Sweat gland differentiation in mammary adenoid cystic carcinoma
Upload
khangminh22Category
view
3download
0
U L T R A S O U N DC L I N I C S
Ultrasound Clin 1 (2006) 15–24
15
Sonography of Benign RenalCystic DiseaseTherese M. Weber, MD
& Simple cortical cysts & Tuberous sclerosis
& Complex renal cysts& Renal sinus cysts& Medullary cystic disease& Multiple renal cysts& Autosomal dominant polycystic kidneydisease& Autosomal recessive polycystic kidney
disease& Von Hippel-Lindau disease
Department of Radiology, Wake Forest UniversityWinston-Salem, NC 27157-1088, USAE-mail address: [email protected]
1556-858X/06/$ – see front matter © 2005 Elsevier Inc. All rightsultrasound.theclinics.com
& Acquired cystic kidney disease associatedwith dialysis
& Multiloculated cystic renal masses& Multicystic dysplastic kidney& Multilocular cystic nephroma& Summary& Acknowledgments& References
When evaluating renal masses, differentiatingcysts from solid lesions is the primary role of ultra-sound (US). US is also helpful and frequentlysuperior to CT, in demonstrating the complex inter-nal architecture of cystic lesions in terms of in-ternal fluid content, septations, tiny nodules, andwall abnormalities, including associated soft tissuemasses. Renal cysts are common in the populationolder than 50 years, occurring in at least 50% ofpeople [1]. Scanning technique is important to thesuccess of demonstrating renal masses with US. Thekidneys should be evaluated in multiple patientpositions, including supine, lateral decubitus, andoccasionally oblique or prone positions. The massshould be scanned with an appropriate focal zone.Simple renal cysts will frequently be better demon-strated with tissue harmonic imaging, which caneliminate low-level internal echoes by reducingbackground noise [2]. The Bosniak ClassificationSystem of renal cysts, shown in Box 1, has becomean important tool used by radiologists and urolo-gists to communicate the significance of renal cystimaging characteristics [3,4]. The primary goal ofthe radiologist in evaluating cystic renal masses is
the differentiation of nonsurgical from surgical le-sions [5].
Simple cortical cysts
The sonographic criteria used to diagnose a simplecyst include the following characteristics: internallyanechoic, posterior acoustic enhancement, and asharply defined, imperceptible, smooth far wall.Simple cysts are usually round or ovoid in shape.If all these sonographic criteria are met, furtherevaluation or follow-up is not required. Maintain-ing rigid criteria is necessary to ensure the highestpossible accuracy with US [6]. The simple renal cystis a Bosniak category I cyst [Fig. 1] [3].
Complex renal cysts
Complex cysts do not meet the strict US criteria of asimple renal cyst. Five to ten percent of all renalcysts are not simple cysts, and 5% to 10% of renalcysts with complex features prove to be tumors [7].These complex renal cysts may contain complexfluid, septations, calcification, perceptible defined
School of Medicine, Medical Center Boulevard,
reserved. doi:10.1016/j.cult.2005.09.005

Box 1: Bosniak classification of renal cysticdisease
Category I
Simple benign cyst by imaging criteria
Category II
Cystic lesions characterized by:
• One or two thin (≤ 1 mm thick) septations orthin, fine calcification in the wall or septa
• Hyperdence, homogeneous benign cysts• Diameter of 3 cm or less• One quarter of its wall extending outside
the kidney so the wall can be assessed• No contrast enhancement
Category IIF
Cystic lesions that are minimally complicatedthat need follow-up. Some suspicious featuresin these lesions need follow-up to detect anychange in character.
