How Should Transection of the Liver Be Performed?
10
ORIGINAL ARTICLES How Should Transection of the Liver Be Performed? A Prospective Randomized Study in 100 Consecutive Patients: Comparing Four Different Transection Strategies Mickael Lesurtel, MD, Markus Selzner, MD, Henrik Petrowsky, MD, Lucas McCormack, MD, and Pierre-Alain Clavien, MD, PhD Objective: To identify the most efficient parenchyma transection technique for liver resection using a prospective randomized protocol. Summary Background Data: Liver resection can be performed by different transection devices with or without inflow occlusion (Prin- gle maneuver). Only limited data are currently available on the best transection technique. Methods: A randomized controlled trial was performed in noncir- rhotic and noncholestatic patients undergoing liver resection com- paring the clamp crushing technique with Pringle maneuver versus CUSA versus Hydrojet versus dissecting sealer without Pringle maneuver (25 patients each group). Primary endpoints were intra- operative blood loss, resection time, and postoperative liver injury. Secondary end points included the use of inflow occlusion, postop- erative complications, and costs. Results: The clamp crushing technique had the highest transection velocity (3.9 0.3 cm 2 /min) and lowest blood loss (1.5 0.3 mL/cm 2 ) compared with CUSA (2.3 0.2 cm 2 /min and 4 0.7 mL/cm 2 ), Hydrojet (2.4 0.3 cm 2 /min and 3.5 0.5 mL/cm 2 ), and dissecting sealer (2.5 0.3 cm 2 /min and 3.4 0.4 mL/cm 2 ) (velocity: P 0.001; blood loss: P 0.003). Clamp crushing technique was associated with the lowest need for postoperative blood transfusions. The degree of postoperative reperfusion injury and complications were not significantly different among the groups. The clamp crushing technique proved to be most cost-efficient device and had a cost-saving potential of 600 € to 2400 € per case. Conclusions: The clamp crushing technique was the most efficient device in terms of resection time, blood loss, and blood transfusion frequency compared with CUSA, Hydrojet, and dissecting sealer, and proved to be also the most cost-efficient device. (Ann Surg 2005;242: 814 – 823) L iver resection has been increasingly performed over the last 2 decades worldwide because of improved postoper- ative outcomes and evidence that this approach offers the only chance of cure in many patients. 1–4 Technical innova- tions have mainly focused on minimizing bleeding during transection of the hepatic parenchyma 5,6 because excessive hemorrhage and the need for blood transfusion are associated with increased postoperative morbidity and mortality, 7 as well as reduced long-term outcome. 7–9 Inflow occlusion (Pringle maneuver) has been used since the early 20th cen- tury 10 to prevent bleeding during parenchyma transec- tion. 11–14 The concomitant use of low central venous pressure (CVP) anesthesia further minimizes blood loss by preventing retrograde bleeding from the hepatic veins. 15,16 Assuming that inflow occlusion and low CVP anesthesia cause signifi- cant damages by ischemia and reperfusion, there has been a growing interest in using new devices that facilitate bloodless transection, obviating the need for inflow occlusion. The most popular devices facilitating bloodless tran- section include the ultrasonic dissector (CUSA, Tyco Health- care, Mansfield, MA) using ultrasonic energy, the Hydrojet (Hydro-Jet, Erbe, Tubingen, Germany) using a pressurized jet of water and the dissecting sealer (TissueLink, Dover, NH) using radiofrequency energy. Parenchymal transection under routine inflow occlusion has been performed with finger frac- ture technique (digitoclasy), 17 where liver parenchyma was crushed between the thumb and one finger isolating vessels and bile ducts, which can then be ligated and divided. This technique was subsequently improved through the use of surgical instru- ments such as small Kelly or Pe ´an clamps (clamp crushing) for blunt transection. 18 Some of these devices have gained wide acceptance for hepatectomy, although, to our knowledge, their efficacy has been tested in only 2 randomized controlled trials (RCTs) comparing clamp crushing technique versus CUSA 19 and CUSA versus Hydrojet, 20 using inflow occlusion in all cases. Both RCTs had critical limitations as Takayama et al 19 included normal and cirrhotic livers and the RCT by Rau et al 20 was not based on a sample size and power calculation. There is no RCT that compares the most commonly used devices to each other, such as the clamp crushing technique, CUSA, Hydrojet, and dissecting sealer. Further experience From the Department of Visceral and Transplant Surgery, University Hos- pital, Zurich, Switzerland. The current address of Dr. Lesurtel is Depart- ment of Digestive Surgery, St Antoine Hospital, Paris, France. Supported in an equivalent amount by Erbe (Tubingen, Germany), Tissuelink (Dover, NH), and Tyco Healthcare (Mansfield, MA). Dr. Selzner and Dr. Petrowsky are the recipients of the Novartis fellowship in HPB surgery and liver transplantation. Reprints: Pierre-Alain Clavien, MD, PhD, Department of Visceral and Trans- plant Surgery, University Hospital of Zurich, Ra ¨mistrasse 100, CH-8091 Zu ¨rich, Switzerland. E-mail: [email protected]. Copyright © 2005 by Lippincott Williams & Wilkins ISSN: 0003-4932/05/24206-0814 DOI: 10.1097/01.sla.0000189121.35617.d7 Annals of Surgery • Volume 242, Number 6, December 2005 814
Transcript of How Should Transection of the Liver Be Performed?

ORIGINAL ARTICLES
How Should Transection of the Liver Be Performed?A Prospective Randomized Study in 100 Consecutive Patients:
Comparing Four Different Transection Strategies
Mickael Lesurtel, MD, Markus Selzner, MD, Henrik Petrowsky, MD, Lucas McCormack, MD,and Pierre-Alain Clavien, MD, PhD
Objective: To identify the most efficient parenchyma transectiontechnique for liver resection using a prospective randomized protocol.Summary Background Data: Liver resection can be performed bydifferent transection devices with or without inflow occlusion (Prin-gle maneuver). Only limited data are currently available on the besttransection technique.Methods: A randomized controlled trial was performed in noncir-rhotic and noncholestatic patients undergoing liver resection com-paring the clamp crushing technique with Pringle maneuver versusCUSA versus Hydrojet versus dissecting sealer without Pringlemaneuver (25 patients each group). Primary endpoints were intra-operative blood loss, resection time, and postoperative liver injury.Secondary end points included the use of inflow occlusion, postop-erative complications, and costs.Results: The clamp crushing technique had the highest transectionvelocity (3.9 � 0.3 cm2/min) and lowest blood loss (1.5 � 0.3mL/cm2) compared with CUSA (2.3 � 0.2 cm2/min and 4 � 0.7mL/cm2), Hydrojet (2.4 � 0.3 cm2/min and 3.5 � 0.5 mL/cm2), anddissecting sealer (2.5 � 0.3 cm2/min and 3.4 � 0.4 mL/cm2)(velocity: P � 0.001; blood loss: P � 0.003). Clamp crushingtechnique was associated with the lowest need for postoperativeblood transfusions. The degree of postoperative reperfusion injuryand complications were not significantly different among the groups.The clamp crushing technique proved to be most cost-efficientdevice and had a cost-saving potential of 600 € to 2400 € per case.Conclusions: The clamp crushing technique was the most efficientdevice in terms of resection time, blood loss, and blood transfusionfrequency compared with CUSA, Hydrojet, and dissecting sealer,and proved to be also the most cost-efficient device.
