Tissue Damage Caused by Partial Dentures Dr Hamada mahross
27
Tissue Damage Caused by Partial Dentures Dr Hamada mahross dr hamada mahross
Transcript of Tissue Damage Caused by Partial Dentures Dr Hamada mahross
Tissue Damage Caused byPartial Dentures
Dr Hamada mahross
dr hamada mahross
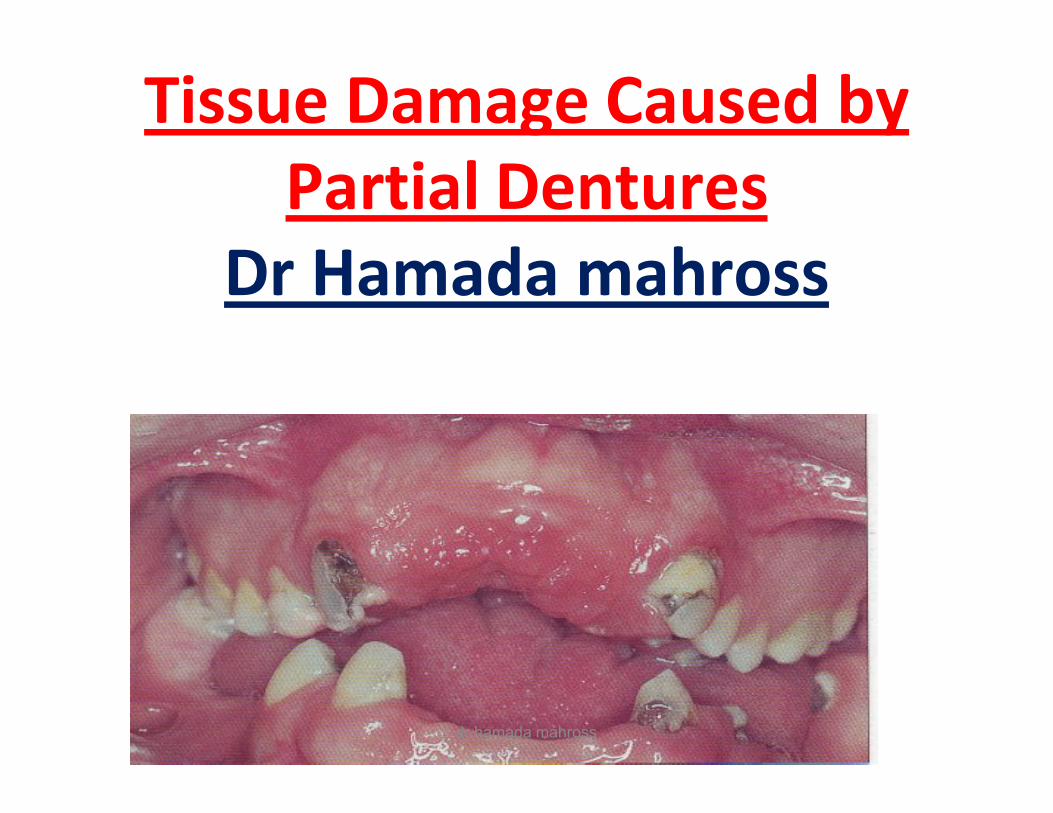
“the preservation of that which “the preservation of that which remains and not the meticulous remains and not the meticulous replacement of that which has been replacement of that which has been lost.”lost.”
-- Muller Muller DeVanDeVan ((19521952))
dr hamada mahross
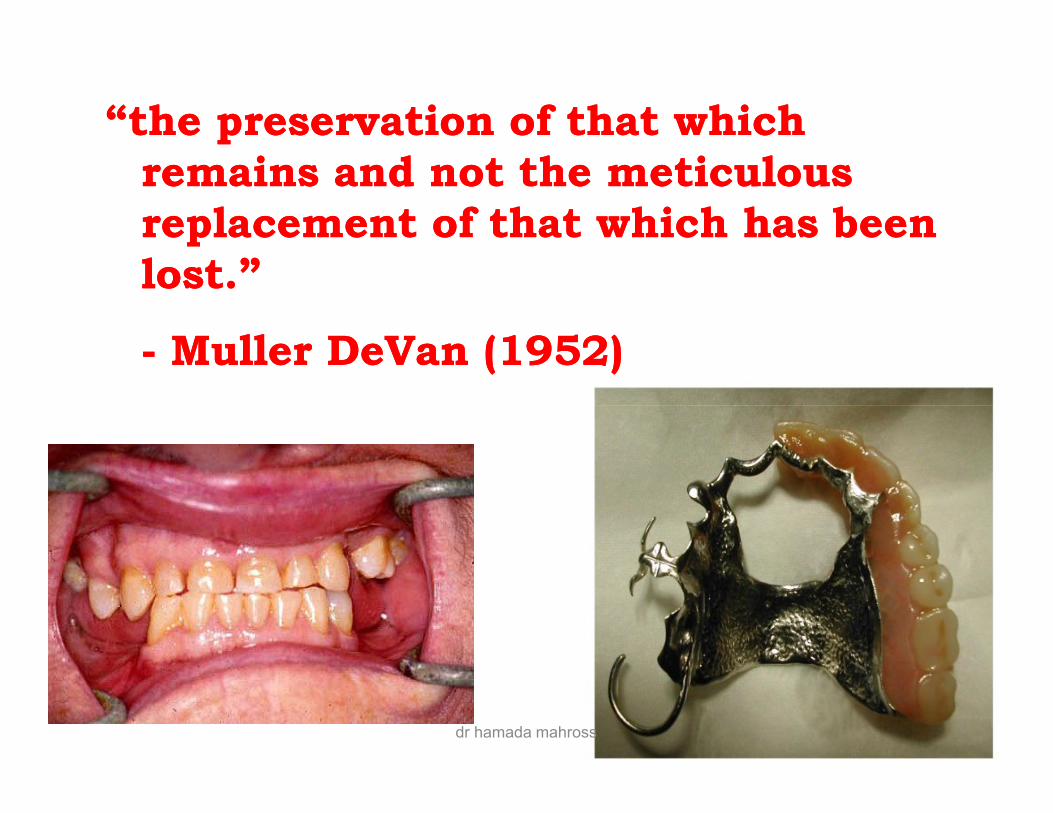
Partial dentures sometimes damage the teeth and tissues (dentoalveolar), which support them.
