
Pneumonia Prevention to Decrease Mortality in Intensive Care ...
Upload
independentCategory
view
1download
0
BCFT
B
M
R
C
Fbpcipasbdt
Fs
2
SS8CTj
lood Transfusions Decrease the Incidence of Acute Rejection inardiac Allograft Recipients
élix G. Fernández, MD, Andres Jaramillo, PhD, Greg Ewald, MD, Joseph Rogers, MD, Michael K. Pasque, MD,. Mohanakumar, PhD, and Nader Moazami, MD
ackground: Cardiac transplant recipients frequently receive a large number of transfusions. The objective of thisstudy was to determine whether there is an association between total number of blood transfusionsand cardiac allograft rejection.
ethods: A retrospective analysis of all cardiac transplants between October 1, 1997, and December 31, 2001,was performed. Total number of transfusions, total number of rejection episodes Grade 3A or more,rejection-free survival, and overall survival were analyzed. Comparisons between patients bridged totransplantation with a Novacor left ventricular assist device (LVAD) and the primary transplantgroup were also made.
esults: Eighty-two patients were transplanted. Fifteen were bridged to transplantation, and 67 underwentprimary heart transplantation. Age and sex were similar for the LVAD group and the primarytransplant group (45 � 11 vs 47 � 15 years and 67% vs 58% male sex, respectively). Mean follow-upwas 658 � 486 days for the LVAD group and 708 � 548 days for the primary transplant group.Transfusions received were 50 � 34 U of packed red blood cells for the LVAD group and 7 � 12for the primary transplant group (p � 0.001). There were no differences in donor characteristicsbetween the 2 groups. The incidence of acute rejection within 1 year was 27% for the LVAD groupand 39% for the primary transplant group (p � .28). Freedom from rejection was 71% at 1 year inthe LVAD group compared with 59% for the primary transplant group (p � 0.39). In all 82 patients,the total number of transfusions was inversely correlated with the development of acute rejection(p � 0.011). Survival was 80% and 62% for the LVAD group at 1 and 3 years after transplantation and88% and 85%, respectively, for the primary transplant group (p � 0.045).
onclusions: The number of blood transfusions received by heart transplant recipients is inversely related withthe number of acute rejection episodes. J Heart Lung Transplant 2005;24:S255–S261. Copyright ©
2005 by the International Society for Heart and Lung Transplantation.htbpaDasmu
wtacpohglb
or more than 30 years, an association has been notedetween pretransplantation blood transfusions and im-roved kidney allograft survival.1,2 This association hasontinued to be observed, even in the modern era ofmmunosuppression.3,4 A beneficial effect of pretrans-lantation transfusion has also been noted in cardiacllograft recipients.5 Enhanced survival was demon-trated in cardiac transplant recipients who receivedlood before transplantation compared with those whoid not. Several mechanisms for the immunomodula-ory properties of pretransplantation blood transfusions
rom the Washington University School of Medicine, St Louis, Mis-ouri.
Submitted April 12, 2004; revised June 22, 2004; accepted July 19,004.Reprint requests: Nader Moazami, MD, Washington University
chool of Medicine, Division of Cardiothoracic Surgery, Box 8234,uite 3108, Queeny Tower, St Louis, MO 63110. Telephone: 314-362-008. Fax: 314-747-4216. E-mail: [email protected] © 2005 by the International Society for Heart and Lungransplantation. 1053-2498/05/$–see front matter. doi:10.1016/
m.healun.2004.07.009
ave been proposed, although none has been defini-ively proven. It seems essential that viable leukocytese present in the transfusate, because leukocyte-de-leted blood has been found to be ineffective.6,7 Anssociation between human leukocyte antigen (HLA)R antigen shared pretransplantation blood transfusionnd cardiac allograft survival has also been ob-erved.8–10 The optimal number or cumulative effect ofultiple pretransplantation blood transfusions remains
nknown.In recent years, there has been increasing experienceith left ventricular assist devices (LVADs) as a bridge
o cardiac transplantation.11–13 Both the LVAD implantnd subsequent explant and heart transplantation pro-edures can be associated with a significant amount oferioperative hemorrhage, necessitating a large numberf transfusions. Factors associated with perioperativeemorrhage in these patients include reoperative sur-ery, preexisting coagulopathy, and the use of antiplate-et agents and anticoagulants. The result is that patientsridged to heart transplantation with a LVAD receive
any pretransplantation blood transfusions. Transfu-S255

spccpnrcbc
MS
FocrAdfpipiratsb
I
Aocdswntaia
R
Topctwm3wdt
cHr
S
SvfbFwllt
R
Oucp6ddLpRwgead
pif(5cmmtpScg
w86StthP
S256 Fernández et al. The Journal of Heart and Lung TransplantationJuly (Suppl) 2005
ions have been associated with elevated levels ofreformed antibodies against HLA and a possible in-reased risk for allograft rejection. Although this asso-iation has never been adequately demonstrated, theossibility remains that transfusions may have an immu-osuppressive effect, similar to that observed in theenal transplant population. We demonstrate an inverseorrelation between the number of pretransplantationlood transfusions and episodes of significant acuteardiac allograft rejection.
