
Cortical bone drilling and thermal osteonecrosis
13
Review Cortical bone drilling and thermal osteonecrosis Goran Augustin a, ⁎, Tomislav Zigman a, 1 , Slavko Davila a, 2 , Toma Udilljak b, 3 , Tomislav Staroveski b, 3 , Danko Brezak b, 4 , Slaven Babic c, 5 a University Hospital Center Zagreb and School of Medicine, University of Zagreb, Zagreb, Croatia b Faculty of Mechanical Engineering and Naval Architecture, University of Zagreb, Zagreb, Croatia c Clinical Hospital Center Sestre Milosrdnice, Zagreb, Croatia abstract article info Article history: Received 28 April 2011 Accepted 13 October 2011 Keywords: Bone Drill Drilling Parameters Temperature Thermal osteonecrosis Background: Bone drilling is a common step in operative fracture treatment and reconstructive surgery. During drilling elevated bone temperature is generated. Temperatures above 47 °C cause thermal osteonecrosis which contributes to screw loosening and subsequently implant failures and refractures. Methods: The current literature on bone drilling and thermal osteonecrosis is reviewed. The methodologies involved in the experimental and clinical studies are described and compared. Findings: Areas which require further investigation are highlighted and the potential use of more precise experimental setup and future technologies are addressed. Interpretation: Important drill and drilling parameters that could cause increase in bone temperature and hence thermal osteonecrosis are reviewed and discussed: drilling speed, drill feed rate, cooling, drill diameter, drill point angle, drill material and wearing, drilling depth, pre-drilling, drill geometry and bone cortical thickness. Experimental methods of temperature measurement during bone drilling are defined and thermal osteonecrosis is discussed with its pathophysiology, significance in bone surgery and methods for its minimization. © 2011 Elsevier Ltd. All rights reserved. 1. Introduction Most articles concerning drilling are published in engineering journals, but the question is if those are applicable in medical practice. Most of research, focused on bone drilling, is done in dentistry. Nevertheless, there is significant number of orthopedic/traumatologic articles concerning drilling but some contradictions are still present. In this review the literature is summarized with intention to define parameters affecting the quality of cortical bone drilling, primarily heat transfer and heat induced damage to the bone. With the development of modern surgery, bone drilling became a common step of an everyday procedure in orthopedics/traumatology and dentistry. Frictional heat from these operations may result in thermal necrosis of bone. In respect to current fracture fixation prin- ciples or reconstructive surgery, every loosening of implants in bone is adverse side effect. The implant failure rate for lower leg osteo- synthesis is 2–7% (Augustin et al., 2007) and is higher compared to upper extremity due to physiologic stress during locomotion. Many parameters influence loosening of bone–implant interface. One of them is thermal osteonecrosis explained in the section Thermal osteonecrosis. Bone temperature must be below the temperature of 47 °C during drilling to avoid thermal osteonecrosis (Eriksson and Adell, 1986; Eriksson and Albrektsson, 1984). Various parameters have been studied to reduce heat generation during bone drilling, in- cluding variations in drill design, drilling parameters and coolant de- livery. Many factors contribute to heat generation during drilling but many articles focused only on a single or only several parameters of this rather complicated issue. However, there is lack of unity regard- ing the optimal combination of drill design, drilling process and cool- ant delivery. The ideal method for determining the bone temperature during drilling is difficult to define because bone is a complex aniso- tropic biological tissue, with organic and inorganic components. The interaction of the different components accounts for its complex me- chanical and thermological properties which are difficult to study due Clinical Biomechanics 27 (2012) 313–325 ⁎ Corresponding author at: Department of Surgery, University Hospital Center Zagreb and School of Medicine, University of Zagreb, Kišpatićeva 12, 10000 Zagreb, Croatia. E-mail addresses: [email protected] (G. Augustin), [email protected] (T. Zigman), [email protected] (S. Davila), [email protected] (T. Udilljak), [email protected] (T. Staroveski), [email protected] (D. Brezak), [email protected] (S. Babic). 1 Department of Surgery, University Hospital Center Zagreb, Kišpatićeva 12, 10000 Zagreb, Croatia. 2 Department of Surgery, University Hospital Center Zagreb and School of Medicine University of Zagreb, Kišpatićeva 12, 10000 Zagreb, Croatia. 3 Department of Technology, Chair of Machine Tools, Faculty of Mechanical Engi- neering and Naval Architecture, University of Zagreb, Ivana Lučića 5, 10000 Zagreb, Croatia. 4 Department of Robotics and Production System Automation, Chair of Engineering Automation, Faculty of Mechanical Engineering and Naval Architecture, University of Zagreb, Ivana Lučića 5, 10000 Zagreb, Croatia. 5 Department of Traumatology, Clinical Hospital Center Sestre Milosrdnice (Trauma- tology Clinic), Draškovićeva 19, 10000 Zagreb, Croatia. 0268-0033/$ – see front matter © 2011 Elsevier Ltd. All rights reserved. doi:10.1016/j.clinbiomech.2011.10.010 Contents lists available at SciVerse ScienceDirect Clinical Biomechanics journal homepage: www.elsevier.com/locate/clinbiomech
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Cortical bone drilling and thermal osteonecrosis

Clinical Biomechanics 27 (2012) 313–325
Contents lists available at SciVerse ScienceDirect
Clinical Biomechanics
j ourna l homepage: www.e lsev ie r .com/ locate /c l inb iomech
Review
Cortical bone drilling and thermal osteonecrosis
Goran Augustin a,⁎, Tomislav Zigman a,1, Slavko Davila a,2, Toma Udilljak b,3, Tomislav Staroveski b,3,Danko Brezak b,4, Slaven Babic c,5
a University Hospital Center Zagreb and School of Medicine, University of Zagreb, Zagreb, Croatiab Faculty of Mechanical Engineering and Naval Architecture, University of Zagreb, Zagreb, Croatiac Clinical Hospital Center Sestre Milosrdnice, Zagreb, Croatia
⁎ Corresponding author at: Department of Surgery, Unand School of Medicine, University of Zagreb, Kišpatićeva
E-mail addresses: [email protected] (G. [email protected] (T. Zigman), [email protected]@fsb.hr (T. Udilljak), [email protected]@gmail.com (D. Brezak), slaven.babic@gm
1 Department of Surgery, University Hospital CenterZagreb, Croatia.
2 Department of Surgery, University Hospital Center ZUniversity of Zagreb, Kišpatićeva 12, 10000 Zagreb, Croa
3 Department of Technology, Chair of Machine Toolsneering and Naval Architecture, University of Zagreb,Croatia.
4 Department of Robotics and Production System AutAutomation, Faculty of Mechanical Engineering and NaZagreb, Ivana Lučića 5, 10000 Zagreb, Croatia.
5 Department of Traumatology, Clinical Hospital Centetology Clinic), Draškovićeva 19, 10000 Zagreb, Croatia.
0268-0033/$ – see front matter © 2011 Elsevier Ltd. Alldoi:10.1016/j.clinbiomech.2011.10.010
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 28 April 2011Accepted 13 October 2011Keywords:BoneDrillDrillingParametersTemperatureThermal osteonecrosis
Background: Bone drilling is a common step in operative fracture treatment and reconstructive surgery. Duringdrilling elevated bone temperature is generated. Temperatures above 47 °C cause thermal osteonecrosis whichcontributes to screw loosening and subsequently implant failures and refractures.Methods: The current literature on bone drilling and thermal osteonecrosis is reviewed. The methodologiesinvolved in the experimental and clinical studies are described and compared.Findings: Areas which require further investigation are highlighted and the potential use of more preciseexperimental setup and future technologies are addressed.Interpretation: Important drill and drilling parameters that could cause increase in bone temperature and hencethermal osteonecrosis are reviewed and discussed: drilling speed, drill feed rate, cooling, drill diameter, drillpoint angle, drill material and wearing, drilling depth, pre-drilling, drill geometry and bone cortical thickness.
Experimentalmethods of temperaturemeasurement during bone drilling are defined and thermal osteonecrosisis discussed with its pathophysiology, significance in bone surgery and methods for its minimization.© 2011 Elsevier Ltd. All rights reserved.
1. Introduction
Most articles concerning drilling are published in engineeringjournals, but the question is if those are applicable in medical practice.Most of research, focused on bone drilling, is done in dentistry.Nevertheless, there is significant number of orthopedic/traumatologicarticles concerning drilling but some contradictions are still present.In this review the literature is summarized with intention to define
iversity Hospital Center Zagreb12, 10000 Zagreb, Croatia.gustin),yahoo.com (S. Davila),(T. Staroveski),
ail.com (S. Babic).Zagreb, Kišpatićeva 12, 10000
agreb and School of Medicinetia., Faculty of Mechanical Engi-Ivana Lučića 5, 10000 Zagreb,
omation, Chair of Engineeringval Architecture, University of
r Sestre Milosrdnice (Trauma-
rights reserved.
parameters affecting the quality of cortical bone drilling, primarilyheat transfer and heat induced damage to the bone.
With the development of modern surgery, bone drilling became acommon step of an everyday procedure in orthopedics/traumatologyand dentistry. Frictional heat from these operations may result inthermal necrosis of bone. In respect to current fracture fixation prin-ciples or reconstructive surgery, every loosening of implants in boneis adverse side effect. The implant failure rate for lower leg osteo-synthesis is 2–7% (Augustin et al., 2007) and is higher compared toupper extremity due to physiologic stress during locomotion.
Many parameters influence loosening of bone–implant interface.One of them is thermal osteonecrosis explained in the section Thermalosteonecrosis. Bone temperature must be below the temperature of47 °C during drilling to avoid thermal osteonecrosis (Eriksson andAdell, 1986; Eriksson and Albrektsson, 1984). Various parametershave been studied to reduce heat generation during bone drilling, in-cluding variations in drill design, drilling parameters and coolant de-livery. Many factors contribute to heat generation during drilling butmany articles focused only on a single or only several parameters ofthis rather complicated issue. However, there is lack of unity regard-ing the optimal combination of drill design, drilling process and cool-ant delivery. The ideal method for determining the bone temperatureduring drilling is difficult to define because bone is a complex aniso-tropic biological tissue, with organic and inorganic components. Theinteraction of the different components accounts for its complex me-chanical and thermological properties which are difficult to study due

314 G. Augustin et al. / Clinical Biomechanics 27 (2012) 313–325
to sensitivity to testing conditions and specimen preparation (Zelenov,1985).
2. Historical remarks
Bone drilling is not a novelty in medicine. Human skeletons fromancient civilizations show surgically perforated holes in their skulls.Bone drilling was described in ancient Egyptian, Greek and Romanmedicine. Accelerated development of medicine in late 19th and 20thcentury, due to asepsis, anesthesia/analgesia and antibiotics, led toblooming of dentistry and traumatology/orthopedics, two fields whichdemanded research on bone drilling. Initial studies of thermal changesduring teeth burring were published by Anderson and Van Proagh(1942), Henschel (1943), Walsh and Symmons (1949) but are beyondthe scope of this review.
