
Repair of canine mandibular bone defects with bone marrow stromal cells and porous β-tricalcium...
9
Biomaterials 28 (2007) 1005–1013 Repair of canine mandibular bone defects with bone marrow stromal cells and porous b-tricalcium phosphate Jie Yuan a,b,1 , Lei Cui a,b,1 , Wen Jie Zhang a,b , Wei Liu a,b , Yilin Cao a,b, a Shanghai Key Laboratory of Tissue Engineering, Department of Plastic and Reconstructive Surgery, Shanghai 9th People’s Hospital, Shanghai Jiao Tong University School of Medicine, 639 Zhi Zao Ju Road, Shanghai 200011, China b National Tissue Engineering Center of China, Shanghai, China Received 15 August 2006; accepted 9 October 2006 Available online 7 November 2006 Abstract Tissue engineering has become a new approach for repairing bone defects. Previous studies have been limited to the use of slow- degradable scaffolds with bone marrow stromal cells (BMSCs) in mandibular reconstruction. In this study, a 30 mm long mandibular segmental defect was repaired by engineered bone graft using osteogenically induced autologouse BMSCs seeded on porous b-tricalcium phosphate (b-TCP, n ¼ 5). The repair of defects was compared with those treated with b-TCP alone (n ¼ 6) or with autologous mandibular segment (n ¼ 4). In the BMSCs/b-TCP group, new bone formation was observed from 4 weeks post-operation, and bony- union was achieved after 32 weeks, which was detected by radiographic and histological examination. In contrast, minimal bone formation with almost fibrous connection was observed in the group treated with b-TCP alone. More importantly, the engineered bone with BMSCs/b-TCP achieved a satisfactory biomechanical property in terms of bending load strength, bending displacement, bending stress and Young’s modulus at 32 weeks post-operation, which was very close to those of contralateral edentulous mandible and autograft bone (p40.05). Based on these results, we conclude that engineered bone from osteogenically induced BMSCs and biodegradable b-TCP can well repair the critical-sized segmental mandibular defects in canines. r 2006 Elsevier Ltd. All rights reserved. Keywords: Tissue engineering; Bone marrow stromal cells; b-tricalcium phosphate; Mandibular reconstruction 1. Introduction Mandible keeps the integrity of maxillofacial complex for mastication and speech in oral-maxillofacial region. Repair of large mandibular bone defects caused by trauma, infection, cancer or congenital malformation remains a big challenge in reconstructive surgery [1]. Autogenous bone transplantation is the ‘‘gold standard’’ approach for repairing the bone defects at present [2]. The grafts can provide three elements, which are critical for bone regeneration: scaffolds for osteo-conduction, growth fac- tors for osteo-induction, and cells for osteogenesis [3]. However, the major problem of this approach is that patients need to sacrifice their healthy tissue from donor site which could result in donor site morbidity [4]. Recently, tissue engineering approach has been shown to be very effective in bone regeneration. The successful repair of bone defects has been demonstrated in immuno-deficient animals, such as athymic mice and rats [5,6], as well as in immuno-competent animals like canine and sheep [7–9]. Bone marrow stromal cells (BMSCs) have been found to be a major seed cell source for bone engineering. The osteogenic potential of BMSCs has been demonstrated both in vitro and in vivo [5–8,10]. In addition, many studies have succeeded in the repairing of bone defects by using BMSCs in animal model as well as in human beings [7–9,11,12]. Regarding scaffold, both nature and synthetic materials have been utilized for bone engineering [7–9,12–17]. In mandibular reconstruction, Abukawa et al. [18] have used poly-DL-lactic-co-glycolic acid (PLGA) ARTICLE IN PRESS www.elsevier.com/locate/biomaterials 0142-9612/$ - see front matter r 2006 Elsevier Ltd. All rights reserved. doi:10.1016/j.biomaterials.2006.10.015 Corresponding author. Department of Plastic Surgery, Shanghai 9th People’s Hospital, 639 Zhi Zao Ju Road, Shanghai 200011, PR China. Tel.: +86 21 63138341x5192; fax: +86 21 53078128. E-mail address: [email protected] (Y. Cao). 1 These authors contributed equally to this work.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Repair of canine mandibular bone defects with bone marrow stromal cells and porous β-tricalcium...

ARTICLE IN PRESS
0142-9612/$ - se
doi:10.1016/j.bi
�CorrespondPeople’s Hospi
Tel.: +8621 63
E-mail addr1These autho
Biomaterials 28 (2007) 1005–1013
www.elsevier.com/locate/biomaterials
Repair of canine mandibular bone defects with bone marrowstromal cells and porous b-tricalcium phosphate
Jie Yuana,b,1, Lei Cuia,b,1, Wen Jie Zhanga,b, Wei Liua,b, Yilin Caoa,b,�
aShanghai Key Laboratory of Tissue Engineering, Department of Plastic and Reconstructive Surgery, Shanghai 9th People’s Hospital,
Shanghai Jiao Tong University School of Medicine, 639 Zhi Zao Ju Road, Shanghai 200011, ChinabNational Tissue Engineering Center of China, Shanghai, China
Received 15 August 2006; accepted 9 October 2006
Available online 7 November 2006
Abstract
Tissue engineering has become a new approach for repairing bone defects. Previous studies have been limited to the use of slow-
degradable scaffolds with bone marrow stromal cells (BMSCs) in mandibular reconstruction. In this study, a 30mm long mandibular
segmental defect was repaired by engineered bone graft using osteogenically induced autologouse BMSCs seeded on porous b-tricalciumphosphate (b-TCP, n ¼ 5). The repair of defects was compared with those treated with b-TCP alone (n ¼ 6) or with autologous
mandibular segment (n ¼ 4). In the BMSCs/b-TCP group, new bone formation was observed from 4 weeks post-operation, and bony-
union was achieved after 32 weeks, which was detected by radiographic and histological examination. In contrast, minimal bone
formation with almost fibrous connection was observed in the group treated with b-TCP alone. More importantly, the engineered bone
with BMSCs/b-TCP achieved a satisfactory biomechanical property in terms of bending load strength, bending displacement, bending
stress and Young’s modulus at 32 weeks post-operation, which was very close to those of contralateral edentulous mandible and
autograft bone (p40.05). Based on these results, we conclude that engineered bone from osteogenically induced BMSCs and
biodegradable b-TCP can well repair the critical-sized segmental mandibular defects in canines.
r 2006 Elsevier Ltd. All rights reserved.
