
Neural cells derived from adult bone marrow and umbilical cord blood
Upload
independentCategory
view
6download
0
ORIGINAL ARTICLE
18F-FDG PET/CT bone/bone marrow findings in Hodgkin’slymphoma may circumvent the use of bone marrow trephinebiopsy at diagnosis staging
Gerard Moulin-Romsee & Elif Hindié & Xavier Cuenca & Pauline Brice &
Didier Decaudin & Myriam Bénamor & Josette Brière & Marcela Anitei &Jean-Emmanuel Filmont & David Sibon & Eric de Kerviler & Jean-Luc Moretti
Received: 30 October 2009 /Accepted: 24 December 2009 /Published online: 4 March 2010# Springer-Verlag 2010
AbstractPurpose Accurate staging of Hodgkin’s lymphoma (HL) isnecessary in selecting appropriate treatment. Bone marrowtrephine biopsy (BMB) is the standard procedure for depictingbone marrow involvement. BMB is invasive and explores alimited part of the bone marrow. 18F-FDG PET/CT is nowwidely used for assessing response to therapy in HL and abaseline study is obtained to improve accuracy. The aim ofthis retrospective analysis was to assess whether routineBMB remains necessary with concomitant 18F-FDG PET/CT.
Methods Data from 83 patients (newly diagnosed HL) werereviewed. All patients had received contrast-enhanced CT,BMB and 18F-FDG PET/CT. Results of BMB were notavailable at the time of 18F-FDG PET/CT imaging.Results Seven patients had lymphomatous involvement onBMB. Four patients had bone involvement on conventionalCT (two with negative BMB). All patients with bonemarrow and/or bone lesions at conventional staging werealso diagnosed on 18F-FDG PET/CT scan. PET/CTdepicted FDG-avid bone/bone marrow foci in nine addi-tional patients. Four of them had only one or two foci,while the other had multiple foci. However, the iliac crest,site of the BMB, was not involved on 18F-FDG PET/CT.Osteolytic/sclerotic lesions matching FDG-avid foci werevisible on the CT part of PET/CT in three patients. MRIordered in three other patients suggested bone marrowinvolvement. Interim and/or end-therapy 18F-FDG PET/CTdocumented response of FDG-avid bone/bone marrow focito chemotherapy in every patient.Conclusion 18F-FDG PET/CT highly improves sensitivityfor diagnosis of bone/bone marrow lesions in HL comparedto conventional staging.
Keywords Hodgkin’s lymphoma . PET/CT. 18F-FDG .
Bone marrow trephine biopsy . Staging
Introduction
Hodgkin’s lymphoma (HL) represents about 12% oflymphoma cases and 1% of all malignancies [1]. Thegreatest chance for eradicating the disease lies in first-linetherapy. Although most patients with HL are cured withmodern treatment, about 10% of patients with localized,
Gerard Moulin-Romsee and Elif Hindié contributed equally to thiswork.
G. Moulin-Romsee : E. Hindié (*) : J.-E. Filmont : J.-L. MorettiService de Médicine Nucléaire, Hôpital Saint-Louis, AssistancePublique-Hôpitaux de Paris, Université Paris 7,1, avenue Claude Vellefaux,75475 Paris cedex 10, Francee-mail: [email protected]
G. Moulin-Romsee :M. BénamorNuclear Medicine, Institut Curie,Paris, France
X. Cuenca : P. Brice :D. SibonHaemato-Oncology, Hôpital Saint-Louis,Paris, France
D. Decaudin :M. AniteiHaematology, Institut Curie,Paris, France
J. BrièrePathology, Hôpital Saint-Louis,Paris, France
E. de KervilerRadiology, Hôpital Saint-Louis,Paris, France
Eur J Nucl Med Mol Imaging (2010) 37:1095–1105DOI 10.1007/s00259-009-1377-5

and up to 30% of patients with disseminated HL, fail torespond to—or relapse after—initial therapy. The cure rateis only about 50% in relapsing patients and even lower inprimary refractory patients or when relapse occurs earlywith extranodal disease or advanced stage [2–5]. Themodalities of the first-line treatment of patients with HLdepend on the stage of the disease at the time of diagnosis,separating early/localized stages and advanced/disseminat-ed stages [6–8]. Adequate staging is therefore mandatorybefore initiating a risk-adapted therapy, taking into accountthe balance between efficacy and risks of toxicity and long-term adverse effects [9].
Staging is based on the Ann Arbor classification withCotswolds modifications [10, 11] and usually includescomputed tomography (CT) and bone marrow trephine biopsy(BMB). CT may depict cortical bone lesions or late bonemodifications but has low sensitivity for early bone marrowinvolvement (BMI) [11]. BMB is routinely performed, exceptwhen the probability of a positive biopsy is deemed very low(<1%), that is in early or favourable supradiaphragmaticstages I/II patients with no B symptoms or adverse prognosticfactors [11–14]. BMI confers stage IV disease affecting bothtreatment and prognosis. In the study by Hasenclever andDiehl, the 5-year freedom from progression for patients withBMI was 60% only and the 5-year overall survival 70% [15].However, if blind BMB, usually unilateral, is the standardmethod to search for BMI [11], two factors make the BMB anunsatisfactory diagnostic test: it is a painful and invasiveprocedure and, even if the volume of the biopsy is adequate,focal lesions can be missed.
Functional imaging with positron emission tomographyusing 2-(18F)fluoro-2-deoxy-D-glucose (18F-FDG PET) hasgained widespread use in the management of HL. 18F-FDGPET is very efficient at differentiating residual viabletumour tissue from therapy-induced fibrosis [16, 17] andhas therefore been incorporated into the recently revisedcriteria for end-therapy assessment [18]. Moreover, severalrecent studies suggest that 18F-FDG PET may open up aunique opportunity to assess the response early in thecourse of treatment of HL, thus enabling changes in therapyaccording to the patient’s risk of relapse [19–24]. Interimscanning is used within the framework of clinical trials[25]. Accurate assessment of response by 18F-FDG PETbenefits from baseline examination for optimal interpreta-tion. Obtaining a baseline 18F-FDG PET study in HL hastherefore been strongly encouraged [14, 18]. This pre-therapy 18F-FDG PET may also provide useful informationregarding initial staging [26] and also for the implementa-tion of radiotherapy [27]. The recent introduction andgeneralization of PET/CT hybrid instruments has been amajor improvement in technology as it allows correlation ofthe functional information with underlying anatomy [28].18F-FDG PET/CT outperforms 18F-FDG PET alone.
