
Sonography of bone and bone-related diseases of the extremities
11
Pictorial Essay Sonography of Bone and Bone-Related Diseases of the Extremities Kil-Ho Cho, MD, 1 Young-Hwan Lee, MD, 2 Sung-Moon Lee, MD, 3 Muhammad Usman Shahid, MD, 1 Kyung Jin Suh, MD, 4 Joon Hyuk Choi, MD 5 1 Department of Diagnostic Radiology, College of Medicine, Yeungnam University, 317-1, Daemyung-Dong, Nam-Ku, Daegu, 705-717, Korea 2 Department of Diagnostic Radiology, College of Medicine, Daegu Catholic University, Daegu, Korea 3 Department of Diagnostic Radiology, College of Medicine, Keimyung University, Daegu, Korea 4 Soo & Joo MR Clinic, Daegu, Korea 5 Department of Anatomical Pathology, College of Medicine, Yeungnam University, Daegu, Korea Received 23 May 2003; accepted 29 July 2004 R adiography is the baseline modality in the evaluation of bone diseases, commonly fol- lowed by radioisotope scanning, CT, or MRI. Accelerated development of MRI and the initially low-resolution imaging capability of sonography may have resulted in the underutilization of sonog- raphy for bone diseases. 1 However, MRI itself does not have the fine resolution of plain radiog- raphy or CT to define cortical abnormalities of bone. The use of sonography for evaluation of the skeletal system has been hampered by the mis- conception that the lack of propagation of ultra- sound through the bone and small field-of-view images are insurmountable obstacles to evaluate the skeletal system, resulting in reduced use and a lack of literature on musculoskeletal sonography (MSUS). Nevertheless, the high reflectivity of sound at the bone–soft tissue interface and tomo- graphic nature of sonography make it ideal for eval- uation of bone contours. 2 High-resolution sonog- raphy can reveal subtle changes of the bone surface not detected on plain radiographs, such as tiny periosteal reactions and subperiosteal fluid collec- tions, and can differentiate soft tissue lesions from bone lesions (Figure 1). Using the extended-field-of-view function of MSUS, a large lesion can now be displayed on a single sonogram, 3–5 and the relationship of the lesion to adjacent anatomic structures can be depicted with osseous and articular landmarks, as is possible on radiographs. Recent technologic im- provements in ultrasound scanning and increased awareness of the advantages of sonography over other imaging modalities have led to a resurgence in interest. 6 Correlative imaging, however, remains mandatory to avoid errors in interpretation. TECHNICAL CONSIDERATIONS The operator must have sufficient knowledge of regional bone and soft tissue anatomy, including normal anatomic variants, and be familiar with specific sonography-related artifacts. In addition to MSUS findings, results from other imaging studies and laboratory tests should be considered in making the diagnosis. Crucial information can be obtained by history taking from the patients or their guardians, and by continued sonographic and physical examination. In general, high-frequency (10–15-MHz) linear- array transducers are the most appropriate choices for MSUS allowing detailed depiction of pertinent anatomic structures. Using a stand off pad or thick application of acoustic coupling gel on the skin is help- ful for evaluating very superficial bones. Low-fre- quency (3–5-MHz) curved-array transducers have an advantage when the lesion is deep-seated in large or muscular patients, but the resolution is inferior to that of high-frequency transducers, and the operator should identify the artifactual hypoechoic appearance of the bone surface on each side of the sector image. Correspondence to: K.-H. Cho Grant Sponsor: Yeungnam University Academic Fund J Clin Ultrasound 32:511–521, 2004; Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/jcu.20066 Ó 2004 Wiley Periodicals, Inc. VOL. 32, NO. 9, NOVEMBER/DECEMBER 2004 511
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Sonography of bone and bone-related diseases of the extremities
Pictorial Essay
Sonography of Bone and Bone-RelatedDiseases of the Extremities
Kil-Ho Cho, MD,1 Young-Hwan Lee, MD,2 Sung-Moon Lee, MD,3 Muhammad Usman Shahid, MD,1
Kyung Jin Suh, MD,4 Joon Hyuk Choi, MD5
1Department of Diagnostic Radiology, College of Medicine, Yeungnam University, 317-1, Daemyung-Dong,Nam-Ku, Daegu, 705-717, Korea2Department of Diagnostic Radiology, College of Medicine, Daegu Catholic University, Daegu, Korea3Department of Diagnostic Radiology, College of Medicine, Keimyung University, Daegu, Korea4 Soo & Joo MR Clinic, Daegu, Korea5Department of Anatomical Pathology, College of Medicine, Yeungnam University, Daegu, Korea
Received 23 May 2003; accepted 29 July 2004
Radiography is the baseline modality in theevaluation of bone diseases, commonly fol-
lowed by radioisotope scanning, CT, or MRI.Accelerated development of MRI and the initiallylow-resolution imaging capability of sonographymay have resulted in the underutilization of sonog-raphy for bone diseases.1 However, MRI itselfdoes not have the fine resolution of plain radiog-raphy or CT to define cortical abnormalities ofbone. The use of sonography for evaluation of theskeletal system has been hampered by the mis-conception that the lack of propagation of ultra-sound through the bone and small field-of-viewimages are insurmountable obstacles to evaluatethe skeletal system, resulting in reduced use and alack of literature on musculoskeletal sonography(MSUS). Nevertheless, the high reflectivity ofsound at the bone–soft tissue interface and tomo-graphic nature of sonographymake it ideal for eval-uation of bone contours.2 High-resolution sonog-raphy can reveal subtle changes of the bone surfacenot detected on plain radiographs, such as tinyperiosteal reactions and subperiosteal fluid collec-tions, and can differentiate soft tissue lesions frombone lesions (Figure 1).
Using the extended-field-of-view function ofMSUS, a large lesion can now be displayed on a
single sonogram,3–5 and the relationship of thelesion to adjacent anatomic structures can bedepicted with osseous and articular landmarks, asis possible on radiographs. Recent technologic im-provements in ultrasound scanning and increasedawareness of the advantages of sonography overother imaging modalities have led to a resurgencein interest.6 Correlative imaging, however, remainsmandatory to avoid errors in interpretation.
