TWIN-BLOCK: A MANDIBULAR ROCKET- A CASE REPORT
13
Dr Mayuresh J Baheti et al . / IJRID Volume 4 Issue 6 Nov.-Dec. 2014 108 Dr Mayuresh J Baheti et al / IJRID Volume 4 Issue 6 Nov.-Dec. 2014 Available online at www.ordoneardentistrylibrary.org ISSN 2249-488X INTERNATIONAL JOURNAL OF RESEARCH IN DENTISTRY TWIN-BLOCK: A MANDIBULAR ROCKET- A CASE REPORT Dr. Saurabh D. Bagrecha 1 , Dr. Mayuresh J Baheti* 2 , Dr. Nandlal Girijalal Toshniwal 3 1. Private Practitioner, Kopergaon- 423601, Maharashtra, India 2,3. Department of Orthodontics & Dentofacial Orthopedics, Rural Dental College, Pravara Institute of Medical Sciences, Loni – 413736, Maharashtra, India Received: 15 Oct. 2014; Revised:28 Nov. 2014; Accepted: 16 Dec. 2014; Available online: 5 Jan 2015 INTRODUCTION Class II malocclusion is one of the most frequent problem encountered in orthodontic practice, mandibular retrusion being its commonest cause 1 . Sagittal and transverse discrepancies often coexist in skeletal class II malocclusions. 2, 3 Orthopedic growth modification can work well in such cases provided that the remaining pubertal growth is adequate and that the clinician can time the treatment to coincide with the peak growth period. 4, 5 The transverse discrepancy is generally corrected first, establishing a proper base for the sagittal correction to follow 6, 7 functional mandibular advancement. Functional appliances have been in use for almost a hundred years. These appliances are believed to provide a favorable environment to exploit the available growth potential to its maximum. Though the debate as to whether they actually bring about a clinically significant increase in growth has not been resolved, these appliances continue to form an important part of the orthodontist’s armamentarium. Functional appliances cause redirectionof maxillary growth, change in mandibular growth and position, which also change the dental and the muscular relationships. 8 The twin block appliance, originally developed by William Clark, 9 is a widely used functional appliance for the management of class II malocclusion. The appliance can be worn almost full-time. It has the advantage of allowing nearly a full range of mandibular movement. The patients get acclimatized to wearing it very easily. Normal speech is far easier to achieve in the shortest possible time with this appliance. Thus, its popularity comes from its high patient acceptability and a concurrent ability to produce rapid results. Case – report ABSTRACT Functional appliances have been used for many years in the treatment of Class II malocclusions. The use of functional jaw orthopedics, at the correct times during circumpubertal growth spurts, can ultimately result in achieving a beautiful smile, an excellent functional occlusion, a full face with a beautiful jaw line and a profile. They redirect the growth of mandible bringing about a skeletal change in a growing patient. In case of any remaining dental discrepancy, a fixed appliance is obligatory. This patient was a 12-year-old growing female with a convex profile, receding chin, lower lip trap, Class II skeletal and dental relationship, a large over jet and increased overbite. Treatment was started with the Twin-block appliance to position mandible forward to promote growth of the mandible to improve facial profile. This was followed by fixed appliance mechanotherapy to align and level the dentition to achieve the optimal results and harmonious occlusion. Key words: Skeletal Class II, Functional appliance, Twin-block, Growing patient, Two-Phase treatment
-
Upload
pravarares -
Category
Documents
-
view
0 -
download
0
Transcript of TWIN-BLOCK: A MANDIBULAR ROCKET- A CASE REPORT

Dr Mayuresh J Baheti et al . / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
108 Dr Mayuresh J Baheti et al / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
Available online at www.ordoneardentistrylibrary.org ISSN 2249-488X
INTERNATIONAL JOURNAL OF RESEARCH IN DENTISTRY
TWIN-BLOCK: A MANDIBULAR ROCKET- A CASE REPORT
Dr. Saurabh D. Bagrecha1, Dr. Mayuresh J Baheti*2, Dr. Nandlal Girijalal Toshniwal3
1. Private Practitioner, Kopergaon- 423601, Maharashtra, India
2,3. Department of Orthodontics & Dentofacial Orthopedics, Rural Dental College, Pravara Institute of Medical
Sciences, Loni – 413736, Maharashtra, India
Received: 15 Oct. 2014; Revised:28 Nov. 2014; Accepted: 16 Dec. 2014; Available online: 5 Jan 2015
INTRODUCTION
Class II malocclusion is one of the most frequent problem encountered in orthodontic practice, mandibular retrusion being
its commonest cause1. Sagittal and transverse discrepancies often coexist in skeletal class II malocclusions.2, 3Orthopedic
growth modification can work well in such cases provided that the remaining pubertal growth is adequate and that the
clinician can time the treatment to coincide with the peak growth period.4, 5 The transverse discrepancy is generally
corrected first, establishing a proper base for the sagittal correction to follow6, 7functional mandibular advancement.
