Pulmonary Infections After Bone Marrow Transplantation: High-Resolution CT Findings in 111 Patients
8
608 AJR:185, September 2005 AJR 2005; 185:608–615 0361–803X/05/1853–608 © American Roentgen Ray Society Escuissato et al. CT of Pulmonary Infections After Bone Marrow Transplantat ion Chest Imaging • Original Research Pulmonary Infections After Bone Marrow Transplantation: High-Resolution CT Findings in 111 Patients Dante L. Escuissato 1 Emerson L. Gasparetto 1 Edson Marchiori 2 Gabriela de Melo Rocha 1 César Inoue 1 Ricardo Pasquini 3 Nestor L. Müller 4 Escuissato DL, Gasparetto EL, Marchiori E, et al. Received September 13, 2004; accepted after revision November 2, 2004. 1 Department of Diagnostic Radiology, the University of Parana, Curitiba, Brazil. 2 Department of Diagnostic Radiology, the University of Rio de Janeiro, Rio de Janeiro, Brazil. 3 Bone Marrow Transplantation Unit, the University of Parana, Curitiba, Brazil. 4 Department of Radiology, Vancouver General Hospital, 899 W 12th Ave., Vancouver, BC V5Z 1M9, Canada. Address correspondence to N. L. Müller ([email protected]). OBJECTIVE. The purpose of this study was to review the high-resolution CT findings in patients with pulmonary infection after bone marrow transplantation and to determine distin- guishing features among the various types of infection. MATERIALS AND METHODS. This study included 111 consecutive bone marrow transplant recipients who had documented pulmonary infection, high-resolution CT of the chest performed within 24 hr of the beginning of symptoms, and proven diagnosis within 1 week of the onset of symptoms. Two radiologists analyzed the CT scans and reached final de- cisions regarding the findings by consensus. Statistical analysis was performed using the Fisher’s exact test and multivariate analysis; a p value of less than 0.05 was considered statis- tically significant. RESULTS. The pulmonary infections were due to viruses (n = 57), bacteria (n = 26), fungi (n = 21), and protozoa (n = 1). Six patients had more than one organism responsible for the in- fection. Nodules that were 1 cm or more in diameter were seen in 13 (62%) of 21 patients with fungal pneumonia, five (19%) of 26 patients with bacterial pneumonia (p = 0.0059), three (10%) of 30 with respiratory syncytial virus (RSV) pneumonia (p = 0.0001), and three (14%) of 22 with cytomegalovirus pneumonia (p = 0.0016). The halo sign was present in 10 of 21 pa- tients with fungal pneumonia, two of 26 with bacterial pneumonia (p = 0.0026), three of 30 with RSV pneumonia (p = 0.0036), and one of 22 with cytomegalovirus pneumonia (p = 0.0015). There was no statistically significant difference in the prevalence of the other CT patterns including small nodules, ground-glass attenuation, and air-space consolidation among viral, bacterial, and fungal infections (all p > 0.05). CONCLUSION. The presence of large nodules and visualization of the halo sign are most suggestive of fungal infection. Other high-resolution CT patterns are not helpful in dis- tinguishing among the various types of infection seen in bone marrow transplant recipients. ulmonary infections are a com- mon cause of morbidity and mor- tality after bone marrow trans- plantation [1, 2]. These infections occur despite routine prophylaxis for com- mon pathogenic organisms and empiric ther- apy of febrile episodes during the early neu- tropenic period. Pathogens include fungi, bacteria, and viruses. Early and accurate diag- nosis of these complications is important be- cause of the high morbidity and mortality as- sociated with infection and because of the frequent complications associated with the treatment of fungal and viral infections [3–5]. Several authors have emphasized the im- portance of high-resolution CT in the diag- nosis of pulmonary infections after bone marrow transplantation [4–11]. High-reso- lution CT may show pulmonary abnormali- ties in patients with normal findings on ra- diographs and is superior to radiography in depicting the pattern and extent of abnor- malities [4–7]. Several studies have de- scribed the high-resolution CT manifesta- tions of pulmonary infections in bone marrow transplant patients [8–11]. These studies have been limited to a relatively small number of patients and have focused mainly on the description of specific infec- tions. Limited information is available about high-resolution CT features that may allow distinction among the various types of infec- tion. The aim of this study was to review the high-resolution CT findings in 111 patients who had infectious pulmonary complica- tions after bone marrow transplantation and to determine distinguishing imaging features among the various types of infection. P
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Pulmonary Infections After Bone Marrow Transplantation: High-Resolution CT Findings in 111 Patients

608 AJR:185, September 2005
AJR 2005; 185:608–615
0361–803X/05/1853–608
© American Roentgen Ray Society
Escuissato et al.CT of Pulmonary Infections After Bone Marrow Transplantation
C h e s t I m ag i n g • O r i g i n a l R e s e a rc h
Pulmonary Infections After Bone Marrow Transplantation: High-Resolution CT Findings in 111 Patients
Dante L. Escuissato1
Emerson L. Gasparetto1
Edson Marchiori2Gabriela de Melo Rocha1
César Inoue1
Ricardo Pasquini3Nestor L. Müller4
Escuissato DL, Gasparetto EL, Marchiori E, et al.
Received September 13, 2004; accepted after revision November 2, 2004.
1Department of Diagnostic Radiology, the University of Parana, Curitiba, Brazil.
2Department of Diagnostic Radiology, the University of Rio de Janeiro, Rio de Janeiro, Brazil.
