
Atherothrombosis and High-Risk Plaque
10
STATE-OF-THE-ART PAPER Atherothrombosis and High-Risk Plaque Part II: Approaches by Noninvasive Computed Tomographic/ Magnetic Resonance Imaging Valentin Fuster, MD, PHD, FACC,* Zahi A. Fayad, PHD, FACC,* Pedro R. Moreno, MD, FACC,* Michael Poon, MD, FACC,*† Roberto Corti, MD, FACC,‡ Juan J. Badimon, PHD, FACC* New York, New York; and Zurich, Switzerland This second part of the review on atherothrombosis highlights the diffuse nature of the disease analyzing the feasibility and potential of the noninvasive imaging modalities, including computed tomography (electron-beam computed and multi-detector computed tomography) and magnetic resonance imaging for its detection and monitoring. These imaging modalities are being established as promising tools in high-risk cardiovascular patients for identification and/or management of coronary calcification, stenotic or obstruc- tive disease, high-risk plaques (not necessarily stenotic), and overall burden of the disease. In addition, such technology facilitates the understanding of the processes involved in the development and progression of atherothrombosis responsible for coronary, cerebral, and peripheral ischemic events. (J Am Coll Cardiol 2005;46:1209 –18) © 2005 by the American College of Cardiology Foundation ATHEROTHROMBOSIS AS A SYSTEMIC DISEASE: CLINICAL IMPACT Atherothrombotic cardiovascular disease is a diffuse condi- tion involving the coronary arteries, carotid arteries, aorta and peripheral arteries. However, the pathobiology of the disease and clinical consequences vary in the four regions. In patients with atherothrombotic disease, myocardial isch- emia or infarction causes as much as 70% of deaths (1,2). Cerebrovascular disease causes approximately 10% to 17% of deaths in these patients, and another 10% are caused by ruptured aneurysms or visceral infarctions. Peripheral arte- rial disease may be viewed as benign because it does not cause direct mortality. However, it is an ominous manifes- tation of underlying disseminated atherosclerosis and, therefore, of mortality related to coronary disease and cerebrovascular disease (1). Thus, symptomatic individuals (i.e., those presenting with claudication) have a history of myocardial infarction or stroke in 20% to 30% of cases and evidence of underlying coronary disease in 50% to 70% of cases (1–5); an abnormal ankle-brachial index (0.9) with- out symptoms is 90% sensitive and 95% specific for peripheral artery disease and may also indicate underlying disseminated atherosclerosis (4,5). Most importantly, on long-term follow-up, patients with peripheral arterial dis- ease, symptomatic or not, have a two- to three-fold increase in their rate of mortality related to myocardial infarction and stroke compared with age-matched control subjects (6,7). In atherothrombotic disease, the rate of mortality proportion- ally increases with the number of regions involved and degree of distribution of the disease (4,8,9). The concept of multi-territory atherothrombosis has been recently addressed by the Trans-Atlantic Inter-Society Consensus (TASC) (10,11) by pooling the data from available studies of 1,886 patients older than 62 years of age with symptomatic atherothrombotic disease and by the Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events (CAPRIE) trial of 20,000 patients (12). In these two large populations, the data showed that 3% to 8% had symptomatic atherosclerotic disease in all three main arterial territories and 23% to 32% in two (Fig. 1). NONINVASIVE CT/MR IMAGING OF “HIGH-RISK PLAQUES” AND DISEASE “BURDEN” Because the composition of “high-risk plaques” varies de- pending on the arterial region and because striking hetero- geneity exists in the composition of human atherothrom- botic plaques even within the same individual, reliable noninvasive imaging modalities are needed that can detect atherothrombotic disease in various stages and regions, characterize the composition of the plaques, measure the extent of plaque “burden,” further study the mechanisms of plaque progression, assess the response to therapy, and allow for assessment of subclinical disease (13). We will focus on two most promising noninvasive techniques— computed tomography (CT) and magnetic resonance imaging (MRI) (14)—since, eventually, these techniques are likely to be more widely used. From the *Zena and Michael A. Wiener Cardiovascular Institute and the Marie-Josee and Henry R. Kravis Cardiovascular Health Center, The Mount Sinai School of Medicine, and †Cabrini Hospital, New York, New York; and the ‡Zurich University Hospital, Zurich, Switzerland. Manuscript received July 14, 2004; revised manuscript received December 23, 2004, accepted March 4, 2005. Journal of the American College of Cardiology Vol. 46, No. 7, 2005 © 2005 by the American College of Cardiology Foundation ISSN 0735-1097/05/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2005.03.075
Transcript of Atherothrombosis and High-Risk Plaque
S
APMVMN
AC
AtadpeCorrcttc(mecopdleis
MSU
2
Journal of the American College of Cardiology Vol. 46, No. 7, 2005© 2005 by the American College of Cardiology Foundation ISSN 0735-1097/05/$30.00P
TATE-OF-THE-ART PAPER
therothrombosis and High-Risk Plaqueart II: Approaches by Noninvasive Computed Tomographic/agnetic Resonance Imaging
alentin Fuster, MD, PHD, FACC,* Zahi A. Fayad, PHD, FACC,* Pedro R. Moreno, MD, FACC,*ichael Poon, MD, FACC,*† Roberto Corti, MD, FACC,‡ Juan J. Badimon, PHD, FACC*
ew York, New York; and Zurich, Switzerland
This second part of the review on atherothrombosis highlights the diffuse nature of thedisease analyzing the feasibility and potential of the noninvasive imaging modalities,including computed tomography (electron-beam computed and multi-detector computedtomography) and magnetic resonance imaging for its detection and monitoring. Theseimaging modalities are being established as promising tools in high-risk cardiovascularpatients for identification and/or management of coronary calcification, stenotic or obstruc-tive disease, high-risk plaques (not necessarily stenotic), and overall burden of the disease. Inaddition, such technology facilitates the understanding of the processes involved in thedevelopment and progression of atherothrombosis responsible for coronary, cerebral, andperipheral ischemic events. (J Am Coll Cardiol 2005;46:1209–18) © 2005 by the American
ublished by Elsevier Inc. doi:10.1016/j.jacc.2005.03.075
College of Cardiology Foundation
aad
rCawCEtst
NP
Bpgbnacepftt(
THEROTHROMBOSIS AS A SYSTEMIC DISEASE:LINICAL IMPACT
therothrombotic cardiovascular disease is a diffuse condi-ion involving the coronary arteries, carotid arteries, aortand peripheral arteries. However, the pathobiology of theisease and clinical consequences vary in the four regions. Inatients with atherothrombotic disease, myocardial isch-mia or infarction causes as much as 70% of deaths (1,2).erebrovascular disease causes approximately 10% to 17%f deaths in these patients, and another 10% are caused byuptured aneurysms or visceral infarctions. Peripheral arte-ial disease may be viewed as benign because it does notause direct mortality. However, it is an ominous manifes-ation of underlying disseminated atherosclerosis and,herefore, of mortality related to coronary disease anderebrovascular disease (1). Thus, symptomatic individualsi.e., those presenting with claudication) have a history ofyocardial infarction or stroke in 20% to 30% of cases and
vidence of underlying coronary disease in 50% to 70% ofases (1–5); an abnormal ankle-brachial index (�0.9) with-ut symptoms is 90% sensitive and 95% specific foreripheral artery disease and may also indicate underlyingisseminated atherosclerosis (4,5). Most importantly, on
ong-term follow-up, patients with peripheral arterial dis-ase, symptomatic or not, have a two- to three-fold increasen their rate of mortality related to myocardial infarction andtroke compared with age-matched control subjects (6,7). In
From the *Zena and Michael A. Wiener Cardiovascular Institute and thearie-Josee and Henry R. Kravis Cardiovascular Health Center, The Mount Sinai
chool of Medicine, and †Cabrini Hospital, New York, New York; and the ‡Zurichniversity Hospital, Zurich, Switzerland.
mManuscript received July 14, 2004; revised manuscript received December 23,
004, accepted March 4, 2005.
therothrombotic disease, the rate of mortality proportion-lly increases with the number of regions involved andegree of distribution of the disease (4,8,9).The concept of multi-territory atherothrombosis has been
ecently addressed by the Trans-Atlantic Inter-Societyonsensus (TASC) (10,11) by pooling the data from
vailable studies of 1,886 patients older than 62 years of ageith symptomatic atherothrombotic disease and by thelopidogrel versus Aspirin in Patients at Risk of Ischemicvents (CAPRIE) trial of �20,000 patients (12). In these
wo large populations, the data showed that 3% to 8% hadymptomatic atherosclerotic disease in all three main arterialerritories and 23% to 32% in two (Fig. 1).