Harmful effects can arise from1- plaque accumulate around the RPD,2- direct trauma from RPD components, 3- excessive functional force transmitted by ill
designed prosthesisdesigned prosthesis4- errors in occlusion.
dr hamada mahross
Dentoalveolar tissue damage
I- Damage to the gingival margins and periodontium
II- Damage to the mucoperiosteum
III- Damage to the teeth
IV- Torque and tilting of abutments:
dr hamada mahross
I- Damage to the gingival marginsand periodontiumand periodontium
dr hamada mahross
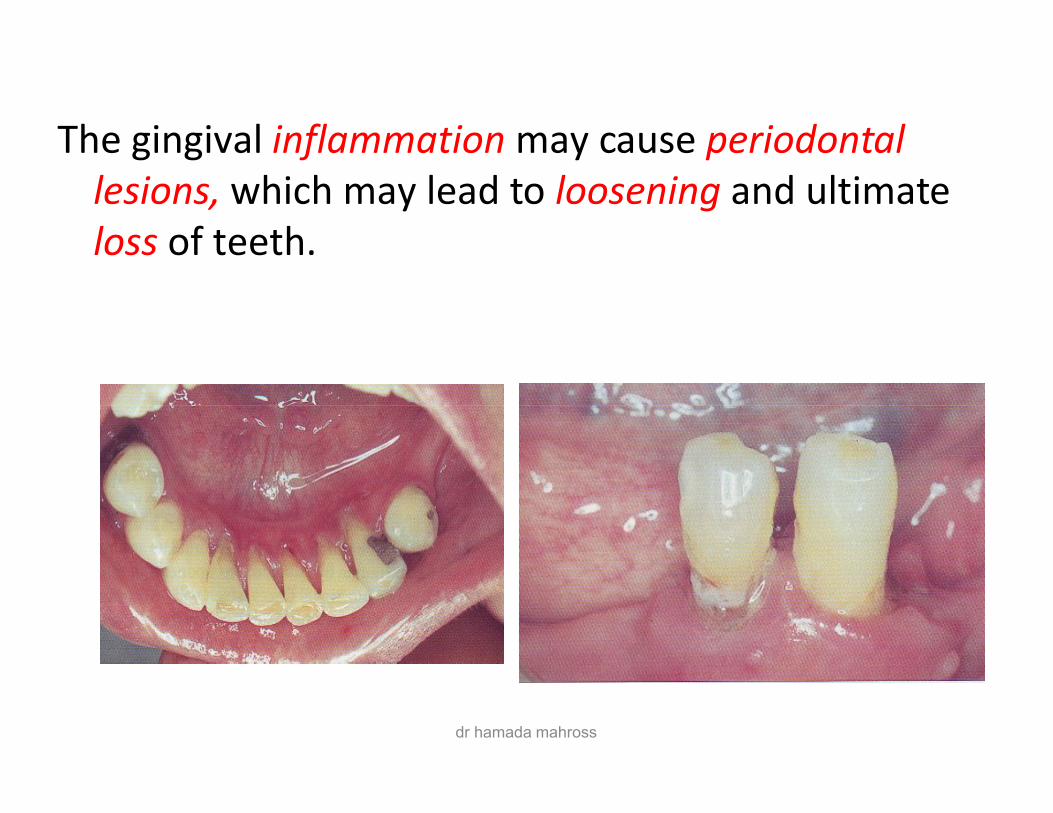
The gingival inflammation may cause periodontal lesions, which may lead to loosening and ultimate loss of teeth.
dr hamada mahross
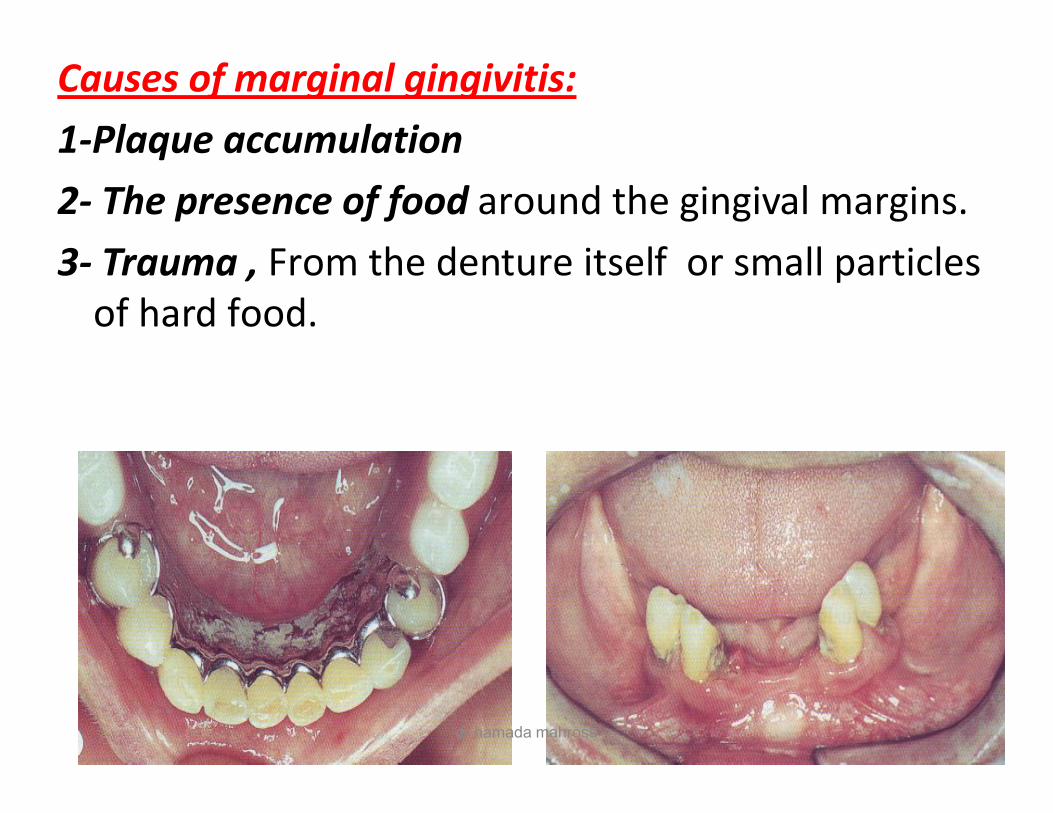
Causes of marginal gingivitis:1-Plaque accumulation2- The presence of food around the gingival margins.3- Trauma , From the denture itself or small particles
of hard food.