Functional appliances have been in use for almost a hundred years. These appliances are believed to provide a
favorable environment to exploit the available growth potential to its maximum. Though the debate as to whether they
actually bring about a clinically significant increase in growth has not been resolved, these appliances continue to form an
important part of the orthodontist’s armamentarium. Functional appliances cause redirectionof maxillary growth, change
in mandibular growth and position, which also change the dental and the muscular relationships.8 The twin block
appliance, originally developed by William Clark,9is a widely used functional appliance for the management of class II
malocclusion. The appliance can be worn almost full-time. It has the advantage of allowing nearly a full range of
mandibular movement. The patients get acclimatized to wearing it very easily. Normal speech is far easier to achieve in
the shortest possible time with this appliance. Thus, its popularity comes from its high patient acceptability and a
concurrent ability to produce rapid results.
Case – report
ABSTRACT Functional appliances have been used for many years in the treatment of Class II malocclusions. The use of functional jaw orthopedics, at the correct times during circumpubertal growth spurts, can ultimately result in achieving a beautiful smile, an excellent functional occlusion, a full face with a beautiful jaw line and a profile. They redirect the growth of mandible bringing about a skeletal change in a growing patient. In case of any remaining dental discrepancy, a fixed appliance is obligatory. This patient was a 12-year-old growing female with a convex profile, receding chin, lower lip trap, Class II skeletal and dental relationship, a large over jet and increased overbite. Treatment was started with the Twin-block appliance to position mandible forward to promote growth of the mandible to improve facial profile. This was followed by fixed appliance mechanotherapy to align and level the dentition to achieve the optimal results and harmonious occlusion. Key words: Skeletal Class II, Functional appliance, Twin-block, Growing patient, Two-Phase treatment

Dr Mayuresh J Baheti et al . / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
109 Dr Mayuresh J Baheti et al / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
In a two-stage treatment, the functional phase involves the use of the twin block appliance (removable/fixed variety) to
reposition the mandible forward until the overjet and overbite are corrected.10 When that occurs, the permanent molars
will be in contact and the maxillary and mandibular incisors will be nicely coupled but the intervening teeth may not
necessarily be in occlusion.11 To ensure that the patient does not have a dual bite, the appliance is worn full time for a
minimum period of 7 to 9 months. After this functional appliance phase is completed, for accurate individual positioning
of teeth in three planes of space, fixed orthodontic treatment is usually necessary for the settling of occlusion and
maintenance of the skeletal correction achieved and correction of any remaining dental discrepancy.