Category III
True indeterminate cystic masses that needsurgical evaluation, although many prove to bebenign, characterized by:
• Uniform wall thickening or nodularity• Thick or irregular peripheral calcification• Multilocular nature with multiple enhancing
septa• Hyperdense lesions that do not meet cate-
gory II criteria
Category IV
Lesions with findings that are clearly malig-nant, including:
• Nonuniform or enhancing thick wall• Enhancing or large nodules in the wall• Clearly solid components in the cystic lesions• Irregular margins
16 Weber
wall, or mural nodularity. Bosniak category II cystsare minimally complicated cysts that may containseptations or thin calcification, and include in-fected cysts and high-density cysts seen on non-contrast CT examination. High-density cysts aredefined as having a density greater than 20 Houns-field units (HU) on noncontrast CT. US may con-firm the cystic nature in 50% of these lesions,especially if larger in size (1.5–3.0 cm). Equivocalcases can be placed in category IIF, created forminimally complicated cysts that require follow-up. Size criterion of 3 cm differentiates between IIand IIF lesions. These cysts need at least 6-monthfollow-up and are most likely benign but some-what suspicious [8]. Many of these cysts, depending
on the degree of abnormality, will require furtherimaging with MR or CT.Internal echoes within a renal cyst may be caused
by a complicating hemorrhage or infection. In-fected cysts on US usually have a thickened walland may exhibit a debris-fluid or gas-fluid level.Aspiration and drainage may be required for diag-nosis and treatment. Hemorrhagic cysts can usuallybe followed with serial US examination if thereis no evidence of malignancy at MR or CT evalua-tion. Septations within a cyst may occur followinghemorrhage, infection, or percutaneous aspiration[Fig. 2]. Two adjacent cysts may share a commonwall and mimic a large septated cyst. There may bea small amount of renal parenchyma between twoadjacent cysts, suggesting a thick septation. If septaare “paper” thin (≤1 mm), smooth, and attached tothe cyst wall without focal thickening or nodularity,a benign cyst can be diagnosed [3,8]. Fewer thanfive septations should be present in a benign cyst. Ifthe cystic lesion shows septal irregularity, septalthickness greater than 1 mm, thick calcifications,or solid elements at the wall attachment, the lesionmust be presumed malignant and requires furtherevaluation with MR or CT.Calcifications in renal cysts may be fine and
linear, or amorphous and thick. The presenceof a small amount of calcium or thin, fine areasof calcification in the wall or a septation, with-out an associated soft tissue nodule, likely repre-sents a complicated cyst rather than malignancy.Thick, irregular, amorphous calcification had beenthought to be more concerning for malignancy;however, a recent report demonstrates that calcifi-cation in a cystic renal mass is not as important inthe diagnosis as the presence of enhancing soft-tissue elements [9]. Renal cysts with milk-of-calcium will show layering, echogenic, dependentmaterial that may be mobile. These cysts are alwaysbenign. At real-time US, bright echogenic foci withringdown may be seen on septa and in the cystwalls; however, calcification may not be of suffi-cient density to be identified on CT examination.Bosniak category III lesions are moderately com-
plicated cysts that have more numerous or thick-ened septae; a thickened wall; thicker, irregularcalcification; or multiloculated features. Benignand malignant tumors may be classified as Bosniakcategory III lesions. Because most category III le-sions will be malignant [10], all category III lesionsrequire surgical resection or biopsy. Benign lesionsin this category include the multilocular cysticnephroma; complex septated and multiloculatedcysts; densely calcified cysts; a complex abscess; aninfected cyst; vascular malformation; xanthogranu-lomatous pyelonephritis (XGP); or echinococcosis.Malignant lesions in this category include cystic

Fig. 1. Simple cyst in the lower renal pole in longitudinal (A) and transverse (B) planes demonstrating characteristicsonographic findings.
17Sonography of Benign Renal Cystic Disease
Wilms’ tumor in a child and cystic adenocarcinomain an adult. Bosniak category IV lesions are cystic ornecrotic carcinomas that may have solid elements,irregular margins, and enhancement demonstratedon CT, MRI, or US with contrast imaging. Theselesions are unequivocally malignant and requiretreatment. Renal cystic lesions with perceptible,defined, thickened wall; thick septae; mural nodu-larity; intracystic soft tissue mass; or abnormal cal-cifications on US are concerning for malignancy.
Renal sinus cysts
Renal sinus cysts (RSCs) are common and havebeen described as peripelvic cysts, parapelvic lym-phatic cysts, parapelvic lymphangiectasia, and para-pelvic cysts [11]. RSCs are likely lymphatic in originor develop from embryologic rests. These cysts donot communicate with the collecting system [12].Most RSCs are asymptomatic, but they may becomeinfected or bleed, and may cause hematuria, hyper-tension, or hydronephrosis [13]. There are two dis-tinct patterns of cyst formation in the renal sinus
Fig. 2. (A) Mildly complicated renal cyst with thin septationseptation is frequently seen at real-time sonography.
that include multiple, small, confluent cysts versusa single, larger cyst that probably arises from theadjacent parenchyma [11]. On US, these are simplecysts located in the medullary or renal sinus areaof the kidney. Multiple renal sinus cysts mimichydronephrosis on US and noncontrasted CT.If communication with the collecting system can-not be demonstrated with US to confirm hydro-nephrosis, additional studies such as intravenouspyelogram, contrasted CT, or MR examinationmay be needed.
