
Conservative surgery and radiotherapy for early breast cancer
12
Conservative Surgery and Radiotherapy for Early Breast Cancer Jay R. Harris, MD,” Abram Recht, MD,* James Connolly, MD,t Blake Cady, MD,$ Steven Come, MD,§ I. Craig Henderson, MD, (1 Clinton Koufman, MD,§ Susan Love, MD,I Stuart Schnitt, MD,t and Robert Osteen, MD# In 1984, as part of a prior American Cancer Society National Conference on Breast Cancer, the authors reported on the status of conservative surgery (CS) and radiotherapy (RT) as primary local treatment for women with early stage breast cancer.’ Since that time, additional data have become available regarding the use of this approach and its comparability to mastectomy. In general, these data support the use of CS and RT and, as a result, this approach is now more widely employed in the United States and abroad than it was in 1984. The current focus of inquiry has shifted from whether or not CS and RT is an acceptable option for patients with early stage breast cancer to the following questions. For which patients are CS and RT suitable? What are the best techniques of surgery and RT? Are there any patients who can be treated safely with CS without RT? How should RT and systemic therapy be integrated when both are to be used? In this report, recent results on the use of CS and RT from both retrospective and prospective trials are summarized, and these current areas of inquiry are addressed. Cancer 661427-1438,1990. HE CRITICAL ISSUE regarding CS and RT is whether T or not it yields survival rates equivalent to those of mastectomy. There are four published trials comparing CS and RT with mastectomy in which modern techniques were used. One such trial was performed at the National Cancer Institute of Italy in Milan. From 1973 to 1980, 701 evaluable patients with primary tumors less than or equal to 2 cm in size and with clinically uninvolved ax- illary nodes (T 1 NO) were randomized to receive either radical mastectomy or CS and RT. Conservative surgery consisted of a resection of the entire involved quadrant of the breast (“quadrantectomy”) and a full axillary dis- Presented at the Amencan Cancer Society National Conference on Breast Cancer, Chicago Westin Hotel, Chicago, Illinois, July 19-2 1, 1989. From the *Joint Center for Radiation Therapy, and Department of Radiation Therapy, the tDepartment of Pathology, Beth Israel Hospital, the $Department of Surgery, New England Deaconess Hospital, the §Department of Medicine, Beth Israel Hospital, the 11 Breast Evaluation Center, Dana-Farber Cancer Institute, the #Department of Surgery, Brigham and Women’s Hospital, Harvard Medical School, and the BDe- partment of Surgery, Faulkner Hospital, Boston, Massachusetts. Address for reprints: Jay R. Harris, MD, Joint Center for Radiation Therapy, 50 Binney Street, Boston, MA 02 1 15. Accepted for publication December 1 1, 1989. section. Radiotherapy was then administered to the breast alone through two opposing tangential fields on a linear accelerator, with a dose of 5000 cGy given in 5 weeks. An additional 1000 cGy was then given to the tumor site using orthovoltage radiation. From 1973 to 1975, patients with pathologically in- volved axillary lymph nodes were further randomized to receive radiotherapy either to the breast alone or to the breast and the draining lymph node areas. After 1975, all patients with involved lymph nodes were treated with 12 cycles of cyclophosphamide, methotrexate, and 5-fluo- rouracil (CMF). The two arms were well balanced with regard to age, tumor size, and axillary nodal status. Mi- croscopically involved axillary nodes were found in 25% of the radical mastectomy group and 27% of the conser- vatively treated group. The latest report of the Milan trial was published in 1986.2 At that time, seven patients from the mastectomy group had developed a chest wall recurrence, and seven in the quadrantectomy group had developed a local re- currence at or near the site of the primary tumor. Seven other patients in the CS and RT group developed a second primary cancer located well away from the site of the 1427
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Conservative surgery and radiotherapy for early breast cancer

Conservative Surgery and Radiotherapy for Early Breast Cancer Jay R. Harris, MD,” Abram Recht, MD,* James Connolly, MD,t Blake Cady, MD,$ Steven Come, MD,§ I. Craig Henderson, MD, ( 1 Clinton Koufman, MD,§ Susan Love, MD,I Stuart Schnitt, MD,t and Robert Osteen, MD#
In 1984, as part of a prior American Cancer Society National Conference on Breast Cancer, the authors reported on the status of conservative surgery (CS) and radiotherapy (RT) as primary local treatment for women with early stage breast cancer.’ Since that time, additional data have become available regarding the use of this approach and its comparability to mastectomy. In general, these data support the use of CS and RT and, as a result, this approach is now more widely employed in the United States and abroad than it was in 1984. The current focus of inquiry has shifted from whether or not CS and RT is an acceptable option for patients with early stage breast cancer to the following questions. For which patients are CS and RT suitable? What are the best techniques of surgery and RT? Are there any patients who can be treated safely with CS without RT? How should RT and systemic therapy be integrated when both are to be used? In this report, recent results on the use of CS and RT from both retrospective and prospective trials are summarized, and these current areas of inquiry are addressed. Cancer 661427-1438,1990.
HE CRITICAL ISSUE regarding CS and RT is whether T or not it yields survival rates equivalent to those of mastectomy. There are four published trials comparing CS and RT with mastectomy in which modern techniques were used. One such trial was performed at the National Cancer Institute of Italy in Milan. From 1973 to 1980, 701 evaluable patients with primary tumors less than or equal to 2 cm in size and with clinically uninvolved ax- illary nodes (T 1 NO) were randomized to receive either radical mastectomy or CS and RT. Conservative surgery consisted of a resection of the entire involved quadrant of the breast (“quadrantectomy”) and a full axillary dis-
Presented at the Amencan Cancer Society National Conference on Breast Cancer, Chicago Westin Hotel, Chicago, Illinois, July 19-2 1, 1989.
From the *Joint Center for Radiation Therapy, and Department of Radiation Therapy, the tDepartment of Pathology, Beth Israel Hospital, the $Department of Surgery, New England Deaconess Hospital, the §Department of Medicine, Beth Israel Hospital, the 11 Breast Evaluation Center, Dana-Farber Cancer Institute, the #Department of Surgery, Brigham and Women’s Hospital, Harvard Medical School, and the BDe- partment of Surgery, Faulkner Hospital, Boston, Massachusetts.
Address for reprints: Jay R. Harris, MD, Joint Center for Radiation Therapy, 50 Binney Street, Boston, MA 02 1 15.
Accepted for publication December 1 1, 1989.
section. Radiotherapy was then administered to the breast alone through two opposing tangential fields on a linear accelerator, with a dose of 5000 cGy given in 5 weeks. An additional 1000 cGy was then given to the tumor site using orthovoltage radiation.
From 1973 to 1975, patients with pathologically in- volved axillary lymph nodes were further randomized to receive radiotherapy either to the breast alone or to the breast and the draining lymph node areas. After 1975, all patients with involved lymph nodes were treated with 12 cycles of cyclophosphamide, methotrexate, and 5-fluo- rouracil (CMF). The two arms were well balanced with regard to age, tumor size, and axillary nodal status. Mi- croscopically involved axillary nodes were found in 25% of the radical mastectomy group and 27% of the conser- vatively treated group.
The latest report of the Milan trial was published in 1986.2 At that time, seven patients from the mastectomy group had developed a chest wall recurrence, and seven in the quadrantectomy group had developed a local re- currence at or near the site of the primary tumor. Seven other patients in the CS and RT group developed a second primary cancer located well away from the site of the
1427
1428 CANCER Septrmher 15 Supplmennt 1990 Vol. 66
- HALSTED *___. QUART
ADJUSTED LOG RANK TEST
I 1 I , I I I ! 1 I 0 , - ~ 1 2 3 4 5 I 7 8 ~ 1 0 1 1 1 2
V E A R S
1.00 OVER ALL SURVIVAL
h- I 1b
ADJUSTED LOG RANK TEST N. 0BS.D. EXP.D. WE
0 352 66 84.3 017 0.50 n 340 07 50.7 1.14 P=0.13
' 1 2 3 4 5 I 7 I # I 0 1 1 1I Y E A R S
o,'o/ , , , , , , , , , , I .