ONINVASIVE CT/MR IMAGING OF “HIGH-RISKLAQUES” AND DISEASE “BURDEN”
ecause the composition of “high-risk plaques” varies de-ending on the arterial region and because striking hetero-eneity exists in the composition of human atherothrom-otic plaques even within the same individual, reliableoninvasive imaging modalities are needed that can detecttherothrombotic disease in various stages and regions,haracterize the composition of the plaques, measure thextent of plaque “burden,” further study the mechanisms oflaque progression, assess the response to therapy, and allowor assessment of subclinical disease (13). We will focus onwo most promising noninvasive techniques—computedomography (CT) and magnetic resonance imaging (MRI)14)—since, eventually, these techniques are likely to be
ore widely used.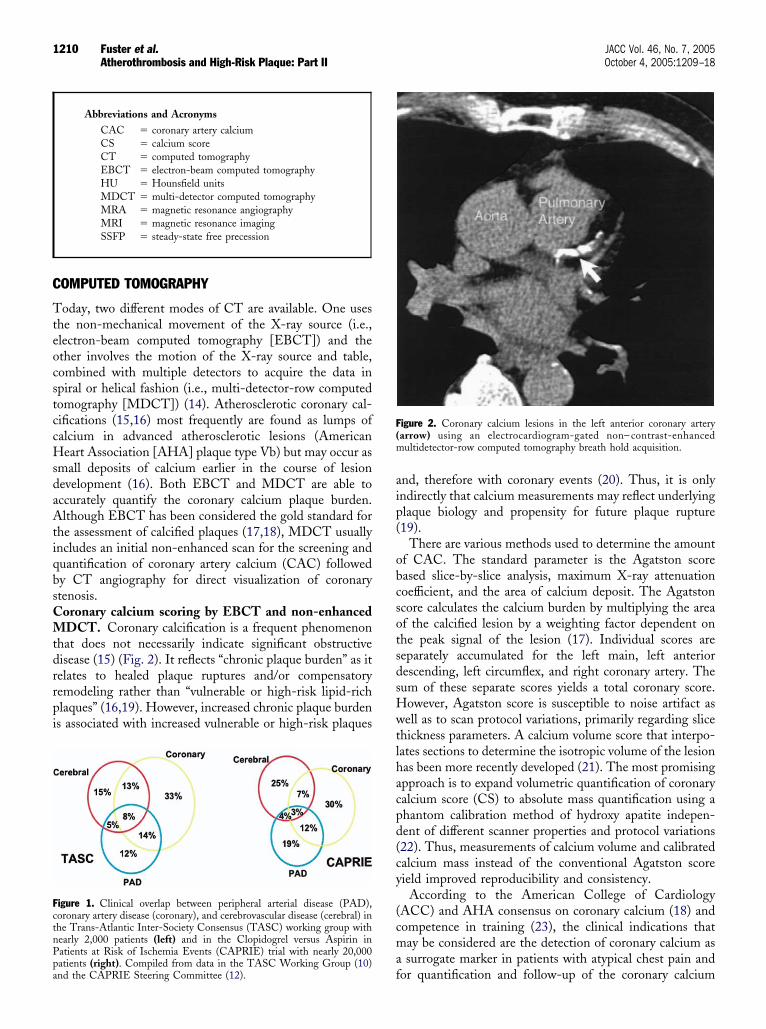
C
TteocstccHsdaAtiqbsCMtdrrpi
aip(
obcsotsdsHwtlhacpd(cy
(cma
FctnPpa
F(m
1210 Fuster et al. JACC Vol. 46, No. 7, 2005Atherothrombosis and High-Risk Plaque: Part II October 4, 2005:1209–18
OMPUTED TOMOGRAPHY
oday, two different modes of CT are available. One useshe non-mechanical movement of the X-ray source (i.e.,lectron-beam computed tomography [EBCT]) and thether involves the motion of the X-ray source and table,ombined with multiple detectors to acquire the data inpiral or helical fashion (i.e., multi-detector-row computedomography [MDCT]) (14). Atherosclerotic coronary cal-ifications (15,16) most frequently are found as lumps ofalcium in advanced atherosclerotic lesions (Americaneart Association [AHA] plaque type Vb) but may occur as
mall deposits of calcium earlier in the course of lesionevelopment (16). Both EBCT and MDCT are able toccurately quantify the coronary calcium plaque burden.lthough EBCT has been considered the gold standard for
he assessment of calcified plaques (17,18), MDCT usuallyncludes an initial non-enhanced scan for the screening anduantification of coronary artery calcium (CAC) followedy CT angiography for direct visualization of coronarytenosis.oronary calcium scoring by EBCT and non-enhancedDCT. Coronary calcification is a frequent phenomenon
hat does not necessarily indicate significant obstructiveisease (15) (Fig. 2). It reflects “chronic plaque burden” as itelates to healed plaque ruptures and/or compensatoryemodeling rather than “vulnerable or high-risk lipid-richlaques” (16,19). However, increased chronic plaque burdens associated with increased vulnerable or high-risk plaques
igure 1. Clinical overlap between peripheral arterial disease (PAD),oronary artery disease (coronary), and cerebrovascular disease (cerebral) inhe Trans-Atlantic Inter-Society Consensus (TASC) working group withearly 2,000 patients (left) and in the Clopidogrel versus Aspirin inatients at Risk of Ischemia Events (CAPRIE) trial with nearly 20,000
Abbreviations and AcronymsCAC � coronary artery calciumCS � calcium scoreCT � computed tomographyEBCT � electron-beam computed tomographyHU � Hounsfield unitsMDCT � multi-detector computed tomographyMRA � magnetic resonance angiographyMRI � magnetic resonance imagingSSFP � steady-state free precession
fatients (right). Compiled from data in the TASC Working Group (10)nd the CAPRIE Steering Committee (12).
nd, therefore with coronary events (20). Thus, it is onlyndirectly that calcium measurements may reflect underlyinglaque biology and propensity for future plaque rupture19).
There are various methods used to determine the amountf CAC. The standard parameter is the Agatston scoreased slice-by-slice analysis, maximum X-ray attenuationoefficient, and the area of calcium deposit. The Agatstoncore calculates the calcium burden by multiplying the areaf the calcified lesion by a weighting factor dependent onhe peak signal of the lesion (17). Individual scores areeparately accumulated for the left main, left anteriorescending, left circumflex, and right coronary artery. Theum of these separate scores yields a total coronary score.owever, Agatston score is susceptible to noise artifact asell as to scan protocol variations, primarily regarding slice
hickness parameters. A calcium volume score that interpo-ates sections to determine the isotropic volume of the lesionas been more recently developed (21). The most promisingpproach is to expand volumetric quantification of coronaryalcium score (CS) to absolute mass quantification using ahantom calibration method of hydroxy apatite indepen-ent of different scanner properties and protocol variations22). Thus, measurements of calcium volume and calibratedalcium mass instead of the conventional Agatston scoreield improved reproducibility and consistency.