Case report:
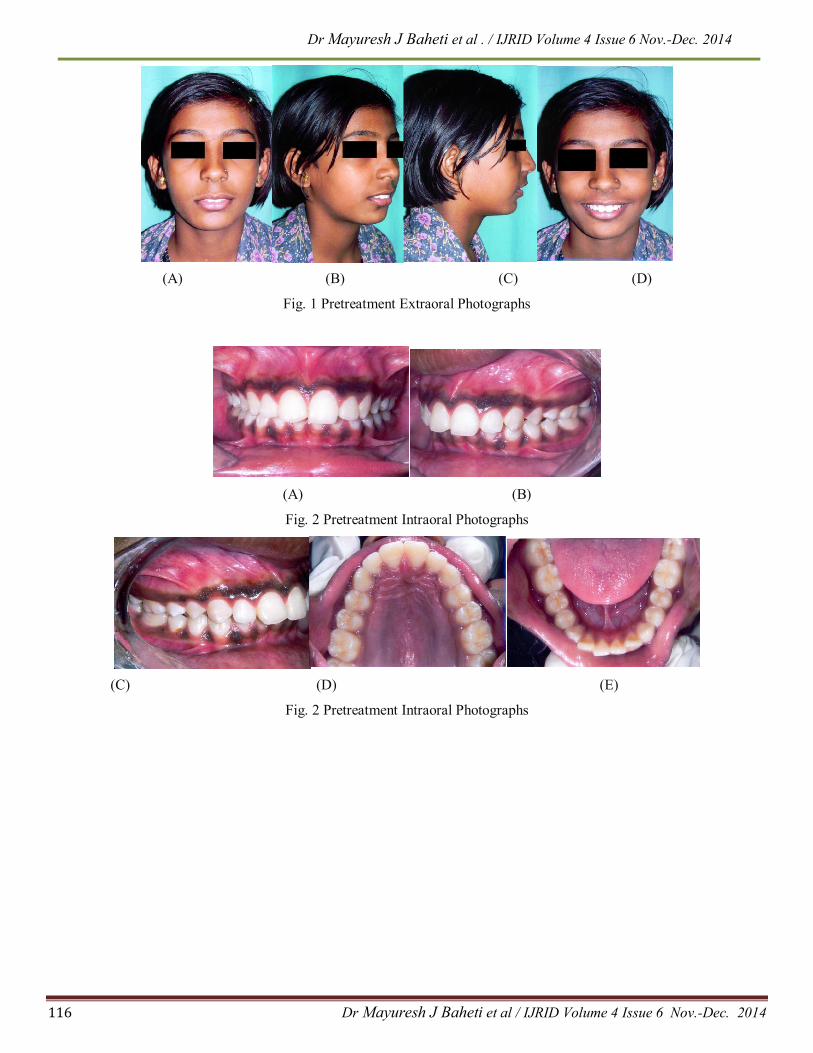
A 12-year-old pubertal female presented with the chief complaint of forwardly placed upper front teeth. She exhibited a
convex profile, an obtuse nasolabial angle, incompetent lips, a protrusive upper lip, a trapped lower lip and a deficient
chin.(Fig. 1)
Intraoral findings showed a full permanent dentition, Class II incisors and molar relationships, end-on cuspid relationship
bilaterally. The total overjet was 8mm and overbite of 6 mm respectively. The maximum mandibular protrusion was
about10 mm. Midlines were not coinciding, It is shifted to left side(Fig. 2)
Radiographic findings :( Fig. 3)
The radiographic findings are given in Table No. 1
Diagnosis:
Cephalometric analysis confirmed the diagnosis of a Circumpubertal with CVMI II female patient with skeletal Class II
malocclusion due to retropositioned mandible and dental class II division 1 malocclusion having horizontal growth
pattern. Evaluation of the patient’s cervical vertebrae maturity indicators (CVMI) indicated she was in the acceleration
phase of growth, with considerable (75%) growth remaining.
Prioritized Problem List:
Skeletal and Dental Class II malocclusion
Increased Overjet
Deep Overbite
Convex Profile
Treatment Objectives:
To achieve skeletal and dental Class I malocclusion
To correct increased overjet
To correct deep overbite
To achieve pleasing soft tissue profile

Dr Mayuresh J Baheti et al . / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
110 Dr Mayuresh J Baheti et al / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
Treatment Plan: Two phase treatment
Phase 1: Mandibular advancement with removable twin block appliance.
Phase 2: Fixed mechanotherapy with MBT 0.022 prescription.
The pubertal growth status of a patient is more critical for sagittal correction and be patient was approachingthe peak of
pubertal growth, so we decided to commence the first phase of treatment by carrying out the sagittal correction along with
a functional orthopedic approach. A removable twin block appliance was chosen to position mandible forward. This was
to be followed by second phase of treatment with fixed- appliance therapy for retraction of the anterior teeth and finishing
and detailing of the occlusion.