The aim of the current study was to correlate BMB andPET/CT results at initial HL staging and to assess whetherBMB remains useful. We therefore performed a retrospec-tive study on patients with newly diagnosed HL, who hadBMB and PET/CT as part of their initial staging.
Materials and methods
All patients newly diagnosed with HL between 2004 and2007, and who had received both BMB and PET/CT atinitial staging, were included in this retrospective analysis.These patients were recruited and treated at either Saint-Louis Hospital (University Paris 7) or Institute Curie, Paris.The study included 83 patients (45 men and 38 women).
All patients had received conventional staging [11],including physical examination, complete blood count,measurement of erythrocyte sedimentation rate, serumbiochemical tests, chest radiography, contrast-enhancedCT of the chest, abdomen and pelvis and iliac bone marrowbiopsy. 18F-FDG PET/CT was performed within a few daysof conventional staging. BMB results were not yet availableat the time of PET/CT imaging.
BMB
A BMB with a sample size of 2 cm length or more wasobtained from at least one side, submitted to step sectioningand read by an experienced pathologist. BM infiltration byHL is characterized by randomly distributed infiltrates andrare atypical cells, usually accompanied by significantfibrosis and occasional epithelioid cell granulomas [29].Immunophenotypic expression of CD30 and CD15 and thenegativity for LCA were exploited in cases of suspiciousdiagnosis. CD3, CD20, LMP and other markers were usedwhenever deemed helpful.
18F-FDG PET/CT scanning
The modalities were similar in both institutions and usedGemini XL PET/CT instruments (Philips Medical Systems,Cleveland, OH, USA), combining a germaniumoxyothosilicate-based PET and a 16-slice CT. Patientsfasted 6 h before imaging and blood glucose level had tobe less than 7 mmol/l. Imaging started 60 min after theinjection of 5 MBq/kg 18F-FDG (maximum 500 MBq).PET/CT scans were performed from the base of the skull tomid-thigh level. CT was performed without injection ofcontrast media and with low radiation dose. On completionof the CT portion of the examination, the patient couch wasadvanced into the field of view, and a multibed (eight to tenpositions) PET study was acquired over the same range asthe CT scan. CT images were used for attenuation
1096 Eur J Nucl Med Mol Imaging (2010) 37:1095–1105

correction of the 18F-FDG PET emission data. PET imageswere reconstructed using a 3-D row action maximumlikelihood algorithm (RAMLA).
Modalities of retrospective analysis
Three reviewers (GMR, EH, XC) extracted all data.Retrospective analysis used the following methodology:
– First: careful reading of the PET/CT report in order todetermine whether the bone/bone marrow (B/BM)compartment was reported as positive, doubtful ornegative.
– Positive and doubtful PET studies were re-read byconsensus of two nuclear medicine physicians (GMR,EH). A positive scan requires the presence of focaluptake over the B/BM compartment that could not beexplained by benign findings on the underlying CTimage or history. The number and location of eachFDG-avid focus was noted, as well as the presence ofsuspicious osteolytic/osteosclerotic lesions on the un-derlying CT. For doubtful FDG scans, the reason forreading the scan as doubtful was recorded. These scanswere considered as a separate group.
– When the PET/CT was reported as negative for B/BMinvolvement, images were not reviewed, since the mainaim was to assess sensitivity in a routine clinical setting.
The sensitivity of 18F-FDG PET/CT was measured usingBMB as the standard of reference. Patients with a positiveBMB, in whom the PET/CT study was not clearly reportedas positive for B/BM involvement, were considered false-negative.
Because BMB is affected by sampling errors, specificityof 18F-FDG PET/CT could not be calculated. This limitaffecting the standard of reference for BMI was stressed byKwee et al. when evaluating the performance of MRI [30].When patients had positive 18F-FDG PET findings for B/BMinvolvement, and a negative BMB, the following points werecarefully assessed:
– Was the presence of bone lesions signalled on thereport of the initial staging CT?
– Was the pattern of involvement on 18F-FDG PETunifocal, bifocal or multifocal (≥3)?
– Were bone lesions apparent on the underlying CTimages of the PET/CT study?
– Were complementary radiological studies (MRI)obtained?
– Was a directed biopsy obtained or deemed necessary?– Was the final decision of the multidisciplinary medical
staff to treat the patient as stage IV disease?– Did the FDG-avid B/BM lesions resolve with chemo-
therapy either on interim PET or at end-therapy PET
scan? The resolution of a PET-positive focus duringchemotherapy was considered as an additional indica-tion of malignancy.
Ethical considerations
All patients had an established diagnosis of HL. Themethods used (BMB and PET/CT) were part of the clinicalroutine. Patients were thoroughly informed about theclinical reasons to undergo the investigations and treatment.Retrospective data analysis and reporting comply with localinstitutional laws. None of the authors had a conflict ofinterest.
Results
Patient characteristics
A total of 83 patients (45 men and 38 women) with newlydiagnosed HL had undergone both BMB and PET/CT atinitial staging. The main patient characteristics were: meanpatient age was 30.7 years (range: 7–82 years); 78 patients(94%) had classic HL subtypes (63 nodular sclerosis, 4mixed cellularity and 11 classic not otherwise specified),while the other 5 patients had nodular lymphocytepredominant HL (NLPHL). Before results of BMB andPET/CT were available, 48 patients were deemed to havelocalized stages (stage I, n=9; stage II, n=39), 22 patientshad stage III and 13 patients stage IV disease.
BMB identified BMI in seven patients. Two of thesepatients were already stage IVon conventional CT based onthe presence of bone, lung and liver involvement in onepatient and of bone and liver lesions in the other patient.The other five patients were upstaged (two from stage IIand three from stage III).
