
Annals of Surgery
184
August 2007, Volume 246, Issue 2,pp.165-341 Feature 165 The Value of Routine Preoperative Electrocardiography in Predicting Myocardial Infarction After Noncardiac Surgery. Wilton A. van Klei, MD, PhD; Gregory L. Bryson, MD, MSc; Homer Yang, MD; Cor J. Kalkman, MD, PhD; George A. Wells, PhD; W Scott Beattie, MD, PhD Postoperative myocardial infarction may be predicted using clinical risk factors; the additional predictive value of the preoperative electrocardiogram was assessed in 2422 patients. Right and left bundle branch blocks were associated with an increased risk of myocardial infarction but did not significantly improve upon clinical factors. Editorial 171 The Preoperative Electrocardiogram: What Is the Role in 2007? Lee A. Fleisher, MD, FACC, FAHA Feature 173 National Failure to Operate on Early Stage Pancreatic Cancer. Karl Y. Bilimoria, MD; David J. Bentrem, MD; Clifford Y. Ko, MD, MS, MSHS; Andrew K. Stewart, MA; David P. Winchester, MD; Mark S. Talamonti, MD Despite studies demonstrating improved outcomes, pessimism persists regarding the effectiveness of surgery for pancreatic cancer. Our objective was to evaluate the utilization of surgery in early stage disease and identify factors predicting failure to undergo surgery. This is the first study to characterize the striking underuse of pancreatectomy in the United States. Editorial 181 Underutilization of Surgical Resection in Patients With Localized Pancreatic Cancer. Taylor S. Riall, MD; Keith D. Lillemoe, MD Review 183 Hepatic Resection for Colorectal Metastases: Value for Risk Scoring Systems? Shaheen Zakaria, MD; John H. Donohue, MD; Florencia G. Que, MD; Michael B. Farnell, MD; Cathy D. Schleck, BS; Duane M. Ilstrup, MS; David M. Nagorney, MD Predictive models for assessing outcome in patients with metastatic colorectal cancer are imperfect. In this study, we aimed to identify predictors of outcome in these patients, develop a prognostic scoring system, and assess the general applicability of 3 current risk scoring systems with our data.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Annals of Surgery
August 2007, Volume 246, Issue 2,pp.165-341 Feature 165 The Value of Routine Preoperative Electrocardiography in
Predicting Myocardial Infarction After Noncardiac Surgery. Wilton A. van Klei, MD, PhD; Gregory L. Bryson, MD, MSc; Homer Yang, MD; Cor J. Kalkman, MD, PhD; George A. Wells, PhD; W Scott Beattie, MD, PhD Postoperative myocardial infarction may be predicted using clinical risk factors; the additional predictive value of the preoperative electrocardiogram was assessed in 2422 patients. Right and left bundle branch blocks were associated with an increased risk of myocardial infarction but did not significantly improve upon clinical factors.
Editorial 171 The Preoperative Electrocardiogram: What Is the Role in 2007?
Lee A. Fleisher, MD, FACC, FAHA
Feature 173 National Failure to Operate on Early Stage Pancreatic Cancer.
Karl Y. Bilimoria, MD; David J. Bentrem, MD; Clifford Y. Ko, MD, MS, MSHS; Andrew K. Stewart, MA; David P. Winchester, MD; Mark S. Talamonti, MD Despite studies demonstrating improved outcomes, pessimism persists regarding the effectiveness of surgery for pancreatic cancer. Our objective was to evaluate the utilization of surgery in early stage disease and identify factors predicting failure to undergo surgery. This is the first study to characterize the striking underuse of pancreatectomy in the United States.
Editorial 181 Underutilization of Surgical Resection in Patients With Localized
Pancreatic Cancer. Taylor S. Riall, MD; Keith D. Lillemoe, MD
Review 183 Hepatic Resection for Colorectal Metastases: Value for Risk
Scoring Systems? Shaheen Zakaria, MD; John H. Donohue, MD; Florencia G. Que, MD; Michael B. Farnell, MD; Cathy D. Schleck, BS; Duane M. Ilstrup, MS; David M. Nagorney, MD Predictive models for assessing outcome in patients with metastatic colorectal cancer are imperfect. In this study, we aimed to identify predictors of outcome in these patients, develop a prognostic scoring system, and assess the general applicability of 3 current risk scoring systems with our data.

Randomized Controlled Trials 192 Systemic Lidocaine Shortens Length of Hospital Stay After
Colorectal Surgery: A Double-blinded, Randomized, Placebo-controlled Trial. Susanne Herroeder, MD; Sabine Pecher, MD; Marianne E. Schönherr, MD; Grit Kaulitz; Klaus Hahnenkamp, MD; Helmut Friess, MD; Bernd W. Böttiger, MD; Harry Bauer, MD; oMarcel G. W. Dijkgraaf, PhD; Marcel E. Durieux, MD, PhD; Markus W. Hollmann, MD, PhD Stimulation of the inflammatory response plays a major role in patients' recovery and outcome after surgery. Perioperative systemic administration of lidocaine not only attenuates various pro-inflammatory mediators and accelerates return of gastrointestinal motility, but most importantly shortens length of hospital stay in patients undergoing colorectal surgery.
201 Comparison of Long-term Outcome of Laparoscopic and Conventional Nissen Fundoplication: A Prospective Randomized Study With an 11-Year Follow-up. Paulina T. P. Salminen, MD; Heikki I. Hiekkanen, MSc; Arto P. T. Rantala, MD, PhD; Jari T. Ovaska, MD, PhD This randomized study compared the long-term objective and subjective outcomes of laparoscopic and open Nissen fundoplication with an 11-year follow-up. Both approaches for the Nissen fundoplication have similar long-term subjective symptomatic outcome despite the significantly higher incidence of incisional hernias and defective fundic wraps at endoscopy in the open group.
207 Defunctioning Stoma Reduces Symptomatic Anastomotic Leakage After Low Anterior Resection of the Rectum for Cancer: A Randomized Multicenter Trial. Peter Matthiessen, MD, PhD; Olof Hallböök, MD, PhD; Jörgen Rutegård, MD, PhD; Göran Simert, MD, PhD; Rune Sjödahl, MD, PhD In this randomized multicenter trial, patients intraoperatively randomized to a defunctioning stoma (n = 116) developed symptomatic anastomotic leakage in 10% compared with 28% in those without stoma (n = 118). A defunctioning stoma is therefore recommended in low anterior resection for rectal cancer.
Original Articles 215 Are We Undertreating Rectal Cancer in the Elderly?: An
Epidemiologic Study. George J. Chang, MD; John M. Skibber, MD; Barry W. Feig, MD; Miguel Rodriguez-Bigas, MD Decreasing rectal cancer-related survival with increasing age is associated with undertreatment and understaging. Further studies addressing the reasons for this association may improve the delivery of stage-appropriate surgical care.
222 Activities of Daily Living and Quality of Life of Elderly Patients After Elective Surgery for Gastric and Colorectal Cancers. Takeshi Amemiya, MD; Koji Oda, MD; Masahiko Ando, MD; Takashi Kawamura, MD; Yuichi Kitagawa, MD; Yayoi Okawa, MD; Akihiro Yasui, MD; Hideyuki Ike, MD; Hiroshi Shimada, MD; Kojiro Kuroiwa, MD; Yuji Nimura, MD; Shinji Fukata, MD Radical surgical treatment should be considered for elderly patients 75 years old or older with gastric or colorectal cancer, as only a few patients who underwent radical surgery showed a protracted decline in ADL and most exhibited better QOL after surgery. Estimation of Physical Ability and Surgical Stress is useful for predicting postoperative declines in ADL and protracted disability in elderly patients.
229 Survival in Nonocclusive Mesenteric Ischemia: Early Diagnosis by Multidetector Row Computed Tomography and Early Treatment With Continuous Intravenous High-dose Prostaglandin E1. Akira Mitsuyoshi, MD; Kazutaka Obama, MD; Nobuhiko Shinkura, MD; Takashi Ito, MD; Masazumi Zaima, MD Nonocclusive mesenteric ischemia (NOMI) has a high mortality rate, and early diagnosis and treatment are important for improving survival. Upon suspicion of NOMI, based on criteria reported here, diagnosis using abdominal contrast multidetector row computed tomography and immediate initiation of continuous intravenous high-dose prostaglandin E1 administration may increase survival in NOMI patients.
236 Congenital Intrahepatic Bile Duct Dilatation is a Potentially Curable Disease: Long-Term Results of a Multi-institutional Study. Jean-Yves Mabrut, MD, PhD; Christian Partensky, MD, FACS; Daniel Jaeck, MD, PhD, FRCS; Elie Oussoultzoglou, MD; Jacques Baulieux, MD, FRCS; Olivier Boillot, MD, PhD; Jan Lerut, MD, PhD, FACS; Jean de Ville de Goyet, MD, PhD; Catherine Hubert, MD; Jean-Bernard Otte, MD; Maxime Audet, MD; Christian Ducerf, MD, FACS; Jean-François Gigot, MD, PhD, FRCS A retrospective study from 5 European surgical centers enrolled 33 patients with congenital intrahepatic bile duct dilatations, who had undergone liver resection or transplantation. Postoperative mortality was nil and during a median follow-up of 80 months, 87% of the patients achieved satisfactory late outcome.
246 Perioperative Mortality for Pancreatectomy: A National Perspective. James T. McPhee, MD; Joshua S. Hill, MD; Giles F. Whalen, MD; Maksim Zayaruzny, MD, MPH; Demetrius E. Litwin, MD, MBA; Mary E. Sullivan, MS; Frederick A. Anderson, PhD; Jennifer F. Tseng, MD The Nationwide Inpatient Sample was used to identify 39,463 patients who underwent pancreatectomy for neoplasm from 1998 to 2003. Perioperative mortality was analyzed by χ2 and logistic regression analysis to determine which factors are predictive of outcomes for pancreatectomy.

254 Clinical Implications of Peritoneal Cytology in Potentially Resectable Pancreatic Cancer: Positive Peritoneal Cytology May Not Confer an Adverse Prognosis. Suguru Yamada, MD; Shin Takeda, MD, PhD; Tsutomu Fujii, MD, PhD; Shuji Nomoto, MD, PhD; Naohito Kanazumi, MD, PhD; Hiroyuki Sugimoto, MD, PhD; Hideki Kasuya, MD, PhD; Yasuhiro Kodera, MD, PhD; Tetsuro Nagasaka, MD, PhD; Satoshi Morita, PhD; Akimasa Nakao, MD, PhD Correlations between peritoneal washing cytology (CY) status and clinicopathologic parameters with overall survival rates were analyzed. CY status has little predictive value for survival, and patients whose pancreatic cancer would otherwise be considered resectable should not be denied curative resection solely because they are CY+.
259 Type I Interferons in the Treatment of Pancreatic Cancer: Mechanisms of Action and Role of Related Receptors. Giovanni Vitale, MD; Casper H. J. van Eijck, MD, PhD; Peter M. van Koetsveld Ing; Joris I. Erdmann, MD; Ernst Jan M. Speel, PhD; Katy van der Wansem Ing; Diana M. Mooij; Annamaria Colao, MD, PhD; Gaetano Lombardi, MD; Ed Croze, PhD; Steven W. J. Lamberts, MD, PhD; Leo J. Hofland, PhD Treatment with IFN-β showed a potent inhibitory effect on the proliferation of pancreatic cancer cell lines. The expression, distribution, and localization of type I IFN receptor subtypes (IFNAR-1 and IFNAR-2c) seem to predict the response to IFN treatment in these cells. However, further studies will need to confirm this observation in vivo.
269 Postpancreatectomy Hemorrhage: Diagnosis and Treatment: An Analysis in 1669 Consecutive Pancreatic Resections. Emre F. Yekebas, MD; Lars Wolfram, MD; Guellue Cataldegirmen, MD; Christian R. Habermann, MD; Dean Bogoevski, MD; Alexandra M. Koenig, MD; Jussuf Kaifi, MD; Paulus G. Schurr, MD; Michael Bubenheim, MD; Claus Nolte-Ernsting, MD; Gerhard Adam, MD; Jakob R. Izbicki, MD The armory of interventional options for treatment of postpancreatectomy hemorrhage encompasses endoscopy, angiography, or relaparotomy. A standardized therapeutic algorithm has to consider an individual risk profile. The risk of lethal course is increased when hemorrhage occurs after the sixth postoperative day, especially when it is associated with pancreatic fistula.
281 Amylase Value in Drains After Pancreatic Resection as Predictive Factor of Postoperative Pancreatic Fistula: Results of a Prospective Study in 137 Patients. Enrico Molinari, MD; Claudio Bassi, Prof.; Roberto Salvia, MD, PhD; Giovanni Butturini, MD, PhD; Stefano Crippa, MD; Giorgio Talamini, MD; Massimo Falconi, MD; Paolo Pederzoli, Prof. The range of postoperative fistula after pancreatic resections is reported from 2% to 30% of cases and in the literature there are few studies that investigate the predictive role of different risks factors in the development of pancreatic fistula, including the amylase value in drains. The authors show that the drain's amylase value on postoperative day 1 is the only significant predictive factor of pancreatic fistula development.

288 Feasibility of Navigated Resection of Liver Tumors Using Multiplanar Visualization of Intraoperative 3-dimensional Ultrasound Data. Siegfried Beller, MD; Michael Hünerbein, MD; Sebastian Eulenstein, PhD; Thomas Lange, PhD; Peter M. Schlag, MD, PhD, FSSO Accuracy of a 3-dimensional ultrasound-based navigation system was evaluated in a tumor model first. Clinical application was feasible in 52 of 54 patients and provided complete anatomic orientation and accurate position control of surgical instruments. Sufficient visualization was obtained with two orthogonal section planes. It enables accurate navigation of liver resections.
295 The Impact of Margins on Outcome After Hepatic Resection for Colorectal Metastasis. Chandrakanth Are, MD, FRCS; Mithat Gonen, PhD; Kathleen Zazzali, DO; Ronald P. DeMatteo, MD, FACS; William R. Jarnagin, MD, FACS; Yuman Fong, MD, FACS; Leslie H. Blumgart, MD, FACS, FRCS; Michael D'Angelica, MD, FACS The prognostic significance of margin width on long-term survival after hepatic resection for colorectal metastasis is unclear. The results of this study demonstrate that a >1 cm margin is an independent predictor of improved outcome when analyzed in the context of other well-known prognostic factors.
301 Impact of Graft Type on Outcome in Pediatric Liver Transplantation: A Report From Studies of Pediatric Liver Transplantation (SPLIT). Ivan R. Diamond, MD; Annie Fecteau, MD; J Michael Millis, MD; Julian E. Losanoff, MD; Vicky Ng, MD; Ravinder Anand, PhD; Changhong Song, PhD; the SPLIT Research Group Technical variant liver transplantation comprising reduced, split, and live-donor grafts evolved to address the need for size appropriate organs for pediatric liver recipients. This study will examine the outcome and morbidity of the technical variant techniques relative to whole organ transplants in the Studies of Pediatric Liver Transplantation (SPLIT) database.
311 Calprotectin: A Novel Noninvasive Marker for Intestinal Allograft Monitoring. Debra Sudan, MD; Luciano Vargas, MD; Yimin Sun, MD; Lisette Bok; Gerard Dijkstra, MD; Alan Langnas, DO This pilot study of stool calprotectin levels shows tremendous promise as a noninvasive screening test for the intestinal allograft. No treated rejection episode was missed, and no viral enteritis had an elevated level. False-positive elevations were rare, but confirmatory biopsy would exclude unnecessary addition of immunosuppression in these cases.
316 Mediastinal Carcinosis Involving the Esophagus in Breast Cancer: The "Breast-Esophagus" Syndrome: Report on 25 Cases and Guidelines for Diagnosis and Treatment. Sabrina Rampado, MD; Alberto Ruol, MD, FACS; Maria Guido, MD; Giovanni Zaninotto, MD, FACS; Giorgio Battaglia, MD; Mario Costantini, MD; Giuseppe Portale, MD; Alessandra Amico, MD; Ermanno Ancona, MD, FACS Esophageal involvement from breast cancer is usually part of a mediastinal carcinosis. Patients present with worsening dysphagia. Diagnosis and treatment are both challenging. Given the high related risk of perforation from endoscopic procedures (dilations/prostheses used in the past decades), the treatments of choice are currently hormone therapy or chemotherapy/radiotherapy.
323 Predictors and Outcome of Gastrointestinal Complications in Patients Undergoing Cardiac Surgery. Farzan Filsoufi, MD; Parwis B. Rahmanian, MD; Javier G. Castillo, MD; Corey Scurlock, MD; Peter E. Legnani, MD; David H. Adams, MD We determined the incidence and independent predictors of gastrointestinal complications following cardiac surgery in a recent era and demonstrated a decrease of these complications during the study period. The key to a lower incidence lies in systematic application of preventive measures and advances in intraoperative management.
330 Treatment of Palmar Hyperhidrosis: T4 Level Compared With T3 and T2. Yu-Tang Chang, MD; Hsien-Pin Li, MD; Jui-Ying Lee, MD; Pei-Jung Lin, MD; Chien-Chih Lin, MD; Eing-Long Kao, MD; Shah-Hwa Chou, MD; Meei-Feng Huang, RN The aim of this study was to analyze and compare the long-term outcome of palmar hyperhidrosis treated by endoscopic thoracoscopic sympathectomy at 3 different levels. T4 sympathectomy preserved the purpose in solving excessive palmar sweating and simultaneously caused the least compensatory sweating.
Book Reviews 337 Multiorgan Resections for Cancer, Advanced Surgical Techniques.
Neal Wilkinson, MD
337 Current Therapy in Colon and Rectal Surgery, 2nd ed. Daniel L. Feingold, MD
Letters to the Editor 338 Hormone Receptor Status as a Prognostic Factor in Breast Cancer
Patients With Hepatic Metastases Treated by Liver Resection. Tugrul Purnak, MD; Kadri Altundag, MD
338 Hormone Receptor Status as a Prognostic Factor in Breast Cancer Patients With Hepatic Metastases Treated by Liver Resection. René Adam, MD, PhD; Thomas Aloia, MD
338 Impact of Laparoscopic Resection for Colorectal Cancer on Operative Outcomes and Survival. Brian K. P. Goh, MBBS, MRCS, MMed

339 Impact of Laparoscopic Resection for Colorectal Cancer on Operative Outcomes and Survival. Wai Lun LAW, MS, FRCS (Edin.), FACS
340 Steatosis as a Risk Factor in Liver Surgery. Eddie K. Abdalla, MD; Jean-Nicolas Vauthey, MD
341 Steatosis as a Risk Factor in Liver Surgery. Thomas M. van Gulik, MD; Reeta Vetelaïnen, MD

FEATURE
The Value of Routine Preoperative Electrocardiography inPredicting Myocardial Infarction After Noncardiac Surgery
Wilton A. van Klei, MD, PhD,† Gregory L. Bryson, MD, MSc,* Homer Yang, MD,*Cor J. Kalkman, MD, PhD,† George A. Wells, PhD,‡ and W. Scott Beattie, MD, PhD§
Objective: The added value of a preoperative electrocardiogram(ECG) in the prediction of postoperative myocardial infarction(POMI) and death was compared with clinical risk factors identifiedfrom the patient’s history.Summary of Background Data: An ECG is frequently performedbefore surgery to screen for asymptomatic coronary artery disease.However, the value of ECG abnormalities to predict POMI has beenquestioned.Methods: The study included 2967 noncardiac surgery patients �50years of age from 2 university hospitals, who were expected to stayin the hospital for �24 hours. All data were obtained from electronicrecord-keeping systems. Patient history and ECG abnormalitieswere considered as potential predictors. Multivariate logistic regres-sion analysis was used to obtain the independent predictors of POMIand all-cause in-hospital mortality. The area under the receiveroperating characteristic curve (ROC area) was estimated to evaluatethe ability of different models to discriminate between patients withand without the outcome.Results: A preoperative ECG was available in 2422 patients (80%)and 1087 (45%) of the ECGs showed at least one abnormality. TheROC area of the model that included the independent predictors ofPOMI obtained from patient history, ie, ischemic heart disease andhigh-risk surgery, was 0.80. ECG abnormalities that were associatedwith POMI were a right and a left bundle branch block. After addingthese abnormalities in the regression model, the ROC area remained0.80. Similar results were found for all-cause mortality.Conclusions: Bundle branch blocks identified on the preoperativeECG were related to POMI and death but did not improve predictionbeyond risk factors identified on patient history.
(Ann Surg 2007;246: 165–170)
All patients scheduled for surgery are evaluated by thesurgeon and anesthesiologist to identify conditions that
predispose the patient to adverse perioperative outcomes.1–4
Postoperative cardiovascular morbidity and mortality are ac-curately predicted by variables determined from the patienthistory (eg, the Revised Cardiac Risk Index5), yet additionallaboratory testing is frequently ordered as a means of iden-tifying the asymptomatic patient at risk.1–4
Electrocardiograms (ECGs) are frequently performedin patients aged over 50 or 60 years to screen for asymptom-atic coronary artery disease.1–4 The predictive value of ECGabnormalities has been questioned, and ECG results appear toexert weak influence on clinician behavior.3,4,6–8 Recentstudies suggest that abnormalities detected on the preopera-tive ECG in patients undergoing higher risk surgery maypredict postoperative or long-term cardiovascular death.9,10 Itis unclear if preoperative ECG abnormalities improve uponpatient history in identifying the patient at risk for adversepostoperative outcomes, like myocardial infarction.
The purpose of this study was to estimate the value ofa preoperative ECG in addition to patient history in theprediction of myocardial infarction and death from all causesduring the postoperative hospital stay. Patients from 2 uni-versity hospitals from different countries were included toincrease the generalizability of the results of this study.
METHODS
PatientsThe study included noncardiac surgery patients aged
over 50 years who were expected to stay in the hospital formore than 24 hours. Patients scheduled for lung and livertransplantations were excluded. Patients were operated onbetween February 2002 and August 2003 at the UniversityMedical Center Utrecht (UMCU), The Netherlands, and be-tween March 2003 and July 2004 at the University HealthNetwork Toronto (UHNT), Canada.
UMCU DataData on patients from the UMCU were prospectively
collected during a previous study including 4540 adult pa-tients, which was approved by the hospital ethics board.11
Data on preoperative history, physical examination, and ad-ditional testing (including preoperative ECG results) werecollected in an electronic record-keeping system. An ECGwas performed in all patients over 60 years of age or when
From the *Ottawa Hospital, Civic Site, Department of Anesthesiology,Ottawa, Ontario, Canada; †University Medical Center Utrecht, DeptPerioperative Care and Emergency Medicine, Utrecht, The Netherlands;‡University of Ottawa, Department of Epidemiology, Ottawa, Ontario,Canada; and §University Health Network Toronto (Toronto GeneralHospital), Department of Anesthesia, Toronto, Ontario, Canada.
Supported by a personal grant (to W.A.vK.) for a sabbatical leave from“Catharijne stichting,” a non-profit organization affiliated to the UMCUtrecht supporting young physicians.
Reprints: Wilton A van Klei, MD, PhD, Department of Anesthesiology, Box249C, Ottawa Hospital, Civic Site, 1053 Carling Ave., Ottawa ON K1Y4E9. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0165DOI: 10.1097/01.sla.0000261737.62514.63
Annals of Surgery • Volume 246, Number 2, August 2007 165

clinically indicated. Postoperative outcome data on generalsurgery and vascular surgery patients were stored in anelectronic record keeping system used by the general andvascular surgeons. All laboratory test results (coded with timeof the test) were stored in a laboratory data warehouse. Apostoperative Troponin I was ordered only when clinicallyindicated. Data on in-hospital death were stored in the hos-pital information system database. After linking these data-bases using unique hospital identification numbers, the datadownload included 766 patients admitted at the general andvascular surgery wards.
UHNT DataFollowing approval by the institutional research ethics
board, preoperative history data on all patients undergoingsurgery at the UHNT were prospectively stored in a clinicalregistry system. An ECG was normally done in patients over50 years of age. Preoperative ECG results were archived in aCardiology database. All laboratory test results (coded withtime of the test) were stored in a data warehouse along withICD 9 and 10 codes. In all patients identified as high riskbefore surgery (Revised Cardiac Risk Index5 �2), a TroponinI was drawn in the Post Anesthetic Care Unit. This was alsodone in patients noted to have intraoperative hypotensionand/or ST changes. Thereafter, Troponin I was ordered whenclinically indicated. Postoperative outcome data were col-lected in an Acute Pain Service database. Data on in-hospitaldeath were stored in the hospital information system data-base. Linking all these diverse databases using the patient’sunique hospital identification resulted in a comprehensivereport of each patient’s in-hospital visit. The download of thedata comprised in total 2201 patients from different surgicalspecialties.
Thus, the final sample for the present study included2967 patients, aged 50 years or older, who underwent non-cardiac surgery in 2 different hospitals.
PredictorsPatient history data that were considered as potential
predictors for postoperative myocardial infarction (POMI)included gender, age, the Revised Cardiac Risk Index (RCRI)5
and the single predictors that are included in this risk index,ie, scheduled for high-risk surgery, a history of ischemic heartdisease (IHD), a history of congestive heart failure (CHF), ahistory of chronic renal failure (CRF), a history of cerebro-vascular accident (CVA) or a history of insulin dependentdiabetes. Definitions of these conditions were similar to thoseused by Lee et al5 The RCRI groups patients into 4 classes,according to the existence of 0, 1, 2, or 3 or more predictors.
The computerized interpretation of the ECG was re-viewed and verified by a cardiologist before entry into thepatient’s electronic record. ECG abnormalities were catego-rized as: normal ECG, right bundle branch block (RBBB),left bundle branch block (LBBB), any ST-T changes, isch-emia specific ST-T changes, old myocardial infarction (Qwave), atrial fibrillation, and left ventricular hypertrophy.
OutcomeThe primary outcome was POMI, which was defined as
a maximal Troponin I greater than 0.7 ng/mL and associated
with at least one of the following: new Q waves at the ECG,persistent ST changes at the ECG, a new regional wall motionabnormality using echocardiography or clinical symptoms(chest pain or shortness of breath). The diagnosis of MI wasconfirmed independently. Death from all causes during hos-pital admission was considered as a secondary outcome.
AnalysisSPSS for Windows release 12.0.1 (SPSS Inc., Chicago,
IL) was used for the analysis. Odds ratios (OR) were chosento describe the relationship between predictors and outcomes.OR are equivalent to the more common relative risk ratiowhen the occurrence of outcome is less than 5%. A univariateOR with 95% confidence interval (95% CI) and a P value wascalculated for each predictor using univariate logistic regres-sion analysis. Any OR with a P value of �0.10 was consid-ered as a potential independent predictor.12 A similar ap-proach was followed to estimate the incidences of outcomesfor the different ECG abnormalities and to estimate theunivariate associations with outcome.
The incidences of POMI and all-cause mortality wereestimated for each of the 4 categories of the RCRI as well asfor the single predictors included in the RCRI and for age andgender. Logistic regression models predicting POMI werefitted using RCRI as the only predictor (Model 1). Subse-quently, backward stepwise multivariable logistic regressionmodeling was used to quantify the predictive ability of eachof the 6 single predictors that are included in the RCRI(model 2). Gender and age (included as a continuous vari-able) were added to model 2 and their independent value inthe prediction of POMI was quantified (model 3). Finally, toquantify the added value of the ECG, all ECG abnormalitiesthat were found to be significantly associated with POMI inthe univariable analysis were entered into model 3 and againbackward stepwise regression was used to found the inde-pendent associations with POMI (model 4). As an ECG wasnot available in all patients, we did a complete case analysisin this final model.
A similar multistep modeling approach was used toidentify predictors of all-cause mortality. Model 2 includedCRF and CHF in addition to IHD and high-risk surgery. Malegender and age were added in model 3. ECG abnormalitieswere added in model 4.
The area under the receiver operating characteristiccurve (ROC area) with 95% CI was estimated to evaluate theability of the models to discriminate between patients with andwithout outcome.12–15 The reliability (calibration or goodness offit) of all models was quantified using the Hosmer & Lemeshowtest.15
RESULTSThe baseline characteristics of the included patients
from both hospitals differed with respect to gender, age, andtype of surgery (Table 1). Patients from the UHNT were morefrequently scheduled for high-risk surgery, but UMCU pa-tients were more frequently scheduled for vascular surgery,resulting in significantly more patients with IHD and CVAfrom the UMCU (Table 1). As a result of the different agethreshold for performing a routine ECG before surgery, an
van Klei et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins166

ECG was available more frequently at the UHNT (89% vs.61% at the UMCU). The proportion of ECGs with abnormal-ities did not differ between the 2 hospitals. POMI wassignificantly more common at UHNT (2.9%) when comparedwith UMCU (1.2%). This may reflect the use of routinepostoperative troponin surveillance at UHNT in patients withan RCRI score �2.
Univariate AnalysisThe likelihood of POMI increased with increasing
RCRI, with incidences of 0.3%, 1.8%, 4.4%, and 11.4% for
the RCRI class I, II, III, and IV, respectively. With RCRIgroup I as a reference, the OR for suffering a POMI for groupII, III, and IV were 6 (95% CI, 2–19), 14 (5–48), and 40(12–135), respectively. POMI was further associated withage, male gender, high-risk surgery, a history of IHD, and ahistory of CVA (Table 2). Postoperative death had the sameassociations except for a history of CVA but was furtherassociated with a history of CHF and CRF (Table 2). BothPOMI and postoperative death were significantly associatedwith any ECG abnormalities in univariate analysis (Table 3).POMI was associated with RBBB, LBBB, and Q waves;death was related to RBBB, LBBB, and atrial fibrillation.
Multivariate AnalysisOf the 6 predictors included in the RCRI, only IHD and
high-risk surgery were significantly associated with POMI inthe multivariate analysis (Table 4, models 1 and 2). The ROCarea of the model that included these 2 predictors only wasslightly higher than the model that included the RCRI as awhole (0.80 compared with 0.78). After entering age andgender into model 2, males appeared to be at higher risk ofPOMI (OR, 2.1; 95% CI, 1.1–3.7), but the ROC area re-mained 0.80 (Table 4, model 3). ECG abnormalities that werefound to be associated with POMI in the univariable analysiswere entered into model 3. Q waves were not associated withPOMI. Thus, the final model (model 4) included high-risksurgery, history of IHD, male gender, LBBB, and RBBB(Table 4). The model’s ROC area remained 0.80 (95% CI,0.74–0.86). For all these models, the Hosmer & Lemeshowtest had P values of �0.50, indicating that predicted andobserved outcome rates were highly comparable.
A similar approach was followed to predict the occur-rence of death during admission. The ROC area of the finalmodel to predict death (Table 5) was 0.69 (95% CI, 0.62–0.75) and the P value of the Hosmer & Lemeshow test was0.57. When LBBB was excluded the ROC area remained 0.69(95% CI, 0.64–0.76).
DISCUSSIONClinical risk factors identified on patient history accu-
rately predicted postoperative myocardial infarction (ROCarea of 0.80). Only 2 risk factors seem to be associated withPOMI, ie, a history of ischemic heart disease and high-risksurgery (defined as intrathoracic, intra-abdominal or suprain-guinal vascular procedures). Although male gender and theexistence of bundle branch blocks at the preoperative ECGwere also related to POMI, they did not provide addedpredictive value. Similarly, ECG abnormalities failed to pro-vide added value in the prediction of all-cause in-hospitalmortality.
Clinical ImplicationsThe present results confirm the importance of clinical
risk factors in the prediction of adverse postoperative events.Similar findings have been reported by others.5,9 It should benoted, however, that of the 6 variables in the RCRI, only ahistory of IHD and a high-risk surgical procedure were requiredto accurately predict POMI, suggesting that the identification ofpatients at high risk for POMI can be simplified. Although Q
TABLE 1. Baseline Characteristics
Toronto(n � 2201)
Utrecht(n � 766)
Total(n � 2967) P*
Male gender 1260 (57.2) 401 (52.3) 1661 (56.0) 0.02
Age (yr) �mean (SD)� 65.2 (9.2) 64.2 (9.1) 64.9 (9.2) 0.02
Surgery
General surgery 1132 (51.5) 515 (67.2) 1647 (55.5) �0.01
Vascular surgery 301 (13.7) 190 (24.8) 491 (16.6) �0.01
Other surgery 768 (34.9) 61 (8.0) 827 (27.9) �0.01
Revised Cardiac RiskIndex† variables
High-risk surgery‡ 1251 (56.8) 345 (45.0) 1596 (53.8) �0.01
Ischemic heartdisease
200 (9.1) 113 (14.8) 313 (10.5) �0.01
Congestive heartfailure
36 (1.6) 17 (2.2) 53 (1.8) 0.29
Cerebrovascularaccident
21 (1.0) 101 (13.2) 122 (4.1) �0.01
Chronic renal failure 60 (2.7) 21 (2.7) 81 (2.7) 0.98
Insulin-dependentdiabetes
115 (5.2) 48 (6.3) 163 (5.5) 0.28
Revised Cardiac RiskIndex†
�0.01
I 622 (28.3) 317 (41.4) 939 (31.6)
II 973 (44.2) 391 (38.0) 1264 (42.6)
III 461 (20.9) 126 (16.4) 587 (19.8)
IV 145 (6.6) 32 (4.2) 177 (6.0)
ECG available 1952 (88.7) 470 (61.4) 2422 (81.6) �0.01
Normal ECG 1063 (54.5) 272 (57.9) 1335 (55.1) 0.18
Atrial fibrillation 78 (4.0) 14 (3.0) 92 (3.8) 0.29
Left ventricularhypertrophy
167 (8.6) 34 (7.2) 201 (8.3) 0.35
Right bundle branchblock
119 (6.1) 27 (5.7) 146 (5.0) 0.77
Left bundle branchblock
30 (1.5) 13 (2.8) 43 (1.8) 0.07
Any ST-T changes 275 (14.1) 74 (15.7) 349 (14.4) 0.36
Old myocardialinfarction
162 (8.3) 39 (8.2) 201 (8.3) 0.90
Postoperativemyocardialinfarction
63 (2.9) 9 (1.2) 72 (2.3) 0.01
Death duringadmission
56 (2.5) 21 (2.7) 77 (2.5) 0.85
Values are no. (%) unless otherwise specified.*Toronto data compared with Utrecht data.†As published by Lee et al.5‡Intrathoracic or intra-abdominal or suprainguinal vascular surgery, according to
the Revised Cardiac Risk Index.5
Annals of Surgery • Volume 246, Number 2, August 2007 Predictive Value of Preoperative ECG
© 2007 Lippincott Williams & Wilkins 167

TABLE 2. Univariate Associations of Patient Characteristics to Postoperative Myocardial Infarction (n � 2967) and DeathDuring Admission (n � 2908, as survival data on 59 cases �2%� were missing)
POMI(n � 72)
No POMI(n � 2895)
Odds Ratio(95% CI) P
Death(n � 77)
Alive(n � 2831)
Odds Ratio(95% CI) P
Age (yr) �mean (SD)� 68.4 (9.8) 64.8 (9.2) 3.6 (1.4–5.7)* �0.01 68.8 (9.9) 64.8 (9.1) 4.0 (1.9–6.1)* �0.01
Male gender 57 (79.2) 1604 (55.4) 3.1 (1.7–5.4) �0.01 54 (70.1) 1581 (55.8) 1.9 (1.1–3.0) 0.01
High-risk surgery† 53 (73.6) 1543 (53.3) 2.4 (1.4–4.1) �0.01 59 (76.6) 1500 (53.0) 2.9 (1.7–5.0) �0.01
Ischemic heart disease 38 (52.8) 275 (9.5) 11 (6.6–17) �0.01 18 (23.4) 294 (10.4) 2.6 (1.5–4.5) �0.01
Congestive heartfailure
3 (4.2) 50 (1.7) 2.5 (0.8–8.1) 0.12 10 (13.0) 42 (1.5) 9.9 (4.8–21) �0.01
Cerebrovascularaccident
7 (9.7) 115 (4.0) 2.6 (1.2–5.8) 0.02 4 (5.2) 118 (4.2) 1.3 (0.5–3.5) 0.66
Chronic renal failure 4 (5.6) 77 (2.7) 2.2 (0.8–6.1) 0.14 8 (10.4) 73 (2.6) 4.4 (2.0–9.4) �0.01
Insulin-dependentdiabetes
3 (4.2) 160 (5.5) 0.7 (0.2–2.4) 0.62 2 (2.6) 161 (5.7) 0.4 (0.1–1.8) 0.25
Values are numbers (column %) unless otherwise specified. POMI, postoperative myocardial infarction.*Mean difference in years.†Intrathoracic or intra-abdominal or suprainguinal vascular surgery, according to the Revised Cardiac Risk Index.8
TABLE 3. Univariate Associations of Electrocardiogram Characteristics to Postoperative Myocardial Infarction (n � 2422) andDeath During Admission (n � 2416)
POMI(n � 69)
No POMI(n � 2353)
Odds Ratio(95% CI) P
Death(n � 71)
Alive(n � 2345)
Odds Ratio(95% CI) P
Normal ECG 24 (34.8) 1311 (55.7) 0.4 (0.3–0.7) �0.01 23 (32.4) 1308 (55.8) 0.4 (0.2–0.6) �0.01
Right bundle branch block 9 (13.0) 137 (5.8) 2.4 (1.2–5.0) 0.01 8 (11.3) 138 (5.9) 2.0 (1.0–4.3) 0.06
Left bundle branch block 4 (5.8) 39 (1.7) 3.7 (1.3–11) 0.01 5 (7.0) 38 (1.6) 4.6 (1.8–12) �0.01
Old myocardial infarction 14 (20.3) 187 (8.0) 2.9 (1.6–5.4) �0.01 9 (13.0) 192 (8.2) 1.7 (0.8–3.4) 0.15
Atrial fibrillation 4 (5.8) 88 (3.8) 1.6 (0.6–4.4) 0.38 7 (10.3) 85 (3.6) 3.0 (1.4–6.8) �0.01
Left ventricular hypertrophy 6 (8.7) 195 (8.3) 1.1 (0.5–2.5) 0.90 7 (9.9) 194 (8.3) 1.2 (0.5–2.7) 0.63
Ischemia specific STT changes 3 (4.3) 63 (2.7) 1.7 (0.5–5.4) 0.40 5 (7.0) 61 (2.6) 2.8 (1.1–7.3) 0.02
Any STT changes 11 (15.9) 338 (14.4) 1.1 (0.6–2.2) 0.71 14 (19.7) 333 (14.2) 1.5 (0.8–2.7) 0.19
Values are numbers (column %).POMI indicates postoperative myocardial infarction.
TABLE 4. Multivariate Associations With Postoperative Myocardial Infarction
Odds Ratio (95% CI) P ROC Area (95% CI)
Model 1 (n � 2967) 0.780 (0.730–0.829)
RCRI I Reference
RCRI II 5.8 (1.7–19) �0.01
RCRI III 14 (4.4–48) �0.01
RCRI IV 40 (12–135) �0.01
Model 2 (n � 2967) 0.796 (0.742–0.850)
High-risk surgery* 2.2 (1.2–3.7) �0.01
Ischemic heart disease 10 (6.2–16) �0.01
Model 3 (n � 2967) 0.798 (0.744–0.852)
High-risk surgery* 2.0 (1.2–3.4) 0.01
Ischemic heart disease 9.1 (5.6–15) �0.01
Male gender 2.1 (1.1–3.7) 0.02
Model 4 (n � 2422) 0.800 (0.742–0.857)
High-risk surgery* 1.8 (1.0–3.1) 0.04
Ischemic heart disease 8.8 (5.3–15) �0.01
Male gender 1.9 (1.0–3.4) 0.04
Right bundle branch block 2.1 (1.0–4.5) 0.06
Left bundle branch block 3.1 (1.0–9.9) 0.05
*Intrathoracic or intra-abdominal or suprainguinal vascular surgery, according to the Revised Cardiac Risk Index.5
van Klei et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins168

waves on the preoperative ECG and conduction defects likeRBBB and LBBB were associated with POMI, they revealed noadditional predictive value.
One might therefore reasonably question the utility of apreoperative ECG even among those patients at increased riskof cardiac complications. It can be argued that a preoperativeECG is still of value as a reference when ischemic events ordysrhythmias occur after surgery. Interval changes in theECG are indeed still included among diagnostic criteria formyocardial infarction in the nonperioperative setting.16 How-ever, with a POMI incidence of 2.3% in the present study, 43preoperative ECGs (100/2.3) have to be made to diagnoseone case of POMI. Furthermore, the use of sensitive bio-chemical markers of myocardial injury, such as troponin Tand I, have decreased reliance on ECG abnormalities in dailypractice and clinical research, especially in the perioperativesetting where myocardial infarctions are often limited insize.16,17 For example, the ongoing POISE trial relies ontroponin assay primarily and uses ECG abnormalities assecondary criteria.18 ECG monitoring during anesthesia canbe used as a reference for any new rhythm abnormalities thatmay occur after surgery.
Other StudiesThe predictive value of a routine ECG before surgery
has been questioned before.3,6–9 Landesberg et al noted STsegment depression on the preoperative ECG in 98 of 405(24%) patients awaiting vascular surgery.19 Nineteen patients(4.7%) suffered postoperative cardiac complications. Patientswith ST segment depression were at increased risk (OR, 4.7;95% CI, 1.2–12.1) of cardiac events. Jeger et al also studiedthe prognostic value of a routine ECG in 172 noncardiacsurgery patients with known or highly suspected coronaryartery disease.10 ST segment abnormalities were present in38% of those studied. Thirty-one major adverse cardiacevents (18%) and 40 (23%) deaths from all causes occurred inthe 2 years following surgery. Multivariate analysis identifiedST segment depression as an independent predictor of bothcardiac events and all-cause mortality. The findings of thepresent study contrast these trials, probably because data inthe present study were collected from clinical databases in arange of high- and lower-risk patients and procedures ratherthan from prospective research on high-risk vascular surgerypatients only. Event rates in the present study (POMI, 2.3%;all-cause mortality, 2.5%), therefore, were substantially lower
than that reported by Jeger and Landesberg.10,19 Finally,these latter studies did not assess if ECG abnormalitiesoffered any improvement in predicting events above clinicalrisk factors.
The present results are comparable to those of Liu et alwho noted abnormalities on 75% of preoperative ECGs in acohort of 513 geriatric patients undergoing a variety ofsurgical procedures.8 Nineteen deaths (3.7%) and 9 (1.8%)nonfatal myocardial infarctions were reported prior to hospi-tal discharge. ECG abnormalities including ST segment de-pression, bundle branch blocks, and Q waves were not foundto be independent predictors of postoperative events. Instead,physical status and a history of congestive heart failure werethe only factors associated with poor outcome. Noordzij et alrecently evaluated the added value of preoperative ECGabnormalities in the prediction of postoperative cardiovascu-lar death.9 They used a hospital administrative database toinclude 28,457 (from a total cohort of 108,593 procedures)noncardiac surgery procedures for which ECG results wereavailable. A variety of ECG abnormalities were present in25% of patients and were independently associated withpostoperative cardiac events. ECG abnormalities slightly im-proved the predictive value of the RCRI, increasing theC-index from 0.72 to 0.78. They reported that the preopera-tive ECG did not predict postoperative events in those pa-tients undergoing low- to intermediate-risk surgery. The find-ings of these latter 2 studies support the present study insuggesting that preoperative ECGs add little benefit in pa-tients with a broader spectrum of patient and surgical riskfactors.
LimitationsFirst, patients from the 2 hospitals differed significantly
with respect to baseline characteristics (Table 1). However,this study did not aim to compare any effect of a newtreatment but aimed to evaluate the additional value of acertain test (ECG) upon information that should be availableroutinely (patient history). Therefore, it may be an advantageto include patients who differ in baseline characteristics toincrease generalizability of the study results to different typesof hospitals in different countries. Second, outcome assess-ments were driven by clinical care rather than by a prospec-tive research protocol suggesting that events may have beenunderestimated. Lastly, as this was a retrospective study, wewere unable to assess the impact of the ECG results onclinical patient management. Isolating the impact of an ECGfrom the remainder of the clinical assessment would presenta formidable research design challenge. At a minimum, alarge-sized prospective trial with a randomized assignment to“ECG” or “no ECG” arms would be required. The results ofthe current study suggest that ECG results were not anessential part of the preoperative evaluation as 11% of sub-jects in whom an ECG was indicated proceeded directly tosurgery without an ECG on record. Failure to change man-agement based on preoperative laboratory testing has beenwell described in a systematic review.6
TABLE 5. Multivariate Associations With Death DuringAdmission (n � 2416)
Odds Ratio (95% CI) P
High-risk surgery* 2.5 (1.4–4.4) �0.01
Congestive heart failure 3 (2.7–15) �0.01
Chronic renal failure 3.2 (1.4–7.5) �0.01
Ischemic heart disease 1.7 (0.9–3.1) 0.08
Age (per year) 1.03 (0.99–1.06) 0.06
Left bundle branch block 3.5 (1.3–10) 0.02
*Intrathoracic or intra-abdominal or suprainguinal vascular surgery, according tothe Revised Cardiac Risk Index.5
Annals of Surgery • Volume 246, Number 2, August 2007 Predictive Value of Preoperative ECG
© 2007 Lippincott Williams & Wilkins 169

CONCLUSIONPostoperative myocardial infarction is related to a his-
tory of ischemic heart disease and to type of surgery. Al-though the existence of bundle branch blocks at the preoper-ative ECG was related to POMI and death during hospitaladmission, they did not provide added predictive value. It istherefore reasonable to question the utility of a preoperativeECG for screening asymptomatic individuals undergoing avariety of surgical procedures. Clinical risk factors shouldform the basis of risk assessment and prediction.
REFERENCES1. Fischer SP. Development and effectiveness of an anesthesia preoperative
evaluation clinic in a teaching hospital. Anesthesiology. 1996;85:196–206.
2. van Klei WA, Moons KGM, Rutten CLG, et al. The effect of outpatientpreoperative evaluation of hospital inpatients on cancellation of surgeryand length of hospital stay. Anesth Analg. 2002;94:644–649.
3. van Klei WA, Grobbee DE, Rutten CLG, et al. The role of history andphysical examination in preoperative evaluation: much “opinion” and“little” evidence. Eur J Anesth. 2003;20:612–618.
4. Roizen MF. Preoperative evaluation. In: Miller RD, ed. Anaesthesia.New York: Churchill Livingstone; 2000:824–883.
5. Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospec-tive validation of a simple index for prediction of cardiac risk of majornoncardiac surgery. Circulation. 1999;100:1043–1049.
6. Munro J, Booth A, Nicholl J. Routine preoperative testing: a systematicreview of the evidence. Health Technol Assess. 1997;1:1–63.
7. Schein OD, Katz J. The value of routine preoperative testing beforecataract surgery. N Engl J Med. 2000;342:168–175.
8. Liu LL, Dzankic S, Leung JM. Preoperative electrocardiogram abnor-
malities do not predict postoperative cardiac complications in geriatricsurgical patients. J Am Geriatr Soc. 2002;50:1186–1191.
9. Noordzij PG, Boersma E, Bax JJ, et al. Prognostic value of routinepreoperative electrocardiography in patients undergoing noncardiac sur-gery. Am J Cardiol. 2006;97:1103–1106.
10. Jeger RV, Probst C, Arsenic R, et al. Long-term prognostic value of thepreoperative 12-lead electrocardiogram before major noncardiac surgeryin coronary artery disease. Am Heart J. 2006;151:508–513.
11. van Klei WA, Hennis PJ, Moen J, et al. The accuracy of trained nursesin pre-operative health assessment: results of the OPEN study. Anaes-thesia. 2004;59:971–978.
12. Harrell FE, Lee KL, Mark DB. Multivariable prognostic models: issuesin developing models, evaluating assumptions and adequacy, and mea-suring and reducing errors. Stat Med. 1996;15:361–387.
13. Hanley JA, McNeil BJ. The meaning and use of the area under a receiveroperating characteristic (ROC) curve. Radiology. 1982;143:29–36.
14. Hanley JA, McNeil BJ. A method of comparing the areas under receiveroperating characteristic curves derived from the same cases. Radiology.1983;148:839–43.
15. Hosmer DW, Lemeshow S. Applied Logistic Regression. New York: J.Wiley and Sons; 1989:140–145.
16. Joint ECC/ACC Committee. Myocardial infarction redefined: a consen-sus document of the Joint European Society of Cardiology/AmericanCollege of Cardiology Committee for the Redefinition of MyocardialInfarction. J Am Coll Cardiol. 2000;36:959–969.
17. Devereaux PJ, Goldman L, Yusuf S, et al. Surveillance and preventionof major perioperative ischemic cardiac events in patients undergoingnoncardiac surgery: a review. CMAJ. 2005;173:779–788.
18. Canadian Cardiovascular Collaboration MUHC. Perioperative IschemiaEvaluation (POISE) study. www.sati.org ar/newstyle/protocols/poise_sppdf. 2004.
19. Landesberg G, Einav S, Christopherson R, et al. Perioperative ischemia andcardiac complications in major vascular surgery: importance of the preop-erative twelve-lead electrocardiogram. J Vasc Surg. 1997;26:570–578.
van Klei et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins170

EDITORIAL
The Preoperative ElectrocardiogramWhat Is the Role in 2007?
Lee A. Fleisher, MD, FACC, FAHA
There has been a tremendous change in practice during the last 3 decades with regardto the need for preoperative diagnostic testing. When I was a resident in the 1980s,
virtually all patients received a standard battery of tests including a 12-lead electrocar-diogram (ECG). It was not uncommon for healthy 20 year olds to have an ECG on thechart. Beginning in the 1980s and throughout much of the 1990s, the value of routinelaboratory screening was questioned with respect to the utility of these routine tests, andin some cases whether testing in an inappropriate patient population could actually lead toincreased harm.1–6 This led a Task Force of the American Society of Anesthesiologists todevelop a Practice Advisory on Preanesthesia Evaluation, which incorporates the inte-gration of patient history and surgical procedure in the decision to perform diagnostictesting.7 With respect to the ECG, the Task Force recognized that age alone may not bean indication for an ECG, but reported an absence of studies to make a more conclusiverecommendation. In this issue, van Klei and colleagues provide additional evidence withrespect to the indication for obtaining a preoperative ECG and the interpretation of anynew findings.8
From a clinical standpoint, a key question is the need to obtain an ECG in anypatient without documented or risk factors for coronary artery disease before noncardiacsurgery. The current study attempts to address this by examining the additive value ofECG abnormalities beyond information obtained from clinical history for predictingperioperative myocardial infarction. They queried their large clinical databases from 2institutions, which is a useful method to generate hypotheses by demonstrating anassociation between specific practices with outcomes.9 The limitations of databaseanalyses is that they are retrospective in nature and data collection on risk factors,processes, and outcomes may be incomplete. This is particularly true with this dataset inthat the trigger to obtain tests to diagnose a perioperative myocardial infraction wasdependent on signs and symptoms of cardiovascular complications as opposed to routinesurveillance in all patients. Despite these limitations, the authors were able to determinethat left and right bundle branch block were independently predictive of perioperativemyocardial infraction. Importantly, this information from the preoperative ECG did notadd predictive value over a history of ischemic heart disease and high-risk surgery. Ininterpreting data like this, the face validity of such conclusions is important. As describedin the article, other authors have similarly shown the predictive value of preoperative ECGchanges for cardiac events but did not specifically determine whether the information fromthe ECG added information beyond clinical history. However, Schein and colleagues wereunable to demonstrate the utility of routine ECG before cataract surgery in a large scalerandomized trial; however, the overall incidence of complications was extremely low.10
If an ECG is obtained in a patient without documented or risk factors for coronaryartery disease, then how might the information be used? Several recent randomized trialssuggest that coronary revascularization before major noncardiac surgery is not indicatedif appropriate perioperative medical therapy is employed, even in patients with interme-
From the Robert D. Dripps Professor and Chair of Anesthesiology and Critical Care, Professor of Medicine, University of Pennsylvania, Philadelphia, PA.Reprints: Lee A. Fleisher, MD, FACC, Robert Dunning Dripps Professor and Chair, Department of Anesthesiology and Critical Care, Professor of Medicine,
University of Pennsylvania School of Medicine, 3400 Spruce Street, Dulles 680, Philadelphia, PA 19104. E-mail: [email protected] © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0171DOI: 10.1097/SLA.0b013e31811eb927
© 2007 Lippincott Williams & Wilkins 171

diate clinical risk.11,12 Coronary artery bypass grafting mayonly benefit patients with severe triple vessel disease, andeven this finding has been questioned.13–15 Therefore, theincidental findings of Q waves or bundle branch block on aperioperative ECG in an asymptomatic patient will rarely, ifever, lead to a decision to perform preoperative coronaryrevascularization, since surgery would not be indicated in anasymptomatic individual. However, medical therapy may bemodified for patients with occult disease. The diagnosis ofunrecognized coronary artery disease by ECG criteria maylead to the institution of perioperative beta blockade, al-though the evidence is conflicting regarding the benefit ofacute administration of beta blockers in patients withoutactive ischemia or a positive stress test.16
In summary, the current study should be viewed ashypothesis-generating and unlike a randomized controlledtrial cannot specifically address the question of whetherelimination of preoperative ECGs in patients without knownrisk factors for coronary disease, regardless of age, wouldlead to an increase in adverse events. While we await suchrandomized controlled trials or natural history experiments, Ibelieve that there continues to be some value in providing abaseline ECG in those patients over 60 years of age, althoughit does not have to be performed within the last 30 days. Froman efficiency standpoint, the first observation of changes onan ECG may be at the time of induction of anesthesia, whichmay lead to a need to determine if these are old or acutechanges. The availability of an old ECG may be of value indetermining if it is appropriate to proceed. In the interim, acareful discussion should occur among the surgeons, anes-thesiologists, and primary caregivers at a given hospital todefine the best protocols and paradigms with respect to apreoperative ECG for their own institution.
REFERENCES1. Velanovich V. How much routine preoperative laboratory testing is
enough? Am J Med Qual. 1993;8:145–151.2. Golub R, Cantu R, Sorrento JJ, Stein HD. Efficacy of preadmission
testing in ambulatory surgical patients �see comments�. Am J Surg.1992;163:565–570; discussion 571.
3. Kaplan EB, Sheiner LB, Boeckmann AJ, et al. The usefulness ofpreoperative laboratory screening. JAMA. 1985;253:3576–3581.
4. Narr BJ, Hansen TR, Warner MA. Preoperative laboratory screening in
healthy Mayo patients: cost-effective elimination of tests and unchangedoutcomes. Mayo Clin Proc. 1991;66:155–159.
5. Narr BJ, Warner ME, Schroeder DR, Warner MA. Outcomes of patientswith no laboratory assessment before anesthesia and a surgical proce-dure. Mayo Clin Proc. 1997;72:505–509.
6. Silverstein MD, Boland BJ. Conceptual framework for evaluating lab-oratory tests: case-finding in ambulatory patients. Clin Chem. 1994;40:1621–1627.
7. Practice advisory for preanesthesia evaluation: a report by the AmericanSociety of Anesthesiologists Task Force on Preanesthesia Evaluation.Anesthesiology. 2002;96:485–496.
8. van Klei WA, Bryson GL, Yang H, et al. The value of routine preop-erative electrocardiography in predicting myocardial infarction afternoncardiac surgery. Ann Surg. 2007;246:165–170.
9. Reich DL, Bodian CA, Krol M, et al. Intraoperative hemodynamicpredictors of mortality, stroke, and myocardial infarction followingcoronary artery bypass surgery. Anesth Analg. 1999;89:814–822.
10. Schein OD, Katz J, Bass EB, et al. The value of routine preoperativemedical testing before cataract surgery. Study of Medical Testing forCataract Surgery. N Engl J Med. 2000;342:168–175.
11. McFalls EO, Ward HB, Moritz TE, et al. Coronary-artery revascular-ization before elective major vascular surgery. N Engl J Med. 2004;351:2795–2804.
12. Poldermans D, Bax JJ, Schouten O, et al. Should major vascular surgerybe delayed because of preoperative cardiac testing in intermediate-riskpatients receiving beta-blocker therapy with tight heart rate control?J Am Coll Cardiol. 2006;48:964–969.
13. Landesberg G, Berlatzky Y, Bocher M, et al. A clinical survival scorepredicts the likelihood to benefit from preoperative thallium scanningand coronary revascularization before major vascular surgery. EurHeart J. 2007;28:533–539.
14. Ward HB, Kelly RF, Thottapurathu L, et al. Coronary artery bypassgrafting is superior to percutaneous coronary intervention in preventionof perioperative myocardial infarctions during subsequent vascular sur-gery. Ann Thorac Surg. 2006;82:795–800; discussion 800–801.
15. Poldermans D, Schouten O, Vidakovic R, et al. A clinical randomizedtrial to evaluate the safety of a noninvasive approach in high-riskpatients undergoing major vascular surgery: the DECREASE-V PilotStudy. J Am Coll Cardiol. 2007;49:1763–1769.
16. Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2006 guidelineupdate on perioperative cardiovascular evaluation for noncardiac sur-gery: focused update on perioperative beta-blocker therapy: a report ofthe American College of Cardiology/American Heart Association TaskForce on Practice Guidelines (Writing Committee to Update the 2002Guidelines on Perioperative Cardiovascular Evaluation for NoncardiacSurgery): developed in collaboration with the American Society ofEchocardiography, American Society of Nuclear Cardiology, HeartRhythm Society, Society of Cardiovascular Anesthesiologists, Societyfor Cardiovascular Angiography and Interventions, and Society forVascular Medicine and Biology. Circulation. 2006;113:2662–2674.
Fleisher Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins172

FEATURE
National Failure to Operate on Early StagePancreatic Cancer
Karl Y. Bilimoria, MD,*† David J. Bentrem, MD,* Clifford Y. Ko, MD, MS, MSHS,†‡Andrew K. Stewart, MA,† David P. Winchester, MD,†§ and Mark S. Talamonti, MD*
Background: Despite studies demonstrating improved outcomes,pessimism persists regarding the effectiveness of surgery for pan-creatic cancer. Our objective was to evaluate utilization of surgery inearly stage disease and identify factors predicting failure to undergosurgery.Methods: Using the National Cancer Data Base (1995–2004), 9559patients were identified with potentially resectable tumors (pretreat-ment clinical Stage I: T1N0M0 and T2N0M0). Multivariate modelswere employed to identify factors predicting failure to undergosurgery and assess the impact of pancreatectomy on survival.Results: Of clinical Stage I patients 71.4% (6823/9559) did notundergo surgery; 6.4% (616/9559) were excluded due to comorbidi-ties; 4.2% (403/9559) refused surgery; 9.1% (869/9559) were ex-cluded due to age; and 38.2% (3,644/9559) with potentially resect-able cancers were classified as “not offered surgery.” Of the 28.6%(2736/9559) of patients who underwent surgery, 96.0% (2630/2736)underwent pancreatectomy, and 4.0% (458/2736) had unresectabletumors.
Patients were less likely to undergo surgery if they were olderthan 65 years, were black, were on Medicare or Medicaid, hadpancreatic head lesions, earned lower annual incomes, or had lesseducation (P � 0.0001). Patients were less likely to receive surgeryat low-volume and community centers. Patients underwent surgerymore frequently at National Cancer Institute/National Comprehen-sive Cancer Network-designated cancer centers (P � 0.0001). Pa-tients who were not offered surgery had significantly better survivalthan those with Stage III or IV disease but worse survival thanpatients who underwent pancreatectomy for Stage I disease (P �0.0001).Conclusions: This is the first study to characterize the strikingunderuse of pancreatectomy in the United States. Of early stage
pancreatic cancer patients without any identifiable contraindications,38.2% failed to undergo surgery.
(Ann Surg 2007;246: 173–180)
Pancreatic cancer is the fourth leading cause of cancerdeaths in the United States. In 2007, the American Cancer
Society estimates that over 37,000 patients will be diagnosedwith pancreatic cancer, and more than 33,000 will die of thedisease.1 Patients with pancreatic cancer have a particularlydismal prognosis due to multiple factors, including late pre-sentation, aggressive tumor biology, complex surgical man-agement, and the lack of effective systemic therapies.2,3
Overall survival rates have remained relatively unaffectedwith fewer than 5% of all patients surviving 5 years afterdiagnosis.4
Surgery remains the only potentially curative treatmentof localized pancreatic cancer.3 During the last 20 years,significant advances in preoperative evaluation, surgicaltechniques, and postoperative care have reduced the peri-operative morbidity and mortality associated with pancreaticsurgery.5–8 Mortality after pancreaticoduodenectomy hasdropped from �25% in the 1960s to less than 3% in somehigh-volume centers,7–11 and recent studies have suggestedimprovements in long-term survival rates after resection forlocalized disease that approach 30%.12
Despite numerous studies and guidelines establishingpancreatectomy as the primary treatment modality for local-ized pancreatic adenocarcinoma, pessimistic attitudes towardall patients with pancreatic cancer have perhaps led to skep-ticism regarding the efficacy of resection. Clinicians havelong recognized that a diagnosis of pancreatic cancer encom-passes little variability in long-term outcomes; however,these views are outdated in light of recent evidence. Ourhypothesis was that these attitudes affect utilization of sur-gery for early stage pancreatic cancer after controlling forage, comorbidities, and patient refusal to undergo surgery.The objectives of this study were 1) to evaluate and charac-terize the utilization of surgery for pancreatic adenocarci-noma, 2) to identify factors predicting failure to undergosurgery for localized disease, and 3) to evaluate the effect ofsurgery on survival.
From the *Department of Surgery, Feinberg School of Medicine, Northwest-ern University, Chicago, IL; †National Cancer Data Base, Cancer Pro-grams, American College of Surgeons, Chicago, IL; ‡Department ofSurgery, University of California, Los Angeles (UCLA) and VA GreaterLos Angeles Healthcare System, Los Angeles, CA; and §Department ofSurgery, Evanston Northwestern Healthcare, Evanston, IL.
KYB is supported by the American College of Surgeons, Clinical Scholars inResidence program and a clinical research grant from the NorthwesternUniversity Department of Surgery.
Reprints: Mark S. Talamonti, MD, Department of Surgery, Feinberg Schoolof Medicine, Northwestern University, 675 N. St. Clair Street, Galter10-105, Chicago, IL 60611. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0173DOI: 10.1097/SLA.0b013e3180691579
Annals of Surgery • Volume 246, Number 2, August 2007 173

METHODS
Data Acquisition and Patient SelectionThe National Cancer Data Base (NCDB) is a program
of the American College of Surgeons (ACS) and the Com-mission on Cancer (CoC).13 The NCDB now contains data onover 19 million patients from over 1440 hospitals accountingfor greater than 75% of all cancers in the United Statesannually. The NCDB collects data regarding patient demo-graphics, socioeconomic status, tumor variables, clinical andpathologic staging, treatment details, recurrence, survival,and health systems/provider information. Based on nationalincidence estimates from the American Cancer Society, theNCDB captures greater than 76% of all pancreatic cancers inthe United States.1 This study protocol was approved by theNorthwestern University Institutional Review Board.
Patients from 1995 to 2004 with International Classifica-tion of Disease – Oncology, 2nd and 3rd Edition (ICD-O-2/3) codes specific for pancreas were selected (C25.0, C25.1,C25.2, C25.3, C25.7, C25.8, C25.9).14,15 Patients were limitedby ICD-O-2/3 codes for histologies consistent with pancreaticadenocarcinoma yielding 192,565 patients. Due to variations inthe American Joint Committee on Cancer (AJCC) Cancer Stag-ing Manual from 1995 to 2004 (editions 4 to 6), all patients wererestaged based on the AJCC 6th Edition TNM classification.16
Unique to the NCDB is the requirement to report bothclinical and pathologic staging information. A pretreatmentclinical stage is recorded in the database as judged by thetreating physicians based on clinical findings and radio-graphic imaging. If the patient undergoes a surgical resection,pathologic staging information is separately recorded. Welimited our analysis to patients with complete staging infor-mation who had clinical Stage I disease (n � 9559), whichincludes T1N0M0 and T2N0M0. Based on clinical and ra-diographic evaluation, these patients have potentially resect-able disease because the tumor is localized to the pancreasand there are no obviously involved lymph nodes or distantmetastases.
Patients who underwent pancreatectomy were identi-fied based on the CoC’s Registry Operations and DataStandards (ROADS) and the Facility Oncology RegistryData Standards (FORDS) site-specific procedure coding.17,18
In addition, if a patient did not undergo pancreatectomy, areason is recorded in the database as detailed in the FORDSmanual. These potential explanations include “not offeredsurgery”; “excluded due to comorbidities”; “patient refusedrecommended surgery”; and “unknown”. Patients who un-dergo surgery but who do not undergo pancreatectomy (pre-sumably unresectable at laparotomy) are also recorded sepa-rately. In addition, we categorized patients older than 85years at the time of diagnosis as “advanced age”.
The NCDB began requiring reporting of 6 preexistingcomorbidities based on International Classification of Dis-ease, 9th Edition (ICD-9-CM) classification in 2003.19 Theprimary cancer diagnosis and postoperative complications arenot included when these 6 codes are reported, and comor-bidities are recorded regardless of whether the patient under-goes surgery. A modified Charlson Comorbidity score (thenumber of coexisting medical conditions weighted according
to their relative effects on survival) was calculated to assessthe severity of preexisting comorbidities.20,21
Hospital ClassificationHospitals in the NCDB are classified by the CoC into
academic and community cancer centers based on case vol-ume and services offered.22 Academic hospitals must beaffiliated with teaching and research institutions, meet annualcase-volume requirements, and fulfill criteria regarding theability to provide a wide range of cancer-specific specialistsand services. Academic institutions comprise 23.6% of CoChospitals and account for 37.3% of cases in the NCDB.National Comprehensive Cancer Network (NCCN) hospitalsand National Cancer Institute (NCI)-designated cancer cen-ters contribute data to the NCDB. NCCN and NCI hospitalswere combined for analysis. Hospital volume was based onthe average annual volume of pancreatic cancer cases re-ported. Quartiles were calculated with equal numbers ofpatients in each quartile. Hospital volume was evaluated as acontinuous and categorical variable, but because results weresimilar, volume is only shown as a categorical variable.
Statistical AnalysisContinuous variables were compared using indepen-
dent-sample t tests. Categorical variables were analyzed withPearson �2 tests with Bonferroni correction. Graphs andtables were used as needed to examine the distribution ofeach variable; Pearson correlation coefficients were deter-mined for each pair of variables to aid in model building.Multivariate analysis was performed with a binary logisticregression model to identify factors predicting failure toundergo surgery in clinical Stage I patients. The level ofstatistical significance was set to P � 0.05. All P valuesreported are 2-tailed. As surgical and nonsurgical patientswere evaluated, 5-year survival rates were calculated as thetime from the date of diagnosis to death or last follow-up.Five-year overall and relative survival was estimated by theKaplan–Meier method and compared using the log-ranktest.23 Overall and relative survival (ratio of observed toexpected survival based on United States Census datamatched for gender, age, race, and no history of cancer) weresimilar due to the short median survival for pancreatic ade-nocarcinoma patients, thus only overall survival is shown.Median follow-up was 13.1 months.
Cox proportional hazards modeling was used to evalu-ate the impact of surgery on survival while adjusting forpotential confounders, including age (�55, 56–65, 66–75,76–85, �85 years), race (white, black, Asian, Hispanic,Other), median income (quartiles), college education (quar-tiles by percent with a degree per zip code), insurance status(private, Medicaid, Medicare, governmental, uninsured), an-atomic location within the pancreas (head, body, tail), hospi-tal factors (case volume quartiles, academic versus commu-nity, and NCCN/NCI versus non-NCCN/NCI were insertedseparately into the model due to a high degree of collinear-ity), year of diagnosis, and census region.24 Since patient-level socioeconomic data are not recorded, median householdincome and education (percent of patients with college de-grees) were assessed at the zip code level based on 2000
Bilimoria et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins174

United States Census Bureau data.25 Utilization of surgerywas also examined by United States census region based on2000 Census Bureau data. Statistical analyses were per-formed using SPSS, version 14 (Chicago, IL).
RESULTSOf the 192,565 patients with pancreatic adenocarci-
noma in the NCDB from 1995 to 2004, 9559 patients wereselected who had pretreatment clinical Stage I disease andwere thus thought to be potentially resectable (Table 1). Themedian age was 71.9 years (mean 72.4, range 18–107). Morethan 60% of the patients had Medicare or private insurance.The tumors were located in the head of the pancreas in69.8%, body in 8.0%, and tail in 5.7%. The percentage ofpatients treated at academic hospitals was 45.2%, whereas54.8% were treated at community hospitals. NCCN/NCIcenters collectively cared for 11.3% of patients.
Utilization of SurgeryFrom 1995 to 2004, pancreatectomy utilization in Stage
I patients increased from 21.8% to 35.7% (P � 0.0001);
while the percentage of patients who did not receive treat-ment decreased (Fig. 1). Of the 9559 patients with clinical,pretreatment Stage I pancreatic cancer, only 28.6% under-went surgery (Fig. 2). Of those who underwent surgery,96.0% were resectable and underwent pancreatectomy, while4.0% were unresectable at laparotomy. Of clinical Stage Ipatients, 6.4% were excluded due to comorbidities, 4.2%refused surgery, and an additional 9.1% were excluded due toadvanced age. Of patients with potentially resectable tumors38.2% were not offered surgery. The reason for why theremaining 13.5% of patients did not undergo surgery was listedas unknown. Thus, 51.7% (38.2% not offered surgery � 13.5%unknown) of pancreatic cancer patients with clinical Stage Idisease did not have a documented or identifiable reason for whythey did not undergo surgery. Moreover, there was a minimalchange in the reasons for not undergoing surgery from 1995 to2004 (Fig. 3).
Factors Predicting Utilization of SurgeryTo identify factors predicting failure to undergo sur-
gery, patients who underwent surgery were compared with
FIGURE 1. Treatment trends for Stage I pancreatic adenocar-cinoma comparing utilization of pancreatectomy, nonsurgi-cal treatment, and no treatment.
FIGURE 2. Management of 9559 patients with pretreatment,clinical Stage I pancreatic adenocarcinoma from 1995 to2004.
TABLE 1. Characteristics of Patients With Clinical Stage IPancreatic Cancer
Number of patients 9559
Gender
Male 4330 (45.3%)
Female 9552 (54.6%)
Age
�55 yr 1112 (1.6%)
56–65 yr 1603 (16.8%)
66–75 yr 2742 (28.7%)
76–85 yr 3017 (31.6%)
�85 yr 1085 (11.3%)
Race
White 7708 (80.6%)
Black 1118 (11.7%)
Hispanic 397 (4.2%)
Asian 169 (1.85)
Other 167 (1.7%)
Insurance
Private 2340 (24.5%)
Medicaid 246 (2.6%)
Medicare 3515 (36.8%)
Governmental 123 (1.3%)
Uninsured 175 (1.8%)
Tumor location
Head 6676 (69.8%)
Body 766 (8.0%)
Tail 549 (5.7%)
Facility type
Academic 4322 (45.2%)
Community 5237 (54.8%)
NCCN/NCI centers
NCCN/NCI 1081 (11.3%)
Academic (Non-NCCN/NCI) 3241 (33.9%)
Community (Non-NCCN/NCI) 5237 (54.8%)
Annals of Surgery • Volume 246, Number 2, August 2007 Pancreatic Surgery Underutilization
© 2007 Lippincott Williams & Wilkins 175

those who were not offered surgery. The age of patients whowere not offered surgery was higher than those who wereselected to undergo surgery: 71.7 versus 65.1 years, P �0.0001. The average age of patients not offered surgery andof those who underwent surgery remained similar over thecourse of the study (not offered surgery: 73.6 years in 1995 to74.8 years in 2004, P � 0.34; underwent surgery: 63.3 yearsin 1995 to 64.7 years in 2004, P � 0.28). Charlson scoresreflected more severe comorbidities in the group that under-went surgery compared with the group that was not offeredsurgery (Charlson �2: 32.3% versus 30.6%, P � 0.0001).Logistic regression was used to identify factors predictingfailure to be offered surgery. Patients were significantly lesslikely to receive surgery if they were older, were black, hadlower annual incomes, had less education, or were on Medi-care or Medicaid (P � 0.0001) (Table 2). Patients were alsonearly 3-fold less likely to undergo resection if the tumor wasin the head/body of the pancreas compared with the tail (P �0.0001). In addition, patients were less likely to receivesurgery at low-volume centers (odds ratio �OR� 0.36, 95%confidence interval �CI� 0.30–0.45, P � 0.0001) and com-munity hospitals (OR 0.41, 95% CI 0.35–0.47, P � 0.0001)than at high-volume and academic institutions. Moreover,patients treated at NCCN/NCI cancer centers were signifi-cantly more likely to undergo pancreatectomy than patientstreated at other academic centers (OR 0.43, 95% CI 0.34–0.54, P � 0.0001) and community hospitals (OR 0.23, 95%CI 0.19–0.29, P � 0.0001).
Further analysis was done to compare patients whorefused surgery to those who received surgery. Patients whorefused surgery were older: 77.4 versus 65.1 year, P �0.0001. Charlson scores reflected more severe comorbiditiesin the group who refused surgery compared with the groupthat underwent surgery (Charlson �2: 38.7% vs. 32.3%, P �0.0001). On multivariate analysis, patients who refused sur-gery were significantly more likely to be older, black, onMedicaid, or to have lesions in the head/body of the pancreas(P � 0.0001) (Table 2). Patients treated at low-volume and
community hospitals refused surgery more often than patientsseen at high-volume and academic institutions (P � 0.0001).Patients treated at NCCN/NCI institutions were significantly lesslikely to refuse surgery (P � 0.0001). Annual income and levelof education did not affect whether patients refused surgery.
Impact on SurvivalTo evaluate the impact of surgery on survival, we
compared 3 groups: clinical Stage I patients undergoingpancreatectomy, clinical Stage I patients who were not of-fered surgery, and patients with Stage III or IV disease whodid not undergo any surgical treatment (n � 68,521). Five-year overall survival rates for clinical Stage I patients whounderwent pancreatectomy were higher than for those pa-tients with Stage III/IV disease, 19.3% versus 0.8%, P �0.0001 (median survival 19.1 vs. 4.2 months) (Fig. 4). How-ever, survival for clinical Stage I patients who were notoffered surgery (median survival 8.4 months) was initiallybetter than Stage III/IV patients but became more similar topatients with unresectable disease at �36 months from diag-nosis. A Cox proportional hazards model was used to com-pare survival among these 3 groups while controlling forpotential confounders (Table 3). Pancreatectomy was anindependent predictor of a greater than 2-fold increase in thelikelihood of survival when compared with patients who werenot offered surgery and a greater than 4-fold increase com-pared with Stage III/IV patients (P � 0.0001). Clinical StageI patients who were not offered surgery had better adjustedsurvival compared with Stage III/IV patients (P � 0.0001).
DISCUSSIONPancreatectomy is the only curative therapy for early
stage pancreatic cancer.4,26 However, nihilistic attitudes to-ward the disease may result in underuse of cancer-directedsurgery. This study demonstrates that despite better survivalafter pancreatectomy, 51.7% of Stage I patients did notundergo surgery for potentially resectable pancreatic cancereven after accounting for patients who did not undergosurgery due to severe comorbidities, advanced age, or patientrefusal. Patients were less likely to undergo surgery if theywere older, were black, had lower annual incomes, had lesseducation, or were on Medicare or Medicaid. Patients weremore likely to receive surgery at academic institutions,high-volume hospitals, and NCCN/NCI centers. This is thefirst study to describe and characterize such striking un-deruse of pancreatectomy and identify factors predictingunderutilization.
Our first objective was to assess and characterize utili-zation of pancreatic surgery. In 1996 Sener et al27 reportedtreatment and survival trends on 100,313 patients from theNCDB. They noted that 21.9% of Stage I patients from 1985to 1995 underwent cancer-directed therapy. Similarly, ourgroup’s report on rising utilization of multimodality therapyfound a similarly small percentage of patients receivingpancreatectomy for early stage disease.28 Two recent studiesutilizing the NCI’s Surveillance Epidemiology and End Re-sults (SEER) database focused on the increasing utilization ofsurgery and reported that surgical management of resectablepancreatic cancer had increased to �35% in 2002.12,29 How-
FIGURE 3. Reasons why patients did not undergo surgeryfor clinical Stage I pancreatic cancer over time comparedwith those undergoing surgery.
Bilimoria et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins176

TABLE 2. Unadjusted and Adjusted Analysis of Patients Who Were Not Offered Surgery or Who Refused Surgery Comparedto Stage I Patients Who Underwent Pancreatectomy
Not Offered Surgery Adjusted Refused Surgery Adjusted
Unadjusted (%) Significance*Odds Ratio(95% CI) Unadjusted (%) Significance*
Odds Ratio(95% CI)
Gender P � 0.008 P � 0.05
Male 38.5 1.00 (Referent) 3.5 1.00 (Referent)
Female 37.6 1.01 (0.88–1.15) 4.8 0.72 (0.52–1.01)
Age P � 0.0001 P � 0.0001
�55 yr 27.8 1.00 (Referent) 2.3 1.00 (Referent)
56–65 yr 34.6 0.71 (0.57–0.88) 1.6 0.98 (0.47–2.08)
66–75 yr 43.4 0.47 (0.37–0.60) 3.3 0.44 (0.21–0.89)
�75 yr 52.3 0.19 (0.15–0.25) 6.1 0.08 (0.04–0.16)
Race P � 0.003 P � 0.0001
White 37.7 1.00 (Referent) 4.2 1.00 (Referent)
Black 41.7 0.71 (0.57–0.88) 4.8 0.33 (0.20–0.55)
Hispanic 34.5 0.84 (0.59–1.19) 3.0 0.57 (0.26–1.22)
Asian 34.9 0.97 (0.59–1.59) 3.8 1.22 (0.35–4.43)
Other 37.1 0.75 (0.46–1.23) 1.2 0.85 (0.54–1.34)
Median Income P � 0.0001 P � 0.04
75–99th percentile 35.5 1.00 (Referent) 3.9 1.00 (Referent)
50–74th percentile 39.1 0.88 (0.57–1.36) 4.2 0.84 (0.71–1.00)
25–49th percentile 39.3 0.75 (0.47–1.20) 4.0 0.86 (0.71–1.04)
0–25th percentile 39.5 0.56 (0.33–0.94) 4.8 0.85 (0.68–1.05)
% with College Degree P � 0.0001 P � 0.21
75–99th percentile 35.1 1.00 (Referent) 4.5 1.00 (Referent)
50–74th percentile 38.5 0.82 (0.69–0.97) 3.4 1.37 (0.91–2.07)
25–49th percentile 41.7 0.73 (0.60–0.89) 4.6 0.81 (0.51–1.29)
0–25th percentile 41.0 0.70 (0.55–0.88) 4.3 0.72 (0.43–1.22)
4.2
Insurance P � 0.0001 P � 0.0001
Private 31.4 1.00 (Referent) 4.0 1.00 (Referent)
Medicaid 32.6 0.63 (0.44–0.90) 2.4 0.37 (0.15–0.94)
Medicare 38.6 0.78 (0.64–0.95) 3.3 0.47 (0.19–1.18)
Governmental 41.8 1.60 (1.03–2.46) 5.1 0.59 (0.37–0.94)
Uninsured 43.9 1.03 (0.68–1.05) 0.8 †
Anatomic location P � 0.0001 P � 0.001
Head 37.6 0.42 (0.31–0.55) 4.7 0.22 (0.01–0.50)
Body 45.4 0.25 (0.17–0.36) 2.7 0.38 (0.14–1.05)
Tail 26.4 1.00 (Referent) 2.65 1.00 (Referent)
Volume P � 0.0001 P � 0.0001
75–99th percentile 27.5 1.00 (Referent) 3.4 1.00 (Referent)
50–74th percentile 41.9 0.44 (0.37–0.52) 3.7 0.46 (0.29–0.71)
25–49th percentile 43.9 0.34 (0.28–0.41) 5.3 0.28 (0.18–0.43)
0–25th percentile 41.1 0.36 (0.30–0.45) 4.8 0.28 (0.17–0.46)
Facility Type P � 0.0001 P � 0.0001
Academic 30.7 1.00 (Referent) 4.7 1.00 (Referent)
Community 43.2 0.41 (0.35–0.47) 3.3 0.36 (0.25–0.51)
P � 0.0001 P � 0.0001
NCCN/NCI 21.0 1.00 (Referent) 2.8 1.00 (Referent)
Academic (Non-NCCN/NCI) 35.3 0.43 (0.34–0.54) 3.9 0.45 (0.25–0.81)
Community (Non-NCCN/NCI) 43.2 0.23 (0.19–0.29) 4.7 0.21 (0.12–0.37)
Odds ratios represent likelihood of undergoing surgery. There were no significant differences in “census region” and the variable was dropped from the model.*Significance based on Pearson �2 test for unadjusted percentages of patients “not offered surgery” and “refused surgery”.†Not enough cases to estimate odds ratio.CI indicates confidence interval.
Annals of Surgery • Volume 246, Number 2, August 2007 Pancreatic Surgery Underutilization
© 2007 Lippincott Williams & Wilkins 177

ever, no study has attempted to define and characterize theunderutilization of surgery. We found that after controllingfor comorbidities, age, and patient refusal, 54.7% of patientdid not have a documented or identifiable reason for why theydid not undergo surgery for presumably resectable pancreaticmalignancy. Of patients with potentially resectable pancreaticcancer 38.2% were simply not offered surgery.
Our second objective was to identify disparities in careassociated with the failure to operate on clinical Stage Ipatients. Racial disparities in the care of pancreatic cancerhave been well-described.30,31 In our analysis, patients weremore likely to not be offered surgery if they were black. Wealso found that older age was associated with decreasedutilization of surgery. Interestingly, we found that the meanage of patients undergoing surgery and not offered surgeryremained unchanged over the past decade. While studies ofpancreaticoduodenectomy in patients over 85 years of agehave reported that surgery can be done safely in olderpatients, they do show an increase in morbidity and mortalitywith increasing age.26,32,33 Regardless of whether these racialand age discrepancies in the care of pancreatic cancer patientsare due to access to care or hospital/physician factors, em-phasis needs to be placed on offering resection to all appro-priate patients.
In our analysis, patients were more likely to receivesurgery for lesions in the tail compared with the head or bodyof the pancreas. This is an intriguing finding that may dem-
onstrate historically nihilistic attitudes toward lesions in thehead of the pancreas. Referring physicians, surgeons, andpatients may be affected by historical data regarding theconsiderable perioperative morbidity and mortality of pan-creaticoduodenectomy. Multiple studies in the last 20 yearsfrom academic and community institutions have demon-strated improved safety of surgery for lesions in the head ofthe pancreas.5,7,8,10,11,34,35 Our previous work on survival hasdemonstrated similar outcomes for patients undergoing sur-gery regardless of lesion location within the pancreas.36 Inthese Stage I patients with resectable disease, surgery is theonly chance for cure and, if medically suitable, the location ofthe lesion within the pancreas should not preclude resection.
Numerous reports in recent years have demonstrateddecreased perioperative complications and improved survivalfor patients undergoing pancreatectomy at academic, high-volume centers.11,26,37–43 We found that patients treated athigh-volume hospitals, academic centers, and NCCN/NCIinstitutions were more likely to undergo surgery. This may bedue to the increased willingness of surgeons at designatedcancer centers to operate on pancreatic cancer. Similarly, itmay be a function of the patient population served by NCCN/NCI institutions. Our results suggest that not only do spe-cialty cancer centers have better outcomes, but they also offerstage-specific treatments more frequently.
A recent study focusing on pancreatic surgery in Afri-can American patients found that black patients were more
TABLE 3. Unadjusted and Adjusted Survival Analysis Comparing Patients Who Underwent Pancreatectomy (Clinical Stage I),Were Not Offered Surgery (Clinical Stage I), and Those With Metastatic Disease (Stage III or IV and Did Not Undergo Surgery)
1-yr Survival (%) 5-yr Survival (%)Median Survival
(mos.)Unadjusted Hazard
Ratio (95% CI)Adjusted HazardRatio (95% CI)
Pancreatectomy (clinical stage I) 69.8 24.6 19.3 1.00 (Referent) 1.00 (Referent)
Not offered surgery (clinical stage I) 26.8 2.9 8.4 2.50 (2.31–2.71) 2.24 (2.07–2.43)
Stage III or IV disease (no surgery) 7.8 0.8 4.2 5.15 (4.82–5.51) 4.16 (3.86–4.48)
Adjusted for gender, age, race, stage, anatomic location within the pancreas, hospital volume, and adjuvant therapy.CI indicates confidence interval.
FIGURE 4. Five-year survival for pancreaticadenocarcinoma comparing patients whounderwent pancreatectomy for clinicalStage I (n � 2736), were not offered sur-gery despite being clinical Stage I (n �3644), and those with Stage III or IV whodid not undergo surgery (n � 68,521).
Bilimoria et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins178

likely to refuse surgery than white patients.30 Our resultsdemonstrate similar findings in that black patients were 3times more likely to refuse an operation. We also found thatrefusal of surgery for early stage pancreatic cancer wasassociated with advanced age, insurance status (Medicaid),and tumor location within the pancreas (head and bodytumors). Moreover, patients treated at NCCN/NCI centerswere significantly less likely to refuse surgery. This poten-tially reflects the type of patients who seek attention atNCCN/NCI centers but may also be associated with theincreased willingness of surgeons at these hospitals to under-take high complexity operations.
Our third objective was to assess the impact of pancre-atectomy on survival. Numerous studies have shown thatsurgery is the only potentially curative treatment of earlystage pancreatic cancer.4 Similarly, we found that clinicalStage I patients selected to undergo pancreatectomy hadsignificantly improved survival compared with Stage III/IVpatients. More interesting was the pattern of survival in theclinical Stage I patients who were not offered surgery. For thefirst 2 years after diagnosis, these patients had survival thatwas clearly better than Stage III/IV patients who have unre-sectable disease; however, by the 3-year mark, that differencehad nearly disappeared, and patients who were clinical StageI at diagnosis and did not undergo surgery now had survivalrates that were no different from patients presenting withadvanced disease. Thus, although it may be tempting totheorize that the patients not offered surgery simply had theirstage recorded improperly in the cancer registry or by thephysician, these survival data demonstrate a clear differencebetween these potentially resectable patients who were notoffered surgery and those that underwent pancreatectomy,implying that these patients initially had disease that waspotentially resectable.
Our study has several potential limitations. First, welimited our analysis to patients with clinical, pretreatmentStage I (T1N0M0 and T2N0M0) disease to establish a pop-ulation of pancreatic cancer patients who are potential can-didates for resection.16 Certainly patients with T3 and/ornode-positive disease are also candidates for surgical extir-pation; however, we limited the ambiguity in the appropri-ateness of resection for these patients. Moreover, the AJCCpancreatic cancer staging system has changed during the last10 years, particularly with respect to the definitions of StageII and III disease. As such, we chose not to confound theanalyses with the inclusion of Stage II patients. The finding ofpancreatectomy underuse is likely to be strengthened bybroadening our study to include Stage II patients because ifpatients with Stage I disease are not receiving surgery, then itis likely that a higher percentage of appropriate, resectablepatients with Stage II disease are not undergoing surgery. Asecond potential limitation of this study is the under-reportinginherent to cancer registry data.44–47 It is possible that thenumber of patients receiving surgery or the reason for whythey did not undergo pancreatectomy is under-reported. How-ever, studies examining the accuracy of registry data havefound that procedures are coded with high accuracy whencompared with patient charts, with considerably more accu-
racy than diagnosis and comorbidity codes.48–50 Further-more, the number of patients missing data on whether theyhad surgery or were excluded (age, comorbidities, patientrefusal) is less than 5% in 2004. Thus, nearly all patients whodo not undergo pancreatectomy have a documented reasonexplaining why they did not undergo cancer-directed surgery.Finally, the patients not offered surgery may have unreportedcomorbidities or performance status that cannot be evaluatedin our dataset. However, our examination of available comor-bidity data demonstrated that patients not offered surgeryactually had lower Charlson score than those patients whounderwent surgery.
CONCLUSIONSThe recognition of treatment underuse in other disease
sites has led to numerous quality improvement measuresthrough joint efforts of the American College of Surgeons,NCDB, CoC, and the National Quality Forum (NQF). Forexample, a standard of care is that Stage III colon cancerpatients should receive adjuvant chemotherapy. Cases ofStage III colon cancer submitted to the NCDB are required tohave a detailed explanation regarding why the patient did notreceive chemotherapy, and “not offered” is not an acceptablejustification. If a reason is not documented, the chart is sentback to the hospital and physician for an explanation. Adeeper understanding of the underuse of pancreatectomy maybe discovered by implementing a similar mechanism forpancreatic cancer where the hospital’s cancer registrar ortreating physician can provide a brief narrative explainingwhy the patient failed to undergo surgery, thus providing abetter understanding of the not offered surgery category.Hospitals with outlying utilization rates can be identified andnotified in the hope of improving cancer care.
Despite a demonstrated survival benefit for Stage Ipancreatic adenocarcinoma patients who undergo curativeresection, more than half of patients with resectable cancerfail to receive surgery. Patients treated at academic hospitals,NCCN/NCI institutions, and high-volume centers were morelikely to undergo surgery. The only opportunity for cure inearly stage patients is surgical resection, but nihilistic atti-tudes toward pancreatic cancer likely contribute to this strik-ing underuse of curative resection for pancreatic adenocarci-noma. There is an opportunity to improve the care ofpancreatic cancer patients in the United States by offeringsurgery to all appropriate patients with resectable disease.
ACKNOWLEDGMENTSThe authors thank the staff of the American College of
Surgeons, National Cancer Data Base, for their assistance,particularly James Banasiak, MS, and E. Greer Gay, RN,MPH, PhD.
REFERENCES1. American Cancer Society: Cancer Facts and Figures. Available at http://
www.cancer.org/docroot/stt/stt_0.asp. Accessed December 15, 2006.2. Brennan MF. Adjuvant therapy following resection for pancreatic ade-
nocarcinoma. Surg Oncol Clin N Am. 2004;13:555–566, vii.3. Stojadinovic A, Hoos A, Brennan MF, Conlon KC. Randomized clinical
trials in pancreatic cancer. Surg Oncol Clin N Am. 2002;11:207–229, x.
Annals of Surgery • Volume 246, Number 2, August 2007 Pancreatic Surgery Underutilization
© 2007 Lippincott Williams & Wilkins 179

