San Martino, Genoa, Italy Ann Hematol (2012) 91:1013–1022 DOI 10.1007/s00277-012-1422-5
Transcript of Bendamustine with or without rituximab for the treatment of heavily pretreated non-Hodgkin’s...

ORIGINAL ARTICLE
Bendamustine with or without rituximab for the treatmentof heavily pretreated non-Hodgkin’s lymphoma patientsA multicenter retrospective study on behalf of the Italian Lymphoma Foundation (FIL)
Luigi Rigacci & Benedetta Puccini & Sergio Cortelazzo &
Gianluca Gaidano & Andrea Piccin & Alfonso D’Arco &
Roberto Freilone & Sergio Storti & Enrico Orciuolo &
Pier Luigi Zinzani & Francesco Zaja & Velia Bongarzoni &Monica Balzarotti & Delia Rota-Scalabrini &Caterina Patti & Marco Gobbi & Andrea Carpaneto &
Anna Marina Liberati & Alberto Bosi & Emilio Iannitto
Received: 10 May 2011 /Accepted: 31 January 2012 /Published online: 15 February 2012# Springer-Verlag 2012
Abstract Bendamustine is an alkylating agent with a nitro-gen mustard group and a purine-like benzimidazole group.The aim of this study was to collect all the Italian experi-ences with this drug in order to evaluate the results in termof response to therapy and toxicities. We analyzed lymphoma
patients treated in 24 Italian haematological centres withbendamustine alone or in combination with anti-CD20 anti-body. One hundred seventy-five relapsed or refractory lym-phoma patients were enrolled. The median age was 69 years(range 26–87). Seventy-nine patients were relapsed, 35 were
L. Rigacci :B. Puccini :A. BosiSOD Ematologia, Azienda Ospedaliero Universitaria Careggi,Florence, Italy
S. Cortelazzo :A. PiccinUO Ematologia e TMO, Ospedale Regionale San Maurizio,Bolzano, Italy
G. GaidanoDivision of Hematology, Department of Clinical and ExperimentalMedicine, Università del Piemonte Orientale Amedeo Avogadro,Novara, Italy
A. D’ArcoUO Ematologia,Nocera Inferiore, Italy
R. FreiloneSC Medicina Trasfusionale ed Ematologia ASLTO4 Ciriè,Torino, Italy
S. StortiU.O OncoEmatologia, Università Cattolica del Sacro Cuore,Campobasso, Italy
E. OrciuoloUO Ematologia, Azienda Ospedaliero Universitaria Pisana,Pisa, Italy
P. L. ZinzaniIstituto di Ematologia “Seràgnoli”,Università e Ospedale S. Orsola,Bologna, Italy
F. ZajaClinica Ematologica, Centro Trapianti e Terapia Cellulari “CarloMelzi”, Azienda Ospedaliero Universitaria S. M. Misericordia,Udine, Italy
V. BongarzoniUO Ematologia, Azienda Ospedaliera “S. Giovanni Addolorata”,Rome, Italy
M. BalzarottiHematology Unit, Humanitas Cancer Center Rozzano,Milan, Italy
D. Rota-ScalabriniIRCC FPO,Candiolo, Italy
C. PattiU.O. Ematologia, A.O. Villa Sofia-Cervello,Palermo, Italy
M. GobbiClinica Ematologica, Dipartimento di Ematologia e Oncologia,Ospedale San Martino,Genoa, Italy
Ann Hematol (2012) 91:1013–1022DOI 10.1007/s00277-012-1422-5

refractory and 61 presented a progressive disease after partialresponse. The diagnoses were 60 indolent non-follicular lym-phomas, 34 diffuse large B-cell lymphomas, 48 follicularlymphomas, 30 mantle cell lymphomas and three peripheralT-cell lymphomas. All patients were evaluable for response:52 (29%) with complete remission, 72 (43%) with partialresponse with an overall response rate of 71%, and 51 non-responders. With a median observation period of 10 months(1–43), 70% of patients are alive. In summary, this retrospec-tive study shows that treatment with bendamustine alone or incombination with rituximab is a safe and effective regimen ina subset of multi-resistant patients.
Keywords Bendamustine . Rituximab . Relapsedlymphoma . Antineoplastic agents
Introduction
Non-Hodgkin’s lymphomas (NHL) are a heterogeneousgroup of malignancies. The cellular classification of NHLcomprises more than 30 clinicopathological entities basedon morphology and cell lineage, with the most recent clas-sification system being the WHO modification of theRevised European American Lymphoma (REAL) Classifi-cation (1–3). Patients refractory to chemotherapy or pluri-relapsing have a very poor prognosis particularly in aggres-sive lymphomas (4, 5). Bendamustine has demonstratedclinical activity in several different types of cancer, as pre-viously reported by Barman Balfour in 2001 (6). Bendamus-tine does not show cross-resistance with other cytotoxicdrugs, and it is active in primary NHL cells refractory toconventional chemotherapeutic agents, such as cyclophos-phamide, doxorubicin, etoposide (7–10). In vitro studiesdemonstrate rapid production of DNA crosslinks and strandbreaks after bendamustine exposure (8). In addition to direct
DNA damage and apoptosis, other mechanisms includeinhibition of mitotic checkpoints and induction of themitotic catastrophe (7). These characteristics explain theefficacy of this drug in refractory lymphoma patients andin drug-resistant cells (11). Its proved efficacy as salvagetherapy in indolent mantle cell lymphoma is especiallyinteresting (12, 13). Since 2007 this drug has been used ascompassionate treatment in several Italian hematologicalcenters. We have retrospectively collected the data from allpatients treated with bendamustine with or without rituxi-mab and notwithstanding the histotype. The aim of thisretrospective evaluation was to test the feasibility and effi-cacy of bendamustine with or without immunotherapy inrefractory or heavily pre-treated NHL patients.
