
Temporal and Demographic Patterns of Non-Hodgkin's Lymphoma Incidence in Pennsylvania
Upload
independentCategory
view
1download
0
ht. J. R&i&on Oncology Bwl. Phys., Vol. 10, pp. 197-210 0360-3016/64 $3.00 + .oO
Printed in the U.S.A. All tights reserved. Copyright 0 1984 Pergamoo Press Ltd.
??Original Contribution
THE EORTC TREATMENT OF EARLY STAGES OF HODGKIN’S DISEASE: THE ROLE OF RADIOTHERAPY
M. TURIANA, M.D.,7 M. HENRY-AMAR, M.Sc.,$ M. HAYAT, M.D.,7 M. BURGERS, M.D.,5 M. QASIM, M.D.,T[ R. SOMERS, M.D.&
W. SIZGG, M.D.,1 AND E. VAN DER %XUEREN, M.D.1 EORTC Radiotherapy, Chemotherapy Group
Since 1964, the European Organisation for Research and Treatment of Cancer has conducted three subsequent dinical trials on clinical Stages (CS) I + II Hodgkin’s disease (I-ID) in which 1059 patients have been entered. The iirst trial compared regional radiotherapy (RT) with mantle geld or inverted Y, versus the same RT followed by a weelcly injection of vinblastine for 2 years. The relapse free survival (RI%) and overall survival (S) were higher in patients treated by RT and chemotherapy (CT). This heneiit, however, was sign&leant only in patients with a mixed cellularity histologic type. The second trial compared the therapeutic eilkacy of splenic irradiation versus splenectomy and found that in both arms, RPS and S were identical. Moreover, it was found that splenic involvement was correlated with an increased incidence of relapse in extraaodal sites and in non irradiated lymphatic areas. In this trial, CT was given only to patients with poor histologic types, mixed cellularity or lymphocytic depletion. In the third trial, staging Iaparotomy was performed only to further delineate a good prognostic group which could be treated by RT alone. In this Iimited treatment group, there was no difference in RFS and S between mantle geld and mantle field + para-aortic RT. In the extensive treatment group, total nodal irradiation (INI) was compared with RT + MOPP. The RIB was slightly lower in the TNI arm, but there was no significant difference in S. The data of the 3 trials underline the importance of proguo& factors in the choice of optimal treatment and show that their significauce depends upon the type of treatment. Multivariate statistical analyses showed that the main prognostic factors, which can help to identify the subsets of patients who can be treated by RT alone, are (1) systemic symptoms and elevated erythrocyte sedimentation rate (ESR), (2) the number of involved lymphatic areas, and (3) staging laparotomy. Extended RT (mantle + para-aortic + spleen treatment) gives satisfactory results in patients without systemic symptoms and/or elevated ESR and one or two involved sites, whereas TNI or combined modality treatment becomes mandatory for patients with 3 or more involved sites or spienic involvement and/or systemic symptoms. With proper adjustment of the irradiated volume, a very large proportion of CS I + II patients can be best treated by RT alone.
Hodgkin’s disease, Radiotherapy, Prognostic factors, Staging Iaparotomy.
INTRODUCTION
Very high survival rates can be obtained in patients with clinical Stages (CS) I + II Hodgkin’s disease (HD) treated by combined extended field radiotherapy (RT) and multi-agent chemotherapy (CT). However, such aggressive treatment is a heavy burden to the patient and carries the well known risks of gonadal damage and secondary cancers.
On the other hand, several studies3.8~9,‘1,*3,‘9,22.23 in particular the European Organization for Research on Treatment of Cancer (EORTC) trials’2~25J7~30 have shown that very high survival rates can be obtained by RT
alone in certain subsets of patients. However, the precise definition of these subsets requires the identification of the relevant prognostic factors. For this reason we undertook an analysis of the various prognostic factors in 1059 patients with CS I + II HD who had been entered into the three controlled clinical trials conducted by the EORTC. In these series of patients, several prognostic indicators had been registered prospectively in order to allow such an analysis. As we have shown previouslyr4g” the various prognostic indicators are strongly correlated with one another, and their relative importance varies with the type of treatment. We there-
tInstitut GustavaRoussy, Villejuif, France. &Jnitk de Recherches Statistiques, INSERM. §Antoni van Leeuwenhoek Ziekenhuis, Amsterdam, The
Netherlands. %Rotterdam-Radiotherapeutisch Instituut, Rotterdam, The
Netherlands. tAcad. Ziekenhuis, St. Rafael, Leuven, Belgium.
197
Reprint requests to: Prof. M. Tubiana, Institut Gustave- Roussy, Rue Camille Desmoulins, 94805 Villejuif Cedex, France. Acknowledgements-The authors wish to express their grat- itude to Dr. D. Clarke for his careful reading of the text and for his helpful criticisms and suggestions.
Accepted for publication 23 September 1983.

198 Radiation Oncology 0 Biology ??Physics February 1984, Volume 10, Number 2
fore performed multivariate analyses for the diff- erent treatment groups. This paper has two aims. The first is to report or update the results of the three trials, the second is to discuss the role of RT in the treatment of early stages HD in light of the results obtained during this 20 years experience. The data show that with the help of a few prognostic indicators, it is poss- ible to define a strategy for: (1) the staging procedure, and (2) the treatment of patients with CS I + II HD.
delivered to the para-aortic lymph nodes by an anterior and a posterior field. For patients assigned to the splenic irradiation group, the abdominal radiation field encom- passed the para-aortic area, the spleen and the splenic hilar nodes.
Patients with mixed cellularity (MC) or lymphocytic depletion (LD) histologic subtypes subsequently re- ceived adjuvant CT for 2 years: either VLB alone as in the Hl trial, or a combination of VLB and procarbazine (PCZ) (Table 1).
METHODS AND MATERIALS Since 1963, the radiotherapy-chemotherapy group of
EORTC (see Appendix) had conducted 3 controlled trials on previously untreated patients with CS I + II HD; 1059 patients have been enrolled in these trials. Fourteen hospital centers participated.
Between 1972 to 1976, 300 patients were included in the trial (Table 2) from 9 hospital centers. Of these, 284 had their slides reviewed by the histological review c0mmitee.t The multivariate study of prognostic factors was performed on the 256 patients from whom all the information was available.
The first trial (H, : 1964-1971) compared regional RT alone with a combination of the same RT followed by single agent CT. The patients were staged with careful clinical and radiological examination. No laparotomy was performed. Radiotherapy was carried out using the mantle field or the inverted Y technique (40 Gy were delivered over a 4 week period). No prophylactic irra- diation was given to the other side of the diaphragm. Four weeks after completion of irradiation, the patients were randomly assigned to one of two groups: (a) no further treatment, and (b) a weekly injection of vin- blastine (VLB) for 2 years (Table 1). Two hundred- eighty-eight patients were included in the study (Table 2). Multivariate analyses were performed for the 206 patients for whom information on all the prognostic factors had been coded and stored in the Villejuif computer.
H, TRIAL. The trial started in 1977 and ended in July 1982. It was designed on the basis of the H, trial data and on the preliminary results of H2 trial. Its aim was to further delineate the subgroups of patients with CS I + II who had a more or less favorable prognosis. New factors, then considered to be unfavorable, were intro- duced: age, erythrocyte sedimentation rate (ESR), sys- temic symptoms (SS), and pattern of presentation. His- tologic MC and LD remained unfavorable indicators. Thus in the limited treatment group were patients who met all the following criteria: age less than 40 years, favorable histologic subtype [lymphocytic predominance (LP) or nodular sclerosis (NS)], ESR less than 70mm/lst hr. CS II patients without mediastinal in- volvement were considered unfavorable. All the patients eligible for the limited treatment group underwent diag- nostic laparotomy. They remained in this group only if the staging laparotomy was negative.
