
Implantable functional neuromuscular stimulation in the tetraplegic hand
Upload
independentCategory
view
0download
0
GENERAL ARTICLES
Duration of Vecuronium-Induced Neuromuscular Block as a Predictor of Liver Allograft Dysfunction Cara L. Lukin, MD, H. A. Tillmann Hein, MD, Thomas H. Swygert, MD,
Thomas C. Gunning III, MD, Timothy R. Valek, MD, Steven K. Donica, MD,
Ross B. Nelson III, MD, and Michael A. E. Ramsay, MD
Departments of Anesthesiology and Pain Management, Baylor University Medical Center, and University of Texas Southwestern Medical Center, Dallas, Texas
The major causes of liver graft failure are acute rejec- tion, technical failure, and primary nonfunction (PNF). This study was undertaken to determine whether de- layed return of neuromuscular function correlates with allograft primary dysfunction in humans given vecuro- nium. Twenty-two adult patients undergoing ortho- topic liver transplantation were given an initial dose of vecuronium, 0.1 mg/kg intravenously (IV). All patients recovered from vecuronium-induced neuromuscular block prior to explantation. No additional neuromuscu- lar blocker was given until the liver graft was implanted and reperfused. Fifteen minutes after reperfusion an- other 0.1 mg/kg vecuronium was given IV and recov- ery time from attaining complete neuromuscular block to return of the fourth twitch of a train-of-four was re- corded. Patients were divided into three groups accord- ing to postoperative liver function. Group I consisted of 17 patients with immediate normal liver graft function. Group II consisted of four patients with primary dys- function (PDF) [peak aspartate aminotransferase CAST)
and alanine aminotransferase (ALT) >2000 U/L, pro- thrombin time >16 s, and poor quality and quantity of bile within 3 days postoperatively] which eventually recovered normal function. Group III consisted of one patient with PNF (uncorrectable coagulopathy, severe metabolic acidosis, rising AST and ALT, and minimal or no bile output), whose graft never recovered. Recov- ery time in Groups II and III was prolonged compared to Group I (P < 0.05). Recovery time in Group III was prolonged compared to Group II (P < 0.05). A test based on these results using a recovery time of >135 min as a predictor of PDF has a sensitivity and specific- ity of 80% and 76%, respectively. The positive and neg- ative predictive values are 50% and 93%. Duration of neuromuscular block after vecuronium administration appears to be an early predictor of liver allograft func- tion.
(Anesth Analg 1995;80:526-33)
A llograft failure remains a significant cause of morbidity and mortality and has led to re- transplantation in lo%-20% of all liver trans-
plants performed (1). The major causes of graft failure are acute rejection, technical failure, and primary non- function (PNF); PNF occurs in 2%-23% of transplants and is the most severe form of the spectrum of post- transplant primary dysfunction (PDF) (2). PNF is irre- versible and retransplantation is the only treatment. Prostaglandin E, @‘GE,) is efficacious in reversing the course of lesser degrees of PDF (3). The most rapid possible diagnosis of PDF will enable early interven- tion with PGE, and possible graft salvage.
Accepted for publication October 4, 1994. Address correspondence and reprint requests to Michael A. E.
Ramsay, MD, Department of Anesthesiology and Pain Manage- ment, Baylor University Medical Center, 3500 Gaston Avenue, Dal- las, TX 75246.
526 An&h Analg 1995;80:526-33
Investigators have evaluated many different mark- ers for PDF, but none is ideal. Some are nonspecific for liver function and others are cumbersome, expensive, or slow in turn-around time (4). Moreover, none of these tests can definitively distinguish a graft with irreversible dysfunction (PNF) from one that has re- versible initial poor function.
Vecuronium, a monoquaternary steroidal neuro- muscular blocking drug, is sequestered in, and me- tabolized predominantly by, the liver (5). The return of neuromuscular function is monitored with the use of a peripheral nerve stimulator which is efficient, quick, and inexpensive. Prolonged vecuronium block thus may be an early indicator of PDF. Pittet et al. (6) have demonstrated -in pigs that prolonged vecuro- nium neuromuscular block may be an early indicator of graft dysfunction. This study was undertaken to determine whether delayed return of neuromuscular function after vecuronium-induced neuromuscular
01995 by the International Anesthesia Research Society 0003-2999/95/$5.00
ANESTH ANALG 1995;80:526-33
LUKIN ET AL. 527 VECURONIUM PREDICTOR OF LIVER FUNCTION
block in the early neohepatic period correlates with allograft PDF in humans.
Methods After obtaining institutional approval and informed consent, 22 patients underwent orthotopic liver trans- plantation. Two patients were undergoing retrans- plantation; the first patient because of hepatic artery thrombosis, and the second because of cholestatic fail- ure of the initial graft.
