Fine Needle Aspiration Cytology (FNAC) for Chinese Patients ...
Upload
khangminh22Category
view
0download
0
How to cite this article: Swapnil B Galat, M A Sameer. Study of bone marrow aspiration and basic haematological features for evaluation of anemia cases. MedPulse International Journal of Pathology. February 2020; 13(2): 86-91. https://www.medpulse.in/Pathology/
Original Research Article
Study of bone marrow aspiration and basic haematological features for evaluation of anemia cases
Swapnil B Galat1*, M A Sameer2
1Assistant Professor, Department of Pathology, Government Medical College, Chandrapur, Maharashtra, INDIA. 2Professor & HOD, Department of Pathology, Dr. Shankarrao Chavan Government Medical College, Nanded, Maharashtra, INDIA. Email: [email protected]
Abstract Background: Anaemia is common worldwide but prevalence of anaemia is disproportionately high in developing countries. It is only through the clinical, haematological and bone marrow examination findings that proper evaluation and management of patients with anaemia and hematological disorders can be made. Aim: To study the bone marrow aspiration and basic haematological features for evaluation of anemia cases. Material and Methods: Eighty-five patients with suspected haematological disorders were evaluated for different types of anaemia. These patients were subjected to routine haematological investigations and bone marrow aspiration. Results: Out of 55 anaemia cases, maximum number of cases were of Dimorphic anaemia i.e. 34 (61.8%%) cases, 11 (20%) cases were of Megaloblastic anaemia, 8 (14.5%) cases were of Iron deficiency anaemia, 2 (3.63%) cases were of Aplastic anemia. Conclusion: The present study concludes that detailed primary haematological investigations along with bone marrow aspiration are helpful for understanding the disease process. In a developing nation like ours bone marrow aspiration examination can be an easy and cost effective procedure in order to combat the nutritional anaemia. Keywords: Anaemia, peripheral smear, bone marrow aspiration, dimorphic anaemia
*Address for Correspondence: Dr. Swapnil B. Galat, Assistant Professor, Department of Pathology, Government Medical College, Chandrapur, Maharashtra, INDIA. Email: [email protected] Received Date: 18/12/2019 Revised Date: 14/01/2020 Accepted Date: 11/02/2020 DOI: https://doi.org/10.26611/10513212
INTRODUCTION Anaemia is common worldwide but prevalence of anaemia is disproportionately high in developing countries due to poverty, inadequate diet and poor access to health resources. Anaemia is not a diagnosis, but a manifestation of an underlying disorder. Thus, even mild asymptomatic anaemia should be investigated to diagnose and treat the primary cause.1 Without bone marrow examination the diagnosis of anaemia is not confirmatory. Bone marrow
examination also gives explanation for unexplained cytopenias, leukaemias and bleeding disorders.2 It gives more complete picture of the reaction of haematological tissue to anaemia.3 It is only through the clinical, haematological and bone marrow examination findings that proper evaluation and management of patients with anaemia and hematological disorders can be made. The present study was conducted to study the bone marrow aspiration and basic haematological features for evaluation of anemia cases. MATERIAL AND METHODS The present observational study was carried out in Department of Pathology, at tertiary care hospital after obtaining permission from Institutional Ethics Committee. The study subjects were enrolled using convenient sampling method through screening patients admitted from the clinical departments. Sample size Eighty-five patients with suspected haematological disorders.
Access this article online
Quick Response Code: Website: www.medpulse.in
Accessed Date:
10 February 2020
MedPulse International Journal of Pathology, Print ISSN: 2550-7605, Online ISSN: 2636-4697, Volume 13, Issue 2, February 2020 pp 86-91
Copyright © 2020, Medpulse Publishing Corporation, MedPulse International Journal of Pathology, Volume 13, Issue 2 February 2020
Inclusion criteria All cases of suspected haematological disorders
admitted at tertiary care centre in which bone marrow aspiration was advised by clinician.
Exclusion criteria Already diagnosed cases of haematological
disorders. Patients taking anticoagulant medications or those
with serious haemorrhagic disorders. Pregnant women.
