
Morphologic characteristics of benign and malignant adrenocortical tumors
8
Morphologic Characteristics of Benign and Malignant Adrenocortical Tumors HENK v. SLOOTEN, MD,’ AARD SCHABERG, MD,t DON SMEENK, MD,’ AND ABRAHAM J. MOOLENAAR, PHDS Differentiation between benign and malignant tumors of the adrenal cortex was studied by means of seven histologic parameters. Each separate criterion was significantly different in two groups, one consisting of patients without metastases within 10 years after operation and one of patients with metastatic tumors. Discrimination on the basis of single parameters in individual patients, however, was of little value. When a histologic index was calculated using the same parameters but after “weighing,” a much better discrimination was obtained. The histologic index and, to a lesser degree, the mitotic activity seems to be related to the survival time of the patients with adrenal cortical carcinoma. The authors conclude that the calculation of a histologic index based on a summation of different parameters makes it possible to differentiate between malignant and benign adrenal cortical tumors. As single parameters, tumor weight and mitotic activity have the highest discriminating value. Cancer 55766-773, 1985. DRENOCORTICAL CANCER was included in the de- A scription of tumors of the kidney given by Grawitz’ in 1884. Wilms2 and Geschickter’ later differentiated between hypernephromas and AC on histologic grounds. The histologic features of the adrenal tumors associated with Cushing’s syndrome have recently been r e ~ i e w e d . ~ It appears that malignant tumors often have lobular structures and are usually surrounded by a capsule. In most tumors, hemorrhagic and necrotic areas are appar- ent. The tumors mainly consist of cells with granular eosinophilic compact and lipid-depleted cytoplasm with a fascicular or alveolar cellular arrangement. The cells often have large multiple nuclei with a coarse vacuolated structure. The nuclei frequently contain large multiple nucleoli. The cells show a widely varying mitotic activity. Invasion of the surrounding structures is often evident. Vascular or capsular invasion is not always easy to assess, however, as tumor cells can often be seen in the vascular lumina. Benign adrenocortical tumors are generally small (<70 g), rounded, encapsulated, and have a yellow cut surface, in which dark or brown foci may be seen. Necrosis and hemorrhage are uncommon. On microscopic examina- tion, the yellow areas correspond to lipid-laden clear cells, morphologically similar to the cells of the zona From the Departments of *Endocrinology. tPathology. and $Patho- Address for reprints: Henk v. Slooten. MU. 1)iaccincsscnhuis. Hout- Accepted for publication February 24. 1984. logical Chemistry, University Hospital Leiden. ‘l’hc Ncthcrlands. laan 55, 2300 RD Leiden. The Netherlands. fasciculata of the normal adrenal cortex; the brown areas consist of compact cells with eosinophilic lipid- poor granular cytoplasm, similar to the cells of the zona reticularis. The tumor cells are arranged in small cords and alveoli. Nuclear or cellular pleomorphism is uncommon. Differentiation between malignant and benign tumors is diffic~lt.~-l~ The course of the disease is sometimes the only distinguishing parameter.”-” Although the weight of the tumor seems to be important in the differentiation between malignant and benign tu- mor~,~.~~-~~ malignant tumors of low weight with metas- tases have also been des~ribed.’-’~.’~ There is no consensus concerning the histologic differentiation between clini- cally hormonal active and nonactive carcinomas. Some aUthors4.9.25-27 have found no differences, whereas others16.28.2y have found more cord-like and alveolar- like structures in carcinomas of patients without a hormonal syndrome. Hough’” used a metastasis-free survival of 5 years as the criterion for the benign state of adrenocortical tumors. He studied the value of several morphologic parameters in 14 adrenal cortical carcinomas and 22 adrenal cortical adenomas. Fibrous bands, diffuse growth pattern, vascular invasion, and tumor cell necrosis had some discriminating value. Single criteria could not separate the two groups, however. An index based on a number of pathologic or clinical parameters at diagnosis was also not decisive. Only when clinical and pathologic parameters were combined could a clear separation between the two groups be obtained. 766
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Morphologic characteristics of benign and malignant adrenocortical tumors

Morphologic Characteristics of Benign and Malignant Adrenocortical Tumors
HENK v. SLOOTEN, MD,’ AARD SCHABERG, MD,t DON SMEENK, MD,’ AND ABRAHAM J. MOOLENAAR, PHDS
Differentiation between benign and malignant tumors of the adrenal cortex was studied by means of seven histologic parameters. Each separate criterion was significantly different in two groups, one consisting of patients without metastases within 10 years after operation and one of patients with metastatic tumors. Discrimination on the basis of single parameters in individual patients, however, was of little value. When a histologic index was calculated using the same parameters but after “weighing,” a much better discrimination was obtained. The histologic index and, to a lesser degree, the mitotic activity seems to be related to the survival time of the patients with adrenal cortical carcinoma. The authors conclude that the calculation of a histologic index based on a summation of different parameters makes it possible to differentiate between malignant and benign adrenal cortical tumors. As single parameters, tumor weight and mitotic activity have the highest discriminating value.