Anesthesia was induced in a rapid sequence man- ner with thiopental (3-4 mg/kg intravenously [IV] and either fentanyl (3-4 pg/kg IV) or sufentanil(O.2- 0.3 pg/kg IV>. Skeletal muscle relaxation for endotra- cheal intubation was accomplished by administration of succinylcholine (1.3-1.5 mg/kg IV). Positive pres- sure ventilation was initiated with 50% oxygen in air, tidal volume lo-12 mL/kg, and respiratory rate of 6-12 breaths/min. Anesthesia was maintained with isoflurane (0.3-0.8 end-tidal vol %) and supplements of either fentanyl or sufentanil titrated to maintain hemodynamic stability.
The depth of neuromuscular block was monitored by stimulating the facial nerve with a MiniStim MS-II peripheral nerve stimulator (Life-Tech, Inc., Houston, TX) via cutaneous electrodes. The facial nerve was chosen as it was easily accessible, whereas access to the ulnar nerve was impeded by other patient care instrumentation. The train-of-four mode was applied, wherein supramaximal stimuli were delivered at a frequency of 2 Hz for 2 s to yield one group of four stimulus pulses. The number of resulting contractions of the orbicularis oculi muscle was visually counted by two observers.
After ascertaining the return of four baseline twitches after succinylcholine administration, vecuro- nium (0.1 mg/kg) was given IV. This dose was chosen because it is already part of the clinical routine and one of the aims of the study was to stay as closely as possible within the bounds of clinical practice. This initial administration of vecuronium occurred before commencement of the surgical procedure. The train- of-four was monitored to assure that all patients had the ability to recover from vecuronium-induced neu- romuscular block prior to explantation of their dis- eased liver. In a subset of patients, when there were O/4 twitches on the train-of-four, the time was re- corded. The response to the train-of-four was then monitored every 5 min until three twitches recovered; thereafter, it was observed every 2 min until four of four twitches were attained. The time of recovery of four twitches was recorded (in minutes), and there- fore, the time of baseline return of neuromuscular function was known. After the return of four twitches no additional neuromuscular blocker was given until
the donor liver was implanted and reperfused. It was again confirmed that all four twitches on the train-of- four returned to baseline before administration of the second, neohepatic dose of vecuronium, which oc- curred 15 min after reperfusion. The depth of neuro- muscular block was again monitored as described above, and the time (in minutes) for return of four twitches after the neohepatic dose of vecuronium was recorded. All donor livers were preserved in Univer- sity of Wisconsin solution and veno-venous bypass was used in all procedures.
Body temperature was monitored via the tempera- ture thermistor of an indwelling pulmonary artery catheter and was maintained with the use of a warm- ing blanket, forced-air warming device, warmed IV fluids, and warmed inspiratory gases. End-tidal isoflurane concentration was monitored with contin- uous mass spectrometry. The average end-tidal con- centration during the operation was recorded.
Except for one patient, all received amphotericin B and either imipenem or vancomycin and ciprofloxacin preoperatively. One patient received gentamicin, met- ronidazole, and ceftazidime in addition to amphoter- icin and vancomycin preoperatively.
The effect of temperature on return of neuromuscu- lar function was evaluated using measurements doc- umented on the continuous temperature record. Im- mediately upon arrival to the intensive care unit, and at regular intervals thereafter, serum creatinine and serum aspartate aminotransferase (AST), and serum alanine aminotransferase (ALT) were measured. For the purpose of this study, initial serum creatinine val- ues and peak serum transaminases were recorded. Peak transaminases were the highest AST and ALT values within three postoperative days.
The postoperative course was observed closely, and the patients were divided into three groups according to outcome. Group I consisted of patients who had immediate normal liver graft function as defined by peak postoperative AST and ALT ~2000 U/L, normal quality and quantity of bile production, and lack of coagulopathy. Groups II and III represented all pa- tients with abnormal postoperative liver function. Group II consisted of patients with initially poor func- tioning grafts, defined as AST and ALT >2000 U/L and prothrombin time >16 see within the first 3 days posttransplant (7). Group III consisted of patients with primary nonfunctioning grafts; PNF was defined as non-life-sustaining liver graft function, manifested by uncorrectable coagulopathy, metabolic acidosis, rising AST and ALT, and minimal or no bile output.