(Ann Surg 2005;242: 814–823)
Liver resection has been increasingly performed over thelast 2 decades worldwide because of improved postoper-
ative outcomes and evidence that this approach offers theonly chance of cure in many patients.1–4 Technical innova-tions have mainly focused on minimizing bleeding duringtransection of the hepatic parenchyma5,6 because excessivehemorrhage and the need for blood transfusion are associatedwith increased postoperative morbidity and mortality,7 aswell as reduced long-term outcome.7–9 Inflow occlusion(Pringle maneuver) has been used since the early 20th cen-tury10 to prevent bleeding during parenchyma transec-tion.11–14 The concomitant use of low central venous pressure(CVP) anesthesia further minimizes blood loss by preventingretrograde bleeding from the hepatic veins.15,16 Assumingthat inflow occlusion and low CVP anesthesia cause signifi-cant damages by ischemia and reperfusion, there has been agrowing interest in using new devices that facilitate bloodlesstransection, obviating the need for inflow occlusion.
The most popular devices facilitating bloodless tran-section include the ultrasonic dissector (CUSA, Tyco Health-care, Mansfield, MA) using ultrasonic energy, the Hydrojet(Hydro-Jet, Erbe, Tubingen, Germany) using a pressurized jetof water and the dissecting sealer (TissueLink, Dover, NH)using radiofrequency energy. Parenchymal transection underroutine inflow occlusion has been performed with finger frac-ture technique (digitoclasy),17 where liver parenchyma wascrushed between the thumb and one finger isolating vessels andbile ducts, which can then be ligated and divided. This techniquewas subsequently improved through the use of surgical instru-ments such as small Kelly or Pean clamps (clamp crushing) forblunt transection.18
Some of these devices have gained wide acceptance forhepatectomy, although, to our knowledge, their efficacy hasbeen tested in only 2 randomized controlled trials (RCTs)comparing clamp crushing technique versus CUSA19 andCUSA versus Hydrojet,20 using inflow occlusion in all cases.Both RCTs had critical limitations as Takayama et al19
included normal and cirrhotic livers and the RCT by Rau etal20 was not based on a sample size and power calculation.There is no RCT that compares the most commonly useddevices to each other, such as the clamp crushing technique,CUSA, Hydrojet, and dissecting sealer. Further experience
From the Department of Visceral and Transplant Surgery, University Hos-pital, Zurich, Switzerland. The current address of Dr. Lesurtel is Depart-ment of Digestive Surgery, St Antoine Hospital, Paris, France.
Supported in an equivalent amount by Erbe (Tubingen, Germany), Tissuelink(Dover, NH), and Tyco Healthcare (Mansfield, MA). Dr. Selzner and Dr.Petrowsky are the recipients of the Novartis fellowship in HPB surgeryand liver transplantation.
Reprints: Pierre-Alain Clavien, MD, PhD, Department of Visceral and Trans-plant Surgery, University Hospital of Zurich, Ramistrasse 100, CH-8091Zurich, Switzerland. E-mail: [email protected].
Copyright © 2005 by Lippincott Williams & WilkinsISSN: 0003-4932/05/24206-0814DOI: 10.1097/01.sla.0000189121.35617.d7
Annals of Surgery • Volume 242, Number 6, December 2005814

with transection devices has only been reported by lowerevidence retrospective studies.21–30
It is surprising that often expensive devices are introducedin routine surgical practice without proper proof of their efficacyor superiority over simpler techniques. Especially, the economicpressure on health care costs scrutinizes the appropriateness ofexpensive transection devices if simpler techniques with com-parable efficacy profile are available.
Therefore, in the lack of available convincing data, wedesigned an RCT in noncirrhotic and noncholestatic patientsundergoing liver resection comparing 4 different techniquesof parenchyma transection, including clamp crushing tech-nique under inflow occlusion, CUSA, Hydrojet, and dissect-ing sealer. Inflow occlusion was used in the 3 latter groupsonly when needed (see experimental design). Endpoints, suchas intraoperative blood loss, transection time, degree of reper-fusion injury (as assessed by postoperative transaminase andbilirubin levels), and postoperative complications, were de-termined to identify the most efficient device for liver paren-chyma transection in terms of safety and costs.
MATERIALS AND METHODS
Experimental DesignBetween June 2003 and September 2004, 100 consec-
utive patients were randomized to undergo liver resection,with 1 of 4 different parenchyma transection strategies. Liv-ing donors for liver transplantation were not included in thestudy. The transection strategies included: 1) the clampcrushing technique under routine inflow occlusion (Pringlemaneuver) and 3 other frequently used techniques withoutroutine Pringle maneuver; 2) ultrasonic dissector (CUSAExcel, Tyco Healthcare); 3) Hydrojet (Helix Hydro-Jet,Erbe); and 4) DS3.0 dissecting sealer (TissueLink). Eachpatient was operated by the same hepatobiliary surgeon(P.-A.C.), and more than 30 patients were operated with eachtransection device prior to the initiation of the study. Eligi-bility criteria included partial hepatectomy (�2 segments) forbenign and malignant tumors, and acceptable clotting profile(platelet count �100 � 109/L and prothrombin activity�60%). Cirrhotic and cholestatic (serum bilirubin �100�mol/L) patients were excluded from the study.
Surgical ProcedureThe procedure was approved by the ethic committee of
the University of Zurich, and an informed consent wasobtained from each patient prior to surgery. Each patient wasrandomized the night prior to surgery using sealed envelopes(25 for each technique). The reason to randomize the daybefore relies on the need for the nursing staff to prepare thematerial when CUSA and Hydrojet were selected. The sur-gical team was, however, informed of the allocation only inthe operating room. When liver resection could not be per-formed, the envelope was sealed again and returned in thepool of sealed envelopes. Major hepatectomy was defined asa liver resection �3 segments. All resections were performedwith the requirement of a low CVP (0–5 mm Hg). Eachpatient underwent an intraoperative ultrasound (US) to definethe tumor localization in relation to the major vascular and
biliary structures. Anatomic hemi-hepatectomy was per-formed in a standardized manner with a selective devascu-larization of the resected specimen as previously described.31
A stapler device was only used for the transection of thehepatic veins. The 4 different transection techniques aredefined below:
Clamp Crushing TechniqueA continuous Pringle maneuver was routinely used
with the clamp crushing technique. The tourniquet techniquearound the portal triad with a 4-mm mersilene tape was usedto achieve inflow occlusion. Liver transection was performedby parenchyma crushing using a small Kelly clamp (3-mm-diameter tip). Small vessels (�2 mm) were coagulated withthe irrigated bipolar forceps set at 120 Watts. All otherstructures including major intrahepatic bile ducts were ligatedor clipped.