TECHNICAL CONSIDERATIONS
The operator must have sufficient knowledge ofregional bone and soft tissue anatomy, includingnormal anatomic variants, and be familiar withspecific sonography-related artifacts. In additionto MSUS findings, results from other imagingstudies and laboratory tests should be consideredin making the diagnosis. Crucial information canbe obtained by history taking from the patients ortheir guardians, and by continued sonographic andphysical examination.
In general, high-frequency (10–15-MHz) linear-array transducers are the most appropriate choicesfor MSUS allowing detailed depiction of pertinentanatomic structures. Using a stand off pad or thickapplicationofacoustic couplinggelontheskin ishelp-ful for evaluating very superficial bones. Low-fre-quency (3–5-MHz) curved-array transducers havean advantage when the lesion is deep-seated in largeormuscular patients, but the resolution is inferior tothat of high-frequency transducers, and the operatorshould identifytheartifactualhypoechoicappearanceof the bone surface on each side of the sector image.
Correspondence to: K.-H. Cho
Grant Sponsor: Yeungnam University Academic Fund
J Clin Ultrasound 32:511–521, 2004; Published online in Wiley
InterScience (www.interscience.wiley.com).DOI:10.1002/jcu.20066
� 2004 Wiley Periodicals, Inc.
VOL. 32, NO. 9, NOVEMBER/DECEMBER 2004 511

Scanning methods for bone are similar to theaccepted protocol for MSUS.5–9 Examiners surveythe symptomatic area first, and then compare it withthe contralateral and usually asymptomatic side,helpingdifferentiateabnormal fromnormal findings,avoiding diagnosis of normal variants as pathologicand occasionally revealing unsuspected abnormal-ities crucial for diagnosis (Figure 2). Color and powerDoppler sonography show the vascularity associatedwith pathologic conditions and the relationshipbetween lesions and adjacent neurovascular bundles.
NORMAL BONE
The normal periosteum, a dense, fibrous connectivetissue, is adherent to the surfaceof thebone, attachedby Sharpey’s fiber, and currently cannot be recog-nized as a separate structure sonographically. Thus,the term ‘‘bone surface’’ is applied to describe theregular hyperechoic line at the interface betweenthebone and soft tissues, producedby a strong reflec-tionof sounddue to themarkeddifference in acousticimpedance of the soft tissues and bone. The acousticshadow deep to the hyperechoic bone surface repre-sents the normal appearance of the bone. Reverbera-
tion artifacts projecting in the shadow beyond thebone can be seen onboth longitudinal and transversescans.1,2,7–9
There are some pitfalls in the interpretation of thesonographic appearance of the normal bone surface(Table 1). The growth plate in the immature skele-ton, the canals for perforating vessels or grooves fornutrient arteries, and accessory ossicles may appearas interruptions along the continuity of the bone sur-face, mimicking fractures (Figure 3). The fascialthickening of the normal myelotendinous attach-ment sites onto the bonemay also result in irregular-ity of the bone surface.2 Right-left side comparison ofpaired structures and supplementary dynamic eval-uation are very helpful MSUS maneuvers wheneverthere is doubt regarding the normal appearance.
PATHOLOGIC CONDITIONS OF THE BONE
Diseasedbonemaypresent, sooner or later, as a bonealteration, a consequential soft tissue change, orboth. MSUS can diagnose lesions directly by depict-ing bone surface changes,whether caused by bone orperiosseous soft tissue disease, and indirectly bydemonstrating soft tissue changes in the case of
FIGURE 1. Myositis ossificans in a 37-year-old woman after trauma
about 1 month previously. (A) Longitudinal sonogram of the anterior
aspect of the proximal thigh shows the irregular hyperechoic line
(arrows), with posterior acoustic shadowing in the muscle juxta-
cortically. On dynamic examination, the calcific shadow could be dif-
ferentiated from the cortical surface (arrowheads) of the femur, which
is visible deep to the calcific shadow. (B) Lateral radiograph of the right
thigh obtained 1 day before the sonographic examination shows no
abnormality. (C) Lateral radiograph obtained 10 days later shows the
multipennate calcific density (arrows) in the soft tissues.
CHO ET AL
512 JOURNAL OF CLINICAL ULTRASOUND

bone diseases that have an effect on the adjacent softtissues.6–10
Bone surface changes can be categorized sonogra-phically as follows: thinning or thickening of thehyperechoic line; interruption of the bone continu-ity, including a step-off deformity, expansion, orexcavation; periosteal reactions; and cortical dis-
ruption, with visualization of intraosseous compo-nents. It is important to interpret sonographicallydocumented abnormalities of the bone surface inthe context of findings on plain radiographs. Cur-rently, sonography is unable to depict intraosseouschanges unless the cortex is sufficiently thinned ordestroyed.
FIGURE 2. A 64-year-old womanwith pain in the left hip for 2 weeks. Anteroposterior radiographs of the right (A) and left (B) hips show the transverse
sclerosis (arrow, B) at the left femoral neck. Anterior longitudinal sonogramsof the right (C) and left (D) hips show the abrupt interruption (white arrow,
D) of the cortical continuity at the upper portion of the left femoral neck. The contralateral image (C) shows the normal bone surface, with continuity.
(E) Fat-suppressed T2-weighted coronal MR image shows the hypointense transverse fracture line (arrow) and bone marrow edema.
SONOGRAPHY OF EXTREMITY BONES
VOL. 32, NO. 9, NOVEMBER/DECEMBER 2004 513
Traumatic Lesions
MSUS is not the first-line imaging modality whenbone trauma is suspected. However, it is worthwhilefor detecting occult fractures that are not shownon radiographs,11–18 as it may avoid more costlyMRI.6,11 MSUS can detect rib fractures in 6 timesas many patients as radiography and will detect 10times more fractures overall.13 It can uncover frac-tures coincidentally, while being used to examinesoft tissue,14 and can be useful in further assessingfractures after initial radiography19 (Figure 4).Sonographically guided monitoring during closedreduction of fractures has reportedly yielded resultscomparable to those obtained using a conventionalradiographic technique.20,21
A fracture may be demonstrated sonograph-ically as an abrupt discontinuity of the bone sur-face, with or without a step-off deformity, anangular or buckle deformity of the cortex at thefracture site, hypoechoic subperiosteal blood col-
lection, and overlying soft tissue edema, with orwithout a soft tissue injury (Figure 2 and 3).