Keywords: Tissue engineering; Bone marrow stromal cells; b-tricalcium phosphate; Mandibular reconstruction
1. Introduction
Mandible keeps the integrity of maxillofacial complexfor mastication and speech in oral-maxillofacial region.Repair of large mandibular bone defects caused by trauma,infection, cancer or congenital malformation remains a bigchallenge in reconstructive surgery [1]. Autogenous bonetransplantation is the ‘‘gold standard’’ approach forrepairing the bone defects at present [2]. The grafts canprovide three elements, which are critical for boneregeneration: scaffolds for osteo-conduction, growth fac-tors for osteo-induction, and cells for osteogenesis [3].
e front matter r 2006 Elsevier Ltd. All rights reserved.
omaterials.2006.10.015
ing author. Department of Plastic Surgery, Shanghai 9th
tal, 639 Zhi Zao Ju Road, Shanghai 200011, PR China.
138341x5192; fax: +8621 53078128.
ess: [email protected] (Y. Cao).
rs contributed equally to this work.
However, the major problem of this approach is thatpatients need to sacrifice their healthy tissue from donorsite which could result in donor site morbidity [4].Recently, tissue engineering approach has been shown tobe very effective in bone regeneration. The successful repairof bone defects has been demonstrated in immuno-deficientanimals, such as athymic mice and rats [5,6], as well as inimmuno-competent animals like canine and sheep [7–9].Bone marrow stromal cells (BMSCs) have been found to
be a major seed cell source for bone engineering. Theosteogenic potential of BMSCs has been demonstratedboth in vitro and in vivo [5–8,10]. In addition, many studieshave succeeded in the repairing of bone defects by usingBMSCs in animal model as well as in human beings[7–9,11,12]. Regarding scaffold, both nature and syntheticmaterials have been utilized for bone engineering[7–9,12–17]. In mandibular reconstruction, Abukawaet al. [18] have used poly-DL-lactic-co-glycolic acid (PLGA)

ARTICLE IN PRESSJ. Yuan et al. / Biomaterials 28 (2007) 1005–10131006
scaffold seeded with osteogenic induced autologousBMSCs to repair a 2� 2 cm partial mandibular defect ina porcine model, while Schliephake et al. [19] have repaireda 35mm length segmental mandibular defect with pyrolizedbovine bone as scaffold in a sheep model. It is known thatPLGA scaffold is difficult to shape for repairing large bonedefects, while pyrolized bovine bone is nearly undegradablein vivo. In addition, as a natural material, pyrolized bovinebone still remains the risk of pathogen transmission [20].Thus, other potential synthetic materials should be testedfor mandibular bone engineering.
Porous b-tricalcium phosphate (b-TCP) is a syntheticand biodegradable ceramic material that has been com-monly used in various applications in oral and maxilo-facial surgery, such as alveolar ridge augmentation, sinusfloor augmentation [21,22], and has also been widely usedin benign bone tumor filling [23]. In a sheep model offemoral condyle implantation, it has been reported that55% of the b-TCP could be degraded after 24 weeks ofimplantation [24]. Porous b-TCP is also known as amaterial with good osteo-conductive capacity due to it’shigh porosity and interconnectivity that can provideintercellular communication among osteogeneic cells restedin lacunae [25,26]. However, porous b-TCP is very fragile,the scaffold solely made of b-TCP cannot bear strongmechanical forces [27]. Whether pure b-TCP scaffold couldbe used to repair load-bearing bone defect in large animalmodel become an attractive issue.
In this study, porous b-TCP seeded with in vitro cultureexpanded, osteogenically induced BMSCs had been im-planted to repair a 30mm length critical-sized segmentalmandibular defect in a canine model. A satisfactory repairwas achieved at 32 weeks post-implantation, suggestingthat autologous BMSCs, along with porous b-TCP, couldbe potentially used for the clinical repair of mandibularbone defects.
2. Materials and methods
2.1. Animals
A total of 16 adult mongrel dogs in healthy condition, aged 18 months
old with an average weight of 20.9 kg were used in this study. All dogs
were prepared by extraction of the upper and lower premolar and first
molar teeth at right sides 8 weeks before segmental mandibular resection.
The dogs were kept on a soft diet during the study and were allowed
complete gingival healing before mandibular resection surgery. The
experimental protocol was approved by the Animal Care and Experiment
Committee of Shanghai Jiao Tong University School of Medicine.
2.2. Cell culture and induction
After intravenous anesthesia with 5% sodium pentobarbital (0.5mL/kg),
3mL of bone marrow aspirates were harvested from the iliac crests of each
dog and transferred into a pre-heparinized centrifuge tube. Mononuclear
cells were separated by percoll (1.073 g/mL, Sigma, St Louise, MO) gradient
centrifugation [28], and were plated in 100-mm dishes (Falcon, Franklin
Lakes, NJ) at a density of 1� 105 cells/cm2. Cells were cultured in osteogenic
induction media (Dulbecco’s Modified Eagle Medium (DMEM, Gibco,
Grand Island, NY) supplemented with 10% fetal bovine serum (FBS,
Gibco), 10�8mol/L dexamethasone, 10mmol/L b-phosphoglycerol and
50mmol/L L-2-ascorbic acid (all from Sigma)) at 37 1C with 5% CO2. The
culture medium was changed after 48h and then every 3 days. When BMSCs
reached 80–90% confluence, cells were detached with 0.25% trypsin/EDTA
(Gibco), subcultured at a density of 1� 105 cells/cm2 in 100-mm dishes.
2.3. Preparation of BMSCs/b-TCP construct
b-TCP scaffolds (purchased from Shanghai Bio-Lu Biomaterials Co.,
Ltd., Shanghai, China) were molded into cuboids (30� 15� 10mm) with
a 3mm diameter tunnel which mimicking a normal structure of mandible
(Fig. 1), and were sterilized by 60Co irradiation before use. The scaffolds
have volume porosity of 70% with pore diameter of 450750mm. Scanning
electron microscope showed that all pores were interconnected with inter-
pore diameter of 150750 mm (Fig. 2A). The initial compression strength
was 2–4MPa [29]. For cell seeding, osteogenically induced BMSCs at
passage 2 were detached from culture dishes, centrifuged to remove
supernatant, and then resuspended in the culture media at a density of
2� 107 cells/mL. Cells in suspension were slowly injected into the b-TCPcuboids using a syringe (3mL/cuboid). After being incubated for 4 h to
allow cell attachment, 30mL of osteogenic induction medium were then
added to cover the constructs. The BMSCs/b-TCP constructs were
subsequently cultured for 7 days in vitro before implantation.
In a parallel experiment, 3� 3� 3mm cuboids were prepared and
seeded with BMSCs at an identical cell density. After 7 days of incubation,
the constructs were fixed in 2% formalin for 2 h, cut into two halves, and
then subjected for scanning electron microscopy (Philips SEM XL-30,
Amsterdam, Netherlands) examination.
