
Regulation of NAMPT in Human Gingival Fibroblasts and Biopsies
Upload
independentCategory
view
5download
0
The Value of Needle Renal Allograft Biopsy
I. A Retrospective Study of Biopsies PerformedDuring Putative Rejection Episodes
ARTHUR J. MATAS, M.D., RICHARD SIBLEY, M.D., MICHAEL MAUER, M.D., DAVID E. R. SUTHERLAND, M.D.,RICHARD L. SIMMONS, M.D., JOHN S. NAJARIAN, M.D.
Following renal transplantation, immunosuppression is usuallyincreased to treat presumed rejection episodes. However, a)many conditions mimic rejection in the post-transplant period,and b) many rejection episodes are irreversible. As increasedimmunosuppressive therapy is associated with an increasedrisk of infection, it would be ideal to limit antirejection therapyto only the rejection episodes that are reversible. The role ofpercutaneous allograft biopsy was studied as an aid to decidewhich patients to treat for rejection, to limit unnecessary im-munosuppression and to predict allograft survival. One hundredthirty-five patients with suspected rejection underwent 206allograft biopsies without complication. Two hundred fourbiopsies were available for study. Biopsies were coded on a 1-4 scale (minimal, mild, moderate, severe) for acute and chronictubulointerstitial infiltrate and vascular rejection, as well asno rejection (e.g., recurrence of original disease). Treatmentdecisions were made on the basis of the biopsy combined withclinical data. All patients have been followed two years andoutcome correlated with biopsy findings (death, nephrectomy,and return to dialysis defined as kidney loss). The results werethe following: 1) biopsies represented changes within the kid-ney. Of 16 kidneys removed within one month of biopsy, nonephrectomy specimen showed less rejection than that seen onbiopsy. 2) Eighty-one biopsies (39.7%) led to tapering or notincreasing immunosuppression (either no rejection, minimalrejection, or irreversible changes). 3) Kidneys having eithersevere acute or chronic vascular rejection (<30% function atthree months) had significantly (p < 0.05) decreased survivalthree to 24 months postbiopsy than those with minimal or mildvascular rejection or tubulointerstitial infiltrate (83% functionat three months). 4) Kidneys with moderate chronic vascularrejection and those with severe acute tubulointerstitial infil-trate had significantly (p < 0.05) decreased survival at six to24 months. 5) Kidneys with moderate chronic vascular rejec-tion (MCV) without an acute infiltrate (ATI) had significantlybetter survival than those having both MCV and ATI. 6) Sim-ilarly, kidneys having severe ATI alone had better survivalthan those with ATI plus vascular rejection. It was concludedthat a) percutaneous allograft biopsy can be done without graftloss or infection; b) biopsy represents changes throughout the
Supported by National Institutes of Health Grant #AM 13083-09.Submitted for publication: July 7, 1982.
From the Departments of Surgery, Pediatrics, andLaboratory Medicine and Pathology, University of
Minnesota, Minneapolis, Minnesota
kidney; c) biopsy aids in deciding when to treat for rejectionand in deciding when to withhold increased immunosuppres-sion, and d) allograft biopsy predicts the outcome of treatmentof a rejection episode.
THE MOST SIGNIFICANT complication of post-trans-1 plant immunosuppression is infection; the greater
the cumulative dose of immunosuppressive drugs, thegreater the risk of infection. Approaches leading to alowering ofthe total dose ofimmunosuppressive therapyhave resulted in a substantial decrease in infection rateand increased patient survival compared with a decadeago.'`3 The transplant recipient, however, remains atsignificant risk for the development ofinfection through-out the post-transplant course.4
Following the immediate postoperative period, im-munosuppression is usually increased only to treat apresumed rejection episode. This results in increased riskfor infection, both during the time that the drug dosesare increased and afterwards as a result of a higher cu-mulative dose.56 Unfortunately, the clinical signs andsymptoms of rejection can be mimicked by many otherconditions.7 In addition, some rejection episodes cannotbe reversed with additional immunosuppressive therapy,thus increasing risk without potential benefit. An idealapproach would be to increase the dose of immunosup-pressive drugs only for those true rejection episodes thatare potentially reversible. In this retrospective study, thevalue of renal allograft biopsy was examined as a guideto management of patients presenting with elevated cre-atinine level. Biopsy and clinical data were combinedin making subsequent patient management decisions.
0003-4932/83/0200/0226 $01.40 C J. B. Lippincott Company
226

NEEDLE RENAL ALLOGRAFT BIOPSY
The following questions were asked: 1) are biopsy find-ings representative of changes throughout the kidney?2) will the biopsy predict when not to treat for rejection?3) will biopsy help in discontinuing immunosuppres-sion? 4) will biopsy predict early and late outcome oftreatment of a rejection episode? 5) does the benefit ofbiopsy outweigh the risks?
Materials and MethodsPatients who received renal transplants at the Uni-
versity of Minnesota between July 1, 1976 and June 30,1978 and who subsequently underwent percutaneousallograft biopsy were studied. The preoperative evalua-tion, operative technique, and postoperative immuno-suppression for this group have been described previ-ously.8 Briefly, during this time period, all patients atthe University ofMinnesota received azathioprine, pred-nisone, and antilymphocyte serum in the postoperativeperiod. Following discharge, patients have blood drawnfor serum creatinine determination three times per weekfor the first three months; this frequency is graduallydecreased over the post-transplant course. Patients hav-ing significant elevations in creatinine level (.25% morethan baseline post-transplant levels) and clinical signsand symptoms suggestive of rejection are admitted tothe hospital. Asymptomatic patients with elevated cre-atinine levels have the creatinine level repeated; if cre-atinine is still elevated, the patient is admitted. Diag-nosed rejection episodes are treated with increased oralprednisone and more recently by a repeated course ofantilymphocyte serum.9
After admission to the hospital, the patient is evalu-ated to determine if the elevated creatinine level is dueto rejection or to another cause. History and physicalexamination are performed as well as complete bloodcount, repeat creatinine level, blood glucose determi-nation, renal sonography, and I'3' hippuran renal scan.This battery of tests may help rule out elevated creati-nine due to infection, hyperglycemia, ureteral obstruc-tion, or lymphocele.7 Even when these diagnoses havebeen ruled out, however, the diagnosis of rejection re-mains in doubt. One hundred thirty-five patients trans-planted between July 1, 1976 and July 1, 1978 and whosubsequent to discharge were found to have an elevatedcreatinine level underwent 206 percutaneous allograftbiopsies. The biopsies were processed rapidly (vide in-fra), and the slides were ready for interpretation on thesame day. The data obtained from the biopsy were usedin concert with the clinical information in determiningpatient management.