For statistical analysis, Student’s t-test and the Wil- coxon rank sum test were used for comparisons be- tween groups. The Wilcoxon test was applied when there was a small sample size in one group. Spear- man’s correlation was used to evaluate the association
528 LUKIN ET AL. ANESTH ANALG VECURONIUM PREDICTOR OF LIVER FUNCTION 1995;80:526-33
Table 1. Etiology of Liver Failure in Patients Undergoing Orthotopic Liver Transplantation (n = 22)
Number Percent
Chronic active hepatitis (C) 9 41 Cryptogenic cirrhosis 4 18 Primary biliary cirrhosis 3 14 Sclerosing cholangitis 2 9 Failure of initial graft 2 9 Laennec’s cirrhosis 1 4.5 Autoimmune hepatitis 1 4.5
between duration of neuromuscular block and peak AST and ALT. It was also used to determine the impact of weight, temperature, renal function, end- tidal isoflurane concentration, and exposure time to isoflurane on the duration of the neuromuscular block. Exposure time to isoflurane was calculated by divid- ing the average end-tidal isoflurane concentration by 1.15, the minimal alveolar anesthetic concentration, and then multiplying by the time from induction to the neohepatic return of the train-of-four. A P value <Cl.05 was considered statistically significant. An anal- ysis of sensitivity and specificity of recovery time as an indicator of allograft function was performed.
Results
Twenty-two patients, 9 women and 13 men, aged 21-68 yr, none suffering from neuromuscular disor- ders, were included in this study. The etiologies of their end-stage liver disease are displayed in Table 1.
All 22 patients had experienced the return of the train-of-four prior to veno-venous bypass and explan- tation of the liver. In 17 patients the time of the return of the train-of-four was recorded. The paleohepatic phase recovery time of the train-of-four in patients who later proved to have received a normally func- tioning liver transplant was not significantly different from that in patients who later had primary graft dysfunction (Table 2).
Recovery time from neuromuscular block was re- corded in 22 patients in the neohepatic phase. Of these, 17 had normal postoperative liver function and five did not. Of the five with PDF, four patients met the criteria for Group II (initial poor function) and one met the criteria for Group III (PNF). All patients in Group II eventually developed adequate liver func- tion, two of them after having received PGE,. The patient in Group III required explantation of the first graft within 24 h. Retransplantation was performed within 36 h with a non-cross-matched liver; this sec- ond organ functioned well for 2 days but then under- went severe acute rejection. A third liver was im- planted; this organ functioned well, but the patient eventually died of sepsis.
The 17 patients in Group I with normal postopera- tive liver function had a significantly shorter recovery time on the train-of-four (113.5 + 8.7 min) as com- pared to the five patients with PDF in Groups II and III (165.4 t 26.9 min, P < 0.05). A comparison between patients with normal postoperative liver function (Group I) and those without (Groups II and III) is shown in Table 2.
In most patients recovery from vecuronium- induced block required more time in the neohepatic phase than prior to explantation of the diseased liver. The mean time difference was not significantly differ- ent in regard to graft function classification. Two pa- tients in Group I had shorter recovery times in the neohepatic phase than prior to explantation. Both of these patients were in fulminant hepatic failure.
A comparison between the patient with PNF and all others is shown in Table 3. This patient had a signifi- cantly prolonged recovery time as compared to all others (267 min for Group III, 117.2 ? 7.9 min for Groups I and II; P < 0.05). When the second, initially functioning graft was implanted into this same pa- tient, the time for return of four twitches was shorter, being 125 min.
A strong correlation was found between peak AST and ALT and time of return of four twitches, as shown in Tables 2 and 3. The Spearman correlation coefficient was 0.62 (P < 0.05) for AST; for ALT it was 0.70 (P < 0.05). There was a negative correlation between the average end-tidal concentration of isoflurane and re- covery time of the train-of-four, the Spearman corre- lation coefficient being -0.49 (P < 0.05). In the group comparison, however, no difference between Groups I and II/III in regard to isoflurane concentration could be detected (Table 4).
There was no correlation between the return of the train-of-four in the neohepatic period and weight, se- rum creatinin, body temperature, exposure time to isoflurane, or age (Tables 4 and 5).