dr hamada mahross
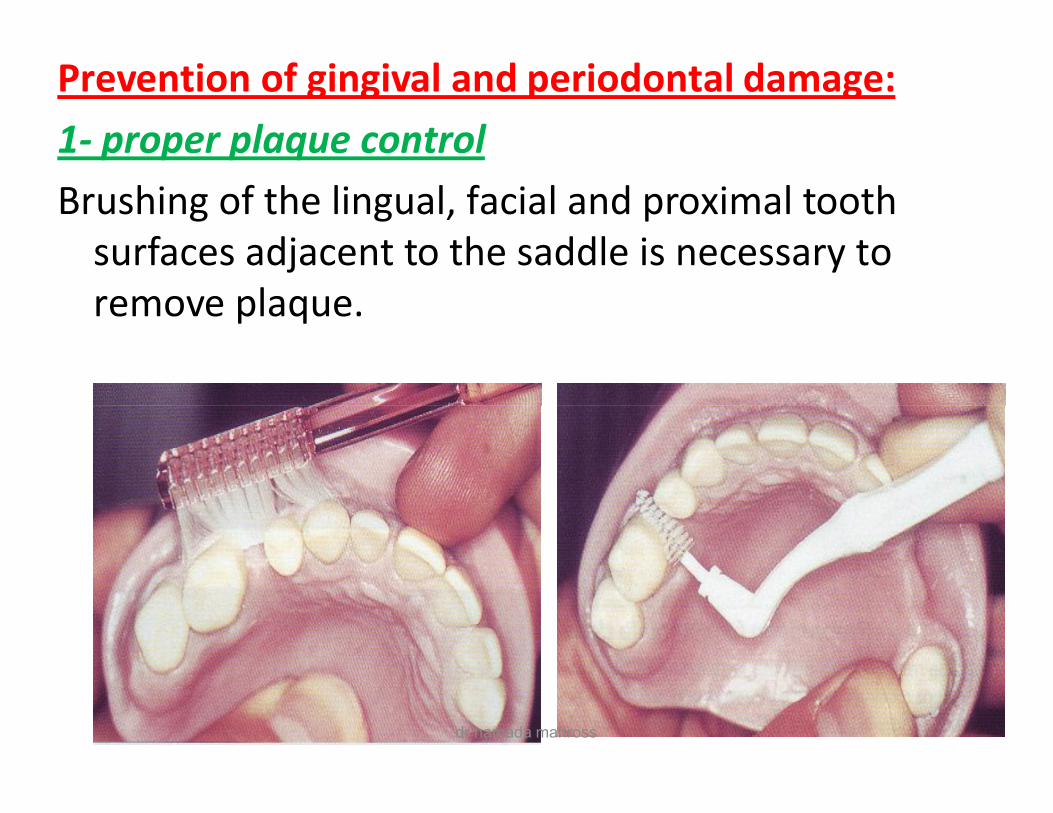
Prevention of gingival and periodontal damage:1- proper plaque controlBrushing of the lingual, facial and proximal tooth
surfaces adjacent to the saddle is necessary to remove plaque.
dr hamada mahross
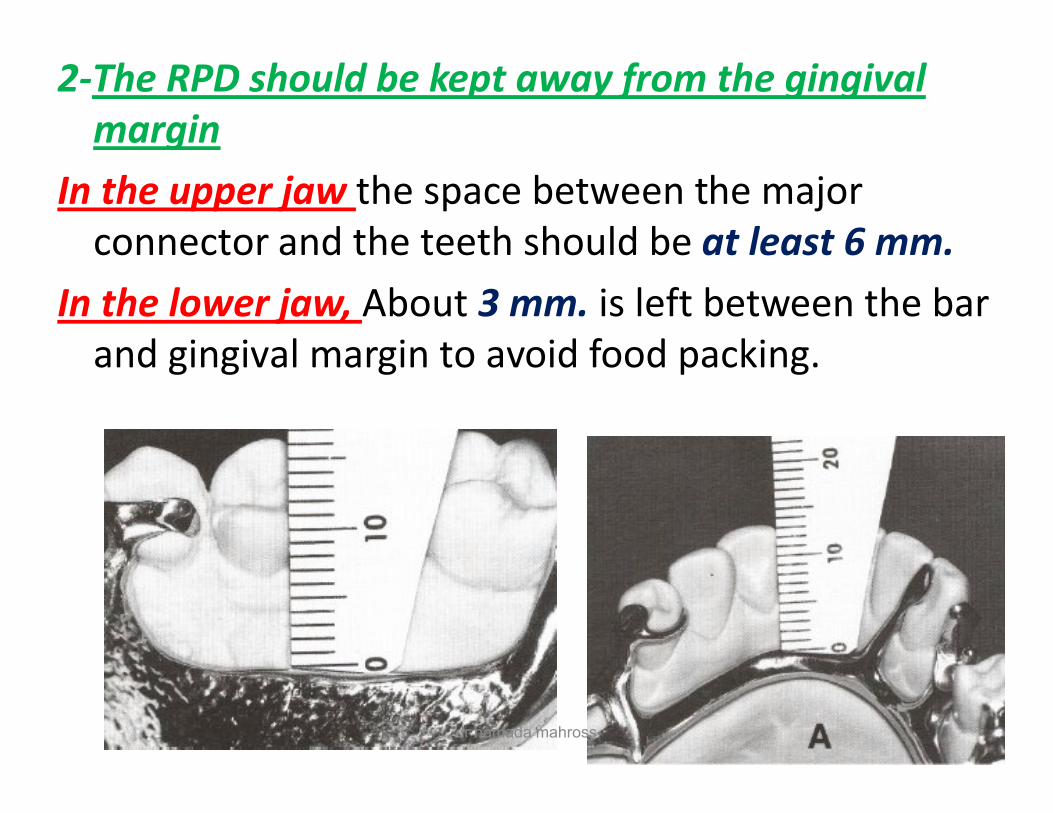
2-The RPD should be kept away from the gingival margin
In the upper jaw the space between the major connector and the teeth should be at least 6 mm.
In the lower jaw, About 3 mm. is left between the bar and gingival margin to avoid food packing.
dr hamada mahross
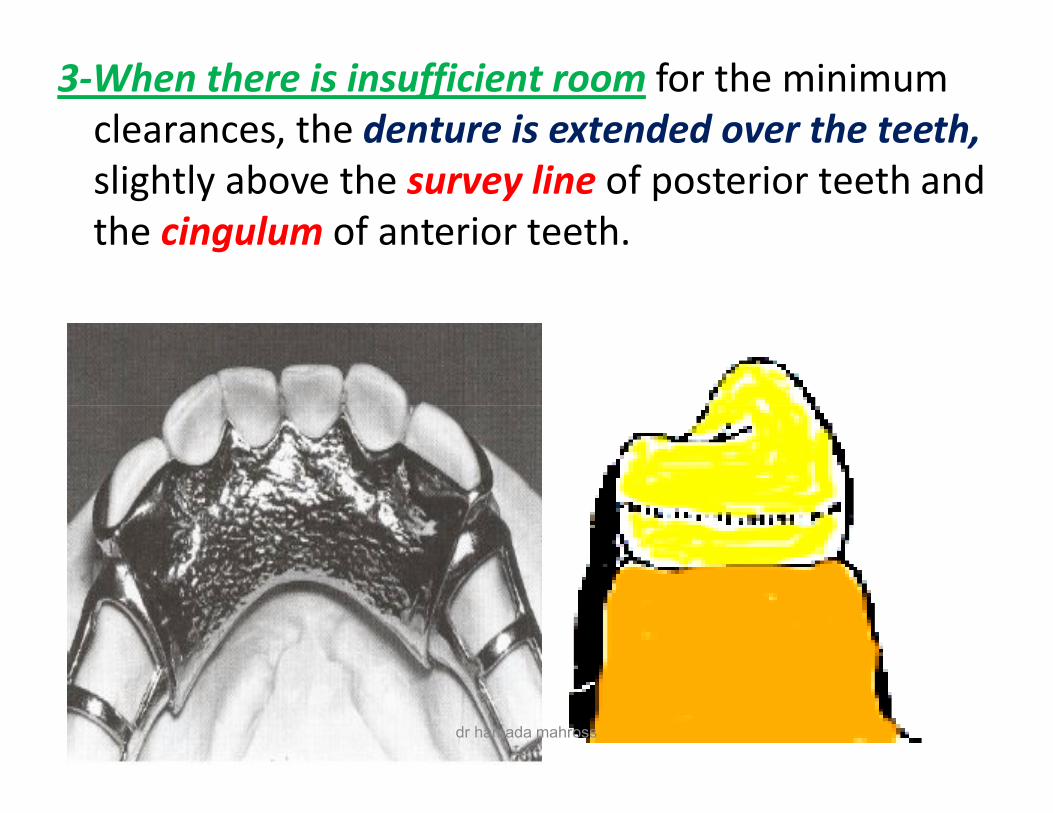
3-When there is insufficient room for the minimum clearances, the denture is extended over the teeth, slightly above the survey line of posterior teeth and the cingulum of anterior teeth.