PET/CT results
PET/CT results were classified into three categories:negative, doubtful and positive:
1. PET/CT was reported as negative for B/BM in 60patients. All of these patients also had negative BMBresults.
2. PET/CT was reported as doubtful in five patients. Theyhad intense, but strictly homogeneous, uptake by thebone marrow of the axial skeleton and proximalappendicular skeleton. The reports mentioned that thepattern is more likely to reflect benign enhancementdue to inflammation or cytokine release, but BMI couldnot be formally excluded. At reviewing the cases, bothreviewers confirmed absence of any FDG-avid foci
Eur J Nucl Med Mol Imaging (2010) 37:1095–1105 1097

over the bone or bone marrow. We measured FDGuptake (standardized uptake value) at the level of thelumbar vertebrae. The maximum standardized uptakevalue (SUVmax) was ≥4 (range: 4–4.8 in the fivepatients). Figure 1 shows one of these patients withenhanced bone marrow. None of these five patients hada positive BMB. None of these patients has beentreated as stage IV disease.
3. PET/CT was reported as positive for B/BM involve-ment in 18 patients because of the presence of clear-cutFDG-avid foci. All seven patients with positive BMBwere reported as unambiguously positive on PET/CTscan (Fig. 2).
18F-FDG PET/CT depicted 11 patients which hadpositive B/BM findings despite a negative BMB at initialstaging. Seven of these patients had multiple (≥3) FDG-avid lesions, two patients had two FDG-avid foci each and
the last two patients had only one FDG-avid focus. It is ofinterest that in none of these 11 patients was the region ofthe iliac crest, site of the BMB, involved on PET/CT.Figure 3 shows a typical scan of a patient with multiplefoci. Of the 11 patients, 2 were recognized to have bonelesions by conventional CT before PET/CT examination(1 of them had also undergone MRI). In another threepatients, guided reading of the CT portion of PET/CTuncovered abnormal medullar density or bone destructionunderlying the FDG-avid foci (Figs. 3 and 4). MRI wasobtained in three more patients and showed focal bonemarrow alterations suggestive of lymphoma infiltration.Figure 5 shows one example.
Treatment
All 18 patients with positive B/BM findings were treatedand monitored according to the clinic’s guidelines fordisseminated HL, taking into account patient age andspecific patient characteristics. In every case, this decisionwas taken following case discussion by a multidisciplinarylymphoma “group”, involving onco-haematologists, radiol-ogists, nuclear physicians and pathologists. Further confir-mation of imaging results by PET-guided biopsies was notjudged necessary. Twelve adult patients with classic HLreceived eight cycles of ABVD or BEACOPP regimens.One patient with NLPHL received chemotherapy + ritux-imab. Five patients, 16 years old or younger, were treatedaccording to paediatric regimens.
An interim and/or end-therapy 18F-FDG PET examina-tion was used to assess response to chemotherapy. Thisfollow-up PET showed complete resolution of FDG-avidlymph node and B/BM foci in 16 patients and minimalresidual uptake (MRU) in two patients. Availability of thebaseline PET was helpful in the reading of response studiesin patients with B/BM lesions. The median follow-up was22 months (range: 9–48 months). One patient, with MRUon interim 18F-FDG PET after three cycles of therapy,progressed at six cycles and died rapidly from disease. Allother patients were in complete remission (CR) at lastfollow-up (Table 2).
The results of PET/CT versus BMB are summarized in a2 × 2 table (Table 1). Negative PET/CT and patients withintense but homogeneous marrow uptake were merged intoa single group.
Table 2 gives detailed data for all 18 patients withpositive B/BM findings on PET/CT, independent of resultsof BMB. Patient’s stage before BMB and PET/CT isindicated, as well as the International Prognostic Score forthose with advanced stages [15]. Table 2 shows that ninepatients were recognized by conventional staging (BMBand/or initial CT) to have B/BM involvement. FDG-avidB/BM lesions were also clearly seen on PET/CT in all of
Fig. 1 A 29-year-old woman with clinical stage II HL (classic,nodular sclerosis). The 18F-FDG PET image displayed as maximumintensity projection (MIP) shows intense uptake by the mediastinal,supraclavicular and left axillary enlarged lymph nodes. There is amoderate hypermetabolism of the bone marrow (SUVmax=4.2 atlumbar level). This diffuse, homogeneous and symmetrical uptake isrestricted to the axial skeleton and proximal appendicular skeleton.This pattern is typical of reactive bone marrow or bone marrowhyperplasia. In the absence of clear-cut FDG-avid foci, PET/CTshould not be considered positive
1098 Eur J Nucl Med Mol Imaging (2010) 37:1095–1105

them. In nine more patients, PET/CT depicted B/BM lesions,missed by conventional staging (Table 2). Based on 18F-FDGPET B/BM findings, three patients were upstaged from stageII to stage IV and treated as advanced stage; another fivepatients were upstaged from stage III to stage IV; the lastpatient was already stage IV (lung nodules).
Discussion
HL is highly FDG avid. Hutchings and colleaguesmeasured uptake over 208 lesions in 60 patients [31]. Themean value of the SUVmax was 11.9 in classic HL [95%confidence interval (CI): 11.1–12.8] and 8.3 (5.7–10.9) inNLPHL. A characteristic feature of HL is the rareness ofthe tumour cells which represent only a small fraction of thecellular infiltrate. The HL microenvironment is dominatedby an extensive mixed, potentially inflammatory cellularinfiltrate [32]. Thus, probably both tumour and non-tumourcells contribute to the high FDG uptake.
We found that all seven patients who had lymphomainvolvement on routine BMB were also reported as positiveon PET/CT based on the presence of clear-cut FDG-avidB/BM lesions. These results suggest that routine BMBmight be unnecessary when 18F-FDG PET/CT is negative.More important was the finding that PET/CT may uncoverB/BM lesions that were undetected by conventionalstaging. Nine patients in this series had FDG-avid B/BMfoci with negative BMB for bone marrow lesions and inwhom conventional staging CT was also reported asnegative for bone lesions.
Unilateral BMB is the standard approach in the stagingof the bone marrow. In an unselected Hodgkin population,the rate of positive unilateral BMB is close to 5%.Prevalence was 4.8% in the study by Munker et al. [33],5.2% in the study of Howell et al. [12] and 5.5% in thestudy by Vassilakopoulos et al. [13]. The prevalence ofBMI is less than 1% among patients with early-stagedisease and no B symptoms, and BMB is not recommendedin these patients in the absence of adverse prognosticfactors [11–14]. In the present study, 7 of 84 patients hadpositive BMB, but patients with stages IA/IIA andfavourable prognostic factors are not represented.