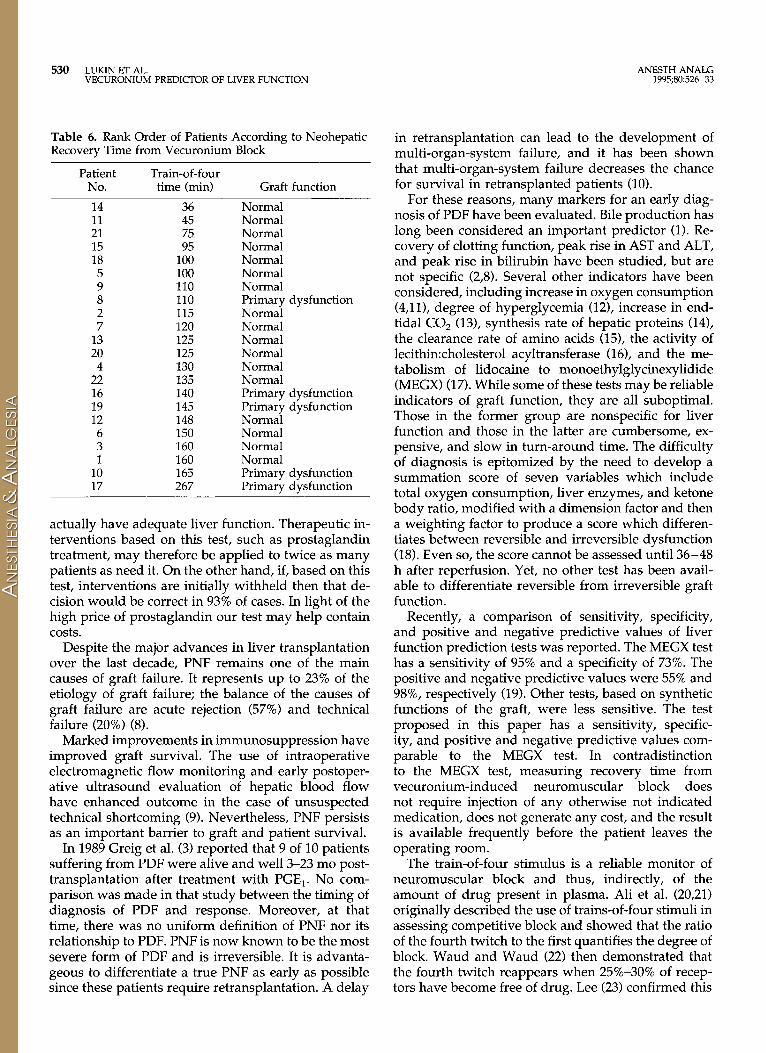
To assess sensitivity and specificity of a test to pre- dict liver graft function based on these results, we grouped patients in the order of increasing neohepatic train-of-four time (Table 6).
Using a neohepatic train-of-four time of ~135 min as an indicator of graft dysfunction, this test has a sensitivity of 80% and a specificity of 76%. The posi- tive predictive value is 50%, and the negative predic- tive value is 93% (Table 7).
Discussion
Our results suggest that recovery from vecuronium- induced neuromuscular block required more time af- ter reperfusion of a liver allograft than prior to the
ANESTH ANALG LUKIN ET AL. 529 1995;80:526-33 VECURONIUM PREDICTOR OF LIVER FUNCTION
Table 2. Comparison Between Patients with Normal Immediate Postoperative Allograft Function and Those with Primary Dysfunction
Normal function Primary dysfunction P value
Paleohepatic recovery time of TOF (min) 74.9 + 7.5 (n = 15) 60.0 t 19.9(n = 2) NS Neohepatic recovery time of TOF (min) 113.5 + 9.0 (n = 17) 165.4 ” 27.3 (n = 5) co.05 Difference between paleo- and neohepatic TOF times (mm) 37.0 c 11.9 (n = 15) 128.5 + 93.5 (n = 2) NS Peak aspartate aminotransferase (U/L) 835.5 2 130.3(n = 17) 5892.8 k 2161.3 (n = 5) CO.05 Peak alanine aminotransferase (U/L) 737.8 + 129.1(n = 17) 3648.2 + 477.2(n = 5) co.05 Peak prothrombin time (s) 17.7 t 0.5 (n = 17) 19.4 + 1.6 (n = 5) co.05
All data expressed as mean t sli. NS = not significant; TOF = train-of-four.
Table 3. Comparison Between Patients with Primary Nonfunction and all Others
Recovery time TOF (mm) Peak aspartate aminotransferase (U/L) Peak alanine aminotransferase (U/L) Peak prothrombin time (s)
All data expressed as mean -C SE. TOF = train-of-four. *Normal and initially poor graft function.
All others”
117.2 + 7.9 1426.2 + 274.5 1254.3 t 276.5
21.2 2 0.4
Primary nonfunction
267.0 14488.0 4442.0
25.2
P value
co.05 co.05 co.05 co.05
Table 4. Comparison Between Variables Affecting Vecuronium Metabolism in Patients with Normal Immediate Allograft Function Versus Primary Dysfunction
Variable P value
Serum creatinine (mg/dL) Average temperature (“C) Average end-tidal isoflurane concentration (vol %) Exposure time to isoflurane (MAC hours) Age (yr) Weight (kg)
All data presented as mean 2 SB. NS = not significant; MAC = minimum alveolar anesthetic concentration.
Normal
1.01
Primary function
+- 0.14
dysfunction
1.00 t 0.10 NS 34.27 + 0.24 34.61 + 0.32 NS 0.524 2 0.035 0.428 + 0.085 NS 2.737 2 0.126 2.992 + 0.364 NS
50.1 If: 0.5 55.6 + 4.9 NS 69.69 ? 3.86 71.52 + 7.83 NS
Table 5. Comparison Between Variables Affecting Vecuronium Metabolism in Patients with Primary Nonfunction Versus all Others
Variable All others Primary
nonfunction P value
Serum creatinine (mg/dL) 1.01 2 0.12 0.90 NS Average temperature (“C) 34.29 2 0.20 35.50 NS Average end-tidal isoflurane concentration (vol %) 0.518 + 0.031 0.175 NS Exposure time to isoflurane (MAC hours) 2.75 rt 0.75 1.28 NS Age (yr) 51.9 + 2.6 38.0 NS Weight (kg) 69.4 + 17.0 85.6 NS
All data expressed as mean IT SB. NS = not significant; MAC = minimum alveolar anesthetic concentration.
explantation of the native liver. This probably indi- cates temporary functional impairment of the trans- planted organ. In some patients, as in two of our series, the functional status of the allograft may be better than that of the failing native liver. In those patients recovery time from vecuronium was shorter.
