
Reconstruction of Posterior Mandibular Alveolar Ridge ...
7
Case Series Reconstruction of Posterior Mandibular Alveolar Ridge Deficiencies With the Piezoelectric Hinge–Assisted Ridge Split Technique: A Retrospective Observational Report Dan J. Holtzclaw,* Nicholas J. Toscano, † and Paul S. Rosen ‡§ Background: Reconstruction of alveolar defects in the posterior edentulous mandible can be a difficult task. In addition to complicating anatomic features, such as the inferior alveolar nerve, mental foramen, oblique ridge, and lingual un- dercut of the mylohyoid ridge, edentulous ridges in the posterior mandible have thicker cortices and decreased volumes of vascular trabecular bone than their max- illary counterparts. Traditionally, these areas have been treated with autogenous block grafts. Significant resorption of these grafts, in combination with patient mor- bidity at secondary donor sites, has led clinicians to seek alternatives for augment- ing the edentulous posterior mandible. The aim of this retrospective consecutive case series is to report on both the technique of the piezoelectric hinge–assisted ridge split procedure for augmenting these sites and the results that were achieved. Methods: Thirteen patients with 17 horizontal alveolar ridge deficiencies of the posterior mandible were treated with the piezoelectric hinge–assisted ridge split procedure. After an average healing period of 14 weeks, dental implants were placed into the augmented sites. Intrasurgical alveolar ridge measurements taken at the initial surgery and subsequently at the time of implant placement docu- mented the horizontal gains achieved by this procedure. Results: Overall mean gain in horizontal width was 4.03 mm (– 0.67). For sin- gle implant–site augmentations, the mean gain was 3.38 mm (– 0.25). For mul- tiple adjacent implant–site augmentations, mean gain was 4.25 mm (– 0.62). A total of 31 dental implants were successfully placed in all sites and none required additional augmentation procedures. There were no instances of adverse out- comes, such as neurosensory deficits or sequestration of mobilized buccal plates. After a minimum of 6 months of loading, all dental implants have been successful. Conclusions: This retrospective observational report demonstrates that the pi- ezoelectric hinge–assisted ridge split procedure can achieve substantial gains in horizontal ridge width of the edentulous posterior mandible without associated morbidity. Further prospective and larger observational studies are warranted to see if this is true over a larger patient population and to compare this technique to other more traditionally used approaches. J Periodontol 2010;81:1580-1586. KEY WORDS Alveolar ridge augmentation; bone regeneration; grafting, bone; mandible; partially edentulous jaw. I n some instances, edentulous spaces planned for dental im- plant treatment require reconstruction of alveo- lar ridge deficiencies be- fore fixture placement. Recommendations for minimum dental implant alveolar housings range from 5 to 6 mm of re- sidual bone width before implant placement 1,2 or 1 to 1.5 mm of bone width around all lateral aspects of the implant after its delivery. 3,4 To achieve such bony di- mensions, a variety of augmentation techniques have been successfully used including guided bone regeneration with particulate graft; 5 block grafts obtained from ra- mus, 6 symphysis, 7 iliac crest, 8 or calvarial bone; 9 distraction osteogene- sis; 10 ridge expansion osteotomy; 11 and ridge * Private practice, Austin, TX. † Private practice, New York, NY. ‡ Department of Periodontics, University of Maryland Dental School, Baltimore, MD. § Private practice, Yardley, PA. doi: 10.1902/jop.2010.100093 Volume 81 • Number 11 1580
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Reconstruction of Posterior Mandibular Alveolar Ridge ...
Case Series
Reconstruction of Posterior MandibularAlveolar Ridge Deficiencies With thePiezoelectric Hinge–Assisted Ridge SplitTechnique: A RetrospectiveObservational ReportDan J. Holtzclaw,* Nicholas J. Toscano,† and Paul S. Rosen‡§
Background: Reconstruction of alveolar defects in the posterior edentulousmandible can be a difficult task. In addition to complicating anatomic features,such as the inferior alveolar nerve, mental foramen, oblique ridge, and lingual un-dercut of the mylohyoid ridge, edentulous ridges in the posterior mandible havethickercorticesanddecreasedvolumesofvascular trabecularbone than theirmax-illary counterparts. Traditionally, these areas have been treated with autogenousblock grafts. Significant resorption of these grafts, in combination with patient mor-bidity at secondary donor sites, has led clinicians to seek alternatives for augment-ing the edentulous posterior mandible. The aim of this retrospective consecutivecase series is to report on both the technique of the piezoelectric hinge–assistedridge split procedure for augmenting these sites and the results that were achieved.
