Evidence for a Strong Genetic Influence on Carotid Plaque Characteristics: An International Twin...
15
3168 C arotid artery plaques have been associated with multiple complications such as cardiovascular events, retinal or cerebral ischemia, 1 and all-cause mortality. 2,3 Brain or retinal ischemia can be attributable to microembolic dissemination from a complicated plaque or to the hemodynamic consequences of carotid occlusion. Moreover, complex, vulnerable plaques are frequently found in association with hypertension and diabetes, often in subjects without clinically overt cardiovascular disease. 4 The grade of carotid stenosis related to carotid plaques can be assessed by ultrasound, CT, MRI, or angiography. Carotid artery ultrasound is a well-established method to visualize and Background and Purpose—Few family studies reported moderate genetic impact on the presence and scores of carotid plaques. However, the heritability of carotid plaque characteristics remains still unclear. Twin studies more reliably estimate the relative contribution of genes to these traits in contrast to family study design. Methods—One hundred ninety-two monozygotic and 83 dizygotic adult twin pairs (age 49 ± 15 years) from Italy, Hungary, and the United States underwent B-mode and color Doppler ultrasound of bilateral common, internal, and external carotid arteries. Results—Age-, sex-, and country-adjusted heritability was 78% for the presence of carotid plaque (95% CI, 55%–90%), 74% for plaque echogenicity (hypoechoic, hyperechoic, or mixed; 95% CI, 38%–87%), 69% for plaque size (area in mm 2 in longitudinal plane; < or >50 percentile; 95% CI, 16%–86%), 74% for plaque sidedness (unilateral or bilateral; 95% CI, 25%–90%), 74% for plaque numerosity (95% CI, 26%–86%), 68% (95% CI, 40%–84%), and 66% (95% CI, 32%– 90%) for the presence of plaque in carotid bulbs and proximal internal carotid arteries. No role of shared environmental factors was found. Unique environmental factors were responsible for the remaining variance (22%–34%). Controlling for relevant covariates did not change the results significantly. Conclusions—The heritability of ultrasound characteristics of carotid plaque is high. Unshared environmental effects account for a modest portion of the variance. Our findings should stimulate the search for genes responsible for these traits. (Stroke. 2012;43:3168-3172.) Key Words: carotid atherosclerosis ◼ genetics ◼ plaque composition ◼ twin study Evidence for a Strong Genetic Influence on Carotid Plaque Characteristics An International Twin Study Adam Domonkos Tarnoki, MD*; Claudio Baracchini, MD, PhD*; David Laszlo Tarnoki, MD*; Pierleone Lucatelli, MD; Emanuele Boatta, MD; Chiara Zini, MD; Fabrizio Fanelli, MD, PhD, DSc; Andrea Agnes Molnar, MD, PhD; Giorgio Meneghetti, MD, PhD, DSc; Maria Antonietta Stazi, MSc; Emanuela Medda, BSc; Rodolfo Cotichini, BSc; Lorenza Nisticò, MD, PhD; Corrado Fagnani, BSc; Janos Osztovits, MD, PhD; Gyorgy Jermendy, MD, PhD, DSc; Istvan Preda, MD, PhD, DSc; Robert Gabor Kiss, MD, PhD; Julia Metneki, PhD; Tamas Horvath, MD; Giacomo Pucci, MD; Pal Bata, MD; Kinga Karlinger, MD, PhD; Levente Littvay, PhD; Viktor Berczi, MD, PhD, DSc; Zsolt Garami, MD; Giuseppe Schillaci, MD, PhD Received June 2, 2012; final revision received August 22, 2012; accepted August 27, 2012. From the Department of Radiology and Oncotherapy, Semmelweis University, Budapest, Hungary (A.D.T., D.L.T., P.B., K.K., V.B.); the Department of Neurosciences, School of Medicine, University of Padua, Padua, Italy (C.B., G.M.); the Vascular and Interventional Radiology Unit, Department of Radiological Sciences, Sapienza University of Rome, Rome, Italy (P.L., E.B., C.Z., F.F.); the Research Group for Inflammation Biology and Immunogenomics of Hungarian Academy of Sciences and Semmelweis University, Budapest, Hungary (A.A.M., I.P., R.G.); the Department of Cardiology, Military Hospital, Budapest, Hungary (A.A.M., I.P., R.G.); the Genetic Epidemiology Unit, National Centre of Epidemiology, Istituto Superiore di Sanità, Rome, Italy (M.A.S., E.M., R.C., L.N., C.F.); Bajcsy Zsilinszky Hospital, III, Department of Internal Medicine, Surveillance and Health Promotion, Budapest, Hungary (J.O., G.J.); the National Institute for Health Development, Budapest, Hungary (J.M.); the Institute of Human Physiology and Clinical Experimental Research, Semmelweis University, Budapest, Hungary (T.H.); Università degli Studi di Perugia, Unità di Medicina Interna, Ospedale “S. Maria,” Terni, Italy (G.P., G.S.); Central European University, Budapest, Hungary (L.L.); and The Methodist Hospital DeBakey Heart and Vascular Center, Houston, TX (Z.G.). *Drs Tarnoki and Baracchini contributed equally to this article. The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA.112. 666016/-/DC1. Correspondence to Adam Domonkos Tarnoki, MD, Department of Radiology and Oncotherapy, Semmelweis University, 78/a Ulloi St, Budapest, H-1082, Hungary. E-mail [email protected] © 2012 American Heart Association, Inc. Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.112.666016 by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on May 20, 2016 http://stroke.ahajournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Evidence for a Strong Genetic Influence on Carotid Plaque Characteristics: An International Twin...

3168
Carotid artery plaques have been associated with multiple complications such as cardiovascular events, retinal or
cerebral ischemia,1 and all-cause mortality.2,3 Brain or retinal ischemia can be attributable to microembolic dissemination from a complicated plaque or to the hemodynamic consequences of carotid occlusion. Moreover, complex,
vulnerable plaques are frequently found in association with hypertension and diabetes, often in subjects without clinically overt cardiovascular disease.4
The grade of carotid stenosis related to carotid plaques can be assessed by ultrasound, CT, MRI, or angiography. Carotid artery ultrasound is a well-established method to visualize and
Background and Purpose—Few family studies reported moderate genetic impact on the presence and scores of carotid plaques. However, the heritability of carotid plaque characteristics remains still unclear. Twin studies more reliably estimate the relative contribution of genes to these traits in contrast to family study design.
Methods—One hundred ninety-two monozygotic and 83 dizygotic adult twin pairs (age 49 ± 15 years) from Italy, Hungary, and the United States underwent B-mode and color Doppler ultrasound of bilateral common, internal, and external carotid arteries.
Results—Age-, sex-, and country-adjusted heritability was 78% for the presence of carotid plaque (95% CI, 55%–90%), 74% for plaque echogenicity (hypoechoic, hyperechoic, or mixed; 95% CI, 38%–87%), 69% for plaque size (area in mm2 in longitudinal plane; < or >50 percentile; 95% CI, 16%–86%), 74% for plaque sidedness (unilateral or bilateral; 95% CI, 25%–90%), 74% for plaque numerosity (95% CI, 26%–86%), 68% (95% CI, 40%–84%), and 66% (95% CI, 32%–90%) for the presence of plaque in carotid bulbs and proximal internal carotid arteries. No role of shared environmental factors was found. Unique environmental factors were responsible for the remaining variance (22%–34%). Controlling for relevant covariates did not change the results significantly.
Conclusions—The heritability of ultrasound characteristics of carotid plaque is high. Unshared environmental effects account for a modest portion of the variance. Our findings should stimulate the search for genes responsible for these traits. (Stroke. 2012;43:3168-3172.)