Although BMB is the reference standard for BMI, it hasbeen recognized as an imperfect tool for a long time.Studies examining the yield of a bilateral biopsy haveshown that, in HL patients with positive biopsy, only oneside is involved in about 40% of cases [34, 35]. Thus, aunilateral biopsy would miss 20% of cases compared to abilateral biopsy. However, the number of additionaldetectable cases (1–2% of all patients) was not judgedsufficient to recommend routine bilateral biopsy [11].Disease outside the iliac crests would be missed anyway.BMI in HL has a focal pattern [36]. In the present study, 11patients had B/BM lesions on 18F-FDG PET/CT withnegative BMB. In every case, the iliac crest had no FDG-avid foci.
There have been only a few studies examining thesensitivity of 18F-FDG PET for BMI in a pure population ofHL. The meta-analysis by Pakos et al. reported on fivestudies published before 2004, with a total of 191 patientswith HL and 11 positive BMB [37]. The estimated
Fig. 2 A 16-year-old girl(patient 15) with classic HL,clinical stage IV (lymph nodes,spleen, liver, lung and bonelesions on conventional CT).18F-FDG PET/CT depictedmultiple B/BM lesions. Thetransaxial PET image (upperrow) at the level of the iliaccrests shows a hypermetabolicfocus of the right ilium. The CTand PET/CT fusion images(lower row) show that the FDG-avid focus corresponds to anosteolytic lesion. The patientreceived bilateral iliac crestbiopsy. BMB was positive onlyon the right side
Eur J Nucl Med Mol Imaging (2010) 37:1095–1105 1099

sensitivity of 18F-FDG PET was 76%. Commenting on thisfigure, some experts suggest that routine BMB is stillnecessary in a patient with negative 18F-FDG PET [38]. Weagree that 18F-FDG PET might miss early limited infiltra-tion of the bone marrow, while still detectable by BMB iflocated at the site of biopsy. However, the impact ofminimal BMI on prognosis and relapse after standardtherapy is not known. A sensitivity of 76% means that100 BMB procedures would be performed in patients withnegative 18F-FDG PET to detect at most 1 or 2 positivecases of BMI. Previously, this small yield has not justifiedthe use of routine bilateral biopsy instead of unilateralbiopsy [11]. BMB is generally safe but should not bethought of as a risk-free procedure. Adverse events(haemorrhage, infection, etc.) are reported in about 0.12%of cases [39]. It is also a painful and stressful procedureeven with good local anaesthesia and sedation.
Five studies, not included in the meta-analysis by Pakoset al., were recently reported [40–44]. Table 3 summarizesfindings from these studies and our own data. Jointly, 42patients had positive BMB. 18F-FDG PET identified 36 ofthem (85.7%). Thus, the sensitivity reported in the previous
meta-analysis [37] is confirmed and even further improvedin these recent studies with a larger number of patients.Omitting BMB would have missed only 6 cases of BMI outof 561 patients (1.1%).
Routine reading of CT has a low yield in depicting B/BMlesions. Schaefer and colleagues examined a selected popu-lation of 50 lymphoma patients (22 HL) with FDG-avid bonelesions on PET/CT. On CT, only 32 of the 193 lesions (16.6%)were detected without the PET information [45]. Likeprevious studies with 18F-FDG [40–45], we decided toreport on B/BM lesions together and did not try to make aclear-cut distinction between bony involvement and BMI inevery patient and for each lesion. It is true that even with18F-FDG PET/CT it would be difficult to make a cleardistinction in every patient and every lesion. Moreover, onetype of invasion may lead to the other by local spreadmaking distinction less easy. In many patients with multipleB/BM foci, both types of lesions coexisted.
In this series of 83 HL patients, 18F-FDG PET depicted 9cases (10.7%) of B/BM involvement that were missed byconventional staging (BMB + CT). Other studies have alsoshown that uncovering B/BM lesions was the most
Fig. 3 A 54-year-old man (patient 2) with classic HL staged IIIB atconventional staging (CT + BMB). Pre-treatment PET/CT showsmultiple hypermetabolic bone lesions involving mainly the axialskeleton (dotted arrows), ribs and proximal femurs. The solid arrow
shows that the region of BMB does not exhibit hypermetabolic foci,thus explaining the false-negative BMB. Guided reading of the CTpart of PET/CT shows sclerotic changes (abnormal bone marrowdensity) underlying some of the FDG-avid lesions (dotted arrows)
1100 Eur J Nucl Med Mol Imaging (2010) 37:1095–1105
