
The Relationship Between the Angiographic Findings and the Clinical Features of Carotid Artery...
6
Surg Today Jpn J Surg (2000) 30:37–42 The Relationship Between the Angiographic Findings and the Clinical Features of Carotid Artery Plaque Dong-Ik Kim 1 , Sun-Joung Lee 1 , Byung-Boong Lee 1 , Yong-il Kim 1 , Chin-Sang Chung 2 , Dae-Won Seo 2 , Kwang-Ho Lee 2 , Young-Hyeh Ko 3 , Duk-Kyung Kim 4 , Young-Soo Do 5 , and Hong-Sik Byun 5 1 Division of Vascular Surgery, 2 Department of Neurology, 3 Department of Diagnostic Pathology, 4 Division of Cardiology, and 5 Department of Radiology, Samsung Medical Center, College of Medicine, Sungkyunkwan University, 50 IL Won Dong, Kangnam-Ku, Seoul 135-710, Korea Key Words: carotid, atherosclerosis, endarterectomy, stroke, pathology Introduction Strokes are responsible for major disabilities among its survivors, at an immense cost not only to health care, but also to the quality of life. The composition of carotid artery plaque could affect the preoperative history of transient ischemic attack, stroke, and the process of identifying the endarterectomy layer. Surface ulcer- ation of carotid plaque can be the source of small emboli which form at the site of exposed plaque con- tents and thereafter cause neurologic symptoms. 1 Cal- cium deposits in atheromatous plaque are one of the features of complicated atherosclerotic plaque which makes an endarterectomy difficult. In this study, we reviewed the histological characteristics of atheroma- tous carotid plaque and analyzed the relationship among the histological, clinical, and angiographic features. Materials and Methods We retrospectively reviewed 55 patients who under- went carotid endarterectomy (46 men, 9 women; mean age 58.5 6 4.9 years in men, 71.0 6 1.4 years in women) for extracranial internal carotid artery (ICA) stenosis at our institute from January 1995 to December 1997 (Table 1). The degree of ICA stenosis was calculated by comparing the residual lumen at the point of maximum stenosis to the distal cervical ICA of the arteriogram. 2 The degrees of stenosis were categorized into two strata: those with 30% to 69% stenosis (moderate) and those with 70% to 99% (severe or high-grade) stenosis. Carotid plaque surface ulcerations were categorized Abstract: The purpose of this study was to investigate the histological characteristics of atheromatous carotid plaque, and to analyze the relationship between the angiographic find- ings and the clinical features. We retrospectively reviewed 55 cases of carotid endarterectomy for extracranial internal ca- rotid artery stenosis, who were treated at our institute from January 1995 to December 1997. The histological examination included hematoxylin–eosin staining, Masson-trichrome stain- ing, and immunostaining for antismooth muscle antibody and anti-CD68 antibody. The main compositions of the carotid plaque included synthetic type vascular smooth muscle cells and extracellular matrix. The histological findings showed ul- ceration in 49 (89.1%) cases, calcium deposits in 42 (76.4%) cases, and an inflammatory reaction in 44 (80.0%) cases. Neu- rological abnormalities were strongly associated with plaque ulceration (P 5 0.045) and an inflammatory reaction (P 5 0.013), whereas no correlation existed regarding calcium deposits (P 5 0.173). The angiographic findings showed ulcer- ation in 46 (83.6%) cases. Plaque ulceration in the angiogra- phy findings showed no statistically significant correlation with the histologic findings (P 5 0.410) and preoperative neu- rologic abnormalities (P 5 0.059). All of the atherosclerotic risk factors such as hypertension, smoking, diabetes mellitus, hyperlipidemia, and myocardial infarction had no statistically significant correlation with the histological features of the carotid plaque. In conclusion, the main compositions of ca- rotid plaque were synthetic-type vascular smooth muscle cells and extracellular matrix. The histological ulceration and inflammatory reaction of the plaque showed a statistically significant correlation with the preoperative neurologic symp- toms, whereas no correlation was seen in the calcium deposits. Angiographic ulceration showed no correlation with the histo- logical findings or preoperative neurologic abnormalities. In addition, the histological findings showed no correlation with the atherosclerotic risk factors. Reprint requests to: D.I. Kim (Received for publication on July 6, 1998; accepted on May 27, 1999)
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of The Relationship Between the Angiographic Findings and the Clinical Features of Carotid Artery...