Patients and methods
This study was registered in ClinicalTrial.gov (NCT01224769),and the protocol was accepted by the appropriate re-search ethics committees. Patients with a diagnosis ofNHL, age >18 years, progressed or relapsed after at leastone cytostatic treatment and treated with at least one completebendamustine cycle, were consecutively included in the study.Hematological centers were asked to report clinical character-istics and response to therapy of patients treated with bend-amustine as salvage therapy considered a last resort in almostall cases. All patients were evaluable for response to therapyaccording to Cheson criteria (14) and toxicity according to theNational Cancer Institute’s Common Toxicity Criteria (NCI-CTC). Patients treated with one or two cycles of bendamustinewithout any restaging were considered non-responders. Anypatient who otherwise met the criteria for a complete response(CR) but did not have a bone marrow biopsy at the time ofresponsewas considered a partial response (PR). The treatmentsreported were bendamustine 90 mg/m2 on 2 consecutive daysevery 4 weeks, bendamustine 90 mg/m2 on 2 days plus ritux-imab 375 mg/m2 on day 1 every 4 weeks, and bendamustine60 mg/m2 on 2 days plus rituximab 375 mg/m2 on day 1every 3 weeks. The primary objectives of this study were theassessment of overall response rate (ORR) and the toxicityevaluation. Secondary objectives were outcome assessmentand the identification of prognostic factors predictive of re-sponse or survival.
We performed a statistical analysis considering the singlehistotype and dividing the histotypes into indolent (lympho-cytic lymphoma, follicular lymphoma, marginal lymphoma,lymphoplasmacytic lymphoma) and aggressive (diffuse largeB-cell lymphoma, mantle cell lymphoma, peripheral T-celllymphoma). We evaluated adverse features at bendamustinetreatment such as advanced age (> 65 years), advanced AnnArbor stage (III–IV), elevated LDH, poor ECOG-PS, Bsymptoms, bone marrow infiltration and number of previous
A. CarpanetoU.O Ematologia,Ronciglione, VT, Italy
A. M. LiberatiSezione Medicina Interna e Scienza Oncologiche,Azienda Ospedaliera S. Maria Terni,Terni, Italy
E. IannittoUO Ematologia, AOUP Paolo Giaccone,Palermo, Italy
L. Rigacci (*)Division of Hematology and Bone Marrow Transplantation,Azienda Ospedaliera Universitaria Careggi,Via delle Oblate 1,50141 Florence, Italye-mail: [email protected]
1014 Ann Hematol (2012) 91:1013–1022

treatments with or without rituximab, including autologousbone marrow transplantation (ASCT). Overall survival (OS)was considered from the start of salvage therapy with bend-amustine to the last follow-up, relapse or death for any cause.Progression-free survival (PFS) was calculated as the numberof months from the first dose of study drug to the firstdocumentation of disease progression, death regardless ofcause or change in therapy caused by disease progression.The duration of response was calculated as the number ofmonths from the first documentation of response to diseaseprogression or death. If disease progression did not occur bythe end of treatment, patients were evaluated every 3 monthsuntil progression. All included patients were considered in thestatistical analysis. OS and PFS were estimated according tothe Kaplan–Meier method. The log rank test was used toassess the significance of differences for each prognosticfactor in the univariate analysis. The Cox proportional hazardsregressionmodel and the logistic regressionmodels were usedto assess how patients’ characteristics predicted PFS and OS.Statistical analysis was carried out using the Statistical Pack-age for Social Science (15). The limit of significance for allanalyses was defined as p<0.05.
Results
Between January 2007 and December 2009, a total of 175patients were enrolled at 24 institutions and constituted thefinal clinical database. Patients’ characteristics are reported inTable 1. The median age was 69 years (range 26–87 years).According to histology, 67 patients had aggressive lympho-mas (34 diffuse large B-cell NHL, 30 mantle cell NHL andthree peripheral T-cell NHL); 108 had indolent lymphomas(48 follicular NHL, 40 small lymphocytic NHL, 14 marginalNHL and six lymphoplasmacytic NHL). One hundred fifty-five patients had advanced-stage disease (III–IV stage). Priortreatments included rituximab as single agent, chemoimmu-notherapy with rituximab, autologous stem cell transplanta-tion and radiotherapy. Patients received a median of threeprior treatments (range: one to nine). Thirty-nine patients werenot previously treated with rituximab, and 38 were treatedwith an ASCT. Of the 175 patients who were treated withbendamustine, 79 had relapsed, 61 had progressive and 35refractory disease to one or more treatments. Patients receiveda median of four cycles of bendamustine (range: one to nine).Forty-one patients discontinued bendamustine treatment be-cause of an adverse event or disease progression, 18 after onebendamustine cycle and 23 after two cycles. Twenty-fivepatients were treated with three cycles, 42 patients with fourcycles, 12 patients with five cycles and 55 patients with sixcycles. Forty-one patients (23%) were treated with bendamus-tine alone and 134 (77%) with the combination of bendamus-tine and rituximab.