Medullary cystic disease
Medullary cystic disease is a group of similar dis-eases that occur as a result of progressive renaltubular atrophy with secondary glomerular scle-rosis and medullary cystic formation [14,15].Medullary cystic disease is an important cause ofend-stage renal disease (ESRD) in children, ac-counting for 10% to 25% of the cases of ESRD.Two distinct presentations occur. The childhoodform, which is most common, is inherited as an
(white arrow). (B) Artifact (white arrowheads) from the

18 Weber
autosomal recessive disorder. There is an associa-tion with extrarenal, ophthalmologic abnormali-ties. The adult form, inherited as an autosomaldominant pattern, tends to present in early adult-hood and is not associated with extrarenal abnor-malities. US findings include kidneys that are smallto normal in size, are hyperechoic, and have small(0.1 to 1.0 cm) cysts in the medulla and at thecorticomedullary junction [16,17]. Acquired cystickidney disease may resemble medullary cystic dis-ease; however, cyst location in the cortex and a his-tory of dialysis supports the diagnosis of acquiredcystic kidney disease.
Multiple renal cysts
With increased use of CT, US, and MR, patientswho are harboring multiple simple cysts or lesionstoo small to characterize are being seen with in-creasing frequency. Multiple renal cysts can be seenin polycystic kidney disease, Von Hippel-Lindaudisease (VHL), tuberous sclerosis (TS), acquiredcystic kidney disease associated with dialysis(ACKDD), and mulitcystic dysplastic kidney.
Autosomal dominant polycystic kidneydisease
Autosomal dominant polycystic kidney disease(ADPKD) is the third most common systemic he-reditary condition and accounts for 10% to 15%of all patients on dialysis [18]. Because the diseaseis characterized by variable expression and occurswith spontaneous mutation, up to 50% of patientswill have no family history of the disease [19].Renal failure develops in 50% of patients and isusually present by 60 years of age. Early signs ofthe disease include hypertension and flank or backpain with variable progression to ESRD. Nephro-lithiasis occurs in 20% to 36% of patients because
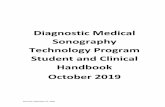
Fig. 3. Bilaterally enlarged kidneys (A, B) with multiple cystkidneys measure 15.6 cm in length bilaterally.
of metabolic (lower glomerular filtration rate andurine volume) and anatomic (associated with largerand more numerous renal cysts) factors [20]. Extra-renal manifestations of ADPKD include hepatic,pancreatic, ovarian, splenic, arachnoid, and othercysts, and intracranial berry aneurysms with asso-ciated intracranial hemorrhage, abdominal aorticaneurysm, cardiac valve abnormalities, and her-nias. The vascular abnormalities and cyst develop-ment are related to a basement membrane defect[18]. Eighty percent of people who have ADPKDand ESRD will have colonic diverticulosis. At leasttwo different genes involving chromosomes 4and 16 have been found to be associated withADPKD [21].US, because of high sensitivity and low cost, has
become the primary method of diagnosing ADPKDand following the cysts. US screening for ADPKDtypically begins between ages 10 and 15 years, buthas the problem of false negatives in about 14% ofpatients younger than 30 years. Bear and colleagues[22] developed criteria that are widely used to diag-nose ADPKD. In adults who have a family historyof ADPKD, the presence of at least three cysts inboth kidneys, with at least one cyst in each kidney,is a positive finding [23]. The cysts tend to involveall portions of the kidney and are of variable size.US typically reveals kidneys that are bilaterallyenlarged with compression of the central sinusecho complex [Fig. 3]. When the kidneys are mark-edly enlarged with multiple complex cysts, de-tection of solid lesions may be difficult, andcorrelation with MR may be necessary to evalu-ate for renal cell carcinoma (RCC). When a solidmass is seen it can be confirmed with confidencesonographically [Fig. 4]. Nephrolithiasis may bedifficult to demonstrate sonographically becauseof distortion of the collecting system by numerouslarge cysts. There is no increased risk for RCC inpatients who have ADPKD, except for increased risk
s of various sizes in adult polycystic kidney disease. The

Fig. 4. (A) Adult polycystic kidney disease with (B) solid renal masses (white arrows) in the right kidney confirmedas papillary renal cell carcinoma following nephrectomy.