4. Conlon KC, Klimstra DS, Brennan MF. Long-term survival after cura-tive resection for pancreatic ductal adenocarcinoma. Clinicopathologicanalysis of 5-year survivors. Ann Surg. 1996;223:273–279.
5. Fernandez-del Castillo C, Rattner DW, Warshaw AL. Standards forpancreatic resection in the 1990s. Arch Surg. 1995;130:295–299, dis-cussion 299–300.
6. Richter A, Niedergethmann M, Sturm JW, et al. Long-term results ofpartial pancreaticoduodenectomy for ductal adenocarcinoma of the pan-creatic head: 25-year experience. World J Surg. 2003;27:324–329.
7. Schmidt CM, Powell ES, Yiannoutsos CT, et al. Pancreaticoduodenec-tomy: a 20-year experience in 516 patients. Arch Surg. 2004;139:718–725, discussion 725–727.
8. Sohn TA, Yeo CJ, Cameron JL, et al. Resected adenocarcinoma of thepancreas-616 patients: results, outcomes, and prognostic indicators.J Gastrointest Surg. 2000;4:567–579.
9. Whipple AO. An evaluation of radical surgery for carcinoma of thepancreas and ampullary region. Ann Intern Med. 1949;31:624–627.
10. Cameron JL, Riall TS, Coleman J, Belcher KA. One thousand consec-utive pancreaticoduodenectomies. Ann Surg. 2006;244:10–15.
11. Lieberman MD, Kilburn H, Lindsey M, Brennan MF. Relation ofperioperative deaths to hospital volume among patients undergoingpancreatic resection for malignancy. Ann Surg. 1995;222:638–645.
12. Riall TS, Nealon WH, Goodwin JS, et al. Pancreatic cancer in thegeneral population: improvements in survival over the last decade.J Gastrointest Surg. 2006;10:1212–1223, discussion 1223–1224.
13. Winchester DP, Stewart AK, Bura C, Jones RS. The National CancerData Base: a clinical surveillance and quality improvement tool. J SurgOncol. 2004;85:1–3.
14. International Classification of Disease for Oncology. 2nd ed. Geneva:World Health Organization, 1990.
15. International Classification of Disease for Oncology. 3rd ed. Geneva:World Health Organization, 2000.
16. AJCC Cancer Staging Manual. 6th ed. Chicago, IL: Springer, 2002.17. Standards of the Commission on Cancer Volume II: Registry Operations
and Data Standards. Vol. II: Commission on Cancer, 1998.18. Facility Oncology Registry Data Standards. Chicago: Commission on
Cancer, 2004.19. Department of Health and Human Services. The International Classifi-
cation of Diseases. 9th revised. Clinical modification: ICD-9-CM.Washington, DC: Government Printing Office, 1998.
20. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method ofclassifying prognostic comorbidity in longitudinal studies: developmentand validation. J Chronic Dis. 1987;40:373–383.
21. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity indexfor use with ICD-9-CM administrative databases. J Clin Epidemiol.1992;45:613–619.
22. Commission on Cancer: Approvals Categories. Available at http://www.facs.org/cancer/coc/categories.html. Accessed December 17, 2006.
23. Kaplan E, Meier P. Nonparametric estimation from incomplete obser-vations. J Am Stat Assoc. 1958;53:457–481.
24. Cox D. Regression models and life tables. J R Stat Soc. 1972;34:187–220.
25. United States Census Bureau. Census 2000. Available at http://www.census.gov/main/www/cen2000. html. Accessed January 21,2007.
26. Fong Y, Gonen M, Rubin D, et al. Long-term survival is superior afterresection for cancer in high-volume centers. Ann Surg. 2005;242:540–544, discussion 544–547.
27. Sener SF, Fremgen A, Menck HR, Winchester DP. Pancreatic cancer: areport of treatment and survival trends for 100,313 patients diagnosedfrom 1985–1995, using the National Cancer Database. J Am Coll Surg.1999;189:1–7.
28. Bilimoria K, Bentrem D, Ko C, et al. Multimodality therapy for pan-creatic surgery in the United States: utilization, outcomes, and the effectof hospital volume. 2006. Submitted for publication.
29. Baxter NN, Whitson BA, Tuttle TM. Trends in the treatment andoutcome of pancreatic cancer in the United States. Ann Surg Oncol.2007;14:1320–1326.
30. Eloubeidi MA, Desmond RA, Wilcox CM, et al. Prognostic factors forsurvival in pancreatic cancer: a population-based study. Am J Surg.2006;192:322–329.
31. Lucas FL, Stukel TA, Morris AM, et al. Race and surgical mortality inthe United States. Ann Surg. 2006;243:281–286.
32. Sohn TA, Yeo CJ, Cameron JL, et al. Should pancreaticoduodenectomybe performed in octogenarians? J Gastrointest Surg. 1998;2:207–216.
33. Makary MA, Winter JM, Cameron JL, et al. Pancreaticoduodenectomyin the very elderly. J Gastrointest Surg. 2006;10:347–356.
34. Cameron JL, Pitt HA, Yeo CJ, et al. One hundred and forty-fiveconsecutive pancreaticoduodenectomies without mortality. Ann Surg.1993;217:430–435, discussion 435–438.
35. Afsari A, Zhandoug Z, Young S, et al. Outcome analysis of pancreati-coduodenectomy at a community hospital. Am Surg. 2002;68:281–284,discussion 284–285.
36. Bilimoria K, Bentrem D, Ko C, et al. Validation of the AJCC StagingSystem for Pancreatic Cancer. Cancer. 2007. In press.
37. Birkmeyer JD, Stukel TA, Siewers AE, et al. Surgeon volume andoperative mortality in the United States. N Engl J Med. 2003;349:2117–2127.
38. Birkmeyer JD, Warshaw AL, Finlayson SR, et al. Relationship betweenhospital volume and late survival after pancreaticoduodenectomy. Sur-gery. 1999;126:178–183.
39. Birkmeyer NJ, Goodney PP, Stukel TA, et al. Do cancer centersdesignated by the National Cancer Institute have better surgical out-comes? Cancer. 2005;103:435–441.
40. Finlayson EV, Goodney PP, Birkmeyer JD. Hospital volume and oper-ative mortality in cancer surgery: a national study. Arch Surg. 2003;138:721–725, discussion 726.
41. Gordon TA, Bowman HM, Tielsch JM, et al. Statewide regionalizationof pancreaticoduodenectomy and its effect on in-hospital mortality. AnnSurg. 1998;228:71–78.
42. Sosa JA, Bowman HM, Gordon TA, et al. Importance of hospitalvolume in the overall management of pancreatic cancer. Ann Surg.1998;228:429–438.
43. Begg CB, Cramer LD, Hoskins WJ, Brennan MF. Impact of hospitalvolume on operative mortality for major cancer surgery. JAMA. 1998;280:1747–1751.
44. Ayanian JZ, Zaslavsky AM, Fuchs CS, et al. Use of adjuvant chemo-therapy and radiation therapy for colorectal cancer in a population-basedcohort. J Clin Oncol. 2003;21:1293–1300.
45. Bickell NA, Chassin MR. Determining the quality of breast cancer care:do tumor registries measure up? Ann Intern Med. 2000;132:705–710.
46. Cress RD, Zaslavsky AM, West DW, et al. Completeness of informationon adjuvant therapies for colorectal cancer in population-based cancerregistries. Med Care. 2003;41:1006–1112.
47. Malin JL, Kahn KL, Adams J, et al. Validity of cancer registry data formeasuring the quality of breast cancer care. J Natl Cancer Inst. 2002;94:835–844.
48. Hawker GA, Coyte PC, Wright JG, et al. Accuracy of administrativedata for assessing outcomes after knee replacement surgery. J ClinEpidemiol. 1997;50:265–273.
49. Henderson T, Shepheard J, Sundararajan V. Quality of diagnosis andprocedure coding in ICD-10 administrative data. Med Care. 2006;44:1011–1019.
50. Kahn LH, Blustein J, Arons RR, et al. The validity of hospital admin-istrative data in monitoring variations in breast cancer surgery. Am JPublic Health. 1996;86:243–245.
Bilimoria et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins180

EDITORIAL
Underutilization of Surgical Resection in Patients WithLocalized Pancreatic Cancer
Taylor S. Riall, MD,* and Keith D. Lillemoe, MD†
Pancreatic cancer remains the fourth leading cause of cancer deaths in men and womenin the United States. Ductal carcinoma (adenocarcinoma) is the most common form,
with an annual incidence of approximately 9 cases per 100,000 people. In 2006, there werean estimated 33,730 cases of pancreatic cancer diagnosed and 32,300 deaths from thedisease. The mean age at diagnosis is 70 years. The incidence is roughly equal in malesand females, but slightly higher in African Americans compared with that in Caucasians.The overall 5-year survival rate is less than 4%.1
Approximately two-thirds of patients with pancreatic cancer present with advancedstage disease. Such patients are not candidates for surgical resection. Chemotherapy andradiotherapy regimens, although modestly improving survival, are not curative. Forpatients with locoregional disease, surgical resection is the only hope for long-termsurvival or cure. Over the last 3 decades, the mortality after pancreatic resection forpancreatic cancer at high-volume centers (�25 cases per year) has decreased to less than5%, and the 5-year actuarial survival after resection has improved to 15% to 30%.2–4
Finally, in response to critics who suggest that the actuarial survival reported inthese studies overestimates 5-year survival,5 a recent report evaluating actual 5-yearsurvival after resection for pancreatic and other periampullary cancers demonstrated anactual 5-year survival rate of 17%. In addition, of those patients who survived to the5-year landmark, 55% survive to the 10-year landmark.6
Although clear evidence supports surgical resection as the standard of care forpatients with locoregional pancreatic cancer, surgical resection remains underutilized. Ina recent population-based study by Cress et al using the California tumor registry,7 only35% of patients with locoregional disease underwent surgical resection. Likewise, in arecent population-based study using the SEER tumor registry data, only 27% of patientswith locoregional disease underwent surgical resection.8 The percentage of patientsundergoing surgical resection did increase from 19% to 31% over the period of 1988 to2001. However, although this trend is promising, still less than one-third of patients withlocoregional disease are being resected.
Bilimoria and colleagues in this issue of Annals of Surgery use data from theNational Cancer Data Bank (NCDB) to evaluate and characterize the reasons for theobserved underutilization of surgery in patients with localized pancreatic cancer. Similarto previous reports, only 28.6% of patients with clinical stage I pancreatic cancerunderwent surgical resection. Between 1995 and 2004, the percentage of patients resectedincreased from 21.8% to 35.7%. Although encouraging, surgical resection is still strik-ingly underutilized.
In the analysis of those patients not undergoing pancreatic resection, 51.7% did nothave an identifiable reason for not undergoing potentially curative resection (38.2% notoffered surgery and 13.5% unknown reason), and the remaining 19.4% refused surgery(4.2%), cited age as a contraindication (9.1%), or had too many comorbidities (6.4%). Ina multivariate analysis, patients who were older, black, had a lower annual income, less
From the *Department of Surgery, University of Texas Medical Branch, Galveston, TX; and †Department of Surgery, Indiana University School of Medicine,Indianapolis, IN.
Reprints: Taylor S. Riall, MD, Assistant Professor of Surgery, Department of Surgery, University of Texas Medical Branch, 301 University Boulevard, JohnsSealy Annex 6.312b, Galveston, TX 77555-0542. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0181DOI: 10.1097/SLA.0b013e31811eaa2c
© 2007 Lippincott Williams & Wilkins 181

education, Medicare or Medicaid insurance, lesions in thepancreatic head, or were seen at a low-volume center orcommunity hospital were less likely to undergo surgery. Inaddition, patients seen at NCI designated cancer centers weremore likely to undergo surgical resection.
The analysis by Bilimoria and colleagues providesinsight into the reasons for underutilization of surgery inpatients with localized pancreatic cancer. However, this anal-ysis needs to be expanded. First, the authors limited theiranalysis to clinical stage I (T1N0M0) patients. These resultswould also likely apply to patients with more advanced, butresectable, regional disease with even more striking under-utilization of pancreatic resection expected.
Some of these patients with locoregional disease maynot be candidates for surgical resection based on individualcharacteristics such as severe comorbidities or tumor charac-teristics such as major vascular involvement. However, if themore favorable stage I patients reported in this series arebeing inappropriately denied surgical resection, it is likelythat this could be even more pronounced for more formidabletumors.
We hypothesize that the main reasons why people donot receive surgical resection for locoregional pancreaticcancer are 2-fold. First, they may never be evaluated by asurgeon due to the nihilistic views of their primary physi-cian including oncologists and gastroenterologists. In ourpreliminary analysis of SEER-Medicare data, only 75% ofpatients with locoregional pancreatic cancer underwentsurgical evaluation (data unpublished). Second, these pa-tients are evaluated by a surgeon who is not experienced inperforming pancreatic resection. This latter point providesfurther evidence to support the referral of these patients toregional high-volume centers, which have been consis-tently demonstrated to improve both short-term and long-term survival.9 –12
Finally, these types of studies should be extended toinclude referral to and treatment of pancreatic cancer bynonsurgical oncology specialists. New and effective regimensfor neoadjuvant, adjuvant, and palliative therapy13 are alsolikely being denied to a large proportion of patients. The datafrom this study and those of our group and others support theidea of regionalizing the care of pancreatic cancer patients toexperienced centers or surgeons. The data should be used togenerate health policy for patients with locoregional pancre-atic cancer. We can define minimal appropriate care stan-dards for patients with locoregional pancreatic cancer toassure adequate assessment of resectability from both a tech-nical standpoint and based on patient comorbidities. “Appro-priate care” should include the steps necessary to make aninformed decision on appropriate treatment. We feel that allpatients with locoregional pancreatic cancer should: (1) un-dergo state-of-the-art abdominal imaging, either with pan-creas protocol 3D-computed tomography or MRI, (2) be
evaluated by a qualified, experienced pancreatic surgeon, and(3) be evaluated by a medical oncologist.
In conclusion, although scientists and clinicians strivefor screening tools for earlier diagnosis and to develop betterchemotherapy and other novel therapies for pancreatic can-cer, surgical resection currently remains the only potential forcure. Although such efforts are of major importance, bysimply maximizing rates of surgical resection, for all appro-priate surgical candidates, we can make an immediate im-provement in survival and impact thousands of patients.
The article by Bilimoria and colleagues is certainlyappropriate for Annals of Surgery. However, this informationneeds to be disseminated to a wider audience. The nihilisticattitude toward pancreatic cancer is likely at the level of theprimary care physician or internists who are the first line ofphysicians who see these patients. To influence practice andimprove care for these patients, this message needs to bedelivered to primary care physicians, gastroenterologists,general surgeons, medical oncologists, and the community.Finally, we need to make easily accessible referral networkssuch that all patients with locoregional pancreatic cancer getan adequate and experienced assessment for resectability.
REFERENCES1. Jemal A, Siegel R, Ward E, et al. Cancer Statistics, 2006. CA Cancer
J Clin. 2006;56:106–130.2. Winter JM, Cameron JL, Campbell KA, et al. 1423 Pancreaticoduo-
denectomies for pancreatic cancer: a single institution experience.J Gastrointest Surg. 2006;10:1199 –1211.
3. Conlon KC, Klimstra DS, Brennan MF. Long-term survival after cura-tive resection for pancreatic ductal adenocarcinoma. Clinicopathologicanalysis of 5-year survivors. Ann Surg. 1996;223:273–279.
4. Yeo CJ, Sohn TA, Cameron JL, et al. Periampullary adenocarcinoma:analysis of 5-year survivors. Ann Surg. 1998;227:821–831.
5. Gudjonsson B. Survival statistics gone awry: pancreatic cancer, a case inpoint. J Clin Gastroenterol. 2002;35:180–184.
6. Riall TS, Cameron JL, Lillemoe KD, et al. Resected periampullarycancer: 5-year survivors and their 6- to 10-year follow-up. Surgery.2006;140:754–762.
7. Cress RD, Yin D, Clarke L, et al. Survival among patients withadenocarcinoma of the pancreas: a population-based study. CancerCauses Control. 2006;17:403–409.
8. Riall TS, Freeman JL, Townsend CM Jr, et al. Pancreatic cancer in thegeneral population: Improvements in survival over the last decade.J Gastrointest Surg. 2006;10:1212–1224.
9. Fong Y, Gonen N, Rubin D, Radzyner M, Brennan MF. Long-termsurvival is superior after resection for cancer in high-volume centers.Ann Surg. 2005;242:540–547.
10. Gordon TA, Bowman HM, Tielsch JM, Bass EB, Burleyson GP,Cameron JL. Statewide regionalization of pancreaticoduodenectomy andits effect on in-hospital mortality. Ann Surg. 1998;228:71–78.
11. Birkmeyer JD, Warshaw AL, Finlayson SRG, Grove MR, TostesonANA. Relationship between hospital volume and late survival afterpancreaticoduodenectomy. Surgery. 1999;126:178–183.
12. Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, Wennberg DE,Lucas FL. Surgeon volume and operative mortality in the United States.N Engl J Med. 2003;349:2117–2127.
13. Krzyzanowska MK, Weeks JC, Earle CC. Treatment of locally advancedpancreatic cancer in the real world: population-based practices andeffectiveness. J Clin Oncol. 2003;21:3409–3414.
Riall and Lillemoe Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins182

REVIEW
Hepatic Resection for Colorectal MetastasesValue for Risk Scoring Systems?
Shaheen Zakaria, MD,* John H. Donohue, MD,* Florencia G. Que, MD,* Michael B. Farnell, MD,*Cathy D. Schleck, BS,† Duane M. Ilstrup, MS,† and David M. Nagorney, MD*
Introduction: Predictors of outcome in patients with metastaticcolorectal cancer remain inconsistent. We aimed to identify predic-tors of outcome in these patients, to develop a prognostic scoringsystem, and to assess the general applicability of the current majorrisk scoring systems.Materials and Methods: Following IRB approval, medical recordsof 662 consecutive patients undergoing resection of colorectal me-tastases to the liver during 1960 to 1995 were reviewed. Clinico-pathologic and outcome data were assessed from records and mailedquestionnaire. Clinicopathologic variables were tested using univar-iate and multivariate analyses; best-fit models were then generatedto study the effect of each independent risk factor on outcome. Tovalidate existing scoring models, our independent data set wasapplied to those scores. The relative concordance probability esti-mates were calculated for these models and compared with that ofthe proposed Mayo model.Results: The overall and disease-specific 5-year survival rates were37% and 42%, respectively. The probability of recurrence at any sitewas 65% at 5 years. Perioperative blood transfusion and positivehepatoduodenal nodes were the major determinants of survival andrecurrence. To assess the general applicability of the proposed riskscoring systems, we imported the data from our patient populationinto 3 other scoring systems. Neither survival nor recurrence amongour patients was stratified discretely by any of the scoring systems.Based on probability estimates, all models were only marginallybetter than chance alone in predicting outcome.Conclusion: Broad application of risk scoring systems for patientswith metastatic colorectal cancer has limited clinical value and refine-ment and external validation should be undertaken before utilization.
(Ann Surg 2007;246: 183–191)
Hepatic resection of metastatic colorectal cancer has be-come the treatment of choice for selected patients after
resection of the primary colorectal cancer. Despite variability
in criteria for patient selection, survival outcomes haveranged consistently from 25% to 45%.1–6 These data havesupported repeatedly the clinical contention that cure isachieved in some of these patients because of the long-term(�5 years) absence of recurrence7–9 and the disparate sur-vival compared with the natural history of similar patient co-horts with unresected hepatic metastases.10–12 Although selec-tion criteria for resection have expanded over the last 2 decades,the specific criteria for selection remain controversial.
Patient selection for resection of hepatic metastases forcolorectal cancer is based primarily on documentation ofresectable intrahepatic disease and exclusion of extrahepaticdisease with the exception of selected pulmonary metastases.However, despite numerous studies correlating patient, tu-mor, and interventional factors to survival,3–6,13 reliable pre-dictors of survival in patients with metastatic colorectalcancer remain inconsistent. To refine candidacy for selectionof patient for resection and for adjuvant therapy, severalprognostic scoring systems have been proposed to stratifypatients into risk categories for clinical management.4–6,14–16
Although these scoring systems have a sound statistical andclinical validity within referral centers, general applicabilityto more heterogeneous patient populations has not beenconfirmed. Predictive scoring models calculated on quantita-tive data have numerous benefits. Such models permit accu-rate comparisons of patient populations among studies, pro-vide proper prognostic information to the patient, and, ifdistinct stratification levels are evident, guide treatment strat-egies and stratification of patients among institutions. Scoringmodels should be validated independently before generalizedapplication and acceptance. Although prospective validationof scoring systems is preferable, the actual frequency ofpatient accrual for hepatic resection of colorectal metastasesand duration of follow-up required to assess survival (5 years)limit this approach. As an alternative for validation and todetermine whether currently proposed risk scoring systemswere applicable to our independent patient population, wehave updated our experience with hepatic resection of meta-static colorectal cancer and have imported our findings into 3proposed scoring systems4–6 to determine whether outcomesfor risk stratification were similar.
Specifically, we assessed the mortality, survival, andrecurrence patterns among our patients with hepatic resectionfor colorectal metastases. We attempted to identify predictorsof outcome from our patient population and develop a scoring
From the Divisions of *Gastroenterologic and General Surgery and †Biosta-tistics, Mayo Clinic and Mayo Foundation, Rochester, Minnesota, MN.
Reprints: David M. Nagorney, MD, Mayo Clinic, 200 First Street SW,Rochester, MN 55905. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0183DOI: 10.1097/SLA.0b013e3180603039
Annals of Surgery • Volume 246, Number 2, August 2007 183

system. The issue of general applicability of several currentlyproposed risk scores was addressed by calculating survivalbased on the number of specific risk factors cited in thestratification schemes of those risk scoring systems. Weevaluated patients managed within the time frame duringwhich those scoring systems were developed to provide asimilar patient population because current outcomes follow-ing resection of metastatic colorectal cancer to the liver maydiffer from earlier reports.
MATERIALS AND METHODSFollowing approval of the Mayo Clinic Institutional
Review Board, the medical records of 662 consecutive pa-tients who underwent resection of colorectal metastases to theliver during the period 1960 to 1995 were reviewed. Histo-pathology of each metastasis confirmed metastatic colorectalcancer. Patients who had initial hepatic resection elsewhere(n � 10) or had only local ablative therapy (n � 7) wereexcluded.
DefinitionsThe primary colorectal cancer was staged using UICC/
AJCC staging system for colorectal cancer.17 Synchronousliver metastases were defined as those detected within 3months of diagnosis of primary colorectal cancer. The ana-tomic distribution of liver lesions was defined by Couinaudnomenclature.18 Size of the liver lesion was measured by thepathologist, in centimeters, before fixation of the specimen.The Broder’s system17 was used to histologically grademetastases. Surgical margins were defined by histology aseither cancer negative or positive. Margin of resection wasmeasured in centimeters by the pathologist, before fixation ofthe specimen. Blood transfusions 1 week prior to and/or 2weeks following hepatic resection were defined as perioper-ative. Postoperative mortality was defined as death occurringin the hospital or within 60 days of resection.
Follow-upQuestionnaires were sent to all patients who had an
incomplete follow-up. Two mailings were done for nonre-sponders, and after that the patients were labeled as lost tofollow-up. The results are reported.
The follow-up was complete, until death or within 1year of data collection, in 93% of the patients.
EndpointsThe primary endpoints of this study were overall sur-
vival, disease-specific survival, and recurrence at the mostrecent follow-up evaluation. Overall survival was defined asthe time interval between the date of hepatic resection and thedate of death or most recent date of follow-up if the patientwas alive. Disease-specific survival was defined as the timefrom hepatic resection to death from primary cancer. Patientswho died in the postoperative period or during hospitalizationwere excluded from the survival analysis. Recurrence wasdefined as the time from hepatic resection to first documenteddisease recurrence. The probability of recurrence representsthe chance of developing the first recurrence at 5 years. Thecriteria for establishing recurrent disease were histologic
confirmation, radiologic evidence of progression with subse-quent clinical progression, and supportive biochemical data(eg, rising serum level of carcinoembryonic antigen, CEA).Patients with recurrence were defined in terms of local,hepatic, or distant recurrence. Local recurrence was confinedto the colon, rectum, pelvis, or adjacent organs. Recurrence inthe liver was defined as a new lesion detected in the livermore than 1 month after hepatic resection; other extrahepaticrecurrences were labeled as distant.
Surgical ProceduresMajor liver resection was defined as right hepatectomy
(segments V, VI, VII, and VIII), extended right hepatectomy(segments IV, V, VI, VII, and VIII), left hepatectomy (seg-ments II, III, IV � I), extended left hepatectomy (segments II,III, IV, V, VIII � I) or resection of more than 2 liversegments.19 Liver resections were defined as minor if sub-segmental, unisegmental, or bisegmental.
Statistical AnalysisData are presented as median (range) or mean (standard
deviation). The Kaplan-Meier method was used to analyzesurvival and recurrence patterns. The study period providedpotential follow-up of a minimum of 5 years for patientssurviving operation; thus, survival was actual. Two-tailedlog-rank test was used to assess differences between num-bers. Sixteen clinicopathologic variables were tested for theireffect on overall survival, disease-specific survival, and prob-ability of recurrence using univariate analysis. The statisti-cally significant variables were used to construct a multiva-riable model using the Cox proportional hazards method(backward elimination method). Using parameter estimates,best-fit models were generated to study the effect of eachindependent risk factor on outcome. A 2-sided P value of�0.05 was considered statistically significant. Patients withmissing variables were excluded from multivariable analysisand model building.
The predictive accuracy of our model was evaluated bycalculating the concordance probabilities. The concordanceprobability is defined as the proportion of all possible pairs ofobservations in the data in which the ordering of that patientpair as predicted by the model agrees with the observedoutcome (ignoring tied survival times).20 Values range from0 to 1, with values close to 1 indicating that the model almostperfectly discriminated between patients with higher andlower risks of death (or recurrence), while values close to 0.5suggested that the predictive ability of the model was nobetter than chance alone. Ninety-five percent confidenceintervals (CIs) for the estimated concordance were calculatedusing bootstrap resampling with 1000 replications.
Evaluation of Proposed Risk ScoresSeveral institutions have proposed risk scoring systems
with the aim of optimizing patient selection for hepatic resectionand to stratify patients for the need of adjuvant therapies.Scoring systems proposed by Schindl et al16 (n � 131, includesstage of colorectal cancer, number of liver metastases, CEAlevels, albumin and alkaline phosphatase levels), Ueno et al14 etal (n � 85, includes aggressiveness of primary tumor, early liver
Zakaria et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins184

metastases, number of liver metastases), and Lise et al15 (n �135, includes percentage of liver invasion, metastases to lymphnodes at the primary tumor site, number of liver metastases,preoperative glutamic pyruvic transaminase levels, and type ofliver resection) have been developed on small study populationsand their clinical utility has not been established. Three otherscoring systems were developed on large patient populations.Nordlinger et al,4 through a national collective registry of 1513patients, developed a prognostic scoring system based on 7identified risk factors: age �60 years; primary cancer extendinginto serosa; positive regional lymph nodes; liver metastasesconfirmed within 24 months of the primary cancer; CEA levels;size of metastasis greater than 5 cm and �1 cm resection marginof the metastases. Three risk groups were defined: low risk (0–2risk factors), intermediate risk (3 or 4 risk factors), and high risk(5–7 risk factors). Fong et al,6 through a single institution studyof 1001 patients, similarly devised a system based on nodepositive primary cancer, hepatic metastases confirmed within 12months of the primary cancer, �1 metastases, size of metastasis�5 cm, and CEA level �200 ng/mL. Six risk groups werestratified by the sum of the individual prognostic variables.Iwatsuki et al,5 also through a single institution study of 230patients, proposed a risk-score based on �3 hepatic metastases,size of metastasis �8 cm, hepatic metastases confirmed within�30 months of the primary cancer, and bilobar hepatic metas-tases. Five risk grades were stratified based on the sum of theindividual prognostic variables: grade 1 being no risk factorpresent to grade 5, including patients with 4 risk factors. These3 scoring systems were chosen for validation utilizing data fromour institution.
Statistical methods used to construct these risk scoringsystems, though similar, varied by method. To validate thesescoring models, our independent data set was applied to eachof the 3 major risk scoring systems. We used each describedscoring criteria to stratify our patients to determine thegeneral applicability of each scoring system. The predictiveaccuracy of these models was determined using relativeconcordance probability estimates which were then comparedwith that of the proposed Mayo model.
RESULTS
Patient PopulationBetween 1960 and 1995, 662 consecutive patients un-
derwent resection of hepatic metastases from colorectal can-cer. There were 404 men and 258 women. Mean age was60 � 11 years and did not differ by gender.
Primary Tumor CharacteristicsThe primary cancer was located in the colon in 497
patients (right, 154; transverse, 39; left, 57; sigmoid, 247) andin the rectum in 166. At the time of initial presentation, 49(7.7%) patients had stage I and 193 (30.3%) had stage IIcolon cancer. Stage III represented the largest group with 291patients (45.7%), while 104 (16.3%) patients had stage IVdisease. Staging of the primary cancer was unavailable for 25patients. Two percent of tumors were Broder’s grade 1,67.8% grade 2, 28.7% grade 3, and 1.5% grade 4. Data ontumor grade were absent for 119 patients.
Liver MetastasesHepatic metastases were identified synchronously (ie,
within 3 months of primary operation) in 221 (33.4%) pa-tients. A total of 396 patients (59.9%) had a solitary metas-tasis, 198 (30%) had 2 or 3 metastases, and 68 patients (10%)had 4 or more metastases. The median size of the metastaseswas 4.5 cm (range, 0.2–26 cm). The hepatic metastases wereunilobar in 502 (75.8%) patients and bilobar in 160 (24.2%).
The metastases were histologically grade 2 in 380(58.3%), grade 3 in 259 (39.7%), and grade 4 in 13 (2%)patients. Tumor grade was not assessable for 10 patients. Thefrequency distribution of tumor grade for the hepatic metas-tases showed significant dedifferentiation compared with thedistribution of the primary cancer (P � 0.0001).
Surgical ResectionsThe frequency of minor resections (356; 54%) and major
resections (306; 46%) was similar (Table 1). A total of 350patients (56%) received blood transfusions perioperatively, butthe frequency of blood transfusions has decreased over time.
Although each patient had complete resection of themetastases macroscopically, 62 (9.4%) patients had microscop-ically positive pathologic surgical margins. Pathologic marginswere microscopically negative in 478 (72.1%) and were notassessable by pathology report in 122 (18.4%) patients.
Of 662 patients undergoing hepatic resection, 100 alsohad extrahepatic disease. The majority (44) had involvement ofother organs by direct extension: diaphragm (n � 21), perineph-ric fascia (n � 3), extrahepatic portal vein (n � 9), extrahepaticbiliary tree (n � 6), and abdominal wall (n � 5). Hepaticresection was performed in the setting of discontiguous extra-hepatic metastases in 56 cases: portal nodal disease (n � 36),pulmonary metastases (n � 10), peritoneal disease (n � 7), andpelvic metastases (n � 3). Adjuvant chemotherapy (primarily5-fluorouracil based) was administered to 207 (33.3%) patients.
Surgical MortalityThe 30- and 60-day mortality was 2% and 3%, respec-
tively. Of the 19 deaths, 5 patients had minor and 14 patientshad major liver resection. Causes of death were abdominalsepsis (4), hepatic failure (4), bleeding from liver parenchyma(2), unknown (4), abdominal wound dehiscence (2), myocar-dial infarction (1), pulmonary embolism (1), and brainsteminfarction (1).
TABLE 1. Type and Frequency of Hepatic Resection inPatients With Metastatic Colorectal Cancer
Type of Resection n %
Wedge 243 36.7
Right hepatectomy 108 16.3
Left hepatectomy 31 4.7
Extended right hepatectomy 101 15.3
Extended left hepatectomy 8 1.2
One segment � wedge 41 6.2
Two segments � wedge 72 10.8
Three or 4 segments � wedge 58 8.8
Annals of Surgery • Volume 246, Number 2, August 2007 Hepatic Resection for Colorectal Metastases
© 2007 Lippincott Williams & Wilkins 185

Long-Term OutcomesOverall median follow-up for the study period was 3
years (range, 5 days to 37 years). At last follow-up, 234(35%) patients were alive and 428 (65%) were dead. Recur-rence at any site was diagnosed in 414 (62.5%) patients; 215(32.5%) patients remained free of disease. The disease statuswas uncertain in 33 (5%) patients. Recurrent hepatic metas-tases after initial hepatic resection developed in 208 (31%)patients and were removed surgically in 28 (12%) patients.
Survival and RecurrenceThe overall and disease-specific 5-year survival were 37%
and 42%, respectively (Fig. 1A, B). The probability of tumorrecurrence after hepatic resection is shown in Fig. 1C. Thecumulative probability of developing a recurrence at any sitewas 65% at 5 years. Eighty percent of patients developedrecurrence within 3 years of the hepatic resection. The distribu-
tion sites of recurrence or metastases was in the liver in 224(34%), lung in 171 (26%), and other sites in 18 (28%) patients.
Resection of recurrent hepatic metastases was possiblein 28 patients and was associated with an actuarial 5-yearsurvival rate of 73%.
Analysis of Risk FactorsAll host and tumor factors were correlated to overall
survival, disease-specific survival, and recurrence (Table 2).Patients who died postoperatively were excluded from riskanalysis.
Univariate AnalysisDisease-specific survival was significantly reduced for the
following factors: site of primary cancer in the rectum, hepaticmetastases confirmed within 30 months of the primary colorec-tal cancer, �1 hepatic metastasis, size of metastases �8 cm,
FIGURE 1. Overall expected and observed survival (A) and disease-specific survival (B) of patients undergoing hepatic resec-tion for colorectal metastases. C, Recurrence of patients undergoing hepatic resection for colorectal metastases.
TABLE 2. Correlation of Clinical and Pathologic Factors to Disease-Specific Survival and Recurrence: Univariate Analysis (RiskFactor Analysis)
Risk Factor
Disease-Specific Survival Recurrence
n 5 yr (%) 95% CI 10 yr (%) 95% CI P 5 yr (%) 95% CI 10 yr (%) 95% CI P
Host factors
Gender 0.17 0.39
M 379 40.5 35.2, 46.4 31.3 24.5, 37.8 65.3 59.4, 70.6 68.3 60.9, 74.8
F 246 46.6 40.1, 54.2 35.2 28.0, 44.1 65.3 58.3, 71.3 67.7 60.4, 75.7
Age 0.95 0.45
�60 yr 294 41.3 35.4, 48.1 32.1 25.6, 39.9 66.1 59.7, 71.6 68.7 61.4, 74.9
�60 yr 331 44.3 38.6, 50.7 32.8 26.5, 40.5 64.3 57.9, 70.1 66.9 60.1, 74.9
Primary tumor
Site 0.02 0.56
Colon 462 45.4 40.5, 50.8 34.4 28.9, 40.9 66.5 56.9, 74.5 73.7 58.6, 84.0
Rectum 157 36.1 28.1, 45.3 26.8 17.3, 36.5 64.7 59.5, 69.3 66.4 61.0, 72.8
Stage 0.28 0.26
I 48 55.5 41.0, 74.4 40.2 23.8, 65.1 59.7 40.7, 72.6 59.7 40.7, 76.6
II 183 41.1 33.7, 49.8 34.9 25.3, 44.1 59.5 50.9, 66.7 62.9 53.3, 71.2
III 276 39.8 33.8, 46.8 30.6 23.9, 38.7 68 61.1, 73.9 70.1 62.8, 78.6
IV 93 48.8 38.3, 61.1 27.2 16.1, 46.1 69.9 57.4, 79.3 72.6 59.4, 87.1
Colonic nodes 0.11 0.01
Neg. 292 46.6 40.6, 53.4 35.3 28.7, 43.4 58.8 52.2, 64.7 62.8 55.3, 69.5
Pos. 333 39.6 34.1, 46.0 29.9 23.8, 37.4 71 64.9, 76.4 72 65.7, 89.7
(Continued)
Zakaria et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins186

hepatoduodenal lymph node metastases, perioperative bloodtransfusion, and adjuvant chemotherapy (Table 2).
Disease recurrence was significantly associated withthe following factors: stage III and IV colorectal cancer at
initial presentation, �1 hepatic metastasis, bilobar hepaticmetastases, positive hepatoduodenal lymph nodes, positivemargins after hepatic resection, and perioperative bloodtransfusions.
TABLE 2. (Continued)
Risk Factor
Disease-Specific Survival Recurrence
n 5 yr (%) 95% CI 10 yr (%) 95% CI P 5 yr (%) 95% CI 10 yr (%) 95% CI P
Hepatic metastases
Interval 0.14 0.52
�6 mo 206 36 29.2, 44.0 24 17.0, 33.8 66.5 58.4, 73.4 70.6 61.8, 81.0
6–12 mo 73 50 38.9, 64.0 42.5 29.9, 58.0 58.9 44.2, 69.8 58.9 44.2, 73.4
12–18 mo 92 43.3 32.4, 56.3 37.1 23.1, 55.4 61.4 48.3, 71.3 64.2 50.3, 77.5
18–24 mo 63 42.5 30.6, 58.9 34.1 20.2, 53.6 68.9 53.7, 79.3 76.6 53.4, 88.3
24–30 mo 42 28.4 15.3, 50.9 23.7 9.0, 46.9 73.1 53.3, 85.8 73.1 53.3, 89.1
�30 mo 122 54.4 44.8, 65.4 38.6 25.1, 51.5 65.5 55.0, 74.2 65.5 55.0, 82.2
No. tumors 0.03 �0.001
1 371 46.4 41.1, 52.2 35.5 29.7, 42.2 59.9 54.1, 65.1 63 56.6, 68.9
2, 3 193 40.2 32.3, 49.3 28.6 19.2, 42.7 71.8 63.3, 78.6 73.7 64.6, 84.3
�4 61 29.1 18.8, 45.1 21 10.1, 37.4 79 64.2, 88.9 79 64.2, 93.6
Size (cm) 0.08 0.15
�2 83 36.4 26.4, 49.6 20.2 9.8, 41.3 59.1 45.8, 70.0 65.7 50.2, 81.5
�2–�5 289 46.6 40.4, 53.5 36.5 28.5, 44.6 64.9 58.1, 70.6 65.9 58.9, 74.1
�5–�10 178 43.7 36.0, 53.1 32.4 24.2, 43.3 64.5 55.7, 71.7 68.3 58.2, 76.8
�10 65 37.8 26.1, 52.5 31.2 18.1, 47.7 72 56.8, 82.2 72 56.8, 85.9
Distribution 0.73 0.03
Unilobar 475 43.1 38.4, 48.3 32.4 27.3, 38.4 63.4 58.2, 68.0 66.4 60.8, 71.6
Bilobar 150 42.2 33.2, 52.7 33.7 21.4, 45.5 71.1 61.6, 78.5 71.1 61.6, 87.1
Differentiation 0.28 0.53
Grade 1 0
Grade 2 366 38.4 33.2, 44.5 29.6 23.2, 36.0 66 61.1, 71.1 68.7 62.2, 74.5
Grade 3 236 48 41.0, 55.6 35.8 27.8, 45.6 65 57.5, 71.3 66.2 58.4, 76.0
Grade 4 13 60.6 34.4, 94.7 30.3 7.1, 100.0 71.2 29.7, 88.2 85.6 25.1, 97.2
CEA levels (ng/mL) 0.48 0.16
�5 72 50.9 38.3, 65.8 36.1 22.2, 58.8 55.5 41.5, 68.3 63.6 46.2, 80.3
�5–�50 186 55 47.3, 63.8 46.4 36.7, 56.6 61 52.4, 68.1 63.5 53.7, 71.6
�50–�100 64 42.9 30.9, 58.5 32.4 17.0, 51.1 67.8 52.2, 79.2 67.8 52.2, 85.3
�101–�200 30 43.1 26.8, 67.6 28.7 9.3, 71.9 65.7 39.4, 80.6
�200 32 52.5 34.4, 78.4 35 14.3, 70.0 78.7 57.3, 90.0 78.7 57.9, 92.6
Operation
Margins 0.13 0.05
Neg. 453 48 43.1, 53.5 37.9 32.2, 44.6 62.4 57.2, 67.1 65.4 59.6, 70.8
Pos. 59 35.4 23.1, 53.2 31.5 16.8, 50.3 80.1 61.4, 70.4 80.1 61.4, 92.2
Type of resection 0.45 0.33
Major 284 45.6 39.5, 52.6 38.6 31.5, 46.4 65.5 58.9, 71.0 68 60.6, 74.6
Minor 341 40.9 35.4, 47.1 27.3 21.4, 34.9 65.1 58.9, 70.7 67.7 61.1, 75.3
Hepatoduodenal nodes �0.001 �0.001
Clinically neg. 399 37.7 32.7, 43.3 27.5 22.3, 33.6 65.3 59.7, 70.2 68 61.7, 73.7
Histologically neg. 190 58.1 50.5, 66.6 47.6 38.0, 58.8 59.6 51.1, 66.9 62.3 53.3, 72.4
Histologically pos. 35 18.8 6.3, 48.9 9.4 1.8, 50.7 94.6 66.7, 99.1
Periop. transfusion �0.001 0.03
No 266 51.9 45.3, 59.3 42.6 34.7, 51.7 60.4 53.3, 66.5 64.1 56.0, 71.3
Yes 328 35.7 30.3, 41.9 27.4 20.5, 34.0 69.6 63.3, 74.9 70.4 64.1, 78.2
Adjuvant chemotherapy 0.07 0.62
No 389 42.2 37.1, 48.1 30.7 25.1, 37.5 62.9 57.2, 68.1 66.9 60.4, 72.6
Yes 197 46.1 38.9, 54.5 36.9 27.4, 46.6 71 63.2, 77.1 71 63.2, 82.1
Annals of Surgery • Volume 246, Number 2, August 2007 Hepatic Resection for Colorectal Metastases
© 2007 Lippincott Williams & Wilkins 187

Multivariable AnalysisMultivariable analysis was performed on those factors
correlating significantly to disease-specific survival and re-currence by univariate analysis (Table 3). Disease-specificsurvival was significantly associated with metastases con-firmed in an interval of �30 months after the diagnosis ofprimary colorectal cancer and size of metastases �8 cm. Thesurvival hazard ratio was 1.4 in the presence of either of thesefactors. Perioperative blood transfusion and positive hepa-toduodenal lymph nodes were associated with 1.5 and 2.8times the risk of death, respectively. For recurrence, stage III
colorectal cancer, �1 hepatic metastasis, perioperative bloodtransfusions, and positive hepatoduodenal nodes were asso-ciated with hazard ratio of 1.3 to 2.5.
Clinical Risk ScoreTo study the effect of each statistically significant
factor from multivariate analysis on long-term outcome, best-fit models were generated. These variables were organizedinto 3 groups, using disease-specific survival as the outcomevariable (Table 4). Patients with any risk factors except forperioperative blood transfusion and positive hepatoduodenallymph nodes comprised group I. Patients having any riskfactors except for positive hepatoduodenal lymph nodes com-prised group II. Patients with positive hepatoduodenal lymphnodes, with or without any other risk factor, comprised groupIII. The disease-specific survival of these 3 groups is shownin Figure 2A. Five-year disease-related survival was 55% ingroup I, 39% in group II, and only 20% in group III.
Recurrence as the outcome variable was analyzed sim-ilarly (Table 4). Patients with no risk factors comprised groupI, those with any risk factor except for positive hepatoduo-denal lymph nodes comprised group II, and patients withpositive hepatoduodenal lymph nodes regardless of the pres-ence of any other risk factor comprised group III. At 5 years,46% of patients develop recurrence in group I, 67% in groupII, and 95% in group III (Fig. 2B). This risk analysis showedthat perioperative blood transfusion and positive hepatoduo-
TABLE 3. Correlation of Clinical and Pathologic Factors to Disease-Specific Survival and Recurrence: Multivariable Analysis
Variable
Survival Recurrence
Hazard Ratio 95% CI P Hazard Ratio 95% CI P
Metastasis diameter �8 cm 1.4 1.0–1.8 0.03
Interval to metastases �30 mo 1.4 1.0–1.9 0.03
Hepatoduodenal lymph node 2.8 1.8–4.4 0.0001 2.4 1.6–3.6 0.0001
Transfusions 1.5 1.2–2.0 0.0002 1.3 1.1–1.6 0.009
Primary cancer regional lymph node 1.3 1.1–1.6 0.01
No. metastases �2 1.3 1.1–1.6 0.01
TABLE 4. Best-Fit Models
Group1
Group2
Group3
With disease-specific survival as outcomevariable
Metastasis �30 mo � � �
Metastasis diameter �8 cm � � �
Transfusions � � �
Hepatoduodenal lymph node � � �
With recurrence as outcome variable
Primary cancer regional lymph nodes � � �
No. metastases �2 � � �
Transfusions � � �
Hepatoduodenal node � � �
FIGURE 2. Mayo Risk Groups. (A) Disease-specific survival (A) and recurrence (B) of patients undergoing hepatic resection forcolorectal metastases using best fit models.
Zakaria et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins188

denal lymph nodes were the 2 most important determinants oflong term survival and recurrence.
Evaluation of Proposed Risk ScoresTo assess the general applicability of the proposed risk
scoring systems, we imported the data from our patientpopulation into the 3 scoring systems (Material and Meth-ods).4–6 We used the same inclusion and exclusion criteriadetailed in the methodology for those respective scoringsystems. For the systems of Nordlinger et al4 and Fong et al,6
648 and 536 patients, respectively, met the outlined criteria.No patients were excluded from risk analysis proposed by theIwatsuki et al system.5 Figure 3 (A1, B1, C1) depicts thedisease-specific survival of our patients based on the criteriaof the 3 risk scoring systems. Figure 3 (A2, B2, C2) depictsthe probability of recurrence for the 3 scoring systems.Neither survival nor recurrence among our patients wasstratified discretely by any of the scoring systems. Survivalwas stratified best by the risk scoring system of Fong et al6
and least by that of Nordlinger.4 However, overlap of survival
FIGURE 3. Disease-specific survival (A1, B1, C1) and recurrence (A2, B2, C2) using existent scoring systems where A, B, and Crepresent Nordlinger, Fong, and Iwatsuki scores, respectively.
Annals of Surgery • Volume 246, Number 2, August 2007 Hepatic Resection for Colorectal Metastases
© 2007 Lippincott Williams & Wilkins 189

for various risk scores from each system is evident. Althoughsurvival between low- and high-risk scores for the systems ofFong and Iwatsuki diverged, only a risk score of 4 from theFong scoring system identified a patient subset without 5-yearsurvival among our patients. Similar limitations in stratifyingdisease recurrence for patients with resected hepatic metas-tases were evident for each of the scoring systems (Fig. 3 A2,B2, C2). Recurrence was again stratified best by the risk scoringsystem of Fong et al6 and least by that of Iwatsuki et al.5
Concordance probability estimates for disease-specificsurvival and recurrence for all the models are shown in Table5. Although the proposed Mayo model performed marginallybetter in discriminating patients at high/low risk of deathfrom disease, all models were only marginally better thanchance alone in predicting disease-specific survival and re-currence.
DISCUSSIONWe report a large, single-institution experience of he-
patic resection for colorectal metastases with a 5-year fol-low-up of 93%. Our study period spanned over 35 years.Although there are few large series reporting actual 5-yearsurvival, disease-specific survival herein was 42% at 5 years,32% at 10 years, and 26% at 15 years, which is consistentwith the predicted survival of other large series.1–8 Wecorrelated various clinical, pathologic, and interventionalfactors with survival and recurrence and developed a riskscoring system from factors that were significant by multiva-riable analysis. However, our risk scoring system had limitedutility and had only an average predictive accuracy based onconcordance probability estimates. Finally, we examinedother risk scoring systems to validate the usefulness forselecting patients for hepatic resection or subsequent adjuvanttreatment but similarly found limited utility and suboptimaldiscriminatory ability. Although our findings further confirmthe efficacy of hepatic resection of colorectal metastases, thebroad application of risk scoring systems currently has lim-ited clinical value.
Our study and numerous others4–6,10,14–16 have corre-lated a number of clinical, pathologic, and interventionalfactors with overall survival, disease-specific survival, andrecurrence for patients with resected hepatic metastases fromcolorectal cancer by univariate and multivariable analyses.Many of the correlates to survival have been reported previ-ously, but there remains inconsistency interinstitutionally.Indeed, even intrainstitutionally, correlates of survival havevaried.2,8 Selection of patients for hepatic resection of colo-rectal metastases has likely affected the consistency of the
correlates to survival. Most reports have spanned many yearsto decades to accumulate a substantive experience. Selectionof patients for operation initially was stringent because op-erative mortality was significant, the accuracy of imaging forstaging metastatic disease was limited, and the survival ben-efits for resection were unknown. Selection currently hasexpanded because accumulated evidence supporting survivalbenefit for resection has emerged, perioperative risk hasdecreased, and the accuracy of imaging has improved. In-deed, hepatic resection is the current treatment of choice formetastatic colorectal cancer if all disease grossly is resect-able. Indeed, even staged resections of hepatic metastases areundertaken with or without neoadjuvant chemotherapy toaccomplish complete resection.21
Our univariate analysis identified a number of variablesaffecting outcome. However, multivariable logistic regres-sion analysis identified only perioperative blood transfusionand positive hepatoduodenal lymph nodes as independent andclinically significant correlates of both survival and recur-rence. Unfortunately, neither variable is identifiable preoper-atively. Thus, the “Mayo Scoring System” has limited clinicalutility for selection of patients for operation or for furtherpreoperative imaging or staging but may be used to counselpatients postoperatively regarding prognosis and for selectionof various adjuvant therapies. Indeed, more aggressive adju-vant therapy may be warranted, particularly for those patientsat high risk as proposed by others.6 Interestingly, we haveobserved that significant predictors of survival and recurrencehave changed between reports from our center. Previously,satellite configuration of hepatic metastases and clinical de-tection of metastases were significant correlates.8 These ob-servations coupled with the differences in risk factors ob-served by others2,4–6,8,10,14–16 and the low concordanceprobability estimates suggest that stratification of patients byclinical and pathologic factors, although statistically sound,may be clinically unreliable and are not widely applicable forselection of patients for operation or a basis for comparison ofpatient cohorts between institutions unless validated.
The utility of a prognostic model or scoring system forhepatic metastases from colorectal cancer requires internaland external validation before general use.22 Methods ofinternal validation or reproducibility of a prognostic systemare based on data resampling techniques, such as bootstrap-ping. Although bootstrapping is widely accepted for internalvalidation, it is computer and labor intensive. Because we hadonly 2 independently significant variables, we did not per-form bootstrapping for internal validation. Moreover, internalstatistical validation techniques do not address the issue ofgeneralizability or general use. Generalizability or externalvalidity of a prognostic model can be tested by differentforms of validations, including prospective, independent,multi-institutional, and multiple independent validations withvarying follow-up periods.23 We attempted to address thegeneralizability of 3 current clinical scoring systems by use ofour patient population. These risk scoring systems failed toconfirm predictive stratification for our patients with meta-static colorectal cancer undergoing hepatic resection. Thisphenomenon or lack of validation has been observed and
TABLE 5. Concordance Probability Estimates
Model
Concordance Estimates (95% CI)
Disease-Specific Survival Recurrence
Mayo 0.61 (0.57, 0.64) 0.58 (0.55, 0.61)
Nordlinger 0.55 (0.51, 0.59) 0.56 (0.52, 0.59)
Fong 0.56 (0.50, 0.62) 0.58 (0.54, 0.63)
Iwatsuki 0.53 (0.50, 0.56) 0.55 (0.53, 0.58)
Zakaria et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins190

reported by others. Indeed, Iwatsuki et al5 failed to identify60% of their study population with the best prognosis basedon their scoring system after applying the French scoringsystem.4 Indeed, in repeat analysis of the French risk scoringsystem, only 3 of 7 risk factors significantly correlated withoutcome.7 These results confirm the necessity of externalvalidation of models of risk scoring between institutionsbefore general use for selection or comparison of data sets.Although statistical methods can ensure model reliability, itdoes not mean that data from 1 institution will fit exactly intoanother model addressing the same disease, but the clearstratification should be evident. Unrecognized selection bi-ases, population differences, risk of overfitting through toofew events per variable, changing diagnostic modalities, andmodifications in surgical techniques or other therapy may alladversely influence the transportability of risk scores betweeninstitutions. Finally, the actual duration and completeness offollow-up are particularly relevant to predictive models ofsurvival. Although the models4–6 addressed in this study hadsimilar mean duration of patient follow-up with appropriatelycomplete follow-up, the actual follow-up herein was substan-tially longer by design. It is unlikely that our prolongedfollow-up did not provide the opportunity for event of interestto occur as predicted by the other models. In other words,models developed on shorter durations of follow-up tend toless accurately predict survival and recurrences.
The remarkably consistent finding of this study, previ-ous reports from our institution, and other studies is thatlong-term survival occurs after potentially curative liver re-section.2,4–8,12 Despite extensive worldwide experience withliver resection for metastatic colorectal cancer, the issue ofpatient selection remains controversial. Neither the previ-ously proposed risk scores nor our Mayo scoring system canbe applied preoperatively for patient selection or interinstitu-tional comparison of patient populations. Risk scoring maybe appropriate for postoperative counseling of patients re-garding prognosis. Although current data suggest that the5-year survival of patients with a solitary hepatic metastasisexceeds 50% to 60% after hepatic resection,24 the overallsurvival of all patients undergoing hepatic resection for colo-rectal metastases is not great enough to obviate adjuvanttherapy on the basis of risk scoring to date.
CONCLUSIONCurrently, there are no reliable scoring systems for
selection of patients with hepatic metastases for resection.Hepatic resection should be undertaken if all gross diseasecan be addressed. The future development of risk scoringmodels for patients with colorectal cancer, while potentiallyimportant to patient and physician, will likely require largerpatient populations and analyses of additional clinicopatho-logic factors, such as genetic markers, to provide accuratestratification of patients and external confirmation for validityfor uses other than counseling of patients.
REFERENCES1. Registry of Hepatic Metastases. Resection of the liver for colorectal
carcinoma metastases: a multi-institutional study of indications forresection. Surgery. 1988;103:278–288.
2. Rosen CB, Nagorney DM, Taswell HF, et al. Perioperative bloodtransfusion and determinants of survival after liver resection for meta-static colorectal carcinoma. Ann Surg. 1992;216:493–504.
3. Scheele J, Rudroff C, Altendorf-Hofmann A. Resection of colorectalliver metastases revisited. J Gastrointest Surg. 1997;1:408–422.
4. Nordlinger B, Guiguet M, Vaillant JC, et al. Surgical resection ofcolorectal carcinoma metastases to the liver: a prognostic scoring systemto improve case selection, based on 1568 patients. Association Francaisede Chirurgie. Cancer. 1996;77:1254–1262.
5. Iwatsuki S, Dvorchik I, Madariaga JR, et al. Hepatic resection formetastatic colorectal adenocarcinoma: a proposal of a prognostic scoringsystem. J Am Coll Surg. 1999;189:291–299.
6. Fong Y, Fortner J, Sun RL, et al. Clinical score for predicting recurrenceafter hepatic resection for metastatic colorectal cancer: analysis of 1001consecutive cases. Ann Surg. 1999;230:309–321.
7. Jaeck D, Bachellier P, Guiguet M, et al. Long-term survival followingresection of colorectal hepatic metastases. Br J Surg 1997;84:977–980.
8. Jamison RL, Donohue JH, Nagorney DM, et al. Hepatic resection formetastatic colorectal cancer results in cure for some patients. Arch Surg.1997;132:505–510.
9. D’Angelica M, Brennan MF, Fortner JG, et al. Ninety-six five-yearsurvivors after liver resection for metastatic colorectal cancer. J Am CollSurg. 1997;185:554–559.
10. Lahr CJ, Soong S-J, Cloud G, et al. A multifactorial analysis ofprognostic factors in patients with liver metastases from colorectalcarcinoma. J Clin Oncol. 1983;1:720–726.
11. Wagner JS, Adson MA, van Heerden JA, et al. The natural history ofhepatic metastases from colorectal cancer. Ann Surg. 1984;199:502–507.
12. Scheele J, Stangl R, Altendorf-Hofmann A. Hepatic metastases fromcolorectal carcinoma: impact of surgical resection on the natural history.Br J Surg. 1990;77:1241–1246.
13. Rosen CB, Donohue JH, Nagorney DM. Liver resection for metastaticcolonic and rectal carcinoma. In: Cohen AM, et al, eds. Cancer of theColon, Rectum, and Anus. New York: McGraw-Hill; 1995:805–821.
14. Ueno H, Mochizuki H, Hatsuse K, et al. Indicators for treatmentstrategies of colorectal liver metastases. Ann Surg. 2000;231:59–66.
15. Lise M, Bacchetti S, Da Pian P, et al. Patterns of recurrence afterresection of colorectal liver metastases: prediction by models of outcomeanalysis. World J Surg. 2001;25:638–644.
16. Schindl M, Wigmore SJ, Currie EJ, et al. Prognostic scoring in colo-rectal cancer liver metastases: development and validation. Arch Surg.2005;140:183–189.
17. American Joint Committee on Cancer. AJCC Cancer Staging Manual,5th ed. Philadelphia: Lippincott-Raven; 1997:66–69.
18. Bismuth H. Surgical anatomy and anatomical surgery of the liver. WorldJ Surg. 1982;6:3–9.
19. Bismuth H, Houssin D, Casting D. Major and minor segmentectomies‘reglees’ in liver surgery. World J Surg. 1982;6:10–24.
20. Oakes DA. Concordance test for independence in the presence ofcensoring. Biometrics. 1982;38:451–455.
21. Meric F, Patt YZ, Curley SA, et al. Surgery after downstaging ofunresectable hepatic tumors with intra-arterial chemotherapy. Ann SurgOncol. 2000;7:490–495.
22. Altman DG, Royston P. What do we mean by validating a prognosticmodel? Stat Med. 2000;19:453–473.
23. Justice AC, Covinsky KE, Berlin JA. Assessing the generalizability ofprognostic information. Ann Intern Med. 1999;130:515–524.
24. Abdalla EK, Vauthey J-N, Ellis LM, et al. Recurrence and outcomesfollowing hepatic resection, radiofrequency ablation, and combinedresection/ablation for colorectal liver metastases. Ann Surg. 2004;239:818–827.
Annals of Surgery • Volume 246, Number 2, August 2007 Hepatic Resection for Colorectal Metastases
© 2007 Lippincott Williams & Wilkins 191

RANDOMIZED CONTROLLED TRIALS
Systemic Lidocaine Shortens Length of Hospital Stay AfterColorectal Surgery
A Double-blinded, Randomized, Placebo-controlled Trial
Susanne Herroeder, MD,†* Sabine Pecher, MD,† Marianne E. Schonherr, MD,† Grit Kaulitz,†Klaus Hahnenkamp, MD,‡ Helmut Friess, MD,§ Bernd W. Bottiger, MD,† Harry Bauer, MD,† �oMarcel G. W.
Dijkgraaf, PhD,� Marcel E. Durieux, MD, PhD,¶and Markus W. Hollmann, MD, PhD*#
Objective: To characterize the beneficial effects of perioperativesystemic lidocaine on length of hospital stay, gastrointestinal motil-ity, and the inflammatory response after colorectal surgery.Summary Background Data: Surgery-induced stimulation of theinflammatory response plays a major role in the development ofseveral postoperative disorders. Local anesthetics possess anti-in-flammatory activity and are thought to positively affect patients’outcome after surgery. This double-blinded, randomized, and pla-cebo-controlled trial aimed to evaluate beneficial effects of systemiclidocaine and to provide insights into underlying mechanisms.Methods: Sixty patients undergoing colorectal surgery, not willingor unable to receive an epidural catheter, were randomly assigned tolidocaine or placebo treatment. Before induction of general anesthe-sia, an intravenous lidocaine bolus (1.5 mg/kg) was administeredfollowed by a continuous lidocaine infusion (2 mg/min) until 4hours postoperatively. Length of hospital stay, gastrointestinal mo-tility, and pain scores were recorded and plasma levels or expressionof pro- and anti-inflammatory mediators determined.Results: Lidocaine significantly accelerated return of bowel func-tion and shortened length of hospital stay by one day. No differencecould be observed in daily pain ratings. Elevated plasma levels ofIL-6, IL-8, complement C3a, and IL-1ra as well as expression ofCD11b, L- and P-selectin, and platelet-leukocyte aggregates weresignificantly attenuated by systemic lidocaine.
Conclusions: Perioperative intravenous lidocaine not only improvedgastrointestinal motility but also shortened length of hospital staysignificantly. Anti-inflammatory activity modulating the surgery-in-duced stress response may be one potential mechanism. Systemiclidocaine may thus provide a convenient and inexpensive approach toimprove outcome for patients not suitable for epidural anesthesia.
(Ann Surg 2007;246: 192–200)
Major abdominal surgery elicits a broad variety of alter-ations in hemodynamic, endocrine-metabolic, and im-
mune responses.1 Although inflammation is crucial for struc-tural and functional repair of tissue damage, excessivestimulation of the inflammatory response has major impact onthe development of several inflammatory disorders periop-eratively, such as impaired gastrointestinal motility. Anes-thetic interventions that modulate inflammatory responsesmight thus decrease frequency and severity of such compli-cations, thereby minimizing morbidity and mortality.
Epidural administration of local anesthetics was ini-tially designed to provide optimal perioperative anesthesiaand analgesia, but numerous studies have shown that thisanesthetic technique exerts far more effects than pain relief.As it attenuates the surgery-induced stress response andimproves postoperative gastrointestinal function, epidural an-esthesia has become a popular anesthetic strategy to improveoutcome after major surgery.2 However, insertion of anepidural catheter is not without risks in certain patient pop-ulations. Especially patients after coronary stenting receiveanticoagulant therapy and thus require careful assessment asto the risks and benefits of administering a regional anesthetictechnique. Because of the strongly increasing numbers ofthese patients, alternative therapeutic interventions for opti-mal perioperative care are needed.
Local anesthetics, reabsorbed from the epidural space,may contribute to the beneficial nonanalgesic effects of epi-dural anesthesia. Originally known for inhibition of voltage-gated sodium channels, local anesthetics have significant
From the *Laboratory of Experimental Intensive Care & Anesthesiology,�Department of Clinical Epidemiology, Biostatistics and Bioinformatics, and#Department of Anesthesiology, Academic Medical Center Amsterdam,Amsterdam, The Netherlands; Departments of †Anesthesiology and §Gen-eral Surgery, University of Heidelberg, Heidelberg, Germany; ‡Departmentof Anesthesiology, University of Muenster, Muenster, Germany; and ¶De-partment of Anesthesiology, University of Virginia, Charlottesville, VA.Drs. Herroeder and Pecher contributed equally to this study.
Supported in part by the Medical Faculty, University of Heidelberg, Germany(F203699 to S.P. and M.W.H; F206639 to S.H. and M.W.H.) and byinstitutional money from the Department of Anesthesiology, University ofHeidelberg, Germany.
Reprints: Markus W. Hollmann, MD, PhD, Department of Anesthesiology,Academic Medical Center Amsterdam, P.O. Box 22600, 1105 DDAmsterdam, The Netherlands. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0192DOI: 10.1097/SLA.0b013e31805dac11
Annals of Surgery • Volume 246, Number 2, August 2007192

anti-inflammatory properties and may allow modulation ofexcessive inflammatory responses without impairing thephysiologic host defense.3 By characterizing the beneficialeffects of intravenous lidocaine in patients undergoing colo-rectal surgery and identifying underlying mechanisms, sys-temic lidocaine may become a safe and alternative strategyfor patients not willing or able to receive epidural anesthesiafor improving perioperative outcome.4
METHODSThe study was carried out between September 2002 and
December 2004 at the Departments of Anesthesiology andSurgery, University of Heidelberg, Germany, following ICHGCP guidelines. ELISA measurements of cytokines wereconducted at the Department of Anesthesiology, Universityof Amsterdam, The Netherlands. After approval of the pro-tocol by the Institutional review board of the University ofHeidelberg and after obtaining written informed consent, weenrolled 60 patients of American Society of Anesthesiologistsphysical status I to III, and between 18 and 75 years of age,scheduled for elective colorectal surgery in this double-blinded, randomized, and placebo-controlled clinical trial.Inclusion criteria were refusal or contraindication for place-ment of an epidural catheter, whereas criteria for exclusionwere known allergies to local anesthetics, chronic use ofanalgesics or corticosteroids, underlying inflammatory boweldisease (Crohn’s disease or ulcerative colitis), prolongedpostoperative ventilatory support, impaired liver function,and severe cardiac arrhythmia.
Patients were randomly assigned to either lidocaine orplacebo treatment using the following multistep protocol tominimize effects of type and length of surgery. Dependent onthe surgical procedure performed, patients were allocated to 2different groups (colectomy vs. rectum resection). Eachgroup was subdivided into blocks consisting of 6 patients.According to numbers on a drawn lot, patients were assignedto the lidocaine or placebo groups subsequently. Both groupswere randomized separately and blockwise.
The study medication was prepared by an anesthesiol-ogist not involved in further treatment of the patients. Theanesthesia team and all other staff involved in patient carewere blinded to study group assignments.
One day before surgery, all patients were instructedhow to use a patient controlled analgesia (PCA) pump andrate pain intensity on a visual analog scale (VAS), identifying0 as “no pain” and 10 as “worst imaginable pain.” In addition,each patient was requested to record the first appearance ofbowel sounds, flatus, and defecation postoperatively.
Perioperative ProtocolAll anesthetic procedures were performed in a stan-
dardized fashion. For premedication, all patients receivedclorazepate dipotassium by mouth. Standard monitoring wasapplied and general anesthesia induced with fentanyl, propo-fol, and vecuronium. Anesthesia was maintained usingsevoflurane and 40% oxygen in 60% nitrous oxide. Sevoflu-rane concentration was adjusted to keep blood pressure andheart rate within �15% of baseline values. Mechanical ven-tilation facilitated normocapnia. Before surgical incision, a fen-
tanyl bolus was administered and further analgesia was providedusing continuous infusion of remifentanil individually adapted.Thirty minutes before the end of surgery, piritramide for post-operative analgesia was administered intravenously and all pa-tients received dolasetron for postoperative nausea and vomitingprophylaxis. Train-of-four monitoring guided relaxation, facili-tating extubation (train-of-four �90%) without using reversalagents. Normothermia was maintained during surgery using awarm touch warming system (Mallinckrodt Medical Inc., St.Louis, MO).
Study Drug AdministrationPatients in the lidocaine group received 1.5 mg/kg
lidocaine intravenously as a loading dose before induction ofgeneral anesthesia. Immediately after tracheal intubation, acontinuous systemic lidocaine infusion (2 mg/min) was ini-tiated and terminated 4 hours after skin closure. Patients inthe control group were treated likewise using NaCl 0.9% in adouble-blinded fashion.
PACU and Postoperative CareAfter surgery, patients were transferred to the postop-
erative anesthesia care unit (PACU) and discharged notearlier than 30 minutes after completion of lidocaine/salinetreatment. PCA devices were adjusted to a demand dose of 2mg piritramide and a lockout period of 10 minutes withoutbasal infusion. Additionally, after transfer to the ward, 1 gmetamizol or in case of contraindications 1 g paracetamolwas given every 6 hours. Diet was advanced according to thefast-track concept established at our institution, facilitatingsolid food intake as soon as possible.
Outcome MeasuresThe primary outcome measure was length of hospital
stay. Secondary outcome measures included length of PACUstay, time until return of bowel function, postoperative painand opioid consumption, plasma levels of several pro- andanti-inflammatory interleukins (�IL�-6, IL-8, IL-1�, TNF-�and IL-1ra, IL-10, respectively), complement C3a, leukocyteactivation (CD11b, CD62L, CD62P) as well as platelet-leukocyte-interactions (PLAs).
Data CollectionLidocaine plasma levels were determined at 5 minutes,
2 hours, and 4 hours after application of the loading dose,using high-pressure liquid chromatography.
Time until discharge from PACU was evaluated every15 minutes by assessment of the Aldrete score.5 Aldrete �8defined readiness for discharge. To determine return of gas-trointestinal motility, bowel sounds were auscultated andpatients asked twice daily if first flatus and defecation hadoccurred. Nausea, vomiting, type of diet, wound healingdisturbances, and surgery-related complications were re-corded. Pain intensities at rest and during coughing weremeasured using a VAS at 2 and 4 hours postoperatively aswell as every 12 hours on the following days. Opioid demandby PCA was monitored daily. Length of hospital stay wasdetermined as time until patients met standardized dischargecriteria according to our surgeons’ protocol to exclude socialfactors delaying real discharge times. Discharge criteria in-
Annals of Surgery • Volume 246, Number 2, August 2007 Lidocaine and Colorectal Surgery
© 2007 Lippincott Williams & Wilkins 193

clude: return to light diet without nausea and vomiting, abilityto self-care and mobilize or to be able to be cared for byexisting-home arrangements, no signs of wound healing dis-turbances, absence of increased infectious parameters inblood chemistry, pain control with oral analgesics, and asbowel movements before discharge.
Blood samples for measurement of inflammatory cellsand mediators were taken immediately before induction ofanesthesia, at the end of surgery, 2 hours postoperatively, andon postoperative day (POD) 3.
Quantitative measurements of plasma cytokine levelswere made using commercial “sandwich” enzyme-linked im-munosorbent assay kits according to the manufacturer’s in-structions. IL-6, IL-8, IL-10, TNF-�, IL-1� (Quantikine,R&D Systems GmbH, Wiesbaden, Germany), IL-1ra (Bio-Source Deutschland, Solingen, Germany), and C3a (QuidelDeutschland, Marburg, Germany). Sensitivities of the assaysused were 0.7, 4.4, 3.9, 0.5, 0.3, 4.0 pg/ml and 1.0 ng/ml,respectively. Intraassay and interassay coefficients of varia-tion were all less than 10% in each measurement. Crossreactivity with other factors was negligible. Activation of leu-kocytes and PLAs was analyzed with a three-color FACSCali-bur flow cytometer and CellQuestPro software (BD Bioscience,Heidelberg, Germany), using the following antibodies: anti-CD11b-FITC, anti-CD45-PE, anti-CD42b-FITC, anti-CD62L-FITC, anti-CD62P-PE: all Dako, Heidelberg, Germany, exceptanti-CD11b-FITC (Dianova, Hamburg, Germany) and anti-CD62P-PE (BD Bioscience). PLA formation is expressed aspercentage of platelet-bound leukocytes. All samples and stan-dards were run in duplicate.
StatisticsStatistical analysis was performed using SPSS version
12.0.2 for Windows (SPSS Inc., Chicago, IL). With respect toour primary endpoint, length of hospital stay, sample sizeanalysis revealed a required number of patients of 28 pergroup (expected mean difference 1.0 day, expected standarddeviation 1.3 days, based on data of Groudine et al,6 and ourown pilot study; power 80%, P � 0.05). Baseline values werecompared using Student t test, Wilcoxon test, and Fisherexact test. The effect of treatment on gastrointestinal motility,piritramide consumption, and length of hospital stay wasanalyzed by Student t test or Mann-Whitney U test, depend-ing on distributional properties. Differences in cytokineplasma levels were assessed using repeated-measures analy-sis of variance and corrected with a post hoc Bonferroni test.Linear mixed modeling was performed to study the overalland time-dependent influence of lidocaine treatment onCD11b, CD62P/L, and PLA (relative to baseline). Akaike’sinformation criterion was used to decide upon the best modelfit. A P value �0.05 was considered to represent a significantdifference. Data are mean � SD or median with interquartileranges, unless otherwise indicated.
RESULTS
Demographic DataSeventy-seven patients undergoing elective colorectal
surgery met our study criteria. Nine patients refused to
participate, whereas delay of surgery led to exclusion of 2patients. Thus, 66 patients were randomized and assignedequally to both groups. Because of intraoperative hypother-mia, 2 patients in each group required prolonged ventilatorysupport and had to be excluded during the postoperativecourse. In addition, 2 patients of the control group droppedout because of preoperative unrecognized chronic drug abuse(analgesics). Altogether, 60 patients (29 in the control and 31in the lidocaine group) completed the study and were ana-lyzed (Fig. 1). The relevant demographic and intraoperativedata are given in Tables 1 and 2, respectively. A significantproportion of patients in the lidocaine group presented withpreexisting hypertension (P � 0.046), whereas in other as-pects no significant differences between the groups could beobserved. Colectomies and rectum resections were equallydistributed, and one patient of each group underwent anadditional hemihepatectomy.
Length of Hospital StayAnalysis of the primary endpoint showed a significant
difference (P � 0.004) in length of hospital stay; lidocaine-treated patients were discharged home 1 day earlier than theircontrol counterparts: 7 days �6, 8� versus 8 days �7, 11�respectively (Fig. 2).
Length of PACU StayThere was no difference regarding length of PACU stay
between groups (76 � 74 and 84 � 77 minutes for controland lidocaine patients, respectively).
Gastrointestinal MotilityReturn of bowel function was significantly accelerated
in patients receiving intravenous lidocaine. Bowel sounds andfirst flatus occurred approximately 8 hours earlier (Fig. 3a)compared with control and time until first defecation wassignificantly decreased in patients after administration of
FIGURE 1. Study design according to the CONSORT statement.
Herroeder et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins194
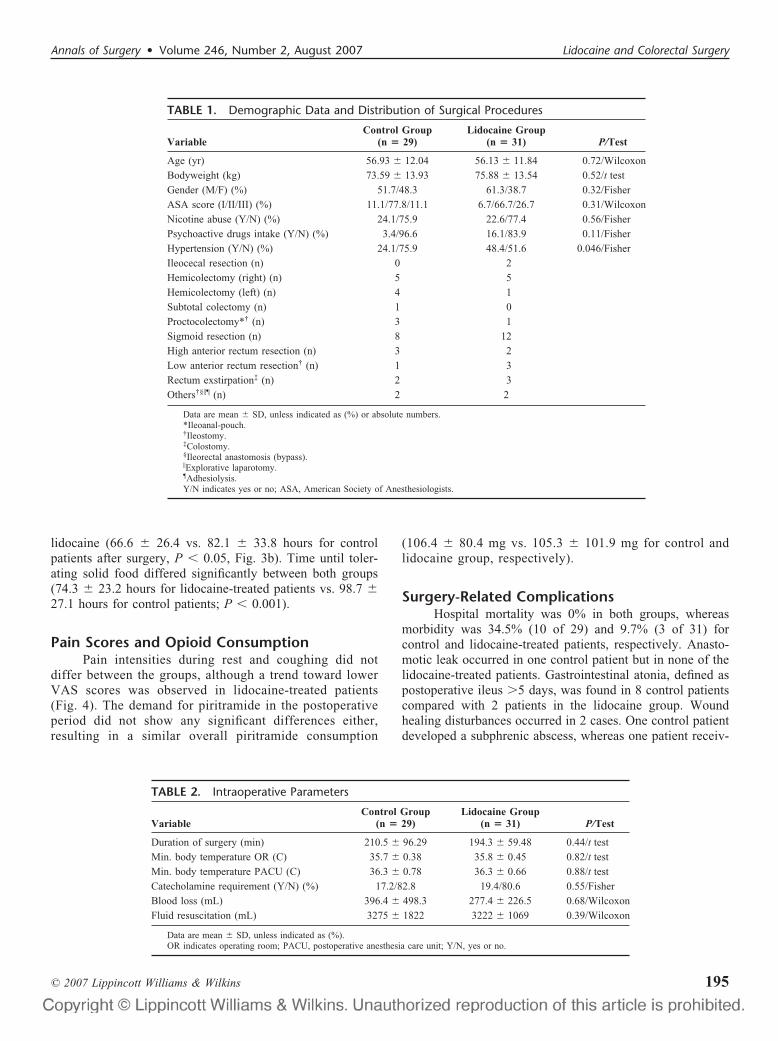
lidocaine (66.6 � 26.4 vs. 82.1 � 33.8 hours for controlpatients after surgery, P � 0.05, Fig. 3b). Time until toler-ating solid food differed significantly between both groups(74.3 � 23.2 hours for lidocaine-treated patients vs. 98.7 �27.1 hours for control patients; P � 0.001).
Pain Scores and Opioid ConsumptionPain intensities during rest and coughing did not
differ between the groups, although a trend toward lowerVAS scores was observed in lidocaine-treated patients(Fig. 4). The demand for piritramide in the postoperativeperiod did not show any significant differences either,resulting in a similar overall piritramide consumption
(106.4 � 80.4 mg vs. 105.3 � 101.9 mg for control andlidocaine group, respectively).
Surgery-Related ComplicationsHospital mortality was 0% in both groups, whereas
morbidity was 34.5% (10 of 29) and 9.7% (3 of 31) forcontrol and lidocaine-treated patients, respectively. Anasto-motic leak occurred in one control patient but in none of thelidocaine-treated patients. Gastrointestinal atonia, defined aspostoperative ileus �5 days, was found in 8 control patientscompared with 2 patients in the lidocaine group. Woundhealing disturbances occurred in 2 cases. One control patientdeveloped a subphrenic abscess, whereas one patient receiv-
TABLE 1. Demographic Data and Distribution of Surgical Procedures
VariableControl Group
(n � 29)Lidocaine Group
(n � 31) P/Test
Age (yr) 56.93 � 12.04 56.13 � 11.84 0.72/Wilcoxon
Bodyweight (kg) 73.59 � 13.93 75.88 � 13.54 0.52/t test
Gender (M/F) (%) 51.7/48.3 61.3/38.7 0.32/Fisher
ASA score (I/II/III) (%) 11.1/77.8/11.1 6.7/66.7/26.7 0.31/Wilcoxon
Nicotine abuse (Y/N) (%) 24.1/75.9 22.6/77.4 0.56/Fisher
Psychoactive drugs intake (Y/N) (%) 3.4/96.6 16.1/83.9 0.11/Fisher
Hypertension (Y/N) (%) 24.1/75.9 48.4/51.6 0.046/Fisher
Ileocecal resection (n) 0 2
Hemicolectomy (right) (n) 5 5
Hemicolectomy (left) (n) 4 1
Subtotal colectomy (n) 1 0
Proctocolectomy*† (n) 3 1
Sigmoid resection (n) 8 12
High anterior rectum resection (n) 3 2
Low anterior rectum resection† (n) 1 3
Rectum exstirpation‡ (n) 2 3
Others†§�¶ (n) 2 2
Data are mean � SD, unless indicated as (%) or absolute numbers.*Ileoanal-pouch.†Ileostomy.‡Colostomy.§Ileorectal anastomosis (bypass).�Explorative laparotomy.¶Adhesiolysis.Y/N indicates yes or no; ASA, American Society of Anesthesiologists.
TABLE 2. Intraoperative Parameters
VariableControl Group
(n � 29)Lidocaine Group
(n � 31) P/Test
Duration of surgery (min) 210.5 � 96.29 194.3 � 59.48 0.44/t test
Min. body temperature OR (C) 35.7 � 0.38 35.8 � 0.45 0.82/t test
Min. body temperature PACU (C) 36.3 � 0.78 36.3 � 0.66 0.88/t test
Catecholamine requirement (Y/N) (%) 17.2/82.8 19.4/80.6 0.55/Fisher
Blood loss (mL) 396.4 � 498.3 277.4 � 226.5 0.68/Wilcoxon
Fluid resuscitation (mL) 3275 � 1822 3222 � 1069 0.39/Wilcoxon
Data are mean � SD, unless indicated as (%).OR indicates operating room; PACU, postoperative anesthesia care unit; Y/N, yes or no.
Annals of Surgery • Volume 246, Number 2, August 2007 Lidocaine and Colorectal Surgery
© 2007 Lippincott Williams & Wilkins 195

ing lidocaine showed minor signs of skin wound irritation,which did not require any surgical intervention.
Lidocaine Plasma LevelsMean plasma levels of lidocaine were in the range of
1.1 to 4.2 �g/mL, with the exception of one patient present-ing with a peak value of 5.8 �g/mL after lidocaine bolusadministration. All patients started on the lidocaine infusionfinished their full course of drug and did not experience anyadverse events, such as arrhythmias or neurologic symptoms,related to the local anesthetic.
Cytokines, Integrins, and PLAsSystemic lidocaine significantly attenuated plasma lev-
els of IL-6, IL-8, IL-1ra, complement C3a, as well as expres-sion of CD11b, CD62L, CD62P and formation of PLAs.Plasma levels of TNF-� and IL-1�, however, did not increasein response to surgery, whereas IL-10 was not affected by thelocal anesthetic at any time point (Tables 3 and 4).
FIGURE 3. First occurrence of bowel sounds and flatus (A)and defecation (B) postoperatively. Data are mean � SD.*Statistical significance (P � 0.05) compared with control(unpaired Student t test). Black bars, control patients; whitebars, lidocaine-treated patients.
FIGURE 2. Effects of continuous administration of systemiclidocaine on length of hospital stay. Data are shown as me-dian with 25th and 75th percentiles. *Statistical significance(P � 0.004) compared with control (Mann-Whitney U test).
FIGURE 4. Visual analog scale (VAS) pain scores at rest (A)and during coughing (B). Data are mean � SD. Black dots,control patients; white dots, lidocaine-treated patients.
Herroeder et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins196