According to the American College of CardiologyACC) and AHA consensus on coronary calcium (18) andompetence in training (23), the clinical indications thatay be considered are the detection of coronary calcium assurrogate marker in patients with atypical chest pain and
igure 2. Coronary calcium lesions in the left anterior coronary arteryarrow) using an electrocardiogram-gated non– contrast-enhancedultidetector-row computed tomography breath hold acquisition.
or quantification and follow-up of the coronary calcium

pretoeptwcohtlrpbgmNrcr
rfwrstmmfosFerbaterfrfifEnaM
ccf
tysccs
tefetupriCbspVtwranrdcamgwin(ri
Fcc(
1211JACC Vol. 46, No. 7, 2005 Fuster et al.October 4, 2005:1209–18 Atherothrombosis and High-Risk Plaque: Part II
laque load in asymptomatic patients with cardiovascularisk factors. However, although the 34th Bethesda Confer-nce provides an encouraging document about the diagnos-ic and prognostic future of noninvasive imaging (24), anutline of clear clinical indications of CAC is still consid-red to be premature until ongoing prospective studiesrovide more definitive answers (25). Thus far, it appearshat the presence of CAC is a sensitive marker of patientsith significant obstructive disease but that only a signifi-
ant extent of CAC is reliable regarding specificity (18). Inther words, patients with no or a low calcium CAC scoreave lower probabilities of developing clinical events thanhose of high scores (26–28). Nevertheless, although estab-ished as an indicator of overall disease extent, its percentileanking adjusted to age and gender is more powerful forredicting coronary events (29). As a general guideline and,ased on the CS, plaque burden interpretation has beenraded as minimal (CS 0 to 10), mild (CS 11 to 100),oderate (CS 101 to 400), or extensive (CS �400) (30).evertheless, a CS of 45 in a 45-year-old man, which would
epresent above the 95th percentile, would exceed the risk ofardiac events of a 75-year-old with similar CS, who wouldank at less than the 10th percentile (29).
Whether coronary calcium is an independent and supe-ior marker of risk to conventional (28) or emerging riskactors (31) as a predictor for future cardiac events is not yetell established. In terms of risk stratification, the algo-
ithms that combine the conventional major risk factors,uch as those of the Framingham Heart Study or Prospec-ive Cardiovascular Munster (PROCAM) study, remain theost widely used methods to estimate absolute risk forajor coronary events (24). The AHA Prevention V Con-
erence (32) established the use of CS assessment, amongther noninvasive tests, as a potential tool for furthertratification in selected groups of asymptomatic patients.or example, in patients with a pretest coronary event riskstimated between 6% and 20% in 10 years (intermediateisk patient) a positive CS of more than 300 to 400 woulde useful in further stratification toward a high-risk statusnd assist in decisions regarding the need for preventiveherapies (Fig. 3) (33). Indeed, there is recent supportingvidence that a promising approach to further estimate riskesults from this combination of CS with conventional riskactor profile (34–36). Moreover, added to a high CS andisk factor profile, a stress test with perfusion and/orunction can provide further diagnostic and prognosticnformation (Table 1). The coronary calcium measurementrom non-enhanced MDCT appears to correlate well withBCT (37,38). Although further comparative studies areeeded, particularly at lower CS levels (39), acquisition timend radiation are less with EBCT (40), but non-enhanced
DCT yields greater reproducibility (38).Whole-body EBCT has been performed to evaluate
oronary, carotid, and aorto-iliac arteries for atheroscleroticalcifications. Age and hypertension were the dominant risk
actors for systemic calcified atherosclerosis. Thus, in regard ro age, approximately one-third of subjects younger than 50ears of age were free of calcified disease, whereas allubjects older than 70 years of age were found to have somealcium (41). This study suggests that there are significantorrelations and risk factor associations for calcified athero-clerosis in different vascular beds.
For clinical purposes, the specific patient who may benefithe most from calcium scores is the patient with anstimated 10-year risk of 10% to 20% (two or more riskactors) according to the most recent national cholesterolducation program adult treatment panel (National Choles-erol Education Program-Adult Treatment Panel III) exec-tive summary (42). The rationale to perform a CS in thisatient is supported by the significant increase in the actualisk if the test is positive, and the dramatic reduction in riskf the test is negative, as shown in Table 1 (34).
oronary non-calcified components of plaque imagingy contrast-enhanced MDCT. Recently, it has beenhown that CT has the potential to identify non-calcifiedlaques in the coronary arteries in vivo (Fig. 4) (23,43,44).arious components of atherosclerotic plaque may be dis-
inguished and characterized by contrast-enhanced MDCT,hich holds the promise of identifying vulnerable or high-
isk plaques (45). In an ex vivo study on human coronaryrteries, it has been shown that various imaging features ofon-calcified and calcified plaques depicted with CT cor-elate well with histopathologic stages of atherosclerosisefined by the AHA (46). As groups, lipid-rich, fibrous andalcified plaques display different Hounsfield units (HU),nd could be differentiated reliably. However, the HU unitsay overlap when differentiating individual plaques. Table 2
ives an overview of the typical morphologic appearanceith contrast-enhanced MDCT attenuation (HU), for var-
ous plaque components. Overall, for assessment of theon-calcified (47) components of the atherosclerotic plaque,including coronary, carotid, and aorta), the limited spatialesolution of contrast-enhanced MDCT will need to bemproved for better sensitivity and accuracy; in addition,
igure 3. Predicted seven-year event rates from Cox regression model fororonary heart disease death or non-fatal myocardial infarction (MI) forategories of Framingham Risk Score or coronary artery calcium scoreCACS). Reprinted with permission from Greenland et al. (33).
adiation dose will need to be reduced (35,40).

CMichihmrsocr
a(adMmd
tcbtcMtpw
M
BsacrMvi
Fiapp
reasedP et a
1212 Fuster et al. JACC Vol. 46, No. 7, 2005Atherothrombosis and High-Risk Plaque: Part II October 4, 2005:1209–18
oronary artery disease visualization by contrast-enhancedDCT. Results of a number of promising studies concern-
ng the use of contrast-enhanced MDCT for noninvasiveoronary angiography (computed tomography angiography)ave been published. It appears that the diagnostic accuracy
s reasonable (Fig. 5), but complete assessment can beindered by calcium deposits in the vessel wall and byotion artifacts, particularly in patients with high heart
ates (23,48–51). In case the heart rate of a patient isignificantly greater than 60 beats/min, the administrationf beta-blocker medication to slow down the heart isommonly used. Contrast-induced nephropathy could be aisk for some patients.
Studies with 16-slice scanners showed improved accuracys compared with previous reports with four-slice scanners52–54). These studies reported sensitivity of 73% to 95%nd specificity of 86% to 93%, for detection of obstructiveisease (Table 3). However, some of the contrast-enhancedDCT coronary angiography studies excluded approxi-ately 30% of coronary segments mainly because of image
egradation from cardiac motion. The image artifacts and
igure 4. Contrast-enhanced, 16 detector-row computed tomography anntensity projection along the course of the proximal left coronary artery shrtery (arrow). (B) A cross-sectional image reconstruction of the correspo
Table 1. Changes in 10-Year Risk According
Pre-test Probability of aCoronary Event Within
10 yrs (%)
Probab10 yrs Accord
Electron
Calcium Score >80
1.0 3.02.0 6.53.0 9.54.0 12.55.0 15.06.0 18.07.0 20.0
10.0 27.015.0 38.020.0 46.0
Pre-test probability of a coronary event within 10 years is decoronary event were calculated on the basis of the resuelectrocardiography. Please note that a 10% probability is incscore is �80. Reproduced with permission from Greenland
laque. (C) Using dedicated post-processing tools, the vessel can be stretched lolaque.
he number of excluded coronary segments may be signifi-antly reduced (to approximately 10%) by the use ofeta-blockers to minimize cardiac motion and careful pa-ient selection, which allows the imaging of the entireoronary tree within one breath hold. Improvements in
DCT using the 64-slice systems equipped with more andhinner detector rows and increased rotation speed have aotential to allow a more reliable coronary stenosis detectionith a very short scan time (55,56).