Modern use of orthopedic/traumatologic bone drilling startedaround 1850 as a part of the operation for fracture fixation with screws(Cucuel and Rigaud, 1850), as external fixation (Cucuel and Rigaud,1850) and with screws and plates (Hansmann, 1886). Bone drillingper se was not studied then because it was performed manually usingself-threading and self-taping screws. There was no systematic studyon the development of a more suitable drilling tool until Bechtol pre-sented a set of guidelines for bone drilling and manufacturing of drillpoints (Bechtol, 1956). Sneath, in similar study presented recommen-dations for drill point configuration of a twist drill (Sneath, 1964).Matthews and Hirsch introduced temperature measurement in vitrodrilling using bone specimens (Matthews and Hirsch, 1972). Jacobs etal. defined drill point geometry in relation to bone properties (Jacobset al., 1976). Saha et al. followed his work, in 1982, proposing newdrill with improved design and performance, based on research ondrill geometry (Saha et al., 1982). Finally, Eriksson and Albrektsson(1982–1986), defined in vivo experiments with precise temperaturemeasurement and histologic analysis of bone specimens and facilitateddevelopment of modern research on bone drillng (Eriksson and Adell,1986; Eriksson and Albrektsson, 1982, 1984).
3. Bone drilling parameters
These parameters do not influence temperature rise and drillingefficiency independently — drilling parameters are interrelated.Therefore, absolute values of temperature rise in different articlesshould be considered carefully, taking in account the experimentalsetup — i.e. experiments were conducted 1) at room temperature,2) at body temperature in a tank of solution and 3)with orwithout sub-stitute for cooling effect of circulating blood. Regarding this, the princi-ples of influence of the two groups of the most important parameters(Table 1) are more interesting than the absolute values of temperaturerise reported in literature.
Table 1The most influential parameters of the drill and drilling process on efficiency and in-crease in bone temperature.
Parameters of the drill Parameters of bone drilling
Drill design Drilling speed (spindle speed, rotational speed)Flutes Low speed drillingDrill point design High speed drillingDrill point angle Drill feed rate
Drill diameter Drilling energy (power)Drill material and wearing Cooling
Internal coolingOpen systemClosed system
External coolingDrilling depthPre-drillingBone cortical thickness
3.1. Drill design
Drill design has several important interrelated structural elementsthat contribute to the efficacy of the bone drilling making analysis of asingle parameter difficult (Fig. 1). Drill consists of shank, body (partwith the flutes) and drill point. The peripheral portions of the bodybetween adjacent flutes are called lands. Drill diameter is the largestdiameter measured across the top of the lands behind the point.Drill point is the cutting end of a drill, made up of the ends of thelands and the web. In form it resembles a cone, but departs from atrue cone to furnish clearance behind the cutting lips. Angle betweencutting lips is called point angle. Fig. 1 shows drill point of two cuttinglips, which are the cutting edges of a two fluted drill extending fromthe chisel edqe to the periphery (Fig. 1).
Other important drill geometry parameters are presented in Fig. 2.Helix angle is the angle made by the leading edge of the land with aplane containing the axis of the drill. Larger angles are used for largerdiameter drills. Rake angle is the angle between the leading edge ofthe land and an axial plane at the drill point; it is the angle at whichthe cutting face is presented to thematerial. Helix and rake angle are re-lated, that is larger helix angle will generate larger rake angle. Wedgeangle is the angle between the cutting face and the flank. Bodydiameterclearance is that portion of the land that has been cut away to preventrubbing against the walls of the hole. Clearance angle is the angle bywhich the flank (non-cutting portion of the blade) clears the material.Lip relief angle is the axial relief angle at the outer corner of the lip. Itis measured by projection into a plane tangent to the periphery at theouter corner of the lip (Karmani and Lam, 2004).
The process of drilling is complex, as the various elements of thecutting tip act in different ways during drilling. Chisel edge displacesmaterial ahead of it as it thrusts forward. Cutting lip engages the bonesurface producing plastic deformation along shear planes. The resultis failure of the bone in shear generating chip that flows on rakeface of the drill tip and is directed along the drill flutes.
3.1.1. FlutesFlutes are helical or straight grooves cut or formed in the body of
the drill to provide cutting lips, to permit removal of chips, and toallow cutting fluid to reach the cutting lips. Drills can be constructedwith two or three flutes with various helix angles (Fig. 3). The com-mon drill used is a twist drill with two helical flutes. Bertollo et al.(2008) showed that the 3-fluted drill significantly out-performs the2-fluted drill not only in targeting ability but also in the range of per-missible approach angles and has superior bending stiffness. In hismore recent study (Bertollo et al., 2010) the feed rates for two exam-ined 3-fluted drills were found to be higher compared to the 2-fluted
Fig. 1. Spiral drill design. The peripheral portions of the body between adjacent flutesare lands. Drill diameter is the largest diameter measured across the top of the landsbehind the point. Drill consists of shank, body (part with the flutes) and drill point.Drill point is the cutting end of a drill, made up of the ends of the lands and the web.Angle between cutting lips is point angle. There are two cutting lips on this type ofdrill point, which are the cutting edges of a two flute drill extending from the chiseledge to the periphery (Karmani and Lam, 2004).

Fig. 2. Drill tip geometry parameters. Helix angle is made by the leading edge of theland with a plane containing the axis of the drill. Rake angle is between the leadingedge of the land and an axial plane at the drill point; it is the angle at which the cuttingface is presented to the material. Helix and rake angle are related — larger helix anglewill generate larger rake angle. Wedge angle is between the cutting face and the flank.Body diameter clearance is that portion of the land that has been cut away so it will notrub against the walls of the hole. Clearance angle is the angle by which the flank (non-cutting portion of the blade) clears the material. Lip relief angle is the axial relief angleat the outer corner of the lip. It is measured by projection into a plane tangent to theperiphery at the outer corner of the lip (Chacon et al., 2006; Karmani and Lam, 2004).
315G. Augustin et al. / Clinical Biomechanics 27 (2012) 313–325
drill. Examinations were carried at 79 N and 149 N, which were foundto be the upper and lower bounds of the 95% confidence interval foraxial thrust force applied by the surgeons. The inclusion of the addition-al cutting face in the 3-fluted drill design removes additional bone dur-ing each rotation, reducing drilling time. Since feed rate is a directmeasure of cutting efficiency, the study suggested that the 3-fluteddrills had a higher cutting efficiency reduction of heat generation than
Fig. 3. Drawings showingvariations in helix angle andaworm spiral bit (Natali et al., 1996).
the 2-fluted drill. It should be noted that 2-fluted drill had drill pointangle of 97° and 3-flutted drill of 44°. In spite of these results, the ob-served increases in cutting efficiency of the 3-fluted drills tested didnot translate into a reduction in heat generation or improvement inbone healing or screw fixation. Dry bone is described as short chipping,as the debris generated are small particles that are easily cleared by thedrill bit. The optimal helix angle for such materials is small. At surgerybone debris is mixed with blood and marrow fat and in this wet stateit flows differently and tends to clog slow helix flutes; in this situationquick helix flutes are more suitable (Natali et al., 1996). These resultsare confirmed by Davidson (1999) where the temperature decreasesuniformly with increasing helix angle.
3.1.2. Drill point designJacobs examined extendedly drill point geometry in bone surgery
(Jacobs et al., 1976). He proposed appreciable positive rake angle(25–30°). Wiggins and Malkin (1976) identified the factor of cloggingof drill flutes as having a deleterious effect on drilling performance. Itcauses a substantial increase in drilling torque which is proportionalto the hole depth, and a corresponding increase in the specific cuttingenergy. Studies by Saha et al. (1982), despite the differences in pointangle suggestions, confirmed earlier proposed rake angle. Authorsalso proposed relatively large clearance angle of 15–18°. Natali et al.(1996) compared commercially available drill bits with their orthope-dic equivalents and found that commercially available drill bits per-formed better, producing significantly less thermal injury to thesurrounding bone and halving the force required for cortical penetra-tion. Their results suggested that the optimal drill bit for orthopedicpurposes should have a split point and a quick helix (larger helixangle, and rake angle as well). Several authors analyzed influence of re-lief and clearance angle on increase on bone temperature but withsomewhat conflicting results (Chacon et al., 2006; Oberg et al., 1989).More research is needed to firmly establish a relation between relief/clearance angles and increased temperatures.
3.1.3. Drill point angleWith smaller or sharper (≤90°) point angle, drill bit ‘stabs’ in ma-
terial easier, and ‘walking’ of the drill on the curved bone surface isminimized. Using sharper point angle drill temperature is higher ona small surface in the first moments of drilling, because a relativelysmall percentage of cutting lip involved in cutting action. Drills witha larger or blunter (>90°) point angle accomplish a full contact ofthe cutting lip and the bone earlier. Generally drills with larger pointangle are more suitable for hard materials, and those with the smallerangle for softer materials such as bone (Karmani and Lam, 2004). Cut-ting force has axial and radial component— the sharper the drill pointangle the higher is the radial component. The drill point angle has sig-nificant influence on the axial force — the sharper (more acute) thedrill point angle the lower is the axial drilling force. Reduction below80° is not desirable. Smaller point angles cause elliptic bores andtherefore the drill should be ground to this point angle (Augustin etal., 2007).Wiggins andMalkin (1976) did not notice this phenomenonof elliptic holes during the experiment with 60° point angle. Jacobs etal. focused on measuring drill torque and thrusts and proposed pointangle of 90° (Jacobs et al., 1976) and Saha et al. (1982) suggestedpoint angle in range of 110–118°. Later works (Natali et al., 1996) con-firmed those results. Augustin et al. (2007) using drill point angle of80°, 100° and 120° did not show significant difference on the increasein bone temperature during drilling for 2.7, 3.2 and 4.5 mm drills(with and without cooling). Also, Hillerya and Shuaib did not demon-strated significant difference using drill point angle of 70, 80 and 90°with 23° positive rake angle (Hillerya and Shuaib, 1999). Recentwork by Paszenda and Basiaga is a finite element modeling analysisdetermining strains and stresses in working part of the drill. For thedrill point angle of 90° (both for standard and martensitic stainlesssteel) strains and stresses are lesser than for the point angle of 120°.

Fig. 4. Photographs of the three drills, side view and tip. The upper photographs are ofthe new drill, the center photographs are of the drill that had drilled 600 holes, and thelower photographs are of the drill from operating theater after several months of use(Allan et al., 2005).
316 G. Augustin et al. / Clinical Biomechanics 27 (2012) 313–325
This analysis is simulation model without correlation of influence ofdrill point angle on bone temperature elevation (Paszenda andBasiaga, 2009).
3.2. Drill diameter
Influence of drill diameter on increase in bone temperature is signif-icant. Increase in drill diameter increases energy transfer to the bonecausing temperature rise. This is due to increased friction because of in-crease of contact surface between drill and the bone. Karaca et al.(2011) analyzed drills from 2 to 6 mm diameter but did not metionedinfluence of diameter on the increase in bone temperature. Kalidindi(2004) and Augustin et al. (2007) showed that increase of the drill di-ameter exponentially increases temperature. Both studies show thatthe drill diameters of 4–4.5 mm cause increase of bone temperatureabove critical of 47 °C in comparison with smaller drill diameters(2–3.5 mm). In the study by Augustin et al. 2-fluted twist drill wasused and in the study by Kalidindi the geometry of the drill is not de-scribed. There are no studies for larger drills and therefore 4–4.5 mmdi-ameter is defined as critical and irrigation is mandatory. Theseconclusions are in accordance with experiments on bone intramedul-lary reaming, which imply that the wider the reamer diameter themore thermal damage to the bone is present (Riquelme Garcia et al.,2004).
