
Clinical and Genetic Analysis of Unclassifiable Inherited Bone Marrow Failure Syndromes
12
DOI: 10.1542/peds.2007-3415 2008;122;e139 Pediatrics Hand, Elena Tsangaris, Isaac Odame, Joseph Beyene and Yigal Dror Sharon Abish, MacGregor Steele, Kaiser Ali, Uma Athale, Lawrence Jardine, John P. Josette Champagne, Mariana Silva, Jeffrey H. Lipton, Jossee Brossard, Yvan Samson, Juliana T. Teo, Robert Klaassen, Conrad V. Fernandez, Rochelle Yanofsky, John Wu, Syndromes Clinical and Genetic Analysis of Unclassifiable Inherited Bone Marrow Failure http://pediatrics.aappublications.org/content/122/1/e139.full.html located on the World Wide Web at: The online version of this article, along with updated information and services, is of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2008 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point publication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly by guest on June 5, 2013 pediatrics.aappublications.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Clinical and Genetic Analysis of Unclassifiable Inherited Bone Marrow Failure Syndromes

DOI: 10.1542/peds.2007-3415 2008;122;e139Pediatrics
Hand, Elena Tsangaris, Isaac Odame, Joseph Beyene and Yigal DrorSharon Abish, MacGregor Steele, Kaiser Ali, Uma Athale, Lawrence Jardine, John P.Josette Champagne, Mariana Silva, Jeffrey H. Lipton, Jossee Brossard, Yvan Samson, Juliana T. Teo, Robert Klaassen, Conrad V. Fernandez, Rochelle Yanofsky, John Wu,
SyndromesClinical and Genetic Analysis of Unclassifiable Inherited Bone Marrow Failure
http://pediatrics.aappublications.org/content/122/1/e139.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2008 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on June 5, 2013pediatrics.aappublications.orgDownloaded from

ARTICLE
Clinical and Genetic Analysis of UnclassifiableInherited Bone Marrow Failure SyndromesJuliana T. Teo, MBBS, FRACP, FRCPAa, Robert Klaassen, MD, FRCPCb, Conrad V. Fernandez, Hon BSc, MD, FRCPCc,
Rochelle Yanofsky, MD, FRCPCd, John Wu, MD, FRCPCe, Josette Champagne, MD, FRCPCf, Mariana Silva, MD, FRCPCg,
Jeffrey H. Lipton, MD, PhD, FRCPCh, Jossee Brossard, MD, FRCPCi, Yvan Samson, MD, FRCPCj, Sharon Abish, MD, FRCPCk,
MacGregor Steele, MD, FRCPCl, Kaiser Alim, Uma Athale, MD, FRCPCn, Lawrence Jardine, BmS, MD, FRCPCo, John P. Hand, MD, FRCPCp,
Elena Tsangaris, MSc, Sca, Isaac Odame, MB, ChB, MRCP, FRCPCH, FRCPath, FRCPCa, Joseph Beyene, PhD, MSc, BScq, Yigal Dror, MD, FRCPCa
aMarrow Failure and Myelodysplasia Program, Division of Haematology/Oncology and Cell Biology Program, Research Institute, The Hospital for Sick Children and theUniversity of Toronto, Toronto, Ontario; bDivision of Haematology/Oncology, Children’s Hospital of Eastern Ontario, Ottawa, Ontario; cDivision of Haematology/Oncology,Isaak Walton Killam Hospital for Children, Halifax, Nova Scotia ; dDivision of Haematology/Oncology, CancerCare Manitoba, Winnipeg, Manitoba; eDivision ofHaematology/Oncology, British Columbia Children’s Hospital, Vancouver, British Columbia ; fDivision of Haematology/Oncology, Hopital Ste. Justine, Montreal, Quebec;gDepartment of Medicine, Queen’s University, Kingston, Ontario; hDepartment of Haematology, Princess Margaret Hospital, Toronto, Ontario; iDivision of Haematology/Oncology, Centre U Sante de l’Estrie-Fleur, Sherbrooke, Quebec ; jDivision of Haematology/Oncology, Centre Hospital University Quebec-Pav CHUL, Sainte-Foy, Quebec;kDivision of Haematology/Oncology, Montreal Children’s Hospital, Montreal, Quebec ; lDepartment of Medicine, Alberta Children’s Hospital, Calgary, Alberta; mDivision ofHaematology/Oncology, University of Saskatchewan, Saskatoon, Saskatchewan ; nDivision of Haematology/Oncology McMaster Children’s Hospital/McMaster UniversityHealth Sciences Centre, Hamilton, Ontario; oChildren’s Hospital of Western Ontario, London, Ontario; pDivision of Haematology/Oncology Janeway Child Health Centre,St. John’s, Newfoundland ; qPopulation Health Sciences, Research Institute, The Hospital For Sick Children, Toronto, Ontario
The authors have indicated they have no financial relationships relevant to this article to disclose.
What’s Known on This Subject
Thus far, only case reports of UC-IBMFSs have been published, and the clinical andeconomic challenges posed by patients with such disorders are unknown.
What This Study Adds
This is the first comprehensive analysis of a cohort of patientswithUC-IBMFSs.We reportthe prevalence, clinical characteristics, and cost of genetic testing. The results provideuseful information for general pediatricians and pediatric hematologists.
ABSTRACT
OBJECTIVE.Unclassified inherited bone marrow failure syndromes are a heterogeneousgroup of genetic disorders that represent either new syndromes or atypical clinicalcourses of known inherited bone marrow failure syndromes. The relative prevalenceof the unclassified inherited bone marrow failure syndromes and their characteristicsand the clinical and economic challenges that they create have never been studied.
METHODS.We analyzed cases of inherited bone marrow failure syndrome in the Cana-dian Inherited Marrow Failure Registry that were deemed unclassifiable at studyentry.
RESULTS. From October 2001 to March 2006, 39 of the 162 patients enrolled in theCanadian Inherited Marrow Failure Registry were registered as having unclassifiedinherited bone marrow failure syndromes. These patients presented at a significantlyolder age (median: 9 months) than the patients with classified inherited bonemarrow failure syndrome (median: 1 month) and had substantial variation in theclinical presentations. The hematologic phenotype, however, was similar to theclassified inherited bone marrow failure syndromes and included single- or multiple-lineage cytopenia, severe aplastic anemia, myelodysplasia, and malignancy. Group-ing patients according to the affected blood cell lineage(s) and to the presence ofassociated physical malformations was not always sufficient to characterize a condi-tion, because affected members from several families fit into different phenotypicgroups. Compared with the classified inherited bone marrow failure syndromes, thepatients with unclassified inherited bone marrow failure syndromes had 3.2 morespecific diagnostic tests at 4.5 times higher cost per evaluated patient to attempt tocategorize their syndrome. At last follow-up, only 20% of the unclassified inheritedbone marrow failure syndromes were ultimately diagnosed with a specific syndrome on the basis of the developmentof new clinical findings or positive genetic tests.