When pain, with or without swelling, is present innewborns and children after suspected bone traumaaround a joint, findings on physical examination areusually nonspecific and radiographs are commonlynondiagnostic because the nonossified epiphyses arenot visualized.6,17,18,22–24 In this situation, MSUSmay become a reliable substitute for the plain radio-graphs in selected cases,17,22 not only by visualizingthe unossified cartilaginous bone, but also by corre-lating the symptoms and physical signs with sono-graphic findings (Figure 5). Tenderness or painelicited from a suspected lesion as the transducerpasses over it is known as positive ‘‘sonographicpalpation.’’
Rotator cuff tears, arthritis, and rarely calcifictendinitis may cause periarticular bone erosion,which may reflect repetitive pressure, stress, ortraction force on the insertion site of tendons orlocal hyperemia due to inflammation.25–27 Thesebone changes sometimes may have an MSUSappearance similar to that of fractures. Becausea stress fracture may be chronic, a focally thickhyperechoic callus commonly overlies the corticalinterruption at the fracture site, a finding thatmay contribute to diagnosis in conjunction withthe findings on radiographs.
MSUS can be used to assess fracture healing in itsearly phase because radiographic findings are insuf-ficient. The initial hypoechoic appearance of thefracture is replaced by the image of a hyperechoiccallus bridging the fracture gap; this hyperechoicregion progressively increases in volume as the cal-lus matures and casts a greater posterior shadow.Serial correlation of histologic findings with
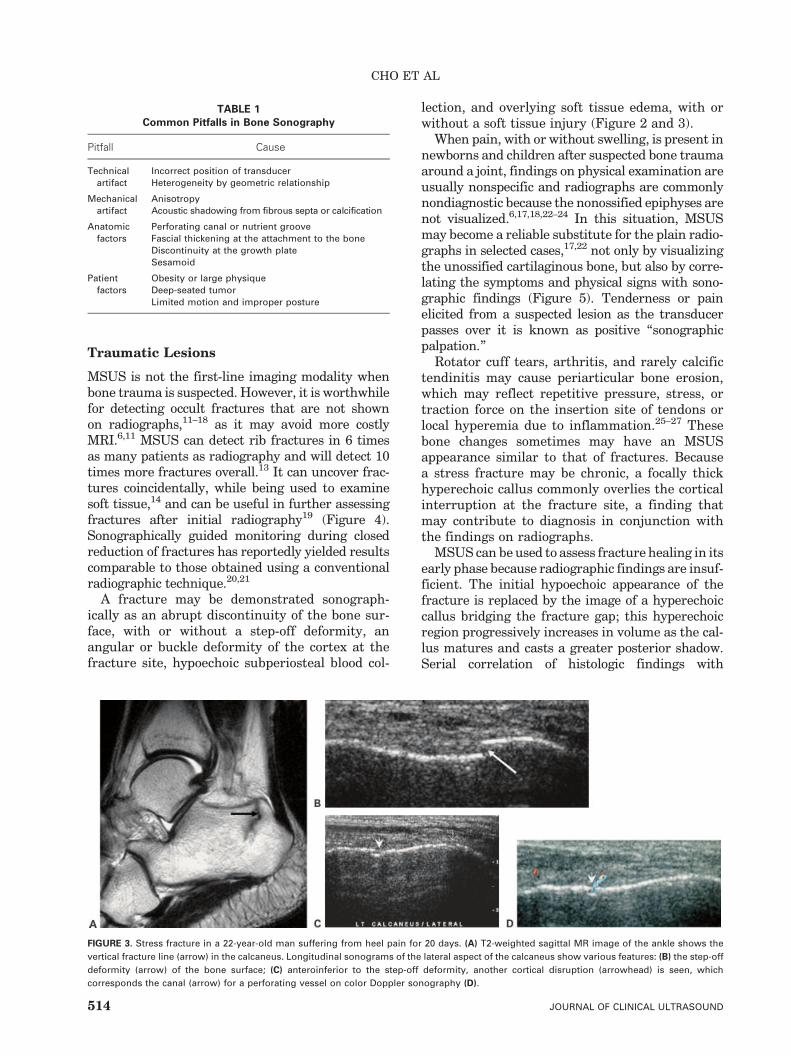
FIGURE 3. Stress fracture in a 22-year-old man suffering from heel pain for 20 days. (A) T2-weighted sagittal MR image of the ankle shows the
vertical fracture line (arrow) in the calcaneus. Longitudinal sonograms of the lateral aspect of the calcaneus show various features: (B) the step-off
deformity (arrow) of the bone surface; (C) anteroinferior to the step-off deformity, another cortical disruption (arrowhead) is seen, which
corresponds the canal (arrow) for a perforating vessel on color Doppler sonography (D).
TABLE 1
Common Pitfalls in Bone Sonography
Pitfall Cause
Technical
artifact
Incorrect position of transducer
Heterogeneity by geometric relationship
Mechanical
artifact
Anisotropy
Acoustic shadowing from fibrous septa or calcification
Anatomic
factors
Perforating canal or nutrient groove
Fascial thickening at the attachment to the bone
Discontinuity at the growth plate
Sesamoid
Patient
factors
Obesity or large physique
Deep-seated tumor
Limited motion and improper posture
CHO ET AL
514 JOURNAL OF CLINICAL ULTRASOUND

sonographic appearance in a healing fracture inhumanshasnotbeenpossiblebecause itwouldbeun-ethical to biopsy the fracture site in patients who donothave any complication.28 In canines, thepresenceof a hyperechoic appearance at a fracture site report-edly represents neo-osteogenesis histologically.29
On serialMSUS examinations, the normal healingprocess of a fracture goes through 5 stages: (1) initialsonolucency at the fracture gap; (2) progressiveincrease of dot-like hyperechoic foci at the fracturesite; (3) formationofapoorlydefinedechogenicbridgeacross the fracture site (probable primary callus); (4)prominence of a thin hyperechoic line at the super-ficialaspectof theprimarycallusalongthe longaxisofthe bone; and (5) development of a thick hyperechoicregular line continuouswith theadjacentnormal cor-tex (probable secondary callus). ColorDoppler sonog-raphy may demonstrate progressive formation ofnew vessels at the site of the developing callus untilabout 100 days after surgery, from which time flow
signals decrease and bone remodeling continues.2,30
The resistance index tends to decrease in the earlyweeksaftersurgeryandthenincreaseslightlyastibialfractures heal. In contrast, a lack of development offlowsignals andpersistence of ahighresistance indexis observedwhen fracture healing is delayed.