On the other hand, larger drills have larger flutes which contributeto better elimination of heated bone chips and debris resulting inmore efficient drillingwith lesser increase in bone temperature. Despitethis phenomenon increase in drill diameter causes increase in bonetemperature. When drilling metals, metal chips carry away around85% of the heat generated. Unlike metals and due to poor thermal ca-pacity and conductivity, bone chips carry away smaller percentage ofheat.
Another problem is that with decreased drill diameters (≤3.2 mm)a relevant drill bending within the bone can occur. The deviation ofthe actual to theplanned target point ranges from1 to 10 mmand is sig-nificantly influenced by the drilling channel length and the drill bitlength (Hüfner et al., 2005). Additional negative effect of larger drillholes is that drill holes of up to 20% of the diameter of the bone de-creased the strength of the bone by 40% of its original strength (Bechtolet al., 1959). After removal of the osteosynthetic material the drill holesare present up to 12 weeks postoperatively (visible on X-rays) whenthere is increased risk of fracture or refracture due to decreased bonestrength (Burstein et al., 1972).
3.3. Drill material and wear
Medical drills wore out during repeated drilling and sterilization.This process leads to reducing the sharpness of drill cutting lipscausing increased heat production (Matthews and Hirsch, 1972).Factors that contribute to drill wear are bone density, clogged debrisreleased during drilling, cooling, drill material, geometry and surfacetreatment. Drill wear can be detected by macrophotograph, light orelectron microscopy. Chacon et al. (2006) examined heat productionby three drill systems (with different clearance, relief and edge angle)after repeated drilling and sterilization at constant drill speed, diameter,depth and drilling force, using external cooling. Light microscope wasused to evaluate drill wear. Temperature increase was present after 25uses, but it was significantly different in three drill systems (significant-ly higher in drill without a relief angle). Similar observation is foundduring bone reaming, as reamer sharpness is pointed out as a key factorin avoidance of thermal damage to the bone (Riquelme Garcia et al.,2004). Canteroa et al. (2005) made an comprehensive study on factorsaffecting drill wear, and techniques to detect this wear. The end of toollifewas reached because of catastrophic failure of the drill, but no signif-icant progressive wear in cutting zone was observed previously, usingoptical microscope. Fine hole quality was observed even near tool
catastrophic failure, evaluated from the point of view of dimensions,surface roughness and burr height. Allan et al. (2005) examined threedrills (Leibinger 1.5 mm diameter twist drill, with two flutes): newdrill, another after 600 holes drilled, and the third after usage in the the-ater for several months (number of drilling not specified). There was asignificant difference in the temperature rise which was proportionalto the amount of wear (Fig. 4). Considering drill material, recent workby Karaca et al. (Karaca et al., 2011) found that the TiBN coated drillscaused higher temperatures than uncoated ones but without detaileddiscussion of its cause.
3.4. Drill speed
3.4.1. Low speed drillingThere are various results published about the optimal speed for
bone drilling. Researchers focused primary on low speed drilling(up to 3000 rpm), and concluded that increase of drilling speed in-creases bone temperature (Thompson, 1958). However, this is onlytrue up to drilling speed of approximately 10,000 rpm. These resultsare confirmed later by Eriksson, Nam et al. (2006), Kalidindi (2004)and Augustin et al. (2007). Only Matthews and Hirsch (1972) didnot find any significant change in temperature with speeds ranging345–2900 rpm while drilling human cadaveric femora, implyingthat the temperature rise was more dependent on the drilling pres-sure. Brisman (1996) concluded that drilling of bovine cortical boneat a low speed of 1800 rpm and at a minimal load of 1.2 kg producedthe same heat as higher speed of 2400 rpm and higher load of 2.4 kg.Independently, increase of either speed or load caused an increase inbone temperature. However, increasing both the speed and the loadtogether allowed for more efficient cutting with no significant in-crease in temperature. Sharawy conducted similar study showingthat the higher the speed, the less was the heat generated for speedsfrom 1225 to 2500 rpm (Sharawy et al., 2002). The mean rise in tem-perature, the time of drilling, and the time needed for a pig jaw boneto return to the baseline temperature were monitored using 4 ther-mocouple technology (compared to one thermocouple measure-ments in of previously mentioned articles). No attempt was madeduring this study to assess the pressure (load) applied on the drill.Thompson, in 1958, showed that during speed below 250 rpm in-creased the degree of fragmentation of the hole edge (Thompson,

317G. Augustin et al. / Clinical Biomechanics 27 (2012) 313–325
1958) confirming that optimal drill and drilling parameters are im-portant for adequate osteosynthesis.
3.4.2. High speed drillingSome of the first studies were done in 1960s. These histological
studies showed that high speed drilling could have less deleteriouseffect on bone than conventional speeds used (Boyne, 1966; Moss,1964; Spatz, 1965). Krause et al. showed that thermal effect of highspeed drilling depends on the drill design (Krause et al., 1982).
There is a difficulty in defining a high speed drilling. Classical den-tal burs operate at speeds of 3600–7500 rpm compared to orthopedicdrills at 60–800 rpm (Karmani, 2006). In neurosurgery high speeddrilling is more affiliated. Roitenberg defines high speed drilling as70,000 rpm, and low speed drilling as 20,000 rpm. Authors comparedseveral ultra power drilling systems without comparison with ortho-pedic drilling (Roitberg et al., 1997). Similar results were publishedby Kondo et al. showing that high speed drilling is safe in clinicalpraxis; again without comparison to orthopedic drilling. This type ofdrilling was used for removing bone flaps, and not for osteosynthesisor dental implanting (Kondo et al., 2000).
The experiments by Abouzgia (Abouzgia and James, 1997; Abouzgiaand Symington, 1996) and Reingewirtz (Reingewirtz et al., 1997) in-cluded high drill speeds up to 100,000 rpm, and pointed out that the de-pendence of temperature increase regarding drill speed is not simplelinear function, but rather a function with increase, peek, decrease andplateau. When drilling speed exceeds 10,000 rpm, temperatures de-creasewith increase of drilling speed until it reaches a plateau at around40,000–50,000 rpm (Fig. 5). Also, drill speed is not an independent fac-tor in heat production, but it is primarily associated with drill feed rateand pressure. Following these results, Davidson used a numerical simu-lation to perform a parametric analysis of the importance of individualdrilling parameters. He showed that the maximum temperature in-creases with drill speed in range of 100,000–200,000 rpm. This workcontinued controversies about high speed drilling (Davidson, 1999).
Udiljak et al. investigated high speed drilling in range 3000–24,000 rpm. The results were expressed in cutting speed (m/min),which is usual in engineering literature, and stands for rotational speedof the exterior point of the drill (depending on rpm and drill diameter).High speed drilling (140 m/min) causes less temperature increase thanstandard drilling speed (6.53 m/min), for both types of drills tested(standard surgical twist drill and two-step drill). They concluded thatthere is no sense to increase cutting speed above 140 m/min (Udiljaket al., 2007).
Special consideration of machining stability in high-speed drillingis pointed out in an engineering study by Arvejah and Ismail, sincestability becomes important factor with increase in drilling speed. Itis shown that, gyroscopic effect (the torque on the gyroscope appliedperpendicular to its axis of rotation and also perpendicular to its
Fig. 5. a) Influence of the rotational speed on the temperature rise. The continuous line is an erotational speed on the drilling time. The straight line represents the best fit of a linear fun
angular momentum causes it to rotate about an axis perpendicularto both the torque and the angular momentum) has a profound effecton the resulting stability lobes, especially at very high speeds; also itmakes the lobes wider but at the same time lowers the minimum sta-bility boundary (Arvajeh and Ismail, 2006).
3.5. Drill feed rate
The drill feed rate is another influential parameter with dual im-portance. With its increase, shorter drilling time is achieved andthereby lesser heat transfer to the bone. On the other hand, withhigher axial force applied during drilling on the bone increases fric-tion, which could lead to temperature increase and drill failure. It is,therefore, necessary to find the optimal feed rate so that the force isnot excessive and the drilling time as short as possible to minimizeduration of friction between the drill and the bone. Data from the lit-erature are insufficient, but general conclusion is that influence of thedrilling axial force on the feed rate can significantly contribute to thereduction of the drilling time and subsequently heat production(Udiljak et al., 2003). Reingewirtz found that (at drill speeds of 400and 800 rpm) increase in pressure (0.8, 1.3 and 2 kg) only slightly in-creases temperature, but it significantly decreases drilling time, andits function has been represented as a reciprocal of the square of theload (Reingewirtz et al., 1997). Kalidindi similarly concluded thatthe increase of the axial load and feed rate decreases drilling time, ifthe drilling depth is constant (Kalidindi, 2004). The results of somestudies show that as drilling force increases, not only does the durationabove 50 °C decrease, but also maximum temperatures are lower(Bachus et al., 2000). Nam et al. proposed that the optimal conditionsduring the experimental testing are combination of low speed(600 rpm) and high pressure (1000 g), and high speed (1200 rpm) andlow pressure (500 g) which produced temperature rise to 40–45 °C(Nam et al., 2006). Augustin et al. pointed out that higher feed ratecauses lower increase in bone temperature. However, for the deliveredcombination of parameters that are used in orthopedics/traumatologyit is not clinically important as an isolated parameter (Augustin et al.,2007).
3.6. Drilling energy, power and efficiency
One of the major problems is the lack of consistency in the litera-ture. Minority of studies included majority of factors important forbone drilling. Amongst these there are still great differences in exper-imental setup and examination of these factors. Temperature rise, asone of the unfavorable effects of bone drilling, is good predictor ofoutcome; often it cannot be compared between studies with differentexperimental setup. In engineering papers drilling energy, power andefficiency are often used to compare different factors regarding drilling,
mpirical fit to the experimental data which serves merely as a guide. b) Influence of thection to the experimental data (Reingewirtz et al., 1997).

Fig. 6. External (a) and internal (b) cooling approaches (Eyup and Babur, 2007).
318 G. Augustin et al. / Clinical Biomechanics 27 (2012) 313–325
but because of specificity ofmetal machining, generally these are not ap-plicable in bone drilling. In medical literature there are a few articles onthe subject. Specific cutting energy is defined as the energy expendedperunit volume of material removal (Wiggins and Malkin, 1976). Power isthe measure of how much work (energy) can be done in a specifiedtime. Power of a drilling machine is calculated as a product of drillingspeed (in rpm) and torque. Torque is defined as a force around a givenpoint, applied at a radius from that point. This means that the torquerises with drill diameter. Mechanical efficiency is a ratio of actual workoutput to ideal work output expressed as a percentage. This means thatsome of the work put into the system is transformed (lost) into thermalenergy (heat). In a mechanical system, friction is common cause of heatproduction.