CONCLUSIONS.Unclassified inherited bone marrow failure syndromes are relatively common among the inherited bonemarrow failure syndromes and present a major diagnostic and therapeutic dilemma. Pediatrics 2008;122:e139–e148
www.pediatrics.org/cgi/doi/10.1542/peds.2007-3415
doi:10.1542/peds.2007-3415
KeyWordsunclassifiable inherited marrow failure,myelodysplastic syndrome, aplastic anemia
AbbreviationsIBMFS—inherited bone marrow failuresyndromeUC-IBMFS—unclassifiable inherited bonemarrow failure syndromeCIMFR—Canadian Inherited MarrowFailure RegistryC-IBMFS—classifiable inherited bonemarrow failure syndrome
Accepted for publication Jan 14, 2008
Address correspondence to Yigal Dror, MD,Hospital for Sick Children, Division ofHaematology/Oncology and the Cell BiologyProgram, 555 University Ave, Toronto, Ontario,Canada M5G 1X8. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005;Online, 1098-4275). Copyright © 2008 by theAmerican Academy of Pediatrics
PEDIATRICS Volume 122, Number 1, July 2008 e139 by guest on June 5, 2013pediatrics.aappublications.orgDownloaded from

INHERITED BONE MARROW failure syndromes (IBMFSs)are a heterogeneous group of genetic disorders char-
acterized by varying degrees of peripheral cytopenias,resulting from inadequate hematopoiesis.1,2 These disor-ders may involve multiple lineages (eg, Fanconi anemia)or predominantly single cytopenias (eg, Kostmann neu-tropenia, Diamond-Blackfan anemia) and, hence, havebeen traditionally classified according to the affectedlineage(s). Disorders involving multiple lineages maypresent with single cytopenia before progressing to pan-cytopenia. The composition and severity of physical mal-formations varies widely within each syndrome, and thecomplete phenotypes of some IBMFSs remain unclear.There is also a substantial overlap in hematologic andphysical manifestations between the disorders. Further-more, because characteristic hematologic abnormalitiesor physical malformations can develop later in life andare not always congenital (eg, nail dystrophy in dysker-atosis congenita), the diagnostic criteria do not alwaysexist at presentation. For these reasons, the diagnosis ofa specific IBMFS in an individual patient is frequentlydifficult, which may lead to misdiagnosis and impropertreatment.
Individual cases of IBMFSs that could not be catego-rized as having a known syndrome have been reportedand were partially reviewed elsewhere.2 Such cases maylead to multiple invasive and costly investigations, delayin diagnosis, misdiagnosis, inappropriate treatment, oruncertainties with regard to the natural history. Theprevalence and characteristics of unclassified IBMFSs(UC-IBMFSs) have never been prospectively studied,and the magnitude of the problem is unknown. TheCanadian Inherited Marrow Failure Registry (CIMFR)was established in January 2001.3 It is a prospective,multicenter study that intends to register all patientswith IBMFSs in Canada. The CIMFR aims to investigatethe prevalence, clinical phenotype, and the natural his-tory of IBMFSs. Herein, we analyzed 39 cases with UC-IBMFS at the time of enrollment on the CIMFR. Weasked whether the cases can be grouped according totheir hematologic and nonhematologic manifestations toidentify patterns and propose guidelines for workup. Theclinical, laboratory, and genetic workup were comparedwith cases of classified IBMFSs (C-IBMFSs), and thediagnostic challenges are described.
METHODS
RegistryThe CIMFR study was approved by the institutionalethics board of all of the participating institutions, whichinclude 15 of 17 pediatric tertiary care centers across allprovinces in Canada. Patients who received a diagnosisof an IBMFS (criterion 2 in Table 1) were recruited byhematologists at each center. Published diagnostic crite-ria were used for the specific syndromes.1,2 Patients withthe following groups of disorders were excluded: (1)leukemia with an inherited syndrome not associatedwith antecedent marrow failure; (2) acquired aplasticanemia (patients who have aplastic anemia and do notfulfill the criteria in Table 1); (3) de novo myelodysplas-
tic syndrome; and (4) de novo leukemia. Written con-sent was obtained from recruited patients or guardians.
Information collected on standardized forms includeddemographics, diagnosis, symptoms, family history,physical malformations, laboratory tests and imagingstudies, treatment, and outcomes. Outcomes recordedincluded severe cytopenia(s), aplastic anemia, myelo-dysplasia, marrow cytogenetic abnormalities, leukemia,solid tumors, marrow transplantation, and death. Fol-low-up information was collected on an annual basis.The data collected were managed by the central CIMFRoffice located at the Hospital for Sick Children (Toronto,Ontario, Canada).
Data AnalysisWe analyzed the clinical phenotype and short-term out-come of patients with UC-IBMFSs on the registry as ofMarch 2006, by using data from the CIMFR database.The criteria for the diagnosis of UC-IBMFSs are summa-rized in Table 1. We performed descriptive analysis. Stu-dent’s t test was used to determine the statistical signif-icance of differences between the UC-IBMFSs and theclassifiable IBMFSs (C-IBMFSs) for continuous vari-ables, and Fisher’s exact test was used to compare cate-gorical variables. P � .05 was considered statisticallysignificant. Statistical analyses were conducted by usingSAS 9.1 (SAS Institute, Inc Cary, NC). Probability ofdeath according to age was estimated by using a Kaplan-Meier plot.
RESULTS
General Characteristics of the Patients With UC-IBMFSsOf the 162 patients enrolled on the CIMFR study as ofMarch 2006, 39 (24%) were registered in the category ofUC-IBMFSs at study entry. The patients were from 30
TABLE 1 CIMFR Criteria for UC-IBMFSs
Fulfill criteria 1 and 21. Does not fulfill criteria for any categorized IBMFSa
2. Fulfills both of the followingFulfill at least 2 of the following:a. Chronic cytopenia(s) detected on at least 2 occasions over at least 3mob
b. Reduced marrow progenitors or reduced clonogenic potential ofhematopoietic progenitor cells or evidence of ineffectivehematopoiesisc
c. High fetal hemoglobin for agec
d. Red blood cell macrocytosis (not caused by hemolysis or a nutritionaldeficiency)
Fulfill at least 1 of the followinga. Family history of bone marrow failureb. Presentation at age �1 yc. Anomalies involving multiple systems to suggest an inheritedsyndrome
a TheCIMFRdiagnostic guidelines for selected syndromeswere adapted from the literature andare available at www.sickkids.ca/cimfr.b Cytopenia was defined as follows: neutropenia, neutrophil count of�1.5� 109/L; thrombo-cytopenia, platelet count of �150 � 109/L; anemia, hemoglobin concentration of �2 SDsbelow mean, adjusted for age.14c Hemoglobinopathies with ineffective erythropoiesis and high hemoglobin F should be ex-cluded by clinical or laboratory testing.
e140 TEO et al by guest on June 5, 2013pediatrics.aappublications.orgDownloaded from

families, including 5 families of affected siblings and 7families with affected members in at least 2 successivegenerations. Of the 37 patients who had UC-IBMFSs andfor whom family history was available, 23 (63%) had afirst-degree relative affected with a bone marrow failure.