Key Words: carotid atherosclerosis ◼ genetics ◼ plaque composition ◼ twin study
Evidence for a Strong Genetic Influence on Carotid Plaque Characteristics
An International Twin Study
Adam Domonkos Tarnoki, MD*; Claudio Baracchini, MD, PhD*; David Laszlo Tarnoki, MD*; Pierleone Lucatelli, MD; Emanuele Boatta, MD; Chiara Zini, MD; Fabrizio Fanelli, MD, PhD, DSc; Andrea Agnes Molnar, MD, PhD; Giorgio Meneghetti, MD, PhD, DSc; Maria Antonietta Stazi, MSc; Emanuela Medda, BSc; Rodolfo Cotichini, BSc; Lorenza Nisticò, MD, PhD; Corrado Fagnani, BSc;
Janos Osztovits, MD, PhD; Gyorgy Jermendy, MD, PhD, DSc; Istvan Preda, MD, PhD, DSc; Robert Gabor Kiss, MD, PhD; Julia Metneki, PhD; Tamas Horvath, MD; Giacomo Pucci, MD;
Pal Bata, MD; Kinga Karlinger, MD, PhD; Levente Littvay, PhD; Viktor Berczi, MD, PhD, DSc; Zsolt Garami, MD; Giuseppe Schillaci, MD, PhD
Received June 2, 2012; final revision received August 22, 2012; accepted August 27, 2012.From the Department of Radiology and Oncotherapy, Semmelweis University, Budapest, Hungary (A.D.T., D.L.T., P.B., K.K., V.B.); the Department
of Neurosciences, School of Medicine, University of Padua, Padua, Italy (C.B., G.M.); the Vascular and Interventional Radiology Unit, Department of Radiological Sciences, Sapienza University of Rome, Rome, Italy (P.L., E.B., C.Z., F.F.); the Research Group for Inflammation Biology and Immunogenomics of Hungarian Academy of Sciences and Semmelweis University, Budapest, Hungary (A.A.M., I.P., R.G.); the Department of Cardiology, Military Hospital, Budapest, Hungary (A.A.M., I.P., R.G.); the Genetic Epidemiology Unit, National Centre of Epidemiology, Istituto Superiore di Sanità, Rome, Italy (M.A.S., E.M., R.C., L.N., C.F.); Bajcsy Zsilinszky Hospital, III, Department of Internal Medicine, Surveillance and Health Promotion, Budapest, Hungary (J.O., G.J.); the National Institute for Health Development, Budapest, Hungary (J.M.); the Institute of Human Physiology and Clinical Experimental Research, Semmelweis University, Budapest, Hungary (T.H.); Università degli Studi di Perugia, Unità di Medicina Interna, Ospedale “S. Maria,” Terni, Italy (G.P., G.S.); Central European University, Budapest, Hungary (L.L.); and The Methodist Hospital DeBakey Heart and Vascular Center, Houston, TX (Z.G.).
*Drs Tarnoki and Baracchini contributed equally to this article.The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA.112.
666016/-/DC1.Correspondence to Adam Domonkos Tarnoki, MD, Department of Radiology and Oncotherapy, Semmelweis University, 78/a Ulloi St, Budapest,
H-1082, Hungary. E-mail [email protected]© 2012 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.112.666016
by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from

Tarnoki et al Genetic Impact on Carotid Plaque Characteristics 3169
quantify atherosclerotic lesions (composition, vascularization, thickness of cap, plaque motion, and ulceration) and its vul-nerability.3,5,6 The ultrasonographically determined composi-tion of carotid plaques was reported to be a better predictor of adverse events than plaque size.7 In particular, echo-lucent lipid-rich, histologically “soft” plaques are associated with more complications compared with calcified or mixed plaques.3,6 Heterogeneous plaques including a hypoechoic component are associated with frequent intraplaque hemor-rhage, ulceration, and adverse cardiovascular events.8–10
The underlying atherosclerotic phenotypes associated with carotid plaque formation (eg, intima-media thickness, grade of stenosis, arterial stiffness) have moderate heritability accord-ing to multiple studies,11–14 but the genetic effects related directly to carotid plaque characteristics remain unclear. The aim of our study was to assess the heritability of carotid plaque characteristics in a twin population.
Materials and MethodsSubjects and Study DesignTwo hundred seventy-five white Italian, Hungarian, and American adult twin pairs (192 monozygotic and 83 dizygotic; age 49 ± 15.5 years, mean±SD) were recruited in this classical twin study. Twin pairs from other ethnicities were not involved in the study. Opposite-sex dizygotic twin pairs were excluded because their inclusion could bias the heritability estimates upward in the presence of sex-specific environmental or X chromosome effects, which could not be modeled because of a limited statistical power. Additional exclusion criteria were pregnancy and individuals with past carotid surgery. Zygosity was assigned according to a 7-part self-reported response.15,16 The re-search was conducted in accordance with the Declaration of Helsinki; the local ethical committees approved the study and all subjects gave informed consent before study entry. All subjects were restricted from smoking for 3 hours, from eating for 1 hour, and from drinking alcohol or coffee for 10 hours before measurements. See more details in the Supplemental Data.
Carotid UltrasonographyThe measurement of carotid ultrasound was performed by B-mode and color Doppler ultrasound with linear array high-frequency (5–10 MHz) transducers (in Rome: Esaote Technos MPX, in Padua: Philips iU22, in Perugia: Esaote Technos MP, in Hungary: Toshiba Power Vision and Esaote Mylab40, in the United States: Sonosite Titan). Sonographers were professional internists, neurologists, or radiolo-gists. Bilateral carotid arteries were assessed from the origin of the common carotid artery until the proximal 3 to 4 cm of the internal and external carotid arteries. Carotid plaque was defined as an endolumi-nal protrusion of at least 1.5 mm or a focal thickening >50% of the intima-media thickness relative to the adjacent wall segment.17 The investigators assessed bilaterally the presence, sidedness, number of carotid plaques, and their size (mm2) on common carotid artery, proximal internal carotid artery, and external carotid artery. See more details in the Supplemental Data.
Statistical AnalysisDescriptive analysis (mean±SD for continuous variables, percentage for categorical variables) for age, zygosity, smoking history, body mass index, and the investigated carotid plaque characteristics was conducted using SPSS (SPSS 17.0 for Windows; SPSS, Chicago, IL). Differences among sex, zygosity, and countries were calculat-ed using independent-sample t tests. P value <0.05 was considered significant. Due to the zero-inflated distribution of the plaque area values, 3 categories were created and analyzed as ordinal: no plaque and < or >50 percentile. To investigate whether the anthropometric
or cardiovascular risk factors have a substantial influence on the ca-rotid plaque parameters beyond age, sex, and country, bivariate probit regression analyses were performed. The corresponding covariates have been added to the list of possibly relevant covariates in the heri-tability models. A descriptive estimate of the genetic influence was calculated using the within-pair correlation in monozygotic and di-zygotic twin pairs with the corresponding bootstrapped 95% CIs.18 Structural equation modeling was used to estimate heritability using the Mplus Version 6.1 (Muthén and Muthén) weighted least squares estimation due to the categorical nature of variables of interest.19 Empirical CIs were calculated with a Bollen-Stine bootstrap proce-dure.20 For each phenotype 2 ACE models were estimated. Model 1 follows convention and corrects for the twins’ age, sex, and country. Model 2, in addition to age, sex, and country, also corrects for all risk factors with a significant relationship. These results tell us the impact of genes and of the environment after the influence of known risk factors is controlled for. See more details in the Supplemental Data.
ResultsClinical CharacteristicsSupplemental Table 1 presents clinical characteristics of the study population by zygosity, sex, and country. Seventy per-cent of the twins were monozygotic. Dizygotic twins were older and had higher active smoking rate (P<0.05). Seventy-one percent of the subjects were female. Carotid plaque prev-alence and size and body mass index were higher in males compared with females (all P<0.05). Significant differences were detected for age of participants, plaque area, and smok-ing rate across countries (P<0.05). These differences were taken into account in cotwin correlation estimation and quan-titative genetic models by regressing out age, sex, country (in Model 1), and significant covariates (in Model 2).
The age, sex, country, zygosity, and family corrected pro-bit regression coefficients of the investigated carotid plaque characteristics with anthropometric measurements and car-diovascular risk factors are shown in Supplemental Table 2. Some carotid plaque characteristics, smoking, and age showed a positive relationship. On the other hand, no associa-tion (2 exceptions: presence of carotid plaque and diabetes; plaque sidedness and hyperlipidemia) was observed between carotid plaque characteristics and sex, country, body mass index, central blood pressure, diabetes, and hyperlipidemia (Supplemental Table 2).