Treatment Progress:
The twin block appliance was fabricated with a 7 mm single step sagittal advancement and a 5 mm vertical opening in the
premolar region. The patient was instructed to wear the appliance full-time except contact sports.(Fig.4)
After 11 months of good compliance, the patient showed a super class I molar relationship without a dual bite and a
considerably improved facial profile. At the end of this phase of treatment, the patient now presented a class I molar and
cuspid relationship, an overjet and overbite of 2 mm. (Fig. 5,6)
Phase II treatment with a preadjusted edgewise appliance (PEA) was now initiated with McLaughlin Bennet Trevisi
(MBT) prescription 0.022” brackets being then direct bonded. Alignment and leveling was done using round 0.016”
thermal nickel-titanium (NiTi), followed by rectangular 0.019x 0.025” nickel-titanium (NiTi) and followed by rectangular
0.019x 0.025” stainless steel. During fixed-appliance therapy, we have used a fixed anterior maxillary inclined plane to
maintain the achieved sagittal correction. Finally class II settling elastic is used for finishing and detailing.The molar,
cuspid as well as incisorsarein class I relationship(Fig. 7).
After 12 months of fixed appliance treatment, the patient was highly satisfied with the treatment results. The fixed
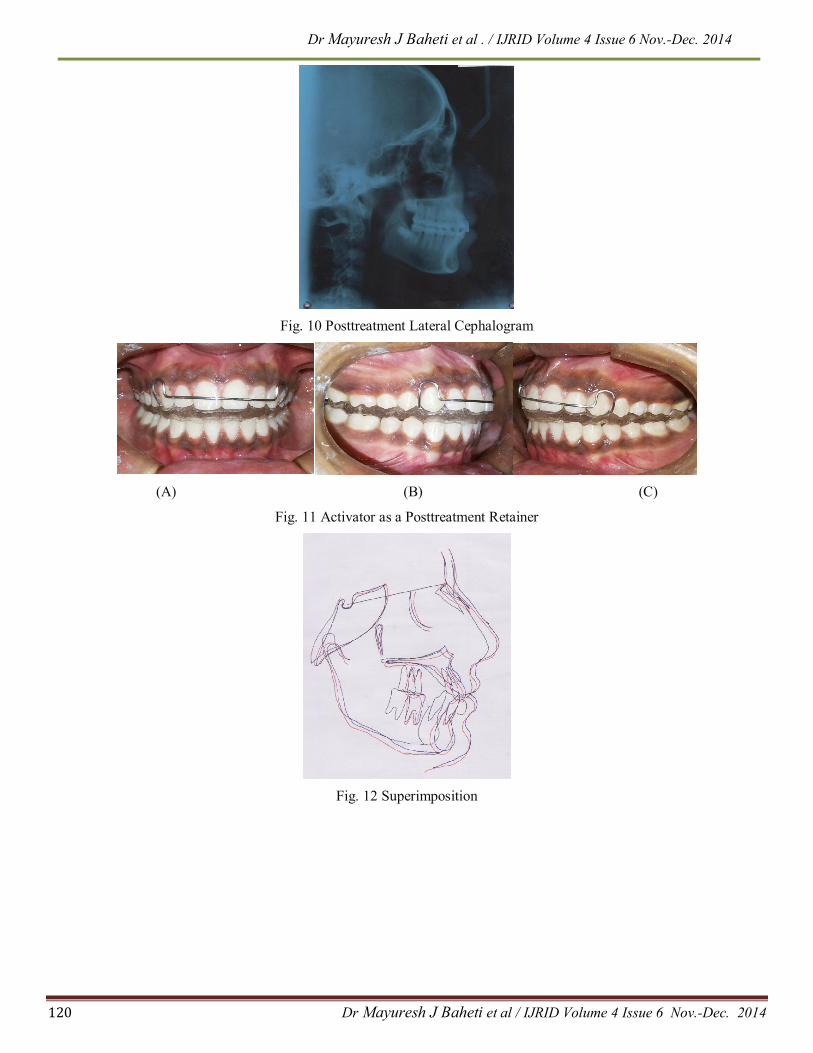
appliances were debonded and a total treatment time was 23 months (Fig. 8 & 9). The retention protocol was FSW for
lower arch and nighttime monoblock (Fig.11).
Post treatment radiographic findings: (Fig. 10)
Comparison of pretreatment cephalometric values with posttreatment cephalometric values given in Table No. 2
Superimposition :( Fig. 12)
Superimposition of the cephalometric tracing shows that considerable forward movement of the mandible, resulting in a
harmonious basal relationship. The molar and canine relationship had corrected. The chin lip contour improved with
decreased protrusion of the lips. Lower facial height remained constant.