important change resulting from using 18F-FDG PET atinitial staging. The percentage of extra cases detected inthese series ranges from 4.9 to 13.4% (Table 3). Thenumber of biopsies directed at PET/CT-positive sites is lowin all of these studies; therefore, specificity cannot bemeasured. However, when biopsies were performed on
FDG-avid foci in newly diagnosed HL patients, whether onnodal lesions [46] or on bone lesions [45, 47], the positivepredictive value was uniformly high. Young et al. reportedon 11 patients with HL in whom FDG-avid foci wereverified by staging laparotomy; the positive predictivevalue of 18F-FDG PET was 100% [46]. In the study of
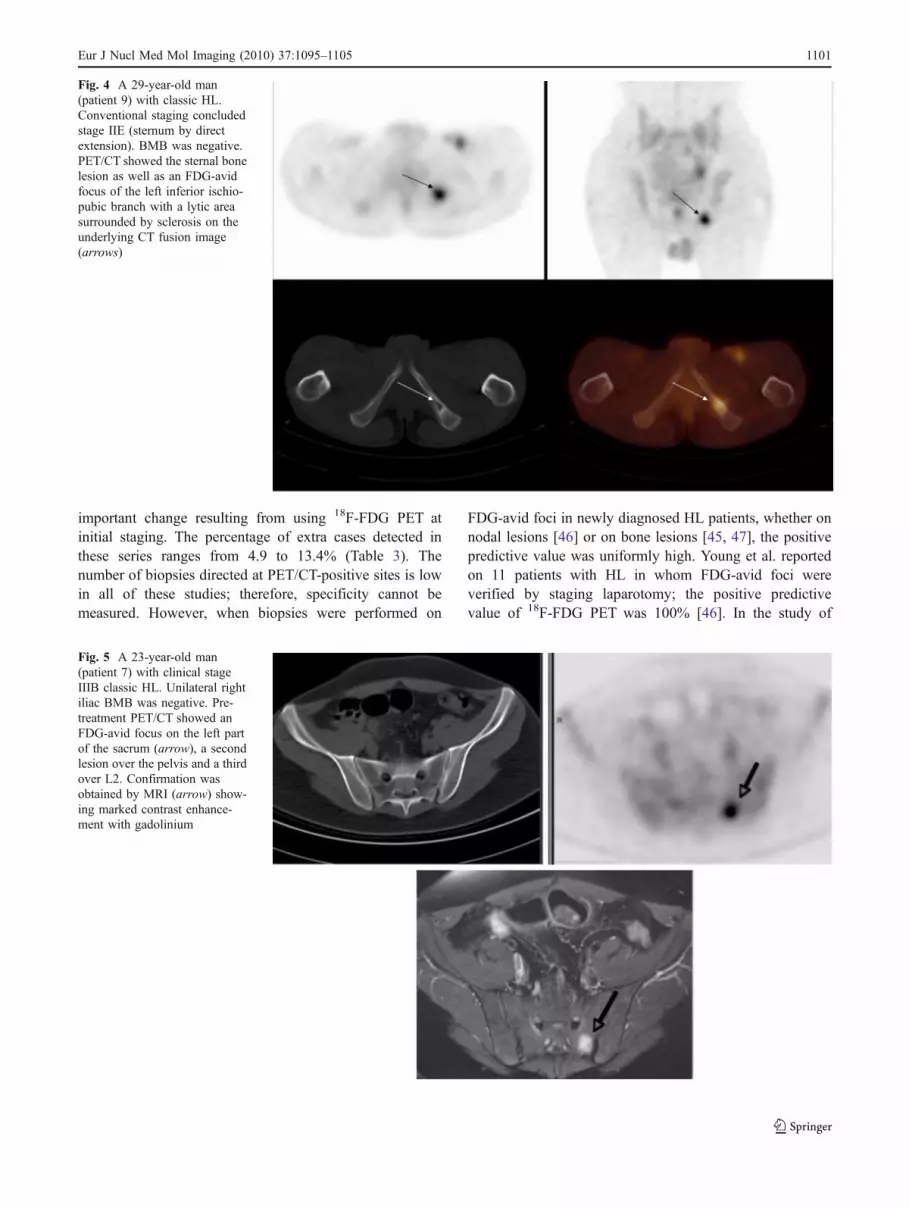
Fig. 4 A 29-year-old man(patient 9) with classic HL.Conventional staging concludedstage IIE (sternum by directextension). BMB was negative.PET/CT showed the sternal bonelesion as well as an FDG-avidfocus of the left inferior ischio-pubic branch with a lytic areasurrounded by sclerosis on theunderlying CT fusion image(arrows)
Fig. 5 A 23-year-old man(patient 7) with clinical stageIIIB classic HL. Unilateral rightiliac BMB was negative. Pre-treatment PET/CT showed anFDG-avid focus on the left partof the sacrum (arrow), a secondlesion over the pelvis and a thirdover L2. Confirmation wasobtained by MRI (arrow) show-ing marked contrast enhance-ment with gadolinium
Eur J Nucl Med Mol Imaging (2010) 37:1095–1105 1101

Schaefer et al., 24 bone biopsies were directed at FDG-avidlesions in lymphoma patients (6 with HL, 18 with NHL).All proved the presence of lymphomatous infiltration [45].
The impact of staging 18F-FDG PET/CT on outcomecannot be assessed in the absence of a randomized study. All
nine extra cases of B/BM involvement detected by 18F-FDGPET/CT were treated as stage IV disease and adult patientsreceived eight cycles of ABVD or BEACOPP regimens [48].B/BM foci showed response to therapy on an interim and/orend-therapy PET examination (negative study in eight, MRU
Table 2 Patients with positive B/BM findings on 18F-FDG PET/CT (patients with positive BMB are listed in the lower rows)
Patient Sex Age Stage beforeBMB and PET
BMB FDG-avid B/BMfocia
CT: bone findings MRI Response 18F-FDGPETb
Follow-up(months)
Status
1 M 49 IIIB (IPS=3) Neg. Multiplea + (CT of PET/CT) ND CMR (interim) 36 CR
2 M 54 III (IPS=3) Neg. Multiple (Fig. 3) + (CT of PET/CT) ND CMR (interim) 18 CRc
3 M 43 IIB Neg. Multiple ND CMR (end-therapy) 42 CR
4 F 16 IVB lung nodules(IPS=1)
Neg. Multiple ND CMR (interim) 24 CR
5 M 13 IV lung, liver, bone(IPS=4)
Neg. Multiple + (initial CT) + CMR (interim) 9 CR
6 M 28 IVB bone (IPS=3) Neg. Multiple + (initial CT) ND CMR (interim) 48 CR
7 M 23 IIIB (IPS=1) Neg. Multiple (Fig. 5) + MRU end-therapy 28 CR
8 M 9 III (IPS=1) Neg. 2 (L1 and L4) + CMR (end-therapy) 25 CR
9 M 29 IIB, IIE (sternumby contiguity)
Neg. 2 (sternal, ischion)(Fig. 4)
+ (CT of PET/CT) ND CMR (interim) 24 CR
10 F 47 II (unfavourable) Neg. 1 (T3 vertebra) + CMR (end-therapy) 36 CR
11 M 19 IIIB (IPS=1) Neg. 1 (left sacrum)(Fig. 6)
ND CMR (interim) 15 CR
12 F 41 III (IPS=2) + Multiple CMR (end-therapy) 48 CR
13 M 44 IIIB (IPS=1) + Multiple MRU (interim) 12 Diedd
14 M 29 IIB, IIE (thoracicwall)
+ Multiple CMR (interim) 10 CR
15 F 16 IV bone, lung,liver (IPS=2)
+ Multiple (Fig. 2) + (initial CT) CMR (interim) 13 CR
16 M 7 IV bone, liver(IPS=4)
+ 2 (T12 and L5) + (initial CT) CMR (interim) 18 CR
17 F 61 II (unfavourable) + 1 (left ischion) CMR (interim) 22 CR
18 M 27 IIIB (IPS=3) + 1 (T8 vertebra) CMR (interim) 18 CR
All patients had classic HL except patient 13 who had NLPHL histology
IPS International Prognostic Score [15], Neg. negative, ND not done, CR complete remissionaMultiple = presence of three or more FDG-avid B/BM lesions on 18 F-FDG PET/CTb 18 F-FDG PET results after two to four cycles of chemotherapy (interim) or at the end of treatment. CMR compete metabolic response, MRUminimal residual uptakec Complete remission of HL. Lung cancer diagnosed at last follow-upd HL progressed at six cycles. Salvage therapy failed
Table 1 Summary of BMB and PET/CT results in 83 patients with HL
BMB positive (n=7) BMB negative (n=76)
PET/CT positive (n=18)a 7 11
• 2 with bone lesions also seen on initial CT
• 3 with osteolytic/sclerotic changes on CT part of PET/CT
• 4 MRI positive
• 10 complete metabolic response on interim and/or end-therapy 18F-FDG PET; 1 MRU
PET/CT negative (n=65)b 0 65
a Positive PET/CT = presence of clear-cut 18 F-FDG-avid B/BM focib Negative PET/CT = absence of clear-cut 18 F-FDG-avid B/BM foci (intense but homogeneous uptake is considered negative; n=5 patients)