2.4. Surgical procedure
The canines were anesthetized through intramuscular injection of
ketamine (10mg/kg) and were placed in a supine position. The body of
right mandible was exposed through a submental midline skin incision.
After adjustment of the titanium plate, an osteoperiosteal segmental defect
of 30mm length was made at the mid-portion of mandible using
an oscillating bone saw that was cooled continuously by saline irrigation
(Fig. 3A). The neurovascular bundle was cut off and stanched by filling
bone wax into mandibular canal. Then, the titanium plate was secured in
place with six screws (three at the mesial side and three at the distal side).
The defects were filled either with osteogenically induced BMSCs/b-TCPconstructs (experimental group, n ¼ 6), resected autologous mandibular
segments (autograft group, n ¼ 4), or with b-TCP cuboids alone (scaffold
group, n ¼ 6) (Fig. 3B). The incisions were closed with 3-0 silk suture.
Meanwhile, the lower premolar and first molar teeth at left side were
extracted and the edentulous mandibles were served as normal control
(n ¼ 16). All animals were kept on a soft diet during the study. In order to
give newly formed tissue a mechanical loading, the titanium plates were
removed from all dogs at 22 weeks post-operation.
2.5. Radiographic and dual energy X-ray absorptiometry analyses
Mandibular radiograms were obtained under general anesthesia at 4,
12, 26 and 32 weeks post-operation. Maxillofacial CT images were
obtained and the three-dimensional images were reconstructed using a
multi-slice spiral CT (GE Lightspeed Ultra 16, Milwaukee, WI) at 32
weeks post-operation. For dual energy X-ray absorptiometry (DXA)
analysis, animals were sacrificed at 32 weeks post-operation, and the
mandibles were harvested. The local bone mineral densities (BMD) were
measured on a DXA system (Hologic Discovery A, Bedford, MA).
2.6. Biomechanical analysis
For biomechanical analysis, mandibles of all groups were harvested at
32 weeks post-operation. The left side mandible of each animal was also
ARTICLE IN PRESS
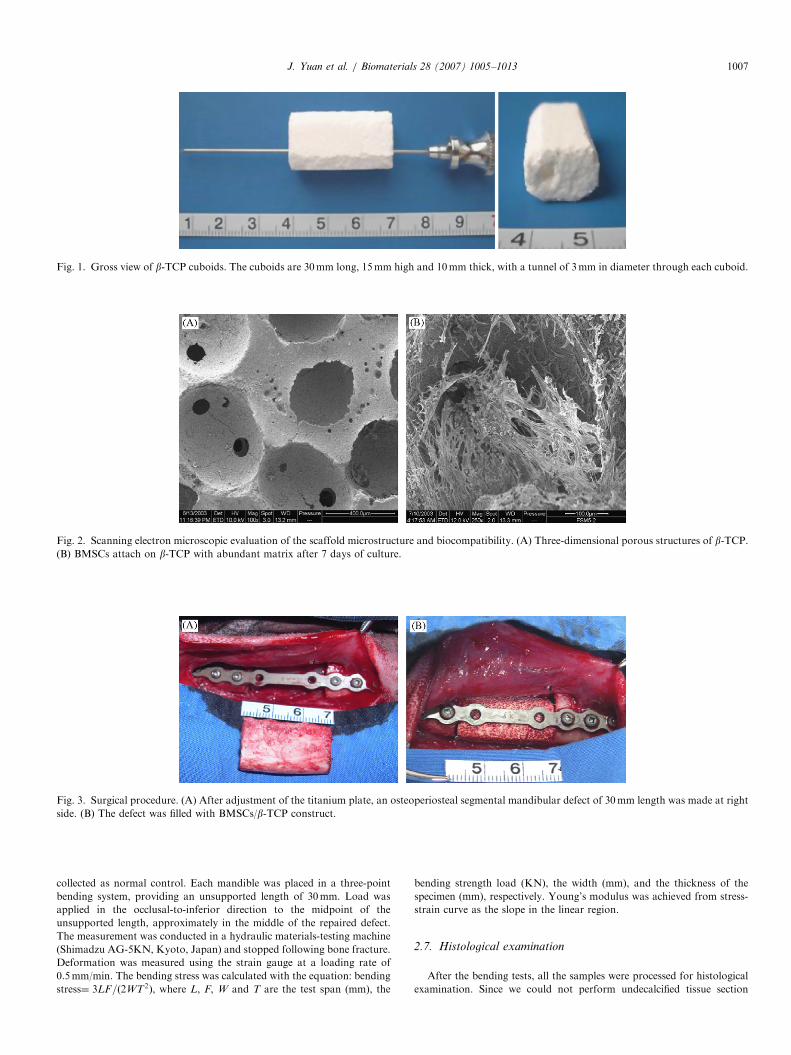
Fig. 1. Gross view of b-TCP cuboids. The cuboids are 30mm long, 15mm high and 10mm thick, with a tunnel of 3mm in diameter through each cuboid.
Fig. 2. Scanning electron microscopic evaluation of the scaffold microstructure and biocompatibility. (A) Three-dimensional porous structures of b-TCP.(B) BMSCs attach on b-TCP with abundant matrix after 7 days of culture.
Fig. 3. Surgical procedure. (A) After adjustment of the titanium plate, an osteoperiosteal segmental mandibular defect of 30mm length was made at right
side. (B) The defect was filled with BMSCs/b-TCP construct.
J. Yuan et al. / Biomaterials 28 (2007) 1005–1013 1007
collected as normal control. Each mandible was placed in a three-point
bending system, providing an unsupported length of 30mm. Load was
applied in the occlusal-to-inferior direction to the midpoint of the
unsupported length, approximately in the middle of the repaired defect.
The measurement was conducted in a hydraulic materials-testing machine
(Shimadzu AG-5KN, Kyoto, Japan) and stopped following bone fracture.
Deformation was measured using the strain gauge at a loading rate of
0.5mm/min. The bending stress was calculated with the equation: bending
stress¼ 3LF=ð2WT2Þ, where L, F, W and T are the test span (mm), the
bending strength load (KN), the width (mm), and the thickness of the
specimen (mm), respectively. Young’s modulus was achieved from stress-
strain curve as the slope in the linear region.
2.7. Histological examination
After the bending tests, all the samples were processed for histological
examination. Since we could not perform undecalcified tissue section
ARTICLE IN PRESSJ. Yuan et al. / Biomaterials 28 (2007) 1005–10131008
due to the limited condition, tissues from original defect area of all groups
were fixed in buffered 10% formalin in PBS for 72 h, and decalcified in
15% formic acid in PBS for 2–10 weeks. The decalcified tissues of
interfacial portion were then embedded in paraffin. Tissue sections in 5 mmthickness were obtained for hematoxylin and eosin (H&E) staining.