Surg TodayJpn J Surg (2000) 30:37–42
The Relationship Between the Angiographic Findings andthe Clinical Features of Carotid Artery Plaque
Dong-Ik Kim1, Sun-Joung Lee1, Byung-Boong Lee1, Yong-il Kim1, Chin-Sang Chung2, Dae-Won Seo2,Kwang-Ho Lee2, Young-Hyeh Ko3, Duk-Kyung Kim4, Young-Soo Do5, and Hong-Sik Byun5
1 Division of Vascular Surgery, 2 Department of Neurology, 3 Department of Diagnostic Pathology, 4 Division of Cardiology,and 5 Department of Radiology, Samsung Medical Center, College of Medicine, Sungkyunkwan University, 50 IL Won Dong, Kangnam-Ku,Seoul 135-710, Korea
Key Words: carotid, atherosclerosis, endarterectomy, stroke,pathology
Introduction
Strokes are responsible for major disabilities among itssurvivors, at an immense cost not only to health care,but also to the quality of life. The composition of carotidartery plaque could affect the preoperative history oftransient ischemic attack, stroke, and the process ofidentifying the endarterectomy layer. Surface ulcer-ation of carotid plaque can be the source of smallemboli which form at the site of exposed plaque con-tents and thereafter cause neurologic symptoms.1 Cal-cium deposits in atheromatous plaque are one of thefeatures of complicated atherosclerotic plaque whichmakes an endarterectomy difficult. In this study, wereviewed the histological characteristics of atheroma-tous carotid plaque and analyzed the relationshipamong the histological, clinical, and angiographicfeatures.
Materials and Methods
We retrospectively reviewed 55 patients who under-went carotid endarterectomy (46 men, 9 women; meanage 58.5 6 4.9 years in men, 71.0 6 1.4 years in women)for extracranial internal carotid artery (ICA) stenosisat our institute from January 1995 to December 1997(Table 1). The degree of ICA stenosis was calculated bycomparing the residual lumen at the point of maximumstenosis to the distal cervical ICA of the arteriogram.2
The degrees of stenosis were categorized into twostrata: those with 30% to 69% stenosis (moderate) andthose with 70% to 99% (severe or high-grade) stenosis.Carotid plaque surface ulcerations were categorized
Abstract: The purpose of this study was to investigate thehistological characteristics of atheromatous carotid plaque,and to analyze the relationship between the angiographic find-ings and the clinical features. We retrospectively reviewed 55cases of carotid endarterectomy for extracranial internal ca-rotid artery stenosis, who were treated at our institute fromJanuary 1995 to December 1997. The histological examinationincluded hematoxylin–eosin staining, Masson-trichrome stain-ing, and immunostaining for antismooth muscle antibody andanti-CD68 antibody. The main compositions of the carotidplaque included synthetic type vascular smooth muscle cellsand extracellular matrix. The histological findings showed ul-ceration in 49 (89.1%) cases, calcium deposits in 42 (76.4%)cases, and an inflammatory reaction in 44 (80.0%) cases. Neu-rological abnormalities were strongly associated with plaqueulceration (P 5 0.045) and an inflammatory reaction (P 50.013), whereas no correlation existed regarding calciumdeposits (P 5 0.173). The angiographic findings showed ulcer-ation in 46 (83.6%) cases. Plaque ulceration in the angiogra-phy findings showed no statistically significant correlationwith the histologic findings (P 5 0.410) and preoperative neu-rologic abnormalities (P 5 0.059). All of the atheroscleroticrisk factors such as hypertension, smoking, diabetes mellitus,hyperlipidemia, and myocardial infarction had no statisticallysignificant correlation with the histological features of thecarotid plaque. In conclusion, the main compositions of ca-rotid plaque were synthetic-type vascular smooth muscle cellsand extracellular matrix. The histological ulceration andinflammatory reaction of the plaque showed a statisticallysignificant correlation with the preoperative neurologic symp-toms, whereas no correlation was seen in the calcium deposits.Angiographic ulceration showed no correlation with the histo-logical findings or preoperative neurologic abnormalities. Inaddition, the histological findings showed no correlation withthe atherosclerotic risk factors.