Heritability AnalysisCotwin correlations as well as genetic and environmen-tal proportions of variance, and their 95% CIs, are shown in the Table. In Model 1 (with only age, sex, and country adjusted for), additive genetic factors appear to contribute highly to all investigated carotid plaque phenotypes: 78.0% for the presence of carotid plaque (95% CI, 54.5%–90.3%), 74.3% for plaque echogenicity (95% CI, 38.3%–87.3%), 69.8% for plaque area (95% CI, 15.5%–85.9%), 74.0% for plaque sidedness (95% CI, 25.4%–89.8%), 73.5% for plaque numerosity (95% CI, 26.0%–86.2%), and 67.5% (95% CI, 40.4%–84.0%) and 66.0% (95% CI, 32.3%–90.2%) for the presence of plaques in carotid bulbs and proximal inter-nal carotid arteries. No role of shared environmental factors was found. Unshared environmental effects accounted for the additional minor part of the variance (22.0%–34.0%).
by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from

3170 Stroke December 2012
In multivariable-adjusted heritability estimates (Model 2 ACE), the magnitude of the genetic and environmental effects has not changed significantly.
DiscussionTo the best of our knowledge, this is the first study that inves-tigated heritability of carotid plaque characteristics (presence, numerosity, sidedness echogenicity, area) in an international twin population. We have shown that heritability is high and the influence of unique environmental factors is moderate.
Only few studies have investigated, indeed partially, the genetic determinants of carotid plaque characteristics.12,21,22 Moskau et al12 reported no genetic base for the carotid plaque score but demonstrated a moderate heritability of maximal carotid stenosis using a family study design; however, the sample size was small. A moderate (23%–28%) heritability of the presence of carotid plaques was reported in the San Antonio Family Heart Study.21 Their analysis was limited to the largest plaque identified in either the carotid bulb or inter-nal carotid artery only; this might explain the lower heritability compared with our findings. Twenty-eight percent heritability of the carotid plaque score was found in the Erasmus Rucphen Family study by measuring the common carotid artery, carotid bifurcation, and internal carotid artery.22
It must be taken into consideration that the family design is useful in the determination of intergeneration resemblance or difference, but in contrast to the twin study design, it does not tangibly express outside factors such as family environment and culture.23 Family studies, especially the ones limited to 2 generations, make more assumptions than the classical twin design concerning the sources of within-family transmission of a trait. Two-generation studies cannot reliably distinguish heritability from vertical cultural transmission and 3-generation designs still make several assumptions about the family environment. Our twin study reports higher genetic
heritability than the cited family studies on additional key carotid plaque phenotypes. Our findings indicate that common environmental factors are not responsible for the total variance of these phenotypes, whereas unshared environmental factors affecting individual twins separately have a moderate impact. One possible explanation for the sizably higher heritability of the study at hand is better plaque measurements thanks to more advanced ultrasound devices.
A genomewide linkage analysis obtained a bit higher heri-tability estimates for plaque presence (50%),24 yet these kind of studies usually underreport heritability.25,26 Noteworthy, their heritability CIs overlapped with ours. The same study identified loci on chromosomes 11p15, 14q32, and 15q23, which might influence heritability and stated that the SOX6 gene within the bone morphogenic protein pathway could be a candidate for carotid plaque formation.24 The heterogeneity of percentage heritability reported in the various studies might derive from dissimilar study designs, different study popula-tions, adjustments for various covariates, and population-spe-cific environmental contributions to the phenotypic variances. Key findings of the family, twin, and genomewide linkage analysis studies investigating carotid plaque heritability are summarized in Supplemental Table 3.
In our study, heritability of carotid plaque characteristics was much higher than previously reported in family studies, ranging between 66% and 78%.12,21,22 We hypothesized that the genetic influence on these traits might be similar to other functional and structural parameters of the arterial wall such as arterial stiffness (characterized by carotid pulse wave veloc-ity or augmentation index), central blood pressure, or carotid intima-media thickness11,13,14 or to some cardiometabolic risk factors, which are known to be moderately heritable.27–29 In a previous work, we investigated the heritability of vascular parameters on a smaller twin cohort and found that low to moderate genetic variance is responsible for the determination of these traits with heritabilities ranging between 0% and 38%
Table. Cotwin Correlations and Genetic and Environmental Variance Components as Estimated Under the Univariate ACE Models in Percentage
Twin Correlations Variance Components
Measure Models rMZ rDZ A C E
Presence of carotid plaque
Model 1 ACEModel 2 ACE
0.788 (0.560–0.914)0.802 (0.537–0.928)
0.205 (–0.610 to 0.719)0.208 (–0.771 to 1.000)
78.0% (54.5–90.3)79.2% (54.2–92.0)
0.0% (0.0–0.0)0.0% (0.0–0.0)
22.0% (9.6–44.7)20.8% (8.0–44.9)
Plaque composition Model 1 ACEModel 2 ACE
0.754 (0.553–0.876)0.715 (0.522–0.855)
0.121 (–0.426 to 0.519)0.114 (–0.450 to 0.615)
74.3% (38.3–87.3)70.4% (36.8–84.3)
0.0% (0.0–0.0)0.0% (0.0–75.9)
25.7% (13.3–45.0)29.6% (16.1–48.5)
Plaque area* Model 1 ACE† 0.698 (0.448–0.837) 0.258 (–0.499 to 0.798) 69.1% (15.5–85.9) 0.0% (0.0–39.3) 30.9% (17.3–52.7)
Plaque sidedness Model 1 ACEModel 2 ACE
0.741 (0.531–0.852)0.700 (0.503–0.834)
0.346 (–0.218 to 0.738)0.402 (–0.224 to 0.990)
74.0% (25.4–89.8)59.7% (0.0–81.0)
0.0% (0.0–68.9)10.3% (0.0–77.9)
26.0% (14.6–45.5)30.0% (16.0–48.2)
Plaque quantity Model 1 ACEModel 2 ACE
0.745 (0.564–0.835)0.726 (0.541–0.840)
0.267 (–0.421 to 0.652)0.264 (–0.467 to 0.661)
73.5% (26.0–86.2)71.4% (34.9–91.1)
0.0% (0.0–48.8)0.0% (0.0–73.3)
26.5% (17.2–42.8)28.6% (16.7–43.7)
Presence of plaque in carotid bulbs
Model 1 ACEModel 2 ACE
0.708 (0.459–0.877)0.740 (0.416–0.874)
–0.259 (–1.000 to 0.281)–0.176 (–1.000 to 0.442)
67.5% (40.4–84.0)71.6% (9.4–86.6)
0.0% (0.0–0.0)0.0% (0.0–0.0)
32.5% (16.1–56.8)28.4% (14.0–54.1)
Presence of plaque in internal carotid arteries
Model 1 ACEModel 2 ACE
0.667 (0.337–0.841)0.625 (0.316–0.804)
0.228 (–0.998 to 1.000)0.193 (–1.019 to 0.760)
66.0% (32.3–90.2)61.7% (32.7–83.9)
0.0% (0.0–0.0)0.0% (0.0–53.1)
34.0% (13.7–57.9)38.3% (16.1–63.0)
Model 1 results are age-, sex-, and country-adjusted. Model 2 results, in addition, adjust for significant covariates. Numbers in parentheses are 95% CIs. rMZ indicates monozygotic correlation; rDZ, dizygotic correlation; A, heritability; C, shared environmental variance component; E, unique environmental variance component.
*Based on 240 twin pairs only (American subjects not included in the analysis).†No Model 2 because none of the covariates was significant.
by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from

Tarnoki et al Genetic Impact on Carotid Plaque Characteristics 3171
for segment-specific carotid intima-media thickness, 45% for brachial augmentation index, and 42% for aortic pulse wave velocity assessed by oscillometry (TensioMed Arteriograph).13 In contrast to those heritability estimates, in the present study we found an unexpectedly high genetic influence on the inves-tigated carotid plaque traits. Of note, we found no influence of additional cardiovascular and anthropometric covariates on the heritability analyses (Model 2 ACE). The Healthy Twin Study provided evidence for segment-specific heritability of carotid intima-media thickness (heritability of intima-media thickness was 48% for common, 38% for carotid bifurcation, and 45% for internal carotid artery, respectively) and a shared genetic variation was reported on the 3 carotid segments.30 Therefore, we also investigated whether the presence of carotid plaques are segment-specific in our sample. Because the number of plaques on the proximal common and external carotid arteries was too low, only the heritability of the carotid plaques in the bulbs and proximal internal carotid arteries was calculated, which indicated also higher heritability estimates (67.5% and 66.0%, respectively). These findings should stim-ulate the search for novel genes responsible for these promis-ing candidate phenotypes in atherosclerosis.