Ultrasonic DissectorAn ultrasonic dissector (Cavitron Ultrasonic Surgical
Aspirator, CUSA) (23 kHz standard tip, cauter 70 Watt, flush4 mL/min, sensitivity 100%) was used for parenchyma tran-section. Inflow occlusion was performed only in the presenceof significant bleeding preventing selective coagulation orligation of small structures or when blood loss exceeded 500mL. The use of bipolar forceps, ligatures, and clips wasidentical to the clamp crushing technique.
HydrojetThe soft liver tissue was washed off the more resistant
vessels and bile ducts by a jet of water, which was pressur-ized by a high pressure pump and conducted by a highpressure hose to the nozzle (Helix Hydro-Jet) (30–40 barwater pressure). The use of the Pringle maneuver, bipolarforceps, ligatures, and clips were similar to the CUSA tech-nique.
Dissecting SealerThis device (TissueLink) couples radiofrequency with a
conductive fluid to seal liver tissue to precoagulate paren-chyma and isolate small and larger intrahepatic structure. Theuse of the Pringle maneuver, ligatures, and clips were similarto the CUSA and Hydrojet techniques. In the liver hilus and5 mm around biliary structures, we avoided the use of dissectingsealer because of the risk of biliary leaks.
Neither intermittent clamping nor ischemic precondi-tioning was applied in any technique. Prophylactic postoper-ative drainage was only used when a bilioenteric anastomosiswas performed.
Outcome MeasuresEach patient was followed for 3 months. The primary
endpoints were blood loss during parenchyma transection,resection time, and postoperative hepatocyte injury. The de-gree of postoperative hepatic injury was assessed by dailymeasurements of postoperative AST and ALT levels, biliru-bin levels, and prothrombin times until hospital discharge.Resection time was defined as the duration between thebeginning and the end of parenchyma transection. Another
Annals of Surgery • Volume 242, Number 6, December 2005 Strategies for Liver Transection
© 2005 Lippincott Williams & Wilkins 815

time was recorded until complete satisfaction with the hemo-stasis. Blood loss was carefully monitored until the beginningof the parenchyma transection, during transection, and afterhepatectomy. The amount of blood loss was estimated byincluding the suction volume after subtraction of rinse fluidsand weighting the swabs that were used during transection(assuming that 1 mL of blood � 1 g). As soon as liverresection was completed, the cut surface was put on a spongeand the area of liver transection surface was drawn on a sheetof paper. The paper area was cut and weight to calculate areasurface according to the paper density (80 mg/m2). The datafor blood loss were standardized to the transection areaexpressed as cm2. The speed of transection was calculated astransection area divided by transection time (cm2/min).
Secondary endpoints included the duration of inflowocclusion, the degree of liver damage by serial postoperativebilirubin and prothrombin levels, the need of blood transfu-sion, and morbidity and mortality according to a new classi-fication of complications by severity,32 with an additionalemphasis on bile leaks, hospital stay, and cost. The indica-tions for blood transfusion were a massive hemorrhage(�1500 mL) during surgery or a hemoglobin level �7 g/dLwithin 24 hours following surgery. Each negative or adverseintraoperative and postoperative event was recorded. Anabdominal US was performed at postoperative day 5 and aCT scan at 3 months to assess fluid collections.
Cost AnalysisWe performed a comprehensive actual cost analysis
focusing on the cost of liver resection since the study did notshow significant differences in postoperative complications,ICU, and hospital stay among the groups (see below). Thecost of each case was estimated considering 4 items: the costsof the device (ie, clamp crushing technique, CUSA, Hydrojet,and dissecting sealer), costs of the operating room time, costsof additional methods to control bleeding, and costs of trans-fused red blood cell units. The cost of each device wascalculated on the basis of capital charge, maintenance ofmaterial, and disposal material. Capital charge per case wasbased on capital equipment with a 5-year depreciation. Sincecosts of capital equipment and maintenance depend on thenumber of cases performed per year, we provided a costanalysis on a basis of 3 different scenarios according to thecenter volume of 10, 50, or 100 liver resections performed peryear, respectively. The price of the operating room was 466€
per hour, excluding physicians’ fees. Physician fees are calcu-lated on the basis of the type of operation, not the duration, andare therefore equivalent among the groups. Each clip staplerdevice contained 20 clips per stapler (Ligaclip MCM 20Medium clips, Ethicon Endo-Surgery, Cincinnati, OH) andpurchased for 113€ per device. The price of a red blood cellunit was 127€. The costs of operating room time, clip sta-plers, and red blood cell transfusion were provided by ouraccounting department and reflect actual costs for the year2004. Costs are expressed in Euros (€) (�1.3 U.S.$).
Statistical AnalysisThe analysis was performed in “an intention-to-treat”
manner. Summary statistics are expressed as mean � SEM or
median (range), as appropriate. According to previous pub-lished data19,20 and previous experience with each device, thesample size calculation was performed with the expectationof a 30% difference in blood loss or resection time duringparenchyma transection in at least 1 group with a level ofstatistical significance of 0.05 and a power of 0.80, using aposthoc 2-sample t test with a Bonferroni correction. We alsocalculate a sample size to detect a 100 IU/L difference in theopening (6 hours after surgery) or peak AST levels with a SDof 100 IU/L. These calculations included 25 patients in eachgroup. Comparisons between groups were performed byusing the ANOVA test followed by the post hoc Bonferronitest when needed. For qualitative variables, comparisonsbetween groups were performed by the �2 test followed bythe posthoc 2 � 2 Fisher exact test, when needed. All thecalculations were performed with the SPSS 12.0 statisticalpackage (SPSS, Inc., Chicago, IL).
RESULTS
Was the Randomization Process Adequate andWere the 4 Groups Comparable?
A total of 110 consecutive patients were considered forthis study. Four patients refused to sign the consent form; andin 6 cases, liver resection was not performed because ofextrahepatic disease or unresectable tumor found at the timeof laparoscopy or laparotomy. No patient was excludedthereafter. Of the 100 randomized patients (25 each group),53 were men and 47 were women, with a mean age of 56 �1 years. The mean area of liver resection was 117 � 10 cm2.Prior to liver resection, chemotherapy was applied within 2months of surgery in 38 (38%) of patients. Sixty-one patients(61%) underwent a major (�3 segments) hepatectomy, ofwhom 34 had an anatomic right (SV–VIII) hemi-hepatec-tomy, 16 had a left (SI–IV) hemi-hepatectomy, 5 hadextended right hemi-hepatectomy (SIV–VIII), 5 had anextended left liver resection (SI–IV), and 1 had a centralhepatectomy (SIV, SV, SVIII). Thirty-three patients un-derwent a bi-segmentectomy, including 9 patients withanatomic SII–III bisegmentectomy. Six patients underwentan atypical wedge resection of ranging about 20% and 30%of the liver mass. Patient age, gender, the surface of liverresection, the use of chemotherapy prior resection, and thetype of hepatectomy were comparable among the groups(Table 1).
Thirty-three patients were operated for liver metastasesfrom a colorectal carcinoma, 13 for cholangiocarcinoma, 8for hepatocellular carcinoma, 7 for gallbladder carcinoma,and 20 for various kinds of metastatic diseases. In 19 patients,liver resection was performed for benign diseases, such asliver adenoma, focal nodular hyperplasia, echinococcosiscyst, or hemangioma. The different diagnoses were distrib-uted homogeneously among the 4 groups.