Patients who later met established criteria for PDF
of the allograft proved to have significantly longer recovery times than patients with normal graft func- tion. This difference can be used as a test to predict graft function. This test has a positive predictive value of 50% and a negative predictive value of 93%. There- fore, obtaining a positive test would result in 50% correctly identified cases of PDF; the other 50% would
530 LUKIN ET AL. ANESTH ANALG VECURONIUM PREDICTOR OF LIVER FUNCTION 1995;80:526-33
Table 6. Rank Order of Patients According to Neohepatic Recovery Time from Vecuronium Block
Patient No.
Train-of-four time (min) Graft function
14 11 21 15 18 5 9 8 2 7
13 20
4 22 16 19 12
6 3 1
10 17
36 Normal 45 Normal 75 Normal 95 Normal
100 Normal 100 Normal 110 Normal 110 Primary dysfunction 115 Normal 120 Normal 125 Normal 125 Normal 130 Normal 135 Normal 140 Primary dysfunction 145 Primary dysfunction 148 Normal 150 Normal 160 Normal 160 Normal 165 Primary dysfunction 267 Primary dysfunction
actually have adequate liver function. Therapeutic in- terventions based on this test, such as prostaglandin treatment, may therefore be applied to twice as many patients as need it. On the other hand, if, based on this test, interventions are initially withheld then that de- cision would be correct in 93% of cases. In light of the high price of prostaglandin our test may help contain costs.
Despite the major advances in liver transplantation over the last decade, PNF remains one of the main causes of graft failure. It represents up to 23% of the etiology of graft failure; the balance of the causes of graft failure are acute rejection (57%) and technical failure (20%) (8).
Marked improvements in immunosuppression have improved graft survival. The use of intraoperative electromagnetic flow monitoring and early postoper- ative ultrasound evaluation of hepatic blood flow have enhanced outcome in the case of unsuspected technical shortcoming (9). Nevertheless, PNF persists as an important barrier to graft and patient survival.
In 1989 Greig et al. (3) reported that 9 of 10 patients suffering from PDF were alive and well 3-23 mo post- transplantation after treatment with PGE,. No com- parison was made in that study between the timing of diagnosis of PDF and response. Moreover, at that time, there was no uniform definition of PNF nor its relationship to PDF. PNF is now known to be the most severe form of PDF and is irreversible. It is advanta- geous to differentiate a true PNF as early as possible since these patients require retransplantation. A delay
in retransplantation can lead to the development of multi-organ-system failure, and it has been shown that multi-organ-system failure decreases the chance for survival in retransplanted patients (10).
For these reasons, many markers for an early diag- nosis of PDF have been evaluated. Bile production has long been considered an important predictor (1). Re- covery of clotting function, peak rise in AST and ALT, and peak rise in bilirubin have been studied, but are not specific (2,8). Several other indicators have been considered, including increase in oxygen consumption (4,111, degree of hyperglycemia (121, increase in end- tidal CO2 (13), synthesis rate of hepatic proteins (14), the clearance rate of amino acids (151, the activity of 1ecithin:cholesterol acyltransferase (16), and the me- tabolism of lidocaine to monoethylglycinexylidide (MEGX) (17). While some of these tests may be reliable indicators of graft function, they are all suboptimal. Those in the former group are nonspecific for liver function and those in the latter are cumbersome, ex- pensive, and slow in turn-around time. The difficulty of diagnosis is epitomized by the need to develop a summation score of seven variables which include total oxygen consumption, liver enzymes, and ketone body ratio, modified with a dimension factor and then a weighting factor to produce a score which differen- tiates between reversible and irreversible dysfunction (18). Even so, the score cannot be assessed until 36-48 h after reperfusion. Yet, no other test has been avail- able to differentiate reversible from irreversible graft function.
Recently, a comparison of sensitivity, specificity, and positive and negative predictive values of liver function prediction tests was reported. The MEGX test has a sensitivity of 95% and a specificity of 73%. The positive and negative predictive values were 55% and 98%, respectively (19). Other tests, based on synthetic functions of the graft, were less sensitive. The test proposed in this paper has a sensitivity, specific- ity, and positive and negative predictive values com- parable to the MEGX test. In contradistinction to the MEGX test, measuring recovery time from vecuronium-induced neuromuscular block does not require injection of any otherwise not indicated medication, does not generate any cost, and the result is available frequently before the patient leaves the operating room.