TABLE 3. Effects of Lidocaine on Cytokine Plasma Levels
Cytokine TimeControl Group
(n � 29)Lidocaine Group
(n � 31)
IL-6 (pg/mL) Preop. 10 � 7 13 � 7
End of operation 44 � 28* 29 � 17*†
2-hr Postop. 118 � 73* 63 � 50*†
POD 3 18 � 11* 11 � 8†
IL-8 (pg/mL) Preop. ND ND
End of operation 27 � 14* 18 � 12*†
2-hr Postop. 42 � 34* 27 � 19*†
POD 3 9 � 7* 6 � 4*†
IL-1� (pg/mL) Preop. 3 � 2 3 � 2
End of operation 3 � 2 3 � 2
2-hr Postop. 4 � 2 3 � 2†
POD 3 3 � 2 3 � 2
TNF-� (pg/mL) Preop. 4 � 3 5 � 3
End of operation 5 � 4 5 � 3
2-hr Postop. 5 � 3 4 � 3
POD 3 4 � 3 5 � 3
C3a (ng/mL) Preop. 128 � 46 138 � 71
End of operation 135 � 56 129 � 44*†
2-hr Postop. 287 � 77* 201 � 101
POD 3 187 � 89* 167 � 90
IL-1ra (pg/mL) Preop. 275 � 163 296 � 189
End of operation 1576 � 934* 987 � 642*†
2-hr Postop. 1489 � 812* 866 � 537*†
POD 3 333 � 196 282 � 198
IL-10 (pg/mL) Preop. ND ND
End of operation 32 � 31* 28 � 25*
2-hr Postop. 46 � 36* 45 � 31*
POD 3 ND ND
Data are mean � SD.*P � 0.05 vs. baseline values.†P � 0.05 vs. control patients (RM-ANOVA, corrected with a post hoc Bonferroni test).POD indicates postoperative day; ND, nondetectable by the assay used.
TABLE 4. Effects of Lidocaine on Expression of Integrins, Selectins, and PLA Formation
TimeControl Group
(n � 29)Lidocaine Group
(n � 31)
CD11b (% preop.) End of operation 106 � 23* 87 � 22†
2-hr Postop. 131 � 29* 89 � 24†
POD 3 136 � 38* 103 � 22†
CD62L (% preop.) End of operation 113 � 24* 94 � 14†
2-hr Postop. 127 � 23* 102 � 13†
POD 3 127 � 28* 100 � 23†
CD62P (% preop.) End of operation 100 � 14* 95 � 35†
2-hr Postop. 114 � 23* 89 � 29†
POD 3 126 � 23* 104 � 29†
PLA (% preop.) End of operation 76 � 40 66 � 42
2-hr Postop. 94 � 78 77 � 67
POD 3 147 � 70* 100 � 55†
Data are mean � SD.*P � 0.05 vs. preoperative values.†P � 0.05 vs. control patients (Linear mixed modeling/Akaike’s information criterion).POD indicates postoperative day; PLA, platelet-leukocyte-aggregate.
Annals of Surgery • Volume 246, Number 2, August 2007 Lidocaine and Colorectal Surgery
© 2007 Lippincott Williams & Wilkins 197

DISCUSSIONOur study demonstrates that perioperative systemic
administration of lidocaine significantly shortened length ofhospital stay by 1 day in patients undergoing colorectalsurgery.
The underlying mechanisms might be multifactorial.However, the accelerated return of bowel function seemsto be a major contributor. Abdominal surgery is oftenaccompanied by postoperative ileus; and despite its nor-mally benign and self-limiting character, it is associatedwith patient discomfort, prolonged hospitalization, andincreased postoperative morbidity. Prevention and/or treat-ment are difficult; thus, management remains mainly sup-portive.7 Postoperative ileus also has a significant economicimpact since it results in additional costs of approximately $1billion in the United States each year.8 Its etiology is complexand involves different mechanisms for initiation and prolon-gation. The acute phase is neurally mediated, whereas the latephase depends upon both leukocyte migration into the ma-nipulated segment and subsequent activation of an inhibitoryadrenergic pathway.7,9–11 Since inflammation plays a crucialrole in sustaining postoperative ileus, intravenous local anes-thetics may mediate their beneficial effects on promotinggastrointestinal motility by targeting different steps withinthis inflammatory cascade. Perioperative administration oflidocaine significantly attenuated the surgery-induced in-crease of complement and pro-inflammatory cytokines, suchas IL-8 and IL-6. The latter is well known for its role inmaintaining postoperative ileus and intestinal permeabilitydisorders.12,13 Absence of an expected increase of IL-1� andTNF-� may have different reasons. Plasma levels of IL-1�may be low, although tissue damage is severe and the pre-defined schedule for sample measurements may have covereddifferent cytokine peaks. However, in various studies, bothcytokines have not been found to be elevated in patientsundergoing different types of surgery.14–17 Lidocaine did notaffect generation of the anti-inflammatory cytokine IL-10, butsignificantly attenuated plasma levels of IL-1ra. Since IL-1rais an assumed marker for the presence of IL-1�, it may reflectotherwise nondetectable changes in IL-1� plasma levels dueto lidocaine treatment. Yet, a direct effect of the local anes-thetic on IL-1ra generation cannot be excluded. Recruitmentof leukocytes to sites of inflammation requires multistepadhesive events that depend on the coordinated interactionsof selectins, integrins, and adhesion molecules.18 Surgery-induced increased expression of L (CD62L)- and P (CD62P)-selectin as well as CD11b, the � subunit of leukocyte integrinMAC-1, was completely prevented by lidocaine. However,effects of local anesthetics on selectin expression remaincontroversial up to now.19,20 Inhibition of fMLP- or Staphy-lococcus aureus-induced CD11b expression in neutrophilshas been documented more definitely, but concentrationsrequired to achieve these effects exceed systemic concentra-tions at least 10- to 100-fold.21 Length of exposure (10–60minutes in most in vitro studies19,21) might explain thisdifference since local anesthetics in the micromolar range areknown to exert their anti-inflammatory properties in a time-dependent manner.22,23 Hence, the effect of low concentra-
tions of local anesthetics on selectin and integrin expressionin our study may result from the fact that lidocaine wasadministered continuously for at least 7 hours. Functionalinteractions of platelets and leukocytes play an important rolein inflammation and thrombosis and could be detected inmyocardial infarction or sepsis. Lidocaine treatment signifi-cantly reduced PLA formation. Underlying mechanisms maybe many, but attenuated expression of P-selectin as one majorcontributor by lidocaine might be a promising candidate.24 Ifinflammation was severely disturbed, repair of tissue damagemight be delayed and the incidence of postoperative compli-cations potentially increased. In line with findings obtainedin several in vivo studies, patients receiving lidocaine didnot show seriously impaired wound healing in this trial.25
Altogether, lidocaine indeed may exert its beneficial ef-fects on postoperative ileus by diminishing the inflamma-tory response, although our data have to be consideredassociative and additional mechanisms of action may exist.
Epidural anesthesia, using local anesthetics, is thoughtto promote gastrointestinal motility by inhibition of thoraco-lumbar sympathetic fibers and its opioid-sparing effects.26,27
It is unlikely, however, that sympathetic blockade is the mainunderlying mechanism for the effects of intravenous lido-caine. Concentrations of lidocaine required for inhibition ofnerve conduction were shown to range between 60 and 100�mol/L, whereas mean lidocaine plasma levels did not ex-ceed 4.2 �g/mL (�10 �M3) in the present study. An effect onopioid consumption cannot explain the findings either be-cause VAS pain scores, rated at rest and during coughing, aswell as piritramide consumption did not differ between bothgroups. This is in contrast to findings of Koppert et al, whoshowed attenuated postoperative pain and decreased mor-phine consumption after major abdominal surgery due toprevention of central hyperalgesia by intravenous lidocaine.28
There are obviously some limitations of the present study.Patients in this study underwent conventional colorectal sur-gery, although laparoscopy is frequently used for the surgicaltreatment of colorectal diseases and thought to better preserveimmunity than open surgery.29 However, perioperative lido-caine is still able to positively affect postoperative ileus andoutcome even if inflammation is less pronounced. Kaba et alfound intravenous lidocaine to have similar beneficial effectson outcome as epidural anesthesia after laparoscopic colec-tomy.30 In this regard, length of hospital stay after colorectalsurgery is of interest. Days spent in hospital after conven-tional surgery vary from 5 to 6 days in the United States andScandinavia to 8 days and more in Germany and otherEuropean countries.31–34 Explanations for this difference mayinclude a less stringent recovery program patients adhere toor organizational differences in postoperative care after dis-charge. Nevertheless, on the basis of available literature,lidocaine positively affects recovery and outcome data,even if hospital stay is shortened per se.6,30 Most recently,Kuo et al failed to find a difference regarding length ofhospital stay in patients undergoing colorectal surgery,when comparing the effects of thoracic epidural anesthesiaand intravenous lidocaine, though.35 As this study waspowered for observing differences in postoperative opioid
Herroeder et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins198

consumption, study groups may have been simply toosmall. Administration of lidocaine limited to the intraop-erative period or weak exclusion criteria, such as permis-sion of patients on corticosteroids, may have affectedlidocaine’s potential benefit additionally.
Although never reported for its intended use, systemiclidocaine may have undesired effects on several organ func-tions as it inhibits voltage-gated sodium channels, therebyinterrupting nerve conduction. Proportional to its plasmalevels, it may cause central nervous system stimulation,producing drowsiness and tremor or depresses myocardialfunction by decreasing electrical excitability and conductionrate. First clinical signs of toxicity, however, occur at con-siderably high concentrations (�5 �g/mL), not evenachieved when intravenous lidocaine was given continuouslyover 14 days in case of severe migraine.36
CONCLUSIONOur results show that perioperative intravenous ad-
ministration of lidocaine provides an inexpensive andconvenient approach to attenuate the initiation of theexcessive inflammatory response during colorectal sur-gery. Associated with a shortened hospital stay and im-proved patient comfort, systemic lidocaine may be ofclinical interest with respect to economics and optimalperioperative management. The growing number of pa-tients not suitable for neuraxial anesthesia could stillbenefit from the protective effects of local anesthetics butwould not have to face the potential risks of epiduralanesthesia.
ACKNOWLEDGMENTSThe authors thank Prof. Dr. Wolfgang S. Schlack (De-
partment of Anesthesiology, Academic Medical Center Am-sterdam, The Netherlands) for critically reviewing the manu-script, Ute Krauser for expert technical assistance, and Prof.Dr. Eike Martin (Department of Anesthesiology, University ofHeidelberg, Germany) for his support.
REFERENCES1. Herroeder S, Durieux ME, Hollmann MW. Inflammatory responses after
surgery. Hosp Med. 2002;63:99–103.2. Kozian A, Schilling T, Hachenberg T. Non-analgetic effects of thoracic
epidural anaesthesia. Curr Opin Anaesthesiol. 2005;18:29–34.3. Hollmann MW, Durieux ME. Local anesthetics and the inflammatory
response: a new therapeutic indication? Anesthesiology. 2000;93:858–875.
4. Hollmann MW, Strumper D, Durieux ME. The poor man’s epidural:systemic local anesthetics for improving postoperative outcomes. MedHypotheses. 2004;63:386–389.
5. Aldrete JA, Kroulik D. A postanesthetic recovery score. Anesth Analg.1970;49:924–934.
6. Groudine SB, Fisher HAG, Kaufman RP, et al. Intravenous lidocainespeeds the return of bowel function, decreases postoperative pain, andshortens hospital stay in patients undergoing radical retropubic prosta-tectomy. Anesth Analg. 1998;86:235–239.
7. Bauer AJ, Boeckxstaens GE. Mechanisms of postoperative ileus. Neu-rogastroenterol Motil. 2004;16(Suppl 2):54–60.
8. Prasad M, Matthews JB. Deflating postoperative ileus. Gastroenterol-ogy. 1999;117:489–492.
9. de Jonge WJ, van den Wijngaard RM, The FO, et al. Postoperative ileus
is maintained by intestinal immune infiltrates that activate inhibitoryneural pathways in mice. Gastroenterology. 2003;125:1137–1147.
10. Collins SM. The immunomodulation of enteric neuromuscular function:implications for motility and inflammatory disorders. Gastroenterology.1996;111:1683–1699.
11. The FO, de Jonge WJ, Bennink RJ, et al. The ICAM-1 antisenseoligonucleotide ISIS-3082 prevents the development of postoperativeileus in mice. Br J Pharmacol. 2005;146:252–258.
12. Cruickshank AM, Fraser WD, Burns HJ, et al. Response of seruminterleukin-6 in patients undergoing elective surgery of varying severity.Clin Sci (Lond). 1990;79:161–165.
13. Wang W, Smail N, Wang P, et al. Increased gut permeability afterhemorrhage is associated with upregulation of local and systemic IL-6.J Surg Res. 1998;79:39–46.
14. Wu CT, Jao SW, Borel CO, et al. The effect of epidural clonidine onperioperative cytokine response, postoperative pain, and bowel functionin patients undergoing colorectal surgery. Anesth Analg. 2004;99:502–509.
15. Slotwinski R, Olszewski WL, Chaber A, et al. The soluble tumornecrosis factor receptor I is an early predictor of local infective compli-cations after colorectal surgery. J Clin Immunol. 2002;22:289–296.
16. Pruitt JH, Welborn MB, Edwards PD, et al. Increased soluble interleu-kin-1 type II receptor concentrations in postoperative patients and inpatients with sepsis syndrome. Blood. 1996;87:3282–3288.
17. Keel M, Ecknauer E, Stocker R, et al. Different pattern of local andsystemic release of proinflammatory and anti-inflammatory mediators inseverely injured patients with chest trauma. J Trauma. 1996;40:907–912.
18. von Andrian UH, Mackay CR. T-cell function and migration: two sidesof the same coin. N Engl J Med. 2000;343:1020–1034.
19. Martinsson T, Oda T, Fernvik E, et al. Ropivacaine inhibits leukocyterolling, adhesion and CD11b/CD18 expression. J Pharmacol Exp Ther.1997;283:59–65.
20. Chen Y, Ke Q, Xiao YF, et al. Cocaine and catecholamines enhanceinflammatory cell retention in the coronary circulation of mice byupregulation of adhesion molecules. Am J Physiol Heart Circ Physiol.2005;288:H2323–H2331.
21. Kiefer RT, Ploppa A, Krueger WA, et al. Local anesthetics impairhuman granulocyte phagocytosis activity, oxidative burst, and CD11bexpression in response to Staphylococcus aureus. Anesthesiology. 2003;98:842–848.
22. Hollmann MW, Herroeder S, Kurz KS, et al. Time-dependent inhibitionof G protein-coupled receptor signaling by local anesthetics. Anesthesi-ology. 2004;100:852–860.
23. Kohrs R, Hoenemann CW, Feirer N, et al. Bupivacaine inhibits wholeblood coagulation in vitro. Reg Anesth Pain Med. 1999;24:326–330.
24. Rinder HM, Bonan JL, Rinder CS, et al. Dynamics of leukocyte-plateletadhesion in whole blood. Blood. 1991;78:1730–1737.
25. Drucker M, Cardenas E, Arizti P, et al. Experimental studies on theeffect of lidocaine on wound healing. World J Surg. 1998;22:394–397.
26. Bonnet F, Marret E. Influence of anaesthetic and analgesic techniques onoutcome after surgery. Br J Anaesth. 2005;95:52–58.
27. Kehlet H, Dahl JB. Anaesthesia, surgery, and challenges in postopera-tive recovery. Lancet. 2003;362:1921–1928.
28. Koppert W, Weigand M, Neumann F, et al. Perioperative intravenouslidocaine has preventive effects on postoperative pain and morphineconsumption after major abdominal surgery. Anesth Analg. 2004;98:1050–1055.
29. Buunen M, Gholghesaei M, Veldkamp R, et al. Stress response tolaparoscopic surgery: a review. Surg Endosc. 2004;18:1022–1028.
30. Kaba A, Detroz BJ, Laurent SR, et al. Acute rehabilitation program afterlaparoscopic colectomy using intravenous lidocaine. Acta Chir Belg.2005;105:53–58.
31. Moiniche S, Bulow S, Hesselfeldt P, et al. Convalescence and hospitalstay after colonic surgery with balanced analgesia, early oral feeding,and enforced mobilisation. Eur J Surg. 1995;161:283–288.
32. Clinical Outcomes of Surgical Therapy Study Group. A comparison oflaparoscopically assisted and open colectomy for colon cancer. N EnglJ Med. 2004;350:2050–2059.
33. Braga M, Vignali A, Gianotti L, et al. Laparoscopic versus open
Annals of Surgery • Volume 246, Number 2, August 2007 Lidocaine and Colorectal Surgery
© 2007 Lippincott Williams & Wilkins 199

colorectal surgery: a randomized trial on short-term outcome. Ann Surg.2002;236:759––766.
34. Alves A, Panis Y, Slim K, et al. French multicentre prospective obser-vational study of laparoscopic versus open colectomy for sigmoiddiverticular disease. Br J Surg. 2005;92:1520–1525.
35. Kuo CP, Jao SW, Chen KM, et al. Comparison of the effects of thoracic
epidural analgesia and i. v. infusion with lidocaine on cytokine response,postoperative pain and bowel function in patients undergoing colonicsurgery. Br J Anaesth. 2006;97:640–646.
36. Williams DR, Stark RJ. Intravenous lignocaine (lidocaine) infusion forthe treatment of chronic daily headache with substantial medicationoveruse. Cephalalgia. 2003;23:963–971.
Herroeder et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins200

RANDOMIZED CONTROLLED TRIALS
Comparison of Long-term Outcome of Laparoscopic andConventional Nissen Fundoplication
A Prospective Randomized Study With an 11-Year Follow-up
Paulina T. P. Salminen, MD,* Heikki I. Hiekkanen, MSc,† Arto P. T. Rantala, MD, PhD,*and Jari T. Ovaska, MD, PhD*
Objective: The aim of this study was to compare the long-termobjective and subjective outcomes of laparoscopic and openNissen fundoplication in a randomized clinical trial with an11-year follow-up.Summary Background Data: Laparoscopic Nissen fundoplicationhas become the method of choice in antireflux surgery, replacing itsopen counterpart despite the lack of long-term results from con-trolled clinical studies.Methods: Between April 1992 and June 1995, 110 consecutivepatients were randomized to either laparoscopic (LAP) or conven-tional (open) Nissen fundoplication. The objective long-term fol-low-up consisted of an upper gastrointestinal endoscopy and aclinical assessment; the subjective long-term outcome was investi-gated by personal interviews using a structured questionnaire.Results: Forty-nine patients in the LAP group and 37 patients in theopen group were available for evaluation. Late subjective results,including postoperative symptoms and evaluation of the surgicalresult, were similar in both groups. With the benefit of hindsight,73.7% of the patients in the open group and 81.8% in the LAP groupwould again choose surgical treatment (P � 0.3042). In the LAPgroup, there were 5 (13.2%) partially or totally disrupted plicationscompared with the 14 (40.0%) disrupted plications in the open group(P � 0.0152). There were 10 incisional hernias in the open groupcompared with none in the LAP group (P � 0.001).Conclusions: At long-term follow-up, the open and LAP ap-proaches for the Nissen fundoplication have similar long-term sub-jective symptomatic outcome despite the significantly higher inci-dence of incisional hernias and defective fundic wraps at endoscopyin the open group defining laparoscopic Nissen fundoplication as the
procedure of choice in surgical management of gastroesophagealreflux disease.
(Ann Surg 2007;246: 201–206)
To date, laparoscopic fundoplication is generally acceptedas a routine surgical approach in the treatment of moder-
ate or severe gastroesophageal reflux disease. In a review byCatarci et al,1 laparoscopic fundoplication was as effective asits open counterpart with reduced morbidity, shorter hospitalstay, and recovery but without any significant differences inearly functional results and outcome. However, there are onlyfew randomized studies comparing the laparoscopic and openapproach for Nissen fundoplication2–13 and only 2 studies9,14
have published a follow-up of 5 years after surgery. So far,there have been no reports of randomized studies with fol-low-up exceeding 10 years after this procedure. In this study,we compared the long-term results of laparoscopic (LAP) andopen Nissen fundoplication at a mean follow-up of 11 yearsand 5 months after surgery.
PATIENTS AND METHODS
Patients and OperationsBetween April 1992 and June 1995, 110 consecutive
patients were randomized to either LAP or conventional(open) Nissen fundoplication, 55 to each procedure. Theclinical details of the patients enrolled in the study, themethods, and the operative techniques have previously beendescribed in detail.2 This study was a review of late resultsafter a randomized clinical trial.
Of the original patient series, 94 patients were availablefor long-term follow-up. Sixteen patients died of unrelatedcauses: 12 in the open group and 4 in the LAP group. Thecauses of death are detailed in Table 1. One patient in theopen group underwent refundoplication during the originalstudy period due to a disrupted plication; the late outcomewas thus excluded from this study, but the refundoplicationwas included in the reoperation rate analysis. In addition, 3patients were excluded from the long-term follow-up basedon their current medical condition: 1 for disseminated ovarian
From the *Department of Surgery, Turku University Central Hospital,Turku, Finland; and †Institute of Clinical Medicine, Department ofBiostatistics, Turku, Finland.
Supported by a research grant from the Department of Surgery, TurkuUniversity Central Hospital.
Reprints will not be available from the author.Correspondence: Paulina Salminen, MD, Kiinamyllynkatu 4-8, 20520
Turku, Finland. E-mail: [email protected] © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0201DOI: 10.1097/01.sla.0000263508.53334.af
Annals of Surgery • Volume 246, Number 2, August 2007 201

cancer, 1 for metastasized renal cancer, and 1 for severedementia. Of the remaining 90 patients, 86 patients (95.6%)were available for long-term follow-up: 37 open group pa-tients and 49 LAP group patients, including 4 conversions toopen surgery. A total of 75 patients (83.3%) underwent boththe upper gastrointestinal endoscopy and the symptomaticoutcome interview: 35 in the open group and 40 in the LAPgroup. Informed consent was obtained from all the patients.The additional 11 patients underwent a personal phone inter-view by the same researcher using the same structured ques-tionnaire; the response rate was thus 95.6% at a medianfollow-up of 11 years and 5 months. The researcher(P.T.P.S.) collecting and analyzing the results was indepen-dent of the surgical team and she (P.T.P.S.) also performed93.3% (n � 70) of all clinical examinations and endoscopies.Five endoscopies were performed by 4 other surgeons; 2 dueto local arrangements concerning endoscopies needing seda-tion, 2 due to a patient’s choice and one due to a recentendoscopy just before initiation of this study. The mean ageof the patients at follow-up was 60 years (range, 38–87years), 50 men (58.1%) and 36 women (41.9%). Both thesepatient characteristics and the mean follow-up were compa-rable in both groups.
In this study, we primarily compared the patients in aper-protocol analysis to better detect and elucidate possibledifferences between laparoscopic and open approach for aNissen fundoplication; the 4 conversions were excluded fromthis analysis, leaving a total of 82 patients: 38 in the opengroup and 44 in the LAP group. Of these 82 patients, 3 opengroup patients and 6 LAP group patients underwent only thephone interview. A total of 73 upper gastrointestinal endos-copies were included in the per-protocol analysis. Of these 73patients, 38 were LAP group and 35 were open group pa-tients. Patients and results were also compared in a separateintention-to-treat analysis, including the 4 conversions tolaparotomy in the LAP group; the results of the intention-to-
treat analysis did not differ from the per-protocol analysisresults.
Senior surgeons performed both the laparoscopic andopen operations. In the initial patient series, all of the lapa-roscopic procedures were performed by the same seniorsurgeon (J.T.O.) with a personal laparoscopic fundoplicationexperience of 20 procedures before the initiation of thisrandomized study. This surgeon (J.T.O.) also operated 11 ofthe patients in the open group of this follow-up patient series.Of the remaining 26 open group patients, 13 patients wereoperated on by another senior surgeon (A.P.T.R.) and theother 13 open procedures were performed by 6 senior sur-geons (5, 1, 2, 1, 3, and 1 operations per surgeon).
Follow-upThe objective long-term follow-up consisted of an
upper gastrointestinal endoscopy, a clinical examination ofpossible incisional hernias, and an evaluation of the need forfurther examinations. The presence of esophagitis, Barrettesophagus, hiatal hernia, and the endoscopic appearance ofthe plication and lower esophageal sphincter (LES) wasnoted. Esophagitis was evaluated by the Los Angeles classi-fication.15 The diagnosis of Barrett esophagus was confirmedby histology in all cases. The state of the fundic wrap wasevaluated at retroflexed endoscopy and was assessed normalwhen a 270° elevated fold resembling an inverted cone waspresent (Fig. 1). The plication was evaluated disrupted whenno folds or only loose distorted loose folds were visible (Fig.2). In addition to the researcher’s evaluation of the plication,all of the plications were documented by print photographyduring endoscopy. These photos were then used to achieve asecond opinion on the plication appearances by anotherexperienced surgeon. This second evaluation was done inde-pendent of the researcher with similar plication assessmentresults; all of the disrupted plications were also rated dis-rupted in this second analysis.
TABLE 1. Causes of Death in the Open and Laparoscopic Groups
PatientNo.
Age(yr)
OperationYear Open/Laparoscopic
Time ofDeath Cause of Death
1 63 1994 Open 2002 Cholangiocarcinoma
2 77 1994 Open 1997 Acute myocardial infarction
3 75 1994 Open 2004 Pneumonia
4 75 1994 Open 1995 Intracerebral hemorrhage
5 75 1993 Laparoscopic 2002 Pulmonal carcinoma
6 76 1993 Laparoscopic 1996 Prostate carcinoma
7 57 1994 Laparoscopic 1994 Colon carcinoma with liver metastasis
8 59 1994 Open 2001 Alcohol intoxication
9 30 1994 Laparoscopic 1996 Traumatic subdural hematoma
10 74 1994 Open 1999 Acute myocardial infarction
11 57 1994 Open 1995 Liver cirrhosis
12 56 1994 Open 2001 Acute leukemia
13 53 1993 Open 1998 Connective tissue disease
14 56 1995 Open 2003 Alcohol intoxication
15 55 1994 Open 2001 Alcohol intoxication
16 56 1992 Open 1999 Suicide
Salminen et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins202

The long-term subjective symptomatic outcome wasinvestigated by personal interviews using a structured ques-tionnaire. Patients were asked to grade their postoperativesymptoms on a scale ranging from 1 (being absent) to 5(having severe symptoms). In the questionnaire, even theslightest symptoms were taken into account; but it was onlythe difficult and severe symptoms that had an impact on thepatients’ everyday life. The following symptoms were asked:heartburn, regurgitation and upper abdominal pain, dyspha-gia, and bloating or increased flatulence. The patients were
also asked to rate the result of their surgery and to statewhether they would still prefer surgery to medication as theoptimal treatment of their gastroesophageal reflux disease.Information on the use of acid suppression medications afterantireflux surgery was acquired. The possible operative pro-cedures (dilatations and reoperations) were registered fromthe hospital records.
When comparing categorical variables between surgi-cal approaches, �2 was used. In case of low frequencies,Fisher exact test was applied. T test was used to compare ageand follow-up time between open and LAP groups. P valuesless than 0.05 were considered significant. The statisticalanalyses were carried out using SAS/STAT software, version9.1.3 SP3 of the SAS System for Windows.
RESULTS
Upper Gastrointestinal EndoscopyThe group-specific endoscopic findings are shown in
detail in Table 2. In the whole study group, 4 patients (5.5%)had esophagitis at endoscopy; all of them were grade Aesophagitis and none of these patients used proton pumpinhibitors (PPIs) at the time of endoscopy. Barrett esophaguswas noted in 8 patients; in 3 patients, the condition wasalready previously noted and the only long-segment Barrettesophagus was one of these patients. New-onset Barrettesophagus was discovered in 5 patients: 4 in the LAP groupand one in the open group. All of these LAP group patientshad a very-short-segment Barrett esophagus with an intactplication without esophagitis at endoscopy. The one opengroup patient with a 4-cm-long Barrett esophagus had adisrupted wrap and grade A esophagitis. The appearance ofLES was evaluated normal in 61 patients (83.6%) and loosein 11 patients (15.1%); all of the patients in the latter categoryhad a disrupted plication. In addition, one patient (1.3%) hada relative esophageal stricture at the LES level due to recur-
FIGURE 1. Normal plication at endoscopy.
FIGURE 2. A partially disrupted plication and a hiatal hernia.
TABLE 2. Group-Specific Endoscopic Findings
EndoscopicFindings
Open Group(n � 35)�% (no.)�
Laparoscopic Group(n � 38)�% (no.)� P
Esophagitis 5.7 (2) 5.3 (2) 1.000
Barrett esophagus 5.7 (2) 15.8 (6) 0.2643
LES evaluatedloose
25.7 (9) 5.3 (2) 0.0080*
Esophagealstricture
2.9 (1) 0.0 (0)
Hiatal hernia 37.1 (14) 26.3 (10) 0.4498
Partial plicationdisruption
28.6 (10) 10.5 (4) 0.0296†
Total plicationdisruption
11.4 (4) 2.6 (1)
Ventricular ulcer 5.7 (2) 5.3 (2) —
Duodenal ulcer 0.0 (0) 2.6 (1) —
*The one esophageal stricture was included in the statistical analysis of LESappearance.
†Both partial and total wrap disruptions were analyzed together as disruptedplications versus intact plications.
LES indicates lower esophageal sphincter.
Annals of Surgery • Volume 246, Number 2, August 2007 Open vs. Laparoscopic Fundoplication
© 2007 Lippincott Williams & Wilkins 203

rent reflux resulting from a disrupted plication. Hiatal herniawas noted in 23 patients (31.5%). In the whole study group,there were 3 ventricular ulcers and one duodenal ulcer; all butone of these patients were asymptomatic. Helicobacter pyloriwas detected in 14 patients; 2 of the ventricular ulcer patientswere Helicobacter pylori-positive.
At follow-up endoscopy, 14 of 35 (40.0%) fundicwraps were defective in the open group. Of these 14 plica-tions, 10 were evaluated partially disrupted and in the remain-ing 4 patients there were no plication folds visible. Corre-spondingly in the LAP group 5 of 38 (13.2%) plications weredefective: one totally disrupted wrap and 4 partially disruptedplications (P � 0.0152). Four of these patients (5.5%) hadesophagitis at follow-up endoscopy: 2 patients in bothgroups. The remaining 15 of 19 patients with disruptedplications presented no esophagitis, but 10 of these 15 pa-tients used PPI at the time of follow-up endoscopy. Com-pared with patients with an intact plication, the incidence ofesophagitis was significantly higher with a defective plication(P � 0.0032). There was no correlation between the use ofantireflux medication and fundoplication failure; 52.6% ofthe patients with a disrupted wrap had reinstated the medi-cation compared with 35.7% of the patients with an intactplication (P � 0.2785); 26.3% (n � 5) of the patients with adefective wrap complained of difficult or severe upper ab-dominal symptoms, 21.1% (n � 4) had moderate symptomsand 52.6% (n � 10) presented no or only mild symptoms. Inpatients with an intact fundoplication wrap, these percentageswere 16.7% (n � 9), 7.4% (n � 4), and 76.8% (n � 41),respectively.
Incisional HerniasA careful clinical examination of incisional hernias was
conducted during the outpatient visit; none of the patients hadundergone hernia repair prior to this study period. None ofthe patients in the LAP group had incisional hernias. Tenpatients (28.6%) in the open group had an incisional hernia(P � 0.001), but all of them were yet small and asymptomaticand thus none of them were referred to surgery at this point.
Reoperations and DilatationsThree patients in the open group needed a refundopli-
cation: 2 due to a disrupted plication and one due thedysphagia based on a distorted plication. There was onereoperation in the LAP group due to a problematic ventricleretention suspected to result from a vagus nerve lesion; thispatient underwent a successful gastrojejunostomy. In addi-tion, there were 2 LAP group patients that needed one to 2dilatations due to dysphagia.
Subjective Symptomatic OutcomeFigures 3 to 5 show the group-specific results on a
5-point scale; the occurrence percentages are quite similar inboth groups. In the whole study group, 73.2% (n � 60) ofthe patients had no or only mild upper abdominal symp-toms, including heartburn or regurgitation; 9.8% of thepatients (n � 8) had moderate symptoms and 17.0% of thepatients (n � 14) suffered from difficult upper abdominalsymptoms; 83.0% (n � 68) of the patients had no signif-
icant dysphagia postoperatively, 13.4% (n � 11) hadoccasional difficulties with swallowing and 3.6% (n � 3)had difficult or severe dysphagia. Bloating and the presenceof increased passage of flatus were the most common post-operative complaint; 45.1% (n � 37) of the patients reportedthe severity of this symptom to be clearly disturbing, 19.5%(n � 16) had moderate symptoms, and 35.4% (n � 29)reported of absent or only mild symptoms.
The patients were also given a 5-point scale to evaluatethe result of their surgery, ranging from the result beingexcellent to a poor result; and the group-specific evaluationsare shown in Figure 6. In the whole study group, 85.4% (n �70) of the patients rated their surgical result to be excellent,good, or satisfactory; 14.6% (n � 12) of the patients felt thattheir surgical result was only fair or poor; 73.7% (n � 28) ofthe patients in the open group and 81.8% (n � 36) in the LAPgroup would still choose surgery; 7.9% (n � 3) of the patientsin the open group would abstain from surgery and 18.4%
FIGURE 3. Late subjective results of heartburn and regurgita-tion. P � 0.6241.
FIGURE 4. Late subjective results of dysphagia. P � 0.0682.
FIGURE 5. Late subjective results of bloating and flatulence.P � 0.1734.
Salminen et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins204

(n � 7) of the patients in this group were hesitant of theirchoice; these percentages were 11.4% (n � 5) and 6.8% (n �3) in the LAP group.
A total of 39.5% (n � 15) of the patients in the opengroup and 40.9% (n � 18) of the patients in the LAP grouphad started taking acid suppression medications postopera-tively (P � 1.0000). In both groups, the majority of thesepatients used PPIs; 33.3% (n � 5) of these patients in theopen group and 26.3% (n � 5) in the LAP group neededmedication on a daily basis (P � 0.4027); for the rest of thepatients, the need for acid suppression medication was onlyoccasional.
DISCUSSIONLaparoscopic fundoplication is shown to be as effective
as its open counterpart with reduced morbidity, shorter hos-pital stay, and recovery but without any significant differ-ences in early functional results and short-term outcome.1
However, so far, there are only 2 randomized studies com-paring the laparoscopic and open approach for Nissen fun-doplication with a 5-year-follow-up9,14 and long-term fol-low-up of randomized trials exceeding this has not yet beenpublished. In this study, we compared the long-term results oflaparoscopic and open Nissen fundoplication at a mean fol-low-up of 11 years and 5 months after surgery.
In this study, we tried to minimize the risk of biasassociated with the researcher being part of the surgical teamby having an independent surgeon performing the follow-up.The additional strong elements of this present study includethe long mean follow-up and the high attendance rate regard-ing endoscopies and personal interviews. The potential sub-jectivity of postoperative upper gastrointestinal endoscopy wasminimized both by using a single independent researcher per-forming most of the endoscopies and by photographing all of theendoscopic findings for an additional blinded evaluation of theplication by another surgeon experienced in the field.
A distinct disadvantage of this present study is the lackof preoperative symptom scores because in recent years bothdysphagia and bloating have increasingly been considered tobe related to gastroesophageal reflux disease itself, instead ofoccurring as postoperative side effects.16,17 This study wasinitiated in the early 1990s, and at that time the moreobjective validated scoring systems for measuring health-related quality of life had not yet become a standard.
In this study, no statistically significant differenceswere found between the LAP and open group patients inlong-term subjective outcomes such as heartburn and regur-gitation, dysphagia, bloating and increased flatulence, patientsatisfaction, and preference to surgical treatment. Some ran-domized studies comparing laparoscopic and open fundopli-cation have shown somewhat higher incidence of dysphagiain laparoscopically operated patients.3,4,7,10,12 Bais et al5
reported a significantly higher incidence of dysphagia in thelaparoscopic arm in a multicenter trial, which was stopped atinterterm analysis due to this dysphagia incidence. However,in their recently published long-term follow-up evaluation ofthis prematurely terminated randomized trial, Draaisma etal14 found no differences between the subjective and objec-tive results of laparoscopic and conventional Nissen fundo-plication. Other randomized studies also reported similarpostoperative dysphagia incidences in both laparoscopic andopen approaches.11,13 In the long-term follow-up results ofNilsson et al,9 there were also no differences in postoperativedysphagia between the 2 groups in comparison to the some-what higher incidence of mild dysphagia in their laparoscopicgroup at 6 months after surgery.7 As previously reported inour initial study,2 there was no difference in the amount ofdysphagia between the LAP and open groups at 3 or 12months after surgery; and correspondingly in this study, thepostoperative dysphagia rate was similar in both groups.
The number of partially or totally disrupted plicationswas significantly higher (P � 0.0152) in the open group; 14of 35 plications (40.0%) were defective compared with 5 of38 plications (13.2%) in the LAP group. Franzen et al18
reported the durability of open partial fundoplication exceed-ing 90% using patient satisfaction as a definition for durabil-ity of the surgical procedure with a follow-up of 10 years.Rantanen et al19 reported 37% endoscopically documenteddefective plications at 6.5 years after open fundoplication ina community hospital. In a study by Luostarinen,20 109patients treated with open Nissen fundoplication underwentendoscopy at 6 years after surgery; endoscopy showed 24defective wraps (22.9%). One of the weaknesses in our studyis the number of surgeons in the open group compared withone surgeon performing all of the operations in the LAPgroup; and this might have an effect on the higher incidenceof defective wraps in the open group. On the other hand, ofthe 14 patients with defective plications in the open group, 2patients were asymptomatic, 5 had occasional symptoms, 3had moderate symptoms, and only 4 suffered from difficult orsevere heartburn and regurgitation affecting daily life. De-spite the objective plication failure rate of 40% in the opengroup, only 18.4% of the open group patients regarded theirsurgical result only fair or poor and 73.7% would againchoose surgery. This constitutes discrepancies between subjec-tive symptomatic outcome and objective endoscopic findings inthe present study as previously found by other studies.20
In this study, approximately 40% of the patients hadreinstated acid suppression medication postoperatively;39.5% (n � 15) in the open group and 40.9% (n � 18) in theLAP group. However, it has to be taken into account that theuse of antireflux medication following antireflux surgery does
FIGURE 6. Subjective results of the evaluation of the surgicalresult. P � 0.7361.
Annals of Surgery • Volume 246, Number 2, August 2007 Open vs. Laparoscopic Fundoplication
© 2007 Lippincott Williams & Wilkins 205

not necessarily correspond to a failure of the surgical proce-dure. A significant proportion of these patients are treated forundifferentiated and vague abdominal or chest symptoms.21
Despite the symptomatic failure of surgical therapy in thesepatients using antireflux medications postoperatively, only asmall proportion of the patients have abnormal distal esoph-ageal acid exposure on 24-hour pH monitoring.14,22 Never-theless, this suggests that patients considering antireflux sur-gery should not be guaranteed a postoperative life without theneed for antisecretory medications.
At long-term follow-up, the open and laparoscopicapproaches for the Nissen fundoplication have similar long-term subjective symptomatic outcome; there was virtually nodifference in terms of clinical outcome between the groupsdespite the significantly higher incidence of incisional herniasand defective fundic wraps at endoscopy in the open group.The most important long-term quality measurement is indeedthe patients’ subjective symptomatic outcome due to gastro-esophageal reflux disease being a benign functional disorder.However, the objective endoscopic findings of defectiveplication rates of 40.0% (open) and 13.1% (LAP) somewhatquestion the durability of the procedure at long-term follow-up, and this suggests that patients considering antirefluxsurgery should not be guaranteed a permanent relief of refluxsymptoms or a postoperative life without the need for anti-secretory medications. This emphasizes the importance ofadequate preoperative information and appropriate patientselection in securing good outcomes and long-term patientsatisfaction.
CONCLUSIONAt long-term follow-up, laparoscopic Nissen fundopli-
cation is as safe and effective as its open counterpart and isassociated with significantly fewer defective plications andincisional hernias. It should thus be considered as the proce-dure of choice in surgical management of gastroesophagealreflux disease.
REFERENCES1. Catarci M, Gentileschi P, Papi C, et al. Evidence-based appraisal of
antireflux fundoplication. Ann Surg. 2004;239:325–337.2. Laine S, Rantala A, Gullichsen R, et al. Laparoscopic vs conventional
Nissen fundoplication: a prospective randomized study. Surg Endosc.1997;11:441–444.
3. Heikkinen TJ, Haukipuro K, Koivukangas P, et al. Comparison of costsbetween laparoscopic and open Nissen fundoplication: a prospectiverandomized study with a 3-month followup. J Am Coll Surg. 1999;188:368–376.
4. Heikkinen TJ, Haukipuro K, Bringman S, et al. Comparison of laparo-
scopic and open Nissen fundoplication 2 years after operation: a pro-spective randomized trial. Surg Endosc. 2000;14:1019–1023.
5. Bais JE, Bartelsman JF, Bonjer HJ, et al. Laparoscopic or conventionalNissen fundoplication for gastro-oesophageal reflux disease: randomisedclinical trial. The Netherlands Antireflux Surgery Study Group. Lancet.2000;355:170–174.
6. Nilsson G, Larsson S, Johnsson F. Randomized clinical trial of laparo-scopic versus open fundoplication: blind evaluation of recovery anddischarge period. Br J Surg. 2000;87:873–878.
7. Wenner J, Nilsson G, Oberg S, et al. Short-term outcome after laparo-scopic and open 360 degrees fundoplication: a prospective randomizedtrial. Surg Endosc. 2001;15:1124–1128.
8. Nilsson G, Larsson S, Johnsson F. Randomized clinical trial of laparo-scopic versus open fundoplication: evaluation of psychological well-being and changes in everyday life from a patient perspective. Scand JGastroenterol. 2002;37:385–391.
9. Nilsson G, Wenner J, Larsson S, et al. Randomized clinical trial oflaparoscopic versus open fundoplication for gastro-oesophageal reflux.Br J Surg. 2004;91:552–559.
10. Luostarinen M, Virtanen J, Koskinen M, et al. Dysphagia and oesoph-ageal clearance after laparoscopic versus open Nissen fundoplication: arandomized, prospective trial. Scand J Gastroenterol. 2001;36:565–571.
11. Chrysos E, Tsiaoussis J, Athanasakis E, et al. Laparoscopic vs openapproach for Nissen fundoplication: a comparative study. Surg Endosc.2002;16:1679–1684.
12. Franzen T, Anderberg B, Wiren M, et al. Long-term outcome is worseafter laparoscopic than after conventional Nissen fundoplication. ScandJ Gastroenterol. 2005;40:1261–1268.
13. Ackroyd R, Watson DI, Majeed AW, et al. Randomized clinical trial oflaparoscopic versus open fundoplication for gastro-oesophageal refluxdisease. Br J Surg. 2004;91:975–982.
14. Draaisma WA, Rijnhart-de Jong HG, Broeders IA, et al. Five-yearsubjective and objective results of laparoscopic and conventional Nissenfundoplication: a randomized trial. Ann Surg. 2006;244:34–41.
15. Armstrong D, Bennett JR, Blum AL, et al. The endoscopic assessmentof esophagitis: a progress report on observer agreement. Gastroenterol-ogy. 1996;111:85–92.
16. Wetscher GJ, Glaser K, Gadenstaetter M, et al. The effect of medicaltherapy and antireflux surgery on dysphagia in patients with gastro-esophageal reflux disease without esophageal stricture. Am J Surg.1999;177:189–192.
17. Anvari M, Allen C. Postprandial bloating after laparoscopic Nissenfundoplication. Can J Surg. 2001;44:440–444.
18. Franzen T, Bostrom J, Tibbling Grahn L, et al. Prospective study ofsymptoms and gastro-oesophageal reflux 10 years after posterior partialfundoplication. Br J Surg. 1999;86:956–960.
19. Rantanen TK, Halme TV, Luostarinen ME, et al. The long term resultsof open antireflux surgery in a community-based health care center. Am JGastroenterol. 1999;94:1777–1781.
20. Luostarinen M. Nissen fundoplication for reflux esophagitis: long-termclinical and endoscopic results in 109 of 127 consecutive patients. AnnSurg. 1993;217:329–337.
21. Bammer T, Hinder RA, Klaus A, et al. Five- to eight-year outcome ofthe first laparoscopic Nissen fundoplications. J Gastrointest Surg. 2001;5:42–48.
22. Lord RV, Kaminski A, Oberg S, et al. Absence of gastroesophagealreflux disease in a majority of patients taking acid suppression medica-tions after Nissen fundoplication. J Gastrointest Surg. 2002;6:3–9;discussion 10.
Salminen et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins206

RANDOMIZED CONTROLLED TRIALS
Defunctioning Stoma Reduces Symptomatic AnastomoticLeakage After Low Anterior Resection of the Rectum
for CancerA Randomized Multicenter Trial
Peter Matthiessen, MD, PhD,* Olof Hallbook, MD, PhD,‡ Jorgen Rutegård, MD, PhD,*Goran Simert, MD, PhD,† and Rune Sjodahl, MD, PhD‡
Objective: The aim of this randomized multicenter trial was toassess the rate of symptomatic anastomotic leakage in patientsoperated on with low anterior resection for rectal cancer and whowere intraoperatively randomized to a defunctioning stoma or not.Summary Background Data: The introduction of total mesorectalexcision surgery as the surgical technique of choice for carcinoma inthe lower and mid rectum has led to decreased local recurrence andimproved oncological results. Despite these advances, perioperativemorbidity remains a major issue, and the most feared complication
is symptomatic anastomotic leakage. The role of the defunctioningstoma in regard to anastomotic leakage is controversial and has notbeen assessed in any randomized trial of sufficient size.Methods: From December 1999 to June 2005, a total of 234 patientswere randomized to a defunctioning loop stoma or no loop stoma.Loop ileostomy or loop transverse colostomy was at the choice ofthe surgeon. Inclusion criteria for randomization were expectedsurvival �6 months, informed consent, anastomosis �7 cm abovethe anal verge, negative air leakage test, intact anastomotic rings,and absence of major intraoperative adverse events.Results: The overall rate of symptomatic leakage was 19.2% (45 of234). Patients randomized to a defunctioning stoma (n � 116) hadleakage in 10.3% (12 of 116) and those without stoma (n � 118) in28.0% (33 of 118) (odds ratio � 3.4; 95% confidence interval,1.6–6.9; P � 0.001). The need for urgent abdominal reoperationwas 8.6% (10 of 116) in those randomized to stoma and 25.4% (30of 118) in those without (P � 0.001). After a follow-up of median42 months (range, 6–72 months), 13.8% (16 of 116) of the initiallydefunctioned patients still had a stoma of any kind, compared with16.9% (20 of 118) those not defunctioned (not significant). The30-day mortality after anterior resection was 0.4% (1 of 234) andafter elective reversal a defunctioning stoma 0.9% (1 of 111).Median age was 68 years (range, 32–86 years), 45.3% (106 of 234)were females, 79.1% (185 of 234) had preoperative radiotherapy, thelevel of anastomosis was median 5 cm, and intraoperative blood loss550 mL, without differences between the groups.Conclusion: Defunctioning loop stoma decreased the rate of symp-tomatic anastomotic leakage and is therefore recommended in lowanterior resection for rectal cancer.
(Ann Surg 2007;246: 207–214)
The understanding of the mesorectal spread in rectal cancerand the introduction of total mesorectal excision surgery
as the surgical technique of choice for carcinoma in the lowerand mid rectum has led to decreased local recurrence andimproved oncologic outcome.1–3 Improved results have alsobeen demonstrated by centralization of surgery and educa-tional programs for colorectal surgeons.4,5 Despite these
From the *Department of Surgery, at *Orebro University Hospital, Orebro,Sweden; †Department of Surgery, Hoglandssjukhuset, Eksjo, Sweden;and ‡Department of Surgery, Linkoping University Hospital, Linkoping,Sweden, for the RECTODES study group (Rectal Cancer Trial onDefunctioning Stoma).
The following units participated in the RECTODES study group (REctalCancer Trial On DEfunctioning Stoma) and the surgeons responsible forthe trial were:
Lars Påhlman, Akademiska Sjukhuset, UppsalaPeter Andersson, Blekingesjukhuset, KarlskronaJohan Ottosson, Centralsjukhuset, KristianstadBjorn Ojerskog, Sahlgrenska Universitetssjukhuset/Ostra, GoteborgTorbjorn Holm, Karolinska Universitetssjukhuset/Solna, StockholmAsbjorn Osterberg, Mora LasarettInger Magnusson, Sodersjukhuset, StockholmIngvar Syk, Universitetssjukhuset MAS, MalmoGeorge Falco de Mats, Karlskoga LasarettMichael Dahlberg, Sunderby Sjukhus, LuleåDisa Kalman, Vrinnevisjukhuset, NorrkopingBo Fagerkvist, Sjukhuset i LidkopingUlf Kressner, Uddevalla SjukhusMartin Jansson, Karolinska Universitetssjukhuset/Huddinge, StockholmConny Svensson, Ostersunds LasarettÅke Oberg, Norrlands Universitetssjukhus, UmeåRolf Hellberg, Malarsjukhuset, EskilstunaHåkan Olsson, Skellefteå LasarettGoran Simert, Hoglandssjukhuset, EksjoOlof Hallbook, Universitetssjukhuset, LinkopingPeter Matthiessen, Universitetssjukhuset, OrebroSupported by a grant from the Research Committee, Orebro County Council,
Sweden.Reprints: Peter Matthiessen, MD, PhD, Department of Surgery, Orebro Uni-
versity Hospital, 701 85 Orebro, Sweden. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0207DOI: 10.1097/SLA.0b013e3180603024
Annals of Surgery • Volume 246, Number 2, August 2007 207

important advances, postoperative morbidity and early mor-tality after anterior resection of the rectum remain importantissues.6 The overall early postoperative mortality rate isreported to be between 1% and 8%.4 Symptomatic anasto-motic leakage is the most feared complication and has beenreported to occur in between 1% and 24%,7–12 and whenpresent, the associated risk of postoperative mortality isincreased to between 6% and 22%.11 One can anticipate thatanastomotic leakage occurs in a medically fragile patient, orafter a technically difficult operation, or if intraoperativeadverse events were present. However, anastomotic leakagealso occurs in patients with no obvious risk factors.13 Thedifficulty in predicting anastomotic leakage, including pa-tients considered to be at low risk, has generated severalstudies in recent years with the aim of identifying riskfactors.10–12,14 The most common risk factors for leakage inretrospective studies with multivariable analysis are lowanastomosis and male gender.11,12 One risk factor demon-strated in retrospective studies with multivariable analysis isthe absence of a defunctioning stoma.9,15 However, data areconflicting and in population-based retrospective studies, in-cluding multivariable analysis, lower leakage rates have notbeen demonstrated in patients with defunctioning stoma.16 Thereare 3 randomized studies addressing this issue, by Graffner etal,17 Pakkastie et al,8 and Pimentel et al,18 comprising 50, 38 and36 randomized patients, respectively. In these studies, no firmconclusions could be drawn due to small numbers.
The primary aim of the present trial was to assesswhether there was a difference in the rate of symptomaticanastomotic leakage in patients randomized intraoperativelyto fecal deviation or not. When the present trial was plannedin the late 1990s, there was no consensus in Sweden regard-ing type of defunctioning stoma; therefore, the study protocolaccepted the use of loop ileostomy as well as loop transversecolostomy. Secondary aims were the assessment of postop-erative morbidity and the outcome regarding reversal of thedefunctioning stoma.
METHODS AND PATIENTS
Study DesignAll hospitals in Sweden performing rectal cancer sur-
gery in 1999 (n � 65) were asked to participate in the presentstudy, the REctal Cancer Trial On DEfunctioning Stoma(RECTODES). All patients operated on with anterior resec-tion of the rectum for cancer during the period of participa-tion of each hospital were analyzed. To assess possibleselection bias, the randomized patients were compared withthe nonrandomized patients. Data on the randomized patientswere obtained from the RECTODES study protocol. Data onpatients not randomized were obtained from the SwedishRectal Cancer Registry.19 All randomized patients were as-sessed according to the study protocol: preoperatively, duringthe hospital stay, at one and at 12 months after the initialrectal resection, and, in patients with a defunctioning stoma,at the time of the reversal of the stoma, and when the patienthad been free of stoma for 12 months. The study wasapproved by the local ethics committee of the Linkoping
healthcare region and by the local ethic committees of each ofthe participating hospitals.
Inclusion Criteria and RandomizationProcedure
Preoperative inclusion criteria were biopsy proven ad-enocarcinoma of the rectum located at �15 cm above the analverge measured with a rigid rectoscope, age �18 years,informed consent, ability to understand the study information,and estimated survival of �6 months as judged by thesurgeon. Intraoperative inclusion criteria were anastomosis at�7 cm above the anal verge, negative air leakage test, intactanastomotic stapler rings, and the absence of major intraop-erative adverse events as judged by the operating surgeon.
If no exclusion criteria were present, the patient wasrandomized intraoperatively after the construction and testingof the anastomosis, by opening a sealed envelope in theoperating room. All patients had preoperative bowel prepa-ration and prophylactic antibiotics according to the standardtreatment of each hospital. Furthermore, preoperative irradi-ation, chemotherapy, and the use of pelvic drainage were atthe choice of the surgeon.
Definition of Anastomotic LeakageThe definition of anastomotic leakage was clinical;
peritonitis caused by leakage from any staple line, rectovagi-nal fistula, and pelvic abscess without radiologically provenleakage mechanism were included. Leakage was verified byclinical (digital palpation, inspection of drain contents), en-doscopic (rigid rectoscopy, flexible sigmoidoscopy), or radio-logic (rectal contrast study, CT scan) investigations. Radio-logically demonstrated leakage without clinical symptomswas not included.
Study Hypothesis and Statistical AnalysisThe study hypothesis was that a defunctioning stoma
decreases the rate of symptomatic leakage from 15% to 7.5%.With a statistical power of 80% and a level of significance at5%, randomization of 220 patients was required. For com-parison between groups, the �2 test was used for categoricaldata and the Mann-Whitney U test for continuous data.
A P value of less than 5% was considered significant.For statistical analysis, the SPSS for Windows version 12(Chicago, IL) and the Statistix version 8 (Tallahassee, FL)were used.
RESULTS
Comparison Between Randomized andNonrandomized Patients
Between December 1999 and June 2005, a total of 234patients were randomized by 21 hospitals participating for amean of 21 months during this time period. Of all the anteriorresections performed by the participating hospitals, 28.5%(234 of 821) were randomized and 71.5% (587 of 821) werenot. The most frequent reasons for not randomizing patientswere the presence of intraoperative adverse events promptinga defunctioning stoma (28%), absence of patient consent(25%), anastomosis �7 cm above the anal verge (18%), and
Matthiessen et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins208

advanced TNM stage IV cancer or T4 cancer (10%) (Table1). The randomized patients had a lower proportion of TNMstage IV cancer and more often had preoperative radiotherapycompared with those not randomized, but in all other respectsthere were no differences between the groups (Table 2).
Patient Demography and Operative Details inthe Randomized Patients
The operation time was longer in those randomized toa stoma, 220 versus 200 minutes; otherwise, there were no
differences between the groups regarding patient demographyand intraoperative details (Table 3).
Anastomotic LeakageThe total rate of symptomatic anastomotic leakage was
19.2% (45 of 234 patients). Randomization yielded 116patients with defunctioning stoma and 118 without defunc-tioning stoma. In patients with a defunctioning stoma, asymptomatic leakage occurred in 10.3% (12 of 116), com-pared with 28.0% (33 of 118) of those without defunctioningstoma (28.0% vs. 10.3%; odds ratio �OR� � 3.4; 95%confidence interval �CI�, 1.6–6.9; P � 0.001) (Table 4). In 27patients (60% of those with a leak), the symptomatic leakagewas diagnosed during the initial hospital stay at median day8 (range, 3–18 days). The other 18 patients (40% of thosewith a leak) with symptomatic leakage were initially dis-charged from hospital on median day 10 (range, 7–31 days)and had their leakage diagnosed upon readmission during asecond hospital stay on median day 24 (range, 13–172 days).Nine of 106 women (8.5%) developed rectovaginal fistula,which accounted for 9 of 45 of all the leakages and 9 of 21 ofall leakages in women. In the patients initially not defunc-tioned who had a rectovaginal fistula, 6 of 7 were reoperatedwith a laparotomy and a loop stoma on median day 26 (range,12–152 days). In those initially not defunctioned who had aleakage other than rectovaginal fistula, 22 of 26 patients werereoperated with a laparotomy and loop stoma. There was nodifference in leakage rates between those irradiated and notirradiated (20.7% vs. 13.3%; not significant). The most com-mon ways of initial diagnosis of the leakage were by CT scan(n � 13), rectal contrast study (n � 11), and rectal digitalpalpation (n � 8).
Anastomotic Leakage and Type of AnastomosisAll 234 anastomoses were made with a circular stapler
device, and none was hand-sewn. A J-pouch was constructedin 43.6% (102 of 234), a side-to-end anastomosis in 38.9%(91 of 234), an end-to-end anastomosis in 16.2% (n � 38 of234), and 1.3% (3 of 234) the type of anastomosis was not
TABLE 1. Reasons for Not Randomizing Patients Operatedon for Anterior Resection of the Rectum for Cancer in 21Swedish Hospitals During the Time of Participation of EachHospital
Reason %
Preop. reason
No patient consent 25
Patient not asked by the surgeon 6
Patient unable to understand trial information 2
Advanced stage IV cancer or T4 cancer 10
Major comorbidity 3
Two primary cancers 2
Rectal cancer recurrence 1
Planned as partial mesorectal excision 1
Other reasons 1
Intraop. reason
Intraop. adverse events 28
Whereof technically difficult operation 14
Pos. air leakage test 5
Anastomotic stapler rings not intact 4
Major intraop. bleeding 4
Perforation of the tumor or rectum 1
Anastomosis �7 cm 18
Anastomosis considered ultra-low 3
Based on prospectively reported nonrandomized patients (n � 307); retrospectivelyreported nonrandomized patients or data missing (n � 280).
TABLE 2. Study Population Demography
Not Randomized*(n � 587)
Randomized to Stoma(n � 116)
Randomized to No Stoma(n � 118) P†
Age (yr) �median (range)� 69 (28–90) 68 (32–86) 67.5 (4–84) NS‡
Female gender 44.3% 39.7% (46/116) 50.8% (60/118) NS§
Body mass index Not stated 25.0 (19.3–35.9) 24.8 (21.1–36.6) —‡
ASA score 1 or 2 Not stated 83.2% 89.2% —§
Tumor level above the anal
Verge (cm) �median (range)� 10 (3–15) 10 (4–15) 10 (3–15) NS‡
TNM stage IV cancer 17.0% 4.3% 3.4% �0.001§
Preop. radiotherapy 54.9% 81.0% (94/116) 77.1% (91/118) �0.001§
The total cohort of patients operated on with low anterior resection for rectal cancer in the population served by the participating hospitals duringtheir time period of participation in this trial.
*Data on patients not randomized from the Swedish Rectal Cancer Registry (SRCR). Data from the SRCR available until December 31, 2004.Data from January 1 to June 30, 2005 not included in the analysis.
†Comparison between the nonrandomized patients and the group of all randomized patients.‡Mann-Whitney U test.§�2 test.NS indicates not significant; ASA, American Society of Anesthesiologists.
Annals of Surgery • Volume 246, Number 2, August 2007 Defunctioning Stoma
© 2007 Lippincott Williams & Wilkins 209

stated. There were no differences in leakage rates between thedifferent types of anastomoses: J-pouch 21.6% (22 of 102),side to end 19.8.% (18 of 91), and end to end 13.2% (5 of 38)(not significant, �2 test for trend).
Duration of Hospital StayThe initial hospital stay was median 11 days (range,
5–81 days) for the whole group. For patients initially defunc-tioned, it was median 13 days (range, 6–60 days); and forpatients initially not defunctioned, it was median 9 days(range, 5–81 days). When adding the time for scheduled andunscheduled readmission, hospital stay was median 18 days(range, 8–66 days) and 10 days (range, 5–85 days) ininitially defunctioned and nondefunctioned patients, respec-tively (Table 5).
Outcome in Patients Initially DefunctionedStoma Reversal
In the 116 patients with a defunctioning stoma, 112(96.6%) had a loop ileostomy and 4 a transverse loop colos-tomy. Of these patients, 86.2% (100 of 116) had their stomareversed at median 5 months (range, 1–22 months) after therectal excision, while 16 had not been reversed for variousreasons at median 42 months of follow-up (range, 6–72months) (Table 6). Of 12 patients with defunctioning stomaand leakage, 8 were electively reversed after median 8months (range, 2–22 months) of whom one later had a
permanent end sigmoidostomy because of poor anorectalfunction after reversal of the defunctioning stoma. Subse-quently, 7 of 12 patients with leakage in this group werefree of stoma at median 42 months (range, 6 –72 months)follow-up.
ReoperationsSeven patients (6.0%) were urgently reoperated during
the initial hospital stay on median day 10 (range, 7–37 days),one patient was urgently reoperated after hospital dischargeafter 2 months, 2 patients were urgently reoperated afterstoma reversal, and 2 were electively reoperated after stomareversal. One patient with an abscess after stoma reversal waspercutaneously drained (Table 7).
Outcome in Patients Initially Not DefunctionedReoperation for Leakage and Stoma Reversal
In 118 patients without defunctioning stoma, 33 pa-tients (28.0%) developed symptomatic leakage, of which 28were reoperated urgently with laparotomy and loop ileostomy(n � 25) or permanent end sigmoidostomy (n � 3). Fivepatients were treated with anorectal drainage but withoutabdominal surgery (“conservative treatment”). Eleven of 25patients with a loop stoma (44.0%) had their stomas reversedafter median 10 months (range, 4–11 months) and 3 of thesepatients later had a permanent end sigmoidostomy fashionedbecause of poor anorectal function. Thus, 8 of 25 patientswith leakage were free of stoma at median 42 months (range,6–72 months) follow-up. One patient died in septic compli-cations after 8 months and 5 reoperations, and one patientdied in septic complications after an elective conversion of aloop ileostomy to a permanent sigmoidostomy, 30 monthsafter the rectal resection
Other ReoperationsTwo patients, not defunctioned, were urgently reoper-
ated during the initial hospital stay (postoperative day 18 and21), and 2 patients were electively reoperated (after 7 and 22months) (Table 7). One urgently defunctioned patient devel-oped an enterocutaneous fistula from the loop ileostomy, andthis fistula was managed conservatively.
TABLE 3. Operative Details in the Randomized Patients
Stoma*(n � 116)
No Stoma†
(n � 118)
Operation time (min) 220 (110–605) 200 (100–541)
Intraop. bleeding (mL) 550 (50–4500) 550 (50–2500)
Anastomotic level (cm)�median (range)�
5 (2–7) 5 (2–7)
Defunctioning stoma (%) 99.1 0.8
Patients operated on with low anterior resection for rectal cancer in the 21 hospitalsparticipating in the present study from December 1999 to June 2005 and randomized todefunctioning stoma (n � 116) or no defunctioning stoma (n � 118).
*Including 1 case of violation of the study protocol analyzed on intention to treatbasis.
†Including 1 case of violation of the study protocol analyzed on intention to treatbasis.
TABLE 4. Symptomatic Anastomotic Leakage Rate
Stoma(n � 116)
No Stoma(n � 118) P
Leakage, all patients 10.3% (12/116) 28.2% (33/118) �0.001*
Leakage, men 10.0% (7/70) 29.3% (17/58) 0.005*
Leakage, women 10.9% (5/46) 26.7% (16/60) 0.043*
Leakage, women, not including rectovaginal fistula 6.5% (3/46) 15.0% (9/60) 0.172*
Leakage, all patients, not including rectovaginal fistula 8.6% (10/116) 22.2% (26/118) 0.003*
Patients with stoma (loop stoma or end colostomy) atmedian 42 mo (range, 6–72 mo) follow-up
13.8% (16/116) 16.9% (20/118) NS*
Aspects on symptomatic leakage rate and prevailing stoma in patients operated on with low anterior resection for rectal cancer and randomizedto defunctioning stoma (n � 116) or no defunctioning stoma (n � 118).
*�2 test.NS indicates not significant.
Matthiessen et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins210

Early MortalityThe 30-day mortality after anterior resection was 0.4%
(1 of 234). An 82-year-old man with hypertension and epi-lepsy, residing alone, randomized to defunctioning stoma,
discharged on day 8, was readmitted on day 13 without feverand with normal CRP because of a minor infection in thestoma wound. He was treated with antibiotics and dischargedon day 21. The pathology report demonstrated a TNM stage
TABLE 5. Hospital Stay
Stoma (n) No Stoma (n) P
Initial hospital stay (days) n � 116 n � 118
Median (range) 13 (6–60) 9 (5–81) �0.001*
Hospital stay including scheduled and unscheduledreadmission† (days)
n � 116 n � 118
Median (range) 18 (8–66) 10 (5–85) �0.001*
Initial hospital stay, no leakage, (days) n � 104 n � 85
Median (range) 11.5 (6–60) 9 (5–21) �0.001*
Hospital stay, no leakage, scheduled andunscheduled readmission† (days)
n � 104 n � 85
Median (range) 17 (8–66) 9 (5–21) �0.001*
Hospital stay, leakage, scheduled and unscheduledreadmission† (days)
n � 12 n � 33
Median (range) 31 (12–42) 27 (8–85) NS*
Aspects on hospital stay in patients operated on with low anterior resection for rectal cancer and randomized to defunctioning stoma (n � 116)or no defunctioning stoma (n � 118).
*Mann-Whitney U test.†Including reversal of defunctioning stoma.NS indicates not significant.
TABLE 6. Reoperations
Stoma(n � 116)
No Stoma(n � 118) P
Urgent reoperation, any type, any hospital stay 10 (8.6%) 30 (25.4%) �0.001*
Elective reoperation, any type, any hospital stay 2 (1.7%) 2 (1.7%)
Urgent reoperation, initial hospital stay
Laparotomy and defunctioning loop stoma — 25
Laparotomy and end sigmoid stoma — 3
Laparotomy and drainage 1 —
Small bowel perforation — 1
Small bowel obstruction, no relation to stoma 3† —
Small bowel obstruction because of stomal hernia 2‡ —
Enterocutaneous fistula from loop ileostomy 1§ —
Wound dehiscence 1� 1
Urgent reoperation after stoma reversal
Anastomotic leakage in ileoileal anastomosis 1 —
Peritonitis due to perforation of the colon 1¶ —
Elective reoperation with stoma present
Stomal hernia — 1
Elective reoperation after stoma reversal
Chronic wound in stoma cicatrix 1 —
Colovesical fistula, permanent colostomy 1 —
Chronic small bowel obstruction — 1
Reoperations in patients operated on with low anterior resection of the rectum for cancer randomized to defunctioning stoma(n � 116) or no defunctioning stoma (n � 118).
*�2 test.†Including one operation upon urgent readmission.‡Including urgent reversal of the stoma in one patient.§Including urgent reversal of the stoma.�One patient operated 3 times.¶Patient died of septic complications on postoperative day 18.
Annals of Surgery • Volume 246, Number 2, August 2007 Defunctioning Stoma
© 2007 Lippincott Williams & Wilkins 211

I cancer. He was found dead in his home on postoperative day29. Autopsy revealed no signs of anastomotic leakage orintra-abdominal infection, and the final cause of death wasdeemed cardiac arrhythmia.
The 30-day mortality after elective reversal of a de-functioning stoma was 0.9% (1 of 111). An 84-year-old manwith pulmonary disease randomized to defunctioning stomaand without leakage after the anterior resection had thedefunctioning stoma reversed 7 months after the anteriorresection and was discharged after an uneventful postopera-tive course on day 5. He was readmitted and urgently reop-erated on postoperative day 10 due to peritonitis and aperforation of the colon was found. Postoperatively pneumo-nia, myocardial infarction, and multiorgan failure developedand death occurred on postoperative day 18.
Violation of the Study ProtocolIn 3 patients (1.3%), there was violation of the study
protocol. One patient was randomized to no stoma before theintegrity of the anastomotic rings was verified and because ofdefective anastomotic rings the patient had a defunctioningstoma. One patient was converted from low anterior resectionto a low Hartmann’s procedure after randomization becauseof massive presacral bleeding, which needed packing. Twodays later, the patient was reoperated with construction of alow anastomosis and a defunctioning stoma.
In 1 patient randomized to defunctioning stoma, previ-ously operated with open cholecystectomy and a jejunoilealshunt because of obesity and, loop ileostomy as well as looptransverse colostomy were abandoned by the surgeon becauseof a short distal ileum and massive post cholecystectomyadhesions. These patients were analyzed on an intention totreat basis and none developed symptomatic leakage.
DISCUSSIONIn this randomized multicenter trial, patients without de-
functioning stoma leaked in 28.0% compared with 10.3% inthose defunctioned. (OR � 3.4; 95% CI, 1.6–6.9; P � 0.001),a result not previously demonstrated in any randomized trial.The overall rate of symptomatic leakage of 19.2% in this trial ishigher than in several previously presented investigations,7,11
comparable with some series21 and lower than some.11 Theleakage rate may appear high taking into account that theoperations were considered free of adverse events at the end ofthe procedure when randomization was performed. However, itis of importance that the definition of symptomatic anastomoticleakage in the present study included leakage from any stapleline, as well as rectovaginal fistula, pelvic abscess withoutradiologically proven leakage mechanism, and also leakagesdiagnosed after hospital discharge.
Defunctioning stoma in low anterior resection has beenconsidered to decrease the leakage rate by some, includingone large retrospective multicenter study by Peeters et al, inwhich defunctioned patients leaked in 9%, compared with24% of those not defunctioned.15 Others have argued that thestoma mitigates the consequences of a leakage but does notlower the leakage rate itself, as was the result in a largeretrospective multicenter study by Gastinger et al, in whichthe leakage rate was 14% with and without defunctioningstoma.16 However, the weakness of these studies, as well asany nonrandomized study, is that it was the surgeon whodecided which patient should have a defunctioning stoma ornot, and that possible selection bias cannot be ruled out inretrospect. The present study, which is based on a powercalculation with a sufficient number of patients, has demon-strated a lower leakage rate in patients randomized to adefunctioning stoma. Therefore, we conclude that the pres-ence of a defunctioning stoma significantly decreases the rateof symptomatic leakage.
The need for urgent laparotomy for any reason wasincreased in patients randomized to no stoma compared withthose defunctioned, 25% and 9%, respectively. In the patientsrandomized to no stoma, 28 of 30 with urgent laparotomy wereoperated on because of leakage and had a stoma. This was notthe situation in those initially defunctioned in whom urgentabdominal surgery was performed only in one patientbecause of symptomatic leakage, but in 9 of 10 for reasonsrelated to the loop stoma or small bowel obstruction. Thus,not only were the patients not defunctioned operated ur-gently more often, but the reasons to operate were alsodifferent. There was a tendency that leakage in patients notdefunctioned was associated with poorer anorectal functioncompared with those with leakage initially defunctioned. Thisobservation is based on the finding that, albeit limited num-bers, nearly two thirds of those initially defunctioned (7 of12) who developed leakage could have their stoma perma-nently reversed, compared with only one third (8 of 25) ofthose initially not defunctioned.
Of the initially defunctioned patients, 13.8% had astoma of any kind after a follow-up of median 3.5 years,compared with 16.9% in those initially not defunctioned (notsignificant). This puts focus on the idea of the defunctioning
TABLE 7. Reasons for Prevailing Stoma
DefunctionedInitially(n � 16)
Not DefunctionedInitially(n � 20)
Poor anorectal function 4 4
Anastomotic stricture — 3
Conversion to end colostomy aturgent reoperation
— 3
Poor medical condition 2 1
Patient refusal of further surgery 1 1*
Loop ileostomy at 24 mo, deemedpermanent
— 1
No decision of reversal at median13 mo (range, 6–22 mo)
— 4
Progressive liver metastases 5 1
New non colorectal cancer 1 1
Waiting for scheduled reversal 2 1
Unexpected death before reversal 1 —
Reasons for prevailing stoma (loop stoma or end colostomy) in patients operated onwith low anterior resection of the rectum for cancer initially defunctioned (n � 16) orinitially not defunctioned (n � 20) at follow-up of median 42 mo (range, 6–72 mo).
*Anastomotic leakage after reversal of loop ileostomy and reoperated with a secondloop ileostomy.
Matthiessen et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins212

stoma, sometimes called temporary stoma, which in one of 6patients, regardless of initial defunctioning or not, in realitybecame a permanent stoma. The expression temporary stomais therefore not appropriate.
The 30-day mortality rate after elective reversal ofelectively and urgently defunctioned patients was 0.9% (1 of111), which compares to 0.5% recently described.16,20 Thisadditional risk of mortality should be included in the totalearly mortality.
Twenty percent of the leakages (9 of 45) were recto-vaginal fistulas. The reported incidence of rectovaginal fistu-las following rectal excision is often low,21 but findingscomparable to the present study were recently reported byKosugi et al.22 In the present trial, 6 of 7 patients withrectovaginal fistulas, initially not defunctioned, were reoper-ated with a laparotomy and a defunctioning stoma. Thiscompares with the nondefunctioned patients with symptom-atic leakage other than rectovaginal fistula of whom 22 of 26were reoperated with a laparotomy and a stoma. This findingsupports both the view that rectovaginal fistula should beregarded as any other symptomatic anastomotic leakage, andthe definition of anastomotic leakage chosen in this trial.
Hospital stay was longer in patients randomized todefunctioning stoma, median 13 versus 9 days. This differ-ence in length of initial hospital stay can probably be ex-plained by the time needed for the patient to learn how tohandle the stoma appliance. If adding scheduled and unsched-uled readmissions, the difference was even more pronounced,median 18 compared with 10 days, and obviously affectshealthcare costs. Late leakages, diagnosed after hospital dis-charge, are not often reported in the literature.23
In the present study, 40% (18 of 45) of the symptomaticleakages were diagnosed after hospital discharge, upon read-mission on median day 24. Late leakages may have a ten-dency to be underdiagnosed, or even underreported, as indi-cated in one meta-analysis.24
In the present study, the randomized patients had pre-operative radiotherapy more often than the nonrandomizedpatients (79.1% vs. 54.9%), which could be one factor ex-plaining the high leak rate as preoperative radiotherapy hasbeen shown to be an independent risk factor in retrospectivemultivariate analysis.12,14 Moreover, there were fewer pa-tients with TNM stage IV cancer (3.9% vs. 17.0%). Theincreased proportion of stage IV cancer in the nonrandomizedgroup explains to a certain degree the decreased proportion ofirradiated patients.
Moreover, these findings could possibly also representa selection bias in the way that the randomized patients,classified as ASA score 1 or 2 in 86%, were considered asmore fit and that there were fewer contraindications forpreoperative radiotherapy, although this cannot be provedsince ASA score is not registered in the Swedish RectalCancer Registry.19
The issue of whether to use a defunctioning loopileostomy or loop colostomy has been the subject of muchdebate.25,26 The participating surgeons in this trial clearlydemonstrated a preference for the loop ileostomy, which wasused in 97% (112 of 116) of all the elective defunctioning
stomas and in all (25 of 25) of the urgent defunctioningstomas. The use of pelvic drainage in rectal cancer surgeryhas recently been questioned.27,28 In the present trial, the useof pelvic drainage was at the choice of the surgeon, whichresulted in pelvic drainage in 97% (227 of 234) of thepatients.
The proportion of eligible patients randomized is notoften stated in surgical trials and needs consideration also inthis trial, in which less than a third of the patients (28.5%)were randomized. Importantly, however, the most frequentexclusion criteria were the presence of intraoperative adverseevents and patient refusal to participate, which accounted formore than half of the reported excluded patients; and becauseof the nature of these exclusion criteria, they could not beinfluenced by the surgeon. All of these factors must be consid-ered when evaluating to what degree the results of this trial canbe generalized and applied on other patient populations.
CONCLUSIONThis randomized multicenter trial has demonstrated a
decreased rate of symptomatic anastomotic leakage in de-functioned patients in low anterior resection, a result notpreviously shown in any randomized trial. Based on theseresults, and taking into account all aspects of the defunction-ing stoma, we can recommend the use of a defunctioningstoma in low anterior resection of the rectum.
ACKNOWLEDGMENTSThe authors thank Anders Magnusson, Department of
Medical Statistics, Orebro University Hospital, for statisticaladvice, and Robert Johansson, Oncological Centre, Univer-sity Hospital, Umeå, for providing data from the SwedishRectal Cancer Registry.
REFERENCES1. Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal cancer
surgery: the clue to pelvic recurrence? Br J Surg. 1982;69:613–616.2. Quirke P, Durdey P, Dixon MF, et al. Local recurrence of rectal
adenocarcinoma due to inadequate surgical resection: histopathologicalstudy of lateral tumour spread and surgical excision. Lancet. 1986;2:996–999.
3. Wibe A, Eriksen MT, Syse A, et al. Total mesorectal excision for rectalcancer: what can be achieved by a national audit? Colorectal Dis.2003;5:471–477.
4. Smedh K, Olsson L, Johansson H, et al. Reduction of postoperativemorbidity and mortality in patients with rectal cancer following theintroduction of a colorectal unit. Br J Surg. 2001;88:273–277.
5. Martling A, Holm T, Rutqvist LE, et al. Impact of a surgical trainingprogramme on rectal cancer outcomes in Stockholm. Br J Surg. 2005;92:225–229.
6. Bokey EL, Chapuis PH, Hughes WJ, et al. Morbidity, mortality andsurvival following resection for carcinoma of the rectum at ConcordHospital. Aust NZ J Surg. 1990;60:253–259.
7. Enker WE, Merchant N, Cohen AM, et al. Safety and efficacy of lowanterior resection for rectal cancer: 681 consecutive cases from aspecialty service. Ann Surg. 1999;230:544–552; discussion 552–554.
8. Pakkastie TE, Ovaska JT, Pekkala ES, et al. A randomized study ofcolostomies in low colorectal anastomoses. Eur J Surg. 1997;163:929–933.
9. Dehni N, Schlegel RD, Cunningham C, et al. Influence of a defunction-ing stoma on leakage rates after low colorectal anastomosis and colonicJ pouch-anal anastomosis �see comment�. Br J Surg. 1998;85:1114–1117.
Annals of Surgery • Volume 246, Number 2, August 2007 Defunctioning Stoma
© 2007 Lippincott Williams & Wilkins 213

10. Law WL, Chu KW. Anterior resection for rectal cancer with mesorectalexcision: a prospective evaluation of 622 patients. Ann Surg. 2004;240:260–268.
11. Rullier E, Laurent C, Garrelon JL, et al. Risk factors for anastomoticleakage after resection of rectal cancer �see comment�. Br J Surg.1998;85:355–358.
12. Matthiessen P, Hallbook O, Andersson M, et al. Risk factors foranastomotic leakage after anterior resection of the rectum. ColorectalDis. 2004;6:462–469.
13. Poon RT, Chu KW, Ho JW, et al. Prospective evaluation of selectivedefunctioning stoma for low anterior resection with total mesorectalexcision. World J Surg. 1999;23:463–467; discussion 467–468.
14. Eriksen MT, Wibe A, Norstein J, et al. Anastomotic leakage followingroutine mesorectal excision for rectal cancer in a national cohort ofpatients. Colorectal Dis. 2005;7:51–57.
15. Peeters KC, Tollenaar RA, Marijnen CA, et al. Risk factors for anasto-motic failure after total mesorectal excision of rectal cancer. Br J Surg.2005;92:211–216.
16. Gastinger I, Marusch F, Steinert R, et al. Protective defunctioning stomain low anterior resection for rectal carcinoma. Br J Surg. 2005;92:1137–1142.
17. Graffner H, Fredlund P, Olsson SA, et al. Protective colostomy in lowanterior resection of the rectum using the EEA stapling instrument: arandomized study. Dis Colon Rectum. 1983;26:87–90.
18. Pimentel JM, Duarte A, Patricio J. The role of a protecting stoma in lowanterior resection with TME and colonic J-pouch for rectal cancer;results of a prospective randomized trial �Abstract�. Colorectal Dis2003;5(suppl 2):P83.
19. Pahlman L, Bohe M, Cedermark B, et al. The Swedish Rectal CancerRegistry. Br J Surg. In press.
20. Hallbook O, Matthiessen P, Leinskold T, et al. Safety of the temporaryloop ileostomy. Colorectal Dis. 2002;4:361–364.
21. Fleshner PR, Schoetz DJ Jr, Roberts PL, et al. Anastomotic-vaginalfistula after colorectal surgery. Dis Colon Rectum. 1992;35:938–943.
22. Kosugi C, Saito N, Kimata Y, et al. Rectovaginal fistulas after rectalcancer surgery: incidence and operative repair by gluteal-fold flap repair.Surgery. 2005;137:329–336.
23. DuBrow RA, David CL, Curley SA. Anastomotic leaks after lowanterior resection for rectal carcinoma: evaluation with CT and bariumenema. AJR Am J Roentgenol. 1995;165:567–571.
24. Bruce J, Krukowski ZH, Al-Khairy G, et al. Systematic review of thedefinition and measurement of anastomotic leak after gastrointestinalsurgery. Br J Surg. 2001;88:1157–1168.
25. Rullier E, Le Toux N, Laurent C, et al. Loop ileostomy versus loopcolostomy for defunctioning low anastomoses during rectal cancersurgery. World J Surg. 2001;25:274–277; discussion 277–278.
26. Law WL, Chu KW, Choi HK. Randomized clinical trial comparing loopileostomy and loop transverse colostomy for faecal diversion followingtotal mesorectal excision. Br J Surg. 2002;89:704–708.
27. Urbach DR, Kennedy ED, Cohen MM. Colon and rectal anastomoses donot require routine drainage: a systematic review and meta-analysis. AnnSurg. 1999;229:174–180.
28. Petrowsky H, Demartines N, Rousson V, et al. Evidence-based value ofprophylactic drainage in gastrointestinal surgery: a systematic reviewand meta-analyses. Ann Surg. 2004;240:1074–1084; discussion 1084–1075.
Matthiessen et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins214

ORIGINAL ARTICLES
Are We Undertreating Rectal Cancer in the Elderly?An Epidemiologic Study
George J. Chang, MD, John M. Skibber, MD, Barry W. Feig, MD, and Miguel Rodriguez-Bigas, MD
Objective: To better understand the reasons for decreased survivalrates in elderly patients with rectal cancer by performing an epide-miologic evaluation of age-related differences in treatment andsurvival.Summary Background Data: The incidence of rectal cancer in-creases with older age, and localized disease can be curativelytreated with stage-appropriate radical surgery. However, older pa-tients have been noted to experience decreased survival.Methods: Patients with localized rectal adenocarcinoma were iden-tified in the Surveillance, Epidemiology, and End Results database(1991–2002). Cancer-specific survival by age, sex, surgery type,tumor grade, lymph node status, and use of radiation therapy wasevaluated using univariate and multivariate regression analysis.Results: We identified 21,390 patients who met the selection crite-ria. The median age was 68 years. Each half-decade increase in age�70 years was associated with a 37% increase in the relative risk(RR) for cancer-related mortality (RR � 1.37; 95% confidenceinterval �CI�, 1.33–1.42); decreased receipt of cancer-directed sur-gery (odds ratio �OR� � 0.56; 95% CI, 0.36–0.63); more localexcision and less radical surgery (OR � 0.76; 95% CI, 0.72–0.81);less radiotherapy (OR � 0.64; 95% CI, 0.61–0.67); and greaterlikelihood of N0 pathologic stage classification (OR � 1.10; 95%CI, 1.05–1.15) (P � 0.0001 for each factor). The effect of age oncancer-specific mortality persisted in multivariate analysis with eachhalf-decade increase in age �70 years resulting in a 31% increase incancer-specific mortality (RR � 1.31; 95% CI, 1.25–1.36; P �0.0001).Conclusions: In elderly patients, rectal cancer is characterized bydecreased cancer-related survival rates that are associated with lessaggressive treatment overall and decreased disease stages at presen-tation. Investigation into the reasons for these treatment differencesmay help to define interventions to improve cancer outcomes.
(Ann Surg 2007;246: 215–221)
Approximately 41,000 new cases and about 15,000 deathsdue to rectal cancer were reported in the United States in
2005, and the incidence increases with increasing age.1 Un-fortunately, a disproportionately poor survival after colorectalcancer diagnosis in elderly patients has been reported.2–5
There are many reasons for the poor survival in these pa-tients, ranging from less aggressive screening strategies todecreased adherence to accepted surgical and adjuvant treat-ment guidelines for rectal cancer.4,6,7 These factors are be-coming increasingly important as the population in the UnitedStates continues to age; in 2003, the average life expectancyat 70 years of age was 14.9 years, and that at 80 years of agewas 9.0 years.
The primary method of curative treatment of local-ized rectal cancer remains surgical resection. Surgicaloptions include transanal excision and radical surgery. Inall but the earliest stages of rectal cancer (T1N0) withoutadverse histologic features, curative treatment is radicalsurgery consisting of surgical removal of the affectedrectum along with its associated lymphatic drainage. Whencompared with radical surgery, use of local excision re-sults in higher local failure rates and decreased survivalrates as the procedures carry the risk of leaving unresectedviable tumor cells within the draining lymph nodes.8
Furthermore, a full evaluation of the nodal basin fordefinitive staging of and further treatment planning forrectal cancer can only be performed after adequate radicalsurgery. Therefore, the proper selection of the appropriatesurgical treatment of rectal cancer is essential both fortherapy and for prognosis.
The data on the types of surgical therapy for rectalcancer used in elderly patients are limited. As clear rela-tionships exist between the use of stage-appropriate surgi-cal treatment and survival for rectal cancer, it is importantto investigate the relationship between the type of surgicaltherapy for rectal cancer and age.8 Therefore, we per-formed an epidemiologic evaluation of age-related differ-ences in rectal cancer treatment and survival using Sur-veillance Epidemiology and End Results (SEER) data tocharacterize the treatment factors that influence outcomeof this disease in elderly patients. We hypothesized thatincreasing age among patients with rectal cancer wasassociated with decreasing cancer-specific survival andthat this difference is related to a decrease in the use ofradical surgery.
From the Department of Surgical Oncology, University of Texas, M.D.Anderson, Cancer Center, Houston, TX.
Presented at the 92nd Clinical Congress of the American College of Sur-geons, Chicago, IL, October 11, 2006.
Reprints: George J. Chang, MD, Department of Surgical Oncology, Univer-sity of Texas, M.D. Anderson Cancer Center, 1515 Holcombe Blvd.,Houston, TX 77030. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0215DOI: 10.1097/SLA.0b013e318070838f
Annals of Surgery • Volume 246, Number 2, August 2007 215