Reprint requests to: D.I. Kim(Received for publication on July 6, 1998; accepted on May 27,1999)

into three strata. The maximal depth and length of theulcer in millimeters on the arteriograms were multipliedto provide the ulcer area, in square millimeters: thosewith 10 or less (type A), those with 10 to 40 (type B),and those with greater than 40 (type C). The indicationsfor a carotid endarterectomy in our institute are: (1)symptomatic stenosis of greater than 70%, (2) symp-tomatic stenosis of 30% to 69% with type C plaqueulcer, (3) asymptomatic stenosis of greater than 70%with contralateral ICA complete occlusion, and (4) as-ymptomatic stenosis of greater than 70% with type Cplaque ulceration.
Pathologic Examination
The atheromatous carotid plaque was endarterec-tomized by two well-trained vascular surgeons. After alongitudinal arteriotomy from common carotid arteryto ICA distal to the stenotic lesion, the surface ofthe atheromatous plaque was observed to determinewhether surface ulceration were present or not. Duringthe endarterectomy procedures, we checked for grosscalcium deposits. Gross photographs of endarterec-tomized specimens were taken. The specimens weredivided longitudinally into two sections: half for trans-mission electron microscopy (TEM) and half for lightmicroscopy. The details of the histological procedureswere identical to those in our previous reports.3,4
For light microscopy, the specimens were fixed in10% buffered formaldehyde solution at room tempera-ture, embedded in paraffin, sectioned, and stained withhematoxylin–eosin and Masson-trichrome. Immunos-taining for antismooth muscle antibody and anti-CD68antibody was performed using the peroxidase-antiperoxidase technique.
For transmission electron microscopy, the specimenswere placed in a 2.5% glutaraldehyde solution and werefurther diced into smaller pieces. These pieces werethen washed in a 0.1M phosphate buffer solution for 2 h,and postfixed with osmium tetroxide for 2h at 4°C.After these double fixations, the pieces were washedwith 0.1M sodium acetate, stained en bloc with 1%uranyl acetate for 15min at 4°C, washed again with0.1M sodium acetate for 10 min at 4°C, dehydratedthrough a graded ethanol series, then were finally em-
bedded in Epon 812. Thin sections, which were stainedwith 0.5% toluidine blue and 0.5% sodium burox, wereprepared for the purpose of orientation, and ultrathinsections were then cut with an ultramicrotome (SorvalMT 1, Harford, CT, USA). The ultrathin sections werestained with 1% uranyl acetate and Raynold’s leadcitrate. Observations were carried out using Hitachi(Tokyo, Japan) HU-11A and HU-11DS electronmicroscopes.
Histological examinations were performed indepen-dently by one pathologist and the first author, whilefocusing on plaque ulcerations, calcium deposits, andinflammation. The prevalences of these features werebased on a consensus opinion between the pathologistand the first author at a joint reevaluation of their pre-viously obtained independent data.
Statistics
All values were expressed as the mean 6 SD. Statisticalsignificance was determined by the Student’s t-test. PValues of less than 0.05 were considered to be statisti-cally significant.