3Bone Marrow Transplantation Unit, the University of Parana, Curitiba, Brazil.
4Department of Radiology, Vancouver General Hospital, 899 W 12th Ave., Vancouver, BC V5Z 1M9, Canada. Address correspondence to N. L. Müller ([email protected]).
OBJECTIVE. The purpose of this study was to review the high-resolution CT findings inpatients with pulmonary infection after bone marrow transplantation and to determine distin-guishing features among the various types of infection.
MATERIALS AND METHODS. This study included 111 consecutive bone marrowtransplant recipients who had documented pulmonary infection, high-resolution CT of thechest performed within 24 hr of the beginning of symptoms, and proven diagnosis within 1week of the onset of symptoms. Two radiologists analyzed the CT scans and reached final de-cisions regarding the findings by consensus. Statistical analysis was performed using theFisher’s exact test and multivariate analysis; a p value of less than 0.05 was considered statis-tically significant.
RESULTS. The pulmonary infections were due to viruses (n = 57), bacteria (n = 26), fungi(n = 21), and protozoa (n = 1). Six patients had more than one organism responsible for the in-fection. Nodules that were 1 cm or more in diameter were seen in 13 (62%) of 21 patients withfungal pneumonia, five (19%) of 26 patients with bacterial pneumonia (p = 0.0059), three(10%) of 30 with respiratory syncytial virus (RSV) pneumonia (p = 0.0001), and three (14%)of 22 with cytomegalovirus pneumonia (p = 0.0016). The halo sign was present in 10 of 21 pa-tients with fungal pneumonia, two of 26 with bacterial pneumonia (p = 0.0026), three of 30with RSV pneumonia (p = 0.0036), and one of 22 with cytomegalovirus pneumonia(p = 0.0015). There was no statistically significant difference in the prevalence of the other CTpatterns including small nodules, ground-glass attenuation, and air-space consolidation amongviral, bacterial, and fungal infections (all p > 0.05).
CONCLUSION. The presence of large nodules and visualization of the halo sign aremost suggestive of fungal infection. Other high-resolution CT patterns are not helpful in dis-tinguishing among the various types of infection seen in bone marrow transplant recipients.
ulmonary infections are a com-mon cause of morbidity and mor-tality after bone marrow trans-plantation [1, 2]. These infections
occur despite routine prophylaxis for com-mon pathogenic organisms and empiric ther-apy of febrile episodes during the early neu-tropenic period. Pathogens include fungi,bacteria, and viruses. Early and accurate diag-nosis of these complications is important be-cause of the high morbidity and mortality as-sociated with infection and because of thefrequent complications associated with thetreatment of fungal and viral infections [3–5].
Several authors have emphasized the im-portance of high-resolution CT in the diag-nosis of pulmonary infections after bonemarrow transplantation [4–11]. High-reso-lution CT may show pulmonary abnormali-
ties in patients with normal findings on ra-diographs and is superior to radiography indepicting the pattern and extent of abnor-malities [4–7]. Several studies have de-scribed the high-resolution CT manifesta-tions of pulmonary infections in bonemarrow transplant patients [8–11]. Thesestudies have been limited to a relativelysmall number of patients and have focusedmainly on the description of specific infec-tions. Limited information is available abouthigh-resolution CT features that may allowdistinction among the various types of infec-tion. The aim of this study was to review thehigh-resolution CT findings in 111 patientswho had infectious pulmonary complica-tions after bone marrow transplantation andto determine distinguishing imaging featuresamong the various types of infection.
P

CT of Pulmonary Infections After Bone Marrow Transplantation
AJR:185, September 2005 609
Materials and MethodsThis study was retrospective and included 111
consecutive patients who had proven pulmonaryinfection after bone marrow transplantation andwho had high-resolution CT of the chest performedwithin 24 hr of the onset of symptoms. The patientswere selected by a review of the medical recordsand came from a population of 774 patients whounderwent bone marrow transplantation at our in-stitution from January 1993 to December 2003. Ofthese 774 patients, 348 had documented pulmonarycomplications, 212 of whom underwent high-reso-lution CT. We reviewed the medical records of all212 patients and identified 111 patients who hadproven pulmonary infection and who had under-gone high-resolution CT within 24 hr of the onsetof symptoms and proven diagnosis within 1 weekof the onset of symptoms. The remaining 101 pa-tients were excluded because they had no definitediagnosis, because they had diagnosis other than in-fection, or because the high-resolution CT exami-nation was performed more than 24 hr after the on-set of symptoms. The symptoms included fever,cough, and dyspnea.
The study group was composed of 45 femalesand 66 males who ranged in age from 1 to 56 years(mean age, 23.7 years; median age, 22 years). Allbut one patient received allogeneic bone marrowtransplantation. The transplantation was performedfor the treatment of the following diseases: chronicmyelogenous leukemia (n = 42), severe aplasticanemia (n = 33), acute nonlymphocytic leukemia(n = 11), myelodysplastic syndrome (n = 8), Fan-coni’s anemia (n = 8), acute lymphocytic leukemia(n = 7), and Hodgkin’s disease (n = 2).