Methods: Thirteen patients with 17 horizontal alveolar ridge deficiencies of theposterior mandible were treated with the piezoelectric hinge–assisted ridge splitprocedure. After an average healing period of 14 weeks, dental implants wereplaced into the augmented sites. Intrasurgical alveolar ridge measurements takenat the initial surgery and subsequently at the time of implant placement docu-mented the horizontal gains achieved by this procedure.
Results: Overall mean gain in horizontal width was 4.03 mm (– 0.67). For sin-gle implant–site augmentations, the mean gain was 3.38 mm (– 0.25). For mul-tiple adjacent implant–site augmentations, mean gain was 4.25 mm (– 0.62). Atotal of 31 dental implants were successfully placed in all sites and none requiredadditional augmentation procedures. There were no instances of adverse out-comes, such as neurosensory deficits or sequestration of mobilized buccal plates.After a minimum of 6 months of loading, all dental implants have been successful.
Conclusions: This retrospective observational report demonstrates that the pi-ezoelectric hinge–assisted ridge split procedure can achieve substantial gains inhorizontal ridge width of the edentulous posterior mandible without associatedmorbidity. Further prospective and larger observational studies are warranted tosee if this is true over a larger patient population and to compare this techniqueto other more traditionally used approaches. J Periodontol 2010;81:1580-1586.
KEY WORDS
Alveolar ridge augmentation; bone regeneration; grafting, bone; mandible;partially edentulous jaw.
In some instances,edentulous spacesplanned for dental im-
plant treatment requirereconstruction of alveo-lar ridge deficiencies be-fore fixture placement.Recommendations forminimum dental implantalveolar housings rangefrom 5 to 6 mm of re-sidual bone width beforeimplant placement1,2 or1 to 1.5 mm of bonewidth around all lateralaspects of the implantafter its delivery.3,4 Toachieve such bony di-mensions, a variety ofaugmentation techniqueshave been successfullyused including guidedbone regeneration withparticulate graft;5 blockgrafts obtained from ra-mus,6 symphysis,7 iliaccrest,8 or calvarial bone;9
distraction osteogene-sis;10 ridge expansionosteotomy;11 and ridge* Private practice, Austin, TX.
† Private practice, New York, NY.‡ Department of Periodontics, University of Maryland Dental School, Baltimore, MD.§ Private practice, Yardley, PA. doi: 10.1902/jop.2010.100093
Volume 81 • Number 11
1580

splitting.12 Depending on the intraoral location oftreatment, each procedure has inherent advantagesand limitations.
The posterior mandible has been referred to as ‘‘themost difficult region for reconstruction and early im-plant placement in cases of severe alveolar resorptionin the maxillomandibular complex.’’13 In addition tocomplicating anatomic features, such as the inferioralveolar nerve, mental foramen, oblique ridge, andlingual undercut of the mylohyoid ridge, edentulousmandibular ridges have thicker cortices and de-creased volumes of vascular trabecular bone thantheir maxillary counterparts.14,15 Traditionally, re-sorbed alveolar ridges of the most severe nature havebeen treated with autogenous block grafts.16,17 Al-though these grafts can provide substantial augmen-tation, use has been associated with patient morbidityat donor sites18 and, as such, alternative proceduresyielding comparable gains to autogenous block graftshave been sought. The aim of this retrospective caseseries is to report on both the technique of the piezo-electric hinge–assisted ridge split (PHARS) procedurefor augmenting posterior mandibular alveolar ridgedeficiencies and the results that may be achieved.