Results
The mean carotid stenosis according to the luminal di-ameter reduction was 89.0% 6 1.4% (Table 1). Therewere 38 (69.1%) cases with symptomatic stenosis and 17(30.9%) cases with asymptomatic stenosis. A histologi-cal examination revealed the main compositions ofthe carotid plaque to be synthetic-type vascular smoothmuscle cells and extracellular matrix (Figs. 1–5).Among the 55 cases with carotid plaque, ulcerationwas found in 49 (89.1%) cases, calcium deposits in 42(76.4%) cases, and an inflammatory reaction in 44(80.0%) cases. The relationship between the histologi-cal features of the carotid plaque and the preoperativehistory of neurological abnormalities is shown in Table2. Neurological abnormalities were strongly associated
Table 1. Characteristics of the patients and the degreea ofinternal carotid artery stenosis
Sex Age (years) StenosisMale Female Male Female (%)
46 (83.6%) 9 (16.4%) 58.5 6 4.9 71.0 6 1.4 89.0 6 1.4
a Internal carotid artery (ICA) stenosis was calculated by comparingthe residual lumen at the point of maximun stenosis to the distalcervical ICA
Table 2. Relationship between the histological features ofcarotid plaque and preoperative neurologic symptoms
Asymptomatic Symptomatic
Ulceration (1) 13 36(2) 4 2
P 5 0.045Calcium deposit (1) 11 31
(2) 6 7P 5 0.173
Inflammation (1) 17 27(2) 0 11
P 5 0.013
38 D.I. Kim et al.: Histological Features of Carotid Artery Plaque

Fig. 1. a Central lipid core of atheromatous plaque with anoverlying fibrous cap. Dystrophic calcification is present in thelipid core showing a cholesterol cleft (H&E, 3400). b Well-developed atheromatous plaque showing massive dystrophic
calcification in the superficial intimal layer (H&E, 340). cDiffuse calcification (H&E, 3100). d Higher magnification ofc (H&E, 3400)
Fig. 2a,b. Masson-trichrome stain. aFibrosis of the intimal fibrous capand the media is high lighted (340).b Diffuse fibrosis of the entire layer isshown (340)
D.I. Kim et al.: Histological Features of Carotid Artery Plaque 39
with plaque ulceration (P 5 0.045) and inflammatoryreaction (P 5 0.013), whereas no such correlation ex-isted for calcium deposits (P 5 0.173). Angiographicfindings showed ulceration in 46 (83.6%) cases (Table3). Plaque ulceration in angiography showed no statisti-cally significant correlation with the histologic findings(P 5 0.410) or preoperative neurologic abnormalities(P 5 0.059). The relationship between the histologicalfeatures of carotid plaque and the atherosclerotic riskfactors is shown in Table 4. None of the atheroscleroticrisk factors had any statistically significant correlation
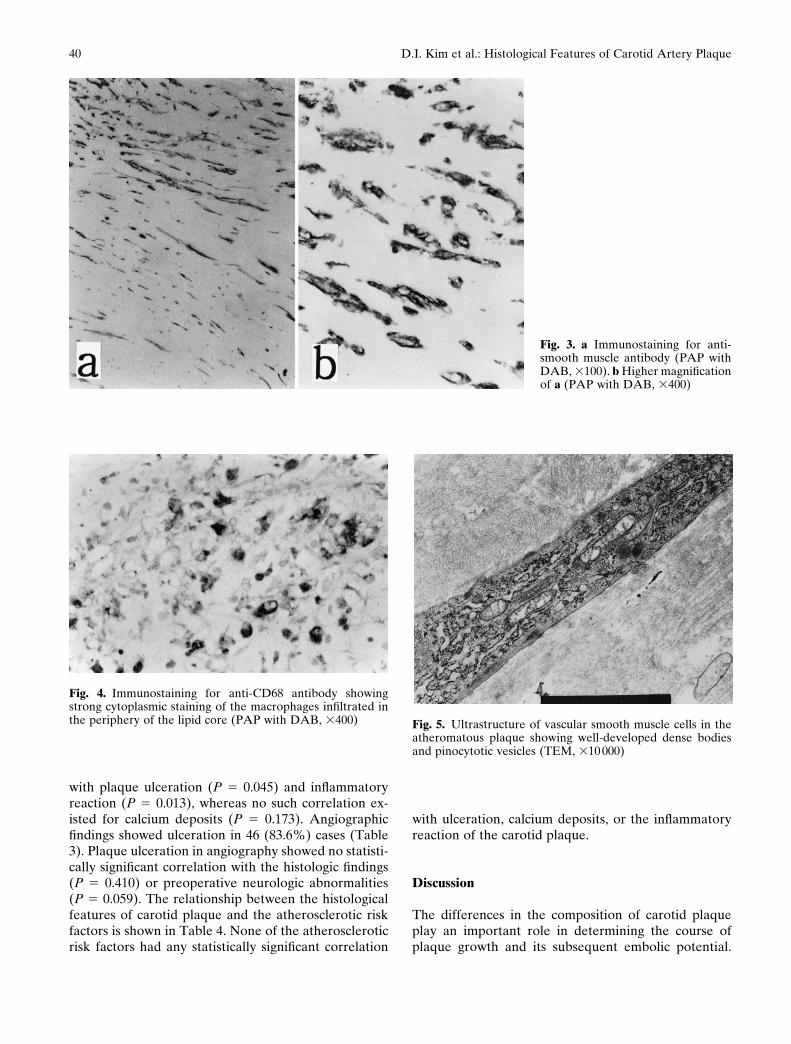
Fig. 3. a Immunostaining for anti-smooth muscle antibody (PAP withDAB, 3100). b Higher magnificationof a (PAP with DAB, 3400)
Fig. 4. Immunostaining for anti-CD68 antibody showingstrong cytoplasmic staining of the macrophages infiltrated inthe periphery of the lipid core (PAP with DAB, 3400) Fig. 5. Ultrastructure of vascular smooth muscle cells in the
atheromatous plaque showing well-developed dense bodiesand pinocytotic vesicles (TEM, 310 000)
with ulceration, calcium deposits, or the inflammatoryreaction of the carotid plaque.