Cancer 55766-773, 1985.
DRENOCORTICAL CANCER was included in the de- A scription of tumors of the kidney given by Grawitz’ in 1884. Wilms2 and Geschickter’ later differentiated between hypernephromas and AC on histologic grounds. The histologic features of the adrenal tumors associated with Cushing’s syndrome have recently been r e~ iewed .~
It appears that malignant tumors often have lobular structures and are usually surrounded by a capsule. In most tumors, hemorrhagic and necrotic areas are appar- ent. The tumors mainly consist of cells with granular eosinophilic compact and lipid-depleted cytoplasm with a fascicular or alveolar cellular arrangement. The cells often have large multiple nuclei with a coarse vacuolated structure. The nuclei frequently contain large multiple nucleoli. The cells show a widely varying mitotic activity. Invasion of the surrounding structures is often evident. Vascular or capsular invasion is not always easy to assess, however, as tumor cells can often be seen in the vascular lumina.
Benign adrenocortical tumors are generally small (<70 g), rounded, encapsulated, and have a yellow cut surface, in which dark or brown foci may be seen. Necrosis and hemorrhage are uncommon. On microscopic examina- tion, the yellow areas correspond to lipid-laden clear cells, morphologically similar to the cells of the zona
From the Departments of *Endocrinology. tPathology. and $Patho-
Address for reprints: Henk v. Slooten. MU. 1)iaccincsscnhuis. Hout-
Accepted for publication February 24. 1984.
logical Chemistry, University Hospital Leiden. ‘l’hc Ncthcrlands.
laan 5 5 , 2300 RD Leiden. The Netherlands.
fasciculata of the normal adrenal cortex; the brown areas consist of compact cells with eosinophilic lipid- poor granular cytoplasm, similar to the cells of the zona reticularis. The tumor cells are arranged in small cords and alveoli. Nuclear or cellular pleomorphism is uncommon.
Differentiation between malignant and benign tumors is d i f f ic~l t .~- l~ The course of the disease is sometimes the only distinguishing parameter.”-” Although the weight of the tumor seems to be important in the differentiation between malignant and benign tu- m o r ~ , ~ . ~ ~ - ~ ~ malignant tumors of low weight with metas- tases have also been des~ribed.’-’~.’~ There is no consensus concerning the histologic differentiation between clini- cally hormonal active and nonactive carcinomas. Some aUthors4.9.25-27 have found no differences, whereas others16.28.2y have found more cord-like and alveolar- like structures in carcinomas of patients without a hormonal syndrome.
Hough’” used a metastasis-free survival of 5 years as the criterion for the benign state of adrenocortical tumors. He studied the value of several morphologic parameters in 14 adrenal cortical carcinomas and 22 adrenal cortical adenomas. Fibrous bands, diffuse growth pattern, vascular invasion, and tumor cell necrosis had some discriminating value. Single criteria could not separate the two groups, however. An index based on a number of pathologic or clinical parameters at diagnosis was also not decisive. Only when clinical and pathologic parameters were combined could a clear separation between the two groups be obtained.
766
No. 4 MORPHOLOGY OF ADRENOCORTICAL TUMORS - Slooten el al. 767
TABLE I . Classification and Frequency of Histologic Cr i te r ia of P r i m a r y Adrenocort ical T u m o r s
Capsular and/or Regressive Structural vascular
changes changes Nuclear atypia Hyperchromasia Nucleoli Mitotic activity invasion Classi-
Grouo No. ficationt No. Percent. No. Percent' No. Percent' No. Percent. KO. Percent. No. Percent' No. Percent.