There was no significant difference between the ratioof male to female patients with UC-IBMFSs (23:16) andwith C-IBMFSs (56:64) (P � .18). For 3 of the 162 caseson the registry, the gender of the patients was unknown.
All patients had their diagnosis of an IBMFS madebetween 1995 and 2006. The patients with UC-IBMFSspresented with their disease and received a diagnosis atan older age than the patients with C-IBMFSs. The me-dian age at presentation with hematologic or nonhema-tologic manifestations was 9 months (range: 0 to 10years, 11 months) compared with 1 month (range: 0–14years) in the C-IBMFS group (P � .04). The diagnosis ofbone marrow failure was made at a median age of 4.2years (range: 0.0–30.1 years), compared with 12 months(range: 0.0–16.8 years) in the C-IBMFS group (P � .01).The median age at study entry was 7.25 years (range:0.19–34.00 years), and median age at last follow-up was8.46 years (range: 0.25–35.00 years). The median fol-low-up of the patients with UC-IBMFS on the CIMFRwas 16 months (range: 0–45 months).
General Clinical Manifestations of the UC-IBMFSsManifestations related to cytopenias were the most com-mon mode of presentation (25 [64%] patients). Physicalmalformations led to a diagnosis of an IBMFS for 12patients. In 2 cases, the diagnosis was made on familyscreening.
The most common hematologic abnormality waspancytopenia (20 patients). Other hematologic abnor-malities included isolated anemia (3 patients), isolatedneutropenia (4 patients), and isolated thrombocytopenia(12 patients). At a median age of 8.4 years and a medianof 21 months after study entry, 7 patients developedsevere aplastic anemia, 2 patients progressed to myelo-dysplasia, 1 patient progressed to acute lymphoblasticleukemia, 1 patient progressed to lymphoma, 1 patientprogressed to multifocal hemangioendothelioma, and 8patients died.
Identifiable IBMFSs are mainly classified according tothe predominant cytopenia and the characteristic extra-hematologic manifestations.2 On the basis of hemato-logic manifestations and the presence or absence of as-sociated physical malformations, we divided the patientswith UC-IBMFSs into 8 groups to characterize the con-ditions. In a limited number of multiplex families and incases in which a specific diagnosis was ultimately estab-lished, this also enabled us to correlate such groupingwith the specific condition:
Group 1: Multilineage cytopenias with physical malfor-mations.
Group 2: Multilineage cytopenias without physical mal-formations.
Group 3: Isolated anemia with physical malformations.
Group 4: Isolated anemia without physical malforma-tions.
Group 5: Isolated neutropenia with physical malforma-tions.
Group 6: Isolated neutropenia without physical malfor-mations.
Group 7: Isolated thrombocytopenia with physicalmalformations.
Group 8: Isolated thrombocytopenia without physicalmalformations.
Group 1: Multilineage Cytopenias With PhysicalMalformationsIn this largest group of UC-IBMFSs, 15 patients had mul-tilineage cytopenias and physical malformations (Table 2).Two thirds were female. The patients belonged to 13 fam-ilies. Parental consanguinity was present in 3 patients, and6 patients had affected siblings. Median age at presentationwith either hematologic or nonhematologic manifestationswas 5 months (range: 0.0–to 8.5 years).
Peripheral blood cytopenia was apparent by 12months of age in 8 (53%) patients (Table 3). Similar topatients with C-IBMFS with pancytopenia, most patientshad high fetal hemoglobin levels and red blood cellmean corpuscular volume for their age (Table 3). Bonemarrow testing was done in all cases. The most commonabnormality was hypocellularity either at diagnosis (9patients) or at follow-up (1 patient). As also seen inC-IBMFSs, sometimes the bone marrow specimens werenormocellular (1 patient) or hypercellular (1 patient) oronly 1 cell line was found reduced (1 patient). Six pa-tients developed severe aplastic anemia according to pre-viously published criteria4 (Table 3). One patient devel-oped trilineage dysplasia with excess blasts and complexclonal marrow cytogenetic abnormality consistent with46, XY,�7/46, XY,�7q 1.5 years after presentation.
The patients in this group had a variety of extrahe-matologic manifestations; however, these malforma-tions appeared in multiple combinations, and no clearpatterns were identified (Table 4). Five patients died atfollow-up either as a result of their disease (1 patient) orafter bone marrow transplantation (4 patients).
Group 2: Multilineage Cytopenias Without PhysicalMalformationsFive patients had multilineage cytopenia without phys-ical malformations; all of them were boys. Two patientswere a father and a son. In another case, the mother anda sister were reported as being affected, but they werenot enrolled on the study. There were no consanguine-ous parents in this group. This suggests an autosomaldominant inheritance pattern in at least 2 of the 4 fam-ilies in this group (Table 2).