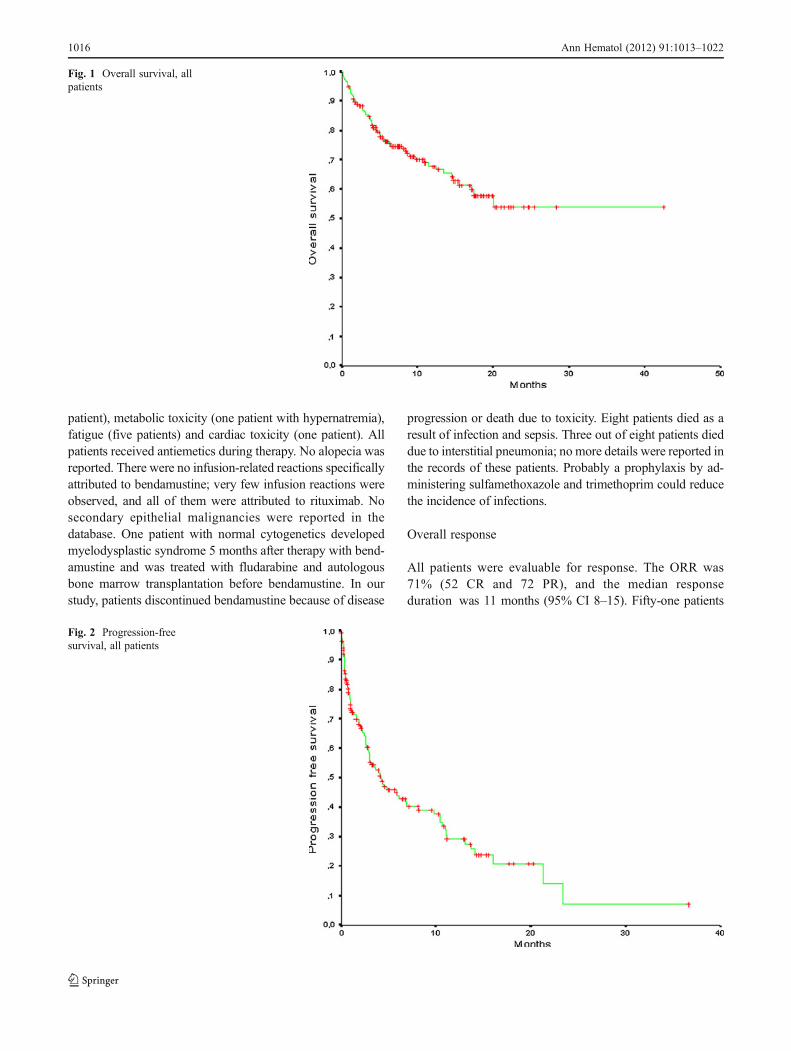
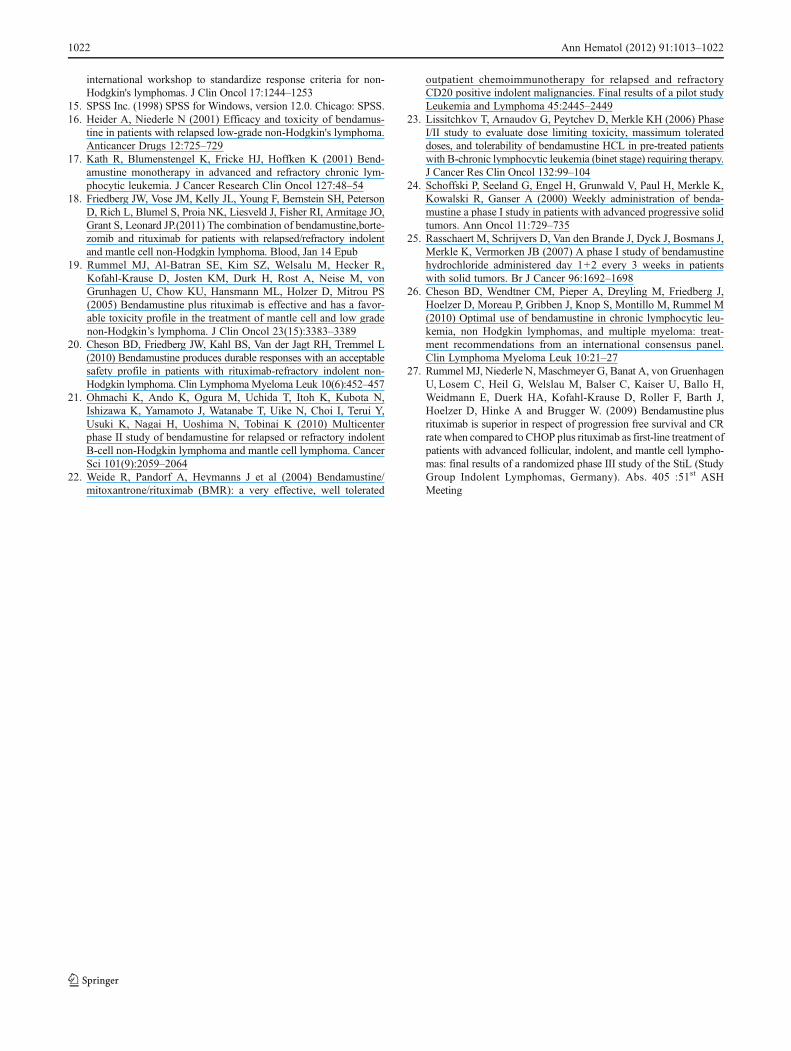
After a median follow-up of 12 months (range 1–48months), the estimated overall survival at 24 months was54%, and after a median follow-up of 10 months (range 0–37 months) (Fig. 1), the estimated PFS at 20 months was20% (Fig. 2). Sixty-six patients (38%) were alive withoutevidence of active disease, 56 (32%) were alive with diseaseand 53 patients (30%) had died. The causes of death wereprogressive disease (78%), infections or other complications(16%) and other unspecified causes (6%).
Safety
Overall, bendamustine was relatively well tolerated in thisheavily pretreated population. No dose reductions werereported in the database. Hematological toxicities, includingneutropenia, anemia and thrombocytopenia, were primarilygrade 0/1/2 in severity (Table 2). Thirty-one patients (18%)presented with grade 3/4 neutropenia, 14 (8%) had grade 3/4anemia and 18 (10%) grade 3/4 thrombocytopenia. Non-hematological adverse events attributed to bendamustineincluded (all grades) nausea and vomiting (ten patients),infection (eight patients, three patients developed interstitialpneumonia), diarrhea (two patients), hepatic toxicity (threepatients), skin rash (15 patients), neurologic toxicity (one
Table 1 Patient characteristics
Characteristics Number Percent
Male 108 62
Female 67 36
Histotype
Lymphocytic 40 23
Lymphoplasmacytic 6 4
Marginal 14 8
Follicular 48 27
Mantle 30 17
Large B cell 34 19
Peripheral T cell 3 2
Pre-bendamustine therapies
≤ 3 113 65
>3 62 35
Pre-bendamustine status
Relapse 79 45
Progression after PR 35 20
Refractory disease 61 35
Previous rituximab
Yes 136 78
No 39 22
Previous transplant
Yes 37 21
No 138 79
Ann Hematol (2012) 91:1013–1022 1015
patient), metabolic toxicity (one patient with hypernatremia),fatigue (five patients) and cardiac toxicity (one patient). Allpatients received antiemetics during therapy. No alopecia wasreported. There were no infusion-related reactions specificallyattributed to bendamustine; very few infusion reactions wereobserved, and all of them were attributed to