Are Transection Time, Blood Loss, and Needfor Blood Transfusion Influenced by theResection Technique?
The overall mean transection time was 46 � 4 minutes(median, 42 minutes; range, 14–128 minutes). The mean
Lesurtel et al Annals of Surgery • Volume 242, Number 6, December 2005
© 2005 Lippincott Williams & Wilkins816

transection speed was 2.8 � 1.6 cm2/min. The clamp crush-ing technique was associated with a significantly faster tran-section speed (about twice) than any of the 3 other techniques(P � 0.001) (Table 2). The overall mean blood loss was 326 �52 mL (median, 300 mL; range, 10–1200 mL). The bloodloss per resection surface was significantly lower for theclamp crushing technique than for the 3 other resectiondevices (about 2-fold lower; P � 0.003). Twenty-two patients(22%) received blood transfusion during or within 24 hoursfollowing surgery. There was an about 5-fold less require-ment for blood transfusion in the clamp crushing group,although this did not reached significance (P � 0.06). Clips,sutures, or ligatures were used during parenchyma transectionas additional methods to avoid hemorrhage and bile leaks. Asshown in Table 2, the cumulative number of clips, sutures,and ligatures used per area of liver resection surface was notsignificantly different among groups (P � 0.53). The hemo-stasis time from the end of transection until completion ofhemostasis was not different among the groups.
Does the Resection Technique Impact on theUse of Inflow Occlusion (Pringle Maneuver)and Postoperative Liver Injury?
The data are summarized in Table 3. The Pringlemaneuver was applied in each patient receiving the clampcrushing technique according to the study protocol, while itwas applied in only 5 patients (20%), 7 patients (28%), and 9patients (36%) in the CUSA, Hydrojet, and dissecting sealer
groups, respectively (P � 0.001 clamp crushing versus othertechniques). In patients in whom Pringle was applied, theoverall mean Pringle time was 28 � 2 minutes (median, 28minutes; range, 10–60 minutes). Evaluating only patientswith the Pringle maneuver in the last 3 groups, the ischemictime was about half of the resection time.
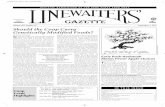
The peak of the transaminases occurred between 6hours after surgery and the third postoperative day in eachcase. In most patients, AST and ALT levels returned tonormal values within 7 days. There was no significant differ-ence among the 4 groups. Postoperative peak values of ASTand ALT are presented in Figure 1. Similarly, there was nosignificant difference among the groups regarding the post-operative prothrombin time (70% � 4%, 71% � 4%, 68% �4%, and 71% � 13% for clamp crushing technique, CUSA,Hydrojet, and dissecting sealer, respectively, P � 0.69).Similarly, no differences were found in bilirubin levels (43 � 7,38 � 7, 56 � 8, and 43 � 7 �mol/L for clamp crushingtechnique, CUSA, Hydrojet, and dissecting sealer, respec-tively, P � 0.12).
Do the Respective Techniques Impact onPostoperative Complications, ICU, andHospital Stay?
Four patients died within 30 days following majorhepatectomy. Two of these patients were operated for chol-angiocarcinoma and the 2 others for gallbladder carcinoma.Postoperative deaths were due in 1 case to mesenteric arterial
TABLE 1. Patient Demographics and Surgical Characteristics
ClampCrushing CUSA Hydrojet
DissectingSealer P
No. of patients 25 25 25 25 —
Gender (F/M) 13/12 12/13 9/16 13/12 0.63
Age (yr) 54 � 3 59 � 2 61 � 2 52 � 2 0.60
Area of liver resection (cm2) 124 � 11 109 � 10 125 � 9 110 � 9 0.56
Major hepatectomy* (%) 64 52 76 52 0.25
Benign/malignant tumors (%) 16/84 16/84 16/84 38/72 0.62
Use of Roux-en-Y bilio-digestive anastomosis 2 2 3 2 0.94
Anatomic hemi-hepatectomy right/left 11/2 7/4 10/6 6/4 0.63
Preoperative chemotherapy (%) 32 30 44 40 0.83
Continuous variables are expressed as mean � SEM.*Major hepatectomy was defined as �3 segments.
TABLE 2. Intraoperative Transection-Related Features
ClampCrushing(n � 25)
CUSA(n � 25)
Hydrojet(n � 25)
DissectingSealer
(n � 25) P
Mean transection speed (cm2/min) 3.9 � 0.3* 2.3 � 0.2 2.4 � 0.3 2.5 � 0.3 0.001
Mean blood loss (mL/cm2) 1.5 � 0.3* 4 � 0.7 3.5 � 0.5 3.4 � 0.4 0.003
No. of transfused patients 1 8 8 5 0.06
No. of clips, sutures, and ligatures/cm2 0.42 � 0.06 0.43 � 0.04 0.45 � 0.04 0.36 � 0.04 0.53
Hemostasis time† (min/cm2) 0.05 � 0.01 0.07 � 0.02 0.05 � 0.01 0.07 � 0.007 0.41
Continuous variables are expressed as mean � SEM; cm2 refers to the area of resection surface.*Significant versus all other techniques.†Time from the end of transection to completion of hemostasis divided by area of resection surface.
Annals of Surgery • Volume 242, Number 6, December 2005 Strategies for Liver Transection
© 2005 Lippincott Williams & Wilkins 817

infarction at the fifth postoperative day with an otherwisenormal course, and in 3 patients to sepsis and multiorgan-failure. Death occurred in these cases between the 10th and28th postoperative days. Two of the patients who died un-derwent liver resection with the CUSA, whereas the other 2patients were operated with the Hydrojet.
Asymptomatic intraperitoneal collections were as-sessed with an abdominal ultrasound at postoperative day 5and CT scan at 3 months. Only collections �3 cm were taken
into account. The overall rate of collections was 31% andwere documented in 8 (32%), 9 (36%), 6 (24%), and 8 (32%)patients in clamp crushing, CUSA, WaterJet, and dissectingsealer groups, respectively (P � 0.82). Additionally, percu-taneous drainage (symptomatic biloma) was necessary in 5patients, and 1 patient was reoperated for an infected biloma.
Complications were ranked according to our recentlyreported classification of surgical complications.32 The over-all complication rate was 32%, including the 4 deaths (grade5) (Table 4). There was no significant difference among the 4groups regarding postoperative minor (grade 1 and 2) ormajor (grade 3, 4, and 5) complications. The overall medianICU and hospital stay were 1 day (range, 0–26 days) and 9days (range, 4–34 days), respectively, and were not signifi-cantly different among the groups (Table 4).
Do the Respective Transection TechniquesInfluence Costs?
The cost of each device is given in Table 5 according tocapital equipment with a 5-year depreciation, costs of main-tenance, and costs of disposal material.
The mean price for a liver resection per case is given inTable 6. The clamp crushing technique was the least expen-sive device and appeared to provide significant cost savingsregardless of the volume of liver resections performed peryear. Inversely, CUSA was the most expensive technique, butits cost equaled the cost of the dissecting sealer for high-volume centers performing 100 liver resections per year.