1 Tumors withcut
metastases IX A 15 (83.3) 7 (39.9) II (61.1) I 2 (66.7) 15 (83.3) 17 (94.4) 13 (72.2) within 10 >r B 3 (16.7) II (61.1) 7 (38.9) 6 (33.3) 3 (16.7) I (5.6) 5 (27.8)
Tumors with I I
metastases 42 A 2 (4.8) I (2.4) 8 (19.0) 6 (14.3) 13 (31.0) 21 (50.0) 3 (7.1) B 40 (95.2) 41 (97.6) 34 (81.0) 36 (85.7) 29 (69.0) 21 (50.0) 39 (92.9)
Discriminating value* 5.1 I .6 2. I 2.6 4. I 9 3.3
Frequency of distribution of tumors over A and B classification within the
t A and B. cldssification of hislologic parameters (see text). group.
In this study, we have examined, in addition to tumor weight, a number of histologic parameters that may discriminate between benign and malignant tumors. The discriminating value of these parameters has been eval- uated whereby a malignancy index was calculated, based on the summation of the individual parameters. The survival time of the patients with a malignant adreno- cortical tumor was correlated with the histologic char- acteristics of the tumor.
Patients and Methods
In the period from 1960 to 1981, 45 patients who had been referred to our clinic were diagnosed on the then current morphologic criteria as suffering from AC. Of these patients, 25 showed no endocrine symptoms. A clinical hormonal syndrome was found in 20 patients, 3 showed virilization, 6 a Cushing's syndrome with virilization. 10 a pure Cushing's syndrome, and 1 a hyperaldosteronism. Metastases developed in 42 of the 45 patients within 10 years after operation. The mor- phologic aspects of the tumors of these 42 patients were studied. Three patients are still free of metastases, more than 10 years after radical surgery. During the same period, the diagnosis of adrenocortical adenoma was made in 15 patients. Of this group 14 had a pure Cushing's syndrome and 1 showed virilization. All of the patients were divided into two groups. Group I consisted of those who survived 10 years without signs of metastases ( 1 5 adenomas and 3 carcinomas); Group I1 comprised 42 patients who showed metastases within 10 years.
Seven histologic parameters were evaluated to assess their discriminatory value with respect to benign state and malignancy.
+ Discriminating value o f classification B: ratio between the frequency o f clas- sification B in Group I I and the frequency o f classification B in Group 1.
1. Regressive changes such as necrosis, hemorrhage, fibrosis, or calcification: (A) little or no change; (B) moderate or extensive change.
2. Preservation of normal structure: (A) mainly nor- mal structure; (B) mainly abnormal structure.
3. Nuclear atypia: (A) no or only slight atypia; (B) moderate or strong nuclear atypia.
4. Nuclear hyperchromasia: (A) no or only slight hyperchromasia; (B) moderate or marked hyperchro- masia.
5. Structure of nucleoli: (A) normal structure; (B) abnormal structure.
6. Mitotic activity, defined as number of mitotic figures per ten high-power (X400) fields (10 HPF): (A) no or not more than two mitotic figures per 10 HPF; (B) more than two mitotic figures per 10 HPF.
7. Invasion of the capsule and/or of the blood vessel wall: (A) no invasion; (B) invasion.
Histologic examinations were carried out by light microscopy after routine staining (Hematoxylin and Eosin (H & E,) elastin, and Sudan). Statistical evaluations were carried out using the standard method as described by A~mitage.~ ' The value of each parameter for discrim- inating between malignant and benign tumors was as- sessed. This was attempted ( 1 ) by calculating the per- centage distribution (frequency) of cases between the A and B classifications for each tumor parameter as well for the group without (Group I) and the group with (Group 11) proven metastases (Table 1); (2) by calculating the discriminating value for a given parameter between benign and malignant tumors by dividing the frequency of B found in Group I1 by that of Group I (Table 1); (3) by calculating the histologic index of each individual tumor by summating the discriminating values of each parameter.

768 CANCER February 15 1985 VOl. 5 5
Four typical cases demonstrating benign or malignant disease are reported. Examples of the calculation of the histologic index are given.
Case Reports
Patient 1
A 23-year-old woman had a slowly developing Cushing’s syndrome. At operation, a well-encapsulated tumor measuring 6 X 3 X 2.5 cm, and weighing 20 g, was removed. The cut surface of the tumor had a brown-yellow color. Microscopic examination showed no regressive changes; the general structure was characterized by irregularly arranged compact zona retic-
FIG. I . Irregularly arranged compact cells and lipid-laden clear cells ( H & E, X 160).
ularis-type cells (Fig. I ) , there was neither atypia nor hyper- chromasia of the nuclei, the nucleoli appeared normal, and the mitotic activity was low (<2 mitoses/lO HPF). There was no capsular or vascular invasion. The diagnosis was adenoma of the adrenal cortex. The calculated index based on the seven evaluated parameters was 1.6 (0 + 1.6 + 0 + 0 + 0 + 0 + 0). The patient has remained in good health for more than 10 years.