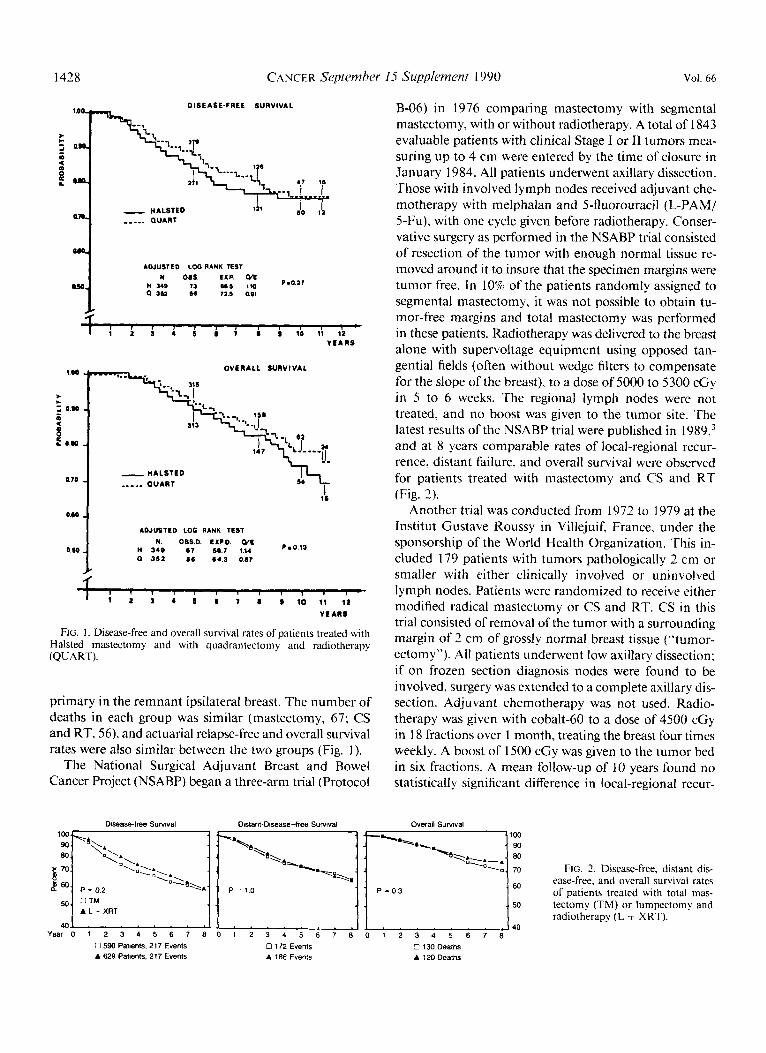
FIG. 1 . Disease-free and overall survival rates of patients treated with Halsted mastectomy and with quadrantectomy and radiotherapy (QUART).
primary in the remnant ipsilateral breast. The number of deaths in each group was similar (mastectomy, 67; CS and RT, 56), and actuarial relapse-free and overall survival rates were also similar between the two groups (Fig. I).
The National Surgical Adjuvant Breast and Bowel Cancer Project (NSABP) began a three-arm trial (Protocol
Disease-free Survival Distant-Disease-free Survival
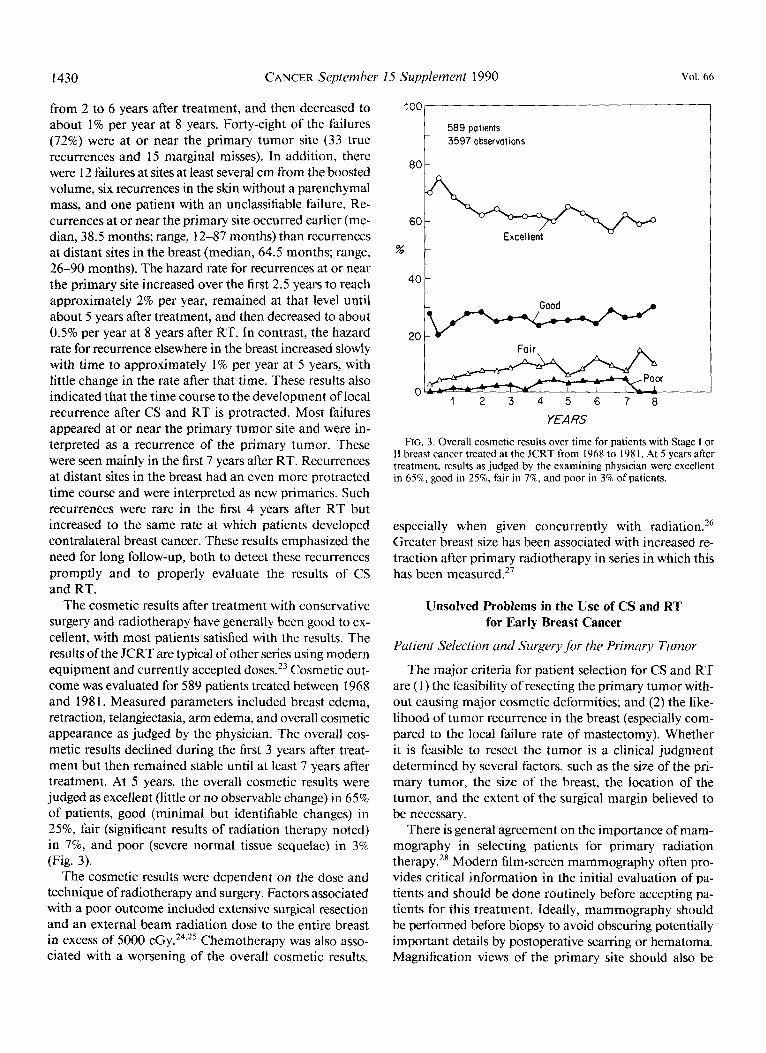
B-06) in 1976 comparing mastectomy with segmental mastectomy, with or without radiotherapy. A total of 1843 evaluable patients with clinical Stage I or I1 tumors mea- suring up to 4 cm were entered by the time of closure in January 1984. All patients underwent axillary dissection. Those with involved lymph nodes received adjuvant che- motherapy with melphalan and 5-fluorouracil (L-PAM/ 5-Fu), with one cycle given before radiotherapy. Conser- vative surgery as performed in the NSABP trial consisted of resection of the tumor with enough normal tissue re- moved around it to insure that the specimen margins were tumor free. In 10% of the patients randomly assigned to segmental mastectomy, it was not possible to obtain tu- mor-free margins and total mastectomy was performed in these patients. Radiotherapy was delivered to the breast alone with supervoltage equipment using opposed tan- gential fields (often without wedge filters to compensate for the slope of the breast), to a dose of 5000 to 5300 cGy in 5 to 6 weeks. The regional lymph nodes were not treated, and no boost was given to the tumor site. The latest results ofthe NSABP trial were published in 1989,3 and at 8 years comparable rates of local-regional recur- rence, distant failure, and overall survival were observed for patients treated with mastectomy and CS and RT (Fig. 3).
Another trial was conducted from 1972 to 1979 at the Institut Gustave Roussy in Villejuif, France, under the sponsorship of the World Health Organization. This in- cluded 179 patients with tumors pathologically 2 cm or smaller with either clinically involved or uninvolved lymph nodes. Patients were randomized to receive either modified radical mastectomy or CS and RT. CS in this trial consisted of removal of the tumor with a surrounding margin of 2 cm of grossly normal breast tissue ("tumor- ectomy"). All patients underwent low axillary dissection; if on frozen section diagnosis nodes were found to be involved, surgery was extended to a complete axillary dis- section. Adjuvant chemotherapy was not used. Radio- therapy was given with cobalt-60 to a dose of 4500 cGy in 18 fractions over 1 month, treating the breast four times weekly. A boost of 1500 cGy was given to the tumor bed in six fractions. A mean follow-up of 10 years found no statistically significant difference in local-regional recur-
Overall Survival
P = 0.2 P = 0 3
A L + XRT
40 40
0 172 Events A 186 Events
Y e a r 0 1 2 3 4 5 6 7 8 0 1 2 3 4 5 6 7 8 0 1 2 3 4 5 6 7 8 0 590 Patients, 217 Events A 629 Patients, 217 Events
0 130 Deaths A 120 Deaths
FIG. 2. Disease-free, distant dis- ease-free, and overall survival rates of patients treated with total mas- tectomy (TM) or lumpectomy and radiotherapy (L + XRT).

No. 6 TREATMENT OF EARLY BREAST CANCER - Harris et al. 1429
rence, metastases, or overall survival between the two treatment group^.^
The fourth prospective randomized trial was begun by the National Cancer Institute of the United States in 1979. By September 1986, 224 patients with clinical Stage I or I1 breast cancer had been entered and randomized to un- dergo either modified radical mastectomy or conservative excision, full axillary dissection, and radiotherapy to the breast. Patients with histologically involved nodes also received doxorubicin-cyclophosphamide chemotherapy. A median follow-up of 48 months found no significant difference in outcome between these two group^.^ This study is still accruing patients.