AGNETIC RESONANCE IMAGING
ecause atherothrombotic disease affects the entire arterialystem, simultaneous assessment of coronary and peripheralrteries to the distal runoff vessels has been proposed usingontrast-enhanced whole-body magnetic resonance angiog-aphy (MRA) (23,57). Most important, high-resolution
RI has emerged as the potential leading noninvasive inivo imaging modality for atherosclerotic plaque character-zation (13,14).
aphy of the coronary arteries in a 65-year-old patient. (A) Maximum-large non-calcified coronary artery plaque in the distal left main coronaryvessel region proves significant lumen obstruction due to the concentric
lcium Scores and Exercise Testing
ithino Results ofCT (%)
Probability Within10 yrs According toResults of Exercise
Electrocardiography(%)
Calcium Score <80 Abnormal Normal
0.2 4.0 0.40.4 8.0 0.90.6 12.0 1.30.9 15.0 1.91.0 19.0 2.31.2 22.0 2.81.4 25.0 3.32.2 33.0 4.83.4 44.0 7.44.8 52.0 10.0
rom the data on coronary risk factors. Other probabilities ofelectron-beam computed tomography (CT) or exercise
to 27% if a calcium score is �80 and reduced to 2.2% if thel. (34).
giogrows anding
to Ca
ility Wing t
Beam
rived flts of
ngitudinally and rotated in any direction for improved visualization of the
WMhrTcrpps
abaMStSn
TA
R
LFC
*
tpT
Ftsnc
T
4
1
1
F
1213JACC Vol. 46, No. 7, 2005 Fuster et al.October 4, 2005:1209–18 Atherothrombosis and High-Risk Plaque: Part II
hole-body contrast-enhanced MRA and coronaryRA. Magnetic resonance angiography was found to have
igh specificity and sensitivity compared with X-ray angiog-aphy for the detection of luminal narrowing �50% (57).oday, whole-body MRA excludes the intracranial and
oronary arteries, for which a dedicated examination is stillequired. Several coronary MRA techniques have beenroposed for the assessment of stenosis, anomalies, andatency of bypass grafts. T2-weighted navigator-gated fat-uppressed free-breathing gradient-echo sequences usually
able 2. Contrast at CT and MRI of Main Components oftherothrombotic Plaque
Sequence
CT (HU) MRI (SI*)
200† T1W PDW T2W TOF
ecentthrombus
20 � to � � to � � to � �
ipid 50 � � � �ibrous 100 � � � to � � to �alcium �300 � � � �
Signal intensity (SI) relative to adjacent muscle. †Vessel contrast enhancement.� � hyperintense; � � isointense; � � hypointense. CT � computed
omography; HU � Hounsfield unit; MRI � magnetic resonance imaging; PDW �roton density-weighted; TOF � time-of-flight; T1W � T1-weighted; T2W �2-weighted.
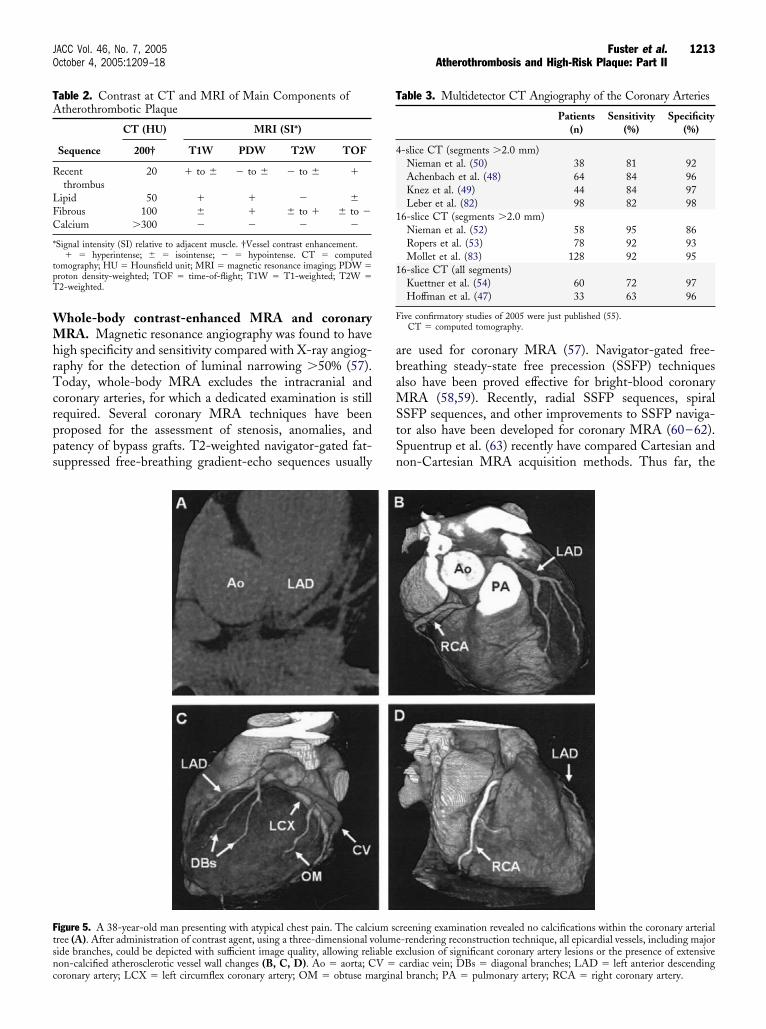
igure 5. A 38-year-old man presenting with atypical chest pain. The calciree (A). After administration of contrast agent, using a three-dimensional vide branches, could be depicted with sufficient image quality, allowing rel
on-calcified atherosclerotic vessel wall changes (B, C, D). Ao � aorta; CV �oronary artery; LCX � left circumflex coronary artery; OM � obtuse marginare used for coronary MRA (57). Navigator-gated free-reathing steady-state free precession (SSFP) techniqueslso have been proved effective for bright-blood coronary
RA (58,59). Recently, radial SSFP sequences, spiralSFP sequences, and other improvements to SSFP naviga-or also have been developed for coronary MRA (60–62).puentrup et al. (63) recently have compared Cartesian andon-Cartesian MRA acquisition methods. Thus far, the
reening examination revealed no calcifications within the coronary arterial-rendering reconstruction technique, all epicardial vessels, including majorxclusion of significant coronary artery lesions or the presence of extensive
able 3. Multidetector CT Angiography of the Coronary Arteries
Patients(n)
Sensitivity(%)
Specificity(%)
-slice CT (segments �2.0 mm)Nieman et al. (50) 38 81 92Achenbach et al. (48) 64 84 96Knez et al. (49) 44 84 97Leber et al. (82) 98 82 98
6-slice CT (segments �2.0 mm)Nieman et al. (52) 58 95 86Ropers et al. (53) 78 92 93Mollet et al. (83) 128 92 95
6-slice CT (all segments)Kuettner et al. (54) 60 72 97Hoffman et al. (47) 33 63 96
ive confirmatory studies of 2005 were just published (55).CT � computed tomography.
um scolumeiable e
cardiac vein; DBs � diagonal branches; LAD � left anterior descendingl branch; PA � pulmonary artery; RCA � right coronary artery.

sOdmwrRacppcbtscd(i
icmsceMcvasav
omMslsnfictioodtMc
aatntts�a(MasoTa7cfcsaa
FTcc
Fa
1214 Fuster et al. JACC Vol. 46, No. 7, 2005Atherothrombosis and High-Risk Plaque: Part II October 4, 2005:1209–18
ensitivity and specificity are quite promising (14,57,64).verall, it is likely that in the near future, and just for
iagnostic purposes, MRA will provide complete assess-ent of the systemic arterial tree, whereas noninvasive CTith intravenous injection of contrast medium may, in part,
eplace conventional diagnostic coronary angiography (14).egional high-spatial resolution MRI for plaque char-
cterization. Magnetic resonance differentiates plaqueomponents on the basis of biophysical and biochemicalarameters, such as chemical composition, water content,hysical state, molecular motion, or diffusion (57). Specifi-ally, recent improvements in MR techniques (e.g., black-lood MRI, faster imaging, and detection coils), conduciveo high-resolution and contrast imaging, have permitted thetudy of the different plaque components using multi-ontrast MR, generated by T1- and T2-weighted, proton-ensity-weighted, and time-of-flight imaging (Table 2)13,14,65,66). Moreover, MR provides imaging withoutonizing radiation and can be repeated over time.