Patient 2
A 37-year-old woman had a virilizing syndrome. At opera- tion, a well-encapsulated adrenal tumor measuring I I X 10
FIG. 2. Numerous necrotic areas and marked regressive changes (H & E, X 160).

No. 4 MORPHOLOGY OF ADRENOCORTICAL TLJMORS S/oolcw El a / .
FIG. 3. Tumor cells showing atypia and hyperchrornasia ( H & E. X400).
X 6 cm, weighing 350 g, was removed. The cut surface of the tumor had an orange-yellow color and several small hemor- rhagic necrotic areas. Microscopic examination confirmed the observed regressive changes (Fig. 2); the normal cortical archi- tecture had disappeared, the nuclei showed atypia and hyper- chromasia. (Fig. 3), the nucleoli appeared normal, fewer than two mitotic figures per 10 HPF were found, and no capsular or vascular invasion was noticed. The diagnosis was adreno- cortical carcinoma. The calculated index based on the seven evaluated parameters was 12 (5.7 + I .6 + 2. I + 2.6 + 0 + 0 + 0). The patient has been free from disease for more than 20 years.
769
Patient 3
A 47-year-old woman had Cushing’s syndrome. At operation, an adrenal tumor weighing 300 g was removed. The tumor was presented in several partly hemorrhagic, partly necrotic fragments. Microscopic examination showed extensive regres- sive changes (Fig. 4). The normal cortical structure had dis- appeared completely and the nuclei were hyperchromatic but did not show a marked atypia (Fig. 5). The nucleoli appeared normal, and fewer than two mitotic figures per 10 HPF were seen. There was no capsular or vascular invasion. The diagnosis was adrenocortical carcinoma. The calculated index based on