Median age at presentation was 2 months. Two pa-tients who belonged to the same family had high meancorpuscular volume and fetal hemoglobin for age (Table3). Bone marrow examination showed a hypocellularspecimen in 4 of the 5 cases. One patient had erythroidhypoplasia despite peripheral blood pancytopenia, al-
PEDIATRICS Volume 122, Number 1, July 2008 e141 by guest on June 5, 2013pediatrics.aappublications.orgDownloaded from

TABLE2
Gen
eralCh
aracteristicsof
thePatien
tsWithUC-IBMFSs
Characteristic
Group
1(P,PM)
Group
2(P,NoPM
)Group
3(A,PM)
Group
4(A,NoPM
)Group
5(N,PM)
Group
6(N,NoPM
)Group
7(T,PM)
Group
8(T,NoPM
)
No.ofpatients
155
12
23
29
Male/female
6:9
5:0
1:0
0:2
2:0
2:1
2:0
5:4
Ageatdiagnosis,m
edian(range),m
o24.0(0.0–170.0)
9.0(1.0–160.0)
49.0(49.0–49.0)
61.0(2.0–120.0)
96.0(60.0–132.0)
93.0(27.0–116.0)
40.0(10.0–70.0)
60.0(5.0–204.0)
Ageatstudyentry,m
edian(range),m
o27.0(5.0–173.0)
14.0(2.5–408.0)
49.0(49.0–49.0)
19.5(3.0–216.0)
132.0(96.0–168.0)
124.0(28.0–124.0)
69.0(14.0–124.0)
159.0(89.0–658.0)
Ageatlastfollow-up,median(range),m
o66.0(24.0–204.0)
54.0(4.0–411.0)
91.0(91.0–91.0)
111.0(6.0–216.0)
132.0(96.0–168.0)
124.0(27.0–127.0)
86.5(24.0–149.0)
190.0(105.5–708.0)
Ethnicity
White
54
11
4EasternAsian
41
1MiddleEastern
3Black
1Inuit
1Mixed
11
11
4Unknown
11
21
Consanguinity
Yes
31
No
123
12
16
Unknown
21
12
11
2Familyhistory
Affected
sibling
61
22
4Affected
parent/child
31
21
9Affected
otherrelative
52
2None
31
2Unknown
11
Group1,multilineage
cytopenias
with
physicalmalform
ations;group
2,multilineage
cytopenias
withoutp
hysicalmalform
ations;group
3,iso
latedanem
iawith
physicalmalform
ations;group
4,iso
latedanem
iawithoutp
hysicalmalform
ations;group
5,iso
lated
neutropeniawith
physicalmalform
ations;group
6,iso
latedneutropeniawithoutphysicalmalform
ations;group
7,iso
latedthrombocytopeniawith
physicalmalform
ations;group
8,iso
latedthrombocytopeniawithoutphysicalmalform
ations.A
indicatesanemia;N,
neutropenia;P,pancytopenia;PM,physicalmalform
ation;T,thrombocytopenia.
e142 TEO et al by guest on June 5, 2013pediatrics.aappublications.orgDownloaded from

TABLE3
Hem
atolog
icAbn
ormalitiesinthePatien
tsWithUC-IBMFSs
Parameter
Group
1(P,PM)
Group
2(P,NoPM
)Group
3(A,PM)
Group
4(A,
NoPM
)Group
5(N,PM)
Group
6(N,NoPM
)Group
7(T,PM)
Group
8(T,NoPM
)
No.ofpatients
155
12
23
29
Anem
iaNo.ofpatients
71
12
00
00
Ageatpresentation,median
(range),m
o0.25
(0.00–72.00)
237
(0.00–72.00)
Neutro
penia
No.ofpatients
34
00
23
00
Ageatpresentation,median
(range),m
o4.50
(0.00–9.00)
63.50(0.00–120.00)
105.50
(60.00–151.00)
116.00
(27.00–121.00)
Thrombocytopenia
No.ofpatients
5.00
30
00
02
9Ag
eatpresentation,median
(range),m
o0.00
(0.00–0.50)
030.00(0.00–0.00)
57.00(0.00–168.00)
Pancytopenia
No.ofpatients
70
00
00
00
Ageatpresentation,median
(range),m
o20.00(5.00–84.00)
Severeaplasticanem
iaNo.ofpatients
61
00
00
00
Ageatpresentation,median
(range),m
o360
HighMCV
forage
62
11
01
00
HighHbF
forage
9(3UK)
2(1UK)
10(2UK)
11
0(1UK)
1(3UK)
Bone
marrow
Hypocellularity
9,1a
41
1Hypercellularity
1Change
from
norm
o/hypercellularityto
hypocellularity
1
Isolatederythroid
hypoplasia
11
1Ery
�Meg
hypoplasia
2
Isolatedgranulocytic
hypoplasia
1(�
myeloidarrest)
Isolatedmegakaryocytic
hypoplasia
Normal
11
1b1
5ND
14
Eryindicateserythroid;HbF,hem
oglobinF;MCV;M
eg,m
egakaryocytic;N,neutro
penia;ND,notdone;UK,unknow
n.aOne
patientinthisgrouphadnorm
almarrowcytogeneticsatdiagnosisbutlaterdeveloped45(X,Y)(�
7)/46(X,Y)(-7
q).
b45(X,Y)(�
7).
PEDIATRICS Volume 122, Number 1, July 2008 e143 by guest on June 5, 2013pediatrics.aappublications.orgDownloaded from

though his father had general reduction in bone marrowcellularity. Three patients died at follow-up: 1 of non-Hodgkin’s lymphoma, 1 of sepsis, and 1 at home ofunknown cause (Table 4).
Group 3: Isolated Anemia With Physical MalformationsOne male patient in this group eventually received adiagnosis of Diamond-Blackfan anemia. The patient wasincidentally noted to have macrocytic anemia with rel-ative reticulocytopenia at 3 years of age, when he wasevaluated for growth failure and subtle nonspecificphysical malformations. The diagnosis of Diamond-Blackfan anemia could not be initially established be-cause of the late presentation, the absence of familyhistory, and lack of positive genetic testing; however, 3years after study entry, red blood cell adenosine deami-nase levels were found to be high, and a diagnosis ofDiamond-Blackfan anemia was established. Mutationanalysis of the RPS19 gene was negative (Tables 2–4).
Group 4: Isolated Anemia Without Physical MalformationsThere were 2 female patients from 2 different families inthis group. One patient presented at birth; the other hadsevere chronic anemia from early childhood.
In 1 case, the marrow erythroid precursor cells weredysplastic with vacuolated forms, and the patient had atransient prominent increase in the number of ring sid-eroblasts in the erythroid precursors in bone marrowbetween 10 years and 14 years of age. Metabolic workupand mitochondrial DNA deletion analysis was negative.It is noteworthy that the other patient in this group, whodid not have prominence of marrow ringed sideroblasts,had increased erythropoiesis on the first bone marrowtesting at the age of 2 months; however, 2 subsequentbone marrow tests revealed pure red blood cell aplasia,and a diagnosis of Diamond-Blackfan anemia was ulti-mately made. This might reflect an initial phase of ery-throid hyperplasia as a compensatory mechanism, whichis of limited capacity and duration (Tables 2–4).
Group 5: Isolated Neutropenia With Physical MalformationsThere were 2 brothers in this group. They had an addi-tional affected brother who did not have physical malfor-mations and was assigned to group 6. The patients pre-sented at age 5 years and 12.6 years, respectively, withmoderate neutropenia. Both had previously received a di-agnosis of autism, strabismus, and delayed speech devel-opment. The clinical manifestations were not typical ofsevere congenital neutropenia or Kostmann neutropeniaor the reported cases caused by WASP or GLI1 mutations(Tables 2–4).
Group 6: Isolated Neutropenia Without PhysicalMalformationsThere were 3 patients in this group. One female childhad a brother with fulminant hepatic failure and severeaplastic anemia (group 1). The parents were healthy andnonconsanguineous. This patient had mild neutropeniawith a hypocellular bone marrow at study entry anddeveloped acute lymphoblastic leukemia 28 monthslater.