2.8. Statistical analysis
Data from DXA and biomechanical examination were analyzed by
one-way ANOVA test. The differences between experimental group
(n ¼ 5), scaffold group (n ¼ 6), autograft group (n ¼ 4), and normal
group (n ¼ 5) were assessed with Student-Newman-Kewls test. A p value
less than 0.05 was considered statistically significant.
3. Results
3.1. Growth of osteogenically induced BMSCs on b-TCP
After being cultivated in the presence of dexamethasoneand b-phosphoglycerol for 2 passages, BMSCs showed atypical osteogenic phenotype as previously described,including calcium deposition and positive alkaline phos-phatase (AKP) staining (data not shown).
To evaluate the compatibility of the scaffold, BMSCswere seed on the b-TCP scaffolds, incubated in vitro for 7days, and cell-scaffold complexes were subjected for SEMexamination. As shown in Fig. 2B, the pores were filled bycells together with abundant extracellular matrices after7 days of incubation, indicating that the scaffold has good
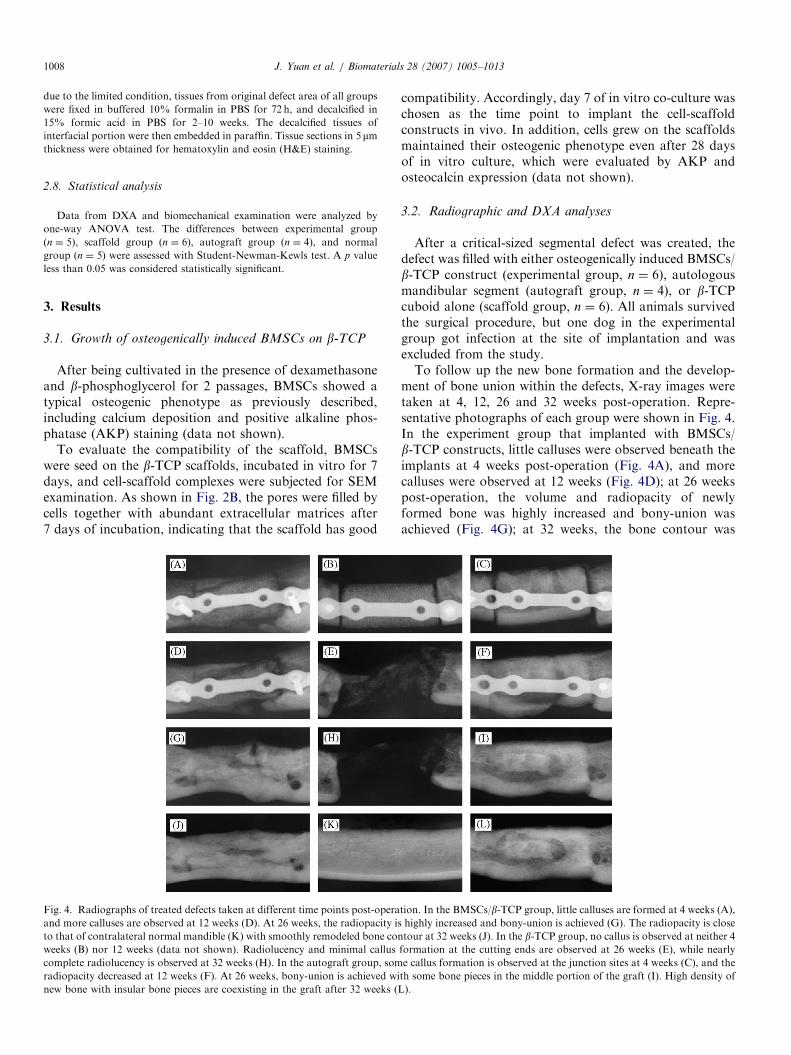
Fig. 4. Radiographs of treated defects taken at different time points post-opera
and more calluses are observed at 12 weeks (D). At 26 weeks, the radiopacity is
to that of contralateral normal mandible (K) with smoothly remodeled bone con
weeks (B) nor 12 weeks (data not shown). Radiolucency and minimal callus
complete radiolucency is observed at 32 weeks (H). In the autograft group, som
radiopacity decreased at 12 weeks (F). At 26 weeks, bony-union is achieved wi
new bone with insular bone pieces are coexisting in the graft after 32 weeks (L
compatibility. Accordingly, day 7 of in vitro co-culture waschosen as the time point to implant the cell-scaffoldconstructs in vivo. In addition, cells grew on the scaffoldsmaintained their osteogenic phenotype even after 28 daysof in vitro culture, which were evaluated by AKP andosteocalcin expression (data not shown).
3.2. Radiographic and DXA analyses
After a critical-sized segmental defect was created, thedefect was filled with either osteogenically induced BMSCs/b-TCP construct (experimental group, n ¼ 6), autologousmandibular segment (autograft group, n ¼ 4), or b-TCPcuboid alone (scaffold group, n ¼ 6). All animals survivedthe surgical procedure, but one dog in the experimentalgroup got infection at the site of implantation and wasexcluded from the study.To follow up the new bone formation and the develop-
ment of bone union within the defects, X-ray images weretaken at 4, 12, 26 and 32 weeks post-operation. Repre-sentative photographs of each group were shown in Fig. 4.In the experiment group that implanted with BMSCs/b-TCP constructs, little calluses were observed beneath theimplants at 4 weeks post-operation (Fig. 4A), and morecalluses were observed at 12 weeks (Fig. 4D); at 26 weekspost-operation, the volume and radiopacity of newlyformed bone was highly increased and bony-union wasachieved (Fig. 4G); at 32 weeks, the bone contour was
tion. In the BMSCs/b-TCP group, little calluses are formed at 4 weeks (A),
highly increased and bony-union is achieved (G). The radiopacity is close
tour at 32 weeks (J). In the b-TCP group, no callus is observed at neither 4
formation at the cutting ends are observed at 26 weeks (E), while nearly
e callus formation is observed at the junction sites at 4 weeks (C), and the
th some bone pieces in the middle portion of the graft (I). High density of
).