Discussion:
There are obvious advantages of treating class II patients with a removable functional appliance prior to fixed appliance
therapy. Management of distal occlusion with functional appliances can lead to improvement in orofacial function through
Dr Mayuresh J Baheti et al . / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
111 Dr Mayuresh J Baheti et al / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
better muscle adaptation concurrent to the dental and skeletal changes achieved.12 Ideal timing for orthopedic treatment
for mandibular deficiency is after onset of pubertal growth spurt.13
The orthopedic phase and orthodontic treatment phase should be combined in one single treatment, as studies have
demonstrated that very early treatment involving two separate phases of therapy do not have any benefits14 ,15 other than a
positive effect on self-esteem. Success with this treatment result depends upon slight over-correction of the buccal
segments (molars and canines) to a super Class I, which builds anchorage into the system prior to placement of the fixed
appliances and allows for slight rebound. Class II correction is maintained with an inclined clip overbite plane during the
transition to fixed appliances. In twin-block therapy Class II correction is due to dentoalveolar changes15 and in most
cases IMPA is increased after twin block therapy but in this case report the IMPA is decreased and that is significant
finding in this case report. Lateral open bite reduction is commenced in the twin block phase by removal of the lower
Adams clasps and judicious trimming of the upper blocks. Any residual open bites, characteristically seen at the end of the
functional phase, will correct by buccal segment eruption during the leveling and aligning phase.
Conclusion:
The advantages of the two-phase treatment approach have been made evident and in the opinion, we think that Twin-
block is useful tools in the armamentarium of the clinician. The all-round improvement in having achieved a better soft
tissue balance, a near perfect occlusion and imparting a positive personality change with a concurrent improved self-
esteem have underlined the merits of this approach.
References:
1. McNamara J. Components of Class II maocclusion in children 8-10 yrs of age. Angle Ortho. 1981; 51: p. 571-74.
2. Staley RN, Stumtz WR, Peterson LC. A comparison of arch width in adults with normal occlusion and adults with
class II, Division 1 malocclusion. Am J Orthod. 1985; 88: p. 163-69.
3. Tollaro L, Baccetti T, Franchi L, Tanasescu CD. Role of posterior transverse interarch discrepancy in class II,
Division 1 malocclusion during the mixed dentition phase. Am J Orthod. 1996; 110: p. 417-22.
4. Pancherz H. Hgg U. Dentofcial orhtopaedies in relation to somatic maturation. Am J Orthod. 1985; 88: p. 273-87.
5. Hagg U, Pancherz H. Dentofacial orhtopaedics in relation to chronological age. Growth period and skeletal
development: An analysis of 72 male patients with class II Division I malocclusion treated with the Herbst appliance.
Eur J Orthod. 1988; 10: p. 169-76.
6. McNamara JA Jr. Brudon WL. Orthodontics and orthopedic treatment in the mixed dentition.: Ann Arbor Needham
Press; 1993.
7. McNamara JA Jr. Peterson JE Jr, Alexander RG. Three dimensional diagnosis and management of class II
Dr Mayuresh J Baheti et al . / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
112 Dr Mayuresh J Baheti et al / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
malocclusion in the mixed dentition. Semin Orthod. 1996; 2: p. 114-37.
8. Jena AK, Duggal R. Parkash H. Skeletal and dentoalveolar effects of twin-block and bionator appliances in the
treatment of class II malocclusion: A comparative study. Am J Orthod Dentofacial Orthop. 2006; 130: p. 594-602.
9. Clark WJ. The twin block traction technique. Eur J Orthod. 1982; 4: p. 129-38.
10. Dyer FMV, McKeown HF, Sandier PJ. The modified twin block appliance in the treatment of class II Division 2
malocciusions. J Orthodont. 2001; 28((4)): p. 271-80.
11. Mills CM, Ma Culloch KJ. Treatment effects of twin block appliance: A cephalometric study. Am J Orthod
Dentofacial Orthop. 19981; 14: p. 15-24.
12. Harzer, et al. Molecular diagnosis in Orthodontics, Facial orthopedics and orthognathic surgery: Implications for
treatment progress and relapse. Semin Ortho. 2010; 16: p. 118-27.