Only 1 twin study has dealt with plaques so far, namely cal-cified aortic plaques assessed by CT, and reported a similarly high heritability (61%).30 In addition, Cecelja and coworkers31 suggested that the association between aortic wall calcifica-tion and increased arterial stiffness is explained by a common genetic background.
If our finding of a high genetic determinacy of carotid plaque characteristics is confirmed by future studies, carotid ultrasound might represent a very useful screening method in individuals with a family history of early cardio- and cere-brovascular events. A worldwide epidemic of cerebrovascu-lar disease has been anticipated32 and ultrasound evidence of carotid artery wall thickening or plaque is considered a key measure of target organ damage in hypertensive subjects.33 In addition, arterial stiffness assessment might be helpful in identifying high-risk individuals, because atherosclerotic plaque formation can be genetically associated with arterial stiffening.31
On the other hand, our study shows that environmental con-tribution has a moderate role in preventing, delaying, or atten-uating carotid plaque formation. The “traditional” concept of the deterministic role of individual-specific modifiable envi-ronmental factors such as smoking, unhealthy nutrition, or reduced physical activity34,35 still remains important, because in societies where everyone is exposed to cardiovascular risk factors, genetics will become relatively more important in determining who will be affected by carotid atherosclero-sis (ie, high heritability), yet management of cardiovascular risk factors remains the cornerstone to eradicating this dis-ease, because these risk factors might be necessary for the disease to appear. Accordingly, these environmental factors might contribute to the atherosclerotic plaque composition and vulnerability modestly. However, environmental factors might be more relevant in genetically susceptible individuals, and therefore gene×environment interactions—not modeled here for reasons of power—should be investigated in future studies.
Potential limitations of our study should be considered: (1) carotid plaque size was assessed only in 2 dimensions; (2) the proportion of dizygotic twins was relatively small compared with other twin studies, which may lead to biased estimates in quantitative genetic analysis; (3) carotid ultrasound reading was not blinded to monozygotic/dizygotic status, which may increase our heritability estimates; (4) the study was carried out in cohorts of different ethnicity. However, no evidence of heterogeneity between countries was detected, and all the analyses were adjusted for country; (5) the unique environ-mental factor (E) category can be biased upward by random measurement error; and (6) the sample size did not allow us to test for sex differences in genetic and environmental vari-ance components or to explore gene×environment interactive effects.
ConclusionOur study showed for the first time in adult twins that the heritability of the key carotid plaque characteristics is high. Unshared environmental effects account for a modest portion of the variance. These findings, if validated by other laboratories, should stimulate the search for genes responsible for these traits.
AcknowledgmentsWe acknowledge the support of the Twins Days Festival committee and Stephen F. Luczek, MD, for the American part of the study.
Sources of FundingMedexpert Ltd has provided financial support for the development and maintenance of this study (financial support for the American and Perugian measurements). The Italian part of the research was sup-ported by the Balassi Institute–Hungarian Scholarship Board Office, Foreign Affairs of Republic of Italy.
DisclosuresDr Tarnoki received travel reimbursement from Medexpert Ltd (American and Perugian measurements). Dr Garami is in the advi-sory board of Edwards (TAVI) and W.L. Gore (CAS-TCD).
References 1. Hollander M, Bots ML, Del Sol AI, Koudstaal PJ, Witteman JC, Grobbee
DE, et al. Carotid plaques increase the risk of stroke and subtypes of cerebral infarction in asymptomatic elderly: the Rotterdam study. Circulation. 2002;105:2872–2877.
2. Lernfelt B, Forsberg M, Blomstrand C, Mellström D, Volkmann R. Cerebral atherosclerosis as predictor of stroke and mortality in represen-tative elderly population. Stroke. 2002;33:224–229.
3. Joakimsen O, Bonaa KH, Mathiesen EB, Stensland-Bugge E, Arnesen E. Prediction of mortality by ultrasound screening of a general population for carotid stenosis: the Tromsø Study. Stroke. 2000;31:1871–1876.
4. Vicenzini E, Ricciardi MC, Puccinelli F, Altieri M, Vanacore N, Di Piero V, et al. Sonographic carotid plaque morphologic characteristics and vascular risk factors: results from a population study. J Ultrasound Med. 2008;27:1313–1319.
5. von Reutern GM, Goertler MW, Bornstein NM, Del Sette M, Evans DH, Hetzel A, et al; Neurosonology Research Group of the World Federation of Neurology. Grading carotid stenosis using ultrasonic methods. Stroke. 2012;43:916–921.
6. Grønholdt ML, Nordestgaard BG, Schroeder TV, Vorstrup S, Sillesen H. Ultrasonic echolucent carotid plaques predict future strokes. Circulation. 2001;104:68–73.
7. Falk E. Why do plaques rupture? Circulation. 1992;86(suppl):III30–III42.
by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from

3172 Stroke December 2012
8. Reilly LM, Lusby RJ, Hughes L, Ferrell LD, Stoney RJ, Ehrenfeld WK. Carotid plaque histology using real-time ultrasonography. Clinical and therapeutic implications. Am J Surg. 1983;146:188–193.
9. AbuRahma AF, Wulu JT Jr, Crotty B. Carotid plaque ultrasonic hetero-geneity and severity of stenosis. Stroke. 2002;33:1772–1775.
10. Geroulakos G, Hobson RW, Nicolaides A. Ultrasonographic carotid plaque morphology in predicting stroke risk. Br J Surg. 1996;83:582–587.
11. Franklin SS, Lopez VA, Wong ND, Mitchell GF, Larson MG, Vasan RS, et al. Single versus combined blood pressure components and risk for cardiovascular disease: the Framingham Heart Study. Circulation. 2009;119:243–250.
12. Moskau S, Golla A, Grothe C, Boes M, Pohl C, Klockgether T. Heritability of carotid artery atherosclerotic lesions: an ultrasound study in 154 families. Stroke. 2005;36:5–8.
13. Tarnoki AD, Tarnoki DL, Stazi MA, Medda E, Cotichini R, Fagnani C, et al. Twins lead to the prevention of atherosclerosis. Preliminary find-ings of International twin study 2009. J Vasc Ultras. 2011;35:61–71.
14. Tarnoki AD, Tarnoki DL, Stazi MA, Medda E, Cotichini R, Nisticò L, et al. Heritability of central blood pressure and arterial stiffness: a twin study. J Hypertens. 2012;30:1564–1571.
15. Heath AC, Nyholt DR, Neuman R, Madden PA, Bucholz KK, Todd RD, et al. Zygosity diagnosis in the absence of genotypic data: an approach using latent class analysis. Twin Res. 2003;6:22–26.
16. Fagnani C, Brescianini S, Cotichini R, D’Ippolito C, Dukic T, Giannantonio L, et al. The Italian Twin Register: new cohorts and tools, current projects and future perspectives of a developing resource. Twin Res Hum Genet. 2006;9:799–805.
17. Kobayashi E, Ono J, Hirai S, Yamakami I, Saeki N, Yamaura A. Detection of unstable plaques in patients with carotid stenosis using B-mode ultra-sonography. Interv Neuroradiol. 2000;6(suppl 1):165–170.
18. Neale MC, Cardon LR. Methodology for Genetic Studies of Twins and Families. Dordrecht, The Netherlands: Kluwer Academic; 1992.
19. Muthén LK, Muthén BO. Mplus User’s Guide. 6th ed. Los Angeles, CA: Muthén and Muthén; 1998–2010.
20. Bollen KA, Stine RA. Bootstrapping goodness-of-fit measures in structural equation models. Sociological Methods and Research. 1992;201:205–229.
21. Hunt KJ, Duggirala R, Göring HH, Williams JT, Almasy L, Blangero J, et al. Genetic basis of variation in carotid artery plaque in the San Antonio Family Heart Study. Stroke. 2002;33:2775–2780.
22. Sayed-Tabatabaei FA, van Rijn MJ, Schut AF, Aulchenko YS, Croes EA, Zillikens MC, et al. Heritability of the function and structure of the arte-rial wall: findings of the Erasmus Rucphen Family (ERF) study. Stroke. 2005;36:2351–2356.