ATERIAL AND METHODStudy Subjects
rom October 1997 through December 2001, 82 adultrthotopic heart transplants were performed on theardiac surgery service at Barnes-Jewish Hospital. Aetrospective analysis of these patients was performed.ll recipient and donor demographic data, as well asata on rejection episodes and mortality, were obtainedrom our institutional database, which is maintainedrospectively. Transfusion data were obtained from the
nstitutional blood bank database. It has been ourractice to use leukocyte-depleted blood; however, this
s very often not possible because of patient hemor-hage, which requires the use of the most rapidlyvailable blood. The result is that the majority of bloodransfused is often not leukocyte depleted. This re-earch project was approved by the institutional reviewoard of the Washington University School of Medicine.
mmunosuppression Protocol
fter heart transplantation, all patients were maintainedn a triple-drug immunosuppression regimen based onyclosporine, prednisone, and azathioprine. Cytolytic in-uction therapy with either ATGAM or OKT3 was usedelectively in 4 cases. Rejection episodes were treatedith high pulsed doses of prednisone or methylpred-isolone. OKT3, thymoglobulin, and ATGAM were usedo treat rejection in 2 instances each, and 1 patient wasdditionally treated with photopheresis. In 8 patients themmunosuppressive regimen was switched to tacrolimusnd mycophenolate mofetil.
ejection Diagnosis
he diagnosis of acute rejection was made on the basisf histology obtained from endomyocardial biopsy sam-les. Biopsies were performed on the basis of a suspi-ion of acute rejection, as assessed by clinical parame-ers. Additionally, surveillance endomyocardial biopsiesere performed weekly for the first posttransplantationonth, monthly for the first 6 months, and then everymonths for the first year. Endomyocardial biopsiesere then performed every 3 to 6 months thereafter,epending on the clinical circumstance. Cellular rejec-
ion was graded histologically on the basis of the dlassification proposed by the International Society ofeart and Lung Transplantation.14 Patients were not
outinely tested for humoral rejection.
tatistical Analysis
tatistical analysis of data were performed by SASersion 8 (SAS Institute, Cary, NC). Group differencesor continuous and categorical variables were analyzedy Student’s t-test and Pearson �2 analysis, respectively.reedom from rejection and overall patient survivalere determined by Kaplan-Meier analysis, and the
og-rank test was used for comparison of groups. A Coxogistic regression analysis was performed to examinehe effect of blood transfusions on acute rejection.