The infectious complications after bone marrowtransplantation were due to respiratory syncytial vi-rus (RSV) (n = 30), bacteria (n = 26), fungi(n = 21), cytomegalovirus (CMV) (n = 22), herpessimplex virus type 2 (n = 3), influenza virus(n = 1), parainfluenza virus (n = 1), and toxoplas-mosis (n = 1). Six patients had more than one or-ganism responsible for the infection, including fivecases of fungus and bacteria and one case of fungusand CMV. The bacterial pneumonias were due toStaphylococcus aureus in 12 patients, Pseudomo-nas aeruginosa in eight patients, Streptococcusviridans in four patients, Klebsiella pneumoniae inone patient, and Enterococcus faecalis in one pa-tient. Fungal infections were caused by Aspergillusspecies in 17 patients, Candida albicans in threepatients, and both Aspergillus and Candida speciesin one patient (Table 1).
The pathogens responsible for the infectious ep-isodes were documented by the following methods:bronchoalveolar lavage (n = 26), sputum culture(n = 22), sputum culture and bronchoalveolar la-vage (n = 14), biopsy (n = 8), and autopsy (n = 10).
Fungal infection was diagnosed from culture andhistologic evidence of tissue invasion (n = 15). Apositive blood culture in the presence of compatibleclinical and radiologic findings was considered di-agnostic in six cases of fungal pneumonia [11–13].Diagnosis of RSV pneumonia was based on posi-tive direct fluorescence antibody testing in speci-mens obtained at nasal washings, nasopharyngealswab, and bronchoalveolar lavage [14]. The 20 pa-tients with positive direct fluorescence antibodytesting in specimens from nasal washings had res-piratory symptoms and showed clinical and radio-logic improvement after specific treatment [15,16]. The diagnosis of CMV pneumonia was basedon detection of the characteristic inclusion bodiesin material obtained at bronchoalveolar lavage, au-topsy, or lung biopsy. Positive polymerase chainreaction test results of blood, CMV antigenemia,clinical and imaging evidence of pulmonary dis-ease, or improvement after specific treatment wasconsidered diagnostic of CMV pneumonia in fivecases [17]. Diagnosis of bacterial infection wasbased on a positive culture of sputum or broncho-scopic aspirate in most cases combined with posi-tive blood or pleural fluid cultures.
All CT examinations were performed on a So-matom ART scanner (Siemens Medical Solutions).The images were obtained at end-inspiration usinga 2-mm collimation at 10-mm intervals and werereconstructed with a high-spatial-frequency algo-rithm and photographed using window settings ap-propriate to lung parenchyma (width, 1,500 H;level, –700 H) and mediastinum (width, 400 H;level, 20 H).
Two radiologists analyzed the high-resolutionCT scans and reached final decisions regarding thefindings by consensus. The following high-resolu-tion CT findings were evaluated: pattern of thepulmonary abnormalities (nodules, tree-in-budpattern, air-space opacities, and ground-glass atten-uation), distribution of the lesions (central or pe-ripheral; unilateral or bilateral; symmetric or asym-metric; and upper, middle, or lower zones),bronchial wall thickening, mediastinal lymph nodeenlargement, and pleural effusions. The noduleswere classified as large (1 cm in diameter) or small(< 1 cm in diameter).
Ground-glass attenuation was defined as hazyincreased attenuation of the lung without obscura-tion of the bronchial and vascular margins; air-space consolidation, as homogeneous increase inpulmonary parenchymal attenuation that obscuredthe margins of vessels and airway walls; small nod-ule, as a round opacity less than 10 mm in diameter;large nodule, as round opacity equal to or greaterthan 10 mm; tree-in-bud pattern, as centrilobularbranching structures that resemble a budding tree;bronchial wall thickening, as thickness of the bron-
chial wall greater than one sixth of the bronchial di-ameter; and lymph node enlargement, as lymphnodes with short-axis diameter of greater than 10mm. The pattern of ground-glass opacities wasclassified as diffuse, patchy, or focal. The distribu-tion of air-space consolidation was classified assegmental or nonsegmental and as patchy or focal.Criteria for these findings were those defined in theFleischner Society’s glossary of terms [18].
The clinical and high-resolution CT data wereentered into a spreadsheet (Excel 2003, Microsoft).Statistical analysis was performed using theFisher’s exact test and multivariate analysis, and ap value of less than 0.05 was considered staticallysignificant.
ResultsOne hundred four patients (94%) had pa-
renchymal abnormalities visible on high-res-olution CT, and seven patients (6%) had nor-mal findings on CT. Of the patients withnormal CT findings, six had RSV infectionand one had bacterial pneumonia. These sixpatients had similar symptoms as the remain-ing patients—namely, fever, cough, and dys-pnea. Like the remaining patients, they hadhigh-resolution CT performed within 24 hr ofthe onset of symptoms. These patients had theinfection 17, 20, 31, 34, 62, and 65 days afterundergoing bone marrow transplantation.
The parenchymal abnormalities seen onhigh-resolution CT in the various pulmonaryinfections and their time of occurrence aresummarized in Table 1. Pleural effusion wasseen in two patients with fungal pneumonia,four with bacterial pneumonia, and two withviral pneumonia. None of the patients hadmediastinal lymphadenopathy.
Fungal PneumoniaSeventeen of the 21 cases of fungal pneu-
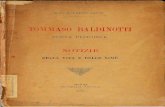
monias were caused by Aspergillus organ-isms, three by Candida albicans, and one byboth organisms. Nodules were the mostcommon finding in these patients (Table 1).Large nodules were seen in 13 patients(62%); in 10 of these 13 patients, one ormore nodules were surrounded by a halo ofground-glass attenuation (halo sign)(Fig. 1). Small nodules in a predominantlycentrilobular distribution were noted in eightcases (38%), and a tree-in-bud pattern wasseen in three patients (Fig. 2). Nodules werethe only abnormality in 11 patients. In fivecases, the nodules were associated with ar-eas of air-space consolidation; in one case,with ground-glass opacities; and in one case,with both.