19Sonography of Benign Renal Cystic Disease
related to dialysis and the generally increased riskfor RCC in men.
Autosomal recessive polycystic kidneydisease
Autosomal recessive polycystic kidney disease(ARPKD) is characterized by varying degrees ofrenal failure and portal hypertension as a resultof dilatation of renal collecting tubules, dilatationof biliary radicals, and periportal fibrosis that influ-ences its presentation. The involved gene is locatedon chromosome 6 [24]. In its severest form, renaldisease predominates and ARPKD manifests itselfimmediately after birth with the early complicationof severe pulmonary failure. The diagnosis may bemade at fetal or neonatal US. Characteristically, thekidneys are enlarged bilaterally, and oligohydram-nios, Potter’s facies, and pulmonary complicationsmay be encountered. Children who present laterwill have some element of renal impairment withthe complications of congenital hepatic fibrosis,including portal hypertension, splenomegaly, andbleeding varices [25]. With US, the kidneys main-tain a reniform shape, but may be normal to bilat-erally enlarged and echogenic [Fig. 5].
Fig. 5. Newborn who has bilaterally enlarged, echogen(A) measures 10 cm in length and the left kidney (B) meas
Von Hippel-Lindau disease
VHL disease is an uncommon condition character-ized by multiple lesions, including hemangioblas-tomas in the central nervous system (CNS) andretina; RCC; pheochromocytomas; pancreatic neu-roendocrine tumors; epididymal cystadenomas; en-dolymphatic sac tumors; carcinoid tumors; andmultiple cysts of the kidney, pancreas, and epididy-mis. The condition is inherited in an autosomaldominant pattern [26]. The VHL tumor suppressorgene is located on chromosome 3 [27]. Inactivationof the VHL suppressor gene gives rise to premalig-nant renal cysts. Additional genetic alterations areprobably required for conversion of these cysts toRCC. Renal involvement in VHL includes multiple,bilateral renal cysts and solid tumors. RCC, one ofthe major complications of VHL disease, occurs inup to 75% of patients by the age of 60 and occurs25 years earlier than sporadic RCC [28]. In additionto the development of RCC at a younger age, thesetumors tend to be bilateral and multicentric. Cysts,as the most common renal manifestation of thedisease, are seen in 75% of patients. Although mul-tiple, these cysts are generally fewer than in patientswho have ADPKD. In ADPKD, pancreatic cysts almost
ic kidneys consistent with ARPKD. The right kidneyures 9.8 cm in length.

20 Weber
never occur in the absence of liver cysts, whereas inVHL they are common. On US the cysts tend to becortical in location and range in size from 0.5 to3.0 cm. RCC in VHL disease may show solid renalmasses without cystic components or predomi-nantly cystic lesions with enhancing solid compo-nents that contain the RCC. US may be used forscreening these patients, especially those youngerthan 18 years; however, CT and MR are more sensi-tive in detecting small enhancing solid masses [18].
Tuberous sclerosis
TS is a neurophakomatosis involving the skin andCNS that most commonly occurs sporadically in60% of patients. This condition is also inherited asan autosomal dominant pattern and is character-ized by hamartomatous growths in the CNS, eyes,skin, heart, liver, kidney, and adrenal glands. Themajor presenting symptom is seizures. CNS mani-festations occur in up to 90% of patients. Theclassic clinical triad is mental retardation, seizures,and adenoma sebaceum. At least two genetic locihave been associated with TS, involving chromo-some 9 and 16 [18]. The leading causes of death inTS are renal failure, cardiac tumors, increased intra-cranial pressure, and bleeding [29]. Renal manifes-tations occur in about half of patients who haveTS and include cysts, angiomyolipomas (AML), tu-mors, and perirenal lymphangiomas. There is anincreased incidence of clear cell carcinomas in pa-tients who have TS, especially women. RCC occursbilaterally in 43% of affected TS patients, andtumors occur at a younger age than sporadic RCC[18,30,31]. The risk for malignancy is lower in TSthan in VHL disease [18]. On US, renal cysts areseen in the cortex and medulla [Fig. 6]. The renalcysts in TS appear at an earlier age than the cystsseen in APKD. Renal cysts are not the primarydiagnostic feature of TS, however. Multiple renalAML are a primary diagnostic feature of TS, occurin about 15% of patients who have TS, and aremore common in women. The rate of hemorrhagein TS-related AML is higher than in sporadic AML[32]. If TS is a consideration, the diagnosis canusually be confirmed on CNS imaging with sub-ependymal hamartomas or giant cell astrocytomas.