ESULTS
ut of 82 orthotopic cardiac transplants, 67 patientsnderwent primary heart transplantation and 15 re-eived pretransplantation mechanical circulatory sup-ort with a Novacor LVAD. Mean follow-up time was99 days (range 1–1860 days): 708 days (range 1–1860ays) for the primary heart transplant group and 658ays (range 1–1614 days) for the LVAD group. The 15VAD patients bridged to transplantation were sup-orted for a mean of 174 days (range 4–497 days).ecipient and donor characteristics for the group as ahole and the LVAD and primary heart transplant
roups individually are listed in Tables 1 and 2. With thexception of the LVAD group having a greater percent-ge of male donors, the 2 groups were similar inemographics.There were no differences in the levels of pretrans-
lantation panel-reactive antibodies (PRA) or allograftschemic time. The number of blood and platelet trans-usions was significantly greater in the LVAD groupTable 3). The LVAD patients received a mean total of0.1 U of packed red blood cells and 6.7 U of plateletsompared with 6.9 and 1.6, respectively, for the pri-ary heart transplant patients. A prospective cross-atch was performed in 80% (66 of 82) cases before
ransplantation: 78% (52 of 67) in the primary trans-lant group and 87% (13 of 15) in the LVAD group.even patients were transplanted across a positiverossmatch, 6 in the primary group and 1 in the LVADroup.The incidence of Grade 3A or more acute rejectionithin the first posttransplantation year was 37% (30 of
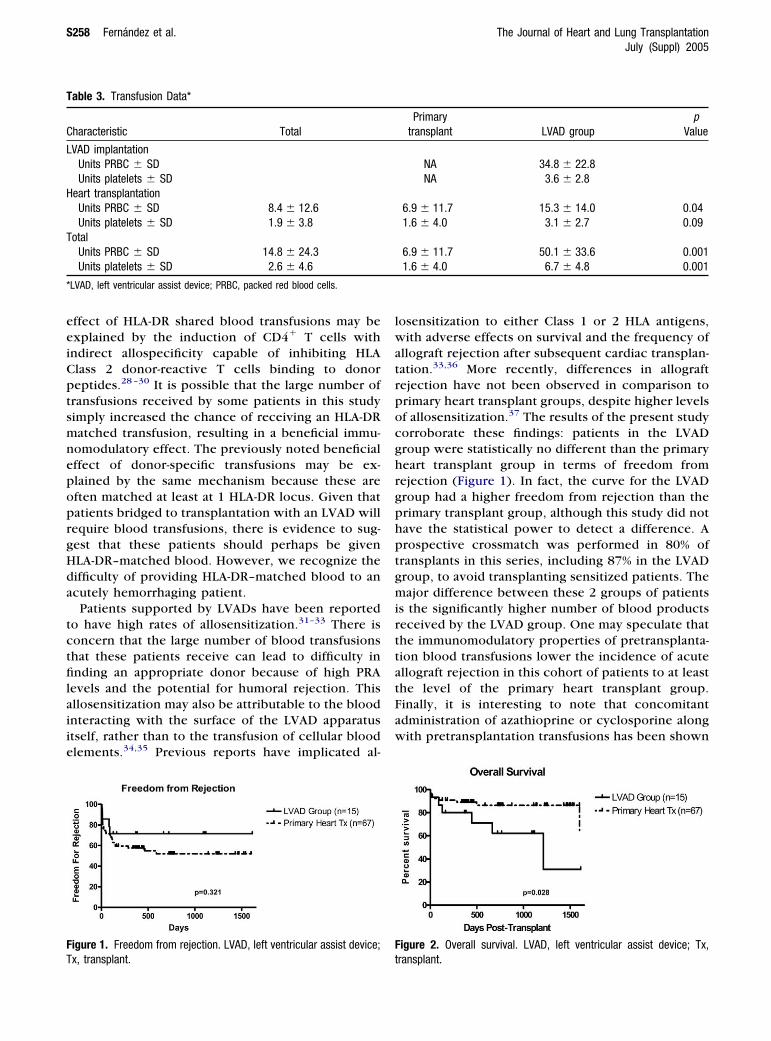
2): 27% (4 of 15) in the LVAD group and 39% (26 of7) in the primary heart transplant group (p � 0.28).hort-term freedom from acute rejection was not statis-ically different between the LVAD and primary heartransplant groups (Figure 1). Short-term overall survival,owever, was worse in the LVAD group (Figure 2).erioperative mortality, defined as a death within 30
ays of transplantation, was 8.5% (7 of 82): 6.6% (1 of
1hddpti(
gtsddtiip(iht
g(
D
Tbeihpkfiietprisitr
csffdsFtpbHs
T
C
NAS
E
CPPPI
*
T
C
NAS
C
C
*
The Journal of Heart and Lung Transplantation Fernández et al. S257Volume 24, Number 7S
5) in the LVAD group and 9.0% (6 of 67) in primaryeart transplant recipients (p � 0.61). There were 2eaths from acute rejection, 1 in each group. Causes ofeath in each group are listed in Table 4. Finally, whenatients were assigned to high and low PRA groups,here was no difference in freedom from acute rejectionn patients with a pretransplantation PRA �10 vs �10Figure 3).