DISCUSSIONThis is the first randomized controlled trial investigat-
ing the efficacy, safety, and cost-effectiveness of 4 differentparenchyma transection strategies in noncirrhotic and non-cholestatic patients undergoing liver resection. We found thatclamp crushing technique with routine inflow occlusion wassignificantly associated with decrease blood loss and shorterresection time when compared with transection with CUSA,Hydrojet, or dissecting sealer. The degree of postoperative(reperfusion) liver injury as measured by serial serum levelsof transaminases, bilirubin, or prothrombin times, as well asthe incidence and severity of complications were comparableamong all groups. Furthermore, the actual cost analysis of theuse of each respective device indicated that the clamp crush-
FIGURE 1. Peak AST and ALT levels (n � 25 in each group,P � 0.71 for AST and P � 0.80 for ALT).
TABLE 3. Use of Inflow Occlusion (Pringle Maneuver)
ClampCrushing(n � 25)
CUSA(n � 25)
Hydrojet(n � 25)
DissectingSealer
(n � 25) P
No. of patients with Pringle (%) 25 (100)* 5 (20) 7 (28) 9 (36) �0.001
Mean ischemic time† considering patients withPringle (min/cm2)
0.25 � 0.04 0.23 � 0.002 0.21 � 0.02 0.15 � 0.002 0.24
Percentage ratio of ischemic time referred tototal resection time in patients subjected toinflow occlusion (%)
100* 62 � 11 45 � 6 44 � 11 0.001
Continuous variables are expressed as mean � SEM.*Significant versus all other techniques.†Ischemic time is divided by the resection area.
Lesurtel et al Annals of Surgery • Volume 242, Number 6, December 2005
© 2005 Lippincott Williams & Wilkins818

ing technique is the most cost-efficient strategy regardless ofthe volume of liver resection performed.
The study protocol was designed with careful attentionto minimize potential bias. Each procedure was performed bythe same surgical team with a standardized resection tech-nique. Prior to the initiation of the study, at least 30 liverresections were performed with each transection device toexclude the negative effects of a potential learning curve. A
single anesthesia team experienced in liver resection, espe-cially in low CVP anesthesia, was involved in all cases,which enabled performance of each case under a CVP main-tained between 0 and 5 mm Hg. The use of the Pringlemaneuver and blood transfusion was standardized to preventindividual variations. It can also be argued that sponsoringfrom companies may potentially influence on the study pro-tocol. We accepted sponsorship from the 3 device companies
TABLE 4. Postoperative Complications, ICU, and Hospital Stay in the 4 Groups
ComplicationsClamp
Crushing CUSA HydrojetDissecting
Sealer P
Grade 1 Wound infection 1 0 0 6
Grade 2 Cardiac arrhythmia 0 2 1 0
Pneumonia 1 2 0 0
Urine infection 2 0 1 0
Total minor complications (grade 1 � 2) 4 4 2 6 0.51
Grade 3 Bilioma* 2 1 0 3
Intra-abdominal bleeding 0 0 1 0
Grade 4 Hepatic failure† 1 1 1 0
Pulmonary embolism 1 0 0 0
Renal failure‡ 0 0 1 0
Grade 5 Death 0 2 2 0
Total major complications (grade 3 � 4 � 5) 4 4 5 3 0.51
ICU stay (days) �median (range) 1 (0–4) 1 (0–9) 1 (0–26) 1 (0–8) 0.35
Hospital stay (days) �median (range) 9 (5–24) 9 (4–21) 9 (4–26) 9 (5–34) 0.67
Complications are expressed as no. of patients. Complications were briefly defined as follows32: grade 1, any deviation from the normalpostoperative course without the need of specific drugs treatment or intervention; grade 2, requiring specific pharmacologic treatment; grade 3,requiring surgical, endoscopic, or radiologic intervention; grade 4, life-threatening complications requiring ICU management; grade 5, death ofa patient due to a complication.
*Bilioma refers to the symptomatic biliary fluid collection requiring external drainage.†Hepatic failure: patients requiring ICU stay because of transitory hepatic dysfunction or encephalopathy.‡Renal failure: this patient required hemofiltration between postoperative day 3 and 7.
TABLE 5. Material-Related Cost of Each Device (Euro �€)
ClampCrushing (€) CUSA (€) Hydrojet (€)
DissectingSealer (€)
Equipment* cost per case (€)
10 cases/yr 0 1471 1233 0
50 cases/yr 0 294 246 0
100 cases/yr 0 146 123 0
Cost of disposal material per case (€) 0 661 191 980
*Equipment cost is based on capital charge with 5-yr depreciation and maintenance of material.
TABLE 6. Cost (Euro �€) of Liver Resection per Case According to the Transection Technique
Center Volume
Cost per Case (€)
ClampCrushing CUSA Hydrojet
DissectingSealer P
10 cases/yr 497 � 38* 2912 � 73* 2235 � 97* 1618 � 45* �0.001
50 cases/yr 497 � 38* 1735 � 73 1248 � 97* 1618 � 45 �0.001
100 cases/yr 497 � 38* 1587 � 73 1125 � 97* 1618 � 45 �0.001
Continuous variables are expressed as mean � SEM. The cost of liver resection was calculated on the basis of capital charge andmaintenance of material, disposal material, operating room time, additional methods to control bleeding, and the need for blood transfusion.In each column, SEM is constant because the difference among lines is based on cost of each device, which is a constant value in each patient.
*Significant versus all other techniques.
Annals of Surgery • Volume 242, Number 6, December 2005 Strategies for Liver Transection
© 2005 Lippincott Williams & Wilkins 819

(CUSA, Hydrojet, and dissecting sealer) at the same amount,and the study protocol was solely prepared by the authors.The surgeons were informed about the randomization onlyafter the decision to proceed with hepatectomy was madeintraoperatively. Finally, the analysis of the data indicatedexcellent matching in terms of patient demographics and typeof resection among the 4 groups (Table 1). The exclusion ofpatients with liver cirrhosis and cholestasis further securedhomogeneity among the groups.
However, the experimental design of such trial is in-herently associated with a few limitations. The study wasonly powered to evaluate blood loss, resection time, andreperfusion injury; thus, the sample size was not sufficient todetect differences in postoperative mortality and morbidity,as well as bile leak. To overcome the failure of detecting bileleak, we included routine US at the fifth postoperative dayand a CT scan at 3 months. The study did not look atlong-term outcome as data were collected only for 3 monthsafter surgery. While we failed to show significant differencesamong the groups in terms of ischemia and reperfusioninjury, ie, postoperative levels of serum liver transaminasesand bilirubin were comparable in patients subjected or not toinflow occlusion, other more subtle changes were not inves-tigated. For example, we did not look at hepatocyte apoptosis,area of necrosis, and activation of pathways of injury aspostoperative liver biopsy was not included in the studyprotocol due to safety reason.