Clinical history recording and examination of all the identified cases of pancytopenia were done. These patients were subjected to routine haematological investigations like; Complete blood count. Peripheral smear study. Bone marrow smears study. Serological study - For HIV infection. Hepatitis B surface antigen (HBs Ag), For
Dengue. Whole procedure was explained and written consent of patient was taken in each case either from patient or relative before starting the procedure. Bone marrow aspiration was performed from Posterior superior iliac spine under all aseptic conditions. Patients were referred to higher center for bone marrow biopsy in following conditions –Dry tap, to confirm diagnosis established on BM aspirate such as in aplastic anaemia. Bone marrow aspiration - These aspiration smears were dried, fixed and stained with Leishman’sstain and field stain. The peripheral smear was studied after staining with Leishman’s stain. Statistical analysis The data were entered into an MS Excel sheet, tabulated and was analysed using percentages, mean and median. Median was calculated by non-normalized data.
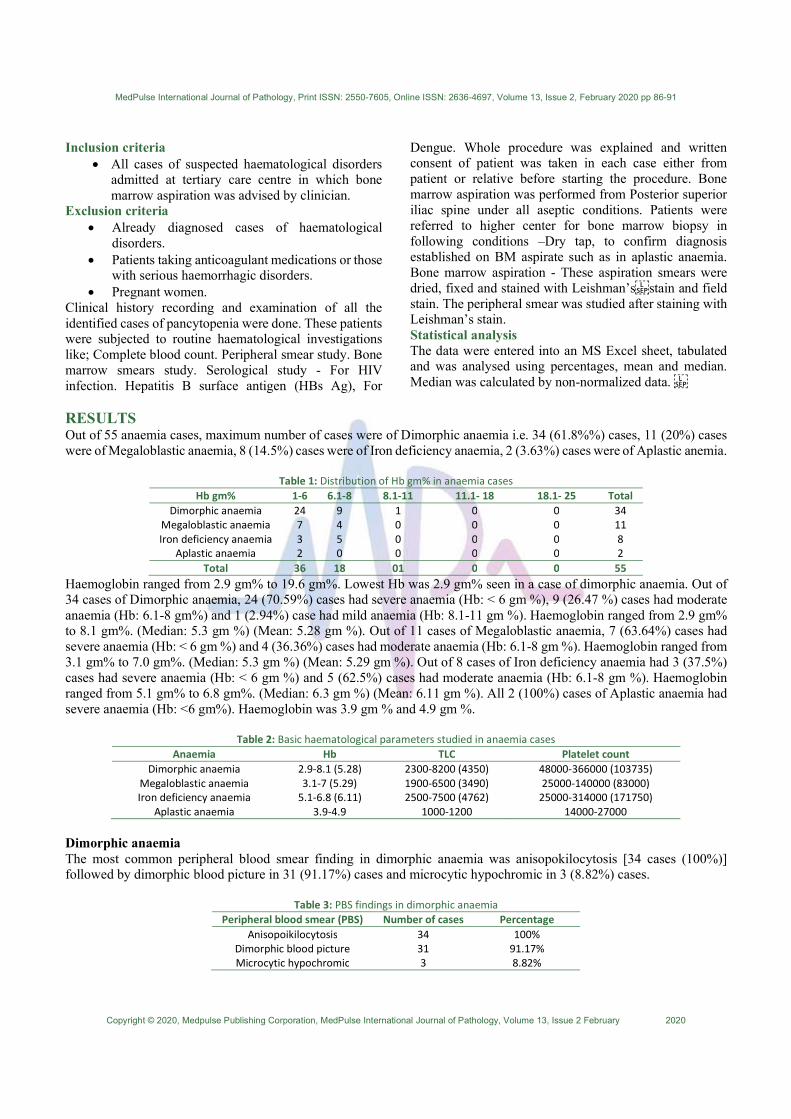
RESULTS Out of 55 anaemia cases, maximum number of cases were of Dimorphic anaemia i.e. 34 (61.8%%) cases, 11 (20%) cases were of Megaloblastic anaemia, 8 (14.5%) cases were of Iron deficiency anaemia, 2 (3.63%) cases were of Aplastic anemia.