Osteochondral injury can be evaluated sonogra-phically by assessing the subchondral bone andoverlying cartilage simultaneously.31 However, theintra-articular deep portion is difficult to examine.
MSUS in Patients with Orthopedic MetallicImplants/Hardware
MSUS has potential value stemming from its abilitytodemonstratenewbone formationandmeasure thedistraction gap in patients who undergo Ilizarovlimb-lengthening procedures. MSUS can demon-
FIGURE 4. A 40-year-old man complaining of ankle pain for 6 months
after treatment of multiple fractures of the tibia and foot. Radio-
graphs of the ankle obtained over the previous 6 months (not shown)
were unremarkable. (A) Coronal T2-weighted MR image shows a
small amount of low-signal material (arrow) between the lateral
malleolus (L) and lateral aspect of the talus (T). (B) Sonogram obtained
along the intact anterior talofibular ligament (small arrows) shows
the curved echogenic line (thick arrow) with posterior shadowing.
This line was surgically confirmed to correspond to a bone fragment.
After surgical removal of the fragment, the ankle pain was relieved.
FIGURE 5. A 2-year-old girl refusing to use her right arm. (A) Oblique
radiograph of the right elbow shows the equivocal curvilinear dense
area (arrow) in the lateral condyle of the distal humerus. (B) Lateral
longitudinal sonogram of the right elbow shows the focal cortical
disruption (small arrow) at the distal end of the metaphysis, periosteal
elevation (arrowhead), and separation (large arrow) of the meta-
epiphyseal junction. (C) Contralateral asymptomatic left elbow shows
intact bone surface and the junction between the metaphysis (M) and
epiphysis (E) of the distal humerus.
SONOGRAPHY OF EXTREMITY BONES
VOL. 32, NO. 9, NOVEMBER/DECEMBER 2004 515
strate neo-osteogenesis several weeks before itbecomes evident on plain radiographs.32 Accuratemeasurement of neo-osteogenesis at the distractionsite is important to determine the appropriateadjustment rate of bone lengthening: Overly fastdistraction inhibits bone formation, and overly slowdistraction leads to premature consolidation. Sono-grams also can depict cyst formation at the distrac-tion site, enabling timely aspiration of persistentcysts (Figure 6).32–35However,MSUS isnot as usefulas radiography in detecting the angular deformity.34
Initially, an osteotomy site appears as a sonolucentarea.Hyperechoic foci representingneo-osteogenesisare visible as early as 4–14 days after corticotomy.New bone tissue, visualized as thin, echogenicstrands at the distraction gap, increases and showslongitudinal alignment in 14–28 days after surgery.
In3–6weeks, thedistractiongapbecomesmoreecho-genic, being filled with hyperechoic foci secondary tomineralization, but is still penetrable by ultrasound.At this time, plain radiographs may show an equivo-cal periosteal reaction.
Sonography can be a noninvasive predictor of‘‘boneregenerate strength’’ in theearly consolidationphase after cessation of lengthening, which mayreduce the need for repeat radiography.36 Fromboth ends of the corticotomy margins, there is pro-gressive bridging of the distraction gap. As the gap isfilled, it changes froman almost rectangular shape toa ‘‘V’’ shape.Theultrasound’s ability topenetrate thedistraction site is progressively limited by callus for-mation, and the signal is almost completely reflectedusually with in 5–9 weeks (mean, 7 weeks) aftersurgery,making sonographicmonitoring impossible.
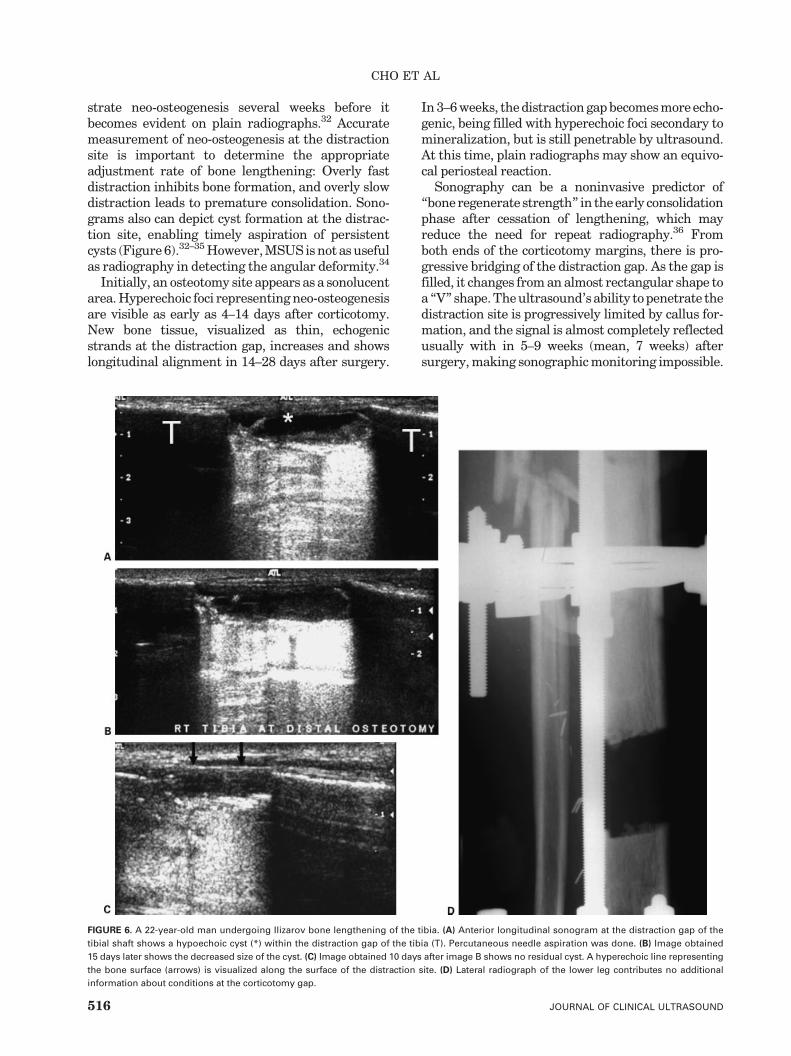
FIGURE 6. A 22-year-old man undergoing Ilizarov bone lengthening of the tibia. (A) Anterior longitudinal sonogram at the distraction gap of the
tibial shaft shows a hypoechoic cyst (*) within the distraction gap of the tibia (T). Percutaneous needle aspiration was done. (B) Image obtained
15 days later shows the decreased size of the cyst. (C) Image obtained 10 days after image B shows no residual cyst. A hyperechoic line representing
the bone surface (arrows) is visualized along the surface of the distraction site. (D) Lateral radiograph of the lower leg contributes no additional
information about conditions at the corticotomy gap.