MATERIALS AND METHODS
PatientsThis retrospective case series reports on consecutivepatientswhowere treated in separateprivatepracticesin Texas, Washington DC, and Pennsylvania with thePHARS technique. Information was gained after ex-haustive chart review. A total of 13 patients with 17horizontal alveolar ridge deficiencies of the posteriormandible were found who had been referred for dentalimplant treatment between 2008 and 2009. Patientsincluded seven males and six females with a meanage of 35.15 years (range, 22 to 43 years). Becausethis was a retrospective observational report, patientswere treated as they presented, and there were noexclusionary parameters. All patients were eithersystemically healthy or had well-controlled medicalconditions (i.e., hypertension, gastric esophageal re-flux disease, asthma, and so forth). Written informedconsent was obtained from each patient. Site-specificindications for the PHARS technique typically used bythe authors are as follows: 1) ‡2 mm of horizontal bonethickness at crest; 2) ‡10 mm of vertical bone height tovital structures; 3) non-concave cross-sectional anat-omy;4)corticotomiesmust remain1mmawayfromad-jacent teeth; and 5) single tooth sites difficult (onlymolars if single tooth).
Surgical ProcedureAt all edentulous sites (Fig. 1), crestal incisions wereplaced after obtaining local or block anesthesia. Ver-tical incisions were used at the mesial and distal most
aspects of the edentulous area and elevation of full-thickness flaps was performed (Fig. 2A). Piezoelectricsurgical cutting tipsi¶ were used to make corticotomycuts in preparation for controlled fracture of the buc-cal cortical plate. The initial corticotomy was madeat the mid-crest and terminated approximately 1 mmfrom any adjacent teeth. The precise cutting natureof the piezoelectric surgical units provided a marginof safety allowing for closer cuts to adjacent teethcompared to traditional cutting instruments.19 Whena tooth was extracted adjacent to an edentulousspace, the ridge splitting technique was slightly mod-ified. The initial horizontal cut was initiated at the mid-crest of the edentulous ridge from the inner aspect ofthe extraction site. The initial crestal cut was then re-traced and deepened up to a depth of 10 mm. Apicalflaring of the residual alveolar bone typically nega-ted the need to deepen the horizontal cut any fur-ther than this. At the terminus of the horizontalcorticotomy, vertical cuts were made approximatingthe length and depth of the crestal horizontal cut. Ver-tical cuts completely transected the buccal corticalplate into the marrow space. In cases of severelyresorbed ridges with little to no marrow space, thedepth of the vertical cuts approximated one half ofthe total ridge width. Finally, apical ‘‘hinge cuts’’ con-nected the vertical corticotomies (Fig. 2B) to gain bet-ter control of greenstick fracturing and allow for moreextensive lateral mobilization of the buccal plate. Thiscut required careful attention to detail and is the mostdifficult cut of the procedure. Complete transectionof the buccal plate is to be avoided. Apical hinge cutsdid not fully transect the cortical plate because theirintent was to act as a ‘‘guide’’ for the fracture and a‘‘hinge’’ for lateral positioning of the bony segment.
On completion of the corticotomies, ridge expan-sion chisels were sequentially used to widen the
Figure 1.Presurgical view of left posterior mandibular Siebert 1 ridge defect.
i Acteon, Mount Laurel, NJ.¶ Piezosurgery, Columbus, OH.