Table 1: Distribution of Hb gm% in anaemia cases Hb gm% 1-6 6.1-8 8.1-11 11.1- 18 18.1- 25 Total
Dimorphic anaemia 24 9 1 0 0 34 Megaloblastic anaemia 7 4 0 0 0 11 Iron deficiency anaemia 3 5 0 0 0 8
Aplastic anaemia 2 0 0 0 0 2 Total 36 18 01 0 0 55
Haemoglobin ranged from 2.9 gm% to 19.6 gm%. Lowest Hb was 2.9 gm% seen in a case of dimorphic anaemia. Out of 34 cases of Dimorphic anaemia, 24 (70.59%) cases had severe anaemia (Hb: < 6 gm %), 9 (26.47 %) cases had moderate anaemia (Hb: 6.1-8 gm%) and 1 (2.94%) case had mild anaemia (Hb: 8.1-11 gm %). Haemoglobin ranged from 2.9 gm% to 8.1 gm%. (Median: 5.3 gm %) (Mean: 5.28 gm %). Out of 11 cases of Megaloblastic anaemia, 7 (63.64%) cases had severe anaemia (Hb: < 6 gm %) and 4 (36.36%) cases had moderate anaemia (Hb: 6.1-8 gm %). Haemoglobin ranged from 3.1 gm% to 7.0 gm%. (Median: 5.3 gm %) (Mean: 5.29 gm %). Out of 8 cases of Iron deficiency anaemia had 3 (37.5%) cases had severe anaemia (Hb: < 6 gm %) and 5 (62.5%) cases had moderate anaemia (Hb: 6.1-8 gm %). Haemoglobin ranged from 5.1 gm% to 6.8 gm%. (Median: 6.3 gm %) (Mean: 6.11 gm %). All 2 (100%) cases of Aplastic anaemia had severe anaemia (Hb: <6 gm%). Haemoglobin was 3.9 gm % and 4.9 gm %.
Table 2: Basic haematological parameters studied in anaemia cases Anaemia Hb TLC Platelet count
Dimorphic anaemia 2.9-8.1 (5.28) 2300-8200 (4350) 48000-366000 (103735) Megaloblastic anaemia 3.1-7 (5.29) 1900-6500 (3490) 25000-140000 (83000) Iron deficiency anaemia 5.1-6.8 (6.11) 2500-7500 (4762) 25000-314000 (171750)
Aplastic anaemia 3.9-4.9 1000-1200 14000-27000 Dimorphic anaemia The most common peripheral blood smear finding in dimorphic anaemia was anisopokilocytosis [34 cases (100%)] followed by dimorphic blood picture in 31 (91.17%) cases and microcytic hypochromic in 3 (8.82%) cases.
Table 3: PBS findings in dimorphic anaemia Peripheral blood smear (PBS) Number of cases Percentage
Anisopoikilocytosis 34 100% Dimorphic blood picture 31 91.17% Microcytic hypochromic 3 8.82%

Swapnil B Galat, M A Sameer
MedPulse International Journal of Pathology, Print ISSN: 2550-7605, Online ISSN: 2636-4697, Volume 13, Issue 2, February 2020 Page 88
Bone marrow aspirate from 33 (97.06%) cases showed hypercellularity while 1 (2.94%) case showed normocellularity. All 34 (100%) cases showed erythroid hyperplasia with micronormoblastic and megaloblastic maturation with giant metamyelocytes and band forms while megakaryocytic series was normal in number and morphology. In our study, assessment of bone marrow iron store by Perl’s Prussian blue reaction was done in 34 cases of dimorphic anaemia out of which ,15 cases (44.12%) showed 2+ grade, 8 cases (23.53%) grade 1+, 5 cases (14.71%) grade zero, 4 cases(11.76%) grade 3+, and 2 cases(5.88%) grade 4+ of iron store.
Table 4: Bone marrow (BM) findings in dimorphic anaemia
BM aspiration finding Cellularity M:E ratio Erythroid series Myeloid series Megakaryocyte
series
Dimorphic anaemia Hyper- cellular Decreased
Erythroid hyperplasia with micronormoblastic and
megaloblastic maturation
Normal progressive maturation with giant metamyelocytes and
band form
Normal in number and morphology
Megaloblastic anaemia The most common peripheral blood smear finding in megaloblastic anemia was macrocytic hypochromic in all 11
(100%) followed by Hypersegmented neutrophil in 9 (81.81%) cases whereas anisopokilocytosis was found in 3 (27.27%) cases.