dr hamada mahross
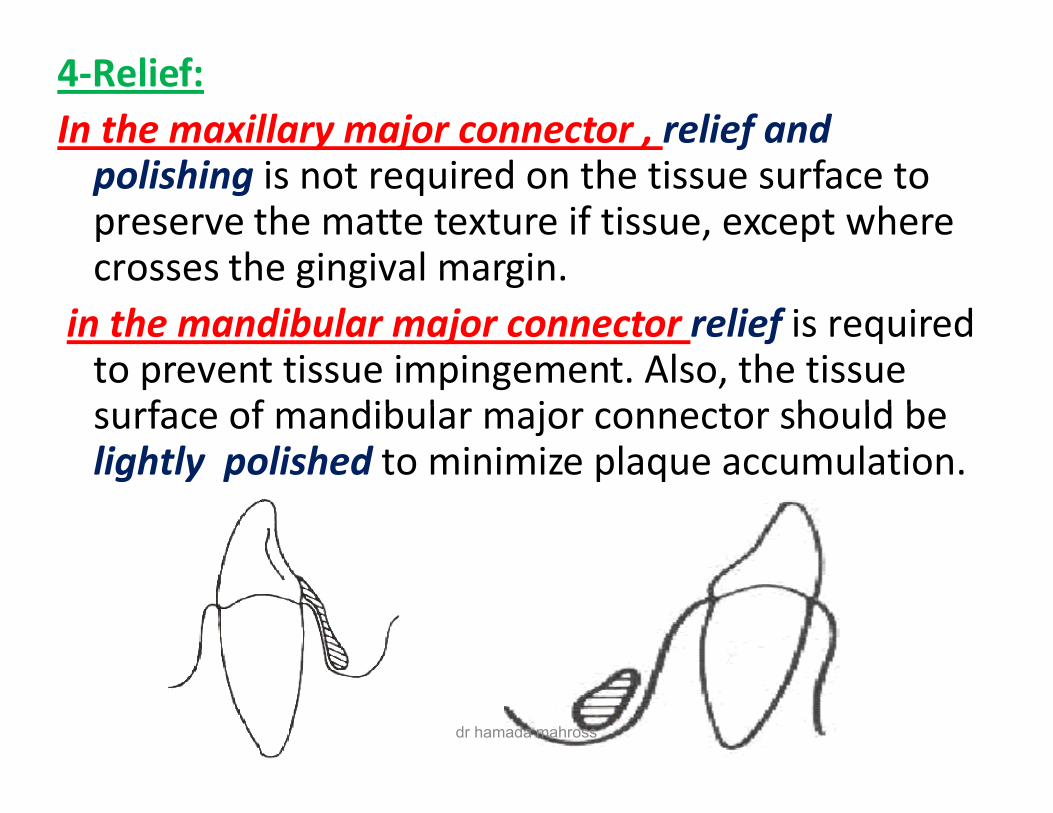
4-Relief:In the maxillary major connector , relief and
polishing is not required on the tissue surface to preserve the matte texture if tissue, except where crosses the gingival margin.
in the mandibular major connector relief is required to prevent tissue impingement. Also, the tissue surface of mandibular major connector should be surface of mandibular major connector should be lightly polished to minimize plaque accumulation.
dr hamada mahross
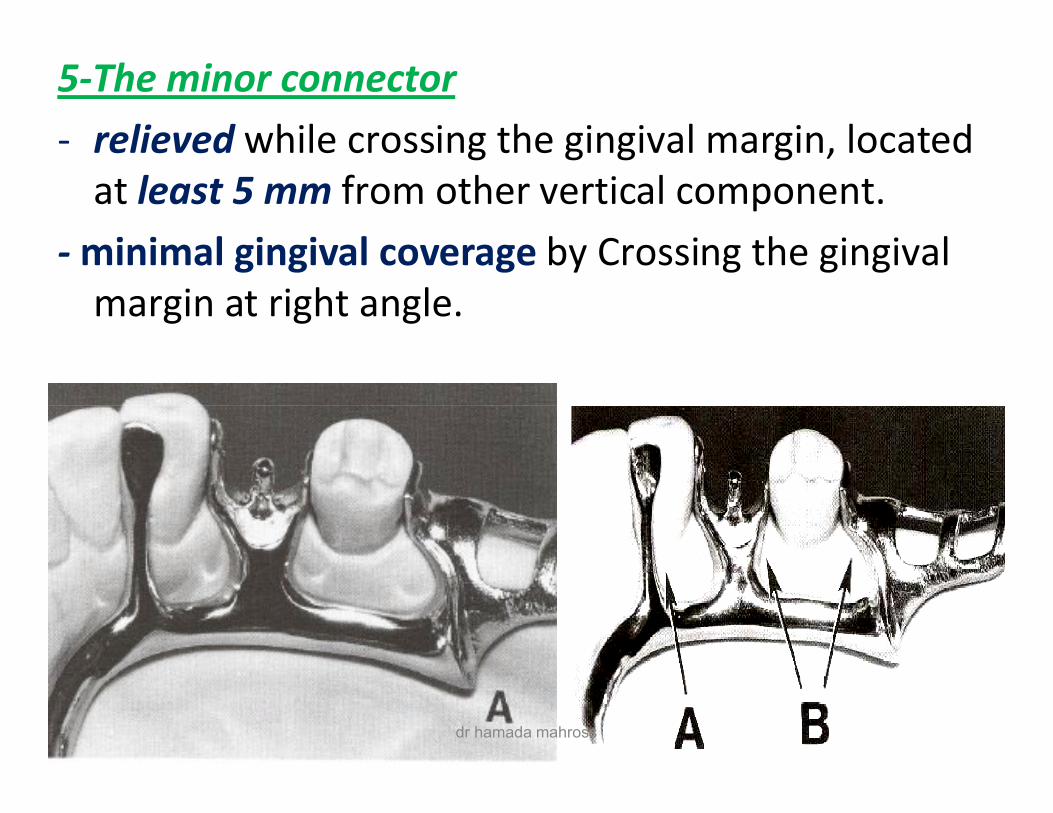
5-The minor connector- relieved while crossing the gingival margin, located
at least 5 mm from other vertical component.- minimal gingival coverage by Crossing the gingival
margin at right angle.