All patients have been followed a minimum of twoyears and the clinical course correlated with the biopsyfindings. When a biopsy was given more than one in-terpretation, the course was correlated with each inter-
227pretation individually as well as with the combined in-terpretation. The abnormalities in all subsequent trans-plant nephrectomies were compared with the histologicfindings of previous biopsies. Patient death, transplantnephrectomy, and return to hemodialysis were consid-ered as graft loss.
Biopsy Procedure
Percutaneous biopsies were performed under localanesthesia using the Franklin modified Vim-Silvermanneedle. The procedure, described in detail elsewhere,'0is done at the bedside, only after coagulation parametersand platelet number are found to be adequate and severehypertension is controlled. Sterile technique is used. Thelateral border of the graft is palpated and an appropriatesite, usually adjacent to the anterior iliac spine, is se-lected. The needle is directed close to the perpendicularplane in order to avoid injury to the deeper renal struc-tures, including large vessels. If there is doubt about theposition and orientation of the kidney, a sonogram isobtained for confirmation. Specimens consisting of cor-tex and corticomedullary junction are ideal, as the his-topathology of rejection may be confined to subcorticaltissue. Local manual pressure is applied to the biopsysite for 15 to 20 minutes, and the patient is kept at bedrest for 24 hours subsequent to the procedure.
Biopsy Processing and Interpretation
Biopsy tissue for light microscopic examination wasfixed in Zenker's fluid, washed in water, dehydrated, andembedded in paraffin. Serial 1-2 micrometer thick sec-tions were stained alternately with hematoxylin andeosin and PAS-alcian blue. Biopsies were studied by lightmicroscopy on the day ofbiopsy and coded for the pres-ence or absence of rejection. The various biopsy inter-pretations are listed in Table 1. A semiquantitative his-tologic analysis ofthe degree of rejection was made usinga scale of minimal (Min) = (+ 1), mild (Mi) = (+2),moderate (Mo) = (+3), and severe (S) = (+4). The di-agnosis and grading were based on the extent and natureof the tubular, interstitial, arterial, and arteriolar in-volvement. The histopathologic criteria for each diag-nosis were as follows: acute tubulointerstitial rejection(ATI) was defined by varying degrees of mononuclearinterstitial infiltrate, interstitial edema, extravasation oferythrocytes, and tubular damage-from ectasia andsimplification to attenuation and sloughing of the epi-thelium and mononuclear infiltration of the epithelium.Rare patches of this process were graded as minimal(Fig. 1) and diffuse involvement as severe (Fig. 2). Acutevascular rejection (AV), characterized by subendothelialinfiltrates of mononuclear cells with endothelial slough-ing (endothelialitis), was graded as minimal to moderate
Vol. 197 * No. 2

228TABLE 1. Coding for Interpretation ofRenal Allograft Biopsies 4
1. Acute minimal tubulointerstitial rejection (Min ATI)4 Acute mild tubulointerstitial rejection (MoATI)3. Acute moderate tubulointerstitial rejection (MoATI)4. Acute severe tubulointerstitial rejection (SATI)5. Acute minimal vascular rejection (i V6. Acute mild vascular rejection (Mi AV)7. Acute moderate vascular rejection (Mo AV)8. Acute severe vascular rejection (S AV)9. Chronic minimal tubulointerstitial rejection (Mi CTI)a
10. Chronic mild tubulointerstitial rejection (iCI11. Chronic moderate tubulointerstitial rejection (Mo CTI)12. Chronic severe tubulointerstitial rejection . TIp13. Chronic minimal vascular rejection (Min CV)14. Chronic mild vascular rejection wal CVa15. Chronic moderate vascular rejection (MO CV) (no16. Chronic severe vascular rejection (S CV)17. Acute tubular necrosis of m18. Pyelonephritis19. Recurrent disease20. Viral associated nephropathy ec nt21. Normal22. Infarction23. Antilymphocyte globulin reaction ist
(Fig. 3). Minimal changes were those in which a fewcells were found in one or two vessels, while moderateacute vascular rejection was diagnosed when five or
FIG-. Mid acte tbulontertitil reectin. Fcal olletion FIG. 2. Severe c tubulointerstitial rejection. n parenchymamononuclear4ells withassociatededemaandminorte is diffusely infiltrated by mononuclear cells. The tubules are dilated,
and there is interstitial edema. The arterioles show minimal endothe-
lialitis (PAS-alcian blue X 160).
more vessels showed a prominent endothelialitis; mildfell in between. A necrotizing inflammatory process of
* the media, fibrinoid necrosis ofthe wall or fibrin-plateletthrombosis were graded as severe acute vascular rejec-tion (Fig.4).-
I ,y ~~~~~~~~~~~~Fibrointimal thickening of arteries and arterioles (not, elastica reduplication) of progressing severity was coded
as minimal (Fig. 5) to severe chronic vascular rejection~~~~~ ~(CV); the latter consisted of marked onion skinning as
demonstrated on the PAS-alcian blue stained sections(Fig. 6). These changes were encountered in interlobularor larger arteries, rarely in arterioles.
Chronic tubulointerstitial rejection (CTI) refers to tu-bular atrophy and interstitial fibrosis. Round cell infil-trates found in areas of tubular atrophy and interstitialfibrosis were not coded as acute tubular interstitial re-jection, but were considered a component of a chronicprocess. These lesions are usually found when modest
FIG. 1. Mild acute tubulointerstitial rejection. Focal collections of to severe chronic vascular changes and chronic trans-mononuclear cells with associated edema and minor tubular damage plant glomerulopathy are present, but may result fromare seen (hematoxylin = eosin, X240). previous episodes of ATI.