ARTICLE IN PRESSJ. Yuan et al. / Biomaterials 28 (2007) 1005–1013 1009
remodeled smoothly (Fig. 4J) and the radiopacity was closeto that of contralateral normal mandible (Fig. 4K). On thecontrary, no callus could be observed in the groupimplanted with b-TCP alone, neither at 4 weeks (Fig. 4B)nor at 12 weeks (data not shown). At 26 weeks, obviousradiolucency and minimal callus formation at the cuttingends was observed in this group (Fig. 4E), and nearlycomplete radiolucency was observed at 32 weeks post-operation (Fig. 4H). As a positive control, the autograftgroup showed some callus formation at the junction sites at4 weeks post-operation (Fig. 4C), and the radiopacity wasdecrease in the middle portion of the graft at 12 weeks(Fig. 4F); at 26 weeks post-operation, bony-union was alsoachieved with some insular bone pieces observed in themiddle portion of the grafts (Fig. 4I). The bone densitycontinuously increased with newly formed bone and insularbone pieces coexisting in the graft after 32 weeks (Fig. 4L).Radiographic union was observed in all of the experimentgroup (5/5) and autograft group (4/4), but not in thescaffold group (0/6).
To detect the three-dimensional structure of repairedmandibles, 3D-CT images were taken at 32 weeks post-operation. Representative images from each group werepresent in Fig. 5. In the experimental group which wastreated with BMSCs/b-TCP constructs, bony-union and anice mandibular body shape were observed (Fig. 5A).
Fig. 5. 3D-CT images of treated mandibles at 32 weeks post-operation. (A) I
observed. (B) In the b-TCP group, non-union and minimal callus are formed. (C
at buccal side.
However, in the group treated with b-TCP alone, non-union was observed and only minimal calluses weredetected (Fig. 5B). In the autograft group, bony-unionwas achieved while insular bone pieces were also observedat the buccal side (Fig. 5C).To quantify the calcification of repaired mandibles, local
bone mineral densities (BMD) of all animals weremeasured on DXA at 32 weeks post-operation (Fig. 6).The BMSCs/b-TCP grafts showed relatively high BMD of0.5570.06 g/cm2, which was similar to the contralateralnormal group (0.6070.06 g/cm2, p40.05). Whereas in thescaffold group, the local BMD was 0.1970.05 g/cm2,which was significantly lower than that of the BMSCs/b-TCP grafts (po0.01). Meanwhile, the BMD of autograftgroup was significantly higher than other three groups(0.8770.17 g/cm2, po0.05).
3.3. Gross view and biomechanical analysis
Correlated with radiographic analyses, gross view of themandibles repaired with either BMSCs/b-TCP constructsor autologous bones achieved bony-union at 32 weekspost-operation (Fig. 7A, C). The shapes of repairmandibles were very close to that of normal edentulousmandibles (Fig. 7D). On the contrary, none bony-unionwas observed when implanted with b-TCP alone, obvious
n the BMSCs/b-TCP group, bony-union with mandibular body shape is
) In the autograft group, bony-union is observed together with bone piece

ARTICLE IN PRESSJ. Yuan et al. / Biomaterials 28 (2007) 1005–10131010
soft tissues were detected in the original defect area in thisgroup (Fig. 7B).
To evaluate the biomechanical property of repairedmandibles, three-point bending test was performed at 32weeks post-operation. As shown in Table 1, the bendingload strength and bending stress in the BMSCs/b-TCPgroup were 1.8070.42 kN and 44.73710.12MPa, reached65.16721.41% and 81.63712.88% of the contralateralnormal edentulous mandible, respectively. Furthermore,comparing with the normal mandible, tissue-engineeredsegmental bone revealed similarities with respects tobending load strength, bending displacement, bendingstress and Young’s modulus (p40.05, Table 1). Thebending load strength and bending stress of the autograftgroup were 2.7170.30 kN and 43.12711.98MPa, respec-tively. Again, no significant differences were found betweenthe experimental and autograft group in terms of all the
Fig. 7. Gross view of repaired mandibles at 32 weeks post-operation. (A) In t
notches are observed. (B) In the b-TCP group, soft tissues are detected in the de
is observed. (D) Contralateral edentulous native mandible. Arrows indicate th
Fig. 6. Dual energy X-ray absorptiometry analysis at 32 weeks post-
operation. The local bone mineral density (BMD) of BMSCs/b-TCPimplants (n ¼ 5) was similar to that of normal control group (n ¼ 5,
p40.05), but significantly higher than that of b-TCP implants (n ¼ 6,
po0.01), and lower than that of bone autografts (n ¼ 4, po0.05).
biomechanical parameters tested (p40.05, Table 1). Sincethere is no bony-union in the scaffold group, which wastreated with b-TCP alone, three-point bending test couldnot be applied in this group.
3.4. Histological examination
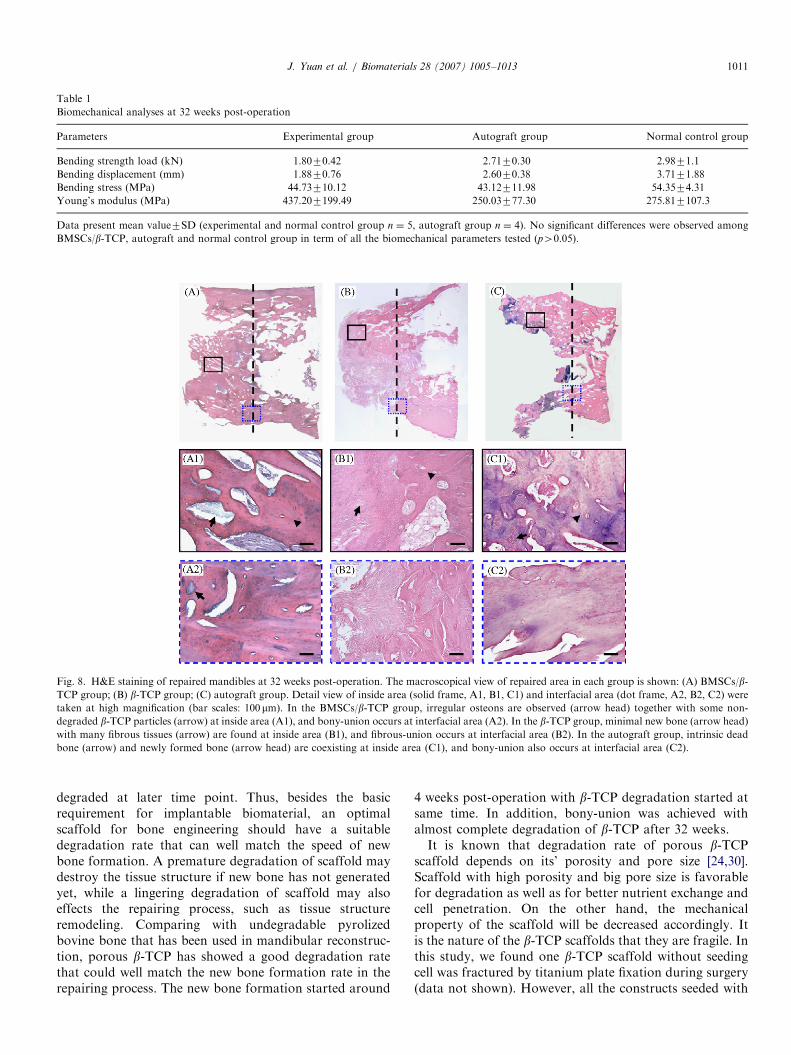
To further confirm the above findings, the histology ofrepaired defects at 32 weeks post-operation was detectedafter bending tests by decalcified tissue section with H&Estaining. Representative photographs from each groupwere present in Fig. 8. In the experimental group, irregularosteon formation was observed together with some‘‘ghost’’ structures of undegraded b-TCP particles in therepaired area (Fig. 8A1), which has been previouslydescribed by Dong et al. [27]. In addition, a bony-unionwas observed without clear boundary between newlyformed bone and native bone in this group (Fig. 8A2). Inthe autograft group, a bony-union was also observed withintrinsic dead bone and newly formed bone coexisting inthe repaired area (Fig. 8C1 and C2). However, in thescaffold group, only fibrous tissues were observed in thedefect area with minimal new bone formation at cuttingend (Fig. 8B1 and B2). Similar results were observed withAzan-Mallory staining (data not shown).