It is also of interest to examine two of the earliest trials comparing CS and RT with mastectomy from Guy's Hospital in London6-' The inadequacy of the treatment in these trials, however, makes it difficult to assess their implications for the use of CS and RT with modern tech- niques. In the first trial, carried out from 1961 to 1971, 376 patients with T 1 or T2, NO or N 1 breast cancer were randomly assigned to undergo either wide excision (WE) or radical mastectomy (RM). Both groups also received radiotherapy. In the second trial, conducted from 1971 to 1975, entry was restricted to patients with a clinically negative axilla (NO). Two hundred fifty-two patients were similarly randomized to undergo either WE or RM. Of note, patients randomized to WE did not undergo axillary dissection, and the doses and technique of RT used to treat the axilla are now known to be inadequate. As a result, axillary recurrence was considerably more common in patients treated with WE and RT ( 17%) than in patients treated with RM and RT (2%). Recurrence in the breast was seen in only 23 of the 300 patients (7%) treated with WE and RT. The latest published results indicated that N 1 patients treated in the first trial and NO patients treated in the second trial had fewer distant metastases and a higher likelihood of survival when treated with RM and RT than when treated with WE and RT.8
The interpretation of these results is not straightforward. They suggest that eradication of axillary disease is im- portant to prevent distant metastases and to improve long- term survival. The Joint Center for Radiation Therapy (JCRT) and others have argued that there may be a small survival benefit to effective axillary There are, however, several other sources of evidence that suggest that axillary treatment is not associated with improved long-term survival.".12 In a recent subset analysis of the Guy's Hospital trial,8 Hayward and Caleffi found that, for NO patients, the improvement in survival seen with RM and RT was restricted to patients with smaller (TI) can- cers. This analysis suggests that axillary tumor control is most important in patients with small tumors, who have the greatest likelihood of long-term survival using local treatment alone. Given the inadequacy of the radiotherapy
in the Guy's trial, it is difficult to assess its implications for the use of CS and RT with modern techniques.
Retrospective Studies of CS and RT
Since the mid- 1950s there have been numerous reports from centers in Europe and North America on the use of CS and RT to treat patients with clinical Stage I and I1 breast carcinoma^.'^-^^ These series demonstrated that high levels of local tumor control and satisfactory cosmetic results can be achieved by the use of CS and RT. These retrospective studies, often with long follow-up and from a single institution, have documented various features af- ter CS and RT, such as the time course and pattern of recurrence in the breast, factors influencing the risk of recurrence in the breast, and factors influencing cosmetic results.
One important conclusion drawn from these retro- spective analyses concerns the time course to local recur- rence. Whereas most local-regional recurrences after mastectomy manifest within the first several years after treatment, patients treated with CS and RT must be ob- served for local recurrence for a much longer period. To examine this issue, a collaborative retrospective review was done of the results of treatment of 152 patients ir- radiated before 1967 at the Institut Curie, the Marseilles Cancer Institute, and the Princess Margaret Hospital.21 Minimum follow-up time was 15 years. The techniques and doses used during this period were less satisfactory than current ones. Although most tumor recurrences in the breast occurred during the first 5 years after treatment, the actuarial risk of local recurrence was nearly constant for 14 years after treatment. No local recurrences were seen between 15 and 20 years, although the number of patients at risk was small. The cumulative 15-year risk of developing a breast recurrence was 29%. This incidence, however, was different for each of the three institutions, and was lowest for the center that gave the highest doses of radiation. The actuarial 15-year freedom from distant metastases and survival rates were 71% and 52% respec- tively. These data demonstrate the long period during which patients may be at risk for recurrence in the breast after CS and RT.
A more modern study from our institution on the time course to tumor recurrence in the breast was recently published.22 In that study, we examined the time course and patterns of breast recurrence as a first site of treatment failure in 607 clinical Stage I or I1 invasive breast carci- nomas treated from 1968 to 1981. Sixty-seven patients had a recurrence in the breast ( I I%), corresponding to 5- and l0-year actuarial rates of 10% and 1670, respectively. The hazard rate ( i e . , the risk per unit time of a failure) for any breast failure increased over the first 2 years, was fairly constant at about 2.5% per year over the period
1430 CANCER September 15 Supplement 1990 Vol. 66
from 2 to 6 years after treatment, and then decreased to about 1% per year at 8 years. Forty-eight of the failures (72%) were at or near the primary tumor site (33 true recurrences and 15 marginal misses). In addition, there were 12 failures at sites at least several cm from the boosted volume, six recurrences in the skin without a parenchymal mass, and one patient with an unclassifiable failure. Re- currences at or near the primary site occurred earlier (me- dian, 38.5 months; range, 12-87 months) than recurrences at distant sites in the breast (median, 64.5 months; range, 26-90 months). The hazard rate for recurrences at or near the primary site increased over the first 2.5 years to reach approximately 2% per year, remained at that level until about 5 years after treatment, and then decreased to about 0.5% per year at 8 years after RT. In contrast, the hazard rate for recurrence elsewhere in the breast increased slowly with time to approximately 1% per year at 5 years, with little change in the rate after that time. These results also indicated that the time course to the development of local recurrence after CS and RT is protracted. Most failures appeared at or near the primary tumor site and were in- terpreted as a recurrence of the primary tumor. These were seen mainly in the first 7 years after RT. Recurrences at distant sites in the breast had an even more protracted time course and were interpreted as new primaries. Such recurrences were rare in the first 4 years after RT but increased to the same rate at which patients developed contralateral breast cancer. These results emphasized the need for long follow-up, both to detect these recurrences promptly and to properly evaluate the results of CS and RT.
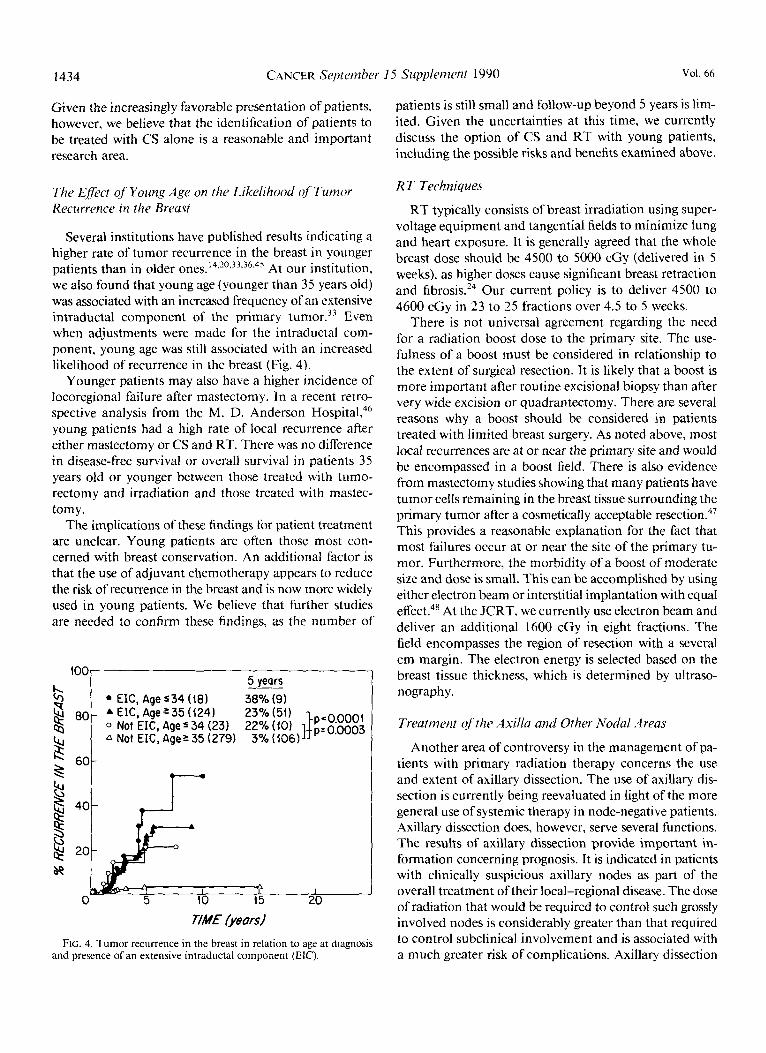
The cosmetic results after treatment with conservative surgery and radiotherapy have generally been good to ex- cellent, with most patients satisfied with the results. The results of the JCRT are typical of other series using modem equipment and currently accepted doses.23 Cosmetic out- come was evaluated for 589 patients treated between 1968 and 198 1. Measured parameters included breast edema, retraction, telangiectasia, arm edema, and overall cosmetic appearance as judged by the physician. The overall cos- metic results declined during the first 3 years after treat- ment but then remained stable until at least 7 years after treatment. At 5 years, the overall cosmetic results were judged as excellent (little or no observable change) in 65% of patients, good (minimal but identifiable changes) in 25% fair (significant results of radiation therapy noted) in 7%, and poor (severe normal tissue sequelae) in 370 (Fig. 3).