13. McNamara. et al. Treatment timing for twin-block therapy. Am Orthod Dentofacial Orthop. 2000; 118: p. 159-70.
14. Camilla Tulloch, William R.Profitt, and Ceib Phillips. Outcomes in a 2-phase randomized clinical trial of early ClassII
treatment. Am J Orthod Dentofacial Orthop. 2004; 125: p. 657-67.
15. Kevin O’Brien et al. Early treatment for Class II Division 1 malocclusion with the Twin-block appliance:A multi-
center, randomized, controlled trial. Am J Orthod Dentofacial Orthop. 2009; 135: p. 573-9.
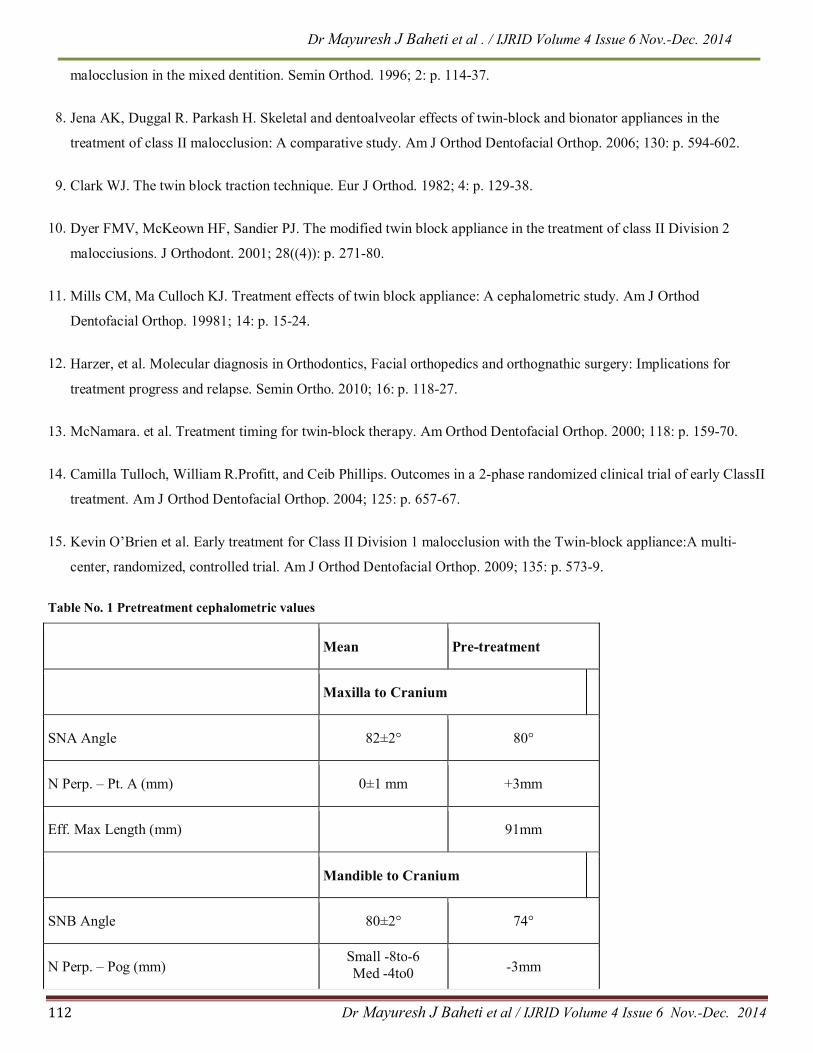
Table No. 1 Pretreatment cephalometric values
Mean Pre-treatment
Maxilla to Cranium
SNA Angle 82±2° 80°
N Perp. – Pt. A (mm) 0±1 mm +3mm
Eff. Max Length (mm) 91mm
Mandible to Cranium
SNB Angle 80±2° 74°
N Perp. – Pog (mm) Small -8to-6 Med -4to0 -3mm

Dr Mayuresh J Baheti et al . / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
113 Dr Mayuresh J Baheti et al / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
Large -2to2
Eff. Mand. Length (mm) 110mm
Saddle angle 1230±5 1280
Articular Angle (effect of ramus orientation) 1430±6 1400
Gonial Angle 1280±7 1280
Maxilla to Mandible (Skeletal)
ANB Angle 2±2° 6°
Wits (mm) 0 mm AO ahead of BO by
4mm
Difference between
Co Gn – Co A (mm)
19mm
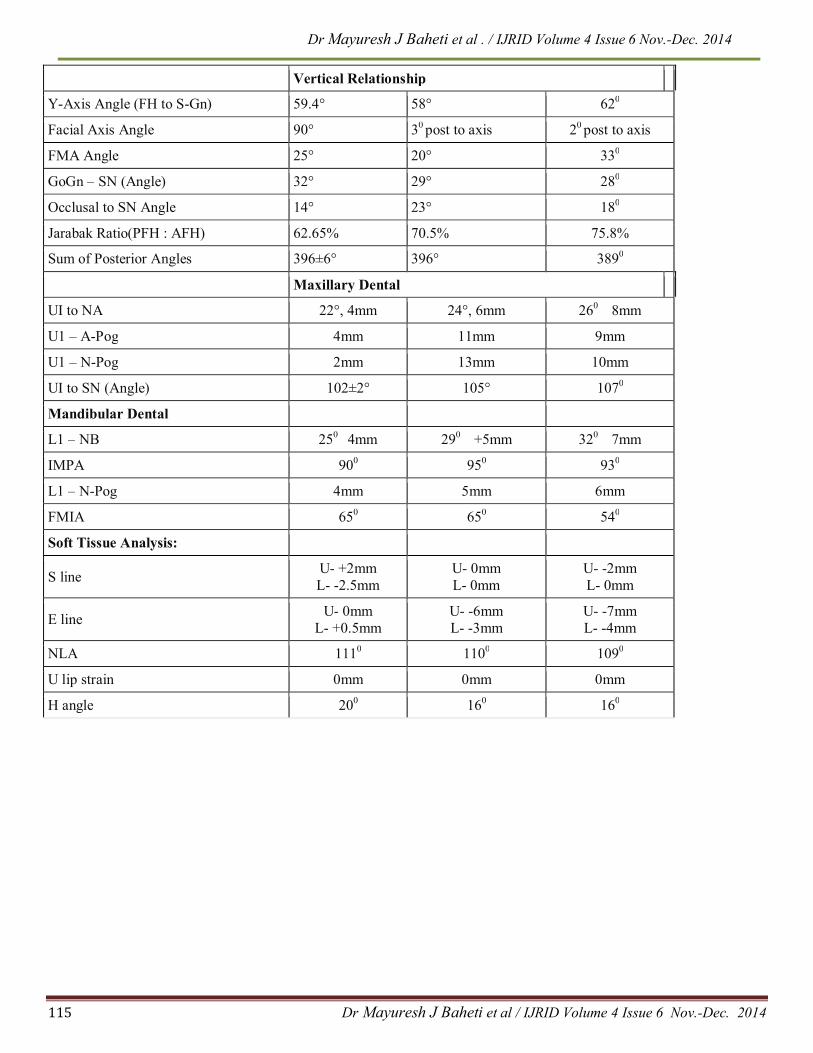
Vertical Relationship
Y-Axis Angle (FH to S-Gn) 59.4° 58°
Facial Axis Angle 90° 30 post to axis
FMA Angle 25° 20°
GoGn – SN (Angle) 32° 29°
Occlusal to SN Angle 14° 23°
Jarabak Ratio(PFH : AFH) 62.65% 70.5%
Sum of Posterior Angles 396±6° 396°
Maxillary Dental
UI to NA 22°, 4mm 24°, 6mm
U1 – A-Pog 4mm 11mm
U1 – N-Pog 2mm 13mm
UI to SN (Angle) 102±2° 105°
Mandibular Dental
L1 – NB 250 4mm 290 +5mm
IMPA 900 950
L1 – N-Pog 4mm 5mm
FMIA 650 650
Soft Tissue Analysis:
S line U- +2mm L- -2.5mm
U- 0mm L- 0mm

Dr Mayuresh J Baheti et al . / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
114 Dr Mayuresh J Baheti et al / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
E line U- 0mm
L- +0.5mm U- -6mm L- -3mm
NLA 1110 1100
U lip strain 0mm 0mm
H angle 200 160
Table No. 2 Comparison of pretreatment cephalometric values with posttreatment cephalometric values
Mean Pre-treatment Post-treatment
Maxilla to Cranium
SNA Angle 82±2° 80° 810
N Perp. – Pt. A (mm) 0±1 mm +3mm 0mm
Eff. Max Length (mm) 91mm 91mm
Mandible to Cranium
SNB Angle 80±2° 74° 790
N Perp. – Pog (mm) Small -8to-6 Med -4to0
Large -2to2
-3mm -3mm
Eff. Mand. Length (mm) 110mm 111mm
Saddle angle 1230±5 1280 1230
Articular Angle (effect of ramus orientation)
1430±6 1400 1410
Gonial Angle 1280±7 1280 1250
Maxilla to Mandible (Skeletal)
ANB Angle 2±2° 6° 20
Wits (mm) 0 mm AO ahead of BO by 4mm
BO ahead of AO by 3mm
Difference between
Co Gn – Co A (mm)
19mm 20mm
Dr Mayuresh J Baheti et al . / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
115 Dr Mayuresh J Baheti et al / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
Vertical Relationship
Y-Axis Angle (FH to S-Gn) 59.4° 58° 620
Facial Axis Angle 90° 30 post to axis 20 post to axis
FMA Angle 25° 20° 330
GoGn – SN (Angle) 32° 29° 280
Occlusal to SN Angle 14° 23° 180
Jarabak Ratio(PFH : AFH) 62.65% 70.5% 75.8%
Sum of Posterior Angles 396±6° 396° 3890
Maxillary Dental
UI to NA 22°, 4mm 24°, 6mm 260 8mm
U1 – A-Pog 4mm 11mm 9mm
U1 – N-Pog 2mm 13mm 10mm
UI to SN (Angle) 102±2° 105° 1070
Mandibular Dental
L1 – NB 250 4mm 290 +5mm 320 7mm
IMPA 900 950 930
L1 – N-Pog 4mm 5mm 6mm
FMIA 650 650 540
Soft Tissue Analysis:
S line U- +2mm L- -2.5mm
U- 0mm L- 0mm
U- -2mm L- 0mm
E line U- 0mm