Table 5: Distribution of PBS finding in megaloblastic anaemia
Peripheral blood smear (PBS) Number of cases Percentage Macrocytic hypochromic 11 100%
Hypersegmented neutrophil 9 81.81% Anisopoikilocytosis 3 27.27%
Table 6: Bone marrow (BM) findings in megaloblastic anaemia
BM aspiration finding
Cellularity M:E ratio Erythroid series Myeloid series Megakaryo- cyte series
Megaloblastic anaemia
Hyper- cellular Decre- ased Erythroid hyperplasia with
megaloblastic maturation
Normal progressive maturation with giant metamyelocytes and
giant band form
Normal to increase in
number, increase in size
Bone marrow aspirate from all cases of megaloblastic anaemia showed hypercellularity with erythroid hyperplasia with megaloblastic change. Myelopoiesis showed giant metamyelocytes and giant band forms while megakaryocytic series was normal to increase in number and increase in size. Bone marrow iron study assessment was done in 11 cases of megaloblastic anaemia out of which 6 cases (54.55%) showed 3+ grade, 4 cases (36.36%)grade 4+, 1 case(9.09%) grade 1+ of iron store. Iron deficiency anaemia
In Present Study, the most common peripheral blood smear finding in iron deficiency anaemia was microcytic hypochromic in all 8 (100%) cases.
Table 7: Bone marrow (BM) findings in Iron Deficiency anaemia BM aspiration
finding Cellularity M:E ratio Erythroid series Myeloid series Megakaryocyte series
Iron deficiency anaemia
Hyper- cellular Decre- ased Erythroid hyperplasia with micronormoblastic
maturation
Normal in maturation and morphology
Normal in maturation and morphology
Bone marrow aspirate from all cases of iron deficiency anaemia showed hypercellularity with erythroid hyperplasia with micronormoblastic change while myeloid and megakaryocytes series showed normal maturation and morphology. Bone marrow iron study assessment was done in 8 cases of iron deficiency anaemia out of which 6 cases (75%) showed zero grades and 2 cases (25%) grade 1+ of iron store.

MedPulse International Journal of Pathology, Print ISSN: 2550-7605, Online ISSN: 2636-4697, Volume 13, Issue 2, February 2020 pp 86-91
Copyright © 2020, Medpulse Publishing Corporation, MedPulse International Journal of Pathology, Volume 13, Issue 2 February 2020
Aplastic anaemia Peripheral smears of both the cases of aplastic anaemia were normocytic hypochromic.
Table 8: Bone marrow (BM) findings in aplastic anaemia BM aspiration
finding Cellu- larity M:E ratio Erythroid series
Myeloid series Megakaryocyte series
Aplastic anaemia
Hypo- cellular
Altered/ Decreased
Suppressed Suppressed Suppressed
Bone marrow aspirate from all cases of aplastic anaemia showed increase fat spaces and decreased cellularity. Myelopoiesis, erythropoiesis and megakaryopoiesis markedly decreased and relatively increase in lymphocytes and plasma cells are seen. Bone marrow iron study assessment was done in 2 cases of aplastic anemia out of which 1 case (50%) showed 2+ grade and 1 case (50%) grade 1+.
Figure 1a Figure 1b Figure 2a Figure 2b Figure 3 Figure. 1: a. Peripheral Blood Smear showing microcytes, macrocytes and macro-ovalocytes- Dimorphic Anaemia (Leishman’s stain, 40x); b. Bone marrow aspirate showing erythroid hyperplasia with micronormoblastic and megaloblastic maturation - Dimorphic anaemia (Leishman’s stain- 40x); Figure 2: Peripheral smear showing Hypersegmented neutrophil from a case of Megaloblastic anaemia. (Leishman’s stain, 100x magnified); b. Bone marrow aspiration smear showing megaloblastic maturation with royal blue cytoplasm and sieve like chromatin along with Band form (band form) - Megaloblastic anaemia. (Leishman’s Stain, 100x); Figure 3: Bone marrow aspirate showing erythroid hyperplasia with micronormoblastic maturation - Iron Deficiency anaemia (Leishman’s stain- 40x). DISCUSSION In our study we found dimorphic anaemia as the most common haematological disorder followed by megaloblastic anaemia. The high prevalence of dimorphic maturation is explained by the occurrence of nutritional deficiencies in rural areas. Nutritional deficiencies of both iron and folate commonly occur together, more commonly in pregnant women. Iron deficiency occurring concurrently with megaloblastic anaemia has been reported in many areas. In some instances, the megaloblastosis may be intermediate in degree but may become more marked after administration of iron, and some cases of severe dimorphic anaemia