CHO ET AL
516 JOURNAL OF CLINICAL ULTRASOUND
At this time, however, signs of mineralization at thedistraction gap become visible on radiographs.
Plain radiography is unsuitable for evaluation ofsoft tissue complications in patients with orthopedicmetallic implants because it cannot visualize thechanges in the soft tissues. CT and MRI are alsousually inadequate because of image degradationdue to artifacts from the metallic devices.37 MSUS,conversely, may visualize soft tissue complications,such as impingement by implants, cystic degenera-tion, hematoma formation, or infection after sur-gery, and often also provides information aboutosseous complications (Figure 7).37–39
Infection
MSUScan be used to diagnose acute osteomyelitis asearlyas24hours after theonset of fever, radiographyfindings become positive usually only after 7–10days. MSUS findings include deep soft tissue swel-ling adjacent to the bone, with a hypoechoic layerrepresenting pus collection beneath the periosteum,increasing the periosteal thickness beyond the nor-mal 2 mm. Serial scans show a progressive increaseof focal bone resorption. MSUS findings in acuteosteomyelitis represent a continuum of the evolvingpathologic processes, rather than discrete stages.Initially, the periosteummay be involved along only1 side of the bone. It is important, therefore, that theMSUS examination cover the entire bone circum-ference. The site of ‘‘point tenderness’’ often cor-responds to the site of the periosteal reaction.40
The subperiosteal anechoic or hypoechoic pus collec-tion is oftendifficult todifferentiate fromasubperios-teal fluid or blood collection, osteoid osteoma, and(rarely) tumor metastasis.40–43 If soft tissues areinterposed between the anechoic pus collectionand the bone surface, osteomyelitis is less likely.
Extensive abscess formation and multiple min-ute calcifications may be suggestive of tuberculousosteomyelitis,43 but not always. In chronic osteo-myelitis, MSUS can readily demonstrate inhomo-geneous cortical irregularity, abscess formation,and formation of a sinus fistula tract in the softtissues.2,7 However, it is not easy to determinewhether the bone infection is active or not, evenon MRI. Clinical and laboratory data, in conjunc-tion with radiographs or CT or MR images, maybe sufficient for diagnosis. If not, sonographicallyguided percutaneous needle aspiration or surgicalbiopsy is mandatory for definitive diagnosis.
Bone Neoplasms and Percutaneous NeedleBiopsy
The use of MSUS in diagnosing bone neoplasms isvery limited.However,MSUScanprovide important
information when the tumor metamorphoses at thebone surface, extends into soft tissue, or destroys orthins the cortex sufficiently for transmissionof sound
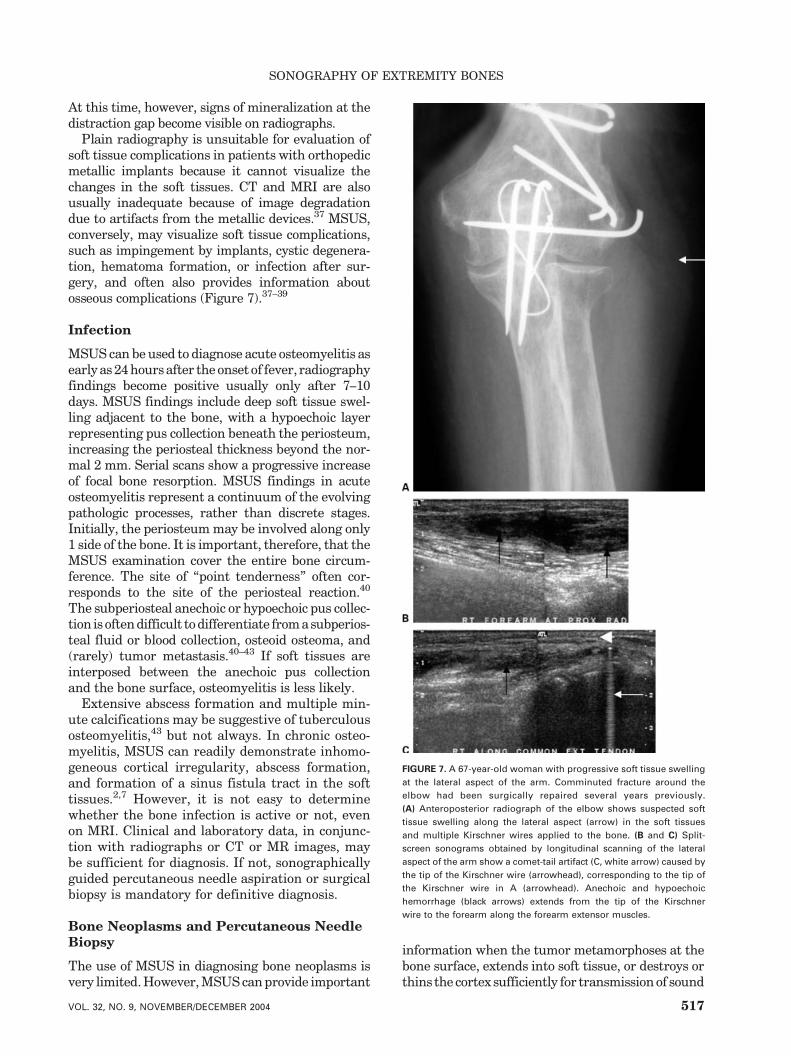
FIGURE 7. A 67-year-old woman with progressive soft tissue swelling
at the lateral aspect of the arm. Comminuted fracture around the
elbow had been surgically repaired several years previously.