The cosmetic results were dependent on the dose and technique of radiotherapy and surgery. Factors associated with a poor outcome included extensive surgical resection and an external beam radiation dose to the entire breast in excess of 5000 cGy.24,25 Chemotherapy was also asso- ciated with a worsening of the overall cosmetic results,
589 patients 3597 observations t
40 t Good
20 I fair^ A
Poor 73- -
I n - - " -~ 1 2 3 4 5 6 7 8
YEARS
FIG. 3. Overall cosmetic results over time for patients with Stage I or I1 breast cancer treated at the JCRT from 1968 to 198 I . At 5 years after treatment, results as judged by the examining physician were excellent in 65%, good in 25%, fair in 7%, and poor in 3% of patients.
especially when given concurrently with radiation.26 Greater breast size has been associated with increased re- traction after primary radiotherapy in series in which this has been mea~ured.~'
Unsolved Problems in the Use of CS and RT for Early Breast Cancer
Patient Selection and Surgery.for the Primary Tumor
The major criteria for patient selection for CS and RT are (1) the feasibility of resecting the primary tumor with- out causing major cosmetic deformities; and (2) the like- lihood of tumor recurrence in the breast (especially com- pared to the local failure rate of mastectomy). Whether it is feasible to resect the tumor is a clinical judgment determined by several factors, such as the size of the pri- mary tumor, the size of the breast, the location of the tumor, and the extent of the surgical margin believed to be necessary.
There is general agreement on the importance of mam- mography in selecting patients for primary radiation therapy.28 Modern film-screen mammography often pro- vides critical information in the initial evaluation of pa- tients and should be done routinely before accepting pa- tients for this treatment. Ideally, mammography should be performed before biopsy to avoid obscuring potentially important details by postoperative scarring or hematoma. Magnification views of the primary site should also be

No. 6 TREATMENT OF EARLY BREAST CANCER * Harris et a/. 1431
performed, because they may show unsuspected extension of the lesion. Mammograms after biopsy are used to assess the completeness of resection in tumors with microcal- cifications.
Patients with two nonadjacent primary tumors (i. e., separated by more than several centimeters) in the same breast, demonstrated either by palpation or mammogram, are poor candidates for breast-conserving treatment for two reasons. First, the cosmetic results of multiple wide, local excisions and radiation boosts are likely to be un- desirable. Second, these patients may well have other rel- atively large concentrations of tumor cells within the breast. Similar concerns exist for patients whose mam- mograms reveal extensive microcalcifications that appear to be malignant. Just over half of the patients in each of these groups will have more than one quadrant of the breast involved pathologically when mastectomy is per- formed.29 The rate of tumor recurrence in the breast would be expected to be substantially higher in these patients because they are more likely to have a large number of residual tumor cells in the breast after excisional biopsy than patients with a single gross lesion. The radiation dose that can be tolerated by the entire breast is smaller than the dose directed to the primary site and is less likely to control these residual tumor cells extending away from the primary. We recently reviewed a group of ten patients who had excision of two primary tumors in the same breast followed by radiotherapy. To date, four of the ten have had a recurrence in the breast.30
The location of the tumor is also a consideration in treatment selection. For patients with subareolar tumors, there is concern of spread of the disease along the ducts that might not be excised by a nipple-conserving resection. For such lesions to be treated successfully with CS and RT, resection of the nipple-areola complex may be nec- essary, and many patients consider this surgery acceptable because the appearance, texture, and sensation of the breast are preserved. Others may prefer mastectomy and reconstruction.
There is controversy concerning the maximum size of the tumor acceptable for treatment, although tumor size itself has not been shown to be a significant risk factor for local recurrence after excisional biopsy and radio- therapy. In the JCRT series, local recurrence rates were similar for all tumor sizes up to 5 ~ m . ~ ’ In the NSABP B-06 trial, local recurrence rates were 6.5% for TI patients and 9.6% for T2 tumors ( P = NS).”
A final but critical factor regarding the use of CS and RT is the psychological attitude of the patient. The ideal patient is one who is concerned about preserving body image and the normal sensation of the breast, but is not concerned about the use and inconvenience of radio- therapy. On the other hand, there are patients who are technically suitable for CS and RT who simply choose
mastectomy (given a clear and honest discussion of the options).
The extent of surgical resection required before radio- therapy is controversial. Recurrence in the breast is clearly more frequent among patients who do not have a com- plete gross excision of the primary tumor.” Hence, com- plete gross excision of the primary tumor is mandatory. When patients are seen for treatment at the JCRT after a biopsy at an outside institution, a re-excision is per- formed if there is uncertainty about the adequacy of the initial excision. Some centers routinely advocate a wide resection, removing up to 2 cm of grossly uninvolved breast tissue around the primary mass, or even removal of the entire affected quadrant. Such wide resections do not appear necessary to achieve excellent local control rates provided an adequate dose of radiation is given. The high level of local tumor control in the JCRT series was obtained by removing only a small rim of normal tissue around the primary tumor, followed by whole breast ir- radiation and a “boost” to the primary site. At the Institut Gustave Roussy, where a boost dose was also typically employed, local-regional recurrence was seen in four of 47 or 9% of patients treated with quadrantectomy, com- pared with 20 of 389 or 5% of patients treated with ex- cisional biopsy.32 Similarly, Chu et al. did not find an advantage to quadrantectomy over excisional biopsy for patients treated with radiotherapy that included a boost to the primary site. It appears likely that an inverse re- lationship links these two aspects of therapy: that is, equal results can be achieved with wider excisions and lower doses of radiation, or with smaller gross total excisions and higher doses of radiation.
A related controversy is whether patients who have mi- croscopically involved (or “positive”) margins can be treated as successfully as patients with microscopically uninvolved margins. The experiences of the JCRT and the Institut Gustave Roussy3’ suggest that, by the use of a boost to the primary site to doses of at least 6000 cGy, local tumor control can be achieved in patients with close or involved margins (with the possible exception of pa- tients in certain pathologic subgroups discussed below). There are, however, technical problems in assessing mar- gins. It is essential that the pathologist ink the margins of resection before cutting the specimen so that they can be clearly identified on microscopic examination. If the tu- mor is resected in two or more specimens, it is often not possible to orient the specimens to determine the margins even if ink is used. There is also no clear definition of what constitutes “involved margins.” This can imply that cancer is seen either directly at an inked surface or within some arbitrary distance from an inked margin. Such a definition is obviously influenced by the number of sec- tions assessed for involvement, and in clinical practice sampling error may be a significant problem in determin-

1432 CANCER Septeizber 15 Supplement 1990 Vol. 66
ing margin involvement. It may also be clinically impor- tant to distinguish between “focal” or “minimal” in- volvement of the margins and more extensive involve- ment. We do not believe that the mere presence of tumor at or near a margin should prevent a patient from receiving treatment with CS and RT.
Our institution investigated the influence of various pathologic features in the excision specimen on the sub- sequent risk of local recurrence. We recently reported the risk of local recurrence in 445 patients with infiltrating ductal carcinoma treated between 1968 and 1981. All specimens had sufficient adjacent breast tissue for patho- logic review, and all patients received a boost dose to give the tumor bed a minimum dose of 60 The median follow-up in this group was 63 months. In most patients, the tumor was excised grossly with a small rim of adjacent breast tissue, without regard to the microscopic margins of resection. The margins were not routinely inked or labeled during this period and therefore were not evaluable in most cases on review. A variety of clinical and patho- logic factors were examined, and the major factor shown to have a statistically significant association with local re- currence was the presence of what we have termed an “extensive intraductal component” (EIC). Tumors were described as being in this category when two features were simultaneously present: intraductal carcinoma promi- nently present within the tumor and intraductal carci- noma clearly extending beyond the infiltrating margin of the tumor or present in sections of grossly normal adjacent breast tissue. Tumors that were predominantly intraductal with focal invasion were also scored as having an EIC. Overall, an extensive intraductal component was found in 31% of patients. This group had a 25% actuarial risk of tumor recurrence in the breast at 5 years, compared with only 5% for patients without an ElC (P < 0.0001). Of note, the presence of both prominent intraductal car- cinoma “within” the primary tumor and any amount of intraductal cancer “adjacent” to it was necessary to be associated with this increased risk of local recurrence; nei- ther factor alone was a risk factor.