Acquired cystic kidney disease associatedwith dialysis
Acquired cystic kidney disease consists of renal cystsfound in individuals who have chronic renal failurewho may have a history of dialysis, but do not havea history of hereditary cystic renal disease. Dunnilland colleagues [33] first described this process in1977. The most important factor in developing
ACKDD is the duration of ESRD or maintenancedialysis [34]. ACKDD is seen in 8% to 13% ofpatients who have ESRD, 10% to 20% of patientswho have a 1- to 3-year history of dialysis, 40% to60% of patients who have history of 3 to 5 years ofdialysis, and greater than 90% of patients who havea history of 5 to 10 years of dialysis. Cysts occurwith equal frequency in patients receiving perito-neal or hemodialysis. The cysts are of tubular origin(arising from the proximal tubules), thought to becaused by nondialyzable mitogenic or cytogenicsubstances; tubular obstruction from fibrosis oroxalate crystals; and ischemia. There is a histologiccontinuum from cysts with single-layered epitheliato multilayered (atypical) cysts to renal adenomaand RCC. RCC occurs in a younger population inACKDD patients compared with sporadic RCC,with a mean age at diagnosis of about 49 years ascompared with 62 years for patients who do nothave ESRD [35]. RCC in patients undergoing dialy-sis is seven times more common in men thanwomen, in contrast to the 2/1 ratio in patientswho do not have ESRD [36]. Criteria used to defineACKDD include the presence of three to five cysts ineach kidney in a patient who has chronic renalfailure, which are not related to inherited renalcystic disease. On US, multiple bilateral renal cystsinvolving the cortex and medulla are seen in thesetting of medical renal disease [Fig. 7]. The cystsare usually small, many measuring 0.5 cm or less.Confirmation of the simple cystic nature may bedifficult because of the small size [37]. The cystsmay increase in size and number with time, and theoverall size of the kidneys may increase. This appear-ancemay resemble ADPKD.Complications associatedwith ACKDD include cyst infection or hemorrhage,renal calculi, erythocytosis, and solid neoplasms.
Multiloculated cystic renal masses
A multiloculated appearance can be seen in neoplas-tic disease such as renal cell carcinoma, multilocularcystic nephroma, Wilms’ tumor, and solid tumorswith central necrosis, which are Bosniak category IIIlesions. Multiloculated renal masses can be seen inrenal cystic disease such as localized renal cysticdisease, septated cyst, and segmental multicystic dys-plastic kidney. Inflammatory disease such as echino-coccosis, segmental XGP, and abscess can appear asa multiloculated cystic renal mass. An organizinghematoma and vascular malformation can alsoappear as a multiloculated cystic renal mass.
Multicystic dysplastic kidney
The pathogenesis of multicystic dysplastic kidney(MCDK) is complete ureteral obstruction early in

Fig. 6. Ten-year-old who has bilateral enlarged kidneys with multiple simple renal cysts on US (A, B) and CT (C ).The right kidney measures 11 cm in length and the left kidney measures 11.5 cm in length. MR of the braindemonstrated multiple subependymal nodules protruding into the lateral ventricle on axial (D) and coronal(E ) T2-weighted images.
21Sonography of Benign Renal Cystic Disease
fetal life before the eighth to tenth week, or incom-plete ureteral obstruction occurring later in fetal lifebetween the 10th and 36th week. Contralateralrenal anomalies, most commonly uretero pelvicjunction (UPJ) obstruction, occur in 33% of patients.
Imaging characteristics vary depending on age ofthe patient at diagnosis. Fetal US may show largecysts with no intercommunication between cysts,absence of identifiable cortical parenchyma, or cen-tral sinus structures [Fig. 8]. TheMCDKmay calcify or

Fig. 7. Longitudinal US images of the right (A) and left (B) kidneys and noncontrast CT (C ) demonstrate markedincreased cortical echogenicity and loss of cortical-medullary distinction in this patient who has ESRD and multiplebilateral simple renal cysts consistent with acquired renal cystic disease.