Recent developments in MR imaging sequences havemproved the speed of acquisition, enabling rapid extendedoverage of aorta and carotid arteries (67). This develop-ent was accomplished by modifying existing double inver-
ion recovery black blood MRI. Improvements in receiveroil design (such as 8-channel carotid array) also havenabled high-resolution imaging of carotid arteries (68).
ulti-contrast imaging coupled with spatially enhancedluster analysis has allowed the quantitative evaluation ofarious plaque components (69). New, targeted contrastgents that are being developed to selectively image athero-clerotic plaques (70) and are currently being tested innimal models with new methods for nulling the blood with
igure 6. In vivo black-blood magnetic resonance imaging cross-sectional2-weighted image of a patient with a significant plaque in the right
arotid artery (arrow). The magnified image (bottom left) shows aomplex lipid-rich plaque.
ery short T1 relaxation time (71). In vivo characterizationaa
f aortic arch atherosclerosis in apolipoprotein E knockoutice transplant model has also been recently shown (72).RI studies of carotid artery plaques. Carotid arteries’
uperficial location and relative absence of motion presentess of a technical challenge. Some carotid plaque MRtudies (Fig. 6) showed the imaging and characterization oformal and pathological arterial walls (66,73), the quanti-cation of plaque size (74,75), and the assessment of fibrousap integrity (76). A strong association between fibrous caphinning or rupture, as determined by MR vessel wallmaging, and the history of recent transient ischemic attackr stroke was recently demonstrated (77). The MRA dem-nstrates the severity of stenotic lesions and their spatialistribution, whereas the high-resolution wall characteriza-ion technique may show the composition of the plaques.
RA and high-resolution MR imaging of the vessel wallan be combined (14).
Using a T1-weighted method, MR-direct thrombus im-ging sensitive to thrombus and methemoglobin, Moody etl. (78,79) studied patients suffering acute cerebral infarction orransient ischemic attacks and showed that a significantumber of them had a complicated carotid plaque ipsilateralo the side of their cerebral event that was corroborated inhe carotid endarterectomy specimens. Interestingly, in aignificant minority this occurred in vessels with stenoses50% to 70%. The occurrence of high signal material was
lso found in the contralateral side in 30% of these patients80).
RI studies of aortic plaques. The principal challengesssociated with MRI of the thoracic aorta are obtainingufficient sensitivity for submillimeter imaging and exclusionf artifacts caused by respiratory motion and blood flow.horacic aorta plaque composition and size have been
ssessed using high-resolution multi-contrast images (Fig.). Matched MRI and transesophageal echocardiographyross-sectional aortic segments showed a strong correlationor plaque thickness, whereas MRI was better for plaqueharacterization (81). In a recent study of asymptomaticubjects, the Framingham Heart Study showed by MRI thatortic plaque prevalence and burden (i.e., plaque volume/ortic volume) significantly increased with age and were
igure 7. In vivo black-blood magnetic resonance images of a patient withlarge plaque in the aortic arch (right panel) at the level of the descending
orta (left panel). The arrows indicate plaque. The asterisk indicates thereas of most prominent ulcerations.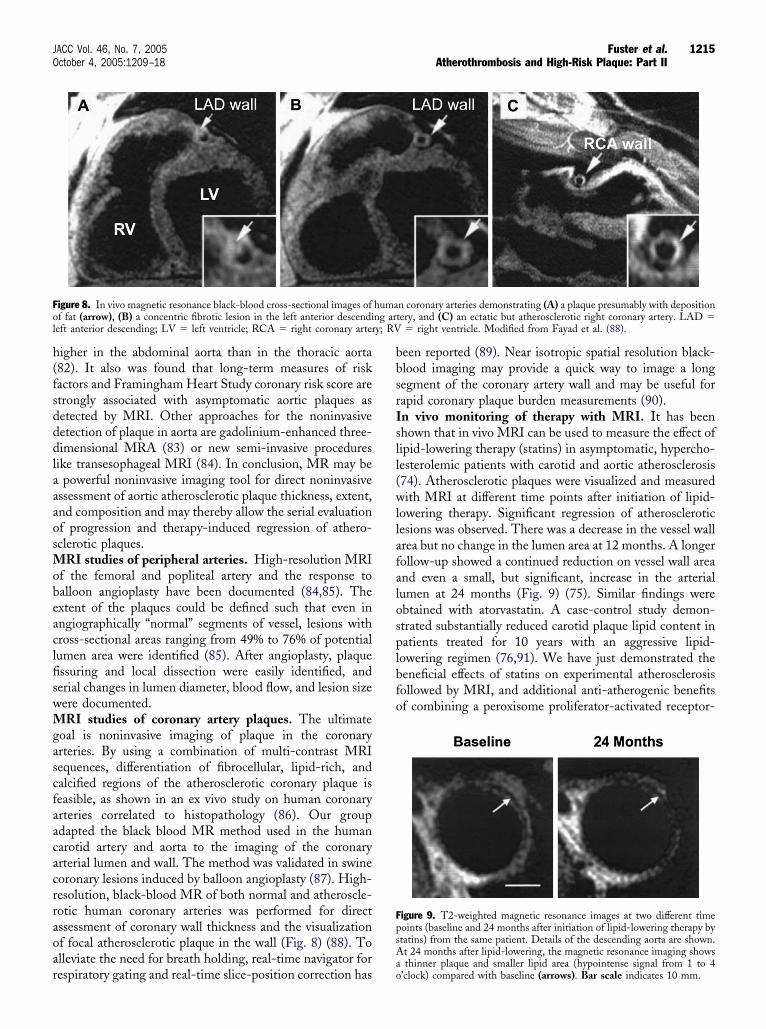
h(fsdddlaaaosMobeaclfiswMgascfaacacrraoar
bbsrIsll(wllafalosplbfo
Fol y; RV
FpsA
1215JACC Vol. 46, No. 7, 2005 Fuster et al.October 4, 2005:1209–18 Atherothrombosis and High-Risk Plaque: Part II
igher in the abdominal aorta than in the thoracic aorta82). It also was found that long-term measures of riskactors and Framingham Heart Study coronary risk score aretrongly associated with asymptomatic aortic plaques asetected by MRI. Other approaches for the noninvasiveetection of plaque in aorta are gadolinium-enhanced three-imensional MRA (83) or new semi-invasive procedures
ike transesophageal MRI (84). In conclusion, MR may bepowerful noninvasive imaging tool for direct noninvasive
ssessment of aortic atherosclerotic plaque thickness, extent,nd composition and may thereby allow the serial evaluationf progression and therapy-induced regression of athero-clerotic plaques.
RI studies of peripheral arteries. High-resolution MRIf the femoral and popliteal artery and the response toalloon angioplasty have been documented (84,85). Thextent of the plaques could be defined such that even inngiographically “normal” segments of vessel, lesions withross-sectional areas ranging from 49% to 76% of potentialumen area were identified (85). After angioplasty, plaquessuring and local dissection were easily identified, anderial changes in lumen diameter, blood flow, and lesion sizeere documented.RI studies of coronary artery plaques. The ultimate
oal is noninvasive imaging of plaque in the coronaryrteries. By using a combination of multi-contrast MRIequences, differentiation of fibrocellular, lipid-rich, andalcified regions of the atherosclerotic coronary plaque iseasible, as shown in an ex vivo study on human coronaryrteries correlated to histopathology (86). Our groupdapted the black blood MR method used in the humanarotid artery and aorta to the imaging of the coronaryrterial lumen and wall. The method was validated in swineoronary lesions induced by balloon angioplasty (87). High-esolution, black-blood MR of both normal and atheroscle-otic human coronary arteries was performed for directssessment of coronary wall thickness and the visualizationf focal atherosclerotic plaque in the wall (Fig. 8) (88). Tolleviate the need for breath holding, real-time navigator for
igure 8. In vivo magnetic resonance black-blood cross-sectional images off fat (arrow), (B) a concentric fibrotic lesion in the left anterior descendieft anterior descending; LV � left ventricle; RCA � right coronary arter
espiratory gating and real-time slice-position correction hasao
een reported (89). Near isotropic spatial resolution black-lood imaging may provide a quick way to image a longegment of the coronary artery wall and may be useful forapid coronary plaque burden measurements (90).n vivo monitoring of therapy with MRI. It has beenhown that in vivo MRI can be used to measure the effect ofipid-lowering therapy (statins) in asymptomatic, hypercho-esterolemic patients with carotid and aortic atherosclerosis74). Atherosclerotic plaques were visualized and measuredith MRI at different time points after initiation of lipid-
owering therapy. Significant regression of atheroscleroticesions was observed. There was a decrease in the vessel wallrea but no change in the lumen area at 12 months. A longerollow-up showed a continued reduction on vessel wall areand even a small, but significant, increase in the arterialumen at 24 months (Fig. 9) (75). Similar findings werebtained with atorvastatin. A case-control study demon-trated substantially reduced carotid plaque lipid content inatients treated for 10 years with an aggressive lipid-
owering regimen (76,91). We have just demonstrated theeneficial effects of statins on experimental atherosclerosisollowed by MRI, and additional anti-atherogenic benefitsf combining a peroxisome proliferator-activated receptor-
n coronary arteries demonstrating (A) a plaque presumably with depositiontery, and (C) an ectatic but atherosclerotic right coronary artery. LAD �
� right ventricle. Modified from Fayad et al. (88).