The central finding in this study was the significantlylower blood loss in patients undergoing liver transection withthe clamp crushing technique under inflow occlusion com-pared with CUSA, Hydrojet, and dissecting sealer (Table 2).Although blood loss and the need of blood transfusion (mean,300 mL; only 22% of patients received blood transfusion)compared favorably to many other series,1,2,15 the clampcrushing technique resulted in about 3- to 5-fold lower bloodloss during hepatectomy and transfusion frequency than anyof the other techniques. Our interpretation for the favorableresults of the clamp crushing technique is that the associatedinflow occlusion and low CVP very efficiently preventedbleeding enabling optimal identification of all tiny intrahe-patic structures, which could be selectively coagulated, li-gated, or clipped. Hemorrhage after release of the inflowocclusion was also minimal and comparable to the othertechniques supporting the safety of the clamp crushing tech-nique. Although CUSA, Hydrojet, and dissecting sealer the-oretically divide liver parenchyma without vessel injury,bleedings from smaller vessels, particularly veins, do occurimpairing optimal visibility of the transection plane. Thefinding that inflow occlusion was needed in about 20% to36% of patients further supports the significance of hemor-rhage during transection (Table 3). Similar experience wasalso reported by others; for example Rau et al compared liverresections with CUSA and Hydrojet in an RCT.20 Althoughinflow occlusion was applied to all resections, the authorsreported a significant intraoperative blood loss of 1800 mLfor CUSA and 1500 mL for Hydrojet. Over the recent years,we, as many others, have learned to perform hemi-hepatectomyfor living donation with the Hydrojet or CUSA without inflow
occlusion and intraoperative blood loss of less than 500 mL.However, these procedures are performed exclusively in healthyand usually young patients with the ability to respect perfectanatomic plan as safety margins are not an issue.
We found a comparable degree of postoperative injury(transaminase and bilirubin levels, and prothrombin time) inpatients resected with the clamp crushing technique and inflowocclusion and those without inflow occlusion. The majority ofpatients (65%) had low AST levels (�400 U/mL) aftersurgery. This observation is likewise related to several fac-tors. First, the clamp crushing technique enabled a fastresection requiring inflow occlusion for less than 30 minutes inmost cases. We previously showed that ischemic time less than30 minutes is associated with minimal reperfusion injury.33
Second, patients with particularly sensitive livers to ischemicinjury, such as those with cirrhosis and cholestasis, were notincluded in the study. Third, the decreased blood loss in theclamp crushing technique group might result in improvedliver perfusion and therefore decreased reperfusion injury.Assuming that the current data (mean AST level of 400 IU/L,SD 350 IU/L) would be used to calculate a new sample size,we would need 250 patients per group to show a significantdifference between the clamp crushing technique and theother devices.
Postoperative mortality and morbidity were evaluatedusing a standardized classification system enabling to stratifycomplications by severity.32 The 4% mortality is in the rangeof previous reports1–3 and was related to the nonselectivity ofthe population studied including extensive liver resection (eg,for cholangiocarcinoma) and many patients at risk. Compli-cations were documented in 32% of patients, with an inci-dence of severe complications (grades 3–5) of 16% (Table 4).The rate of minor and major complications was not signifi-cantly different among the 4 groups. This observation corre-sponds to the findings of the 2 published RCTs, whichreported a similar overall complication profile between theuse of clamp crushing, CUSA, and Hydrojet.19,20 Bile leaksremain a challenging complication, occurring in 5% to 14%of patients undergoing hepatectomy.29,34,35 Symptomatic bileleaks requiring an intervention occurred in 6% of our patientswithout difference among the groups. Of note, our samplesize was not calculated to identify a difference in bile leaks orother complications. Since we do not use prophylactic drains,except in presence of hepato-jejunostomy, we performed anUS at the fifth postoperative day and a CT scan at 3 months.The incidence of asymptomatic fluid collection was compa-rable among the groups ranging from 24% to 36%. Therefore,our data suggest that each technique is suitable to performsafe liver resections with a similar complication profile and aminimal risk for bile leaks.
Another important finding was the significant fasterparenchyma transection with the clamp crushing techniquecompared with the other devices. Sakamoto et al reportedsimilar data in a retrospective analysis comparing the clampcrushing technique with the floating ball device, which rep-resents the first generation of the dissecting sealer.28 Incontrast, the RCT by Takayama et al revealed comparabletransection times in patients undergoing liver resection with
Lesurtel et al Annals of Surgery • Volume 242, Number 6, December 2005
© 2005 Lippincott Williams & Wilkins820

clamp crushing technique or CUSA.19 However, the studypopulation of this trial included patients with normal (48%)and chronic diseased (52%) livers, and all patients underwentroutine inflow occlusion, therefore not comparable with ourpopulation. The duration of surgery is an increasingly impor-tant cost factor, and the use of the operation room is chargedper minute in many countries. In addition, more proceduresper day could be possible with the shorter duration of surgeryin each case.
The forces of cost control on health care raise thequestion of how costs can be saved without reducing thequality of treatment. This issue has also special implicationfor the operation equipment in our study since costs ofpurchase, maintenance, and disposal material are largelydifferent for the 4 transection devices investigated. Therefore,a comparative cost analysis was included into the study toestimate the appropriateness of each device in terms of costsand efficacy. The clamp crushing technique proved to be themost cost-efficient device. The cost advantage of the clampcrushing technique is not only attributed to the very lowequipment costs but is also related to the shorter resectiontime, lower blood loss with less need for blood transfusion.The equipment costs of CUSA and Hydrojet depend stronglyon the number of cases per year since both devices require alarge initial purchase with lower costs for disposal material.Thus, the costs of these devices decrease by increasing thecase load. However, CUSA and Hydrojet were, respectively,3- to 6-fold and 2- to 4-fold more expensive compared withthe clamp crushing technique. In contrast, the dissectingsealer caused only costs of disposal material without the needto purchase a machine, but costs were also 3 times higherthan the clamp crushing technique. These data demonstratethat the clamp crushing technique has the highest cost-savings potential compared with the other devices. Even ifthe advantageous results of the clamp crushing techniquesuch as shorter resection time and lesser blood loss areignored, the cost of the equipment itself would still signifi-cantly favor the clamp crushing technique.
CONCLUSIONLiver resection with the clamp crushing technique was
associated with a shorter resection time, less blood loss, anda lower frequency of blood transfusion compared with CUSA,Hydrojet, and dissecting sealer. Furthermore, the clampcrushing technique proved to be the most cost-efficient devicewith the highest cost-saving potential among all 4 testeddevices. Based on these findings, we propose that the clampcrushing technique should be considered as standard tech-nique in noncirrhotic and noncholestatic patients undergoingelective liver resection. The role of CUSA, Hydrojet, anddissecting sealer in patients with diseased liver still needs tobe evaluated.
ACKNOWLEDGMENTSThe authors thank Tyco Healthcare (Mansfield, MA),
Erbe (Tubingen, Germany), and TissueLink (Dover, NH) fortheir sponsorship; as well as the anesthesiologist team for itsassistance in the management of the patients; the study
coordinators, especially Cornelia Ortlieb, for their excellentjob in collecting data; and Valentin Rousson for his assis-tance in the statistical analysis.
REFERENCES1. Belghiti J, Hiramatsu K, Benoist S, et al. Seven hundred forty-seven
hepatectomies in the 1990s: an update to evaluate the actual risk of liverresection. J Am Coll Surg. 2000;191:38–46.