dr hamada mahross
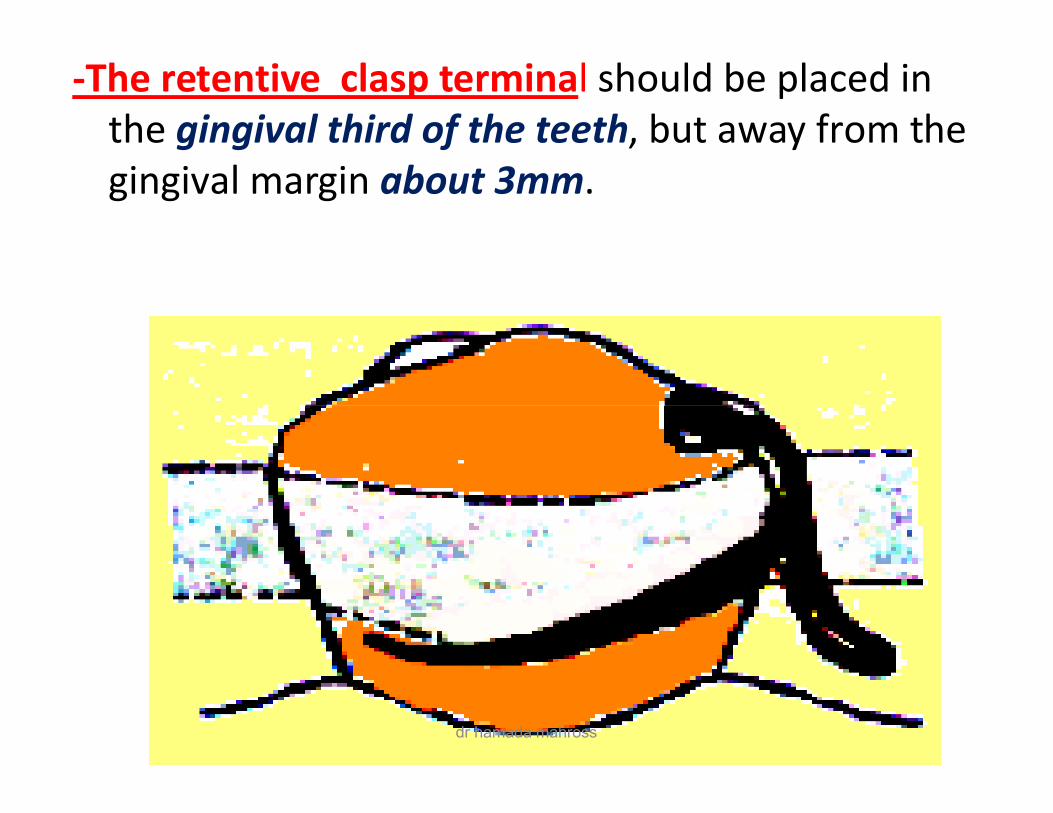
-The retentive clasp terminal should be placed in the gingival third of the teeth, but away from the gingival margin about 3mm.
dr hamada mahross
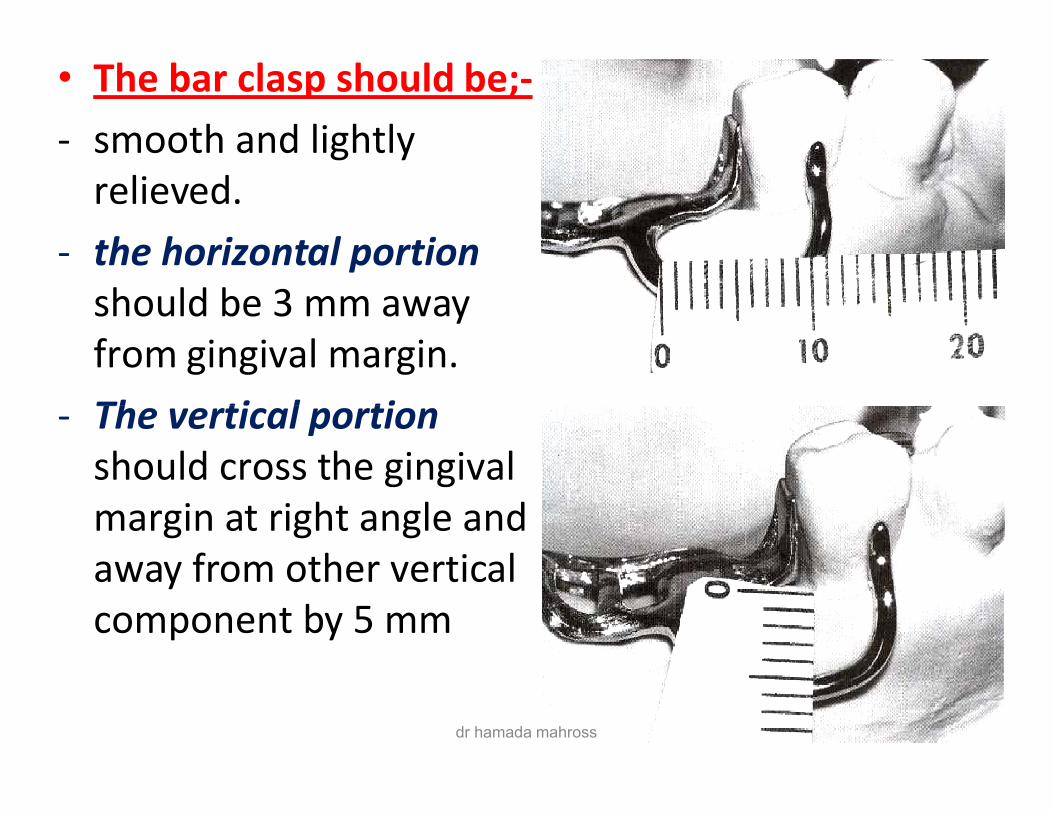
• The bar clasp should be;-- smooth and lightly
relieved. - the horizontal portion
should be 3 mm away from gingival margin.