H, TRIAL. In 1971, on the basis of the preliminary results of the H, trial, a second clinical trial (H,) was designed in which untreated patients with supra- diaphragmatic CS I + II HD were randomized to un- dergo staging laparotomy or splenic irradiation. All patients received mantle field irradiation as well as para-aortic lymph node irradiation. The aims of this trial were: (a) to compare the therapeutic efficacy of splenic irradiation versus splenectomy, and (b) to assess the prognostic significance of the information provided by laparotomy. In order to achieve this goal, all patients received the same treatment regardless of the results of the laparotomy, unless there was liver or bone marrow involvement.
Hence in this trial, laparotomy was intented to select a group of patients with a good prognosis and for whom RT alone might be sufficient. These patients were ran- domized to receive a mantle field alone or mantle field plus para-aortic lymph node irradiation. The dose was 40 Gy over 4 weeks, followed by a boost to bulky masses when deemed necessary.
Patients were first treated by mantle field irradiation (4OGy over 4 weeks plus a booster of 5 Gy to slowly regressing bulky masses). Two to four weeks after completion of this irradiation, 40 Gy over 4 weeks were
Patients who were categorized as high risk were not submitted to staging laparotomy since more extensive treatment was thought to be necessary. Patients in this group and patients of the previous group with positive laparotomies were randomized to receive either com- bined modality treatment (3 MOPP-RT-3 MOPP) or total nodal irradiation (TNI) (Table 1). Four hundred and seventy-one patients were included at 14 cooper- ating centers (Table 2). Of the 144 patients allocated to TNI, 40 did not receive pelvic irradiation in order to avoid gonadal damage. These were mostly young women. They are therefore not comparable to patients treated by TNI.
tThe histological review committee was composed of R. Girard-Marchant and J. A. M. Van Unnik.

Role of radiotherapy in Hodgkin’s disease ??M. TUBIANA et al. 199
Table 1. Design of the three consecutive EORTC trials Hl, H2 and H5
Hl trial Mantle RT or
(1964-71) inverted Y RT /No further treatment
\VLB for 2 years
H2 trial (1972-76)
, Mantle + spleen + para-aortic RT
\Splenectomy + mantle + para-aortic RT
for histologic types MC or LD
,VLB 2 years
\VLB + PCZ 2 years
H5 trial ??Patients < 40 years and LP-NS and ESR < 70 and CS I or CS II med. + : Staging laparotomy
/ mantle RT
If negative laparotomy \mantle + para-aortic RT
(1977-82) MOPP /
x 3-Mantle RT-MOPP x 3 ??Other patients (no laparotomy or positive laparotomy
\Total nodal irradiation
Table 2. Number of patients included in the 3 EORTC trials by the cooperating centers
Hi H, H, 19671 1972-76 1977-82 Total
The Netherlands Amsterdam Leiden Nijmegen Rotterdam The Hague Utrecht
Belgium Brussels (IJB) La Louvitre Liege Leuven
Italy Florence
France Bordeaux Caen Lyon Nice Paris (Hotel-Dieu) Reims Rouen Villejuif (IGR)
Total
37 25
4 87
1
11
6 1
4 13 10
64
17 84
9
11
15
7
100 201 37 62 14 35 53 224
3 13 8 8
021 6
46
21
11 21
1 67
288
11
82
300
11 37
103
471
43 6 6
41
15
4 41 10 11 21 22 38
252
1059
Statistical analyses. A registration form was used for absence (A) or presence (B) of each patient at entry to one of these trials: prior to subtype, mediastinal involvement.
SS, ESR, histologic
treatment the data were entered in the Villejuif data It was shown in a previous paper2’j that ESR and SS bank. The following potential prognostic factors were are strongly correlated (p < 0.001) but that they never- analyzed: age, sex, the number of clinically involved theless have an independent prognostic influence. Thus lymph nodes (Stages I, II, with two involved lymph node the combined influence of these two parameters has an areas, and II, with 3 or more involved lymphatic areas), even greater prognostic significance than either alone.26

200 Radiation Oncology ??Biology ??Physics February 1984, Volume 10, Number 2
The following combinations, e.g., A, ESR < 50 or B, ESR < 30 (called a subgroup), and A, ESR > 50 or B, ESR > 30 (called j subgroup) are considered in the present multivariate studies.
The Cox model’ was employed because it permits the evaluation of the independent influence of each of the prognostic factors on overall survival (S) and relapse- free survival (RFS). The influence of treatment indepen- dent of the distribution of the prognostic factors can also be studied. Each combination of prognostic factors considered corresponds to a risk coefficient for relapse (or death).
On the basis of the risk coefficient, one can calculate the relative risk [RR, = exp.(&j] which expresses the ratio of the relapse (or death) probabilities for values of the prognostic indicators coded 0 or 1. For example the H, trial, when the risk coefficient for RFS and histologic subtype is /?y= 0.72, then Rii, = 2.05. This means that with all other factors remaining constant, the probability of relapse is 2.05 times greater for patients with MC histology than for patients with LP or NS histology.
No multivariate analyses have been performed for patients in the H, trial because the average follow-up is too short. However, the significance of a few prognostic indicators was assessed.
RESULTS In the first trial (H,), all patients were randomly
assigned to either RT alone or RT + VLB. No RT was carried out on the clinically uninvolved side of the diaphragm. The results have been previously re- ported*‘“’ and are updated in Fig. 1. In the RT alone arm, the long term RFS was only 38 vs 61% in RT + CT arm (p < 0.001). There was a high incidence of relapse in the para-aortic region in patients treated by RT alone (Table 3). The long term survival was slightly higher in the RT + CT arm (Fig. 1): 70 vs 60% (p = 0.08). These results demonstrated for the first time the efficacy of combining RT and CT in the treatment of early stages HD. However, the benefit of RT + CT combination was significant only in patients with MC histologic type. Since most of relapsing patients were treated with CT with or without RT, 47% of patients in the RT alone arm and 41% of the long term suroiuors in this arm received CT during the course of the disease. Multivariate anal- yses (Table 4) showed that the 2 prominent prognostic factors were histologic type and the combined effect of ESR and SS.
Figure 2 and Table 5 update the results of the second trial, HZ. They confirm the previously published pre- liminary results25 and show that splenic irradiation and splenectomy have the same therapeutic efficacy, while the sequellae caused by the irradiation of the left kidney are small”. The data also underline the prognostic significance of the laparotomy findings: splenic in- volvement is correlated with an increased incidence of relapse (RFS at 7 years: 57 + 8% vs 80 f 4% in negative
Fig. 1. H 1 trial: relapse-free survival (RFS) and overall survival (S) of the 2 treatment arms (with 95% confidence limits).
Table 3. H 1 trial (favorable patients): Incidence of para-aortic relapses in patients with supradiaphragmatic disease treated by mantle field irradiation (RT) with or without vinblastine (VLB); Incidence of deaths following para-aortic relapse
Histologic types RT RT + VLB
LP NS Relapses 7/63 11% 4142 10YO Deaths 317 114
MC Relapses 12/30 40% 5!32 16”” Deaths 9112 3:s
Relapses p < 0.01 NS Deaths NS NS
Note: H, trial-Favorable patients/relapses in para-aortic areas and deaths.
laparotomy group, p < 0.01) not only in extra nodal sites but also in non irradiated lymphatic areas.” The proto- col of this second trial (H,) was designed partly on the basis of the preliminary results of the H, trial: thus the only prognostic factor which was taken into account for the treatment was the histologic type. Patients with unfavorable histologic types (MC + LD) received CT; all patients were given extended field RT (mantle field + para-aortic lymph node irradiation + splenic RT or splenectomy). Sixty-seven percent of the patients were therefore treated initially by RT alone; the long term RFS among them was 65%. This improvement in RFS over the H1 results was a result of the selection of patients according to histologically subtype and the implementation of more appropriate RT. On the whole, taking into account patients treated with CT following a relapse, about 44% of the patients and 49% of long term survivors did not receive CT during the course of their disease.