The reason for the association of an EIC with a high risk of recurrence in the breast is not entirely clear. Patients with EIC-positive tumors do not have a greater risk of distant metastases than patients with ElC-negative tumors. Recently, we analyzed the risk of distant metastases in our patients and found that patients with EIC-positive tumors had a somewhat lower risk than patients with ElC- negative tumors (21% vs. 26%; P = 0.21).34 It is therefore unlikely that an EIC represents a more aggressive form of disease. It seems more likely that the factor that links an EIC to recurrence in the breast is that EIC-positive patients have a greater residual tumor burden after gross excision than do other patients. We found that, in a group of patients who underwent reexcision of the primary site,
those with an ElC in the initial specimen were more likely to have residual cancer on reexcision than other patients. The likelihood of finding substantial residual cancer (typ- ically intraductal in nature) in the reexcision specimen was 44% for patients with an EIC in the initial excision, compared with only 2% for other patients.35
A recent series from the Netherlands Cancer Institute also examined the influence of EIC on local recurrence.36 A statistically significant difference in local recurrence was seen between EIC-positive and ElC-negative tumors (9% vs. 1% at 6 years). The median follow-up in this study was between 2 and 3 years. Their treatment policy included a wider excision (1 cm grossly around the tumor) and higher doses to the entire breast (50 cGy in 25 fractions) and to the boost volume (usually 25 cGy with a two-plane implant) than in the JCRT series. Other recent clinical- pathologic studies corroborated the association between an EIC and recurrence in the breast after CS and RT.37.3X
The results of the JCRT series suggest that the optimal extent of breast resection may depend on the extent of associated intraductal carcinoma. Patients without exten- sive intraductal involvement are well treated with exci- sional biopsy, whereas patients with extensive intraductal involvement probably require a wide resection to achieve an equal rate of local control. Our policy for patients with an ElC is to carefully review the specimen and mam- mograms to be certain that the areas of associated intra- ductal involvement have been adequately excised. If an EIC is present and the excision specimen is small or the margins are microscopically involved or equivocal, then a reexcision of the biopsy site is done if CS and RT are to be considered further. If the margins of the reexcision are clear, we recommend RT as reasonable treatment. We are in the process of reviewing the results in patients with EIC-positive tumors with clear margins to verify that recurrence in the breast is, in fact, low. If the margins of the reexcision specimen in patients with EIC-positive tu- mors are involved, then the patient should understand that she may be at greater risk of local recurrence if treated with RT than if treated with mastectomy, despite the reexcision. In this situation, mastectomy is usually rec- ommended. Mastectomy may also be more desirable in cases in which reexcision is not technically possible or cannot be done without severe deformity of the breast.
In practice we are also influenced by the status of the axillary nodes. When axillary nodes are pathologically in- volved, patients are typically treated with adjuvant sys- temic therapy. As discussed below, the use of adjuvant systemic therapy appears to reduce the risk of tumor re- currence in the breast after CS and RT. The rate of local- regional recurrence after mastectomy in node-positive patients is substantial (10% to 25% in various series, even with the use of adjuvant chemotherapy or hormonal ther- apy), making mastectomy a less effective option than it

No. 6 TREATMENT OF EARLY BREAST CANCER - Harris et al. 1433
is in patients with negative nodes. In contrast, for patients with negative nodes mastectomy is a highly effective form of local treatment, and the possible adverse impact of local recurrence on survival is of more concern. Hence, we generally recommend mastectomy more strongly for node-negative patients whose tumors have an EIC and positive margins on reexcision.
Omission ofRT .4fer CS
It is questionable whether RT can be safely omitted after CS in certain patients. Retrospective studies of pa- tients treated with CS alone have demonstrated recurrence rates of 15% to 40%.3,'4,39-42 To address this question, it is important to first answer questions such as the following: Is a high rate of recurrence in the breast associated with an increased risk of breast cancer mortality? Are there subsets of patients who have a low risk of recurrence in the breast after CS? Can recurrence in the breast after CS be treated with further CS and RT or will mastectomy be required? Can adjuvant tamoxifen decrease the risk of recurrence in the breast after CS? What are the long-term toxicities of breast RT?
The data from the NSABP trial B-06 are relevant to consideration of the possible use of CS alone.3 In the recent update of this trial, the 8-year actuarial incidence of re- currence in the breast was 10% in the patients who re- ceived radiotherapy, compared with 39% in patients who did not have radiotherapy ( P < 0.01). This marked dif- ference was seen both in patients with histologically in- volved and uninvolved lymph nodes. Of note, patients with involved lymph nodes treated with segmental mas- tectomy and adjuvant chemotherapy (but not radiother- apy) had a greater risk of recurrence in the breast (43%) than did patients with uninvolved nodes treated with only segmental mastectomy (37%). However, patients with in- volved nodes who received radiotherapy as well as che- motherapy had a smaller risk of tumor recurrence in the breast (6%) than did patients with uninvolved nodes treated with radiotherapy without chemotherapy ( 12%). This suggests that chemotherapy by itself does little to prevent recurrence in the breast, but that radiotherapy and chemotherapy may be additive or synergistic in re- ducing tumor recurrence in the breast.
The overall 39% rate of recurrence in the breast after CS alone seen in the NSABP trial is a major problem in clinical practice. Even if such recurrence does not affect survival, it can have considerable psychological effects. The critical question of whether or not such recurrences affect survival is, we believe, still unanswered. In the NSABP trial, there was an advantage in disease-free sur- vival for patients treated with CS and RT compared with those treated with CS alone ( P = 0.01). This advantage was seen both for patients with negative nodes (66.1% for
CS and RT vs. 60.7% for CS, P = 0.02) and for patients with positive nodes (49% for CS and RT vs. 43% for CS, P = 0.3). Of note, only distant failure or inability to salvage a breast recurrence was scored in the NSABP calculation of disease-free survival. Thus, the difference in disease- free survival is of some concern. The 8-year survival results for patients treated with CS alone were worse when com- pared with patients treated with CS and RT, but the dif- ference was not statistically significant. For patients with negative nodes, the 8-year survival rate was 82% for CS and RT versus 76.7% for CS alone ( P = 0.5), and for patients with positive nodes it was 70% for CS and RT versus 6 1.6% for CS ( P = 0.5). Additional follow-up time from the study is required to assess the influence of a 39% rate of recurrence in the breast on survival.
A subset of patients at low risk of recurrence after CS alone has not been identified. The NSABP has not pub- lished a subset analysis of breast recurrence risk for pa- tients treated with CS alone. A recent study of patients with TlNO tumors treated with an extensive resection (at least a 2.5 cm margin macroscopically) showed a 16% rate of recurrence in the breast.42 It is unlikely, however, that such an extensive resection will be useful clinically in this country. In an attempt to identify a possible group for treatment with CS alone, we initiated an experimental protocol of CS alone 4 years ago for patients with TI infiltrating ductal cancers with pathologically negative nodes, 1 cm microscopic margins, and without lymphatic or blood vessel invasion or an extensive intraductal com- ponent. Follow-up in this study has been too short to have meaningful results.
Another issue regarding the possible use of CS alone is whether recurrence in the breast after CS can be managed with further CS and RT or if mastectomy will be required. The NSABP B-06 protocol has provided no information on this issue since it called for mastectomy for patients with an isolated recurrence in the breast. Initial RT may be important simply to maximize the chances of breast conservation.
It is also possible that adjuvant tamoxifen reduces the risk of recurrence in the breast in some patients, making CS alone a more acceptable option. At present, however, no long-term results are available using this approach. Another reason to consider CS alone instead of CS and RT is the long-term toxicities of RT. At present, the in- cidence of long-term toxicities from breast RT is very
but more years of follow-up are required to establish this with greater certainty. It is possible that attempts to include regional lymph nodes in the target volume may be associated with increased toxicity, and this must be addressed ~eparately.~~
At present, given the available information, we do not believe CS alone has been established as a treatment op- tion for any group of patients with invasive breast cancer.
1434 CANCER September I 5 Supplement 1990 Vol. 66
Given the increasingly favorable presentation of patients, however, we believe that the identification of patients to be treated with CS alone is a reasonable and important research area.
The Efect of Yoling Age on the Likelihood qf Tumor Recurrence in the Breast
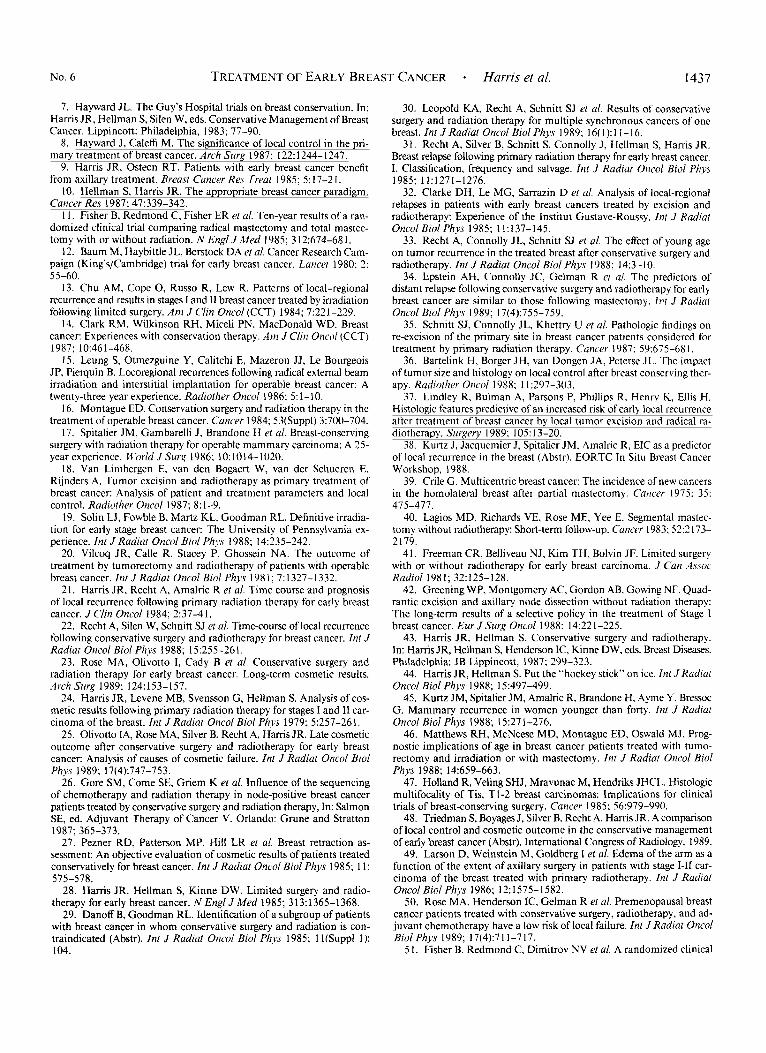
Several institutions have published results indicating a higher rate of tumor recurrence in the breast in younger patients than in older ones.'4~'0233336,45 At our institution, we also found that young age (younger than 35 years old) was associated with an increased frequency of an extensive intraductal component of the primary tumor.33 Even when adjustments were made for the intraductal com- ponent, young age was still associated with an increased likelihood of recurrence in the breast (Fig. 4).