- The vertical portion - The vertical portion should cross the gingival margin at right angle and away from other vertical component by 5 mm
dr hamada mahross
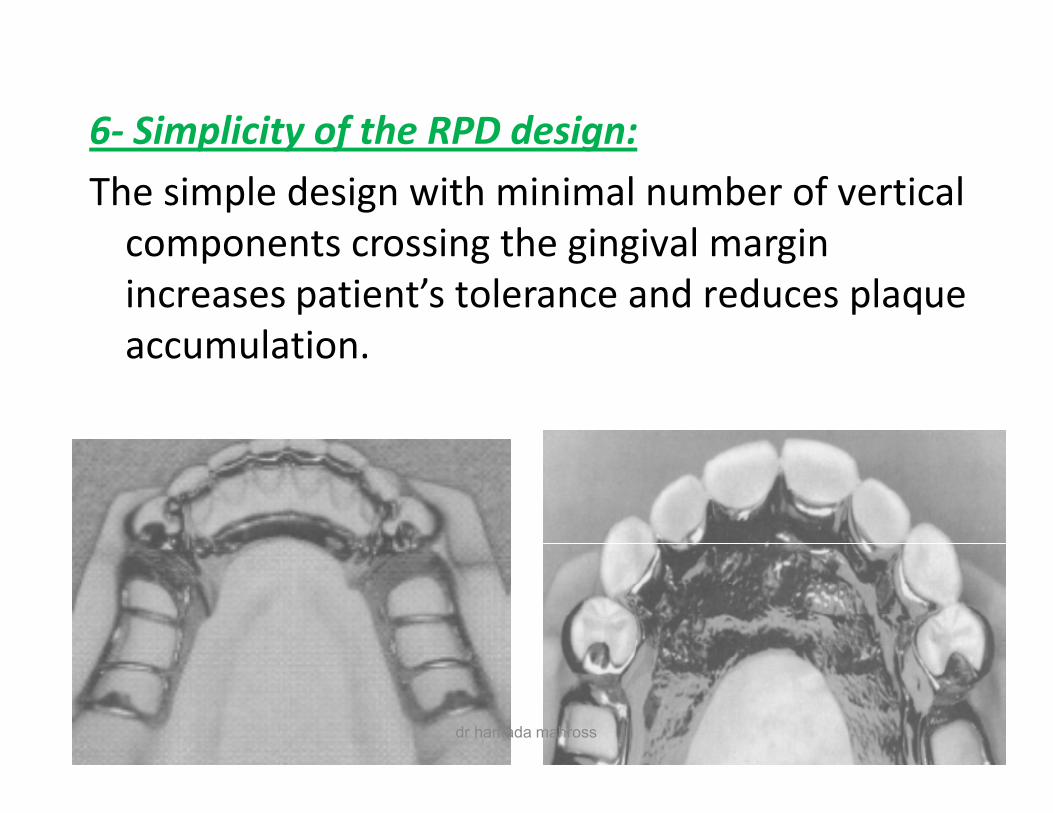
6- Simplicity of the RPD design: The simple design with minimal number of vertical
components crossing the gingival margin increases patient’s tolerance and reduces plaque accumulation.
dr hamada mahross
II- Damage to themucoperiosteummucoperiosteum
dr hamada mahross
dr hamada mahross
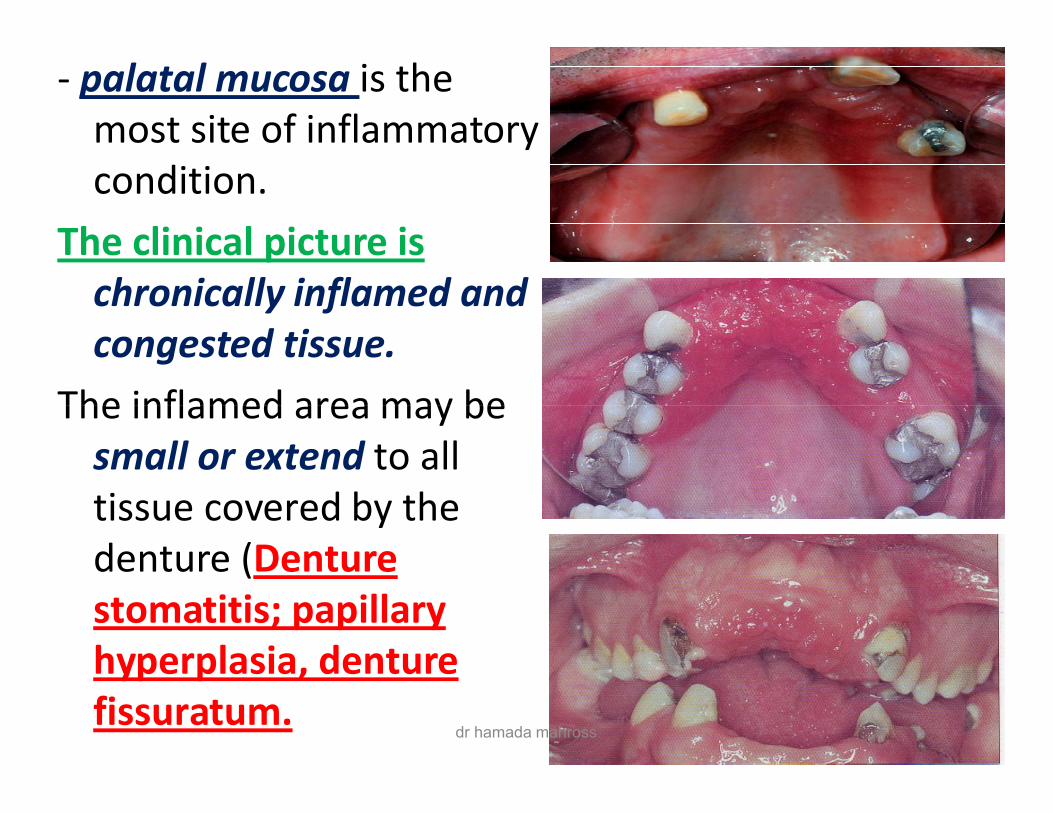
- palatal mucosa is the most site of inflammatory condition.
The clinical picture is chronically inflamed and congested tissue.
The inflamed area may be The inflamed area may be small or extend to all tissue covered by the denture (Denture stomatitis; papillary hyperplasia, denture fissuratum.
dr hamada mahross
Causes: (1) rough denture-fitting surface.(2) Excessive pressure .(3) Poor oral hygiene.(4) Infection; candidal infection play a role in denture
stomatitis. (5) patient wears the denture at night. (6) Occlusal errors causing trauma.