J Periodontol • November 2010 Holtzclaw, Toscano, Rosen
1581
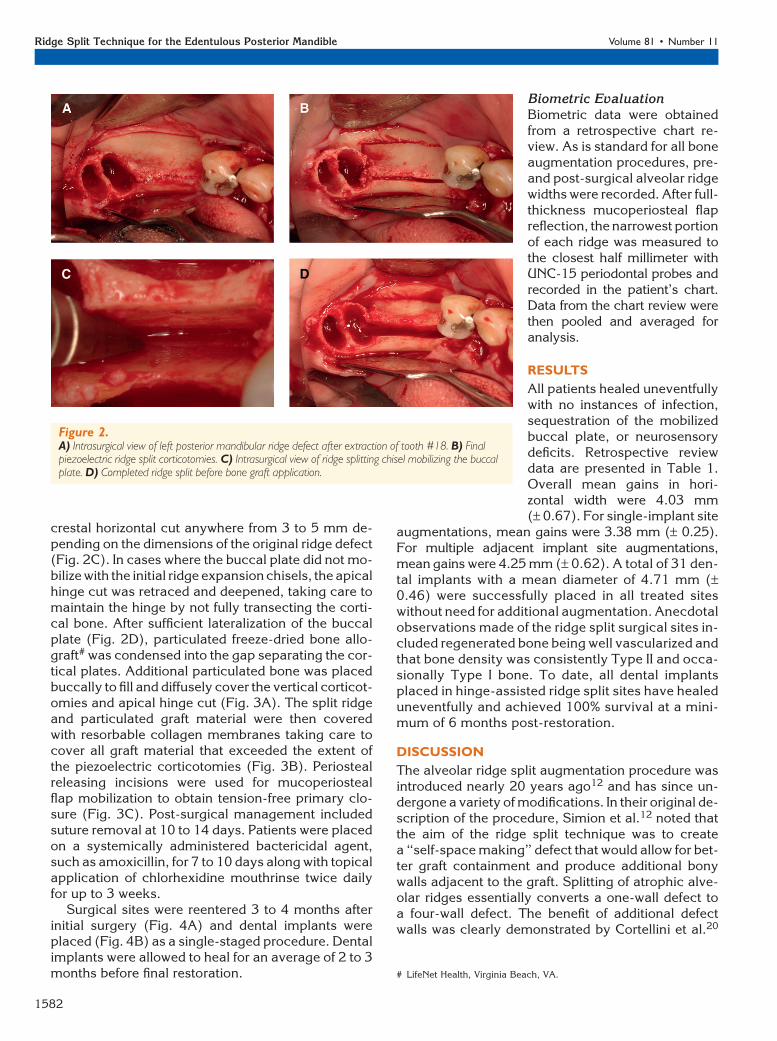
crestal horizontal cut anywhere from 3 to 5 mm de-pending on the dimensions of the original ridge defect(Fig. 2C). In cases where the buccal plate did not mo-bilize with the initial ridge expansion chisels, the apicalhinge cut was retraced and deepened, taking care tomaintain the hinge by not fully transecting the corti-cal bone. After sufficient lateralization of the buccalplate (Fig. 2D), particulated freeze-dried bone allo-graft# was condensed into the gap separating the cor-tical plates. Additional particulated bone was placedbuccally to fill and diffusely cover the vertical corticot-omies and apical hinge cut (Fig. 3A). The split ridgeand particulated graft material were then coveredwith resorbable collagen membranes taking care tocover all graft material that exceeded the extent ofthe piezoelectric corticotomies (Fig. 3B). Periostealreleasing incisions were used for mucoperiostealflap mobilization to obtain tension-free primary clo-sure (Fig. 3C). Post-surgical management includedsuture removal at 10 to 14 days. Patients were placedon a systemically administered bactericidal agent,such as amoxicillin, for 7 to 10 days along with topicalapplication of chlorhexidine mouthrinse twice dailyfor up to 3 weeks.
Surgical sites were reentered 3 to 4 months afterinitial surgery (Fig. 4A) and dental implants wereplaced (Fig. 4B) as a single-staged procedure. Dentalimplants were allowed to heal for an average of 2 to 3months before final restoration.
Biometric EvaluationBiometric data were obtainedfrom a retrospective chart re-view. As is standard for all boneaugmentation procedures, pre-and post-surgical alveolar ridgewidths were recorded. After full-thickness mucoperiosteal flapreflection, the narrowest portionof each ridge was measured tothe closest half millimeter withUNC-15 periodontal probes andrecorded in the patient’s chart.Data from the chart review werethen pooled and averaged foranalysis.
RESULTS
All patients healed uneventfullywith no instances of infection,sequestration of the mobilizedbuccal plate, or neurosensorydeficits. Retrospective reviewdata are presented in Table 1.Overall mean gains in hori-zontal width were 4.03 mm(– 0.67). For single-implant site
augmentations, mean gains were 3.38 mm (– 0.25).For multiple adjacent implant site augmentations,mean gains were 4.25 mm (– 0.62). A total of 31 den-tal implants with a mean diameter of 4.71 mm (–0.46) were successfully placed in all treated siteswithout need for additional augmentation. Anecdotalobservations made of the ridge split surgical sites in-cluded regenerated bone being well vascularized andthat bone density was consistently Type II and occa-sionally Type I bone. To date, all dental implantsplaced in hinge-assisted ridge split sites have healeduneventfully and achieved 100% survival at a mini-mum of 6 months post-restoration.