Younger patients may also have a higher incidence of locoregional failure after mastectomy. In a recent retro- spective analysis from the M. D. Anderson Hospital,46 young patients had a high rate of local recurrence after either mastectomy or CS and RT. There was no difference in disease-free survival or overall survival in patients 35 years old or younger between those treated with tumo- rectomy and irradiation and those treated with mastec- tomy.
The implications of these findings for patient treatment are unclear. Young patients are often those most con- cerned with breast conservation. An additional factor is that the use of adjuvant chemotherapy appears to reduce the risk of recurrence in the breast and is now more widely used in young patients. We believe that further studies are needed to confirm these findings, as the number of
I 20
77M€ fjeard FIG. 4. Tumor recurrence in the breast in relation to age at diagnosis
and presence of an extensive intraductal component (EJC).
patients is still small and follow-up beyond 5 years is lim- ited. Given the uncertainties at this time, we currently discuss the option of CS and RT with young patients, including the possible risks and benefits examined above.
R T Techniques
RT typically consists of breast irradiation using super- voltage equipment and tangential fields to minimize lung and heart exposure. It is generally agreed that the whole breast dose should be 4500 to 5000 cGy (delivered in 5 weeks), as higher doses cause significant breast retraction and fibrosis.24 Our current policy is to deliver 4500 to 4600 cGy in 23 to 25 fractions over 4.5 to 5 weeks.
There is not universal agreement regarding the need for a radiation boost dose to the primary site. The use- fulness of a boost must be considered in relationship to the extent of surgical resection. It is likely that a boost is more important after routine excisional biopsy than after very wide excision or quadrantectomy. There are several reasons why a boost should be considered in patients treated with limited breast surgery. As noted above, most local recurrences are at or near the primary site and would be encompassed in a boost field. There is also evidence from mastectomy studies showing that many patients have tumor cells remaining in the breast tissue surrounding the primary tumor after a cosmetically acceptable resection.47 This provides a reasonable explanation for the fact that most failures occur at or near the site of the primary tu- mor. Furthermore, the morbidity of a boost of moderate size and dose is small. This can be accomplished by using either electron beam or interstitial implantation with equal effect.48 At the JCRT, we currently use electron beam and deliver an additional 1600 cGy in eight fractions. The field encompasses the region of resection with a several cm margin. The electron energy is selected based on the breast tissue thickness, which is determined by ultraso- nography.
Treatment oj'the Axilla and Other Nodal '4 rea.5
Another area of controversy in the management of pa- tients with primary radiation therapy concerns the use and extent of axillary dissection. The use of axillary dis- section is currently being reevaluated in light of the more general use of systemic therapy in node-negative patients. Axillary dissection does, however, serve several functions. The results of axillary dissection provide important in- formation concerning prognosis. It is indicated in patients with clinically suspicious axillary nodes as part of the overall treatment of their local-regional disease. The dose of radiation that would be required to control such grossly involved nodes is considerably greater than that required to control subclinical involvement and is associated with a much greater risk of complications. Axillary dissection

1435 No. 6 TREATMENT OF EARLY BREAST CANCER - Harris et al.
itself is also an effective means of preventing tumor re- currence in the axilla. It allows the radiotherapist to treat the disease with tangential fields directed towards the breast in most cases. This eliminates the risk of compli- cations due to overlap between multiple treatment fields. For these reasons, we still recommend axillary dissection in nearly all patients.
The surgical technique that is generally employed is a “Level 1/11 dissection.” The boundaries of this dissection are the latissimus dorsi, laterally: the medial border of the pectoralis minor muscle, medially: the axillary vein, su- periorly; and the tail of the breast, inferiorly. This provides a high rate of lymph node involvement detection, as well as local tumor control in the axilla. In our experience, removal of the Level I11 nodes, stripping of the axillary vein, or both have increased the likelihood of arm edema.49 Also, the combination of full axillary dissection and axillary irradiation results in a significant risk of arm edema and should generally be avoided.49
Patients who have involved axillary nodes or medial lesions are known to be at significant risk for subclinical involvement of the internal mammary and supraclavic- ular nodal areas, and some radiotherapists favor treatment of these to prevent tumor recurrence. At present it is un- clear whether such treatment improves overall survival rates. The results of the randomized trials of Milan and of the NSABP comparing treatment with mastectomy with treatment with CS and RT were achieved with ir- radiation of the breast alone, thus establishing this ap- proach as a standard option to be considered. Treatment of these other regional nodal areas requires technical ex- pertise to avoid overlapping of fields and to minimize irradiation of the underlying lung. For patients with left- sided lesions, substantial doses to the heart may accom- pany irradiation of the internal mammary nodes (IMN) or with certain RT techniques, such as the photon-only hockey-stick. This technique appears to have been asso- ciated with late cardiac deaths in at least some studies, and should be avoided.44
On the other hand, it is possible that the maximum effectiveness of adjuvant systemic therapy might be seen only in a situation of maximal local-regional control. Al- though the appearance of clinically evident supraclavicular and internal mammary nodal recurrences may not influ- ence prognosis, they can be psychologically and at times physically harmful to the patient. At present we believe that treatment to the breast alone is acceptable in all sit- uations, but that it is reasonable to treat the internal mammary and supraclavicular areas in patients who have involved axillary nodes or in whom the primary tumor is located medially, provided that the treatment techniques available to the radiotherapist allow this to be done with only limited potential morbidity. At our institution, most patients are treated with breast irradiation alone.
Impuct and Integration of R T With Adjuvant Systemic Therapy
There is evidence suggesting that the use of adjuvant chemotherapy might reduce the risk of recurrence in the breast when used in conjunction with CS and RT. As noted above, the rate of recurrence in the breast in the NSABP B-06 trial was lower for patients treated with CS and RT who received chemotherapy than for those who did not.3 We recently found similar results in our own patients treated with adjuvant ~hemotherapy.~’ The 5- year actuarial rate of recurrence in the breast in pre- menopausal patients who received minimum tumor-bed doses of 6000 cGy or more was 15% in 192 patients treated with irradiation alone, compared with 4% in 74 patients treated with irradiation and chemotherapy ( P = 0.02). The number of postmenopausal patients treated with ad- juvant chemotherapy was small, and no effect was ob- served in this group. In both the NSABP B-06 and JCRT series, the effects of chemotherapy were assessed by in- direct comparisons because the patients who received chemotherapy were node-positive, and patients who did not were node-negative, and therefore may be dissimilar.
The more recent NSABP B- 13 trial comparing outcome for node-negative patients who received chemotherapy with that of controls who did not, may allow a more sci- entifically valid assessment of the effect of ~hemotherapy.~’ In this trial, 32% of the 679 patients were treated with CS and RT. With a median follow-up of approximately 2 years, four recurrences in the breast were observed in the CS and RT group (3.7%) compared with one in the CS, RT, and chemotherapy group (0.9%; P = 0.15). Additional follow-up in this study, as well as from other trials, will be required to determine whether or not chemotherapy reduces the risk of recurrence in the breast when used in conjunction with CS and RT.
Adjuvant tamoxifen may reduce the risk of recurrence in the breast when used in conjunction with CS and RT. This was examined in the NSABP B-14 trial that com- pared outcome after adjuvant tamoxifen with that of con- trols among 2644 node-negative patients, 38% of whom received CS and RT.52 With a median follow-up time of approximately 2 years, 11 recurrences in the breast were observed in the CS and RT group compared to none in the CS, RT, and tamoxifen group ( P = 0.0008). Here too, however, additional follow-up will be required before firm conclusions can be reached.