igure 9. T2-weighted magnetic resonance images at two different timeoints (baseline and 24 months after initiation of lipid-lowering therapy bytatins) from the same patient. Details of the descending aorta are shown.t 24 months after lipid-lowering, the magnetic resonance imaging shows
humang ar
thinner plaque and smaller lipid area (hypointense signal from 1 to 4’clock) compared with baseline (arrows). Bar scale indicates 10 mm.

gMfbtp
wiceccof
I
TttCcwdlp
RDN
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
1216 Fuster et al. JACC Vol. 46, No. 7, 2005Atherothrombosis and High-Risk Plaque: Part II October 4, 2005:1209–18
amma agonist with simvastatin (92). Overall, such role ofRI on the in vivo monitoring of therapies can be pivotal
or the better understanding of new pharmacological agentsefore undergoing clinical trials. It also can serve as a guideo assess the vascular wall response by individual patients toroven beneficial therapies.A clear distinction between imaging the coronary arteries,
hich move, and the larger arteries, which have less motion,s important when considering CT/MRI for research orlinical purposes. Evaluation of plaque composition byither technique is superior in larger arteries, includingarotids and the aorta. Despite of great advances with theoronaries, plaque characterization in the epicardial vesselsf the heart remains a challenge that requires further workor complete clinical application.
NTEGRATION OF NONINVASIVE CT AND MRI
ogether, CT and MRI may provide unique information,hus allowing the assessment of subclinical disease, athero-hrombotic progression, and its response to therapy (14,57).omputed tomography may first be used to localize suspi-
ious atherothrombotic lesions in the coronary arteriesithin a short scan time. Magnetic resonance angiographyoes the same in the systemic arteries, but within a much
onger scan time. Magnetic resonance imaging can thenroceed with tissue characterization of the problem sites.
eprint requests and correspondence: Dr. Pedro R. Moreno andr. Zahi A. Fayad, Mount Sinai School of Medicine, Box 1030,ew York, New York 10029. E-mail: [email protected].
EFERENCES
1. Fowkes FG, Housley E, Cawood EH, Macintyre CC, Ruckley CV,Prescott RJ. Edinburgh Artery Study: prevalence of asymptomatic andsymptomatic peripheral arterial disease in the general population. Int JEpidemiol 1991;20:384–92.
2. Coccheri S, Palareti G. The cardiovascular risk burden of intermittentclaudication. Eur Heart J 2002;4 Suppl B:B46–9.
3. Criqui MH, Denenberg JO, Langer RD, Fronek A. The epidemiologyof peripheral arterial disease: importance of identifying the populationat risk. Vasc Med 1997;2:221–6.
4. Leng GC, Fowkes FG, Lee AJ, Dunbar J, Housley E, Ruckley CV.Use of ankle brachial pressure index to predict cardiovascular eventsand death: a cohort study. BMJ 1996;313:1440–4.
5. Zheng ZJ, Sharrett AR, Chambless LE, et al. Associations of ankle-brachial index with clinical coronary heart disease, stroke and preclinicalcarotid and popliteal atherosclerosis: the Atherosclerosis Risk in Commu-nities (ARIC) study. Atherosclerosis 1997;131:115–25.
6. Jackson MR, Clagett GP. Antithrombotic therapy in peripheralarterial occlusive disease. Chest 2001;119:283S–99S.
7. Ogren M, Hedblad B, Isacsson SO, Janzon L, Jungquist G, LindellSE. Non-invasively detected carotid stenosis and ischaemic heartdisease in men with leg arteriosclerosis. Lancet 1993;342:1138–41.
8. Eagle KA, Rihal CS, Foster ED, Mickel MC, Gersh BJ. Long-termsurvival in patients with coronary artery disease: importance of periph-eral vascular disease. The Coronary Artery Surgery Study (CASS)Investigators. J Am Coll Cardiol 1994;23:1091–5.
9. Sutton-Tyrrell K, Rihal C, Sellers MA, et al. Long-term prognosticvalue of clinically evident noncoronary vascular disease in patients under-
going coronary revascularization in the Bypass Angioplasty Revascular-ization Investigation (BARI). Am J Cardiol 1998;81:375–81.0. Dormandy JA, Rutherford RB. Management of peripheral arterialdisease (PAD). TASC Working Group. TransAtlantic Inter-SocietyConsensus (TASC). J Vasc Surg 2000;31:S1–296.
1. Aronow WS, Ahn C. Prevalence of coexistence of coronary arterydisease, peripheral arterial disease, and atherothrombotic brain infarc-tion in men and women �62 years of age. Am J Cardiol 1994;74:64–5.
2. CAPRIE Steering Committee. A randomised, blinded, trial of Clo-pidogrel versus Aspirin in Patients at Risk of Ischaemic Events(CAPRIE). Lancet 1996;348:1329–39.
3. Fayad ZA, Fuster V. Clinical imaging of the high-risk or vulnerableatherosclerotic plaque. Circ Res 2001;89:305–16.
4. Fayad ZA, Fuster V, Nikolaou K, Becker C. Computed tomographyand magnetic resonance imaging for noninvasive coronary angiographyand plaque imaging: current and potential future concepts. Circulation2002;106:2026–34.
5. Stary HC. The development of calcium deposits in atheroscleroticlesions and their persistence after lipid regression. Am J Cardiol2001;88:16E–9E.
6. Schmermund A, Erbel R. Unstable coronary plaque and its relation tocoronary calcium. Circulation 2001;104:1682–7.
7. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte MJr., Detrano R. Quantification of coronary artery calcium usingultrafast computed tomography. J Am Coll Cardiol 1990;15:827–32.
8. O’Rourke RA, Brundage BH, Froelicher VF, et al. American Collegeof Cardiology/American Heart Association expert consensus docu-ment on electron-beam computed tomography for the diagnosis andprognosis of coronary artery disease. Circulation 2000;102:126–40.
9. Burke AP, Virmani R, Galis Z, Haudenschild CC, Muller JE. 34thBethesda Conference: task force 2—what is the pathologic basis fornew atherosclerosis imaging techniques? J Am Coll Cardiol 2003;41:1874–86.
0. Falk E, Shah PK, Fuster V. Coronary plaque disruption. Circulation1995;92:657–71.
1. Callister TQ, Cooil B, Raya SP, Lippolis NJ, Russo DJ, Raggi P.Coronary artery disease: improved reproducibility of calcium scoringwith an electron-beam CT volumetric method. Radiology 1998;208:807–14.
2. Hong C, Becker CR, Schoepf UJ, Ohnesorge B, Bruening R, ReiserMF. Coronary artery calcium: absolute quantification in nonenhancedand contrast-enhanced multi-detector row CT studies. Radiology2002;223:474–80.