do not respond initially to iron therapy, probably owing to concomitant severe folate and occasionally Vitamin B12 deficiency. Hence, findings of the present study correlate well with other studies from India and other sub-continental studies. This seems to reflect the higher prevalence of nutritional anaemia in Indian subjects. Tilak V and Jain R4 found megaloblastic anaemia (68%) as the commonest cause followed by aplastic anaemia (7.70%). BN Gayathri and Kadam SR5 found megaloblastic anaemia (74.04%) as the most common cause followed by aplastic anaemia (18.26%). Thiyagarajan P et al6 found Dimorphic anaemia (38.4) as most common haematological disorder
followed by megaloblastic anaemia (33.4%). Merla J et al7 found Dimorphic anaemia (26.59%) as most common followed by iron deficiency anaemia (16.92%). Dimorphic anaemia Dimorphic anaemia showed combination of varying proportion of iron deficiency and megaloblastic anaemia. Dimorphic anaemia was the commonest (40%) non-malignant cause of anaemia in our study and it is consistent with study by Thiyagarajan et al6 and Kulkarni N et al.8 In the study by Gore CR et al9 dimorphic anaemia (49.3%) was the most common finding. Majority of these patients are usually diagnosed on basis of complete blood count, red cell indices, red cell distribution width, peripheral blood smear examination, serum ferritin/ iron levels, serum vitamin B12 levels, serum and red cell folate levels. These patients needed bone marrow for diagnosis because many of them had atypical presentations like concomitant fever, organomegaly and petechiae. Also bone marrow was needed to confirm nutritional deficiency anaemia or rule out haematological malignancies. Most common peripheral smears findings in our study were anisopoikilocytosis with dimorphic blood picture that was consistent with the study by R Athar et al.10 Bone Marrow findings in cases of Dimorphic anaemia showed usually hypercellularity in 33 (97.06%) cases and normocellularity

Swapnil B Galat, M A Sameer
MedPulse International Journal of Pathology, Print ISSN: 2550-7605, Online ISSN: 2636-4697, Volume 13, Issue 2, February 2020 Page 90
in 1 (2.94%) case. All cases showed erythroid hyperplasia with micronormoblastic and megaloblastic maturation. Giant band form, giant metamyelocytes were also seen. In study by R Athar et al,10 bone marrow studied in 58 cases of dimorphic anaemia which showed hypercellularity with micronormoblastic and megaloblastic change and trilineage dyspoiesis. In the study by Garg P et al.11 All marrows were hypercellular, showing erythroid hyperplasia (100%). Giant metamyelocytes were seen in all the bone marrow. In the study by Deepthi A et al.12 bone marrow examinations showed normocellular marrow (32.36%) and hypercellular marrow (67.74%). Erythroid series showed hyperplasia with megaloblastic and micronormoblastic maturation. All of these cases also showed giant metamyelocytes. Bone marrow iron stores were reduced (grade 0 to 1+) in 13 cases (38.23%) and were normal to increased (grade 2+ to 4+) in 21 (61.77%) cases. Pujara et al13 found observation close to our study and all of the cases in their study showed normal to increased (2+ to 3+) iron store in cases of dimorphic anaemia. Megaloblastic anaemia In the study by Kumar R et al14 in megaloblastic anaemia patients Hb was in range of 2.4-7 gm/dl, TLC in range of 700-3600/cumm and platelet in range of 10,000-130000/cumm. In the study by Jha A et al.15 Hb was in range of 2.3-9.8 gm/dl, TLC in range of 1200-3900/cumm and platelet in range of 2000-137000/cumm. BN Gayathri and Kadam SR,5 in megaloblastic anaemia patients found Hb in range of 1.8-9.2 gm/dl, TLC in range of 500-3900/cumm and platelet in range of 12,000-95,000/cumm. Anaemia, Leukopenia and Thrombocytopenia are attributed to ineffective haematopoiesis in megaloblastic anaemia. The principal hematologic manifestations are varying degrees of anaemia, leukopenia and thrombocytopenia, anisopoikilocytosis, macro-ovalocytes and hypersegmented neutrophils. In the present study macro-ovalocytes (100%), hypersegmented neutrophils (81.81%) along with considerable degree of anisopoikilocytosis (27.27%) were the main features on peripheral blood smear examination. In the study by Tilak V et al4 96.22% cases showed anisocytosis, 84.90% cases showed hypersegmented neutrophils, 24.52% cases showed circulating erythroblasts. In the study by Khodke K et al16 90.90% cases showed anisocytosis and 90.90% cases showed hypersegmented neutrophils. In the study BN Gayathri and Kadam SR5 hypersegmented neutrophils were noted in 51.35% cases. Hence, peripheral blood smear findings are consistent with above studies and are attributed to ineffective haematopoiesis in megaloblastic anaemia. In the present study bone marrow aspirate from all the cases [11 (100%)] showed erythroid hyperplasia with