FIG. 4. Tumor with extensive regressive changes ( H & E, X160).

770 CANCER February 15 1985 VOl. 5 5
the seven evaluated parameters was 9.9 (5.7 + 1.6 + 2.6 + 0 + 0 + 0 + 0). Three years after operation, pulmonary metastases were found. Treatment with mitotanc (0.p'-DDD) was started, resulting in a slow regression of the metastases. The patient is alive 8 years after primary surgery with persisting lung metas- tases. ' I
Patient 4
A 52-year-old woman had Cushing's syndrome. At operation, a lobulated tumor was removed from the left adrenal region. The tumor measured 12 X 8 X 7 cm and weighed 400 g. The
FIG. 5. Irregularly arranged cortical cells showing hyperchromasia but no marked atypia ( H & E. Xl60) .
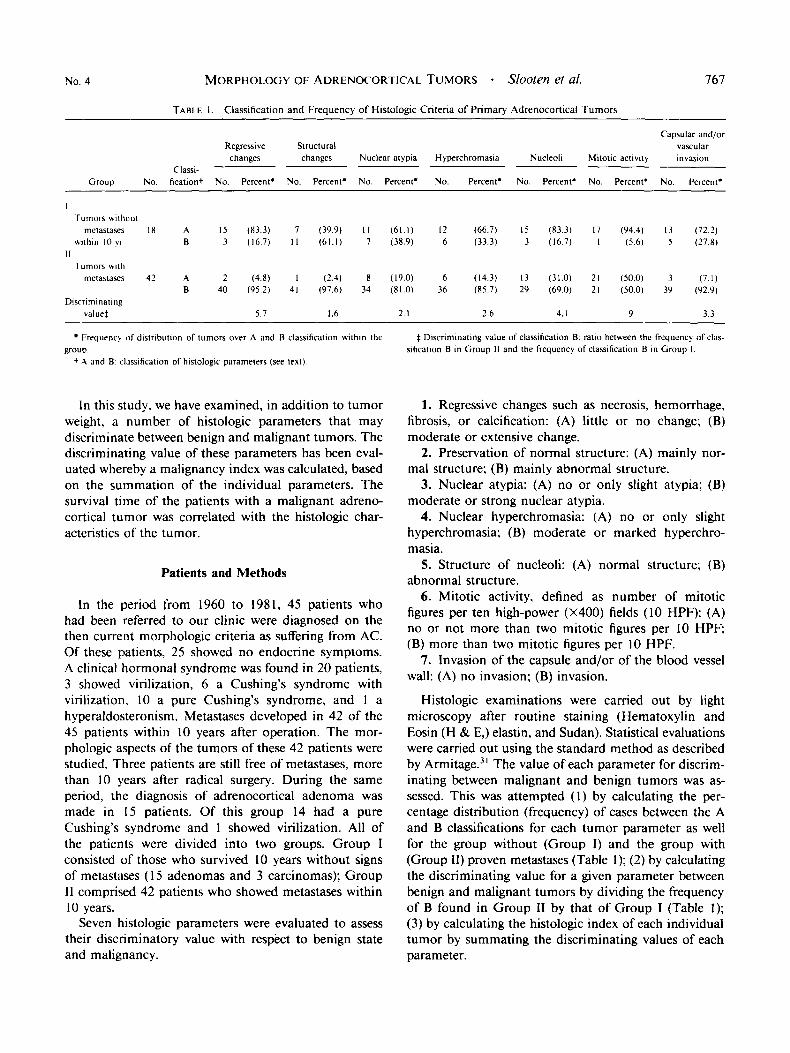
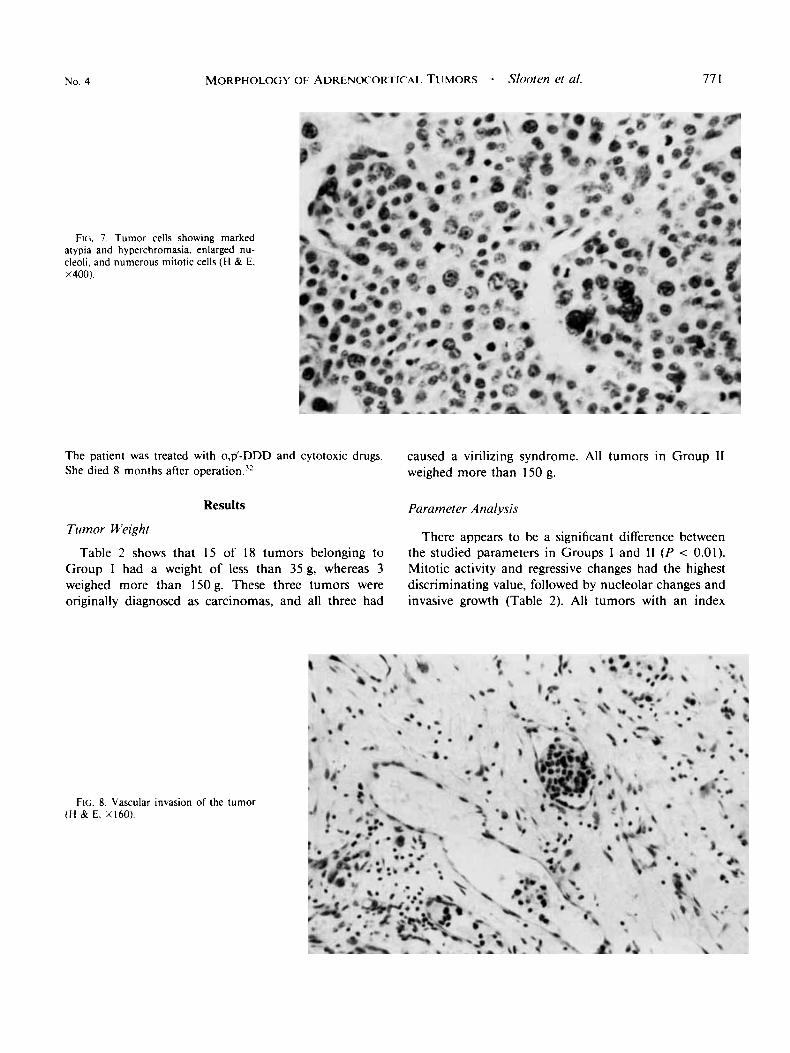
cut surface of the tumor showed dark-red hemorrhagic areas. It appeared that the tumor had already metastasized to the liver and para-aortic lymph nodes. Microscopic examination showed extensive necrosis and hemorrhage (Fig. 6), the normal cortical structure had disappeared, and the nuclei were hyper- chromatic and showed marked atypia (Fig. 7). Nucleoli were enlarged, and some nuclei contained several nucleoli. More than two mitotic figures per 10 HPF were found (Fig. 7), and vascular and capsular invasion was present (Fig. 8). The diagnosis was adrenocortical carcinoma with metastases in liver and lymph nodes. The calculated index based on the seven parameters was 28.4 (5.7 + I .6 + 2. I + 4. I + 9 + 3.3).
FIG. 6. Numerous necrotic areas and marked regressive changes (H & E. Xl60).