DISCUSSION
The alveolar ridge split augmentation procedure wasintroduced nearly 20 years ago12 and has since un-dergone a variety of modifications. In their original de-scription of the procedure, Simion et al.12 noted thatthe aim of the ridge split technique was to createa ‘‘self-space making’’ defect that would allow for bet-ter graft containment and produce additional bonywalls adjacent to the graft. Splitting of atrophic alve-olar ridges essentially converts a one-wall defect toa four-wall defect. The benefit of additional defectwalls was clearly demonstrated by Cortellini et al.20
Figure 2.A) Intrasurgical view of left posterior mandibular ridge defect after extraction of tooth #18. B) Finalpiezoelectric ridge split corticotomies. C) Intrasurgical view of ridge splitting chisel mobilizing the buccalplate. D) Completed ridge split before bone graft application.
# LifeNet Health, Virginia Beach, VA.
Ridge Split Technique for the Edentulous Posterior Mandible Volume 81 • Number 11
1582

who found that bone defect fill improved proportion-ally to the number of residual defect walls.
Multiple studies have documented that lateral gainsup to 5 mm may be achieved with ridge-splitting pro-cedures.12,21,22 Most of these studies, however, dealtwith maxillary sites composed of softer bone densitiesthan those of the mandible, making this procedureeasier to perform.23 This was noted by Bravi et al.24
in a long-term multicenter retrospective clinical studyof 1,715 implants placed with the edentulous ridge ex-pansion technique.24 In this study, 44% of implants
placed in mandibular sites required two-stage deliv-ery because of what the authors24 described as ‘‘in-elastic bone.’’ The reason for this lack of elasticityrelates to the mandibular posterior having thickercortical bone measurements versus those in theposterior maxilla.15 One study evaluating ridge splitprocedures performed in the mandible noted that‘‘greenstick fracture is not possible in this arch dueto the high risk for complete fracture of the mobilizedsegment.’’25 To avoid a ‘‘mal fracture’’ from occur-ring, the authors modified the original technique byplacing apical hinge cuts (Fig. 2B). The intent of thismodification is to guide the apical ridge split frac-ture and allow for additional horizontal mobilizationof the buccal plate. Other ridge split articles involv-ing the posterior mandible have found the need touse similar cuts or variations thereof.22,26,27 Moreextreme variations were described by Enislidiset al.28 and Basa et al.13 Mandibular ridge splittingin the Enislidis et al.28 study used a three-staged ap-proach with apical scoring cuts performed during thefirst stage of the technique. In the Basa et al.13 study,the apical cuts fully transected the buccal plate
Figure 3.A) Ridge split and all corticotomies grafted with bone allograft. B) Surgicalsite covered with resorbable collagen membrane.C) Tension-free primaryclosure of surgical site.
Figure 4.A) Ridge split healing at 3 months. Faint outlines of the crestal and mesialcorticotomies are still visible. Note improved ridge width. B) Placementof 5-mm diameter dental implants into the ridge split augmented site.Note that bone completely houses both implants.
J Periodontol • November 2010 Holtzclaw, Toscano, Rosen
1583

resulting in a completely detached bone segment,which required subsequent screw fixation. The apicalhinge cuts used in this report did not fully transect thebuccal plate, which allowed for mobilization of thebuccal segment without the need for fixation.
Fixation is one of the many variations that havebeen associated with ridge split procedures. Otherstudies have stressed the importance of stabilizingthe mobilized buccal plate through the use of metallicligatures,29 resorbable ligatures,30 screws,13 or tita-nium mesh to avoid its sequestration.21 Absolutelyno attempt was made to stabilize or fixate the mobi-lized buccal plates in this report, and there were nocomplications during healing.