Discussion
The differences in the composition of carotid plaqueplay an important role in determining the course ofplaque growth and its subsequent embolic potential.
40 D.I. Kim et al.: Histological Features of Carotid Artery Plaque
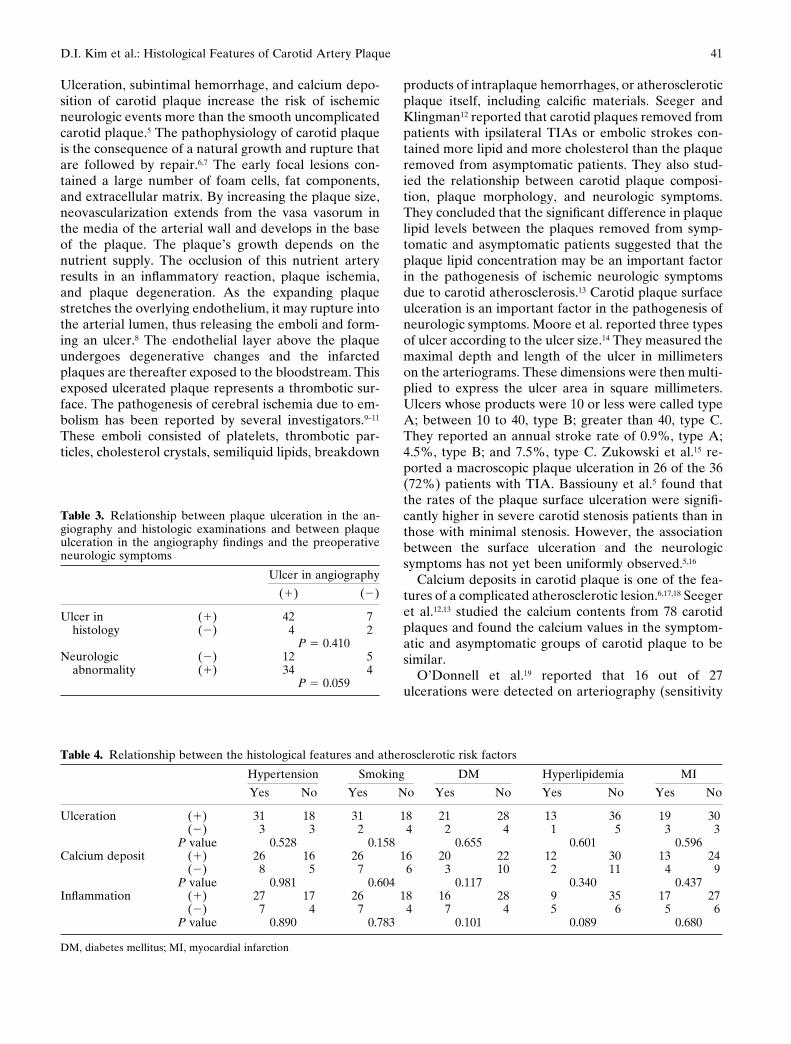
Table 3. Relationship between plaque ulceration in the an-giography and histologic examinations and between plaqueulceration in the angiography findings and the preoperativeneurologic symptoms
Ulcer in angiography
(1) (2)
Ulcer in (1) 42 7histology (2) 4 2
P 5 0.410Neurologic (2) 12 5
abnormality (1) 34 4P 5 0.059
Ulceration, subintimal hemorrhage, and calcium depo-sition of carotid plaque increase the risk of ischemicneurologic events more than the smooth uncomplicatedcarotid plaque.5 The pathophysiology of carotid plaqueis the consequence of a natural growth and rupture thatare followed by repair.6,7 The early focal lesions con-tained a large number of foam cells, fat components,and extracellular matrix. By increasing the plaque size,neovascularization extends from the vasa vasorum inthe media of the arterial wall and develops in the baseof the plaque. The plaque’s growth depends on thenutrient supply. The occlusion of this nutrient arteryresults in an inflammatory reaction, plaque ischemia,and plaque degeneration. As the expanding plaquestretches the overlying endothelium, it may rupture intothe arterial lumen, thus releasing the emboli and form-ing an ulcer.8 The endothelial layer above the plaqueundergoes degenerative changes and the infarctedplaques are thereafter exposed to the bloodstream. Thisexposed ulcerated plaque represents a thrombotic sur-face. The pathogenesis of cerebral ischemia due to em-bolism has been reported by several investigators.9–11
These emboli consisted of platelets, thrombotic par-ticles, cholesterol crystals, semiliquid lipids, breakdown
products of intraplaque hemorrhages, or atheroscleroticplaque itself, including calcific materials. Seeger andKlingman12 reported that carotid plaques removed frompatients with ipsilateral TIAs or embolic strokes con-tained more lipid and more cholesterol than the plaqueremoved from asymptomatic patients. They also stud-ied the relationship between carotid plaque composi-tion, plaque morphology, and neurologic symptoms.They concluded that the significant difference in plaquelipid levels between the plaques removed from symp-tomatic and asymptomatic patients suggested that theplaque lipid concentration may be an important factorin the pathogenesis of ischemic neurologic symptomsdue to carotid atherosclerosis.13 Carotid plaque surfaceulceration is an important factor in the pathogenesis ofneurologic symptoms. Moore et al. reported three typesof ulcer according to the ulcer size.14 They measured themaximal depth and length of the ulcer in millimeterson the arteriograms. These dimensions were then