Escuissato et al.
610 AJR:185, September 2005
Eleven patients had areas of air-space con-solidation, which were bilateral and asym-metric, and two patients had bilateral areas ofground-glass attenuation.
Bacterial PneumoniaTwenty-six patients had bacterial pneumo-
nia (Table 1). Twenty-one of these patients(81%) had nodular opacities, including 16 pa-tients (61%) with small centrilobular nodulesand five (19%) with large nodules (Fig. 3). Inthree patients, the small centrilobular noduleswere associated with a tree-in-bud pattern.Two patients had a halo of ground-glass at-tenuation surrounding the nodules, and onehad large nodule cavitation.
Air-space consolidation was seen in 18 pa-tients (69%) with bacterial pneumonia(Fig. 4). The areas of consolidation were fo-cal nonsegmental in eight patients, multifocalnonsegmental in five, and segmental in fivepatients. The consolidation was bilateral andasymmetric in 11 patients and involvedmainly the middle lung zones in nine patientsand the lower lung zones in eight patients.
Nine patients had areas of ground-glass at-tenuation, three of which were diffuse; three,patchy; and three, focal. The ground-glassopacities were bilateral symmetric in six pa-tients and asymmetric in three. There was nopredominant lung zone distribution.
Overall, of the patients with bacterialpneumonia four (15%) had only nodules andthree (12%) had only consolidation; the re-maining patients (73%) had various combi-nations of nodules, consolidation, andground-glass attenuation.
Viral PneumoniaRSV pneumonia—Six of the 30 patients
with RSV pneumonia had normal findings onCT scans. Nodular lesions were seen in 19 pa-tients (63%) (Fig. 5 and Table 1). Sixteencases (53%) had small centrilobular nodules,three had branching opacities (tree-in-budpattern), and three had large nodules. Three ofthe 16 patients with centrilobular nodules hada tree-in-bud pattern. In three patients, thenodules were surrounded by a halo of ground-glass attenuation.
Areas of air-space consolidation were seenin 10 patients (33%) (Fig. 5). The consolida-tion was segmental in four patients, patchynonsegmental in three patients, and focal inthree patients. The consolidation was unilat-eral in three patients, bilateral and asymmetricin distribution in five, and symmetric in two.
Seven patients (23%) had areas ofground-glass attenuation, which was diffusein four cases, focal in two, and patchy in one(Fig. 6). The ground-glass opacities were bi-lateral and symmetric in four patients andasymmetric in three.
Overall, six (20%) of the 30 patients withRSV pneumonia had normal CT scans, six(20%) had only nodules, two (6%) had onlyground-glass attenuation, and one (3%) hadonly consolidation. The remaining patients(50%) had various combinations of nodules,ground-glass attenuation, and consolidation.
TABLE 1: High-Resolution CT Findings in the Major Groups of Pulmonary Infections After Bone Marrow Transplantation
High-Resolution CT Findings Fungal Pneumonia (n = 21) Bacterial Pneumonia (n = 26)Respiratory Syncytial Virus
Pneumonia (n = 30)Cytomegalovirus
Pneumonia (n = 22)
Nodules
Small nodules 8 (3/1/4) 13 (3/3/7) 13 (8/3/2) 11 (2/7/2)
Large nodules 13 (4/2/7) 5 (1/1/3) 3 (0/0/3) 3 (0/2/1)
Tree-in-bud pattern 3 (1/1/1) 3 (1/0/2) 3 (1/2/0) 2 (1/0/1)
Ground-glass attenuation
Diffuse 1 (0/1/0) 3 (1/1/1) 4 (2/1/1) 7 (0/5/2)
Patchy 1 (0/0/1) 3 (1/0/2) 1 (1/0/0) 7 (2/4/1)
Focal — 3 (1/0/2) 2 (1/0/1) 1 (0/0/1)
Air-space consolidation
Nonsegmental focal 5 (3/1/1) 8 (1/1/6) 3 (3/0/0) 4 (1/1/2)
Nonsegmental multifocal 1 (0/1/0) 5 (2/2/1) 3 (2/1/0) 3 (1/1/1)
Segmental 5 (1/2/2) 5 (2/1/2) 4 (3/0/1) —
Other signs
Bronchial wall thickening 3 (0/1/2) 5 (1/1/3) 11 (7/2/2) 3 (0/2/1)
Halo sign 10 (3/0/7) 2 (0/0/2) 3 (2/1/0) 1 (1/0/0)
Note—The numbers in parentheses are related to the frequency of the findings in the neutropenic, early, and late phases, respectively, after bone marrow transplantation. Dash (—) indicates no cases with that finding.
Fig. 1—28-year-old woman with invasive aspergillosis 104 days after bone marrow transplantation. High-res-olution CT scan obtained at level of middle lobe shows large nodule surrounded by ground-glass attenuation (arrows) (CT halo sign).

CT of Pulmonary Infections After Bone Marrow Transplantation
AJR:185, September 2005 611
CMV pneumonia—All 22 patients withCMV pneumonia had abnormal findings onCT scans. Multiple small nodules were seenin 13 patients (59%), and large nodules weredetected in three (14%) (Fig. 7). The distribu-tion of the lesions most commonly was bilat-eral and symmetric (n = 11) and peripheral(n = 14) and had no zonal predominance.