No. 4 MORPHOLOGY OF ADRENOCORTICAL TUMORS - S/OoftW ef a/.
FIG;. 7 . Tumor cells showing marked atypia and hyperchromasia. enlarged nu- cleoli, and numerous mitotic cells ( H & €, X400).
The patient was treated with 0.p'-DDD and cytotoxic drugs. She died 8 months after ~peration.~'
Results
Tumor Weight
Table 2 shows that 15 of 18 tumors belonging to Group 1 had a weight of less than 35 g, whereas 3 weighed more than 15Og. These three tumors were originally diagnosed as carcinomas, and all three had
77 I
caused a virilizing syndrome. All tumors in Group 11 weighed more than 150 g.
Parameter Anal-vsis
There appears to be a significant difference between the studied parameters in Groups I and I1 ( P < 0.01). Mitotic activity and regressive changes had the highest discriminating value, followed by nucleolar changes and invasive growth (Table 2). All tumors with an index
FIG. 8. Vascular invasion of the tumor (H & E. X l 6 0 ) .
772 CANCER February I5 1985 Vol. 55
TABLE 2. Weight (in g) of Adrenocortical Tumors
Group No. Range Median Mean
I Tumors without metastases A I 5 7-34 I I 16 within 10 yr C 3 350-1200 840 790
I f Tumors with metastases 42 160-3000 1043 I210
A lurnors originally diagnosed as adenoma. C tumors onginally diagnosed as carcinoma
N
10 l 2 1
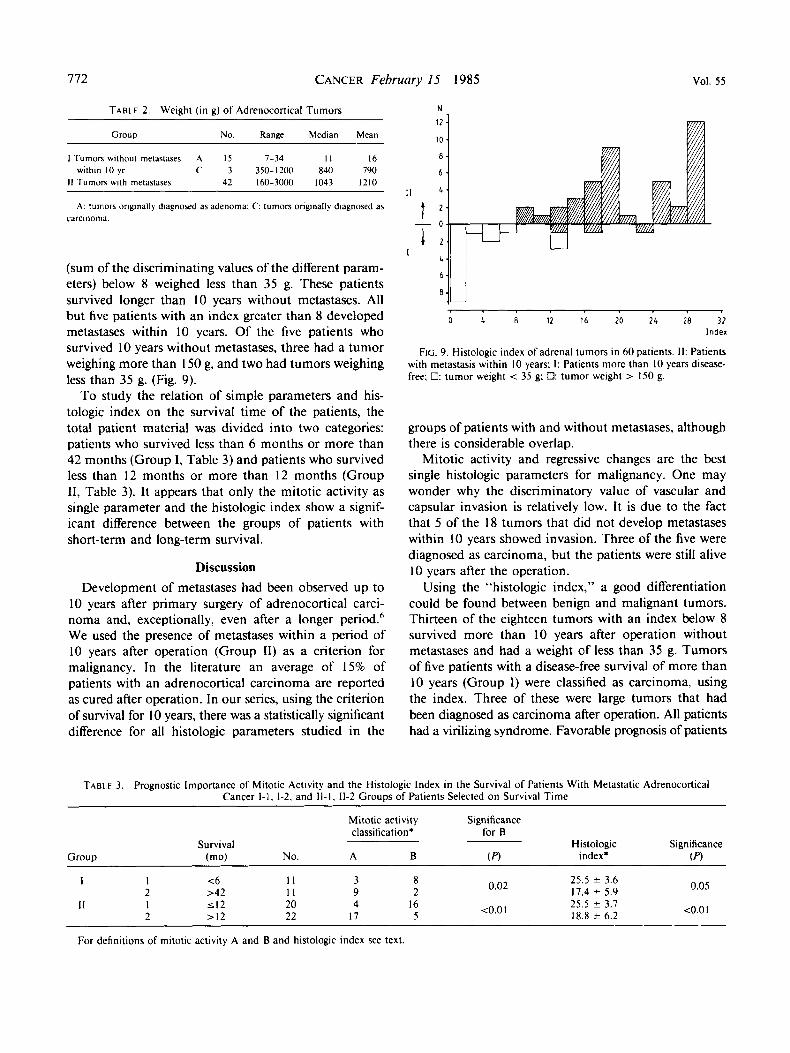
(sum of the discriminating values of the different param- eters) below 8 weighed less than 35 g. These patients survived longer than 10 years without metastases. All but five patients with an index greater than 8 developed metastases within 10 years. Of the five patients who survived 10 years without metastases, three had a tumor weighing more than I50 g, and two had tumors weighing less than 35 g. (Fig. 9).