METHODS
Data Source and Case IdentificationA cohort study of all cases of localized rectal cancer
collected in the SEER registry from 1991 to 2002 wasperformed. SEER is a National Cancer Institute program thatobtains and publishes cancer incidence and survival data frompopulation-based cancer registries for approximately 26% ofthe U.S. population; specifically, the program collects data onpatient demographics, primary tumor site, tumor morphologyand stage at diagnosis, first course of treatment, and vitalstatus.9 The time span of 1991 to 2002 was chosen to evaluatethe outcomes of rectal cancer treatment since the publicationof the National Institutes of Health Consensus ConferenceGuidelines for adjuvant therapy for colorectal cancer in1990.10
All patients with adenocarcinoma of the rectum (ex-cluding rectosigmoid) without distant metastases were iden-tified. Patients in whom the diagnosis of rectal cancer was nottheir only cancer diagnosis were excluded. This left a total of21,390 patients with locoregional rectal adenocarcinoma.Baseline patient demographics, including age at diagnosis,sex, race/ethnicity, and year of diagnosis, were evaluated.Because this study used preexisting data with no personalidentifiers, it was exempt from review by our institutionalreview board.
Cancer-related DataThe cancer-related data evaluated for each patient con-
sisted of identification of the use and the type of surgery (eg,local excision versus radical resection) performed using the
SEER variables “site-specific surgery” codes for cases priorto 1998 and “surgery of primary site” codes for cases startingin 1998 (Table 1); use of radiation; tumor grade (well-differentiated, moderately differentiated, poorly differenti-ated, or undifferentiated or anaplastic); and tumor stage usingthe SEER-modified American Joint Committee on Cancerstaging system.11 Patients were considered to have undergonecancer-directed surgery according to the SEER definition (ie,if local excision or radical resection was performed and aspecimen was available for pathologic review). The SEERregistry also codes cause of death; therefore, cancer-specificsurvival was analyzed. Cases were censored if death was dueto a cause other than rectal cancer or the patient was alive atfollow-up.
Survival and Statistical AnalysisBecause colorectal cancers in patients under 50 years of
age are more likely to be associated with genetic predisposi-tion, have a delay in diagnosis, and not be identified byconventional screening, we evaluated actuarial cancer-spe-cific survival rates using Cox regression analysis amongpatients 50 years of age or older. This group consisted of18,890 patients, or 88.3% of the total group. Patients werecategorized into half-decade age groups, which were used asa continuous predictor variable to determine the relative riskfor each half-decade change in age. Patients were thengrouped to those between 50 to 69 years of age and those�70 years of age for further survival and treatment analysis.Univariate analysis was performed to evaluate the effect ofsex, race/ethnicity, tumor grade, tumor stage (stage I or II vs.
TABLE 1. SEER Codes for Type of Surgery Performed
Code Description Classification
SEER Site-Specific Surgery Codes(prior to 1998)
0–10 Eg, no surgical procedure or local destruction without pathologic evaluation No cancer-directed surgery
20 Local surgical excision WITH pathology specimen (includes polypectomy,snare, or laser surgery)
Local excision
30 Anterior/posterior resection, wedge or segmental resection, transsacralrectosigmoidectomy, Hartmann’s operation, partial resection, NOS
Radical surgery
40 Pull-through resection WITH sphincter preservation Radical surgery
50 Abdominoperineal resection Radical surgery
60 Any of codes 30–50 PLUS partial or total removal of other organs Radical surgery
70 Pelvic exenteration (partial or total) Radical surgery
80–90 Surgery of regional and/or distant site(s)/nodes ONLY or surgery NOS Unknown
SEER surgery of the primary site(since 1998)
0–14 Eg, no surgical procedure or local destruction without pathologic evaluation No cancer-directed surgery
20–29 Local tumor excision (WITH PATHOLOGY SPECIMEN) Local excision
30 Wedge or segmental resection; partial proctectomy, NOS Radical surgery
40 Pull through WITH sphincter preservation Radical surgery
50 Total proctectomy Radical surgery
60 Total proctocolectomy, NOS Radical surgery
70 Proctectomy or proctocolectomy WITH an en bloc resection of other organs;pelvic
Radical surgery
80 Proctectomy, NOS Radical surgery
90–99 Surgery, NOS or unknown if cancer-directed surgery performed Unknown
Chang et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins216

III), surgery (local excision vs. radical surgery), radiationtherapy use, and tumor grade on survival using the Kaplan-Meier product-limit method after evaluation for regressionmodel assumptions. Univariate comparisons of survivalamong the categorical groups were performed using theCox-Mantel log-rank test and univariate Cox regression wasperformed to estimate hazard ratios.
Multivariate Cox proportional hazards regression wasperformed to evaluate risk-adjusted outcomes, predicting therisk of dying of rectal cancer. For the multivariate analyses,the independent covariates included those identified by theunivariate comparisons of survival. In addition, the Coxproportional hazards model was evaluated for interactionsbetween the predictor variables. Age-related differences inthe types of surgery performed and tumor related variableswere evaluated using logistic and linear regression models forcategorical and continuous predictor variables, respectively.The proportions of patients receiving different surgical inter-ventions and having different pathologic tumor stages werecompared using logistic regression analysis and the �2 test.Furthermore, the data were evaluated for interactions be-tween age and tumor stage, age and use of any cancer-directed surgery, age and the use radical surgery when can-cer-directed surgery was performed, age and use of radiationtherapy, age and tumor stage, and age and tumor grade.
Statistical analyses were performed using the NumberCruncher Statistical Software program (version 2004, Num-ber Cruncher Statistical Analysis System, Kaysville, UT). Pvalues less than 0.05 were considered statistically significant.
RESULTSThe baseline characteristics of the study patients are
listed in Table 2. Of the 21,390 patients with rectal cancerwho met the study inclusion criteria, the mean age was 66.5years and median age was 68 years with an interquartile rangeof 57 to 77 years. Overall, more patients were male (57.1%)and most patients were white (82.0%, including Hispanic).Most tumors were moderately differentiated (66.4%) andlocalized without apparent regional lymph node involvement(64.8%). The type of surgery performed could be evaluated inall but 128 (0.6%) of the patients.
We could identify the cause of death in all but 389 (5%)of the patients who died during follow-up (n � 8364). Ofthose patients who died, 61.5% had deaths recorded as beingdue to their cancer. The overall 5-year survival rates were70.8%, 54.3%, and 45.5% in patients with stage I, II, and IIIdisease, respectively. The cancer-specific survival rates werebetter (85.8%, 67.8%, and 54.1% in patients with stage I, II,and III disease, respectively).
We next evaluated age (half-decade increments) as aunivariate predictor of cancer-specific survival using Coxregression. Older patients had lower cancer-specific survivalrates than younger patients did (HRdeath 1.12; 95% confidenceinterval �CI�, 1.11–1.14, P � 0.0001) and this associationbetween cancer-specific survival and age was markedly morepronounced in patients �70-year-old (HRdeath 1.37; 95% CI,1.33–1.42, P � 0.0001). We also evaluated other patient-related predictors of survival, including sex and race/ethnic-
ity. The patients’ sex did not affect cancer-specific survival(P � 0.40); however, black patients were more likely to dieof their cancer than were white patients (risk ratio �RR� �1.50; 95% CI, 1.34–1.69, P � 0.0001), whereas Asianpatients were less likely to die of their cancer than whitepatients were (RR � 0.87; 95% CI, 0.79–0.95, P � 0.005)(Table 3).
Tumor factors, including tumor grade (P � 0.0001) andstage (P � 0.0001), were significantly associated with can-cer-specific survival. Because the tumor stage at diagnosismay determine the type of surgery performed as well as theuse of radiation therapy, we evaluated these variables afterstratifying the patients by stage. We compared survival ratesafter radical surgery versus local excision in patients witheach tumor stage at diagnosis. There was no significantdifference in outcome in patients with stage I tumors whounderwent local excision or radical surgery (P � 0.17), butthere was a significant improvement in outcome in patientswith stage II disease after radical surgery when comparedwith local excision (P � 0.0001). We also identified anassociation between the use of adjuvant radiation therapy andpoorer outcomes in patients with stage I disease (P � 0.0001)
TABLE 2. Baseline Patient and Tumor Characteristics
Characteristic No. (%) Patients
Sex
Female 9186 (43.0)
Male 12,204 (57.1)
Ethnicity
White (including Hispanic) 17,537 (82.0)
Asian (including Pacific Island) 2220 (10.4)
Black 1395 (6.5)
Other 238 (1.1)
Tumor grade*
Well differentiated 1896 (8.9)
Moderately differentiated 14,201 (66.4)
Poorly differentiated 3180 (14.9)
Undifferentiated 70 (0.3)
Tumor stage†
I 8549 (40.0)
II 5321 (24.9)
III 5771 (27.0)
Surgery performed‡
No cancer-directed surgery 2312 (10.8)
Local excision 3246 (15.2)
Low anterior resection§ 9324 (43.6)
Abdominoperineal resection 5592 (26.1)
Multivisceral resection 789 (3.7)
Adjuvant radiation therapy�
No 11,404 (53.3)
Yes 9951 (46.5)
*Tumor grade could not be determined in 2043 (9.6%) of patients.†Tumor stage could not be determined in 1749 (8.1%) of patients.‡Type of surgery performed could not be determined for 127 (0.6%) patients.§Includes coloanal anastomosis.�Data regarding the use of radiation therapy could not be determined for 397 (1.9%)
of patients.
Annals of Surgery • Volume 246, Number 2, August 2007 Rectal Cancer in the Elderly
© 2007 Lippincott Williams & Wilkins 217

and better survival outcomes in patients with stage III disease(P � 0.0001) (Table 3).
We also performed Cox multivariate regression analy-sis to adjust for potential confounder effects of the univariatepredictor variables. The use of radical surgery or radiation didnot have consistent effects on outcomes across all stages (eg,radiation associated with increased risk for death for stage Iand improved risk for stage III), in part related to lack of stageappropriate utilization; therefore, these terms were excludedfrom multivariate analysis. Sex was clinically expected topotentially influence age-related life expectancy; therefore, itwas included in the multivariate analysis despite the univar-iate findings. Univariate analysis of age demonstrated that thegreatest age-related effects on cancer-specific survival oc-curred in the patients who were �70 years of age (perhalf-decade: RR � 1.04; 95% CI, 1.0–1.09, P � 0.07 forpatients 50–69 years of age vs. RR � 1.37; 95% CI, 1.33–1.42, P � 0.0001 for patients �70 years of age). Therefore,we performed separate multivariate regression analysis in the2 cohorts. The results of these analyses are shown in Table 4.
Among patients who underwent cancer-directed surgery, in-creasing age was significantly associated with an increasedlikelihood of dying from rectal cancer even after adjustmentfor sex, race/ethnicity, grade, and stage (RR � 1.31; 95% CI,1.25–1.36, P � 0.0001).
We then sought to identify the reasons for the age-related decrease in cancer-specific survival rates. Table 5 liststhe odds ratios associated with each half-decade increase inage for each of the variables listed. The odds of undergoingany cancer directed surgery decreased by 44% (OR � 0.56;95% CI, 0.36–0.63, P � 0.0001) for each 5-year incrementalincrease in age �70 years. When cancer directed surgery wasperformed, each 5-year incremental increase in age over �70years was associated with a 24% reduction in the odds ofundergoing radical surgery (OR � 0.76; 95% CI, 0.72–0.81,P � 0.0001) (Table 5). As age increased, patients weresignificantly more likely to be staged with lymph nodenegative disease than lymph node-positive disease (P �0.0001), but no significant difference existed for classificationwithin one of the 2 node-negative stages (ie, stage I vs. stageII) (P � 0.51) or for histologic grade (P � 0.25–0.90). Asage increased, patients were also less likely to receive adju-vant radiation therapy and more likely to undergo localexcision rather than radical surgery. We determined if agewas associated with an increased use in radiation therapyamong those patients undergoing local excision. Despite anincreased use of local excision, older patients undergoinglocal excision were still less likely to receive radiation ther-apy (OR � 0.90; 95% CI, 0.87–0.94, P � 0.0001, age 50–69years), and this effect was more pronounced among patients�69 years of age (OR � 0.64; 95% CI, 0.61–0.67, P �0.0001).
We then evaluated the association between cancer-specific survival and age for each tumor stage and eachsurgery type (local excision or radical surgery). The effect ofincreasing age on survival after cancer-directed surgery wasgreater in patients with stage I disease when compared withother stages (Table 6). Also, the effect of increasing age wasgreater in patients who underwent local excision than in thosewho underwent radical surgery.
DISCUSSIONOur examination of the SEER registry data demon-
strated that the rectal cancer-specific survival rates decreasedas patient age increased. We also found a decreased use ofany cancer directed treatment, an increased use of localexcision, a decreased use of radical surgery, and a decreasedstage at presentation as the patients’ age increased. The latterobservation is likely to have been a result of understagingbecause of surgical undertreatment, as accurate stage assign-ment may not be possible with local excision.
Cancer-directed and stage-appropriate surgical resec-tion for localized rectal cancer is essential for optimal sur-vival outcomes. The oncologically appropriate treatment,therefore, is local excision for T1 lesions without adverseprognostic features or evidence of lymph node metastasis andradical en bloc resection of the rectum and mesorectum for allother lesions.8,12 Local excision with neoadjuvant chemora-
TABLE 3. Univariate Regression Analysis of Predictors ofCancer-Related Survival
Variable RR 95% CI P
Age 1.12* 1.11–1.14 �0.0001
Age (�70-yr-old cohort) 1.37† 1.33–1.42 �0.0001
Sex
Female 1.0‡
Male 1.02 0.92–1.03 0.40
Ethnicity
White 1.0‡
Black 1.50 1.34–1.69 �0.0001
Asian 0.87 0.79–0.95 0.005
Tumor grade
Well differentiated 1.0‡
Moderately differentiated 1.25 1.13–1.38 0.0001
Poorly differentiated 2.10 1.89–2.33 �0.0001
Undifferentiated 3.37 1.74–6.50 �0.0001
Stage
I 1.0‡
II 2.41 2.21–2.63 �0.0001
III 3.69 3.42–3.98 �0.0001
Radical surgery§
Stage I 1.11 0.96–1.29 0.17
Stage II 0.5 0.43–0.78 �0.0001
Radiation therapy�
Stage I 1.77 1.48–2.12 �0.0001
Stage II 0.93 0.83–1.04 0.19
Stage III 0.71 0.64–0.79 �0.0001
Year of diagnosis¶ 0.96 0.95–0.97 �0.0001
*RR per half decade increase in age �50 years of age, Cox regression.†RR per half decade increase in age for patients �70 years of age, Cox regression.‡Cox regression.§RR versus local excision. Local excision was performed in only 0.8% of patients
with stage III cancers.�RR no radiation therapy.¶RR per year.RR indicates risk ratio.
Chang et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins218

diotherapy for T2N0 lesions is currently being investigated inan ongoing American College of Surgeons Oncology Groupmulticentered clinical trial as local excision alone in thissetting has been associated with increased risk for localfailure and decreased long-term survival rates.13,14
Our findings provide further insight beyond prior re-ports of decreased overall survival among elderly patients
with colorectal cancer.2,4,5 Multiple factors have been proposedto contribute to this decrease in survival including treatmentutilization and patient factors. A potential confounding factor isthat older patients are more likely to die of causes other thantheir cancer resulting in an apparent decrease in the overallsurvival. We therefore evaluated cancer-related survival. In theSEER dataset, misclassification of the cause of death is possible,
TABLE 4. Cox Proportional Hazards Multiple Regression Analysis of Cancer-Related Survival
Variable
Age 50–69 yr (n � 8634)† Age >70 yr (n � 8011)†
RR 95% CI P RR 95% CI P
Age* 1.10 1.05–1.15 �0.0001 1.31 1.25–1.36 �0.0001
Sex
Female 1.0 1.0
Male 1.12 1.01–1.24 0.03 1.10 1.01–1.21 0.036
Ethnicity
White 1.0 1.0
Black 1.50 1.26–1.78 �0.0001 1.45 1.20–1.75 �0.0001
Asian 0.92 0.78–1.08 0.31 0.84 0.70–1.00 0.047
Grade
Well differentiated 1.0 1.0
Moderately differentiated 1.03 0.84–1.27 0.78 1.12 0.94–1.35 0.22
Poorly differentiated 1.53 1.22–1.92 0.0002 1.77 1.45–2.17 �0.0001
Undifferentiated 4.63 2.76–7.76 �0.0001 0.99 0.76–1.28 0.93
Stage
I 1.0 1.0
II 3.05 2.61–3.56 �0.0001 2.22 1.95–2.52 �0.0001
III 5.44 4.71–6.27 �0.0001 3.93 3.48–4.43 �0.0001
*Multivariate model based on covariates identified to be significant or clinically important predictors on univariate analysis.†Includes only patients who underwent cancer-directed surgery.RR indicates risk ratio per half-decade increase in age.
TABLE 5. Univariate Logistic Regression Analysis of Associations Between Predictor Variables and Age
Variable
Age 50–69 yr Age >70 yr
OR 95% CI P OR 95% CI P
Any cancer-directed surgery* 0.99 0.92–1.07 0.79 0.56 0.36–0.63 �0.0001
Radical surgery† 0.95 0.24–0.99 0.08 0.76 0.72–0.81 �0.0001
Grade*
1 1.0 1.0
2 1.05 0.98–1.12 0.20 1.0 0.93–1.06 0.90
3 0.97 0.90–1.06 0.52 0.96 0.89–1.04 0.34
4 1.51 0.98–1.19 0.02 0.80 0.54–1.17 0.25
Stage†
N0 vs. N� 1.06 1.02–1.11 0.004 1.10 1.05–1.15 0.0001
I vs. III 1.07 1.02–1.12 0.004 1.09 1.04–1.15 0.0008
II vs. III 1.05 1.00–1.11 0.05 1.11 1.05–1.18 0.0003
I vs. II 1.02 0.97–1.07 0.54 0.98 0.93–1.03 0.51
Use of adjuvant radiation therapy†
All stages 0.90 0.87–0.94 �0.0001 0.64 0.61–0.67 �0.0001
Stage I 0.96 0.90–1.03 0.29 0.85 0.78–0.93 0.0003
Stages II–III 0.84 0.79–0.89 �0.0001 0.53 0.50–0.57 �0.0001
OR indicates odds ratio for each half-decade increase in age.*Age 50–69 yr group, n � 9308; age �70 yr group, n � 8059.†Among patients undergoing cancer-directed surgery: age 50–69 yr group, n � 8634; age �70 yr group, n � 8011.
Annals of Surgery • Volume 246, Number 2, August 2007 Rectal Cancer in the Elderly
© 2007 Lippincott Williams & Wilkins 219

but our method of censoring cases by cause of death would haveresulted in a bias toward underestimation of the effect of age oncancer-related deaths in our analysis.
To determine the potential contribution of the type ofsurgical therapy to decreased survival rates among the elderlypatients with rectal cancer, we first examined the use of anycancer-directed surgery and identified a significantly de-creased use of cancer-directed surgery among the elderly. Inthis study, elderly patients were less likely to undergo anycancer-directed surgery and with each one-half-decade in-crease in age �70 years, the odds for receiving cancer-directed surgery was reduced by 44%. Whereas a previousstudy of the SEER registry found that only patients above theage of 80 years were less likely to undergo cancer-directedsurgery for rectal cancer, we demonstrated a larger effect ofage that may have been related to our more stringent studyinclusion criteria.15
To control for the survival effect of the lack of rectalcancer-directed surgery, we evaluated the effect of age on thetype of surgery performed in patients who underwent cancer-directed surgery. We identified a significant association be-tween increasing age and both decreasing use of radicalsurgery and increasing use of local excision. We also foundthat increasing age was associated with decreasing likelihoodof node-positive rectal cancer stage (stage III vs. stage I or II)but was not associated with a change in T stage at presenta-tion (stage I vs. stage II). We also did not find an associationbetween tumor grade at presentation and age.
Taken together, these data suggest that increasing agewith rectal cancer is associated with an increasing likelihoodfor surgical undertreatment with local excision rather thanradical surgery, where few if any lymph nodes are evaluatedand therefore resulting in pathologic understaging. A previ-ous analysis of aggregated data obtained from the surgicalliterature demonstrated higher stages of rectal cancer at pre-sentation in elderly patients when compared with youngerpatients,2 a finding that suggests a selection bias in the reportedsurgical series but nonetheless argues that our findings regardingstage at diagnosis are related to the treatment rather than thedisease. These factors may lead to differences in the use ofsubsequent postsurgical treatment such as adjuvant chemother-apy, further resulting in impaired survival outcomes.
To determine whether patients with rectal cancer weremore likely to undergo a combined approach of radiationtherapy and local excision to avoid radical surgery as theyaged, we evaluated the associations between age, tumor
stage, and use of adjuvant radiation therapy. At each stage,patients were less likely to receive adjuvant radiation as theyaged. Moreover, increased use of local excision among theelderly patients was not associated with increased use ofradiation therapy; indeed, older patients who underwent localexcision were less likely to undergo adjuvant radiation ther-apy for rectal cancer than younger patients were. Thesefindings are consistent with the results of prior studies of dataobtained from population-based registries in several othercountries.7,16 However, we found that patients who under-went local excision and adjuvant radiation therapy had poorersurvival when compared with patients who underwent localexcision without radiation therapy, suggesting that radiationtherapy may have been used as a substitute for radical surgeryin a subset of patients who underwent local excision.
This study is subject to limitations inherent to thedataset. The SEER registry does not collect comorbidity data.One reason that the elderly patients may be undergoing lesscancer-directed surgery may be that surgery may be contra-indicated due to comorbidities or that a patient chose toundergo local excision when radical surgery may have beenindicated. Unfortunately, in this analysis, it is not possible todetermine why a patient underwent local excision or radicalresection and this is an important unanswered question.However, by using cancer-specific survival data censoring fornon–cancer-related causes of death, we have made an effortto minimize the impact of this limitation. Despite the influ-ence of comorbidity, age has been demonstrated to be anindependent predictor of receipt of treatment. Within theOntario Cancer Registry, breast and colorectal cancer patientswith a Charlson comorbidity score �2 were less likely toundergo any cancer-directed treatment when compared withpatients with a score of 0 to 1 (multivariate OR � 0.68; 95%CI, 0.45–1.03; P � 0.07). But it should be noted that, afteradjusting for Charlson score, age was still an importantindependent predictor of receiving treatment of breast orcolorectal cancer (multivariate OR � 0.50; 95% CI, 0.33–0.76; P � 0.001).7 An evaluation of data obtained from aSEER-Medicare linked database regarding the use of adju-vant chemotherapy for colorectal cancer demonstrated thatage was the strongest determinant of adjuvant chemotherapyuse even after adjustment for confounding effects based onvariation in patients’ demographic and clinical characteristicsand after exclusion of patients with evident comorbidities.17
In a separate population-based evaluation of patients withcolorectal cancer in the Netherlands, increasing age was
TABLE 6. Stratified Adjusted Associations Between Cancer-Related Survival and Age
Age 50–69 yr Age >70 yr
RR 95% CI P RR 95% CI P
Stage I 1.02 0.91–1.18 0.81 1.46 1.33–1.60 �0.0001
Stage II 1.12 1.02–1.22 0.01 1.26 1.16–1.36 �0.0001
Stage III 1.11 1.04–1.18 0.0009 1.27 1.18–1.36 �0.0001
Local excision 0.96 0.79–1.16 0.66 1.58 1.40–1.78 �0.0001
Radical resection 1.11 1.06–1.16 �0.0001 1.221 1.165–1.280 �0.0001
RR indicates adjusted risk ratio for each half-decade increase in age within indicated stratum.
Chang et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins220

highly predictive of decreasing survival in a multivariatemodel adjusted for comorbidities.16
A second limitation of our study was the lack of data inthe SEER registry on the use of adjuvant chemotherapy.However, the most significant effects of age on survivaloutcome were in patients with stage I rectal cancer, for whomadjuvant chemotherapy is not indicated. Thus, one would notexpect our findings in patients with stage I rectal cancer to beaffected by the addition of data regarding the use of adjuvantchemotherapy in this cohort.
Studies have demonstrated the safety of cancer-directed,stage-appropriate surgery in elderly patients with a low risk ofdeath and morbidity after elective surgery.18–20 The 5-yearcancer-related survival rates have been shown to be equivalentamong older and younger patients when stage-appropriate can-cer-directed treatment is performed.21 Other studies have shownslightly increased but not prohibitively high in-hospital mortalityrates (1.2%–10%) after radical surgery for colorectal canceramong even patients over 75 to 80 years of age.21–23
The decreased utilization of stage-appropriate surgicaltreatment of rectal cancer in elderly patients demonstrated in thisstudy parallels the decreased utilization of stage-appropriateadjuvant chemotherapy for colorectal cancer among elderlypatients. Pooled data from several randomized trials of 5-flu-orouracil-based chemotherapy demonstrated no significant inter-action between being greater than 70 years and toxicity (with thepossible exception of leukopenia) or efficacy of treatment.24 Amore recent report of pooled data from trials of 5-fluorouraciland oxaliplatin demonstrated similar findings with respect toefficacy and toxicity in patients over the age of 70 years.25 Thus,the tendency to undertreat older patients with colorectal cancerexists for both surgical and medical therapy.
CONCLUSIONThis study demonstrates an association between surgi-
cal undertreatment and subsequent understaging of rectalcancer in elderly patients that provides insight into the rea-sons for decreased cancer-related survival rates in elderlypatients. These findings emphasize the need for studies todetermine the factors that determine providers’ and patients’decisions regarding the type of treatments rendered or re-ceived for rectal cancer. However, given the establishedsafety of major abdominal surgery among the elderly, when-ever possible, stage-appropriate radical surgery should beoffered as the first-line therapy for elderly patients with rectalcancer.
ACKNOWLEDGMENTSThe authors thank Charles C. Miller, III, PhD, Univer-
sity of Texas Health Sciences Center at Houston for hisreview of the study design, Virginia A. Moyer, MD, MPH,Department of Pediatrics, Baylor College of Medicine, Hous-ton, for her critical review of the manuscript, and the Na-tional Cancer Institute for establishing the SEER registry,without which this research would not have been possible.
REFERENCES1. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA Cancer
J Clin. 2006;56:106–130.
2. Colorectal Cancer Collaborative Group. Surgery for colorectal cancer inelderly patients: a systematic review. Lancet. 2000;356:968–974.
3. Clark AJ, Stockton D, Elder A, et al. Assessment of outcomes aftercolorectal cancer resection in the elderly as a rationale for screening andearly detection. Br J Surg. 2004;91:1345–1351.
4. Fietkau R, Zettl H, Klocking S, et al. Incidence, therapy and prognosisof colorectal cancer in different age groups: a population-based cohortstudy of the Rostock Cancer Registry. Strahlenther Onkol. 2004;180:478–487.
5. Vercelli M, Capocaccia R, Quaglia A, et al. Relative survival in elderlyEuropean cancer patients: evidence for health care inequalities. The EU-ROCARE Working Group. Crit Rev Oncol Hematol. 2000;35:161–179.
6. Iversen LH, Pedersen L, Riis A, et al. Age and colorectal cancer with focuson the elderly: trends in relative survival and initial treatment from a Danishpopulation-based study. Dis Colon Rectum. 2005;48:1755–1763.
7. Townsley C, Pond GR, Peloza B, et al. Analysis of treatment practicesfor elderly cancer patients in Ontario, Canada. J Clin Oncol. 2005;23:3802–3810.
8. Mellgren A, Sirivongs P, Rothenberger DA, et al. Is local excisionadequate therapy for early rectal cancer? Dis Colon Rectum. 2000;43:1064–1071; discussion 1071–1074.
9. National Cancer Institute D, Surveillance Research Program, CancerStatistics Branch. Surveillance, Epidemiology, and End Results (SEER)Program (www.seer.cancer.gov) Public-Use Data (1973–2002), releasedApril 2005, based on the November 2004 submission.
10. NIH Consensus Conference. Adjuvant therapy for patients with colonand rectal cancer. JAMA. 1990;264:1444–1450.
11. Young JL, Roffers SD, Ries LAG, et al. SEER Summary StagingManual-2000: Codes and Coding Instructions �NIH Publication No.01–4969�. Bethesda, MD: National Cancer Institute; 2001.
12. Engstrom PF, Benson AB 3rd, Chen YJ, et al. Rectal cancer clinical practiceguidelines in oncology. J Natl Compr Canc Netw. 2005;3:492–508.
13. Paty PB, Nash GM, Baron P, et al. Long-term results of local excisionfor rectal cancer. Ann Surg. 2002;236:522–529; discussion 529–530.
14. Garcia-Aguilar J, Mellgren A, Sirivongs P, et al. Local excision of rectalcancer without adjuvant therapy: a word of caution. Ann Surg. 2000;231:345–351.
15. O’Connell JB, Maggard MA, Ko CY. Cancer-directed surgery forlocalized disease: decreased use in the elderly. Ann Surg Oncol. 2004;11:962–969.
16. Lemmens VE, Janssen-Heijnen ML, Verheij CD, et al. Co-morbidityleads to altered treatment and worse survival of elderly patients withcolorectal cancer. Br J Surg. 2005;92:615–623.
17. Schrag D, Cramer LD, Bach PB, et al. Age and adjuvant chemotherapyuse after surgery for stage III colon cancer. J Natl Cancer Inst. 2001;93:850–857.
18. Limpert P, Longo WE, Kelemen PR, et al. Colon and rectal cancer in theelderly: high incidence of asymptomatic disease, less surgical emergen-cies, and a favorable short-term outcome. Crit Rev Oncol Hematol.2003;48:159–163.
19. Abir F, Alva S, Longo WE. The management of rectal cancer in theelderly. Surg Oncol. 2004;13:223–234.
20. Au HJ, Mulder KE, Fields AL. Systematic review of management ofcolorectal cancer in elderly patients. Clin Colorectal Cancer. 2003;3:165–171.
21. Puig-La Calle J Jr, Quayle J, Thaler HT, et al. Favorable short-term andlong-term outcome after elective radical rectal cancer resection in patients75 years of age or older. Dis Colon Rectum. 2000;43:1704–1709.
22. Smith JJ, Lee J, Burke C, et al. Major colorectal cancer resection shouldnot be denied to the elderly. Eur J Surg Oncol. 2002;28:661–666.
23. Barrier A, Ferro L, Houry S, et al. Rectal cancer surgery in patients morethan 80 years of age. Am J Surg. 2003;185:54–57.
24. Sargent DJ, Goldberg RM, Jacobson SD, et al. A pooled analysis ofadjuvant chemotherapy for resected colon cancer in elderly patients.N Engl J Med. 2001;345:1091–1097.
25. Goldberg R, Sargent D, Bleiberg A, et al. A pooled safety and efficacyanalysis of the FOLFOX4 regimen (bi-monthly oxaliplatin plus fluorou-racil/leucovorin) in elderly compared to younger patients with colorectalcancer. ASCO Gastrointestinal Cancers Symposium, San Francisco, CA,2006.
Annals of Surgery • Volume 246, Number 2, August 2007 Rectal Cancer in the Elderly
© 2007 Lippincott Williams & Wilkins 221

ORIGINAL ARTICLES
Activities of Daily Living and Quality of Life of ElderlyPatients After Elective Surgery for Gastric
and Colorectal Cancers
Takeshi Amemiya, MD,* Koji Oda, MD,* Masahiko Ando, MD,† Takashi Kawamura, MD,†Yuichi Kitagawa, MD,‡ Yayoi Okawa, MD,§ Akihiro Yasui, MD,¶ Hideyuki Ike, MD,�
Hiroshi Shimada, MD,� Kojiro Kuroiwa, MD,** Yuji Nimura, MD,* and Shinji Fukata, MD‡
Objective: To establish reliable standards for surgical application toelderly patients 75 years old or older with gastric or colorectalcancer with special reference to the postoperative recovery ofactivities of daily living (ADL) and quality of life (QOL).Summary Background Data: ADL and QOL are important out-comes of surgery for the elderly. However, there has been onlylimited evidence on the natural course of recovery of functionalindependence.Methods: Two hundred twenty-three patients 75 years old or olderwith gastric or colorectal cancer were prospectively examined.Physical conditions, ADL, and QOL were evaluated preoperativelyand at the first, third, and sixth postoperative month.Results: The mortality and morbidity rates were 0.4% and 28%,respectively. Twenty-four percent of patients showed a decrease inADL at 1 month postoperatively, but most patients recovered fromthis transient reduction, with only 3% showing a decline at the sixthpostoperative month (6POM). ADL of these patients was likely todecrease after discharge from the hospital. QOL of the patientsshowed a recovery to an extent equal to or better than their averagepreoperative scores.Conclusions: Of the patients 75 years old or older who underwentelective surgery for gastric or colorectal cancer, only a few showeda protracted decline in ADL and most exhibited better QOL aftersurgery. This indicates that surgical treatment should be considered,whenever needed, for elderly patients 75 years old or older withgastric or colorectal cancer. Estimation of Physical Ability and
Surgical Stress is useful for predicting postoperative declines inADL and protracted disability; this could aid in establishing adirected rehabilitation program for preventing protracted disabilityin elderly patients.
(Ann Surg 2007;246: 222–228)
In 2004 Japanese citizens 75 to 80 years old were expectedon average to live for an additional 8 to 11 years, respec-
tively. Even 85-year-olds were likely to live for additionalyears, 8 for women and 6 for men.1 With such rapid growthin the elderly population, numbers of surgical procedures atthis age have been increasing.2 Major surgery, such as aorticaneurysm repair, gastrointestinal resection, and joint replace-ment can be performed in elderly patients with considerablesafety due to recent advances in anesthesia, metabolic andcritical care, and surgical techniques.2 The surgical treatmentof elderly patients, however, remains controversial. Gener-ally, the overall outcome of surgery represents a balancebetween beneficial effects on a patient and risk of mortality ormorbidity. Accordingly, surgical treatment of a disease isattempted for a particular patient only if expected mortalityand morbidity are acceptably low. In elderly patients, espe-cially those with comorbidities, surgical procedures consideredstandard when performed in younger individuals for a particulardisease sometimes are inappropriate; that is, patients treated bysurgical operation may recover from the disease, but become sodisabled that they are bedridden for the remainder of their lives.According to previous reports, more than 10% of elderly patientsolder than 80 years may have protracted postoperativedisability.3 Postoperative functions of patients, assessed byactivities of daily living (ADL) and quality of life (QOL),have become an especially important measure of outcomes ofsurgical treatment for the elderly.4–10 When one considerselderly patients with malignancies, the problem is moreserious because there has been an increase in the number ofaged patients who develop cancers as a result of the rapidexpansion of the elderly population. It seems that surgicaltreatment decisions for elderly cancer patients, especiallythose with comorbidities, are based mostly on the subjective
From the *Division of Surgical Oncology, Department of Surgery, NagoyaUniversity Graduate School of Medicine, Nagoya, Japan; †Kyoto UniversityHealth Service, Kyoto, Japan; ‡Department of Surgery & Intensive Care,National Center for Geriatrics and Gerontology, Obu, Japan; §Department ofFunctioning Activity, National Center for Geriatrics and Gerontology, Obu,Japan; ¶Department of Surgery, Aichi Saiseikai Hospital, Nagoya, Japan;�Department of Gastroenterological Surgery, Yokohama City University,School of Medicine, Yokohama, Japan; and **Department of Surgery,Tokyo Metropolitan Geriatric Hospital, Tokyo, Japan.
Supported by Research Grant for Longevity Sciences (14C-3) from theMinistry of Health, Labour and Welfare of Japan (to S.F.).
Reprints: Shinji Fukata MD, National Center for Geriatrics and Gerontology,36-3 Gengo, Morioka-cho, Obu, Aichi, 474-8511, Japan. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0222DOI: 10.1097/SLA.0b013e3180caa3fb
Annals of Surgery • Volume 246, Number 2, August 2007222

judgment of surgeons from their individual experiences. Fur-thermore, “ageism,” a negative attitude toward elderly indi-viduals, does exist so that elderly patients with sufficientfunction are sometimes not treated using the same standardsurgical procedures used for younger patients and receive lessaggressive surgery based on their age alone.2,11 Yet, only aradical operation that removes the primary tumors and re-gional lymph nodes can cure patients with advanced stages ofcancer. Thus, reliable standards for surgery on elderly cancerpatients supported by scientific data that include informationon postoperative functions of patients are urgently needed.Toward this goal, we systematically examined postoperativerecovery of physical conditions, ADL and QOL, and identi-fied predictors for the functional recovery of patients 75 yearsold or older who underwent elective surgery for gastric orcolorectal cancer. Gastric and colorectal cancers were chosenbecause these are the most common gastroenterological ma-lignant tumors occurring in the elderly worldwide. We de-signed and performed this prospective study with specialreference to the postoperative functions of elderly patients toestablish criteria that might help surgeons decide whetherstandard surgical treatment should or should not be applied toelderly patients with gastric or colorectal cancer.
PATIENTS AND METHODSA total of 232 eligible patients 75 years old or older
with gastric or colorectal cancer who were referred to thesurgical department in 29 affiliated hospitals between June2003 and June 2004 were enrolled consecutively in thisstudy. All 232 patients underwent surgical resection of gastricor colorectal cancer at those hospitals.
Physical Status, Operative Severity, Morbidity,and Mortality
The parameters examined were physical status, operativeseverity, and morbidity. They were measured by the Physiolog-ical and Operative Severity Scoring system for enUmeration ofMortality and morbidity (POSSUM),12 the Estimation of Phys-ical Ability and Surgical Stress (E-PASS),13 and the AcutePhysiology And Chronic Health Evaluation (APACHE II).14
The severity of each comorbidity and postoperative complica-tion was categorized from grade 1 to grade 4 using the NationalCancer Institute - Common Toxicity Criteria (NCI-CTC) v2.0.15 Postoperative complications of grades 3 and 4 weredefined as major complications. Outcomes in all patients as ofApril 1, 2005, which was 6 months after entry of the last patient
into the study, were examined, and a mortality rate for the entirepatient population was calculated.
Activities of Daily LivingFunctional dependence in basic ADL was evaluated
using the Katz Index.16 Necessity of supervision, direction,personal assistance, or total care for any dependent func-tion of the Katz Index also were recorded as parameters toassess minute declines or increments of patients’ ADL.17
In addition to the Katz Index, the following functionsimportant for elderly postoperative patients also wereevaluated; (Table 1) maintaining a sitting position in thebed (impossible, sitting with Gatch up, sitting withoutGatch up), sitting down on a chair or stool from a standingposition (bedridden, unable to sit down on a chair from astanding position, sitting down in a chair, sitting upright ona chair or stool); maintaining a standing posture (impos-sible, possible with both hands held, possible with 1 handheld, possible unassisted); and walking on a level surfaceor, if unable to walk, moving in a wheelchair (impossible,using a wheel chair with help, propelling a wheel chair indepen-dently, walking with help, walking independently).16
Quality of LifeQOL was evaluated using the SF-12 and EuroQoL 5-D
(EQ5D). The SF-12 is a set of generic, coherent, and easilyadministered QOL measures that produce 2 summary mea-sures of physical and mental aspects of health, based on 12questions.18 The EQ5D is a short, 5-item self-completionmeasure of health status in terms of mobility, self care, usualactivities, pain or discomfort, and anxiety or depression,which are used to produce a combined single index score thatranges from �0.111 (worse than death) to 1.000 (besthealth).19
Additional MeasuresAdditional measures included the Folstein Mini-Mental
State Examination (MMSE).20,21
Data CollectionThe attending physician made physical assessments of
participants and recorded operative severity using their oper-ative records. Physical conditions and QOL were assessed atthe time of admission to the surgical department and at 1, 3,and 6 months postoperatively. ADL were evaluated at thetime of admission and 4 times postoperatively (at 7 to 10
TABLE 1. Activities Exhibiting a Decline After Surgery
Katz IndexPatients Showing Decline
at 6POM (%) Additional FunctionsPatients Showing Decline
at 6POM (%)
Transferring 10/193 (5.2) Sitting in a bed 5/193 (2.6)
Feeding 5/193 (2.6) Sitting down on a chair or stool 6/193 (3.1)
Toileting 7/193 (3.6) Maintaining a standing posture 5/193 (2.6)
Grooming 8/193 (4.1) Moving in a wheelchair 9/193 (4.7)
Dressing 6/193 (3.1) Walking on a level surface 7/193 (3.6)
Bathing 5/193 (2.6)
The number of patients showing declines at the 6th postoperative month: 21/193 (11%).
Annals of Surgery • Volume 246, Number 2, August 2007 ADL and QOL After Surgery in Elderly Patients
© 2007 Lippincott Williams & Wilkins 223

days, and 1, 3 and 6 months) by a researcher in each institutewho had taken a training course for this prospective studybeforehand. In some cases, data collection at 1 month wasreplaced by that at the time of discharge (Fig. 1). Whenpatients were referred to other hospitals postoperatively, theattending physicians of the hospital where the patients stayedwere interviewed by telephone. At the end of the study, weassessed the patients for interim health events that wouldmodify the course of recovery such as fractures, other signif-icant operations, and cerebrovascular accidents.
Statistical AnalysisTo identify the risk factors for a decline in ADL after
surgery, the odds ratio for the postoperative decline wascalculated using a Generalized Estimating Equations (GEE)model.22 To make a direct comparison between the oddsratios of surgical scores (POSSUM, E-PASS, and APACHEII), these scores were transformed linearly to range from 0(best score) to 10 (worst score) before inclusion into themodel. Besides the surgical scores, age, gender, cancer site(stomach or colorectum), pathologic stage, and MMSE wereincluded in the GEE model. We then examined whether thesevariables correlated significantly with postoperative ADLdeclines. A �2 log likelihood value for fitting a model withall the explanatory variables was calculated for each GEEmodel, which included POSSUM or E-PASS or APACHE II,and was used to compare the performance of these 3 models.The adjusted means of QOL scores were calculated preoper-atively, and 1, 3 and 6 months after surgery using a MIXEDprocedure with the repeated statement. All statistical analyseswere performed by SAS Version 9 software (SAS Institute,Cary, NC).
Ethical and Human ConsiderationsThis study was approved by the institutional Review
Board of National Center for Geriatrics and Gerontology andall participating hospitals, and all participants gave theirwritten informed consent.
RESULTS
Patient Recruitment and Follow-UpThe outline of patient recruitment and follow-up is
shown in Figure 2. Of 232 patients enrolled 9 (4%) declineddata collection and 223 patients were followed and evaluated.The rates of data collection were 99.6% at 1 week, 99.1% at1 month, 88.3% at 3 months, and 86.5% at 6 months. Patientdata were available for 833 (96%) of the 870 total potentialpostoperative assessments.
Baseline CharacteristicsThe study population consisted of 132 men and
91women. Ages ranged from 75 to 92 years with a mean of80.1 � 4.3: 37, 71, and 115 patients were aged 85 years orolder, 80 to 84 years, and 75 to79 years, respectively. Ninety-six patients had gastric cancer and 127 patients had colorectalcancer. Their pathologic cancer stages and operative proce-dures were summarized in Table 2.
FIGURE 1. Study design.
FIGURE 2. Study recruitment and follow-up. POW, postoper-ative week; POM, postoperative month.
TABLE 2. Stage and Operation for Studied Patients
Stage* Gastric Cancer Colorectal Cancer
0 — 3
I 51 18
II 15 44
III 26 53
IV 4 9
Lymphadenectomy32,33
D0 2 2
D1 48 22
D2 44 58
D3 2 45
Residual tumor34
R0, R1 92 119
R2 4 8
Operation time (min) 178 � 4.9
Blood loss (g) 310 � 28.8
Amemiya et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins224
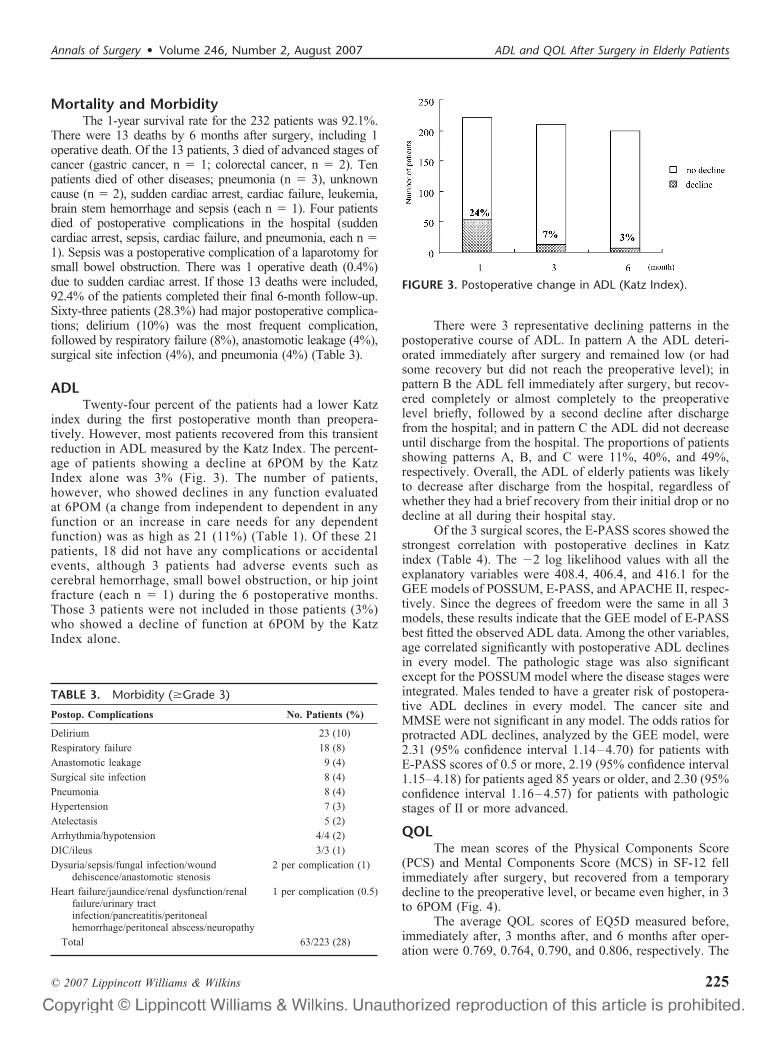
Mortality and MorbidityThe 1-year survival rate for the 232 patients was 92.1%.
There were 13 deaths by 6 months after surgery, including 1operative death. Of the 13 patients, 3 died of advanced stages ofcancer (gastric cancer, n � 1; colorectal cancer, n � 2). Tenpatients died of other diseases; pneumonia (n � 3), unknowncause (n � 2), sudden cardiac arrest, cardiac failure, leukemia,brain stem hemorrhage and sepsis (each n � 1). Four patientsdied of postoperative complications in the hospital (suddencardiac arrest, sepsis, cardiac failure, and pneumonia, each n �1). Sepsis was a postoperative complication of a laparotomy forsmall bowel obstruction. There was 1 operative death (0.4%)due to sudden cardiac arrest. If those 13 deaths were included,92.4% of the patients completed their final 6-month follow-up.Sixty-three patients (28.3%) had major postoperative complica-tions; delirium (10%) was the most frequent complication,followed by respiratory failure (8%), anastomotic leakage (4%),surgical site infection (4%), and pneumonia (4%) (Table 3).
ADLTwenty-four percent of the patients had a lower Katz
index during the first postoperative month than preopera-tively. However, most patients recovered from this transientreduction in ADL measured by the Katz Index. The percent-age of patients showing a decline at 6POM by the KatzIndex alone was 3% (Fig. 3). The number of patients,however, who showed declines in any function evaluatedat 6POM (a change from independent to dependent in anyfunction or an increase in care needs for any dependentfunction) was as high as 21 (11%) (Table 1). Of these 21patients, 18 did not have any complications or accidentalevents, although 3 patients had adverse events such ascerebral hemorrhage, small bowel obstruction, or hip jointfracture (each n � 1) during the 6 postoperative months.Those 3 patients were not included in those patients (3%)who showed a decline of function at 6POM by the KatzIndex alone.
There were 3 representative declining patterns in thepostoperative course of ADL. In pattern A the ADL deteri-orated immediately after surgery and remained low (or hadsome recovery but did not reach the preoperative level); inpattern B the ADL fell immediately after surgery, but recov-ered completely or almost completely to the preoperativelevel briefly, followed by a second decline after dischargefrom the hospital; and in pattern C the ADL did not decreaseuntil discharge from the hospital. The proportions of patientsshowing patterns A, B, and C were 11%, 40%, and 49%,respectively. Overall, the ADL of elderly patients was likelyto decrease after discharge from the hospital, regardless ofwhether they had a brief recovery from their initial drop or nodecline at all during their hospital stay.
Of the 3 surgical scores, the E-PASS scores showed thestrongest correlation with postoperative declines in Katzindex (Table 4). The �2 log likelihood values with all theexplanatory variables were 408.4, 406.4, and 416.1 for theGEE models of POSSUM, E-PASS, and APACHE II, respec-tively. Since the degrees of freedom were the same in all 3models, these results indicate that the GEE model of E-PASSbest fitted the observed ADL data. Among the other variables,age correlated significantly with postoperative ADL declinesin every model. The pathologic stage was also significantexcept for the POSSUM model where the disease stages wereintegrated. Males tended to have a greater risk of postopera-tive ADL declines in every model. The cancer site andMMSE were not significant in any model. The odds ratios forprotracted ADL declines, analyzed by the GEE model, were2.31 (95% confidence interval 1.14–4.70) for patients withE-PASS scores of 0.5 or more, 2.19 (95% confidence interval1.15–4.18) for patients aged 85 years or older, and 2.30 (95%confidence interval 1.16–4.57) for patients with pathologicstages of II or more advanced.
QOLThe mean scores of the Physical Components Score
(PCS) and Mental Components Score (MCS) in SF-12 fellimmediately after surgery, but recovered from a temporarydecline to the preoperative level, or became even higher, in 3to 6POM (Fig. 4).
The average QOL scores of EQ5D measured before,immediately after, 3 months after, and 6 months after oper-ation were 0.769, 0.764, 0.790, and 0.806, respectively. The
TABLE 3. Morbidity (�Grade 3)
Postop. Complications No. Patients (%)
Delirium 23 (10)
Respiratory failure 18 (8)
Anastomotic leakage 9 (4)
Surgical site infection 8 (4)
Pneumonia 8 (4)
Hypertension 7 (3)
Atelectasis 5 (2)
Arrhythmia/hypotension 4/4 (2)
DIC/ileus 3/3 (1)
Dysuria/sepsis/fungal infection/wounddehiscence/anastomotic stenosis
2 per complication (1)
Heart failure/jaundice/renal dysfunction/renalfailure/urinary tractinfection/pancreatitis/peritonealhemorrhage/peritoneal abscess/neuropathy
1 per complication (0.5)
Total 63/223 (28)
FIGURE 3. Postoperative change in ADL (Katz Index).
Annals of Surgery • Volume 246, Number 2, August 2007 ADL and QOL After Surgery in Elderly Patients
© 2007 Lippincott Williams & Wilkins 225

average EQ5D score was significantly higher at 6POM thanpreoperatively (P � 0.005) (Fig. 5).
DISCUSSIONAs medical and surgical problems affecting elderly
patients cover multiple fields and require a coordinatedapproach among medical and surgical professionals, elderlypatients often have multiple additional needs: social, psycho-logic, economic, rehabilitative, and nursing when they be-come disabled after surgery. From medical, social, and func-tional points of view, it is important to anticipate the expectedpostoperative function and care needs prior to surgery, and to
inform patients and their families. Although the postoperativefunctions of patients such as ADL and QOL are importantamong the outcomes of surgical treatment for the elderly,there has been only a limited number of reports on the naturalcourse of recovery of functional independence.4,23 We haveconducted a prospective study with special reference to thepostoperative functions of patients 75 years or older whounderwent elective surgical resection of gastric or colorectalcancer. Standard tools were used for the preoperative, intra-operative, and postoperative evaluation of physical condi-tions, psychologic conditions, postoperative complications,ADL, and QOL, so that the results obtained from this studycan be widely applied to gastric and colorectal cancer pa-tients. The systematic study on the postoperative recovery ofADL showed that elderly patients frequently showed a tran-sient decrease in ADL immediately after surgery. However,patients displaying a decrease at 1 week or at 1 month aftersurgery recovered, and there was no difference in the post-operative mid- to long-term ADL between the patients with andwithout temporary postoperative disability. Moreover, the num-ber of patients showing declines in any ADL parameter at 6POM did not exceed 21 (11%). These findings indicate that mostpatients are unlikely to develop a mid- to long-term decrease inADL after they survive the perioperative period.
One interesting finding was that most late-developingdisabilities occurred after a transient recovery of certainaspects of function, sometimes during the period of follow-upafter discharge from the hospital. Ferrucci et al24 reportedsimilar findings. Either some complications or accidentalevents that occur after a transient recovery or less effectivephysical rehabilitation at home and in outpatient clinics maybe responsible for the protracted disability. Since only 3patients showing protracted disability in our series had anycomplications or accidental events after discharge, their life-style after discharge and/or less effective physical rehabilita-tion at home may be responsible. Traditionally, senior citi-zens are highly respected in Japan whose culture has beengreatly influenced by Confucianism. Too much care by theirfamily members that leads to lack of exercise by elderlypatients at home might accelerate the decrease in ADL.Timonen et al25 reported that a multicomponent trainingprogram that included strength training after an illness was an
TABLE 4. Predictive Value of Clinical Factors for Postoperative Declines in Katz ADL Index: Results of GEE Analyses
Variables
POSSUM Model
P
E-PASS Model
P
APACHE II Model
POddsRatio 95% CI
OddsRatio 95% CI
OddsRatio 95% CI
Surgical score* 1.19 1.05–1.34 0.005 1.26 1.08–1.47 0.003 1.08 0.97–1.20 0.171
Age 1.10 1.03–1.17 0.003 1.08 1.01–1.14 0.014 1.08 1.02–1.15 0.014
Male 1.72 0.95–3.12 0.071 1.71 0.94–3.14 0.081 1.79 0.99–3.20 0.051
Colon cancer† 0.89 0.52–1.51 0.656 0.86 0.52–1.43 0.563 0.79 0.47–1.32 0.364
MMSE 0.95 0.87–1.03 0.213 0.97 0.87–1.08 0.572 0.94 0.86–1.03 0.179
Pathologic cancer stage 1.27 0.93–1.74 0.137 1.39 1.04–1.87 0.026 1.42 1.05–1.92 0.021
�2 log likelihood 408.4 406.4 416.1
*POSSUM score, E-PASS CRS score, and APACHE II score were included separately in the GEE model.†Colon cancer/gastric cancer.
FIGURE 4. Change in mean scores of Physical ComponentsScore (PCS) and Mental Components Score (MCS) (SF-12).
FIGURE 5. Postoperative change in QOL (EQ5D).
Amemiya et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins226

effective form of rehabilitation for frail woman older than 75years old, and that its beneficial effects lasted for at least 9months after training. Frail and aged patients may need moreactive and intensive rehabilitation that includes exercise athome, at outpatient clinics, or in nursing homes to restore andstimulate their function after discharge.26,27
We were able to identify several risk factors for thetransient and protracted decline in ADL. The patients whodeveloped postoperative complications were more likely toshow a transient drop in ADL than those who did not, andolder patients tended to develop a temporary decrease. Age,gender, and cancer stages were risk factors for the protracteddecline in ADL. Analysis of these risk factors using the GEEmodel allowed us to construct such criteria that might helpselect a population at very high risk for long-term postoper-ative declines in ADL. Such criteria will be more valuablewhen more practical and useful scoring systems are estab-lished that predict the functional recovery of elderly patientsfrom major elective gastroenterological surgeries.
We also found that POSSUM and E-PASS were usefulfor predicting protracted disability of patients. The efficacy ofE-PASS was the best of all the scoring systems examined.Our study may be the first to directly compare the efficacy ofthese surgical scores for the prediction of postoperative re-covery in ADL.
Our present study clearly shows that surgical treatmentdoes improve the QOL of elderly patients 75 years old orolder with gastric and colorectal cancers. Patients in ourseries displayed a recovery in their SF-12 scores to an extentequal to or better than their average preoperative scores. Ourpreliminary results, however, show that QOL scores in sev-eral items of some patients decreased after surgery andremained low on more detailed examination of individualcases (unpublished data). Additional studies, on which itemsare more likely to decrease and on what causes the decreasein these items, will not only further improve the QOLchanges of elderly patients but also enable us to informpatients and their families of expected moderate- to long-termpostoperative QOL during the preoperative period.
Patients with advanced gastric or colorectal cancers canonly be cured by radical surgery, and an improvement in thesurvival rate by radical surgery has been reported in recentyears.28,29 Resection of primary gastric or colorectal cancerwith extended lymphadenectomy is the standard procedure inJapan.30,31 In the present study, radical surgery was per-formed for 92 (96%) gastric and 119 (94%) colorectal cancerpatients. Our result showing as low as a 0.4% mortality rateconfirms that radical surgery for gastric or colorectal cancersrarely results in death, even for elderly patients 75 years oldor older. In addition, our data also show that radical surgeryis unlikely to decrease the ADL and QOL in most of thepatients 75 years old or older with gastric or colorectal cancerat 6POM. This then indicates that elderly patients who aremedically fit before surgery have little more risk than doyounger ones and implies that major gastroenterological sur-geries accompanying similar surgical stress with radical sur-geries for gastric or colorectal cancers can also be applied tothe elderly. A systematic evaluation of the postoperative
complications using a standard tool (NCI-CTC), however,suggested that the incidence of major complications (catego-rized as � grade 3) in elderly patients was as high as 28%. Toreduce morbidity, therefore, it is necessary to establish aneffective method for selecting frail subpopulations with post-operative complications requiring special intensive care andto improve our current intensive care system for them duringthe perioperative period. Randomized trials may be needed totest the hypothesis that preoperative and postoperative phys-ical rehabilitation programs can prevent the protracted dis-ability observed in 10% of the elderly patients examined.27
CONCLUSIONSOf the patients 75 years old or older who underwent
elective surgery for gastric or colorectal cancer, only a fewshowed a protracted decline in ADL and most exhibitedbetter QOL after surgery. This indicates that surgical treat-ment can be offered to elderly patients 75 years old or olderwith gastric or colorectal cancer. E-PASS is more usefulcompared with POSSUM and APACHE II for predictingpostoperative declines in ADL. E-PASS is able to predict theprotracted disability, and may be helpful for establishing aneffective rehabilitation program for restoring their functionand thereby preventing the protracted disability observed insome elderly patients.
ACKNOWLEDGMENTSThe authors thank the attending physicians, their fam-
ilies, and nursing and personal care staff from many facilitiesfor their contribution.
REFERENCES1. Ministry of Health, Labour and Welfere of Japan. Abridged Life Table
For Japan 2004. September 18, 2005. Available at: http://www1. mhlw.go.jp/english/database/db-hw/index.html. Accessed November 25,2006.
2. Crosby D. Surgical care for the elderly in the United Kingdom. In:Adkins RB Jr, Scott H Jr, eds. Surgical Care for the Elderly. 2nd ed.Philadelphia: Lipponcott-Raven;1998:503–511.
3. Ulander K, Jeppsson B, Grahn G. Quality of life and independence inactivities of daily living preoperatively and at follow-up in patients withcolorectal cancer. Support Care Cancer. 1997;5:402–409.
4. Williamson WK, Nicoloff AD, Taylor LM Jr, et al. Functional outcomeafter open repair of abdominal aortic aneurysm. J Vasc Surg. 2001;33:913–920.
5. Thybusch-Bernhardt A, Schmidt C, Kuchler T, et al. Quality of lifefollowing radical surgical treatment of gastric carcinoma. World J Surg.1999;23:503–508.
6. Temple Pc, Travis B, Sachs I, et al. Functioning and well-being ofpatients before and after elective surgical procedures. J Am Coll Surg.1995;181:17–25.
7. Perkins JM, Magee TR, Iland IJ, et al. Prospective evalution of qualityof life after conversional abdominal aortic aneurysm surgery. Eur J VascEndovasc Surg. 1998;16:203–207.
8. Mangione CM, Goldman I, Oray EJ, et al. Health-related quality of lifeafter elective surgery. Measurement of longitudinal changes. J GenIntern Med. 1997;12:686–697.
9. McKenna RJ Sr. Clinical aspects of cancer in the elderly. Treatmentdecisions, treatment choices, and follow-up. Cancer. 1994;74:2107–2117.
10. Walsh TH. Audit of outcome of major surgery in the elderly. Br J Surg.1996;83:92–97.
11. Katlic M. Principles of geriatric surgery. In: Rosenthal RA, ZenilmanME, eds. Principles and Practice of Geriatric Surgery. New York:Springer; 2001;92–104.
Annals of Surgery • Volume 246, Number 2, August 2007 ADL and QOL After Surgery in Elderly Patients
© 2007 Lippincott Williams & Wilkins 227

12. Copeland GP, Jones D, Walters M. POSSUM: a scoring system forsurgical audit. Br J Surg. 1991;78:355–360.
13. Haga Y, Ikei S, Ogawa M. Estimation of Physiologic Ability andSurgical Stress (E-PASS) as a new prediction scoring system for post-operative morbidity and mortality following elective gastrointestinalsurgery. Surg Today. 1999;29:219–225.
14. Knaus WA, Draper EA, Wagner DP, et al. APACHE II: a severity ofdisease classification system. Crit Care Med. 1985;13:818–829.
15. The National Cancer Institute. Common Toxicity Criteria v2. 0. (CTC).March 23, 1998. Available at: http://ctep.cancer.gov/reporting/ctc.html.Accessed November 25, 2006.
16. Shelkey M, Wallace M. Katz index of independence in activity of dailyliving (ADL). October, 1998. Available at: http://www.hartfordign.org/publications/trythis/issue02. pdfx. Accessed November 25, 2006.
17. Katz S, Downs TD, Cash HR, et al. Progress in development of the indexof ADL. Gerontologist. 1970;10:20–30.
18. Ware JE, Kosinski M, Turner-Bowker, et al. How to Score Version 2 ofthe SF-12 Health Survey (with a supplement documenting version 1).Boston, MA: Health Assessment Lab; 2002.
19. Rosalind R, Frank C. EQ-5D: a measure of health status from theEuroQol Group. Ann Med. 2001;33:337–343.
20. Cockrell JR, Folstein MF. Mini-Mental State Examination (MMSE).Psychopharmacol Bull. 1988;24:689–692.
21. Anthony JC, LeResche L, Niaz U, et al. Limits of the ‘Mini-MentalState’ as a screening test for dementia and delirium among hospitalpatients. Psychol Med. 1982;12:397–408.
22. Diggle PJ, Liang KY, Zeger SL. Analysis of Longitudinal Data. NewYork: Oxford University Press; 1994.
23. Lawrence VA, Hazuda HP, Cornell JE, et al. Functional independence aftermajor abdominal surgery in the elderly. J Am Coll Surg. 2004;199:762–772.
24. Ferrucci L, Guralnik JM, Studenski S, et al. Designing randomized,
controlled trials aimed at preventing or delaying functional decline anddisability in frail, older persons: a consensus report. J Am Geriatr Soc.2004;52:625–634.
25. Timonen L, Rantanen T, Ryynanen OP, et al. A randomized controlledtrial of rehabilitation after hospitalization in frail older women: effectson strength, balance and mobility. Scand J Med Sci Sports. 2002;12:186–192.
26. Pendergast DR, Fisher NM, Calkins E. Cardiovascular, neuromuscular,and metabolic alterations with age leading to frailty. J Gerontol. 1993;48:61–67.
27. Siebens H, Aronow H, Edwards D, et al. A randomized controlled trialof exercise to improve outcomes of acute hospitalization in older adults.J Am Geriatr Soc. 2000;48:1545–1552.
28. Stevannovic D, Radovanovic D, Pavlovic, et al. Effects of systematiclymphadenectomy on length of survival in patients with gastric carci-noma. Med Preg. 2004;57:175–180.
29. Mukai M, Ito I, Mukoyama S, et al. Improvement of 10-year survival byJapanese radical lymph node dissection in patients with Dukes’ B and Ccolorectal cancer: a 17-year retrospective study. Oncol Rep. 2003;10:927–934.
30. Kanemitsu Y, Hirai T, Komori K, et al. Survival benefit of high ligationof the inferior mesenteric artery in sigmoid colon or rectal cancersurgery. Br J Surg. 2006;93:609–15.
31. Sasako M. What is reasonable treatment for gastric adenocarcinoma?Gastroenterology. 2000;35(Suppl 12):116–20.
32. Japanese Research Society for Gastric Cancer. Japanese classification ofgastric carcinoma. 1st English ed. Tokyo: Kanehara; 1999.
33. Japanese Society for Cancer of the Colon and Rectum. Japanese classi-fication of colorectal carcinoma. 7th ed. Tokyo: Kanehara; 2006.
34. AJCC. Cancer Staging Manual. 6th ed. New York: Springer; 2002.
Amemiya et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins228

ORIGINAL ARTICLES
Survival in Nonocclusive Mesenteric IschemiaEarly Diagnosis by Multidetector Row Computed Tomography and
Early Treatment With Continuous Intravenous High-doseProstaglandin E1
Akira Mitsuyoshi, MD,* Kazutaka Obama, MD,* Nobuhiko Shinkura, MD,* Takashi Ito, MD,*and Masazumi Zaima, MD†
Objectives: The aim of the study was to establish a procedure forearly diagnosis and treatment of nonocclusive mesenteric ischemia(NOMI).Background: NOMI has a high mortality rate, and early diagnosisand treatment are important for improving survival in patients withthis condition.Methods: The subjects were 22 patients treated at our hospital over13 years. Diagnostic criteria for NOMI were established based onthe first 13 cases. In the 9 more recent cases, we performed abdominalcontrast multidetector row computed tomography (MDCT) uponsuspicion of NOMI based on these criteria. Imaging allowed definitediagnosis of NOMI, and continuous intravenous high-dose PGE1
administration was initiated immediately after diagnosis (dose,0.01–0.03 �g/kg per min; mean administration period, 4.8 days).Results: Nine of the first 13 patients died of multiple organ failureassociated with multiple intestinal necrosis. These cases suggestedthat NOMI may develop when 3 of the following 4 criteria are metafter cardiovascular surgery or maintenance dialysis in elderlypatients: symptoms of the ileus develop slowly from abdominalsymptoms, such as an unpleasant abdominal feeling or pain; arequirement for catecholamine treatment; an episode of hypoten-sion; and slow elevation of the serum transaminase level. In the 9recent cases, definite diagnosis was made from spasm of the prin-cipal arteries in arterial volume rendering and curved planar refor-mation MDCT images. Early treatment with PGE1 prevented acute-stage NOMI in 8 of the 9 cases.Conclusions: Early diagnosis of NOMI is possible using the abovecriteria and MDCT, and initiation of PGE1 treatment may increasesurvival in patients with NOMI.
(Ann Surg 2007;246: 229–235)
Nonocclusive mesenteric ischemia (NOMI) is an acutemesenteric circulatory disorder that, in contrast to mes-
enteric arterial occlusion induced by blockage of blood flowby emboli and thrombi, is not caused by organic occlusion ofblood vessels. Early diagnosis and early treatment are veryimportant in NOMI, but the early symptoms and character-istics are unclear; and in many cases, the disease has ad-vanced to an irreversible stage before a definite diagnosis ismade. Our experience with diagnosis and treatment of NOMIhas led us to establish new diagnostic criteria, and we nowperform abdominal contrast multidetector row computed to-mography (MDCT) for suspected NOMI. Abnormalities in3-dimensional images of the principal arteries enable earlydefinite diagnosis, and we have achieved good outcomes withsubsequent early treatment with continuous intravenous high-dose prostaglandin E1 (PGE1).
METHODSThe cases of 22 NOMI patients treated at our hospital
in the last 13 years were investigated. Diagnostic criteria forsuspected NOMI were established based on the first 13 ofthese cases, and abdominal contrast MDCT, rather than abdom-inal angiography, was performed in the 9 most recent cases,following application of the new diagnostic criteria. A definitediagnosis of NOMI was made from characteristic abnormalfindings in VR and CPR images, and continuous intravenoushigh-dose PGE1 administration was immediately initiated.
The acquisition conditions using a 16-row MDCT (Aq-uilion 16, Toshiba Co.) were as follows: tube voltage, 120 to135 kVp: tube current, 350 to 400 mA; scan time, 0.5seconds/rotation; slice thickness, 1 mm; and helical pitch, 15.The volume of the contrast medium concentration was 300 or320 mg/ml, the injection volume was set equal to the bodyweight � 2 to 2.5 ml, and the infusion rate was 3.5 to 4.0mL/s. Image editing software was used on an AquariusWorkstation (Terarecon Co.).
RESULTS
Cases Untreated With ContinuousIntravenous PGE1
Of the 22 NOMI cases at our hospital in the last 13years, 13 were not treated with PGE1 at onset; the details of
From the *Department of Surgery, Mitsubishi Kyoto Hospital; and †Depart-ment of Surgery, Shiga Medical Center for Adults,
Reprints: Akira Mitsuyoshi, MD, Department of Surgery, Mitsubishi KyotoHospital, 1 Katsura Gosho-machi, Nishikyo-ku, Kyoto, 615-8087, Japan.E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0229DOI: 10.1097/01.sla.0000263157.59422.76
Annals of Surgery • Volume 246, Number 2, August 2007 229

these cases are shown in Table 1. The patients comprised 10males and 3 females, and the mean age at onset was 71.0years. NOMI occurred frequently after cardiovascular sur-gery: 5 cases after surgery for thoracic and abdominal aorticaneurysms, 2 cases after valve replacement, and 1 case aftercoronary arterial bypass. Three cases occurred after mainte-nance dialysis. Four patients had an episode of transienthypotension before onset, and 9 were under treatment withcatecholamines such as dopamine hydrochloride. Early ab-dominal symptoms were noted in all cases, but no patientsreported severe pain. Identification of the onset time wasdifficult; however, the disease began with mild abdominalpain or an unpleasant feeling in the abdomen, and thesesymptoms gradually worsened. Finally, typical symptoms ofintestinal obstruction, such as sensation of an enlarged abdo-men, and vomiting developed.
Elevation of glutamic oxaloacetic transaminase (GOT),glutamic pyruvic transaminase (GPT), and lactate dehydro-
genase (LDH) corresponding to the degree of intestinal ne-crosis was noted in all cases, but no other characteristic bloodfindings were noted. Diagnosis of NOMI by abdominal an-giography was possible in only 1 of the 13 cases (case 6). Thedisease was diagnosed comprehensively based on abdominalCT images (planar slices on conventional CT) and laboratorytests in 4 cases (cases 4, 5, 8, and 9), and final diagnosis wasmade by laparotomy and histopathological examination in theremaining cases.
One case was treated with PGE1 administration throughan indwelled arterial catheter (case 6) and one case resolvedwith conservative treatment (case 8). In the other 11 cases,excision of the necrotic intestine or enterostomy was per-formed, but 9 of these patients died, with the cause of deathbeing multiple organ failure associated with massive intesti-nal necrosis. Excision of the necrotic intestine was initiated24 to 72 hours after onset, with PGE1 administration alsoinitiated in cases 6 during this time.
TABLE 1. Background of 13 Patients Who Did Not Receive Continuous PGE1 Intravenous Administration
Case No./Gender/Age (yr)
PreexistingDisease Onset Background
InitialSymptoms/Findings
Use ofCatecholamines
(CA�/�) Findings in Laparotomy Outcome
1/Male/58 Ischemic heartdisease
Transient hypotension Shock symptoms,including abdominalpain, hypotension, andloss of consciousness
� Small intestinal segmentalnecrosis
Death
2/Male/77 Ischemic heartdisease
After aortic valvereplacement
Abdominal pain andbloating
� Small intestinal segmentalnecrosis
Death
3/Female/62 On dialysis dueto chronicrenal failure
After aortic valvereplacement
Abdominal pain andbloating
� Small intestinal segmentalnecrosis
Death
4/Male/76 Ischemic heartdisease
After surgery for thoracicaortic aneurysm(transient hypotension)
Nausea, abdominal pain,and bloating
� Large and small intestinalsegmental necrosis
Survival
5/Male/74 Ischemic heartdisease
After surgery forabdominal aorticaneurysm
Nausea, abdominal pain,and bloating
� Not conducted Death
6/Male/72 Arteriosclerosis After surgery forobstructivearteriosclerosis
Abdominal pain andbloating
� Small intestinal segmentalnecrosis
Death
7/Male/77 Arteriosclerosis After surgery forabdominal aorticaneurysm
Free air in abdominal XP � Small intestinal segmentalnecrosis
Death
8/Male/68 Arteriosclerosis After surgery forabdominal aorticaneurysm
Nausea, abdominal pain,and bloating
� Not conducted Survival
9/Male/73 Ischemic heartdisease,arteriosclerosis
After coronary arterybypass surgery
Abdominal bloating � Small intestinal segmentalnecrosis
Death
10/Female/81 Ischemic heartdisease,arteriosclerosis
After cardiac angiography Abdominal pain � Large and small intestinalsegmental necrosis
Death
11/Female/76 On dialysis dueto chronicrenal failure
After dialysis (transienthypotension)
Abdominal pain andbloating
� Large and small intestinalsegmental necrosis
Death
12/Female56 On dialysis dueto chronicrenal failure
After dialysis (transienthypotension)
Abdominal pain andbloating
� Large intestinal segmentalnecrosis
Survival
13/Male/73 On dialysis dueto chronicrenal failure
After dialysis (transienthypotension)
Abdominal pain � Large and small intestinalsegmental necrosis
Survival
Mitsuyoshi et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins230

Based on our first 13 cases, we concluded that it islikely that NOMI has developed in elderly patients when thefollowing items are found after cardiovascular surgery ormaintenance dialysis: 1) symptoms of the ileus that slowlyappear after initial abdominal symptoms, such as an unpleas-ant feeling in the abdomen and abdominal pain; 2) a require-ment for catecholamine treatment; 3) an episode of hypoten-sion; and 4) slow elevation of the transaminase level.
Cases Treated With ContinuousIntravenous PGE1
After the initial 13 cases, subsequent patients meeting 3of the 4 criteria above were suspected to have NOMI. Ninesuch cases arose, and continuous intravenous high-dose PGE1administration was initiated immediately before completionof all diagnostic examinations (Table 2). The patients com-prised 6 males and 3 females, and the disease occurred aftersurgery for abdominal aortic aneurysm in 4 cases, after valvereplacement in 2 cases, and after maintenance dialysis in 1case. The mean age was 70.2 years. Various early abdominalsymptoms were noted, including abdominal pain and anunpleasant feeling in the abdomen. Two of the patients hadtransient hypotension before onset, 6 were receiving cat-echolamines, and the transaminase level was significantlyelevated in all 9 patients.
PGE1 was administered intravenously at a dose of 0.01to 0.03 �g/kg per min, and the mean duration of administra-tion was 4.8 days after onset. Abdominal contrast MDCT wasperformed in all 9 cases, rather than abdominal angiography.In 7 cases, enhancement of principal arteries could be tracedto the periphery close to the marginal arteries in CT slices,and the staining intensity varied in the intestinal wall in thesame slice (showing a difference between regions of theintestinal wall with good and poor blood flow). This findingmay be useful as supplemental information in diagnosis ofNOMI. In the other 2 cases (cases P6 and P8), sharp spasm-induced narrowing was noted at a site 5 cm peripheral fromthe root of the superior mesenteric artery in VR and CPRMDCT images, and definite diagnosis of NOMI was achievedby acquisition of an image showing retention of blood flowup to the marginal arteries of the intestine (the details of caseP6 are described below).
Of the 9 recent cases, acute-stage NOMI resolved in 1patient with recovery of oral ingestion, but then the patientcomplicated with infectious disease and died on the 65th dayafter onset of NOMI. In another case, PGE1 was not effective,NOMI progressed, and the patient died of multiple intestinalnecrosis and sepsis. However, the other 7 PGE1-treated pa-tients recovered smoothly and were discharged.
Case in Which Resolution by PEG1 WasMonitored by MDCT
An 82-year-old man (case P6) with a medical history ofhypertension, arteriosclerosis, and tachyarrhythmia (forwhich he had not received regular medication) was admittedfor upper abdominal pain, nausea, and vomiting that hadstarted on the previous day. Blood pressure on admission was125/65 (usually 160/100) with a slight fever at 37.0°C. Theabdomen was enlarged and moderate tenderness was noted.
Niveau formation was found on plain abdominal XP images.In abdominal contrast MDCT slices, a large volume of ascitesand poor enhancement over the entire small intestinal wallwere noted, despite retention of the superior mesentericarterial blood flow to the periphery. In arterial VR and CPRimages in abdominal MDCT, spasm-induced narrowing wasnoted at a site about 5 cm peripheral from the root of thesuperior mesenteric artery, but the blood flow to the intestinalmarginal arteries was maintained (Fig. 1).
After admission, NOMI due to vomiting-induced dehy-dration was diagnosed, and continuous intravenous high-dosePGE1 administration was immediately initiated (the dose wasescalated to a final dose of 100 �g/h). Spasm and narrowingof the superior mesenteric artery were improved in abdominalMDCT images on the following day. After 5 days, asciteswas reduced, contrast enhancement of the small intestinalwall had improved, and spasm and narrowing of the superiormesenteric artery were resolved in MDCT (Fig. 2). Intrave-nous PGE1 administration was stopped at this point, since thedisease symptoms had resolved, and the patient was dis-charged on the 19th day of hospitalization.
DISCUSSIONNOMI accounts for more than 10% to 20% of cases of
acute mesenteric circulatory disorders and leads to extensiveirreversible intestinal necrosis for which the prognosis is verypoor, despite the absence of organic obstruction in the prin-cipal arteries. Ende et al described what are considered to bethe first reported cases of NOMI in 3 patients with heartfailure-associated low output in 1958.1 Subsequently, manymore cases have been described, mainly in Europe andAmerica, with a mortality rate of 70% to 90% that has notchanged over time; furthermore, the cause of death has beenrelated to NOMI in 9% of fatal dialysis cases.2 Regardingpathogenesis, intestinal vasospasm due to persistent low per-fusion is thought to cause ischemic disorder due to decreasedcardiac output and blood pressure.3,4 Digitalis preparationsand catecholamines often induce vasospasm, and associationsof NOMI with activation of the renin-angiotensin system andvasopressin secretion from the pituitary gland have also beenreported.5
Most NOMI patients are elderly, and the disease ismore likely to occur in ICU and CCU patients after cardio-vascular surgery and dialysis. NOMI can be induced byabdominal pain, nausea, vomiting, and ileus symptoms, butthe characteristic early symptoms and laboratory test resultsare unclear. Compared with mesenteric thrombosis, NOMIalso frequently occurs postoperatively in patients with un-clear consciousness and severe disease. Early diagnosis isdifficult, and during the diagnostic process the disease slowlyadvances to an irreversible state with extensive intestinalnecrosis. Detection of subjective symptoms is difficult incases that develop after surgery because the effects of generaland epidural anesthesia may remain and the disease maydevelop and advance unnoticed. Laparotomic characteristicsare inevitably present in patients who underwent laparotomy,but mesenteric blood flow may be retained, even in marginalarteries reaching the lesions, despite extensive necrotization
Annals of Surgery • Volume 246, Number 2, August 2007 Survival in Patients With NOMI
© 2007 Lippincott Williams & Wilkins 231