One patient had a significant family history of mono-somy 7 and leukemia in successive generations withoutconsanguinity, which suggested an autosomal dominantdisease. The child was found to have neutropenia andmonosomy 7 at routine checkup at the age of 9 years, 8months. He had high mean corpuscular volume butnormal fetal hemoglobin. The later features are not con-sistent with severe congenital neutropenia, and ELA2gene sequencing was normal. The third patient hadmoderate neutropenia and has 2 brothers who haveneutropenia, autism, and speech delay and were classi-fied as having group 5 disease (Tables 2–4).
Group 7: Isolated Thrombocytopenia With PhysicalMalformationsThere were 2 male patients in this group. In both cases,bone marrow aspirates did not show reduced megakaryo-poiesis; however, antiplatelet antibodies were negative,
TABLE 4 Physical Malformations in Patients With UC-IBMFSs
Parameter Group 1(P, PM)
Group 2(P, No PM)
Group 3(A, PM)
Group 4(A, No PM)
Group 5(N, PM)
Group 6(N, No PM)
Group 7(T, PM)
Group 8(T, No PM)
No. of patients 15 5 1 2 2 3 2 9Developmental delay 9 1 2 (� autism) 1Failure to thrive 6Short stature 4 1Dysmorphic facies 3Hearing loss 3Renal failure 3Liver failure 2Congenital heart disease 3 1Cerebral calcifications 2 1Limb anomalies 1 1 1Eye anomalies 1 1 2Teeth anomalies 1Hydrocephalus 1Hemangioendothelioma 1None 5 2 3 9
No patterns consistent with a C-IBMFS were identified.
e144 TEO et al by guest on June 5, 2013pediatrics.aappublications.orgDownloaded from

and the patients responded to platelet transfusions but notto prednisone or intravenous � globulins. One patient hadmultiple physical malformations, including facial dysmor-phism, oligodontia, patent ductus arteriosus, atrial septaldefect, obstructive hydrocephalus, and developmental de-lay. The hypocellular bone marrow, reduced in vitro col-ony growth of marrow progenitors, increased marrowmegakaryocytes, normal platelet morphology, and low re-ticulated platelet count were consistent with bone marrowfailure with ineffective platelet production. Cytogeneticanalyses of the bone marrow and peripheral blood lym-phocytes as well as subtelomeric fluorescent in situ hybrid-ization analysis of chromosome 11 were normal, which didnot support a diagnosis of Paris-Trousseau/Jacobsen syn-drome.5 The second patient had severe thrombocytopeniaand intermittent severe gastrointestinal bleeding frombirth. This patient lacked a family history and the physicalstigmata of the other patient in this group but developedmultifocal hemagioendothelioma at 4 years of age (Tables2–4).
Group 8: Isolated Thrombocytopenia Without PhysicalMalformationsNine patients had isolated thrombocytopenia. All hadpositive family histories in their first-degree relatives inat least 2 successive generations, suggesting autosomaldominant inheritance. Of the families in which the in-formation about consanguinity was available, 1 pair ofparents was consanguineous. Of note was the absence ofmyelodysplastic syndrome or acute myeloblastic leuke-mia in the affected family members. As of the last CIMFRfollow-up, the patients in this subgroup were still as-signed to the UC-IBMFS group. The differential diagno-sis in these families includes MASTL-related autosomaldominant thrombocytopenia and AML1-related familialthrombocytopenia with predilection to acute myeloblas-tic leukemia (Tables 2–4).
Follow-up DiagnosesOn follow-up, specific diagnoses were assigned to 8 ofthe 39 patients with UC-IBMFSs on the CIMFR. Twosiblings from group 1 initially presented with pancyto-penia but later developed pancreatic lipomatosis bycomputed tomography of the pancreas and metaphysealdysplasia. At this stage, they were diagnosed with Sh-wachman-Diamond syndromes, although sequencing ofall 5 exons of the SBDS gene was normal. Two othersiblings from group 1 were found to have biallelic mu-tations in the SBDS gene, and combined with the hema-tologic abnormalities and short stature in 1 of them, thediagnosis of Shwachman-Diamond syndrome was made.Before the genetic testing, these siblings did not receivea diagnosis of pancreatic insufficiency by the treatingcenter because of lack of clinical findings. One patientfrom group 1 had failure to thrive, retinal dystrophy,developmental delay, thoracic kyphosis, hypotonia, andmicrocephaly and was found to have biallelic COH1 mu-tations, and a diagnosis of Cohen syndrome was made.Another patient from group 1 developed oral leukopla-kia, and a clinical diagnosis of probable dyskeratosis
congenita was made; however the patient lacked anynail or skin abnormalities and tested negative for TERC,TERT, DKC1, and NOP10. Two other patients, 1 fromgroup 3 and 1 from group 4, ultimately received a diag-nosis of Diamond-Blackfan anemia on the basis of highred blood cell adenosine deaminase levels or clinicalcourse.
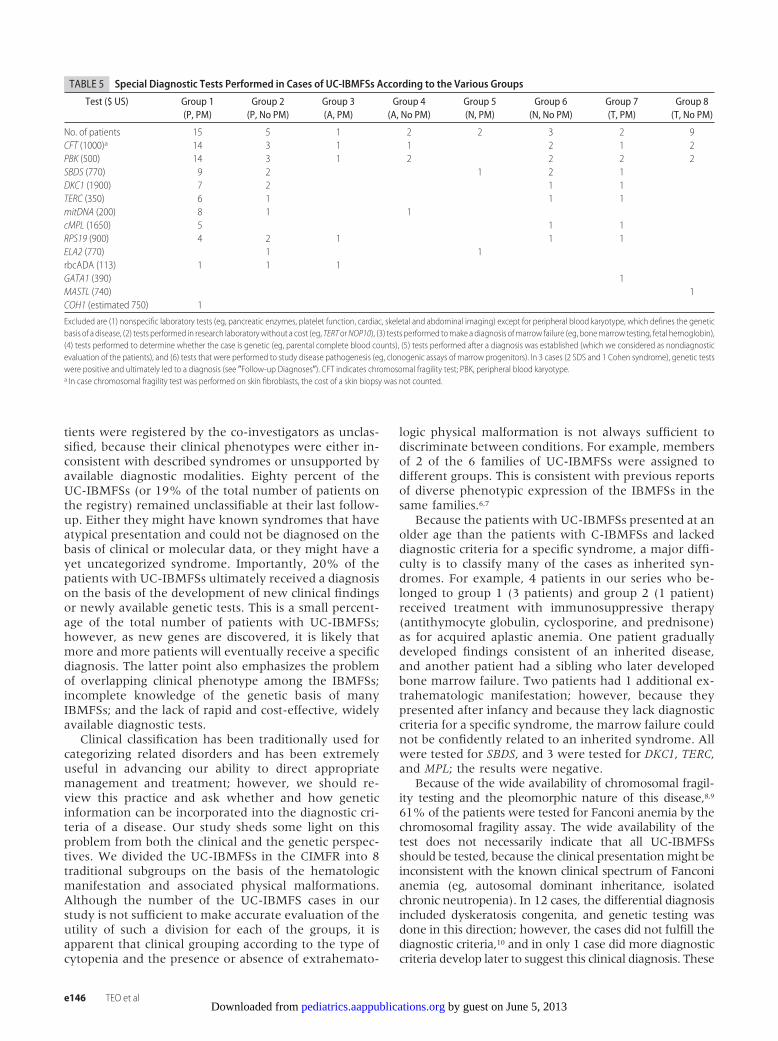
Diagnostic Tests and CostAll patients underwent extensive diagnostic testing atthe discretion of the treating physicians. To assess thecost of the diagnostic workup of a UC-IBMFS case, wecollected information from the various laboratoriesabout the cost of genetic tests and tests done in specialreferral laboratories (eg, red blood cell adenosine deami-nase), which had been done in our cohort to establish adiagnosis (Table 5). We excluded from the cost analysis(1) nonspecific laboratory tests (eg, pancreatic enzymes;platelet function or imaging of the heart, abdomen, andskeleton), (2) tests done in research laboratory without acost (eg, TERT, NOP10), (3) tests done to make a diag-nosis of marrow failure (eg, bone marrow testing, fetalhemoglobin), (4) tests done to determine whether thecase is genetic (eg, parental complete blood counts), (5)tests done after a diagnosis was established (which weconsidered as nondiagnostic evaluation of the patients),and (6) tests that were done to study disease pathogen-esis (eg, clonogenic assays of marrow progenitors).