Two multivariate analyses of prognostic factors had to be performed for the Hz trial, one for patients treated with RT alone (Table 6) and the other for patients treated with RT + CT (Table 7). However: since the choice of treatment was based on the histologic

Role of radiotherapy in Hodgkin’s disease ??M. TUBIANA et al. 201
Table 4. Results of the multivariate analysis (Cox model) of the prognostic indicators in the Hl trial, patients with supra- diaphragmatic presentation
Prognostic indicators
Clinical Mediastinal Histology Age ESR and SS stage involv. Sex Treatment
LP-NS MC 15-39 < 15 a B I II, II3 Med 0 Med + M F RT RT+VLB >, 40
Relative 1 2.05 1 1.40 1 2.36 1 1.16 0.88 1 0.84 1 0.85 1 0.43 RFS risk RRi p < 0.001 p < 0.10 p < 0.001 NS NS NS p < 0.001
Relative 1 2.25 1 1.43 1 1.43 1 1.07 0.34 1 1.11 1 0.62 1 0.64 S risk RRi p < 0.001 NS NS p < 0.05 NS NS p < 0.10
a = No SS, ESR < 50 or SS, ESR < 30. fi = No SS, ESR 2 50 or SS, ESR > 30. Note: The values of the risk coefficients of each parameter are calculated simultaneously. For RFS histology, ESR and SS have
a significant prognostic influence (p c 0.001) independently of all other prognostic indicators, but for survival only histology (p < 0.01) and CS II3 (p < 0.05) are significant independently of other indicators. For RFS, the prognostic influence remains significant dependent of treatment for histology (p < O.OOl), age (p < 0.05), ESR and SS @ < 0.01) and sex (p < 0.05). For survival, significant indicators were histology (p < O.OOl), sex (p < O.Ol), age (p < 0.05) and mediastinum involvement (p < 0.05) of treatment.
Table 5. RFS and survival (S) rates in the various subsets of patients of the H2 trial
Number of patients
RFS at 7 years S at 7 years (mean % + SD) (mean % + SD)
All patients
; p value
CS I + III negative laparotomy
; CS II, negative laparotomy
a B
Systemic symptoms and ESR after adjustment for number of involved areas, p value
Number of involved areas after adjustment for systemic symptoms and ESR, p value
300 71 f3 203 80 f 3 92 50 f 6
< 0.001
62 93 f 3 14 79+ 11
17 67+_12 11 42+ 16
0.03
< 0.005
83+2 84 f 3 80+ 5
NS
90 + 5 78+11
85 + 10 82+ 12
NS
NS
a = No SS and ESR < 50 or SS and ESR < 30. fl = No SS and ESR >, 50 or SS and ESR > 30. Note: Influence of the number of involved areas, and, in patients with a negative
laparotomy, systemic symptoms and ESR. Patients with MC or LD histologic types were given chemotherapy.
classification as determined by the hospital pathologist, some patients classified as NS by the histology review committee received CT because they had been initially classified as MC (28 out of 181, 15%). On the other hand, some patients initially classified as NS and reclassified as MC at the time of the histologic review did not receive CT (26 out of 90, 29%). Therefore, the revised histology could be studied as a prognostic factor as indicated in Tables 6 and 7. However, it should be
remembered that patients with MC subtype who did not receive CT and patients with NS subtype who did receive CT may not be representative of those histologic sub- types since they represent reclassified patients.
For patients treated without CT, in whom splenic irradiation and splenectomy have the same therapeutic efficacy (Fig. 3), the most important prognostic factor for RFS was the number of involved lymph node sites 0, < 0.001); other important factors included the combi-

202 Radiation Oncology ??Biology ??Physics February 1984. Volume 10. Number 2
Table 6. Multivariate analysis of the prognostic indicators
Prognostic indicators
Clinical Mediastinal Sex Age ESR and SS stage involv, Histology Laparotomk
_-.__ ____- .~ ~...____.~ ~
M F < 40 > 40 z a I 111 II, Med 0 Med + Lp NS MC-LD ;p” PS 1.1, PS ,,,_, \
RFS ~&dive 1 0.67 1 1.40 1 2.56 1 0.74 2.80 1 0.88 I 2.05 0.51 I 0.61 2 18 nsk Rl% NS NS p < 0.001 p < 0.001 NS p <0.10 p < 0.01
S Relative 1 0.68 1 2.27 1 1.60 1 0.36 1.32 1 1.88 I 0.77 0.91 1 0.76 1.30 risk Ri?i NS p <O.lO NS p <O.lO NS NS NS
Note: Patients from the H2 trial treated initially without chemotherapy (mainly patients with nodular sclerosis histologic type). H, trial: Patients without chemotherapy. Multivariate analysis (Cox model). Values of the risk coefficients. For RFS all the risk
coefficients are significantly different from zero (p < 0.001); ESR and SS (p < O.OOl), number of involved areas 0, < 0.001). mediastinum involvement (p < 0.01) and histology (p < 0.05) retain significance independent of the results of laparotomy; number of involved areas (p < O.OOl), ESR and SS (p < 0.001) and results of laparotomy (p < 0.01) retain significance independent of all other prognostic factors. For survival, only clinical stage (number of involved areas) has a significant influence independent of the results of laparotomy (p < 0.05), and age and the number of involved areas have borderline significance 0, < 0.10) independent of all other prognostic indicators.
a = No SS, ESR < 50 or SS, ESR < 30. /I = No SS, ESR > 50 or SS, ESR 2 30.
Table 7. Multivariate analysis of the prognostic indicators
Sex Age ESR and SS Clinical
stage Mediastinal
involv. Histology Laparotoml
Prognostic indicators
M F < 40 > 40 a B I 11, 11, MedO Med + LP(t) NS MC-LD No ps lap l-l,
ps 111 I\
RFS Relative 1 0.66 1 0.73 1 3.32 1 0.41 0.57 1 2.18 - 1 0.64 1 0.51 I.16 risk, Rl% NS NS p < 0.05 NS NS NS NS
S Relative 1 1.38 1 14.88 1 1.13 1 0.73 2.92 1 1.63 I 0.41 1.54 I 1.25 7.46 risk RI% NS p < 0.001 NS NS NS NS NS
Note: Patients from the H2 trial treated initially with combination RT and CT (mainly patients with mixed cellularity histologrc type).
H2 trial: Patients treated initially with chemotherapy. Multivariate analysis (Cox Model). Values of the risk coefficients. For RFS, only the combination ESR-SS is statistically significant (p < 0.05) independent of all other prognostic indicators. For survival, only age is significant (p < 0.001) independent of all other prognostic indicators.