The train-of-four stimulus is a reliable monitor of neuromuscular block and thus, indirectly, of the amount of drug present in plasma. Ali et al. (20,21) originally described the use of trains-of-four stimuli in assessing competitive block and showed that the ratio of the fourth twitch to the first quantifies the degree of block. Waud and Waud (22) then demonstrated that the fourth twitch reappears when 25%30% of recep- tors have become free of drug. Lee (23) confirmed this

ANESTH ANALG LUKIN ET AL. 531 1995;80:526-33 VECURONIUM PREDICTOR OF LIVER FUNCTION
Table 7. Sensitivity, Specificity, Positive Predictive Value, and Negative Predictive Value of the Vecuronium Recovery Test for Liver Graft Function
Definition Calculation
Sensitivity True positive true positive + false negative
Specificity
Positive predictive value
Negative predictive value
True negative false positive + true negative
True positive true positve + false positive
True negative false negative + true negative
finding and showed that the visual reappearance of the fourth twitch (determined by visually counting the number of responses to train-of-four stimulation) ac- curately corresponds to this degree of block. He showed that the train-of-four count method is as ac- curate as measuring fade and virtually free from in- strumental errors.
In this study, the train-of-four count was used as described above. The return of the fourth twitch was used to represent the state when 25%-30% of receptors were free of drug. Vecuronium effect, as measured by twitch, is closely related to plasma drug concentration (24). Hepatic sequestration and clearance are the main routes of disappearance of vecuronium from plasma, thus linking hepatic function to return of the fourth twitch.
Vecuronium bromide is a monoquaternary neuro- muscular blocking drug originally derived from pan- curonium (25). Because its disposition is determined mainly by the liver and its pharmacokinetics have been shown by most investigators to be unchanged in patients with renal disease, it is a suitable drug with which to monitor liver function (5,26). Bencini et al. (5) have shown that greater than 50% of an IV dose of vecuronium is present in the human liver 30 min after injection and that both unchanged drug and its me- tabolites are excreted in bile. In a rat model they found that 70% of a dose of vecuronium administered into the portal circulation was excreted in the bile within 2 h and 22% remained in the liver; of the drug excreted in bile almost 50% was present as the 3-hydroxy me- tabolite (27). Lynam et al. (281, on the other hand, found with isoflurane anesthesia a prolongation of vecuronium effect in patients without renal function when compared to patients with normal renal func- tion. The clinical duration of the vecuronium effect varies quite widely among patients. It is possible that this variation in duration is responsible for the false- positive test results, thereby lowering the specificity of the test.
Intraoperatively assessing the return of neuromus- cular function after vecuronium block by monitoring the train-of-four appears to be a good method of pre- dicting primary graft dysfunction. Our data demon- strate a statistically significant prolongation of recov- ery time in patients with PDF. This diagnosis enables early commencement of treatment with PGE,.
As vecuronium appears to be sequestered in the liver before it is metabolized, it follows that either impaired hepatic uptake or impaired hepatic metabo- lism (or both) may be responsible for the defect in drug clearance in PDF grafts (29).
Our data are controlled for renal function. There was no significant association between renal function as measured by serum creatinine and time of return of the fourth twitch. Obesity may prolong vecuronium effect (30). We saw no correlation between weight and recovery time from vecuronium in our patients. There was also no impact by temperature or age on recovery of the train-of-four. There was an association between end-tidal isoflurane concentration and time of fourth twitch return. However, the relationship is opposite to the one expected if isoflurane concentration had con- tributed to duration of block; as volatile anesthetics are known to enhance neuromuscular block, a higher isoflurane concentration should have led to a longer time of block. An opposite effect was seen in this study, leading to the deduction that longer block times were probably not caused by isoflurane enhancement. It may, however, be possible that patients with better functioning liver grafts needed higher concentrations of volatile anesthetic, because their new livers dis- posed of the narcotics more rapidly. There also was no correlation with the duration of isoflurane exposure. Antibiotics may influence the duration of vecuronium effect (31). All patients received amphotericin B which is not known to have an effect on block. Antibiotics used in our study patients that are known to prolong

532 LUKIN ET AL. VECURONIUM PREDICTOR OF LIVER FUNCTION
ANESTH ANALG 1995;80:526-33
neuromuscular block include gentamicin and metron- idazol. Only one patient received these drugs, and he demonstrated a relatively short recovery time (100 min).
