
18FDG PET and Ultrasound Echolucency in Carotid Artery Plaques
Upload
independentCategory
view
4download
0
Radiotherapy and Oncology xxx (2013) xxx–xxx
Contents lists available at ScienceDirect
Radiotherapy and Oncology
journal homepage: www.thegreenjournal .com
Original article
Radiation-induced carotid artery atherosclerosis
0167-8140/$ - see front matter � 2013 Elsevier Ireland Ltd. All rights reserved.http://dx.doi.org/10.1016/j.radonc.2013.08.009
⇑ Corresponding author. Address: Head and Neck Unit, Royal Marsden Hospital,Fulham Rd, London SW3 6JJ, United Kingdom.
E-mail addresses: [email protected], [email protected](C.M. Nutting).
Please cite this article in press as: Gujral DM et al. Radiation-induced carotid artery atherosclerosis. Radiother Oncol (2013), http://dx.doi.org/1j.radonc.2013.08.009
Dorothy M. Gujral a, Navtej Chahal b, Roxy Senior b, Kevin J. Harrington a, Christopher M. Nutting a,⇑a Head and Neck Unit, Royal Marsden Hospital; and b Department of Echocardiography, Royal Brompton Hospital, London, United Kingdom
a r t i c l e i n f o a b s t r a c t
Article history:Received 24 October 2012Received in revised form 5 June 2013Accepted 7 August 2013Available online xxxx
Keywords:Carotid arteryRadiotherapyAtherosclerosis
Purpose: Carotid arteries frequently receive significant doses of radiation as collateral structures in thetreatment of malignant diseases. Vascular injury following treatment may result in carotid artery stenosis(CAS) and increased risk of stroke and transient ischaemic attack (TIA). This systematic review examinesthe effect of radiotherapy (RT) on the carotid arteries, looking at the incidence of stroke in patients receiv-ing neck radiotherapy. In addition, we consider possible surrogate endpoints such as CAS and carotidintima-medial thickness (CIMT) and summarise the evidence for radiation-induced carotid atherosclero-sis.Materials and methods: From 853 references, 34 articles met the criteria for inclusion in this systematicreview. These papers described 9 studies investigating the incidence of stroke/TIA in irradiated patients,11 looking at CAS, and 14 examining CIMT.Results: The majority of studies utilised suboptimally-matched controls for each endpoint. The relativerisk of stroke in irradiated patients ranged from 1.12 in patients with breast cancer to 5.6 in patients trea-ted for head and neck cancer. The prevalence of CAS was increased by 16–55%, with the more modestincrease seen in a study using matched controls. CIMT was increased in irradiated carotid arteries by18–40%. Only two matched-control studies demonstrated a significant increase in CIMT of 36% and22% (p = 0.003 and <0.001, respectively). Early prospective data demonstrated a significant increase inCIMT in irradiated arteries at 1 and 2 years after RT (p < 0.001 and <0.01, respectively).Conclusions: The incidence of stroke was significantly increased in patients receiving RT to the neck.There was a consistent difference in CAS and CIMT between irradiated and unirradiated carotid arteries.Future studies should optimise control groups.
� 2013 Elsevier Ireland Ltd. All rights reserved. Radiotherapy and Oncology xxx (2013) xxx–xxx
Radiation-induced atherosclerosis was first described as earlyas 1959 [1]. Tissue necrosis and inflammation resulting in endothe-lial damage, proliferation and fibrosis as well as accelerated ath-erosclerosis are thought to be key mechanisms responsible forthe injury. These mechanisms are thought to result in morpholog-ical features similar to those seen in spontaneous atherosclerosis[2]. Vascular injury to smaller vessels following radiotherapy (RT)has been well described. Historically, the left anterior descendingcoronary artery was exposed to significant radiation dose in pa-tients undergoing treatment for left-sided breast cancer using old-er RT techniques [3]. Subsequent longitudinal, cohort studies haveshown increased cardiovascular risk in these patients compared tocontrols [4,5]. Radiation damage to larger vessels, like the carotidarteries, and the underlying processes involved has received moreinterest in recent decades.
The precursor for stroke and transient ischaemic attack (TIA) isatherosclerosis, which precedes this clinical endpoint by many
years and is characterised by arterial wall thickening and plaquedevelopment with subsequent stenosis. The risk of stroke increaseswith time. Risk factors associated with increased risk of atheroscle-rosis include: increasing age, diabetes mellitus, hypertension,hypercholesterolemia, obesity, smoking and RT to the affected ves-sels [6]. Atherosclerosis associated with radiation therapy, whilehistologically similar to spontaneous atherosclerosis, is a clinicallydistinct entity. The disease is limited to the irradiated area and isless likely to be associated with atherogenic risk factors [7].
Carotid artery stenosis (CAS) is diagnosed on Doppler ultra-sound. Grading of CAS is well defined [8], with stenosis of P70%(i.e. percentage reduction of internal carotid artery diameter) con-sidered significant and requiring intervention in case of neurolog-ical symptoms. The ultrasound features of plaques correlate withhistological findings [9] and the risk of stroke [10].
Carotid intimal-medial thickness (CIMT) is a measure of thethickness of the artery wall, using B-mode ultrasound. IncreasedCIMT is an early marker of atherosclerosis and predicts for subse-quent risk of death from myocardial infarction and stroke [11]. In-creased CIMT is a strong predictor of future vascular events [12].Measurement of CIMT for cardiovascular risk assessment has been
0.1016/

2 Radiation-induced carotid atherosclerosis
included in the American College of Cardiology Foundation andAmerican Heart Association guidelines [13].
The aim of this systematic review is to investigate the incidenceof stroke in patients treated with RT to the neck compared to unir-radiated controls and to evaluate surrogate endpoints for stroke(CIMT as a measure of arterial thickening, and CAS as a measureof plaque development). We hypothesise that there is an increasedincidence of stroke in irradiated patients and that CIMT and CASwill be increased in irradiated carotid arteries compared tocontrols.
Fig. 1. Flow diagram of literature search.