(A) Anteroposterior radiograph of the elbow shows suspected soft
tissue swelling along the lateral aspect (arrow) in the soft tissues
and multiple Kirschner wires applied to the bone. (B and C) Split-
screen sonograms obtained by longitudinal scanning of the lateral
aspect of the arm show a comet-tail artifact (C, white arrow) caused by
the tip of the Kirschner wire (arrowhead), corresponding to the tip of
the Kirschner wire in A (arrowhead). Anechoic and hypoechoic
hemorrhage (black arrows) extends from the tip of the Kirschner
wire to the forearm along the forearm extensor muscles.
SONOGRAPHY OF EXTREMITY BONES
VOL. 32, NO. 9, NOVEMBER/DECEMBER 2004 517

waves.1,7–9,10,44 Aneurysmal bone cysts and giant celltumors of the bonemay create a bulge on the surfaceof the bone, with cortical thinning sufficient to allowbeam penetration; sonography would reveal a cyst-like appearance, with intraosseous fluid-fluid levelsand septa.1,44–46 Sonography is also valuable in eval-uating the cartilaginous cap of osteochondroma,47
which appears as a hypoechoic layer superficial tothe highly reflective bone surface, with outpouch-ings. When the cartilaginous cap is thinner than1 cm, the tumor is usually benign, whereas a capthicker than 2 cm generally indicates malignancy.An irregularly contoured cartilaginous cap thickerthan 1 cm is regarded as a sign of borderlinemalignancy. With MSUS, it is easy to differentiate areal osseous overgrowth from enlargement due tohemorrhage or tumors of the soft tissues or adventi-tial bursae between the bone and soft tissue.1
Osteoid osteoma of the long bone shaft is similarto osteomyelitis sonographically and clinically.MSUS may reveal a mild convex deformity of thebone surface, with spur-like irregularity and fluidcollection between the bone surface and soft tis-sue.48–50 In the case of intra-articular osteoidosteoma, the nidus of the tumor is often overlookedat radiography because of minimal or absent reac-tive sclerosis and the nonspecificity of the clinicalfeatures, resulting in a delay of diagnosis formonths
or even years. Color and power Doppler imagingmay help define the nidus of the tumor.49,50 Find-ings from sonography must be combined with thosefrom radiography and with the patient history fordiagnosis. In subperiosteal osteoid osteoma, thenidus appears as a small round area or cortical dis-continuity; however, the findings may be similar tothose in arthritic bone erosion, osteochondritis dis-secans, and intra-articular fracture. MSUS may beable to aid in diagnosis by visualizing subtle perios-teal reactions of early stage bone tumors, which arenot visualizable on radiographs (Figure 8).
Otherwise, MSUS is less useful than radiographyand MRI in diagnosing, differentiating benign frommalignant, and staging bone tumors.45–52 Sonog-raphy is of great value in not only guiding percu-taneous needle biopsy of bone tumors with anextraosseous component, but also localizing specificsites for surgical biopsy,1,7,12,45,53–59 providing a safeand reliable alternative to fluoroscopy and CT.55,58
Themain advantages of sonographically guided nee-dle biopsy of bone tumors are as follows: (1) contin-uous real-time tracing of the tip of the movingneedle allows the practitioner to avoid major neuro-vascular structures within the portal; (2) color andpower Doppler functions are helpful for identifyingregions of viable tissue; and (3) sonography allowssimultaneous needle placement, imaging, and tissue
FIGURE 8. A 12-year-old girl with osteosarcoma of the distal femur. (A) Anteroposterior radiograph of the distal femur shows sclerosis (*) in the
medial aspect of the distal metaphysis, but no periosteal abnormality is evident. Longitudinal sonograms along the medial (B) and lateral (C)
aspects of the distal femur show the fine sawtooth appearance of periosteal reaction (arrows) and the smooth adjacent normal bone surface
(arrowheads). The cortical space (curved arrow, C) is the growth plate of the distal femur.
CHO ET AL
518 JOURNAL OF CLINICAL ULTRASOUND

sampling, reducing time, cost, and patient manipu-lation.55 Percutaneous needle biopsy may representa viable alternative to surgical biopsy for the pri-mary histologic diagnosis of sarcoma and maybe sufficient for histologic subtyping in certaininstances.59 MSUS can be used to monitor fortumor recurrences by periodic re-examination ofresection sites, especially in patients with metallicimplants.37–39,53
Miscellaneous and Soft Tissue LesionsAffecting the Bone
Abnormalities of the bone and soft tissues, espe-cially in the articular and periarticular regions,may cause changes in the bone surface; these areseen in arthritides, intra-articular loose bodies,rotator cuff tears, habitual dislocation of theshoulder (eg, Hill-Sachs’ lesion of the shoulder),Osgood-Schlatter disease, and calcific tendini-tis.1,6–10,25–27,60 Surface contours of the bone mayin rare cases also be changed by bursitis, perioss-eous ganglia, myositis ossificans, giant cell tumorsof the tendon sheath, and various juxtacortical softtissue tumors. Therefore, bone abnormalities foundduring assessment of the soft tissues or joints, andvice versa, should be incorporated in differentialdiagnosis, as should information from radiographyand other imaging studies. So, for instance, in thosecases where myositis ossificans looks like a perios-teal reaction of the underlying bone (Figure 1),differentiation between the conditions is usuallypossible on dynamic MSUS examination.
In conclusion, high-frequency sonography, withits ‘‘low-power microscope–like’’ functionality, candemonstrate subtle cortical and juxtacortical ab-normalities related to bone disease. Sonographycan be employed as the principal imaging modal-ity in certain instances, although the potential ofMSUS with respect to bone tumors and purelyintraosseous lesions is still being investigated.The application of MSUS to bone diseases is likelyto be expanded as acceptance of and familiaritywith the technique grows.