There has been a recent report of prolonged vecu- ronium paralysis due to the active 3-desacetyl metab- olite after long-term administration of the drug (32), however, this mechanism does not appear to be re- sponsible for the prolonged neuromuscular block in the PDF patients in our study. The patients in that report received large total doses of vecuronium over a prolonged period of time (337 mg over 6 days for the first patient and 83 mg over 2 days for the second). They both had severely impaired renal function (cre- atinine clearance of 5.0 mL/min for the first patient and 3.6 mL/min for the second). The prolonged pa- ralysis was thought to be due to the active 3-desacetyl metabolite, which is not only excreted in the urine, but also sequestered in a theoretic storage compartment which then equilibrates slowly with the central com- partment (plasma). Increased vecuronium require- ment during periods of heavy blood loss has also recently been reported (33). In our study one patient with PDF received 10 units of packed red blood cells during the postreperfusion stage. It may well be that the prolonged recovery time in this patient was fore- shortened. In the other patients red cell replacement as an indicator of blood loss was small, apparently unrelated to graft function or recovery time from vecuronium-induced block. In our study, no patient with prolonged block had severe renal impairment and no patient received large enough doses of vecu- ronium over a long enough period of time to be likely to develop sequestration of 3-desacetylvecuronium into a separate storage compartment. Finally, the pa- tient with PNF who received a second graft allowed a direct comparison to be made between the presence and absence of renal failure and its impact on duration of neuromuscular block. Despite receiving a higher cumulative dose of drug and having worse renal func- tion during the second transplant (serum creatinine was 2.6 mg/dL vs 0.9 mg/dL after the first trans- plant), it took a markedly shorter time to recover neuromuscular function (125 min vs 267 min during the first transplant).
Fortunately, only one of our patients met the criteria for PNF. We realize that a group of one weakens the statistical analysis. However, the clinical importance of a diagnosis of PNF, and the fact that the recovery time in this patient was so much longer than in the other patients with PDF, prompted us to speculate that this test may enable an early diagnosis of irrevers- ible PNF. We believe this merits further study. An earlier diagnosis of PNF may reduce delay in retrans- plantation, which is known to lead to the development
of multi-organ-system failure, decreasing the chance of survival in retransplanted patients. It is also of interest that when this patient underwent retransplan- tation with the second liver, a comparison was al- lowed wherein other variables affecting vecuronium metabolism and neuromuscular block were isolated, and the effect of liver function on duration of block was evaluated. The recovery time with the second liver graft was 125 min, as opposed to 267 min with the first liver graft. Other variables remained constant, except for the renal function: the serum creatinine had increased to 2.6 mg/dL during the second transplant from 0.9 mg/dL at the time of the first transplant. This decrease in renal function would have tended to pro- long the recovery time if it had been an important variable. As the recovery time was impressively shorter in the same patient after the second liver trans- plant, it appears that renal function did not have an important role in the duration of the block and that the effect of liver function alone on block duration was observed. This second liver graft functioned well for 2 days, although it underwent severe, acute rejection (biopsy proven) after that time.
In conclusion, the duration of neuromuscular block after vecuronium administration in the neohepatic phase appears to be a good predictor of graft dysfunc- tion. This test is expedient, efficient, and inexpensive. In addition, further experience may confirm that this method distinguishes irreversible PNF from reversible initial poor function.
References 1. Starzl TE, Demetris AJ, Van Thiel D. Liver transplantation (first
of two parts). N Engl J Med 1989;321:1014-22. 2. Ploeg RJ, D’Alessandro AM, Knechtle SJ, et al. Malfunction of
the liver after transplantation: an analysis of potential risk fac- tors. Transplant Proc 1993;25(1):1659-61.
3. Greig I’D, Woolf GM, Sinclair SB, et al. Treatment of primary liver graft nonfunction with prostaglandin E,. Transplantation 1989;48:447-53.
4. Steltzer H, Hiesmayr M, Tiichy G, Zimpfer M. Perioperative liver graft function: the role of oxygen transport and utilization. Anesth Analg 1993;76:574-9.
5. Bencini AF, Scaf AH, Sohn YJ, et al. Hepatobiliary disposition of vecuronium bromide in man. Br J Anaesth 1986;58:988-95.
6. Pittet JF, Morel DR, Mentha G, et al. Vecuronium neuromuscu- lar block reflects liver function during hepatic autotransplanta- tion in pigs. Anesthesiology 1994;81:168-75.
7. Ploeg RJ, D’Alessandro AM, Knechtle SJ, et al. Risk factors for primary dysfunction after liver transplantation-a multivariate analysis. Transplantation 1993;55:807-13.
8. Shaw BW Jr, Gordon RD, Iwatsuki S, Starzl TE. Hepatic retrans- plantation. Transplant Proc 1985;17:26471.
9. Klintmalm GBG, Olson LM, Paulsen AW, et al. Hepatic arterial thrombosis after liver transplantation: intraoperative electro- magnetic flow evaluation. Transplant Proc 1988;2O(S1):616-8.