Materials and methods
Search strategy
We performed a systematic search of pubmed (1st January 1970to 31st December 2010) for English language articles using thesearch terms: ‘‘carotid’’, ‘‘artery’’, and ‘‘radiotherapy’’. The abstractsor available data obtained from this search were read indepen-dently by two authors (DMG and NC) to include or exclude refer-ences for full text review. Articles reporting on patients who hadreceived RT to the neck (one or both sides) for malignant or benigndisease were eligible for inclusion. Publications had to report oncase-controlled study designs with a clearly defined control groupto be eligible for inclusion or had to be prospective studies report-ing on the incidence of CAS, CIMT, or stroke. Case reports and caseseries were excluded from this review.
Selection criteria for full text review
References were included if they described journal articlesreporting case-controlled studies investigating the following end-points: CAS, CIMT, or stroke. Relevant references not clearly iden-tifying patient populations or study design were included in theinitial review to avoid erroneous exclusion. The full-text articlesfrom the selected references were read independently by twoauthors (DMG, NC) to select the final set of articles for reviewand analysis. The reference lists of these articles were also re-viewed, and references from relevant titles were obtained and re-viewed according to the above selection criteria.
Data abstraction and analysis
The outcomes of interest were: stroke, CIMT, and CAS in case-controlled studies where patients had received RT to the neck. Eachoutcome was considered separately and the appropriateness of thecontrol groups was reviewed. The aim of the literature review wasto identify studies reporting on prevalence of stroke and interme-diate surrogate endpoints for stroke.
Results
The initial database search produced 853 references [Fig. 1].During screening, the abstracts or available data from 43 of theseinitially satisfied the selection criteria and their full-text articleswere obtained. Nine of the 43 were excluded after reading the fulltext articles due to lack of a control group (N = 6) and repeatedreporting of studies (N = 3) (for these studies, the earlier publica-tions did not include defined control groups and were excludedin favour of the updated versions which were reported as case-con-trolled studies). Two studies were prospective studies reporting onthe change in CIMT over time and will be discussed separately.Therefore, a total of 34 studies were included in this review.
Please cite this article in press as: Gujral DM et al. Radiation-induced carotidj.radonc.2013.08.009
Stroke/TIA
The studies reporting on the incidence of stroke and/or TIA inpatients who had received RT to the neck are highlighted in Table 1[14–22]. Seven of the 9 studies showed an increased incidence ofstroke in irradiated patients with the relative risk (RR)/hazard ratio(HR) for stroke/TIA ranging from 1.12 [17] in patients with breastcancer to 5.6 [14] in patients with head and neck cancer. The mainpoint to note is that, for all of these studies, there was a lack of anappropriately matched control group. Five of the 9 studies[14,15,17–19] utilised large population databases as a controlgroup, matched primarily for age and sex [23–26] and the other4 studies used a defined group as controls. The study by Dor-resteijn et al. [14] compared stroke rates in patients treated forhead and neck cancer to those reported in the Oxfordshire Commu-nity Stroke Project (OCSP) [23]. The authors stated that, at the timeof the study, there were no large Dutch studies documenting theincidence of stroke in the population and that the expected ratesof stroke in the Netherlands and United Kingdom were similar.Therefore, they felt it was justified to use the expected stroke ratesfrom the large, published OCSP as age- and sex-matched controls.The study by Haynes et al. [15] compared stroke rates in Americanpatients treated for head and neck cancer to the expected inci-dence, based on population data from Stockholm [24]. This studyshowed a RR of stroke of 2.09 (95% confidence interval (CI) 1.28–3.22) in patients with head and neck cancer treated with RT(p = 0.0007). It is important to note, however, that these patientswere only matched for age, gender, and smoking status and, there-fore, the true RR may be more conservative as the other risk factorsfor atherosclerosis are not accounted for.
Carotid artery stenosis
Early studies utilised older techniques such as angiography andpanoramic radiographs as diagnostic tools and are summarised inTable 2 [27–29]. These studies demonstrated a significantly in-creased prevalence of CAS in irradiated patients (17–25%) com-pared to those who did not receive RT.
Retrospective studies examining the prevalence of CAS in irradi-ated patients using Doppler ultrasound are listed in Table 2 [7,30–36]. Nine of the 10 studies demonstrated a significantly increasedprevalence of CAS in patients with irradiated carotid arteries; 5studies used unmatched controls. The difference in CAS rangedfrom 16% [7] to 55% [33]. The study by Halek et al. [7] showed ahigher prevalence of CAS in the irradiated distal carotid artery
artery atherosclerosis. Radiother Oncol (2013), http://dx.doi.org/10.1016/

Table 1Studies investigating the incidence of neurological events in patients treated with cervical radiotherapy.
Study No. ofpatients
No of controls Radiation dose(Gy)
Interval fromradiotherapy(months)
Incidence of stroke/TIA(patients) (%)
Incidence ofstroke/TIA(controls)
Relative risk (95%CI) or Hazardratio (HR) (95%CI)
p Value
Total Mean/median(range)
Median(range)Tumour
type
Dorresteijn2002[14]
367 OCSPa (50–66 Gy) 93.6 (6–271.2)
14/367 (3.8%) 2.5/367 (0.7%) 5.6 (3.1–9.4)
Head andneck
(age/sex match)
Haynes2002[15]
413 Stockholmb
Project (age/gender/smokingmatched)
Mean 64.1 Gy 33.5 (2–146) 20/413 (4.8%) Not stated 2.09 (1.28–3.22) p = 0.0007
Head andneck
(40–80 Gy)
Bowers2005[16]
1926 3846 40 Gy (29.8–48 Gy) (pts whodevelopedstroke)
Mean 234(SD 70.8)
24/1386 (1.73%) 9/3846 (0.23%) 5.62 (2.59–12.25) p < 0.0001
Hodgkin Siblings Median timetostroke = 210
1386 –mantle RT
Nilsson2005[17]
25171 Backgroundpopulation(unmatched)
Not stated 64.8 (IQR27.6–124.8)
7% 6.30% 1.12 (1.07–1.17) NotstatedAny breast
cancerdiagnosis
Hooning2006[18]
4368 CMRNc Mean 50 Gy Median 212.4 164/4368 = 3.8% 217.6/4368 = 5% HR 1.04 (0.69–1.58) – stroke
p = NS
Breast (Age/sexmatched)
HR 1.45 (0.85–2.46) - TIA
1061 –SCFd RT
135/1061 = 12.7% 175/1061 = 16.5%
Jagsi 2006[19]
826 NHDSe Not stated 81.6 (1.2–243.6)
Overall – 2.4% Not stated HR 1.9 (0.9–3.7)CVA or TIA
p = 0.072
Breast (age/sex/racematched)
SCF RT = 10/222 = 4.5% HR 2.8 (1.2–6.7)CVA alone
222 – SCFRT
p = 0.021
Woodward2006[20]
471 5281 Not stated 90 15 yr freedom fromhospitalisation forstroke = 81.6%
15 yr freedomfromhospitalisation forstroke = 79%
HR 1.0 (0.6–1.68)for stroke
Breast –SCF RT
Breast – no SCF RT 12 yr actuarial causespecific strokesurvival = 95.4%
12 yr actuarialcause specificstrokesurvival = 95.1%
Unmatched
p = 0.13Smith 2008
[21]4806 2056 Not stated 28.8 (IQR
16.8–52.8)42.8/1000 person yrs 30.7/1000 person
yrsp < 0.001
Head andneck – RTor RT + Sx
Head and neck –Sx alone(unmatched)
DeBruin2009[22]
1787 414 40 Gy (36–44 Gy)
208.8 (61.2–451.2)
SCF ± neck = 5/136 (3.7%) 8/414 = 1.9% HR 2.3 (0.7–7.6) NotstatedHodgkin –
neck RTHodgkin – noneck RT(unmatched)
Mediastinum + neck = 75/1651 (4.5%)
HR 2.5 (1.1–5.6)
a OCSP – Oxfordshire Community Stroke project [23].b Stockholm Project [24].c CMRN – Continuous Morbidity Registration-Nijmegen [25].d SCF – supraclavicular fossa.e NHDS – National Hospital Discharge Survey [26].