Air-space consolidation was present inseven patients (31%), and in all cases, it in-volved mainly the peripheral lung regions of
the middle and lower zones. Ground-glassopacities were observed in 15 patients (68%),being diffuse in seven patients, patchy in sevenpatients, and focal in one patient (Fig. 8).
Overall, of the patients with CMV pneu-monia, four (18%) had only nodules, two(9%) had only consolidation, and two (9%)had only ground-glass attenuation. The re-maining patients (64%) had various combina-tions of nodules, ground-glass attenuation,and consolidation.
Other viral pneumonias—Three patientshad herpes simplex virus type 2 pneumonia.Small centrilobular nodules were seen in twopatients, and large nodules with a halo signwere found in one patient. Diffuse or patchyareas of ground-glass attenuation were notedin all patients.
Influenza pneumonia was diagnosed in onepatient. High-resolution CT showed small cen-trilobular nodules and patchy nonsegmentalconsolidation. The patient with parainfluenza Bpneumonia presented with focal nonsegmentalconsolidation and areas of mosaic perfusion.
Other Organisms and Mixed PneumoniasOne patient had Toxoplasma gondii pneu-
monia. On high-resolution CT, this patienthad diffuse ground-glass attenuation with su-perimposed smooth interlobular septal thick-ening and intralobular linear opacities result-ing in a crazy paving pattern.
Five patients had mixed pneumonia caused bybacteria plus fungi (n = 5). One of these patientshad small centrilobular nodules, one had large
nodules, two had bilateral ground-glass opacities,and two had bilateral areas of consolidation. Onepatient had mixed pneumonia caused by CMVplus fungi. The only finding in this patient wasdiffuse bronchial wall thickening.
Comparison of the CT Findings of the Various Infections
Large nodules were most common in pa-tients with fungal pneumonia, being seen in 13(62%) of the 21 patients with fungal pneumo-nia, five (19%) of 26 with bacterial pneumonia(p = 0.0059), three (10%) of 30 with RSVpneumonia (p = 0.0001), and three (14%) of22 with CMV pneumonia (p = 0.0016)(Table 2). The halo sign also was more fre-quent in patients with fungal pneumonia, beingseen in 10 (48%) of the 21 patients with fungalpneumonia, two (8%) of 26 with bacterialpneumonia (p = 0.0026), three (10%) of 30with RSV pneumonia (p = 0.0036), and one(5%) of 22 with CMV pneumonia(p = 0.0015). There was no other statisticallysignificant difference among viral, fungal, andbacterial pneumonias (Table 2). There was astatistical difference in the presence of patchyground-glass attenuation between CMV andRSV (p = 0.0072). However, there was no sta-tistical difference overall in patchy ground-glass attenuation between viral pneumoniasand fungal or bacterial pneumonias (Table 2).
DiscussionInfection is the most common cause of pul-
monary complication after bone marrow
Fig. 2—15-year-old boy with Aspergillus infection 133 days after bone marrow trans-plantation. High-resolution CT scan obtained at level of pulmonary veins shows large nodule with irregular margins in lingula and several small nodules. Some small nod-ules are centrilobular (curved arrows), and some are in a random distribution (straight arrow).
Fig. 3—25-year-old woman with Pseudomonas aeruginosa pneumonia 18 days after bone marrow transplantation. High-resolution CT scan obtained at level of main bronchi shows multiple bilateral nodules of variable sizes, some of them with sur-rounding ground-glass attenuation.
Fig. 4—22-year-old woman with Staphylococcus aureus pneumonia 46 days after bone marrow transplantation. High-resolution CT scan of right lung shows focal areas of air-space consolidation in right upper lobe.

Escuissato et al.
612 AJR:185, September 2005
transplantation. The course of immunosup-pression and recovery in these patients influ-ences the type of infection. During the periodbefore engraftment (0–30 days)—that is, be-fore successful establishment of the graft inpatients after bone marrow transplantation—profound neutropenia and damaged mucosalmembranes are the main abnormalities in hostdefense. These predispose patients to fungal,bacterial, and RSV pneumonias [19, 20]. Dur-ing the period after engraftment (31–100days), there is impairment of both cellular andhumoral immunity that predisposes the pa-tient to mainly CMV and RSV infections [19,
21]. During the late posttransplantation pe-riod (> 100 days), infection in the absence ofgraft-versus-host disease is uncommon be-cause of the relative normal immunologicfunction at this phase. However, in patientswith graft-versus-host disease, the defectsmay persist indefinitely, and patients remainsusceptible to bacterial, fungal, and viral in-fections [1, 4, 7, 19–22]. Patients with graft-versus-host disease have increased suscepti-bility to infection because graft-versus-hostdisease involves the mucosal surfaces, thereticuloendothelial system, and bone marrow,causing an immunodeficient state, and be-
cause these patients require immunosuppres-sive agents [6].
Fungal pneumonia is one of the main causesof morbidity and mortality after bone marrowtransplantation [13, 23, 24]. The most commonorganism of fungal pneumonia is Aspergillusspecies, being responsible for 90% of such in-fections [7]. Candida species, usually Candidaalbicans, is the second most frequent fungalorganism and is seen most commonly in pa-tients with leukemia and lymphoma [25].