23. Susser M, Susser E. Indicators and designs in genetic epidemiology: separating heredity and environment. Rev Epidemiol Sante Publique. 1987;35:54–77.
24. Dong C, Beecham A, Slifer S, Wang L, Blanton SH, Wright CB, et al. Genomewide linkage and peakwide association analyses of carotid plaque in Caribbean Hispanics. Stroke. 2010;41:2750–2756.
25. Vineis P, Pearce N. Missing heritability in genome-wide association study research. Nat Rev Genet. 2010;11:589.
26. Eichler EE, Flint J, Gibson G, Kong A, Leal SM, Moore JH, et al. Missing heritability and strategies for finding the underlying causes of complex disease. Nat Rev Genet. 2010;11:446–450.
27. Bouchard C, Tremblay A. Genetic effects in human energy expenditure components. Int J Obes. 1990;14(suppl 1):49–55; discussion 55–58.
28. Jermendy G, Horváth T, Littvay L, Steinbach R, Jermendy AL, Tárnoki AD, et al. Effect of genetic and environmental influences on cardiometa-bolic risk factors: a twin study. Cardiovasc Diabetol. 2011;10:96.
29. Jermendy G, Littvay L, Steinbach R, Jermendy A, Tárnoki A, Tárnoki D, et al. [Heritability of the risk factors characteristic for the meta-bolic syndrome: a twin study] [in Hungarian]. Orv Hetil. 2011;152: 1265–1271.
30. Lee K, Sung J, Lee SC, Park SW, Kim YS, Lee JY, et al. Segment-specific carotid intima-media thickness and cardiovascular risk factors in Koreans: the Healthy Twin Study. Eur J Cardiovasc Prev Rehabil. 2012;19:1161–1172.
31. Cecelja M, Jiang B, Bevan L, Frost ML, Spector TD, Chowienczyk PJ. Arterial stiffening relates to arterial calcification but not to non-calcified atheroma in women. A twin study. J Am Coll Cardiol. 2011;57:1480–1486.
32. Husten L. Global epidemic of cardiovascular disease predicted. Lancet. 1998;352:1530.
33. Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, et al; Management of Arterial Hypertension of the European Society of Hypertension; European Society of Cardiology. 2007 Guidelines for the Management of Arterial Hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2007;25:1105–1187.
34. Meyer WW, Lind J, Yao AC, Kauffman SL. Early arterial lesions in infancy and childhood and ways of prevention. Paediatrician. 1982;11:136–156.
35. Kiechl S, Werner P, Egger G, Oberhollenzer F, Mayr M, Xu, et al. Active and passive smoking, chronic infections, and the risk of carotid atherosclerosis: prospective results from the Bruneck Study. Stroke. 2002;33:2170–2176.
by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from
Zsolt Garami and Giuseppe SchillaciTamas Horvath, Giacomo Pucci, Pal Bata, Kinga Karlinger, Levente Littvay, Viktor Berczi,
Fagnani, Janos Osztovits, Gyorgy Jermendy, Istvan Preda, Robert Gabor Kiss, Julia Metneki, Maria Antonietta Stazi, Emanuela Medda, Rodolfo Cotichini, Lorenza Nisticò, Corrado
Emanuele Boatta, Chiara Zini, Fabrizio Fanelli, Andrea Agnes Molnar, Giorgio Meneghetti, Adam Domonkos Tarnoki, Claudio Baracchini, David Laszlo Tarnoki, Pierleone Lucatelli,
International Twin StudyEvidence for a Strong Genetic Influence on Carotid Plaque Characteristics: An
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2012 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STROKEAHA.112.666016
2012;43:3168-3172; originally published online October 18, 2012;Stroke.
http://stroke.ahajournals.org/content/43/12/3168World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2012/10/18/STROKEAHA.112.666016.DC1.htmlData Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 20, 2016http://stroke.ahajournals.org/Downloaded from
SUPPLEMENTAL MATERIAL
Evidence for a strong genetic influence on carotid plaque characteristics: an international
twin study
Supplemental Methods
Subjects and study design
The history of vascular risk factors (hypertension, diabetes, stroke, etc.) was determined by a
detailed questionnaire which was completed by a personal interview prior or after the
ultrasound tests. If the patient brought his medical records, we reviewed the documents in
order to confirm the history. Smoking history was recorded by a questionnaire: each subject
was categorized as never, ex- or active smoker. Body mass index was measured by a clinically
validated OMRON BF500 body composition monitor (Omron Healthcare Ltd., Kyoto, Japan).
Current height was verified simultaneously. Central blood pressure was assessed by
oscillometry (TensioMed Arteriograph, TensioMed Ltd., Budapest). Twins above the age of 18
years living in Hungary, Italy and USA were invited to participate. Italian twins were enrolled
in Rome, Padua and Perugia by the Italian Twin Registry [1] in 2009 and 2010. Hungarian
twins were measured at two large hospitals in Budapest in 2009 and 2010. American twin pairs
were recruited during the Twins Days Festival in Twinsburg, OH, in 2009.
Carotid ultrasonography
A participant was considered to be without plaques if the morphology of carotid arteries was
reported to be normal on both sides. No automatic image analyzer program was used. The
presence of plaque was categorized as a dichotomous variable (no plaque, plaque), while
sidedness of the plaque was reported accordingly (no plaque, unilateral or bilateral). The images
were stored digitally for further analysis which included the determination of echogenicity and
calculation of plaque area in mm2. Plaque echogenicity was compared to the echogenicity of the
sternocleidomastoid muscle and was classified in three categories as low (hypoechoic), high
(hyperechoic) and mixed (containing both hypoechoic and hyperechoic parts) [2]. Carotid plaque
numerosity indicated the total number of separate plaques found bilaterally; it was categorized as
no plaque, one, two or more than two plaques. The size of the each carotid plaque in mm2 was
calculated by multiplying the largest thickness measured from the intimal line to the most
protruding point in the lumen by the largest length in a longitudinal plane parallel to the carotid
wall. In order to achieve a normal distribution, this variable was further used as a dichotomous
parameter (below or above 50th
percentile). Presence of plaque in the bulbs and in the internal
carotid arteries was categorized as no plaque, unilateral or bilateral presence. Since the number of
plaques in the proximal common carotid arteries (n=7) and external carotid arteries (n=4) were
low, the heritabilities of the plaques located at these sites were not analyzed. Both members of a
twin pair were investigated by the same researcher and device in order to decrease inter-observer
variability.