D.M. Gujral et al. / Radiotherapy and Oncology xxx (2013) xxx–xxx 3
and not the irradiated internal or external carotid artery. Brownet al. [34] demonstrated a significant difference in CAS in patientswho had been irradiated more than 15 years earlier. Patients whohad received RT tended to develop more haemodynamically signif-icant lesions [30].
Later studies [34,35] more appropriately used the unirradiatedside of the neck as an internal matched control, thereby accountingfor all the other risk factors of atherosclerosis. Woodward et al.[35] showed no difference in prevalence of CAS in irradiated versusunirradiated carotid arteries in breast cancer patients receiving RT
Please cite this article in press as: Gujral DM et al. Radiation-induced carotidj.radonc.2013.08.009
to the supraclavicular fossa. However, as the study was underpow-ered to show a difference and closed after accruing fewer than half(n = 46) the required number of patients, no firm conclusions canbe drawn from this study. The second study [34] showed a moremodest difference in CAS than earlier studies (16%).
CIMT
Details of retrospective studies investigating CIMT, the majorityof which used suboptimal age and sex matched controls, are
artery atherosclerosis. Radiother Oncol (2013), http://dx.doi.org/10.1016/
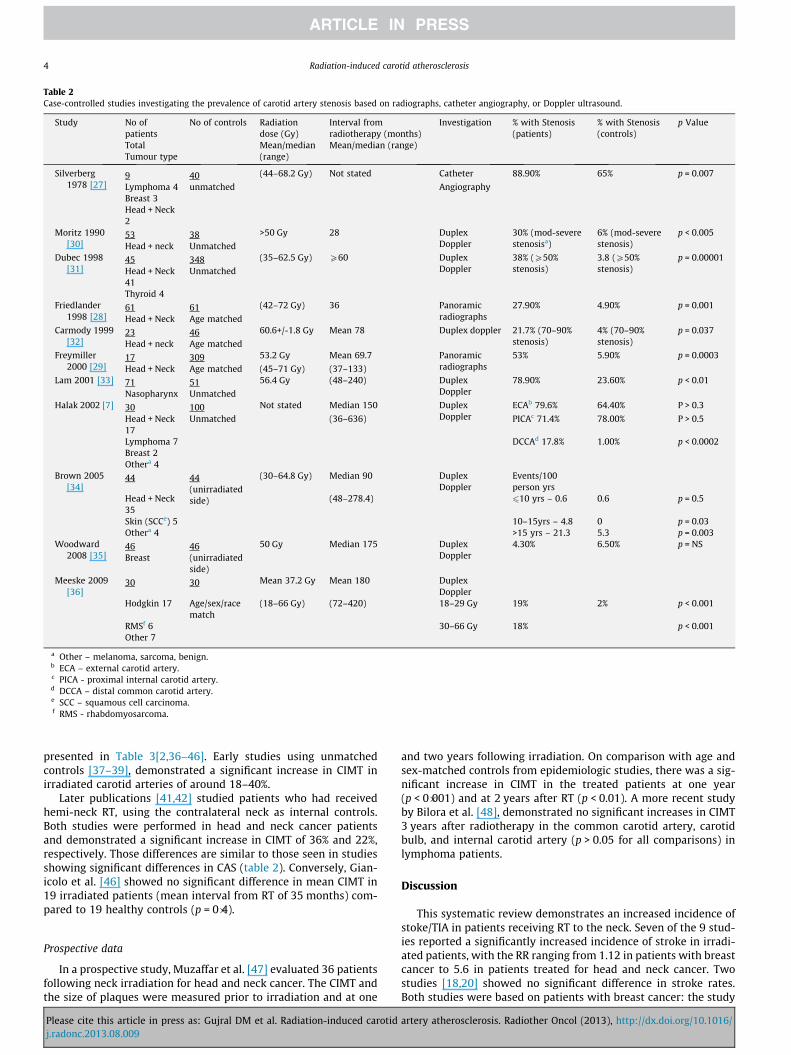
Table 2Case-controlled studies investigating the prevalence of carotid artery stenosis based on radiographs, catheter angiography, or Doppler ultrasound.