MATAS AND OTHERS Ann. Surg. * February 1983

NEEDLE RENAL ALI
FIG. 3. Mild acute vascular rejection. Low-grade acute vascular rejec-tion consists ofmononuclear cells beneath the endothelium. One othervessel in this biopsy was similarly involved. There is also interstitialrejection (hematoxylin-eosin, X160).
Acute tubular necrosis (ATN) was diagnosed whenvarying degrees of tubular damage were encountered-ectasia, epithelial attenuation or sloughing, and mi-toses-without an associated interstitial mononuclearinfiltrate (Fig. 7). Acute pyelonephritis was characterizedby interstitial and tubular collections of polymorpho-nuclear leukocytes often with microabscess formation.
In order to diagnose recurrent disease in the allograft,light microscopic, immunofluorescent, and electronmicroscopic findings compatible with the original dis-ease in addition to appropriate clinical and laboratoryparameters were necessary. A membranoproliferativeglomerulonephritis-like lesion is often encountered inchronic rejection which is separated from recurrent dis-ease on the basis of histopathologic and clinical corre-lation.
Changes suggesting systemic viral infection usuallydue to cytomegalovirus occur infrequently in allograftbiopsies." When present, they are recognized by diffusetubular ectasia, sometimes with epithelial sloughing, as-sociated with discrete patches of plasma cells and plas-
LOGRAFT BIOPSY 229
macytoid lymphocytes (Fig. 8) or by obstruction of glo-merular capillaries by a poorly defined PAS positive fi-brillar material, as recently reported'2 (Fig. 9).
Acute vascular rejection, anastomotic site occlusionor emboli (usually atheromatous) may result in corticalinfarction. Biopsies often cannot delineate the etiologyof the infarcted kidney.
Antilymphocyte globulin (ALG) reaction, using Min-nesota ALG,'3 is characterized by fibrin-platelet throm-bosis of glomerular capillaries without arteriolar or ar-terial lesions or ATI (Fig. 10). These lesions appear dur-ing the course of ALG administration, and clinicallythere is thrombocytopenia, microangiopathic hemolyticanemia (red blood cell fragmentation) and renal insuf-ficiency, correctable by cessation ofALG. These changescan be confused with hyperacute or severe acceleratedacute rejection, but graft morphology, onset after ALGand absence of circulating cytotoxic antibodies againstdonor lymphocytes, aid in the differential diagnosis.
Mild arteriosclerosis, focal tubular atrophy, or globalglomerular sclerosis were sometimes encountered in oth-erwise normal biopsies.
FIG. 4. Severe acute vascular rejection. Fibrinoid necrosis, necrotizingvasculitis, and thrombosis characterize severe acute vascular rejection.This vessel shows segmental fibrinoid necrosis of the wall (hematox-ylin-eosin, X256).
Vol. 197 - No. 2

230 MATAS AND OTHERS Ann. urg. * February 1983
verse the acute changes. When there was no improve-:W~2..MSh.r6 t tj ment in renal function, immunosuppression was ta-
i.4 .pered, and the allograft was subsequently removed.;^0 When allograft pathology was com with findingson biopsy, it was found that biopsy changes accuratelyrepresented the severity of rejection within the allograft.In no instance did biopsy overestimate the amount of
pdamage to the kidney.
Correlation of Biopsy Findings with Outcome
The functional survival after biopsy of 169 kidneyshaving rejection is shown in Table 2 and Figure 2. Al-though each biopsy may have a combination of diag-noses (e.g., severe ATI, mild AV), each diagnosis is con-
4: iE ^ I?e§> H f ~sidered separately in these data. Combined interpreta-*X 'ia m'tions will be presented later. Using individual diagnoses,
the best long-term graft survival is seen in patients withminimal or mild ATI and/or AV and those with min-imal CV rejection (greater than 75% graft survival at
...<'5;0ti two years).
FiG 5iMildi *
;IG. 5. Mild chronic vascular rejection. In chronic vascular rejection,varying degrees of myofibrointimal proliferation or onion skinning areseen. This vessel shows a mild degree of lumen obliteration (PAS-alcian blue, X400). -'.
Results
Two hundred six allograft biopsies were done for 204episodes of severe creatinine elevations in 135 patients. !Two biopsies did not contain renal parenchyma andwere not included in this study. There was neither in-fection, complications, nor graft loss as a result of thebiopsy. Data obtained from the biopsy were combined ~with clinical data in determining patient management.All patients have been followed a minimum oftwo yearsfrom biopsy.
Correlation ofBiopsy Findings with Subsequent Trans-plant Nephrectomy Pathology
Sixteen patients had their allografts removed withinone month of biopsy. In 12 the biopsy findings led di- FIG. 6. Severe chronic vascular rejection. These small arteries showonemonthofbiops .In12the biopsyfindinprominent onion skinning with obliteration of the lumens. The glo-rectly to the cessation of high-dose immunosuppression meruli show evidence of chronic transplant glomerulopathy. There is
and subsequent nephrectomy. The remaining four pa- mild tubular atrophy and no evidence of acute rejection (PAS-alcian
tients had continued immunosuppression to try to re- blue, X160).
A-- C.- .-

NEEDLE RENAL ALLOGRAFT BIOPSY 231Ten biopsies in eight patients showed severe chronic
vascular rejection (Table 2; Fig. 1 1). Two kidneys func-tioned for longer than three months; only one currentlyfunctions. The two allografts that functioned longer thanthree months did not show significant acute rejectionand neither patient had an increase in immunosuppres-sion after the biopsy. The value of a biopsy demonstrat-ing severe vascular rejection lies in the confidence interminating or not increasing immunosuppression.Moderate vascular rejection (MoV). Fifty-three biop-
sies were interpreted as showing moderate vascular re-jection. Twenty-three biopsies in 21 patients showedacute moderate vascular rejection. Functional survivalin this group was lower, but not significantly differentthan in those with mild changes. Each biopsy was con-sidered a separate event. Following biopsy, 17 (of 23)kidneys functioned for three months, 14 for one year,and 13 continue to function (Table 2; Fig. 1 1). Eighteenof the biopsies showed acute MoV plus moderate tosevere interstitial infiltrate (Table 3). Eleven kidneys
FIG. 7. Acute tubular necrosis is characterized by varying degrees oftubular damage without an associated interstitial infiltrate. The tubulesare ectatic, and many are lined by attenuated cells. Some epithelialcells sluffed, and a mitosis, evidence for regeneration, is evident (rightof center) (PAS-alcian blue, X205).