rituximab. Nosecondary epithelial malignancies were reported in thedatabase. One patient with normal cytogenetics developedmyelodysplastic syndrome 5 months after therapy with bend-amustine and was treated with fludarabine and autologousbone marrow transplantation before bendamustine. In ourstudy, patients discontinued bendamustine because of disease
progression or death due to toxicity. Eight patients died as aresult of infection and sepsis. Three out of eight patients dieddue to interstitial pneumonia; no more details were reported inthe records of these patients. Probably a prophylaxis by ad-ministering sulfamethoxazole and trimethoprim could reducethe incidence of infections.
Overall response
All patients were evaluable for response. The ORR was71% (52 CR and 72 PR), and the median responseduration was 11 months (95% CI 8–15). Fifty-one patients
Fig. 1 Overall survival, allpatients
Fig. 2 Progression-freesurvival, all patients
1016 Ann Hematol (2012) 91:1013–1022

(29%) were refractory to treatment and rapidly pro-gressed. The clinical characteristics associated with theresponse to therapy are reported in Table 3. The group with
indolent lymphoma had a better ORR compared with aggres-sive (85% vs. 48%, p00.000); patients without systemicsymptoms at relapse had a better ORR in comparison with
Table 2 Severity of hematolog-ical and extrahematologicaltoxicities
Number of patients who experi-enced the maximum grade oftoxicity: ainterstitial pneumonia,bincluded nausea and vomitus,cone hypercalcemia and onehyponatriemia
Toxicity WHO 0 WHO 1 WHO 2 WHO 3 WHO 4
Hematological toxicity
Neutropenia (2 missing) 111 8 23 23 8
Anemia (1 missing) 122 24 14 8 6
Trombocytopenia (3 missing) 137 6 11 11 7
Extrahematological toxicity
Infections 2 5 4
Lung toxicitya 1 2 3
Herpes zoster 1 3
Hepatic 2 1 1
Gastro-intestinalb 2 4 1
Neurological 1 1
Metabolicc 1 1
Cardiac 1
Thrombosis 1
Cutaneus erythroderma 5
Table 3 Clinical characteristicsassociated with response totherapy
n.s. not significant
Characteristics Number CR (%) PR (%) NR (%) p
Male 108 28 (26) 44 (41) 36 (33)
Female 67 24 (36) 28 (42) 15 (22) n.s.