Study No ofpatients
No of controls Radiationdose (Gy)
Interval fromradiotherapy (months)
Investigation % with Stenosis(patients)
% with Stenosis(controls)
p Value
Total Mean/median(range)
Mean/median (range)Tumour type
Silverberg1978 [27]
9 40 (44–68.2 Gy) Not stated Catheter 88.90% 65% p = 0.007
Lymphoma 4 unmatched AngiographyBreast 3Head + Neck2
Moritz 1990[30]
53 38 >50 Gy 28 DuplexDoppler
30% (mod-severestenosisa)
6% (mod-severestenosis)
p < 0.005
Head + neck UnmatchedDubec 1998
[31]45 348 (35–62.5 Gy) P60 Duplex
Doppler38% (P50%stenosis)
3.8 (P50%stenosis)
p = 0.00001
Head + Neck41
Unmatched
Thyroid 4Friedlander
1998 [28]61 61 (42–72 Gy) 36 Panoramic
radiographs27.90% 4.90% p = 0.001
Head + Neck Age matchedCarmody 1999
[32]23 46 60.6+/-1.8 Gy Mean 78 Duplex doppler 21.7% (70–90%
stenosis)4% (70–90%stenosis)
p = 0.037
Head + neck Age matchedFreymiller
2000 [29]17 309 53.2 Gy Mean 69.7 Panoramic
radiographs53% 5.90% p = 0.0003
Head + Neck Age matched (45–71 Gy) (37–133)Lam 2001 [33] 71 51 56.4 Gy (48–240) Duplex
Doppler78.90% 23.60% p < 0.01
Nasopharynx UnmatchedHalak 2002 [7] 30 100 Not stated Median 150 Duplex
DopplerECAb 79.6% 64.40% P > 0.3
Head + Neck17
Unmatched (36–636) PICAc 71.4% 78.00% P > 0.5
Lymphoma 7 DCCAd 17.8% 1.00% p < 0.0002Breast 2Othera 4
Brown 2005[34]
44 44(unirradiatedside)
(30–64.8 Gy) Median 90 DuplexDoppler
Events/100person yrs
Head + Neck35
(48–278.4) 610 yrs – 0.6 0.6 p = 0.5
Skin (SCCe) 5 10–15yrs – 4.8 0 p = 0.03Othera 4 >15 yrs – 21.3 5.3 p = 0.003
Woodward2008 [35]
46 46(unirradiatedside)
50 Gy Median 175 DuplexDoppler
4.30% 6.50% p = NS
Breast
Meeske 2009[36]
30 30 Mean 37.2 Gy Mean 180 DuplexDoppler
Hodgkin 17 Age/sex/racematch
(18–66 Gy) (72–420) 18–29 Gy 19% 2% p < 0.001
RMSf 6 30–66 Gy 18% p < 0.001Other 7
a Other – melanoma, sarcoma, benign.b ECA – external carotid artery.c PICA - proximal internal carotid artery.d DCCA – distal common carotid artery.e SCC – squamous cell carcinoma.f RMS - rhabdomyosarcoma.
4 Radiation-induced carotid atherosclerosis
presented in Table 3[2,36–46]. Early studies using unmatchedcontrols [37–39], demonstrated a significant increase in CIMT inirradiated carotid arteries of around 18–40%.
Later publications [41,42] studied patients who had receivedhemi-neck RT, using the contralateral neck as internal controls.Both studies were performed in head and neck cancer patientsand demonstrated a significant increase in CIMT of 36% and 22%,respectively. Those differences are similar to those seen in studiesshowing significant differences in CAS (table 2). Conversely, Gian-icolo et al. [46] showed no significant difference in mean CIMT in19 irradiated patients (mean interval from RT of 35 months) com-pared to 19 healthy controls (p = 0�4).
Prospective data
In a prospective study, Muzaffar et al. [47] evaluated 36 patientsfollowing neck irradiation for head and neck cancer. The CIMT andthe size of plaques were measured prior to irradiation and at one
Please cite this article in press as: Gujral DM et al. Radiation-induced carotidj.radonc.2013.08.009
and two years following irradiation. On comparison with age andsex-matched controls from epidemiologic studies, there was a sig-nificant increase in CIMT in the treated patients at one year(p < 0�001) and at 2 years after RT (p < 0.01). A more recent studyby Bilora et al. [48], demonstrated no significant increases in CIMT3 years after radiotherapy in the common carotid artery, carotidbulb, and internal carotid artery (p > 0.05 for all comparisons) inlymphoma patients.
Discussion
This systematic review demonstrates an increased incidence ofstoke/TIA in patients receiving RT to the neck. Seven of the 9 stud-ies reported a significantly increased incidence of stroke in irradi-ated patients, with the RR ranging from 1.12 in patients with breastcancer to 5.6 in patients treated for head and neck cancer. Twostudies [18,20] showed no significant difference in stroke rates.Both studies were based on patients with breast cancer: the study
artery atherosclerosis. Radiother Oncol (2013), http://dx.doi.org/10.1016/

Table 3Case-controlled studies investigating the effect of radiotherapy on carotid artery intima-medial thickness.