(t) No relapse among the 3 LP patients. a = No SS, ESR < 50 or SS, ESR < 30. fi = No SS, ESR > 50 or SS, ESR 2 30.
nation of ESR-SS @ < 0.001) and splenic involvement at laparotomy @ < 0.01). With respect to survival, the number of involved sites and age were of borderline significance, only (p < 0.10). By combining the two factors, number of involved sites and ESR-SS, one can identify a favorable and an unfavorable prognostic group (Table 8). It is of interest to note that in this poor prognostic group the incidence of positive laparotomies was significantly higher (p < 0.02), and the extent of abdominal disease was greater as reflected by the num-
ber of involved sites below the diaphragm (Table 9). We observed a higher RFS in those patients initially
treated with RT + CT (Table 7), and subsequent anal- yses of prognostic factors revealed that the only factor that influenced RFS was the combined effect of ESR-SS (p < 0.05). Age was the only indicator which significantly influenced survival in patients initially treated by RT + CT (p < 0.001). The influence of age is very interesting because while it has little influence on RFS, it has a marked impact on survival. This suggests

Role of radiotherapy in Hodgkin’s disease 0 M. TUBMNA et al. 203
Fig. 2. H2 trial: relapse-free survival (RFS) and overall survival (S) of the 2 treatment arms (with 95% confidence limits).
I PATIENTS WITHOUT CHEMOTHERAPY
.25 _ ,#l,.“,C ,rr.*mion ,loI,
---- *pl*ll.ctoln, (0.)
Ii2 TRIAL
01 , 1 2 3 4 5 0 yrs 7
Fig. 3. H2 trial: relapse-free survival (RFS) and overall survival (S) of the 2 treatment arms for patients treated without chemotherapy (with 95% confidence limits).
MOPP (141 pta 1
u (90 - )
M+PA (99 - 1
TNI (99 - 1
TNI (40-j incompl*le
.5 H5 TRIAL I OISEASE -FREE SURVIVAL
w
0 1 2 3 year*
Fig. 4. HS trial: relapse-free survival (RFS) by treatment group (with 95% confidence limits). M =mantle RT, PA = para-aortic RT, TN1 = total nodal RT, MOPP = 3 cycles + M + 3 cycles.
that patients over the age of 40 are salvaged much less effectively after relapse than are their younger counter- parts.
In the third trial (H,), the favorable prognostic group was categorized based on the five prognostic indicators which had been identified in the H, trial and in the preliminary data of the Hz trial. They comprised approx- imately 40% of the patients entered into this trial (Figs. 4 and 5, Table 10). In these patients, the RFS was about 85% at 3.5 years in both arms, either mantle field or
mantle field + para-aortic irradiation (Fig. 4). The pa- tients in the unfavorable group received either combined modality treatment (MOPP + RT) or TNI. In fact, pelvic irradiation was not delivered to 40 of the patients below the age of 40 so that the gonads would not be irradiated. TN1 yielded a RFS of 82 + 5% at 3.5 years; in those treated without pelvic RT the RFS was 74%. The difference between these two RT groups is mar- ginally significant (p = 0.06). However it should be noted that those patients who did not receive pelvic RT comprised mostly young women. Therefore the beneficial effect of pelvic RT might well be under- estimated.
Survival after relapse In both the H, (Fig. 6) and H, trials, the survival after
relapse is slightly lower in patients initially treated by a combination of RT and CT. Additionally, survival after relapse is strongly correlated with age with survival being significantly lower for patients over 40 (p < 0.02). Furthermore, the salvage rate for patients over 40 who were initially treated by CT was particularly poor.
Comparison between the three trials The proportion of patients having received CT either
initially or for treatment of a relapse were respectively 72, 56 and 40% in the H,, H2 and H, trials. However, comparison of the H, trial with the previous trials is difficult, since half of these we presently consider as unfavorable patients, were treated by TNI. If the entire group of high risk patients had received CT and if all of the low risk patients had been spared CT initially, the proportion of patients ultimately receiving CT either initially or for relapse would have been greater (50%). Conversely if all of the high risk patients had been treated by TN1 alone, the proportion of patients re- ceiving CT would have been only 15%.
There is a clear improvement in RFS and S from H, to H2 and from Hz to HS (Fig. 7). This advance has resulted from the identification of certain prognostic factors and the subsequent implementation of more
SURVIVAL
(0 .,
0 1 2 Yf I
Fig. 5. H5 trial: overall survival (S) by treatment group (with 95% confidence limits).
204
1.00
.80
60
.40
.20
Radiation Oncology ??Biology ??Physics February 1984, Volume 10, Number Z
RT*VLB
(36) (29) (62)
(17)
SURVIVAL AFTER RELAPSE
0 2 4 6 8 IO yrs 12
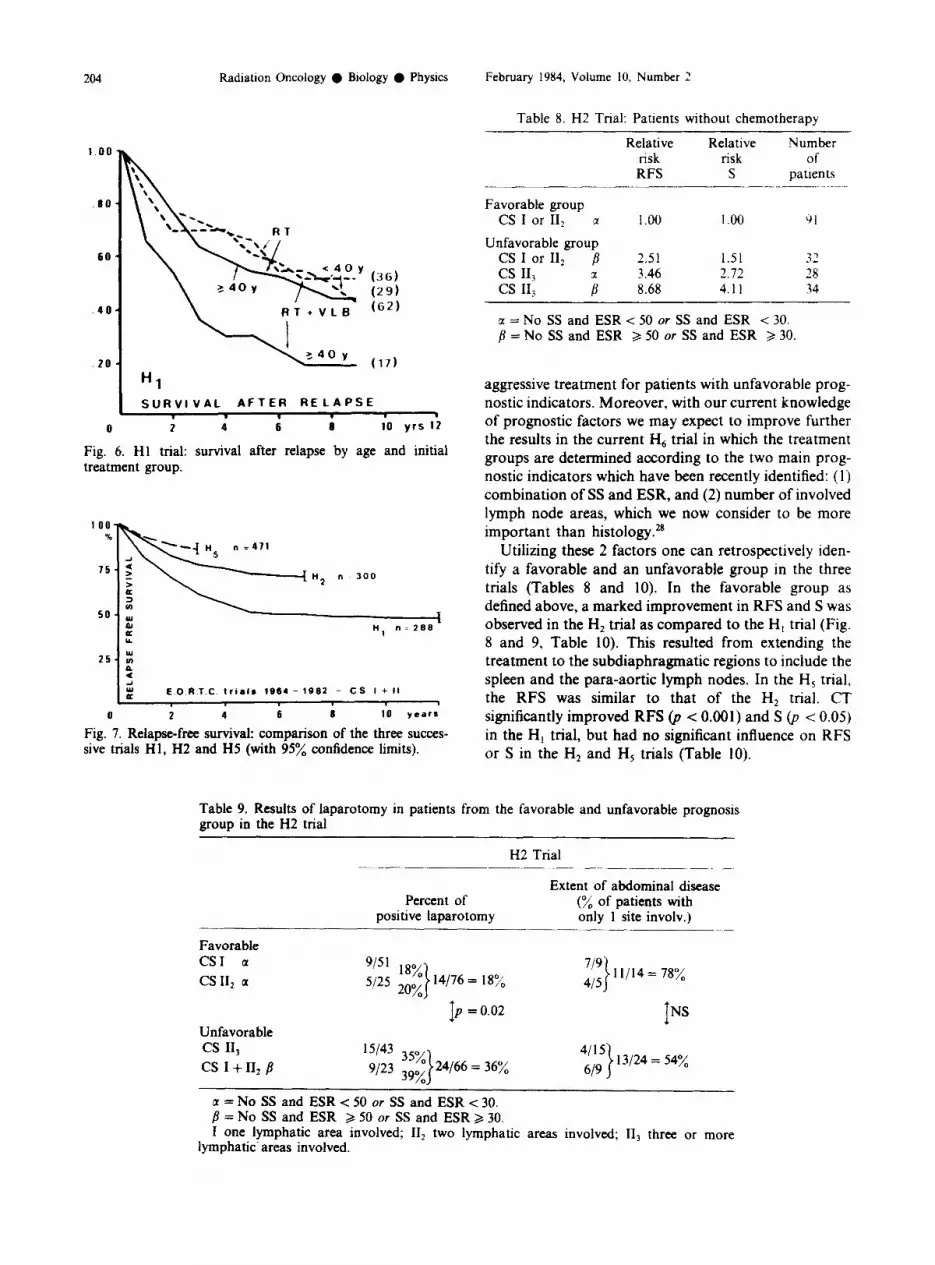
Fig. 6. Hl trial: survival after relapse by age and initial treatment group.
n 300
I E “1 ” 1299
25- ii P : w E O.RT C trials 1964 - 1992 - CS I + II
0 2 4 6 8 10 year*
Fig. 7. Relapse-free survival: comparison of the three succes- sive trials HI, H2 and H5 (with 95% confidence limits).