TAB
LE2.
Back
grou
ndof
9Pa
tient
sW
hoRe
ceiv
edC
ontin
uous
PGE 1
Intr
aven
ous
Adm
inis
trat
ion
Cas
eN
o./
Gen
der/
Age
(yr)
Pre
exis
ting
Dis
ease
Ons
etB
ackg
roun
dIn
itia
lSy
mpt
oms/
Fin
ding
s
Use
ofC
atec
hola
min
es(C
A�
/�)
Dos
ean
dP
erio
dof
PG
E1
Intr
aven
ous
Adm
inis
trat
ion
Fin
ding
sin
Lap
arot
omy
Out
com
e
P1/
Mal
e/69
Isch
emic
hear
tdi
seas
e,ar
teri
oscl
eros
isA
fter
surg
ery
for
abdo
min
alao
rtic
aneu
rysm
(tra
nsie
nthy
pote
nsio
n)
Abd
omin
alpa
inan
dsh
ock
sym
ptom
s(h
ypot
ensi
onan
dlo
ssof
cons
ciou
snes
s)
�0.
01�
g/kg
per
min
for
5d
Not
cond
ucte
dS
urvi
val
P2/
Mal
e/81
Isch
emic
hear
tdi
seas
e,ar
teri
oscl
eros
isA
fter
surg
ery
for
abdo
min
alao
rtic
aneu
rysm
Abd
omin
alpa
inan
dbl
oati
ng�
0.01
–0.0
2�
g/kg
per
min
for
3d
Not
cond
ucte
dS
urvi
val
P3/
Mal
e/68
Isch
emic
hear
tdi
seas
e,ar
teri
oscl
eros
isA
fter
surg
ery
for
abdo
min
alao
rtic
aneu
rysm
Abd
omin
alpa
inan
dbl
oati
ng,
bloo
dyst
ool
�0.
03�
g/kg
per
min
for
7d
Not
cond
ucte
dS
urvi
val
P4/
Fem
ale/
83Is
chem
iche
art
dise
ase,
arte
rios
cler
osis
Aft
ersu
rger
yfo
rab
dom
inal
aort
ican
eury
smN
ause
a,ab
dom
inal
pain
,an
dbl
oati
ng(F
ig.
1:an
giog
raph
ofsu
peri
orm
esen
tery
)
�0.
03�
g/kg
per
min
for
5d
Lar
gean
dsm
all
inte
stin
alse
gmen
tal
necr
osis
Dea
thdu
eto
anot
her
caus
e
P5/
Mal
e/73
Isch
emic
hear
tdi
seas
e,ar
teri
oscl
eros
isA
fter
aort
icva
lve
repl
acem
ent
Abd
omin
alpa
inan
dbl
oati
ng�
0.03
�g/
kgpe
rm
info
r5
dN
otco
nduc
ted
Sur
viva
l
P6/
Mal
e/82
Tac
hyar
rhyt
hmia
,hi
stor
yof
surg
ery
for
gast
ric
canc
er
Deh
ydra
tion
Nau
sea,
abdo
min
alpa
in,
and
vom
itin
g�
0.01
–0.0
3�
g/kg
per
min
for
3d
Not
cond
ucte
dS
urvi
val
P7/
Fem
ale/
38A
rter
iosc
lero
sis,
SL
EA
dvan
ced
rena
ldy
sfun
ctio
nN
ause
a,ab
dom
inal
pain
,an
dvo
mit
ing
�0.
03�
g/kg
per
min
for
3d
Not
cond
ucte
dS
urvi
val
P8/
Mal
e/58
On
dial
ysis
due
toch
roni
cre
nal
fail
ure
Aft
erdi
alys
is(t
rans
ient
hypo
tens
ion)
Nau
sea,
abdo
min
alpa
in,
and
gene
ral
mal
aise
�0.
01–0
.03
�g/
kgpe
rm
info
r7
dN
otco
nduc
ted
Sur
viva
l
P9/
Fem
ale/
80Is
chem
iche
art
dise
ase,
arte
rios
cler
osis
Aft
erao
rtic
and
mit
ral
valv
ere
plac
emen
t(t
rans
ient
hypo
tens
ion)
Abd
omin
albl
oati
ng�
0.03
�g/
kgpe
rm
info
r9
dN
otco
nduc
ted
Dea
th
Mitsuyoshi et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins232
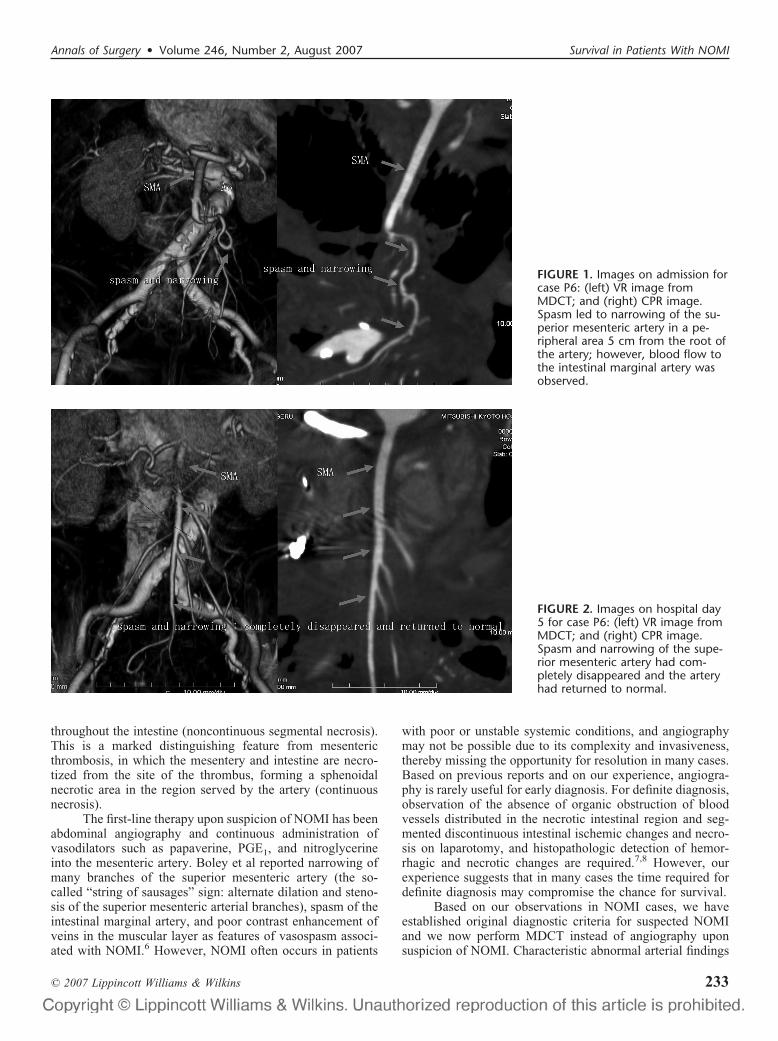
throughout the intestine (noncontinuous segmental necrosis).This is a marked distinguishing feature from mesentericthrombosis, in which the mesentery and intestine are necro-tized from the site of the thrombus, forming a sphenoidalnecrotic area in the region served by the artery (continuousnecrosis).
The first-line therapy upon suspicion of NOMI has beenabdominal angiography and continuous administration ofvasodilators such as papaverine, PGE1, and nitroglycerineinto the mesenteric artery. Boley et al reported narrowing ofmany branches of the superior mesenteric artery (the so-called “string of sausages” sign: alternate dilation and steno-sis of the superior mesenteric arterial branches), spasm of theintestinal marginal artery, and poor contrast enhancement ofveins in the muscular layer as features of vasospasm associ-ated with NOMI.6 However, NOMI often occurs in patients
with poor or unstable systemic conditions, and angiographymay not be possible due to its complexity and invasiveness,thereby missing the opportunity for resolution in many cases.Based on previous reports and on our experience, angiogra-phy is rarely useful for early diagnosis. For definite diagnosis,observation of the absence of organic obstruction of bloodvessels distributed in the necrotic intestinal region and seg-mented discontinuous intestinal ischemic changes and necro-sis on laparotomy, and histopathologic detection of hemor-rhagic and necrotic changes are required.7,8 However, ourexperience suggests that in many cases the time required fordefinite diagnosis may compromise the chance for survival.
Based on our observations in NOMI cases, we haveestablished original diagnostic criteria for suspected NOMIand we now perform MDCT instead of angiography uponsuspicion of NOMI. Characteristic abnormal arterial findings
FIGURE 1. Images on admission forcase P6: (left) VR image fromMDCT; and (right) CPR image.Spasm led to narrowing of the su-perior mesenteric artery in a pe-ripheral area 5 cm from the root ofthe artery; however, blood flow tothe intestinal marginal artery wasobserved.
FIGURE 2. Images on hospital day5 for case P6: (left) VR image fromMDCT; and (right) CPR image.Spasm and narrowing of the supe-rior mesenteric artery had com-pletely disappeared and the arteryhad returned to normal.
Annals of Surgery • Volume 246, Number 2, August 2007 Survival in Patients With NOMI
© 2007 Lippincott Williams & Wilkins 233

in MDCT enable a rapid definite diagnosis. Data collected bymultirow detectors can be reconstructed rapidly to give 3-di-mensional images that provide vascular information compa-rable to that obtained in angiography. Before introduction ofMDCT, the principal arteries could be traced to a peripherallevel close to the marginal arteries using conventional con-trast CT. However, the staining intensity in these imagesvaried due to differences between regions with good and poorblood flow in the intestinal wall, and this information couldonly be used to supplement other observations in diagnosis ofNOMI. In contrast, performance of abdominal contrastMDCT upon suspicion of NOMI allows definite diagnosisand permits subsequent early initiation of therapy and mon-itoring of disease resolution (Fig. 3).
Immediate initiation of continuous intravenous high-dose PGE1 administration at the time of suspected onset ofNOMI achieved good outcomes in 8 of our 9 recent cases.Laparotomy was unnecessary in 7 of the 8 successfullytreated cases (excluding cases P4); thus, a definite diagnosisby laparotomy and histopathologic examination was notmade; therefore, it cannot be formally ruled out that thedisease was something other than NOMI, based on previousdiagnostic criteria. However, the time required for definitediagnosis based on laparotomic findings and pathologic ex-amination of excised specimens may compromise successfultreatment. Marked increases in GOT, GPT, LDH, and cre-
atine phosphokinase (CPK), and advanced metabolic acidosisdue to intestinal ischemia indicate progression of intestinalnecrosis, and the chance of survival is reduced.
The main goal of current therapy for NOMI is reductionof spasm and improved perfusion of the mesenteric arteryusing vasodilators, and the role of surgery is limited to diagnos-tic laparotomy and excision of irreversibly necrotized intestine.PGE1 is a potent vascular smooth-muscle relaxant due to itsperipheral vasodilatory activity, inhibition of platelet aggrega-tion, effect on reduction of erythrocyte deformation, and inhibi-tion of production of reactive oxygen. It has been used as a drugfor vascular obstructive lesions in the extremities, such as arte-riosclerosis obliterans and thromboangitis, and is known toimprove blood flow in the digestive tract. Elimination of PGE1from blood is biphasic, with half-lives of 0.2 minutes (� phase)and 8.2 minutes (� phase),9 and PGE1 in blood is mostlymetabolized rapidly in the liver. Thus, a continuous effect cannotbe expected with intermittent administration, and continuousadministration through a catheter inserted into the principalartery is more effective.
PGE1 administered into blood is 65% metabolizedin the liver, with the remaining 35% being circulatedsystemically,10 and intravenous administration at a constantrate results in maintenance of a constant blood concentra-tion.9 Theoretically, continuous intravenous administration ata high dose may exhibit an effect similar to that of continuous
FIGURE 3. NOMI diagnosis and treatment plan in our hospital.
Mitsuyoshi et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins234

local arterial administration; therefore, we immediately initi-ated continuous intravenous high-dose PGE1 administrationupon suspicion of NOMI and achieved good outcomes usingthis approach. Although no standard dose for continuousmesenteric arterial administration has been established, weset the dose at 0.01 to 0.03 �g/kg per min, which is lowerthan that used for treatment of abnormally high blood pres-sure (0.05–0.1 �g/kg per min). PGE1 was continuouslyadministered for a maximum of 5 days (until abdominalsymptoms had improved) within a dose range that did notinfluence the systemic circulatory dynamics, thus avoidingheart failure and shock. The target period of PGE1 adminis-tration was set to 5 days because a tendency for changes inthe condition became apparent within 5 days after onset inmost early NOMI cases we encountered, regardless of thetreatment method and improvement or aggravation of thecondition. The PGE1 dose should be carefully set whenNOMI is accompanied by hemorrhage of the digestive tract,or when mesenteric thrombosis is suspected and treated withconcomitant thrombolytic agents, since PGE1 has potentinhibitory action on platelet aggregation and shows a ten-dency to enhance hemorrhage.
Cases of NOMI are increasingly common due to theaging of society and an increase in the dialysis population,but the disease concept has not been fully established. More-over, NOMI is not recognized easily and is difficult todiagnose; therefore, many NOMI patients may not have beendiagnosed correctly and consequently may have died withoutreceiving adequate treatment. The time of treatment initiationafter onset determines the prognosis of this disease, but thecurrent approach using diagnostic and therapeutic abdominalangiography and subsequent continuous mesenteric arterial
administration of vasodilators is unlikely to increase thesurvival rate. In contrast, it is important to identify possibleNOMI based on the background at the time of diseaseonset, since the disease lacks characteristic symptoms andis fatal in the advanced stage. As we have shown, earlydiagnosis in suspected cases can be made using abdominalcontrast MDCT and reconstruction of 3-dimensional imagesof the principal arteries, and early initiation of continuousintravenous high-dose PGE1 administration may increasesurvival of NOMI patients.
REFERENCES1. Ende N. Infarction of the bowel in cardiac failure. N Engl J Med.
1958;258:879–881.2. Han SY, Kwon XJ, Shin JH, et al. Nonocclusive mesenteric ischemia in
a patient on maintenance hemodialysis. Korean J Intern Med. 2000;15:81–84.
3. Bassiounty HS. Nonocclusive mesenteric ischemia. Surg Clin North Am.1997;77:319–326.
4. Bailey RW, Bulkley GB, Hamilton SR, et al. Protection of the smallintestine from nonocclusive mesenteric ischemic injury due to cardio-genic shock. Am J Surg. 1987;153:108–116.
5. Lock G, Scholmerich J. Nonocclusive mesenteric ischemia. Hepatogas-troenterology. 1995;42:234–239.
6. Boley SJ, Sprayregan S, Siegelman SS, et al. Initial results from anaggressive roentgenological and surgical approach to acute mesentericischemia. Surgery. 1977;82:848–855.
7. Heer FW, Silen W, French SW. Intestinal gangrene without apparentvascular occlusion. Am J Surg. 1965;110:231–238.
8. Fogarty JT, Fletcher SW. Genesis to nonocclusive mesenteric ischemia.Am J Surg. 1966;111:130–137.
9. Cawello W, Schweer H, Muller R, et al. Metabolism and pharmacoki-netics of prostaglandin E1 administered by intravenous infusion inhuman subjects. Eur J Clin Pharmacol. 1994;46:275–277.
10. Golub M, Zia P, Matsuno M, et al. Metabolism of prostaglandins A1 andE1 in man. J Clin Invest. 1975;56:1404–1408.
Annals of Surgery • Volume 246, Number 2, August 2007 Survival in Patients With NOMI
© 2007 Lippincott Williams & Wilkins 235

ORIGINAL ARTICLES
Congenital Intrahepatic Bile Duct Dilatation is a PotentiallyCurable Disease
Long-Term Results of a Multi-institutional Study
Jean-Yves Mabrut, MD, PhD,*† Christian Partensky, MD, FACS,‡ Daniel Jaeck, MD, PhD, FRCS,§Elie Oussoultzoglou, MD,§ Jacques Baulieux, MD, FRCS,† Olivier Boillot, MD, PhD,‡
Jan Lerut, MD, PhD, FACS,* Jean de Ville de Goyet, MD, PhD,* Catherine Hubert, MD,*Jean-Bernard Otte, MD,* Maxime Audet, MD,§ Christian Ducerf, MD, FACS,†
and Jean-Francois Gigot, MD, PhD, FRCS*
Objective: To report clinical presentation, perioperative outcome,and long-term results of surgical management of congenital intra-hepatic bile duct (IHBD) dilatations (including Caroli disease) in amulti-institutional setting.Summary Background Data: Congenital IHBD dilatations are arare congenital disorder predisposing to intrahepatic stones, cholan-gitis, and cholangiocarcinoma. The management remains difficultand controversial for bilobar forms of the disease or when concur-rent congenital hepatic fibrosis is associated.Methods: From 1976 to 2004, 33 patients (range 11 to 79 years)were retrospectively enrolled. Disease extent into the liver wasunilobar in 26 patients and bilobar in 7 patients (21%). Cholangio-carcinoma, congenital hepatic fibrosis, and intrahepatic stones werepresent in 2, 10, and 20 patients, respectively. Transplantations orliver resections were performed in 5 and 27 patients, respectively,whereas 1 asymptomatic patient was managed conservatively.Results: Postoperative mortality was nil. Postoperative complica-tions occurred in 16 of 32 operated patients (50%) and additionalprocedures for residual stones were required in 5 patients. During amedian follow-up of 80 months (1 patient being lost for follow-up)no patient developed metachronous carcinoma. Six patients (30%)developed recurrent intrahepatic stones but satisfactory late outcomewas achieved in 27 patients (87%).Conclusions: Partial or total liver resection achieves satisfactorylate outcome in congenital IHBD dilatations, when the affection istreated at an early stage and when the extent of liver resection is
tailored to intrahepatic disease extent and takes into considerationthe presence and severity of underlying chronic liver and renaldiseases.
(Ann Surg 2007;246: 236–245)
Congenital intrahepatic bile duct (IHBD) dilatations are arare disorder resulting from abnormal development of
the ductal plate responsive to dilatations of the biliary treelimited to the IHBD,1 belonging thus to the spectrum ofcongenital bile duct cysts (BDC). Congenital IHBD dilata-tions correspond to type V BDC according to the Todani et alclassification.2 This entity was first defined by Caroli et al3 in1958, distinguishing between a simple and a fibrous type ofthe disease, the last one being associated with congenitalhepatic fibrosis (CHF) as previously described by Grumbachet al.4 The initial description by Caroli et al concernedcommunicating IHBD dilatations of peripheral bile ducts.3
However, Guntz et al5 reported later as Caroli disease similarfusiform or saccular IHBD dilatations of large IHBD, theinitial disease form described by Caroli et al corresponding totype I in their classification (Fig. 1).
Intrahepatic BDC predispose to biliary stasis and intrahe-patic stones (IHS) formation leading to cholangitis, liver ab-scesses, septicemia, and ultimately to secondary biliary cirrhosis.Moreover, the tendency to cholangiocarcinoma development onthese abnormal bile ducts is well documented.6–8 CongenitalIHBD dilatations may present itself from a localized formlimited to 1 hepatic lobe or segment to a bilobar and diffuse forminvolving the entire intrahepatic biliary tree. When the disease isassociated with coexistent CHF, possibly responsible for portalhypertension, and sometimes to inconstant associated renal dis-ease (from tubular ectasia to polycystic kidney disease), theentity is then called Caroli syndrome.9,10 The management ofthis rare disease is particularly difficult. The degree ofdisease extension into the liver and the presence of con-current underlying chronic liver or kidney disease and
From the *Department of Abdominal Surgery and Transplantation, Saint-Luc University Hospital, Brussels, Belgium; †Department of DigestiveSurgery and Liver Transplantation, Croix-Rousse University Hospital,Lyon, France; ‡Department of Digestive Surgery and Liver Transplan-tation, Edouard Herriot University Hospital, Lyon, France; and §Depart-ment of Digestive Surgery and Transplantation, Hautepierre UniversityHospital, Strasbourg, France.
Reprints: Jean-Francois Gigot, MD, PhD, FRCS, Hepatobiliary and Pancre-atic Surgical Division, Department of Abdominal Surgery and Trans-plantation, Saint-Luc University Hospital, Avenue Hippocrate 10, B1200 Brussels, Belgium. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0236DOI: 10.1097/SLA.0b013e3180f61abf
Annals of Surgery • Volume 246, Number 2, August 2007236

cancer are decision-making factors influencing the surgicalmanagement. Liver resection is reputed to be the treatmentof choice for localized unilobar forms of the disease butthe management of diffuse bilobar forms remains contro-versial.11 Moreover, few data concerning long-term post-operative results are reported in the literature.
The purpose of the present series is to report clinicalpresentation, perioperative outcome, and to focus on long-term results of the surgical management of congenital IHBDdilatations in a multi-institutional setting according to thedisease extent into the liver and the presence and severity ofconcurrent underlying chronic liver or kidney disease.
PATIENTS AND METHODSDuring a 28-year period of time (1976–2004), 142
consecutive patients with BDC were retrospectively enrolledfrom 5 European academic surgical centers. Liver transplantand pediatric surgery were available in 4 and 2 of thesecenters, respectively. The type of BDC was classified accord-ing to the Todani et al classification,2 based on pre- andintraoperative imaging studies. From this group, 33 patients(23%) issued from 4 of these centers had IHBD dilatations.Four of these patients have already been reported.12,13 IHBDdilatations were defined as the presence of congenital seg-mental communicating biliary dilatations limited to IHBD.1
The intrahepatic disease extent was defined as being unilobaror bilobar from careful review of imaging studies. The Guntzet al5 subclassification concerning the aspect and location ofcongenital IHBD dilatations was used, including fusiform orsaccular dilatations of large IHBD and “grape-bunch-like”saccular communicating dilatations of peripheral IHBD alter-nating with normal IHBD (Figs. 1–4). However, when con-genital IHBD dilatations were associated with extrahepaticbile duct dilatation, as encountered in 22 of the 142 patients,the disease was not considered as type V BDC but wasclassified as type IV-A BDC, according to the Todani et alclassification. Acquired dilatations of IHBD because of prox-imal biliary obstruction, such as benign or malignant stricture
or obstructive primary IHS, were excluded. Pediatric patientswere defined as younger than 15 years. Demographic fea-tures, disease, and operative data were collected using stan-dardized questionnaires. Patient operative risk was evaluatedaccording to the American Society of Anesthesiologists(ASA) physical status score.14 The presence of concurrentCHF was confirmed by histologic examination or liver biop-sies from both sides of the liver. Radiographic studies in-cluded percutaneous ultrasound in 33 patients (100%), com-puted tomography in 27 patients (82%), magnetic resonancecholangio-pancreatography in 15 patients (45%), and T-tubecholangiography in 2 patients (6%). Invasive imaging studiesof the biliary tract, such as endoscopic retrograde cholangio-pancreatography or percutaneous transhepatic cholangiogra-phy were used in 9 patients (27%) and 4 patients (12%),respectively. However, the purpose of endoscopic retrogradecholangio-pancreatography and percutaneous transhepaticcholangiography was therapeutic in 8 and 1 patients, respec-
FIGURE 1. Schematic representationof Guntz et al subclassification ofcongenital IHBD dilatations, accord-ing to the aspect and extent of in-trahepatic bile ducts dilatations.Type 1: grape-bunch-like saccularcommunicating dilatations of pe-ripheral IHBD; type 2: fusiform dila-tations of large IHBD; type 3: saccu-lar dilatations of large IHBD.
FIGURE 2. Magnetic resonance cholangiography. Communi-cating IHBD dilatations of peripheral bile ducts correspond-ing to type I in the Guntz et al classification (Caroli disease).
Annals of Surgery • Volume 246, Number 2, August 2007 Congenital Intrahepatic Biliary Cysts
© 2007 Lippincott Williams & Wilkins 237

tively. The type of hepatic resection was classified accordingto the International Hepato-Pancreato-Biliary Associationclassification reported by Strasberg et al.15 At postoperativefollow-up, all patients were assessed by clinical and radio-logic examination.
Definition of EndpointsEvaluation criteria included type and details of opera-
tive procedures, early postoperative course, including com-plications and reoperation rate, postoperative hospital stay,and late patient outcome. Postoperative mortality and mor-bidity were defined at 2 months or during hospital stay. Theseverity of postoperative complications was categorized ac-cording to the Clavien et al classification.16 Late clinicalresults were evaluated according to a modification of theMayo Clinic score of results evaluation previously reportedfor congenital BDC17: excellent if the patient remained freeof symptoms without further reintervention; good if thepatient presented occasional and mild attacks of cholangitisor pancreatitis not impairing the quality of life; fair if thepatients had repeated episodes of cholangitis or pancreatitis,or had portal hypertension without further reintervention; andpoor, if the patient required later biliary or liver-relatedreoperative procedures, developed biliary cirrhosis or com-plications because of portal hypertension (such as varicealbleeding, for example), or died of cyst-related malignancy orliver and biliary-related complications.
Statistical AnalysisStatistical analysis was performed using Fisher exact
test or �2 tests for categorical variables and Mann-Whitney
nonparametric rank sum tests for continuous variables, whenappropriate. A P value �0.05 was considered statisticallysignificant.
RESULTS
PrevalenceThe annual incidence per center of congenital IHBD
dilatations over a 28-year period was 0.234 (range 0–0.6) inthe present series, indicating an obvious referral bias. Indeed,at the 2 centers where experience in HBP, pediatric, and livertransplant surgery was concentrated, the total number ofpatients varies from 5 to 18, respectively, totaling 70% of thewhole study population.
Demographic FeaturesThirty-two adults and 1 child (an 11-year-old girl) with
congenital IHBD dilatations were included in the present study.The median age of adults (11 women and 21 men) was 55 years(mean age: 53 years, range: 24–79 years). Six patients (18%)were at high risk, being classified ASA III or IV.
Clinical PresentationThe median delay between first symptoms and surgical
treatment was 14 months (mean 54 months, range 1–500
FIGURE 3. Intraoperative cholangiography. Fusiform IHBDdilatations of large IHBD corresponding to type II in theGuntz et al classification.
FIGURE 4. Endoscopic retrograde cholangiography: saccularIHBD dilatations of large IHBD corresponding to type III inthe Guntz et al classification.
Mabrut et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins238

months). This delay was �1 year in 13 patients (39%) but �5years in only 8 patients (24%). Details of clinical patientpresentation are reported in Table 1. Complicated clinicalpresentation was not correlated with unilobar or bilobarintrahepatic disease extent or to duration of symptoms.
Coexistent HBP and Renal DiseasesDetails of HBP and renal coexistent diseases are given
in Table 1. Both hepatobiliary and renal coexistent diseaseswere associated in 6 patients (18%). Synchronous cholangio-carcinoma was encountered in 2 patients (6%), one of whichwas located within the left hepatic duct, presenting a 3-cmpapillary tumor preoperatively diagnosed on imaging studiesand corresponding at final pathology to high-grade dysplasiaand focal microinvasive cancer. In the second patient, havingundergone a left hemihepatectomy, final pathology discov-ered large focal areas of high-grade dysplasia within theIHBDs. Duration of symptoms in these patients was 1 and 22months, respectively. Associated renal disease was signifi-cantly more frequent in patients with coexistent CHF (with-
out CHF: 2 of 23 patients vs. with CHF: 5 of 10 patients;P � 0.016).
Biliary DiseaseBilobar and unilobar (left hemiliver: 20 patients, right
hemiliver: 6 patients) disease extent was observed in 7patients (21%) and 26 patients (79%), respectively. Therewas no difference in terms of patient age, sex ratio, ASAscore, severity of clinical presentation, coexistent HBP orrenal coexistent disease, and previous treatment modalitiesbetween patients with unilobar or bilobar disease extent, andbetween patients with or without CHF, except for coexistentrenal disease and portal hypertension, which were morefrequent in CHF patients.
According to the Guntz et al5 classification, type I, II,and III were encountered in 9, 22, and 2 patients, respec-tively. There was no significant difference among the 3groups in term of patient age, sex ratio, ASA score, severityof clinical presentation, coexistent HBP (including CHF) orrenal coexistent disease, and previous treatment modalities.
Previous Disease-Related TreatmentsDetails of previous biliary-related treatments are re-
ported in Table 1. One patient with CHF associated withportal hypertension had also undergone a surgical portosys-temic shunt. Two of the 5 patients who had undergonecommon bile duct (CBD) exploration at another institution,allowing adequate disease diagnosis, were referred to thesecondary referral treatment center where they underwentliver resection within 1 month after referral.
Type of Surgical ProceduresExcept for 1 asymptomatic patient with a right unilobar
form of congenital IHBD dilatations associated with CHF andwith prior kidney transplantation, 32 patients underwent liverresection (27 patients; 84%) or transplantation (5 patients;16%). The 4 remaining asymptomatic patients who hadundergone liver resection had elevated liver function testsrelated to unilobar or bilobar IHS. No patient underwentemergency operation for control of sepsis. Details of treat-ment according to unilobar or bilobar disease extension andaccording to the presence of CHF with or without portalhypertension are reported in Table 2. Transplanted patientswith the bilobar form of the disease had associated CHF withportal hypertension, except 2 patients without portal hyper-tension who were transplanted for repeated attacks of cholan-gitis from diffuse IHS. Two patients with Caroli diseaseassociated with CHF and chronic renal insufficiency frompolycystic kidney disease underwent combined liver andkidney transplantations. In resected patients with unilobardisease extent, a liver resection smaller than formal hemi-hepatectomy was performed in 10 patients (40%) (Table 2).
Associated procedures were performed in 22 of 32operated patients (69%), including contralateral IHSextraction (2 patients), CBD exploration (8 patients), cho-lecystectomy (11 patients), main biliary convergence ex-cision followed by biliodigestive reconstruction with mu-cosa-to-mucosa hepaticojejunostomy using a 60 cm inlength Roux-Y jejunal loop (5 patients) and kidney trans-
TABLE 1. Clinical Presentation and CoexistentHepatobiliary and Kidney Diseases in Patients Suffering FromCongenital IHBD Dilatations
Clinical presentation
Asymptomatic 5 Patients (15.2%)
Symptomatic 13 (39.4%)
Isolated RUQ pain 11
Jaundice 2
Complicated 15 (45.4%)
Repeated attacks of cholangitis 15
Cholangitis with oesophageal varicealbleeding
2
Coexistent diseases
Hepatobiliary diseases 26 (79%)
Congenital hepatic fibrosis (withportal hypertension: 3 patients)
10 (30%)
Biliary stones 21 (64%)
Intrahepatic stones (HIS) 20
Common bile duct stones 9
Gallstones 4
Associated intrahepatic stricture 2 (6%)
Unilobar liver atrophy 3 (9%)
Synchronous biliary cancer 2 (6%)
Renal diseases 7 (21%)
Chronic renal failure 4 (12%)
Polycystic kidney disease 2
Tubular ectasia 2
Previous kidney transplant 3
Stones kidney formation 3 (1 Requiring nephrectomy)
Previous biliary-related treatment 24 (73%)
Cholecystectomy 17
Common bile duct exploration 5
Endoscopic sphincterotomy (for CBDstone extraction: 8)
9
Bilio-digestive anastomosis for IHS 2
Extracorporeal shock-wave lithotripsy 1
Annals of Surgery • Volume 246, Number 2, August 2007 Congenital Intrahepatic Biliary Cysts
© 2007 Lippincott Williams & Wilkins 239

plantation or retransplantation (1 patient each). The reasonfor main biliary convergence excision was not the presenceof proximal stricture but of cystic disease involving theliver hilum. The 2 patients with synchronous cholangio-carcinoma were radically treated by left hemihepatectomyand left hemihepatectomy extended to segment 1 associ-ated with extrahepatic bile duct excision and hepaticoje-junostomy, respectively.
Postoperative OutcomePostoperative mortality was nil in the present series.
Twenty-two postoperative complications occurred in 16 of the32 operated patients (50%). The type and severity of postoper-ative complications according to the extent of liver resection aredetailed in Table 3. According to the Clavien et al16 classifica-tion, major postoperative complications (namely type 3 and 4)occurred in 7 patients (22%), requiring in all these patients somesort of reoperative procedures. Overall and major postoperativecomplications occurred in 12 (44%) and 5 patients (19%) afterliver resection and in 4 (80%) and 2 patients (40%) after livertransplantation (not significant). Planned postoperative addi-tional therapeutic procedure for residual IHS or CBD stones was
required in 5 patients (16%), including endoscopic or radiologicstones extraction in 4 and 1 patient, respectively. Finally, themedian postoperative hospital stay was 13 days (mean 18 days;range 8-53 days) in the series.
Late OutcomeThe not operated patient is alive and free of symptoms
and complications after 61 months of follow-up. One patientwith left unilobar disease into the liver and without associatedCHF having been treated by left lateral sectionectomy waslost to follow-up after an uneventful postoperative course at2 months. The median follow-up for the 31 remaining pa-tients was 80 months (mean 91 months; range 7–231months). Twenty-one (67%) and 7 patients (23%) had fol-low-up longer than 5 and 10 years, respectively. Twenty-eight patients were alive whereas 3 died of nondisease-relatedevents (including the patient presenting with high-grade dys-plasia at a follow-up of 144 months). The remaining patientpresenting with microinvasive cholangiocarcinoma is aliveand disease-free 89 months after surgery.
Patient status during long-term follow-up accordingto intrahepatic disease extent is reported in Table 4,including symptom-free and disease-free status, details ofcomplications, and reoperative procedures. According tothe modified Mayo Clinic evaluation score, excellent,good, fair and poor late results were achieved in 26, 1, 0,and 4 patients, respectively.
During the follow-up period, 6 of 20 patients (30%)with initial IHS (one of them harboring postoperative residualIHS) developed recurrent IHS, which led to reoperativeprocedures in 3 patients. The type of reoperative proceduresincluded segmentectomy 4 after prior left lateral sectionec-tomy (1 patient), extracorporeal shock-wave lithotripsy ofsegment 4 stones after prior left lateral sectionectomy (1patient) and endoscopic extraction procedure in a bilobarform of the disease (1 patient). The 3 remaining patients withrecurrent IHS were not surgically treated because of associ-ated secondary biliary cirrhosis with decompensated portalhypertension in 1 patient, the absence of symptoms in 1patient, and the refusal of surgery by an elderly patient. Nopatient developed late metachronous carcinoma.
Fair and poor late outcome was observed in 4 patients(13%) in the whole series, which was not significantly dif-ferent according to intrahepatic disease extent (unilobar: 8%;bilobar: 29%, not significant), the presence of associated CHF(with CHF: 0%; without CHF: 18%, not significant), the typeof the disease according to Guntz et al classification (type I:11%, type II: 14%; type III: 0% (not significant), or the typeof surgical resection (liver transplantation: 0%; partial liverresection: 15%, not significant). Fair and poor results wereobserved in 29% of bilobar disease, 0% of right unilobardisease, and 11% of left unilobar disease (not significant)(Table 4). In unilobar disease extent, fair and poor resultswere observed in 0% of patients having undergone a hemi-hepatectomy and in 22% of patients having undergone a liverresection smaller than a hemihepatectomy (not significant)(Table 4).
TABLE 2. Details on Management of Patients SufferingFrom Congenital IHBD Dilatations According to IntrahepaticDisease Extent and Presence of Congenital Hepatic Fibrosis(CHF)
Liver Disease Extension Type of Hepatic Resection Performed
Bilobar (n � 7) With CHF and portal hypertension: 2 patients
Liver transplantation: n � 2
With CHF but without portal hypertension: 2patients
Liver transplantation: n � 2
Without CHF or portal hypertension: 3patients
Left hemihepatectomy extended to segmentI: n � 1
Left trisectionectomy n � 1
Trisegmentectomy 4–5–6: n � 1
Left unilobar (n � 20) With CHF but without portal hypertension:4 patients
Left lateral sectionectomy: n � 1
Left hemihepatectomy: n � 3
Without CHF or portal hypertension:16 patients
Left lateral sectionectomy: n � 8
Left hemihepatectomy: n � 6
Left hemihepatectomy extended to segment1: n � 2
Right unilobar (n � 6) With CHF and portal hypertension: 1 patient
Liver transplantation: n � 1
With CHF but without portal hypertension: 1patient
No treatment (asymptomatic) n � 1
Without CHF or portal hypertension: 4patients
Right hemihepatectomy: n � 3
Bisegmentectomy 5–6: n � 1
Mabrut et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins240
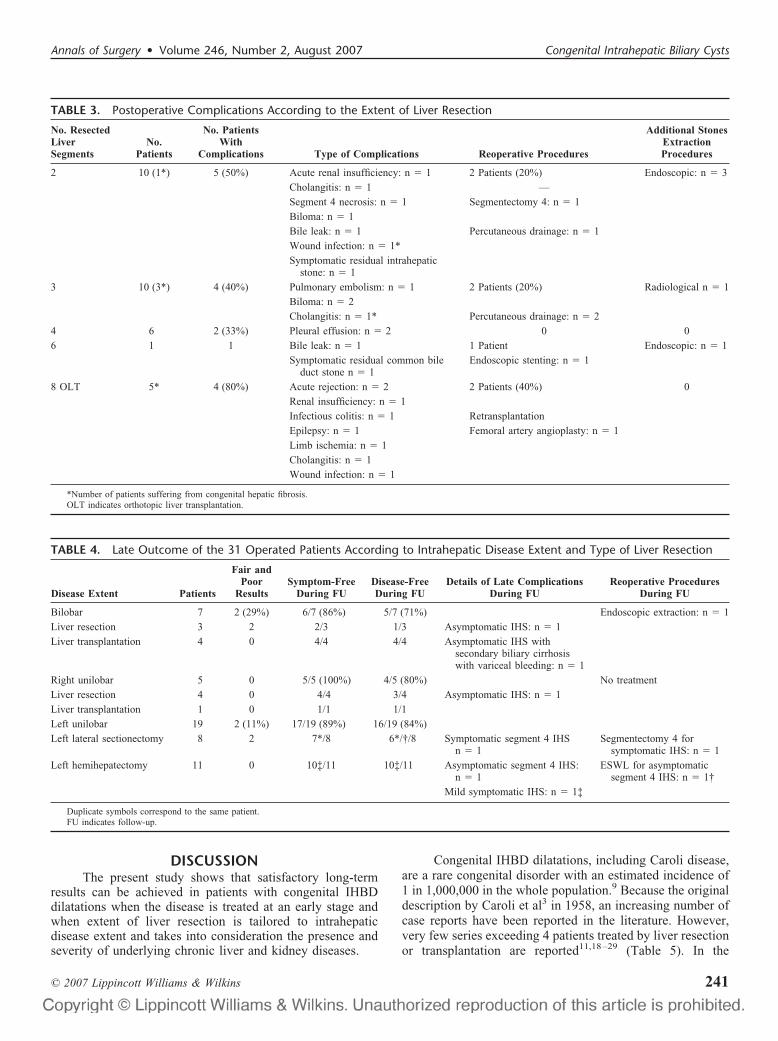
DISCUSSIONThe present study shows that satisfactory long-term
results can be achieved in patients with congenital IHBDdilatations when the disease is treated at an early stage andwhen extent of liver resection is tailored to intrahepaticdisease extent and takes into consideration the presence andseverity of underlying chronic liver and kidney diseases.
Congenital IHBD dilatations, including Caroli disease,are a rare congenital disorder with an estimated incidence of1 in 1,000,000 in the whole population.9 Because the originaldescription by Caroli et al3 in 1958, an increasing number ofcase reports have been reported in the literature. However,very few series exceeding 4 patients treated by liver resectionor transplantation are reported11,18–29 (Table 5). In the
TABLE 3. Postoperative Complications According to the Extent of Liver Resection
No. ResectedLiverSegments
No.Patients
No. PatientsWith
Complications Type of Complications Reoperative Procedures
Additional StonesExtractionProcedures
2 10 (1*) 5 (50%) Acute renal insufficiency: n � 1 2 Patients (20%) Endoscopic: n � 3
Cholangitis: n � 1 —
Segment 4 necrosis: n � 1 Segmentectomy 4: n � 1
Biloma: n � 1
Bile leak: n � 1 Percutaneous drainage: n � 1
Wound infection: n � 1*
Symptomatic residual intrahepaticstone: n � 1
3 10 (3*) 4 (40%) Pulmonary embolism: n � 1 2 Patients (20%) Radiological n � 1
Biloma: n � 2
Cholangitis: n � 1* Percutaneous drainage: n � 2
4 6 2 (33%) Pleural effusion: n � 2 0 0
6 1 1 Bile leak: n � 1 1 Patient Endoscopic: n � 1
Symptomatic residual common bileduct stone n � 1
Endoscopic stenting: n � 1
8 OLT 5* 4 (80%) Acute rejection: n � 2 2 Patients (40%) 0
Renal insufficiency: n � 1
Infectious colitis: n � 1 Retransplantation
Epilepsy: n � 1 Femoral artery angioplasty: n � 1
Limb ischemia: n � 1
Cholangitis: n � 1
Wound infection: n � 1
*Number of patients suffering from congenital hepatic fibrosis.OLT indicates orthotopic liver transplantation.
TABLE 4. Late Outcome of the 31 Operated Patients According to Intrahepatic Disease Extent and Type of Liver Resection
Disease Extent Patients
Fair andPoor
ResultsSymptom-Free
During FUDisease-FreeDuring FU
Details of Late ComplicationsDuring FU
Reoperative ProceduresDuring FU
Bilobar 7 2 (29%) 6/7 (86%) 5/7 (71%) Endoscopic extraction: n � 1
Liver resection 3 2 2/3 1/3 Asymptomatic IHS: n � 1
Liver transplantation 4 0 4/4 4/4 Asymptomatic IHS withsecondary biliary cirrhosiswith variceal bleeding: n � 1
Right unilobar 5 0 5/5 (100%) 4/5 (80%) No treatment
Liver resection 4 0 4/4 3/4 Asymptomatic IHS: n � 1
Liver transplantation 1 0 1/1 1/1
Left unilobar 19 2 (11%) 17/19 (89%) 16/19 (84%)
Left lateral sectionectomy 8 2 7*/8 6*/†/8 Symptomatic segment 4 IHSn � 1
Segmentectomy 4 forsymptomatic IHS: n � 1
Left hemihepatectomy 11 0 10‡/11 10‡/11 Asymptomatic segment 4 IHS:n � 1
ESWL for asymptomaticsegment 4 IHS: n � 1†
Mild symptomatic IHS: n � 1‡
Duplicate symbols correspond to the same patient.FU indicates follow-up.
Annals of Surgery • Volume 246, Number 2, August 2007 Congenital Intrahepatic Biliary Cysts
© 2007 Lippincott Williams & Wilkins 241

TAB
LE5.
Rep
orte
dSe
ries
Exce
edin
g4
Patie
nts
Suffe
ring
From
Con
geni
talI
HBD
Dila
tatio
nsTr
eate
dby
Live
rRe
sect
ion
orLi
ver
Tran
spla
ntat
ion
Aut
hors
Pat
ient
sM
ale/
Fem
ale
Uni
loba
rR
ight
/Lef
tB
iloba
rC
HF
Sync
hron
ous
Car
cino
ma
Liv
erR
esec
tion
(Dea
th)
OL
T(I
ndic
atio
ns�D
eath
�)D
urat
ion
ofF
ollo
w-U
p(M
o)St
atus
atF
ollo
w-U
p
Nag
asue
etal
,19
8418
6(3
M/3
F)
6(1
00%
)(2
R/4
L)
0N
A0
6(0
)0
Mea
n:54
Wel
l
Mer
cadi
eret
al,
1984
19
10(3
M/7
F)
6(6
7%)
3(3
3%)
1(1
0%)
06
(0)
06–
12W
ell
for
loca
lize
dfo
rms
Kno
opet
al,
1994
20
88
(100
%)
0N
A0
8(0
)0
Med
ian:
40W
ell
Dag
liet
al,
1998
21
21(1
3M/8
F)
9(4
3%)
12(5
7%)
2(1
0%)
07
(NA
)N
AN
AN
A
Gil
let
etal
,19
9922
12(6
M/6
F)
12(1
00%
)(3
R/9
L)
02
(17%
)0
12(0
)0
NA
Wel
l
Shi
etal
,20
0123
6N
AN
AN
A0
42
(Bil
iary
cirr
hosi
s�0
�)24
mo
for
OL
TW
ell
Am
mor
iet
al,
2002
24
8(2
M/6
F)
3(3
7%)
(1R
/2L
)5
(63%
)N
A1
(13%
)4
(0)
4(C
irrh
osis
�4
�0�)
Med
ian:
20A
live
�4
Sec
onda
ryO
LT
for
recu
rren
ceaf
ter
prio
rhe
pate
ctom
y:n
�2
Met
achr
onou
sch
olan
gioc
arci
nom
an
�1
Lev
yet
al,
2002
25
17*
(7M
/10F
)14
(82%
)(8
R/6
L)
3(1
8%)
5(2
9%)
4(2
4%)
7(N
A)
5�N
A�
NA
NA
Ull
rich
etal
,20
0226
38(2
0M/1
8F)
NA
NA
NA
NA
32(N
A)
4(1
Bili
ary
cirr
hosi
s3
refr
acto
rych
olan
gitis
�0�)
OL
T:
mea
n:43
OL
T:
wel
l
Esp
inoz
aet
al,
2003
27
66
(100
%)
(3R
/3L
)0
NA
NA
6(0
)0
Mea
n:28
Wel
l
Kas
sahu
met
al,
2005
11
33(1
5M/1
8F)
25(8
1%)
(13R
/12L
)6
(19%
)N
A3
(9%
)27
(2)
2�0
�M
edia
n:44
Wel
l�
93%
Hab
ibet
al,
2006
28
30(1
6M/1
4F)
NA
NA
9(3
0%)
1(3
%)
1(b
efor
eO
LT
)30
(NA
�8,
hepa
tic
deco
mpe
nsat
ion
�20
,re
curr
ent
chol
angi
tis
�1,
diff
use
exte
nt�
1)
Med
ian:
93P
atie
ntsu
rviv
alra
tes
1yr
�76
%5
yr�
65%
10yr
�56
%
Boc
khor
net
al,
2006
29
12(7
M/5
F)
8(6
7%)
(0R
/8L
)4
(33%
)2
(17%
)3
(25%
)9
(0)
2�0
�M
edia
n:31
Ali
vean
dw
ell
�92
%
Cur
rent
seri
es,
2006
33(2
1M/1
2F)
26(7
9%)
(6R
/20L
)7
(21%
)10
(30%
)2
(6%
)27
(0)
5�0
�M
ean:
91m
edia
n:80
Wel
l�
87%
Tot
al24
0*12
3/16
3(3
6R/6
4L)
40/1
63(2
5%)
31/1
35(2
3%)
14/1
96(7
%)
156
54
*Ass
ocia
ted
tofu
sifo
rmdi
lata
tion
(10
–30
mm
indi
amet
er)
ofth
eco
mm
onbi
ledu
ct(n
�9)
.†A
fter
prev
ious
hepa
tect
omy
(n�
2).
CH
Fin
dica
tes
chro
nic
hepa
tic
fibr
osis
;N
A,
data
not
avai
labl
e.
Mabrut et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins242

present series, the mean annual experience per center intreating such patients was less than 0.5. Although the prev-alence of congenital IHBD dilatations was estimated byNagorney30 to be less than 1% of BDC patients, congenitalIHBD dilatations represent 23% of all BDC patients in thepresent series over a 28-year study period. The prevalenceobserved in our patient population is thus clearly higher thanexpected and may be the result of referral bias to tertiaryreferral centers, concentrating experience in pediatric, HBPand liver transplant surgery.
We sticked to the definition of congenital communicat-ing intrahepatic BDC whatever the level of affected IHBD,adopting the Guntz et al classification,5 even if only type I iscorresponding to the initial description of Caroli et al. Indeed,the spectrum of shape and location of IHBD dilatations thathas been categorized by Guntz et al5 may be explained by thetime and the degree of embryological malformation of theductal plate.1
A striking particularity of the present series is that 15%of the patients were completely asymptomatic, thus undergo-ing prophylactic surgery, and that 39% of the patients had aclinical presentation not yet complicated by biliary infection.This feature is in contradiction with other reported series inwhich most patients with severe septic complications.11,29
Patients with congenital IHBD dilatations have a pre-disposition for synchronous cholangiocarcinoma with an es-timated risk of 100 times greater than that of the generalpopulation.31 The prevalence is reported to be 7% by Daytonet al31 in a large literature review of 142 patients, but possiblyreaching 24 and 25%25,29 (Table 5). In the present series, theprevalence was relatively low (6%), but both patients hadearly-stage cholangiocarcinoma leading to long-term cure at89 and 144 months after liver resection, respectively. Theearly disease diagnosis, illustrated by the relatively shortdelay between first symptoms and surgical treatment and theaggressive surgical treatment, even in asymptomatic patients,may concur to the relatively low incidence of synchronouscholangiocarcinoma encountered in the present series. Thesame features may explain why metachronous cholangiocar-cinoma was not encountered in the present series during amean follow-up of 91 months.
Congenital IHBD dilatations may involve the entireintrahepatic biliary tree diffusely or be confined to 1 lobe orsegment. Unilobar extension of the disease is more frequent,especially on the left side of the liver (Table 5).5 Our resultsare consistent with these findings with 79% of our patientswith unilobar extent and 61% from left unilobar diseaseextent. However, as for the rest of the literature, thisfeature is clearly the result in the present surgical series ofreferral bias in patient’s selection to surgical centers, witha false overrepresentation of unilobar disease forms. Theprevalence of bilobar disease forms is also underestimatedbecause of the lack of referral by physicians for potentialsurgical treatment.
The treatment of congenital IHBD dilatations is partic-ularly difficult and remains a challenge because of the rare-ness and the various presentations of the disease, leading to alack of experience for most of the centers. Various endo-
scopic or surgical drainage procedures have been reported,such as biliodigestive anastomoses with or without permanentaccess stoma using a Roux-Y jejunal loop brought to the skin,to allow retrograde access to the intrahepatic biliary tree forfurther treatments.32,33 Furthermore, in case of proximalintrahepatic ductal strictures, intrahepatic bilioenteric anasto-mosis was also reported to provide proximal biliary drain-age.19,34,35 However, all these drainage procedures are pal-liative treatment options, which are ineffective in the longterm and associated with recurrent septic complications.19,36
They should thus clearly be abandoned.Indeed, the only potential surgical treatment remains
resection of the diseased liver and aggressive endoscopicbiliary drainage procedures should be currently strictly lim-ited to inoperable patients.37 The disease extent within IHBD,the presence and severity of concurrent underlying chronicliver and renal diseases and the presence of cholangiocarci-noma are key factors for decision making when curativesurgical treatment is considered.
In case of unilobar form of the disease without anyconcurrent liver fibrosis or cirrhosis, partial hepatectomyachieves satisfactory results by providing a radical solution tothe recurrent problems of cholangitis, stone formation, andintrahepatic cholangiocarcinoma.11,18–20,27,29,38–41 In thepresent series satisfactory long-term results were achieved in21 of 23 patients (91%) with right or left unilobar forms ofthe disease after partial liver resection. These findings are inaccordance with the recent report by Kassahun et al11 andBockhorn et al.29 However, attention should be paid to theclearance of contralateral IHS, requiring additional postoper-ative radiologic or endoscopic procedures in nearly 20% ofthe patients in the present series. A percutaneous transhepaticapproach for flexible choledochoscopic stone clearance withor without intracorporeal lithotripsy could be useful for treat-ing residual IHS.42,43 Additionally, the rate of late complica-tions and reoperation after left lateral sectionectomy in leftunilobar congenital IHBD dilatation in the present seriesemphasized the probable need for performing initially at leasthemihepatectomy to remove the whole biliary tree of theaffected hemiliver. Moreover, extrahepatic bile duct resectionfollowed by biliodigestive reconstruction may be indicated inup to 25% of the patients,11 when the disease is involving themain biliary convergence.
In case of unilobar form of the disease with concurrentliver fibrosis or cirrhosis, treatment of the coexistent chronicliver disease by liver transplantation has emerged as a valu-able option of curative treatment. Indeed, liver transplantationallows radical treatment of both IHBD dilatations (responsi-ble for infectious and malignant complications) and underly-ing chronic liver disease (responsible for portal hypertensionand/or hepatic insufficiency).11,24,26 In the present series, onlyone such patient with Caroli syndrome with right unilobardisease extent (associated with renal insufficiency and con-current CHF with variceal bleeding because of the portalhypertension) has benefited from combined kidney-livertransplantation, with excellent long-term results during apostoperative follow-up of 18 years.
Annals of Surgery • Volume 246, Number 2, August 2007 Congenital Intrahepatic Biliary Cysts
© 2007 Lippincott Williams & Wilkins 243

In case of bilobar congenital IHBD dilatations withoutliver fibrosis or cirrhosis, the radical surgical options includedextended liver resection or liver transplantation, according tointrahepatic disease extent. When the contralateral diseaseextent was limited or localized and extirpable, extended liverresection was performed in 3 selected patients, achievinglong-term symptom-free and disease-free status in 2 and 1patient, respectively, during a median follow-up period of 74months (range: 28–80 months). The limited literature expe-rience with such difficult subgroup of patients confirmed thatunsatisfactory long-term outcome is usually achieved aftersuch major hepatectomies.19,24,26,42,44 On the contrary, incase of diffuse bilobar forms of the disease being complicatedby cholangitis from diffuse IHS, the sole curative option inour opinion is complete removal of IHBD dilatations by livertransplantation, achieving, good results in the literature45–47
(Table 5). Two patients in the present series underwent a livertransplant in this setting with good late outcome, despite theneed for retransplantation for acute humoral rejection in 1patient. However, Habib et al28 have recently reported asignificant poor impact on a 1-year-old patient’s survival inthe presence of preoperative cholangitis before transplanta-tion for Caroli disease.
In case of bilobar congenital IHBD dilatations compli-cated by liver fibrosis or cirrhosis, liver transplantation seemsto be the treatment of choice.11,23,24,26,28 Two such patientshave benefited from this therapeutic option in the presentseries with excellent long-term results.
Although the surgical management of bilobar forms ofcongenital IHBD dilatations remains a difficult challenge andcontroversial, and despite the operative risk in septic patientsand consequences of immunosuppressive therapy, we believethat liver transplantation represents the ultimate successfultreatment option for complicated forms of the disease (septiccomplications from diffuse extent of the disease into the liverand fibrosis or cirrhosis responsive to portal hypertension).De Kerckhove et al13 have recently reviewed the reportedliterature experience concerning 19 patients and the EuropeanLiver Transplant Registry (ELTR) experiences concerning110 patients who had undergone liver transplant for Carolidisease or syndrome, representing 0.2% of the whole numberof liver transplants in the ELTR. In the ELTR experience, themedian follow-up was 27 months and the 5- and 10-yearactuarial survival rates were 86% and 76%, respectively. Incase of chronic renal insufficiency because of the coexistentpolycystic kidney disease, combined liver-kidney transplan-tation should be favored, as illustrated in 2 patients in thepresent series and 14.5% in the ELTR experience. In therecent Habib et al series of 30 transplanted patients for Carolidisease,28 the patient survival rates at 1, 5, and 10 years were76%, 65%, and 56%, respectively, comparable to survivalafter liver transplantation for other aetiologies of chronic liverdisease. However, the 1-year survival rate was worse inpatients with Caroli syndrome whereas there was no differ-ence in long-term survival between Caroli disease and Carolisyndrome patients. However, the appropriate timing for trans-plantation remains difficult to appreciate in this instance. Itshould also be emphasized that early disease diagnosis and
avoidance of multiple ineffective endoscopic or surgicaldrainage procedures will undoubtedly reduce the technicaland septic risk of liver transplantation.9,28 Finally, the man-agement of invasive cholangiocarcinoma developed on con-genital IHBD dilatations is also controversial. Despite thetheoretical advantage of liver transplantation to allow radicalresection of the carcinoma and of the whole intrahepaticbiliary tree at risk for metachronous malignancy,6,8 a highrate of postoperative recurrence has been reported, favored byimmunosuppressive therapy. The introduction of new medi-cation combining immunosuppressive and anticancerous ef-fects might resolve this problem. In localized carcinoma onunilobar disease extent, radical liver resection seems to be anappropriate option, when oncologically possible.
Finally, aggressive surgical management of congenitalIHBD dilatations was safe in the present series, which wasassociated with no mortality but with major postoperativecomplication and reoperation rates of 19% and 6%, respec-tively. Kassahun et al11 reported a mortality rate of 6% afterpartial liver resections and 1 patient with aborted right hemi-hepatectomy for intraoperative septic shock after liver mobi-lization. Early disease diagnosis, treatment at an early diseasestage (including 5 patients at a preclinical stage), strict avoid-ance of endoscopic diagnostic approach and treatment andavoidance of emergency operation on uncontrollable septicpatients without adequate percutaneous transhepatic biliarydrainage are concurrent factors to explain the low morbidityrate achieved in the present series. In contradiction withKassahun et al,11 we promote noninvasive imaging studies,such as magnetic resonance cholangio-pancreatography, toachieve accurate disease diagnosis and staging with no risk ofsuperinfection. Additionally, intraoperative anterior approachusing the hanging maneuver48 may be suggested in right-sided congenital IHBD dilatations when septic presentationwas initially severe or when superinfection is not completelycontrolled by percutaneous transhepatic biliary drainage andwide spectrum antibiotic treatment.
In conclusion, the present series suggests that unilobarforms of congenital IHBD dilatations can be successfullytreated by liver resection, whereas bilobar diseases with CHFand portal hypertension or diffuse IHS are only curable byliver transplantation. Treatment at an early stage of thedisease, and avoidance of an endoscopic approach and of anemergency operation on septic patients are key factors toreduce the operative risk for the patients. Patients with con-genital IHBD dilatations should be referred early for surgicalmanagement.
REFERENCES1. Desmet VJ. Congenital disease of intrahepatic bile ducts: variations on
the ductal plate malformation. Hepatology. 1992;16:1069–1083.2. Todani T, Watanabe Y, Narusue M, et al. Congenital bile duct cyst:
classification, operative procedures, and review of 37 cases includingcancer arising from choledochal cyst. Am J Surg. 1977;134:263–269.
3. Caroli J, Couinaud C, Soupault R, et al. Une affection nouvelle, sansdoute congenitale, des voies biliaires: la dilatation kystique unilobairedes canaux hepatiques. Sem Hop Paris. 1958;34:136–142.
4. Grumbach R, Bourillon J, Auvert JP. Maladie fibro-kystique du foieavec hypertension portale chez l’enfant. Sem Hop Arch Anat Pathol.1954;74:30.
5. Guntz P, Coppo B, Lorimier G, et al. La maladie de Caroli unilobaire:
Mabrut et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins244

aspects anatomocliniques. Demarche diagnostique et therapeutique. Apropos de 3 observations personnelles et de 101 observations de lalitterature. J Chir. 1991;128:167–181.
6. Balsells J, Margarit C, Murio E, et al. Adenocarcinoma in Caroli’sdisease treated by liver transplantation. HPB Surg. 1993;7:81–87.
7. Totkas S, Hohenberger P. Cholangiocarcinoma associated with segmen-tal Caroli’s disease. Eur J Surg Oncol. 2000;26:520–521.
8. Takatsuki M, Uemoto S, Inomata Y, et al. Living-donor liver transplan-tation for Caroli’s disease with intrahepatic adenocarcinoma. J Hepato-biliary Pancreat Surg. 2001;8:284–286.
9. Nagorney DM. Biliary and liver cysts. In: Blumgart LH, Fong Y, eds.Surgery of the Liver and Biliary Tract. Vol. 2. 3rd ed. London: WBSaunders; 2000:1245–1258.
10. Summerfield JA, Nagafuchi Y, Sherlock S, et al. Hepatobiliary fi-bropolycystic diseases. A clinical and histological review of 51 patients.J Hepatol. 1986;2:141–156.
11. Kassahun WT, Kahn T, Wittekind C, et al. Caroli’s disease: liverresection and liver transplantation. Experience in 33 patients. Surgery.2005;138:888–898.
12. Partensky C. Hepatectomie droite pour maladie de Caroli. Lyon Chir.1996;92:165–166.
13. De Kerckhove L, De Meyer M, Verbaandert C, et al. The place of livertransplantation in Caroli’s disease and syndrome. Transpl Int. 2006;19:381–388.
14. American Society of Anaesthesiologists. New classification of physicalstatus. Anesthesiology. 1963;24:111.
15. Strasberg SM, Belghiti J, Clavien PA, et al. Modified from the Brisbane2000 terminology of liver anatomy and resections. Terminology com-mittee of the international HPB association. HPB. 2000;2:333–339.
16. Clavien PA, Sanabria JR, Strasberg SM. Proposed classification ofcomplications of surgery with examples of utility in cholecystectomy.Surgery. 1992;111:518–526.
17. Gigot JF, Nagorney DM, Farnell MB, et al. Bile duct cysts: a changingspectrum of presentation. J Hepatobiliary Pancreat Surg. 1996;3:405–411.
18. Nagasue N. Successful treatment of Caroli’s disease by hepatic resec-tion. Report of six patients. Ann Surg. 1984;200:718–723.
19. Mercadier M, Chigot JP, Clot JP, et al. Caroli’s disease. World J Surg.1984;8:22–29.
20. Knoop M, Keck H, Langrehr JM, et al. Therapy of unilobar Carolisyndrome by liver resection. Chirurg. 1994;65:861–866.
21. Dagli U, Atalay F, Sasmaz N, et al. Caroli’s disease: 1977–1995experiences. Eur J Gastroenterol Hepatol. 1998;10:109–112.
22. Gillet M, Favre S, Fontolliet C, et al. Maladie de Caroli monolobaire. Apropos de 12 cas. Chirurgie. 1999;124:13–18.
23. Shi LB, Peng SY, Meng XK, et al. Diagnosis and treatment of congenitalcholedochal cyst: 20 years’ experience in China. World J Gastroenterol.2001;7:732–734.
24. Ammori BJ, Jenkins BL, Lim PM, et al. Surgical strategy for cysticdisease of the liver in a western hepatobiliary center. World J Surg.2002;26:462–469.
25. Levy AD, Rohrmann CA, Murakata LA, et al. Caroli’s disease: radio-logic spectrum with pathologic correlation. AJR Am J Roentgenol.2002;179:1053–1057.
26. Ulrich F, Steinmuller T, Settmacher U, et al. Therapy of Caroli’s diseaseby orthotopic liver transplantation. Transplant Proc. 2002;34:2279–2280.
27. Espinoza R, San Martin S, Court F, et al. Hepatic resection in localizedCaroli disease. Rev Med Chil. 2003;131:183–189.
28. Habib S, Shakil O, Couto OF, et al. Caroli’s disease and orthotopic livertransplantation. Liver Transpl. 2006;12:416–421.
29. Bockhorn M, Malago M, Lang H, et al. The role of surgery in Caroli’sdisease. J Am Coll Surg. 2006;202:928–932.
30. Nagorney DM. Bile duct cysts in adults. In: Blumgart LH, Fong Y, eds.Surgery of the Liver and Biliary Tract. Vol. 2. 3rd ed. London: WBSaunders; 2000:1229–1244.
31. Dayton MT, Longmire WP, Tomkins R. Caroli’s disease: a premalignantconditions. Am J Surg. 1983;145:41–48.
32. Barker EM, Kallideen JM. Caroli’s disease: successful managementusing permanent-access hepaticojejunostomy. Br J Surg. 1985;72:641–643.
33. Pridgen JE, Aust JB, McInnis D. Primary intrahepatic gallstones. ArchSurg. 1977;112:1037–1044.
34. Watts DR, Lorenzo GA, Beal JM. Congenital dilatation of the intrahe-patic biliary ducts. Arch Surg. 1974;108:592–597.
35. Glenn F, McSherry C. Congenital segmental cystic dilatation of thebiliary ductal system. Ann Surg. 1973;177:705–713.
36. Witlin LT, Gadacz TR, Zuidema GD, et al. Transhepatic decompressionof the biliary tree in Caroli’s disease. Surgery. 1982;97:205–209.
37. Caroli-Bosc FX, Demarquay JF, Conio M, et al. The role of therapeuticassociated with extracorporal shock-wave lithotripsy and bile acid treat-ment in the management of Caroli’s disease. Endoscopy. 1998;30:559–563.
38. Lipsett PA, Pitt HA. Surgical treatment of choledochal cysts. J Hepa-tobiliary Pancreat Surg. 2003;10:352–359.
39. Ramond MJ, Huguet C, Danan G, et al. Partial hepatectomy in thetreatment of Caroli’s disease. Report of a case and review of theliterature. Dig Dis Sci. 1984;29:367–370.
40. Madariaga JR, Iwatsuki S, Starzl TE, et al. Hepatic resection for cysticlesions of the liver. Ann Surg. 1993;218:610–614.
41. Merono-Cabajosa EA, Celdran-Uriarte A, Moreno-CaparrosA, et al.Caroli’s disease: study of six cases, including one with epithelialdysplasia. Int Surg. 1993;78:46–49.
42. Aeberhard P. Surgical management of Caroli’s disease involving bothlobes of the liver. Br J Surg. 1985;72:651–652.
43. Pitt HA, Venbrux AC, Coleman J, et al. Intrahepatic stones: the trans-hepatic team approach. Ann Surg. 1994;219:527–537.
44. Izawa K, Tanaka K, Furui J, et al. Extended right lobectomy for Caroli’sdisease: report of a case and review of hepatectomized cases in Japan.Surg Today. 1993;23:649–655.
45. Sans M, Rimola A, Navasa M, et al. Liver transplantation in patientswith Caroli’s disease and recurrent cholangitis. Transpl Int. 1997;10:241–244.
46. Schiano TD, Fiel MI, Miller CM, et al. Adult presentation of Caroli’ssyndrome treated with orthotopic liver transplantation. Am J Gastroen-terol. 1997;92:1938–1940.
47. Waechter FL, Sampaio JA, Pinto RD, et al. The role of liver transplan-tation in patients with Caroli’s disease. Hepatogastroenterology. 2001;48:672–674.
48. Belghiti J, Guevara OA, Noun R, et al. Liver hanging maneuver: a safeapproach to right hepatectomy without liver mobilization. J Am CollSurg. 2001;193:109–111.
Annals of Surgery • Volume 246, Number 2, August 2007 Congenital Intrahepatic Biliary Cysts
© 2007 Lippincott Williams & Wilkins 245

ORIGINAL ARTICLES
Perioperative Mortality for PancreatectomyA National Perspective
James T. McPhee, MD,* Joshua S. Hill, MD,* Giles F. Whalen, MD,*Maksim Zayaruzny, MD, MPH,* Demetrius E. Litwin, MD, MBA,* Mary E. Sullivan, MS,*
Frederick A. Anderson, PhD,*† and Jennifer F. Tseng, MD*
Objective: To analyze in-hospital mortality after pancreatectomyusing a large national database.Summary and Background Data: Pancreatic resections, includingpancreaticoduodenectomy, distal pancreatectomy, and total pancre-atectomy, remain the only potentially curative interventions forpancreatic cancer. The goal of this study was to define factorsaffecting outcomes after pancreatectomy for neoplasm.Methods: A retrospective analysis was performed using all patientsundergoing pancreatic resections for neoplastic disease identifiedfrom the Nationwide Inpatient Sample from 1998 to 2003. Crudein-hospital mortality was analyzed by �2. A multivariable model wasconstructed to adjust for age, sex, hospital teaching status, hospitalsurgical volume, year of resection, payer status, and selected comor-bid conditions.Results: In all, 279,445 patient discharges were identified with aprimary diagnosis of pancreatic neoplasm. A total of 39,463 (14%)patients underwent resection during that hospitalization. In-hospitalmortality was 5.9% with a significant decrease from 7.8% to 4.6%from 1998 to 2003 by trend analysis (P � 0.0001). Resections doneat low (�5 procedures/year)- and medium (5–18/year)-volume cen-ters had higher mortality compared with those at high (�18/year)-volume centers (low-volume odds ratio � 3.3; 95% confidenceinterval, 2.3–4.; medium-volume, odds ratio � 2.1; 95% confidenceinterval, 1.5–3.0). The proportion of procedures performed at highvolume centers increased from 30% to 39% over the 6-year timeperiod (P � 0.0001) by trend test.Conclusions: This large observational study demonstrates an im-provement in operative mortality for patients undergoing pancrea-tectomy for neoplastic disease from 1998 to 2003. In addition, agreater proportion of pancreatectomies were performed at high-
volume centers in 2003. The regionalization of pancreatic surgerymay have partially contributed to the observed decrease in mortalityrates.
(Ann Surg 2007;246: 246–253)
Pancreatic cancer remains the fourth leading cause ofcancer deaths overall in the United States, killing an
estimated 31,800 people in 2005.1 A number of single-institution and single-state reports have described an im-provement in perioperative mortality in the 1980s and 1990sfor high-risk cancer resections, including pancreaticoduode-nectomy (PD).2–4 In the state of Maryland, concurrent with amove toward statewide regionalization of PD, a decrease inperioperative mortality was described over an 11-year span.2
In contrast, in 2002, a national study based on theMedicare Provider Analysis and Review database evaluatedtrends in operative outcomes over time for high-risk proce-dures.5 This study, which included PD, concluded that nosignificant improvement in perioperative mortality was foundfor the years 1994 to 1999 for PD. While previous studieshave focused on resections of the pancreatic head, there is apaucity of national data focused on distal pancreatectomy andtotal pancreatectomy for neoplastic disease. Several studiesevaluating surgical outcomes are limited by number of sub-jects or by single-institutional design.6–10
The inverse relationship between mortality and hospitalsurgical volume for high-risk procedures, including majorcancer resections, has been demonstrated in prior studies overthe past several years.11–17 Researchers working in collabo-ration with organizations such as the Leapfrog Group haveproposed that patient lives can be saved by the enforcementof volume criteria.18 This information is readily available tothe consumer (www.leapfroggroup.org).19
In the current work, we sought to analyze the nationalpicture on perioperative mortality for pancreatic resection,including PD, distal pancreatectomy, and total pancreatec-tomy, for all neoplastic disease including all periampullarycancers as well as benign neoplastic disease. If perioperativemortality for major pancreatic resection has declined, a por-tion of this decline might be attributable to a change inreferral patterns, with a greater percentage of proceduresbeing performed at higher-volume centers.
From the *Department of Surgery and †Center for Outcomes Research,University of Massachusetts Medical School, Worcester, MA.
Supported by the Pancreatic Cancer Alliance, the PanCan-ASCO SamuelStroum Young Investigator Award, and a Howard Hughes MedicalInstitute Early Career Award (all to J.F.T.).
Presented in part at American Society of Clinical Oncology GI CancerSymposium, San Francisco, January 26–28, 2006, and at the 42nd ASCOAnnual Meeting, Atlanta, June 2–6, 2006.
Reprints: Jennifer F. Tseng, MD, University of Massachusetts MedicalSchool, UMass Memorial Medical Center, 119 Belmont Street, SwiftHouse, Worcester, MA 01605-2982. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0246DOI: 10.1097/01.sla.0000259993.17350.3a
Annals of Surgery • Volume 246, Number 2, August 2007246

MATERIALS AND METHODS
DatabaseTo evaluate trends in pancreatic resection for neoplastic
disease at the national level, we used the Nationwide Inpa-tient Sample (NIS) for the years 1998 to 2003, inclusive. TheNIS is the largest national all-payer hospital inpatient caredatabase in the United States. Data exist for approximately 7million hospital discharges per year from a stratified sampleof 20% of nonfederal U.S. community hospitals from partici-pating states (n � 37 in 2003), including academic and specialtyhospitals.20 The NIS is supported by the Healthcare Cost andUtilization Project and contains all-payer discharge informationfor 100% of patient discharges from participating hospitals. Itcontains hospital level information obtained from a direct link tothe American Hospital Association’s annual survey of hospitals,which includes hospital type (teaching/nonteaching) and geo-graphic region (Northeast, West, South, Midwest as defined bythe U.S. Census Bureau). A weighting strategy is implementedby the NIS to allow population-based estimates to be drawn atthe national level. Sampled hospitals are given appropriateweights based on the number of hospitals they represent in thedatabase for a given year.20 All statistical analyses were per-formed based on these survey weights; therefore, all data pro-vided in the results represent weighted frequencies.
Diagnosis CodesThe primary measured outcome for this study was
in-hospital mortality. Mortality was defined as death fromany cause prior to discharge regardless of time from opera-tion. To identify all patient discharges with the principaldiagnosis of pancreatic neoplasm, including benign lesions,we used selected codes from the International Classificationof Diseases Ninth Revision Clinical Modification (ICD-9-CM).21 We limited the initial cohort to those patients under-going pancreatectomy based on the ICD-9 procedure codesfor pancreatic resections (Table 1).
Volume AnalysisTo evaluate hospital surgical volume, we categorized
the hospitals as low volume (average �5 pancreatic resec-tions/year over the years analyzed), medium volume (average5–18 resections/year), or high volume (average �18 resec-tions/year). These procedure volume numbers were selectedto obtain 3 volume groups of approximately equal sizes forpurposes of comparison prior to any volume–outcome dataanalyses, a technique previously described by other authors.12
Statistical AnalysisAll data were analyzed using the advanced survey
procedures in SAS version 9.1 (SAS Institute, Cary, NC).Univariate analyses of categorical variables were performedusing Rao-Scott �2 tests, with a P value �0.05 consideredstatistically significant. All pancreatic resections were firstevaluated in aggregate form, and then separate univariateanalyses were performed to evaluate PD, distal pancreatec-tomy, and total pancreatectomy. Proximal pancreatectomywas thought to include heterogeneous operations (eg, PD,duodenum-sparing pancreatectomy); thus, a separate analysiswas not included. Trend analyses were performed using theMantel-Haenszel �2 test. A multivariable logistic regressionwas constructed with in-hospital mortality as the dependentvariable. Independent variables included patient age group(�50, 50–69, �70 years), sex, race, and year of resection.Additionally, various comorbid medical conditions were in-cluded in the analyses from previously established comorbid-ity software for use with national datasets (congestive heartfailure, chronic lung disease, valvular heart disease, renalfailure, diabetes mellitus, liver disease, obesity, and periph-eral vascular disease).22 Certain hospital level characteristics,including calculated surgical volume, geographic region (asdescribed above), and teaching status, were also evaluated asindependent variables.
TABLE 1. ICD-9 CM Diagnostic and Procedural Codes
DiagnosticCode Diagnosis
ProceduralCode Procedure
152.0 Malignancy of duodenum 52.6 Pancreatectomy (total) with synchronous duodenectomy
156.1 Malignancy of extrahepatic bile ducts 52.7 Pancreaticoduodenectomy, radical (one-stage) (two-stage)
156.2 Periampullary malignancy 52.51 Proximal pancreatectomy (head) (with part of body)(with synchronous duodenectomy)
156.8 Unspecified bile duct malignancy 52.52 Distal pancreatectomy (tail) (with part of body)
157.0 Malignancy of pancreatic head 52.53 Radical/subtotal pancreatectomy
157.1 Malignancy of pancreatic body 52.59 Pancreatectomy/pancreaticoduodenectomy partial NEC
157.2 Malignancy of pancreatic tail 52.51 Proximal pancreatectomy (head) (with part of body)(with synchronous duodenectomy)
157.3 Malignancy of pancreatic ducts 52.52 Distal pancreatectomy (tail) (with part of body)
157.8 Malignancy of neck, contiguous sites, ectopic tissue 52.53 Radical/subtotal pancreatectomy
157.9 Malignant primary of pancreas 52.59 Pancreatectomy/pancreaticoduodenectomy partial NEC
211.6 Benign neoplasm of pancreas
235.5 Pancreatic neoplasm of uncertain behavior
230.9 Malignant neoplasm in situ
239.0 Unspecified pancreatic neoplasm
Annals of Surgery • Volume 246, Number 2, August 2007 Perioperative Mortality After Pancreatectomy
© 2007 Lippincott Williams & Wilkins 247

Unadjusted and adjusted odds ratios were calculated todetermine the effects of the identified covariates on theoutcome measure of perioperative mortality.
Patient race was evaluated by univariate analysis andwas initially included in the logistic regression. However, dueto a prohibitive amount of missing data, race was ultimatelyexcluded from the multivariate analysis.
RESULTS
DemographicsDuring the sampled time frame 1998 to 2003, 279,445
patient discharges occurred for the principal diagnosis ofpancreatic neoplasm. Overall, 39,463 (14%) patients under-went pancreatic resection during that hospitalization, for anaverage of 6600 resections per year. Of the operative cohort,52% were female. The mean age for all patients was 69 years(range, 18–103 years) while the mean age for operativepatients was 64 years (range, 18–93 years). Patient charac-teristics, including the univariate analysis of mortality, areshown in Table 2. Of patients who underwent resection, 63%had operations for malignancy of the pancreatic head, neck,or periampullary region. Table 3 includes the breakdown ofpatient characteristics by hospital volume strata, includingprocedure type and medical comorbidities.
Univariate AnalysisFor all resected patients, the crude in-hospital mortality
rate was 5.9%. The Mantel-Haenszel test for linear associa-tion, which included all of the studied years, revealed that themortality decrease over time from 7.8% in 1998 to 4.6% in2003 was a significant trend (P � 0.0001) (Fig. 1). Mortalitywas higher for males than for females (P � 0.0001). Inaddition, in-hospital mortality increased with older patientage (P � 0.0001). Institutional annual surgical volume in-versely correlated with mortality in the univariate analysis.The highest-volume centers (�18 resections/year) had a mor-tality of 2.5% compared with medium-volume centers (5–18resections/year) and low-volume centers (�5 resections/year), which had overall mortality rates of 5.9% and 9.2%,respectively (P � 0.0001). This inverse relationship of de-creasing mortality with increasing volume was also signifi-cant by the trend test (P � 0.0001) (Table 2).
Multivariable AnalysisUsing a multivariable logistic regression model, inde-
pendent predictors of in-hospital mortality were evaluated. Ahospital’s annual surgical volume was highly predictive of
TABLE 2. Patient and Hospital Characteristics for AllPancreatic Resections for Neoplasm (1998–2003): Results ofUnivariate Analysis of Mortality Included
FactorOverallNo. (%)
MortalityRate (%) P
No. patients (weighted) 39,463 (100) 5.9 NAAge (yr) �0.0001Mean (SEM) 64.1 (0.19)
�50 5392 (13.7) 1.850–69 18,390 (46.6) 4.7�70 15,652 (39.7) 8.8
Sex �0.0001F 20,329 (51.6) 4.4M 19,082 (48.4) 7.5
Race 0.02White 23,596 (79.6) 5.8Nonwhite 6066 (20.4) 5.7
Year of resection 0.0441998 4893 (12.4) 7.81999 6362 (16.1) 4.82000 5688 (14.4) 6.72001 6609 (16.8) 6.42002 7525 (19.1) 6.02003 8346 (21.1) 4.6
Diagnosis type �0.0001Periampullary malignancy 24,725 (62.7) 6.7Benign/unspecified 6943 (17.6) 3.5Malignancy of body/tail 3807 (9.7) 4.8Biliary tract neoplasm 1823 (4.6) 7.8Ductal malignancy 802 (2.0) 8.8Metastatic disease 703 (1.8) 3.5Islet cell neoplasm 619 (1.6) 1.3
Procedure type 0.0002Pancreaticoduodenectomy 27,289 (72.3) 6.6Distal pancreatectomy 7872 (20.8) 3.5Total pancreatectomy 1399 (3.7) 8.3Other 1201 (3.2) 5.4
Comorbid conditionsOther/none 23,642 (57.2) NA NADiabetes mellitus 7728 (19.6) 4.3 0.003Chronic lung disease 4465 (11.3) 8.6 0.0002Congestive heart failure 1657 (4.2) 16.7 �0.0001Valvular heart disease 1409 (3.6) 7.3 0.36Liver disease 1083 (2.7) 10.9 0.002Obesity 883 (2.2) 1.1 0.006Peripheral vascular disease 690 (1.8) 12.7 0.002Renal failure 395 (1.0) 36.1 �0.0001
Payer status 0.39Private/HMO 35,924 (91.3) 6.0Medicaid/self-pay/other 3416 (8.7) 5.2
Hospital type �0.0001Teaching 28,351 (71.9) 4.5Nonteaching 11,068 (28.1) 9.5
Hospital geographic region 0.06Northeast 8694 (22.1) 5.0Midwest 9605 (24.4) 5.1South 13,323 (33.8) 7.2West 7801 (19.8) 5.6
(Continued )
TABLE 2. (Continued)
FactorOverallNo. (%)
MortalityRate (%) P
Hospital surgical vol. �0.0001
Low (�5/yr) 13,575 (34.4) 9.2
Medium (5–18/yr) 13,047 (33.1) 5.9
High (�18/yr) 12,802 (32.5) 2.4
NA indicates not applicable.
McPhee et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins248

in-hospital mortality. Compared with the high-volume cen-ters (�18 resections/year), the low-volume centers (�5 re-sections/year) had 3.3 times higher likelihood of death in thehospital (95% confidence interval �CI�, 2.3–4.8), while themedium-volume centers (5–18 resections/year) had odds ratioof death of 2.1 (95% CI, 1.5–3.0) compared with high-volume centers (P � 0.0001). Patient factors that weresignificantly predictive of in-hospital mortality included malesex (P � 0.0001), older age (P � 0.0001), and certaincomorbid medical conditions, including renal failure (P �0.0001), congestive heart failure (P � 0.0001), and a historyof liver disease (P � 0.003) (Table 4; Fig. 2).
Overall, the year of resection, when evaluated as acontinuous variable, was not independently predictive of adifference in mortality (P � 0.11). However, when evaluatedas a categorical variable, which included all of the studiedyears; the year 1998, when directly compared with the year2003, demonstrated an adjusted odds ratio of mortality of1.49 (95% CI, 1.04–2.13). The remainder of the years whencompared with 2003 did not demonstrate a significant value.Payer status (P � 0.10), obesity (P � 0.11), chronic lungdisease (P � 0.34), and valvular heart disease (P � 0.63) alsowere not independently predictive of in-hospital mortality inthe adjusted logistic regression model.
To assess whether practice and referral patterns tohigher-volume centers could explain a portion of the ob-served decrease in perioperative mortality rates, the percent-
age of cases performed over time in the different volumedesignated hospitals was evaluated. In 1998, 30% of resec-tions were performed at high-volume centers; and in 2003,39% of pancreatic resections were performed at high-volumecenters. This increasing percentage of cases performed athigh-volume centers over time was significant by the trendtest (P � 0.0001) (Fig. 3).
Using the overall mortality rates for patients at high-,medium-, and low-volume centers, we calculated the ex-pected change in mortality from 1998 to 2003 based on thisshift from low- to high-volume centers. This predicted achange in mortality of 0.8% from 1998 to 2003, whichaccounts for approximately one fourth of the observed changeof 3.3% in our cohort, indicating that, to some degree (ap-proximately 25%), this shift to higher-volume centers hascontributed to the observed decrease in mortality rate.
Mortality by ProcedureSeparate univariate analyses were performed for PD,
distal pancreatectomy, and total pancreatectomy for neoplas-tic disease. The results of these univariate analyses can befound in Table 5. PD was the most frequent procedureperformed (72%). The overall perioperative mortality ratewas 6.6%. By the trend test, there was a significant decreasein mortality from 8.2% in 1998 to 5.5% by 2003 (P � 0.003).The mortality rate was higher for men compared with women(8.2% vs. 4.8%, P � 0.0001), as well as the oldest patient
TABLE 3. Hospital Characteristics for All Pancreatic Resections for Neoplasm by Volume Designations
Low (<5/year) Medium (5–18/year) High (>18/year) Overall P
No. (%) hospitals 1356 (78) 321 (18.4) 66 (3.8) 1743 NA
No. patients* 13,575 13,047 12,802 39,463 0.94
Age (yr) �mean (SEM)� 64.9 (0.23) 64.1 (0.25) 63.3 (0.25) 64.1 (0.14) �0.0001
Age groups 0.003
�50 yr (%) 12.5 13.8 14.8 13.7
50–69 yr (%) 44.8 46.5 48.7 46.6
�70 yr (%) 42.7 39.7 36.5 39.7
Sex 0.09
M (%) 46.6 49.3 49.5 48.4
F (%) 53.4 50.7 50.5 51.6
Procedure type (%) 0.02
Pancreaticoduodenectomy 68.4 74.0 74.6 72.3
Distal pancreatectomy 24.6 19.4 18.4 20.8
Total pancreatectomy 3.8 3.5 3.8 3.7
Other 3.2 3.5 3.2 3.2
Comorbid conditions (%)
Other/none 51.4 46.1 41.4 46.4 NA
Diabetes 20.4 19.8 18.4 19.6 0.23
Chronic lung disease 14.1 10.7 9.0 11.3 �0.0001
Congestive heart failure 5.9 3.8 2.9 4.2 �0.0001
Valvular heart disease 3.3 3.6 3.8 3.6 0.66
Liver disease 2.4 2.7 3.2 2.7 0.38
Obesity 2.3 2.5 1.9 2.2 0.37
Peripheral vascular disease 1.7 1.9 1.7 1.8 0.84
Renal failure 1.3 1.1 0.51 1.0 0.004
*Weighted frequency.NA indicates not applicable.
Annals of Surgery • Volume 246, Number 2, August 2007 Perioperative Mortality After Pancreatectomy
© 2007 Lippincott Williams & Wilkins 249

group (�70 years) compared with the youngest group (�50years) (9.5% vs. 2.6%, P � 0.0001). The lowest-volumepancreatic surgery centers had significantly higher mortalityrates compared with the highest-volume centers (11.1% vs.2.7%, P � 0.0001).
Distal pancreatectomy was the second most commonprocedure performed (21%). This had the lowest overallmortality rate of all studied resection types (3.5%). Mortalityrate was significantly higher for men (4.9% vs. 2.8%, P �0.029), older patients (patients �70 years, 6.5% vs. patients�50 years, 0.3%, P � 0.0001), and patients undergoingoperations at the lowest-volume centers (5.1% vs. 0.43% forhigh-volume centers, P � 0.0001) (Table 5).
Total pancreatectomy was the least common procedure(3.7%). These patients had the highest overall perioperativemortality at 8.3%, a factor that did not significantly vary byhospital volume (P � 0.85). A patient’s sex did not significantlyinfluence mortality, (P � 0.42). The youngest patient group (age�50 years) did not have a significantly lower in-hospital mor-tality compared with the older patient groups (age 50–70 andage �70 years) (3.0% vs. 9.6% and 8.3%, respectively, P �0.49).
DISCUSSIONIn this study, we have demonstrated that pancreatic
resections for neoplastic disease remain operations that areassociated with significant perioperative mortality in the cur-rent era. We found an overall in-hospital mortality rate of5.9% for all pancreatic resections for neoplastic disease. Thisrate has significantly decreased over time. In-hospital mor-tality decreased from 7.8% in 1998 to 4.6% by 2003. Afterpancreatectomy, in-hospital mortality correlated inversely
with volume; the high-volume centers had a crude mortalityrate of 2.4% compared with 9.2% for the low-volume group.After multivariable analysis, a hospital’s annual surgicalvolume, remained strongly associated with in-hospital mortality,with the low-volume centers having odds ratio of death of 3.3compared with the high-volume centers. Intriguingly, our datasuggest that increasing regionalization of these high-risk opera-tions may have contributed in part to the observed improvementin outcome and that approximately one fourth of the observeddecrease in mortality may be attributable to more pancreatecto-mies being performed at high-volume centers. Older patients,males, and individuals with medical comorbidities had higherperioperative mortality for pancreatic resection.
Our results, with an overall mortality of 5.9%, comparefavorably with previously published reports, which arelargely limited to resections involving the pancreatic head.Our overall PD in-hospital mortality rate of 6.6% for 27,323PDs shows a substantial decrease from that reported in previousnational surveys, which typically report values of �10%5,15 upto 14%.11 Of note, the NIS is an all-payer database and includesall adult patients, in contrast to studies using other databases,which may be limited to patients 65 years of age or older.5,13,15
Additionally, the current work reports in-hospital mortality ratesas opposed to 30-day mortality rates.5,13
In our study, mortality rates differed according to thetype of pancreatic resection performed. PD was the mostfrequent procedure performed, and the overall in-hospitalmortality rate for the 27,323 patients by weighted analysisundergoing PD was 6.6%. In analyzing risk factors by type ofprocedure, we found that men had significantly higher mor-tality rates compared with women for PD (8.2% vs. 4.8%).Because of the paucity of published national data on in-hospital mortality for distal pancreatectomy and total pancre-atectomy for neoplastic disease, these procedures were eval-uated as separate analyses. The observed in-hospital mortalityrate for distal pancreatectomy in 7876 patients was 3.5%.Considerable variability exists in the literature, with periop-erative mortality rates for distal pancreatectomy ranging from0% to 21%.6–9 These prior studies are generally limited bytotal number due to single-institution or case series. Totalpancreatectomy for neoplasm is a rarely performed proce-dure; indeed, some authors have questioned it as a viabletreatment option for malignancy due to its poor overallsurvival despite its technical feasibility.10 No specific na-tional benchmark was identified for the purposes of compar-ison to our study, which found an overall mortality rate aftertotal pancreatectomy of 8.3%; however, in smaller series, theperioperative mortality rate ranges from 3% to 28%.10,23 Inthe current work, the relatively small number of patientsundergoing total pancreatectomy (n � 1399) limited thesignificance of comparisons made between groups as seen inthe observed differences in mortality rates between the low-volume (9.6%) and high-volume (7.2%) groups (P � 0.85).
In the literature, conflicting data exist regarding animprovement in perioperative mortality over time for PD.Goodney et al, using the Medicare Provider Analysis andReview database from 1994 to 1999, found no significantimprovement in mortality for pancreatectomy over a 6-year
FIGURE 1. The in-hospital mortality rate (%) for all pancre-atic resections for neoplasm from 1998 to 2003. The de-crease over time was a significant trend (P � 0.0001).
McPhee et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins250

period, with the mortality rate remaining greater than 10%over the duration of the study.5 This may reflect in part adifference in patient case-mix between the databases. In
addition, the current series, which covers the years 1998 to2003, may better capture a national trend toward the region-alization of high-risk surgery. The decreasing mortality rateover time for PD seen in this study is comparable to thefindings by Gordon et al with data from the state of Marylanddemonstrating a decrease in perioperative mortality over a12-year period concurrent with the regionalization of pancre-atic surgery to high-volume centers.2 In addition, Kotwall etal, in their NIS-based analysis, identified a progressive de-crease in mortality from 1988 through 1995, although themortality rate in 1995 was still greater than 8%,11 in contrastto the 5.9% seen in our study from 1998 to 2003. The fact thatthe decreased mortality rate seen in the current study was notuniformly linear indicates that other confounding factors mayexist, such as hospital sampling variability and coding inac-curacies, despite the rigorous sampling methodology used bythe NIS.20
With administrative databases, the difficulty of accu-rately assessing patient case-mix, including severity of co-morbid disease, and distinguishing preexisting comorbidityfrom postoperative complications, is well documented.24,25 Inthis study, these limitations certainly apply. We have no
FIGURE 2. The multivariable logistic regression for in-hospi-tal mortality following pancreatic resection for neoplasm.Data are adjusted odds ratios with 95% confidence intervals.
TABLE 4. Logistic Regression of In-Hospital Mortality (Unadjusted and Adjusted)
FactorOdds Ratio
(Unadjusted)95% Confidence
IntervalOdds Ratio(Adjusted)
95% ConfidenceInterval
Patient sex
Men (vs. women) 1.76 1.45–2.13 1.63 1.32–2.00
Age groups (yr)
�70 (vs. �50) 5.38 3.40–8.51 4.43 2.68–7.30
�70 (vs. 50–69) 1.97 1.63–2.39 1.83 1.48–2.28
Year of resection
1998 (vs. 2003) 1.76 1.14–2.72 1.49 1.04–2.13
1999 (vs.2003) 1.06 0.74–1.53 1.02 0.71–1.46
2000 (vs. 2003) 1.51 1.04–2.20 1.35 0.95–1.91
2001 (vs. 2003) 1.42 0.96–2.10 1.31 0.91–1.90
2002 (vs. 2003) 1.34 0.93–1.95 1.37 0.97–1.94
Insurance type
Medicaid/self-pay (vs. Medicare/private) 0.86 0.60–1.22 1.19 0.81–1.75
Procedure Type
Distal pancreatectomy (vs. pancreaticoduodenectomy) 0.52 0.39–0.69 0.57 0.42–0.77
Total pancreatectomy (vs. pancreaticoduodenectomy) 1.28 0.80–2.06 1.39 0.86–2.25
Comorbidities
Diabetes mellitus (vs. none) 0.66 0.51–0.87 0.59 0.45–0.79
Chronic lung disease (vs. none) 1.59 1.24–2.04 1.17 0.90–1.53
Valvular heart disease (vs. none) 1.27 0.76–2.11 0.90 0.53–1.52
Congestive heart failure (vs. none) 2.45 1.73–3.49
Liver disease (vs. none) 2.01 1.28–3.16 2.07 1.30–3.29
Obesity (vs. none) 3.51 2.58–4.78 0.32 0.08–1.28
Peripheral vascular disease (vs. none) 2.37 1.35–4.15 2.18 1.24–3.82
Renal failure (vs. none) 9.53 5.95–15.3 7.09 4.03–12.5
Hospital surgical vol.
Low (vs. high) 4.12 3.04–5.58 3.33 2.33–4.75
Medium (vs. high) 2.53 1.84–3.48 2.14 1.52–3.01
Hospital teaching status
Nonteaching (vs. teaching) 2.24 1.79–2.81 1.25 0.97–1.62
Annals of Surgery • Volume 246, Number 2, August 2007 Perioperative Mortality After Pancreatectomy
© 2007 Lippincott Williams & Wilkins 251

information on stage of disease or patient preoperative per-formance status; however, other reports have concluded thatpatient level characteristics probably do not account for ob-
served mortality outcomes across hospital volume strata.12,15,16
Likewise, certain patient demographic information such as racewas excluded from the final multivariable regression due to aprohibitive amount of missing data, which is a known limitationof administrative datasets. As noted above, the current worklooks at the outcome measure of in-hospital mortality. This mayreflect a lower mortality rate compared with studies utilizing30-day mortality rates, especially if patients are being dischargedfrom the hospital prior to their death. Other outcomes such asmore comprehensive 30-day and long-term mortality data aswell as postoperative morbidity and complications, includingreoperation, pancreatic leak rates, and hospital readmission, arecrucial in evaluating performance across hospital surgical vol-ume strata in addition to trends over time.
The reasons for a decrease in perioperative mortalityfor pancreatic resection over time are multifactorial. Our datasuggest that a modest proportion (�25%) may be attributableto a shift of high-risk procedures to higher-volume centerswith demonstrated superior outcomes. It should be noted thatat the lowest-volume centers, which had the most room forimprovement, a substantial decrease in perioperative mortal-ity also occurred over time. We can speculate about a referralbias where the higher-risk patients or the more difficultresections were referred to higher-volume centers; however,the mean patient age and comorbidity profiles were similaracross the volume designations. Other factors may includeimprovements in patient selection over time, the developmentof diagnostic modalities for more accurate preoperativestaging, advances in perioperative care, and the presence ofclinical pathways for pancreatic surgery.26,27 These and otherfactors warrant further investigation.
TABLE 5. Univariate Analyses of Mortality for Pancreaticoduodenectomy, Distal Pancreatectomy, and TotalPancreatectomy
Factor
Pancreaticoduodenectomy Distal Pancreatectomy Total Pancreatectomy
Mortality (%) P Mortality (%) P Mortality (%) P
Overall 6.6 NA 3.5 NA 8.3 NA
Sex �0.0001 0.029 0.42
M 8.2 4.9 7.0
F 4.8 2.8 9.8
Age (yr) �0.0001 �0.0001 0.49
�50 2.6 0.3 3.0
50–69 4.8 3.0 9.6
�70 9.5 6.5 8.3
Year of resection 0.003 (trend) 0.007 (trend) 0.039 (trend)
1998 8.2 3.1 17.1
1999 5.4 3.5 4.1
2000 7.3 5.2 12.2
2001 7.0 4.6 5.2
2002 6.7 3.7 8.9
2003 5.5 1.6 6.4
Hospital surgical vol. �0.0001 �0.0001 0.85
Low (�5/yr) 11.1 5.1 9.6
Medium (5–18/yr) 6.2 4.3 8.0
High (�18 yr) 2.7 .43 7.2
NA indicates not applicable.
FIGURE 3. The percentage of pancreatic resections for neo-plasm performed at high volume centers from 1998 to2003. The shift over time was a significant trend (P � 0.0001).
McPhee et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins252