Compared with these groups, kidneys with biopsieshaving severe acute vascular or severe chronic vascularrejection had significantly (p < 0.05) decreased survivalfrom three through 24 months. Those with severe ATIand moderate CV had significantly (p < 0.05) decreasedsurvival from six through 24 months. Those with mod-erate acute vascular rejection and moderate acute tubu-lointerstitial rejection had lower survival, but survivaldid not differ statistically from the minimal or mildgroups. These findings are discussed in greater detail insubsequent sections.
Severe, vascular rejection (SV). Twenty-four biopsiesin 21 patients showed severe vascular rejection. Four-teen biopsies in 13 patients showed severe acute vascularrejection. Ten of the 13 kidneys failed within threemonths ofbiopsy and only two currently function (Table2; Fig. 1 1). One of four kidneys having both severe acutevascular rejection and severe acute tubulointerstitial re-jection continues to function two years postbiopsy.
FIG. 8. Viral infection associated nephropathy. This biopsy revealsmarked tubular ectasia and patchy plasma cellular infiltrate. The glo-meruli contain cytomegaloviral inclusions, but are otherwise unre-markable. A lesser degree of tubular damage is more often seen inpatients with CMV disease (hematoxylin-eosin, X 160).
Vol. 197 * No. 2

MATAS ANE
CV.:'l w ".:
OTHERS Ann. Surg. * February 1983
patients were spared increased immunosuppression;four kidneys currently function, and one patient diedwith a functioning graft.
In general, kidneys with moderate vascular rejectionhad better survival compared with those with severevascular rejection. However, the combination ofchronicMoV and moderate to severe ATI was associated withas low a functional survival as kidneys with severe vas-cular rejection. In the absence of moderate to severeATI, kidneys with chronic MoV had relatively good two-year survival.Mild vascular rejection (MiV). Thirty biopsies (29
patients) showed minimal to mild CV. Twenty-five kid-neys (83%) were functioning at three and six months,24 at one year, and 23 at two years (Table 2; Fig. 1 1).Fifteen of these biopsies showed a combination of mildCV plus moderate to severe ATI. Thirteen (87%) ofthesekidneys functioned three and six months, 12 for oneyear, and 11 for two years.
4FIG. 9. Viral infection associated glomerulopathy. A small per cent ofpatients with systemic viral infections develop a glomerulopathy con-sisting of a PAS-positive stringy material and swollen endothelial cells,which obliterate the capillary lumens. Mononuclear cell exudation isabsent or minimal (PAS-alcian blue, X400).
with these findings functioned for over one year and tencontinue to function. Five biopsies showed acute MoVwith minimal or mild ATI; three kidneys continue tofunction.
Thirty biopsies in 25 patients showed chronic mod-erate vascular rejection. Eighteen (of 30) kidneys (60%)were functioning for three months after biopsy, 15 forone year, and 13 (43%) continue to function (Table 2;Fig. 1 1). Overall functional survival in this group wassignificantly decreased from six to 24 months when com-pared with survival of kidneys with minimal or mildchronic vascular changes. Fifteen biopsies showed acombination ofmoderate chronic vascular rejection andmoderate to severe acute interstitial infiltrate. Six kid-neys (40%) functioned for three months and only four(26.7%) for one year (Table 3). In contrast, 15 kidneyswith moderate chronic vascular rejection and only min-imal or mild ATI had significantly (p < 0.05) better sur-vival (Table 3). Five kidneys in this group showed onlychronic changes without any acute infiltrates. All five
FIG. i0. Antilymphocyte globulin reaction. Some patients developevidence of renal insufficiency, associated with ALG treatment. Biop-sies show fibrin-platelet thrombi in glomerular tufts and axial regionsof the glomerulus. Large vessels, the tubules and interstitium are nor-mal (PAS-alcian blue, X 160).
232

Vol. 197 * No. 2 NEEDLE RENAL ALLOGRAFT BIOPSY
TABLE 2. Per Cent ofAllografts with Each BiopsyInterpretation Functioning vs. Time
Per Cent Kidneys Functioning At:
Biopsy 3 6 12 18 24Interpretation Months Months Months Months Months
SCV (n = 10) 20 20 10 10 10S AV (n = 14) 29 29 29 23 23Mo CV (n = 30) 60 53 50 56 43Mo AV (n = 23) 74 61 61 57 57Min or MI CV(n= 30) 83 83 80 77 77
SATI (n = 32) 59 53 50 47 47Mo ATI (n = 53) 79 72 64 64 62Only Min or Mi ATI,Min or MI AV, CTI(n = 41) 83 80 78 78 78
A = acute; C = chronic; Min = minimal; Mi = mild; Mo = moderate; S= severe; TI = tubulointerstitial rejection, and V = vascular rejection.
The finding of mild vascular rejection on biopsy withor without the presence of ATI was associated with agood outcome. Four patients with mild CV alone onbiopsy were not treated with antirejection therapy; allkidneys are functioning. In those with MiV plus ATI,there was generally a good response to antirejection ther-apy. Significantly more kidneys with MiV on biopsyfunctioned over a two-year period then those with severevascular rejection (p < 0.05) or moderate vascular re-jection (p < 0.05).
Combination ofacute and chronic vascular rejection.Twenty-one biopsies (20 patients) showed both acuteand chronic vascular rejection in association with vary-ing amounts of ATI. Twelve kidneys functioned forthree months, and 11 continue to function.