4. Discussion
The current study demonstrates that the critical-sizedsegmental defects of the canine mandible can be repairedby osteogenically induced BMSCs with biodegradable b-TCP scaffold. Meanwhile, scaffold alone is not sufficientenough to repair such a big defect in this model.Biodegradable scaffold plays a pivotal role in bone
engineering. The scaffold can provide a skeletal support forthe growth of osteogenic cells at early stage and createenough space for new bone formation when they are
he BMSCs/b-TCP group, bony-union with white colored cortex and some
fect. (C) In the autograft group, bony-union with red-white colored cortex
e junction sites.
ARTICLE IN PRESS
Table 1
Biomechanical analyses at 32 weeks post-operation
Parameters Experimental group Autograft group Normal control group
Bending strength load (kN) 1.8070.42 2.7170.30 2.9871.1
Bending displacement (mm) 1.8870.76 2.6070.38 3.7171.88
Bending stress (MPa) 44.73710.12 43.12711.98 54.3574.31
Young’s modulus (MPa) 437.207199.49 250.03777.30 275.817107.3
Data present mean value7SD (experimental and normal control group n ¼ 5, autograft group n ¼ 4). No significant differences were observed among
BMSCs/b-TCP, autograft and normal control group in term of all the biomechanical parameters tested (p40.05).
Fig. 8. H&E staining of repaired mandibles at 32 weeks post-operation. The macroscopical view of repaired area in each group is shown: (A) BMSCs/b-TCP group; (B) b-TCP group; (C) autograft group. Detail view of inside area (solid frame, A1, B1, C1) and interfacial area (dot frame, A2, B2, C2) were
taken at high magnification (bar scales: 100mm). In the BMSCs/b-TCP group, irregular osteons are observed (arrow head) together with some non-
degraded b-TCP particles (arrow) at inside area (A1), and bony-union occurs at interfacial area (A2). In the b-TCP group, minimal new bone (arrow head)
with many fibrous tissues (arrow) are found at inside area (B1), and fibrous-union occurs at interfacial area (B2). In the autograft group, intrinsic dead
bone (arrow) and newly formed bone (arrow head) are coexisting at inside area (C1), and bony-union also occurs at interfacial area (C2).
J. Yuan et al. / Biomaterials 28 (2007) 1005–1013 1011
degraded at later time point. Thus, besides the basicrequirement for implantable biomaterial, an optimalscaffold for bone engineering should have a suitabledegradation rate that can well match the speed of newbone formation. A premature degradation of scaffold maydestroy the tissue structure if new bone has not generatedyet, while a lingering degradation of scaffold may alsoeffects the repairing process, such as tissue structureremodeling. Comparing with undegradable pyrolizedbovine bone that has been used in mandibular reconstruc-tion, porous b-TCP has showed a good degradation ratethat could well match the new bone formation rate in therepairing process. The new bone formation started around
4 weeks post-operation with b-TCP degradation started atsame time. In addition, bony-union was achieved withalmost complete degradation of b-TCP after 32 weeks.It is known that degradation rate of porous b-TCP
scaffold depends on its’ porosity and pore size [24,30].Scaffold with high porosity and big pore size is favorablefor degradation as well as for better nutrient exchange andcell penetration. On the other hand, the mechanicalproperty of the scaffold will be decreased accordingly. Itis the nature of the b-TCP scaffolds that they are fragile. Inthis study, we found one b-TCP scaffold without seedingcell was fractured by titanium plate fixation during surgery(data not shown). However, all the constructs seeded with

ARTICLE IN PRESSJ. Yuan et al. / Biomaterials 28 (2007) 1005–10131012
BMSCs maintained their shape without broken. Inconsistent with our results, Dong et al. [27] found thatthe compressive strength of b-TCP scaffold could besignificantly improved by cell seeding. These resultsindicate that the mechanical property of this scaffold couldbe improved. Further studies of modifying b-TCP scaffoldswith extracellular matrix to improve the mechanicalproperty are under investigation.
Regard to bone regeneration, some groups reported thatscaffold alone or scaffold modified with growth factorscould achieve bone reconstruction without seeding osteo-genic cells [31–34]. However, no bony-union could beobserved in our study with b-TCP alone. Comparing withthose studies, we found that only small defects could berepaired with scaffold alone but not big defects, which isconsistent with other groups reported [32,35]. In smalldefects, native cells could migrate into the scaffold togenerate new tissues and achieve bony-union. While in bigdefects, the migration rate of native cells was not fastenough to match the degradation of scaffold. Thus, onlyfibrous union was achieved. It is known that seededBMSCs can not only provide an osteogenic cell source fornew bone formation, but also secret growth factors torecruit native cells migrate into the defect site [36–40]. Inorder to clarify the repairing mechanism and to follow thelong-term fate of the implanted BMSCs, further study oftreating defects with green fluorescence protein genelabeled BMSCs is ongoing.