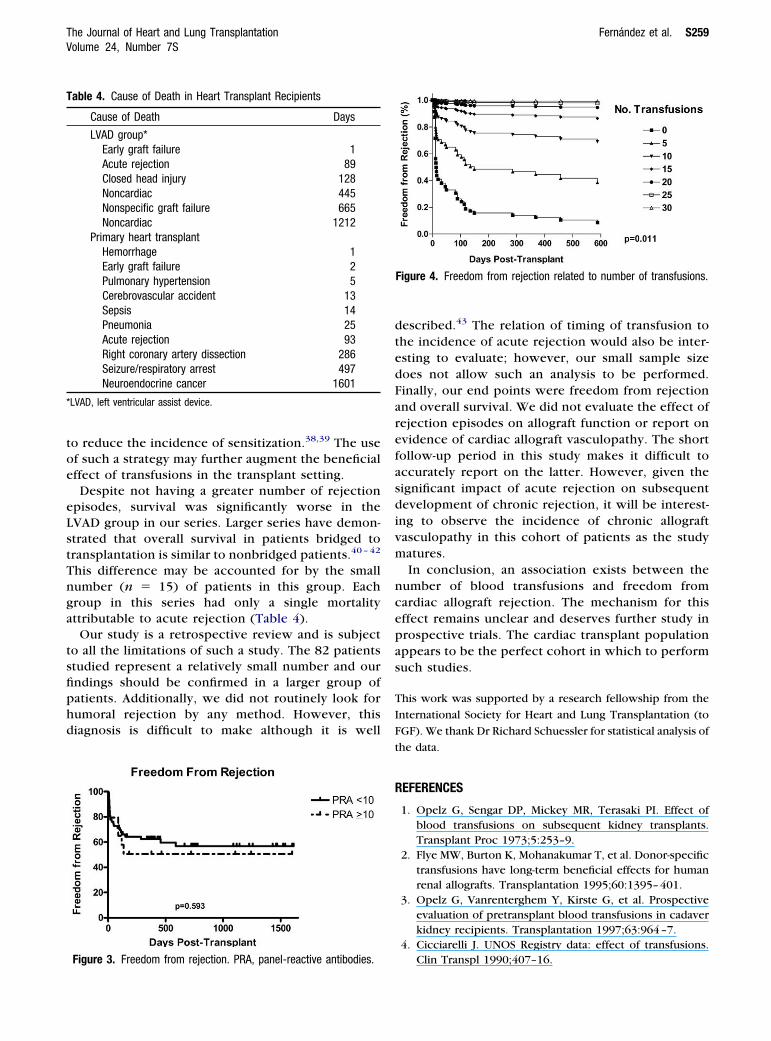
When data from all 82 patients were grouped to-ether and subjected to Cox logistic regression analysis,he overall number of packed red blood cell transfu-ions was significantly inversely correlated with theevelopment of acute rejection episodes (Figure 4). Asepicted in Figure 4, as the number of pretransplanta-ion transfusions a cardiac allograft recipient receivedncreased, the expected freedom from acute rejectionncreased as well. Factors that were not significantredictors of acute rejection on multivariate analysisCox proportional-hazard model) included the follow-ng: donor age, recipient and donor sex, etiology ofeart failure, recipient and donor cytomegalovirus sta-us, previous pregnancy, pretransplantation PRA, allo-
able 1. Recipient Characteristics
haracteristic Total
o. patients 82ge, years, mean � SD 48.1 � 12.2ex, n (%)
Male 49 (60%)Female 33 (40%)
tiology, n (%)Ischemic 34 (41%)Idiopathic dilated CMY 39 (48%)Other 9 (11%)
ytomegalovirus positive, n (%) 45 (55%)revious pregnancy 26/33 (79%)retransplant PRA, % (range) 5.5% (0–100)retransplant PRA �10, n % 16 (20%)
schemic time, minutes 168 (97–308)
LVAD, left ventricular assist device; PRA, panel-reactive antibodies.
able 2. Donor Characteristics
haracteristic TotalPrimary
transplant LVAD group*
o. patients 82 67 15ge, years, mean � SD 29 � 12a 30 � 13 27 � 9ex, n (%)
Male 50 (61%) 36 (54%) 14 (93%)Female 32 (39%) 31 (46%) 1 (7%)
ause of death, n (%)Traumatic 65 (79%) 52 (78%) 13 (87%)Nontraumatic 17 (21%) 15 (22%) 2 (13%)
ytomegalovirus positive, n (%) 47 (57%) 41 (61%) 6 (40%)
hLVAD, left ventricular assist device.
raft ischemic time, and traumatic donor cause of deathdata not shown).