Study No of patients No of controls Radiation dose(Gy)
Interval fromradiotherapy(months)
Investigation Mean IMTa
(patients)Mean IMT (controls) p Value
Total Mean/Median(range)
Mean/median(range)Tumour type
Feehs 1991[36]
29 9 Mean 60.4 Gy(40–87.2 Gy)
Mean 102 B mode IMT mean 1.28 ± SE0.06 mm
IMT mean 0.90 ± SE0.05 mm
p = 0.003
Head + neck Unmatched (36–204)King 1999
[37]42 33 (22–40 Gy) 156 B-mode Median 0.51 mm
(range 0.32–1.99)Median 0.43 mm(range 0.32–0.61)
p < 0.005
Hodgkin Unmatched (61.2–273.6)Heikens
2000 [38]26 29 Mean 54 Gy Median 192 (108–
300)DuplexDoppler
Brain Unmatched (30–62 Gy) CCA 0.57 mm (SD 1.1) 0.58 mm (SD 1.2) p = NSBulb 0.63 mm (SD 1.6) 0.53 mm (SD 1.1) p = 0.02ICA 0.5 mm (SD 1.3) 0.57 (SD 3.2) p = NS
Cheng 2002[2]
46 46 (50–60 Gy) Median 136 DuplexDoppler
Mean0.96 mm ± 0.34 (SD)
Mean0.80 mm ± 0.19 (SD)
p = 0.008
Nasopharynx19
Age/sexmatch
(64–336)
Larynx 20Oropharynx 3Parotid 2Oral cavity 2
So 2002 [39] 51 51 N/S Mean 92.4 B-mode 2.2 mm ± SD 1.5 0.7 mm ± SD 0.15 p < 0.05
Nasopharynx Age/sexmatch
Dorresteijn2005 [40]
42 42(unirradiatedside)
(40–66 Gy) Median 117.6 (40.8–326.4)
B-mode Mean 1.13 mm ± SD0.85 mm
Mean 0.83 mm ± SD0.51 mm
p = 0.031
Parotid
Martin 2005[41]
40 40(unirradiatedside)
(30–60 Gy) Mean 101 DuplexDoppler
35% 12.50%
Lymphoma 14 (24–217) All doses 0.104 mm 0.085 mm p = 0.046Tonsil 18 High dose 0.126 mm 0.081 mm p = 0.031Parotid 8 Low dose 0.089 mm 0.087 mm p = 0.861
Bilora [42]2006
42 42 (36–40 Gy) Mean 60 DuplexDoppler
Mean 1.42 mm Mean 0.90 mm p < 0.05
Lymphoma Age/sexmatch
(24–144)
Shariat 2008[43]
13 13 (46–70 Gy) Mean 37.2 B-mode 0.74 mm (SD0.1767 mm)
0.46 (SD0.1304 mm)
p < 0.001
Nasopharynx11 Age/sex/racematch
(12–96)
Larynx 1Oral cavity 1
Meeske2009 [44]
30 30 Mean 37.2 Gy Mean 180 DuplexDoppler
Hodgkin 17 Age/sex/racematch
(18–66 Gy) (72–420) 18–29 Gy 0.43 mm (SD 0.09) 0.41 mm (SD 0.06) p < 0.01
RMSd 6 0.48 mm (SD 0.14)Othere 7 30–66 Gy p < 0.0001
Shai [45]2009
145 150 Mean 0.09 Gy Mean 614.8 DuplexDoppler
0.68 mm (SD 0.16) 0.61 mm (SD 0.17) p < 0.001
Tinea capitis Age/sex/DMb/IHDc match
Gianicolo2010 [46]
19 19 Mean 40.1 Gy(25–70 Gy)
Mean 34.8 DuplexDoppler
0.59 mm ± 0.16 0.56 mm ± 0.16 p = 0.4
Lymphoma 11 Age/sex/racematch
(1–72)
Head + Neck 6Breast 2
a IMT – intima-medial thickness.b DM – diabetes mellitus.c IHD – ischaemic heart disease.d RMS – rhabdomyosarcoma.e Other – not specified.
D.M. Gujral et al. / Radiotherapy and Oncology xxx (2013) xxx–xxx 5
by Hooning et al. [18] showed no significant difference in incidentstroke rates in 4368 treated patients, a finding that was also truefor the subgroup of 1061 patients who had been treated with RTto the supraclavicular fossa (SCF). The authors suggest several rea-sons for this: women in late menopause may be afforded protec-tion against cerebrovascular disease, a diagnosis of breast cancermay trigger a healthier lifestyle after treatment, and regular mon-itoring may allow more aggressive management of risk factorssuch as hypertension. The second study [35] showed no significantincrease in stroke in 471 patients with breast cancer treated with
Please cite this article in press as: Gujral DM et al. Radiation-induced carotidj.radonc.2013.08.009
RT to the SCF. The control group, although a cohort of breast cancerpatients, were unmatched and this may partially explain this re-sult, in addition to the reasons stated above. The hypothesis thatbreast cancer patients experience a lower risk of stroke than headand neck cancer patients because irradiation of the SCF delivers adose of 45–50 Gy to only 7 cm of the proximal carotid artery [20]is not borne out by other studies in breast cancer and lymphomapatients [16,17,19,22] that do show a significant increase instroke/TIA in these patients. Two of the 3 head and neck cancerstudies [14,15], did make some attempt to use matched controls
artery atherosclerosis. Radiother Oncol (2013), http://dx.doi.org/10.1016/

6 Radiation-induced carotid atherosclerosis
and to appreciate the other risk factors for stroke or TIA. Table 1highlights the difficulty in investigating stroke/TIA as an endpointin radiation-induced carotid atherosclerosis. However, despite thelack of a matched control group, these studies generally show in-creased rates of neurological sequelae after RT. It is unlikely thata prospective study using a matched control group to determinethe RR of stroke will be undertaken due to the long latent intervalfrom radiation treatment to the development of stroke. Conse-quently, it is reasonable to look at surrogate endpoints that occurat earlier time points in matched case-controlled studies to inves-tigate the risk of radiation-induced vascular damage.
The lack of suitable matched controls is also highlighted in theearlier studies investigating CAS and CIMT. The use of unmatchedcontrols is an inherent weakness and does not account for theother risk factors of atherosclerosis, which would be necessary inorder to demonstrate an effect attributable solely to radiation.Recently, CIMT has been used as a surrogate endpoint for stroke.Mean CIMT correlates with degree of CAS [49]. The study byHeikens et al. [39] highlighted a significant difference in CIMT inthe bulb of the carotid artery, but not other arterial sections. Thatstudy did not give an indication of the radiation dose received bythe carotid arteries, as patients received craniospinal irradiation.However, the minimum dose prescribed to the craniospinalaxis was 30 Gy. The small sample size makes it difficult to drawrobust conclusions, but this study does suggest an increased CIMTafter RT. In the only negative study by Gianicolo et al. [46], it isimportant to note that fewer patients were recruited with ashorter mean interval from RT (with a minimum follow-up ofone month following treatment) than previous studies. Thesefactors may explain the difference in results from other reportedseries.
An important factor associated with significant carotid diseaseis the time interval after RT. Cheng et al. [50] demonstrated thatpatients who had undergone treatment more than five years previ-ously had an 8�5 times greater risk of having CAS of P70% thanthose with fewer than five years of follow-up. These authors, there-fore, advocated routine screening in patients who have received RTto the neck more than five years previously. Brown et al. [34] dem-onstrated a significant increase in CAS in patients who had beenirradiated 10–15 years (p = 0.03) and more than 15 years previ-ously (p = 0.003), but no significant increase was noted in patientstreated fewer than 10 years previously (p = 0.5).