22 Weber
may not be identifiable in a few patients who havebeen followed [38].
Multilocular cystic nephroma
Multilocular cystic nephroma (MLCM) is a benign,nonhereditary cystic neoplasm with a bimodal pre-
Fig. 8. Longitudinal (A) and transverse (B) images of the kcentral sinus structures and no identifiable cortical pare
sentation that has greater incidence in males youngerthan 2 years and in women during the fifth toeighth decades. MLCN consists of multiple epithe-lially lined cysts that do not communicate. MLCNis usually a benign neoplasm; however, metastaseshave been reported [5,39]. US will show a masscontaining multiple cysts or internal septations
idney show multiple large renal cysts with absence ofnchyma consistent with multicystic dysplastic kidney.

Fig. 9. Longitudinal US (A) and CT (B) images demonstrating a predominantly cystic mass with multiple internalseptations, proven at surgery to be a multilocular cystic nephroma. Note the better representation of the lesion'sinternal architecture at US.
23Sonography of Benign Renal Cystic Disease
[Fig. 9]. It is not possible to conclusively distin-guish MLCN from multiloculated RCC radiolo-graphically, and these are usually surgical lesions.
Summary
US plays an important role in evaluation of thekidney in cases of medical renal disease becauseof lower cost, ready availability, lack of radiation,and lack of need for iodinated contrast material.The primary role of US in evaluating benign cysticrenal disease is the distinction of a simple cyst froma solid mass, and in defining the characteristics of acomplex cyst.
Acknowledgments
The author would like to acknowledge Raymond B.Dyer, MD, for his editorial assistance.
References
[1] Kissane JM. Congenital malformations. In: He-pinstall RH, editor. Pathology of the kidney.Boston: Little, Brown; 1973. p. 69–119.
[2] Schmidt T, Holh C, Haage P, et al. Diagnosticaccuracy of phase-inversion tissue harmonicimaging versus fundamental B-mode sonographyin the evaluation of focal lesions of the kidney.AJR Am J Roentgenol 2003;180:1639–47.
[3] Bosniak MA. The current radiological approachto renal cysts. Radiology 1986;158:1–10.
[4] Leder RA. Radiological approach to renal cystsand the Bosniak classification system. Curr OpinUrol 1999;9(2):129–33.
[5] Hartman DS, Choyke PL, Hartman MS. Apractical approach to the cystic renal mass.Radiographics 2004;24:S101–15.
[6] Bosniak MA. The small (< 3 cm) renal parenchy-mal tumor: detection, diagnosis, and controver-sies. Radiology 1991;179:307–17.
[7] Zeman RK, Cronan JJ, Rosenfield AT, et al. Imag-ing approach to the suspected renal mass. RadiolClin North Am 1985;23(3):503–29.
[8] Israel GM, Bosniak MA. Follow-up CT ofmoderately complex cystic lesions of the kidney(Bosniak category IIF). AJR Am J Roentgenol2003;181:627–33.
[9] Israel GM, Bosniak MA. Calcification in cysticrenal masses: is it important in diagnosis?Radiology 2003;226:47–52.
[10] Harisingani MG, Maher MM, Gervais DA, et al.Incidence of malignancy in complex cystic renalmasses (Bosniak category III): should imaging-guided biopsy precede surgery? AJR Am JRoentgenol 2003;180:755–8.
[11] Rha SE, Byun JY, Jung SE, et al. The renal sinus:pathologic spectrum and multimodality imagingapproach. Radiographics 2004;24:S117–31.
[12] Hidalgo H, Dunnick NR, Rosenburg ER, et al.Parapelvic cysts: appearance on CT and sonog-raphy. AJR Am J Roentgenol 1982;138:667–71.
[13] Chan JCM, Kodroff MB. Hypertension andhematuria secondary to parapelvic cyst. Pedi-atrics 1980;65:821–3.
[14] Gardner KD. Juvenile nephronophthiasis andrenal medullary cystic disease. In: Gardner KD,editor. Cystic disease of the kidney. New York:John Wiley & Sons; 1976. p. 173–85.
[15] Wise SW, Hartman DS. Medullary cystic diseaseof the kidney. In: Pollack HM, McClennan BL,editors. Clinical urography: an atlas and textbookof urologic imaging. 2nd edition. Philadelphia:W.B. Saunders Company; 2000. p. 1398–403.