dr hamada mahross
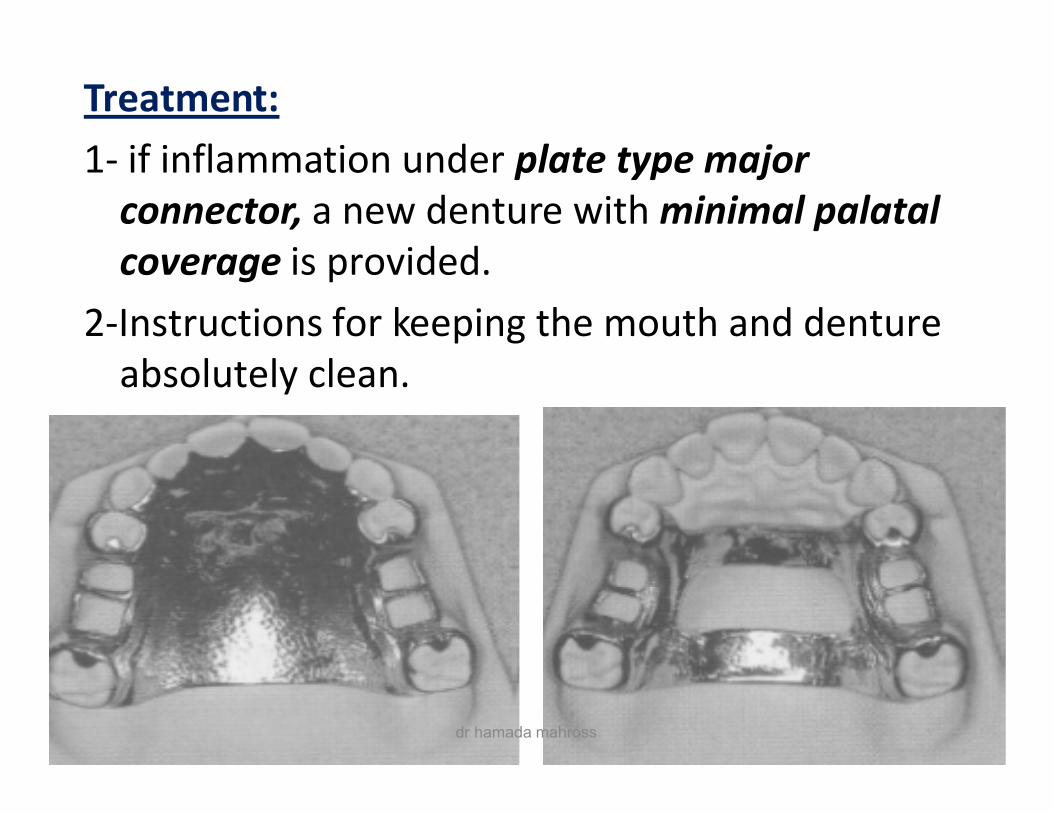
Treatment:1- if inflammation under plate type major
connector, a new denture with minimal palatal coverage is provided.
2-Instructions for keeping the mouth and denture absolutely clean.
dr hamada mahross
III- Damage to the teeth
dr hamada mahross
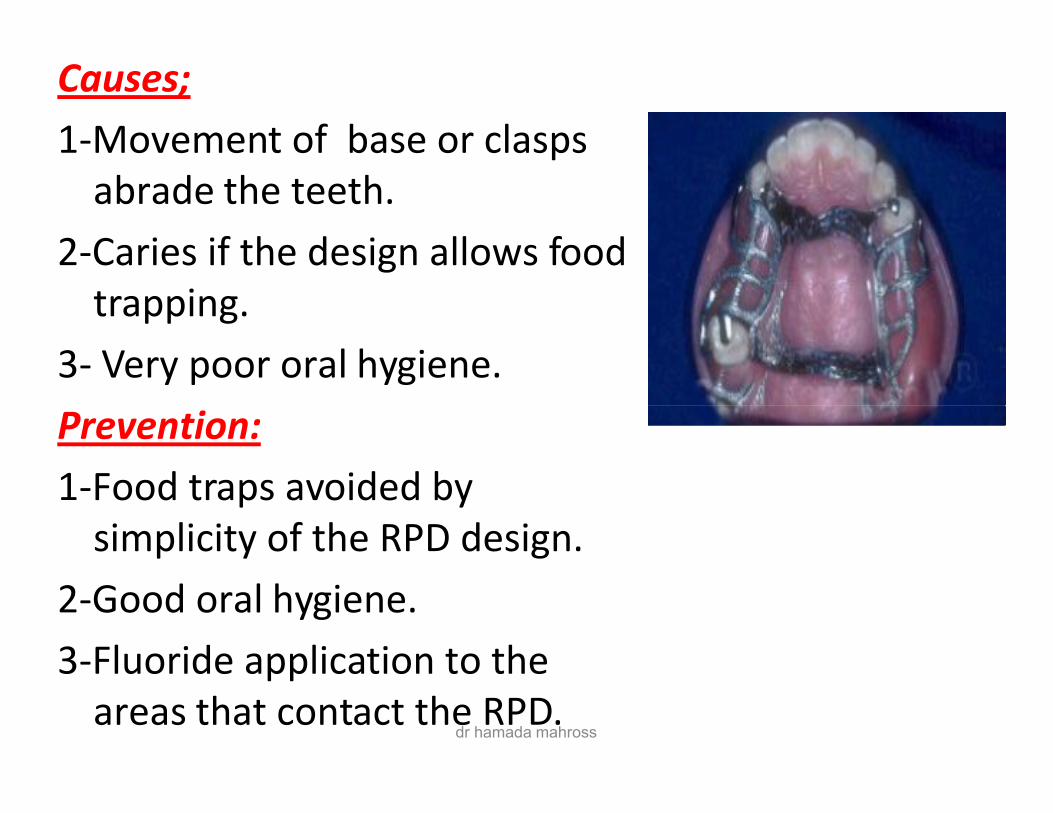
Causes;1-Movement of base or clasps
abrade the teeth.2-Caries if the design allows food
trapping. 3- Very poor oral hygiene. Prevention:Prevention:1-Food traps avoided by
simplicity of the RPD design.2-Good oral hygiene.3-Fluoride application to the
areas that contact the RPD.dr hamada mahross
IV- Torque and tilting ofabutments:abutments:
dr hamada mahross
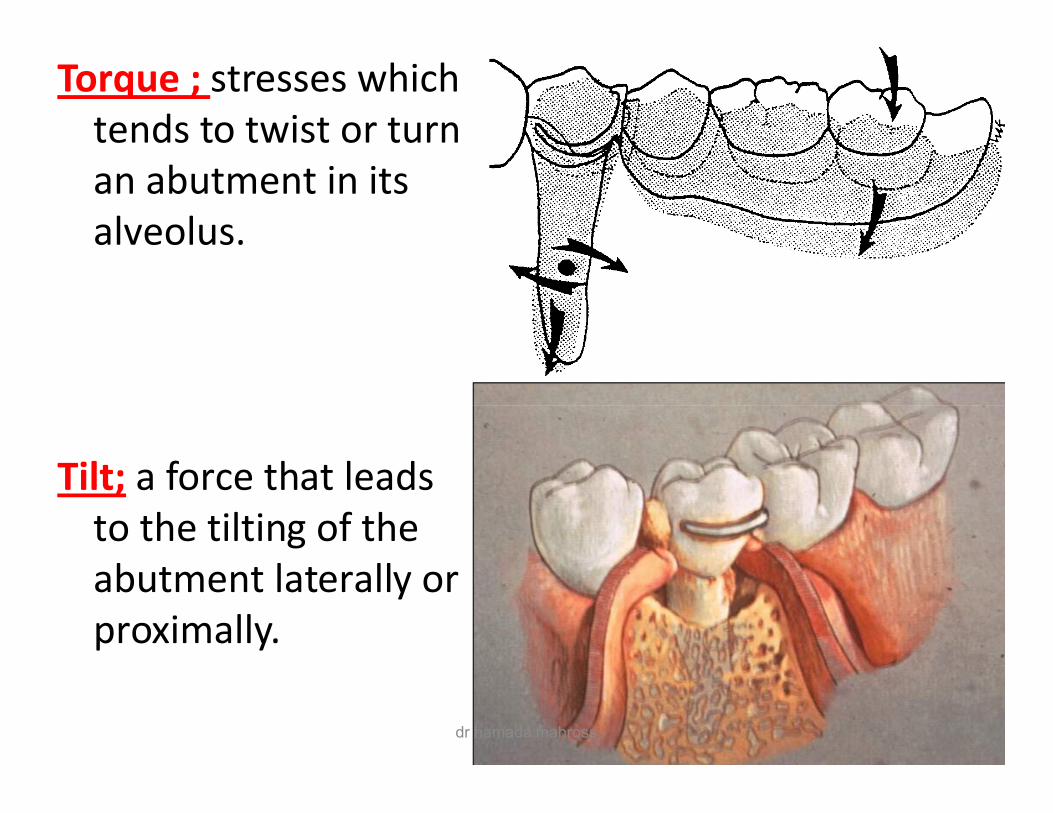
Torque ; stresses which tends to twist or turn an abutment in its alveolus.