Whether the length of carotid artery that is irradiated or thesection of irradiated artery is related to the development of athero-sclerosis requires further investigation. In the study by Dorresteijnet al. [14], 162 of the 367 patients in the cohort had T1 or T2 larynxcancers, and were treated with a 5 � 5 cm field using parallel-op-posed lateral beams. In the whole group, 14 cases of stroke oc-curred (RR, 5.6; 95% confidence interval [CI], 3.1–9.4): eight inpatients with laryngeal carcinoma (RR, 5.1; 95% CI, 2.2–10.1).Therefore, the length/volume/diameter of carotid artery does notappear to be important. Rather, the carotid artery behaves as a se-rial organ and it is the dose of RT to a particular section of arteryresulting in endothelial damage and subsequent accelerated ath-erosclerosis that is important. In other words, a focal point of crit-ical stenosis in the carotid artery may be just as clinicallysignificant as a diffusely narrowed artery and the risk of strokewould be related to the degree of stenosis at any one point of theartery.
The studies investigating CIMT and CAS have predominantlyshown a difference of around 20–50% in these endpoints betweenirradiated and unirradiated carotid arteries. The hypothesis thatradiation-induced injury results in increased arterial wall thicken-ing (increased CIMT) followed by plaque development in a propor-tion of patients (development of CAS) and lead to the development
Please cite this article in press as: Gujral DM et al. Radiation-induced carotidj.radonc.2013.08.009
of stroke/TIA in a subset of these patients, seems feasible from thecurrent data. It is reasonable to surmise that patients without in-creased CIMT are less likely to develop significant CAS and, conse-quently, are less likely to suffer a stroke.
The effect of increasing radiation dose on the incidence of caro-tid atherosclerosis has not been well characterised. Radiation dosesassociated with the development of atherosclerosis range from 35–44 Gy (patients undergoing radiotherapy for Hodgkin and non-Hodgkin lymphoma) to 50–80 Gy (patients undergoing RT forbreast cancer (SCF irradiation) or squamous cell carcinoma of thehead and neck) [38,51]. The latency period (i.e. time from radiationtherapy to neurological symptoms) also varies significantly be-tween patients [52]. There is some evidence to suggest that latencymay be dose-dependent [53]. Bowers et al. [16] reported a medianinterval of 17�5 years to stroke onset in patients treated with amedian of 40 Gy for Hodgkin disease. Dorresteijn et al. [14], onthe other hand, reported a median interval of 10 � 9 years to strokeonset in head and neck cancer patients who received 60–70 Gy.However, the relationship between latency and radiation dose isnot clear and requires further investigation.
Gianicolo et al. [46] showed that CIMT increases with increasingdoses of radiation to the neck over a range of 25–70 Gy. Martinet al. [42] noted increased CIMT at doses greater than 35 Gy, sug-gesting a dose effect with regard to vessel wall changes and dam-age. The retrospective study designs, small sample sizes and shortintervals from RT make it difficult to draw robust conclusions fromthese studies. At present, we do not understand what dose of radi-ation will render a significant risk of atherosclerosis or what doseconstraint would be appropriate for carotid-sparing radiotherapyin specific clinical scenarios, such as T1 or T2 glottic cancers wherenodal treatment is not required. It seems sensible that plan homo-geneity be evaluated for all other clinical scenarios to reduce hot-spots on the carotid arteries.
Measurement of CIMT has been a useful new techniqueenabling investigators to predict future risk of stroke and it hasbeen adopted as a surrogate end-point in many cardiovascularstudies [12]. The increase in CIMT seen in irradiated carotidarteries is most likely to represent the accelerated atherosclerosisthat occurs after treatment. Although further prospectivevalidation studies are required, it is reasonable to surmise thatCIMT may be a surrogate for stroke in this setting. The data alsoindicate that significant increase in CIMT occurs over a shortertime-frame (1–2 years for patients with head and neck cancer),making this an attractive endpoint on which to base studies ofradiation-induced vascular injury. Emerging new techniques,including ultrasound-based techniques such as speckle trackingto measure arterial stiffness (an early marker of atherosclerosis)and contrast-enhanced ultrasound to measure arterial inflamma-tion (a very early marker of arterial wall injury) [54,55], mayprovide useful tools to detect changes to the carotid artery at aneven earlier stage, and these may form suitable, earlier surrogatesfor atherosclerosis. Hopefully, these techniques may play a role inthe evaluation of patients with radiation-induced carotid arterydisease.
Conclusion
Carotid artery irradiation is a significant risk factor for athero-sclerosis and subsequent stroke or TIA. Although the body of evi-dence is limited, this risk appears to be related to radiation doseand interval from radiotherapy. The use of earlier surrogate end-points for neurological events with the advent of new imagingtechniques may provide greater understanding of the underlyingprocesses.
artery atherosclerosis. Radiother Oncol (2013), http://dx.doi.org/10.1016/

D.M. Gujral et al. / Radiotherapy and Oncology xxx (2013) xxx–xxx 7
Funding
None.
Conflict of Interest Notification
We declare no conflicts of interest.
Acknowledgements
None.
References
[1] Thomas E, Forbus WD. Irradiation injury to the aorta and the lung. AMA ArchPathol 1959;67:256–63.
[2] Cheng SW, Ting AC, Wu LL. Ultrasonic analysis of plaque characteristics andintimal-medial thickness in radiation-induced atherosclerotic carotid arteries.Eur J Vasc Endovasc Surg 2002;24:499–504.
[3] Taylor CW, Nisbet A, McGale P, Darby SC. Cardiac exposures in breast cancerradiotherapy: 1950s–1990s. Int J Radiat Oncol Biol Phys 2007;69:1484–95.
[4] Clarke M, Collins R, Darby S, Davies C, Elphinstone P, Evans E, et al. Effects ofradiotherapy and of differences in the extent of surgery for early breast canceron local recurrence and 15-year survival: an overview of the randomised trials.Lancet 2005;366:2087–106.
[5] Darby SC, McGale P, Taylor CW, Peto R. Long-term mortality from heart diseaseand lung cancer after radiotherapy for early breast cancer: prospective cohortstudy of about 300,000 women in US SEER cancer registries. Lancet Oncol2005;6:557–65.
[6] Sidhu PS, Naoumova RP, Maher VM, MacSweeney JE, Neuwirth CK, Hollyer JS,et al. The extracranial carotid artery in familial hypercholesterolaemia:relationship of intimal-medial thickness and plaque morphology withplasma lipids and coronary heart disease. J Cardiovasc Risk 1996;3:61–7.