Jacob et al. measured drill torque and thrust (axial force) to compareseveral commercially available and experimental drill point geometriesusing different feed rate and drill speed. Higher forcesmeanmore ener-gy delivered during drilling, for the same effect (planned drilling hole),deliveringmore heat to the bone. The drawback is that temperature risemeasurements were not carried out, to correlate with the results. Inclinical bone drilling thrust is varied by surgeon, and higher feed rateis desired (Jacobs et al., 1976). Experiments using six different types ofdrills at high and low speeds showed peak vertical force variations be-tween 5.98 and 24.32 N and mean vertical forces between 4.22 and18.93 N. Spear point and twist drills were associated with significantlylower operating pressures and shorter operating times than round andfissure burs. These differences, however, were much less than the inter-operator variations (Hobkirk and Rusiniak, 1977). Wiggins and Malkinmeasured feed rate (mm/rev) for given thrust, comparing commercialdrill bits for metal, standard surgical and one experimental. They alsodescribed dependence of torque and specific cutting energy on feedrate, and showed that both are higher at smaller feed rates, meaningmore heat generated. Authors noticed that specific cutting energy andtorque risewith hole depth,which is explained by clogging of the flutes.Their final conclusion was that performance depends primarily on drillbit. Temperature rise was not measured (Wiggins and Malkin, 1976).Bachus et al. determined that for the same drilling conditions higherthrust produces less heat. This is accomplished by reaching maximumdrill feed rate and minimum drilling time. Torque was not measuredand different drills and other drilling conditions were not compared(Bachus et al., 2000). Karmani and Lam focused on design of surgicaldrill bits and showed that an optimum rake angle facilitates cutting, de-creases deformation of material cut by the tool, improves chip flow andreduces specific cutting energy. Increasing the positive rake angle de-creases the principal cutting force for bone drills, increasing their cut-ting efficiency (Karmani and Lam, 2004). Ercoli et al. showed that drilldesign, material, and mechanical properties significantly affect cuttingefficiency and durability. Among several types of drills tested, 2-mmtwist drill with a low hardness exhibited plastic deformation at thecutting edge, loss of cutting efficiency, and drill fracture; and theTiN-coated drills showed greater wear and significantly lower removalrates (Pb0.05) than noncoated drills (Ercoli et al., 2004).
3.7. Cooling systems
There are many studies in engineering journals considering cool-ing in which different cooling systems and cooling conditions arecompared, but medically applicable data are still insufficient (Eyupand Babur, 2007).
Cooling systems could simply be divided as:
1) Internal cooling systemsa) closed typeb) open type
2) External cooling systems
Internal cooling systems are those inwhich cooling fluid or pressurizedair courses through the drill. Closed type is when fluid/air streams
through a continuous system of tubules through the drill bit up to thetip of the drill bit and back to the cooling container. There is no contactbetween the bone and the coolant. Cooling is achieved only by heattransfer from drill periphery to the center where cooling tubules areplaced. Open type is when coolant exits from the tip of the drill bitthrough holes to the operational field with direct contact of drill tip,coolant and bone (Fig. 6).
External cooling systems deliver fluid/air on the external wall of thedrill and bone from the device that is detached from the drill itself.This is achieved either with automated systems with continuous cool-ing (where flow can be regulated) or manually with simple syringecontaining isotonic fluid (Fig. 6). There are two additional functionsof cooling fluid, which add in temperature reduction: irrigation andlubrication. Irrigation is important in enhancing elimination of bonedebris and chips thus indirectly causing reduction of friction. Lubrica-tion is well described in engineering articles (Rui et al., 2007), wherelubricants are engineering oils, not applicable in medicine. Lubrica-tion properties of medically applied fluids are mentioned in some ar-ticles, but not scientifically tested. It is known that every fluid despiteits viscosity causes reduction in friction. Both irrigation and lubrica-tion cannot be achieved using closed internal coolant systems. Also,there are several limitations of external coolant systems. Limitationis the unknown depth of cooling fluid infiltration. The acceptable ex-planation is that when the drill is in the bone only part of the drilloutside the bone is in contact with coolant thus the warmest part ofthe drill (and the bone) is cooled only indirectly and on the surface.Also the part of the drilling process which causes friction (drill andbone contact) are not lubricated therefore this is also ineffective inlowering the friction. External cooling is partly efficient in preventionand elimination of clogging of drill bit flutes. Study by Matthews andHirsch show that the higher the irrigation rate for external cooling thelower the bone temperature. The irrigation rate of 500 ml/min isadequate for lowering the bone temperature below 50 °C which isnear critical level of 47 °C (Matthews and Hirsch, 1972). The most effi-cient method is open type of internal coolant systems when the flutesare cleansed with the fluid from the tip which is studied in dentistryand oral andmaxillofacial surgery but not in traumatology/orthopedics.
Kirschner and Meyer (1975) introduced internally cooled drills todental surgery in 1975. They used open type internal cooling and con-cluded that since the coolant entered closer to the tip of the drill, itwould create a combined rinsing and cooling effect on the bone, whichwould be superior to the externally cooled drill or a drill with no coolantat all. Haider et al. (1993) conducted histological and histochemical com-parison of internal and external cooling systems in vivo on sheep. Basedon the percentage of newly formed bone-to-implant contacts, externalcooling proved superior at all superficial drill hole levels in compactbone and in all spongy bone beds, while internal cooling was only better

319G. Augustin et al. / Clinical Biomechanics 27 (2012) 313–325
at the deeper drill hole levels in compact bone. Kalidindi (2004) com-pared external cooling to no cooling at all, and observed significant tem-perature rise without cooling. Sharawy et al. (2002) concluded that heatgeneration decreases with drilling speed, regardless the cooling systemused. Lavelle andWedgwood (1980)made an in vitro studyusing low ro-tational speeds and observed that frictional heat generated during bonedrilling was reduced by internal irrigation compared with external or noirrigation. One of the recent articles by Augustin et al. (2007) found thatirrigation evenwithwater at 26 °C is the single, most important factor indecreasing the increase in bone temperature during drilling. There wasno internal cooling system used in this article so there was no compari-son of various cooling systems.
Considering internal cooling there is one more question that im-poses: is it suitable for adequate sterilization? The study of Proff etal. aimed to examine the effects of disinfection and sterilization of in-ternally cooled drills. After contamination of the cooling channel withsuitable bio indicators (Enterococcus faecium and spores of Bacillusstearothermophilus), the drills were disinfected and autoclaved. Au-thors conclude that internally cooled drills can be successfully disin-fected by means of this hygienic procedure routinely used in dentalpractice and no source of infection is created (Proff et al., 2006). Similarquestion is raised with the use of external coolant systems. When thedrill rotates and the fluid is delivered on its surface the centrifugalforce causes sprinkling of drops and droplets to the surrounding space.These drops and droplets could bounce from the non-sterile surroundingobjects into the sterile operative field. Similar physical phenomenon ispresent in open type of internal cooling system but the advantage isthat this type of cooling system is more efficient in eliminating bonechips and lowering friction and bone temperature during drilling.
Recent work by Sener et al. (2009) showed that lower coolanttemperature causes lower increase in bone temperature during dril-ling. They examined effects of external cooling with salines at 25 °Cand 10 °C retrospectively. They also concluded that, since more heatis generated in the superficial part of a cavity, owing to the effectsof the compact and spongious components of bone, external irrigationat room temperature can provide sufficient cooling during drilling tokeep the temperature below the critical value of 47 °C. This results aresimilar to results obtained by Augustin et al. (2007). Both studies didnot compare external to internal cooling.
3.8. Drilling depth
The higher the drilling depth the higher the increase in bone tem-perature! Cordioli and Majzoub (1997) reported a significant increasein temperature at depths of 8 mm versus 4 mm, regardless of the di-ameter of the drill used and regardless of the presence of cooling.Temperature increase concerning depth was dependant on drill de-sign (more for the twist drill than for the triflute drill). However,Tehemar (1999) emphasizes that when using open type of internalcooling, influence of the drilling depth on temperature rise is not animportant factor. Kalidindi (2004) concluded that increase of drillingdepth increases the time of contact between thework piece and drillingtool, which causes overall increase in friction resulting in higher heatgeneration. Cooling effect was not studied.
3.9. Predrilling
Predrilling is the procedure where drilling diameter is increasedgradually using a series of drills from the smallest to the largest diam-eter through the same hole. Idea of incremental drilling is to graduallywiden the drilling site, and thus enhance better dissipation of heat.Predrilling decreases friction when drilling with final diameter. Alsothere is less debris to expel, which also influence on temperaturerise. Adverse effect is extended total drilling time, extending the op-eration time. Also when drilling with hand operated drills, problemswith maintaining the same direction of pre-drilled hole could be
expected. Predrilling was described by Matthews and Hirsch (1972)and popularized by Branemark (1983). The same conclusions weremade by others (Itay and Tsur, 1983; Matthews et al., 1984). Reinge-wirtz (Reingewirtz et al., 1997) did not found significant influence ofpredrilling on temperature, but decreased the drilling time with finaldiameter drill. Kalidindi (2004) confirmed that the maximum tem-perature obtained during incremental drilling is far less than drillinga large diameter hole at a single stretch. Predrilling is not usedroutinely in clinical settings.
3.10. Cortical bone thickness
Cortical bone is the hardest part of the bone. The duration of bonedrilling depends on the cortical bone thickness. The hardness of corti-cal bone correlates to bone mineral density (BMD) and higher theBMD the higher the bone temperature with the same combinationof drilling parameteres (Karaca et al., 2011). The topic is more impor-tant because for stabile osteosynthesis both cortical bones should bedrilled for the fixation of osteosynthetic material. Thickness of rabbitcortical bone is 1.5 mmwith average duration of drilling of 5 s; corticalbone thickness of the femur of a dog is 3.5 mmwith average duration ofdrillign of 15 s and cortical bone thickness of human femur is 6–6.5 mmwith average duration of drilling of 18 s (Eriksson et al., 1984a, 1984b).
4. Temperature measurement
Heat is thermal energy transferred between a system and its sur-roundings. The heat transfer can take place by three differentmechanisms:
• Conduction — Thermal energy is transferred through the substanceof the system.
• Convection — Thermal energy is transferred by relative motion ofcomponents of the system.
• Radiation— Thermal energy is transferred directly between separat-ed parts of the system by electromagnetic radiation.
The heat generated during drilling of bone comes from the drillingprocess. Shear of the surface layer of a material by a drill bit breaksintermolecular bonds releasing energy in form of heat. Secondly, fric-tion from the non-cutting surfaces of a drill, such as the flank, flutesand shaft are another source of heat. The temperature developedwithin a section of bone tissue depends on specific heat capacity(how readily a material heats up) and on the thermal conductivity(how readily a material transfers heat from a source). When a heatsource is applied to a specimen, a thermal gradient exists from thehotter heat source to the cooler specimen. Heat is transferred downthis gradient. The higher the gradient the greater the rate of transfer.Heat continues to transfer as long as the gradient is maintained. Theultimate temperature a specimen develops depends on the balancebetween heat gain and heat loss. When these two phenomena areequal, the specimen is in a state of equilibrium. In the equilibriumstate the temperature reached by a specimen is a function of the expo-sure temperature and thermal conductivity. Temperature equilibriumis, however, not normally reached when biological tissues are exposedto heat in a clinical situation such as drilling, as the exposure timesare usually too short. The temperature reached in the non-equilibriumstate of short exposures is a function of the exposure temperature andtime, the specific heat capacity being constant (Lundskog, 1972).