3. Budoff MJ, Cohen MC, Garcia MJ, et al. ACCF/AHA clinicalcompetence statement on cardiac imaging with computed tomographyand magnetic resonance: a report of the American College of Cardi-ology Foundation/American Heart Association/American College ofPhysicians Task Force on Clinical Competence and Training. J AmColl Cardiol 2005;46:383–402.
4. Taylor AJ, Merz CN, Udelson JE. 34th Bethesda Conference:executive summary—can atherosclerosis imaging techniques improvethe detection of patients at risk for ischemic heart disease? J Am CollCardiol 2003;41:1860–2.
5. Wilson PW, Smith SC Jr., Blumenthal RS, Burke GL, Wong ND.34th Bethesda Conference: task force #4—how do we select patientsfor atherosclerosis imaging? J Am Coll Cardiol 2003;41:1898–906.
6. Raggi P, Cooil B, Callister TQ. Use of electron beam tomography datato develop models for prediction of hard coronary events. Am Heart J2001;141:375–82.
7. Budoff MJ, Achenbach S, Duerinckx A. Clinical utility of computedtomography and magnetic resonance techniques for noninvasive cor-onary angiography. J Am Coll Cardiol 2003;42:1867–78.
8. Wayhs R, Zelinger A, Raggi P. High coronary artery calcium scorespose an extremely elevated risk for hard events. J Am Coll Cardiol2002;39:225–30.
9. Raggi P, Callister TQ, Davidson M, et al. Aggressive versus moderatelipid-lowering therapy in postmenopausal women with hypercholes-terolemia: rationale and design of the Beyond Endorsed Lipid Low-ering with EBT Scanning (BELLES) trial. Am Heart J 2001;141:722–6.
0. Rumberger JA, Brundage BH, Rader DJ, Kondos G. Electron beamcomputed tomographic coronary calcium scanning: a review andguidelines for use in asymptomatic persons. Mayo Clin Proc 1999;74:
243–52.
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
6
7
7
7
7
7
1217JACC Vol. 46, No. 7, 2005 Fuster et al.October 4, 2005:1209–18 Atherothrombosis and High-Risk Plaque: Part II
1. Wang TJ, Larson MG, Levy D, et al. C-reactive protein is associatedwith subclinical epicardial coronary calcification in men and women:the Framingham Heart Study. Circulation 2002;106:1189–91.
2. Greenland P, Abrams J, Aurigemma GP, et al. Prevention ConferenceV: beyond secondary prevention: identifying the high-risk patient forprimary prevention: noninvasive tests of atherosclerotic burden: Writ-ing Group III. Circulation 2000;101:e16–22.
3. Greenland P, LaBree L, Azen SP, Doherty TM, Detrano RC.Coronary artery calcium score combined with Framingham score forrisk prediction in asymptomatic individuals. JAMA 2004;291:210–5.
4. Greenland P, Gaziano JM. Clinical practice. Selecting asymptomaticpatients for coronary computed tomography or electrocardiographicexercise testing. N Engl J Med 2003;349:465–73.
5. Thompson GR, Partridge J. Coronary calcification score: thecoronary-risk impact factor. Lancet 2004;363:557–9.
6. Taylor AJ, Bindeman J, Feuerstein I, et al. Coronary calcium inde-pendently predicts incident premature coronary heart disease overmeasured cardiovascular risk factors mean three-year outcomes in theProspective Army Coronary Calcium (PACC) Project. J Am CollCardiol 2005;46:807–14.
7. Schmermund A, Erbel R, Silber S. Age and gender distribution ofcoronary artery calcium measured by four-slice computed tomographyin 2,030 persons with no symptoms of coronary artery disease. Am JCardiol 2002;90:168–73.
8. Kopp AF, Ohnesorge B, Becker C, et al. Reproducibility and accuracyof coronary calcium measurements with multi-detector row versuselectron-beam CT. Radiology 2001;225:113–9.
9. Nasir K, Budoff MJ, Post WS, et al. Electron beam CT versus helicalCT scans for assessing coronary calcification: current utility and futuredirections. Am Heart J 2003;146:969–77.
0. Morin RL, Gerber TC, McCollough CH. Radiation dose in com-puted tomography of the heart. Circulation 2003;107:917–22.
1. Allison MA, Criqui MH, Wright CM. Patterns and risk factors forsystemic calcified atherosclerosis. Arterioscler Thromb Vasc Biol2004;24:331–6.
2. Executive summary of the third report of the National CholesterolEducation Program (NCEP) Expert Panel on Detection, Evaluation,and Treatment of High Blood Cholesterol in Adults (Adult Treat-ment Panel III). JAMA 2001;285:2486–97.
3. Nikolaou K, Sagmeister S, Knez A, et al. Multidetector-row computedtomography of the coronary arteries: predictive value and quantitativeassessment of non-calcified vessel-wall changes. Eur Radiol 2003;13:2505–12.
4. Schroeder S, Kuettner A, Kopp AF, et al. Noninvasive evaluation ofthe prevalence of noncalcified atherosclerotic plaques by multi-slicedetector computed tomography: results of a pilot study. Int J Cardiol2003;92:151–5.
5. Nieman K, van der Lugt A, Pattynama PM, de Feyter PJ. Noninvasivevisualization of atherosclerotic plaque with electron beam and multi-slice spiral computed tomography. J Interv Cardiol 2003;16:123–8.
6. Becker CR, Nikolaou K, Muders M, et al. Ex vivo coronary athero-sclerotic plaque characterization with multi-detector-row CT. EurRadiol 2003;13:2094–8.
7. Achenbach S, Moselewski F, Ropers D, et al. Detection of calcifiedand noncalcified coronary atherosclerotic plaque by contrast-enhanced,submillimeter multidetector spiral computed tomography: a segment-based comparison with intravascular ultrasound. Circulation 2004;109:14–7.
8. Achenbach S, Giesler T, Ropers D, et al. Detection of coronary arterystenoses by contrast-enhanced, retrospectively electrocardiographically-gated, multislice spiral computed tomography. Circulation 2001;103:2535–8.
9. Knez A, Becker CR, Leber A, et al. Usefulness of multislice spiralcomputed tomography angiography for determination of coronaryartery stenoses. Am J Cardiol 2001;88:1191–4.
0. Nieman K, Oudkerk M, Rensing BJ, et al. Coronary angiography withmulti-slice computed tomography. Lancet 2001;357:599–603.
1. Vogl TJ, Abolmaali ND, Diebold T, et al. Techniques for thedetection of coronary atherosclerosis: multidetector row CT coronaryangiography. Radiology 2002;223:212–20.
2. Nieman K, Cademartiri F, Lemos PA, Raaijmakers R, PattynamaPM, de Feyter PJ. Reliable noninvasive coronary angiography with fast
submillimeter multislice spiral computed tomography. Circulation2002;106:2051–4.3. Ropers D, Baum U, Pohle K, et al. Detection of coronary arterystenoses with thin-slice multi-detector row spiral computed tomogra-phy and multiplanar reconstruction. Circulation 2003;107:664–6.
4. Kuettner A, Kopp AF, Schroeder S, et al. Diagnostic accuracy ofmultidetector computed tomography coronary angiography in patientswith angiographically proven coronary artery disease. J Am CollCardiol 2004;43:831–9.
5. Schmermund A, Erbel R. Non-invasive computed tomographic cor-onary angiography: the end of the beginning. Eur Heart J 2005;15:1451–3.
6. Raff GL, Gallagher MJ, O’Neill WW. Diagnostic accuracy of noninvasivecoronary angiography using 64-slice spiral computed tomography. J AmColl Cardiol 2005;46:552–7.
7. Fuster V, Kim RJ. Frontiers in cardiovascular magnetic resonance.Circulation 2005;112:135–44.
8. Deshpande VS, Shea SM, Laub G, Simonetti OP, Finn JP, Li D. 3Dmagnetization-prepared true-FISP: a new technique for imagingcoronary arteries. Magn Reson Med 2001;46:494–502.
9. Shea SM, Deshpande VS, Chung YC, Li D. Three-dimensionaltrue-FISP imaging of the coronary arteries: improved contrast withT2-preparation. J Magn Reson Imaging 2002;15:597–602.