Table 8. H2 Trial: Patients without chemotherapy
Relative Relative Number risk risk Of RFS S patients
Favorable group CS I or II, a 1.00 1.00 9)l
Unfavorable group CS I or II, /I 2.51 1.51 3’ _i cs II, 3.46 2.72 28 cs II, ; 8.68 4.11 34
I = No SS and ESR < 50 or SS and ESR < 30. /I = No SS and ESR 2 50 or SS and ESR > 30.
aggressive treatment for patients with unfavorable prog- nostic indicators. Moreover, with our current knowledge of prognostic factors we may expect to improve further the results in the current H6 trial in which the treatment groups are determined according to the two main prog- nostic indicators which have been recently identified: (1) combination of SS and ESR, and (2) number of involved lymph node areas, which we now consider to be more important than histology.*’
Utilizing these 2 factors one can retrospectively iden- tify a favorable and an unfavorable group in the three trials (Tables 8 and 10). In the favorable group as defined above, a marked improvement in RFS and S was observed in the H, trial as compared to the H, trial (Fig. 8 and 9, Table 10). This resulted from extending the treatment to the subdiaphragmatic regions to include the spleen and the para-aortic lymph nodes. In the H, trial. the RFS was similar to that of the H, trial. CT significantly improved RFS @ < 0.001) and S 0, < 0.05) in the H, trial, but had no significant influence on RFS or S in the H, and HS trials (Table 10).
Table 9. Results of laparotomy in patients from the favorable and unfavorable prognosis group in the H2 trial
H2 Trial
Favorable
Percent of positive laparotomy
Extent of abdominal disease (% of patients with only 1 site involv.)
CSI a CS II, a
“‘I 18% 5!25 2oX 14/76 = 18% 7’9
415 > 11/14= 78%
Unfavorable cs II, cs I + II* fi
I p = 0.02 I NS
15143 35% 4115
9/23 39% 24166 = 36% 619
13124 = 54%
a = No SS and ESR < 50 or SS and ESR < 30. B = No SS and ESR > 50 or SS and ESR 3 30. I one lymphatic area involved; II, two lymphatic areas involved; II, three or more
lymphatic- areas involved.

Tabl
e 10
.
Perc
ent
of p
atie
nts
with
ini
tial
CT
or C
T du
ring
the
cour
se
of t
he
dise
ase
Perc
ent
of l
ong
term
su
rviv
ors
rece
ived
C
T N
umbe
r of
R
FS f
s.
d. (
“A)
S +
s.d
. (%
) Pe
rcen
t of
pat
ient
s pa
tient
s 3.
5y
7y
;2y
3.5y
7y
12
Y
with
ini
tial
CT
Favo
rabl
e pa
tient
s II
1 tri
al:
all
patie
nts
with
out
initi
al
CT
with
ini
tial
CT
H2
trial
: al
l pa
tient
s w
ithou
t in
itial
C
T w
ith
initi
al
CT
HS
trial
: al
l pa
tient
s w
ithou
t in
itial
C
T:
Mor
M
+PA
R
T Tr
ue
TN1
TN1
with
outp
elvi
c R
w
ith i
nitia
l C
T (M
OPP
)
Unf
avor
able
pa
tient
s H
I fr
ial:
all
patie
nts
with
out
initi
al
CT
with
ini
tial
CT
H2
trial
: al
l pa
tient
s w
ithou
t in
itial
C
T w
ith i
nitia
l C
T H
5 tri
al:
all
patie
nts
with
out
initi
al
CT:
M
orM
+PA
RT
True
TN
1 TN
1 w
ithou
t pe
lvic
RT
with
initi
al C
T (M
OPP
)
170 88
82
152 97
55
279
62k4
55
_+4
53_+
4 53
+ 5
42
+ 5
37 +
5
72 +
5 6
9 +
5 69
f
5 89
+3
87+3
-
85+4
83
k4
- 94
+3
92+4
-
86+3
-
-
85 _
+3 7
5 _+
3 62
_+4
48
72
70
83
f4
68+5
54
k6
- 46
39
88
+4
83+4
71
+5
100
100
100
95+2
88
*3
- 36
47
44
96
f2
90f3
-
- 16
14
93
+4
85+5
-
100
100
100
96+2
-
- 30
38
-
10
14
10
100
121
87+4
-
- 99
*1
- -
52
803-
7 -
- 92
k5
- -
20
86kl
O
- -
100
- -
85
90*5
-
- 93
*3
- -
- -
- -
- loo
83
49 f
6
45 f
6
45 _
+ 6
81 k
4 77
_+5
68f6
47
74
44
43
+8
39 +
7 39
+ 7
75
+ 7
73
f 7
66 *
7
- 50
39
55
48
52 +
8 52
f
8 87
+6
81 f
7 67
+9
100
100
143
6Q*4
55*4
-
85*3
78
+4
- 29
66
10
1 52
+_5
48+_
5 -
85f4
79
f4
- -
52
42
8126
74
+8
- 85
_+6
76_+
7 -
100
100
192
80f3
-
- 89
+3
- -
29
44
65
80&
-5
- -
91*5
-
- -
21
46
78&
8 -
- 86
&7
- -
- 15
20
58
+13
- -
89f7
-
- -
38
55
89_+
5 -
- 92
_+5
- -
100
100
71
42
100 60
45
100
- - - - -
M =
man
tle
field
RT,
PA
= p
ara-
aorti
c R
T; T
N1
= to
tal
noda
l R
T, F
avor
able
=
CS
I or
II2
and
eith
er
no S
S, E
SR c
50
or S
S, E
SR <
30;
Unf
avor
able
=
othe
r pa
tient
s.

206 Radiation Oncology ??Biology ??Physics February 1984, Volume 10, Number 2
.H, (110)
FAVORABLE GROUP
I I I
0 2 4 6 I) 10 VRS 12
Fig. 8. Relapse-free survival: comparison of the three succes- sive trials H 1, H2 and H5, for patients with favorable prognos- tic factors at onset (CS I and II2 and either no SS, ESR < 50 or SS, ESR < 30.
FAVOAIBLE GROUP
0 2 4 6 I 10 VRS 12
Fig. 9. Overall survival: comparison of the three successive trials Hl, H2 and H5 for patients with favorable prognostic factors at onset (CS I and II, and either no SS, ESR < 50 or SS, ESR < 30).
UNFAVORABLE GROUP
0 i 4 6 I ;o YRS Ii
Fig. 10. Relapse-free survival: comparison of the three succes- sive trials Hl, H2 and H5 for patients with unfavorable prognostic factors at onset (CS II3 or no SS, ESR 2 50 or SS, ESR > 30).