The lung lesions in invasive pulmonary as-pergillosis are characterized by vascular inva-sion and occlusion of small- to medium-sized
Fig. 5—40-year-old man with respiratory syncytial virus pneumonia 57 days after bone marrow transplantation. High-resolution CT scan obtained at level of main bronchi shows multiple small nodules in right upper lobe (arrows) and areas of air-space consolidation associated with ground-glass attenuation in left upper lobe.
Fig. 6—20-year-old woman with respiratory syncytial virus pneumonia 33 days after bone marrow transplantation. High-resolution CT scan obtained at level of left upper lobe bronchus shows bronchial wall thickening (arrowheads).
Fig. 7—38-year-old man with cytomegalovirus pneumonia 49 days after bone mar-row transplantation. High-resolution CT scan obtained at level of pulmonary veins shows multiple small nodules (arrows).
Fig. 8—38-year-old man with cytomegalovirus pneumonia 62 days after bone marrow transplantation. High-resolution CT scan obtained at level of main bronchi shows dif-fuse ground-glass attenuation superimposed on mild centrilobular emphysema.

CT of Pulmonary Infections After Bone Marrow Transplantation
AJR:185, September 2005 613
pulmonary arteries by fungal hyphae [26].The resulting areas of hemorrhagic infarctionare seen on CT as nodules surrounded by ar-eas of ground-glass attenuation (halo sign)[11, 27, 28]. Several studies have shown thevalue of high-resolution CT in the diagnosisof invasive pulmonary aspergillosis. Com-mon findings include large nodules, fre-quently with a halo of ground-glass attenua-tion, and focal areas of consolidation [11, 27,28]. Although the halo sign in immunocom-promised patients is most suggestive of inva-sive aspergillosis, this sign has also been de-scribed in patients with Candida infection,cryptococcosis, CMV pneumonia, herpessimplex virus infection, and Kaposi’s sar-coma [12, 27, 29].
Pulmonary candidiasis may spread to thelung via a hematogenic or endobronchialroute. When from endobronchial seeding,candidiasis is limited usually to the lungs,may present with consolidation or nodules,and tends to involve mainly the lower lobes.Hematogenic dissemination results in sym-metric nodular lesions throughout the lungsand often is associated with extrapulmonarydisease. The characteristic pathologic find-ings consist of hemorrhagic nodules that usu-ally measure 2–4 mm in diameter and fre-quently have a necrotic center containing the
organisms [30]. The high-resolution CT find-ings that are suggestive of pulmonary candi-diasis include solitary or multiple nodules,ground-glass opacities, and areas of air-spaceconsolidation [7, 25, 30].
The most common finding of fungal infec-tion in the current study was large nodulesand masses, which were seen in 13 (62%) of21 patients. Small nodules were identified ineight patients. Cavitation was seen in onlyone patient. Large nodules were more com-mon in patients with fungal pneumonia thanin those with bacterial or viral pneumonia.The halo sign was also more frequent in pa-tients with fungal pneumonia than in otherpneumonias.
The most common organisms resulting inbacterial pneumonia in bone marrow trans-plant patients before marrow engraftment aregram-negative bacteria from the intestinalflora or oral mucosa and gram-positive organ-isms, particularly Staphylococcus and Strep-tococcus species. During the early phase afterbone marrow transplantation, the most fre-quent causes of bacterial pneumonia aregram-negative organisms including Pseudo-monas aeruginosa and Escherichia coli [7,10, 19]. Six months after bone marrow trans-plantation bacterial sinopulmonary infectionsare caused most frequently by gram-positive
organisms, such as Streptococcus pneumo-niae and Staphylococcus aureus. Gram-neg-ative bacteria, most commonly Haemophilusinfluenzae and Pseudomonas species, arefound in patients with obstructive airwaydisease [7].
Limited information is available concern-ing the high-resolution CT findings of bacte-rial pneumonia in bone marrow transplanta-tion patients. The chest radiography findingsin this group of patients have been describedas being similar to those seen in immunocom-petent patients, with predominance of focalareas of air-space consolidation [10, 19]. Los-sos et al. [31], in a study of 52 episodes ofbacterial pneumonia after bone marrow trans-plantation, observed 12 cases (23%) with in-volvement of only one lobe or segment. Re-ittner et al. [32] studied the high-resolutionCT findings of 114 patients with pneumonia.That study included 35 cases of bacterialpneumonia (five of them in immunocompro-mised patients), and the most common find-ings were air-space consolidation (85%),ground-glass opacities (31%), reticular opac-ities (22%), and small centrilobular nodules(17%). The frequency of air-space consolida-tion and ground-glass opacities in the currentstudy was similar, being present in 69% and35% of patients, respectively. However,
TABLE 2: p Values for the Comparison of the Frequency of the Various High-Resolution CT Findings in Pulmonary Infections After Bone Marrow Transplantation
High-Resolution CT FindingsFungal and
Bacterial Infections
Respiratory Syncytial Virus and Cytomegalovirus and
Fungal Infection Bacterial Infection Fungal Infection Bacterial Infection Respiratory
Syncytial Virus
Nodules
Small nodules 0.5567 0.7779 0.7887 0.5434 1.0000 0.7795
Large nodules 0.0059 0.0001 0.4507 0.0016 0.7102 0.6890
Tree-in-bud pattern 1.0000 0.6804 1.0000 0.6640 1.0000 1.0000
Ground-glass attenuation
Diffuse 0.6174 0.3908 1.0000 0.0459 0.1523 0.1693
Patchy 0.6174 1.0000 0.3277 0.0459 0.1523 0.0072
Focal 0.2424 0.5059 0.6546 1.0000 0.6142 1.0000
Air-space consolidation
Nonsegmental focal 0.7463 0.2489 0.0897 0.7205 0.5048 0.4385
Nonsegmental patchy 0.2044 0.6345 0.4507 0.6069 0.7102 0.6890
Segmental or lobar 0.7339 0.4601 0.7188 0.0211 0.0538 0.1282
Other signs
Bronchial wall thickening 0.7155 0.1134 0.2357 1.0000 0.7102 0.1123
Halo sign 0.0026 0.0036 1.0000 0.0015 1.0000 0.6288
Note—The values of p that are statistically significant are shown in bold.