All three kidneys having severe chronic vascular re-jection and mild or moderate acute vascular rejectionfailed within three months. Nine kidneys had moderatechronic vascular rejection-three each with severe,moderate, and mild acute vascular rejection. Two ofthree kidneys with mild AV and one each of kidneyshaving moderate AV and severe AV continue to func-tion.
Nine kidneys had mild CV and mild or moderate AV.The three kidneys with mild CV plus mild AV continueto function. Five of six kidneys with mild CV plus mod-erate AV continue to function.
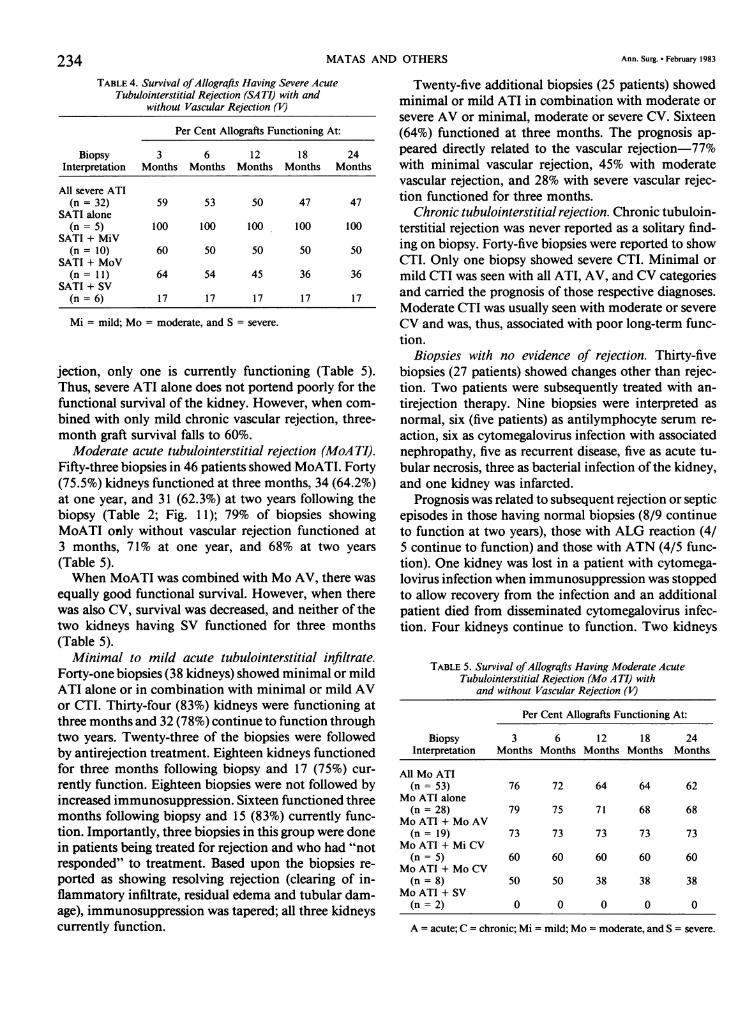
Severe acute tubulointerstitial rejection (SA TI). Thirty-two biopsies in 30 patients showed severe acute tubu-lointerstitial rejection. Nineteen (of 32) functioned forthree months, 16 for one year, and 15 for two years(Table 2; Fig. 1 1). Five of these biopsies showed SATIwithout vascular changes; all kidneys continue to func-tion (Table 4). Ten biopsies in nine patients showedSATI with minimal or mild vascular changes; five kid-neys continue to function (Table 4). Eleven kidneys
0
Li,
233
3 6 12 18 24Time From Biopsy (mos.)
FIG. 11. Per cent allograft function from time of biopsy: A = Acute;C = Chronic; V = Vascular rejection; ATI = Acute tubulointerstitialrejection; S = Severe; Mo = Moderate; Mi = Mild. *Other R = Onlyminimal or Mi ATI, minimal or Mi AV, or CII.
showed SATI plus acute or chronic moderate vascularrejection; five (45%) continue to function. Of six kidneysshowing SATI and severe acute or chronic vascular re-
TABLE 3. Survival ofAllografts Having Moderate Vascular Rejection(MoV) with and without Moderate (Mo) to Severe (S) Acute
Tubulointerstitial Rejection (A TI)
Per Cent Allografts Functioning At:
Biopsy 3 6 12 18 24Interpretation Months Months Months Months Months
All chronic MoV(n= 30) 60 53 50 50 43
Chronic MoV + Moor SATI (n = 15) 40 40 27 27 27
Chronic MoV withoutMo or SATI(n = 15) 80* 73* 73* 73* 73*
All acute MoV(n = 23) 74 61 61 57 57
Acute MoV + Moor SATI (n = 18) 73 61 61 56 56
Acute MoV withoutMo or SATI(n= 5) 80 60 60 60 60
* Patients having MoV without Mo or SATI have significantly better (p< 0.05) graft survival than if Mo or SATI was present.
MATAS AND OTHERS
TABLE 4. Survival ofAllografts Having Severe AcuteTubulointerstitial Rejection (SA TI) with and
without Vascular Rejection (V)
Per Cent Allografts Functioning At:
Biopsy 3 6 12 18 24Interpretation Months Months Months Months Months
All severe ATI(n= 32) 59 53 50 47 47
SATI alone(n = 5) 100 100 100 100 100
SATI + MiV(n= 10) 60 50 50 50 50
SATI + MoV(n= 11) 64 54 45 36 36
SATI + SV(n =6) 17 17 17 17 17
Mi = mild; Mo = moderate, and S = severe.
jection, only one is currently functioning (Table 5).Thus, severe ATI alone does not portend poorly for thefunctional survival of the kidney. However, when com-bined with only mild chronic vascular rejection, three-month graft survival falls to 60%.
Moderate acute tubulointerstitial rejection (MoA TI).Fifty-three biopsies in 46 patients showed MoATI. Forty(75.5%) kidneys functioned at three months, 34 (64.2%)at one year, and 31 (62.3%) at two years following thebiopsy (Table 2; Fig. 11); 79% of biopsies showingMoATI only without vascular rejection functioned at3 months, 71% at one year, and 68% at two years(Table 5).When MoATI was combined with Mo AV, there was
equally good functional survival. However, when therewas also CV, survival was decreased, and neither of thetwo kidneys having SV functioned for three months(Table 5).Minimal to mild acute tubulointerstitial infiltrate.