0. Yang PC, Meyer CH, Terashima M, et al. Spiral magnetic resonancecoronary angiography with rapid real-time localization. J Am CollCardiol 2003;41:1134–41.
1. Larson AC, White RD, Laub G, McVeigh ER, Li D, Simonetti OP.Self-gated cardiac cine MRI. Magn Reson Med 2004;51:93–102.
2. Larson AC, Simonetti OP, Li D. Coronary MRA with 3D under-sampled projection reconstruction TrueFISP. Magn Reson Med2002;48:594–601.
3. Spuentrup E, Katoh M, Buecker A, et al. Free-breathing 3D steady-state free precession coronary MR angiography with radial k-spacesampling: comparison with Cartesian k-space sampling and Cartesiangradient-echo coronary MR angiography—pilot study. Radiology2004;231:581–6.
4. Langerak SE, Vliegen HW, de Roos A, et al. Detection of vein graftdisease using high-resolution magnetic resonance angiography. Circu-lation 2002;105:328–33.
5. Choudhury RP, Fuster V, Badimon JJ, Fisher EA, Fayad ZA. MRI andcharacterization of atherosclerotic plaque: emerging applications andmolecular imaging. Arterioscler Thromb Vasc Biol 2002;22:1065–74.
6. Yuan C, Zhang SH, Polissar NL, et al. In vivo accuracy of multispec-tral magnetic resonance imaging for identifying lipid-rich necroticcores and intraplaque hemorrhage in advanced human carotid plaques.Circulation 2001;104:2051–6.
7. Mani V, Itskovich VV, Szimtenings M, et al. Rapid extended coveragesimultaneous multisection black-blood vessel wall MR imaging. Ra-diology 2004;232:281–8.
8. Itskovich VV, Mani V, Mizsei G, et al. Parallel and nonparallel simulta-neous multislice black-blood double inversion recovery techniques forvessel wall imaging. J Magn Reson Imaging 2004;19:459–67.
9. Itskovich VV, Samber DD, Mani V, et al. Quantification of humanatherosclerotic plaques using spatially enhanced cluster analysis ofmulticontrast-weighted magnetic resonance images. Magn Reson Med2004;52:515–23.
0. Lipinski M, Fuster V, Fisher E, Fayad ZA. Technology insight:targeting of biological molecules for evaluation of high-risk athero-sclerotic plaques with magnetic resonance imaging. Nat Cardiovasc2004;1:48–55.
1. Sirol M, Itskovich VV, Mani V, et al. Lipid-rich atheroscleroticplaques detected by gadofluorine-enhanced in vivo magnetic resonanceimaging. Circulation 2004;109:2890–6.
2. Trogan E, Fayad ZA, Itskovich VV, et al. Serial studies of mouseatherosclerosis by in vivo magnetic resonance imaging detect lesionregression after correction of dyslipidemia. Arterioscler Thromb VascBiol 2004;24:1714–9.
3. Toussaint JF, LaMuraglia GM, Southern JF, Fuster V, Kantor HL.Magnetic resonance images lipid, fibrous, calcified, hemorrhagic, andthrombotic components of human atherosclerosis in vivo. Circulation1996;94:932–8.
4. Corti R, Fayad ZA, Fuster V, et al. Effects of lipid-lowering bysimvastatin on human atherosclerotic lesions: a longitudinal study byhigh-resolution, noninvasive magnetic resonance imaging. Circulation
2001;104:249–52.
7
7
7
7
7
8
8
8
8
8
8
8
8
8
8
9
9
9
1218 Fuster et al. JACC Vol. 46, No. 7, 2005Atherothrombosis and High-Risk Plaque: Part II October 4, 2005:1209–18
5. Corti R, Fuster V, Fayad ZA, et al. Lipid lowering by simvastatininduces regression of human atherosclerotic lesions: two years’follow-up by high-resolution noninvasive magnetic resonance imag-ing. Circulation 2002;106:2884–7.
6. Zhao XQ, Yuan C, Hatsukami TS, et al. Effects of prolongedintensive lipid-lowering therapy on the characteristics of carotidatherosclerotic plaques in vivo by MRI: a case-control study. Arterio-scler Thromb Vasc Biol 2001;21:1623–9.
7. Yuan C, Zhang SH, Polissar NL, et al. Identification of fibrous caprupture with magnetic resonance imaging is highly associated with recenttransient ischemic attack or stroke. Circulation 2002;105:181–5.
8. Moody AR, Allder S, Lennox G, Gladman J, Fentem P. Directmagnetic resonance imaging of carotid artery thrombus in acute stroke.Lancet 1999;353:122–3.
9. Moody AR, Murphy RE, Morgan PS, et al. Characterization ofcomplicated carotid plaque with magnetic resonance direct thrombusimaging in patients with cerebral ischemia. Circulation 2003;107:3047–52.
0. Murphy RE, Moody AR, Morgan PS, et al. Prevalence of complicatedcarotid atheroma as detected by magnetic resonance direct thrombusimaging in patients with suspected carotid artery stenosis and previousacute cerebral ischemia. Circulation 2003;107:3053–8.
1. Fayad ZA, Nahar T, Fallon JT, et al. In vivo MR evaluation ofatherosclerotic plaques in the human thoracic corta: a comparison withTEE. Circulation 2000;101:2503–9.
2. Jaffer FA, O’Donnell CJ, Larson MG, et al. Age and sex distributionof subclinical aortic atherosclerosis: a magnetic resonance imagingexamination of the Framingham Heart Study. Arterioscler ThrombVasc Biol 2002;22:849–54.
3. Prince MR, Narasimham DL, Jacoby WT, et al. Three-dimensionalgadolinium-enhanced MR angiography of the thoracic aorta. AJRAm J Roentgenol 1996;166:1387–97.
4. Wyttenbach R, Gallino A, Alerci M, et al. Effects of percutaneous
remodeling of human femoropopliteal artery by noninvasive magneticresonance imaging. Circulation 2004;110:1156–61.
5. Coulden RA, Moss H, Graves MJ, Lomas DJ, Appleton DS,Weissberg PL. High resolution magnetic resonance imaging of ath-erosclerosis and the response to balloon angioplasty. Heart 2000;83:188–91.
6. Itskovich VV, Samber DD, Aguinaldo JG, et al. Quantification ofhuman coronary atherosclerotic plaques using cluster analysis ofmulticontrast-weighted magnetic resonance images. Magn Reson Med2004;52:15–23.
7. Worthley SG, Helft G, Fuster V, et al. Noninvasive in vivo magneticresonance imaging of experimental coronary artery lesions in a porcinemodel. Circulation 2000;101:2956–61.
8. Fayad ZA, Fuster V, Fallon JT, et al. Noninvasive in vivo humancoronary artery lumen and wall imaging using black-blood magneticresonance imaging. Circulation 2000;102:506–10.
9. Botnar RM, Stuber M, Kissinger KV, Manning WJ. Free-breathing3D coronary MRA: the impact of “isotropic” image resolution. J MagnReson Imaging 2000;11:389–93.
0. Kim WY, Stuber M, Bornert P, Kissinger KV, Manning WJ, BotnarRM. Three-dimensional black-blood cardiac magnetic resonance cor-onary vessel wall imaging detects positive arterial remodeling inpatients with nonsignificant coronary artery disease. Circulation 2002;106:296–9.
1. Yonemura A, Momiyama Y, Fayad ZA, et al. Effect of lipid-loweringtherapy with atorvastatin on atherosclerotic aortic plaques detected bynoninvasive magnetic resonance imaging. J Am Coll Cardiol 2005;45:733–42.
2. Corti R, Osende JI, Fallon JT, et al. The selective peroxisomalproliferator-activated receptor-gamma agonist has an additive effect onplaque regression in combination with simvastatin in experimentalatherosclerosis: in vivo study by high-resolution magnetic resonance
transluminal angioplasty and endovascular brachytherapy on vascular imaging. J Am Coll Cardiol 2004;43:464–73.




