Tilt; a force that leads to the tilting of the abutment laterally or proximally.
dr hamada mahross
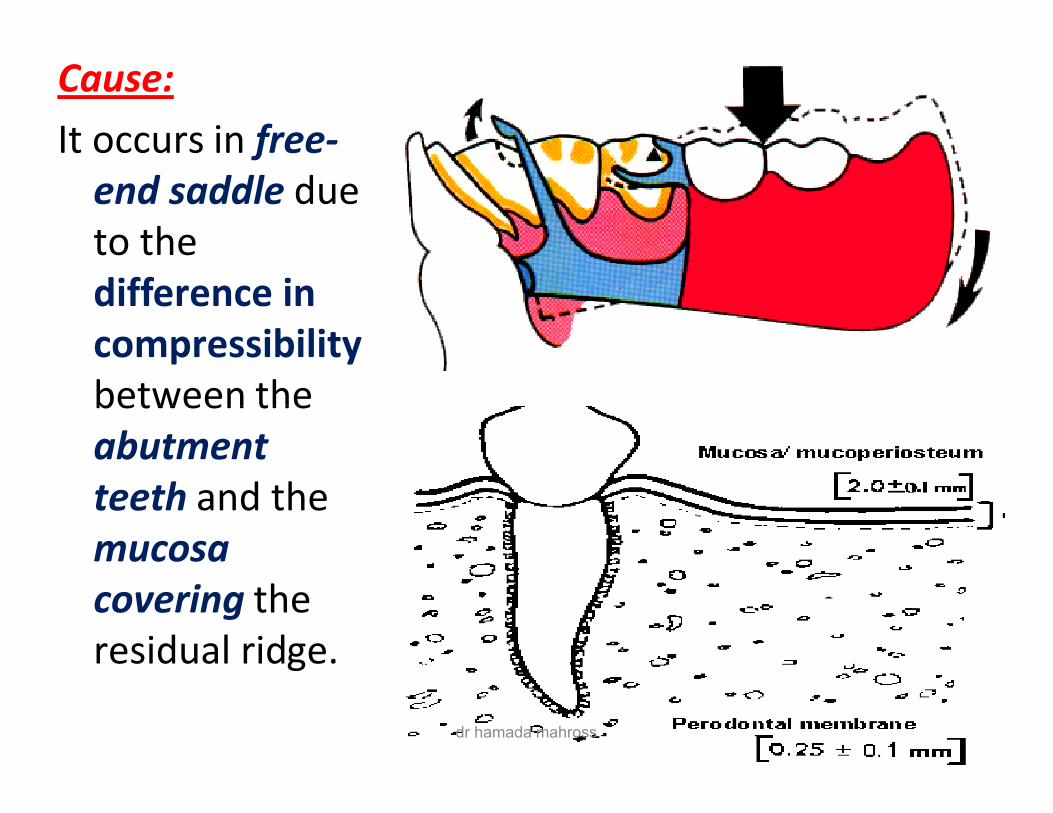
Cause:It occurs in free-
end saddle due to the difference in compressibilitybetween the between the abutment teeth and the mucosa covering the residual ridge.
dr hamada mahross
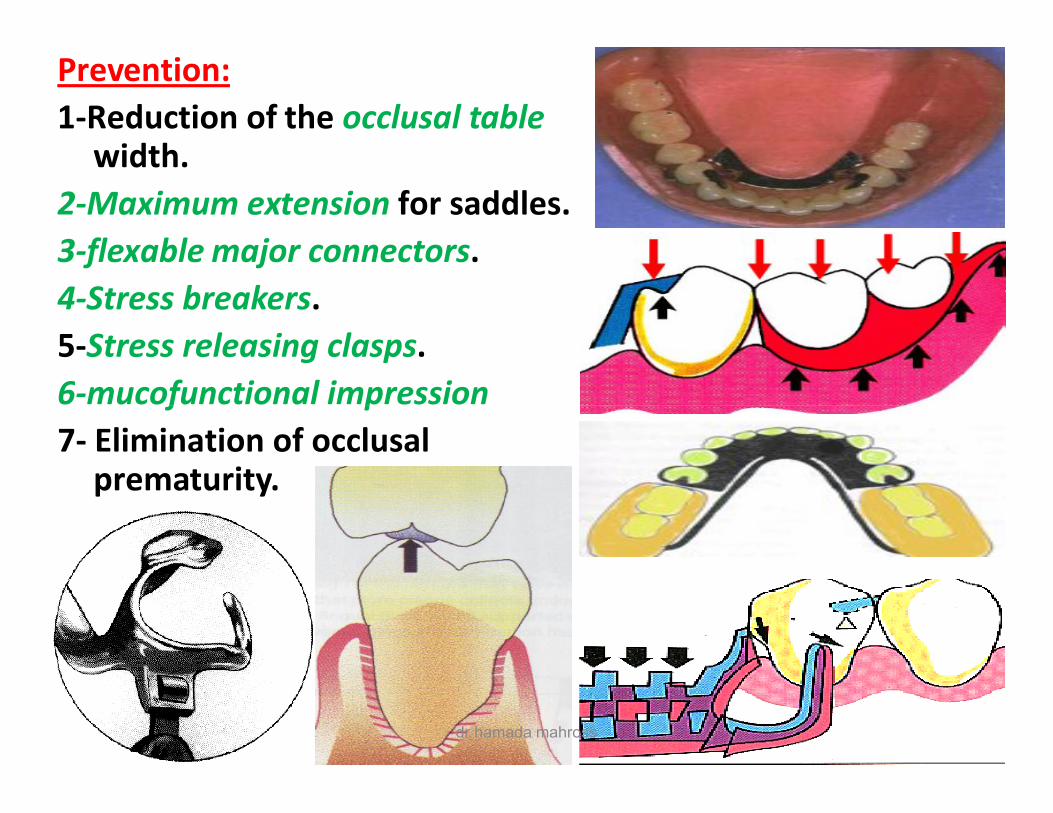
Prevention:1-Reduction of the occlusal table
width.2-Maximum extension for saddles.3-flexable major connectors.4-Stress breakers.5-Stress releasing clasps.6-mucofunctional impression6-mucofunctional impression7- Elimination of occlusal
prematurity.
dr hamada mahross
dr hamada mahross