Thus, MSUS might be routinely used to evaluatepatients with orthopedic hardware, trauma to thegrowing bone, surface cortical and juxtacorticalanatomy, and nonspecific pain in the case of normalor equivocal findings on radiography. MSUS mightalso be used to obtain information that supple-ments or complements that from other imagingstudies; to define the relationships between lesions,nerves, and vessels; and to guide percutaneous nee-dle aspiration procedures. As data accumulate, theapplication of sonography to bone diseases may
change themethodology used in the diagnostic imag-ing of skeletal pathologies.
ACKNOWLEDGMENT
We thank Dr. J. Antonio Bouffard for reviewingthis manuscript.
REFERENCES
1. Cho KH, Bouffard JA, Chhem RK, et al. Currentapplications of ultrasound to bone lesions in theextremities. J Korean Soc Med Ultrasound 1997;16:95.
2. van Holsbeeck MT, Introcaso JH. Sonography of thedermis, hypodermis, periosteum, and bone. In: vanHolsbeeckMT, Introcaso JH, editors.Musculoskeletalultrasound, 2nd edn. St. Louis: Mosby; 2001. p 325.
3. Barberie JE, Wong AD, Cooperberg PL, et al.Extended field-of-view sonography in musculoskel-etal disorders. AJR Am J Roentgenol 1998;171:751.
4. Lin J, Fessell DP, Jacobson JA, et al. An illustratedtutorial of musculoskeletal sonography: part 4,musculoskeletal masses, sonographically guidedinterventions, and miscellaneous topics. AJR Am JRoentgenol 2000;175:1711.
5. Lin J, Fessell DP, Jacobson JA, et al. An illustratedtutorial of musculoskeletal sonography: part 1,introduction and general principles. AJR AmJ Roentgenol 2000;175:637.
6. Roberts CS, Beck DJ Jr, Heinsen J, et al. Diagnosticultrasonography: applications in orthopaedic sur-gery. Clin Orthop 2002;401:248.
7. Chhem RK, Cardinal E, Cho KH: Skeletal and super-ficial soft tissue. In: McGahan JP, Goldberg BG,editors. Diagnostic ultrasound—a logical approach.Philadelphia: Lippincott-Raven; 1998. p 1115.
8. Adler RS. Bone and articular cartilage. In: FornageBD, editor. Musculoskeletal ultrasound. New York:Churchill Livingstone; 1995. p 59.
9. Chhem RK, Cardinal E, Ali SS, et al. Bone. In: Guide-lines and gamuts in musculoskeletal ultrasound.Chhem RK, Cardinal E, editors. New York: Wiley-Liss; 1999. p 281.
10. Steiner GM, Sprigg A. The value of ultrasound inthe assessment of bone. Br J Radiol 1992;65:589.
11. Wang CL, Shieh JY, Wang TG, et al. Sonographicdetection of occult fractures in the foot and ankle.J Clin Ultrasound 1999;27:421.
12. Graif M, Stahl-Kent V, Ben-Ami T, et al. Sono-graphic detection of occult bone fractures. PediatrRadiol 1988;18:383.
13. Griffith JF, Rainer TH, Ching ASC, et al. Sonographycompared with radiography in revealing acute ribfracture. AJR Am J Roentgenol 1999;173:1603.
14. Patten RM, Mack LA, Wang KY, et al. Nondisplacedfractures of the greater tuberosity of the humerus:sonographic detection. Radiology 1992;182:201.
15. Hauger O, Bonnefoy O, Moinard M, et al. Occultfractures of the waist of the scaphoid: early diagno-
SONOGRAPHY OF EXTREMITY BONES
VOL. 32, NO. 9, NOVEMBER/DECEMBER 2004 519

sis by high-spatial-resolution sonography. AJR AmJ Roentgenol 2002;178:1239.
16. Herneth AM, Siegmeth A, Bader TR, et al. Scaphoidfractures: evaluation with high-spatial-resolutionUS—initial result. Radiology 2001;220:231.
17. Kayser R, Mahlfeld K, Heyde C, et al. Ultra-sonographic imaging of fractures of the clavicle innewborn infants. J Bone Joint Surg [Br] 2003;85-B:115.
18. Riebel T, Nasir R. Ultrasound of extremity lesionscaused by birth trauma [in German]. UltraschallMed 1995;16:196.
19. Craig JG, Jacobson JA, Moed BR. Ultrasound offracture and bone healing. Radiol Clin North Am1999;37:737.
20. Durston W, Swartzentruber R. Ultrasound guidedreduction of pediatric forearm fractures in the ED.Am J Emerg Med 2000;18:72.
21. Chern TC, Jou IM, Lai KA, et al. Sonography formonitoring closed reduction of displaced extra-articular distal radial fractures. J Bone Joint Surg2002;84-A:194.
22. Hubner U, Schlicht W, Outzen S, et al. Ultrasoundin the diagnosis of fractures in children. J BoneJoint Surg [Br]. 2000;82-B:1170.
23. Markowitz RI, Davidson RS, Harty MP, et al. Sonog-raphy of the elbow in infants and children. AJRAm J Roentgenol 1992;159:829.
24. Davidson RS, Markowitz RI, Dormans J, et al.Ultrasonographic evaluation of the elbow in infantsand young children after suspected trauma. J BoneJoint Surg 1994;76-A:1804.
25. Wohlwend JR, van Holsbeeck M, Craig J, et al. Theassociation between irregular greater tuberositiesand rotator cuff tears: a sonographic study. AJRAm J Roentgenol 1998;171:229.
26. Hayes CW, Rosenthal DI, Plata MJ, et al. Calcifictendonitis in unusual sites associated with corticalbone erosion. AJR Am J Roentgenol 1987;149:967.
27. Wakefield RJ, Gibbon WW, Conaghan PG, et al.The value of sonography in the detection of boneerosions in patients with rheumatoid arthritis.Arthritis Rheum 2000;43:2762.