ISCUSSION
he salient finding of this study is that as the number oflood transfusions received by cardiac allograft recipi-nts increases, there is a significant reduction in thencidence of acute allograft rejection. Several studiesave previously reported on the association betweenretransplantation blood transfusions and improvedidney or cardiac allograft survival.1,3–5,15–17 The bene-cial effect of transfusions has also been demonstrated
n experimental animal transplant models.18–21 How-ver, the cumulative effect on multiple pretransplanta-ion blood transfusions is not well known. It has beenreviously reported that renal transplant recipients thateceived 5 or more random blood transfusions hadncreased graft survival compared with no transfu-ions.22 The results presented in this study that annverse correlation exists between the number of bloodransfusions and the incidence of acute cardiac allograftejection is in agreement with this concept.
Several mechanisms have been suggested to ac-ount for the blood transfusion effect, although noingle mechanism is generally accepted to accountor this effect. These include a selective loss ofunctional antidonor cytolytic T cell precursors,23
ecreased expression of costimulatory molecules intored blood,24 mixed chimerism,25 soluble HLA andas molecule in transfused blood,26 and induction ofransforming growth factor beta release by donorhosphatidylserine-bearing cells.27 Interestingly, aetter outcome has been observed in recipients ofLA-DR matched pretransplantation blood transfu-
ions in several studies.8,10 In vitro studies with
Primarytransplant LVAD group*
67 1547 � 17 45 � 11
39 (58%) 10 (67%)28 (32%) 5 (33%)
28 (42%) 6 (40%)31 (46%) 8 (53%)8 (12%) 1 (7%)
37 (55%) 8 (53%)22/28 (79%) 4/5 (80%)4.1% (0–36) 11.5% (0–100)
12 (18%) 4 (28%)167 (97–270) 187 (110–308)
uman cell lines have suggested that the beneficial
eeiCptsmnepoprgHda
tctfilaiie
lwatrpocghrgphptgmirttatFaw
FT
F
T
C
L
H
T
*
S258 Fernández et al. The Journal of Heart and Lung TransplantationJuly (Suppl) 2005
ffect of HLA-DR shared blood transfusions may bexplained by the induction of CD4� T cells withndirect allospecificity capable of inhibiting HLAlass 2 donor-reactive T cells binding to donoreptides.28 –30 It is possible that the large number ofransfusions received by some patients in this studyimply increased the chance of receiving an HLA-DRatched transfusion, resulting in a beneficial immu-
omodulatory effect. The previously noted beneficialffect of donor-specific transfusions may be ex-lained by the same mechanism because these areften matched at least at 1 HLA-DR locus. Given thatatients bridged to transplantation with an LVAD willequire blood transfusions, there is evidence to sug-est that these patients should perhaps be givenLA-DR–matched blood. However, we recognize theifficulty of providing HLA-DR–matched blood to ancutely hemorrhaging patient.
Patients supported by LVADs have been reportedo have high rates of allosensitization.31–33 There isoncern that the large number of blood transfusionshat these patients receive can lead to difficulty innding an appropriate donor because of high PRA
evels and the potential for humoral rejection. Thisllosensitization may also be attributable to the bloodnteracting with the surface of the LVAD apparatustself, rather than to the transfusion of cellular bloodlements.34,35 Previous reports have implicated al-
igure 1. Freedom from rejection. LVAD, left ventricular assist device;
able 3. Transfusion Data*
haracteristic Total
VAD implantationUnits PRBC � SDUnits platelets � SD
eart transplantationUnits PRBC � SD 8.4 � 12.6Units platelets � SD 1.9 � 3.8
otalUnits PRBC � SD 14.8 � 24.3Units platelets � SD 2.6 � 4.6
LVAD, left ventricular assist device; PRBC, packed red blood cells.