The degradation of calcium phosphate biomaterials invivo could be through two processes: first, throughextracellular liquid dissolution, and second, throughdisintegration into small particles that would be eitherintra-cellularly digested or be transported to neighboringtissues such as the lymph nodes finally [41]. In this study,the degradation of b-TCP might be also through bothprocesses [24]. The abundant blood circulation of oral-maxillofacial region could promote the dissolution process,which has been well shown in the experimental and scaffoldgroup at early stage (Fig. 4, 4 weeks data). When thescaffold broke into small pieces at late stage (Fig. 4, 12weeks data), the small particles could be either phagocy-tosed or be transported to neighboring tissues, although wehave not found typical osteoclasts in the experimentalgroup by histological analysis. One possible reason couldbe that the decalcification process could partially destroythe tissue structure and affect the results. More accuratehistology could be achieved by undecalcified tissue section.Handschel et al. [42] reported that b-TCP was hardlyresorbed in a non-loading calvarial model, while it could beeasily degraded in the load-bearing area as we and otherresearchers observed [34], indicating that mechanical forcescould also facilitate the degradation of b-TCP scaffold. Inaddition, mechanical forces are believed to be responsiblefor determining the structure of regenerated bone [43]. Togive newly formed bone a mechanical loading, we haveremoved the titanium plate at 22 weeks post-operation inall groups in the study. A mandibular contour remodeling
could be observed in the experiment group when compar-ing the radiographic data at 32 weeks with the data at 26weeks post-operation (Fig. 4G and J). Although thestructure of regenerated bone has not been completelyremodeled into the structure like normal mandible has,biomechanical analysis revealed that the engineered bonewas functionally similar to normal mandible in terms ofmechanical property. Long term follow up is required tosee if engineered bone can be remodeled into a normalmandibular structure with canal finally.Autogenous bone transplantation is the ‘‘gold standard’’
approach for repairing bone defects. The repairing processis called a ‘‘creeping substitution’’ which includes bothresorptive and appositional processes [2]. In this study, wefound that the BMD of the bone graft was significantlyhigher than that of the normal control mandibles at 32weeks after implantation. This is probably due to theexistence of both newly formed bone and intrinsic deadbone in the grafts, which was demonstrated by histologicalanalysis. Accordingly, the bending stress of the autolo-gouse bone grafts was lower than that of engineered bone.It has been reported that it would normally take 1–2 yearsto achieve normal biomechnical property after autologousbone transplantation [44].
5. Conclusions
This study demonstrates that bone substitutes con-structed by porous b-TCP scaffold loaded with osteogeni-cally induced BMSCs could repair the critical-sizedmandibular defects in large mammal. The satisfactoryrepair rate suggests that this might be a feasible approachfor the clinical reconstruction of segmental mandibulardefects.
Acknowledgements
This work was supported by Major State Basic ResearchDevelopment Program of China (G1999054300,2005CB522700), National High Technology Researchand Development Program of China (2002AA205011),and Shanghai Science and Technology DevelopmentFoundation.We thank Drs. Deli Liu, Yulai Weng, Guangdong Zhou,
Lian Zhu, Ming Wang, Li Zhao, Guangpeng Liu, GangCai, Wanyao Xia, and Jinjun Chen for their contributionsto this paper. We also appreciate the technical assistancefrom Drs. Demin Ying, Lijuan Zong, Juanjuan Wu, andBin Zhong.
References
[1] Hadlock TA, Vacanti JP, Cheney ML. Tissue engineering in facial
plastic and reconstructive surgery. Fac Plast Surg 1998;14:197–203.
[2] Burchardt H. The biology of bone graft repair. Clin Orthop Relat
Res 1983(174):28–42.
[3] Vaccaro AR. The role of the osteoconductive scaffold in synthetic
bone graft. Orthopedics 2002;25:S571–8.
ARTICLE IN PRESSJ. Yuan et al. / Biomaterials 28 (2007) 1005–1013 1013
[4] Younger EM, Chapman MW. Morbidity at bone graft donor sites. J
Orthop Trauma 1989;3:192–5.
[5] Muraglia A, Martin I, Cancedda R, Quarto R. A nude mouse model
for human bone formation in unloaded conditions. Bone 1998;22:
S131–4.
[6] Bruder SP, Kurth AA, Shea M, Hayes WC, Jaiswal N, Kadiyala S.
Bone regeneration by implantation of purified, culture-expanded
human mesenchymal stem cells. J Orthop Res 1998;16:155–62.
[7] Bruder SP, Kraus KH, Goldberg VM, Kadiyala S. The effect of
implants loaded with autologous mesenchymal stem cells on the
healing of canine segmental bone defects. J Bone Joint Surg Am 1998;
80:985–96.
[8] Kon E, Muraglia A, Corsi A, Bianco P, Marcacci M, Martin I, et al.
Autologous bone marrow stromal cells loaded onto porous hydro-
xyapatite ceramic accelerate bone repair in critical-size defects of
sheep long bones. J Biomed Mater Res 2000;49:328–37.
[9] Arinzeh TL, Peter SJ, Archambault MP, van den Bos C, Gordon S,
Kraus K, et al. Allogeneic mesenchymal stem cells regenerate bone in
a critical-sized canine segmental defect. J Bone Joint Surg Am 2003;
85A:1927–35.
[10] Maniatopoulos C, Sodek J, Melcher AH. Bone formation in vitro by
stromal cells obtained from bone marrow of young adult rats. Cell
Tissue Res 1988;254:317–30.
[11] Casabona F, Martin I, Muraglia A, Berrino P, Santi P, Cancedda R,
et al. Prefabricated engineered bone flaps: an experimental model of
tissue reconstructionin plastic surgery. Plast Reconstr Surg 1998;101:
577–81.
[12] Quarto R, Mastrogiacomo M, Cancedda R, Kutepov SM, Mukha-
chev V, Lavroukov A, et al. Repair of large bone defects with the use
of autologous bone marrow stromal cells. N Engl J Med 2001;344:
385–6.
[13] Vuola J, Taurio R, Goransson H, Asko-Seljavaara S. Compressive
strength of calcium carbonate and hydroxyapatite implants after
bone-marrow-induced osteogenesis. Biomaterials 1998;19:223–7.
[14] Arnaud E, De Pollak C, Meunier A, Sedel L, Damien C, Petite H.
Osteogenesis with coral is increased by BMP and BMC in a rat
cranioplasty. Biomaterials 1999;20:1909–18.
[15] Petite H, Viateau V, Bensaid W, Meunier A, de Pollak C,
Bourguignon M, et al. Tissue-engineered bone regeneration. Nat
Biotechnol 2000;18:959–63.
[16] Shang Q, Wang Z, Liu W, Shi Y, Cui L, Cao Y. Tissue-engineered
bone repair of sheep cranial defects with autologous bone marrow
stromal cells. J Craniofac Surg 2001;12:586–93.