To study the relation of simple parameters and his- tologic index on the survival time of the patients, the total patient material was divided into two categories: patients who survived less than 6 months or more than 42 months (Group I, Table 3) and patients who survived less than 12 months or more than 12 months (Group 11, Table 3). It appears that only the mitotic activity as single parameter and the histologic index show a signif- icant difference between the groups of patients with short-term and long-term survival.
Discussion Development of metastases had been observed up to
10 years after primary surgery of adrenocortical carci- noma and, exceptionally, even after a longer period.6 We used the presence of metastases within a period of 10 years after operation (Group 11) as a criterion for malignancy. In the literature an average of 15% of patients with an adrenocortical carcinoma are reported as cured after operation. In our series, using the criterion of survival for 10 years, there was a statistically significant difference for all histologic parameters studied in the
0 4 8 12 16 20 2 4 28 32 Index
FIG. 9. Histologic index of adrenal tumors in 60 patients. 11: Patients with metastasis within 10 years: I: Patients more than 10 years disease- free; 0: tumor weight < 35 g; 8: tumor weight > 150 g.
groups of patients with and without metastases, although there is considerable overlap.
Mitotic activity and regressive changes are the best single histologic parameters for malignancy. One may wonder why the discriminatory value of vascular and capsular invasion is relatively low. It is due to the fact that 5 of the 18 tumors that did not develop metastases within 10 years showed invasion. Three of the five were diagnosed as carcinoma, but the patients were still alive 10 years after the operation.
Using the “histologic index,” a good differentiation could be found between benign and malignant tumors. Thirteen of the eighteen tumors with an index below 8 survived more than 10 years after operation without metastases and had a weight of less than 35 g. Tumors of five patients with a disease-free survival of more than 10 years (Group I) were classified as carcinoma. using the index. Three of these were large tumors that had been diagnosed as carcinoma after operation. All patients had a virilizing syndrome. Favorable prognosis of patients
TABLE 3. Prognostic Importance of Mitotic Activity and the Histologic Index in the Survival of Patients With Metastatic Adrenocortical Cancer 1-1. 1-2. and 11-1. 11-2 Groups of Patients Selected on Survival Time
Group
Mitotic activity Significance classification* for B
Survival Histologic Significance (mo) No. A B V) index’ (PI
~
0.05 25.5 * 3.6 17.4 * 5.9 0.02 1 1 <6 I 1 3 8
2 >42 11 9 2 <o.o I 25.5 * 3.7
18.8 * 6.2 <o.o 1 11 I 5 1 2 20 4 16 2 > I 2 22 17 5
For definitions of mitotic activity A and B and histologic index see text

No. 4 MORPHOLOGY OF ADRENOCORTICAL TUMORS * Sooten el a/. 773
with a virilizing adrenocortical cancer after radical surgery has already been reported in the literature.6
The other two tumors had a weight of less than 35 g and were considered to be adenomas at operation. One was found in a girl with a high excretion of 17-oxoste- roids, particularly dehydroandrosterone ( D H E A ) , as often can be found in patients with carcinomas. In the second patient no other signs of malignancy could be found.
In groups of patients with a short survival time, the histologic index is significantly higher than in groups of patients with a longer survival. Of the individual histo- logic parameters, the mitotic activity seems to be of some prognostic value in this respect. In our material, with the exception of two tumors, a high index number corresponded with a high tumor weight. In conclusion, we believe that the histologic index described here is a useful additional diagnostic tool in the differentiation between malignant and benign adrenocortical tumors.
REFERENCES
I . Grawitz P. Die Entstehung van Nierentumoren aus Nebennier- gewebe. Arch ,fur Klin Chir 1884: 30:824.
2. Wilms M. Die Mischgeschwiilste der Niere. Ixipzig: Georgi. 1899.
3. Geschickter CF. Suprarenal tumours. Am J Cancer 1935; 23: 104- 1 1 s .
4. Neville AM. O H a r e J. The Human Adrenal Cortex. Berlin: Springer Verlag. 1982; 186-201.
5 . Huvos AG. Hajdu SI. Rrasfield RD. Foote FW. Adrenal cortical carcinoma: Clinicopathologic study of 34 cases. Cancer 1970; 25:354- 361.
6. Tang ChK. Gray GF. Adrenocortical neoplasms: Prognosis and morphology. Urology 1975; 5:691-695.
7. Schteingart DE, Oberman HA, Friedman BA, Conn JW. Adrenal cortical neoplasms producing Cushing's syndrome: A clinicopathologic study. Cancer 1968: 22:1005-1013.