Escuissato et al.
614 AJR:185, September 2005
small centrilobular nodules were seen morefrequently in our study, being observed in 13(50%) of 26 cases. Five patients (19%) pre-sented with large nodules. In most of the pa-tients with bacterial pneumonia (21/26, 81%),the abnormalities involved more than onelung segment; in five cases (19%), they wereobserved in only one segment or lobe.
Viral infections usually occur in seasonaloutbreaks in the community. The most com-mon organisms in bone marrow transplanta-tion patients are RSV, adenovirus, influenzavirus, and parainfluenza virus [9, 16]. Thedissemination of these infections to the lowerrespiratory tract is associated with a signifi-cant increase in mortality [15]. Ko et al. [14]reviewed the high-resolution CT of patientswith RSV pneumonia after lung transplanta-tion. The most common findings were air-space consolidation and areas of ground-glassattenuation [14]. Gasparetto et al. [33] re-viewed the high-resolution CT features of 20patients with RSV pneumonia after bone mar-row transplantation. The predominant find-ings were small centrilobular nodules andpatchy areas of consolidation and ground-glass opacities in a bilateral asymmetric dis-tribution [33]. In the current study, small cen-trilobular nodules were seen in 16 (53%) of30 patients, air-space consolidation in 10 pa-tients (33%), and ground-glass opacities inseven patients (23%).
CMV is one of the most common causes ofviral infection after bone marrow transplanta-tion [8, 21]. The infection is caused by reacti-vation of the latent virus at a time of profoundimmunosuppression or infusion of CMV-se-ropositive marrow or blood products into aCMV-seronegative recipient [1, 3]. The mostcommon high-resolution CT manifestationsof CMV pneumonia are small centrilobularnodules, air-space consolidation, and ground-glass opacities [9, 17, 34]. Similar findingswere seen in the current study, ground-glassopacities being seen in 68% of patients, smallcentrilobular nodules in 50%, and areas ofair-space consolidation in 32%. These abnor-malities usually are bilateral, diffuse, andasymmetric in distribution. Less commonfindings included large nodules and a tree-in-bud pattern.
Our study has several limitations. It is ret-rospective and includes a relatively smallnumber of patients with each type of infec-tion. The study included consecutive patientswho underwent CT within 24 hr of the onsetof symptoms and who had proven diagnosis.Although the study included nearly equal
subsets of fungal, bacterial, and CMV andRSV pneumonias, it cannot be inferred thatthese infections are equally common. We be-lieve that bacterial and fungal infections aremore common than viral pneumonias in pa-tients with bone marrow transplant. However,many of these patients are treated empiricallyon the basis of clinical and radiologic findingsand do not have a definitive diagnosis.
In conclusion, there is a considerable over-lap among the high-resolution CT manifesta-tions of viral, bacterial, and fungal pneumo-nias in bone marrow transplant patients.Large nodules and the halo sign are findingsthat are statistically more common in patientswith fungal pneumonia. Ground-glass opaci-ties, air-space consolidation, and small nod-ules are not helpful in the differential diagno-sis of various pulmonary infections after bonemarrow transplantation.
References1. Soubani AO, Miller KB, Hassoun PM. Pulmonary
complications of bone marrow transplantation.
Chest 1996; 109:1066–1077
2. Krowka MJ, Rosenow EC 3rd, Hoagland HC. Pul-
monary complications of bone marrow transplanta-
tion. Chest 1985; 87:237–246
3. Breuer R, Lossos IS, Berkman N, Or R. Pulmonary
complications of bone marrow transplantation.
Respir Med 1993; 87:571–579
4. Wah TM, Moss HA, Robertson RJ, Barnard DL.
Pulmonary complications following bone marrow
transplantation. Br J Radiol 2003; 76:373–379
5. Heussel CP, Kauczor HU, Heussel G, Fischer B,
Mildenberger P, Thelen M. Early detection of pneu-
monia in febrile neutropenic patients: use of thin-
section CT. AJR 1997; 169:1347–1353
6. Kotloff RM, Ahya VN, Crawford SW. Pulmonary
complications of solid organ and hematopoietic
stem cell transplantation. Am J Respir Crit Care
Med 2004; 170:22–48
7. Winer-Muram HT, Gurney JW, Bozeman PM,
Krance RA. Pulmonary complications after bone
marrow transplantation. Radiol Clin North Am
1996; 34:97–117
8. Worthy SA, Flint JD, Müller NL. Pulmonary com-
plications after bone marrow transplantation: high-
resolution CT and pathological findings. Radio-
Graphics 1997; 17:1359–1371
9. Choi YH, Leung NA. Radiologic findings: pulmo-
nary infections after bone marrow transplantation.