The optimal sequencing and timing of radiation and chemotherapy are unknown. Possibilities include giving the entire course of chemotherapy before radiation, giving the entire course of chemotherapy after radiation, giving both concurrently, or giving a portion of the chemother- apy before irradiation and then completing chemotherapy afterward (“sandwich technique”). Several studies assessed

1436 CANCER September 15 Supplement 1990 Vol. 66
the results of giving chemotherapy after radiation. With the exception of one retrospective data from these studies suggest that patients receiving prior RT can receive adequate ( ie . , 2 8 5 % of the prescribed) doses of chemo- the rap^.^^-^^ However, an increased incidence of lym- phocytopenia generally has been seen in patients treated after RT. As a result, dose modifications in patients who receive chemotherapy after irradiation should be based on the granulocyte count, rather than on the total white cell count.
Currently, there is no consensus as to the optimal timing of chemotherapy and RT. In an attempt to evaluate this issue, we are performing a prospective randomized trial for patients who will receive CS and RT and are at sig- nificant risk of distant failure. This currently includes node-positive patients, and node-negative patients whose tumors are estrogen receptor protein (ERP)-negative or demonstrate lymphatic vessel invasion. These patients are randomized to receive four cycles of chemotherapy, each lasting 3 weeks, consisting of cyclophosphamide, doxo- rubicin, methotrexate, 5-Fu. and prednisone ( C A M F P ) either before or after completion of RT. (Postmenopausal patients with ERP-positive tumors receive tamoxifen for 5 years after the completion of chemotherapy and RT.) As yet, there is insufficient follow-up in this trial to draw firm conclusions.
Putient FoIIow- Up and Salvage After Recurve~ce in the Breasr
Patients treated with CS and RT require close follow- up to detect treatable recurrences in the breast. In a recent study of patients from the JCRT who had a recurrence in the breast after CS and RT, approximately 35% were detected only by mammography, 40% only on physical examination, and the remainder by both methods5' We currently recommend that patients have a physical ex- amination at least every 6 months and annual mammog- raphy for life, to detect both recurrence in the ipsilateral breast and new contralateral primary tumors. We typically perform the first posttreatment mammogram at 6 months to establish a new baseline. As with the initial evaluation of patients, there is an overlap between benign and ma- lignant lesions in the findings on both physical exami- nation and mammography after CS and RT. Biopsy should be performed in cases in which there is doubt over whether a new finding represents recurrence. We found that a small incisional or core-cutting biopsy has a low false-negative rate and does not cause difficulties in healing or wound infection.60
The prognosis after tumor recurrence in the breast after CS and RT is much better than that after chest-wall re- currence after mastectomy. Approximately one third to one half of chest-wall recurrences after mastectomy are
found simultaneously or after the discovery of distant metastases. Even when apparently isolated, almost all pa- tients with a chest-wall recurrence after mastectomy will eventually develop metastases.6' In contrast, approxi- mately 50% of patients who have a recurrence in the breast after CS and RT are alive and free of distant metastases 5 to 10 years after treatment.6'
Mastectomy is the standard treatment for patients with an isolated recurrence in the breast after CS and RT. Whether less radical procedures in this setting are effective is unclear. It seems unlikely that patients who have a re- currence despite CS combined with RT could subse- quently be well managed with CS alone. It is possible, however, that selected patients (e.g., those with late, small recurrences in another portion of the breast) might be treated with wide local excision. Many patients who de- velop a recurrence in the breast may wish to consider breast reconstruction after mastectomy. Reconstruction with myocutaneous flaps yields excellent results and pro- motes tissue healing.
Assessment
CS and RT has been established as an option, along with mastectomy, in the management of patients with early stage breast cancer based on the results of retro- spective and prospective trials. The major advantages of this treatment approach are cosmetic and psycho-social, as the patient is able to retain both body image and sen- sation. There are still controversies regarding the imple- mentation of the treatment. Further research is required to clearly establish guidelines for patient selection, the optimal techniques of surgery and RT, the optimal inte- gration of chemotherapy and RT (when both are to be used), and whether or not RT can be safely omitted in some patients.
REFERENCES
I . Harris JR, Beadle GF, Hellman S. Clinical studies on the use of radiation therapy as primary treatment of early breast cancer. Cancer 1984; 53:705-7 1 1.
2. Veronesi U, Banfi A, Del Vecchio M el al. Comparison of Halsted mastectomy with quadrantectomy, axillary dissection and radiotherapy in early breast cancer: Long-term results. Eur J Cancer Clin Oncol 1986;
3. Fisher B, Redmond C, Poisson R et al. Eight-year results of a ran- domized clinical trial comparing total mastectomy and lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med
4. Sarrazin D, Le MG, Amagada R ef ul. Ten-year results of a ran- domized trial comparing a conservative treatment to mastectomy in early breast cancer. Radiother Oncol 1989; 14:177-184.
5. Bader J , Lippman M, Swain S el al. Preliminary report of the NCI early breast cancer (BC) study: A prospective randomized comparison of lumpectomy (L) and radiation (XRT) to mastectomy (M) for Stage I and I1 BC (Abstr). Int JRadiat Oncol Biol Phys 1987; 13(Suppl l):160.
6. Atkins H, Hayward JL, Klugman DJ, Wayte AB. Treatment of early breast cancer: A report after ten years of a clinical trial. Br hfed J 1972; 2:423-429.
22:1085-1089.
1989; 320:822-828.
No. 6 TREATMENT OF EARLY BREAST CANCER * Harris el a[. 1437
7. Hayward JL. The Guy’s Hospital trials on breast conservation. In: Hams JR, Hellman S, Silen W, eds. Conservative Management of Breast Cancer. Lippincott: Philadelphia, 1983; 77-90.
8. Hayward J, Caleffi M. The significance of local control in the pri- mary treatment of breast cancer. Arch Surg 1987; 122: 1244- 1247.
9. Hams JR, Osteen RT. Patients with early breast cancer benefit from axillary treatment. Breast Cancer Res Treat 1985; 5: 17-21.
10. Hellman S, Hams JR. The appropriate breast cancer paradigm. Cancer Res 1987; 47:339-342.
I 1. Fisher B, Redmond C, Fisher ER et al. Ten-year results of a ran- domized clinical trial comparing radical mastectomy and total mastec- tomy with or without radiation. N Engl J hfed 1985; 3 12:674-68 1.
12. Baum M, Haybittle JL, Berstock DA ef al. Cancer Research Cam- paign (King’s/Cambridge) trial for early breast cancer. Lancet 1980 2:
13. Chu AM, Cope 0, Russo R, Lew R. Patterns of local-regional recurrence and results in stages I and I1 breast cancer treated by irradiation following limited surgery. Am J Clin Oncol (CCT) 1984; 7221-229.
14. Clark RM, Wilkinson RH, Miceli PN, MacDonald WD. Breast cancer: Experiences with conservation therapy. Am J Clin Oncnl (CCT) 1987: 10:461-468.
15. Leung S, Otmezguine Y, Calitchi E, Mazeron JJ, Le Bourgeois JP, Pierquin B. Locoregional recurrences following radical external beam irradiation and interstitial implantation for operable breast cancer: A twenty-three year experience. Radiothrr Oncol 1986; 5: 1-10,
16. Montague ED. Conservation surgery and radiation therapy in the treatment of operable breast cancer. Cancer 1984: 53(Suppl) 3:700-704.
17. Spitalier JM, Gambarelli J, Brandone H et al. Breast-conserving surgery with radiation therapy for operable mammary carcinoma: A 35- year experience. W’orld JSurg 1986; 10:1014-1020.
18. Van Limbergen E, van den Bogaert W, van der Schueren E, Rijnders A. Tumor excision and radiotherapy as primary treatment of breast cancer: Analysis of patient and treatment parameters and local control. Radiother Oncol 1987; 8: 1-9.
19. Solin LJ, Fowble B, Martz KL, Goodman RL. Definitive irradia- tion for early stage breast cancer: The University of Pennsylvania ex- perience. Int J Radiat Oncol Bin1 Phys 1988; 14235-242,
20. Vilcoq JR, Calle R, Stacey P, Ghossein NA. The outcome of treatment by tumorectomy and radiotherapy of patients with operable breast cancer. Int JRadiat Oncol Bid Phys 1981; 7:1327-1332.
21. Harris JR, Recht A, Amalric R et al. Time course and prognosis of local recurrence following primary radiation therapy for early breast cancer. J Clin Oncol 1984; 237-41.
22. Recht A, Silen W, Schnitt SJ et al. Time-course of local recurrence following conservative surgery and radiotherapy for breast cancer. Int J Radiat Oncol Biol Phys 1988; 15:255-261.
23. Rose MA, Olivotto I, Cady B et a/. Conservative surgery and radiation therapy for early breast cancer. Long-term cosmetic results. Arch Surg 1989; 124:153-157.
34. Hams JR, Levene MB, Svensson G, Hellman S. Analysis of cos- metic results following primary radiation therapy for stages I and I1 car- cinoma of the breast. Int J Radiat Oncol Biol Phys 1979: 5:257-261.
25. Olivotto IA, Rose MA, Silver B, Recht A, Hams JR. Late cosmetic outcome after conservative surgery and radiotherapy for early breast cancer: Analysis of causes of cosmetic failure. Int J Radial Oncol Biol Phys 1989: 17(4):747-753.