Histology
Follicular 48 22 (46) 21 (44) 5 (10)
Lymphocytic 40 8 (20) 24 (60) 8 (20)
DLBCL 34 4 (12) 7 (21) 23 (67)
Mantle 30 12 (40) 9 (30) 9 (30)
Marginal 14 6 (43) 7 (50) 1 (7)
Lymphoplasmacytic 6 0 4 (67) 2 (33)
Peripheral T cell 3 0 0 3 (100) 0.000
Pre bendamustine condition
Relapse 79 28 (35) 27 (35) 24 (30)
Refractory 35 8 (23) 19 (54) 8 (23)
Progression after response 61 16 (26) 26 (43) 19 (31) n.s.
LDH value at relapse (163)
Normal 84 34 (41) 36 (42) 14 (17)
Pathologic 79 14 (18) 31 (39) 34 (43) 0.003
Symptoms at relapse
Yes 126 36 (29) 60 (48) 30 (23)
No 49 16 (33) 12 (24) 21 (43) 0.01
Previous rituximab
Yes 136 43 (32) 55 (40) 38 (28)
No 39 9 (23) 17 (44) 13 (33) n.s.
Previous transplant
Yes 37 10 (27) 10 (27) 17 (46)
No 138 42 (30) 62 (45) 34 (25) 0.03
Ann Hematol (2012) 91:1013–1022 1017

symptomatic patients (75% vs. 56%, p00.01), and patientswith normal LDH value at relapse had a better ORR incomparison with patients with elevated LDH value (83% vs.57%, p00.003).
Patients treated with three or more prior chemotherapyregimens (n062) had an ORR of 73% (15 CRs and 30 PRs)with a median response duration of 7 months (95% CI 3–10), compared to an ORR of 70% (36 CRs and 42 PRs) inpatients receiving three or fewer regimens with a medianresponse duration of 14 months (95% CI 8–20). Among the38 patients treated with ASCTwho relapsed, 10 CRs and 10PRs were observed with a median response duration of 5months (95% CI 3–6).
Single histotype evaluation
Response to therapy according to single histotype is reportedin Table 4.
Indolent non-follicular lymphoma
Fifty-nine patients had a diagnosis of indolent non-follicularlymphoma: 40 small lymphocytic lymphomas (SLL), 14marginal lymphomas and six lymphoplasmacytic lympho-mas. The response to therapy was complete in 14 patients(six with marginal lymphoma and eight with SLL); a partialremission was observed in 35 patients (seven with marginallymphoma, 24 with SLL and four with lymphoplasmacyticlymphoma), and 11 patients were non-responders (one withmarginal lymphoma, eight with SLL and two with lympho-plasmacytic lymphoma). Marginal lymphoma showed anoverall response rate in 94% of patients, SLL in 80% ofpatients and lymphoplasmacytic lymphoma in 67% ofpatients. No significant differences were observed betweenthe two schemes used (monotherapy vs. association). Inunivariate statistical analysis, the only one clinical charac-teristic associated with a better response rate was sex, with91% ORR in women vs. 76% ORR in men (p00.000).
Overall survival was 55% at 10 months, and progression-free survival was 23% at 5 months (Fig. 3).
Follicular lymphoma
Forty-eight patients had a diagnosis of grade I or II follicularlymphoma (FL) according to WHO classification. Accord-ing to response to therapy, ORR was 90% with 22 patients(46%) obtaining a complete remission and 21 (44%) apartial remission. In univariate analysis, a better ORR wasreported in women who showed a higher ORR (100% vs.81%, p00.01), in patients without systemic symptoms (95%vs. 73%, p00.05) and finally in patients with a normal valueof LDH (93% vs. 82%, p00.03). Overall survival was 73%at 12 months, and progression-free survival was 16% at 6months (Fig. 4).
Mantle cell lymphoma
Thirty patients had a diagnosis of mantle cell lymphoma(MCL) according to WHO classification. According to re-sponse to therapy, ORR was 70% with 12 patients (40%)obtaining a complete remission and nine (30%) a partialremission. In univariate analysis, no clinical characteristicsshowed a better ORR reported in patients with a normalLDH value. Overall survival was 39% at 10 months, andprogression-free survival was 10% at 4 months (Fig. 5).
Diffuse large B-cell lymphoma
Thirty-four patients had a diagnosis of diffuse large B-celllymphoma (DLBCL) according to WHO classification.According to response to therapy, ORR was 32% with fourpatients (12%) obtaining a complete remission and seven(20%) a partial remission. In univariate analysis, a betterORR was reported in patients with a normal LDH value atrelapse (70% vs. 17%, p00.001). Overall survival was 35%at 7 months, and progression-free survival was 0 at 3 months(Fig. 6).