J Thorac Imaging 1999; 14:201–206
10. Gosselin MV, Adams RH. Pulmonary complica-
tions in bone marrow transplantation. J Thorac Im-
aging 2002; 17:132–144
11. Mori M, Galvin JR, Barloon TJ, Gingrich RD, Stan-
ford W. Fungal pulmonary infections after bone
marrow transplantation: evaluation with radiogra-
phy and CT. Radiology 1991; 178:721–726
12. Oh YW, Effmann EL, Godwin JD. Pulmonary in-
fections in immunocompromised hosts: the impor-
tance of correlating the conventional radiologic ap-
pearance with the clinical setting. Radiology 2000;
217:647–656
13. Somboonwit C, Greene JN. Diagnostic methodolo-
gies for invasive fungal infections in hematopoietic
stem-cell transplant recipients. Semin Respir Infect
2002; 17:151–157
14. Ko JP, Shepard JAO, Sproule MW, et al. CT man-
ifestations of respiratory syncytial virus infection in
lung transplant recipients. J Comput Assist Tomogr
2000; 24:235–241
15. McCarthy AJ, Kingman HM, Kelly C, et al. The
outcome of 26 patients with respiratory syncytial vi-
rus infection following allogeneic stem cell trans-
plantation. Bone Marrow Transplant 1999;
24:1315–1322
16. McColl MD, Corser RB, Bremner J, Chopra R. Res-
piratory syncytial virus infection in adult BMT re-
cipients: effective therapy with short duration neb-
ulised ribavirin. Bone Marrow Transplant 1998;
21:423–425
17. Kang EY, Patz Jr EF, Müller NL. Cytomegalovirus
in transplant patients: CT findings. J Comput Assist
Tomogr 1996; 20:295–299
18. Austin JHM, Müller NL, Friedman PJ, et al. Glos-
sary of terms for CT of the lung: recommendations
of the Nomenclature Committee of the Fleischner
Society. Radiology 1996; 200:327–330
19. Leung AN, Gosselin MV, Napper CH, et al. Pul-
monary infections after bone marrow transplanta-
tion: clinical and radiographic findings. Radiology
1999; 210:699–710
20. Heussel CP, Kauczor HU, Heussel GE, et al. Pneu-
monia in febrile neutropenic patients and in bone
marrow transplantation and blood stem-cell trans-
plant recipients: use of high-resolution computed
tomography. J Clin Oncol 1999; 17:796–805
21. Chan CK, Hyland RH, Hutcheon MA. Pulmonary
complications following bone marrow transplanta-
tion. Clin Chest Med 1990; 20:323–332
22. Graham NJ, Müller NL, Miller RR, Shepherd JD.
Intrathoracic complications following allogeneic
bone marrow transplantation: CT findings. Radiol-
ogy 1991; 181:153–156
23. Fraser DW, Ward JI, Ajello L, Plikaytis BD. As-
pergillosis and other systemic mycoses: the grow-
ing problem. JAMA 1979; 242:1631–1635
24. Gefter WB, Albelda SM, Talbot GH, Gerson SL,
Cassileth PA, Miller WT. Invasive pulmonary as-
pergillosis and acute leukemia: limitations in the di-
agnostic utility of the air crescent sign. Radiology
1985; 157:605–610
25. Primack SL, Müller NL. High-resolution computed

CT of Pulmonary Infections After Bone Marrow Transplantation
AJR:185, September 2005 615
tomography in acute diffuse lung disease in the im-
munocompromised patient. Radiol Clin North Am
1994; 32:731–744
26. Franquet T, Müller NL, Gimenéz A, Guembe P, de
La Torre J, Baguè S. Spectrum of pulmonary as-
pergillosis: histologic, clinical, and radiologic find-
ings. RadioGraphics 2001; 21:825–837
27. Primack SL, Hartman TE, Lee KS, Müller NL. Pul-
monary nodules and the CT halo sign. Radiology
1994; 190:513–515
28. Kuhlman JE, Fishman EK, Burch PA, Zerhouni
EA, Siegelman SS. CT of invasive pulmonary as-
pergillosis. AJR 1988; 150:1015–1020
29. Zinck SE, Leung AN, Frost M, Berry GJ, Müller
NL. Pulmonary cryptococcosis: CT and patho-
logic findings. J Comput Assist Tomogr 2002;
26:330–334
30. Dubois PJ, Myerowitz RL, Allen CM. Pathoradio-
logic correlation of pulmonary candidiasis in
immunosuppressed patients. Cancer 1977;
40:1026–1036
31. Lossos IS, Breuer R, Or R, et al. Bacterial pneumo-
nia in recipients of bone marrow transplantation.
Transplantation 1995; 60:672–678
32. Reittner P, Ward S, Heyneman L, Johkoh T, Müller
NL. Pneumonia: high-resolution CT findings in 114
patients. Eur Radiol 2003; 13:515–521
33. Gasparetto EL, Escuissato DL, Marchiori E, Ono
S, Frare e Silva RL, Müller NL. High-resolution
CT findings of respiratory syncytial virus pneu-
monia after bone marrow transplantation. AJR
2004; 182:1133–1137
34. Franquet T, Lee KS, Müller NL. Thin-section CT
findings in 32 immunocompromised patients with
cytomegalovirus pneumonia who do not have
AIDS. AJR 2003; 181:1059–1063
F O R Y O U R I N F O R M A T I O N
The full text and images from the American Journal of Roentgenology may also be viewed online at www.ajronline.org.