Thirty-two (82%) of the 39 patients with UC-IBMFSsunderwent specific tests as described previously (Table5). The average number of tests per patient for theseUC-IBMFSs cases was 3.8 at a total cost of US $3160 percase. In comparison, 92 (75%) patients with C-IBMFSsunderwent testing to diagnose their IBMFS. The averagenumber of testing for these patients was 1.2 at a totalcost of US $694 per case. The actual cost is probablyhigher, because we did not include commonly doneradiologic tests, such as skeletal survey, abdominal ul-trasound, and computed tomography.
The group of patients who had the most extensivegenetic testing was group 1, namely, patients with pan-cytopenia and physical malformation. On average, thediagnostic workup included 4.3 tests per patient at a costof US $4102 (range: US $1500–$8183). The patients ingroup 1 who had an affected first-degree family memberunderwent fewer tests (mean: 3.8 vs 5.7 tests per pa-tient). When all 39 UC-IBMFS cases were analyzed, thepatients with an affected first-degree family member alsounderwent fewer tests (mean: 4.4 vs 2.1 tests per pa-tient). Among the 123 patients with C-IBMFSs on theCIMFR, a molecular diagnosis in a family member facil-itated the establishment of a molecular diagnosis in only4 cases; therefore, the higher cost of genetic testing forthe patient with UC-IBMFSs was not attributable only tofewer previous molecular diagnoses in other familymembers.
DISCUSSIONWe found a high prevalence (24%) of UC-IBMFSsamong the IBMFSs registered in the CIMFR. These pa-
PEDIATRICS Volume 122, Number 1, July 2008 e145 by guest on June 5, 2013pediatrics.aappublications.orgDownloaded from
tients were registered by the co-investigators as unclas-sified, because their clinical phenotypes were either in-consistent with described syndromes or unsupported byavailable diagnostic modalities. Eighty percent of theUC-IBMFSs (or 19% of the total number of patients onthe registry) remained unclassifiable at their last follow-up. Either they might have known syndromes that haveatypical presentation and could not be diagnosed on thebasis of clinical or molecular data, or they might have ayet uncategorized syndrome. Importantly, 20% of thepatients with UC-IBMFSs ultimately received a diagnosison the basis of the development of new clinical findingsor newly available genetic tests. This is a small percent-age of the total number of patients with UC-IBMFSs;however, as new genes are discovered, it is likely thatmore and more patients will eventually receive a specificdiagnosis. The latter point also emphasizes the problemof overlapping clinical phenotype among the IBMFSs;incomplete knowledge of the genetic basis of manyIBMFSs; and the lack of rapid and cost-effective, widelyavailable diagnostic tests.
Clinical classification has been traditionally used forcategorizing related disorders and has been extremelyuseful in advancing our ability to direct appropriatemanagement and treatment; however, we should re-view this practice and ask whether and how geneticinformation can be incorporated into the diagnostic cri-teria of a disease. Our study sheds some light on thisproblem from both the clinical and the genetic perspec-tives. We divided the UC-IBMFSs in the CIMFR into 8traditional subgroups on the basis of the hematologicmanifestation and associated physical malformations.Although the number of the UC-IBMFS cases in ourstudy is not sufficient to make accurate evaluation of theutility of such a division for each of the groups, it isapparent that clinical grouping according to the type ofcytopenia and the presence or absence of extrahemato-
logic physical malformation is not always sufficient todiscriminate between conditions. For example, membersof 2 of the 6 families of UC-IBMFSs were assigned todifferent groups. This is consistent with previous reportsof diverse phenotypic expression of the IBMFSs in thesame families.6,7
Because the patients with UC-IBMFSs presented at anolder age than the patients with C-IBMFSs and lackeddiagnostic criteria for a specific syndrome, a major diffi-culty is to classify many of the cases as inherited syn-dromes. For example, 4 patients in our series who be-longed to group 1 (3 patients) and group 2 (1 patient)received treatment with immunosuppressive therapy(antithymocyte globulin, cyclosporine, and prednisone)as for acquired aplastic anemia. One patient graduallydeveloped findings consistent of an inherited disease,and another patient had a sibling who later developedbone marrow failure. Two patients had 1 additional ex-trahematologic manifestation; however, because theypresented after infancy and because they lack diagnosticcriteria for a specific syndrome, the marrow failure couldnot be confidently related to an inherited syndrome. Allwere tested for SBDS, and 3 were tested for DKC1, TERC,and MPL; the results were negative.