[17] Zhu L, Liu W, Cui L, Cao Y. Review article: tissue-engineered bone
repair of goat-femur defects with osteogenically induced bone
marrow stromal cells. Tissue Eng 2006;12:423–33.
[18] Abukawa H, Shin M, Williams WB, Vacanti JP, Kaban LB, Troulis
MJ. Reconstruction of mandibular defects with autologous tissue-
engineered bone. J Oral Maxillofac Surg 2004;62:601–6.
[19] Schliephake H, Knebel JW, Aufderheide M, Tauscher M. Use of
cultivated osteoprogenitor cells to increase bone formation in
segmental mandibular defects: an experimental pilot study in sheep.
Int J Oral Maxillofac Surg 2001;30:531–7.
[20] Sogal A, Tofe AJ. Risk assessment of bovine spongiform encephalo-
pathy transmission through bone graft material derived from bovine
bone used for dental applications. J Periodontol 1999;70:1053–63.
[21] Zerbo IR, Bronckers AL, de Lange GL, van Beek GJ, Burger EH.
Histology of human alveolar bone regeneration with a porous
tricalcium phosphate. A report of two cases. Clin Oral Implants Res
2001;12:379–84.
[22] Horch HH, Sader R, Pautke C, Neff A, Deppe H, Kolk A. Synthetic,
pure-phase beta-tricalcium phosphate ceramic granules (Cerasorb)
for bone regeneration in the reconstructive surgery of the jaws. Int J
Oral Maxillofac Surg 2006;35:708–13.
[23] Ogose A, Hotta T, Kawashima H, Kondo N, GuW, Kamura T, et al.
Comparison of hydroxyapatite and beta tricalcium phosphate as
bone substitutes after excision of bone tumors. J BiomedMater Res B
Appl Biomater 2005;72:94–101.
[24] Lu J, Descamps M, Dejou J, Koubi G, Hardouin P, Lemaitre J, et al.
The biodegradation mechanism of calcium phosphate biomaterials in
bone. J Biomed Mater Res 2002;63:408–12.
[25] Boo JS, Yamada Y, Okazaki Y, Hibino Y, Okada K, Hata K, et al.
Tissue-engineered bone using mesenchymal stem cells and a
biodegradable scaffold. J Craniofac Surg 2002;13:231–9.
[26] Ogose A, Hotta T, Hatano H, Kawashima H, Tokunaga K, Endo N,
et al. Histological examination of beta-tricalcium phosphate graft in
human femur. J Biomed Mater Res 2002;63:601–4.
[27] Dong J, Uemura T, Shirasakie Y, Tateishi T. Promotion of bone
formation using highly pure porous b-TCP combined with bone
marrow-derived osteoprogenitor cells. Biomaterials 2002;23:4493–502.
[28] Guo Z, Yang J, Liu X, Li X, Hou C, Tang PH, et al. Biological
features of mesenchymal stem cells from human bone marrow. Chin
Med J (Engl) 2001;114:950–3.
[29] Guo X, Wang C, Zhang Y, Xia R, Hu M, Duan C, et al. Repair of
large articular cartilage defects with implants of autologous
mesenchymal stem cells seeded into b-tricalcium phosphate in a
sheep model. Tissue Eng 2004;10:1818–29.
[30] Yokozeki H, Hayashi T, Nakagawa T, Kurosawa H, Shibuya K,
Ioku K. Influence of surface microstructure on the reaction of the
active ceramics in vivo. J Mater Sci Mater Med 1998;9:381–4.
[31] Toriumi DM, Kotler HS, Luxenberg DP, Holtrop ME, Wang EA.
Mandibular reconstruction with a recombinant bone-inducing factor.
Functional, histologic, and biomechanical evaluation. Arch Oto-
laryngol Head Neck Surg 1991;117:1101–12.
[32] Gao TJ, Tuominen TK, Lindholm TS, Kommonen B, Lindholm TC.
Morphological and biomechanical difference in healing in segmental
tibial defects implanted with Biocoral or tricalcium phosphate
cylinders. Biomaterials 1997;18:219–23.
[33] Boyne PJ. Application of bone morphogenetic proteins in the
treatment of clinical oral and maxillofacial osseous defects. J Bone
Joint Surg Am 2001;83A:S146–50.
[34] Hoshino M, Egi T, Terai H, Namikawa T, Takaoka K. Repair of
long intercalated rib defects using porous beta-tricalcium phosphate
cylinders containing recombinant human bone morphogenetic
protein-2 in dogs. Biomaterials 2006;27:4934–40.
[35] Johnson KD, Frierson KE, Keller TS, Cook C, Scheinberg R,
Zerwekh J, et al. Porous ceramics as bone graft substitutes in long
bone defects: a biomechanical, histological, and radiographic
analysis. J Orthop Res 1996;14:351–69.
[36] Urist MR. Bone: formation by autoinduction. Science 1965;150:
893–9.
[37] Rickard DJ, Sullivan TA, Shencker BJ, Leboy PS, Kazhdan I.
Induction of rapid osteoblast differentiation in rat bone marrow
stromal cell cultures by dexamethasone and BMP-2. Dev Biol 1994;
161:218–28.
[38] Harris SE, Sabatini MA, Harris MA, Feng JQ, Wozney J, Mundy
GR. Expression of bone morphogenetic protein messenger RNA in
prolonged cultures of fetal rat calvarial cells. J Bone Miner Res 1994;
9:389–94.
[39] Bi LX, Simmons DJ, Mainous E. Expression of BMP-2 by rat bone
marrow stromal cells in culture. Calcif Tissue Int 1999;64:63–8.
[40] Frank O, Heim M, Jakob M, Barbero A, Schafer D, Bendik I, et al.
Real-time quantitative RT-PCR analysis of human bone marrow
stromal cells during osteogenic differentiation in vitro. J Cell
Biochem 2002;85:737–46.
[41] Klein CP, de Groot K, Driessen AA, Ven der Lubbe HBM.
Interaction of biodegradable b-whitlockite with bone tissue: an in
vivo study. Biomaterials 1985;6:189–92.
[42] Handschel J, Wiesmann HP, Stratmann U, Kleinheinz J, Meyer U,
Joos U. TCP is hardly resorbed and not osteoconductive in a non-
loading calvarial model. Biomaterials 2002;23:1689–95.
[43] Hampson D. Facial injury: a review of biomechanical studies and test
procedures for facial injury assessment. J Biomech 1995;28:1–7.
[44] Enneking WF, Burchardt H, Puhl JJ, Piotrowski G. Physical and
biological aspects of repair in dog cortical-bone transplants. J Bone
Joint Surg Am 1975;57:237–52.




