One factor that deserves future consideration is theconcrete definition of a “high volume center” for pancreate-ctomy in practice. In the current and previous works based onnationally abstracted data, the cutoff points used to createvolume designations are predicated by statistical necessity, ie,maintaining equally sized patient groups for the purposes ofcomparison, therefore yielding varying “high-volume” defi-nitions based on the dataset, patient population, or years ofstudy. Of note, the Leapfrog Group, in reporting to consumersand payers alike, on their website (www.leapfroggroup.org),19
requires �11 pancreatic resections/year for an institution toobtain “full-credit” for pancreatectomy.
We have added to the growing body of evidence thatpatients are more likely to survive the postoperative periodfor pancreatic resection at high-volume hospitals. Other au-thors have demonstrated that, beyond in-hospital mortality,long-term survival is also improved through treatment athigh-volume centers.28 In the current era, the only possibilityof cure for a pancreatic neoplasm involves surgical resec-tion.29 Actuarial 5-year survival for pancreatic adenocarci-noma after PD remains only 18% in the most experienced ofhands.30 These facts emphasize the need to minimize periop-erative mortality to improve patients’ chances at long-termsurvival. A critical controllable step for decreasing a patient’srisk of mortality in the management of pancreatic cancer isthe referral to a high-volume pancreatic surgery center.
REFERENCES1. Jemal A, Murray T, Ward E, et al. Cancer Statistics, 2005. Ca Cancer
J Clin. 2005;55:10–30.2. Gordon T, Bowman H, Tielsch J, et al. Statewide regionalization of
pancreaticoduodenectomy and its effect on in-hospital mortality. AnnSurg. 1998;228:71–78.
3. Whooley BP, Law S, Murthy SC, et al. Analysis of reduced death andcomplication rates after esophageal resection. Ann Surg. 2001;233:338–344.
4. Msika S, Benhamiche AM, Tazi MA, et al. Improvement of periopera-tive mortality after curative resection for gastric cancer: population-based study. World J Surg. 2000;24:1137–1142.
5. Goodney P, Siewers A, Stukel T, et al. Is surgery getting safer? Nationaltrends in perioperative mortality. J Am Coll Surg. 2002;195:219–227.
6. Sledzianowski J, Duffas J, Muscari F, et al. Risk factors for mortalityand intra-abdominal morbidity after distal pancreatectomy. Surgery.2005;137:180–185.
7. Fahy B, Frey C, Ho H, et al. Morbidity, mortality, and technical factorsof distal pancreatectomy. Am J Surg. 2002;183:237–241.
8. Christein J, Kendrick M, Iqbal C, et al. Distal pancreatectomy forresectable adenocarcinoma of the body and tail of the pancreas.J Gastrointest Surg. 2005;9:922–927.
9. Wade T, Virgo K, Johnson F, et al. Distal pancreatectomy for cancer:
results in U. S. department of veterans affairs hospitals, 1987–1991.Pan-creas. 1995;11:341–344.
10. Karpoff H, Klimstra D, Brennan M, et al. Results of total pancreatec-tomy for adenocarcinoma of the pancreas. Arch Surg. 2001;136:44–47.
11. Kotwall C, Maxwell J, Brinker C, et al. National estimates of mortalityrates for radical pancreaticoduodenectomy in 25,000 patients. Ann SurgOncol. 2002;9:847–854.
12. Finlayson E, Goodney P, Birkmeyer J. Hospital volume and perioperativemortality in cancer surgery: a national study. Arch Surg. 2003;138:721–725.
13. Begg C, Cramer L, Hoskins W, et al. Impact of hospital volume onperioperative mortality for major cancer surgery. JAMA. 1998;280:1747–1751.
14. Birkmeyer J, Warshaw A, Finlayson S, et al. Relationship betweenhospital volume and late survival after pancreaticoduodenectomy. Sur-gery. 1999;126:178–183.
15. Birkmeyer J, Finlayson S, Tosteson A, et al. Effect of hospital volumeon in-hospital mortality with pancreaticoduodenectomy. Surgery. 1999;125:250–256.
16. Birkmeyer J, Siewers A, Finlayson E, et al. Hospital volume and surgicalmortality in the United States. N Engl J Med. 2002;346:1128–1137.
17. Janes R, Niederhuber J, Chmiel J, et al. National patterns of care forpancreatic cancer: results of a survey by the commission on cancer. AnnSurg. 1996;223:261–272.
18. Birkmeyer J, Finlayson E, Birkmeyer C. Volume standards for high-risksurgical procedures: potential benefits of the Leapfrog initiative. Sur-gery. 2001;130:415–422.
19. The Leapfrog Group homepage. www.leapfroggroup.org. Accessed onSeptember 1, 2006.
20. Nationwide Inpatient Sample overview. Available at: http://www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed on September 1, 2006.
21. U.S. Department of Health and Human Services. International Classi-fication of Diseases, 9th revision, clinical modification. Washington,DC: U.S. Government Printing Office, 1998.
22. Elixhauser A, Steiner C, Harris DR, et al. Comorbidity measures for usewith administrative data. Med Care. 1998;36:3–5.
23. Cooperman A, Herter F, Marboe C, et al. Pancreatoduodenal resectionand total pancreatectomy. Surgery. 1981;90:707–712.
24. Iezzoni L, Foley SM, Daley J, et al. Comorbidities, complications, andcoding bias: does the number of diagnosis codes matter in predictingin-hospital mortality? JAMA. 1992;267:2197–2203.
25. Jencks SF, Williams DK, Kay TL. Assessing hospital-associated deathsfrom discharge data: the role of length of stay and comorbidities. JAMA.1988;260:2240–2246.
26. Porter GA, Pisters PW, Mansyur C, et al. Cost and utilization impact ofa clinical pathway for patients undergoing pancreaticoduodenectomy.Ann Surg Oncol. 2000;7:484–489.
27. Tseng JF, Lee JE, Pisters PW, et al. The learning curve in pancreaticsurgery. Surgery. In press.
28. Fong Y, Gonen M, Rubin D, et al. Long-term survival is superior afterresection for cancer in high-volume centers. Ann Surg. 2005;242:540–547.
29. Warshaw AL, Fernandez-del Castillo C. Pancreatic carcinoma. N EnglJ Med. 1992;326:455–465.
30. Cameron JL, Riall TS, Coleman J, et al. One thousand consecutivepancreaticoduodenectomies. Ann Surg. 2006;244:10–15.
Annals of Surgery • Volume 246, Number 2, August 2007 Perioperative Mortality After Pancreatectomy
© 2007 Lippincott Williams & Wilkins 253

ORIGINAL ARTICLES
Clinical Implications of Peritoneal Cytology in PotentiallyResectable Pancreatic Cancer
Positive Peritoneal Cytology May Not Confer an Adverse Prognosis
Suguru Yamada, MD,* Shin Takeda, MD, PhD,* Tsutomu Fujii, MD, PhD,*Shuji Nomoto, MD, PhD,* Naohito Kanazumi, MD, PhD,* Hiroyuki Sugimoto, MD, PhD,*Hideki Kasuya, MD, PhD,* Yasuhiro Kodera, MD, PhD,* Tetsuro Nagasaka, MD, PhD,†
Satoshi Morita, PhD,‡ and Akimasa Nakao, MD, PhD*
Objectives: To determine the value of peritoneal washing cytology(CY) in determining resectability of pancreatic cancer.Summary Background Data: CY has been used widely in thediagnosis and staging of several cancers. However, its predictivevalue in identifying potentially resectable pancreatic cancer is un-determined.Methods: Peritoneal washing samples were collected from 233patients with pancreatic cancer between June 1991 and August 2006.A total of 157 patients had resectable and 76 had unresectablelesions. Correlations between CY status and clinicopathologic pa-rameters with overall survival rates were analyzed.Results: Malignant cells were identified in samples from 21 patients(13.4%) with resectable tumors and 27 patients (35.5%) with unre-sectable tumors. CY� was more frequent in large tumors (�2 cm)than small tumors (�2 cm; P � 0.034). CY status did not correlatewith any other clinicopathologic parameter. The overall survival ofCY� patients was worse than that of CY� patients (P � 0.047).Median survival following resection was 13.6 months for CY�patients and 13.5 months for CY� patients. Among the patients whohad unresectable lesions, median survival time was 5.9 months forCY� and 6.1 months for CY� patients. However, among CY�patients, those who underwent resection lived longer than those whodid not (P � 0.019).Conclusions: Cytologic status has little predictive value for sur-vival, and patients whose pancreatic cancer would otherwise beconsidered resectable should not be denied curative resection solelybecause they are CY�.
(Ann Surg 2007;246: 254–258)
Pancreatic cancer continues to be the gastrointestinal ma-lignancy with the worst prognosis, and only 3% of pa-
tients survive 5 years after diagnosis. Surgical resectionoffers the only chance for cure; and although the resectionrate has increased gradually, the prognosis remains poor.1
Peritoneal washing cytology (CY) has been used widelyin the diagnosis and staging of ovarian, endometrial, andgastric cancer. Malignant cells can be identified in 7% to 30%of peritoneal washing samples from patients with pancreaticcancer.2–9 However, the clinical significance of their presenceis yet to be determined. Prior studies have suggested thatpositive peritoneal cytology (CY�) may be a marker foradvanced disease, predictive of early metastasis and short-ened survival, and thus should be considered a contraindica-tion for attempts at curative resection.4,5 On the other hand,several authors have found no correlation between CY� andthe development of peritoneal metastasis postoperatively.Consequently, these investigators claim that CY� status inthe absence of macroscopic peritoneal metastasis is not acontraindication for radical surgery.7–9
In the current study, we examined peritoneal washingsfrom 233 patients with pancreatic cancer. The purpose was todetermine what, if any, whether relationship exists betweencytology results and clinicopathologic parameters and peri-toneal washing cytology correlates with survival.
PATIENTS AND METHODS
Patients Selection and Study DesignPeritoneal washing samples were collected from 233
pancreatic cancer patients treated at the Department of Sur-gery II, Nagoya University, between June 1991 and August2006. All 233 patients were considered candidates for cura-tive resection after a meticulous preoperative work-up. Thecohort included 156 men and 77 women, with the median ageof 61.9 years (range, 32–84 years). All patients were fol-lowed until death or through August 2006. The patients werefollowed for mean of 18.3 months or until death. Extendedradical resection (D2) was performed for all cases in theabsence of macroscopic liver or peritoneal metastases. A totalof 157 patients had resectable lesions, while the other 76
From the Departments of *Surgery II, †Laboratory Medicine, and ‡Healthand Community Medicine Program, Graduate School and Faculty ofMedicine, University of Nagoya, Nagoya, Japan.
Reprints: Suguru Yamada, MD, Department of Surgery II, Graduate School andFaculty of Medicine, University of Nagoya. 65 Tsurumai-cho, Showa-ku,Nagoya 466-8550, Japan. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0254DOI: 10.1097/01.sla.0000261596.43439.92
Annals of Surgery • Volume 246, Number 2, August 2007254

patients had macroscopic hepatic metastases, macroscopicperitoneal metastases, or extensive local invasion. Immedi-ately after laparotomy, 200 mL of isotonic heparinized salinewas introduced into the subhepatic space and the pouch ofDouglas. After gentle agitation, as much fluid was collectedas possible using a syringe and quill. Smears were made fromthe centrifuged deposit and, after conventional Papanicolaouand Giemsa staining, examined by at least 2 experiencedpathologists.7 All surgical specimens were examined his-topathologically after being fixed and stained with hematox-ylin and eosin. Pathologic findings were evaluated in accor-dance with the second English edition of the Classification ofPancreatic Carcinoma proposed by the Japan Pancreas So-ciety,10: pT1, tumor limited to the pancreas (�2 cm in thegreatest dimension); pT2, tumor limited to the pancreas (�2cm in the greatest dimension); pT3, tumor extending directlyinto the bile duct, duodenum, or peripancreatic tissues; andpT4, tumor extending directly into the adjacent large vessels,plexus, stomach, colon, or spleen. This classification schemeis more detailed than the classification of the Union Interna-tionale Contre le Cancer.11 The tumor location and extensionwere classified according to the 6th edition of the UICCclassification.
Statistical AnalysisThe significance of correlations between cytologic re-
sults and clinicopathologic parameters were determined usingFisher exact test or the �2 test. Overall survival rates werecalculated using the Kaplan-Meier method, and the differencein survival curves was analyzed using the log-rank test.Independent prognostic factors were identified by multivari-ate analysis using the Cox proportional hazards regressionmodel. Data are expressed as mean � SD. The level ofstatistical significance was set at P � 0.05.
RESULTSOf the 233 patients, 76 had unresectable lesions due to
the presence of macroscopic hepatic metastasis (n � 38),macroscopic peritoneal metastasis (n � 21), both macro-scopic hepatic and peritoneal metastases (n � 5), or extensivelocal invasion (n � 22). The remaining 157 patients under-went pancreatoduodenectomy (n � 81), pylorus-preservingpancreatoduodenectomy (n � 29), distal pancreatectomy(n � 30), and total pancreatectomy (n � 17). The conclusivestages of the 157 patients who underwent resection accord-ing to the TNM classification11 were IA in 2 cases, IB in4 cases, IIA in 31 cases, IIB in 72 cases, III in 15 cases,and IV in 33 cases.
Malignant cells were more often present in the perito-neal washings from patients with unresectable lesions (27cases, 35.5%) than those with resectable disease (21 cases,13.4%; Table 1) (P � 0.0002). Among the 21 patients whohad unresectable lesions due to the presence of macroscopicperitoneal metastasis, 15 (71.4%) were CY�.
Patients with large tumors (�2 cm) were more likely tobe CY� than those with small tumors (�2 cm; P � 0.034).However, no other correlation between cytologic status andclinicopathologic parameter existed (invasion of the anteriorpancreatic capsule or retroperitoneal tissue, bile duct inva-
sion, duodenal invasion, portal vein invasion, arterial inva-sion, perineural invasion, lymph node metastasis, lymphvessel invasion, vascular invasion, local tumor spread, loca-tion, or residual disease status) (Table 2). Of 157 resectablecases, cancer of 6 cases involved the whole pancreas andthose of 32 cases occupied the body. Prognosis of thesepatients were poor compared with lesions localized to thepancreatic head, but no correlation between the CY status andtumor location was found at this time, partially owing to therarity of CY� cases among lesions located in the pancreaticbody. Median survival time of R0 patients (14.5 months) waslonger than that of R1 patients (9.2 months, P � 0.015) evenwhen the CY status was not reflected in the R classification.In addition, no correlation was found between the CY statusand the extent of residual disease. Among patients who hadunresectable lesions, patients with macroscopic peritonealmetastases had a higher incidence of CY� than those withoutmacroscopic peritoneal metastases (P � 0.0001). On theother hand, CY status did not correlate with the presence orabsence of hepatic metastases.
The overall survival of CY� patients was shorter thanof CY� patients (P � 0.047; Fig. 1). For patients whounderwent resection, however, the median survival time ofCY� patients (13.6 months) was almost identical to that ofCY� patients (13.5 months, P � 0.269; Fig. 2). This unex-pected lack of a difference in survival was seen amongpatients with unresectable lesions as well (5.9 months forCY� and 6.1 months for CY�, P � 0.977; Fig. 2). Further-more, no difference in survival according to CY� status wasobserved among patients with stages III and IV disease.There was a marked difference in survival between CY�patients who underwent resection and those who did not (P �0.019; Fig. 2).
To evaluate the value of peritoneal washing cytology asan independent prognostic determinant, multivariate analysiswas performed with prognostic factors that had been found to
TABLE 1. Demographics and Clinical Characteristics ofPatients With Resectable Pancreatic Cancer and PositivePeritoneal Washings
Characteristic Value
Age (yr) �range (mean)� 40–76 (62.5)
Gender (M/F) 9/12
Histopathologic type
Moderate 15
Well 1
Poor 3
Papillary 1
Adenosquamous 1
Stage
IA 0
IB 1
IIA 3
IIB 9
III 0
IV 8
Survival time (mos) �range (mean)� 1.4–41.6 (13.6)
Annals of Surgery • Volume 246, Number 2, August 2007 Peritoneal Cytology in Pancreatic Cancer
© 2007 Lippincott Williams & Wilkins 255

be significant by the univariate analyses. The analysis iden-tified lymph node metastasis as the only variable for inde-pendently predicting overall survival (P � 0.0004; Table 3),whereas CY was found not to be significant.
DISCUSSIONExfoliation of free malignant cells is a well-described
feature of human carcinomas. Malignant transformation ofcells alters the expression of surface adhesion molecules andthus facilitates their release into the peritoneal cavity.12 Mi-croscopic occult peritoneal metastases are thought to precedethe emergence of macroscopic peritoneal metastases.13,14 Ingynecologic malignancies, presence of malignant cells in
FIGURE 1. Comparison of survival curves of patients withpancreatic cancer with (CY�) and without (CY�) tumor cellsin peritoneal washings. The overall survival for CY� patientswas significantly worse than for CY� patients (P � 0.047).
FIGURE 2. Comparison of survival curves of patients withpancreatic cancer who underwent curative resection with(CY�) and without (CY�) tumor cells in cytologic washings.The median survival time of CY� patients was 13.6 monthsand that of CY� patients was 13.5 months (P � 0.269).Comparison of survival curves of patients with pancreaticcancer who did not undergo curative resection with (CY�)and without (CY�) tumor cells in peritoneal washings. Themedian survival time of CY� patients was 5.9 months andthat of CY� patients was 6.1 months (P � 0.977). Amongpancreatic cancer patients with positive peritoneal cytology,patients with resectable lesions lived longer than patientswith nonresectable lesions (P � 0.019).
TABLE 2. Demographics and Clinical Characteristics ofPatients With Pancreatic Cancer Subjected to CytologicExamination of Peritoneal Washings
Clinicopathologic Parameter No. Cases CY� CY� P
Tumor size
�2 cm 24 24 0 0.034*
�2 cm 130 109 21
Invasion of anterior pancreaticcapsule
Neg. 76 68 8 0.355
Pos. 81 68 13
Invasion of retroperitonealtissue
Neg. 58 52 6 0.472
Pos. 99 84 15
Bile duct invasion
Neg. 67 62 5 0.095
Pos. 90 74 16
Duodenal invasion
Neg. 93 83 10 0.340
Pos. 64 53 11
Portal vein invasion
Neg. 75 69 6 0.065
Pos. 82 67 15
Arterial invasion
Neg. 138 117 21 0.068
Pos. 19 19 0
Perineural invasion
Neg. 117 100 17 0.596
Pos. 40 36 4
Lymph node metastasis
Neg. 44 40 4 0.437
Pos. 113 96 17
Lymph vessel invasion
Neg. 24 23 1 0.269
Pos. 127 108 19
Vascular invasion
Neg. 86 76 10 0.629
Pos. 65 55 10
Local tumor spread
pT1 3 3 0 0.267
pT2 7 5 2
pT3 53 49 4
pT4 94 79 15
Location
Head 119 102 17 0.7471
Body 32 29 3
Whole 6 5 1
Residual disease status
R0 114 98 16 0.798
R1 43 38 5
R2 0 0 0
Yamada et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins256

peritoneal washings has been proven to have a strong nega-tive impact on prognosis and therefore has been incorporatedinto the staging systems of these malignancies.15 Similarly,peritoneal washing cytology has been used extensively ingastric cancer,16–18 and the results are reflected in the Japa-nese clinical staging scheme.19 However, the significance andprognostic value of peritoneal washing cytology have yet tobe established in other gastrointestinal malignancies, includ-ing pancreatic cancer.20
Several recent studies have reported that patients withpancreatic cancer who are CY� are more likely to haveadvanced stage disease, early metastasis, and a poor progno-sis.2–9 In some series, overall survival of CY� patients wasshorter than that of CY� patients.2,5,9 CY� status has notbeen reported to be an independent prognostic variable ofsurvival because it seems to be dependent on tumor stage.5
Some investigators have concluded that tumor cells in theperitoneal washings are precursors of macroscopic dissemi-nation, and have recommended that CY� patients not un-dergo resection even if they would otherwise be surgicalcandidates.21 However, we have previously found no corre-lation between CY status and the incidence of peritonealcarcinomatosis during follow-up and concluded that CY� inthe absence of gross peritoneal deposits does not represent anabsolute contraindication to radical surgery.7 In addition,Meszoely et al9 reported that overall survival and disease-freesurvival are not affected by the presence of tumor cells inperitoneal washings of patients who underwent curative re-section. These results suggest that not all cells shed by apancreatic cancer develop into peritoneal metastases.
While maintaining that surgery cannot in theory berecommended for CY� patients, Yachida et al8 acknowl-edged that it may be premature to state this categoricallygiven the paucity of outcome data. To the authors’ knowl-edge, the analysis in the current study is based on the largestdata set in the literature (Table 4). Consequently, these resultsshould be weighted more heavily than those from smallerstudies.
Although the overall survival for CY� patients wasworse than for CY� patients, CY status did not predictsurvival within the group of patients who underwent resection
or in the group who did not. Resectability was a muchstronger determinant of outcome, and long-term survival inCY� patients has been documented in this study and oth-ers.5,7 Thus, it should be considered an independent prognos-tic factor, and patients whose pancreatic cancer is resectableshould not be denied based on CY status alone.
It is unclear why free cancer cells in the abdominalcavity do not have an impact on survival. It may be due inpart to differences in the biology of different histologic types.In gastric cancer, patients with undifferentiated adenocarci-noma have a higher rate of CY� than those with differenti-ated adenocarcinoma,22 whereas most patients with CY� inthe current study had a moderately differentiated phenotype.However, no correlation existed between CY status and thehistopathologic type of pancreatic cancer. Even in gastriccancer, a certain amount of time is needed for isolatedtumor cells to develop into peritoneal carcinomatosis.Thus, some CY� patients may die due to other patterns ofmetastatic spread before signs of peritoneal metastasis candevelop. This may be the case with at least some CY�patients since a high proportion of patients with this cancerdie of liver metastasis.
Of the 21 patients with macroscopic peritoneal depos-its, only 15 patients (71.4%) were CY�, indicating thatsensitivity of the examination is a matter of concern. Varioustechniques such as immunocytochemistry7,23 or reverse-tran-scriptase polymerase chain reaction24 have been used toimprove sensitivity. The authors have previously shown thatimmunocytochemical staining is more sensitive than conven-tional staining,7 and reverse-transcriptase polymerase chainreaction appears to be even more sensitive in gastric cancer.24
Further study is needed to determine the best method fordetecting pancreatic cancer cells in peritoneal washings.However, whether an improvement in sensitivity will in-crease value of this examination as a prognostic determinantremains unknown.
TABLE 3. Multivariate Analysis of Patients With ResectablePancreatic Cancer
Variable Odds Ratio 95% CI P
Tumor size (�2.0 cm) 1.714 0.915–3.208 0.092
Invasion of anteriorpancreatic capsule
1.172 0.757–1.813 0.478
Invasion ofretroperitoneal tissue
1.288 0.827–2.005 0.263
Portal vein invasion 1.371 0.860–2.184 0.184
Perineural invasion 1.481 0.930–2.358 0.098
Lymph node metastasis 2.322 1.456–3.703 0.0004*
Vascular invasion 1.075 0.712–1.623 0.732
CY� 1.061 0.589–1.912 0.843
*Statistically significant.CY� indicates positive peritoneal washing cytology.
TABLE 4. Published Studies on Peritoneal WashingCytology in Pancreatic Cancer
Series Year n
CY�
n (%)Resected
Cases
Martin and Goellner22 1986 20 5 (25) 0
Warshaw2 1991 40 12 (30) 1
Lei et al 1994 36 3 (8) 0
Leach et al4 1995 60 4 (7) 1
Fernandez del Castilloet al3
1995 94 16 (17) 0
Merchant et al5 1999 228 34 (15) 2
Nakao et al1 1999 74 21 (28) 13
Jimenez et al6 2000 117 24 (21) 0
Yachida et al8 2002 134 19 (14) 19
Meszoely et al9 2004 168 27 (16) 13
Current study 2006 233 48 (21) 21
CY� indicates positive peritoneal washing cytology.
Annals of Surgery • Volume 246, Number 2, August 2007 Peritoneal Cytology in Pancreatic Cancer
© 2007 Lippincott Williams & Wilkins 257

CONCLUSIONPresence of free cancer cells in the peritoneal cavity is
not clinically equivalent to the presence of macroscopicmetastases. Since surgical resection remains the only modal-ity that offers a chance for long-term survival, curativeresection may be indicated regardless of the CY status when-ever pancreatic cancer is localized, macroscopically resect-able, and without gross distant metastasis.
REFERENCES1. Nakao A, Fujii T, Sugimoto H, et al. Oncological problems in pancreatic
cancer surgery. World J Gastroenterol. 2006;12:4466–4472.2. Warshaw AL. Implication of peritoneal cytology for staging in early
pancreatic cancer. Am J Surg. 1991;161:26–30.3. Fernandez-del Castillo C, Rattner DW, Warshaw AL. Further experience
with laparoscopy and peritoneal cytology in the staging of pancreaticcancer. Br J Surg. 1995;82:11127–11129.
4. Leach SD, Rose JA, Lowy AM, et al. Significance of peritoneal cytologyin patients with potentially resectable adenocarcinoma of the pancreatichead. Surgery. 1995;82:472–478.
5. Merchant NB, Conlon KC, Saigo P, et al. Positive peritoneal cytologypredicts unresectability of pancreatic adenocarcinoma. J Am Coll Surg.1999;188:421–426.
6. Jimenez RE, Warshaw AL, Fernandez-del Castillo C. Laparoscopy andperitoneal cytology in the staging of pancreatic cancer. J HepatobiliaryPancreat Surg. 2000;7:15–20.
7. Nakao A, Oshima K, Takeda S, et al. Peritoneal washings cytologycombined with immunocytochemical staging in pancreatic cancer.Hepatogastroenterology. 1999;46:2974–2977.
8. Yachida S, Fukushima N, Sakamoto M, et al. Implications of peritonealwashing cytology in patients with potentially resectable pancreaticcancer. Br J Surg. 2002;89:573–578.
9. Meszoely IM, Lee JS, Watson JC, et al. Peritoneal cytology in patientswith potentially resectable adenocarcinoma of the pancreas. Am Surg.2004;70:208–214.
10. Japan Pancreatic Society. Classification of Pancreatic Carcinoma, 2ndEnglish ed. Tokyo: Kanehara, 2003.
11. Sobin LH, Wittekind CH. TNM Classification of Malignant Tumours,6th ed. New York: Wiley-Liss, 2002.
12. Yang AD, Camp ER, Fan F, et al. Vascular endothelial growth factorreceptor-I activation mediates epithelial to mesenchymal transition inhuman pancreatic carcinoma cells. Cancer Res. 2006;66:46–51.
13. Bernstein LR, Liotta LA. Molecular mediators of interactions withextracellular matrix components in metastasis and angiogenesis. CurrOpin Oncol. 1994;6:106–113.
14. Wu CC, Chen JT, Chang MC, et al. Optimal surgical strategy forpotentially curable serosa-involved gastric carcinoma with intraperito-neal free cancer cells. J Am Coll Surg. 1997;184:611–617.
15. Grimshaw RN, Tupper WC, Fraser RC, et al. Prognostic value ofperitoneal cytology in endometrial carcinoma. Gynecol Oncol. 1990;36:97–100.
16. Boku T, Nakane Y, Minoura T, et al. Prognostic significance of serosalinvasion and free intraperitoneal cancer cells in gastric cancer. Br J Surg.1990;77:436–439.
17. Bonenkamp JJ, Songun I, Hermans J, et al. Prognostic value of positivecytology findings from abdominal washings in patients with gastriccancer. Br J Surg. 1996;83:672–674.
18. Kodera Y, Yamamura Y, Shimizu Y, et al. Peritoneal washing cytology:prognostic value of positive findings in patients with gastric carcinomaundergoing a potentially curative resection. J Surg Oncol. 2001;78:175–181.
19. Japanese Gastric Cancer Association. Japanese Classification of GastricCarcinoma-2nd English edition. Gastric Cancer 1998;1:10–24.
20. Kienle P, Koch M. Are micrometastases of the peritoneum equivalent todistant metastases? Dig Surg. 2002;19:453–458.
21. Makary MA, Warshaw AL, Centeno BA, et al. Implications of perito-neal cytology for pancreatic cancer management. Arch Surg. 1998;133:361–365.
22. Bando E, Yonemura Y, Takeshita Y, et al. Intraoperative lavage forcytological examination in 1,297 patients with gastric carcinoma.Am J Surg. 1999;178:256–262.
23. Benevolo M, Mottolese M, Cosimelli M, et al. Diagnostic and prognos-tic value of peritoneal immunocytology in gastric cancer. J Clin Oncol.1998;16:3406–3411.
24. Kodera Y, Nakanishi H, Ito S, et al. Quantitative detection of dissemi-nated free cancer cells in peritoneal washes with real-time reversetranscriptase-polymerase chain reaction. Ann Surg. 2002;235:499–506.
Yamada et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins258

ORIGINAL ARTICLES
Type I Interferons in the Treatment of Pancreatic CancerMechanisms of Action and Role of Related Receptors
Giovanni Vitale, MD,* Casper H. J. van Eijck, MD, PhD,† Peter M. van Koetsveld Ing,*Joris I. Erdmann, MD,*† Ernst Jan M. Speel, PhD,‡ Katy van der Wansem Ing,* Diana M. Mooij,*
Annamaria Colao, MD, PhD,§ Gaetano Lombardi, MD,§ Ed Croze, PhD,�Steven W. J. Lamberts, MD, PhD,* and Leo J. Hofland, PhD*
Objective: We evaluated the role of type I interferons (IFNs) andIFN receptors in the regulation of cell growth in 3 human pancreaticadenocarcinoma cell lines (BxPC-3, MiaPaCa-2, and Panc-1).Background: Chemotherapy and radiotherapy have a marginal rolein the management of pancreatic adenocarcinoma. The addition ofIFN-� showed promising results in early clinical trials.Methods: Cell proliferation and apoptosis were evaluated by DNAmeasurement and DNA fragmentation, respectively. Type I IFNreceptor (IFNAR-1 and IFNAR-2 subunits) was determined byquantitative RT-PCR and immunocytochemistry. Cell cycle dis-tribution was evaluated by propidium iodide staining and flow-cytometric analysis.Results: The incubation with IFN-� for 6 days showed a potentinhibitory effect on the proliferation of BxPC-3 (IC50, 14 IU/mL)and MiaPaCa-2 (IC50, 64 IU/mL). The inhibitory effect of IFN-�was stronger than IFN-� in all 3 cell lines and mainly modulated bythe stimulation of apoptosis, although cell cycle arrest was inducedas well. The expression of the type I IFN receptors was significantlyhigher in BxPC-3 (the most sensitive cell line to IFN) and mainlylocalized on the membrane, whereas in Panc-1 (the most resistantcell line) about 60% to 70% of cells were negative for IFNAR-2cwith a mainly cytoplasmic staining for IFNAR-2c.Conclusion: The antitumor activity of IFN-� is more potent thanIFN-� in pancreatic cancer cell lines through the induction ofapoptosis. Further studies should investigate in vivo whether theintensity and distribution of IFNAR-1 and IFNAR-2c may predictthe response to therapy with IFN-� and IFN-� in pancreatic cancer.
(Ann Surg 2007;246: 259–268)
Pancreatic adenocarcinoma is a highly aggressive malig-nancy.1 Surgery is the only curative therapy. Unfortu-
nately, only 5% to 15% of patients are surgical candidates atthe time of the diagnosis due to a lack of specific symptoms,limitations in diagnostic methods, and the biologically ag-gressive nature of this tumor.1 In this selected group ofpatients, adjuvant chemotherapy has a survival benefit but the5-year survival of 21%, as described by the European StudyGroup for Pancreatic Cancer, remains poor.2 The role ofchemoradiotherapy in the management of pancreatic adeno-carcinoma is unclear.3 However, it has been recently de-scribed4 that interferon (IFN)-� in combination with adjuvantchemoradiotherapy improved 5-year survival to 55%.
In vitro and in vivo studies have demonstrated theefficacy of type I IFNs (eg, IFN-�, IFN-�, IFN-�, IFN-�, andIFN-�), in the treatment of several tumors.5–9 Although theantitumor effects of IFN-� have been studied in detail, thoseof IFN-� are not well clarified. IFN-� is a multifunctionalcytokine that binds the same receptor of IFN-�, but withhigher affinity.10 It seems to be an essential mediator not onlyfor the innate immune responses against microbial infections,but also for a host defense system against oncogenesis.6,11
Moreover, several studies showed that IFN-� has greaterantitumor effects than IFN-�.10,12–16 On the basis of theseobservations, IFN-� represents a promising drug in the treat-ment of cancer.
Importantly, several chromosomal aberrations have beendetected in pancreatic adenocarcinoma, including a frequentloss of chromosome arm 9p, observed in more than 80% ofhuman pancreatic cancer.17 Together with the tumor-suppres-sor genes p16INK4a, p15INK4b, and p14ARF also the IFN-�and IFN-� genes are located on chromosome 9p.18 Therefore,in relation to the defensive role of IFNs against tumors,11 theabsence of the expression of IFNs may have an important rolein the pathogenesis and probably in the treatment of pancre-atic adenocarcinoma.
To further explore the possibilities of new medicaltreatments in pancreatic cancer, we evaluated in the presentstudy the antitumor activity of IFN-� and IFN-� in 3 humanpancreatic adenocarcinoma cell lines (BxPC-3, MiaPaCa-2,and Panc-1), as well as the role of IFN receptors in theresponsiveness to type I IFNs.
From the Departments of *Internal Medicine and †Surgery, Erasmus MC,Rotterdam, The Netherlands; ‡Department of Molecular Cell Biology,Research Institute Growth and Development, University of Maastricht,Maastricht, The Netherlands; §Department of Molecular & ClinicalEndocrinology and Oncology, “Federico II” University of Naples, Na-ples, Italy; and �Department of Immunology, Berlex Bioscience Inc.,Richmond, CA.
Supported by study grants from the Yamagiwa-Yoshida Memorial UICCInternational Cancer.
Reprints: Casper H. J. van Eijck, MD, PhD, Department of Surgery, ErasmusMedical Center, Room H 911, Dr. Molewaterplein 50, 3015 GE Rotter-dam, The Netherlands. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0259DOI: 10.1097/01.sla.0000261460.07110.f2
Annals of Surgery • Volume 246, Number 2, August 2007 259

METHODS
Cell Lines and Culture ConditionsThe human pancreatic cell lines, BxPC-3, MiaPaCa-2,
and Panc-1 were purchased from the American Type CultureCollection. The cells were cultured in a humidified incubatorcontaining 5% CO2 at 37°C. The culture medium consisted ofRPMI 1640 supplemented with 10% FCS, penicillin (1 � 105
U/L) and L-glutamine (2 mmol/l). Periodically, the cells wereconfirmed as Mycoplasma-free. Cells were harvested withtrypsin (0.05%), EDTA (0.02%), and resuspended in me-dium. Before plating, the cells were counted microscopicallyusing a standard hemocytometer. Trypan Blue staining wasused to assess cell viability and always exceeded 95%. Mediaand supplements were obtained from GIBCO Bio-cult Europe(Invitrogen, Breda, The Netherlands).
Drugs and ReagentsHuman recombinant IFN-�-2b (Intron-A) was obtained
from Schering-Plough Corporation (Utrecht, The Nether-lands), while human recombinant IFN-�-1a was acquiredfrom Serono Inc. (Rebif, Rockland, MA). All compoundswere stored at �20°C, and the stock solution was constitutedin distilled water according to the manufacturer instructions.
Cell Proliferation AssayAfter trypsinization the cells were plated in 1 mL of
medium in 48-well plates at a density of 5 � 103 to 4 � 104
cells/well, depending on the length of the incubation period.The plates were then placed in a 37°C, 5% CO2 incubatorovernight. The next day the cell culture medium wasreplaced with 1 mL/well medium containing increasingconcentrations (0–10,000 IU/mL) of IFN-� or IFN-�. Eachtreatment was performed in quadruplicate. After 1, 3, and 6days of treatment, the cells were harvested for DNA mea-surement, at an approximately 70% to 80% confluence. For6-day experiments, the medium was refreshed after 3 daysand compounds were added again. Measurement of totalDNA contents, representative for the number of cells, wasperformed using the bisbenzimide fluorescent dye (Hoechst33258) (Boehring Diagnostics, La Jolla, CA), as previouslydescribed.19
Measurement of DNA Fragmentation(Apoptosis)
Cells (104 to 4 � 104)/well, depending on the lengthof the incubation period, were plated on a 48-well plateand the cells were allowed to adhere overnight. The nextday, the cell culture medium was replaced with 1 mL/wellmedium containing increasing concentrations (0 –10,000IU/mL) of IFN-� or IFN-�. Each treatment was performedin quadruplicate. After an additional incubation of 1 and 3days, apoptosis was assessed using a commercially avail-able ELISA kit (Cell Death Detection ELISAPlus, RocheDiagnostic GmbH, Penzberg, Germany). The standard pro-tocol supplied by the manufacturer was used, as previouslydescribed.20 Relative apoptosis was determined by calcu-lating the ratio of the average absorbance of the treatmentwells to the average absorbance of the control wells. The
data were corrected for the effect on cell number after 1and 3 days of treatment.
Cell Cycle AnalysisCells (1 to 4 � 106) depending on the length of the
incubation period, were plated in 75-cm2 culture flasks (Corn-ing Costar, Amsterdam, The Netherlands). After 1 day me-dium was changed with fresh medium (control group) andwith fresh medium plus IFN-� or IFN-� at the concentrationof 1000 IU/mL. Each treatment was performed in duplicate.After 1, 2, and 3 days of incubation, the cells were harvestedby gentle trypsinization and prepared for cell cycle determi-nation using propidium iodide for DNA staining, as previ-ously described.16 The stained cells were analyzed by FACS-calibur flow cytometer (Becton Dickinson, Erembodegem,Belgium) and CellQuest Pro Software. Cell cycle progressionwas measured with corresponding absorbances for G0/G1, Sand G2-M phases, whereas apoptosis was measured by quan-tifying the sub-G0 peak.
Quantitative RT-PCRThe expression of type I IFN receptors (IFNAR-1,
IFNAR-2 total, the short form IFNAR-2b, and the long formIFNAR-2c) and housekeeping gene hypoxanthine-phosphori-bosyl-transferase (HPRT) mRNA was evaluated by quantita-tive RT-PCR in all 3 pancreatic cancer cell lines, as previ-ously described.16 Briefly, poly A� mRNA was isolatedusing Dynabeads Oligo (dT)25 (Dynal AS, Oslo, Norway)from cell pellets containing approximately 5 � 105 cells.Complementary DNA (cDNA) was synthesized using thepoly A� mRNA in a Tris-buffer together with 1 mmol/L ofeach deoxynucleotide triphosphate, 10 U RNAse inhibitor,and 2 U AMV Super Reverse Transcriptase (HT Biotechnol-ogy Ltd., Cambridge, UK) in a final volume of 40 �L. Thismixture was incubated for 1 hour at 42°C. One fifth of thecDNA library was used for quantification of IFN receptorsand HPRT mRNA levels.
A quantitative PCR was performed by AmpliTaq GoldDNA Polymerase and the ABI PRISM 7700 sequence detec-tion system (Perkin-Elmer Applied Biosystems, Groningen,The Netherlands) for real-time amplifications, according tothe manufacturer’s protocol. Each sample was assayed induplicate. The assay was performed using 15 �L TaqManUniversal PCR Master Mix (Applied Biosystems, Capelleaan de Ijssel, The Netherlands), forward primer, reverseprimer, probe, and 10 �L cDNA template, in a total reactionvolume of 25 �L. PCR amplification started with a first stepfor 2 minutes at 50°C, followed by an initial heating at 95°Cfor 10 minutes, samples were subjected to 40 cycles ofdenaturation at 95°C for 15 seconds and annealing for 1minute at 60°C.
The primer and probe sequences that were used forthe detection of IFNAR-1, IFNAR-2 total, IFNAR-2b,IFNAR-2c, and HPRT have been previously described.16
All the primer and probe sequences were purchased fromBiosource (Nivelles, Belgium).
The detection of HPRT mRNA was used for normal-ization of IFN receptor mRNA levels. Expression ofIFNAR-2a mRNA, the soluble form of IFNAR-2 subunit,
Vitale et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins260

was determined indirectly by subtracting IFNAR-2b andIFNAR-2c from IFNAR-2 total. To exclude contaminationof the PCR reaction mixtures, the reactions were per-formed in the absence of DNA template in parallel withcDNA samples. As a positive control for the PCR reactionsof HPRT and type I IFN receptors human cDNA wasamplified in parallel with the cDNA samples.
ImmunocytochemistryCytospin preparations of BxPC-3, MiaPaCa-2, and
Panc-1 cells were fixed with acetone for 10 minutes. Afterwashing 2 times with PBS, the cells were incubated for 30minutes at room temperature with antibodies to humanIFNAR-1 (rabbit polyclonal antibody, Santa Cruz Biotech-nology, Inc., Santa Cruz, CA) and IFNAR-2c (monoclonalantibody, Dr E. Croze, Berlex Biosciences, Richmond, CA)subunits, and for overnight with antibodies to IFNAR-2b(rabbit polyclonal antibody, Santa Cruz Biotechnology, Inc.).Finally, a peroxidase complex for IFNAR-1 and IFNAR-2b,or standard streptavidin-biotinylated alkaline phosphatase(both from IL Immunologic, Duiven, The Netherlands) forIFNAR-2c, were used according to the manufacturer’s rec-ommendations to visualize the bound antibodies.
Negative controls for the immunohistochemistry in-cluded: 1) omission of the primary antibody; and 2) preab-sorption of the antibody for IFNAR-2b with the respectiveimmunizing receptor peptide.
Statistical AnalysesAll experiments were carried out at least 3 times and
gave comparable results. For statistical analysis GraphPadPrism 3.0 (GraphPad Software, San Diego, CA) was used.Fifty percent growth-inhibitory concentrations (IC50) andmaximal inhibitory effects were calculated using nonlinearregression curve-fitting program. The comparative statisticalevaluation among groups was first performed by the ANOVAtest. When significant differences were found, a comparisonbetween groups was made using the Newman-Keuls test. Theunpaired Student t test was used to analyze the differences inconcentration-effect curves (IC50 and maximal inhibitoryeffect) and effects in cell cycle modulation between differenttypes of IFNs, and the differences of the growth inhibitoryeffects of IFNs after 3 and 6 days of treatment. Correlationanalyses were performed using Pearson’s coefficients.
In all analyses, values of P � 0.05 were consideredstatistically significant. Data are reported as mean � SEM.Statistical analysis was made after logarithmic transformation.
RESULTS
Antiproliferative Effects of Type I IFNsAfter 6 days of incubation, IFN-� and IFN-� signifi-
cantly suppressed the growth of all 3 pancreatic cancer celllines in a dose-dependent manner (Fig. 1), with a mean IC50of 606 IU/mL and 14 IU/mL in BxPC-3, respectively; 1531IU/mL and 64 IU/mL in MiaPaCa-2, respectively; and 1250IU/mL and 112 IU/mL in Panc-1, respectively.
The growth-inhibitory effect of IFN-� was significantlymore potent than that of IFN-�, as shown by the higher
maximal inhibition of proliferation induced by IFN-� com-pared with IFN-� (96.7% � 2% and 72% � 5.7%, respec-tively, P � 0.0001 in BxPC-3; 87.5% � 3.2% and 69.1% �6.1%, respectively, P � 0.0001 in MiaPaCa-2; 70.7% �1.4% and 53% � 5.7%, respectively, P � 0.0001 in Panc-1)after 6 days of treatment, as well as by the lower logIC50 ofIFN-� compared with IFN-� (1.15 � 0.06 and 2.78 � 0.15,respectively, P � 0.00001 in BxPC-3; 1.8 � 0.07 and 3.18 �0.13, respectively, P � 0.00001 in MiaPaCa-2; 2.05 � 0.05and 3.1 � 0.17, respectively, P � 0.0001 in Panc-1). InBxPC-3 and MiaPaCa-2, IFN-� induced a statistically signif-icant cell growth inhibition already at very low concentra-tions (5–10 IU/mL).
In all 3 pancreatic cell lines, the effects of IFN-� andIFN-� were time-dependent. Indeed, the maximal inhibitionof cell proliferation, induced by both cytokines, was higherafter 6 days compared with 3 days of incubation (both P �0.0001 in BxPC-3; P � 0.005 and P � 0.0001, respectively,for IFN-� and IFN-� in MiaPaCa-2; both P � 0.0001 inPanc-1). In addition, there was no difference in IC50 valuesafter 3 and 6 days of incubation with IFN-� or IFN-� in the3 cell lines (data not shown).
The cell lines exhibited different sensitivities to the treat-ment, particularly with IFN-�. BxPC-3 resulted to be the mostsensitive and Panc-1 the most resistant. The maximal inhibitionof proliferation for IFN-� was higher in BxPC-3 compared withMiaPaCa-2 (P � 0.05) and Panc-1 (P � 0.001), while it waslower in Panc-1 compared with MiaPaCa-2 (P � 0.01). Simi-larly, the IC50 of IFN-� was significantly lower in BxPC-3 thanin MiaPaCa-2 and Panc-1 (both P � 0.001), and higher inPanc-1 compared with MiaPaCa-2 (P � 0.05). The maximalinhibition of proliferation for IFN-� was higher in BxPC-3compared with Panc-1 (P � 0.05), while no difference in IC50values of IFN-� was observed between the 3 cell lines.
Effects of Type I IFNs on ApoptosisA crucial step in apoptosis is DNA fragmentation, a
process that results from the activation of endonucleases,which degrade chromatin into smaller fragments. The mea-surement of DNA fragmentation was used to investigate theeffect of treatment with IFN-� and IFN-� on apoptosis (Figs.2 and 3).
After 1 day of incubation, IFN-� had no remarkablestimulatory effects on DNA fragmentation at any concentra-tion up to 1000 IU/mL in all 3 cell lines, only at the very highdose of 10,000 IU/mL IFN-� induced a significant increase inDNA fragmentation (Fig. 2A–C). On the other hand, a dose-dependent induction of apoptosis was observed after IFN-�treatment in BxPC-3 and MiaPaCa-2, with a maximal in-crease of DNA fragmentation of about 3.5 times comparedwith the untreated control (Fig. 2D, E). This effect wasalready statistically significant at very low concentrations(5–10 IU/mL). In Panc-1, a stimulating effect on apoptosiswas observed only for very high concentrations of IFN-�(�500 IU/mL) (Fig. 2F).
After 3 days of treatment with IFN-�, an increase inDNA fragmentation was detected in BxPC-3 and MiaPaCa-2at a moderate to high dose (Fig. 3A, B). Moreover, theinduction of apoptosis by IFN-� remained high, with a
Annals of Surgery • Volume 246, Number 2, August 2007 IFN-� Therapy in Pancreatic Cancer
© 2007 Lippincott Williams & Wilkins 261

maximal stimulation of about 4- and 10-fold, compared withthe control, respectively, in MiaPaCa-2 and BxPC-3 (Fig. 3D,E). In addition, after 3 days of incubation, the stimulatoryeffects on apoptosis persisted in Panc-1 only at high doses ofIFN-� (10,000 IU/mL, Fig. 3C) and IFN-� (�500 IU/mL,Fig. 3F).
These data were also confirmed by morphologic obser-vations. In all 3 cell lines, the treatment with IFN-� inducedclear structural alterations consistent with apoptosis, such ascell shrinkage, pyknotic nucleus, and detachment from theplate after 1 to 3 days, also at very low doses in BxPC-3 cellline (not shown). These morphologic changes were evidentonly at high doses of IFN-� treatment.
The inhibitory effects of IFN-� on the cell growth ofBxPC-3 and MiaPaCa-2 cell lines appeared to be mainly dueto an early pro-apoptotic activity, as shown by the highlysignificant positive correlation between cell proliferation in-hibition after 6 days of treatment and DNA fragmentationinduction after 1 day (r2 � 0.95, P � 0.0001, both forBxPC-3 and MiaPaCa-2) and 3 days of incubation (r2 � 0.95,P � 0.0001, for BxPC-3; r2 � 0.90, P � 0.0001, forMiaPaCa-2). At this early time point, apoptosis seems to benot involved in the antiproliferative effect of IFN-� onpancreatic cancer cells. Indeed, no significant correlation hasbeen observed between cell proliferation inhibition after 6
days and DNA fragmentation variation after 1 day of treat-ment with IFN-�. Only after 3 days of treatment with IFN-�,we observed a positive correlation between DNA fragmenta-tion variation and the 6 days cell proliferation inhibition (r2 �0.74, P � 0.0001, for BxPC-3; r2 � 0.71, P � 0.0001, forMiaPaCa-2).
Effects of Type I IFNs on the Cell CycleWe also evaluated the effect of treatment with IFN-�
(1000 IU/mL) and IFN-� (1000 IU/mL) on cell cycle phasedistribution after 1, 2, and 3 days of incubation in BxPC-3,MiaPaCa-2, and Panc-1 (Fig. 4A–I).
IFN-� treatment induced a significant accumulationin S phase compared with the control in all 3 cell lines anda decrease in the proportion of cells in G0/G1 phase inMiaPaCa-2 and Panc-1. In addition, the histograms of cellcycle revealed a late and slight increase in cells withsubdiploid DNA content (sub-G0 phase) only in BxPC-3and MiaPaCa-2, confirming the induction of apoptosis afterIFN-� treatment, as previously shown by the analysis ofDNA fragmentation. In a comparable manner, the incubationwith IFN-� increased the fraction of all 3 cell lines in the Sphase of the cell cycle, whereas the proportion of cells inG0/G1 phase decreased in comparison with the control. IFN-�
FIGURE 1. Effects of IFN-� (A–C) and IFN-� (D–F) treatment on cell proliferation, as measured by total DNA content, usingHoechst 33258. Pancreatic cancer cell lines were incubated for 6 days without (control) or with the drugs indicated at differ-ent concentrations. Values are expressed as the percentage of control (untreated cells) and represent the mean � SEM of atleast 3 independent experiments in quadruplicate. The mean DNA content in controls were: 2260 ng/well (IFN-�, BxPC-3),2430 ng/well (IFN-�, BxPC-3), 8562 ng/well (IFN-�, MiaPaCa-2), 8803 ng/well (IFN-�, MiaPaCa-2), 4224 ng/well (IFN-�,Panc-1), and 4172 ng/well (IFN-�, Panc-1). *P � 0.001; **P � 0.01; ***P � 0.05 versus control.
Vitale et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins262

induced a variable accumulation of cells in sub-G0 phase inall cell lines (BxPC-3 � MiaPaCa-2 � Panc-1).
These data suggest that pancreatic cancer cells in Sphase fail to transit into G2 and M phases efficiently andexhibit a prolonged stay in S phase after treatment with typeI IFNs.
The cell cycle arrest induced by IFN-� was more potentthan that of IFN-�, considering that the percentage of cells inS phase compared with the control was significantly higherafter 3 days of incubation with IFN-� than after IFN-�(BxPC-3: P � 0.05, MiaPaCa-2: P � 0.001, Panc-1: P �0.001).
Expression of Type I IFN Receptor mRNASince the susceptibility of cells to IFNs could reflect the
different amount of corresponding receptors, we analyzed theexpression of type I IFN receptors (IFNAR-1 and IFNAR-2,short and long form) mRNA by real-time quantitative RT-PCR in the BxPC-3, MiaPaCa-2, and Panc-1 cell lines. Usingsequence specific primers against the type I IFN receptorsubunits, we detected the presence of IFNAR-1, IFNAR-2 total,IFNAR-2b and IFNAR-2c mRNA, normalized for the amountof the housekeeping gene HPRT. As shown in Figure 5, theexpression of IFNAR-1 mRNA was significantly higher inBxPC-3 and MiaPaCa-2 compared with Panc-1 (both P �0.001), whereas no statistically significant difference was ob-served between BxPC-3 and MiaPaCa-2. In addition, the mRNAexpression level of IFNAR-2a, IFNAR-2b, and IFNAR-2c
mRNA was higher in BxPC-3 compared with MiaPaCa-2 andPanc-1 (P � 0.001).
ImmunocytochemistrySpecific immunoreactivity for IFN receptor subunits
(IFNAR-1, IFNAR-2b, and IFNAR-2c) was found in all 3pancreatic cancer cell lines (Fig. 6A–I). It was stronglypositive for IFNAR-1 in BxPC-3 (Fig. 6A) and the stainingwas predominantly at the plasma membrane. On the otherhand, in MiaPaCa-2 (Fig. 6D) and in Panc-1 (Fig. 6G), theexpression of IFNAR-1 was lower and particularly distrib-uted in the cytoplasm, although a proportion of Panc-1cells resulted to be mildly to moderately positive forIFNAR-1 at the plasma membrane as well. IFNAR-2bshowed a comparable expression in BxPC-3 (Fig. 6B) andPanc-1 (Fig. 6H), while in MiaPaCa-2 (Fig. 6E) the ex-pression of this subunit was lower compared with the other2 cell lines. In BxPC-3 and in MiaPaCa-2, the immuno-staining of IFNAR-2b was localized in the cytoplasm andon the membrane, while in Panc-1 the expression ofIFNAR-2b was preferentially on the cytoplasm. IFNAR-2cis mainly expressed on the plasma membrane and in thecytoplasm in BxPC-3 (Fig. 6C) and in MiaPaCa-2 (Fig.6F), respectively. Finally, in Panc-1 (Fig. 6I) this receptorsubunit is primarily expressed in cytoplasm, the IFNAR-2cpattern is heterogeneous and the staining is negative inabout 60% to 70% of the cells.
FIGURE 2. Effects of IFN-� (A–C) and IFN-� (D–F) treatment on apoptosis (DNA fragmentation) in BxPC-3, MiaPaCa-2, andPanc-1 cell lines. The cells were incubated for 1 day without (control) or with the drugs indicated at different concentrations.Values are absorbance units and are expressed as percent of the control. Data are the mean � SEM. *P � 0.001 versus control.
Annals of Surgery • Volume 246, Number 2, August 2007 IFN-� Therapy in Pancreatic Cancer
© 2007 Lippincott Williams & Wilkins 263
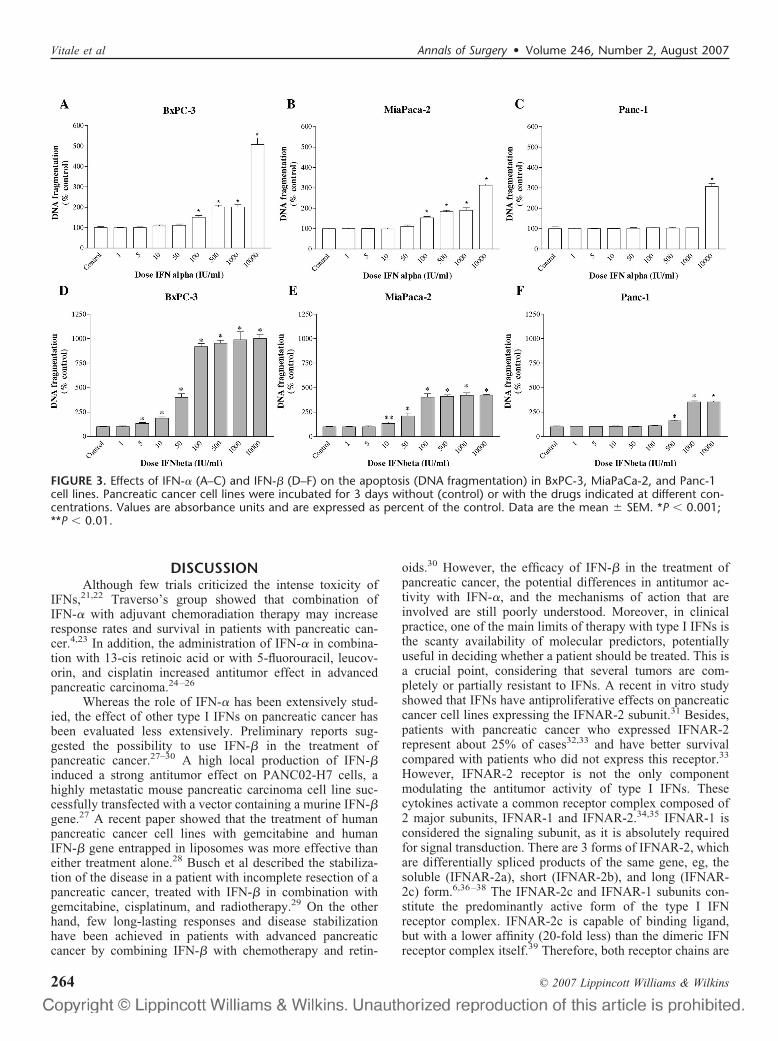
DISCUSSIONAlthough few trials criticized the intense toxicity of
IFNs,21,22 Traverso’s group showed that combination ofIFN-� with adjuvant chemoradiation therapy may increaseresponse rates and survival in patients with pancreatic can-cer.4,23 In addition, the administration of IFN-� in combina-tion with 13-cis retinoic acid or with 5-fluorouracil, leucov-orin, and cisplatin increased antitumor effect in advancedpancreatic carcinoma.24–26
Whereas the role of IFN-� has been extensively stud-ied, the effect of other type I IFNs on pancreatic cancer hasbeen evaluated less extensively. Preliminary reports sug-gested the possibility to use IFN-� in the treatment ofpancreatic cancer.27–30 A high local production of IFN-�induced a strong antitumor effect on PANC02-H7 cells, ahighly metastatic mouse pancreatic carcinoma cell line suc-cessfully transfected with a vector containing a murine IFN-�gene.27 A recent paper showed that the treatment of humanpancreatic cancer cell lines with gemcitabine and humanIFN-� gene entrapped in liposomes was more effective thaneither treatment alone.28 Busch et al described the stabiliza-tion of the disease in a patient with incomplete resection of apancreatic cancer, treated with IFN-� in combination withgemcitabine, cisplatinum, and radiotherapy.29 On the otherhand, few long-lasting responses and disease stabilizationhave been achieved in patients with advanced pancreaticcancer by combining IFN-� with chemotherapy and retin-
oids.30 However, the efficacy of IFN-� in the treatment ofpancreatic cancer, the potential differences in antitumor ac-tivity with IFN-�, and the mechanisms of action that areinvolved are still poorly understood. Moreover, in clinicalpractice, one of the main limits of therapy with type I IFNs isthe scanty availability of molecular predictors, potentiallyuseful in deciding whether a patient should be treated. This isa crucial point, considering that several tumors are com-pletely or partially resistant to IFNs. A recent in vitro studyshowed that IFNs have antiproliferative effects on pancreaticcancer cell lines expressing the IFNAR-2 subunit.31 Besides,patients with pancreatic cancer who expressed IFNAR-2represent about 25% of cases32,33 and have better survivalcompared with patients who did not express this receptor.33
However, IFNAR-2 receptor is not the only componentmodulating the antitumor activity of type I IFNs. Thesecytokines activate a common receptor complex composed of2 major subunits, IFNAR-1 and IFNAR-2.34,35 IFNAR-1 isconsidered the signaling subunit, as it is absolutely requiredfor signal transduction. There are 3 forms of IFNAR-2, whichare differentially spliced products of the same gene, eg, thesoluble (IFNAR-2a), short (IFNAR-2b), and long (IFNAR-2c) form.6,36–38 The IFNAR-2c and IFNAR-1 subunits con-stitute the predominantly active form of the type I IFNreceptor complex. IFNAR-2c is capable of binding ligand,but with a lower affinity (20-fold less) than the dimeric IFNreceptor complex itself.39 Therefore, both receptor chains are
FIGURE 3. Effects of IFN-� (A–C) and IFN-� (D–F) on the apoptosis (DNA fragmentation) in BxPC-3, MiaPaCa-2, and Panc-1cell lines. Pancreatic cancer cell lines were incubated for 3 days without (control) or with the drugs indicated at different con-centrations. Values are absorbance units and are expressed as percent of the control. Data are the mean � SEM. *P � 0.001;**P � 0.01.
Vitale et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins264

required to form a high affinity-binding site and initiate signaltransduction leading to the induction of IFN-responsivegenes. The short form is able to bind type I IFNs but does notcouple to signal transduction.40 The soluble form may act asa regulator of free IFNs and, depending on concentration,leads to the neutralization or even enhancement of IFNbioactivity.41,42
In the present study, we compared the antitumor effectsof IFN-� and IFN-�, as well as the mechanisms that areinvolved in the growth inhibition of 3 human pancreaticcancer cell lines (BxPC-3, MiaPaCa-2, and Panc-1). More-over, for the first time, we evaluated the expression and thesubcellular distribution of type I IFN-receptor subtypes inthese cells. We found that IFN-� potently inhibits cell pro-liferation already at very low concentrations (5–10 IU/mL) inBxPC-3 and MiaPaCa-2. These concentrations can be achievedin vivo after subcutaneous administration of IFN-�.43,44
The direct antitumor effects of IFN-� and -� are asso-ciated with the induction of apoptosis and cell cycle arrest. InBxPC-3 and MiaPaCa-2, both cytokines are able to induce
apoptosis, but the increase in DNA fragmentation after IFN-�treatment occurred earlier and was considerably more potentthan after IFN-� treatment. Panc-1 was the most resistant cellline to both IFNs, showing a stimulation of apoptosis only atvery high doses (IFN-� �10,000 IU/mL, IFN-� �500IU/mL). In all 3 pancreatic cancer cell lines, both IFNs inducea significant accumulation of cells in S phase compared withthe untreated control, suggestive of a cell cycle arrest in thelate S phase. The S-phase block induced by IFN-� is morepotent and earlier than that of IFN-�.
Quantitative RT-PCR study and immunocytochemicalanalysis demonstrate the presence of all type I IFN recep-tor subunit transcripts and proteins in BxPC-3, MiaPaCa-2,and Panc-1 cells. The high expression of IFNAR-1 andIFNAR-2c subunits in BxPC-3 could explain the major sen-sitivity of this cell line to IFN treatment. Indeed, as shown byWagner et al,45 increasing the cell surface levels of IFNAR2cin cancer cells enhances their sensitivity to the antiprolifera-tive and apoptotic effects of type I IFNs. Moreover, long-termcultures of IFNAR1-deficient mouse embryonic fibroblasts,
FIGURE 4. Cell cycle distribution after 1, 2, and 3 days of incubation with 1000 IU/mL IFN-� and 1000 IU/mL IFN-� inBxPC-3 (A–C), MiaPaCa-2 (D–F), and Panc-1 (G–I) cells. Data are expressed as mean � SEM of the percentage of cells in thedifferent phases of the cell cycle, as compared with untreated control cells. Control values have been set to 100%. �, IFN-�;Œ, IFN-�. *P � 0.05; **P � 0.01; ***P � 0.001 versus control.
Annals of Surgery • Volume 246, Number 2, August 2007 IFN-� Therapy in Pancreatic Cancer
© 2007 Lippincott Williams & Wilkins 265

as well as IFN-� deficient cells, resulted in the formation oftransformed colonies in vitro and the formation of tumors innude mice.5 It is interesting to observe striking differencesin the subcellular localization and distribution of IFNsreceptor subunits, as determined by immunocytochemistry.In BxPC-3, the staining for the active subunits of IFNreceptor (IFNAR-1 and IFNAR-2c) is mainly membranous,whereas in Panc-1 the expression of IFNAR-2c is preferen-tially in the cytoplasm. A potential explanation to clarify theantitumor activity of type I IFNs at high doses in PANC-1,where IFNAR-2c subunits is mainly detected in the cyto-plasm, may be that immunohistochemistry is not sensitiveenough to demonstrate very low quantities of IFN membranereceptors. In addition, it has been recently observed thatIFNAR-1, which is mildly to moderately expressed in theplasma membrane of several PANC-1 cells, has an importantrole in antiproliferative activity modulated by type I IFNs.46
These arguments may explain why, even in the presence oflow membrane expression of IFN receptors, antiproliferativeand pro-apoptotic effects of high concentrations of type IIFNs are observed in Panc-1 cells. In Panc-1, about 60% to70% of the cells exhibit no detectable levels of IFNAR-2c.This heterogeneity in IFNAR-2c expression may provide anadditional explanation for the low sensitivity of these cells toIFN-� and IFN-� treatment. In Panc-1, it is possible aselection of cell type during type I IFN treatment, with higherpossibility to survive for IFNAR-2c negative cells. Summariz-ing, these data suggest that the high sensitivity of BxPC-3 toIFNs treatment could be related to the strong expression ofIFNAR-1 and IFNAR-2c and the main membranous localiza-
tion, whereas the low expression, cytoplasmic localization, andheterogeneous staining of IFNAR-2c in Panc-1 could explainthe relative resistance of these cells to IFN treatment. This is thefirst study, as far as we know, showing the importance ofexpression, distribution, and localization of type I IFN receptorsubtypes in the modulation of response to IFN treatment inpancreatic cancer. Our data also suggest that a careful evaluationof both active IFNAR subtypes in pancreatic cancer is requiredbefore treatment with type I IFNs is considered.
Although IFN-� and IFN-� interact with the samereceptor, the induction of a differential response can beexplained by the diversity in the structure between bothcytokines,47,48 generating different interactions and affinitiesfor the related receptor. Indeed, IFN-� has a higher bindingaffinity (10-fold) than IFN-�.10 However, this cannot com-pletely explain the difference in potency of cell growthinhibition between both cytokines, particularly in BxPC-3,where the IC50 for IFN-� is 40 times lower than that ofIFN-�. Differences in the interaction of these IFNs with theirreceptors could be also involved. Both IFNs induce tyrosinephosphorylation of the receptor subunits; IFN-�, but notIFN-�, induces the association of IFNAR-1 and IFNAR-2cchains, indicating that the specificity of signaling for distincttype I IFN subtypes is established by differential conforma-tion of the receptor complex.40,49
CONCLUSIONThis study shows that IFN-� is significantly more
effective than IFN-� in inducing cell growth inhibition in
FIGURE 5. A–E, Relative expression level of type I IFN receptor (IFNAR-1, IFNAR-2 total, IFNAR-2a, IFNAR-2b, IFNAR-2c) mRNAnormalized to HPRT mRNA in human pancreatic cancer cell lines (BxPC-3, MiaPaCa-2, Panc-1), evaluated by quantitative RT-PCR. Values represent the mean � SEM.
Vitale et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins266

pancreatic cancer because it induces a more potent and earlycell cycle arrest and apoptosis activation compared withIFN-�. Considering that IFN-� stimulates apoptosis alreadyat very low dose, this cytokine could be a more promisingagent than IFN-� for the treatment of human pancreaticcancer, particularly in tumors with a high expression ofIFNAR-1 and IFNAR-2c, which is supporting its use infuture clinical investigation. In addition, there is clear in vitroevidence that differential expression levels and distribution ofthe IFNs receptor subunits play a role in the regulation of theresponse to type I IFNs therapy in pancreatic cancer. Futurestudies should investigate in vivo whether the intensity, subcel-lular localization, and distribution of IFNAR-1 and IFNAR-2c atimmunohistochemistry may predict the response to therapy withboth IFN-� and IFN-� in pancreatic cancer.
ACKNOWLEDGMENTSThe authors thank Claessen Sandra, MH, for technical
assistance.
REFERENCES1. Sohn T, Yeo C, Cameron J, et al. Resected adenocarcinoma of the
pancreas—616 patients: results, outcomes, and prognostic indicators.J Gastrointest Surg. 2000;4:567–579.
2. Neoptolemos JP, Stocken DD, Friess H, et al. A randomized trial ofchemoradiotherapy and chemotherapy after resection of pancreatic can-cer. N Engl J Med. 2004;350:1200–1210.
3. Klinkenbijl JH, Jeekel J, Sahmoud T, et al. Adjuvant radiotherapy and5-fluorouracil after curative resection of cancer of the pancreas andperiampullary region: phase III trial of the EORTC gastrointestinal tractcancer cooperative group. Ann Surg. 1999;230:776–782.
4. Picozzi VJ, Kozarek RA, Traverso LW. Interferon-based adjuvant che-moradiation therapy after pancreaticoduodenectomy for pancreatic ade-nocarcinoma. Am J Surg. 2003;185:476–480.
5. Lindner DJ, Borden EC, Kalvakolanu DV. Synergistic antitumor effectsof a combination of interferons and retinoic acid on human tumor cellsin vitro and in vivo. Clin Cancer Res. 1997;3:931–937.
6. Takaoka A, Taniguchi T. New aspects of IFN-�/� signalling in immu-nity, oncogenesis and bone metabolism. Cancer Sci. 2003;94:405–411.
7. Mitchell MS. Combination of anticancer drugs and immunotherapy.Cancer Immunol Immunother. 2003;52:686–692.
8. Vitale G, Tagliaferri P, Caraglia M, et al. Slow release lanreotide in
FIGURE 6. Immunocytochemical detection of IFNAR-1 (A, D, G), IFNAR-2b (B, E, H), and IFNAR-2c (C, F, I) receptors inBxPC-3 (A–C), MiaPaCa-2 (D–F), and Panc-1 (G–I). Original magnification, �400. The expressions of IFNAR-1 and IFNAR-2care mainly membranous in BxPC-3 (A and C, solid arrow). In Panc-1, IFNAR-2c is localized in the cytoplasm (I, solid arrow)and 60% to 70% of the cells are negative for IFNAR-2c (I, dashed arrow).
Annals of Surgery • Volume 246, Number 2, August 2007 IFN-� Therapy in Pancreatic Cancer
© 2007 Lippincott Williams & Wilkins 267

combination with interferon-�2b in the treatment of symptomatic ad-vanced medullary thyroid carcinoma. J Clin Endocrinol Metab. 2000;85:983–988.
9. Vitale G, Caraglia M, Ciccarelli A, et al. Current approaches in thetherapy of medullary thyroid carcinoma. Cancer. 2001;91:1797–1808.
10. Johns TG, Mackay IR, Callister KA, et al. Antiproliferative potencies ofinterferons on melanoma cell lines and xenografts: higher efficacy ofinterferon beta. J Natl Cancer Inst. 1992;84:1185–1190.
11. Xie K, Bielenberg D, Huang S, et al. Abrogation of tumorigenicity andmetastasis of murine and human tumor cells by transfection with themurine IFN-beta gene: possible role of nitric oxide. Clin Cancer Res.1997;3:2283–2294.
12. Giandomenico V, Vaccari G, Fiorucci G, et al. Apoptosis and growthinhibition of squamous carcinoma cells treated with interferon-�, inter-feron-� and retinoic acid are associated with induction of the cyclin-dependent kinase inhibitor p21. Eur Cytokine Netw. 1998;9:619–631.
13. Rosenblum MG, Yung WKA, Kelleher PJ, et al. Growth inhibitoryeffects of interferon-� but not interferon-� on human glioma cells:correlation of receptor binding 2,5–oligoadenylate synthetase andprotein kinase activity. J Interferon Res. 1990;10:141–151.
14. Coradini D, Biffi A, Pirronello E, et al. The effect of �-, �- and�-interferon on the growth of breast cancer cell lines. Anticancer Res.1994;14:1779–1784.
15. Damdinsuren B, Nagano H, Sakon M, et al. Interferon-� is more potentthan interferon-� in inhibition of human hepatocellular carcinoma cellgrowth when used alone and in combination with anticancer drugs. AnnSurg Oncol. 2003;10:1184–1190.
16. Vitale G, de Herder WW, van Koetsveld PM, et al. Interferon-beta is ahighly potent inhibitor of gastroenteropancreatic neuroendocrine tumorcell growth in vitro. Cancer Res. 2006;66:554–562.
17. Hruban RH, Goggins M, Parsons J, et al. Progression model for pan-creatic cancer. Clin Cancer Res. 2000;6:2969–2972.
18. Chen ZH, Zhang H, Savarese TM. Gene deletion chemoselectivity:codelection of the genes for 16INK4, methylthioadenosine phosphorylase,and the �- and �-interferons in human pancreatic cell carcinoma linesand its implications for chemotherapy. Cancer Res. 1996;56:1083–1090.
19. Hofland LJ, van Koetsveld PM, Lamberts SW. Percoll density gradientcentrifugation of rat pituitary tumor cells: a study of functional hetero-geneity within and between tumors with respect to growth rates, prolac-tin production and responsiveness to the somatostatin analog SMS201–995. Eur J Cancer. 1990;26:37–44.
20. Ferone D, Pivonello R, van Hagen PM, et al. Quantitative and functionalexpression of somatostatin receptor subtypes in human thymocytes.Am J Physiol Endocrinol Metab. 2002;283:E1056–E1066.
21. John WJ, Flett MO. Continuous venous infusion of 5-fluorouracil andinterferon-alpha in pancreatic carcinoma. Am J Clin Oncol. 1998;21:147–150.
22. Sparano J, Lipsitz S, Wadler S, et al. Phase II trial of prolongedcontinuous infusion of 5-fluorouracil and interferon-alpha in patientswith advanced pancreatic cancer: Eastern Cooperative Oncology Groupprotocol 3292. Am J Clin Oncol. 1996;19:546–551.
23. Nukui Y, Picozzi VJ, Traverso LW. Interferon-based adjuvant chemo-radiation therapy improves survival after pancreaticoduodenectomy forpancreatic adenocarcinoma. Am J Surg. 2000;179:367–371.
24. Brembeck FH, Schoppmeyer K, Leupold U, et al. A phase II pilot trialof 13-cis retinoic acid and interferon-� in patients with advancedpancreatic carcinoma. Cancer. 1998;83:2317–2323.
25. Sporn JR, Buzaid AC, Slater D, et al. Treatment of advanced pancreaticadenocarcinoma with 5-FU, leucovorin, interferon-alpha-2b, and cispla-tin. Am J Clin Oncol. 1997;20:81–83.
26. Bernhard H, Jager-Arand E, Bernhard G, et al. Treatment of advancedpancreatic cancer with 5-fluorouracil, folinic acid and interferon alpha-2A: results of a phase II trial. Br J Cancer. 1995;71:102–105.
27. Wang B, Xiong Q, Shi Q, et al. Intact nitric oxide synthase II gene isrequired for interferon-�-mediated suppression of growth and metastasisof pancreatic adenocarcinoma. Cancer Res. 2001;61:71–75.
28. Endou M, Mizuno M, Nagata T, et al. Growth inhibition of humanpancreatic cancer cells by human interferon-� gene combined withgemcitabine. Int J Mol Med. 2005;15:277–283.
29. Busch M, Wilkowski R, Schaffer M, et al. Combined chemotherapy,radiotherapy, and immunotherapy for pancreatic carcinoma: a casereport. Adv Ther. 2000;17:133–139.
30. Recchia F, Sica G, Casucci D, et al. Advanced carcinoma of thepancreas: phase II study of combined chemotherapy, beta-interferon, andretinoids. Am J Clin Oncol. 1998;21:275–279.
31. Saidi RF, Williams F, Ng F, et al. Interferon receptors and the caspasecascade regulate the antitumor effects of interferons on human pancre-atic cancer cell lines. Am J Surg. 2006;191:358–363.
32. Ota H, Nagano H, Doki Y, et al. Expression of type I interferon receptoras a predictor of clinical response to interferon-� therapy of gastroin-testinal cancers. Oncol Rep. 2006;16:249–255.
33. Saidi RF, Williams F, Silberberg B, et al. Expression of interferonreceptors in pancreatic cancer: identification of a novel prognostic factor.Surgery. 2006;139:743–748.
34. Mogensen KE, Lewerenz M, Reboul J, et al. The type I interferonreceptor: structure, function, and evolution of a family business. J In-terferon Cytokine Res. 1999;19:1069–1098.
35. Deonarain R, Chan DCM, Platanias LC, et al. Interferon-�/�-receptorinteractions: a complex story unfolding. Curr Pharm Des. 2002;8:2131–2137.
36. Domanski P, Witte M, Kellum M, et al. Cloning and expression of a longform of the beta subunit of the interferon alpha beta receptor that isrequired for signalling. J Biol Chem. 1995;270:21606–21611.
37. Domanski P, Colamonici OR. The type-I interferon receptor: the longand short of it. Cytokine Growth Factor Rev. 1996;7:143–151.
38. Pestka S. The interferon receptors. Semin Oncol. 1997;24(suppl 9):18 – 40.
39. Cohen B, Novick D, Barak S, et al. Ligand-induced association of thetype I interferon receptor components. Mol Cell Biol. 1995;15:4208–4214.
40. Pfeffer LM, Basu L, Pfeffer SR, et al. The short form of the interferonalpha/beta receptor chain 2 acts as a dominant negative for type Iinterferon action. J Biol Chem. 1997;272:11002–11005.
41. Hardy MP, Owczarek CM, Trajanovska S, et al. The soluble murine typeI interferon receptor Ifnar-2 is present in serum, is independentlyregulated, and has both agonistic and antagonistic properties. Blood.2001;97:473–482.
42. McKenna SD, Vergilis K, Arulanandam AR, et al. Formation ofhuman IFN-beta complex with the soluble type I interferon receptorIFNAR-2 leads to enhanced IFN stability, pharmacokinetics, andantitumor activity in xenografted SCID mice. J Interferon CytokineRes. 2004;24:119 –129.
43. Buchwalder PA, Buclin T, Trinchard I, et al. Pharmacokinetics andpharmacodynamics of IFN-beta 1a in healthy volunteers. J InterferonCytokine Res. 2000;20:857–866.
44. Salmon P, Le Cotonnec JY, Galazka A, et al. Pharmacokinetics andpharmacodynamics of recombinant human interferon-beta in healthymale volunteers. J Interferon Cytokine Res. 1996;16:759–764.
45. Wagner TC, Velichko S, Chesney SK, et al. Interferon receptor expres-sion regulates the antiproliferative effects of interferons on cancer cellsand solid tumors. Int J Cancer. 2004;111:32–42.
46. Jaks E, Gavutis M, Uze G, et al. Differential receptor subunit affinitiesof type I interferons govern differential signal activation. J Mol Biol.2006;18 (Epub ahead of print).
47. Klaus W, Gsell B, Labhardt AM, et al. The three-dimensional highresolution structure of human interferon alpha-2a determined by hetero-nuclear NMR spectroscopy in solution. J Mol Biol. 1997;274:661–675.
48. Karpusas M, Nolte M, Benton CB, et al. The crystal structure of humaninterferon beta at 2. 2-A resolution. Proc Natl Acad Sci USA. 1997;94:11813–11818.
49. Platanias LC, Fish EN. Signaling pathways activated by interferons. ExpHematol. 1999;27:1583–1592.
Vitale et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins268