Generally there are two methods used for temperature measure-ment of bone during drilling: either with thermocouples or with infra-red thermographic camera. Few articles used both methods, wherethe images obtained from infrared thermographic camera are utilizedas a template to place thermocouples (Kalidindi, 2004), but there areno studies comparing these methods.
Thermocouple is commonly used sensor for direct temperaturemeasurement. It is a device consisting of two different conductors

320 G. Augustin et al. / Clinical Biomechanics 27 (2012) 313–325
(usually metal alloys) that produce a voltage proportional to a tem-perature difference between either ends of the pair of conductors.Types of thermocouples depend upon composing metals which dic-tate a temperature range and sensitivity. Thermocouples with lowsensitivities (B, R, and S types) have correspondingly lower resolu-tions. For instance J-type of thermocouple (iron–constantan) has a rela-tively restricted range (−40 to +750 °C), but relatively high sensitivityof about 55 μV/°C. Thermocouple can be placed in drill bit butmore oftenin the bone near the drilling site (Fig. 7). Two or more thermocouplescan be placed simultaneously due to bone anisotropy (Hillerya andShuaib, 1999) or due tomeasurement of temeperature gradient throughthe bone. Usually thermocouples are placed 0.5 and 1 mm from drillingsite, which is suitable for comparing results. Sharawy et al. (2002) usedfour thermocouples at the samedepth in four orientations from thehole.Frölke et al. (2001) used axial positioning of thermocouples for determi-nation of the gradient in relation to cortical thickness (drilling depth).Davidson and James (Davidson, 1999; Davidson and James, 2000)found that the differences in thermal conductivity between the longitu-dinal and radial directions and between the longitudinal and circumfer-ential directions are statistically significant. There was no significantdifference between the circumferential and the radial directions. Theseexperimental significant differences are not translated into practical sig-nificance, i.e., the difference between the longitudinal direction and theother two directions may not significantly affect the temperatures gen-erated during drilling. For the parametric analysis (one of the parame-ters is varied while all others are held constant and the importance ofthat parameter is determined by measuring the change in thermal im-pact caused by varying that parameter), it was assumed that corticalbone can be treated as thermally isotropic.
To predict the temperature distribution in bone, one should use theequations of unsteady heat conduction which requires knowledge of
Fig. 7. Thermocouple is a device consisting of two different conductors (usually metalalloys) that produce a voltage proportional to a temperature difference between eitherends of the pair of conductors. It is isolated with plastic cap and placed 0.5 and 1 mmfrom drilling site.
the geometry, the heat input, and two thermal properties of bone: spe-cific heat and thermal conductivity. To avoid aforementioned parame-ters and ensuing errors in measurements, infrared thermographiccamera was used, first at the DaimlerChrysler Research Centre, Ulm infor examination of the quantitative temperature distribution and thecorresponding wear behavior of diamond coated tool inserts duringmachining Fe-based alloys (Müller-Hummel and Lahres, 1994). First or-thodontic use was in 2006 with micro-implant placement using bovineribs to provide cortical bone of a similar quality to the humanmandible(Nam et al., 2006). Thermography is more suitable method to demon-strate 2D image of temperature spread throughout the bone (Augustinet al., 2009). Combining two thermographic cameras placed in rightangle, cannot produce 3D images. Combining two cameras onemay re-construct 3D images that still shows the surface temperature, althoughit is a 3D surface. Disadvantage of thermography is that it is indirect andabsolute values of temperature in particular point of bone could only beextrapolated. Thermographic values should be calibrated thus thermalcouple may still be required. Augustin et al. used single thermographiccamera (Augustin et al., 2009) and showed that increase in bone tem-perature spreads through cortical bone, which is compact and densepart, and generates highest frictional heat during drilling. The medullarcavity, because of its gelatinous structure, contributes only to thermaldissipation (Fig. 8). Another setup is simultaneous determination ofmaximum temperatures occurring on the tip of the drill and the work-piece (bone) during drill insertion (Fig. 9) and is currently used in drymachining of metals (Dörr et al., 2003).
Further issue is the experimental set-up. Few experiments areconducted intraoperatively on humans, as in study of intramedullaryreaming, when thermocouples were percutaneously introduced intothe cortical bone at the short isthmic segment of the tibial shaft(Giannoudis et al., 2002). Similar experimental set-up is more oftendone on animals, for instance dogs (Karunakar et al., 2004), and mini-pigs (Riquelme Garcia et al., 2004.). Series of experiments are done onanimal bone specimens in vitro, for example bovine bone (Chacon etal., 2006.). Question is: Is human bone the same as the animal bone?Aerssens et al. (1998) demonstrated large interspecies variations.The lowest bone density and fracture stress values were found in thehuman samples; porcine and canine bone best resembled these sam-ples. Some authors (Eriksson et al., 1984a, 1984b; Saha et al., 1982)described differences between human and bovine bone with themost influential differences in the bone cortex width. Lundskog gavea comprehensive overview on bone thermal properties of differentspecies (Lundskog, 1972). Even differences between sexes are pre-sent: Karaca et al. (2011) showed that the drilling temperatures ofthe female bovine tibias are higher than themale tibias. Also, the problemis disparity of human cadaveric bone specimens. In order to avoid differ-ences in human bone density and shape depending upon gender, age andother factors, Kalidindi (2004) compared poly(methyl methacrylate)(PMMA) to human bone due to similar thermal conductivity (0.2 W/mK) and slightly different thermal diffusivity (bone 0.3∗10−6 m2/s;PMMA 0.11∗10−6 m2/s). Temperature rise in human bone and PMMAis similar but the maximum temperature is higher for bone comparedto PMMA. This is due to higher thermal diffusivity of bone due to higherdensity values of bone (1860–2900 kg/m3) compared to PMMA(1400 kg/m3) (Huiskes, 1980). There is 15–20% increase in maximumtemperature for human bone compared to PMMA. Despite these differ-ences Kalindindi concluded that PMMA properties are satisfying forbone drilling research. Frölke et al. (2001) used polycarbonate as a sub-stitute for human bone.
Some experiments are done in the container that was filled withphysiologic saline solution with heater and thermostat, so baselinetemperature is held constant (Bachus et al., 2000; Chacon et al.,2006). Authors claim that saline solution aids in heat transfer andeliminates dead space. Orthodontic wax was placed over the hole toact as a sealant and to prevent any irrigation fluid from entering thehole, which could affect temperature readings. Drawback of saline
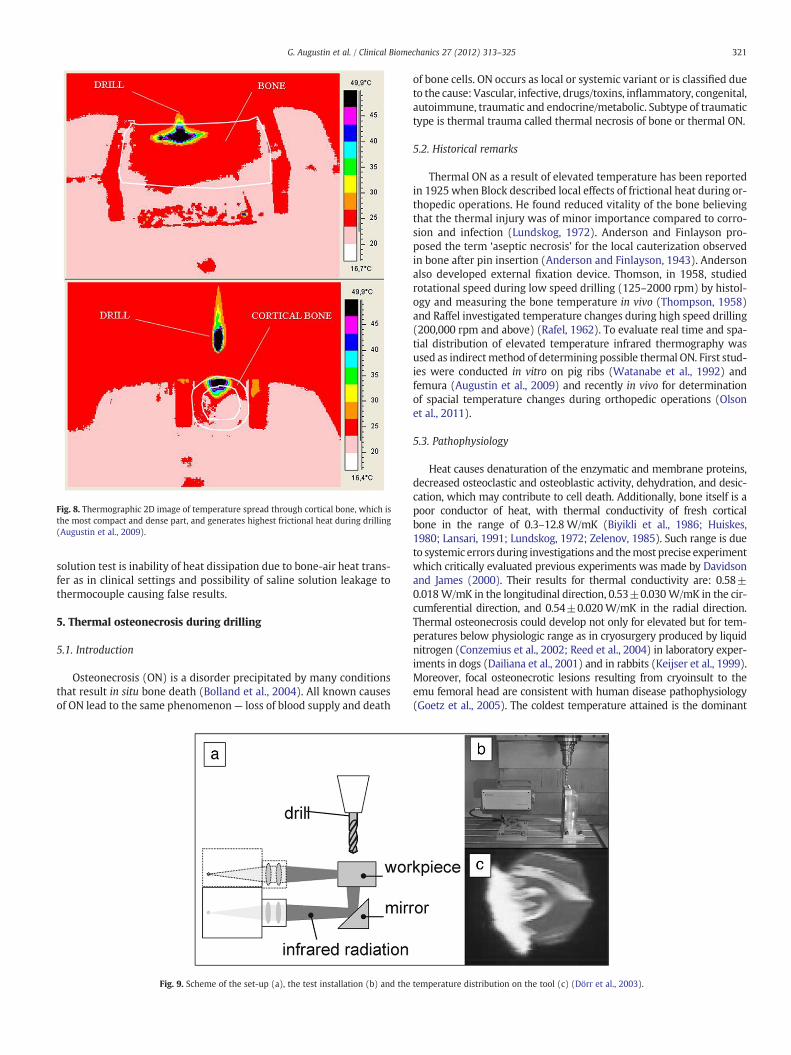
Fig. 8. Thermographic 2D image of temperature spread through cortical bone, which isthe most compact and dense part, and generates highest frictional heat during drilling(Augustin et al., 2009).
321G. Augustin et al. / Clinical Biomechanics 27 (2012) 313–325
solution test is inability of heat dissipation due to bone-air heat trans-fer as in clinical settings and possibility of saline solution leakage tothermocouple causing false results.
5. Thermal osteonecrosis during drilling
5.1. Introduction
Osteonecrosis (ON) is a disorder precipitated by many conditionsthat result in situ bone death (Bolland et al., 2004). All known causesof ON lead to the same phenomenon— loss of blood supply and death
Fig. 9. Scheme of the set-up (a), the test installation (b) and the
of bone cells. ON occurs as local or systemic variant or is classified dueto the cause: Vascular, infective, drugs/toxins, inflammatory, congenital,autoimmune, traumatic and endocrine/metabolic. Subtype of traumatictype is thermal trauma called thermal necrosis of bone or thermal ON.