Table 4 Response to therapyaccording to single histotype
CR complete remission, PRpartial remission, NRnon-responders
Bendamustine–rituximab Bendamustine
CR PR NR CR PR NR
Indolent (60) [n (%)] 13 (22) 25 (42) 8 (13) 1 (2) 10 (17) 3 (5)
Marginal 5 5 0 1 2 1
Lymphocytic 8 17 7 0 7 1
Lymphoplasmacytic 0 3 1 0 1 1
Follicular (48) [n (%)] 16 (33) 19 (39) 4 (8) 6 (12) 2 (5) 1 (3)
Mantle (30) [n (%)] 8 (27) 8 (27) 6 (20) 4 (13) 1 (3) 3 (10)
DLBCL (34) [n (%)] 3 (9) 6 (18) 18 (53) 1 (3) 1 (3) 5 (14)
PTCL (3) [n (%)] 0 0 3 (100)
1018 Ann Hematol (2012) 91:1013–1022

Discussion
The outcome of patients relapsed or refractory to salvagetreatment is very poor, particularly if they have undergone anumber of salvage therapies.
Bendamustine is a cytotoxic compound that acts primar-ily as an alkylating agent, inducing extensive and durableDNA breaks. Its benzimidazole ring structure may explainits differences from other alkylating agents, activity againstmultidrug-resistant cells and only partial cross-resistance
with other alkylating agents (8). Several relatively smallstudies suggest that it is efficacious for indolent lymphoma.Heider and Niederle (16) reported results of a single-institution trial evaluating bendamustine in 52 patients.The response rate was 73%, with 11% of patients obtaininga CR. The majority of patients were refractory to previousalkylating-agent-based chemotherapy regimens, and the me-dian duration of response to bendamustine was 16 months.Bremer (12) reported a trial of 62 patients with variousindolent histologies treated with an alternative regimen of
Fig. 3 Overall survival (dottedline) and progression-freesurvival (solid line) in indolentnon-follicular lymphomas
Fig. 4 Overall survival (dottedline) and progression-freesurvival (solid line) in follicularlymphomas
Ann Hematol (2012) 91:1013–1022 1019

bendamustine 60 mg/m2 daily for 5 days. In this trial,patients showed a very long mean duration of response (39months), including subjects refractory to alkylating agents.Another small series confirmed the efficacy as single agentin refractory CLL (17). Very interesting results have beenreported in a recent paper by Friedberg in indolent andmantle cell lymphomas (18) with the combination of bend-amustine and bortezomib. In general bendamustine is welltolerated (12, 19–21). Friedberg (18) reported that 47% ofpatients experienced grade 3–4 neutropenia, but only 7%had febrile neutropenia. Grade 3–4 thrombocytopenia andgrade 3 anemia were reported in 24% and 9% of patients,
respectively. Because bendamustine is an alkylating agent,secondary malignancies are a potential concern. Friedbergnoted two patients with myelodysplastic syndrome and onewith chronic myelomonocytic leukemia, all heavily pre-treated. Bendamustine has also been administered in com-bination with mitoxantrone and rituximab; in a study (22) of54 patients with relapsed and refractory CD20-positive in-dolent lymphoma, the ORR was 96% including a CR rate of41% similar to our results in indolent histotype.
Our cohort of patients was heavily pretreated, and benda-mustine was administered often as last chance therapy. Ourretrospective experience confirms the efficacy of bendamustine
Fig. 5 Overall survival (dottedline) and progression-freesurvival (solid line) in mantlecell lymphomas
Fig. 6 Overall survival (dottedline) and progression-freesurvival (solid line) in diffuselarge B cell lymphomas
1020 Ann Hematol (2012) 91:1013–1022

in indolent lymphoma both non-follicular and follicular.Multivariate analysis indicated that the only parameterstatistically significant either for OS or PFS was the indolenthistotype at diagnosis. Particularly relevant was the responserate (CR and PR) in marginal NHL (93%). The medianduration of response was 4 months for follicular lymphomapatients and 3 months for indolent non-follicular patients. Inaggressive histologies we observed a high response rate inpatients with mantle cell lymphoma (70%), while in patientswith DLBC, the incidence of response was lower (32%). Inresponding patients with heavily pre-treated DLBCL, themedian duration of response was 4 months (range 1–17months), allowing further treatment (allotransplant).
Considering the characteristics of the patients and espe-cially the high number of previous treatments, bendamustinewas very well tolerated concerning hematological or extra-hematological toxicities. Deaths from infection wereexpected given that these patients were heavily pre-treated.Even if follow-up is short, no second epithelial malignancieswere reported in our group of patients and one myelodis-plastic syndrome in a patient heavily pretreated with alky-lating agents.
The optimal dose and schedule have yet to be determined.In various studies doses have ranged from 100 mg/m2 to 120mg/m2 for 2 days as a single agent and 70 mg/m2 to 90mg/m2 for 2 days when combined with rituximab, vary-ing from every 3 weeks to every 4 weeks (23–26). In ourexperience the maximum dose used was 90 mg/m2 regardlessof histology.