ORIGINAL ARTICLES
Postpancreatectomy Hemorrhage: Diagnosisand Treatment
An Analysis in 1669 Consecutive Pancreatic Resections
Emre F. Yekebas, MD,* Lars Wolfram, MD,* Guellue Cataldegirmen, MD,*Christian R. Habermann, MD,† Dean Bogoevski, MD,* Alexandra M. Koenig, MD,*
Jussuf Kaifi, MD,* Paulus G. Schurr, MD,* Michael Bubenheim, MD,‡ Claus Nolte-Ernsting, MD,†Gerhard Adam, MD,† and Jakob R. Izbicki, MD*
Background: To analyze clinical courses and outcome of postpan-createctomy hemorrhage (PPH) after major pancreatic surgery.Summary Background Data: Although PPH is the most life-threatening complication following pancreatic surgery, standardizedrules for its management do not exist.Methods: Between 1992 and 2006, 1524 patients operated on forpancreatic diseases were included in a prospective database. A riskstratification of PPH according to the following parameters wasperformed: severity of PPH classified as mild (drop of hemoglobinconcentration �3 g/dL) or severe (�3 g/dL), time of PPH occur-rence (early, first to fifth postoperative day; late, after sixth day),coincident pancreatic fistula, intraluminal or extraluminal bleedingmanifestation, and presence of “complex” vascular pathologies (ero-sions, pseudoaneurysms). Success rates of interventional endoscopyand angiography in preventing relaparotomy were analyzed as wellas PPH-related overall outcome.Results: Prevalence of PPH was 5.7% (n � 87) distributed almostequally among patients suffering from malignancies, borderlinetumors, and focal pancreatitis (n � 47) and from chronic pancreatitis(n � 40). PPH-related overall mortality of 16% (n � 14) was closelyassociated with 1) the occurrence of pancreatic fistula (13 of 14); 2)vascular pathologies, ie, erosions and pseudoaneurysms (12 of 14);3) delayed PPH occurrence (14 of 14); and 4) underlying diseasewith lethal PPH found only in patients with soft texture of thepancreatic remnant, while no patient with chronic pancreatitis died.Conversely, primary severity of PPH (mild vs. severe) and the kindof index operation (Whipple resection, pylorus-preserving partialpancreaticoduodenectomy, organ-preserving procedures) had no in-fluence on outcome of PPH. Endoscopy was successful in 3 from 15patients (20%), who had intraluminal PPH within the first or second
postoperative day. “True,” early extraluminal PPH had uniformly tobe treated by relaparotomy. Seventeen patients had “false,” earlyextraluminal PPH due to primarily intraluminal bleeding site fromthe pancreaticoenteric anastomosis with secondary disruption of theanastomosis. From 43 patients subjected to angiography, 25 under-went interventional coiling with a success rate of 80% (n � 20).Overall, relaparotomy was performed in 60 patients among whom33 underwent surgery as first-line treatment, while 27 were relapa-rotomied as rescue treatment after failure of interventional endos-copy or radiology.Conclusion: Prognosis of PPH depends mainly on the presence ofpreceding pancreatic fistula. Decision making as to the indication fornonsurgical interventions should consider time of onset, presence ofpancreatic fistula, vascular pathologies, and the underlying disease.
(Ann Surg 2007;246: 269–280)
Although mortality after pancreatic surgery in most high-volume centers has decreased to less than 3%,1–3 mor-
bidity still remains considerably high, ranging from 18%to 52%.4 –9 The most frequent causes for morbidity areanastomotic insufficiencies (pancreatic, biliary, gastric/duodenal, and enteral), pancreatic fistulas, and delayedgastric emptying.
Postpancreatectomy hemorrhage (PPH) is a less fre-quent, however, in some patients, devastating complication.Since both its pathophysiologic and clinical features maydiffer considerably, it is difficult to establish diagnostic andtherapeutic algorithms for adequate management of PPH: 1)time of onset (early PPH occurring within 24 to 48 hourspostoperatively versus delayed PPH after several days toweeks); 2) severity �(a) mild, (b) moderate, (c) severest, ie,life-threatening�; 3) intraluminal or extraluminal manifesta-tion; 4) underlying disease (pancreatic carcinoma vs. chronicpancreatitis); 5) kind of index operation; and 6) a possibleassociation to erosive vascular pathologies due to pancreaticfistula are factors that are important for estimating the prog-nosis of PPH. A customized risk analysis should precedeindividual decision-making. The armory of diagnostic and
From the Departments of *General, Visceral and Thoracic Surgery, †Diag-nostic and Interventional Radiology, and ‡Medical Biometry and Epide-miology, University Medical Centre Hamburg-Eppendorf, University ofHamburg, Hamburg, Germany.
Reprints: Emre F. Yekebas, MD, Department of Surgery, University HospitalEppendorf, University of Hamburg, Martinistrasse 52, 20251 Hamburg,Germany. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0269DOI: 10.1097/01.sla.0000262953.77735.db
Annals of Surgery • Volume 246, Number 2, August 2007 269

therapeutic means ranges from observant monitoring andfluid replacement, interventional procedures, ie, endoscopyand radiology, to surgical relaparotomy.
Early bleeding within the immediate postoperative pe-riod is unlikely due to vascular erosions but rather a result ofsimple technical failures. In case of PPH in the abdominalcavity, no doubt exists that immediate relaparotomy is indi-cated. However, in case of early bleeding in the gastrointes-tinal tract, endoscopy may also be an option for intervention-ally treating bleeding sites located at the gastrojejunostomyor, if accessible, at the enteroenteric anastomosis.
Because of the life-threatening potential of PPH, stan-dardized rules with respect to its management are urgentlyneeded. So far, in clinical routine, the decision about how tohandle PPH is often arbitrary and is usually based on insti-tutional or even individual experiences.
The aim of the presented evaluation was therefore to“dissect” the heterogeneous causes of PPH. Onset of mani-festations, clinical features, courses, and success rates ofnonsurgical options, ie, interventional radiology and endos-copy, and surgical procedures for treatment of PPH wereanalyzed. Based on a 15-year institutional experience, wesought, in particular, to classify different bleeding types andsuggest a diagnostic and therapeutic algorithm that may helpto allocate patients to a customized therapy (Fig. 1).
METHODSBetween 1992 and 2006, 1524 patients who underwent
a total of 1669 resectional pancreatic operations were in-cluded in a prospective, pancreatic database. Classic resec-tional procedures were performed in 1281 patients. Thisincluded duodenum preserving pancreas head resection(DPPHR, n � 623), Whipple resection (n � 358), pyloruspreserving pancreatoduodenectomy (n � 160), distal pancre-atectomy (n � 116), and total pancreatectomy (n � 24). Inthe remaining 388 patients, other interventions, eg, DPPHRcombined with cystojejunostomy, redo pancreas head resec-tion, segmental resection, and resectional salvage proceduresafter primary treatment failure in both carcinoma and chronicpancreatitis patients were performed. Patients with limiteddraining procedures, eg, simple cystojejunostomy withoutany resectional aspect of the operation, were not included inthis analysis.
The following parameters were evaluated:
HemorrhageThe severity of bleeding was classified with slight
modifications of the recommendation of the InternationalStudy Group of Pancreatic Surgery.10 Mild bleeding wasdefined as a decrease of hemoglobin concentration less than3 g/dL without or with discrete clinical impairment (tachy-cardia, decrease of mean arterial blood pressure), not oblig-atorily requiring surgical or nonsurgical intervention. SeverePPH was defined as a decrease of hemoglobin concentration�3 g/dL, with clinical impairment and requiring either sur-gical or nonsurgical treatment. “Sentinel” bleeding was de-fined as 1) discrete but evident blood loss via abdominaldrains or nasogastric tubes, hematemesis, or melena; 2) de-crease of hemoglobin concentration �1.5 g/dL; 3) spontane-
ous cessation of hemorrhage without need for transfusionwith red blood cells; and 4) rehemorrhage after a symptom-free time frame of at least 12 hours. According to the time ofonset, PPH occurring within the first to fifth postoperativeday was termed “early,” while after the sixth postoperativeday the term “delayed” or “late” PPH was used.
Pancreatic FistulaUntil 2005, we defined fistula as drain fluid �20 mL/24
hours after 3 days postoperatively with amylase activity morethan 3 times the serum activity. In August 2005, we decidedto adopt our definition according to the International StudyGroup for Pancreatic Fistula (ISGPF) classification.11 Afterimplementation of the ISGPF definition, a total of 92 patientswere operated on for pancreatic diseases. Since only marginaldifferences between both definitions existed, an analysis ofthe subset of patients operated on before 2005 showed thatISGPF classification would also have defined all of thesepatients to have pancreatic fistula.
Nonsurgical, Interventional BleedingManagement
Angiographic evaluation or upper gastrointestinal en-doscopy was only performed in case of successful mainte-nance of hemodynamic stability by fluids, transfusion withpacked red blood cells, and fresh frozen plasma.
Angiography sought specifically to exclude bleedingsites originating from the following main vessels and theirbranches: hepatic artery, gastroduodenal artery, splenic ar-tery, and superior mesenteric artery, respectively. In case of atranssection of the gastroduodenal artery, special attentionwas addressed to rule out stump insufficiency. Vascularaccess for interventional embolization was achieved by punc-turing the common femoral artery. Afterward, the catheterwas advanced in the visceral aortic branches, ie, the hepaticartery, gastroduodenal artery, splenic artery, and the superiormesenteric artery. Embolization was performed using a co-axial technique and microcoils, hereby embolizing the provenor assumed site of hemorrhage. In patients in whom indexangiography failed to localize the bleeding source, who werehemodynamically stable at the time of investigation and hadblood requirement �4 units/24 hours, the introducer sheathwas left in the common femoral artery for a maximum of 24hours to maintain vascular access. In case of recurrent bleed-ing within this period, patients underwent immediate rean-giography. After 24 hours, the introducer was removed.
In case of successful bleeding control by interventionalangiography, CT scans and/or abdominal sonographies wereperformed checking for fluid collections close to the pancre-atic anastomosis. When such pathologies suggestive for in-adequately drained pancreatic fistula, eg, due to dislocation oftarget drains, drain clotting, or both, were evidenced, indica-tion for CT-guided placement of further drains within thecollection, if interventionally accessible, or relaparotomy wasestablished, depending on the patient’s clinical condition andon whether patients had pancreatic fistula.
Surgical ReexplorationIndication for surgery was based on the following
findings: 1) acute life-threatening hemodynamic deterioration
Yekebas et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins270

with decrease of hemoglobin �3 g/dL or evident bleedingdrained percutaneously or via the nasogastric tube; and 2)critical hemodynamic instability with continuing requirementof packed red blood cells exceeding 6 units per 12 hourswithout evidence for the bleeding source by angiography/endoscopy. In case of life-threatening situations, bedsidedecisions without measurement of hemoglobin were made.
In patients that had early extraintestinal bleeding with-out vascular erosions or pseudoaneurysms, appropriate he-mostasis was usually achieved by suture ligating the bleedingsite. When hemorrhage originated from ominous vascularerosions or pseudoaneurysms, operative decision making wasbased on the patients individual risk profile. Surgical proce-dures ranged from simple suture ligation or angioplastic
FIGURE 1. Suggested algorithm for treatment of early (A) and delayed (B) postpancreatectomy hemorrhage after major pan-creatic surgery.
Annals of Surgery • Volume 246, Number 2, August 2007 Postpancreatectomy Hemorrhage
© 2007 Lippincott Williams & Wilkins 271

reconstructions to completion pancreatectomy in patientswith severe pancreatic fistula. Only in the absence of severeupper abdominal pancreatitis due to inadequately drainedpancreatic fistula, vascular reconstruction was combined withcompletion pancreatectomy. When significant peri-anasto-motic pancreatitis had occurred, severe vascular damages, ie,erosions and pseudoaneurysms, were treated by oversewingor ligating the bleeding source. In these cases, intraoperativedecision whether 1) to drain pancreatic fistula externally, 2)to perform completion pancreatectomy, or 3) to subject pa-tients to repeated, planned peritoneal lavage was based onseveral aspects, especially on the presence or absence of:concomitant pancreatitis/peritonitis, severe coagulopathy,and severe adhesions.
Our standard method of reconstruction after Whippleresection/PPPD consists of a separate end-to-side anastomo-sis of the pancreatic remnant with the proximal jejunal stumpafter removal of the specimen. Afterward, 30 to 40 cm distalto the pancreaticojejunostomy, the jejunal continuity is inter-rupted. A choledochojejunal anastomosis in end-to-side tech-nique and an antecolic end-to side gastrojejunostomy areperformed. Reconstruction is completed by reinsertion of theisolated, jejunal loop anastomosed with the pancreatic rem-nant in side-to side technique into the alimentary continuity30 to 40 cm distal to the gastrojejunostomy. Intraluminal and“false” extraluminal PPH occurring until the fifth postopera-tive day were consistently located at the pancreaticojejunos-tomy. We treated such pathologies usually by opening thestapled, blind ends of the jejunal loop, which had beenseparated out of the gastrointestinal continuity during theindex operation. This enabled us to maintain the integrity ofthe pancreaticojejunostomy as long as the bleeding site hadnot been clearly proven. When bleeding from the pancreati-cojejunostomy was excluded, the further anastomoses wereexplored depending on the intraoperative situs.
Statistical AnalysisSPSS 11.0 (SPSS Inc., Chicago, IL) was used for
statistical analysis. Data were analyzed using the �2 test,Student t test, and Fisher exact test as appropriate. A P value�0.05 was considered statistically significant. Since thisanalysis was intended to be explorative, no adjustment formultiple testing was carried out.
RESULTS
Patient CharacteristicsThe overall prevalence of PPH was 5.7% (n � 87). The
underlying diseases were in 47 patients, pancreatic carci-noma, neuroendocrine tumors, tumors of borderline pathol-ogy, and focal pancreatitis, whereas 40 patients suffered fromchronic pancreatitis involving the entire gland (Table 1).Intraductal papillary mucinous tumors of the pancreas(IPMT), mucinous-type cystadenoma, and nonmetastatic neu-roendocrine tumors (NET) of the pancreas �3 cm withoutinvasion in adjacent organs, respectively, were defined asborderline pathologies. Mild PPH (decrease of Hb �3 g/dL)was found in 36 patients, while 51 patients had primarilysevere PPH (decrease of Hb �3 g/dL). Seventeen patients
were primarily objected to observational monitoring withoutinterventional procedures because they were hemodynami-cally symptom-free and had a decrease of Hb concentration�1.5 g/dL. However, in 13 of these 17 patients (76%),primarily discrete bleeding turned to be “sentinel PPH” withsevere rehemorrhage (range, 14–85 hours) in their furtherclinical course requiring subsequent intervention, ie, angiog-raphy, endoscopy, or surgery, respectively. This resulted in atotal of 83 patients who had endoscopic, radiologic, or sur-gical interventions, whereas in only 4 patients mild PPHcame spontaneously to rest.
Interventions PerformedIncluding the 13 patients undergoing conservative ther-
apy first but who underwent interventional procedures in theirfurther course, the following first-line interventions wereperformed: 43 of 83 patients (52%) were subjected to angiog-raphy, 15 (18%) patients to endoscopy with an overlap of 8patients subjected first to endoscopy and afterward to angiog-raphy (Table 2). Thirty-three patients (40%) underwent pri-mary surgical relaparotomy either due to extraluminal blood
TABLE 1. Patient Characteristics
n %
PPH overall 87 5
Mild PPH 36 41
Severe PPH 51 59
“Sentinel” bleed* 29 33
Bleeding site
Extraluminal PPH† 51 59
Intraluminal PPH 36 41
“False” extraluminal PPH† 17 20
Underlying disease
Carcinoma/NET/borderline tumors/focal pancreatitis
47 54
Chronic pancreatitis 40 46
Pancreatic fistula
Pancreatic fistula prior to PPH 34 39
Absence of pancreatic fistula 53 (44)‡ 61(51)‡
Post-PPH fistula (9)‡ (10)‡
Treatment-related overall success rates
Observational monitoring 4/17 24
Interventional endoscopy 3/15 20
Interventional radiology§ 20/25 80
(20/43)� (47%)�
PPH-associated mortality
Survival 73 84
Death 14 16
*Sentinel bleed was defined as minor hemorrhage preceding either mild or severePPH after a symptom-free time frame of at least 12 hours.
†In 17 patients with extraluminal PPH, further evaluation revealed that bleedingoriginated either from the resection cavity in chronic pancreatitis patients or from thetranssection surface after Whipple resection/PPPD.
‡In 9 among 53 patients, pancreatic fistula developed subsequent to PPH due to adisruption of the pancreaticoenteric anastomosis, including 3 patients who underwentrepetitive angiography.
§Success rate in the subset of patients in whom therapeutic coiling was performedaccounted for 80%, while overall success rate in all 43 patients subjected to angiographyincluding also those 23 patients in whom diagnostic angiography was not followed byinterventional coiling was 47%.
Yekebas et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins272

TAB
LE2.
Out
com
eof
Prim
ary
Non
surg
ical
Inte
rven
tions
inPo
stp
ancr
eate
ctom
yH
emor
rhag
e
Pat
ient
No.
Ons
etof
PP
H(P
OD
)*
Sent
inel
PP
H(�
/�)
Und
erly
ing
Dis
ease
†In
dex
Ope
rati
on‡
Pan
crea
tic
Fis
tula
(�/�
)§
End
osco
py:
1st
Lin
eIn
terv
enti
onA
ngio
grap
hy:
1st/
2nd
Lin
eT
reat
men
t
Ble
edin
gSi
teA
sses
sed
Intr
aope
rati
vely
Out
com
e(s
urvi
ved/
died
)B
leed
ing
Site
Succ
ess
(Y/N
)P
PH
Vis
ible
(Y/N
)B
leed
ing
Site
Coi
ling
(Y/N
)Su
cces
s(Y
/N)
11
�C
PD
PP
HR
�G
JAY
Sur
vive
d
22
�C
aW
R�
GJA
YS
urvi
ved
31
�C
PD
PP
HR
�E
EA
YS
urvi
ved
44
�C
aD
SP
�N
Om
enta
lbl
eedi
ngS
urvi
ved
53
�C
aP
PP
D�
NR
etro
peri
tone
umS
urvi
ved
63
�C
aP
PP
D�
NC
oron
ary
vein
Sur
vive
d
71
�C
aW
R�
NP
ancr
eati
ccu
tsu
rfac
eS
urvi
ved
82
�C
aW
R�
NN
Por
tal
vein
trib
utar
yS
urvi
ved
915
�C
aP
PP
D�
NN
Ret
rope
rito
neum
Sur
vive
d
101
�C
PP
PP
D�
NN
Rig
htga
stri
car
tery
Sur
vive
d
112
�B
TS
R�
NN
Lef
t-si
ded
panc
reat
icre
mna
ntS
urvi
ved
1212
�C
aW
R�
NY
HA
NU
pper
abdo
min
alab
sces
ser
odin
ghe
pati
car
tery
Die
d
138
�C
aD
SP
�N
YS
AN
Ero
sive
sple
nic
arte
ryst
ump
insu
ffici
ency
Die
d
142
�C
PD
PP
HR
�N
YS
MA
(IP
DA
)Y
YS
urvi
ved
153
�C
PD
PP
HR
�N
NS
MA
(IP
DA
,“b
lind
”co
ilin
g)Y
YS
urvi
ved
162
�C
PP
PP
D�
NG
DA
stum
p(“
blin
d”co
ilin
g)Y
N2n
dbr
anch
ofsu
peri
orm
esen
teri
car
tery
Sur
vive
d
173
�C
PD
PP
HR
�N
SM
A(I
PD
A,
“bli
nd”
coil
ing)
YY
Sur
vive
d
184
�5�
�C
PD
PP
HR
�N
GD
A�
SM
A(“
blin
d”co
ilin
g)Y
Y5
Sur
vive
d
192
�3�
�C
PD
PP
HR
�N
GD
A�
SM
A(“
blin
d”co
ilin
g)Y
Y5
Sur
vive
d
208
�C
aD
SP
�Y
SA
YY
Sur
vive
d
216
�C
aD
SP
�Y
SA
YY
Ero
sion
ofa
maj
orS
Abr
anch
Sur
vive
d
228
�C
aW
R�
YG
DA
YY
Ero
sive
GA
stum
pin
suffi
cien
cyS
urvi
ved
232
�C
PD
PP
HR
�Y
GD
AY
YS
urvi
ved
2411
�C
aW
R�
YG
DA
YY
Sur
vive
d
259
�B
TP
PP
D�
YG
DA
YY
Sur
vive
d
262
�C
PD
PP
HR
�Y
GD
A(S
PD
A)
YY
Sur
vive
d
273
�C
PD
PP
HR
�Y
GD
AY
YS
urvi
ved
286
�F
PD
PP
HR
�Y
SM
A(I
PD
A)
YY
Sur
vive
d
292
�C
PD
PP
HR
�Y
SM
A(I
PD
A)
YY
Sur
vive
d
(Con
tinu
ed)
Annals of Surgery • Volume 246, Number 2, August 2007 Postpancreatectomy Hemorrhage
© 2007 Lippincott Williams & Wilkins 273

TAB
LE2.
(Con
tinue
d)
Pat
ient
No.
Ons
etof
PP
H(P
OD
)*
Sent
inel
PP
H(�
/�)
Und
erly
ing
Dis
ease
†In
dex
Ope
rati
on‡
Pan
crea
tic
Fis
tula
(�/�
)§
End
osco
py:
1st
Lin
eIn
terv
enti
onA
ngio
grap
hy:
1st/
2nd
Lin
eT
reat
men
t
Ble
edin
gSi
teA
sses
sed
Intr
aope
rati
vely
Out
com
e(s
urvi
ved/
died
)B
leed
ing
Site
Succ
ess
(Y/N
)P
PH
Vis
ible
(Y/N
)B
leed
ing
Site
Coi
ling
(Y/N
)Su
cces
s(Y
/N)
303
�C
PD
PP
HR
�Y
SM
A(I
PD
A�
2nd
bran
ch)
YY
Sur
vive
d
314
�5�
�C
PP
PP
D�
YS
MA
(IP
DA
�2n
dbr
anch
)Y
Y5
Sur
vive
d
326
�B
TS
R�
YS
MA
(2nd
bran
ch)
YY
Ero
sive
chan
ges
ofth
e2n
dbr
anch
Sur
vive
d
334
�C
PD
PP
HR
�Y
SM
A(2
ndbr
anch
)Y
YS
urvi
ved
3412
�C
aW
R�
YG
DA
YY
Ero
sion
ofth
eG
DA
stum
pS
urvi
ved
351
�N
ET
WR
�Y
GD
AY
NP
ancr
eati
ccu
tsu
rfac
eS
urvi
ved
362
�4�
�C
PD
PP
HR
�Y
GD
A(S
PD
A)
Y�
NS
uper
ior
panc
reat
oduo
dena
lar
tery
coil
ing
fail
ure
Sur
vive
d
373
�C
PD
PP
HR
�Y
SM
A(I
PD
A)
YN
Sup
erio
rm
esen
teri
car
tery
coil
ing
fail
ure
Sur
vive
d
385
�C
PD
PP
HR
�Y
SM
A(I
PD
A)
YN
Infe
rior
panc
reat
oduo
dena
lar
tery
coil
ing
fail
ure
Sur
vive
d
3912
�B
TW
R�
YG
DA
NG
astr
oduo
dena
lar
tery
stum
pin
suffi
cien
cyS
urvi
ved
408
�9�
�C
PD
PP
HR
�Y
GD
A(S
PD
A)
N�
Sup
erio
rpa
ncre
atod
uode
nal
arte
ryin
suffi
cien
cy
Sur
vive
d
4132
�C
aP
PP
D�
YG
DA
NG
astr
oduo
dena
l�
hepa
tic
arte
ryps
eudo
aneu
rysm
Die
d
422
�3�
�C
PD
PP
HR
�Y
SM
A(I
PD
A)
N�
Infe
rior
panc
reat
oduo
dena
lar
tery
coil
ing
fail
ure
Sur
vive
d
4311
�C
aP
PP
D�
YS
MA
(IP
DA
)N
Ero
sive
SM
Am
ajor
bran
chin
suffi
cien
cyD
ied
448
�C
aW
R�
YS
MA
NE
rosi
onof
2su
peri
orm
esen
teri
car
tery
bran
ches
Die
d
456
�C
aW
R�
YS
MA
NS
uper
ior
mes
ente
ric
arte
ryps
eudo
aneu
rysm
Die
d
463
�C
PD
PP
HR
�Y
SM
AN
Infe
rior
panc
reat
oduo
dena
lar
tery
insu
ffici
ency
Sur
vive
d
4718
�21
��
Ca
WR
�Y
HA
N�
Hep
atic
arte
ryps
eudo
aneu
rysm
Die
d
(Con
tinu
ed)
Yekebas et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins274

loss evidenced by abdominal drains or to severe hemody-namic instability. In 27 patients, relaparotomy as rescuetreatment after failure of interventional endoscopy, interven-tional angiography, or both, was performed. This resulted,overall, in 27 patients (31%) who could successfully treatedby nonsurgical conservative monitoring and interventionalprocedures, while 60 patients (69%) required relaparotomy(Tables 1, 2).
Site and Onset of PPHFifty-one patients had extraluminal PPH, whereas 36
patients had intraluminal PPH. Fifty-three patients had earlyPPH, while in the remainder of 30 patients, PPH occurreddelayed. Seventeen of 34 patients who had extraluminal PPHuntil the fifth postoperative day had “true” extraintestinalbleeding sites due to insufficient hemostasis (eg, retroperito-neal and omental bleeding sites). These patients consistentlyunderwent relaparotomy. In 17 patients, however, PPH wasdue to primary intraluminal bleeding originating from thepancreaticoenteric anastomosis with secondary disruptionand subsequent bleeding into the abdominal cavity (“false”extraluminal PPH). Index operations in the latter subset wereduodenum-preserving pancreatic head resection (n � 11) orWhipple resection/PPPD (n � 6). In 16 patients, the pancre-aticoenteric anastomosis withstood elevated anastomoticpressure, hereby resulting in early intraluminal PPH originat-ing from the pancreatic transsection surface. In only 3 pa-tients who were treated by interventional endoscopy, earlyPPH at the first or second postoperative day was located at thegastroenteric or proximal enteroenteric anastomosis (Table2). Patients with “false” extraluminal PPH until the fifthpostoperative day, especially those who had undergoneDPPHR for chronic pancreatitis, showed a characteristicclinical feature differing considerably from PPH due to otherreasons: 1) in all but one patient, the leading primary symp-tom was an attack of acute, severe upper abdominal pain; 2)no association to pancreatic fistula prior to PPH was detectedin any case; 3) an alteration of abdominal drainage fluidsbeing serous first and becoming sanguineous in the furthercourse and/or hematemesis or melena occurred after a char-acteristic delay of at least 5 hours after the occurrence of pain;and 4) in none of these patients were complex vascularirregularities found angiographically or during relaparotomy.
The likelihood of devastating outcome due to severevascular abnormalities increased in patients with late extralu-minal as well as intraluminal PPH after the fifth postoperativeday (n � 17). Endoscopic intervention failed to achievebleeding control in any of these patients (Table 2).
Pancreatic FistulaIn the subset of the 87 patients with PPH, 34 (39%,) had
proven fistula prior to PPH, while in the entire cohort of 1669cases the overall pancreatic fistula rate was 9% (n � 185,P � 0.001). In 53 patients (61%), fistula did not precedePPH. In the latter subset, 9 patients developed pancreaticfistula subsequent to PPH due to a disruption of the pancre-aticoenteric anastomosis. The detailed analysis of patientdistribution revealed a significantly lower prevalence of fis-tula-associated PPH in patients with chronic pancreatitis (3 ofTA
BLE
2.(C
ontin
ued)
Pat
ient
No.
Ons
etof
PP
H(P
OD
)*
Sent
inel
PP
H(�
/�)
Und
erly
ing
Dis
ease
†In
dex
Ope
rati
on‡
Pan
crea
tic
Fis
tula
(�/�
)§
End
osco
py:
1st
Lin
eIn
terv
enti
onA
ngio
grap
hy:
1st/
2nd
Lin
eT
reat
men
t
Ble
edin
gSi
teA
sses
sed
Intr
aope
rati
vely
Out
com
e(s
urvi
ved/
died
)B
leed
ing
Site
Succ
ess
(Y/N
)P
PH
Vis
ible
(Y/N
)B
leed
ing
Site
Coi
ling
(Y/N
)Su
cces
s(Y
/N)
4822
�C
aW
R�
YH
AN
Hep
atic
arte
ry�
coel
ictr
unc
pseu
doan
eury
sm
Die
d
4928
�C
aP
PP
D�
YH
AN
Abs
cess
erod
ing
hepa
tic
arte
ryD
ied
509
�C
aP
PP
D�
YS
AN
Ero
sive
sple
nic
arte
ryin
jury
Die
d
Cha
ract
eris
tics
ofpa
tien
tsw
ith
PP
Hw
houn
derw
ent
inte
rven
tion
alen
dosc
opy,
radi
olog
y,or
both
.B
oth
pati
ents
wit
hsp
onta
neou
sce
ssat
ion
ofP
PH
(n�
4)an
dth
ose
unde
rgoi
ngpr
imar
yre
lapa
roto
my
are
not
incl
uded
inth
isan
alys
is(n
�33
).O
vera
ll,2
3pa
tien
tsco
uld
besu
cces
sful
lytr
eate
dei
ther
byin
terv
enti
onal
endo
scop
yor
radi
olog
y,re
spec
tive
ly.I
non
ly1
pati
ent(
10),
angi
ogra
phy
fail
edto
iden
tify
apo
tent
iall
yvi
sual
izab
lebl
eedi
ngso
urce
orig
inat
ing
from
the
righ
tgas
tric
arte
ry(“
fals
e”ne
gati
vean
giog
raph
y),w
hile
the
rate
oftr
eatm
entf
ailu
rein
pati
ents
unde
rgoi
ngco
ilin
gba
sed
onan
giog
raph
icev
iden
ceof
the
blee
ding
sour
ce(p
atie
nts
35–3
8),i
eex
clud
ing
pati
ents
unde
rgoi
ng“b
lind
”co
ilin
g,ac
coun
ted
for
25%
(4of
16).
Ove
rall
,8of
17pa
tien
tsw
hoha
dpr
imar
ily
intr
alum
inal
PP
Hw
ith
subs
eque
ntdi
srup
tion
ofth
epa
ncre
atic
ojej
unal
anas
tom
osis
mim
icki
ngan
extr
aint
esti
nal
blee
ding
site
(“fa
lse”
extr
alum
inal
PP
H)
coul
dbe
succ
essf
ully
trea
ted
byin
terv
enti
onal
coil
ing,
whe
reas
8pa
tien
tsun
derw
entr
elap
arot
omy.
In4
of17
pati
ents
wit
hse
vere
vasc
ular
path
olog
ies
(ero
sion
,pse
udoa
neur
ysm
),ra
diol
ogic
inte
rven
tion
succ
eede
din
achi
evin
gbl
eedi
ngco
ntro
l,w
hile
13pa
tien
tsre
quir
edre
lapa
roto
my.
GJA
indi
cate
sga
stro
jeju
nal
anas
tom
osis
;E
EA
,en
tero
ente
ric
anas
tom
osis
.*P
OD
indi
cate
spo
stop
erat
ive
day
wit
hre
spec
tto
the
inde
xop
erat
ion.
†C
ain
dica
tes
duct
alca
rcin
oma/
cyst
aden
ocar
cino
ma;
NE
T,n
euro
endo
crin
etu
mor
;BT
,bor
derl
ine
tum
or;I
PM
N,i
ntra
duct
alpa
pill
ary
muc
inou
sne
opla
sia,
muc
inou
scy
stad
enom
a,et
c.;F
P,f
ocal
chro
nic
panc
reat
itis
;CP
,chr
onic
panc
reat
itis
.‡W
Rin
dica
tes
Whi
pple
rese
ctio
n;P
PP
D,
pylo
rus-
pres
ervi
ngpa
rtia
lpa
ncre
atod
uode
nect
omy;
DS
P,
dist
alsp
leno
panc
reat
ecto
my;
SR
,se
gmen
tal
rese
ctio
n(b
ody)
;D
PP
HR
,du
oden
um-p
rese
rvin
gpa
ncre
atic
head
rese
ctio
n(e
xten
ded
drai
nage
proc
edur
e,F
rey
proc
edur
e,B
eger
proc
edur
e.§O
nly
thos
epa
ncre
atic
fist
ula
that
occu
rred
prio
rto
the
occu
rren
ceof
PP
H.
� Rep
etit
ive
angi
ogra
phy.
Annals of Surgery • Volume 246, Number 2, August 2007 Postpancreatectomy Hemorrhage
© 2007 Lippincott Williams & Wilkins 275

40; 7.5%) compared with those who had other pathologies(31 of 47; 66%; P � 0.001). PPH associated with precedingpancreatic fistula (n � 34) was lethal in 13 patients (38%). Incontrast, in the subgroup of 44 patients without pancreaticfistula, only one died due to PPH (P � 0.001).
Sentinel BleedThe overall prevalence of “sentinel” bleed was 33%
(n � 29). Relaparotomy rate associated with “sentinel” bleedwas 83% (24 of 29). Risk stratification according of whetherpatients with “sentinel” PPH additionally had pancreaticfistula (n � 20) or not showed that mortality in patients withsentinel bleed and concomitant fistula accounted for 57% (8among 14 patients with lethal course).
Interventional AngiographyIn 34 of 43 patients who underwent angiography, the
bleeding site could be localized. However, in 14 of thesepatients, interventional coiling was not feasible due to thedirect vicinity of the bleeding source to the hepatic artery orthe superior mesenteric artery. Further analysis showed thatnone of those 9 instances with negative angiographic findingshad bleeding episodes in their previous course, rendering atemporary cessation of a minor primary sentinel bleed inthese patients rather unlikely. Overall, interventional coilingwas performed in 25 patients (Table 2). Among these, in 20patients, the bleeding site had been angiographically visual-ized. In another 5 patients with chronic pancreatitis, “blind”coiling was performed despite the lack of definitive angio-graphic proof of the bleeding site because PPH was clinicallysuspected to originate from either the gastroduodenal arteryor the first 2 branches of the SMA. In 17 patients withextraluminal PPH evidenced via abdominal drains, the bleed-ing source was found to originate either from the resectioncavity after DPPHR or from the transsection surface afterWhipple resection and PPPD, respectively. Overall, in 8 ofthese patients, “false” extraluminal PPH due to a disruptionof the pancreaticojejunal anastomosis could be successfullytreated by interventional coiling, whereas 8 patients under-went relaparotomy (Tables 1, 2). Repetitive angiography wasperformed in 7 patients with hemodynamic stability at thetime of investigation and transfusion requirement �4 units/24hours. Overall, the success rate of radiologic coiling in termsof definitive hemostasis was 80% (n � 20), including 3patients in whom reangiography was successful (Fig. 2).Among 17 patients with erosive (“complex”) arterial pathol-ogies, 4 could be successfully treated by angiography (Table2). Interestingly, in patients without definitive angiographicvisualization in which, based on the surgeons suspicion,“blind” coiling of either superior or inferior pancreaticoduo-denal branches or the gastroduodenal artery itself was per-formed, interventional angiography was successful in 4among 5 patients, whereas only 1 patient required relapa-rotomy (Table 2).
The following bleeding sites were identified angio-graphically: hepatic artery (n � 4), stump or branches of thegastroduodenal artery or superior pancreaticoduodenal artery(n � 12), proximal branches of the SMA, ie, inferior pancre-
aticoduodenal artery (n � 14), and branches of the splenicartery (n � 4).
After successful bleeding control by interventional coil-ing, 3 patients were subjected to CT-guided interventionalplacement of additional drains close to the pancreaticojeju-nostomy due to considerable fluid collections not reached byabdominal drains. Analysis of fluid secretion in these 3patients confirmed significantly elevated pancreatic enzymeswith amylase activity ranging from 4 to 8 times the serumactivity.
Uncomplicated/Complex Arterial PathologiesIn case of arterial bleeding, PPH was classified accord-
ing to radiologic or intraoperative features either as “uncom-plicated” (n � 63) or “complex” (n � 17) depending on thepresence or absence of arterial erosions or pseudoaneurysms.PPH due to complex vascular pathologies differed consider-ably from uncomplicated bleedings. First, they occurred onlyin patients who had pancreatic fistula first. Second, they wereobserved only in patients who did not suffer from chronicpancreatitis, whereas no patient with chronic pancreatitisexperienced complex arterial erosions or pseudoaneurysmsirrespective from the kind of the index operation (duodenum-preserving procedures versus pylorus-preserving or classicWhipple resection). Last, fistula-associated complex arterialbleedings consistently occurred in a delayed fashion (lateonset PPH) with a peak at the 9th postoperative day (range,sixth to 32nd postoperative day). Conversely, in patients withpancreatic carcinoma without pancreatic fistula and in thosewith chronic pancreatitis, uncomplicated arterial bleedings
FIGURE 2. Definitive treatment of postpancreatectomy hem-orrhage. Endoscopy successfully achieved bleeding controlin only 3 patients with intraluminal PPH within the first andsecond postoperative day after the index operation. After-ward, even in case of intraluminal bleeding site, patientshad either to undergo interventional angiography orrelaparotomy.
Yekebas et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins276

peaked at the fourth postoperative day (range, first to 26thpostoperative day).
Interventional EndoscopyBecause of intraluminal PPH evidenced by apparent
blood loss through the nasogastric tube, 15 patients under-went endoscopy between the first to 15th postoperative day.In 3 patients (20%), all of which experienced PPH within thefirst 48 postoperative hours, endoscopy succeeded in localiz-ing and interventionally treating bleeding at the gastroentericor first enteroenteric anastomosis (Table 2). In the remainderof 12 patients with PPH after 48 hours, intraluminal bleedingwas located beyond endoscopic accessibility, eg, the pancre-aticojejunostomy or the second (distal) enteroenteric anasto-mosis (Fig. 2). These patients underwent either interventionalangiography (n � 8, successful in 2 patients) or relaparotomy(n � 10, Table 2).
RelaparotomyTen of 33 patients undergoing relaparotomy as first-line
treatment of PPH not only had pancreatic fistula but also anepisode of “sentinel” PPH in their previous postoperativecourse. Among the latter, 8 patients died due to disastrousvascular pathologies.
Relaparotomy, which was performed, overall, in 60patients either as first-line procedure or as rescue treatmentafter failure of interventional endoscopy or radiology (Fig. 2),revealed the following bleeding sites: hepatic and gastrodu-odenal arteries (n � 15), splenic artery (n � 3), branches ofthe superior mesenteric artery (n � 16), tributaries of theportal venous axis (n � 2), pancreatic resection surface orsuture line of the pancreaticoenteric anastomosis (n � 8),other anastomosis (n � 3), and other bleeding sites, eg, theretroperitoneal space (n � 13). Relaparotomy due to techni-cal infeasibility of interventional coiling consistently con-firmed bleeding sources identified in preceding diagnosticangiography (Table 2). Only 1 patient underwent relapa-rotomy, although bleeding control had been definitivelyachieved by interventional angiography. This patient who hada huge fluid collection in CT scans due to an insufficiency ofthe pancreaticojejunostomy underwent oversewing of theanastomosis and replacement of dislocated drains.
Thirteen of 17 patients with complex vascular pathol-ogies due to pancreatic fistula underwent relaparotomy en-compassing the following procedures: 1) completion pancre-atectomy with vascular reconstruction of the hepatic artery (n� 3) and the superior mesenteric artery (n � 1), 2) comple-tion pancreatectomy with suture ligating the bleeding source(n � 2), and 3) suture ligating the bleeding source withexternal drainage of pancreatic fistulas with (n � 3) orwithout (n � 4), repeated, planned peritoneal lavage.3
All patients with late PPH after the fifth postoperativeday (n � 17) had either pancreatic fistula or even an insuf-ficiency of the pancreaticoenteric anastomosis.
Overall OutcomeOverall mortality based on the analysis of 1669 pan-
creatic resections, including the 14 patients who died due toPPH accounted for 3% (n � 50). Stratifying patients for
presence or absence of PPH resulted in adjusted mortality of2.3% for patients without PPH (36 of 1582). PPH wasassociated with a mortality of 16% (14 of 87; P � 0.0001, �2
test), while it could be successfully treated in 73 patients(84%). Ten of 14 patients with lethal outcome suffered frompancreatic carcinoma, while the remainder had borderlinepathologies (eg, IPMN, cystadenoma) and focal pancreatitis.No patient with typical chronic pancreatitis involving theentire gland died due to PPH (Table 3). Twelve of 14 patientswith lethal course had complex vascular irregularities subse-quent to pancreatic fistula, ie, pseudoaneurysms and arterialerosions. Thirteen of 14 patients had pancreatic fistula. Initialbleeding severity was severe only in 6 patients, while 8 hadmild PPH. All patients who eventually died had delayed PPHoccurring earliest at the sixth postoperative day (Table 2),hereby resulting in a mortality in this subset of patients (n �30) of even 46.7%. Reasons of lethal outcome were asfollows: diffuse peritonitis (n � 7); hepatic failure (n � 3) inpatients with complex vascular erosions or pseudoaneurysmsof the hepatic artery and the celiac trunk; recurrent, surgicallyintractable PPH episodes (n � 2); pulmonary embolism (n �1); and fungal sepsis (n � 1).
DISCUSSIONDespite a reported prevalence of 5% to 12%,12–14 PPH
remains a diagnostic and therapeutic black box. Standardizedrules as to its management do not exist. Because of thediversity of bleeding types, PPH-associated outcome andmortality are unknown.6,9,15–17 Substantial differences in-clude the onset and intensity of PPH, underlying diseases,kind of index operations, concomitant pancreatic fistula, ex-traluminal or intraluminal manifestation of bleeding, pres-ence or absence of a “sentinel” bleed, and vascular irregular-ities, ie, devastating arterial erosions and pseudoaneurysms.With the aim to produce diagnostic and therapeutical algo-rithms for management of PPH, we retrospectively analyzeda prospective data base in which more than 1500 patientsoperated on for pancreatic pathologies have been includedfrom 1992 on. In particular, we sought to identify risk“profiles” according to the following criteria: 1) early versuslate onset of PPH; 2) presence or absence of concomitantpancreatic fistula; 3) underlying disease (pancreatic malig-nancy and borderline pathologies with “weak” pancreaticremnant texture versus chronic pancreatitis with “fibrotic”texture; and 4) kind of index operation. Taking these vari-ables into account, success rates of interventional endoscopicand radiologic procedures were evaluated.
The distinction of “early” and “late” PPH has an im-portant, if not even crucial impact on therapeutical manage-ment. Regardless of its intraluminal or extraluminal manifes-tation, early PPH is in most series reported to have muchbetter prognosis than does ominous late PPH.12,18 Based oninstitutional experiences, Choi et al18 and Tien et al7 sug-gested setting the cutoff for differentiating early and late PPHat the fifth and seventh postoperative day, respectively.
Early PPH in the presented series was due to 3 reasons:1) technical failures in terms of inadequate hemostasis in theoperative field always associated with extraluminal PPH; 2)
Annals of Surgery • Volume 246, Number 2, August 2007 Postpancreatectomy Hemorrhage
© 2007 Lippincott Williams & Wilkins 277

suture line of gastroenteric or one of the enteroenteric anas-tomosis leading uniformly to intraluminal PPH at the first orsecond postoperative day; and 3) resection cavity (chronicpancreatitis) or transsection surface (Whipple resection) ofthe pancreas resulting in PPH originating from the pancre-atico-enteral anastomosis. The latter bleeding origin was ofparticular interest because in only half (n � 17) of thesepatients it led, as would be expected, to intraluminal PPHwith hematemesis or melena. In the other half (n � 17), theintraluminal bleeding site became clinically apparent by ex-traluminal PPH, which resulted from a bursting of the pan-creaticojejunostomy. Therefore, because it only mimickedextraluminal PPH, we entitled this subset of bleedings “false”extraluminal PPH. Growing experience with these patientshas meanwhile prompted us to change our institutional policyfor management of early bleeding designating patients inwhom “false” extraluminal PPH is assumed to interventionalradiology first, whereas emergency relaparotomy is restrictedas a rescue procedure to patients in whom angiography failsor is technically not feasible.
A key finding of the presented analysis was that thelikelihood of devastating and in 14 patients lethal outcomeincreased the later PPH occurred. Since lethal courses wereonly observed in delayed PPH, “overall” mortality of 16% inthe entire cohort (n � 87) of patients with PPH is in somerespects misleading. When only those 30 patients with de-layed PPH were considered, its mortality was even 47%.
The core difference between early and delayed PPHafter the fifth postoperative day was the high coincidence ofdelayed PPH with preceding pancreatic fistula. This finding isconsistent with the surgical literature reporting significantlyelevated risk of delayed PPH in patients with pancreaticfistula18 as well as a near 100% prevalence of preliminarypancreatic fistula in patients who exhibit delayed arterialbleeding.12 Some surgical series suggest a sequel of events atthe beginning of which pancreatic fistula causes erosions,pseudoaneurysms, and other vascular irregularities, whicheventually result in disastrous bleeding.12,18,19
However, why, overall, only a paucity of patients withpancreatic fistula develops PPH remains enigmatic. Reasonsfor the discrepant prevalence of pancreatic fistula, which isstill the most frequent specific postoperative comorbidity andfistula-related PPH occurring with much lower likelihood,have not been clearly identified so far. Extended lymphade-nectomy in the course of oncologic resections, exocrinecompetency indicated by soft texture of the pancreatic rem-nant producing highly aggressive pancreatic juice, or insuf-ficient drainage of pancreatic fistula, respectively, may becofactors increasing the risk of fistula-induced vascular dam-age with consecutive bleeding. Regarding the prediction ofpostoperative pancreatic juice volume, assessment of preop-erative exocrine function may be helpful in identifying such“at-risk” patients, as suggested in one study.12
Also, the data reported here seem to confirm that thelikelihood of pancreatic fistula depends on the underlyingdisease. It is likely that pancreatic carcinoma patients with“competent” pancreatic remnant as to its excretory functionproduce more pancreatic juice with higher erosive potentialTA
BLE
3.In
fluen
ceof
the
Kind
ofIn
dex
Op
erat
ion,
Und
erly
ing
Dis
ease
s,Pa
ncre
atic
Fist
ula,
and
Vasc
ular
Path
olog
ies
onO
utco
me
ofPP
H
Inde
xO
pera
tion
Pre
vale
nce
ofP
PH
Pre
vale
nce
ofP
ancr
eati
cF
istu
laV
ascu
lar
Ero
sion
s/P
seud
oane
urys
ms
Mor
talit
y
Tot
alN
on-C
PC
PT
otal
Non
-CP
CP
Tot
alN
on-C
PC
PT
otal
Non
-CP
CP
WR
/PP
PD
/(s
ub)t
otal
PT
8%(4
4/54
2)8%
(37/
454)
8%(7
/88)
55%
(24/
44)
65%
(24/
37)
0%(0
/7)
30%
(13/
44)
35%
(13/
37)
—(0
/7)
27%
(12/
44)
32%
(12/
37)
—(0
/7)
DS
P3%
(4/1
16)
4%(4
/97)
0%(0
/19)
75%
(3/4
)75
%(3
/4)
—50
%(2
/4)
50%
(2/4
)—
50%
(2/4
)25
%(1
/4)
—
DP
PH
R5.
5%(3
4/62
3)5%
(2/3
8)5.
5%(3
2/58
5)12
%(4
/34)
50%
(1/2
)9.
4%(3
/32)
—(0
/34)
—(0
/2)
—(0
/32)
—(0
/34)
—(0
/2)
—(0
/32)
Oth
er*
1%(5
/388
)2%
(4/1
99)
0.5%
(1/1
89)
60%
(3/5
)75
%(3
/4)
0%(0
/1)
40%
(2/5
)50
%(2
/4)
—(0
/1)
20%
(1/5
)25
%(1
/4)
—(0
/1)
Ove
rall
5%(8
7/16
69)
6%(4
7/78
8)4.
5%(4
0/88
1)39
%(3
4/87
)66
%(3
1/47
)†7.
5%(3
/40)
20%
(17/
87)
36%
(17/
47)†
—(0
/40)
16%
(14/
87)
30%
(14/
47)†
—(0
/40)
Ove
rall
,the
anal
ysis
ofin
flue
nce
ofsu
rgic
alpr
oced
ures
and
unde
rlyi
ngdi
seas
eson
prev
alen
ceof
PP
Ham
ong
allp
atie
nts
unde
rgoi
ngm
ajor
panc
reat
icre
sect
ion
(n�
1669
)di
dno
tsho
wsi
gnifi
cant
diff
eren
ces
betw
een
pati
ents
wit
hch
roni
cpa
ncre
atit
is(C
P)
com
pare
dw
ith
othe
rpa
thol
ogie
s.H
owev
er,
prev
alen
ceof
panc
reat
icfi
stul
aan
dof
vasc
ular
path
olog
ies
was
sign
ifica
ntly
high
erin
pati
ents
wit
hno
n-C
Ple
sion
s,he
reby
resu
ltin
gin
aP
PH
-rel
ated
mor
tali
tyof
30%
inth
issu
bset
,whi
leno
neof
the
pati
ents
wit
hch
roni
cpa
ncre
atit
isdi
eddu
eto
PP
H.W
Rin
dica
tes
Whi
pple
rese
ctio
n;P
PP
D,p
ylor
us-p
rese
rvin
gpa
rtia
lpa
ncre
atod
uode
nect
omy;
PT
,pan
crea
tect
omy;
DS
P,d
ista
lsp
leno
panc
reat
ecto
my;
DP
PH
R,
duod
enum
-pre
serv
ing
panc
reat
iche
adre
sect
ion.
*Oth
erin
terv
enti
ons
incl
uded
“mod
ified
”D
PP
HR
(eg,
DP
PH
Rw
ith
cyst
ojej
unos
tom
yfo
rch
roni
cps
eudo
cyst
sin
volv
ing
the
body
and
tail
ofth
epa
ncre
as)
and
salv
age
oper
atio
ns(e
g,“r
edo”
-DP
PH
R,W
R/P
PP
D,s
ubto
tal/
tota
lpa
ncre
atec
tom
yaf
ter
trea
tmen
tfa
ilur
eof
prec
edin
gsu
rgic
alpr
oced
ures
)in
CP
pati
ents
,se
gmen
tal
rese
ctio
nfo
rbo
rder
line
lesi
ons
and
foca
lpa
ncre
atit
is,
and
com
plet
ion
panc
reat
ecto
my
for
loca
lre
curr
ence
ofm
alig
nanc
ies,
resp
ecti
vely
.†P
�0.
001
vs.
the
corr
espo
ndin
gva
lues
inC
Ppa
tien
ts.
Yekebas et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins278

than do chronic pancreatitis patients with excretory insuffi-ciency. Indeed, clinical experience seems to support theassumption that patients with oncological indications aremore “at risk” to develop fistula-associated PPH comparedwith chronic pancreatitis patients. In the Johns Hopkinsexperience based on a retrospective analysis of 1891 patientsundergoing pancreaticoduodenectomy, a soft texture of thepancreatic remnant was associated with a 20-fold increase infistula risk over patients with a medium or firm gland.20
Several other studies confirmed the crucial impact of paren-chymal texture on fistula formation.12,21–23 In the presentseries, the prevalence of fistula-related PPH in patients withpancreatic pathologies usually associated with a “physiolog-ical,” soft texture of the pancreatic remnant (carcinoma, NET,borderline tumors, etc.) was significantly higher (66%) thanin patients with a firm glandular texture due to chronicpancreatitis (7.5%). That these few (n � 3) chronic pancre-atitis patients had uniformly undergone duodenum-preservingpancreatic resections, while none of chronic pancreatitis pa-tients subjected to “oncologic” resections, ie, Whipple oper-ation or PPPD, had fistula-related delayed PPH suggested thatits occurrence was associated with the underlying diseaserather than with the kind of index operation. Further evidencethat a soft texture of the pancreatic remnant represents animportant risk factor for delayed PPH is provided by ourobservation that devastating (“complex”) arterial erosionsand pseudoaneurysms, which were the predominant cause forlethal outcome were never found in chronic pancreatitispatients but only occurred in patients operated on for otherreasons.
Last, fistula-related delayed PPH was closely related to“sentinel” bleed defined as insignificant amounts of bloodloss. Minor “sentinel” bleed may herald consecutive devas-tating arterial bleeding originating from pseudoaneurysms orvascular erosions.12 Its reported prevalence ranges from 30%to 100%.7,12,15,24 It has been emphasized that its timelydiagnosis may be essential to prevent fatal outcome,11 whichis confirmed by the presented data. Not only that the greatmajority of patients (83%) with sentinel bleed eventuallyrequired relaparotomy, but its presence considerably wors-ened prognosis of delayed PPH with an increase of mortalityfrom 38% associated with fistula-related PPH to 57% inpatients who additionally had sentinel bleed.
CONCLUSIONWe suggest a therapeutic algorithm, which is depicted
in the figure, and encompasses endoscopy, angiography, andsurgery for interventionally therapy for PPH. In particular, acustomized decision-making should consider the followingaspects:
1. Prognosis of PPH is closely associated with precedingpancreatic fistula. Therefore, devastating in some patients,lethal courses occur predominantly in late-onset PPH afterthe sixth postoperative day, while early PPH until the fifthpostoperative day carries a good prognosis.
2. Management of early PPH within the first 5 days follow-ing the index operation depends on whether bleeding islocated intraluminally or extraluminally. “True” extralu-
minal PPH is mostly due to insufficient hemostasis, occurswithin 24 to 48 hours postoperatively, and requires imme-diate relaparotomy without diagnostic delay. “False” ex-traluminal PPH resulting from disruption of the pancreati-coenteric anastomosis with subsequent evidence ofbleeding via abdominal drains has a reasonable chance tobe treated by interventional angiography.
3. Interventional endoscopy is only indicated within 2 to 3days after primary surgery when intraluminal PPH issuspected to originate from the gastroenteric or enteroen-teric anastomosis. Intraluminal PPH occurring in the laterpostoperative course is unlikely to originate from anasto-motic lesions, except for the pancreaticoenteric anastomo-sis and hence require either interventional angiography orrelaparotomy.
4. Interventional angiography is indicated for “false” extralu-minal PPH within the first 5 days following the indexoperation after exclusion of gastroenteric and enteroen-teric anastomotic bleeding sites by endoscopy. In case oflate PPH usually associated with pancreatic fistula forma-tion, angiography as first-line intervention should be per-formed irrespective of the intraluminal or extraluminal siteof bleeding.
5. In case of nonvisualizable PPH during index angiography,reangiography may be performed within 6 to 24 hourswhen patients remain hemodynamically stable with bloodrequirement �4 units. “Blind” coiling of branches of thegastroduodenal and superior mesenteric arteries may pro-vide bleeding control after duodenum-preserving pancre-atic head resections for chronic pancreatitis.
6. The coincidence of sentinel bleed prior to PPH and pan-creatic fistula is associated with a mortality of �50%.Angiographic evaluation in these patients should be per-formed with the awareness of this specific risk. Therefore,when interventional angiography fails to visualize thebleeding source or when coiling is technically not feasible,relaparotomy is usually mandatory, even in case of tem-porary cessation of PPH.
REFERENCES1. Izbicki JR, Bloechle C, Knoefel WT, et al. Surgical treatment of chronic
pancreatitis and quality of life after operation. Surg Clin North Am.1999;79:913–944.
2. Cameron JL, Pitt HA, Yeo CJ, et al. One hundred and forty-fiveconsecutive pancreaticoduodenectomies without mortality. Ann Surg.1993;217:430–435; discussion 435–438.
3. Buchler MW, Wagner M, Schmied BM, et al. Changes in morbidity afterpancreatic resection: toward the end of completion pancreatectomy.Arch Surg. 2003;138:1310–1314; discussion 1315.
4. Yeo CJ, Cameron JL, Sohn TA, et al. Six hundred fifty consecutivepancreaticoduodenectomies in the 1990s: pathology, complications, andoutcomes. Ann Surg. 1997;226:248–257; discussion 257–260.4
5. van Berge Henegouwen MI, Allema JH, van Gulik TM, et al. Delayedmassive haemorrhage after pancreatic and biliary surgery. Br J Surg.1995;82:1527–1531.
6. Trede M, Schwall G. The complications of pancreatectomy. Ann Surg.1988;207:39–47.
7. Tien YW, Lee PH, Yang CY, et al. Risk factors of massive bleedingrelated to pancreatic leak after pancreaticoduodenectomy. J Am CollSurg. 2005;201:554–559.
8. Miedema BW, Sarr MG, van Heerden JA, et al. Complications followingpancreaticoduodenectomy: current management. Arch Surg. 1992;127:945–949; discussion 949–950.
Annals of Surgery • Volume 246, Number 2, August 2007 Postpancreatectomy Hemorrhage
© 2007 Lippincott Williams & Wilkins 279

9. de Castro SM, Kuhlmann KF, Busch OR, et al. Delayed massivehemorrhage after pancreatic and biliary surgery: embolization or sur-gery? Ann Surg. 2005;241:85–91.
10. Veit J, Wente MN, Bassi C, et al. Postpancreatectomy hemorrhage(PPH): an International Study Group of Pancreatic Surgery definition(ISGPS). Surgery. In press.
11. Bassi C, Dervenis C, Butturini G, et al. Postoperative pancreaticfistula: an international study group (ISGPF) definition. Surgery.2005;138:8 –13.
12. Sato N, Yamaguchi K, Shimizu S, et al. Coil embolization of bleedingvisceral pseudoaneurysms following pancreatectomy: the importance ofearly angiography. Arch Surg. 1998;133:1099–1102.
13. Balladur P, Christophe M, Tiret E, et al. Bleeding of the pancreaticstump following pancreatoduodenectomy for cancer. Hepatogastroen-terology. 1996;43:268–270.
14. Halloran CM, Ghaneh P, Bosonnet L, et al. Complications of pancreaticcancer resection. Dig Surg. 2002;19:138–146.
15. Shankar S, Russell RC. Haemorrhage in pancreatic disease. Br J Surg.1989;76:863–866.
16. Rumstadt B, Schwab M, Korth P, et al. Hemorrhage after pancreatoduo-denectomy. Ann Surg. 1998;227:236–241.
17. Reber PU, Baer HU, Patel AG, et al. Life-threatening upper gastroin-
testinal tract bleeding caused by ruptured extrahepatic pseudoaneurysmafter pancreatoduodenectomy. Surgery. 1998;124:114–115.
18. Choi SH, Moon HJ, Heo JS, et al. Delayed hemorrhage after pancreati-coduodenectomy. J Am Coll Surg. 2004;199:186–191.
19. Munoz-Bongrand N, Sauvanet A, Denys A, et al. Conservative manage-ment of pancreatic fistula after pancreaticoduodenectomy with pancre-aticogastrostomy. J Am Coll Surg. 2004;199:198–203.
20. Lin JW, Cameron JL, Yeo CJ, et al. Risk factors and outcomes inpostpancreaticoduodenectomy pancreaticocutaneous fistula. J Gastroin-test Surg. 2004;8:951–959.
21. Popiela T, Kedra B, Sierzega M, et al. Risk factors of pancreatic fistulafollowing pancreaticoduodenectomy for periampullary cancer. Hepato-gastroenterology. 2004;51:1484–1488.
22. Muscari F, Suc B, Kirzin S, et al. Risk factors for mortality andintra-abdominal complications after pancreatoduodenectomy: multivar-iate analysis in 300 patients. Surgery. 2006;139:591–598.
23. Yang YM, Tian XD, Zhuang Y, et al. Risk factors of pancreatic leakageafter pancreaticoduodenectomy. World J Gastroenterol. 2005;11:2456–2461.
24. Brodsky JT, Turnbull AD. Arterial hemorrhage after pancreatoduode-nectomy: the ‘sentinel bleed. ’ Arch Surg. 1991;126:1037–1040.
Yekebas et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins280

ORIGINAL ARTICLES
Amylase Value in Drains After Pancreatic Resection asPredictive Factor of Postoperative Pancreatic Fistula
Results of a Prospective Study in 137 Patients
Enrico Molinari, MD, Claudio Bassi, Prof., Roberto Salvia, MD, PhD, Giovanni Butturini, MD, PhD,Stefano Crippa, MD, Giorgio Talamini, MD, Massimo Falconi, MD, and Paolo Pederzoli, Prof.
Background: The correlation of the amylase value in drains (AVD)with the development of pancreatic fistula (PF) is still unclear.Aim: The purpose of this study was to identify within the firstpostoperative day (POD1) the predictive role of different risksfactors, including AVD, in the development of PF.Patients and Methods: We prospectively investigated 137 patientswho underwent major pancreatic resections. PF was defined andgraded in accordance with the International Study Group on PF.Results: We considered 101 pancreaticoduodenectomies and 36distal resections. The overall incidence of PF (A, B, and C grades)was 19.7% and it was 14.8% after pancreaticoduodenectomy and33.3% after distal resection. All PF occurred in “soft” remnantpancreas. The PF developed in patients with a POD1 median AVDof 10,000 U/L, whereas patients without PF had a median AVD of1222 U/L (P � 0.001). We established a cut-off of 5000 U/L POD1AVD for univariate and multivariate analysis. The area under thereceiver operating characteristic (ROC) curve was 0.922 (P �0.001). The predicting risk factors selected in the univariate settingwere “soft” pancreas (P � 0.005; odds ratio �OR�: 1.54; 95% CI:1.32–1.79) and AVD (P � 0.001; OR: 5.66; 95% CI: 3.6–8.7;positive predictive value 59%; negative predictive value 98%),whereas in multivariate analysis the predicting risk factor was thePOD1 AVD (P � 0.001; OR: 68.4; 95% CI: 14.8–315). Only 2 PFswere detected with AVD �5000 U/L and both were in pancreato-gastric anastomosis (P � 0.053).Conclusions: AVD in POD1 �5000 U/L is the only significantpredictive factor of PF development.
(Ann Surg 2007;246: 281–287)
Pancreaticoduodenectomy (PD) and distal pancreatic resec-tion (DP) are now standardized interventions for benign
and malignant pancreatic lesions. Because of recent improve-ments in surgical techniques and perioperative management,the incidence of mortality and morbidity have decreased,even if the latter is still around 20% to 50% in high volumecenters.1–22 The most frequent postoperative complicationis pancreatic fistula (PF), which is often associated withabdominal collections, abscesses, sepsis, and hemorrhage,with the necessity of reintervention, extended hospitaliza-tion, and postoperative mortality in 40% of cases withcomplications.1– 8
Despite its importance, PF has still not been uniformlydefined.12,13 Recently, the International Study Group on Pan-creatic Fistula (ISGPF)13 established that the most appropri-ate PF definition and grading should be based on the clinicalimpact of PF-related complications. In addition, there are stillno reliable correlations between the output of drains and theirconcentration of amylase contained within, which is usefulfor the diagnosis of chemical PF; moreover only a few studieshave attempted to correlate the concentration of amylase indrain fluid with the risk of developing complications.23–26
In the present study we examined, within the firstpostoperative day (POD1), the predictive role of differentrisks factors, including the value of amylase in drains in thedevelopment of PF.
PATIENTS AND METHODSAt the Department of Surgical and Gastroenterological
Sciences at the University of Verona, 137 consecutive pa-tients who underwent pancreatic resection (101 PD and 36DP) between April 2005 and February 2006 were admitted tothe study. In all patients daily drainage output and drain fluidquality, and the levels of serum and drain fluid amylase weredetermined starting from POD1 to POD5. If the drains hadnot been removed, then measurements were also made onPOD7 and POD9. For measurement of amylase, 10 mL ofliquid was used. The upper limit of normal serum amylase inour laboratory is 100 U/L.
Patient demographics, histology, type of intervention,surgical operator, type of pancreatic anastomosis (ie, pancre-atojejunal anastomosis �PJ�, pancreatogastric anastomosis�PG�), risk factors for PF (diameter of main pancreatic duct
From the Department of Surgery and Gastroenterology, University of Ve-rona, Italy.
Supported by Fondazione Cariverona, Fondazione Zanotto Verona, MIURCofin 2005060715_004.
Reprints: Claudio Bassi, MD, Department of Surgery and Gastroenterology,Hospital “GB Rossi” University of Verona, Piazzale LA Scuro, 10,37134 Verona, Italy. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0281DOI: 10.1097/SLA.0b013e3180caa42f
Annals of Surgery • Volume 246, Number 2, August 2007 281

�3 mm or �3 mm, soft or hard pancreatic texture, andduration of operation),14–17 and days of postoperative lengthof stay were recorded. In the postoperative period the devel-opment of complications (PF, abdominal hemorrhage, de-layed gastric emptying, acute pancreatitis of the pancreaticstump, enteric drainage from bedsore fistula), percutaneousdrainage of abdominal collections, reintervention, readmis-sion to the hospital, and mortality were collected. The defi-nitions of the complications are provided in Table 1. Thedefinition of PF used was that proposed by the ISGPF. Agrading system was also used (A, B, and C)13 and, whenindicated, a fistulography was performed.
All patients were administered preoperative antibioticprophylaxis with amoxicillin plus clavulanic acid (2.4 g);antithrombic prophylaxis was given for 30 days (low molec-ular weight heparin, 0.4 mL subcutaneously once a day). Inpatients undergoing PD octreotide prophylaxis was also given(0.1 mg subcutaneously for 3 times/24 h for 5 days afterintervention).27
Surgical TechniqueFor PD a pylorus-preserving resection (PPPD) was
performed in 91 cases (90%) whereas a Whipple resectionwas done in 10 cases (10%). The surgical operator was freeto choose the type of anastomosis. During PG the anastomo-sis was performed on the posterior wall of the stomach in asingle layer with nonresorbable button sutures with an ante-rior gastrostomy.28 PJ was performed in a single layer withnonresorbable button sutures. In both types of reconstructions2 “easy-flow” drains (12 mm; Chimed R Livorno, Italy) werepositioned, one behind the pancreatic anastomosis and theother at the level of the biliary anastomosis. DP was per-formed by using a TIA mechanical stapler to suture the distalshear. An “easy flow” drain (12 mm; Chimed R Livorno,Italy) was positioned near the pancreatic stump.
Statistical AnalysisNonparametric tests (Kruskal-Wallis, Mann-Whitney
U) were used to evaluate ordinal data, while a �2 test wasused for nominal data. Yate’s continuous correction in a2-way contingency table or Fisher exact test was used in thecase of a small expected frequency. Study of potential prog-nostic factors for PF was carried out by employing logisticanalysis; only variables available within 24 hours after inter-vention were considered. The diagnosis or lack thereof of aPF within the postsurgical observation was considered as a
dependent dichotomy variable. The process that led to theidentification of the most parsimonious model was performedusing a backward technique by elimination of a variable thatdid not reach a P � 0.05 according to Wald’s test. The oddsratios are presented with the respective confidence intervalsto 95%. For logistic regression analysis, the amylase drainvalue in POD1 was considered as a continuous value; then foreasier reading of the data an arbitrary cut-off in POD1 wasinserted (70th percentiles corresponding to 5000 U/L). SPSS(rel. 13) programs were used for statistical analysis (SPSSInc., Chicago, IL).
RESULTSOf the 137 consecutive patients enrolled in the study,
101 underwent PD (73.6%) (PJ 78, PG 23) and 36 DP. Therewere 71 males (51.8%; mean age 58.5 � 12.7 years) and 66females (mean age 56 � 12.5 years). For DP the mean timeof intervention was 194 � 19 minutes, while for PD the meaninterventional time was 346 � 36.8 minutes. The indicationsfor surgical resection are described in Table 2. In PD thepancreatic texture of the stump was “soft” in 71 cases (52 PJand 19 PG), whereas the diameter of the main pancreatic ductwas divided into 2 groups according to the risk of developingPF (�3 mm; �3 mm).15 There were 39 cases (38.6%) with adiameter �3 mm and 62 (61.4%) with a diameter �3 mm.Abdominal complications were recorded in 47 cases (34%),31.6% in PD, and 41% in DP.
The most frequent abdominal complication was clini-cally suspected PF, observed in 27 patients (19.7%): 15patients (14.8%) who underwent PD (10 PJ, 5 PG) and 12
TABLE 1. Definitions of Abdominal Complications After Pancreatic Resection
Type of Complication Clinical Definition
Pancreatic fistula Output rich in amylase content confirmed by fistulography. Stadiation by ISGPF.
Abdominal collection Collection of fluid measuring at least 5 cm in diameter, diagnosed with CT scan ultrasound.
Hemorrhage Requirement of �3 units of pRBCs (1000 mL) 24 h after the operation.
Delayed gastric emptying Need to retain nasogastric tube decompression for �10 d.
Enteric fistula Persistent enteric secretions for more after POD5 with drain into intestinal loop of the anastomosed Rouxwith the pancreas confirmed by fistulography.
Acute pancreatitis At least a 3-fold increase of normal plasma amylase or lipase values 48 h after the operation confirmedby CT scan or clinical course.
TABLE 2. Indications for Pancreatic Resection
Final Diagnosis Total N (%) PD (%) DP (%)
Ductal adenocarcinoma 49 (35.7) 45 (44) 4 (11.1)
Adenocarcinoma of the papilla 10 (7.3) 10 (10) 0
Endocrine neoplasia 14 (10.2) 8 (8) 6 (16.6)
Intraductal mucinous neoplasm 14 (10.2) 8 (8) 6 (16.6)
Duodenal neoplasm 7 (5.1) 7 (7) 0
Neoplasm of the biliary tract 4 (3.1) 4 (4) 0
Cystic neoplasm 22 (16) 6 (6) 16 (44.6)
Duodenal cystic dystrophy 7 (5.1) 7 (7) 0
Other 10 (7.3) 6 (6) 4 (11.1)
Total 137 (100) 101 (100) 36 (100)
Molinari et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins282

(33.3%) who underwent DP. Considering the ISGPF grading,PF were classified as follows: 12 grade A (5 PD, 7 DP); 11grade B (6 PD, 5 DP); and 4 grade C (4 PD, 0 DP). Theincidence of PF with clinically significant impact (grade B �C) was therefore present in 15 patients (10.9%): 10 (9.9%)after PD and 5 (13.8%) after DP.
Abdominal collections were present in 15 patients(11%) requiring interventional radiologic procedures in 6cases. An enteric drainage bedsore fistula was present in 8cases (7.9% of patients undergoing PD), and in all cases thepancreatic texture was “soft.” A reoperation was performedin 6 cases (4%): 5 for hemorrhage (4 PD and 1 DP) and 1 forsepsis following a complete dehiscence of the pancreaticanastomosis. Acute pancreatitis of the pancreatic stump waspresent in 19 cases undergoing PD (13.6%; 10 PJ and 9 PG),which in 5 cases was associated with PF (3 grade B and 2grade C). Overall complications are reported in Table 3.There was no mortality.
The median of the level of amylase in pancreatic drainstended to decrease from POD1 to POD5 (Fig. 1) in patients
with normal postoperative recovery as well as in those with acomplicated postoperative course. Although the amylase lev-els were higher in the latter group of patients, this differencewas not statistically significant.
In univariate analysis, the median value of amylase indrains on POD1 was 1222 U/L (10th and 90th percentiles:14–10,400 U/L) in patients who did not develop PF and10,000 U/L (10–90 percentiles: 2849–74,800 U/L) in pa-tients who developed PF (P � 0.001) (Table 4). This differ-ence was independent of the type of intervention, the type ofpancreas in PD (soft or hard, P � 0.001), and diameter ofmain pancreatic duct (�3 mm and �3 mm, P � 0.001). Themedian difference of the level of amylase on POD1 was notstatistically significant in the PG group (P � 0.053). More-over, in univariate analysis, the presence of PF was signifi-cantly dependent on the “soft” texture of pancreas (P �0.005; OR: 1.54; 95% CI: 1.32–1.79) and value of amylase indrains on POD1 (P � 0.001). For all analyses only thoseparameters available within the first postoperative day wereconsidered.
The univariate analysis was repeated by inserting avalue of amylase at 5000 U/L in drains on POD1 as anarbitrary cut-off value (70th percentile). Even in this case theconcentration of amylase was the variable selected (P �0.001; OR: 5.66; 95% CI: 3.6–8.7).
For logistic regression analysis the dependent di-chotomic variable considered was the development of PF,whereas the independent variables with a potential prognosticsignificance were gender, age, concentration of amylase indrains in POD1, drainage output, serum amylase, type ofintervention, type of pancreatic texture, diameter of mainpancreatic duct, surgical operator, and acute postoperativepancreatitis. The only significant variable was the quantityof amylase in the left drain (that placed near the pancreaticstump) on POD1 (P � 0.001; OR: 68.4; 95% CI: 14.8 –315) without relationship with high or low amylase serumlevel.
TABLE 3. Types of Complications in 137 PancreaticResections
Type of Complication N %
Abdominal collection 15 11
Pancreatic fistula 27 19.7
Grade A 12 8.7
Grade B 11 8
Grade C 4 2.9
Enteric fistula 8 7.9
Acute pancreatitis 19 13.6
Delayed gastric emptying 8 5.8
Percutaneous drainage 6 4.3
Readmission to hospital 4 2.9
Reoperation 6 4.3
Mortality 0 0
FIGURE 1. Median values of amylase in drainsduring postoperative recovery. Vertical barsshow 25th and 75th percentiles.
Annals of Surgery • Volume 246, Number 2, August 2007 AVD as Predictive Factor of Pancreatic Fistula
© 2007 Lippincott Williams & Wilkins 283
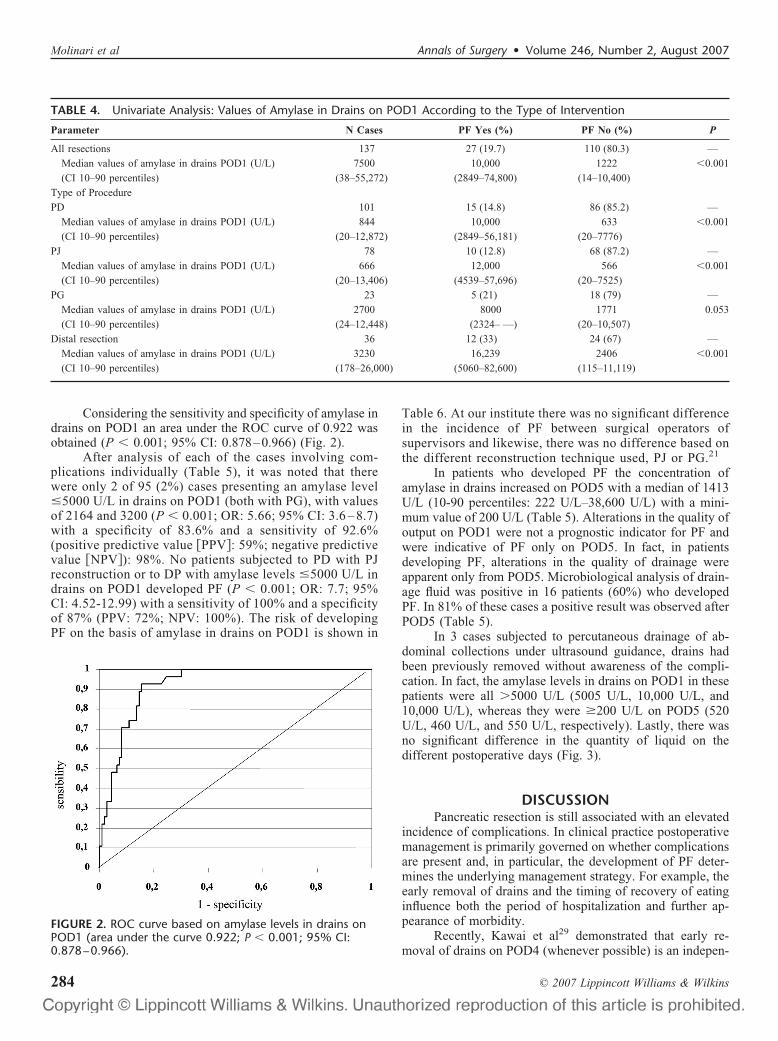
Considering the sensitivity and specificity of amylase indrains on POD1 an area under the ROC curve of 0.922 wasobtained (P � 0.001; 95% CI: 0.878–0.966) (Fig. 2).
After analysis of each of the cases involving com-plications individually (Table 5), it was noted that therewere only 2 of 95 (2%) cases presenting an amylase level�5000 U/L in drains on POD1 (both with PG), with valuesof 2164 and 3200 (P � 0.001; OR: 5.66; 95% CI: 3.6 – 8.7)with a specificity of 83.6% and a sensitivity of 92.6%(positive predictive value �PPV�: 59%; negative predictivevalue �NPV�): 98%. No patients subjected to PD with PJreconstruction or to DP with amylase levels �5000 U/L indrains on POD1 developed PF (P � 0.001; OR: 7.7; 95%CI: 4.52-12.99) with a sensitivity of 100% and a specificityof 87% (PPV: 72%; NPV: 100%). The risk of developingPF on the basis of amylase in drains on POD1 is shown in
Table 6. At our institute there was no significant differencein the incidence of PF between surgical operators ofsupervisors and likewise, there was no difference based onthe different reconstruction technique used, PJ or PG.21
In patients who developed PF the concentration ofamylase in drains increased on POD5 with a median of 1413U/L (10-90 percentiles: 222 U/L–38,600 U/L) with a mini-mum value of 200 U/L (Table 5). Alterations in the quality ofoutput on POD1 were not a prognostic indicator for PF andwere indicative of PF only on POD5. In fact, in patientsdeveloping PF, alterations in the quality of drainage wereapparent only from POD5. Microbiological analysis of drain-age fluid was positive in 16 patients (60%) who developedPF. In 81% of these cases a positive result was observed afterPOD5 (Table 5).
In 3 cases subjected to percutaneous drainage of ab-dominal collections under ultrasound guidance, drains hadbeen previously removed without awareness of the compli-cation. In fact, the amylase levels in drains on POD1 in thesepatients were all �5000 U/L (5005 U/L, 10,000 U/L, and10,000 U/L), whereas they were �200 U/L on POD5 (520U/L, 460 U/L, and 550 U/L, respectively). Lastly, there wasno significant difference in the quantity of liquid on thedifferent postoperative days (Fig. 3).
DISCUSSIONPancreatic resection is still associated with an elevated
incidence of complications. In clinical practice postoperativemanagement is primarily governed on whether complicationsare present and, in particular, the development of PF deter-mines the underlying management strategy. For example, theearly removal of drains and the timing of recovery of eatinginfluence both the period of hospitalization and further ap-pearance of morbidity.
Recently, Kawai et al29 demonstrated that early re-moval of drains on POD4 (whenever possible) is an indepen-
TABLE 4. Univariate Analysis: Values of Amylase in Drains on POD1 According to the Type of Intervention
Parameter N Cases PF Yes (%) PF No (%) P
All resections 137 27 (19.7) 110 (80.3) —
Median values of amylase in drains POD1 (U/L) 7500 10,000 1222 �0.001
(CI 10–90 percentiles) (38–55,272) (2849–74,800) (14–10,400)
Type of Procedure
PD 101 15 (14.8) 86 (85.2) —
Median values of amylase in drains POD1 (U/L) 844 10,000 633 �0.001
(CI 10–90 percentiles) (20–12,872) (2849–56,181) (20–7776)
PJ 78 10 (12.8) 68 (87.2) —
Median values of amylase in drains POD1 (U/L) 666 12,000 566 �0.001
(CI 10–90 percentiles) (20–13,406) (4539–57,696) (20–7525)
PG 23 5 (21) 18 (79) —
Median values of amylase in drains POD1 (U/L) 2700 8000 1771 0.053
(CI 10–90 percentiles) (24–12,448) (2324– —) (20–10,507)
Distal resection 36 12 (33) 24 (67) —
Median values of amylase in drains POD1 (U/L) 3230 16,239 2406 �0.001
(CI 10–90 percentiles) (178–26,000) (5060–82,600) (115–11,119)
FIGURE 2. ROC curve based on amylase levels in drains onPOD1 (area under the curve 0.922; P � 0.001; 95% CI:0.878–0.966).
Molinari et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins284

dent factor for reducing the incidence of abdominal infec-tions; patients with drains still in place after POD8 had asignificantly higher incidence of abdominal complications ingeneral (P � 0.00003) and PF (P � 0.003), suggesting thatinfection of drains occurs around POD7 (positive cultures in94% in patients in which the drain was not removed; OR: 6.7;95% CI: 1.9–22.7). These data were also confirmed in thepresent study, since 81% of infected drains were revealedafter POD5 in cases that developed PF.
In the literature there are few studies that have at-tempted to evaluate the predictive value of amylase in drainswith the risk of developing PF, despite the fact that amylasevalues significantly influence postoperative management.23,26
The retrospective study by Shinchi et al26 on 207 PD defined
pancreatic leak as an output �30 mL/24 h with amylasevalues on POD5 that were more than 5 times the serum value.Using this definition, a positive biochemical predictive value(59%) was not sufficient to justify the incidence of PFreported (29 cases, 14%). Likewise, the study by Shyr et al23
on 37 PD and with the development of a single case of PFwith amylase in drains on POD7 of 74 U/L provides littleinsight into the physiological mechanisms of complications.Only a single study25 with a small patient cohort (n � 26) anda high incidence of PF (46%) reported a mean level ofamylase in drains on POD1, 10,878 � 14,800 U/L in caseswith complications compared with 1482 � 1615 U/L(maximal level 4838 U/L) in cases without complications(P � 0.01).
TABLE 6. Risk of Developing Pancreatic Fistula According to Amylase Levels in Drains on POD1 (cut-off 5000 U/L)
PF Yes PF No OR 95% CI P SP SE PPV NPV
All resections 27 110 5.66 3.6–8.7 �0.001 83.6% 92.6% 59% 98%
PD 15 86 5.32 3.1–8.9 �0.001 83.7% 86.7% 48% 97%
PJ 10 68 8.5 4.4–16.3 �0.001 88.2% 100% 56% 100%
PG 5 18 1.8 0.7–4.7 0.053 66% 60% 32% 86.2%
DP 12 24 6 2.4–14.7 �0.001 83% 100% 75% 100%
SP indicates specificity; SE, sensitivity; PPV, positive predictive value; NPV, negative predictive value.
TABLE 5. Characteristics of Patients Developing Pancreatic Fistula in 137 Pancreatic Resections
N CasesValues of Amylase inDrains POD1 (U/L)
Values of Amylase inDrains POD5 (U/L)
Type ofProcedure
POD DrainageFluid Culture
DrainageFluid Culture
1 2164 340 PD (PG) 7 Escherichia coli
2 3200 640 PD (PG) 5 Enterococcus faecalis
3 5005 490 DP 18 Staphylococcus aureus
4 5162 200 PD (PJ) 6 E. coli
5 5200 665 DP 6 S. aureus
6 6336 300 DP 5 Neg.
7 6991 200 PD (PJ) 6 Enterococcus cloacae
8 8000 2958 PD (PG) 14 Enterococcus avium
9 8905 618 DP 5 Neg.
10 9370 1673 PD (PG) 7 Enterococcus faecalis
11 10,000 530 PD (PJ) 7 Enterococcus avium
12 10,000 3140 DP 7 E. coli
13 10,257 1413 PD (PJ) 7 Neg.
14 10,800 550 PD (PJ) 8 Neg.
15 13,200 421 PD (PJ) 7 E. coli
16 14,478 430 DP 5 Neg.
17 14,500 318 PD (PG) 10 Klebisiella
18 15,000 430 PD (PJ) 6 Neg.
19 15,264 416 PD (PJ) 5 Neg.
20 18,000 1000 DP 20 S. aureus
21 18,141 2307 DP 5 Neg.
22 28,000 31,000 DP 5 Enterococcus faecalis
23 40,000 919 DP 5 Neg.
24 42,000 1900 DP 7 Neg.
25 55,000 2234 PD (PJ) 10 S. aureus
26 58,000 6390 PD (PJ) 5 Serratia
27 1,000,000 50,000 DP 5 Neg.
Neg. indicates no bacterial growth.
Annals of Surgery • Volume 246, Number 2, August 2007 AVD as Predictive Factor of Pancreatic Fistula
© 2007 Lippincott Williams & Wilkins 285