Statistical analysis
Higher correlation in MZ than in DZ pairs provides evidence for additive genetic influence (A)
on a phenotype, while similarity of correlations suggests a contribution of the common familial
environmental factors (C) shared by the twins; unique environmental factors (E), or
environmental factors that affect one twin but not the other, are estimated using the deviation
from perfect MZ co-twin correlation [3]. Univariate quantitative genetic ACE-models were fitted
to decompose phenotypic variance of the considered parameters into additive genetic effects, or
heritability [3]. The ACE model is able to estimate these components capitalizing on several
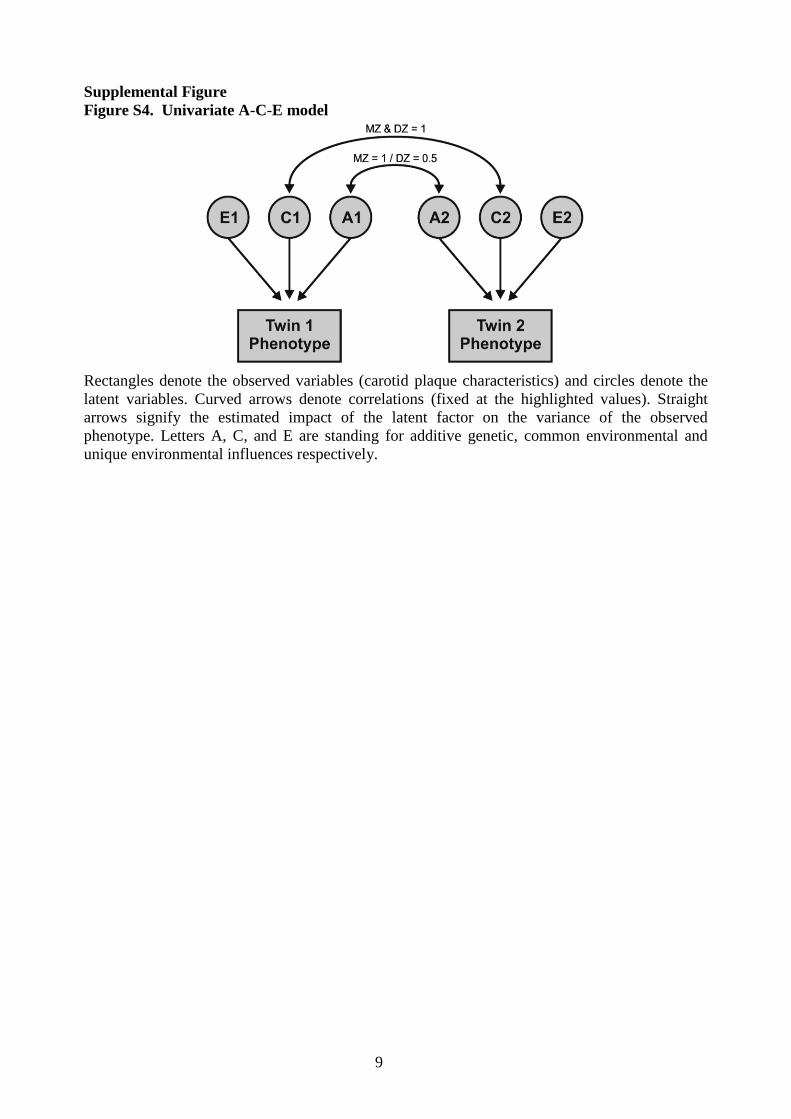
reasonable assumptions that can be made (Figure S4). We know that identical twins share their
genome (r=1) while this correlates r=0.5 for fraternal twins. We also know that on average, both
MZ and DZ twins equally share their common environment (r=1 for both MZ and DZ twins).
The unique environment of the co-twins remains uncorrelated for both zygosities. In the

structural equation model A, C and E components are latent variables but for both co-twins these
latent variables are related to each other based on the described structure giving us the possibility
to estimate the proportions of interest.
References
1. Fagnani C, Brescianini S, Cotichini R, D'Ippolito C, Dukic T, Giannantonio L, et al. The
Italian Twin Register: new cohorts and tools, current projects and future perspectives of a
developing resource. Twin Res Hum Genet. 2006;9:799-805.
2. Kobayashi E, Ono J, Hirai S, Yamakami I, Saeki N, Yamaura A. Detection of Unstable
Plaques in Patients with Carotid Stenosis using B-Mode Ultrasonography. Interv Neuroradiol.
2000;6:165-170.
3. Neale MC, Cardon LR. Methodology for genetic studies of twins and families. Dordrecht, The
Netherlands: Kluwer Academic; 1992.
4. Moskau S, Golla A, Grothe C, Boes M, Pohl C, Klockgether T. Heritability of carotid artery
atherosclerotic lesions: an ultrasound study in 154 families. Stroke. 2005;36:5-8.
5. Hunt KJ, Duggirala R, Göring HH, Williams JT, Almasy L, Blangero J, et al. Genetic basis of
variation in carotid artery plaque in the San Antonio Family Heart Study. Stroke. 2002;33:2775-
2780.
6. Sayed-Tabatabaei FA, van Rijn MJ, Schut AF, Aulchenko YS, Croes EA, Zillikens MC, et al.
Heritability of the function and structure of the arterial wall: findings of the Erasmus Rucphen
Family (ERF) study. Stroke. 2005;36:2351-2356.
7. Dong C, Beecham A, Slifer S, Wang L, Blanton SH, Wright CB, et al. Genomewide linkage
and peakwide association analyses of carotid plaque in Caribbean Hispanics. Stroke.
2010;41:2750-2756.
8. Lee K, Sung J, Lee SC, Park SW, Kim YS, Lee JY, Ebrahim S, Song YM. Segment-specific
carotid intima-media thickness and cardiovascular risk factors in Koreans: the Healthy Twin
Study. Eur J Cardiovasc Prev Rehabil. 2011 Sep 13. [Epub ahead of print]
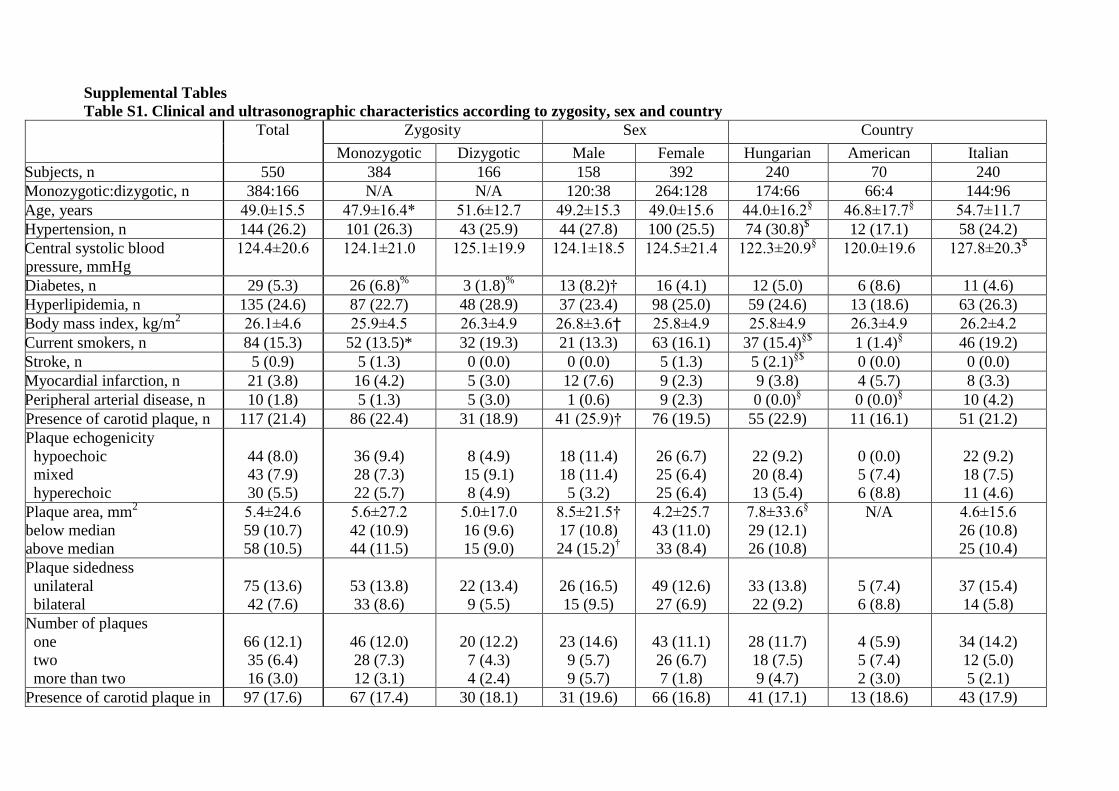
Supplemental Tables
Table S1. Clinical and ultrasonographic characteristics according to zygosity, sex and country
Total Zygosity Sex Country
Monozygotic Dizygotic Male Female Hungarian American Italian
Subjects, n 550 384 166 158 392 240 70 240
Monozygotic:dizygotic, n 384:166 N/A N/A 120:38 264:128 174:66 66:4 144:96
Age, years 49.0±15.5 47.9±16.4* 51.6±12.7 49.2±15.3 49.0±15.6 44.0±16.2§
46.8±17.7§
54.7±11.7
Hypertension, n 144 (26.2) 101 (26.3) 43 (25.9) 44 (27.8) 100 (25.5) 74 (30.8)$
12 (17.1) 58 (24.2)
Central systolic blood