Because of the wide availability of chromosomal fragil-ity testing and the pleomorphic nature of this disease,8,9
61% of the patients were tested for Fanconi anemia by thechromosomal fragility assay. The wide availability of thetest does not necessarily indicate that all UC-IBMFSsshould be tested, because the clinical presentation might beinconsistent with the known clinical spectrum of Fanconianemia (eg, autosomal dominant inheritance, isolatedchronic neutropenia). In 12 cases, the differential diagnosisincluded dyskeratosis congenita, and genetic testing wasdone in this direction; however, the cases did not fulfill thediagnostic criteria,10 and in only 1 case did more diagnosticcriteria develop later to suggest this clinical diagnosis. These
TABLE 5 Special Diagnostic Tests Performed in Cases of UC-IBMFSs According to the Various Groups
Test ($ US) Group 1(P, PM)
Group 2(P, No PM)
Group 3(A, PM)
Group 4(A, No PM)
Group 5(N, PM)
Group 6(N, No PM)
Group 7(T, PM)
Group 8(T, No PM)
No. of patients 15 5 1 2 2 3 2 9CFT (1000)a 14 3 1 1 2 1 2PBK (500) 14 3 1 2 2 2 2SBDS (770) 9 2 1 2 1DKC1 (1900) 7 2 1 1TERC (350) 6 1 1 1mitDNA (200) 8 1 1cMPL (1650) 5 1 1RPS19 (900) 4 2 1 1 1ELA2 (770) 1 1rbcADA (113) 1 1 1GATA1 (390) 1MASTL (740) 1COH1 (estimated 750) 1
Excluded are (1) nonspecific laboratory tests (eg, pancreatic enzymes, platelet function, cardiac, skeletal and abdominal imaging) except for peripheral blood karyotype, which defines the geneticbasis of a disease, (2) tests performed in research laboratorywithout a cost (eg, TERTorNOP10), (3) tests performed tomake a diagnosis ofmarrow failure (eg, bonemarrow testing, fetal hemoglobin),(4) tests performed to determine whether the case is genetic (eg, parental complete blood counts), (5) tests performed after a diagnosis was established (which we considered as nondiagnosticevaluation of the patients), and (6) tests that were performed to study disease pathogenesis (eg, clonogenic assays of marrow progenitors). In 3 cases (2 SDS and 1 Cohen syndrome), genetic testswere positive and ultimately led to a diagnosis (see �Follow-up Diagnoses�). CFT indicates chromosomal fragility test; PBK, peripheral blood karyotype.a In case chromosomal fragility test was performed on skin fibroblasts, the cost of a skin biopsy was not counted.
e146 TEO et al by guest on June 5, 2013pediatrics.aappublications.orgDownloaded from

patients might still have dyskeratosis congenita, becauseeven among those families with typical presentation ofdyskeratosis congenita, �50% can be genotyped, and be-cause most of the patients in our series who belonged tothis group were not tested for TERT or NOP10. In 14 cases,the differential diagnosis included Shwachman-Diamondsyndrome; however, the patients did not have signs ofexocrine pancreatic dysfunction, which is a major clinicalcriterion for the diagnosis of this disorder.11 Establishmentof a diagnosis of Shwachman-Diamond syndrome afterSBDS gene mutation analysis in 2 cases from group 1 and
identification of clinically affected family members by fam-ily screening by using genetic testing (unpublished data)clearly demonstrate that genotypically proven Shwach-man-Diamond syndrome has a much broader phenotypethan initially recognized clinically. Larger numbers of pa-tients, longer follow-up, and complete molecular testingare necessary to evaluate accurately the frequency ofknown and new syndromes among cases of UC-IBMFSs.
Inability to classify a disease can have a major impacton the family and the treating medical facility. First,some of the patients may receive unnecessary treatment.
TABLE 6 Proposed Laboratory and Genetic Tests for Patients With UC-IBMFS According to Type of Presentation
Type of Presentation Screening Tests Genetic Tests Second-Line Tests
Group 1: multilineage cytopenias withphysical anomalies
Chromosomal fragility testing, peripheralblood karyotype, ultrasound orcomputed tomography of theabdomen, skeletal survey, exocrinepancreatic tests, telomere length,blood gases and serum lactate, othersas clinically indicated
FANCA, FANCB, FANCC, FANCD1, FANCD2, FANCE,FANCF, FANCG, FANCI, FANCJ, FANCL, FANCM,SBDS, DKC1, TERT, TERC, NOP1, C-MPL,mitDNA, HOXA11
RPS19, RPS24, LIG4, SMARCL
Group 2: multilineage cytopeniaswithout physical anomalies
Chromosomal fragility testing, peripheralblood karyotype, ultrasound orcomputed tomography of theabdomen, skeletal survey, exocrinepancreatic tests, telomere length,blood gases and serum lactate, othersas clinically indicated
FANCA, FANCB, FANCC, FANCD1, FANCD2, FANCE,FANCF, FANCG, FANCI, FANCJ, FANCL, FANCM,SBDS, DKC1, TERT, TERC, NOP1, C-MPL,mitDNA, HOXA11
RPS19, RPS24
Group 3: isolated anemia withphysical anomalies
rbcADA, Chromosomal fragility testing,peripheral blood karyotype,ultrasound or computed tomographyof the abdomen, skeletal survey,blood gases and serum lactate, othersas clinically indicated
RPS19, RPS24, RPS35a,mitDNA, ALAS2, ABC7,CDAN1, SLC19A2
Exocrine pancreatic tests,telomere length
Group 4: isolated anemia withoutphysical anomalies
rbcADA, Chromosomal fragility testing,peripheral blood karyotype,ultrasound or computed tomographyof the abdomen, skeletal survey,blood gases and serum lactate, othersas clinically indicated
RPS19, RPS24, RPS35a,mitDNA Exocrine pancreatic tests,telomere length
Group 5: isolated neutropenia withphysical anomalies
Exocrine pancreatic tests, telomerelength, chromosomal fragility testing,Peripheral blood karyotype,ultrasound or computed tomographyof the abdomen, skeletal survey,others as clinically indicated
CXCR4, TAZ, G6PT ELA2, HAX1, SBDS
Group 6: isolated neutropenia withoutphysical anomalies
Exocrine pancreatic tests, telomerelength, chromosomal fragility testing,peripheral blood karyotype,ultrasound or computed tomographyof the abdomen, skeletal survey,others as clinically indicated
ELA2, GLI1,WASP SBDS
Group 8: isolated thrombocytopeniawith physical anomalies
Chromosomal fragility testing, peripheralblood karyotype, ultrasound orcomputed tomography of theabdomen, skeletal survey, others asclinically indicated
MYH9, HOXA11 WASP, GPIBA,MASTL, AML1,exocrine pancreatictests, telomere length
Group 9: isolated thrombocytopeniawithout physical anomalies
Chromosomal fragility testing, peripheralblood karyotype, ultrasound orcomputed tomography of theabdomen, skeletal survey, others asclinically indicated
GPIBA,MASTL, AML1,WASP, HOXA11 Exocrine pancreatic tests,telomere length
The order of the proposed tests depends of the individual case (eg, age, gender, family history, type of extrahematologic manifestations). rbcADA indicates red blood cell adenosine deaminase.