For the unfavorable group there was only a modest gain in RFS for the H2 patients as compared to H! patients, but the improvement in RFS was most evident from H, to H, (Figs. 10 and 11). In the H, study patients either received more extensive RT, i.e. TNI, as compared to mantle + para-aortic and splenic treatment as given in the Hz trial, or the patients received more effective chemotherapy, MOPP instead of VLB alone or VLB + PCZ. However the survival advantage was very small, if any (Fig. ll), and there remains room for improvement. In this subset of patients CT did not improve RFS or S in the H, trial; in the H, and H, trials (Table 10) it had a significant effect on RFS @ < 0.01 and p < 0.05, respectively) but not on S. The data of Table 10 show that when RFS is very high the efficacy of salvage treatment becomes low, especially for patients initially treated with CT,
DISCUSSION Multiple agent CT in combination with RT is a very
effective weapon. However, its side effects are significant. A notable incidence of secondary malignancies has been observed by several groups;4s6,16*20 ovarian and testicular reproductive functions are adversely affected by MOPP. Therefore, it appears desirable to avoid MOPP or other combination CT when possible. Vinblastine alone does not have this drawback according to our data in so far as it does not increase the incidence of second cancers.14 It is less effective, however, than combination CT, and moreover it may lower both the patient tolerance and tumor susceptibility when CT is administered for re- lapse. This is particularly important for patients over 40 because salvage treatment following relapse has been very ineffective for those more elderly patients who received CT (VLB or VLB + PCZ) as a part of their initial treatment program as compared to the same age group who was initially treated by RT alone @ = 0.02).
Since 1963, when these trials began, we sought to identify a subset of patients for whom RT alone was a
25 1 i,,,,,,,, 1,,,
UNFAVORABLE ORO"p
0 I 4 6 I to VRS 12
Fig. 11. Overall survival: comparison of the three successive trials H 1, H2 and H5 for patients with unfavorable prognostic factors at onset (CS II, or no SS, ESR 2 50 or SS, ESR 2 30).

Role of radiotherapy in Hodgkin’s disease ??M. TUBIANA et al. 207
satisfactory treatment. For this reason we undertook the study of prognostic factors. The results of the multi- variate analyses revealed that in all therapeutic groups, ESR and SS are of high prognostic significance.26 The impact of the other prognostic factors is greatly influenced by the type of treatment. This is particularly true for patients treated by RT alone, where the extent of RT (regional, extended field or TNI) greatly influences the significance of various prognostic factors. This suggests that occult dissemination is strongly cor- related with these prognostic factors, the most important being the number of involved lymphatic areas.28 These data show that in several subgroups of patients, RT alone can obtain results equal to those of RT + multi-agent CT as long as the size of the irradiated field is properly adjusted with respect to the prognostic indicators.
In most patients, RT limited to one side of the diaphragm, as performed in the H, trial, is insufficient since the RFS is low even in the favorable prognostic group. Additionally the proportion of patients requiring salvage CT is considerable and, most importantly, the overall survival rate is lower than can be achieved with more aggressive primary treatment. Extended field RT such as mantle field + spleen + para-aortic RT as in the H2 trial,is more satisfactory because it” obtains better RFS and avoids irradiation of the pelvis and the sub- sequent gonadal damage that can result from scatter irradiation. Thus the identification of prognostic factors that can allow us to treat favorable subsets of patients with extended field irradiation alone is of great im- portance. Indeed multivariate analyses showed that in addition to the combination of ESR and SS, the two main prognostic factors are (1) the number of involved lymph node sites, and (2) the laparotomy findings. The prognostic information gained from these studies pro- vides all of the information necessary to delineate a treatment program since all of the other prognostic factors such as sex, age, etc. are strongly correlated with those above and do not carry any further independent prognostic information. On the basis of these prognostic factors it is thus possible to identify 2 groups of patients, favorable and unfavorable. In the favorable group, mantle, para-aortic and spleen treatment give excellent results, whereas in the unfavorable group the results of this treatment are less satisfactory, suggesting that the disease has spread outside of this irradiated volume. The number of involved sites was not considered in the H, trial, which was started before this information was available. However, at the initiation of this trial the preliminary results of the H, trial were known, which helped to define a policy based on the results of the staging laparotomy to delineate the good prognostic group.25
In the HS trial, all CS I + II patients with supra- diaphragmatic disease who had what was considered at this time low risk prognostic factors, were submitted to
staging laparotomy. They were treated by RT alone only if they were laparotomy negative, PS I + II. Conversely, for patients with poor prognostic factors, staging lap- arotomy was considered unnecessary because the pre- liminary H, trial data had already indicated that even when the spleen or para-aortic lymph nodes were not involved the long term RFS was lower than 70% follow- ing treatment by RT alone (Table 5).
The preliminary results of the H, trial showed that basically the general principles of this staging policy were adequate. Indeed other institutions such as Stan- ford have recently adopted a similar approach: staging laparotomy for patients with good prognostic factors, but no laparotomy for patients with poor prognostic indicators who require combination CT in any event.22
As stated above, the H, trial was initiated prior to the analysis of the long term results of the H2 trial. There- fore, the indicators which were used to delineate the two therapeutic groups were largely those identified in the H, trial and thus were not optimal for selecting those patients to be treated by mantle and para-aortic RT following laparotomy. Nevertheless, the analysis of the H, data confirms the validity of the main prognostic factors which emerged from the H, trial. One can identify those patients of the H, trial who would be considered favorable for unfavorable on the basis of the number of involved lymph node areas and ESR (Table 10). For favorable patients, excellent results were ob- tained in the treatment arm which included mantle field or mantle field + para-aortic lymph node irradiation. Excellent results were, of course, also obtained for those included in the TN1 arm. What is more interesting is that for these favorable patients, equal results were obtained with incomplete TN1 (no pelvic RT) or complete TNI, whereas for patients classified as unfavorable by the new criteria, RFS was significantly lower for those treated by incomplete TNI. Hence the H, data indirectly confirm the validity of a distinction between a favorable group and an unfavorable one based on the factors described above. The favorable group comprised patients 1) with- out SS and with an ESR < 50 or with SS and an ESR < 30, and 2) with one or two involved, lymphatic areas. The delineation of this favorable group can be further improved by taking into account the results of staging laparotomy. Patients with 3 or more involved lymphatic areas and/or SS and an elevated ESR consti- tute the unfavorable prognostic group.
This delineation of two prognostic groups is currently being used in the H, trial and is similar to that proposed by St. Louis Hospital group in Paris,‘,2 although our therapeutic protocols differ considerably. Recent data suggest that one might also take into account the size of the mediastinal mass,‘8~‘9 the extent of hilar adenopathy and the bulk of splenic in- volvement.‘5 However the value of this further refinement of the prognostic indicators remains to be prospectively tested.

208 Radiation Oncology 0 Biology ??Physics February 1984, Volume 10. Number 2
Nonetheless at least two questions remain un- answered. The first is the usefulness of para-aortic RT in spleen negative patients of the favorable group. The preliminary data from the H, trial suggest that for laparotomy negative patients in the favorable prognostic group with NS + LP histology, mantle field RT is proba- bly adequate and thus para-aortic RT can be omitted. This is in accordance with other data such as those of the H, trial (Table 3). On the other hand, for patients of MC histologic type, the data of the H, and H, trials cannot be used to assess optimal RT since most of them received adjuvant CT. In the H, trial,25 the incidence of para-aortic lymph node relapses is unacceptably high in patients with MC subtype (Table 3). The H, trial shows that the incidence of splenic involvement in this sub- group of patients is not sufficient to explain the difference observed. This suggests that this difference is in part attributable to para-aortic involvement un- detected by lymphangiogram and lymph node biopsy. This is why in the on-going EORTC (H,) trial, spleen negative patients in the good prognosis group with MC histologic subtype receive para-aortic lymph node irra- diation.