2. Jarnagin WR, Gonen M, Fong Y, et al. Improvement in perioperativeoutcome after hepatic resection: analysis of 1,803 consecutive cases overthe past decade. Ann Surg. 2002;236:397–406; discussion 406–407.
3. Poon RT, Fan ST, Lo CM, et al. Improving perioperative outcomeexpands the role of hepatectomy in management of benign and malig-nant hepatobiliary diseases: analysis of 1222 consecutive patients froma prospective database. Ann Surg. 2004;240:698–708; discussion 708–710.
4. Clavien PA. Malignant Liver Tumor: Current and Emerging Therapies.Malden, MA: Blackwell Science, 1999.
5. Cunningham JD, Fong Y, Shriver C, et al. One hundred consecutivehepatic resections: blood loss, transfusion, and operative technique. ArchSurg. 1994;129:1050–1056.
6. Sitzmann JV, Greene PS. Perioperative predictors of morbidity follow-ing hepatic resection for neoplasm: a multivariate analysis of a singlesurgeon experience with 105 patients. Ann Surg. 1994;219:13–17.
7. Kooby DA, Stockman J, Ben-Porat L, et al. Influence of transfusions onperioperative and long-term outcome in patients following hepatic re-section for colorectal metastases. Ann Surg. 2003;237:860–869; discus-sion 869–870.
8. Yamamoto J, Kosuge T, Takayama T, et al. Perioperative blood trans-fusion promotes recurrence of hepatocellular carcinoma after hepatec-tomy. Surgery. 1994;115:303–309.
9. Tsao JI, Loftus JP, Nagorney DM, et al. Trends in morbidity andmortality of hepatic resection for malignancy: a matched comparativeanalysis. Ann Surg. 1994;220:199–205.
10. Pringle J. Notes on the arrest of hepatic hemorrhage due to trauma. AnnSurg. 1908;48:541.
11. Huguet C, Gavelli A, Chieco PA, et al. Liver ischemia for hepaticresection: where is the limit? Surgery. 1992;111:251–259.
12. Huguet C, Gavelli A, Bona S. Hepatic resection with ischemia of theliver exceeding one hour. J Am Coll Surg. 1994;178:454–458.
13. Kimura F, Miyazaki M, Suwa T, et al. Evaluation of total hepaticvascular exclusion and Pringle maneuver in liver resection. Hepatogas-troenterology. 2002;49:225–230.
14. Abdalla EK, Noun R, Belghiti J. Hepatic vascular occlusion: whichtechnique? Surg Clin North Am. 2004;84:563–585.
15. Melendez JA, Arslan V, Fischer ME, et al. Perioperative outcomes ofmajor hepatic resections under low central venous pressure anesthesia:blood loss, blood transfusion, and the risk of postoperative renal dys-function. J Am Coll Surg. 1998;187:620–625.
16. Bhattacharya S, Jackson DJ, Beard CI, et al. Central venous pressure and itseffects on blood loss during liver resection. Br J Surg. 1999;86:282–283.
17. Lin T, Tsu K, Mien C, et al. Study on lobectomy of the liver. J FormosaMed Assoc. 1958;57:742–759.
18. Lin TY. A simplified technique for hepatic resection: the crush method.Ann Surg. 1974;180:285–290.
19. Takayama T, Makuuchi M, Kubota K, et al. Randomized comparison ofultrasonic vs clamp transection of the liver. Arch Surg. 2001;136:922–928.
20. Rau HG, Wichmann MW, Schinkel S, et al. Surgical techniques inhepatic resections: ultrasonic aspirator versus Jet-Cutter. A prospectiverandomized clinical trial. Zentralbl Chir. 2001;126:586–590.
21. Papachristou DN, Barters R. Resection of the liver with a water jet.Br J Surg. 1982;69:93–94.
22. Schroder T, Hasselgren P, Brackett K. Techniques of liver resection:comparison of suction knife, ultrasonic dissector and contact neodymi-um-YAG laser. Arch Surg. 1987;122:1166–1171.
23. Rau HG, Schardey HM, Buttler E, et al. A comparison of differenttechniques for liver resection: blunt dissection, ultrasonic aspirator andjet-cutter. Eur J Surg Oncol. 1995;21:183–187.
24. Yamamoto Y, Ikai I, Kume M, et al. New simple technique for hepaticparenchymal resection using a Cavitron Ultrasonic Surgical Aspirator
Annals of Surgery • Volume 242, Number 6, December 2005 Strategies for Liver Transection
© 2005 Lippincott Williams & Wilkins 821

and bipolar cautery equipped with a channel for water dripping. WorldJ Surg. 1999;23:1032–1037.
25. Taniai N, Onda M, Tajiri T, et al. Hepatic parenchymal resection usingan ultrasonic surgical aspirator with electrosurgical coagulation. Hepa-togastroenterology. 2002;49:1649–1651.
26. Schmidbauer S, Hallfeldt KK, Sitzmann G, et al. Experience withultrasound scissors and blades (UltraCision) in open and laparoscopicliver resection. Ann Surg. 2002;235:27–30.
27. Weber JC, Navarra G, Jiao LR, et al. New technique for liver resectionusing heat coagulative necrosis. Ann Surg. 2002;236:560–563.
28. Sakamoto Y, Yamamoto J, Kokudo N, et al. Bloodless liver resectionusing the monopolar floating ball plus ligature diathermy: preliminaryresults of 16 liver resections. World J Surg. 2004;28:166–172.
29. Nakayama H, Masuda H, Shibata M, et al. Incidence of bile leakage afterthree types of hepatic parenchymal transection. Hepatogastroenterology.2003;50:1517–1520.
30. Poon RT, Fan ST, Wong J. Liver resection using a saline-linkedradiofrequency dissecting sealer for transection of the liver. J Am CollSurg. 2005;200:308–313.
31. Clavien PA, Selzner M, Rudiger HA, et al. A prospective randomizedstudy in 100 consecutive patients undergoing major liver resection withversus without ischemic preconditioning. Ann Surg. 2003;238:843–850;discussion 851–852.
32. Dindo D, Demartines N, Clavien PA. Classification of surgical compli-cations: a new proposal with evaluation in a cohort of 6336 patients andresults of a survey. Ann Surg. 2004;240:205–213.
33. Clavien PA, Yadav S, Sindram D, et al. Protective effects of ischemicpreconditioning for liver resection performed under inflow occlusion inhumans. Ann Surg. 2000;232:155–162.
34. Tanaka S, Hirohashi K, Tanaka H, et al. Incidence and management ofbile leakage after hepatic resection for malignant hepatic tumors. J AmColl Surg. 2002;195:484–489.
35. Nagano Y, Togo S, Tanaka K, et al. Risk factors and management of bileleakage after hepatic resection. World J Surg. 2003;27:695–698.
DiscussionsDR. BISMUTH: Face to the number of techniques of liver
transection, the search for the best one is very attractive. Thisjustifies the work of the Clavien’s group, well done, I mustsay, in terms of methodology. I have, however, some criti-cism on the choice of the techniques studied. As for themodality of clamping in the group of the clamp crushing, whydo you use the continuous clamping instead of the intermit-tent one, which appears now to be superior in terms oftolerance for the liver parenchyma? Indeed, in your paper,your maximum ischemic time was 47 minutes, but we mayneed longer transection time.