Recently bendamustine has been used, in combinationwith rituximab, in first-line therapy. Rummel (27) showedfavorable results of the combination compared with R-CHOP in naive patients with indolent lymphoma. Theformer could be a reasonable alternative in olderpatients but should be considered an effective and well toler-ated alternative in young patients too affected by indolentlymphomas.
In conclusion, this retrospective study of a heterogeneousgroup of lymphoma patients confirms the efficacy of bend-amustine even in those who have been heavily pretreated withor without alkylating agents. The low incidence of side effectsconfirms the safety of bendamustine in heavily pretreatedpatients who experienced mostly mild and manageable toxic-ity. This safety profile makes the bendamustine–rituximabcombination worthwhile for patients in an earlier diseasephase or as salvage therapy particularly in indolent lympho-mas, whereas patients with diffuse large B-cell lymphomashould receive more aggressive treatments whenever possible.
Acknowledgements The following researchers have substantiallycontributed to data acquisition: Maurizio Musso, UO Ematologia eTrapianto di Midollo, CDC "La Maddalena", Palermo; PellegrinoMusto, UO di Ematologia e Trapianto di Cellule Staminali, IRCCS-
CROB, Rionero in Vulture; Teodoro Chisesi, UO Ematologia Mestre-Venezia; Nicola Di Renzo, UO Ematologia e Trapianto di cellule Stam-inali, P.O V. Fazzi, Lecce; Nicola Cascavilla, Ematologia IRCS CasaSollievo della Sofferenza, San Giovanni Rotondo; Caterina Stelitano,UO Ematologia Ospedali Melacrino-Morelli, Reggio Calabria; andMariella Sciacca, UO OncoEmatologia AO Sant’Andrea, Vercelli.
Financial disclosures There are no financial disclosures from anyauthors.
References
1. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ(2008) Cancer statistics 2008. CA Cancer J Clin 58:71–96
2. Boyle P, Ferlay J (2005) Cancer incidence and mortality in Europe,2004. Ann Oncol 16:481–488
3. Harris NL, Jaffe ES, Diebold J, Flandrin G, Muller-Hermelik HK,Vardiman J, Lister TA, Bloomfield CD (2000) The Word HealthOrganization Classification of hematological malignancies reportof the clinical advisory committee meeting, Airlie House, Virginia,November 1997. Mod Pathol 13(2):193–207
4. Vose JM, Bierman PJ, Anderson JR, Kessinger A, Pierson J,Nelson J, Prappier B, Schmit-Pokorny K, Weisenburger DD,Armitage JO (1992) Progressive disease after high-dose therapyand autologous transplantation for lymphoid malignancy: clinicalcourse and patient follow-up. Blood 80(8):2142–2148
5. Elstrom RL, Martin P, Ostrow K, Barrientos J, Chadburn A, FurmanR, Ruan J, Shore T, Schuster M, Cerchietti L, Melnick A, ColemanM, Leonard JP (2010) Response to second-line therapy defines thepotential for cure in patients with recurrent diffuse large B-celllymphoma: implications for the development of novel therapeuticstrategies. Clin Lymphoma Myeloma Leuk 10(3):192–196
6. Barman Balfour JA, Goa KL (2001) Bendamustine. Drugs 61(5):631–638
7. Leoni LM, Bailey B, Reifert J, Bendall HH, Zeller RW, Corbeil J,Elliot G, Niemeyer CC (2008) Bendamustine (Treanda) displays adistinct pattern of cytotoxicity and unique mechanistic featurescompared with other alkilating agents. Clin Cancer Res 14:309–317
8. Strumberg D, Harsdtrick A, Doll K, Hoffmann B, Seeber S (1996)Bendamustine hydrochloride activity against doxorubicin-resistenthuman breast carcinoma cell lines. Anticancer Drugs 7:415–421
9. Leoni LM, Bailey B, Reifert J (2003) SDX-105 (bendamustine), aclinically active antineoplastic agent posesses a unique mechanismof action. Blood; 102:640a
10. Montillo M, Ricci F, Tedeschi A, Vismara E, Morra E (2010) Bend-amustine: new perspective for an old drug in lymphoprolipherativedisorders. Expert Rev Hematol 3(2):131–148
11. Friedberg JW, Cohen P, Chen L, Robinson KS, Forero-Torres A,La Casce AS, Fayad LE, Bessudo A, Camacho ES, Williams ME,van der Jagt RH, Oliver JW, Cheson BD (2008) Bendamustine inpatients with rituximab-refractory indolent and transformed non-Hodgkin's lymphoma: results from a phase II multicenter, single-agent study. J Clin Oncol 26:204–210
12. Bremer K (2002) High rates of long-lasting remissions after 5-daybendamustine chemotherapy cycles in pre-treated low-grade non-Hodgkin's lymphoma. J Cancer Res Clin Oncol 128:603–609