26. Gore SM, Come SE, Griem K ef al. Influence of the sequencing of chemotherapy and radiation therapy in node-positive breast cancer patients treated by conservative surgery and radiation therapy, In: Salmon SE, ed. Adjuvant Therapy of Cancer V. Orlando: Grune and Stratton
27. Pezner RD, Patterson MP, Hill LR et al. Breast retraction as- sessment: An objective evaluation of cosmetic results of patients treated conservatively for breast cancer. Int J Radiat Oncol Biol Phys 1985; 1 1: 575-578.
28. Hams JR, Hellman S, Kinne DW. Limited surgery and radio- therapy for early breast cancer. N Engl J Med 1985; 3 13: 1365-1 368.
29. Danoff B, Goodman RL. Identification of a subgroup of patients with breast cancer in whom conservative surgery and radiation is con- traindicated (Abstr). Int J Radiat Oncol Biol Phys 1985: 1 I(Supp1 I) : 104.
55-60.
1987; 365-373.
30. Leopold KA, Recht A, Schnitt SJ et al. Results of conservative surgery and radiation therapy for multiple synchronous cancers of one breast. Int JRadiat Oncol Biol Phys 1989; 16(1):11-16.
31. Recht A, Silver B, Schnitt S, Connolly J, Hellman S, Hams JR. Breast relapse following primary radiation therapy for early breast cancer. I. Classification, frequency and salvage. Int J Rudiat Oncol Biol Phys
32. Clarke DH, Le MG, Sarrazin D ef al. Analysis of local-regional relapses in patients with early breast cancers treated by excision and radiotherapy: Experience of the Institut Gustave-Roussy. Inf J Radiat Oncol Bid Phys 1985; 11:137-145.
33. Recht A, Connolly JL, Schnitt SJ et al. The effect of young age on tumor recurrence in the treated breast after conservative surgery and radiotherapy. Int J Radiat Oncol Biol Phys 1988; 14:3-10.
34. Epstein AH, Connolly JC, Gelman R rt al. The predictors of distant relapse following conservative surgery and radiotherapy for early breast cancer are similar to those following mastectomy. Int J Radiat Oncol Biol Phjs 1989; 17(4):755-759.
35. Schnitt SJ, Connolly JL, Khettry U et al. Pathologic findings on re-excision of the primary site in breast cancer patients considered for treatment by primary radiation therapy. Cancer 1987; 59:675-68 1.
36. Bartelink H, Borger JH, van Dongen JA, Peterse JL. The impact of tumor size and histology on local control after breast conserving ther- apy. Radiother Oncol 1988; I1:297-303.
37. Lindley R, Bulman A, Parsons P, Phillips R, Henry I(, Ellis H. Histologic features predictive of an increased risk of early local recurrence after treatment of breast cancer by local tumor excision and radical ra- diotherapy. Surgery 1989: 105: 13-20.
38. Kurtz J, Jacquemier J, Spitalier JM, Amalric R, EIC as a predictor of local recurrence in the breast (Abstr). EORTC In Situ Breast Cancer Workshop, 1988.
39. Crile G. Multicentric breast cancer: The incidence of new cancers in the homolateral breast after partial mastectomy. Canwr 1975; 35: 475-477.
40. Lagios MD, Richards VE, Rose ME, Yee E. Segmental mastec- tomy without radiotherapy: Short-term follow-up. Cancer 1983; 5 2 2 173- 2 179.
4 I . Freeman CR, Belliveau NJ, Kim TH, Bolvin JF. Limited surgery with or without radiotherapy for early breast carcinoma. J Cun A s . m Radio1 1981; 32:125-128.
42. Greening WP, Montgomery AC, Gordon AB, Cowing NF. Quad- rantic excision and axillary node dissection without radiation therapy: The long-term results of a selective policy in the treatment of Stage I breast cancer. Eur JSurg Oncol 1988: 14:221-225.
43. Hams JR, Hellman S. Conservative surgery and radiotherapy. In: Hams JR, Hellman S, Henderson IC, Kinne DW, eds. Breast Diseases. Philadelphia: JB Lippincott, 1987; 299-323.
44. Hams JR, Hellman S. Put the “hockey stick” on ice. Int J Radial Oncol Biol Phys 1988; 15:497-499.
45. Kurtz JM, Spitalier JM, Amalric R, Brandone H, Ayme Y, Bressoc G. Mammary recurrence in women younger than forty. Int J Radiat Oncol Biol Phys 1988; 15271-276.
46. Matthews RH, McNeese MD, Montague ED, Oswald MJ. Prog- nostic implications of age in breast cancer patients treated with tumo- rectomy and irradiation or with mastectomy. Inf J Radiat Oncol Biol
47. Holland R, Veling SHJ, Mravunac M, Hendriks JHCL. Histologic multifocality of Tis, T 1-2 breast carcinomas: Implications for clinical trials of breast-conserving surgery. Cancer 1985; 56:979-990.
48. Triedman S, Boyages J, Silver B, Recht A, Hams JR. A comparison of local control and cosmetic outcome in the conservative management of early breast cancer (Abstr). International Congress of Radiology, 1989.
49. Larson D, Weinstein M, Goldberg I et al. Edema of the arm as a function of the extent of axillary surgery in patients with stage 1-11 car- cinoma of the breast treated with primary radiotherapy. Int J Radiat Oncol Biol Phys 1986; 12:1575-1582.
50. Rose MA, Henderson IC, Gelman R ef a/. Premenopausal breast cancer patients treated with conservative surgery, radiotherapy, and ad- juvant chemotherapy have a low risk of local failure. Int JRadiat Oncol Biol Phjs 1989; 17(4):711-717.
5 I . Fisher B, Redmond C, Dimitrov NV et al. A randomized clinical
1985: 11:1271-1276.
Phy.7 1988; 1416.59-663.

1438 CANCER September 15 Supplement 1990 Vol. 66
trial evaluating sequential methotrexate and fluorouracil in the treatment of patients with node-negative breast cancer who have estrogen-receptor- negative tumors. N Engl JMed 1989: 320:473-478.
52. Fisher B, Costantino J, Redmond C et ul. A randomized clinical trial evaluating tamoxifen in the treatment of patients with node-negative breast cancer who have estrogen-receptor-positive tumors. N Engl J Med
53. Levine JF, Coleman CN, Cox RS el ul. The effect ofpostoperative and primary radiation therapy on delivered dose of adjuvant cyclo- phosphamide, methotrexate, and 5-fluorouracil (CMF) chemotherapy in breast cancer. Cancer 1984; 53237-241.
54. Bonadonna G , Valagussa P, Zucali R, DelVecchio M, Veronesi U. Feasibility of adjuvant chemotherapy plus radiotherapy of operable breast cancer. In: Hams JR, Hellman S, Silen W, eds. Conservative Management of Breast Cancer. Philadelphia: JB Lippincott, 1983; 32 1- 328.
55. Danoff BF, Goodman RL, Glick JH, Haller DG, Pajak TF. The effect of adjuvant chemotherapy on cosmesis and complications in pa- tients with breast cancer treated by definitive irradiation. Int J Radzuf Oncol Biol Phys 1983; 9:1625-1630.
56. Lippman ME, Lichter AS, Edwards BK, Gorrell CR, D’Angelo T, DeMoss EV. The impact ofprimary irradiation treatment of localized
1989; 320:479-484.
breast cancer on the ability to administer systemic adjuvant chemo- therapy. J Clin Oncol 1984; 221-27.
57. Botnick LE, Come S, Rose CM el a/. Primary breast irradiation and concomitant adjuvant chemotherapy. In: Hams JR, Hellman S, Silen W, eds. Conservative Management of Breast Cancer. Philadelphia: JB Lippincott, 1983; 321-328.
58. Habibollahi F, Fentiman IS, Chaudary MA el a/. Conservation treatment of operable breast cancer (Abstr). Proc Am Soc Clin Oncol 1987; 659 .
59. Stomper PC, Recht A, Berenberg AL, Jochelson MS, Harris JR: Mammographic detection of recurrent cancer in the irradiated breast. Am J Roentgen01 1987; 148:39-43.
60. Recht A, Harris JR. Negative breast biopsies after primary radia- tion therapy: safety and accuracy (Abstr). Int J Radial Oncol Biol Phy.s 1985: lI(Suppl 1):13l.
6 1. Aberizk WJ, Silver B, Henderson IC, Cady B, Hams JR. The use of radiotherapy for treatment of isolated locoregional recurrence of breast carcinoma after mastectomy. Cancer 1986: 58:1214-1218.
62. Recht A, Schnitt SJ, Connolly JL et a/. Prognosis following local or regional recurrence after conservative surgery and radiotherapy for early stage breast carcinoma. Int J Radial Oncol Bid Phys 1989; 16:3-9.




