megaloblastic maturation. Myelopoiesis showed giant metamyelocytes and giant band forms. In the study by Chandra K et al17 bone marrows in cases of megaloblastic anaemia was hypercellular (100%) with characteristic megaloblastic erythropoiesis overrepresented by early erythroid cells in comparison with mature forms due to ineffective erythropoiesis. Features of dysmyelopoiesis were evident in the form of giant metamyelocytes and band forms. Megakaryocytes were hyperlobated. In a study by Gandhi P et al,18 bone marrow aspirates were hypercellular (67.91%) and showed megaloblastosis. Bone marrow iron stores were decreased (grade 0 to 1+) in 1 (9.10%) case and were normal to increased (grade 2 + to 4+) in 10 (90.9%) cases. In the study by Pujara et al13 found increased (3+ to 4+) iron store in 70% cases of megaloblastic anaemia, which is consistent with our study. Findings in present study are consistent with findings of above studies and are attributed to ineffective haematopoiesis in megaloblastic anaemia. Iron Deficiency Anaemia In present study microcytic hypochromic (100%) was most common blood picture. The bone marrow was hypercellular with reduction of fat cells in all patients (100%). Erythroid hyperplasia with micronormoblastic maturation was seen in all the cases. Myeloid and megakaryocytes series showed normal maturation and morphology. The bone marrow study by Javalgi et al19 showed hypercellularity with altered M: E ratio and increased erythropoiesis showing micronormoblasts in most of the cases. Myelopoiesis was normal and there was slight increase in megakaryocytes. In our study, bone marrow iron stores were within 0 to 1+ that is decreased to completely absence of iron store was seen in all the (100%) cases. It is consistent with study by Pujara et al13 found 92.7% cases iron store in iron deficiency anaemia within range of 0 to 1+ grades. Aplastic anaemia Among haematological parameters, Hb was 3.9 gm% and 4.9 gm%. TLC was 1000/cumm and 1200/cumm while Platelet count was 14000/cumm and 27000/cumm. Both cases had normocytic and hypochromic blood picture on peripheral smear. Bone marrow aspirate was hypocellular and the aspirate was mostly composed of fat cells in all (100%) the patients. There was relative increase in plasma cells and lymphocytes. Both cases were referred to higher haematological centre where bone marrow trephine biopsy was done and it revealed replacement of marrow by fat cells. Daniel NM et al.20 in their analysis of 50 cases reported 74 % of patients with hypocellular marrow, 16% of patients had normocellular marrow which later became hypocellular. 10% had acellular marrow. In a study by Gandhi P et al,18 bone marrow was hypocellular in 100%

MedPulse International Journal of Pathology, Print ISSN: 2550-7605, Online ISSN: 2636-4697, Volume 13, Issue 2, February 2020 pp 86-91
Copyright © 2020, Medpulse Publishing Corporation, MedPulse International Journal of Pathology, Volume 13, Issue 2 February 2020
of aplastic anaemia cases. Cellularity of bone marrow in aplastic anaemia is very much reduced. It can be hypocellular or acellular. Lymphocytes and plasma cells are prominent. Bone marrow iron stores were decreased (grade 0 to 1+) in both cases. Pujara et al (2014)57, found 66.6 % cases in received in the range of zero to 1+ grade. CONCLUSION The present study concludes that detailed primary haematological investigations along with bone marrow aspiration are helpful for understanding the disease process. Bone marrow aspiration examination is an important step to arrive at the confirmatory diagnosis of broad-spectrum haematological disorders and anaemia. In a developing nation like ours it can be an easy and cost effective procedure in order to combat the nutritional anaemia. REFERENCES 1. Tahlan A, Bansal C, Palta A, Chauhan S. Spectrum and
analysis of bone marrow findings in anemic cases. Indian J Med Sci 2008;62(8):336-9.