[16] Resnick JS, Hartman DS. Medullary cystic diseaseof the kidney. In: Polack HM, editor. Clinicalurology: an atlas and textbook of urologicimaging. Philadelphia: W.B. Saunders Company;1990. p. 1178–84.
[17] Rego JD, Laing FG, Jeffrey RB. Ultrasonicdiagnosis of medullary cystic disease. J Ultra-sound Med 1983;2:433–6.
[18] Choyke PL. Inherited cystic diseases of the kid-ney. Radiol Clin North Am 1996;34(5):925–46.
[19] Dalgaard OZ. Bilateral polycystic disease of the

24 Weber
kidney: A follow-up of 284 patients and theirfamilies. Acta Med Scand 1957;157(S328):1–255.
[20] Grampsas SA, Chandhoke PS, Fan J, et al.Anatomic and metabolic risk factors for nephro-lithiasis in patients with autosomal dominantpolycystic kidney disease. Am J Kidney Dis 2000;36(1):53–7.
[21] Fick GM, Gabow PA. Natural history of auto-somal dominant polycystic kidney disease. AnnuRev Med 1994;45:23–9.
[22] Bear JC, McManamon P, Morgan J, et al. Age atclinical onset and at ultrasound detection ofadult polycystic kidney disease. Data for geneticcounseling. Am J Med Genet 1984;18:45–53.
[23] Parfrey PS, Bear JC, Morgan J, et al. The diagnosisand prognosis of autosomal dominant polycystickidney disease. N Engl J Med 1990;323:1085–90.
[24] Dimitrakov JD, Dimitrakov DI. Autosomal re-cessive polycystic kidney disease. Clinical andgenetic profile. Folia Med (Plovdiv) 2003;45:5–7.
[25] Harris PC, Rosetti S. Molecular genetics ofautosomal recessive polycystic kidney disease.Mol Genet Metab 2004;81:75–85.
[26] Sano T, Horiguchi H. Von Hippel-Lindau dis-ease. Microsc Res Tech 2003;60:159–64.
[27] Kaelin Jr WG. The von Hippel-Lindau tumorsuppressor gene and kidney cancer. Clin CancerRes 2004;10:6290S–5S.
[28] Richard S, David P, Marsot-Dupuch K, et al.Central nervous system hemangioblastomas,endolymphatic sac tumors, and von Hippel-Lindau disease. Neurosurg Rev 2000;23:1–22.
[29] Gomez MR. Tuberous sclerosis. New York: RavenPress; 1988.
[30] Torres VE. Systemic manifestations of renal cysticdisease. In: Gardner KD, Bernstein J, editors. Thecystic kidney. Dordrecht (The Netherlands):Kluwer Academic Publishers; 1990. p. 207.
[31] Zimmerhackl LB, Rehm M, Kaufmehl K, et al.Renal involvement in tuberous sclerosis com-plex: a retrospective survey. Pediatr Nephrol1994;8:451–7.
[32] Hildebrandt F. Genetic renal disease in children.Curr Opin Pediatr 1995;7:182–91.
[33] Dunnill MS, Millard PR, Oliver D. Acquiredcystic kidney disease of the kidneys: a hazard oflong-term intermittent maintenance haemodialy-sis. J Clin Pathol 1977;30:868–77.
[34] Levine E, Slusher SL, Grantham JJ, et al. Naturalhistory of acquired cystic kidney disease indialysis patients: a prospective longitudinal CTstudy. AJR Am J Roentgenol 1991;156:501–6.
[35] Port FK, Ragheb NE, Schwartz AG, et al.Neoplasms in dialysis patients: a population-bases study. Am J Kidney Dis 1989;14:119–23.
[36] Matson MA, Cohen EP. Acquired cystic kidneydisease: occurrence, prevalence, and renal can-cers. Medicine 1990;69:217–26.
[37] Allan PL. Ultrasonography of the native kidneyin dialysis and transplant patients. J Clin Ultra-sound 1992;20:557–67.
[38] Strife JF, Souza AS, Kirks DR, et al. MulticysticDysplastic kidney in children: US follow-up.Radiology 1993;186:785–8.
[39] Madewell JE, Goldman SM, Davis CJ, et al.Multilocular cystic nephroma: a radiographic-pathologic correlation of 58 patients. Radiology1983;146:309–21.
Copyright © 2022 FDOKUMEN