8. Lewinsky BS, Grigor KM, Symington T, Neville AM. The clinical and pathologic features of "non-hormonal" adrenocortical tumors: Report of twenty new cases and review of literature. Cancer 1974;
9. Gabrilove JL, Sharma DC, Wotiz HH, Dorfman RI. Feminizing adrenocortical tumours in the male: A review of 52 cases including a case report. Medic,ine 1965; 44:37-39.
10. Knight ChD. Trichel BE, Mathews WR. Nonfunctioning carci- noma of the adrenal cortex. Ann Surg 1960: 15 I :349-358.
I I . Doran AHG. Cystic tumour of the suprarenal body successfully removed by operation. Br MedJ 1903: 1:558-565.
33:778-790.
12. King DR. Lack EE. Adrenal cortical carcinoma: A clinical and pathologic study of 49 cases. Cancer 1979; 44239-244.
13. Cahill GF, Meijer M. Melicon M, Darby HH. Adrenal cortical tumors: The types of nonhormonal and hormonal tumors. Surg Gynecol Ohstet 1942; 74:28 1-305.
14. McFarlane DA. The natural history. prognosis and treatment in a study of fifty-five cases. Ann R Coll Surg Engl 1958; 23:155-186.
15. Lipsett MB. Hertz R, Ross GT. Clinical and pathological aspects of adrenocortical carcinoma. Am J . Med 1963; 35:374-383.
16. Symington T. The morphology and zoning of the human adrenal cortex. In: Curry AR, Symington T, Grant JK, eds. The Human Adrenal Cortex. Edinburgh: E & S Livingston. 1962.
17. Kirschner MA, Powell RD. Lipsett MB. Cushings Syndrome: Nodular cortical hyperplasia of adrenal glands with clinical and patho- logical features suggesting adrenocortical tumors. J Clin Endo Merah
18. Scott HW, Foster JH, Liddle GW. Davidson ET. Cushing's syndrome due to adrenocortical tumor: I I-Year review of I S patients. Ann Surg 1965; 162505-516.
19. Hamson JH, Mahoney EM. Bennett AH. Tumors of the adrenal cortex. Cancer 1973: 32:1227-1235.
20. Hayles AB. Hahn HB. Sprague RG. Bahn RC. Priestley JT. Hormone-secreting tumors of the adrenal cortex in children. Pediatrics 1966; 37: 19-25.
21. Orth DN. Liddle GW. Results of treatment in I08 patients with Cushing's syndrome. N Eng/ J Med 197 I ; 285:243-247.
22. Soffer W. lannaconne A, Gabrilove JL. Cushing's syndrome: A study of 50 patients. Am JMed 1961: 30:129-146.
23. Neville AM, OHare MJ. The pathology of adrenocortical neoplasia. Human Parhol 1979; 10: 137.
24. Alterman SL, Dominguez C. Lopez-Gomez A, Lieber AL. Primary adrenocortical carcinoma causing aldosteronism. Cancer 1969; 24:602-609.
25. lbanez ML. Endocrine and Nonendocrine hormone producing tumors. Chicago: Yearbook Medical. 197 I : 231-239.
26. Kay S. Hyperplasia and neoplasia of the adrenal gland. Pathol Ann 1976; I1:103-139.
27. Karsner HT. Tumors of the adrenal. In: Atlas of Tumor Pathology Section 8, Part 29P16. Washington, DC: Armed Forces Institute of Pathology. 1950.
28. Heinbecker P, ONeal LW. Ackerman LV. Functioning and nonfunctioning adrenal cortical tumors. Surg Gynecol Ohster 1957;
29. Birke G. Franksson CA. Moberger C, Plantin LO. Adrenal cortical tumours: A study with special reference to possibilities of correlating appearance with hormonal activity. Acra Chir Scand 1959; 117:233-247.
30. Hough AJ, Hollifield JW, Page DL, Hartman WH. A mathe- matical analysis of clinical and morphological data. Am J Clin Parhol
3 I . Armitage P. Statistical Methods in Medical Research. Oxford: Blackwell Scientific, 1980.
32. van Slooten H, Moolenaar AJ. v Seters AP, Smeenk D. The treatment of adrenocortical carcinoma with o,p'-DDD: Prognostic implications of Serum level monitoring. Eur J Cuncer Clin Oncol 1984: 20:47-53.
1964: 241947-954.
I0512 1-33,
1979; 72:390-339.




