A second variation in ridge-splitting studies has re-lated to managing the created four-wall defect. There isno consensus on whether to graft this surgically createddefect, to use an exclusionary barrier, or to use a combi-nation approach of graft and membrane. Resorbablemembranes were used in all cases of this retrospectivereport, whereas other studies used titanium mesh,21
non-resorbable membranes,12 or nothing.13,29,31
Likewise, all surgically created ridge split defects inthe current study were grafted with freeze-dried boneallograft, whereas other studies used particulatedautograft,21 xenograft,22 alloplast,13 or nothing.12
A third variation in many ridge split studies hasbeen the method by which cortical cuts were made.The technique documented in this report used piezo-electric surgery units to create corticotomies, whereasothers used scalpel blades,24 sharp chisels,12 flexiblediamond disks,13 carbide burs,31 or microsaws.26
Studies comparing wound healing of piezoelectricbone cuts to those created with alternative methodshave demonstrated reduced trauma and faster heal-ing with the former and increased inflammation withthe latter.32,33 Furthermore, a study comparing im-plant success rates in alveolar ridges split with piezo-electric surgical units to those where implants wereplaced into wide intact ridges found no difference inoverall outcomes, although more failures did occurin the non-piezoelectric unsplit group.34
Although most other ridge splitstudies allowed 5 to 6 months ofhealing before initiating second-stage implant surgery,27-31,34-36
patients in this retrospective caseseries proceeded to implant place-ment after 3 to 4 months. Dentalimplants were usually placed inasingle-staged fashion, eliminatingthe need for abutment placementat a later surgery. On average, den-tal implants were allowed to healfor 3 months before delivery ofthe final restoration. So, total treat-
ment time and the number of interventions with thecurrent case series were similar to prior studies whereimplants were placed at the time of ridge splitting.Because of the significant lateral mobilization ofthe buccal plates and lack of stabilization proce-dures, the authors believed a two-stage approachto implant delivery was most appropriate. Otherstudies confirm this, noting that nearly half of all im-plants placed in mandibular ridge split sites overa 10-year period required a two-stage approach.24
Additionally, Elian et al.37 noted that a two-stageapproach for ridge splitting procedures allows for‘‘reevaluation of the surgical site before implantplacement and better control over implant position,angulation, and ultimately a more esthetic restora-tion.’’
The horizontal gains documented in this retrospec-tive case series report compare favorably to thosewhere autogenous symphysis and ramus block graftswere used.38-40 Unlike autogenous block grafts, how-ever, ridge splits are not commonly associated withsecondary patient morbidity. Morbidities that havebeen reported at the symphyseal donor site have in-cluded neurosensory deficits, block fracture, exces-sive bleeding, potential damage to adjacent teeth,lip incompetence, and chin ptosis.1,17,41-43 Thoseassociated with ramus graft harvest have includedneurosensory deficits, block fracture, mandible frac-ture, excessive bleeding, and trismus.17,39,44 Addi-tionally, block grating requires the use of fixationscrews, which adds extra time and expense to the pro-cedure.
CONCLUSIONS
This retrospective observational report demonstratesthat the PHARS procedure can achieve substantialgains in horizontal ridge width of the edentulous pos-terior mandible without associated morbidity. Bothfurther prospective and larger observational studiesare warranted to see if this is true over a larger patientpopulation and to compare this technique to othermore traditionally used approaches.
Table 1.
Site-Specific Results After Augmentation With PHARSTechnique
Preoperative
Width (mm)
Postoperative
Width (mm) Change (mm)
Single implant sites 3.13 (– 0.85) 6.51 (– 1.08) 3.38 (– 0.25)
Multiple implant sites 3.79 (– 0.78) 8.04 (– 0.91) 4.25 (– 0.62)
Overall 3.63 (– 0.82) 7.66 (– 1.15) 4.03 (– 0.67)
Ridge Split Technique for the Edentulous Posterior Mandible Volume 81 • Number 11
1584
ACKNOWLEDGMENTS
Dr. Rosen is a consultant to Acteon. Drs. Holtzclawand Toscano report no conflicts of interest related tothis study.
REFERENCES1. Misch CM, Misch CE, Resnik RR, Ismail YH. Recon-
struction of maxillary alveolar defects with mandibularsymphysis grafts for dental implants: A preliminaryprocedural report. Int J Oral Maxillofac Implants 1992;7:360-366.
2. de Wijs FL, Cune MS. Immediate labial contour resto-ration for improved esthetics: A radiographic study onbone splitting in anterior single-tooth replacement. Int JOral Maxillofac Implants 1997;12:686-696.