1102 Eur J Nucl Med Mol Imaging (2010) 37:1095–1105

Fig. 6 A 19-year-old man(patient 11) with clinical stageIIIB classic HL and negativeright iliac crest BMB. Theleft-hand column corresponds topre-treatment PET/CT and theright-hand column to responseassessment after two cycles ofchemotherapy AVBD. Pre-treatment PET shows an FDG-avid focus of the left aspect ofthe sacrum (red cursor onleft-hand column). Interim PETafter two cycles of chemothera-py showed complete metabolicresponse. The bone focus hasalso resolved (right-handcolumn). The patient was treatedwith six cycles ABVD + twocycles ABV. Another PET/CTobtained at the end of therapyconfirmed complete remission
Table 3 Summary of studies published after the meta-analysis by Pakos et al. [37]
Study No. of patients BMBpositive
BMB and 18F-FDG PET positive Extra cases detected by18F-FDG PETa
Extra cases(% of total population)
Munker et al. [40] 73 3 2 6 8.2%
Kabickova et al. [41] 55b 4 4 6 10.9%
Rigacci et al. [42] 186 6 5 14 7.5%
Pelosi et al. [43] 82 6 2 11 13.4%
Cerci et al. [44] 82c 16 16 4 4.9%
Present work 83 7 7 9 10.7%
Total 561 42 36 50 8.9%
a Cases missed by conventional staging (BMB + contrast-enhanced CT)b Study on adolescents and childrenc Population with a high frequency of advanced stages
Eur J Nucl Med Mol Imaging (2010) 37:1095–1105 1103

in one), and all nine patients were in CR after short- tomedium-term follow-up. In the absence of 18F-FDG PET/CT,some of these patients would have received a differentchemotherapy regimen and/or fewer courses. It is known thatabout 15% of patients treated as early-stage unfavourable(intermediate stage) will relapse within 5 years [8]. Most ofthe relapses occur outside the irradiated field [49]. Because18F-FDG PET is a recent technique, it might be that some ofthese patients have been misclassified by conventional stagingand hence do not belong to the early stage and did not receivethe adapted therapy.
MRI is another powerful technique for assessing thebone marrow [30]. However, at difference with whole-bodyMRI, PET/CT has gained a definite role in responseevaluation in HL. Obtaining a baseline PET study hasalready been recommended to improve the interpretation ofresponse studies [14, 18].
Our study confirms the observation of many authors thatintense but homogeneous bone marrow uptake over theaxial skeleton and proximal appendicular skeleton is not apattern of BMI in Hodgkin’s disease and is due toinflammation and effect on bone marrow driven bycytokine release [36, 42]. In the study of Rigacci et al.,four patients reported as positive simply because of intensebut otherwise diffuse uptake were all recognized as false-positive, while all true-positive had a focal pattern on FDGimaging [42]. Thus, in the absence of clear-cut foci, 18F-FDG PET studies should be scored as negative.
On the basis of our findings, we can make the followingrecommendations:
– Whenever possible, 18F-FDG PET/CT should be usedat initial staging of HL patients as it may uncoverunsuspected B/BM lesions.
– In the presence of multiple foci, without explanation byhistory, patients should be treated as stage IV disease.
– Patients with only one or two foci require confirmatorydata (careful reading of the underlying CT forosteolytic/osteosclerotic signs, MRI if underlying CTshows no obvious abnormality). Directed biopsyshould be obtained in cases of discrepancy. This isespecially important in patients with early-stage diseasegiven the prognostic and therapeutic impact. Foci thatdo not resolve under chemotherapy on interim PETmay also require guided biopsy.
Conclusion
18F-FDG PET/CT improves sensitivity for diagnosis of B/BM lesions in HL compared to conventional staging.Prospective studies are now needed to determine whether18F-FDG PET/CT makes bone marrow biopsy in HLsuperfluous or whether the two are complementary.
Acknowledgments The authors are grateful to Drs. ChristianGisselbrecht, Catherine Thieblemont, Patricia Franchi-Rezgui, VéroniqueEdline, Anne Vincent-Salomon, Jean Michon and all physicians and staffwho participated in patient management at St-Louis Hospital and InstitutCurie.
Conflicts of interest None.
References
1. Diehl V. Hodgkin’s disease–from pathology specimen to cure. NEngl J Med 2007;357(19):1968–71.
2. Brice P, Bastion Y, Divine M, Nedellec G, Ferrant A, Gabarre J, etal. Analysis of prognostic factors after the first relapse ofHodgkin’s disease in 187 patients. Cancer 1996;78(6):1293–9.