multi-plied to express the ulcer area in square millimeters.Ulcers whose products were 10 or less were called typeA; between 10 to 40, type B; greater than 40, type C.They reported an annual stroke rate of 0.9%, type A;4.5%, type B; and 7.5%, type C. Zukowski et al.15 re-ported a macroscopic plaque ulceration in 26 of the 36(72%) patients with TIA. Bassiouny et al.5 found thatthe rates of the plaque surface ulceration were signifi-cantly higher in severe carotid stenosis patients than inthose with minimal stenosis. However, the associationbetween the surface ulceration and the neurologicsymptoms has not yet been uniformly observed.5,16
Calcium deposits in carotid plaque is one of the fea-tures of a complicated atherosclerotic lesion.6,17,18 Seegeret al.12,13 studied the calcium contents from 78 carotidplaques and found the calcium values in the symptom-atic and asymptomatic groups of carotid plaque to besimilar.
O’Donnell et al.19 reported that 16 out of 27ulcerations were detected on arteriography (sensitivity
Table 4. Relationship between the histological features and atherosclerotic risk factors
Hypertension Smoking DM Hyperlipidemia MI
Yes No Yes No Yes No Yes No Yes No
Ulceration (1) 31 18 31 18 21 28 13 36 19 30(2) 3 3 2 4 2 4 1 5 3 3
P value 0.528 0.158 0.655 0.601 0.596Calcium deposit (1) 26 16 26 16 20 22 12 30 13 24
(2) 8 5 7 6 3 10 2 11 4 9P value 0.981 0.604 0.117 0.340 0.437
Inflammation (1) 27 17 26 18 16 28 9 35 17 27(2) 7 4 7 4 7 4 5 6 5 6
P value 0.890 0.783 0.101 0.089 0.680
DM, diabetes mellitus; MI, myocardial infarction
D.I. Kim et al.: Histological Features of Carotid Artery Plaque 41

59%). In our study, 42 out of 49 ulcerations were de-tected on arteriography (sensitivity 85.7%). The highsensitivity in our study might be the result of the broadcriteria used to determine the ulcers in arteriography.
Various risk factors are known to contribute to theatherosclerosis of the carotid artery. Hypertension,20
diabetes mellitus,21 smoking,17 and hyperlipidemia18
promote atherosclerosis. Sueyoshi et al.22 reported thatserum cholesterol is an important risk factor in the pro-gression of carotid atherosclerosis.
Conclusion
The results of our study suggest that the main composi-tions of carotid plaque were synthetic-type vascularsmooth muscle cells and the extracellular matrix. Theplaque ulceration and inflammatory reaction of theplaque showed a statistically significant correlation withthe preoperative neurologic symptoms, but no correla-tion with calcium deposits. The angiographic ulcerationof the plaque showed no correlation with either thehistological findings or the preoperative neurologicalabnormalities. The plaque ulceration, calcium deposits,and inflammtory reaction also showed no correlationwith such atherosclerotic risk factors as hypertension,smoking, diabetes mellitus, hyperlipidemia, and myo-cardial infarction.