3. Albrektsson T, Jansson T, Lekholm U. Osseointegrateddental implants. Dent Clin North Am 1986;30:151-174.
4. Shulman LB. Surgical considerations in implant den-tistry. Int J Oral Implantol 1988;5:37-41.
5. Buser D, Dula K, Hirt HP, Schenk RK. Lateral ridgeaugmentation using autografts and barrier mem-branes: A clinical study with 40 partially edentulouspatients. J Oral Maxillofac Surg 1996;54:420-432,discussion 432-433.
6. Capelli M. Autogenous bone graft from the mandibularramus: A technique for bone augmentation. Int JPeriodontics Restorative Dent 2003;23:277-285.
7. Garg AK, Morales MJ, Navarro I, Duarte F. Autoge-nous mandibular bone grafts in the treatment of theresorbed maxillary anterior alveolar ridge: Rationaleand approach. Implant Dent 1998;7:169-176.
8. Sjostrom M, Sennerby L, Nilson H, Lundgren S. Re-construction of the atrophic edentulous maxilla withfree iliac crest grafts and implants: A 3-year report ofa prospective clinical study. Clin Implant Dent RelatRes 2007;9:46-59.
9. Gutta R, Waite PD. Outcomes of calvarial bone graft-ing for alveolar ridge reconstruction. Int J Oral Max-illofac Implants 2009;24:131-136.
10. Elo JA, Herford AS, Boyne PJ. Implant success indistracted bone versus autogenous bone-grafted sites.J Oral Implantol 2009;35:181-184.
11. Nishioka RS, Souza FA. Bone spreader technique: Apreliminary 3-year study. J Oral Implantol 2009;35:289-294.
12. Simion M, Baldoni M, Zaffe D. Jawbone enlargementusing immediate implant placement associated witha split-crest technique and guided tissue regeneration.Int J Periodontics Restorative Dent 1992;12:462-473.
13. Basa S, Varol A, Turker N. Alternative bone expansiontechnique for immediate placement of implants in theedentulous posterior mandibular ridge: A clinical re-port. Int J Oral Maxillofac Implants 2004;19:554-558.
14. Neiva RF, Gapski R, Wang HL. Morphometric analy-sis of implant-related anatomy in Caucasian skulls.J Periodontol 2004;75:1061-1067.
15. Flanagan D. A comparison of facial and lingual corticalthicknesses in edentulous maxillary and mandibularsites measured on computerized tomograms. J OralImplantol 2008;34:256-258.
16. Pikos MA. Block autografts for localized ridge aug-mentation: Part II. The posterior mandible. ImplantDent 2000;9:67-75.
17. Misch CM. Comparison of intraoral donor sites foronlay grafting prior to implant placement. Int J OralMaxillofac Implants 1997;12:767-776.
18. Misch CM. Ridge augmentation using mandibularramus bone grafts for the placement of dental im-plants: Presentation of a technique. Pract PeriodonticsAesthet Dent 1996;8:127-135, quiz 138.
19. Vercellotti T. Piezoelectric surgery in implantology: Acase report—A new piezoelectric ridge expansiontechnique. Int J Periodontics Restorative Dent 2000;20(4):358-365.
20. Cortellini P, Pini Prato G, Tonetti MS. Periodontalregeneration of human infrabony defects. II. Re-entryprocedures and bone measures. J Periodontol 1993;64:261-268.
21. Malchiodi L, Scarano A, Quaranta M, Piattelli A. Rigidfixation by means of titanium mesh in edentulous ridgeexpansion for horizontal ridge augmentation in themaxilla. Int J Oral Maxillofac Implants 1998;13:701-705.
22. Blus C, Szmukler-Moncler S. Split-crest and immedi-ate implant placement with ultra-sonic bone surgery:A 3-year life-table analysis with 230 treated sites. ClinOral Implants Res 2006;17:700-707.
23. Misch CM. Implant site development using ridgesplitting techniques. Oral Maxillofac Surg Clin NorthAm 2004;16:65-74, vi.
24. Bravi F, Bruschi GB, Ferrini F. A 10-year multicenterretrospective clinical study of 1715 implants placedwith the edentulous ridge expansion technique. IntJ Periodontics Restorative Dent 2007;27:557-565.
25. Piccinini M. Mandibular bone expansion technique inconjunction with root form implants: A case report.J Oral Maxillofac Surg 2009;67:1931-1936.