The second question is related to the usefulness of staging laparotomy.” Some centers, instead of staging laparotomy, prefer to combine RT with CT at reduced doses (for example 3 cycles of MOPP instead of 6) for patients with good prognostic indicators.‘.2 The validity of this policy has yet to be assessed. The carcinogenic effect of reduced doses of combination CT is difficult to predict and a follow-up of at least 10 years is required for its assessment. Similarly, the effects of these reduced doses on gonadal function remain to be evaluated. There is also the possibility that other drug combinations such as ABVD are less carcinogenic, and thus these drugs deserve further study. It will be necessary to follow a sufficient number of patients for one decade before these questions are answered.
Another aspect of this same question is whether staging laparotomy is necessary to further delineate the favorable prognostic group. Laparotomy is useful to detect occult infradiaphragmatic involvement; on the other hand it has 3 drawbacks: treatment delay, surgical complications, and possibly late sequellae. These con- siderations lead to the following question: does the identification of a small group of patients with infradiaphragmatic involvement outweigh the dis- advantages of the staging procedure? We can expect on the basis of H, trial data that in the favorable group, laparotomy will discover infradiaphragmatic disease in approximately 20% of the patients. Of these, approximately 40% will relapse, which is about 10% of the whole favorable group. These patients would have benefitted from initial polychemotherapy or TNI. However, the data show that more than half of these will be rescued by CT administered at first relapse.
Therefore, the new EORTC trial (HJ is a pragmatic trial whose end-point is not RFS but overall survival and whose purpose is to evaluate the usefulness of staging laparotomy by comparing, within the favorable prog- nostic group, patients staged with laparotomy as in the H, trial, and patients staged without laparotomy and treated by RT alone: mantle field + splenic and para- aortic RT. One can expect a higher incidence of relapse in the latter arm; however, because of salvage CT. the long term survival rates might not be different, and the aim of the current study is to compare the overall survival in the two therapeutic arms.
Let us consider now the unfavorable patients. It has been claimed that RT alone cannot be used for their treatment because the incidence of relapse would be too high and despite rescue therapy with aggressive combi- nation CT, approximately 40 to 50% of the relapsing patients will ultimately die.3s2’ Therefore it has been argued that patients can be treated by RT alone only if the expectancy of long term RFS is of the order of SOY,,, which corresponds to a long-term survival rate of higher than 90%. However, this reasoning is valid only if the salvage rate is the same regardless of the relapse rate. The data of Table 10 suggest that this might not be true. In fact the proportion of salvaged patients following relapse is smaller when patients have received CT ini- tially (Fig. 6, Table 10). The data of the H, trial suggest that rescue is more effective following TN1 than follow- ing the combination of MOPP and RT, however the follow-up following relapse is too short to make this conclusion with certainty.
Moreover, Fig. 11 shows that little progress has been accomplished in overall survival of the unfavorable group, despite the marked improvement in RFS (Table 10). There is a striking lack of difference in survival between patients initially treated with or without CT. This may be the result of a subgroup of patients yet to be identified for whom our current therapeutic modali- ties are insufficient, both initially or following relapse. Of course this conclusion is tentative, since in the first two trials CT was clearly inadequate by our present stan- dards. Moreover, the follow-up is not long enough for’ a valid comparison between MOPP + RT and TNl; nevertheless the survival appears to be similar with both treatment modalities. Hence it appears acceptable to offer TN1 to young patients who wish to retain re- productive potential. It is clear, however, that for un- favorable patients, as presently defined, mantle field + splenic + para-aortic RT is insufficient; this was demonstrated by both the H2 data and the comparison between TN1 and so-called incomplete TN1 (no pelvic and inguinal RT) in the H5 trial.
In conclusion, the data of the three EORTC trials emphasize the importance of prognostic factors in the choice of optimal treatment. Moreover, they underline that prognostic factors cannot be discussed withour reference to treatment. For patients treated by RT alone

Role of radiotherapy in Hodgkin’s d&a&e ??‘M. TWBIANA et al. 209
the selection of the extent of RT should take into able prognostic group, while we felt that it was not account several prognostic factors, most importantly the warranted for other patients.25 This conclusion remains ESR, SS, the number of involved sites and possibly the valid in light of our present data. Thus the Ann-Arbor histologic type. More limited RT gives satisfactory re- clinical and pathological staging system,5 while useful, is sults in some subsets of patients whereas for patients by itself insufTicient and the clinician must go further in with more than two involved sites, and/or splenic in- tailoring the treatment of individual patients based on volvement, TN1 or combined modality treatment be- individual characteristics. With proper adjustment of the comes mandatory. We advocated, in 1975, the use of treatment volume, a very large proportion of CS I + II staging laparotomy to help further delineate the favor- patients can be best treated by RT alone.
REFERENCES 1.
2.
3.
4.
5.
6.
I.
8.
9.
10.
11.
12.
13.
14.