3. Moskowitz CH, Nimer SD, Zelenetz AD, Trippett T, Hedrick EE,Filippa DA, et al. A 2-step comprehensive high-dose chemo-radiotherapy second-line program for relapsed and refractoryHodgkin disease: analysis by intent to treat and development ofa prognostic model. Blood 2001;97(3):616–23.
4. Josting A, Franklin J, May M, Koch P, Beykirch MK, Heinz J, etal. New prognostic score based on treatment outcome of patientswith relapsed Hodgkin’s lymphoma registered in the database ofthe German Hodgkin’s lymphoma study group. J Clin Oncol2002;20(1):221–30.
5. Brice P. Managing relapsed and refractory Hodgkin lymphoma. BrJ Haematol 2008;141(1):3–13.
6. Eghbali H, Raemaekers J, Carde P, EORTC Lymphoma Group.The EORTC strategy in the treatment of Hodgkin’s lymphoma.Eur J Haematol Suppl 2005 Jul;(66):135–40.
7. Connors JM. State-of-the-art therapeutics: Hodgkin’s lymphoma.J Clin Oncol 2005;23(26):6400–8.
8. Diehl V, Fuchs M. Early, intermediate and advanced Hodgkin’slymphoma: modern treatment strategies. Ann Oncol 2007;18Suppl 9:ix71–9.
9. Favier O, Heutte N, Stamatoullas-Bastard A, Carde P, Van’t VeerMB, Aleman BM, et al. Survival after Hodgkin lymphoma: causesof death and excess mortality in patients treated in 8 consecutivetrials. Cancer 2009;115(8):1680–91.
10. Carbone PP, Kaplan HS, Musshoff K, Smithers DW, Tubiana M.Report of the Committee on Hodgkin’s Disease Staging Classi-fication. Cancer Res 1971;31(11):1860–1.
11. Lister TA, Crowther D, Sutcliffe SB, Glatstein E, Canellos GP,Young RC, et al. Report of a committee convened to discuss theevaluation and staging of patients with Hodgkin’s disease:Cotswolds meeting. J Clin Oncol 1989;7(11):1630–6. Erratumin: J Clin Oncol 1990 Sep;8(9):1602.
12. Howell SJ, Grey M, Chang J, Morgenstern GR, Cowan RA,Deakin DP, et al. The value of bone marrow examination in thestaging of Hodgkin’s lymphoma: a review of 955 cases seen in aregional cancer centre. Br J Haematol 2002;119(2):408–11.
13. Vassilakopoulos TP, Angelopoulou MK, Constantinou N, Karmi-ris T, Repoussis P, Roussou P, et al. Development and validationof a clinical prediction rule for bone marrow involvement inpatients with Hodgkin lymphoma. Blood 2005;105(5):1875–80.
14. Brusamolino E, Bacigalupo A, Barosi G, Biti G, Gobbi PG, LevisA, et al. Classical Hodgkin’s lymphoma in adults: guidelines ofthe Italian Society of Hematology, the Italian Society ofExperimental Hematology, and the Italian Group for BoneMarrow Transplantation on initial work-up, management, andfollow-up. Haematologica 2009;94(4):550–65.
15. Hasenclever D, Diehl V. A prognostic score for advancedHodgkin’s disease. International Prognostic Factors Project on
1104 Eur J Nucl Med Mol Imaging (2010) 37:1095–1105

Advanced Hodgkin’s Disease. N Engl J Med 1998;339(21):1506–14.
16. Spaepen K, Stroobants S, Dupont P, Thomas J, Vandenberghe P,Balzarini J, et al. Can positron emission tomography with [(18)F]-fluorodeoxyglucose after first-line treatment distinguish Hodg-kin’s disease patients who need additional therapy from others inwhom additional therapy would mean avoidable toxicity? Br JHaematol 2001;115(2):272–8.
17. Weihrauch MR, Re D, Scheidhauer K, Ansén S, Dietlein M,Bischoff S, et al. Thoracic positron emission tomography using18F-fluorodeoxyglucose for the evaluation of residual mediastinalHodgkin disease. Blood 2001;98(10):2930–4.
18. Cheson BD, Pfistner B, Juweid ME, Gascoyne RD, Specht L,Horning SJ, et al. Revised response criteria for malignantlymphoma. J Clin Oncol 2007;25(5):579–86.
19. Hutchings M, Mikhaeel NG, Fields PA, Nunan T, Timothy AR.Prognostic value of interim FDG-PET after two or three cycles ofchemotherapy in Hodgkin lymphoma. Ann Oncol 2005;16(7):1160–8.
20. Hutchings M, Loft A, Hansen M, Pedersen LM, Buhl T, JurlanderJ, et al. FDG-PET after two cycles of chemotherapy predictstreatment failure and progression-free survival in Hodgkinlymphoma. Blood 2006;107(1):52–9.
21. Kostakoglu L, Goldsmith SJ, Leonard JP, Christos P, Furman RR,Atasever T, et al. FDG-PET after 1 cycle of therapy predictsoutcome in diffuse large cell lymphoma and classic Hodgkindisease. Cancer 2006;107(11):2678–87.
22. Zinzani PL, Tani M, Fanti S, Alinari L, Musuraca G, Marchi E, etal. Early positron emission tomography (PET) restaging: apredictive final response in Hodgkin’s disease patients. AnnOncol 2006;17(8):1296–300.
23. Gallamini A, Hutchings M, Rigacci L, Specht L, Merli F, Hansen M,et al. Early interim 2-[18F]fluoro-2-deoxy-D-glucose positronemission tomography is prognostically superior to internationalprognostic score in advanced-stage Hodgkin’s lymphoma: a reportfrom a joint Italian-Danish study. J ClinOncol 2007;25(24):3746–52.
24. Furth C, Steffen IG, Amthauer H, Ruf J, Misch D, Schönberger S,et al. Early and late therapy response assessment with [18F]fluorodeoxyglucose positron emission tomography in pediatricHodgkin’s lymphoma: analysis of a prospective multicenter trial. JClin Oncol 2009;27(26):4385–91.