L- +0.5mm U- -6mm L- -3mm
U- -7mm L- -4mm
NLA 1110 1100 1090
U lip strain 0mm 0mm 0mm
H angle 200 160 160
Dr Mayuresh J Baheti et al . / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
116 Dr Mayuresh J Baheti et al / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
(A) (B) (C) (D)
Fig. 1 Pretreatment Extraoral Photographs
(A) (B)
Fig. 2 Pretreatment Intraoral Photographs
(C) (D) (E)
Fig. 2 Pretreatment Intraoral Photographs

Dr Mayuresh J Baheti et al . / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
117 Dr Mayuresh J Baheti et al / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
Fig.3 Pretreatment Lateral Cephalogram
Fig. 4 Intraoral Photographs Showing Twinblock appliance in place
(A) (B) (C) (D)
Fig. 5 MidtreatmentExtraoral Photographs

Dr Mayuresh J Baheti et al . / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
118 Dr Mayuresh J Baheti et al / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
(A) (B) (C)
Fig. 6 Midtreatment Intraoral Photographs
(D) (E)
Fig. 6 Midtreatment Intraoral Photographs
(A) (B) (C)
Fig. 7 Preadjusted Fixed Appliance (MBT)
(D) (E)
Fig. 7 Preadjusted Fixed Appliance (MBT)

Dr Mayuresh J Baheti et al . / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
119 Dr Mayuresh J Baheti et al / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
(A) (B) (C) (D)
Fig. 8 PosttreatmentExtraoral Photographs
(A) (B) (C)
Fig. 9 Posttreatment Intraoral Photographs
(D) (E)
Fig. 9 Posttreatment Intraoral Photographs
Dr Mayuresh J Baheti et al . / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
120 Dr Mayuresh J Baheti et al / IJRID Volume 4 Issue 6 Nov.-Dec. 2014
Fig. 10 Posttreatment Lateral Cephalogram
(A) (B) (C)
Fig. 11 Activator as a Posttreatment Retainer
Fig. 12 Superimposition