5.2. Historical remarks
Thermal ON as a result of elevated temperature has been reportedin 1925 when Block described local effects of frictional heat during or-thopedic operations. He found reduced vitality of the bone believingthat the thermal injury was of minor importance compared to corro-sion and infection (Lundskog, 1972). Anderson and Finlayson pro-posed the term ‘aseptic necrosis’ for the local cauterization observedin bone after pin insertion (Anderson and Finlayson, 1943). Andersonalso developed external fixation device. Thomson, in 1958, studiedrotational speed during low speed drilling (125–2000 rpm) by histol-ogy and measuring the bone temperature in vivo (Thompson, 1958)and Raffel investigated temperature changes during high speed drilling(200,000 rpm and above) (Rafel, 1962). To evaluate real time and spa-tial distribution of elevated temperature infrared thermography wasused as indirectmethod of determining possible thermal ON. First stud-ies were conducted in vitro on pig ribs (Watanabe et al., 1992) andfemura (Augustin et al., 2009) and recently in vivo for determinationof spacial temperature changes during orthopedic operations (Olsonet al., 2011).
5.3. Pathophysiology
Heat causes denaturation of the enzymatic and membrane proteins,decreased osteoclastic and osteoblastic activity, dehydration, and desic-cation, which may contribute to cell death. Additionally, bone itself is apoor conductor of heat, with thermal conductivity of fresh corticalbone in the range of 0.3–12.8 W/mK (Biyikli et al., 1986; Huiskes,1980; Lansari, 1991; Lundskog, 1972; Zelenov, 1985). Such range is dueto systemic errors during investigations and themost precise experimentwhich critically evaluated previous experiments was made by Davidsonand James (2000). Their results for thermal conductivity are: 0.58±0.018W/mK in the longitudinal direction, 0.53±0.030W/mK in the cir-cumferential direction, and 0.54±0.020W/mK in the radial direction.Thermal osteonecrosis could develop not only for elevated but for tem-peratures below physiologic range as in cryosurgery produced by liquidnitrogen (Conzemius et al., 2002; Reed et al., 2004) in laboratory exper-iments in dogs (Dailiana et al., 2001) and in rabbits (Keijser et al., 1999).Moreover, focal osteonecrotic lesions resulting from cryoinsult to theemu femoral head are consistent with human disease pathophysiology(Goetz et al., 2005). The coldest temperature attained is the dominant
temperature distribution on the tool (c) (Dörr et al., 2003).

Fig. 10. Histological appearance of intact (200×) and traumatized (400×) sections ofbone depicting the vascular response. Arrow points to material observed blocking thevessels in the traumatized bone (Field and Sumner-Smith, 2002).
322 G. Augustin et al. / Clinical Biomechanics 27 (2012) 313–325
parameter for local tissue necrosis during single cryoinsult events andthe absolute value is 2–4 °C (Goetz et al., 2008). Detailed analysis onthe thermal effects of cryosurgery on selective cell destruction is pre-sented by Chua et al. which is beyond the scope of this review (Chua etal., 2007).
A precise threshold temperature for thermal ON of human bone isstill unclear. The cellular death caused by heat is immediately evidentwith temperatures above 70 °C (Berman et al., 1984). Lundskog(1972) performed biomechanical, histochemic andmorphologic studieson vital rabbit bone. Demonstrated threshold for irreversible enzymaticdisturbance to cortical bone was 50 °C during 30 s. Bonfield and Lireported irreversible bondweakening of the bone–collagen hydroxyap-atite complex at 50 °C (Bonfield and Li, 1968). Eriksson and Albrektssonheated threaded titanium implants in the vital rabbit tibia and foundthat heating the implants to a temperature of 50 °C for 1 min was suffi-cient to cause 30% of the bone to be resorbed. Thiswas not an immediateoccurrence but a slow-developing process over a period of 4 weeks. Thebone was replaced with fat cells, preventing implant incorporation(osseointegration). The same study demonstrated that heating bone to47 °C for 1 min reduced the amount of bone that grew into the porousimplant. ON was detected with histology using the absence of filled os-teocyte lacunae orwith histochemistry as a lack of oxidative enzyme ac-tivities, respectively. In both cases a wider necrotic border zone wasdetected with histochemistry than with histology. Authors establishedthe threshold level for bone survival during implant site preparation of47 °C, keeping the drilling time below 1 min (Eriksson and Adell,1986; Eriksson and Albrektsson, 1982, 1984; Eriksson et al., 1984a,1984b).
Ochsner et al. described four grades of thermal ON as a conse-quence of intramedullary reaming: Grade 0: no damage; no devascu-larization, no heat induced damage; Grade 1: The heat damaged zoneis cut away during subsequent reaming, the only damage is devascu-larization; Grade 2: The damaged zones are not eliminated by subse-quent reaming. The bone is devascularized and heat damaged; andGrade 3: The entire cross section of the bone including the perioste-um is devitalized by exposure to excessive heat. Depending on the se-verity of additional damage to the soft tissues, grave consequencesare to be expected and further operations are unavoidable. The effectsof heat-induced damage are particularly critical in the presence of in-fection (Ochsner et al., 1998). Later articles (Giannoudis et al., 2002;Karunakar et al., 2004) described clinical practice of limited reaming(‘ream-to-fit’), which should minimize the occurrence of this compli-cation. They also concluded that the risk of thermal ON appears to berelated more to the process of intramedullary reaming than to thetourniquet. Also increasing the time interval between the passagesof successive reamers may allow heat to dissipate and decrease therisk of thermal ON.
ON is a dynamic process that takes several weeks. First noticedchange is osteocyte depletion and blood flow reduction, which arefollowed by osteoclastic resorption. Osteoclastic resorption plays acentral role in the regulation of bone mass and architecture. More-over, osteoclast resorption is a prerequisite to maintaining the struc-tural health of cortical and cancellous bone by removing aged tissueand by initiating the repair of bone micro damage. Conversely, hyper-active osteoclasts and excessive bone resorption can lead to irreversiblebone loss and structurallyweakened bone (Baron andHorne, 2005). ONassociated with drilling is a complex process. Besides thermal injurymicro-damage (microcracks) should be considered caused by drilling.It is described that micro-damage could produce osteocytes apoptosisand that is the signal for ostoclasts activation and bone resorption(Noble, 2003).
5.4. The difference between in vivo and in vitro measurement
Skeletal blood flow is present in clinical experiments. There isblood flow response to surgical trauma. Field and Sumner-Smith
(2002) analyzed bone blood flow response to bone drilling andfound a profound ischaemia immediately adjacent to the drilledholes. It may be a response to thermal changes in response to drillingwhich leads to protein coagulation (Fig. 10). Also it may be a responseto vascular or lymphatic blockage as a result of drill fine accumula-tion, or a result of a regional vasoconstriction in response to the sur-gical insult. Disulphine blue (Fig. 11) and India ink distribution(Fig. 12) have both revealed a regional orientation of perfusion defi-ciency, directly related to the drilled holes. These findings supportthe proposal of a acute (within 30 min) obstruction in cortical bloodflow which may contribute to later adaptational osteopaenia follow-ing bone plate application (Field and Sumner-Smith, 2002). Regionalperfusion is additionally diminished by fracture itself causing inter-ruption of local arterial blood supply which can contribute to largerextent of thermal osteonecrosis. Cortical bloodflow in vivo may dissi-pate some heat produced by drilling during operative procedure butthis effect is unlikely to be significant. Minute cortical bloodflow islow (2–3 ml/100 g) and during drilling coagulation and occlusion ofthe small vessels occurs rapidly (Wootton et al., 1976). Mathewsand Hirsch compared temperatures generated when drilling humanfemora in vivo and in vitro and found them to be equivalent (Matthewsand Hirsch, 1972), the result that confirms non significant influence ofskeletal blood flow on bone temperature during drilling.
6. Future directions
This review analyzes the most influential factors on heat genera-tion during bone drilling, and summarizes general standpoints ofmedical research. There are still some controversies, which will be amaterial for future experiments. Also there are some factors whichare still unknown, or insufficiently examined.

Fig. 11. Disulphine blue perfusion of intact and traumatized metatarsal bones. Arrowsdepict the segmental ischaemia apparent and its proximity to the drilled holes (Fieldand Sumner-Smith, 2002).
323G. Augustin et al. / Clinical Biomechanics 27 (2012) 313–325
Drill guide. A conclusion of study by Misir et al. (2009) is that prep-aration of an implant site using surgical drill guide generates moreheat than preparation without drill guide regardless of the irrigationtype. Explanation is that 1) drill guide iteslf prevents the contact ofthe drill and coolant and 2) contact between the drill and drill guidedue to friction could elevate drill temperature.
Coated drills. Coated cutting tools have several advantages overstandard medical stainless steel. For example, the advantages of lowfriction chromium (LFC) coating include: 1) the high hardness im-prove abrasion and wear resistance which helps tools maintain asharp edge; 2) application to precision instruments without fear ofdistortion of the work piece; 3) application as a final process, therebynegating the need for subsequent machining; 4) LFC coating thick-ness can be precisely controlled for different end uses; 5) applicationuniformly to all surfaces, including recesses and hole cavities; 6) re-sistance to oxidation and discoloration and maintainance of their
Fig. 12. India ink specimen displaying a similar pattern of perfusion disruption(arrows), to that seen with disulphine blue, in drilled bone (Field and Sumner-Smith,2002).
luster even after cycles of high temperature autoclave treatment;7) resistance to chloride-pitting corrosion common to uncoated stain-less steels; 8) tight adherence to the base metal and 9) much lowercoefficient of friction than steel and other metals, which can help de-crease heat generation in applications involving sliding contact of twosurfaces (Paciorek, 2003).
Robotics and navigation systems. Most of the drilling in traumatology/orthopedics is done by handdrills and drilling depends, on great extend,on the surgeon'smanual skills and ‘drilling by feeling’. The required coreskills are: recognizing the drilling endpoint, ability of applying constant,sufficient, but nonexcessive feeding rate and thrust force. The use of ro-botics and navigation systems would have a significant role eliminatingor minimizing human error. Hüfner et al. (2005) determined relevantaccuracy of CT-based navigation for drilling. Twelve drills of varyinglengths and diameters were tested with 2 different set-ups. Testedgroup used free-hand navigated drilling technique with foam blocksequipped with titanium target points. Control group used newly devel-oped 3-dimensional measurement device equipped with titanium tar-get points with a fixed entry for the navigated drill to minimizebending forces. Examiner performed 690 navigated drillings using solelythe monitor screen for control in both groups. The core accuracy of thenavigation system is high as measured with guided drilling using the3-dimensional device. Free-hand navigated drilling is not always accu-rate and the display of the drill bit on the monitor screen of the naviga-tion system may not represent reality. The precision is decreased whenusing smaller diameter (up to 3.2 mm) and longer drill bits.
Simulators and training systems. Esen et al. focused on develop-ment of bone drilling simulators and training systems (Esen et al.,2003). A graphical user interface is developed to complete a medicaltraining system structure. Experimental results for controller perfor-mance are satisfactory. Additional experiments are performed to checkif the developed system improves the skill of trainees or not. Early resultssuggest that training in the developedmedical training system is a prom-ising way to teach drilling into a bone to medical students.
Automated bone drilling. Hsu et al. proposed system which stopsthe penetration of drill point when completing a hole. It is a modularmechatronic system for automated bone drilling. The development ofa “modular system” that is compatiblewithmotor-driven drills, that arecommercially available, rather than developing a new surgical drill, isemphasized. A fuzzy controller analyzes the electric current consumedby the DC motor of the drill. When break-through is detected, thepower will be cut and stops drilling in order to prevent excessive pro-trusion of the drill bit. In extensive drilling tests on real human skulls,there were no unexpected failure, and the overshoots of all tests werewell less than 2 mm (Hsu et al., 2001).