13. Ujjani C, Cheson B (2011) Efficacy of bendamustine in rituximab-refractory indolent B-cell non-Hodgkin lymphoma: review of apivotal trial. Future Oncol 7(1):9–14
14. Cheson BD, Horning SJ, Coiffier B, Shipp MA, Fisher RI, ConnorsJM, Lister TA, Vose J, Grillo-Lopez A, Hagenbeek A, Cabanillas F,Klippensten D, Hiddemann W, Castellino R, Harris NL, ArmitageJO, Carter W, Hoppe R, Canellos GP (1999) Report of an
Ann Hematol (2012) 91:1013–1022 1021
international workshop to standardize response criteria for non-Hodgkin's lymphomas. J Clin Oncol 17:1244–1253
15. SPSS Inc. (1998) SPSS for Windows, version 12.0. Chicago: SPSS.16. Heider A, Niederle N (2001) Efficacy and toxicity of bendamus-
tine in patients with relapsed low-grade non-Hodgkin's lymphoma.Anticancer Drugs 12:725–729
17. Kath R, Blumenstengel K, Fricke HJ, Hoffken K (2001) Bend-amustine monotherapy in advanced and refractory chronic lym-phocytic leukemia. J Cancer Research Clin Oncol 127:48–54
18. Friedberg JW, Vose JM, Kelly JL, Young F, Bernstein SH, PetersonD, Rich L, Blumel S, Proia NK, Liesveld J, Fisher RI, Armitage JO,Grant S, Leonard JP.(2011) The combination of bendamustine,borte-zomib and rituximab for patients with relapsed/refractory indolentand mantle cell non-Hodgkin lymphoma. Blood, Jan 14 Epub
19. Rummel MJ, Al-Batran SE, Kim SZ, Welsalu M, Hecker R,Kofahl-Krause D, Josten KM, Durk H, Rost A, Neise M, vonGrunhagen U, Chow KU, Hansmann ML, Holzer D, Mitrou PS(2005) Bendamustine plus rituximab is effective and has a favor-able toxicity profile in the treatment of mantle cell and low gradenon-Hodgkin’s lymphoma. J Clin Oncol 23(15):3383–3389
20. Cheson BD, Friedberg JW, Kahl BS, Van der Jagt RH, Tremmel L(2010) Bendamustine produces durable responses with an acceptablesafety profile in patients with rituximab-refractory indolent non-Hodgkin lymphoma. Clin LymphomaMyeloma Leuk 10(6):452–457
21. Ohmachi K, Ando K, Ogura M, Uchida T, Itoh K, Kubota N,Ishizawa K, Yamamoto J, Watanabe T, Uike N, Choi I, Terui Y,Usuki K, Nagai H, Uoshima N, Tobinai K (2010) Multicenterphase II study of bendamustine for relapsed or refractory indolentB-cell non-Hodgkin lymphoma and mantle cell lymphoma. CancerSci 101(9):2059–2064
22. Weide R, Pandorf A, Heymanns J et al (2004) Bendamustine/mitoxantrone/rituximab (BMR): a very effective, well tolerated
outpatient chemoimmunotherapy for relapsed and refractoryCD20 positive indolent malignancies. Final results of a pilot studyLeukemia and Lymphoma 45:2445–2449
23. Lissitchkov T, Arnaudov G, Peytchev D, Merkle KH (2006) PhaseI/II study to evaluate dose limiting toxicity, massimum tolerateddoses, and tolerability of bendamustine HCL in pre-treated patientswith B-chronic lymphocytic leukemia (binet stage) requiring therapy.J Cancer Res Clin Oncol 132:99–104
24. Schoffski P, Seeland G, Engel H, Grunwald V, Paul H, Merkle K,Kowalski R, Ganser A (2000) Weekly administration of benda-mustine a phase I study in patients with advanced progressive solidtumors. Ann Oncol 11:729–735
25. Rasschaert M, Schrijvers D, Van den Brande J, Dyck J, Bosmans J,Merkle K, Vermorken JB (2007) A phase I study of bendamustinehydrochloride administered day 1+2 every 3 weeks in patientswith solid tumors. Br J Cancer 96:1692–1698
26. Cheson BD, Wendtner CM, Pieper A, Dreyling M, Friedberg J,Hoelzer D, Moreau P, Gribben J, Knop S, Montillo M, Rummel M(2010) Optimal use of bendamustine in chronic lymphocytic leu-kemia, non Hodgkin lymphomas, and multiple myeloma: treat-ment recommendations from an international consensus panel.Clin Lymphoma Myeloma Leuk 10:21–27
27. Rummel MJ, Niederle N, Maschmeyer G, Banat A, von GruenhagenU, Losem C, Heil G, Welslau M, Balser C, Kaiser U, Ballo H,Weidmann E, Duerk HA, Kofahl-Krause D, Roller F, Barth J,Hoelzer D, Hinke A and Brugger W. (2009) Bendamustine plusrituximab is superior in respect of progression free survival and CRrate when compared to CHOP plus rituximab as first-line treatment ofpatients with advanced follicular, indolent, and mantle cell lympho-mas: final results of a randomized phase III study of the StiL (StudyGroup Indolent Lymphomas, Germany). Abs. 405 :51st ASHMeeting
1022 Ann Hematol (2012) 91:1013–1022




