[7] Halak M, Fajer S, Ben-Meir H, Loberman Z, Weller B, Karmeli R. Neckirradiation: a risk factor for occlusive carotid artery disease. Eur J VascEndovasc Surg 2002;23:299–302.
[8] Neale ML, Chambers JL, Kelly AT, Connard S, Lawton MA, Roche J, et al.Reappraisal of duplex criteria to assess significant carotid stenosis with specialreference to reports from the North American Symptomatic CarotidEndarterectomy Trial and the European Carotid Surgery Trial. J Vasc Surg1994;20:642–9.
[9] Goes E, Janssens W, Maillet B, Freson M, Steyaert L, Osteaux M. Tissuecharacterization of atheromatous plaques: correlation between ultrasoundimage and histological findings. J Clin Ultrasound 1990;18:611–7.
[10] Sterpetti AV, Schultz RD, Feldhaus RJ, Davenport KL, Richardson M, Farina C,et al. Ultrasonographic features of carotid plaque and the risk of subsequentneurologic deficits. Surgery 1988;104:652–60.
[11] O’Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson Jr SK.Carotid-artery intima and media thickness as a risk factor for myocardialinfarction and stroke in older adults. Cardiovascular Health StudyCollaborative Research Group. N Engl J Med 1999;340:14–22.
[12] Lorenz MW, Markus HS, Bots ML, Rosvall M, Sitzer M. Prediction of clinicalcardiovascular events with carotid intima-media thickness: a systematicreview and meta-analysis. Circulation 2007;115:459–67.
[13] Greenland P, Alpert JS, Beller GA, Benjamin EJ, Budoff MJ, Fayad ZA, et al. 2010ACCF/AHA guideline for assessment of cardiovascular risk in asymptomaticadults: a report of the American College of Cardiology Foundation/AmericanHeart Association Task Force on Practice Guidelines. J Am Coll Cardiol2010;56:e50–e103.
[14] Dorresteijn LD, Kappelle AC, Boogerd W, Klokman WJ, Balm AJ, Keus RB, et al.Increased risk of ischemic stroke after radiotherapy on the neck in patientsyounger than 60 years. J Clin Oncol 2002;20:282–8.
[15] Haynes JC, Machtay M, Weber RS, Weinstein GS, Chalian AA, Rosenthal DI.Relative risk of stroke in head and neck carcinoma patients treated withexternal cervical irradiation. Laryngoscope 2002;112:1883–7.
[16] Bowers DC, McNeil DE, Liu Y, Yasui Y, Stovall M, Gurney JG, et al. Stroke as alate treatment effect of Hodgkin’s Disease: a report from the Childhood CancerSurvivor Study. J Clin Oncol 2005;23:6508–15.
[17] Nilsson G, Holmberg L, Garmo H, Terent A, Blomqvist C. Increased incidence ofstroke in women with breast cancer. Eur J Cancer 2005;41:423–9.
[18] Hooning MJ, Dorresteijn LD, Aleman BM, Kappelle AC, Klijn JG, Boogerd W,et al. Decreased risk of stroke among 10-year survivors of breast cancer. J ClinOncol 2006;24:5388–94.
[19] Jagsi R, Griffith KA, Koelling T, Roberts R, Pierce LJ. Stroke rates and risk factorsin patients treated with radiation therapy for early-stage breast cancer. J ClinOncol 2006;24:2779–85.
[20] Woodward WA, Giordano SH, Duan Z, Hortobagyi GN, Buchholz TA.Supraclavicular radiation for breast cancer does not increase the 10-year riskof stroke. Cancer 2006;106:2556–62.
Please cite this article in press as: Gujral DM et al. Radiation-induced carotidj.radonc.2013.08.009
[21] Smith GL, Smith BD, Buchholz TA, Giordano SH, Garden AS, Woodward WA,et al. Cerebrovascular disease risk in older head and neck cancer patients afterradiotherapy. J Clin Oncol 2008;26:5119–25.
[22] De Bruin ML, Dorresteijn LD, Van’t Veer MB, Krol AD, van der Pal HJ,Kappelle AC, et al. Increased risk of stroke and transient ischemic attackin 5-year survivors of Hodgkin lymphoma. J Natl Cancer Inst 2009;101:928–37.
[23] Bamford J, Sandercock P, Dennis M, Burn J, Warlow C. A prospective study ofacute cerebrovascular disease in the community: the Oxfordshire CommunityStroke Project – 1981–86. 2. Incidence, case fatality rates and overall outcomeat one year of cerebral infarction, primary intracerebral and subarachnoidhaemorrhage. J Neurol Neurosurg Psychiatry 1990;53:16–22 [PMCID:1014091].
[24] Alfredsson L, von Arbin M, de Faire U. Mortality from and incidence of stroke inStockholm. Br Med J [Clin Res Ed] 1986;292:1299–303 [PMCID: 1340310].
[25] Lisdonk van de EH BvdW, Huygen FJA. Ziekten in de Huisartsenpraktijk. 3rd ed.Maarssen: Elsevier/Bunge; 1999.
[26] National Center for Health Statistics: National Hospital Discharge Survey[cited]. Available from: http://www.cdc.gov/nchs/about/major/hdasd/nhdsdes.htm.
[27] Silverberg GD, Britt RH, Goffinet DR. Radiation-induced carotid artery disease.Cancer 1978;41:130–7.
[28] Friedlander AH, Eichstaedt RM, Friedlander IK, Lambert PM. Detection ofradiation-induced, accelerated atherosclerosis in patients withosteoradionecrosis by panoramic radiography. J Oral Maxillofac Surg1998;56:455–9.
[29] Freymiller EG, Sung EC, Friedlander AH. Detection of radiation-inducedcervical atheromas by panoramic radiography. Oral Oncol 2000;36:175–9.
[30] Moritz MW, Higgins RF, Jacobs JR. Duplex imaging and incidence of carotidradiation injury after high-dose radiotherapy for tumors of the head and neck.Arch Surg 1990;125:1181–3.
[31] Dubec JJ, Munk PL, Tsang V, Lee MJ, Janzen DL, Buckley J, et al. Carotid arterystenosis in patients who have undergone radiation therapy for head and neckmalignancy. Br J Radiol 1998;71:872–5.
[32] Carmody BJ, Arora S, Avena R, Curry KM, Simpkins J, Cosby K, et al.Accelerated carotid artery disease after high-dose head and neckradiotherapy: is there a role for routine carotid duplex surveillance? JVasc Surg 1999;30:1045–51.