Ultrasonically assisted drilling. This system utilize high-frequencyultrasonic vibration of the drill along its longitudinal axis and im-proves the process of drilling minimizing the invasiveness of the op-eration. Alam et al. (2009) compared surface roughness of holesdrilled in the bovine cortical bone using two methods: conventionaland ultrasonically assisted bone drilling. The surface texture indicatedthat the hole surface produced by ultrasonically assisted drilling wassomewhat smoother than that obtained with conventional drilling.
Low initial drill temperature. In the study by Tu et al. (2009) dynamicelastic–plastic finite element model was used to simulate a process of aKirschner pin drilling through the bone. The results indicate that lower-ing the initial temperature of Kirschner pin can decrease the tempera-ture rise of a drill itself as well as the surrounding zone. Thermalconductivity (in average 14×higher) and thermal diffusivity (in average30× higher) values of stainless steel compared to cortical bone confirmthe possibility of this concept (Huiskes, 1980). It is not known whetherthis wide range of temperature changes during drilling has an effect onchanges of physical properties of the drill or causes changes in drillwear. Temperatures below 3 °C could cause cryoinsult making this adelicate situation: lowering the temperature of the drill for eliminatingthermal osteonecrosis could produce it!

324 G. Augustin et al. / Clinical Biomechanics 27 (2012) 313–325
Conflict of interest
None.
References
Abouzgia, M.B., James, D.F., 1997. Temperature rise during drilling through bone. Int. J.Oral Maxillofac. Implants 12, 342–353.
Abouzgia, M.B., Symington, J.M., 1996. Effect of drill speed on bone temperature. Int. J.Oral Maxillofac. Surg. 25, 394–399.
Aerssens, J., Boonen, S., Lowet, G., Dequeker, J., 1998. Interspecies differences in bonecomposition, density and quality: potential implications for in vivo bone. Endocri-nology 139, 663–670.
Alam, K., Mitrofanov, A.V., Silberschmidt, V.V., 2009. Measurements of surface rough-ness in conventional and ultrasonically assisted bone drilling. Am. J. Biomed. Sci.1, 312–320.
Allan, W., Williams, E.D., Kerawala, C.J., 2005. Effects of repeated drill use on tempera-ture of bone during preparation for osteosynthesis self-tapping screws. Br. J. OralMaxillofac. Surg. 43, 314–319.
Anderson, R., Finlayson, B.L., 1943. Sequele of transfixation of bone. Surgery 13, 46–54.Anderson, D., Van Proagh, G., 1942. Preliminary investigation of the temperature pro-
duced in Burring. Br. Dent. J. 73, 62–68.Arvajeh, T., Ismail, F., 2006. Machining stability in high-speed drilling—part 1: modeling
vibration stability in bending. Int. J. Mach. Tool Manuf. 46, 1563–1572.Augustin, G., Davila, S., Mihoci, K., Udiljak, T., Vedrina, D.S., Antabak, A., 2007. Thermal
osteonecrosis and bone drilling parameters revisited. Arch. Orthop. Trauma Surg.128, 71–77.
Augustin, G., Davila, S., Udiljak, T., Vedrina, D.S., Bagatin, D., 2009. Determination ofspatial distribution of increase in bone temperature during drilling by infraredthermography: preliminary report. Arch. Orthop. Trauma Surg. 129, 703–709.
Bachus, K.N., Rondina, M.T., Hutchinson, D.T., 2000. The effects of drilling force on cor-tical temperatures and theirduration: an in vitro study. Med. Eng. Phys. 22,685–691.
Baron, R., Horne, W.C., 2005. Bone resorption. In: Bronner, F., Farach-Carson, M.C.,Rubin, J. (Eds.), Topics in Bone Biology. Springer, London.
Bechtol, C.O., 1956. A modified hand drill. J. Bone Joint Surg. Am. 38A, 691–692.Bechtol, C.O., Ferguson, A.B., Laing, P.G., 1959. Metals and engineering in bone and joint
surgery. Williams & Wilkins, Baltimore.Berman, A.T., Reid, J.S., Yanicko, D.R., Sih, G.C., Zimmerman, M.R., 1984. Thermally in-
duced bone necrosis in rabbits: relation to implant failure in humans. Clin. Orthop.186, 284–292.
Bertollo, N., Gothelf, T.K., Walsh, W.R., 2008. 3-Fluted orthopaedic drills exhibit superiorbending stiffness to their 2-fluted rivals: clinical implications for targeting abilityand the incidence of drill-bit failure. Injury 39, 734–741.
Bertollo, N., Milne, H.R.M., Ellis, L.P., Stephens, P.C., Gillies, R.M., Walsh, W.R., 2010. Acomparison of the thermal properties of 2- and 3-fluted drills and the effects onbone cell viability and screw pull-out strength in an ovine model. Clin. Biomech.25, 613–617.
Biyikli, S., Modest, M.F., Tarr, R., 1986. Measurements of thermal properties for humanfemora. J. Biomed. Mater. Res. 20, 1335–1345.
Bolland, M.J., Hood, G., Bastin, S.T., King, A.R., Grey, A., 2004. Bilateral femoral headosteonecrosis after septic shock and multiorgan failure. J. Bone Miner. Res. 3,517–520.
Bonfield, W., Li, C.H., 1968. The temperature dependence of the deformation of bone.J. Biomech. 1, 323–329.
Boyne, P.J., 1966. Histologic response of bone to sectioning by high-speed rotary instru-ments. J. Dent. Res. 45, 270–276.
Branemark, P.I., 1983. Osseointegration and its experimental background. J. Prosthet.Dent. 50, 399–410.
Brisman, D.L., 1996. The effect of speed, pressure, and time on bone temperature duringthe drilling of implant sites. Int. J. Oral Maxillofac. Implants 11, 35–37.
Burstein, A., Currey, J., Frankel, V., Heiple, K., Lunseth, P., Vessely, J., 1972. Bonestrength, the effect of screw holes. J. Bone Joint Surg. Am. 54A, 1143–1156.
Canteroa, J.L., Tardío, M.M., Canteli, J.A., Marcos, M., Miguélez, M.H., 2005. Dry drillingof alloy Ti–6Al–4V. Int. J. Mach. Tool Manuf. 45, 1246–1255.
Chacon, G.E., Bower, D.L., Larsen, P.E., McGlumphy, E.A., Beck, F.M., 2006. Heat produc-tion by 3 implant drill systems after repeated drilling and sterilization. J. Oral Max-illofac. Surg. 64, 265–269.
Chua, K.J., Chou, S.K., Ho, J.C., 2007. An analytical study on the thermal effects of cryo-surgery on selective cell destruction. J. Biomech. 40, 100–116.
Conzemius, M.G., Brown, T.D., Zhang, Y., Robinson, R.A., 2002. A new animal model offemoral head osteonecrosis: one that progresses to human-like mechanical failure.J. Orthop. Res. 20, 303–309.
Cordioli, G., Majzoub, Z., 1997. Heat generation during implant site preparation: an invitro study. Journal of Oral and Maxillofacial Implants 12, 186–193.
Cucuel, U., Rigaud, U., 1850. Des Vis Metalliques Enfoncees dans le Tissue des Os, pourle Traitment de Certaines Fractures. Revue de Medecine et Chirurgie Paris 8,113–115.
Dailiana, Z.H., Fink, C., Baust, J.G., Seaber, A.V., Urbaniak, J.R., 2001. Femoral head osteo-necrosis with the use of cryosurgery — a new canine model. 4th Combined Ortho-paedic Research Societies Meeting.
Davidson, S.R.H., 1999. Heat transfer in bone during drilling. A thesis submitted in confor-mity with the requirements for the degree of Master of Applied Science. Graduate
Department of Mechanical and Industrial Engineering. Institute of Biomaterials andBiomedical Engineering, University of Toronto.
Davidson, S.R.H., James, D.F., 2000. Measurement of thermal conductivity of bovinecortical bone. Medical Engineering & Physics 22, 741–747.
Dörr, J., Mertens, Th., Engering, G., Lahres, M., 2003. ‘In-situ’ temperature measurementto determine the machining potential of different tool coatings. Surf. Coat.Technol.174–175, 389–392.
Ercoli, C., Funkenbusch, P.D., Lee, H.J., Moss, M.E., Graser, G.N., 2004. The influence ofdrill wear on cutting efficiency and heat production during osteotomy preparationfor dental implants: a study of drill durability. Int. J. Oral Maxillofac. Implants 19,335–349.
Eriksson, R.A., Adell, R., 1986. Temperatures during drilling for the placement ofimplants using the Osseo integration technique. J. Oral Maxillofac. Surg. 44, 4–7.
Eriksson, R.A., Albrektsson, T., 1982. Thermal injury to bone: a vital-microscopicdescription of heat effects. Int. J. Oral Surg. 11, 115–121.
Eriksson, R.A., Albrektsson, T., 1984. The effect of heat on bone regeneration: an experi-mental study in the rabbit using the bone growth chamber. J. Oral Maxillofac. Surg.42, 705–711.
Eriksson, R.A., Albrektsson, T., Albrektsson, B., 1984a. Heat caused by drilling corticalbone. Acta Orthopedica Scandinavica 55, 629–631.
Eriksson, R.A., Albrektsson, T., Magnusson, B., 1984. Assessment of bone viability afterheat trauma: a histological, histochemical and vital microscopic study in the rabbit.Scandinavian Journal of Plastic and Reconstructive Surgery and Hand Surgery 18,261–268.
Esen, H., Yano, K., Buss, M., 2003. Control algorithm and preliminary user studies for abone drilling medical training system, robot and human interactive communication.Proceedings. ROMAN 2003. The 12th IEEE International Workshop, pp. 153–158.
Eyup, B., Babur, O., 2007. Effects of different cooling conditions on twist drill tempera-ture. International Journal of Advances in Manufacturing Technology 34, 867–877.
Field, J.R., Sumner-Smith, G., 2002. Bone blood flow response to surgical trauma. Injury33, 447–451.
Frölke, J.P.M., Peters, R., Boshuizen, K., Patka, P., Bakker, F.C., Haarman, H.J., 2001. Theassessment of cortical heat during intramedullary reaming of long bones. Injury32, 683–688.
Giannoudis, P.V., Snowden, S., Matthews, S.J., Smye, S.W., Smith, R.M., 2002. Tempera-ture rise during reamed tibial nailing. Clinical Orthopedics and Related Research395, 255–261.
Goetz, J.E., Chung, Y.Y., Zimmerman, D.L., Pedersen, D.R., Robinson, D.A., Conzemius, M.,et al., 2005. Steroid-induced versus cryoinsult-induced femoral head osteonecro-sis: statistical measurement of histologic abnormality focalization. Journal of Mus-culoskeletal Research 9, 161–172.