Forty-one biopsies (38 kidneys) showed minimal or mildATI alone or in combination with minimal or mild AVor CTI. Thirty-four (83%) kidneys were functioning atthree months and 32 (78%) continue to function throughtwo years. Twenty-three of the biopsies were followedby antirejection treatment. Eighteen kidneys functionedfor three months following biopsy and 17 (75%) cur-rently function. Eighteen biopsies were not followed byincreased immunosuppression. Sixteen functioned threemonths following biopsy and 15 (83%) currently func-tion. Importantly, three biopsies in this group were donein patients being treated for rejection and who had "notresponded" to treatment. Based upon the biopsies re-ported as showing resolving rejection (clearing of in-flammatory infiltrate, residual edema and tubular dam-age), immunosuppression was tapered; all three kidneyscurrently function.
Twenty-five additional biopsies (25 patients) showedminimal or mild ATI in combination with moderate orsevere AV or minimal, moderate or severe CV. Sixteen(64%) functioned at three months. The prognosis ap-peared directly related to the vascular rejection-77%with minimal vascular rejection, 45% with moderatevascular rejection, and 28% with severe vascular rejec-tion functioned for three months.
Chronic tubulointerstitial rejection. Chronic tubuloin-terstitial rejection was never reported as a solitary find-ing on biopsy. Forty-five biopsies were reported to showCTI. Only one biopsy showed severe CTI. Minimal ormild CTI was seen with all ATI, AV, and CV categoriesand carried the prognosis of those respective diagnoses.Moderate CTI was usually seen with moderate or severeCV and was, thus, associated with poor long-term func-tion.
Biopsies with no evidence of rejection. Thirty-fivebiopsies (27 patients) showed changes other than rejec-tion. Two patients were subsequently treated with an-tirejection therapy. Nine biopsies were interpreted asnormal, six (five patients) as antilymphocyte serum re-action, six as cytomegalovirus infection with associatednephropathy, five as recurrent disease, five as acute tu-bular necrosis, three as bacterial infection of the kidney,and one kidney was infarcted.
Prognosis was related to subsequent rejection or septicepisodes in those having normal biopsies (8/9 continueto function at two years), those with ALG reaction (4/5 continue to function) and those with ATN (4/5 func-tion). One kidney was lost in a patient with cytomega-lovirus infection when immunosuppression was stoppedto allow recovery from the infection and an additionalpatient died from disseminated cytomegalovirus infec-tion. Four kidneys continue to function. Two kidneys
TABLE 5. Survival ofAllografts Having Moderate AcuteTubulointerstitial Rejection (Mo ATI) with
and without Vascular Rejection (V)
Per Cent Allografts Functioning At:
Biopsy 3 6 12 18 24Interpretation Months Months Months Months Months
All Mo ATI(n= 53) 76 72 64 64 62
Mo ATI alone(n = 28) 79 75 71 68 68
Mo ATI + Mo AV(n= 19) 73 73 73 73 73
Mo ATI + Mi CV(n= 5) 60 60 60 60 60
Mo ATI + Mo CV(n = 8) 50 50 38 38 38
Mo ATI + SV(n =2) 0 0 0 0 0
A = acute; C = chronic; Mi = mild; Mo = moderate, and S = severe.
234 Ann. Surg. * February 1983

NEEDLE RENAL ALLOGRAFT BIOPSY
transplanted to a patient with oxalosis were lost to re-
current disease, whereas one with recurrent focal scle-rosis functioned five years postbiopsy and then was lostto recurrent disease.
Do Changes in Sequential Biopsies in the Same PatientPredict Outcome?
Thirty patients with rejection on an initial biopsy werebiopsied on more than one occasion (total of 72 biop-sies). Twelve patients subsequently lost their kidneys; 18kidneys currently function. Sequential biopsies were
studied to see if they predicted outcome. The develop-ment or worsening of vascular changes suggested sub-sequent kidney loss, whereas an improvement in thedegree of ATI predicted long-term function.
Overall Value ofBiopsy
Two hundred four adequate biopsies were performedin 135 patients with elevated creatinine levels and a pu-
tative diagnosis of rejection. Eighty-one (39.7%) resultedin tapering or not increasing the amount of immuno-suppression (eight severe CV, five moderate CV alone,four mild CV alone, 12 severe AV, one mild AV alone,18 minimal or mild ATI, 33 no rejection). Of these, 38biopsies led to diagnoses other than rejection that sig-nificantly affected patient management (e.g., cytomeg-alovirus infection). Importantly, the risk of increasedimmunosuppression could be decided in the face of his-tologic evidence of rejection rather than a clinicalimpression.
Discussion
There is no laboratory test that will definitively makethe diagnosis of renal allograft rejection. Rejection ep-
isodes are clinically suspected when the patient presentswith any of, or a combination of, elevated creatininelevel, decreased urine output, weight gain, elevatedblood pressure, fever, and a swollen and tender allograft.In patients who have received prophylactic antilympho-cyte globulin or are longer than three months post-trans-plant, an elevated creatinine level may be the only signof rejection. However, serum creatinine levels can beelevated in the post-transplant period due to a numberof conditions other than rejection.7
Acute tubular necrosis is a frequent cause of creati-nine elevation in the early post-transplant period. ATNoccurs occasionally after a living related donor trans-plant, but is much more common following cadaverdonor transplantation. The lesion in the kidney is re-
versible and the kidney will begin to function again ifrejection does not intervene. The time required for renalfunction to resume is variable and may take as long as
six weeks. During this interval, the creatinine level re-
mains elevated and the patient requires maintenancehemodialysis. Creatinine level, in this situation, oftencannot be used as an aid to the diagnosis ofa developingrejection episode. Similarly, other tests of renal function(e.g., I'3' iodo hippuran scan) will not differentiate be-tween ATN and rejection. Biopsy in this situation can
differentiate between ATN (Fig. 6) and ATI (Figs. 1 and2) which have characteristic and different morphologies.