Andrieu, J.A., Montagnon, B., Asselain, B., Bayle- Weisgerber, C., Chastang, C., Teillet, F., Bernard, J.: Chemotherapy-radiotherapy in Hodgkin’s disease clinical Stages IA, II* A. Cancer 46: 2126-2130, 1980. Andrieu, J.M., Asselain, B., Bayle, C., Teillet, F., Clot, P., Dana, M., Katz, M., Briere, J., Jacquillot, C., Bernard, J.: La sequence polychimio-therapie MOPP-irradiation gan- glionnaire selective dans le traitement de la maladie de Hodgkin, stades cliniques IA-IIIB. Bull. Cancer 68: 190-199, 1981. Bergsagel, D.E., Alison, R.E., Beau, H.A., Brown, T.C., Bush, R.S., Clark, R.M., Chua, T., Dalley, D., De Boer, G., Gospodarowicz, M., Hasselback, R., Perrault, D., Rideout, D.F.: Results of treating Hodgkin’s disease with- out a policy of laparotomy staging. Cancer Treat Rep. 66: 717-731, 1982. Boivin, J.F., Hutchison, G.B.: Leukemia and other cancers after radiotherapy and chemotherapy for Hodgkin’s dis- ease. J. Natl. Cancer Inst. 67: 751-760, 1981. Carbone, P.P., Kaplan, H.S., Musshoff, K., Smithers, D.W., Tubiana, M.: Report of the committee on Hodg- kin’s disease staging classification. Cancer Res. 31: 1860-1861, 1971. Coleman, C.N.: Adverse effects of cancer therapy: the risk of secondary neoplasms. Am. J. Pediatr. Hematol. Oncol. 4: 103-111, 1982. Cox, D.R.: Regression model and life tables. J. Royal Stat. Sot. 34: 187-220, 1972. Fuller, L.M., Hutchinson, G.B.: The collaborative clinical trial for Stage I and II Hodgkin’s disease. Cancer Treat. Rep. 66: 775-787, 1982. Fuller, L. M., Madoc Jones, H., Hagemeister, F.B., Rod- gers, R.W., North, L.B., Butler, J.J., Martin, R.G., Gam- ble, J.E., Shullenberger, C.C.: Further follow-up or results of treatment in 90 laparotomy negative Stage I And II Hodgkin’s disease patients. Significance of mediastinal and non mediastinal presentation. Int. J. Radiat. Oncol. Biol. Phys. 6: 799-808; 1980. Glatstein, E., Guernsey, J.M., Rosenberg, S.A., Kaplan, H.S.: The value of laparotomy and splenectomy in the staging of Hodgkin’s disease. Cancer 24: 709-718, 1969. Hagemeister, F.B., Fuller, L.M., Sullivan, J.A., North, L., Velasquez, W., Conrad, F.G., MacLaughlin, P., Butler, J.J., Shullenberger, C.C.: Treatment of Stages I and II mediastinal Hodgkin disease. Radiology 141: 783-789, 1981. Hayat, M.: E.O.R.T.C. Radiotherapy-Chemotherapy Group. A randomized study of irradiation and vinblastine in Stages I and II of Hodgkin’s disease. Preliminary results. Europ. J. Cancer 8: 353-362, 1972. Hellman, S., Mauch, P.: Role of radiation therapy in the treatment of Hodgkin’s disease. Cancer Treat. Rep. 66: 915-923, 1982. Henry-Amar, M., (for the E.O.R.T.C. Radiotherapy- Chemotherapy Group): Second cancers after radiotherapy
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
and chemotherapy for early stages of Hodgkins disease. J. Natl. Cancer Inst. 71: 911-916, 1983. Hoppe, R.T., Rosenberg, S.A., Kaplan, H.S., Cox, R.S.: Prognostic factors in pathological Stage IIIA Hodgkin’s disease. Cancer 46: 1261246, 1980. Kaplan, H.S.: Hodgkin’s Disease 2nd edition. Cambridge, MA, Harvard University Press 1980. Le Bourgeois, J.P., Meignan, M., Parmentier, C., Tubiana, M.: Renal consequences of irradiation of the spleen in lymphoma patients. Brit. J. Radiol. 52: 56-60, 1979. Lee, C.K.K., Bloomfield, C.D., Goldman, A.I., Levitt, S.H.: Prognostic significance of mediastinal involvement in Hodgkin’s disease treated with curative radiotherapy. Cancer 46: 2403-2409, 1980. Mauch, P., Hellman, S.: Supradiaphragmatic Hodgkin’s disease: Is there a role for MOPP Chemotherapy in patients with bulky mediastinal disease. Int. J. Radiat. Oncol. Biol. Phys. 6: 947-949, 1980. Nelson, D-F., Cooper, S., Weston, M.G., Rubin, P.: Second malignant neoplasms in patients treated for Hodg- kin’s disease with radiotherapy or radiotherapy and chemotherapy. Cancer 48: 2386-2393, 1981. Pene, F., Henry-Amar, M., Le Bourgeois, J.P., Hayat, M., Gerard-Marchant, R., Laugier, A., Mathi, G., Tubiana, M.: A study of relapse and course of 153 cases of Hodgkin’s disease (clinical Stages I and II) treated at the Institute Gustave-Roussy from 1963 to 1970 with radio- therapy alone or with adjuvant monochemotherapy. Can- cer 46: 2131-2141, 1980. Rosenberg, S.A., Kaplan, H.S., Hoppe, R.T., Kushlan, P., Horning, S.: An overview of the rationale and results of Stanford randomized trials of the treatment of Hodgkin’s disease, In Adjuvant Therapy of Cancer III, Jones, S.E., Salmon, S.E. (Eds). New York, Grune & Stratton. 1981, pp. 65-76. Thar, T.L., Million, R.R., Hausner, R.J., McKetty, M.H.B.: Hodgkin’s disease Stages I and II: relationship of recurrence to size of disease, radiation dose and number of sites involved. Cancer 43: 1101-1105, 1979. Tubiana, M., Attie, E., Flamant, R., Gerard-Marchant, R., Hayat, M.: Prognostic factors in 454 cases of Hodg- kin’s disease. Cancer Res. 31: 1801-1810, 1971. Tubiana, M., Hayat, M., Henry-Amar, M., Breur, K., Van Der Werf Messing, B., Burgers, M.: Five-year results of the E.O.R.T.C. randomized study of splenectomy and spleen irradiation in clinical stages I and II of Hodgkin’s disease. Europ. J. Cancer 17: 355-363, 1981. Tubiana, M., Henry-Amar, M., Burgers, M.V., Van Der Werf Messing, B., Hayat, M.: Prognostic significance of ESR in clinical Stages I and II Hodgkin’s disease. J. C/in. Oncof. (In press). Tubiana, M., Henry-Amar, M., Hayat, M., Breur, K., Van Der Werf Messing, B., Burgers, M.: Long-Term results of the E.O.R.T.C. randomized study of irradiation and Vin- blastine in clinical Stages I and II of Hodgkin’s disease.

210 Radiation Oncology ??Biology 0 Physics February 1984. Volume 10. Number 2
Europ. J. Cancer 15: 646656, 1979. 28. Tubiana, M., Henry-Amar, M., Hayat, M., Burgers, M.,
Qasim, M., Somers, R., Sizoo, W., Van Der Schueren, E.: Prognostic significance of the number of involved areas in the early stages of Hodgkin’s disease. Cancer (In press).
29. Tubiana, M., Van Der Werf Messing, B., Laugier, A., Hayat, M., Henry-Amar, M., Attit, E., Leroy, T.: Survival
after recurrence: prognostic factors and spread patterns in clinical Stages I and II of Hodgkin’s disease. Narl. Cancer Inst. Monog. 36: 613-530, 1973.
30. Van Der Werf Messing, B.: Morbus Hodgkin’s disease, Stages I and II. Trial of the E.O.R.T.C. Hodgkin’s disease Symposium, Stanford University, 1972, Natl. Cancer Ins. Monog. 36: 381-386, 1973.
APPENDIX The chairmen of this cooperative group were M. Tubiana In Belgium: Institut Jules Bordet, Bruxelles (J. Henry. J
(1964-67), K. Breur (1967-69) B. van der Werf-Messing Lustmann Marechal), Centre Rent? Goffin. La Louviere (J. C. (1969-72), J. Henry (1973-75) J. Abbatucci (1975-77) M. Goffin), Hopital de Baviere, Liege (R. Lemaire). Acad. Zi- Burgers (1977-80), M. Hayat (198&82). Statistician M. ekenhuis St. Rafael, Leuven (E. van der Schueren, J. Thomas): Henry-Amar, scientific secretaries A. Laugier (1964-70) and P. In Italy: Istituto di Radiologia, Universita di Firenze (G. De Carde, sponsor M. Tubiana. Giuli, L. Cionini);
In France: Fondation Bergonit, Bordeaux (C. Lagarde). Cooperating centers were, Centre Franqois-Baclesse, Caen (J. S. Abbatucci). Centre Leon In The Netherlands: Antoni van Leeuwenhoek Ziekenhuis, Berard, Lyon (J. Papillon, L. Revol), Centre Antoine Amsterdam (M. Burgers, R. Somers), University Hospital, Lacassagne, Nice (C. Lalanne, M. Schneider). Hotel- Leiden (P. Thomas), St. Radboud Academic Hospital, Ni- Dieu, Paris (R. Zittoun). Institut Jean-Godinot. Reims jmegen (Wagener), Rotterdamsch-Radiotherapeutisch Insti- (A. Cattan), Centre Henri-Becquerel, Rouen (H. Piguet). tuut, Rotterdam (M. Qasim, W. Sizoo), Ziekenhuis Leyenburg, Institut Gustave Roussy, Villejuif (M. Tubiana, J. L. The Hague (H. Kerkhofs), University Hospital, Utrecht (H. Amiel, M. Hayat), I.C.I.G. Paul-Brousse, Villejuif Van Peperzeel); (G. Mathe).
Copyright © 2022 FDOKUMEN




