[33] Lam WW, Leung SF, So NM, Wong KS, Liu KH, Ku PK, et al. Incidence of carotidstenosis in nasopharyngeal carcinoma patients after radiotherapy. Cancer2001;92:2357–63.
[34] Brown PD, Foote RL, McLaughlin MP, Halyard MY, Ballman KV, Collie AC, et al.A historical prospective cohort study of carotid artery stenosis afterradiotherapy for head and neck malignancies. Int J Radiat Oncol Biol Phys2005;63:1361–7.
[35] Woodward WA, Durand JB, Tucker SL, Strom EA, Perkins GH, Oh J, et al.Prospective analysis of carotid artery flow in breast cancer patients treatedwith supraclavicular irradiation 8 or more years previously: no increase inipsilateral carotid stenosis after radiation noted. Cancer 2008;112:268–73[PMCID: 3402340].
[36] Meeske KA, Siegel SE, Gilsanz V, Bernstein L, Nelson MB, Sposto R, et al.Premature carotid artery disease in pediatric cancer survivors treated withneck irradiation. Pediatr Blood Cancer 2009;53:615–21.
[37] Feehs RS, McGuirt WF, Bond MG, Strickland HL, Craven TE, Hiltbrand JB.Irradiation. A significant risk factor for carotid atherosclerosis. ArchOtolaryngol Head Neck Surg 1991;117:1135–7.
[38] King LJ, Hasnain SN, Webb JA, Kingston JE, Shafford EA, Lister TA, et al.Asymptomatic carotid arterial disease in young patients following neckradiation therapy for Hodgkin lymphoma. Radiology 1999;213:167–72.
[39] Heikens J, Ubbink MC, van der Pal HP, Bakker PJ, Fliers E, Smilde TJ, et al. Longterm survivors of childhood brain cancer have an increased risk forcardiovascular disease. Cancer 2000;88:2116–21.
[40] So NM, Lam WW, Chook P, Woo KS, Liu KH, Leung SF, et al. Carotid intima-media thickness in patients with head and neck irradiation for the treatmentof nasopharyngeal carcinoma. Clin Radiol 2002;57:600–3.
[41] Dorresteijn LD, Kappelle AC, Scholz NM, Munneke M, Scholma JT, Balm AJ, et al.Increased carotid wall thickening after radiotherapy on the neck. Eur J Cancer2005;41:1026–30.
[42] Martin JD, Buckley AR, Graeb D, Walman B, Salvian A, Hay JH. Carotid arterystenosis in asymptomatic patients who have received unilateral head-and-neck irradiation. Int J Radiat Oncol Biol Phys 2005;63:1197–205.
[43] Bilora F, Pietrogrande F, Petrobelli F, Polato G, Pomerri F, Muzzio PC. Isradiation a risk factor for atherosclerosis? An echo-color Doppler study onHodgkin and non-Hodgkin patients. Tumori 2006;92:295–8.
[44] Shariat M, Alias NA, Biswal BM. Radiation effects on the intima-mediathickness of the common carotid artery in post-radiotherapy patients withhead and neck malignancy. Postgrad Med J 2008;84:609–12.
[45] Shai E, Siegal S, Michael Z, Itzhak K, Ronen R, Dror M, et al. Carotidatherosclerotic disease following childhood scalp irradiation. Atherosclerosis2009;204:556–60.
[46] Gianicolo ME, Gianicolo EA, Tramacere F, Andreassi MG, Portaluri M.Effects of external irradiation of the neck region on intima mediathickness of the common carotid artery. Cardiovasc Ultrasound 2010;8:8[PMCID: 2846876].
[47] Muzaffar K, Collins SL, Labropoulos N, Baker WH. A prospective study of theeffects of irradiation on the carotid artery. Laryngoscope 2000;110:1811–4.
artery atherosclerosis. Radiother Oncol (2013), http://dx.doi.org/10.1016/

8 Radiation-induced carotid atherosclerosis
[48] Bilora F, Pietrogrande F, Campagnolo E, Rossato A, Polato G, Pomerri F, et al.Are Hodgkin and non-Hodgkin patients at a greater risk of atherosclerosis? Afollow-up of 3 years. Eur J Cancer Care (Engl) 2010;19:417–9.
[49] Chambless LE, Folsom AR, Clegg LX, Sharrett AR, Shahar E, Nieto FJ, et al.Carotid wall thickness is predictive of incident clinical stroke: theAtherosclerosis Risk in Communities (ARIC) study. Am J Epidemiol2000;151:478–87.
[50] Cheng SW, Wu LL, Ting AC, Lau H, Lam LK, Wei WI. Irradiation-inducedextracranial carotid stenosis in patients with head and neck malignancies. AmJ Surg 1999;178:323–8.
[51] Steele SR, Martin MJ, Mullenix PS, Crawford JV, Cuadrado DS, Andersen CA.Focused high-risk population screening for carotid arterial stenosis afterradiation therapy for head and neck cancer. Am J Surg 2004;187:594–8.
Please cite this article in press as: Gujral DM et al. Radiation-induced carotidj.radonc.2013.08.009
[52] Conomy JP, Kellermeyer RW. Delayed cerebrovascular consequences oftherapeutic radiation. A clinicopathologic study of a stroke associated withradiation-related carotid arteriopathy. Cancer 1975;36:1702–8.
[53] Dorresteijn LD, Stewart FA, Boogerd W. Stroke as a late treatment effect ofHodgkin’s disease. J Clin Oncol 2006;24:1480. author reply – 1.
[54] Bjallmark A, Lind B, Peolsson M, Shahgaldi K, Brodin LA, Nowak J.Ultrasonographic strain imaging is superior to conventional non-invasivemeasures of vascular stiffness in the detection of age-dependent differences inthe mechanical properties of the common carotid artery. Eur J Echocardiogr2010;11:630–6.
[55] Feinstein SB. Contrast ultrasound imaging of the carotid artery vasa vasorumand atherosclerotic plaque neovascularization. J Am Coll Cardiol2006;48:236–43.
artery atherosclerosis. Radiother Oncol (2013), http://dx.doi.org/10.1016/
Copyright © 2022 FDOKUMEN




