My main remark is in the application of the Pringlemaneuver: 100% in the clamp crushing group compared witharound 30% in the other groups. It seems to me that as theblood loss is one primary endpoint of your study, this grouphas evidently an advantage in the comparison. I would havelike to have the same use of portal clamping for all groups,which would have reinforce the value of the comparison.Paradoxically, if I follow your conclusion, the high technol-ogy tools may be overcome by a very simple tool as a clamp.Personally, I am pleased of this statement for it could be thatI was the first in the early 1980s to introduce this way of livertransection. At that time, the method for liver transection wasthe finger fracture (digitoclasy) introduced by the Chinese
surgeons. I found when I started using this technique that theoccidental fingers were too large and I preferred to use aclamp, the Kelly clamp (kellyclasy).
DR. CLAVIEN: Thank you, Professor Bismuth, for theinsightful comments and questions. The first question relatesto the method of inflow occlusion. Should we have usedintermittent rather than continuous inflow occlusion, as somestudies have suggested better tolerance against ischemia withthe intermittent inflow occlusion strategy? Of note, thesestudies have also shown significant bleeding during the suc-cessive reperfusion periods, which of course do not occurwith continuous inflow occlusion. As the Kelly clamp tech-nique enables a relatively quick resection, the clamping timenever exceeded 50 minutes in our study with a mean of 26minutes, we felt that the standard, still widely used, contin-uous inflow occlusion was preferable for the purpose of thisstudy. The data also convincingly show that this strategy issafe, as we failed to detect increased hepatic injury comparedwith the 3 other techniques, where inflow occlusion was usedonly when needed. Your question is also very timely. As afollow-up of this study, assuming now that the Kelly tech-nique with inflow occlusion is superior to the other strategies,we just initiated a trial testing intermittent clamping versusischemic preconditioning using the Kelly technique for majorliver resection. The second question relates to a possible biasin routinely using inflow occlusion only in the Kelly clampgroup, while inflow occlusion was an endpoint in the 3 othergroups. Here we need to go back to the study design and thequestion we wanted to address. We did not test a specificdevice but rather a strategy of liver resection. We and othershave used the Kelly clamp technique with routine inflowocclusion for many years. Over the past 2 decades, severalnovel and often quite expensive devices have been marketedwith the claim that they were safer and can be used withoutthe need of inflow occlusion. Thus, we tested this hypothesisand found that for each endpoint evaluated, including cost,the Kelly clamp strategy was superior. Whether the routineuse of inflow occlusion in each group would have stillfavored the Kelly clamp technique is not addressed by thisstudy. However, even if similar bleeding or duration ofresection would have been achieved, which I doubt, the Kellyclamp would still be the winner in terms of cost-effective-ness, particularly in low-volume centers, as shown in thepaper. Thanks, Professor Bismuth, for the historical insightinto the “kellyclasy” and, of course, for your many contribu-tions to liver surgery, which have paved the way for most of us.
DR. BELGHITI: I would like to congratulate the authorsbecause we need such studies. The surgical community needssuch data to be more flexible and, according to your results,it means that we can use any kind of transection with equaleffectiveness. This is a very important observation.
Lesurtel et al Annals of Surgery • Volume 242, Number 6, December 2005
© 2005 Lippincott Williams & Wilkins822

My first question would be that, although you are veryflexible in the transection technique, why so rigid in usingpedicle clamping during crush clamping alone and why not inother methods of transection?
The second point I would like to mention is that youshould be using the transected liver surface area of each group tocompare the results. What is your opinion regarding this?
Third, I am curious to have your interpretation on whythe postoperative transaminase levels are not significantlyelevated in the clamped group compared with others?
DR. CLAVIEN: Thank you, Prof. Belghiti, for the kindcomment and questions. The first question about why wewere not so flexible with the use of inflow occlusion relatesto the study design. We tested the hypothesis that the “so-called” novel bloodless liver resection techniques, ie, obviat-ing the need for routine inflow occlusion, are superior to the“classic” clamp crushing technique with inflow occlusion.Thus, we applied inflow occlusion in the 3 “bloodless”techniques only based on strict criteria. Of interest, periods ofinflow occlusion were needed in about a third of patients withthe “blood less” devices. Regarding your second question, weindeed standardized the data regarding resection time andblood loss to the calculated surface of resection. This isdescribed in detail in the methodology of the paper. Finally,your third question focuses on the lack of difference inpostoperative AST levels among the groups. We were alsosomewhat surprised with this finding, and I may suggestseveral explanations for this observation. First, clamping timewas less than 30 minutes in half of the patients, a timing thathas been previously shown to be associated with minimaldetectable injury in normal liver. Second, the putative injuryassociated with the routine use of inflow occlusion in theKelly group may have been counterbalanced by injury relatedto increased resection times and blood loss in the othergroups. Of note, based on the current data, we calculated thatwe would need 250 patients to show any differences inpostoperative AST levels.
DR. HEBERER: This is an excellent study with regard tothe design, the sample size calculation, and the randomiza-
tion. We sometimes have difficulties with patients to acceptthe randomization, particularly when a placebo arm is in-cluded. Therefore, my question is: what number of patientsaccepted and did not accept the randomization.
DR. CLAVIEN: Four patients refused to sign the studyprotocol, and in another 6 cases liver resection was notperformed due to extrahepatic disease or unresectable tumorat the time of surgery; thus, we considered 110 patients toinclude 100 patients.
DR. HOCKERSTEDT: I want to ask 3 short questions: werethe same surgeons doing these 100 resections? Since youhave 4 deaths here in patients with noncirrhotic livers, Iwould like to know if these patients had received adjuvanttherapy or anything else that could have predisposed them tosome degree of liver dysfunction. And the final question is: inthe next series of liver resection in patients if they are not ina randomized study, what technique would you use?
DR. CLAVIEN: Prof. Hockerstedt, thank you for thesequestions. To address your first question, I was involved ineach case in this study. Regarding the second point, a dismaloutcome occurred in 4 patients between 10 and 28 days aftersurgery, and these cases are presented in detail in the manu-script. These patients underwent an extended right hemi-hepatectomy for a cholangiocarcinoma in 2 patients and agallbladder cancer in 2 others. One died of a mesentericinfarction of unclear etiology in an otherwise uneventfulcourse, the 3 other patients from multiorgan failure. None hadreceived chemotherapy, and I believe it is fair to state, basedon the intraoperative data, that the dismal outcome was notrelated to the resection strategy. Of note, more than two thirdsof patients in this series underwent major surgeries, and thismortality rate compares favorably with other expert centers.Your final question is very important, and phrased differentlycould sound “do you believe your data?” Yes, we do. Ourcurrent strategy in patients with normal liver, outside of astudy protocol, is inflow occlusion with the Kelly clampcrushing technique.
Annals of Surgery • Volume 242, Number 6, December 2005 Strategies for Liver Transection
© 2005 Lippincott Williams & Wilkins 823