PEDIATRICS Volume 122, Number 1, July 2008 e147 by guest on June 5, 2013pediatrics.aappublications.orgDownloaded from

Second, as evident from this study, a significant numberof patients with IBMFSs undergo many diagnostic testsfor months or even years, and still approximately onefifth cannot receive an accurate diagnosis. An accuratediagnosis is sometimes critical, because treatment of thepatient is tailored according to the specific syndrome.For example, a failure to diagnose IBMFS in a patientbefore hematopoietic stem cell transplantation may befatal12 or may lead to using an affected asymptomaticsibling for transplantation. Third, it is reasonable to as-sume that having a UC-IBMFS whose natural history isunclear but carries a potential risk for life-threateningcomplications and cancer has enormous psychologicalimpact on the patient and the family. Furthermore, thepatient and the family are left with uncertainty withrespect to genetic transmission and without having toolsto offer prenatal diagnosis. Because our study showed ahigh prevalence of UC-IBMFSs, future studies shouldexamine the psychological burden of such a diagnosis onpatients and families.
Genetic tests have become increasingly available fordiagnosing IBMFSs.13 The inability to classify a patientwith a specific syndrome results in multiple testing withvery high cost, as demonstrated in this study. The resultsof our study suggest that refining the clinical classifica-tion of the syndromes may not solve the problem, andnovel diagnostic tools that will easily distinguish be-tween the various syndromes and provide rapid andaccurate diagnosis are necessary.
Because genetic tests remain costly and are notreadily available for diagnostic purposes, they are ideallyperformed in a staged manner, leaving the least likelydiagnosis to be pursued last (Table 6). Because some teststake months to complete or there is urgency in confirm-ing a diagnosis before transplantation, in many cases,multiple tests have been done simultaneously. Retro-spectively, most of these tests did not contribute to es-tablishment of a diagnosis. Because our study is based onanalysis of data from a multicenter registry, the indica-tions for and the extent of genetic testing differ betweencenters. Prospective studies with a uniform approach tothe diagnostic workup of patients may enable determi-nation of the cost-effectiveness of each of the diagnostictools.
CONCLUSIONSOur study shows for the first time that UC-IBMFSs arerelatively common among the IBMFSs and present amajor diagnostic and therapeutic dilemma. By illustrat-ing the difficulty in using phenotype to predict diagnosisand direct diagnostic testing in UC-IBMFSs, our studyraises exciting opportunities for research to identify newgenes that are mutated in bone marrow failure syn-
dromes and determine the phenotypic expression ofknown genetic causes of IBMFSs.
ACKNOWLEDGMENTS
This work was supported by grants from Fanconi AnemiaCanada, C17 Canadian Research Network, the Neutrope-nia Support Association of Canada, Amgen Inc, Canada,and Shwachman-Diamond Syndrome Canada.
We gratefully acknowledge Amanda Ciccolini andMohammad Azouz for help with collecting the data forthis article.
REFERENCES1. Dror Y. Inherited bone marrow failure syndromes. In: Arececi
RJ, Hann CEW, Smith I, eds. Pediatric Hematology. 3rd ed.Oxford, England: Blackwell Publishing; 2006:30–36
2. Alter BP. Inherited bone marrow failure syndromes. In: NathanDG, Orkin SH, Look AT, Ginsburg D, eds. Nathan and Oski’sHematology of Infancy and Childhood. 6th ed. Philadelphia, PA:WB Saunders; 2003:280–365
3. Steele JM, Sung L, Klaassen R, et al. Disease progression inrecently diagnosed patients with inherited marrow failuresyndromes: a Canadian Inherited Marrow Failure Registry(CIMFR) Report. Pediatr Blood Cancer. 2006;47(7):918–925
4. International Agranulocytosis and Aplastic Anemia Study. In-cidence of aplastic anemia: the relevance of diagnostic criteria.Blood. 1987;70(6):1718–1721
5. Grossfeld PD, Mattina T, Lai Z, et al. The 11q terminal deletiondisorder: a prospective study of 110 cases. Am J Med Genet A.2004;129(1):51–61
6. Willig TN, Draptchinskaia N, Dianzani I, et al. Mutations inribosomal protein S19 gene and Diamond Blackfan anemia:wide variations in phenotypic expression. Blood. 1999;94(12):4294–4306
7. Bellanne-Chantelot C, Clauin S, Leblanc T, et al. Mutations inthe ELA2 gene correlate with more severe expression ofneutropenia: a study of 81 patients from the French Neutro-penia Register. Blood. 2004;103(11):4119–4125
8. Kutler DI, Singh B, Satagopan J, et al. A 20-year perspective onthe International Fanconi Anemia Registry (IFAR). Blood.2003;101(4):1249–1256
9. Esmer C, Sanchez S, Ramos S, et al. DEB test for Fanconianemia detection in patients with atypical phenotypes. Am JMed Genet A. 2004;124(1):35–39
10. Dokal I. Dyskeratosis congenita in all its forms. Br J Haematol.2000;110(4):768–779
11. Dror Y, Freedman MH. Shwachman-Diamond syndrome. Br JHaematol. 2002;118(3):701–713
12. Gluckman E, Auerbach AD, Horowitz MM, et al. Bone marrowtransplantation for Fanconi anemia. Blood. 1995;86(7):2856–2862
13. Lieberman L, Dror Y. Advances in understanding the geneticbasis for bone-marrow failure. Curr Opin Pediatr. 2006;18(1):15–21
14. Dallman PR. Blood and blood forming cells. In: Rudolph A, ed.Pediatrics. New York, NY: Appleton-Century Crofts; 1977:1109–1111
e148 TEO et al by guest on June 5, 2013pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2007-3415 2008;122;e139Pediatrics
Hand, Elena Tsangaris, Isaac Odame, Joseph Beyene and Yigal DrorSharon Abish, MacGregor Steele, Kaiser Ali, Uma Athale, Lawrence Jardine, John P.Josette Champagne, Mariana Silva, Jeffrey H. Lipton, Jossee Brossard, Yvan Samson, Juliana T. Teo, Robert Klaassen, Conrad V. Fernandez, Rochelle Yanofsky, John Wu,
SyndromesClinical and Genetic Analysis of Unclassifiable Inherited Bone Marrow Failure
ServicesUpdated Information &
tmlhttp://pediatrics.aappublications.org/content/122/1/e139.full.hincluding high resolution figures, can be found at:
References
tml#ref-list-1http://pediatrics.aappublications.org/content/122/1/e139.full.hat:This article cites 11 articles, 5 of which can be accessed free
Citations
tml#related-urlshttp://pediatrics.aappublications.org/content/122/1/e139.full.hThis article has been cited by 1 HighWire-hosted articles:
Subspecialty Collections
nd_dysmorphologyhttp://pediatrics.aappublications.org/cgi/collection/genetics_aGenetics & Dysmorphologythe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2008 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on June 5, 2013pediatrics.aappublications.orgDownloaded from




