x, transplant. t
osensitization to either Class 1 or 2 HLA antigens,ith adverse effects on survival and the frequency of
llograft rejection after subsequent cardiac transplan-ation.33,36 More recently, differences in allograftejection have not been observed in comparison torimary heart transplant groups, despite higher levelsf allosensitization.37 The results of the present studyorroborate these findings: patients in the LVADroup were statistically no different than the primaryeart transplant group in terms of freedom fromejection (Figure 1). In fact, the curve for the LVADroup had a higher freedom from rejection than therimary transplant group, although this study did notave the statistical power to detect a difference. Arospective crossmatch was performed in 80% ofransplants in this series, including 87% in the LVADroup, to avoid transplanting sensitized patients. Theajor difference between these 2 groups of patients
s the significantly higher number of blood productseceived by the LVAD group. One may speculate thathe immunomodulatory properties of pretransplanta-ion blood transfusions lower the incidence of acutellograft rejection in this cohort of patients to at leasthe level of the primary heart transplant group.inally, it is interesting to note that concomitantdministration of azathioprine or cyclosporine alongith pretransplantation transfusions has been shown
igure 2. Overall survival. LVAD, left ventricular assist device; Tx,
Primarytransplant LVAD group
pValue
NA 34.8 � 22.8NA 3.6 � 2.8
6.9 � 11.7 15.3 � 14.0 0.041.6 � 4.0 3.1 � 2.7 0.09
6.9 � 11.7 50.1 � 33.6 0.0011.6 � 4.0 6.7 � 4.8 0.001
ransplant.
toe
eLstTnga
tsfiphd
dtedFarefasdivm
ncepas
T
I
F
t
R
T
*
The Journal of Heart and Lung Transplantation Fernández et al. S259Volume 24, Number 7S
o reduce the incidence of sensitization.38,39 The usef such a strategy may further augment the beneficialffect of transfusions in the transplant setting.Despite not having a greater number of rejection
pisodes, survival was significantly worse in theVAD group in our series. Larger series have demon-trated that overall survival in patients bridged toransplantation is similar to nonbridged patients.40 – 42
his difference may be accounted for by the smallumber (n � 15) of patients in this group. Eachroup in this series had only a single mortalityttributable to acute rejection (Table 4).
Our study is a retrospective review and is subjecto all the limitations of such a study. The 82 patientstudied represent a relatively small number and ourndings should be confirmed in a larger group ofatients. Additionally, we did not routinely look forumoral rejection by any method. However, thisiagnosis is difficult to make although it is well
able 4. Cause of Death in Heart Transplant Recipients
Cause of Death Days
LVAD group*Early graft failure 1Acute rejection 89Closed head injury 128Noncardiac 445Nonspecific graft failure 665Noncardiac 1212
Primary heart transplantHemorrhage 1Early graft failure 2Pulmonary hypertension 5Cerebrovascular accident 13Sepsis 14Pneumonia 25Acute rejection 93Right coronary artery dissection 286Seizure/respiratory arrest 497Neuroendocrine cancer 1601
LVAD, left ventricular assist device.
Figure 3. Freedom from rejection. PRA, panel-reactive antibodies.
escribed.43 The relation of timing of transfusion tohe incidence of acute rejection would also be inter-sting to evaluate; however, our small sample sizeoes not allow such an analysis to be performed.inally, our end points were freedom from rejectionnd overall survival. We did not evaluate the effect ofejection episodes on allograft function or report onvidence of cardiac allograft vasculopathy. The shortollow-up period in this study makes it difficult toccurately report on the latter. However, given theignificant impact of acute rejection on subsequentevelopment of chronic rejection, it will be interest-
ng to observe the incidence of chronic allograftasculopathy in this cohort of patients as the studyatures.In conclusion, an association exists between the
umber of blood transfusions and freedom fromardiac allograft rejection. The mechanism for thisffect remains unclear and deserves further study inrospective trials. The cardiac transplant populationppears to be the perfect cohort in which to performuch studies.
his work was supported by a research fellowship from the
nternational Society for Heart and Lung Transplantation (to
GF). We thank Dr Richard Schuessler for statistical analysis of
he data.
EFERENCES
1. Opelz G, Sengar DP, Mickey MR, Terasaki PI. Effect ofblood transfusions on subsequent kidney transplants.Transplant Proc 1973;5:253–9.
2. Flye MW, Burton K, Mohanakumar T, et al. Donor-specifictransfusions have long-term beneficial effects for humanrenal allografts. Transplantation 1995;60:1395–401.
3. Opelz G, Vanrenterghem Y, Kirste G, et al. Prospectiveevaluation of pretransplant blood transfusions in cadaverkidney recipients. Transplantation 1997;63:964–7.
4. Cicciarelli J. UNOS Registry data: effect of transfusions.
Figure 4. Freedom from rejection related to number of transfusions.
Clin Transpl 1990;407–16.