pressure, mmHg
124.4±20.6 124.1±21.0 125.1±19.9 124.1±18.5 124.5±21.4 122.3±20.9§
120.0±19.6 127.8±20.3$
Diabetes, n 29 (5.3) 26 (6.8)%
3 (1.8)%
13 (8.2)† 16 (4.1) 12 (5.0) 6 (8.6) 11 (4.6)
Hyperlipidemia, n 135 (24.6) 87 (22.7) 48 (28.9) 37 (23.4) 98 (25.0) 59 (24.6) 13 (18.6) 63 (26.3)
Body mass index, kg/m2
26.1±4.6 25.9±4.5 26.3±4.9 26.8±3.6† 25.8±4.9 25.8±4.9 26.3±4.9 26.2±4.2
Current smokers, n 84 (15.3) 52 (13.5)* 32 (19.3) 21 (13.3) 63 (16.1) 37 (15.4)§$
1 (1.4)§
46 (19.2)
Stroke, n 5 (0.9) 5 (1.3) 0 (0.0) 0 (0.0) 5 (1.3) 5 (2.1)§$
0 (0.0) 0 (0.0)
Myocardial infarction, n 21 (3.8) 16 (4.2) 5 (3.0) 12 (7.6) 9 (2.3) 9 (3.8) 4 (5.7) 8 (3.3)
Peripheral arterial disease, n 10 (1.8) 5 (1.3) 5 (3.0) 1 (0.6) 9 (2.3) 0 (0.0)§
0 (0.0)§
10 (4.2)
Presence of carotid plaque, n 117 (21.4) 86 (22.4) 31 (18.9) 41 (25.9)† 76 (19.5) 55 (22.9) 11 (16.1) 51 (21.2)
Plaque echogenicity
hypoechoic
mixed
hyperechoic
44 (8.0)
43 (7.9)
30 (5.5)
36 (9.4)
28 (7.3)
22 (5.7)
8 (4.9)
15 (9.1)
8 (4.9)
18 (11.4)
18 (11.4)
5 (3.2)
26 (6.7)
25 (6.4)
25 (6.4)
22 (9.2)
20 (8.4)
13 (5.4)
0 (0.0)
5 (7.4)
6 (8.8)
22 (9.2)
18 (7.5)
11 (4.6)
Plaque area, mm2
below median
above median
5.4±24.6
59 (10.7)
58 (10.5)
5.6±27.2
42 (10.9)
44 (11.5)
5.0±17.0
16 (9.6)
15 (9.0)
8.5±21.5†
17 (10.8)
24 (15.2)†
4.2±25.7
43 (11.0)
33 (8.4)
7.8±33.6§
29 (12.1)
26 (10.8)
N/A
4.6±15.6
26 (10.8)
25 (10.4)
Plaque sidedness
unilateral
bilateral
75 (13.6)
42 (7.6)
53 (13.8)
33 (8.6)
22 (13.4)
9 (5.5)
26 (16.5)
15 (9.5)
49 (12.6)
27 (6.9)
33 (13.8)
22 (9.2)
5 (7.4)
6 (8.8)
37 (15.4)
14 (5.8)
Number of plaques
one
two
more than two
66 (12.1)
35 (6.4)
16 (3.0)
46 (12.0)
28 (7.3)
12 (3.1)
20 (12.2)
7 (4.3)
4 (2.4)
23 (14.6)
9 (5.7)
9 (5.7)
43 (11.1)
26 (6.7)
7 (1.8)
28 (11.7)
18 (7.5)
9 (4.7)
4 (5.9)
5 (7.4)
2 (3.0)
34 (14.2)
12 (5.0)
5 (2.1)
Presence of carotid plaque in 97 (17.6) 67 (17.4) 30 (18.1) 31 (19.6) 66 (16.8) 41 (17.1) 13 (18.6) 43 (17.9)
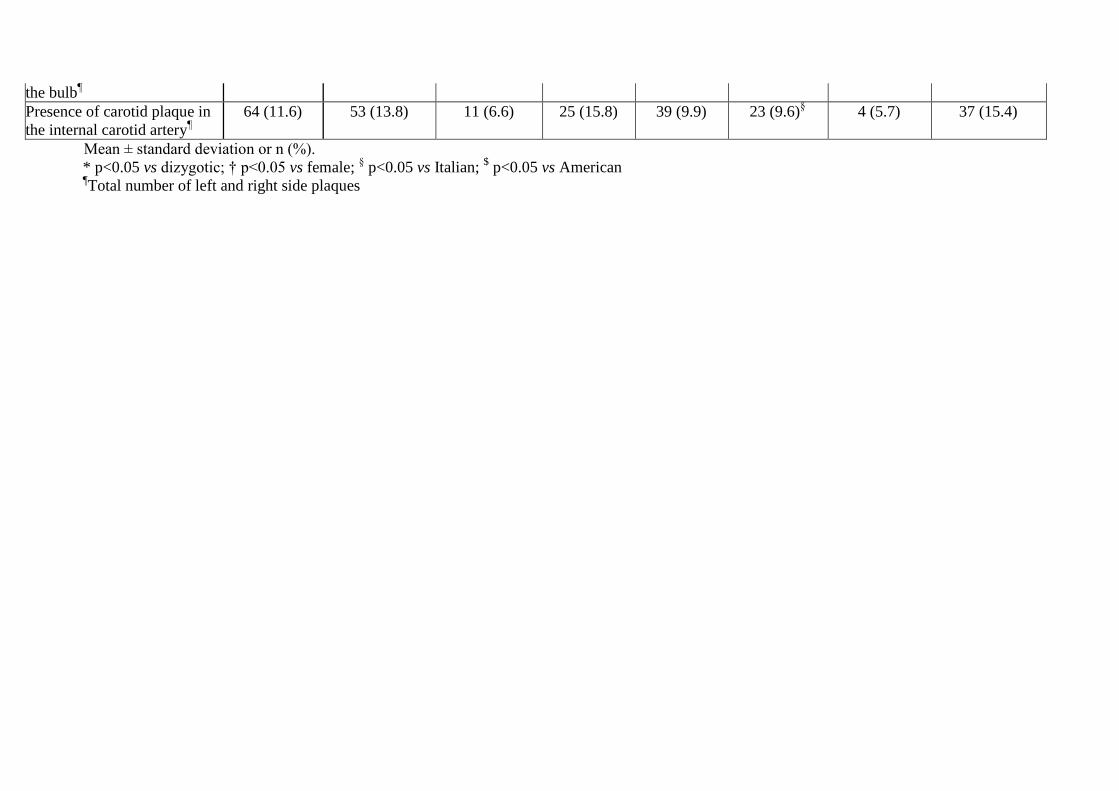
the bulb¶
Presence of carotid plaque in
the internal carotid artery¶
64 (11.6) 53 (13.8) 11 (6.6) 25 (15.8) 39 (9.9) 23 (9.6)§
4 (5.7) 37 (15.4)
Mean ± standard deviation or n (%).
* p<0.05 vs dizygotic; † p<0.05 vs female; § p<0.05 vs Italian;
$ p<0.05 vs American
¶Total number of left and right side plaques

6
Table S2. Relationship between anthropometric parameters, traditional cardiovascular risk factors and carotid plaque characteristics
Presence of
carotid plaque
Plaque
echogenicity
Plaque area Plaque
sidedness
Number of
plaques
Presence of
carotid plaque
in the bulbs
Presence of
carotid plaque
in the internal
carotid arteries
Country, Italy
vs. Hungary
-0.028 -0.026 -0.241 -0.053 -0.043 0.106 0.388*
Country, USA
vs. Hungary
-0.183 -0.036 -4.236 -0.147 -0.453 0.201 -0.261
sex -0.240 -0.139 -0.277 -0.225 -0.254 -0.125 -0.193
age 0.063§
0.060§
0.048§
0.064§
0.064§
0.060§
0.048§
Body mass
index
0.020 0.021 0.010 0.008 0.007 -0.027 -0.006
Central
systolic blood
pressure
0.001 0.000 -0.003 0.000 -0.001 0.006 -0.001
diabetes 2.493§
0.048 -0.107 -0.061 -0.145 -0.289 0.076
smoking 0.304† 0.234* 0.204 0.319§
0.330§
0.370† 0.370†
hyperlipidaem
ia
0.174 0.149 0.179 0.292* 0.225 0.284 0.135
* p<0.05; † p<0.01; § p<0.001
Results show the family and zygosity corrected probit regression results between our dependent variables of interest and relevant covariates. For
age, sex and country bivariate results are shown, for the rest of the covariates age, sex and country are also corrected for much like in Model 1 and
Model 2 ACE analyses.