Other clinical situations may also mimic a rejectionepisode. Infection, hyperglycemia, renal artery stenosis,lymphocele, ureteral obstruction, and recurrence of theoriginal disease have each been associated with elevationin serum creatinine level.7 Hyperglycemia can be diag-nosed with a plasma glucose determination, and at theUniversity of Minnesota, plasma glucose is measuredsimultaneously with each creatinine level in all diabeticpatients. If blood glucose and creatinine are elevated,the hyperglycemia is corrected and the creatinine levelrepeated before antirejection treatment is instituted.'4Renal artery stenosis should be considered if there is a
history of hypertension that is difficult to control. Lym-phocele and ureteral obstruction can be diagnosed bysonography. Patients having infection may present withfever and elevated creatinine level. Since all patients are
receiving immunosuppression, the source of infectionmay be hidden, leading to a mistaken diagnosis of re-
jection.Also important in sparing patients the hazards of in-
creased immunosuppression is not treating patientswhose rejections are irreversible or would be reversiblefor very short time periods. It is generally agreed,'5-'8although it has not been proven in a randomized study,that the presence of severe vascular rejection suggestsa poor prognosis and should not be treated with anti-rejection therapy. This study lends support to that con-
cept. Less than 30% of kidneys with severe acute or
chronic vascular rejection were functioning three monthspostbiopsy. The authors, however, did not treat thesepatients with antirejection therapy, making it impossibleto predict how many kidneys given treatment wouldhave improved function. Others have reported poor
functional survival when patients with vascular rejectionon biopsy were treated with antirejection therapy.'51'8A crucial consideration is whether rejection is a focal
or diffuse process. If focal, a needle biopsy may not berepresentative of what is taking place in the rest of thekidney. Rapaport et al.'9 recently stated "percutaneousrenal biopsy of the renal transplant has been generallyabandoned because rejection injury is not distributeduniformly throughout the transplanted kidney, and thedangers of hemorrhage and infection are far greater."The authors' concept has been that the rejection processis distributed relatively uniformly. Confusion in termi-
235Vol. 197 * No. 2

MATAS AND OTHERS
nology may play a role here. When "focal" patches ofan acute cellular infiltrate in a biopsy are seen (Fig. 1),the rejection process is described as mild, and it is con-ceptualized that similar "focal" patches exist throughoutthe kidney. Severe acute rejection is one in which the"focal" areas are larger and eventually coalesce (Fig. 2).Importantly, in this series, there were neither infectiouscomplications nor graft loss due to the biopsy. Rose etal.20 have studied the reliability of biopsy in cardiactransplantation by comparing endomyocardial biop-tome samples and full thickness sections from 26 for-malin-fixed previously transplanted hearts. Bioptomesamples were assigned a histologic rejection score andthen compared with the score given full thickness tissuesections from the same heart. They found that endomyo-cardial biopsy was highly accurate in detecting the pres-ence of rejection, although biopsy did not always agreewith the severity of rejection seen in a full thicknesssection of the same heart. The authors were not able tosimultaneously compare biopsy with full thickness sec-
tions. However, 16 patients lost their kidneys within onemonth of biopsy (nine within one week). In no case didthe findings on biopsy overestimate the degree of rejec-tion.
It is important to determine the value of allograftbiopsy in post-transplant patient management. In thepast, at this institution, all patients admitted with ele-vated creatinine levels underwent history and physicalexamination, repeat creatinine determination, bloodglucose determination, I'3' iodo hippuran scan, sonog-raphy and chest radiograph. In spite of this battery oftests, the diagnosis of rejection remained in significantdoubt in many cases. More recently, an allograft biopsyhas been performed on all patients readmitted with el-evated creatinine. With interdepartmental cooperation,such biopsies can be performed, processed, and inter-preted on the same day and, thus, a histologic diagnosiscan be available within 24 hours of admission. Themajor objective value of allograft biopsy in this seriescan be seen in the high per cent of patients (39.7%)spared additional immunosuppressive therapy. On 38occasions, biopsy led to a diagnosis other than rejection(e.g., normal, ATN, infection, resolving rejection). How-ever, further subjective benefit was that with a histologicdiagnosis ofan acute rejection episode, the authors weremore comfortable in accepting the risks of an increaseddose of immunosuppression. It would be valuable toshow improved patient morbidity and mortality as a
result of routine use of allograft biopsy. A marked im-provement in morbidity and mortality can be demon-strated in this series from before routine use of biopsyto the present time.2' However, since so many otherfactors in the protocols have changed concurrently, it
is impossible to determine the role of biopsy in this im-provement.
Others have similarly found allograft biopsy helpfulin patient management as well as being predictive oflong-term outcome. Finkelstein et al.,'5 in a retrospec-tive study, found allograft biopsy useful in diagnosingan acute rejection episode and in predicting the short-term (one month) response to anti-rejection therapy.Lack of response was predicted on the basis of the pres-
ence of severe vascular changes or moderate vascularchanges plus acute rejection changes. Twenty-seven of28 patients predicted to respond to therapy had im-proved renal function one month postbiopsy as opposedto three of 18 patients predicted not to respond. Im-portantly, 16 biopsies showed severe vascular changes.All 16 patients received antirejection therapy; 13 had noresponse, three had a partial response (serum creatinineremained greater than 2 mg/100 ml during the one
month period, but fell below pretreatment values).Hsu et al. followed 44 patients whose allograft biopsy
revealed rejection to determine iftwo-month postbiopsyfunction could be predicted.'6 They found certain his-tologic criteria (most significantly, small vessel pathol-ogy) predicted poor function at two months and con-
cluded that biopsy could help the physician decidewhether to begin antirejection therapy. Hebertson et al. '7reported on long-term function of allografts biopsiedduring the first 90 post-transplant days. Biopsies were
done in patients with poor graft function and the di-agnoses included rejection, poor preservation, nonrejec-tion vascular complications, ureteric obstruction, andinfection. They found a highly significant relationshipbetween early graft failure and the presence of medialnecrosis of arteries, acute glomerular lesions, and inter-stitial hemorrhage. Mononuclear cell infiltration of thearterial intima was also associated with poor graft func-tion. Similarly, Kler et al.22 found that, in early post-transplant biopsies, infarction, glomerular capillarythrombosis, or arterial/arteriolar thrombosis were as-
sociated with 100% graft loss within one year.More recently, Magil et al. reported on long-term
function of allografts biopsied during acute rejectionepisodes that were not responding to antirejection ther-apy.'8 Antirejection therapy was continued postbiopsyin all patients. They found that allografts with vascularpathology had significantly decreased survival. Thesestudies plus the authors' own, although using biopsy indifferent clinical situations, uniformly agree that mod-erate to severe vascular rejection is associated with sig-nificantly decreased allograft function.