References
1. Polak JF (1992) Peripheral vascular sonography: a practice guide2. North American Symptomatic Carotid Endarterectomy
(NASCET) Steering Committee (1991) North American Symp-tomatic Carotid Surgery Trial: methods, patient characteristics,and progress. Stroke 22:711–720
3. Kim DI, Lee BB, Joh JW, Lee SK, Kim YI, Kim HH (1997) Cellsin pseudointimal hyperplasia is migrated from extravascularspace. J Cardiovasc Surg 38:277–281
4. Kim DI, Kambayashi J, Shibuya T, Sakon M, Kawasaki T, Mori T(1995) Suppression of pseudointimal hyperplasia by a novelprostacyclin analogue: Beraprost. Surg Today 25:722–728
5. Bassiouny HS, Davis H, Massawa N, Gewertz BL, Glagov S,Zarins CK (1989) Critical carotid stenoses: morphologic and
chemical similarity between symptomatic and asymptomaticplaques. J Vasc Surg 9:202–212
6. Ross R (1986) The pathogenesis of atherosclerosis—an update. NEngl J Med 314:488–500
7. Tracy RE, Strong JP, Toca VT, Lopez CR (1979) Atherosclerosisand its fibroproliferative base and cap in the thoracic aorta. LabInvest 41:546–552
8. Imparato AM, Riles TS, Gorstein F (1979) The carotid bifurca-tion plaque: pathologic findings associated with cerebral ischemia.Stroke 10:238–245
9. Persson AV, Robichaux WT, Silverman M (1983) The naturalhistory of carotid plaque development. Arch Surg 118:1048–1052
10. Edwards JH, Kricheff I, Gorstein F, Riles T, Imparato A (1979)Atherosclerotic subintimal haematoma of the carotid artery.Radiology 133:123–129
11. Millika CH (1965) The pathogenesis of transient focal cerebralischaemia. Circulation 32:438–450
12. Seeger JM, Klingman N (1987) The relationship between carotidplaque composition and neurologic symptoms. J Surg Res 43:78–85
13. Seeger JM, Barratt E, Lawson GA, Klingman N (1995) The rela-tionship between carotid plaque composition, plaque morphol-ogy, and neurologic symptoms. J Surg Res 58:330–336
14. Moore WS, Boren C, Malone JM, Roon AJ, Eisenberg R,Goldstone J, Mani R (1978) Natural history of nonstenotic as-ymptomatic ulcerative lesions of the carotid artery. Arch Surg113:1352–1359
15. Zukowski AJ, Nicolaides AN, Lewis RT, Mansfield AO, WilliamsMA, Helmis E, Malouf GM, Thomas D, Al-Kutoubi A,Kyprianou P, Eastoott HHG (1984) The correlation between ca-rotid plaque ulceration and cerebral infarction on CT scan. J VascSurg 1:782–786
16. Fisher CM, Ojemann RG (1986) A clinico-pathologic study ofcarotid endarterectomy plaques. Rev Neurol 142:573–589
17. Geer JC, Catsulis C, McGill HC Jr, Strong JP (1968) Fine struc-ture of the baboon aortic fatty streak. Am J Pathol 52:265–286
18. Small DM (1988) Progression and regression of atheroscleroticlesions. Arteriosclerosis 8:103–129
19. O’Donnell TF Jr, Erdoes L, Mackey WC, McCullough J, ShepardA, Heggerick P, Isner J, Callow AD (1985) Correlation of B-mode ultrasound imaging and arteriography with pathologicfindings at carotid endarterectomy. Arch Surg 120:443–449
20. Lindeberg S, Nilsson Ehle P, Terent A, Vessby B, Schersten B(1994) Cardiovascular risk factors in a Melanesian populationapparently free from stroke and ischemic heart disease: theKitava Study. J Intern Med 236:331–340
21. Gasecki AP, Eliasziw M, Fox AJ, Hachinski VC, Barnett HJM(1995) Serum cholesterol level is associated with the severity ofcarotid stenosis in symptomatic patients: results from NASCET.Cerebrovasc Dis 4:417–420
22. Sueyoshi K, Tanaka H, Mandai K, Nishino M, Itoh T, FukunagaR, Yamada Y, Abe H (1994) Progression of carotid atherosclero-sis in Japanese patients with coronary artery disease. Int JAngiogr 3:56–60
42 D.I. Kim et al.: Histological Features of Carotid Artery Plaque




