10. Kamath GS, Plevak DJ, Wiesner RH, et al. Primary nonfunction of the liver graft: When should we retransplant? Transplant Proc 1991;23:1954.
ANESTH ANALG LUKIN ET AL. 533 1995;80:526-33 VECURONIUM PREDICTOR OF LIVER FUNCTION
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
Avolio AW, Agnes S, Pelosi G, et al. Intraoperative trends of oxygen consumption and blood lactate as predictors of primary dysfunction after liver transplantation. Transplant Proc 1991;23: 22635. Mallett SV, Kang Y, Freeman JA, et al. Prognostic significance of reperfusion hyperglycemia during liver transplantation. Anesth Analg 1989;68:182-5. Neidecker J, Fame JL, Champetier I’, et al. Does end-tidal CO, pressure reflect hepatic metabolism during orthotopic live; transplantation? Transplant Proc 1989;21:2239-40. Nakagohri T, Asano T, Goto T, et al. Use of hepatic protein synthesis rate in acute ischemic liver to assess degrees of ischemic iniurv. Transolant Proc 1989;21:2292-3. Goto T, Asano’T, Mori$ T, et al. Experimental studies of hepatic clearance rates of amino acids as an initial function test of the liver graft. Transplant Proc 1989;21:2305-7. Shimada M, Yanaga K, Makowka L, et al. Significance of lecithin: cholesterol acyltransferase activity as a prognostic in- dicator of early allograft function in clinical liver transplanta- tion. Transplantation 1989;48:600-03. Schroeder TJ, Gremse DA, Mansour ME, et al. Lidocaine me- tabolism as an index of liver function in hepatic transplant donors and recipients. Transplant Proc 1989;21:2299-2301. Gubernatis G, Bornscheuer A, Taki Y, et al. Total oxygen con- sumption, ketone body ratio and a special score as early indi- cators of irreversible liver allograft dysfunction. Transplant Proc 1989;21:2279-81. Freys G, Pain L, Calon B, et al. Early predictors of transplanted liver function. Anesthesiology 1993;79:A326. Ali HH, Utting JE, Gray TC. Quantitative assessment of residual antidepolarizing block (part I). Br J Anaesth 1971;43:473-7. Ali HH, Utting JE, Gray TC. Quantitative assessment of residual antidepolarizing block (part II). Br J Anaesth 1971;43:478-85. Waud BE, Waud DR. The relation between the response to “train-of-four” stimulation and receptor occlusion during com- petitive neuromuscular block. Anesthesiology 1972;37:413-6.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
Lee CM. Train-of-4 quantitation of competitive neuromuscular block. Anesth Analg 1975;54:649-53. Sohn YJ, Bencini AF, Scaf AHJ, et al. Comparative pharmacoki- netics and dynamics of vecuronium and pancuronium in anes- thetized patients. Anesth Analg 1986;65:233-9. Savage DS, Sleigh T, Carlyle I. The emergence of ORG NC 45, 1-[(2beta, 3alpha, Eialpha, 16beta, 17beta)-3, 17-bis(acetyloxy)-2- (l-piperidinyl)-androstan-16-YLJ-methylpiperidium bromide, from the pancuronium series. Br J Anaesth 1980;52:3%7S. Fahey MR, Morris RB, Miller RD, et al. Pharmacokinetics of ORG NC 45 (Norcuron) in patients with and without renal failure. Br J Anaesth 1981;53:1049-53. Bencini AF, Mol WEM, Scaf AHJ, et al. Uptake and excretion of vecuronium bromide and pancuronium bromide in the isolated perfused rat liver. Anesthesiology 1988;69:487-92. Lynam DP, Cronnelly R, Castagnoli KI-‘, et al. The pharmaco- dynamics and pharmacokinetics kinetics of vecuronium in pa- tients anesthetized with isoflurane with normal renal function or with renal failure. Anesthesiology 1988;69:227-31. Hull CJ. I’harmacokinetics for anaesthesia. Oxford: Butter- worth-Heinemann Ltd, 1991:348. Weinstein JA, Matte0 RS, Ornstein E, et al. Pharmacodynamics of vecuronium and atracurium in the obese surgical patient. Anesth Analg 1988;67:1149-53. McIndewar IC, Marshall RJ. Interactions between the neuro- muscular blocking drug ORG NC 45 and some anaesthetics, analgesics and antimicrobial agents. Br J Anaesth 1981;53: 785-91. Segredo V, Matthay MA, Sharma ML, et al. Prolonged neuro- muscular block after long-term administration of vecuronium in two critically ill patients. Anesthesiology 1990;72:566-70. O’Hara DA, Hexem J, Derbyshire G, et al. Kinetics and dynam- ics of vecuronium using an automated controller for liver trans- plantation. Anesth Analg 1994;78:S323.
Copyright © 2022 FDOKUMEN




