25. Terasawa T, Lau J, Bardet S, Couturier O, Hotta T, Hutchings M,et al. Fluorine-18-fluorodeoxyglucose positron emission tomogra-phy for interim response assessment of advanced-stage Hodgkin’slymphoma and diffuse large B-cell lymphoma: a systematicreview. J Clin Oncol 2009;27(11):1906–14.
26. Hutchings M, Loft A, Hansen M, Pedersen LM, Berthelsen AK,Keiding S, et al. Positron emission tomography with or withoutcomputed tomography in the primary staging of Hodgkin’slymphoma. Haematologica 2006;91(4):482–9.
27. Girinsky T, Specht L, Ghalibafian M, Edeline V, Bonniaud G, VanDer Maazen R, et al. The conundrum of Hodgkin lymphomanodes: to be or not to be included in the involved node radiationfields. The EORTC-GELA lymphoma group guidelines. RadiotherOncol 2008;88(2):202–10.
28. Townsend DW. Positron emission tomography/computed tomog-raphy. Semin Nucl Med 2008;38(3):152–66.
29. Fend F, Kremer M. Diagnosis and classification of malignantlymphoma and related entities in the bone marrow trephinebiopsy. Pathobiology 2007;74(2):133–43.
30. Kwee TC, Kwee RM, Verdonck LF, Bierings MB, NievelsteinRA. Magnetic resonance imaging for the detection of bonemarrow involvement in malignant lymphoma. Br J Haematol2008;141(1):60–8.
31. Hutchings M, Loft A, Hansen M, Ralfkiaer E, Specht L. Differenthistopathological subtypes of Hodgkin lymphoma show signifi-
cantly different levels of FDG uptake. Hematol Oncol 2006;24(3):146–50.
32. Küppers R. The biology of Hodgkin’s lymphoma. Nat Rev Cancer2009;9(1):15–27.
33. Munker R, Hasenclever D, Brosteanu O, Hiller E, Diehl V. Bonemarrow involvement in Hodgkin’ disease: an analysis of 135consecutive cases. German Hodgkin’s Lymphoma Study Group. JClin Oncol 1995;13(2):403–9.
34. Brunning RD, Bloomfield CD, McKenna RW, Peterson LA.Bilateral trephine bone marrow biopsies in lymphoma and otherneoplastic diseases. Ann Intern Med 1975;82(3):365–6.
35. Wang J, Weiss LM, Chang KL, Slovak ML, Gaal K, Forman SJ,et al. Diagnostic utility of bilateral bone marrow examination:significance of morphologic and ancillary technique study inmalignancy. Cancer 2002;94(5):1522–31.
36. Carr R, Barrington SF, Madan B, O’Doherty MJ, Saunders CA,van der Walt J, et al. Detection of lymphoma in bone marrow bywhole-body positron emission tomography. Blood 1998;91(9):3340–6.
37. Pakos EE, Fotopoulos AD, Ioannidis JP. 18F-FDG PET forevaluation of bone marrow infiltration in staging of lymphoma: ameta-analysis. J Nucl Med 2005;46(6):958–63.
38. Juweid ME. Utility of positron emission tomography (PET)scanning in managing patients with Hodgkin lymphoma. Hema-tology Am Soc Hematol Educ Program 2006;259–65:510–1.
39. Bain BJ. Bone marrow biopsy morbidity and mortality: 2002 data.Clin Lab Haematol 2004;26(5):315–8.
40. Munker R, Glass J, Griffeth LK, Sattar T, Zamani R, HeldmannM, et al. Contribution of PET imaging to the initial staging andprognosis of patients with Hodgkin’s disease. Ann Oncol 2004;15(11):1699–704.
41. Kabickova E, Sumerauer D, Cumlivska E, Drahokoupilova E,Nekolna M, Chanova M, et al. Comparison of 18F-FDG-PET andstandard procedures for the pretreatment staging of children andadolescents with Hodgkin’s disease. Eur J Nucl Med Mol Imaging2006;33(9):1025–31.
42. Rigacci L, Vitolo U, Nassi L, Merli F, Gallamini A, Pregno P, et al.Positron emission tomography in the staging of patients withHodgkin’s lymphoma. A prospective multicentric study by theIntergruppo Italiano Linfomi. Ann Hematol 2007;86(12):897–903.
43. Pelosi E, Penna D, Deandreis D, Chiappella A, Skanjeti A, VitoloU, et al. FDG-PET in the detection of bone marrow disease inHodgkin’s disease and aggressive non-Hodgkin’s lymphoma andits impact on clinical management. Q J Nucl Med Mol Imaging2008;52(1):9–16.
44. Cerci JJ, Pracchia LF, Soares Junior J, Linardi Cda C,Meneghetti JC,Buccheri V. Positron emission tomography with 2-[18F]-fluoro-2-deoxy-D-glucose for initial staging of hodgkin lymphoma: a singlecenter experience in Brazil. Clinics (Sao Paulo) 2009;64:491–8.
45. Schaefer NG, Strobel K, Taverna C, Hany TF. Bone involvementin patients with lymphoma: the role of FDG-PET/CT. Eur J NuclMed Mol Imaging 2007;34(1):60–7.
46. Young CS, Young BL, Smith SM. Staging Hodgkin’s disease with18-FDG PET. Comparison with CT and surgery. Clin PositronImaging 1998;1(3):161–4.
47. Moog F, Bangerter M, Kotzerke J, Guhlmann A, Frickhofen N,Reske SN. 18-F-fluorodeoxyglucose-positron emission tomogra-phy as a new approach to detect lymphomatous bone marrow. JClin Oncol 1998;16(2):603–9.
48. Engert A, Diehl V, Franklin J, Lohri A, Dörken B, Ludwig WD, etal. Escalated-dose BEACOPP in the treatment of patients withadvanced-stage Hodgkin’s lymphoma: 10 years of follow-up ofthe GHSG HD9 study. J Clin Oncol 2009;27(27):4548–54.
49. Fermé C, Eghbali H, Meerwaldt JH, Rieux C, Bosq J, Berger F, etal. Chemotherapy plus involved-field radiation in early-stageHodgkin’s disease. N Engl J Med 2007;357(19):1916–27.
Eur J Nucl Med Mol Imaging (2010) 37:1095–1105 1105
Copyright © 2022 FDOKUMEN




