26. Suh JJ, Shelemay A, Choi SH, Chai JK. Alveolar ridgesplitting: A new microsaw technique. Int J PeriodonticsRestorative Dent 2005;25:165-171.
27. Koo S, Dibart S, Weber HP. Ridge-splitting techniquewith simultaneous implant placement. Compend Con-tin Educ Dent 2008;29:106-110.
28. Enislidis G, Wittwer G, Ewers R. Preliminary report ona staged ridge splitting technique for implant place-ment in the mandible: A technical note. Int J OralMaxillofac Implants 2006;21:445-449.
29. Coatoam GW, Mariotti A. The segmental ridge-splitprocedure. J Periodontol 2003;74:757-770.
30. Santagata M, Guariniello L, D’Andrea A, Tartaro G. Amodified crestal ridge expansion technique for imme-diate placement of implants: A report of three cases.J Oral Implantol 2008;34:319-324.
31. Shimoyama T, Kaneko T, Shimizu S, Kasai D, Tojo T,Horie N. Ridge widening and immediate implant place-ment: A case report. Implant Dent 2001;10:108-112.
32. Vercellotti T, Nevins ML, Kim DM, et al. Osseousresponse following resective therapy with piezosur-gery. Int J Periodontics Restorative Dent 2005;25:543-549.
33. Preti G, Martinasso G, Peirone B, et al. Cytokines andgrowth factors involved in the osseointegration of oraltitanium implants positioned using piezoelectric bonesurgery versus a drill technique: A pilot study inminipigs. J Periodontol 2007;78:716-722.
34. Danza M, Guidi R, Carinci F. Comparison betweenimplants inserted into piezo split and unsplit alveolarcrests. J Oral Maxillofac Surg 2009;67:2460-2465.
35. Calvo Guirado JL, Pardo Zamora G, Saez Yuguero MR.Ridge splitting technique in atrophic anterior maxilla
J Periodontol • November 2010 Holtzclaw, Toscano, Rosen
1585
with immediate implants, bone regeneration and im-mediate temporisation: A case report. J Ir Dent Assoc2007;53:187-190.
36. Guirado JL, Yuguero MR, Carrion del Valle MJ,Zamora GP. A maxillary ridge-splitting techniquefollowed by immediate placement of implants: A casereport. Implant Dent 2005;14:14-20.
37. Elian N, Jalbout Z, Ehrlich B, et al. A two-stage full-arch ridge expansion technique: Review of the literatureand clinical guidelines. Implant Dent 2008;17:16-23.
38. Pikos MA. Mandibular block autografts for alveolarridge augmentation. Atlas Oral Maxillofac Surg ClinNorth Am 2005;13:91-107.
39. Pikos MA. Facilitating implant placement with chingrafts as donor sites for maxillary bone augmenta-tion—Part I. Dent Implantol Update 1995;6:89-92.
40. Sethi A, Kaus T. Ridge augmentation using mandibu-lar block bone grafts: Preliminary results of an ongoingprospective study. Int J Oral Maxillofac Implants 2001;16:378-388.
41. Rubens BC, West RA. Ptosis of the chin and lipincompetence: Consequences of lost mentalis musclesupport. J Oral Maxillofac Surg 1989;47:359-366.
42. Zide BM, McCarthy J. The mentalis muscle: Anessential component of chin and lower lip position.Plast Reconstr Surg 1989;83:413-420.
43. McCarthy C, Patel RR, Wragg PF, Brook IM. Dentalimplants and onlay bone grafts in the anterior maxilla:Analysis of clinical outcome. Int J Oral MaxillofacImplants 2003;18:238-241.
44. Pikos MA. Alveolar ridge augmentation with ramusbuccal shelf autografts and impacted third molarremoval. Dent Implantol Update 1999;10:27-31.
Correspondence: Dr. Dan J. Holtzclaw, 3016 Hidden BluffCove, Round Rock, TX 78665. Fax: 888/923-0002;e-mail: [email protected].
Submitted February 16, 2010; accepted for publicationJune 6, 2010.
Ridge Split Technique for the Edentulous Posterior Mandible Volume 81 • Number 11
1586




