28. Maffulli N, Thorton A. Ultrasonic appearance ofexternal callus in long bone fracture. Injury 1995;20:5.
29. Moed BR, Kim EC, van Holsbeeck M, et al. Ultra-sound for the early diagnosis of tibial fracture heal-ing after static interlocked nailing without reaming:histologic correlation using a canine model. J OrthopTrauma 1998;12:200.
30. Caruso G, Lagalla R, Derchi L, et al. Monitoring offracture calluses with color Doppler sonography.J Clin Ultrasound 2000;28:20.
31. TakaharaM,Ogino T, TsuchidaH, et al. Sonographicassessment of osteochondritis dissecans of the hum-eral capitellum. AJR Am J Roentgenol 2000;174:411.
32. Young JW, Kostrubiak JS, Resnick CS, et al. Sono-graphic evaluation of bone production at the distrac-tion site in Ilizarov limb lengthening procedure. AJRAm J Roentgenol 1990;154:125.
33. Eyers KS, Bell MJ, Kanis JA. Methods of assessingnew bone formation during limb lengthening: ultra-sonography, dual energy X-ray absorptiometry andradiography compared. J Bone Joint Surg [Br] 1993;75-B:358.
34. Maffulli N, Hughes T, Fixsen JA. Ultrasonographicmonitoring of limb lengthening. J Bone Joint Surg(Br) 1992;74-B:130.
35. Derbyshire NDJ, Simpson AHRW. A role of ultra-sound in limb-lengthening. Br J Radiol 1992;65:576.
36. Bail HJ, Kolbeck S, Krummrey G, et al. Ultrasoundcan predict regenerate stiffness in distraction osteo-genesis. Clin Orthop 2002;404:362.
37. Gibbon WW, Long G, Barron DA, et al. Complica-tions of orthopedic implants: sonographic evalua-tion. J Clin Ultrasound 2002;30:288.
38. van Holsbeeck M, Eyler WR, Shennan LS, et al.Detection of infection in loosened hip prostheses:efficacy of sonography. AJR Am J Roentgenol 1994;163:381.
39. Gibbon WW, Richard J, Wakefield RJ. Ultrasound ininflammatory disease. Radiol Clin North Am 1999;34:633.
40. Mah ET, Lequesne GW, Gent RJ, et al. Ultrasoundfeatures of acute osteomyelitis in children. J BoneJoint Surg [Br] 1994;76-B:969.
41. Abiri M, Kirpekar M, Ablow RC. Osteomyelitis:detection with US. Radiology 1989;172:509.
42. Wright NB, Abbot GT, Carty HML. Ultrasoundin children with osteomyelitis. Clin Radiol 1995;50:623.
43. Park CM, Chung KB, Suh WH. Osteomyelitis:detection with US [letter]. Radiology 1991;178:890.
44. Mukuno DH, Lee TG, Watanbe AS, et al. Aneurys-mal bone cyst presenting as a pelvic mass on sono-graphic examination. J Ultrasound Med 1986;5:215.
45. Saifuddin A, Burnet SJD, Mitchell R. Ultrasonogra-phy of primary bone tumors. Clin Radiol 1998;53:239.
46. Arslan G, Karaali K, CubukM, et al. Giant cell tumorof the fourth metacarpal bone. J Clin Imaging 2000;24:139.
47. Malghem J, Vande Berg B, Noel H, et al. Benignosteochondromas and exostotic chondrosarcomas:evaluation of cartilage cap thickness by ultrasound.Skeletal Radiol 1992;21:33.
48. Malghem J, Vande Berg B, Clapuyt P, et al. Osteoidosteoma of the femoral neck: evaluation with US(letter). Radiology 1994;190:905.
49. Gil-Sanchez S, Marco-Domenech SF, Arenas J,et al. Doppler duplex color localization of osteoidosteomas. Skeletal Radiol 1999;28:107.
50. Ebrahim FS, Jacobson JA, Lin J, et al. Intraartic-ular osteoid osteoma: Sonographic findings in 3patients with radiographic, CT, and MR imagingcorrelation. AJR Am J Roentgenol 2001;177:1391.
51. Bodner G, Schocke MFH, Rachbauer F, et al. Dif-ferentiation of malignant and benign musculoskel-etal tumors: combined color and power Doppler USand spectral wave analysis. Radiology 2002;223:410.
52. Ng SY, Songra A, Ali N, et al. Ultrasound features ofosteosarcoma of the mandible—a first report. Oral
CHO ET AL
520 JOURNAL OF CLINICAL ULTRASOUND

Surg Oral Med Oral Pathol Oral Radiol Endod 2001;92:582.
53. Garant M, Sarazin L, Cho KH, et al. Soft tissuerecurrence of osteosarcoma: ultrasound findings.Can Assoc Radiol J 1995;46:305.
54. Civardi G, Livraghi T, Colombo P, et al. Lytic bonelesions suspected for metastasis: ultrasonicallyguided fine-needle aspiration biopsy. J Clin Ultra-sound 1994;22:307.
55. Saifuddin A, Mitchell R, Burnett SJD, et al.Ultrasound-guided needle biopsy of primarybone tumours. J Bone Joint Surg [Br] 2000;82-B:50.
56. Yeow KM, Tan CF, Chen JS, et al. Diagnostic sen-sitivity of ultrasound-guided needle biopsy in soft
tissue masses about superficial bone lesions. JUltrasound Med 2000;19:849.
57. Gil-Sanchez S, Marco-Domenech SF, Irurzun-Lopez J, et al. Ultrasound-guided skeletal biopsies.Skeletal Radiol 2001;30:615.
58. Torriani M, Etchebehere M, Amstalden EMI.Sonographically guided core needle biopsy of boneand soft tissue tumors. JUltrasoundMed2002;21:275.
59. Kilpatrick SE, Cappellari JO, Bos GD, et al. Is fine-needle aspiration biopsy a practical alternative toopen biopsy for the primary diagnosis of sarcoma?Experience with 140 patients. Am J Clin Pathol2001;115:59
60. Wang SC, Chhem RK, Cho KH, et al. Joint sonog-raphy. Radiol Clin North Am 1999;37:653.
SONOGRAPHY OF EXTREMITY BONES
VOL. 32, NO. 9, NOVEMBER/DECEMBER 2004 521




