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
S260 Fernández et al. The Journal of Heart and Lung TransplantationJuly (Suppl) 2005
5. Katz MR, Barnhart GR, Goldman MH, et al. Pretransplanttransfusions in cardiac allograft recipients. Transplanta-tion 1987;43:499–501.
6. Persijn GG, van Hooff JP, Kalff MW, Lansbergen Q, vanRood JJ. Effect of blood transfusions and HLA matching onrenal transplantation in the Netherlands. Transplant Proc1977;9:503–5.
7. Persijn GG, Cohen B, Lansbergen Q, van Rood JJ. Retro-spective and prospective studies on the effect of bloodtransfusions in renal transplantation in The Netherlands.Transplantation 1979;28:396–401.
8. van der Mast BJ, Balk AH. Effect of HLA-DR-shared bloodtransfusion on the clinical outcome of heart transplanta-tion. Transplantation 1997;63:1514–9.
9. Vaessen LM, van Miert PP, van der Mast BJ, et al.Immunologic monitoring of the beneficial effect of oneHLA-DR-shared blood transfusion in heart transplant pa-tients. J Heart Lung Transplant 2000;19:1098–107.
0. Lagaaij EL, Hennemann IP, Ruigrok M, et al. Effect ofone-HLA-DR-antigen-matched and completely HLA-DR-mismatched blood transfusions on survival of heart andkidney allografts. N Engl J Med 1989;321:701–5.
1. Oz MC, Argenziano M, Catanese KA, et al. Bridge experi-ence with long-term implantable left ventricular assistdevices: are they an alternative to transplantation? Circu-lation 1997;95:1844–52.
2. Frazier OH, Macris MP, Myers TJ, et al. Improved survivalafter extended bridge to cardiac transplantation. AnnThorac Surg 1994;57:1416–22; discussion 1421–2.
3. McCarthy PM, Portner PM, Tobler HG, Starnes VA, Ra-masamy N, Oyer PE. Clinical experience with the Nova-cor ventricular assist system. Bridge to transplantationand the transition to permanent application. J ThoracCardiovasc Surg 1991;102:578–86; discussion 586–7.
4. Billingham ME, Cary NR, Hammond ME, et al. A workingformulation for the standardization of nomenclature inthe diagnosis of heart and lung rejection: Heart RejectionStudy Group. The International Society for Heart Trans-plantation. J Heart Transplant 1990;9:587–93.
5. van Es AA, Balner H. Effect of pretransplant transfusionson kidney allograft survival. Transplant Proc 1979;11:127–37.
6. Terasaki PI. The beneficial transfusion effect on kidneygraft survival attributed to clonal deletion. Transplanta-tion 1984;37:119–25.
7. Singal DP, Ludwin D, Blajchman MA. Blood transfusion andrenal transplantation. Br J Haematol 1985;61:595–602.
8. Martin DC, Hewitt CW, Osborne JG, et al. Enhancedkidney graft survival in rats by single or multiple bloodtransfusion(s) and various blood products. TransplantProc 1982;14:407–9.
9. van Es AA, Marquet RL, van Rood JJ, Kalff MW, Balner H.Blood-transfusions induce prolonged kidney allograft sur-vival in rhesus monkeys. Lancet 1977;1(8010):506–9.
0. Abouna GM, Barabas AZ, Pazderka V, et al. Effect ofpretreatment with multiple blood transfusions and withskin grafts on the survival of renal allografts in mongreldogs. Transplant Proc 1977;9:265–8.
1. Obertop H, Bijnen AB, Vriesendorp HM, Westbroek DL.
Prolongation of renal allograft survival in DLA tissue-typedbeagles after third-party blood transfusions andimmunosuppressive treatment. Transplantation 1978;26:255–9.
2. Opelz G, Terasaki PI. Improvement of kidney-graft sur-vival with increased numbers of blood transfusions.N Engl J Med 1978;299:799–803.
3. Hadley GA, Anderson CB, Mohanakumar T. Selective lossof functional antidonor cytolytic T cell precursors follow-ing donor-specific blood transfusions in long-term renalallograft recipients. Transplantation 1992;54:333–7.
4. Mincheff MS, Meryman HT, Kapoor V, Alsop P, Wotzel M.Blood transfusion and immunomodulation: a possiblemechanism. Vox Sang 1993;65:18–24.
5. Burlingham WJ, Grailer AP, Fechner JH Jr , et al. Micro-chimerism linked to cytotoxic T lymphocyte functionalunresponsiveness (clonal anergy) in a tolerant renal trans-plant recipient. Transplantation 1995;59:1147–55.