7
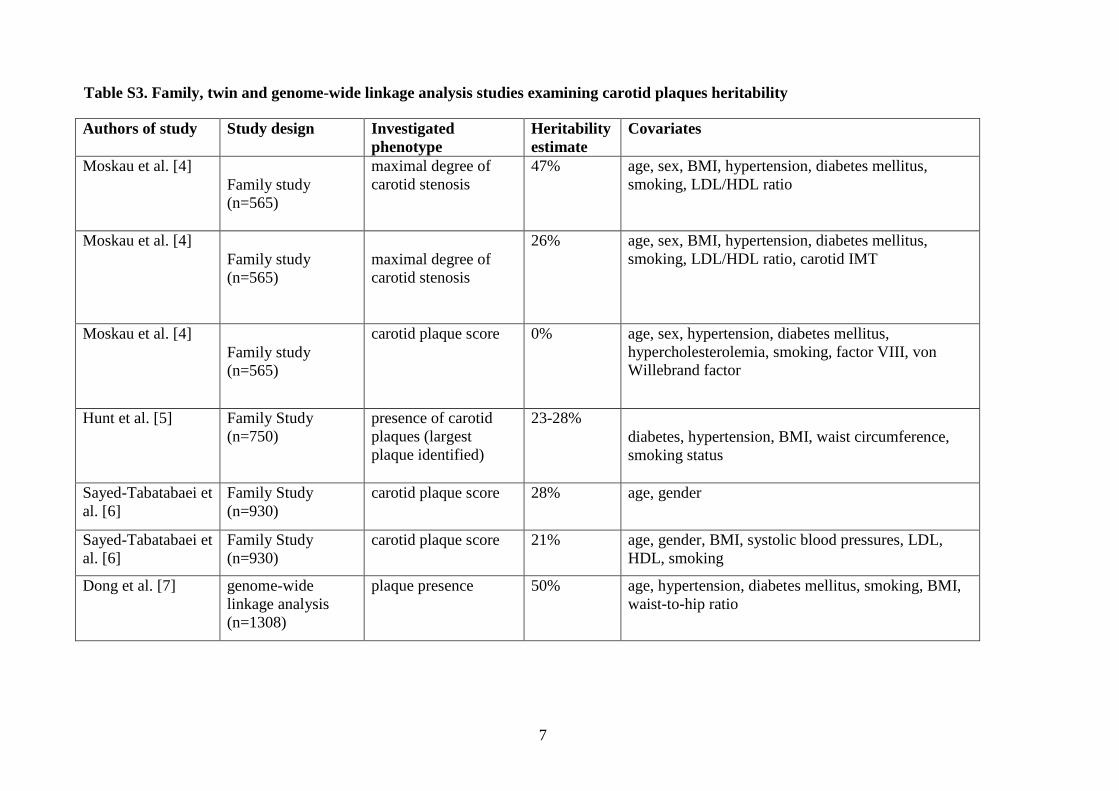
Table S3. Family, twin and genome-wide linkage analysis studies examining carotid plaques heritability
Authors of study Study design Investigated
phenotype
Heritability
estimate
Covariates
Moskau et al. [4]
Family study
(n=565)
maximal degree of
carotid stenosis
47% age, sex, BMI, hypertension, diabetes mellitus,
smoking, LDL/HDL ratio
Moskau et al. [4]
Family study
(n=565)
maximal degree of
carotid stenosis
26% age, sex, BMI, hypertension, diabetes mellitus,
smoking, LDL/HDL ratio, carotid IMT
Moskau et al. [4]
Family study
(n=565)
carotid plaque score 0% age, sex, hypertension, diabetes mellitus,
hypercholesterolemia, smoking, factor VIII, von
Willebrand factor
Hunt et al. [5] Family Study
(n=750)
presence of carotid
plaques (largest
plaque identified)
23-28%
diabetes, hypertension, BMI, waist circumference,
smoking status
Sayed-Tabatabaei et
al. [6]
Family Study
(n=930)
carotid plaque score 28% age, gender
Sayed-Tabatabaei et
al. [6]
Family Study
(n=930)
carotid plaque score 21% age, gender, BMI, systolic blood pressures, LDL,
HDL, smoking
Dong et al. [7] genome-wide
linkage analysis
(n=1308)
plaque presence 50% age, hypertension, diabetes mellitus, smoking, BMI,
waist-to-hip ratio
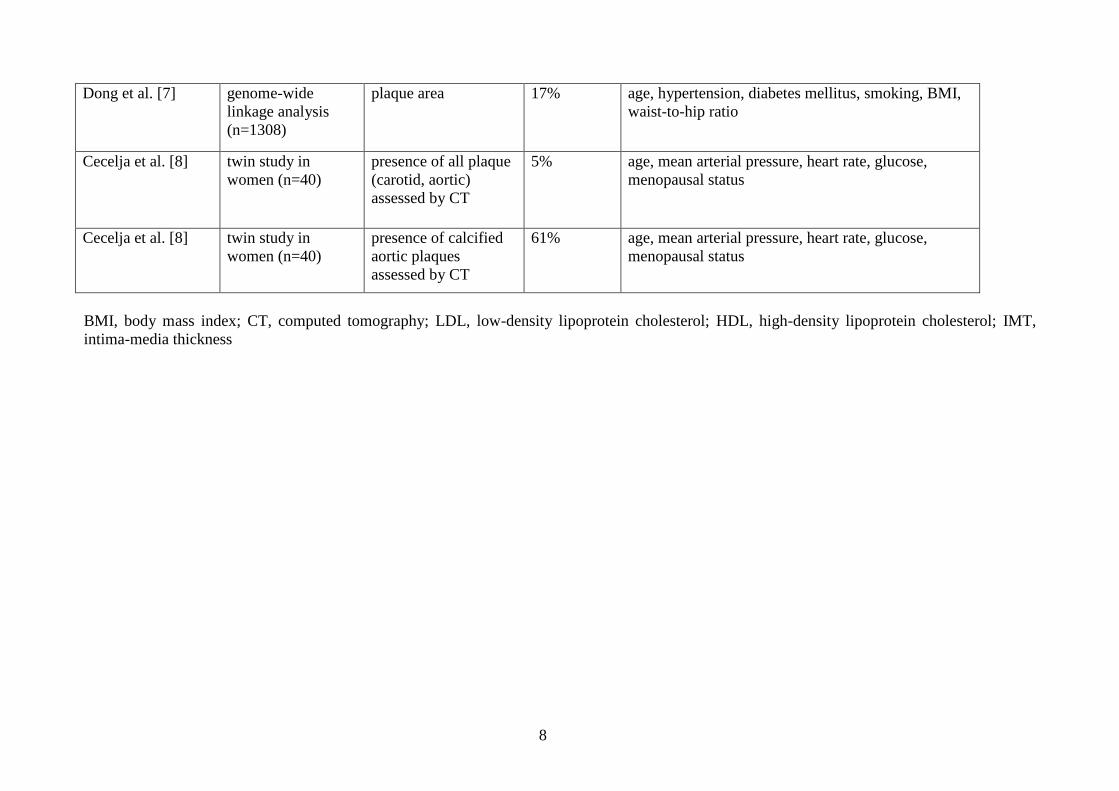
8
Dong et al. [7] genome-wide
linkage analysis
(n=1308)
plaque area 17% age, hypertension, diabetes mellitus, smoking, BMI,
waist-to-hip ratio
Cecelja et al. [8] twin study in
women (n=40)
presence of all plaque
(carotid, aortic)
assessed by CT
5% age, mean arterial pressure, heart rate, glucose,
menopausal status
Cecelja et al. [8] twin study in
women (n=40)
presence of calcified
aortic plaques
assessed by CT
61% age, mean arterial pressure, heart rate, glucose,
menopausal status
BMI, body mass index; CT, computed tomography; LDL, low-density lipoprotein cholesterol; HDL, high-density lipoprotein cholesterol; IMT,
intima-media thickness
9
Supplemental Figure
Figure S4. Univariate A-C-E model
Rectangles denote the observed variables (carotid plaque characteristics) and circles denote the
latent variables. Curved arrows denote correlations (fixed at the highlighted values). Straight
arrows signify the estimated impact of the latent factor on the variance of the observed
phenotype. Letters A, C, and E are standing for additive genetic, common environmental and
unique environmental influences respectively.