In summary, it was attempted in this retrospectivestudy to answer five questions about the value of allo-graft biopsy. It is concluded that 1) allograft biopsy can
236 Ann. Surg. * February 1983

Vol. 197 * No. 2 NEEDLE RENAL ALLOGRAFT BIOPSY 237
be done without graft loss or infection-there were nobiopsy-associated infections or nephrectomies in 206biopsies; 2) biopsy represents changes throughout thekidney-when kidneys were removed subsequent tobiopsy, the pathology of the specimen was similar tothat seen on biopsy; 3) biopsy will predict when not totreat for rejection-biopsy led to a number of nonre-jection diagnoses or showed changes so minimal that itwas elected to not treat with increased immunosuppres-sion; 4) biopsy will help in discontinuing or not increas-ing immunosuppression-biopsies showing severe vas-cular changes should not be followed by aggressive im-munosuppressive therapy; and 5) biopsy predicts earlyand late outcome of treatment of a rejection episode-three-month and two-year graft survival could be pre-dicted using the histopathologic changes present on bi-opsy.
References
1. Salvatierra 0, Potter D, Cochrum C, et al. Improved patient sur-vival in renal transplantation. Surgery 1976; 79:166-174.
2. Tilney NL, Strom TB, Vineyard GC, Merrill JP. Factors contrib-uting to the declining mortality rate in renal transplantation.New Engl J Med 1978; 299:1321-1325.
3. Vincenti F, Amend W, Feduska NJ, et al. Improved outcomefollowing renal transplantation with reduction in the immu-nosuppression therapy for rejection episodes. Am J Med 1980;69:107-112.
4. Matas AJ, Simmons RL, Buselmeier RJ, et al. The fate of patientssurviving three years after renal transplantation. Surgery 1976;80:390-395.
5. Bach MC, Adler JL, Breman J, et al. Influence of reaction therapyon fungal and nocardial infections in renal transplant recipi-ents. Lancet 1973; 1: 180-185.
6. Matas AJ, Simmons RL, Kjellstrand CM, et al. When should thethird renal transplant rejection episode be treated. Ann Surg1977; 186:114-120.
7. Matas AJ, Simmons RL, Kjellstrand CM, Najarian JS. Pseudo-
rejection: factors mimicking rejection in renal allograft recip-ients. Ann Surg 1977; 186:51-59.
8. Simmons RL, Kjellstrand CM, Najarian JS. Technique, compli-cations and results. In: Najarian JS, Simmons RL, eds. Trans-plantation. Philadelphia: Lea & Febiger, 1972; 445-495.
9. Howard RJ, Condie RM, Sutherland DER, et al. The use of an-tilymphoblast globulin in the treatment of renal allograft re-jection. Trans Proc 1981; 13:473-474.
10. Buselmeier TJ, Schauer RM, Mauer SM, et al. A simplifiedmethod of percutaneous allograft biopsy. Nephron 1976;16:318-321.
11. Harmon JB, Sibley RK, Peterson P, Ferguson R. Cytomegalovirusviremic and renal allograft morphology: are there distinctpathologic features? Lab Invest 1982; 46:35A.
12. Richardson WP, Colvin RB, Cheeseman SH, et al. Glomerulo-pathy associated with cytomegalovirus viremia in renal allo-grafts. New Engl J Med 1981; 305:57-63.
13. Najarian JS, Simmons RL, Condie RM, et al. Seven years' ex-perience with antilymphoblast globulin for renal transplanta-tion from cadaver donors. Ann Surg 1976; 184:352-368.
14. Matas AJ, Simmons RL, Kjellstrand CM, Najarian JS. Increasedserum creatinine resulting from hyperglycemia mimicking re-jection. Ann Int Med 1975; 83:519.
15. Finkelstein FO, Siegel NJ, Bastl C, et al. Kidney transplant biop-sies in the diagnosis and management of acute rejection re-actions. Kidney Int 1976; 10: 17 1-178.
16. Hsu AC, Arbus GS, Noriega E, Huber J. Renal allograft biopsy:a satisfactory adjunct for predicting renal function after graftrejection. Clin Nephrol 1976; 5:260-265.
17. Hebertson BM, Evans DB, Calne RY, Banerjee AK. Percutaneousneedle biopsies of renal allografts: the relationship betweenmorphological changes present in biopsies and subsequent al-lograft function. Histopathology 1978; 1: 161-178.
18. Magil A, Rubin J, Ladewig L, et al. Renal biopsy in acute allograftrejection. Nephron 1980; 26:180-183.
19. Rapaport FT, Converse JM, Billingham RE. Recent advances inclinical and experimental transplantation. JAMA 1977;237:2835-2840.
20. Rose AG, Uys CJ, Losman JG, Barnard CN. Evaluation of en-domyocardial biopsy in the diagnosis of cardiac rejection.Transplantation 1978; 26:10-13.
21. Sutherland DER, Fryd DS, Morrow CE, et al. The high risk re-cipient in renal transplantation. Trans Proc 1982; 14:19-27.
22. Kier H, Hanser HE, Olsen S. The predictive value ofpercutaneousbiopsies from human renal allografts with early impaired func-tion. Clin Nephrol 1980; 13:58-63.
Copyright © 2022 FDOKUMEN




