6. Puppo F, Ghio M, Contini P, Mazzei C, Indiveri F. Fas, Fasligand, and transfusion immunomodulation. Transfusion2001;41:416–8.
7. Dzik S, Mincheff M, Puppo F. Apoptosis, transforminggrowth factor-beta, and the immunosuppressive effect oftransfusion. Transfusion 2002;42:1221–3.
8. Van Rood JJ, Claas FH. The influence of allogeneic cellson the human T and B cell repertoire. Science 1990;248:1388–93.
9. Roelen DL, van Bree S, van Hulst P, van Beelen E, ClaasFH. Regulatory functions of human CD4(�) T cells rec-ognizing allopeptides in the context of self-HLA class II.Hum Immunol 2002;63:902–11.
0. Poindexter NJ, Smith MA, Haynes AE, Mohanakumar T.Regulatory function of human CD4� cytolytic T lympho-cytes. Transpl Immunol 1999;7:45–9.
1. Moazami N, Itescu S, Williams MR, Argenziano M, Wein-berg A, Oz MC. Platelet transfusions are associated withthe development of anti–major histocompatibility com-plex class I antibodies in patients with left ventricularassist support. J Heart Lung Transplant 1998;17:876–80.
2. Massad MG, Cook DJ, Schmitt SK, et al. Factors influenc-ing HLA sensitization in implantable LVAD recipients.Ann Thorac Surg 1997;64:1120–5.
3. Itescu S, Tung TC, Burke E, et al. Preformed IgG antibod-ies against major histocompatability complex class IIantigens are major risk factors for high-grade cellularrejection in recipients of heart transplantation. Circula-tion 1998;98:786–93.
4. Stringham JC, Bull DA, Fuller TC, et al. Avoidance ofcellular blood product transfusions in LVAD recipientsdoes not prevent HLA allosensitization. J Heart LungTransplant 1999;18:160–5.
5. Itescu S, John R. Interactions between the recipientimmune system and the left ventricular assist devicesurface: immunological and clinical implications. AnnThorac Surg 2003;75(6 Suppl):S58–65.
6. Kobashigawa JA, Sabad A, Drinkwater D, et al. Pretrans-plant panel reactive–antibody screens. Are they truly amarker for poor outcome after cardiac transplantation?Circulation 1996;94(9 Suppl):II294–7.
7. Pagani FD, Dyke DB, Wright S, Cody R, Aaronson KD.
Development of anti–major histocompatibility complex
3
3
4
4
4
4
The Journal of Heart and Lung Transplantation Fernández et al. S261Volume 24, Number 7S
class I or II antibodies following left ventricular assist deviceimplantation: effects on subsequent allograft rejection andsurvival. J Heart Lung Transplant 2001;20:646–53.
8. Haisa M, Sakagami K, Matsumoto T, et al. Donor-specifictransfusion (DST) with intermittent administration ofazathioprine induces suppressor T cells and MLR-inhibit-ing factors without sensitization. Transplant Proc 1989;21(1 Pt 2):1814–7.
9. Cheigh JS, Suthanthiran M, Fotino M, et al. Minimalsensitization and excellent renal allograft outcome follow-ing donor-specific blood transfusion with a short courseof cyclosporine. Transplantation 1991;51:378–81.
0. Massad MG, McCarthy PM, Smedira NG, et al. Doessuccessful bridging with the implantable left ventricular
assist device affect cardiac transplantation outcome?J Thorac Cardiovasc Surg 1996;112:1275–81; discussion1282–3.
1. John R, Rajasinghe H, Chen JM, et al. Impact of currentmanagement practices on early and late death in morethan 500 consecutive cardiac transplant recipients. AnnSurg 2000;232:302–11.
2. Vitali E, Lanfranconi M, Bruschi G, Russo C, Colombo T,Ribera E. Left ventricular assist devices as bridge to hearttransplantation: The Niguarda Experience. J Card Surg2003;18:107–13.
3. Michaels PJ, Espejo ML, Kobashigawa J, et al. Humoralrejection in cardiac transplantation: risk factors, hemody-namic consequences and relationship to transplant coro-nary artery disease. J Heart Lung Transplant 2003;22:58–
69.Copyright © 2022 FDOKUMEN




