2. Kibria SG, Islam MDU, Chowdhury ASMJ et al. Prevalence 0f Hematological Disorder: A Bone Marrow Study of 177 Cases In A Private Hospital At Faridpur. Faridpur Med. Coll. J., 2010; 5: 11-3.
3. Egesie OJ, Joseph DE, Egesie UG, Ewuga OJ. Epidemiology of anemia necessitating bone marrow aspiration cytology in Jos. Niger Med J., 2009; 50: 61-1.
4. Tilak V, Jain R. Pancytopenia - A clinico-hematologic Analysis of 77 cases. Indian J Pathol Microbiol.1999; 42:399-404.
5. Gayathri BN and Kadam SR. Pancytopenia- A Clinico Hematological Study. J Lab Physicians.2011;3(1):15-20.
6. Thiyagarajan P, Narayanarao Suresh T, Anjanappa R, Harendra Kumar ML. Bone-marrow spectrum in a tertiary care hospital: Clinical indications, peripheral smear correlation and diagnostic value. Med J Dr DY Patil Univ 2015; 8(4):490-494.
7. Merla J, Durai S, Shantaraman K. Bone Marrow Aspiration Evaluation in Clinical Management of Anemia Among Low Socioeconomic Group In A Tertiary Care Hospital. IOSR
Journal of Dental and Medical Sciences (IOSR-JDMS). 2017; 16(7): 89-97.
8. Kulkarni N, Patil A, Karchi S. Study of Pancytopenia in a Tertiary Care Hospital in North Karnataka. International Journal of Medical Research and Health Sciences. 2017;6(3):61-67.
9. Gore CR, Bardapurkar PR, Paranjape S, Patel S, Karia K. Clinico- hematological evaluation of pancytopenic adults in a tertiary care institution. Ind J Pathol Oncol 2018;5(3):391-397.
10. R Athar, Y Khonglah, V Raphael, A Pal, KG Lynrah. Clinico-haematological and Biochemical Profile of Dimorphic Anemia with Bone Marrow Study. The Internet J Lab Med 2014; 6(1):1-8.
11. Garg P, Dey B, Deshpande AH, Bharti JN, Nigam JS. Clinico‐ hematological profile of dimorphic anemia. J Appl Hematol 2017;8:123-4.
12. Deepthi. A, CSBR Prasad, Raghavendra Prasad B. N.. Study of dimorphic anemia in adults with reference to basic etiology. Indian Journal of Pathology and Oncology. 2018;5(1):61-66.
13. Pujara KM, Bhalara RV, Dhruva GA. A study of bone marrow iron storage in hematological disorder. Int J Health Allied Sci 2014;3:221-4.
14. Kumar R, Kalra SP, Kumar H, Anand AC, Madan H. Pancytopenia - A six year Study. JAPI. 2001; 49:1078-1081.
15. Jha A, Sayami G, Adhikari RC, Panta AD, Jha R. Bone marrow examination in cases of pancytopenia. J Nepal Med Assoc. 2008;47(169):12-17.
16. Khodke K, Marwah S, Buxi G, Yadav RB, Chaturvedi NK. Bone Marrow Examination in Cases of Pancytopenia. J Indian Academy of Clin Med. 2001;2:55-59.
17. Chandra K, Kumar P. Morphological Spectrum of Bone Marrow In Pancytopenia – A Retrospective Study In A Tertiary Care Centre. Journal of Evolution of Medical And Dental Sciences. 2014;3(4):1056-1064.
18. Gandhi P, Shankar T, Pasha M, G0uri M. Etiological and clinical spectrum of pancytopenia based on bone marrow examination and case records: A retrospective study. Annals of Applied Bio-Sciences. 2016;3(1):A27-A32.
19. Javalgi AP, Dombale VD. Clinico – Hematological Analysis of Pancytopenia: A Bone Marrow Study. National Journal of Laboratory Medicine. 2013; 2(4): 12-17.
20. Daniel NM, Byrd S. Aplastic anemia: an analysis of 50 cases. Ann intern Med. 1958; 49: 326-336.
Source of Support: None Declared Conflict of Interest: None Declared
Copyright © 2022 FDOKUMEN