Goetz, J.E., Pedersen, D.R., Robinson, D.A., Conzemius, M.G., Baer, T.E., Brown, T.D., 2008.The apparent critical isotherm for cryoinsult-induced osteonecrotic lesions in emufemoral heads. J. Biomech. 41, 2197–2205.
Haider, R., Watzek, G., Plenk Jr., H., 1993. Effects of drill cooling and bone structure onIMZ implant fixation. Int. J. Oral Maxillofac. Implants 8, 83–91.
Hansmann, C., 1886. Eine neue Methode der Fixirung der Fragmente bei kompliciertenFrakturen. Verhandlungen der Deutschen Gesellchaft fur Chirurgie, 15, pp. 134–136.
Henschel, C.J., 1943. Heat impact of revolving instruments on vital dentin tubules.J. Dent. Res. 22, 323–333.
Hillerya, M.T., Shuaib, I., 1999. Temperature effects in the drilling of human and bovinebone. J. Mater. Process. Technol. 92–93, 302–308.
Hobkirk, J.A., Rusiniak, K.J., 1977. Investigation of variable factors in drilling bone. OralSurg 35, 968–973.
Hsu, Y.L., Lee, S.T., Lin, H.W., 2001. A modular mechatronic system for automatic bonedrilling. Biomedical Engineering—Applications, Basis and Communications 13,168–174.
Hüfner, T., Geerling, J., Oldag, G., Richter, M., Kfuri Jr., M., Pohlemann, T., et al., 2005. Accu-racy study of computer-assisted drilling: the effect of bone density, drill bit character-istics, and use of a mechanical guide. J. Orthop. Trauma 19, 317–322.
Huiskes, R., 1980. Some fundamental aspects of human joint replacement. Analyses ofstresses and heat conduction in bone–prosthesis structures. Acta OrthopedicaScandinavica 185, 1–208.
Itay, S., Tsur, H., 1983. Thermal osteonecrosis complicating Steinmann pin insertion inplastic surgery. Plastic and Reconstructive Surgery 72, 557–561.
Jacobs, C.H., Berry, J.T., Pope, M.H., Hoaglund, F.T., 1976. A study of bone machining pro-cess — drilling. J. Biomech. 9, 343–349.
Kalidindi V., 2004. Optimization of drill design and coolant systems during dental im-plant surgery, PhD thesis, University of Kentucky.
Karaca, F., Aksakal, B., Kom, M., 2011. Influence of orthopaedic drilling parameters ontemperature and histopathology of bovine tibia: an in vitro study. Medical Engi-neering & Physics 33, 1221–1227.
Karmani, S., 2006. The thermal properties of bone and the effects of surgical interven-tion. Current Orthopaedics 20, 52–58.
Karmani, S., Lam, F., 2004. The design and function of surgical drills and K-wires. CurrentOrthopedics 18, 484–490.
Karunakar, M.A., Frankenburg, E.P., Le, T.T., Hall, J., 2004. The thermal effects of intra-medullary reaming. Journal of Orthopedic Trauma 18, 674–679.
Keijser, L.C., Schreuder, H.W., Buma, P., Weinans, H., Veth, R.P., 1999. Cryosurgery inlong bones; an experimental study of necrosis and revitalization in rabbits. Ar-chives of Orthopedic and Trauma Surgery 119, 440–444.
Kirschner, H., Meyer, W., 1975. Entwichlung einer Innenkuhlung fur chirurgischeBohrer. Dtsch Zahnaztl Zeitschrift 30, 436–438.
Kondo, S., Okada, Y., Iseki, H., Hori, T., Takakura, K., Kobayashi, A., et al., 2000. Thermo-logical study of drilling bone tissue with a high-speed drill. Neurosurgery 46,1162–1168.

325G. Augustin et al. / Clinical Biomechanics 27 (2012) 313–325
Krause, W.R., Bradbury, D.W., Kelly, J.E., Lunceford, E.M., 1982. Temperature elevationsin orthopaedic cutting operations. J. Biomech. 15, 267–275.
Lansari, A., 1991. Effects of torque and heat generation during direct cortical trochartipped pin insertion. Annals of Biomechanical Engineering 19, 6411.
Lavelle, C., Wedgwood, D., 1980. Effect of internal irrigation on frictional heat generatedfrom bone drilling. J. Oral Surg. 38, 499–503.
Lundskog, J., 1972. Heat and bone tissue. An experimental investigation of the thermalproperties of bone and threshold levels for thermal injury. Scand. J. Plast. Reconstr.Surg. 9, 1–80.
Matthews, L.S., Hirsch, C., 1972. Temperatures measured in human cortical bone whiledrilling. J. Oral Maxillofac. Surg. 54, 297–308.
Matthews, L.S., Green, C.A., Goldstein, S.A., 1984. The thermal effects of skeletalfixation-pin insertion in bone. Journal of Bone and Joint Surgery American 66,1077–1083.
Misir, A.F., Sumer, M., Yenisey, M., Ergioglu, E., 2009. Effect of surgical drill guide onheat generated from implant drilling. Journal of Oral and Maxillofacial Surgery67, 2663–2668.
Moss, R.W., 1964. Histopathologic reaction of bone to surgical cutting. Oral Surg. OralMed. Oral Pathol. 17, 405–414.
Müller-Hummel, P., Lahres, M., 1994. Infrared temperature measurement on diamond-coated tools during machining. Diamond Relat. Mater. 3, 765–769.
Nam, O.H., Yu, W.J., Choi, M.Y., Kyung, H.M., 2006. Monitoring of bone temperatureduring osseous preparation for orhodontic micro-screw implants: effect of motorspeed and pressure. Key Engineering Materials 321–323, 1044–1047.
Natali, C., Ingle, P., Dowell, J., 1996. Orthopaedic bone drills — can they be improved?Temperature changes near the drilling face. Journal of Bone and Joint Surgery British78B, 357–362.
Noble, B., 2003. Bone microdamage and cell apoptosis. Eur. Cell. Mater. 6, 46–55.Oberg, E., Jones, F.D., Horton, H.L., 1989. Machinery's handbook. Industrial Press, New
York, pp. 716–729.Ochsner, P.E., Baumgart, F., Kohler, G., 1998. Heat-induced segmental necrosis after
reaming of one humeral and two tibial fractures with a narrow medullary canal.Injury 29 (Suppl. 2), S1–S10.
Olson, S., Clinton, J.M., Working, Z., Lynch, J.R., Warme, W.J., Womack, W., et al., 2011.Thermal effects of glenoid reaming during shoulder arthroplasty in vivo. Journal ofBone and Joint Surgery American 93, 11–19.
Paciorek, J.F., 2003. Low friction chromium. Good Medicine for Ailing Surgical Instru-ments: BONEZone Summer, pp. 42–47.
Paszenda, Z., Basiaga, M., 2009. FEM analysis of drills used in bone surgery. Archives ofMaterials Science and Engineering 36, 103–109.
Proff, P., Bayerlein, T., Kramer, A., Allegrini Jr., S., Dietze, S., Fanghänel, J., et al., 2006.Requirements and infection prophylaxis for internally cooled implant drills. FoliaMorphol. 65, 34–36.
Rafel, S., 1962. Temperature changes during high-speed drilling on bone. J. Oral Surg.Anesth. Hosp. Dent. Serv. 20, 475–477.
Reed, K.L., Conzemius, M.G., Robinson, R.A., Brown, T.D., 2004. Osteocyte-based imageanalysis for quantitation of histologically apparent femoral head osteonecrosis:
application to an emumodel. Computational Methods in Biomechanical and Biomed-ical Engineering 7, 25–32.
Reingewirtz, Y., Szmukler-Moncler, S., Senger, B., 1997. Influence of different parame-ters on bone heating and drilling time in implantology. Clinical Oral Implants 8,189–197.
Riquelme Garcia, O.G., Mombiela, F.L., De La Fuente, C.J., Aranguez, M.G., Escribano,D.V., Martin, J.V., 2004. The influence of the size and condition of the reamers onbone temperature during intramedullary reaming. Journal of Bone and Joint Sur-gery American 86A, 994–999.
Roitberg, B.Z., Dujovny, M., Lim, I., 1997. UltraPower surgical drill system evaluation.Surg. Neurol. 47, 392–393.
Rui, L., Parag, H., Albert, J.S., 2007. High-throughput drilling of titanium alloys. Interna-tional Journal of Machine Tools Manufacturing 47, 63–74.
Saha, S., Pal, S., Albright, J.A., 1982. Surgical drilling design and performance of an im-proved drill. J. Biomech. Eng. 104, 245–252.
Sener, B.C., Dergin, G., Gursoy, B., Kelesoglu, E., Slih, I., 2009. Effects of irrigation tem-perature on heat control in vitro at different drilling depths. Clin. Oral ImplantsRes. 20, 294–298.
Sharawy, M., Misch, C.E., Weller, N., Tehemar, S., 2002. Heat generation during implantdrilling: the significance of motor speed. J. Oral Maxillofac. Surg. 60, 1160–1169.
Sneath, R.S., 1964. The determination of optimum twist drill shape for bone. Biome-chanics and Related Bioengineering Topics. Proceedings of the Symposium of Glas-gow. Pergamon Press, Oxford, pp. 41–45.
Spatz, S., 1965. Early reaction in bone following the use of burs rotating at conventionaland ultra speeds. Oral Surg. Oral Med. Oral Pathol. 19, 808–816.
Tehemar, S.H., 1999. Factors affecting heat generation during implant site prepara-tions: a review of biologic observations and future considerations. Int. J. Oral Max-illofac. Implants 14, 127–136.
Thompson, H.C., 1958. Effect of drilling on bone. J. Oral Surg. 16, 22–30.Tu, Y.K., Hong, Y.Y., Chen, Y.C., 2009. Finite element modeling of kirschner pin and bone
thermal contact during drilling. Life Science Journal 6, 23–27.Udiljak, T., Ciglar, D., Mihoci, K., 2003. Inflencing parameters in bone drilling. 9th Inter-
national Scientific Conference on Production Engineering CIM 2003, Lumbarda,Korčula, pp. I133–I142.
Udiljak, T., Ciglar, D., Skoric, S., 2007. Investigation into bone drilling and thermal bonenecrosis. Advances in Production Engineering and Management 2, 103–112.
Walsh, J.P., Symmons, H.F., 1949. A comparison of the heat production and mechanicalefficiency of diamond instruments, stones, and burs at 3000 and 60,000 rpm. NewZeland Dental Journal 45, 28–32.
Watanabe, F., Tawada, Y., Komatsu, S., Hata, Y., 1992. Heat distribution in bone duringpreparation of implant sites: heat analysis by real-time thermography. Int. J. OralMaxillofac. Implants 7, 212–219.
Wiggins, K.L., Malkin, S., 1976. Drilling of bone Journal of Biomechanics 9, 553–559.Wootton, R., Reeve, J., Veall, N., 1976. The clinical measurement of skeletal blood flow.
Clin. Sci. Mol. Med. 50, 261–268.Zelenov, E.S., 1985. Thermophysical properties of compact bone. Mechanics of Com-
posite Materials 21, 1092–1095.




