The present study demonstrates that, among all of thedifferent risk factors within the POD1 in the development ofPF, only the level of amylase in drains on POD1 has apredictive value for the appearance of PF, and in particularwhen the level of amylase is greater than 5000 U/L (P �0.001; OR: 5.66; 95% CI 3.6–8.7) with a sensitivity of 92.6%and a specificity of 83.6% (PPV: 59%; NPV: 98%). Consid-ering patients undergoing PD, no PF occurred in those withPJ and amylase in drains on POD1 �5000 U/L (P � 0.001;OR: 8.5; 95% CI: 4.4–16.3) with a sensitivity of 100% and aspecificity of 88.2% (PPV: 56%; NPV: 100%); however, 2patients who were reconstructed with PG developed PF.Therefore, this stresses the utility of amylase levels on POD1,especially in cases with PJ anastomosis, whereas the amylaselevels did not reach statistical significance for PG (P �0.053), perhaps because of the small number of patients (n �23). In the group of patients who underwent DP, the inci-dence of PF was 33% among those presenting amylase levels�5000 U/L on POD1 (P � 0.001; OR: 6; 95% CI: 2.45–14.7)with a sensitivity of 100% and a specificity of 83% (PPV:75%; NPV: 100%). Independently on the normal serumamylase level range, in our experience, the value of amylasedrain level on POD1 �5000 U/L has to be considered inabsolute terms. Moreover, the value we found is close to that(4838 U/L) reported by Hashimoto and Ohyanagi in a smallerseries.25
In agreement with the results of Wada and Traverso,this would suggest that amylase levels on POD1 are increasedin patients who will develop complications due to an earlyand imperceptible leak of the anastomosis.30 During thesuccessive postoperative recovery period, the pancreas seemsto decrease in terms of functionality, thereafter increasing onPOD5 (Fig. 1). As hypothesized by Shinchi et al, the increase
in amylase in drains during this period may be due to thestimulus provided by realimentation.26 We therefore com-pared the amylase levels in drains before and after realimen-tation. In the 27 cases of PF observed, in 9 patients (33%)there was an increase in amylase levels in drains afterrealimentation; thus only in a subgroup of cases amylaselevels might be correlated with realimentation.
Lastly, if we consider that in the group of patients thatpresented amylase levels �5000 U/L (25 of 42 cases) onlythose with amylase levels �200 U/L on POD5 developedcomplications (Table 5). In those patients reconstructed withPJ after PD and treated with DP (114 cases in total), PFdeveloped when amylase levels on POD1 were �5000 U/L(P � 0.001; OR: 7.7; 95% CI: 4.52-13) with a sensitivity of100% and a specificity of 87% (PPV: 72%; NPV: 100%).
Considering the results of this study, the physiopatho-logic mechanism of the development of PF appears in the firstinstance because of a small intraoperative leak that wouldexplain the presence of amylase in drains on POD1 �5000U/L, with a small ischemic necrosis of the anastomosis onPOD5 (amylase �200 U/L). Moreover, from this study it canbe inferred that the quantity of liquid drained is not anessential parameter in defining PF (Fig. 3).
Other studies23–26 do not confirm the results reportedherein, which may be due to a number of factors includingsurgical technique and management of the pancreatic stump(duct-to-mucosa pancreaticojejunostomy, anastomosis per-formed in double or triple layers, and use of a stent in theWirsung duct) and by the different types of abdominal drainsused (closed suction drains or soft easy flow). Surprisingly,no authors have cited the problem of enteric fistula frombedsore drainage,2,21,22 which was observed in our experi-ence between POD5 and POD7 in patients with amylaselevels on POD1 �5000 U/L, and in 8 cases (7.9%) of thoseundergoing PD. It should be stressed that only fistulographyreveals drainage inside the intestinal loop of the anastomosedRoux with the pancreas, and for this reason fistulography isalways performed at our institution when there is the clinicalsuspicion of fistula; in cases with fistula from bedsores, oncethe drain is mobilized under endoscopic guidance, the com-plication resolves within 48 hours in all cases. Lastly, this isthe first prospective study to value amylase content in drainsusing the ISGPF definition and grading system. It should thusbe evident how all of these different factors can influence theoptimal time for the removal of drains.
The mortality rate we report in this cohort of 137 majorresections is nil. Currently, the overall mortality rate for PDin our unit is less than 1% despite the still high morbidityrate.2,21–22,28 This seems to be a common experience, even inother “high volume” centers around the world. In general, we allare approaching a 0 rate of mortality because of our capability tomanage the still high complications rate.1,3–6,10,14–19,27,29,30
As a consequence, we must be careful in changing ouractual drain management, basing each single variation in theprotocols only on the evidence. The data reported in thepresent article have been the background of a prospectiverandomized clinical trial on drain management that is runningin our unit. Such a trial, on the base of amylase drain POD1
FIGURE 3. Median postoperative liquid output in drains.Vertical bars show 25th and 75th percentiles.
Molinari et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins286

value, compares our standard drain management versus anearlier drain withdrawal.
In conclusion, the present study indicates how it ispossible to identify the risk of PF formation on POD1 byanalysis of amylase levels in drains. This possibility opensnew frontiers in postoperative management. In fact, it ispossible to identify a subgroup of patients at high risk fordeveloping complications (POD1 amylase levels �5000 U/L)in which the patient may benefit from lengthening the time ofintensive postoperative therapy including prolonged fastingand “in situ” drainage (Table 6). On the other hand, thosepatients not at risk (NPV 98% on all the pancreatic resectionprocedures) may be candidates for earlier removal of drains,thus avoiding infections, bedsore lesions, and favoring fasterrealimentation and discharge from the hospital.29
REFERENCES1. Yeo CJ, Cameron JL, Sohn TA, et al. Six hundred fifty consecutive
pancreaticoduodenectomies in the 1990s: pathology, complications, andoutcomes. Ann Surg. 1997;226:248–257.
2. Bassi C, Falconi M, Salvia R, et al. Management of complications afterpancreaticoduodenectomy in a high volume centre: results on 150consecutive patients. Dig Surg. 2001;18:453–457.
3. Balcom JH 4th, Rattner DW, Warshaw AL, et al. Ten-year experiencewith 733 pancreatic resections: changing indications, older patients, anddecreasing length of hospitalization. Arch Surg. 2001;136:391–398.
4. Bottger TC, Junginger T. Factors influencing morbidity and mortalityafter pancreaticoduodenectomy: critical analysis of 221 resections.World J Surg. 1999;23:164–171.
5. Cameron JL, Pitt HA, Yeo CJ, et al. One hundred and forty-fiveconsecutive pancreaticoduodenectomies without mortality. Ann Surg.1993;217:430–435.
6. Gouma DJ, van Geenen RC, van Gulik TM, et al. Rates of complicationsand death after pancreaticoduodenectomy: risk factors and the impact ofhospital volume. Ann Surg. 2000;232:786–795.
7. Lillemoe KD, Kaushal S, Cameron JL, et al. Distal pancreatectomy:indications and outcomes in 235 patients. Ann Surg. 1999;229:693–698.
8. Balzano G, Zerbi A, Cristallo M, et al. The unsolved problem of fistulaafter left pancreatectomy: the benefit of cautious drain management.J Gastrointest Surg. 2005;9:837–842.
9. Sheehan MK, Beck K, Creech S, et al. Distal pancreatectomy: does themethod of closure influence fistula formation? Am Surg. 2002;68:264–267.
10. Buchler MW, Friess H, Wagner M, et al. Pancreatic fistula afterpancreatic head resection. Br J Surg. 2000;87:883–889.
11. Knaebel HP, Diener MK, Wente MN, et al. Systematic review andmeta-analysis of technique for closure of the pancreatic remnant afterdistal pancreatectomy. Br J Surg. 2005;92:539–546.
12. Bassi C, Butturini G, Molinari E, et al. Pancreatic fistula rate afterpancreatic resection. The importance of definitions. Dig Surg. 2004;21:
54–59.13. Bassi C, Dervenis C, Butturini G, et al. International Study Group on
Pancreatic Fistula Definition. Postoperative pancreatic fistula: an inter-national study group (ISGPF) definition. Surgery. 2005;138:8–13.
14. Sato N, Yamaguchi K, Chijiiwa K, et al. Risk analysis of pancreaticfistula after pancreatic head resection. Arch Surg. 1998;133:1094–1098.
15. Yang YM, Tian XD, Zhuang Y, et al. Risk factors of pancreatic leakageafter pancreaticoduodenectomy. World J Gastroenterol. 2005;11:2456–2461.
16. Popiela T, Kedra B, Sierzega M, et al. Risk factors of pancreatic fistulafollowing pancreaticoduodenectomy for periampullary cancer. Hepato-gastroenterology. 2004;51:1484–1488.
17. Adam U, Makowiec F, Riediger H, et al. Risk factors for complicationsafter pancreatic head resection. Am J Surg. 2004;187:201–208.
18. De Castro SM, Busch OR, van Gulik TM, et al. Incidence and manage-ment of pancreatic leakage after pancreatoduodenectomy. Br J Surg.2005;92:1117–1123.
19. Marcus SG, Cohen H, Ranson JH. Optimal management of the pancre-atic remnant after pancreaticoduodenectomy. Ann Surg. 1995;221:635–645.
20. Berberat PO, Friess H, Kleeff J, et al. Prevention and treatment ofcomplications in pancreatic cancer surgery. Dig Surg. 1999;16:327–336.
21. Bassi C, Falconi M, Molinari E, et al. Reconstruction by pancreaticoje-junostomy versus pancreaticogastrostomy following pancreatectomy:results of a comparative study. Ann Surg. 2005;242:767–771.
22. Bassi C, Falconi M, Molinari E, et al. Duct-to-mucosa versus end-to-sidepancreaticojejunostomy reconstruction after pancreaticoduodenectomy:results of a prospective randomized trial. Surgery. 2003;134:766–771.
23. Shyr YM, Su CH, Wu CW, et al. Does drainage fluid amylase reflectpancreatic leakage after pancreaticoduodenectomy? World J Surg. 2003;27:606–610.
24. Yamaguchi M, Nakano H, Midorikawa T, et al. Prediction of pancreaticfistula by amylase levels of drainage fluid on the first day after pancre-atectomy. Hepatogastroenterology. 2003;50:1155–1158.
25. Hashimoto N, Ohyanagi H. Pancreatic juice output and amylase level inthe drainage fluid after pancreatoduodenectomy in relation to leakage.Hepatogastroenterology. 2002;49:553–555.
26. Shinchi H, Wada K, Traverso LW. The usefulness of drain data toidentify a clinically relevant pancreatic anastomotic leak after pancre-aticoduodenectomy? J Gastrointest Surg. 2006;10:490–498.
27. Connor S, Alexakis N, Garden OJ, et al. Meta-analysis of the value ofsomatostatin and its analogues in reducing complications associated withpancreatic surgery. Br J Surg. 2005;92:1059–1067.
28. Bassi C, Butturini G, Salvia R, et al. Open pancreaticogastrostomy afterpancreaticoduodenectomy: a pilot study. J Gastrointest Surg. 2006;10:1072–1080.
29. Kawai M, Tani M, Terasawa H, et al. Early removal of prophylacticdrains reduces the risk of intra-abdominal infections in patients withpancreatic head resection: prospective study for 104 consecutive pa-tients. Ann Surg. 2006;244:1–7.
30. Wada K, Traverso LW. Pancreatic anastomotic leak after the Whippleprocedure is reduced using the surgical microscope. Surgery. 2006;139:735–742.
Annals of Surgery • Volume 246, Number 2, August 2007 AVD as Predictive Factor of Pancreatic Fistula
© 2007 Lippincott Williams & Wilkins 287

ORIGINAL ARTICLES
Feasibility of Navigated Resection of Liver Tumors UsingMultiplanar Visualization of Intraoperative 3-dimensional
Ultrasound Data
Siegfried Beller, MD, Michael Hunerbein, MD, Sebastian Eulenstein, PhD, Thomas Lange, PhD,and Peter M. Schlag, MD, PhD, FSSO
Background: Intraoperative ultrasound is widely used in liversurgery, but primarily for diagnostic purposes. We have developedand evaluated a system for navigated liver resections using onintraoperatively acquired 3-dimensional (3D) ultrasound data.Methods: Navigation technique based on 3D ultrasound and anoptical tracking system. Accuracy of the system was validatedexperimentally in a tumor model. Subsequently, clinical applicationwas evaluated in 54 patients for resection of central liver tumors.Clinical feasibility and accuracy of the navigation technique wereassessed with respect to practicability, adequacy of visualization,and precision of navigated resection (free margin).Results: Evaluation of the system in the tumor model showed asignificant increase of the accuracy of navigated resections com-pared with conventional resection (P � 0.05). Clinical application of3D ultrasound-based navigation was feasible in 52 of 54 patients.Sufficient visualization was obtained with 2 orthogonal sectionplanes. This navigation strategy provided complete anatomic orien-tation and accurate position control of surgical instruments. Meanhistologic resection margin was 9 mm with a maximum deviation of8 mm from the planned virtual resection margins.Conclusions: Optoelectronic navigation with section mode visual-ization in 2 orthogonal planes does sufficiently display intraopera-tive 3D data and enables accurate ultrasound-based navigation ofliver resections.
(Ann Surg 2007;246: 288–294)
Liver resection has become increasingly safe as a result ofconsiderable progress in equipment, technology, periop-
erative management, and surgical technique.1 Intraoperativeidentification of the vascular tree, ie, hepatic and portal veinsand the localization of the tumor remains essential for seg-ment oriented surgical resection.
Preoperative 3-dimensional (3D) imaging techniques us-ing computed tomography (CT) or magnetic resonance imaging(MRI) data offer perfect visualization of the anatomy.2 How-ever, 3D simulation models are mainly used for preoperativeplanning. Anatomic information cannot be transferred to theintraoperative situation directly, due to organ shift and deforma-tion of the liver during mobilization for resection.3
The most frequently used intraoperative imaging tech-nique is ultrasound. It is generally available, and its diagnos-tic quality is continuously improving. The main objectives ofintraoperative ultrasound during liver surgery are to deter-mine tumor resectability, to localize nonpalpable tumors, andto guide surgical procedures.4 Intraoperative imaging is par-ticularly useful for resection of malignant liver lesions,5 but atthis time it is mainly used to detect additional metastases.
Two-dimensional ultrasound is mostly displayed on amonoscopic video monitor. Advanced 3D and four-dimen-sional visualization for guidance of interventional procedureshas been only realized in tumor ablation and liver biopsyprocedures.6,7 The spatial relationship of the needle and thetarget lesion was conceived more intuitively with 3D andfour-dimensional ultrasonography and helped in adjusting theneedle to an optimal position.
We have integrated 3D ultrasound and optoelectronictracking into a strategy of navigated liver resection. Opto-electronic tracking was used for this study. Accuracy andprecision of the system were first validated in a tumor modelin an experimental setup. Then a clinical study was per-formed to evaluate feasibility, basic requirements of 3Dultrasound visualization, performance, and resection marginsin relation to the surgical plan.
METHODS
Navigation TechniqueImage-guided orientation was realized using 3D contact
ultrasound (Voluson 730 ultrasound machine; GE Healthcare,Milwaukee, WI) with integrated volume rendering of PowerDoppler. A Polaris infrared-based optical tracking system(Northern Digital Inc., Canada) was used for position mea-surement. A tracker equipped with retroreflective spheres wasattached to the ultrasound probe (Voluson Abdominal trans-ducer RAB 4–8 (P); GE Healthcare), and the position of the
From the Charite Universitatsmedizin Berlin, Robert Rossle Klinik, CampusBerlin-Buch, Berlin, Germany.
Reprints: Peter M. Schlag, MD, PhD, FSSO, Klinik fur Chirurgie undChirurgische Onkologie, Charite Campus Buch, Lindenberger Weg 80,13125 Berlin, Germany. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0288DOI: 10.1097/01.sla.0000264233.48306.99
Annals of Surgery • Volume 246, Number 2, August 2007288

probe was tracked by the Polaris system during acquisition ofultrasound data (Fig. 1).
Because of the preoperative calibration of the trackerposition relative to the ultrasound image coordinates, theseimage coordinates were registered to the physical space andanatomic position of the surgical field. Retroreflectivespheres were also attached to surgical instruments. Instru-ments were calibrated and registered on table and used as apointer and navigated actuator. The position of the trackedinstrument was visualized on the monitor and navigated in thevirtual environment of the registered 3D ultrasound data (Fig. 1).
Experimental SetupA lifelike tumor model was created by embedding a
1-cm3 silicon cylinder into the center of a muscle specimen.The ideal resection margin was specified as 2 cm distancefrom the tumor surface. Navigated surgery was performedwith a tracked electrical scalpel (ValleyLab Inc., Boulder,Colorado, CO). The resected specimens were analyzed byhelical CT imaging (GE Healthcare). A collimation of 1 mm,1.5 pitch, and a reconstruction increment of 2 mm were usedto measure deviation from the ideal resection margin. Resultsof navigated resections were compared with conventionalresections based on palpatory findings. Data were analyzedwith the SPSS for Windows Software (SPSS Inc., Chicago,IL). Differences were established with the Mann–Whitney Utest, whereby P values �0.05 were considered statisticallysignificant.
Clinical ApplicationBetween July 2003 and December 2006, we selected 54
of 130 patients for 3D ultrasound-based navigated surgicalresection: 34 men and 20 women with a median age of 61years (range, 29–78 years). Median tumor number was 2(range, 1–7) with a median tumor diameter of 35 mm (range,6–160 mm).
Selected liver tumors were malignant or suspicious formalignancy and located in close vicinity to major vascular orbiliary structures and/or small, intraparenchymal lesions,which were difficult to palpate. For exact planning of theprocedure, preoperative CT or MRI or 3D ultrasound wasconducted. Depending on the visibility of the tumor andvascular structures, 3D models of the liver surface and thevascular tree were created from one of the data sets with thevisualization software Amira (Mercury Computer Systems
FIGURE 2. Plan of anatomy-oriented resection of liver segmentVIII with a minimum virtual resection margin of 10 mm.
FIGURE 1. Navigation setup duringacquisition of 3D ultrasound data.Data and position information areprocessed in the navigation PC.During surgical resection, ultra-sound data are augmented withthe position of the tracked instru-ment and visualized on the naviga-tion PC after removal of the ultra-sound probe.
Annals of Surgery • Volume 246, Number 2, August 2007 Navigated Resection of Liver Tumors
© 2007 Lippincott Williams & Wilkins 289

Inc.). The models were used for vascular anatomy-orientedplanning of the operation.8,9 Planned preservation of vascularstructures and resection of liver parenchyma was documentedin these 3D models. Virtual resection margins were defined asthe shortest distance between the segmented tumors and theplanned resection plane (Fig. 2).
The surgical procedure began with exploration of theabdominal cavity for additional pathologic findings. Aftermobilization and exposure of the liver, screening was per-formed with conventional 2D ultrasound for additional unde-tected lesions. Accurate anatomic orientation and navigatedresection were realized using the tracked 3D ultrasoundprobe (Fig. 3a) and the tracked ultrasonic surgical aspirator(CUSA Excel Ultrasonic Surgical Aspirator; Integra Radi-onics) (Fig. 3b).
We prospectively documented the complexity and prac-ticability of the visualization and navigation device, the setuptime, the operating time for navigation, and the histopatho-logic findings of the surgical specimen. Setup time wasassessed from the startup of the ultrasound machine to thepoint, when the whole system was ready to use. Navigationtime was defined to start with the diagnostic ultrasoundexamination and to end with the start of the liver dissection.Surgical resection margins were defined as the shortest dis-tance from the tumor to the resection border in native ink-labeled surgical specimen.
RESULTS
Experimental AccuracySix navigated and 6 conventional resections with a
planned free margin of 2 cm were performed in the tumormodel. Median deviation from the ideal resection margin was0.16 cm and 0.42 cm with a standard deviation of 0.13 cmand 0.29 cm (P � 0.05). Results are displayed as boxplots(Fig. 4).
FeasibilityIn 2 patients, navigation could not be performed be-
cause of technical problems with the retroreflective spheres orwith the ultrasound machine. Thus, resection was performed
successfully with assistance of 3D ultrasound-based naviga-tion in 52 of 54 patients (96%). Generally one additionalperson was required in the operating room to set up and
FIGURE 4. Experimental evaluation of resection accuracy ofnavigated and conventional surgery. The deviation from theproposed security margin at 2 cm (red line) is shown as box-plots for each technique. The whiskers represent the minimumand maximum value, the upper and lower boxborders show the75% and 25% quartile and the black bar stands for the median.
FIGURE 3. Ultrasound probeequipped with retroreflectivespheres (a) for registration of posi-tion during acquisition of 3D ultra-sound data and ultrasonic surgicalaspirator mounted with retroreflec-tive spheres (b) for navigated surgi-cal resection.
Beller et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins290

operate the navigation hardware. Mean setup time was only15 minutes (range, 10–20 minutes).
Registration of 3D Ultrasound DataThe application of the probe was easily possible in the
lower liver segments 2 to 6. But the tracked 3D ultrasoundprobe was quite bulky, and its application was sometimesdifficult to accomplish vertically to the liver surface in seg-ments 7, 8, 1, and 4a. In such a situation, particularly inpatients with an acute costal arch, navigation was difficult.However, with some experience, 3D ultrasound data forsurgical navigation could be achieved in all cases when theapplication angle of the ultrasound probe was adjusted. Lon-gitudinal application of the ultrasound probe was preferredin vertical orientation to the liver surface over the tumor.If this could not be achieved, it was oriented vertically tothe patient axis.
VisualizationReal-time visualization of 3 orthogonal ultrasound
planes fixed to the tip of the tracked surgical instrument wasnot helpful. Constant movement of 3 section planes wasconfusing and made anatomic orientation difficult. Virtualorientation was best achieved with 2 section-planes, as it isimpossible for the surgeon to observe multiple sections at the
same time. Generally, 2 orthogonal planes, ie, longitudinal(or transverse) and coronal plane, were sufficient to obtainfull spatial orientation (Fig. 5). Tumor borders as well ascolor-coded vessels were displayed on these planes. Relevantanatomic structures like tumor borders and vessels in thetumor area were projected onto the liver surface and markedwith a tracked electrocautery device used as a pointer andmarker. For this action, the position of the transverse planewas frozen at the level of interest. To map the tumor borders,the transverse plane was set into the largest diameter of thetumor (Fig. 5a). To map vessels, the plane was moved andtilted into the longitudinal axis of the vessel (Fig. 5b).During resection with the tracked CUSA, the transverseplane was again set into the largest diameter of the tumor,and the coronal plane was tilted according to the declina-tion of the resection plane and fixed to the tip of the CUSAhandpiece.
Visualization was also available using volume-ren-dered imaging (Fig. 6a). Intraoperative segmentation of 3Dultrasound data was possible, but rapid semiautomatic seg-mentation including the tumor could not be achieved (Fig.6b). 3D models obtained high quality with additional manualsegmentation only, to be comparable with 3D simulationmodels basing on preoperative segmented CT data (Figs. 6c,
FIGURE 5. Visualization of intraop-erative 3D ultrasound data: To fo-cus the tumor border, the trans-verse plane (red line and redframed section plane) was set intothe largest diameter of the tumor(a). To focus on the vessels course,the transverse plane (red line andred framed section plane) was tiltinto the longitudinal axis of thevessel (b).
Annals of Surgery • Volume 246, Number 2, August 2007 Navigated Resection of Liver Tumors
© 2007 Lippincott Williams & Wilkins 291

d). However, this procedure was time-consuming and hard toaccomplish within 1 hour with the technique available.
Surgical NavigationSurgical navigation required 20 minutes (range, 14–45
minutes), including detailed ultrasound examination of theliver. During surgical resection, navigation control could notbe achieved at the same time, as it was not possible to look onthe liver and the navigation screen at the same time. Navi-gated liver resection was rather a repeated changeover be-tween stepwise resection and repeated position control. How-ever, multiplanar visualization of 3D ultrasound data allowedprecise surgical preparation of anatomic structures and deter-mined surgical dissection. Because of organ shifting, theprecision of navigation decreased with progression of theresection procedure. Median registered sets of ultrasounddata were 2 (range, 1–6).
Resection MarginsPlanned virtual resection margins on preoperative 3D
models were 10 mm (range, 1–12 mm). Planned resectionmargins less than 10 mm were accepted and consideredadequate when the tumor was in close connection to theportal vein or the vena cava. However, histologic examina-tion revealed 3 patients with tumor at the surgical resectionmargin. In 2 patients marginal resection was consideredadequate with tumors in contact with the portal vein and thevena cava. In another patient, tumor invasion was found at the
right portal vein after trisectorectomy. Median histologicresection margins were 9 mm (range, 0–15 mm). Maximumand mean deviation from the planned virtual resection marginwas 8 mm and 13 mm.
DISCUSSIONIntraoperative ultrasound has become an indispensable
tool for liver resections and can modify the surgical strategybecause of additional findings in a considerable number ofpatients.10–14 It can also provide more safety with respect totumor-free resection margins and can support the preserva-tion of vessels close to the tumor.15 However, real-timeimage guidance is only possible with contact ultrasonographyon the liver surface, which prevents surgical dissection ofliver parenchyma at the same place. Therefore, surgeonscontinue to operate intuitively. They can transfer the infor-mation of imaging data to the surgical field only after ultra-sonography.
3D ultrasound offers improved orientation in a virtualenvironment of imaging data,6,7,16 and its combination withnavigation technology could be a promising technique forliver resection. Simultaneous localization of ultrasound dataand surgical instruments enable the transfer of anatomicorientation directly to the individual patient. In this study,optoelectronic tracking was chosen for navigated resection ofliver tumors because it has proved higher precision than theelectromagnetic tracking technique.17 In a laboratory setting
FIGURE 6. Volume-rendered imag-ing basing on 3D Doppler ultra-sonography (a). Model segmentedfrom 3D ultrasound data: semiau-tomatic segmentation (b) andmanual segmentation (c). d, Simu-lation model segmented from pre-operative CT data.
Beller et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins292

for neuronavigation, the accuracy of optoelectronic naviga-tion was found to be 1.40 � 0.45 mm (arithmetic mean).18 Inthe presented experimental evaluation of 3D ultrasound-based navigation, we found a median deviation from theproposed security margin of 1.60 � 1.30 mm. The navigatedresection of a poorly palpable tumor with a free resectionmargin of 2 cm in a tissue model was significantly moreaccurate than conventional resections (P � 0.05). These dataconfirmed a high accuracy of optoelectronic navigation withultrasound data and justified clinical evaluation of the systemin patients with liver tumors.
In the clinical study, 54 of 130 patients with livertumors (41%) were considered to be good candidates forintraoperative navigation because the lesions were adjacent tomajor vessels or impalpable. This proportion appears ratherhigh and may only be observed in tertiary referral centerswith a high number of complex cases.
3D ultrasound-based navigation was feasible in themajority of patients (96%), and technical problems occurredonly in 2 cases. In this series, navigated surgery was per-formed with additional staff in the operating room. However,with additional experience, the surgical team presumably canmanage the navigation system without ancillary personnel.Setup time of the system and intraoperative navigation timewere approximately 20 minutes, which appears to be reason-able. Free line of sight between tracking camera and trackeddevices had to be preserved during navigation to avoid anyinterruption of the registration process. Therefore, an opticalgate control sign should be implemented to the navigationmonitor, which allows the detection of any interruption of theoptoelectronic tracking directly.
We found that multiplanar imaging on a monoscopicmonitor is efficient for navigation purpose. Section modevisualization in 2 orthogonal section planes does sufficientlydisplay the position of instruments during navigated liverresection. A sophisticated arrangement and exposure of thesection planes focusing on a small limited operation area areadvisable. Using this technique, surgeons can rapidly under-stand the anatomy of the vascular tree in relation to the tumor.They can maintain the planned dissection plane and canidentify vascular structures within the dissection plane. In thefuture, rapid segmentation procedures for 3D ultrasound datacould improve navigation by intraoperatively updated 3Dmodels. Currently, high-quality models can only be obtainedwith additional manual segmentation (Fig. 6), which cannot beaccomplished within a reasonable time during the operation.
Three-dimensional ultrasound based optoelectronicnavigation provided improved intraoperative anatomic orien-tation. Resections could be performed with vessels and bileducts oriented away from the tumor, so that these structurescould be preserved. Ultrasound data could be updated in afew seconds, whenever the position of the liver or patient waschanged. The dissecting surgical instruments became virtualactuators under continuous position control.
The results are encouraging in these selected complexcases. In the presented series of patients, with tumors locatedin close vicinity to major vascular or biliary structures,resection margins were free in 94% of the patients. Inade-
quate margins were observed in 3 patients only (6%). In theliterature, tumor-involved resection margins are reported inup to 30% of cases and vary depending on the type ofresection and the localization of the tumor from 2% to 16%in referral centers.19–21
The advantage of using updated ultrasound for naviga-tion is the topicality of the data. By recording 3D dataintraoperatively, liver lesions and additional findings arelocalized directly and are ready for navigation immediately.Anatomic shifting, a major limitation for navigated surgery insoft tissue,22 due to positioning of the patient or mobilizationof the liver, is exactly registered. Clearly, ultrasound is onlyfeasible for tumors that can be identified by ultrasound;therefore, rapid fusion of intraoperative and preoperative CT,MRI, or PET data will be necessary for optimal localizationand navigation.
Further investigations are necessary to evaluate theclinical value of the described method.23 Future improve-ments should focus on continuous navigation and improvedvisualization. Electromagnetic tracking of landmarks andvisualization media, such as holography and the virtual reti-nal display, may possibly be favorable.24–26 Further devel-opments will also be necessary to adapt navigation techniqueto minimally invasive liver surgery with its special need forassistance due to the lack of sense of touch and hapticfeedback.27
ACKNOWLEDGMENTSThe authors thank Prof. Peter Deuflhard, Prof. H. C.
Christian Hege, and Hans Lamecker from the Zuse InstituteBerlin (ZIB) for their close cooperation concerning 3-Dmodeling and statistical shape analysis.
REFERENCES1. Schmidbauer S, Hallfeldt KK, Sitzmann G, et al. Experience with
ultrasound scissors and blades (UltraCision) in open and laparoscopicliver resection. Ann Surg. 2002;235:27–30.
2. Wigmore SJ, Redhead DN, Yan XJ, et al. Virtual hepatic resection usingthree-dimensional reconstruction of helical computed tomography an-gioportograms. Ann Surg. 2001;233:221–226.
3. Hayashibe M, Suzuki N, Kobayashi S, et al. Development of a 3Dvisualization system for surgical field deformation with geometric pat-tern projection. Stud Health Technol Inform. 2005;111:172–177.
4. Machi J, Sigel B, Zaren HA, et al. Operative ultrasonography duringhepatobiliary and pancreatic surgery. World J Surg. 1993;17:640 –645.
5. Cervone A, Sardi A, Conaway GL. Intraoperative ultrasound (IOUS) isessential in the management of metastatic colorectal liver lesions. AmSurg. 2000;66:611–615.
6. Sjolie E, Lango T, Ystgaard B, et al. 3D ultrasound-based navigation forradiofrequency thermal ablation in the treatment of liver malignancies.Surg Endosc. 2003;17:933–938.
7. Stippel DL, Bohm S, Beckurts KT, et al. Experimental evaluation ofaccuracy of radiofrequency ablation using conventional ultrasound or athird-dimension navigation tool. Langenbecks Arch Surg. 2002;387:303–308.
8. Lange T, Eulenstein S, Hunerbein M, et al. Vessel-based non-rigidregistration of MR/CT and 3D ultrasound for navigation in liver surgery.Comput Aided Surg. 2003;8:228–240.
9. Lamecker H, Seebass M, Lange T, et al. Visualization of the variabilityof 3D statistical shape models by animation. Stud Health TechnolInform. 2004;98:190–196.
10. Leen E, Ceccotti P, Moug SJ, et al. Potential value of contrast-enhancedintraoperative ultrasonography during partial hepatectomy for metasta-
Annals of Surgery • Volume 246, Number 2, August 2007 Navigated Resection of Liver Tumors
© 2007 Lippincott Williams & Wilkins 293

ses: an essential investigation before resection. Ann Surg. 2006;243:236–240.
11. Braga L, Guller U, Semelka RC. Modern hepatic imaging. Surg ClinNorth Am. 2004;84:375–400.
12. Benson MD, Gandhi MR. Ultrasound of the hepatobiliary-pancreaticsystem. World J Surg. 2000;24:166–170.
13. Sahani DV, Kalva SP, Tanabe KK, et al. Intraoperative US in patientsundergoing surgery for liver neoplasms: comparison with MR imaging.Radiology. 2004;232:810–814.
14. Conlon R, Jacobs M, Dasgupta D, et al. The value of intraoperativeultrasound during hepatic resection compared with improved preop-erative magnetic resonance imaging. Eur J Ultrasound. 2003;16:211–216.
15. Torzilli G, Montorsi M, Donadon M, et al. ‘Radical but conservative’ isthe main goal for ultrasonography-guided liver resection: prospectivevalidation of this approach. J Am Coll Surg. 2005;201:517–528.
16. Albrecht H, Stroszczynski C, Felix R, et al. Real time 3D (4D) ultra-sound-guided percutaneous biopsy of solid tumours. Ultraschall Med.2006;27:324–328.
17. Wagner A, Schicho K, Birkfellner W, et al. Quantitative analysis offactors affecting intraoperative precision and stability of optoelectronicand electromagnetic tracking systems. Med Phys. 2002;29:905–912.
18. Lindseth F, Lango T, Bang J, et al. Accuracy evaluation of a 3Dultrasound-based neuronavigation system. Comput Aided Surg. 2002;7:197–222.
19. Scheele J, Stangl R, Atendorf-Hofmann A. Hepatic metastases from
colorectal carcinoma: impact of surgical resection on the natural history.Br J Surg. 1990;77:1241–1246.
20. DeMatteo RP, Palese C, Jarnagin WR, et al. Anatomic segmental hepaticresection is superior to wedge resection as an oncologic operation forcolorectal liver metastases. J Gastrointest Surg. 2000;4:178–184.
21. DeMatteo RP, Fong Y, Jarnagin WR, et al. Recent advances in hepaticresection. Semin Surg Oncol. 2000;19:200–207.
22. Sergeeva O, Uhlemann F, Schackert G, et al. Integration of intraopera-tive 3D-ultrasound in a commercial navigation system. Zentralbl Neu-rochir. 2006;67:197–203.
23. Beller S, Hunerbein M, Lange T, et al. Image-guided surgery of livermetastases by 3D ultrasound based optoelectronic navigation. Br J Surg.2007;94:866–875.
24. Kleweno CP, Seibel EJ, Viirre ES, et al. The virtual retinal display as alow-vision computer interface: a pilot study. J Rehabil Res Dev. 2001;38:431–442.
25. Herline AJ, Herring JL, Stefansic JD, et al. Surface registration for usein interactive, image-guided liver surgery. Comput Aided Surg. 2000;5:11–17.
26. Hayashibe M, Suzuki N, Hattori A, et al. Data-fusion display systemwith volume rendering of intraoperatively scanned CT images. MedImage Comput Comput Assist Interv Int Conf Med Image ComputComput Assist Interv. 2005;8:559–566.
27. Lange T, Hunerbein M, Eulenstein S, et al. Development of navigationsystems for image-guided laparoscopic tumor resections in liver surgery.Recent Results Cancer Res. 2006;167:13–36.
Beller et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins294

ORIGINAL ARTICLES
The Impact of Margins on Outcome After HepaticResection for Colorectal Metastasis
Chandrakanth Are, MD, FRCS,* Mithat Gonen, PhD,† Kathleen Zazzali, DO,*Ronald P. DeMatteo, MD, FACS,* William R. Jarnagin, MD, FACS,* Yuman Fong, MD, FACS,*
Leslie H. Blumgart, MD, FACS, FRCS,* and Michael D’Angelica, MD, FACS*
Objective: To analyze the impact of margin width on long-termoutcome after hepatic resection for colorectal metastasis.Summary Background Data: The optimal margin width and itsinfluence on long-term outcome after hepatic resection for colorectalmetastasis are unclear.Methods: All patients undergoing hepatic resection for colorectalmetastasis from 1991 to 2003 were identified, and the prognosticinfluence of margin width and other clinicopathologic factors wereanalyzed.Results: A total of 1019 patients with a clear description of marginwidth were included. Analysis of margin width as a continuousvariable suggested the following grouping: group I, involved (n �112, 11%); group II, �1–10 mm (n � 563, 55%); and group III,�10 mm (n � 344, 33.7%). On univariate analysis, there was astatistically significant difference in median survival between all 3groups: group II versus group I (42 vs. 30 months, P � 0.01) andgroup III versus group II (55 vs. 42 months, P � 0.01). Marginwidth �1 cm retained statistical significance (P � 0.01) on multi-variate analysis after adjusting for established risk factors. Afteradjustment, survival in group III was significantly better than eithergroup I or II (P � 0.01), but there was no difference between groupsI and II (P � 0.31).Conclusions: This study provides evidence that margin width of �1cm is optimal and is an independent predictor of survival afterhepatic resection for colorectal metastasis. However, subcentimeterresections are also associated with favorable outcome and should notpreclude patients from undergoing resection.
(Ann Surg 2007;246: 295–300)
Hepatic resection is the only treatment modality associatedwith long-term survival in patients with colorectal liver
metastasis. Five-year survival rates ranging from 25% to 58%have been reported with hepatic resection.1–3 With improvedsurgical techniques and chemotherapy, more patients aresubjected to resection, including patients previously consid-ered unresectable. Several clinicopathologic factors havebeen analyzed and are now considered to be independentprognostic factors associated with survival.4–13 The role ofresection margin status as a prognostic factor to predictsurvival after hepatic resection for colorectal metastasis iscontroversial. In addition, the optimal margin width, if any, isunclear.
Early documentation by some reports of a potentialbenefit associated with a 1-cm margin led to the generalacceptance of this margin width to guide hepatic resec-tions.14 Since that time, several studies addressing theissue of margin width have yielded conflicting results.Some authors have shown that a margin width �1 cm isassociated with improved survival when compared withsubcentimeter resections.4,15–19 In contrast, other reportshave documented that the margin width does not have anyeffect on survival as long as it is negative,2,20,21 whereassome studies have noted that although a �1 cm margin isdesirable, survival is not influenced by the width of thesubcentimeter margin (0 –9 mm).3,22 Firm conclusionsfrom these studies are limited by small numbers of patientsand limited statistical power. The only reports with a largenumber of patients were multi-institutional studies,2,7,11 inwhich institutional differences in the method of livertransection and pathologic analysis of the margin mayconfound the results. From these conflicting studies, theprognostic significance of margin status and the optimalmargin width remain unclear. This is all the more impor-tant, since an increasing number of complex resections areperformed in which the extent of hepatic involvementfrequently mandates close resection margins.
The aim of this study was to determine the impact ofmargin width on long-term survival after hepatic resection forcolorectal metastasis in a large, consecutive series of patientsfrom a single institution. Second, the study hopes to deter-mine the influence of margin width on survival in the contextof well-established clinicopathologic prognostic factors.
From the *Hepatobiliary Division, Department of Surgery, †Department ofEpidemiology and Biostatistics, Memorial Sloan-Kettering Cancer Cen-ter, New York, NY.
Reprints: Michael D’Angelica, MD, FACS, Assistant Attending, Departmentof Hepatobiliary Surgery, Memorial Sloan-Kettering Cancer Center,1275 York Avenue, Box 404/Room C-898, New York, NY 10021.E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0295DOI: 10.1097/SLA.0b013e31811ea962
Annals of Surgery • Volume 246, Number 2, August 2007 295

PATIENTS AND METHODSAll patients who underwent hepatic resection for colo-
rectal metastasis from 1991 to 2003 were entered into aprospective database and included in the study. The studywas approved by the Institutional Review Board and con-formed to the Health Insurance Portability and AccountabilityAct. Data pertaining to the primary colorectal tumor (site andnodal status), hepatic metastasis (size, number, prehepatec-tomy CEA level, disease-free interval, and synchronous ormetachronous presentation), operative details (type and ex-tent of hepatic resection), and histopathology (margin widthin millimeter) were collected. Patients underwent cross-sec-tional imaging of the abdomen with contrast-enhanced com-puted tomography (CT) and/or magnetic resonance imaging(MRI). The chest was imaged with x-rays or with CT. Allpatients had a colonoscopy within 1 year of liver resection.The operations were performed by 5 different surgeons andtheir approach to hepatic resection for colorectal metastasishas been previously described.1,23 Intraoperative ultrasoundof the liver was carried out in all patients. A central venouspressure less than 5 mm Hg was maintained during paren-chymal transection and monitored by central venous access.Anatomic, segmental-based resections were performed when-ever feasible. In general, the liver was transected with the“Kelly clamp” crush technique.
Since 1991, uniform standards in the final histopatho-logic description of liver tumors were established at ourinstitution and have been followed since. This includes num-ber of tumors, size of the largest tumor, and a numericaldescription of the margin width in millimeters. Patients with-out an accurate numerical description of the margin widthwere excluded from the analysis. In addition, patients inwhom the margins could not be assessed by the pathologistdue to the effect of the method of resection (such as cryoas-sisted resection) were also excluded. In the remaining pa-tients, the distance (in millimeter) of the lesion closest to thetransected liver surface was judged to be the final marginwidth. In the case of multiple tumors, the closest margin wasrecorded as the final margin.
Margin status (categorized) was compared with othercategorical variables using the �2 test and continuous vari-ables using the t test. Survival was measured from time ofresection to death or last follow-up. Categorization of themargin width was based on a plot of median survival versusmargin width. Survival probabilities were estimated using theKaplan-Meier method. Individual groups were compared us-ing log-rank test and the multivariate analysis used stepwiseCox regression.
RESULTS
DemographicsA total of 1119 patients underwent hepatic resection for
colorectal metastasis from 1991 to 2003. Of these, 1019(91%) had a clear numerical description of the margin width(in millimeter) and were included in the study. One hundredpatients (9%) were excluded due to the absence of a clearnumerical description of margin width or the inability to
assess margins secondary to the method of liver transaction.The median age was 63 years (range, 23–89) and 571 patients(56%) were male. The 30-day operative mortality rate was2%, and the incidence of postoperative morbidity was 44%.With a median follow-up of 42 months for the entire cohortof 1019 patients, the median survival was 44 months andoverall 1-, 3-, and 5-year survival rates were 90%, 59%, and37%, respectively.
Clinicopathologic Characteristics of thePrimary and Metastatic Tumors
The primary tumor was in the colon in 850 patients(76%). In 355 patients (34%), the presentation of metastasiswas synchronous with the primary and in 564 patients (55%)the disease-free interval was less than 12 months. Five hun-dred ninety patients (58%) had involved regional lymphnodes associated with the primary tumor. The mean numberof hepatic metastases was 2.4 � 2.3 and 506 patients (50%)had �2 tumors. The mean size of the largest hepatic metas-tasis was 4.8 � 3.2 cm, and 679 patients (67%) had tumorsmeasuring �5 cm. Preoperative chemotherapy was adminis-tered to 302 patients (33%) before liver resection.
Operative DetailsSix hundred and seventy-eight (66.5%) patients under-
went a hemihepatectomy and of these, 287 (28%) weresubjected to an extended hepatectomy (trisegmentectomy). In441 patients (43%), hepatic resection involved both lobes.The average number of segments resected was 3.5 � 1.5, andthe distribution of segmental resection was as follows: 1segment 13%; bisegmentectomy 19%; 3 segments 8%; 4 andabove 60%.
Results With Historical Margin Width CriteriaBased on previous publications, the margin width was
initially analyzed at a 1 cm cut-off, with subcentimetermargins arbitrarily divided into 4 categories: involved, �1mm, 1–5 mm, and 5–10 mm. With increasing margin width,the survival rates increased proportionately when comparedwith that of patients in the reference group (involved margin)(Table 1). When compared with patients with involved mar-gins, this increase in survival was not statistically significantin patients with 1–10 mm margins and assumed statisticalsignificance at �1 cm (P � 0.01).
Analysis of Margin Width as a ContinuousVariable
The influence of margins on survival was then analyzedas a continuous variable. This analysis revealed a survivalbenefit that increased incrementally with the increasing widthof the margin with a plateau effect in the later part of thecurve (Fig. 1). In addition, there were 2 inflection points onthe curve that were associated with more significant differ-ences in survival. The 2 significant cut-off points were atapproximately 0 and 10 mm. Based on these 2 cut-off points(as suggested by the statistical analysis), the patients weredivided into 3 groups: groups I (involved), II (�1–10 mm),and III (�10 mm), respectively.
Are et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins296

The influence of margin width on overall survival inpatients in these 3 groups was analyzed and is graphicallydisplayed in Figure 2. On univariate analysis, there was astatistically significant difference in survival between all 3groups. Patients in group II had an improved median survival
when compared with those in group I (42 vs. 30 months, P �0.01). Similarly, patients in group III had a better mediansurvival when compared with those in both groups II and I(55 vs. 42 and 30 months, P � 0.01) (Table 2).
On univariate analysis, several other factors were asso-ciated with worse long-term survival and are summarized inTable 3. These include resection greater than a hemihepate-ctomy, bilateral resection, resection of �2 hepatic tumors,size �5 cm, perioperative transfusion, preoperative CEA�200 ng/mL, node-positive primary, and margin width. Onmultivariate analysis, bilateral resection, resection of �2hepatic tumors, size �5 cm, perioperative transfusion, node-positive primary and margin width �1 cm (group III) re-tained significance as independent predictors of outcome. Onmultivariate analysis, margin width was a significant factorwhen comparing group III with groups I and II (P � 0.01),but there was no significance between groups II and I (P �0.31).
Factors Associated With Close MarginsFactors potentially associated with a margin width of
�1 cm were also analyzed and are summarized in Table 4.The factors associated with a narrower margin width werebilateral resection and the presence of �2 hepatic tumors.Size �5 cm and CEA �200 ng/mL were marginally associ-ated with closer margins (P � 0.09 and 0.08). Notably, theuse of preoperative chemotherapy was not associated withwider margins.
DISCUSSIONSeveral factors have been documented to be indepen-
dent prognostic factors associated with outcome after hepaticresection for colorectal metastasis.1,3,5,8,14 These includenodal status of the primary colorectal tumor, disease-freeinterval, size of the largest hepatic tumor, prehepatectomyCEA level, number and distribution of metastatic lesions, andextent of resection. The role of margin status as an indepen-
FIGURE 1. Impact of margin width on survival analyzed as acontinuous variable.
TABLE 2. Impact of Margins on Survival Based onGrouping Suggested by Analysis of Margins as a ContinuousVariable
Margins N (%) Median Survival (mo) P
Group I (involved) 112 (11) 30 Reference
Group II (�1–10 mm) 563 (55) 42 �0.01*
Group III (�1 cm) 344 (33) 55 �0.01†
*Comparing group II versus group I.†Comparing group III versus groups II and I combined.
FIGURE 2. Kaplan–Meier survival plot comparing 3 differentmargin width groupings.
TABLE 1. Initial Analysis of the Impact of Margins on Survival (n � 1019)
Margins n (%) Median Survival (mo) 3-yr Survival (%) 5-yr Survival (%) P
Involved: 112 (11) 30 46 26 Reference
�1 mm: 138 (13) 39 53 29 0.59
1–5 mm: 261 (25) 43 59 35 0.09
5–10 mm: 164 (16) 50 58 40 0.07
�1 cm: 344 (33) 55 66 45 �0.01
Annals of Surgery • Volume 246, Number 2, August 2007 Margin Width After Hepatic Resection
© 2007 Lippincott Williams & Wilkins 297

dent predictor of survival and the optimal margin width afterhepatic resection for colorectal metastasis is unclear. This iscompounded by the fact that there is a paucity of reports thathave addressed this issue,2,4,14–18,20,21 most of which arelimited by small numbers of patients and limited statisticalpower.4,16,17,20,21 The studies that included adequate numbersof patients were multi-institutional,2,15 and in such studies,institutional differences in hepatic transection techniques and
histologic analysis of margins make interpretation of resultsdifficult.
Despite the lack of firm evidence, there has been ageneral consensus since the early 1980s that a 1 cm margin isoptimal, with some authors suggesting that inability to obtainsuch a margin should preclude hepatic resection.7,14,19 Forexample, in their series of 72 resections, Ekberg et al con-cluded that, due to the poor outcomes associated with sub-
TABLE 3. Univariate and Multivariate Analysis of the Impact of Margins and OtherClinicopathologic Factors on Survival
Factor N Median Survival (mo) UV P MV P Hazard Ratio
Less than hemihepatectomy 341 51 — — —
Hemihepatectomy or more 678 41 �0.01 NS —
Unilateral resection 578 52
Bilateral resection 441 36 �0.01 0.03 1.20
Solitary 511 53
�2 Tumors 506 37 �0.01 �0.01 1.27
Size
�5 cm 679 51 �0.01 �0.01 1.52
�5 cm 339 34
No transfusion 546 53 �0.01 0.05 1.19
Transfusion 472 37
CEA
�200 429 48 0.04 * —
�200 51 38
Node neg primary 384 57 �0.01 �0.01 1.57
Node pos primary 590 37
DFI
�12 mo 564 46 0.13 NS —
�12 mo 449 40
Metachronous presentation 355 45 0.18 NS —
Synchronous presentation 661 42
Involved margin (group I) 112 30 Reference Reference —
�1–10 mm margin (group II) 563 42 �0.01† 0.31† —
�10 mm margin (group III) 344 55 �0.01‡ �0.01‡ 1.64
*Excluded secondary to insufficient data.†Comparing group II vs. I.‡Comparing group III vs. II and I.UV indicates univariate analysis; MV, multivariate analysis; NS, not significant; neg, negative; pos, positive; DFI,
disease-free interval.
TABLE 4. Influence of Tumor-Related and Technical Factors on Margin Width
Factor
Margin Width
PPositive (n � 112) (%) <1–10 cm (n � 563) (%) >1cm (n � 344) (%)
Lobe or more 80/112 (71) 367/563 (65) 233/344 (68) 0.88
Bilateral resection 72/112 (64) 265/563 (47) 105/344 (30) �0.01
�2 tumors 71/112 (63) 290/563 (52) 145/344 (42) �0.01
Size �5 cm 44/112 (39) 191/563 (34) 105/344 (30) 0.09
Neoadjuvant chemotherapy 41/111 (37) 160/553 (29) 101/342 (30) 0.31
CEA �200 8/56 (14) 31/259 (12) 12/166 (7) 0.08
Node-positive primary 60/107 (56) 320/535 (60) 210/333 (63) 0.17
DFI �12 mo 59/112 (53) 244/563 (43) 147/339 (43) 0.20
Synchronous presentation 66/111 (59) 369/563 (66) 227/343 (66) 0.30
DFI indicates disease-free interval.
Are et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins298

centimeter resections, liver resection should not be performedif a margin width of 1 cm is unobtainable.14 Since then, moststudies that have assessed the impact of margins relied on this1 cm margin cut-off for analysis and have reported conflictingresults.2,3,17,21 In their series of 112 patients, Wray et al foundthat subcentimeter resections were associated with increasedlocal and distant recurrence, and concluded that a �1 cmmargin should be attempted in all cases.17 Conversely, byassessing specimens for K-ras and p53 mutations in 58patients with colorectal liver metastasis, Kokudo et al21 notedthat micrometastasis are very uncommon and most are con-fined to within �2 mm of the tumor. On the basis of thesefindings, the authors concluded that a 1 cm margin is notessential.
It is critical to analyze the effect of margin status onsurvival in the context of well-established clinicopathologicfactors in a multivariate analysis. This is the best way toensure that margin status, as interpreted by the pathologist, isnot simply a surrogate for other parameters that impact onsurvival. Shirabe et al16 found that a resection margin of �10mm was independently associated with poor prognosis onmultivariate analysis; however, their study consisted of only31 patients with limited statistical power to support suchconclusions. In contrast, other reports have found that themargin width does not influence long-term outcome on mul-tivariate analysis.2,3 Scheele et al3 analyzed the effect ofmargins in 414 patients who underwent complete gross re-section. Forty-eight (12%) of these 414 patients had positivemargins and were not included in the analysis. Margin widthhad an influence on overall and disease-free survival onunivariate analysis, but not on multivariate analysis. It ispossible, however, that if the patients with positive margins(and likely the worst outcomes) were also included forcomparison, there may have been an independent survivalbenefit associated with margin width. In a multicenter retro-spective study of 557 patients, Pawlik et al2 found that apositive margin was associated with an increased rate ofsurgical margin recurrence and survival on univariate analy-sis. Interestingly, outcome was the same for patients withnegative margins regardless of margin width. When subjectedto multivariate analysis, margin status was not an indepen-dent predictor of outcome. Definitive conclusions from thisstudy are limited by the relatively small number of patientswith positive margins (n � 45) and the potentially confound-ing issue of different parenchymal transection techniques andhistologic analysis in the different institutions.
These conflicting results leave the question of marginsunanswered. The aim of this study, therefore, was to deter-mine whether margin status is an independent predictor oflong-term outcome following hepatic resection for colorectalmetastasis in a large consecutive series of patients from asingle institution with a uniform approach to parenchymaltransection (Kelly clamp crush technique) and strict standardsof histopathologic analysis.
In contrast to the previous reports, we analyzed theinfluence of margin width on survival as a continuous vari-able. This analysis showed an incremental increase in sur-vival as the margin width increased with 2 inflection points
on the curve at approximately 0 and 10 mm. It is interestingto note a small, but statistically insignificant, increase insurvival beyond 10 mm with an ultimate plateau at 25 mm.On the basis of this analysis, the patients in our study weretherefore divided into 3 groups based on this statisticalsuggestion (involved, �1–10 mm, and �10 mm). On univar-iate analysis, there was a statistically significant difference insurvival between all 3 groups. On multivariate analysis,however, patients with a �1 cm margin had a statisticallysignificant improvement in long-term outcome when com-pared with the remaining patients (P � 0.01). Although therewas a difference in survival between subcentimeter resectionsand positive margins, this did not reach significance onmultivariate analysis (P � 0.31). This analysis confirmed theindependent prognostic importance of a 1 cm margin in thecontext of other well-established clinicopathologic prognosticfactors. It is important to interpret these results in the contextof our parenchymal transection technique. The Kelly clampcrush technique may create a margin of different characterthan other well-known techniques and the margin, as deter-mined by the pathologist, may have different clinical rele-vance. Nonetheless, the linear and independent relationshipbetween margin and survival is strong evidence that themargin width is an important factor.
Our study is the only report to date to document anassociation of a 1 cm margin width with improved long-termoutcome on multivariate analysis in a large series of patients.The large number of patients provided significant statisticalpower and afforded us the ability to detect relatively smalldifferences, and it is important to interpret these data care-fully. Only 9% of patients were excluded from this analysislargely due to inadequate pathologic descriptions or, lesscommonly, techniques in which the margin was not measur-able (such as cryoassisted resection). It is unlikely that thesepatients would have altered the outcome since they are asmall percentage of the overall group and are generallyrelated to the earlier time period in which pathologic report-ing standards were changing at our institution. It must beemphasized that, even in patients with subcentimeter resec-tions, the long-term survival is still favorable (median sur-vival of 30–42 months). Although this is inferior to patientswith �1 cm margins, it is better than in patients who do notundergo hepatic resection or are unresectable for any rea-son.24–26 The outcome after subcentimeter resection is alsobetter than any other single modality of treatment that iscurrently available, including the current chemotherapy reg-imens (median survival of 20–22 months).27–29 Furthermore,chemotherapy “alone” rarely produces 5-year survivors ordurable complete responders.27–29 Therefore, inability to ob-tain �1 cm margin based on preoperative imaging should notpreclude hepatic resection.
Although the authors’ general strategy is to achieve �1cm margins, this was not possible in all cases due to anatomicconstraints or simply misjudgment of the actual margin. Inour study, we found the only factors that were associated witha decrease in the rate of obtaining �1 cm margin werebilateral resection and resection of �2 hepatic tumors. Thisfinding is logical since in many of these patients with multiple
Annals of Surgery • Volume 246, Number 2, August 2007 Margin Width After Hepatic Resection
© 2007 Lippincott Williams & Wilkins 299

bilobar tumors, wide margins are not technically possible.Tumor size �5 cm and CEA level �200 ng/mL were asso-ciated with a reduction in the rate of �1 cm margins, but thisdid not reach statistical significance. It has been suggestedthat administration of preoperative chemotherapy can in-crease the likelihood of clear margins.30 In a series of 108patients, Parikh et al30 found that the 61 patients who wereadministered 5FU based chemotherapy with or without CPT11 tended to have a higher rate of negative margins that didnot reach statistical significance. We did not find that preop-erative chemotherapy increased the incidence of �1 cmmargins in the 302 patients that received it.
In summary, this study provides evidence that marginstatus is an independent predictor of long-term outcome afterhepatic resection for colorectal metastasis. A margin width of�1 cm is independently associated with the best long-termoutcome and should be attempted whenever possible. Despitethe statistical difference, subcentimeter resections are alsoassociated with a favorable outcome when compared withany other single modality of treatment that is currentlyavailable. In patients undergoing hepatic resection for colo-rectal metastasis, a �1 cm margin should be attemptedwhenever possible. However, inability to achieve this shouldnot preclude hepatic resection.
REFERENCES1. Fong Y, Fortner J, Sun RL, et al. Clinical score for predicting recurrence
after hepatic resection for metastatic colorectal cancer: analysis of 1001consecutive cases. Ann Surg. 1999;230:309–318.
2. Pawlik TM, Scoggins CR, Zorzi D, et al. Effect of surgical margin statuson survival and site of recurrence after hepatic resection of colorectalmetastasis. Ann Surg. 2005;241:715–724.
3. Scheele J, Stang R, Altendorf-Hofmann A, et al. Resection of colorectalliver metastasis. World J Surg. 1995;19:59–71.
4. Cady B, Jenkins R, Steele GD, et al. Surgical margin in hepatic resectionfor colorectal metastasis: a critical and improvable determinant ofoutcome. Ann Surg. 1998;227:566–571.
5. Gayowski TJ, Iwatuski S, Madariaga JR, et al. Experience in hepaticresection for metastatic colorectal cancer: analysis of clinical and patho-logical risk factors. Surgery. 1994;116:703–711.
6. Choti MA, Sitzmann JV, Tiburi MF, et al. Trend in long-term outcomesurvival following liver resection for hepatic colorectal metastasis. AnnSurg. 2002;235:759–766.
7. Nordlinger B, Guiguet M, Vaillant JC, et al. Surgical resection ofcolorectal carcinoma metastasis to the liver: a prognostic scoring systemto improve case selection based on 1568 patients. Association Francaisede Chirurgie. Cancer. 1996;77:1254–1262.
8. Doci R, Gennari D, Begnami P, et al. One hundred patients with hepaticmetastases from colorectal cancer treated by resection: analysis ofprognostic determinants. Br J Surg. 1991;78:797–801.
9. Cady B, Stone MD, McDermott WV, et al. Technical and biologicalfactors in disease- free survival after hepatic resection for colorectalcancer metastasis. Arch Surg. 1992;127:561–569.
10. Registry of Hepatic Metastasis. Resection of the liver for colorectalcarcinoma metastasis: a multi-institutional study of indications for re-section. Surgery. 1988;103:278–288.
11. Hughes K, Scheele J, Sugarbaker PH. Surgery for colorectal cancer
metastatic to the liver. Optimizing the results of treatment. Surg ClinNorth Am. 1989;69:339–359.
12. Jamison RL, Donohue JH, Nagorney DM, et al. Hepatic resection formetastatic colorectal cancer results in cure for some patients. Arch Surg.1997;132:505–511.
13. Fortner JG, Silva JS, Golber RB, et al. Multi-variate analysis of apersonal series of 247 consecutive patients with liver metastasis fromcolorectal cancer. Treatment by hepatic resection. Ann Surg. 1984;199:317–324.
14. Ekberg J, Tranberg KG, Andersson R, et al. Determinants of survival inliver resection for colorectal secondaries. Br J Surg. 1986;73:727–731.
15. Kato T, Yasui K, Hirai T, et al. Therapeutic results for hepatic metastasisof colorectal cancer with special reference to effectiveness of hepatec-tomy: analysis of prognostic factors for 763 cases recorded at 18institutions. Dis Colon Rectum. 2003;46:22–31.
16. Shirabe K, Takenaka K, Gioni T, et al. Analysis of prognostic riskfactors in hepatic resection for metastatic colorectal carcinoma withspecial reference to surgical margin. Br J Surg. 1997;84:1077–1080.
17. Wray CJ, Lowy AM, Mathews JB, et al. The significance and clinicalfactors associated with a sub-centimeter resection of colorectal livermetastasis. Ann Surg Onc. 2005;12:1–7.
18. Ambiru S, Miyazaki M, Isono T, et al. Hepatic resection for colorectalmetastasis: analysis of prognostic factors. Dis Colon Rectum. 1999;42:632–639.
19. Hughes KS, Simon R, Songhorabodi S, et al. Resection of liver forcolorectal carcinoma metastasis: a multi-institutional study of patterns ofrecurrence. Surgery. 1986;100:278–284.
20. Yamomoto J, Sugihara K, Kosuge T, et al. Pathologic support for limitedhepatectomy in the treatment of liver metastasis from colorectal cancer.Ann Surg. 1995;22:74–78.
21. Kokudo N, Miki Y, Sugai S, et al. Genetic and histological assessmentof surgical margins in resected liver metastases from colorectal carci-noma. Arch Surg. 2002;137:833–840.
22. Elias D, Cavalcanti A, Sabourin JC, et al. Resection of liver metastasisfrom colorectal cancer: the real impact of surgical margin. Eur J SurgOnc. 1998;24:174–179.
23. Jarnagin WR, Gonen M, Fong Y, et al. Improvement in perioperativeoutcome after hepatic resection: analysis of 1,803 consecutive cases overthe past decade. Ann Surg. 2002;236:397–406.
24. Wood CB, Gillis CR, Blumgart LH. A retrospective study of naturalhistory of patients with liver metastasis from colorectal cancer. ClinOncol. 1976;2:285–288.
25. Wagner JS, Adson MA, van Heerden JA. The natural history of hepaticmetastasis from colorectal cancer. Ann Surg. 1984;199:502–508.
26. Cady B, Moson DO, Swinton NW. Survival of patients after colonicresection for carcinoma with simultaneous liver metastasis. Surg GynObst. 1970;131:697–700.
27. Tournigand C, Andre T, Achille E, et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: a randomizedGERCOR study. J Clin Oncol. 2004;22:229–237.
28. Grothey A, Sargent DJ, Morton RF, et al. Survival of patients withadvanced colorectal cancer improves with the availability of fluoroura-cil-leucovorin, irinotecan and oxaliplatin in the course of treatment.J Clin Oncol. 2004;22:1209–1214.
29. Goldberg RM, Sargent DJ, Morton RF, et al. A randomized controlledtrial of fluorouracil plus leucovorin, irinotecan and oxaliplatin combi-nations in patients with previously untreated metastatic colorectal can-cer. J Clin Oncol. 2004;22:23–30.
30. Parikh AA, Gentner BM, Wu TT, et al. Perioperative complications inpatients undergoing major liver resection with or without neoadjuvantchemotherapy. J Gastrointest Surg. 2003;7:1082–1088.
Are et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins300

ORIGINAL ARTICLES
Impact of Graft Type on Outcome in Pediatric LiverTransplantation
A Report From Studies of Pediatric Liver Transplantation (SPLIT)
Ivan R. Diamond, MD,* Annie Fecteau, MD,* J. Michael Millis, MD,† Julian E. Losanoff, MD,‡Vicky Ng, MD,* Ravinder Anand, PhD,§ Changhong Song, PhD,§ and the SPLIT Research Group
Objective: To examine the outcome of technical variant livertransplant techniques relative to whole organ liver transplantation inpediatric liver transplant recipients.Background: Technical variant liver transplant techniques compris-ing split, reduced, and live-donor liver transplantation evolved toaddress the need for timely and size appropriate grafts for pediatricrecipients.Methods: Analysis of data from the Studies of Pediatric LiverTransplantation (SPLIT) registry, a multicenter database of 44 NorthAmerican pediatric liver transplant programs. The outcome (mor-bidity and mortality) of each of the technical variants were com-pared with that of whole organ recipients.Results: Data were available on 2192 transplant recipients (1183whole, 261 split, 388 reduced, and 360 live donor). Recipients of alltechnical variant graft type were significantly younger than wholeorgan recipients, but on average spent 2.3 months less on the waitinglist. Thirty-day post-transplant morbidity was increased for eachtype of technical variant relative to whole organ (45.1% whole,66.7% split, 65.5% reduced, 51.9% live-donor). Biliary complica-tions (30 day: 7.5% whole, 18.8% split, 16% reduced, 17.5%live-donor) and portal vein thrombosis (30 day: 3.6% whole, 8%split, 8% reduced, 7.5% live-donor) were more common in alltechnical variant types. Graft type was an independent predictor of
graft loss (death or retransplantation) in a multivariate analysis. Splitand reduced (relative risk � 1.74 and 1.77, respectively) grafts hada worse outcome when compared with whole organ recipients.Conclusions: Technical variant techniques expand the pediatricdonor pool and reduce time from listing to transplant, but they areassociated with increased morbidity and mortality.
(Ann Surg 2007;246: 301–310)
Liver transplantation is considered to be an accepted treat-ment method for children and adults with end-stage liver
disease, with survival rates approaching 90%.1 However, thedemand for livers is far greater than the supply, and technicalvariant transplant techniques have been developed to increasethe availability of organs for transplantation. These tech-niques are based on the principle that a partial liver graft withappropriate arterial and portal inflow, the corresponding ve-nous and biliary drainage, and sufficient hepatocyte mass isable to fulfill the role of a whole organ.2 There are 3 technicalvariant techniques, namely, reduced,3 split,4 and live-do-nor.5,6 Reduced grafts arise when a graft is “cut-down” basedon segmental anatomy, and the segments not transplanted arediscarded. Since there is only 1 recipient, there is no need toshare portal structures, thus maximizing the length of conduitfor biliary and vascular anastomosis. Although the reducedtechnique expands the pediatric donor pool, this is to thedetriment of adult recipients.7 Consequently, split techniquesevolved, whereby a liver is divided such that it can betransplanted into 2 recipients. Live-donor techniques were adirect extension of split liver transplantation, whereby apartial liver graft from a live-donor is transplanted.
Studies of Pediatric Liver Transplantation (SPLIT) wasestablished in 1995, with the primary objective to character-ize and follow trends in patient and graft survival, rejection,growth, and immunosuppression to identify the potentialmorbidity and mortality factors and patterns of graft failure.Herein, we present the surgical outcomes from the SPLITdatabase with particular attention to variations in outcome bytype of graft.
From the *Pediatric Academic Multiorgan Transplant Program, The Hospitalfor Sick Children, Toronto, Canada; †Section of Transplantation, Uni-versity of Chicago, Chicago, Illinois; ‡Department of Surgery, John D.Dingell VAMC and Section of Transplantation, Wayne State University,Detroit, Michigan; and §The Emmes Corporation, Rockville, Maryland.
Supported by the National Institute of Diabetes and Digestive and KidneyDiseases, National Institutes of Health (U01-DK061693-01A1), AstellasPharma US, (unrestricted grant), Roche Laboratories (unrestricted grant),Johnson and Johnson Medical Products Surgeon Scientist Program Fel-lowship, Department of Surgery, University of Toronto (I.D.), andFellowship award, Canadian Institutes of Health Research (I.D.).
Presented in part at the 2003 American Transplant Congress in Washington,DC.
Reprints: J. Michael Millis, MD, Section of Transplantation, MC 5026,Room J 517, 5841 South Maryland Avenue, Chicago, Illinois 60637.E-mail: [email protected].
Address correspondence to: Annie Fecteau, MD, Division of General Sur-gery, The Hospital for Sick Children, 555 University Avenue, Room1526, Toronto, Ontario M5M 4N8. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0301DOI: 10.1097/SLA.0b013e3180caa415
Annals of Surgery • Volume 246, Number 2, August 2007 301

METHODSWe analyzed prospectively collected data by SPLIT
since 1995. At the time of data closure for this report, June 1,2006, 44 centers in the United States and Canada had regis-tered 3161 patients, with 2445 of them receiving at least 1transplant (0 to 212 patients per center). Participation in theSPLIT registry was approved by each center’s institutionalreview board, and all parents or legal guardians providedwritten informed consent; subject assent was also obtainedwhen appropriate.
Enrolled patients are followed every 6 months for 2years and then yearly from the time of listing to transplant.After transplant, enrollees are followed every 6-months for 2years and then yearly thereafter until the 18th birthday. Datacaptured include demographics, primary diagnosis, pretrans-plant conditions and morbidity, surgical data, perioperativeand long-term morbidity such as lymphoproliferative disease,rejection, retransplantation, and death.
Data AnalysisWe analyzed data for all children who received their
first liver transplant between the inception of SPLIT in 1995and June 1, 2006. Children were excluded if they receivedany grafts in addition to the liver. Univariate statisticalanalyses included �2 or Fisher exact test to make comparisonsbetween categorical variables, Wilcoxon rank sum test forcomparison of means, and log-rank test for comparison oftime to event outcomes. A P value of 0.05 was considered tobe statistically significant and values between 0.05 and 0.1 atrend. All statistical analyses were performed using the SASSystem for Windows, version 8.02 (SAS Institute, Cary,NC.).
Statistical AnalysesImpact of Graft Type
Subjects were grouped according to graft type (whole,split, reduced, live-donor) for the primary analyses regardingmorbidity. In all cases, each group of patients who receiveda technical variant graft (split, reduced, live-donor) wasindividually compared with those who received a wholeorgan. Morbidity at 30 days was assessed for all patients whounderwent transplantation. However, to obtain estimates oflong-term morbidity (at 24 months), data were only analyzedfor those who survived to that point and had undergone a24-month follow-up visit. Causes of graft loss (death orretransplantation) were also tabulated. Kaplan-Meier curveswere generated to examine the impact of graft type on graftand patient survival, as well as time to first episode ofrejection.
Predictors of Graft LossTo assess the impact of graft type on outcome when
adjusting for other significant predictors, univariate analysesusing a Cox proportional hazards model were performed toexamine factors predictive of a composite outcome of graftloss, which was defined as either death or retransplantation.Both donor and recipient factors were considered for inclu-sion in the model, as was the type of immunosuppressant
used and use of polyclonal antibodies. To account forchanges in the field of liver transplantation over time, year oftransplant was also considered in the analyses.
For the development of the multivariate model to pre-dict post-transplant survival, factors significant at P � 0.20 inthe univariate analyses were initially included. Model reduc-tion was performed using the backward elimination variableselection method. Factors remaining significant at P � 0.05were maintained in the final model. To control for center-specific effects, we performed 2 analyses. In the frailtymethod, each center was assumed to have a random effectthat indicates the possibility of different baseline risks forpatients at different centers. The robust variance method wasalso used to adjust for the possible correlations for thetransplants at the same center using a robust “sandwich”variance approach.
RESULTSDuring the index time period, 2291 children received
their first liver transplant. Data on graft type was unavailablefor 99 (4.3%) children and these were excluded; thus, thestudy population comprised 2192 children. One thousandeight hundred thirty-two liver (1832) transplants were per-formed using deceased donors (1183 whole organ, 261 split,and 388 reduced). Three hundred and sixty (360) childrenreceived grafts from live-donors.
Demographic data are presented in Table 1. Those whoreceived a split or reduced graft were more likely to betransplanted for acute liver failure. Acuity of disease asevidenced by the distribution of the intensity of care received,or the mean calculated pediatric end-stage liver disease scoreper group was greater in all of the technical variant groupsrelative to whole organ. Also, younger children were morelikely to receive a technical variant graft. Only 33.9% (260 of766) of patients 1-year-old or younger received a whole organcompared with 49.1% (358/729) of patients aged 1–5 years,65.3% (309 of 473) aged 5–12, and 79.4% (255 of 321) ofthose 12 years or older. All technical variant graft types spentless time on the waiting list relative to whole organ recipients�5.9 months whole vs. 4.1 month split (P � 0.003), 3.1 monthreduced (P � 0.001), 3.6 months live-donor (P � 0.0002)�.
Operative DetailsDetails of the operative techniques employed are pre-
sented in Table 2. Roux-en-Y choledochojejunostomy wasthe predominant type of biliary reconstruction in all patients,although it was more frequently used in those undergoing atechnical variant transplant. Twenty nine percent of patientswho underwent whole organ transplantation had a duct-to-duct anastomosis, whereas the range for the technical varianttypes was between 5.8% and 10.6%. Although the operatingtime for split and live-donor and transplants were statisticallylonger than for whole organ (7.1 and 7.5 hours vs. 6.7 hours,respectively), the difference was small and not of clinicalsignificance. Similarly, there were small but statistically sig-nificant differences in ischemic and anhepatic times betweenthe technical variants and whole organ transplants. As wouldbe expected, those who underwent a live-donor transplant hada significantly shorter cold-ischemia time (2.8 hours vs. 7.8
Diamond et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins302

hours for whole organ, P � 0.001). The average amount ofblood per kilogram body weight required for transplant re-cipients of whole donor organs was significantly lower thanrequired for each of the technical variant types.
Morbidity Within 30 Days of TransplantData on morbidity within the first 30 days are presented
in Table 3. Those receiving one of the technical variant grafts
were more likely to develop complications within 30 days oftransplant �66.7% (P � 0.001) split, 65.5% (P � 0.001)reduced, 51.9% (P � 0.01) live-donor� than those whoreceived a whole organ graft (45.1%). Those undergoing atechnical variant procedure also were more likely to requirereoperation within 30 days of transplant. 29.5% of those whoreceived a whole-organ underwent reoperation, whereas theproportion in the technical variant groups were 47.1%
TABLE 1. Demographics
Whole Liver Split Reduced Live-Donor
N 1183 261 388 360
Age (yr) �mean (SE)� 6.6 (0.2) 3.2* (0.3) 3.2* (0.2) 2.6* (0.2)
Gender
Male (%) 572 (48.4) 114 (43.7) 166 (42.8) 164 (45.6)
Months from listing to transplant[mean (SE)]
5.9 (0.3) 4.1* (0.5) 3.1* (0.3) 3.6* (0.5)
Months of follow-up �mean (SE)� 32.6 (0.8) 25.9* (1.5) 36.5 (1.7) 33.3 (1.6)
Indication for transplant†(%)
Acute liver failure 160 (13.5) 46 (17.6) 76* (19.6) 37 (10.3)
Chronic liver disease 1023 (86.5) 215* (82.4) 312* (80.4) 323 (89.7)
Pretransplant status†(%)
Intensive care unit 276 (23.3) 95* (36.4) 127* (32.7) 74* (20.6)
Continuous hospital 160 (13.5) 45* (17.2) 81* (20.9) 83* (23.1)
Not hospitalized 741(62.6) 120* (46) 179* (46.1) 203* (56.4)
Calculated PELD score �mean (SE)� 11.6 (0.4) 16.7* (0.9) 18.2* (0.8) 16.6* (0.8)
*P � 0.05.†For categorical variables, the Fisher exact test was used to examine the distribution of categories relative to whole liver.
TABLE 2. Operative Details
Whole Liver Split Reduced Live-Donor
N 1183 261 388 360
Procedure type† (%)
Orthotopic standard 776 (65.6) 69 (26.4) 190 (49) 0 (0)
Piggyback 403 (34.1) 189 (72.4) 194 (50) 341 (94.7)
Auxillary 3 (0.3) 1 (0.4) 3 (1) 2 (0.6)
Biliary reconstruction† (%)
Roux-end-Y 820 (69.3) 223 (85.4) 328 (84.5) 318 (88.3)
Duct-to-duct 345 (29.2) 22 (8.4) 41 (10.6) 21 (5.8)
Other 7 (0.6) 13 (5) 16 (4.1) 8 (2.2)
Arterial reconstruction† (%)
End-to-end 968 (81.8) 210 (80.5) 250 (64.4) 306 (85)
End-to-side 69 (5.8) 26 (10) 85 (21.9) 11 (3.1)
Interposition 127 (10.7) 22 (8.4) 46 (11.9) 25 (6.9)
Portal reconstruction-donor PV to† (%)
Portal vein 1132 (95.7) 238 (91.2) 362 (93.3) 328 (91.1)
Superior mesenteric 12 (1.0) 6 (2.3) 10 (2.6) 6 (1.7)
Other vein 22 (1.9) 11 (4.2) 10 (2.6) 11 (3.1)
Operative time (hr) �mean (SE)� 6.7 (0.1) 7.1* (0.2) 6.7 (0.1) 7.5* (0.2)
Warm ischemia (min) �mean (SE)� 48.9 (0.6) 51.8 (1.6) 51.6* (1.1) 48.8 (1.4)
Cold ischemia (hr) �mean (SE)� 7.8 (0.1) 7.3* (0.2) 8.4* (0.1) 2.8* (0.2)
Anhepatic time (min) �mean (SE)� 67.1 (2.0) 70.2* (2.9) 67.0* (2.1) 68.3* (2.1)
Volume transfused (mL) �mean (SE)� 49.2 (2.3) 88.4* (7.0) 104.0* (5.6) 87.2* (5.5)
*P � 0.05; all P-values are relative to whole liver.†Statistical comparisons not done.
Annals of Surgery • Volume 246, Number 2, August 2007 Pediatric Liver Transplantation
© 2007 Lippincott Williams & Wilkins 303

(P � 0.001) split, 51.0% (P � 0.001) reduced, and 41.9%(P � 0.001) of live-donor grafts. Furthermore, 3 or morereoperations were conducted in 5.0% of those with a splitorgan (P � 0.2), 7.7% of the recipients receiving a reducedorgan (P � 0.001), and in 8.1% of live-donor recipients (P �0.001). Only 3.1% of the whole organ recipients were thusaffected.
Patients who received any of the technical variant graftswere more likely to experience biliary tract leaks. The overallincidence of vascular complications was only increased forthose who received a reduced graft, whereas all technicalvariant graft types were associated with an increased inci-dence of portal vein thrombosis. The incidence of portal veinthrombosis was at least double that of whole organ for allgroups. Mortality within 30 days was increased for recipientsof split and reduced grafts, although only recipients of splitgrafts were more likely to be retransplanted during this timeperiod. The incidence of other gastrointestinal complicationswas increased for the technical variant grafts, as was the inci-dence of pulmonary complications for all technical variant typesand cardiac complications for split and reduced recipients.
Patients who received a graft from a live-donor weresignificantly less likely than those who received a wholeorgan graft (3.6% vs. 7.0%, P � 0.007) to develop diabetesor glucose intolerance. As well, patients who received alive-donor graft were less likely, at any point following thetransplant, (RR 0.82; 95% CI: 0.68–0.99; P � 0.034) toexperience rejection than those who received a whole organ.Recipients of split (P � 0.217) and reduced (P � 0.326)grafts had similar incidences of rejection relative to wholeorgan. By 1-year, 46.6% of those who received a wholeorgan, 49.6% split, 44.4% reduced, and 40.5% live-donor hadexperienced at least 1 rejection episode.
Morbidity at 2 YearsMorbidity experienced by those who survived to 24
month post-transplant is presented in Table 4. This cohortcomprised 1245 patients (672 whole, 130 split, 221 reduced,and 197 live-donor). Before 24 months, 240 children died (88whole, 35 split, 67 reduced, and 41 live-donor). The remain-ing 807 children had not yet reached their 24-month follow-up, or did not have data for that visit. The overall incidenceof complications in the first 24-months was greater for eachof the technical variant types relative to the whole organgroup. The overall incidence of vascular complications wasincreased in recipients of technical variant grafts, primarilydue to an increased risk of portal vein thrombosis in all grafttypes. There was also a significantly greater incidence ofbiliary tract complications among recipients of technicalvariants. All types were associated with an increased inci-dence of leaks; recipients of reduced and live-donor graftshad an increased incidence of intrahepatic biliary strictures�8.1% reduced (P � 0.005), 10.2 live (P � 0.001) vs. 3.6%whole organ�. Recipients of live-donor grafts also had a2-fold increase in the incidence of anastomotic strictures. Theincidence of other gastrointestinal and other nongastrointes-tinal complications was also increased in recipients of thetechnical variant types.
Graft and Patient SurvivalIn univariate analyses graft and patient survival were
superior in children who received a whole organ relative tothose who received a technical variant graft. Kaplan-Meiercurves for graft and patient survival are presented in Figures1 and 2, respectively. All 3 technical variant techniques wereassociated with decreased graft survival relative to wholeorgan (split RR: 1.496, 95% CI: 1.107–2.022; reduced RR:
TABLE 3. Complications Within 30 Days of Transplant
Whole Liver Split Reduced Live-Donor
N 1183 261 388 360
N with complication (%) 533 (45.1) 174* (66.7) 254* (65.5) 187* (51.9)
Death 36 (3.0) 18* (6.9) 29* (7.5) 13 (3.6)
Retransplantation 61 (5.2) 22* (8.4) 20 (5.2) 22 (6.1)
Biliary complication 89 (7.5) 49* (18.8) 62* (16.0) 63* (17.5)
Leak 44 (3.7) 41* (15.7) 46* (12.0) 53* (14.7)
Intrahepatic stricture 8 (0.7) 3 (1.1) 4 (1) 4 (1.1)
Anastomotic stricture 30 (2.5) 3 (1.1) 16 (4.1) 11 (3.1)
Vascular complication 155 (13.1) 36 (13.8) 67* (17.3) 56 (15.6)
Hepatic artery thrombosis 99 (8.4) 15 (5.7) 28 (7.2) 24 (6.7)
Portal vein thrombosis 42 (3.6) 21* (8.0) 31* (8.0) 27* (7.5)
Other vascular 27 (2.3) 7 (2.7) 19* (4.9) 11 (3.1)
Other GI complications 83 (7.0) 38* (14.6) 55* (14.2) 40* (11.1)
CNS complications 90 (7.6) 18 (6.9) 24 (6.2) 21 (5.8)
Renal complication 67 (5.7) 20 (7.7) 34* (8.8) 19 (5.3)
Pulmonary complications 121 (10.2) 52* (19.9) 92* (23.7) 49 (13.6)
Cardiac complications 28 (2.4) 11 (4.2) 21* (5.4) 13 (3.6)
Hematologic complications 38 (3.2) 8 (3.1) 16 (5.4) 15 (4.2)
Diabetes/glucose intolerance 83 (7.0) 21 (8.0) 32 (8.2) 13* (3.6)
Other complications 158 (13.4) 44 (16.9) 90* (23.2) 43 (11.9)
*P � 0.05; all P values are relative to whole liver.
Diamond et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins304

1.841, 95% CI: 1.454–2.322; live donor RR: 1.321, 95% CI:1.007–1.732). In terms of patient survival, those who re-ceived a split (RR: 1.603; 95%CI: 1.094–2.349) or reducedgraft (RR: 2.11; 95% CI: 1.571–2.835) and were less likely tosurvive than recipients of a whole organ. Those who under-went a live-donor transplant had similar survival relative tothose who received a whole-organ (RR: 1.366; 95% CI:0.962–1.941; P � 0.082). Indications for retransplantationand causes of death are listed in Table 5.
Multivariate Predictors of SurvivalTo control for other confounders and to better under-
stand the impact of graft type on survival, we performed amultivariate Cox proportional hazards regression. The out-come for this analysis was graft loss as defined by eitherdeath or retransplantation. The factors that were initially
included the multivariate model (P � 0.2 in univariate anal-yses) were: primary diagnosis (P � 0.001), graft type (P �0.001), donor age (P � 0.001), patient status at transplant (P� 0.001), year of transplant (P � 0.0005), warm ischemiatime (P � 0.001), donor–recipient blood type match (P �0.001), International Normalized Ratio (P � 0.001), bilirubin(P � 0.009), intravenous immune globulin use in the first 7days post-transplantation (P � 0.15), initial immunosuppres-sant (P � 0.002), and monoclonal antibody use (P � 0.013).Although the pediatric end-stage liver disease score metcriteria for inclusion in the model (P � 0.001), due toconcerns of collinearity with its components of internationalnormalized ratio and bilirubin, it was excluded from themodel. Recipient age did not meet statistical criteria forinclusion in the model (P � 0.204), although a secondary
TABLE 4. Complications Experienced by Patients Surviving to 24 Months
Whole Liver Split Reduced Live-Donor
No. 672 130 221 197
No. with complication (%) 480 (71.4) 109* (83.8) 192* (86.9) 163* (82.7)
Biliary complication 116 (17.3) 37* (28.5) 56* (25.3) 79* (40.1)
Leak 39 (5.8) 23* (17.7) 33* (17.8) 43* (21.8)
Intrahepatic stricture 24 (3.6) 7 (5.4) 18* (8.1) 20* (10.2)
Anastomotic stricture 52 (7.7) 14 (10.8) 24 (10.9) 42* (21.3)
Vascular complication 111 (16.5) 31* (23.8) 52* (23.5) 48* (24.4)
Hepatic artery thrombosis 58 (8.6) 6 (4.6) 16 (7.2) 12 (6.1)
Portal vein thrombosis 35 (5.2) 16* (12.3) 21* (9.5) 27* (13.7)
Other vascular 40 (6.0) 14* (10.8) 22* (10) 21* (10.7)
Other GI complications 126 (18.8) 74* (36.2) 64* (29.0) 50* (25.4)
Other complications 416 (61.9) 95* (73.1) 173* (78.3) 127 (64.5)
*P � 0.05; all P values are relative to whole liver.
FIGURE 1. Kaplan-Meier probability of patient survival. FIGURE 2. Kaplan-Meier probability of graft survival.
Annals of Surgery • Volume 246, Number 2, August 2007 Pediatric Liver Transplantation
© 2007 Lippincott Williams & Wilkins 305

analysis was performed, to ensure that its absence did notsignificantly alter the final multivariate model.
The final multivariate model is presented in Table 6.
Graft type, primary diagnosis, donor–recipient blood typematch, donor age, year of transplant, and warm ischemia timeremained significant predictors of graft loss. Children who
TABLE 5. Death and Retransplantation
Whole Liver Split Reduced Live-Donor
N 1183 261 388 360
Retransplantation
Number retransplanted (%)* 107 (9.0) 33 (12.6) 53. (13.7) 40 (11.1)
Indications
Primary graft dysfunction 23 (21.5) 11 (33.3) 11 (20.8) 7 (17.5)
Acute rejection 5 (4.7) 0 (0) 1 (1.9) 2 (5)
Chronic rejection 14 (13.1) 3 (9.1) 8 (15.1) 1 (2.5)
Vascular complication 41 (38.3) 10 (30.3) 16 (30.2) 17 (42.5)
Biliary complication 2 (1.9) 2 (6.1) 6 (11.3) 4 (10)
Infectious complication 2 (1.9) 0 (0) 0 (0) 0 (0)
Other 20 (18.7) 7 (21.2) 11 (20.8) 9 (22.5)
Death
N died (%)* 107 (9.0) 35 (13.4) 75 (19.3) 44 (12.2)
Cause of death
Graft failure 8 (7.5) 7 (20.0) 2 (2.7) 2 (4.5)
Vascular complication 10 (9.3) 2 (5.7) 5 (6.7) 1 (2.3)
Rejection 3 (2.8) 1 (2.9) 0 (0) 0 (0)
Liver tumor 7 (6.5) 3 (8.6) 3 (4.0) 1 (2.3)
Other malignancy 0 (0) 0 (0) 1 (1.3) 0 (0)
Recurrent liver disease 4 (3.7) 2 (5.7) 3 (4.0) 1 (2.3)
Infectious 25 (23.4) 4 (11.4) 26 (34.7) 12 (27.3)
Neurologic 13 (12.1) 4 (11.4) 11 (14.7) 4 (9.1)
Cardiorespiratory 10 (9.3) 2 (5.7) 9 (12.0) 11 (25.0)
Multiple organ failure 16 (15.0) 6 (17.1) 7 (9.3) 7 (15.9)
Other 11 (10.3) 4 (11.4) 8 (10.7) 5 (11.4)
No statistical comparisons done.*Percentage relative to entire cohort, all other percentages are of those who were retransplanted or died.
TABLE 6. Multiple Variable Predictors of Graft Loss
Factor A B Relative Risk* (95% CI)
Graft type Whole Split 1.74† (1.17–2.58)
Reduced 1.77† (1.30–2.41)
Live donor 1.19 (0.77–1.84)
Primary diagnosis Biliary atresia Other cholestatic 0.97 (0.71–1.33)
Fulminant liver failure 1.61† (1.13–2.28)
Cirrhosis 1.28 (0.80–2.03)
Other 1.74† (1.20–2.53)
Donor–recipient blood match Identical Compatible 1.36† (1.01–1.85)
Incompatible 1.53 (0.86–2.72)
Donor age 1–17 yr 0–5 mo 2.54† (1.59–4.05)
6–11 mo 1.67 (0.89–3.15)
18–49 yr 1.24 (0.90–1.69)
� 50 yr 1.61 (0.92–2.80)
Year of transplant �2002 �2001 1.52 (1.18–1.96)
Warm ischemia time continuous predictor (min) 1.01† (1.00–1.02)
*Relative risk �1 implies patients in group B have higher risk of outcome compared with group A. Relative risks and thecorresponding confidence intervals are adjusted for other factors in the model.
†P � 0.05.CI indicates confidence intervals.
Diamond et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins306

received a split (RR � 1.74) or reduced (RR � 1.54) graftwere more likely suffer graft loss than those who received awhole organ. Recipients of grafts from live-donors did nothave a worse outcome. In terms of diagnosis, children withfulminant liver failure as well as those with disease other thanother cholestatic diseases or cirrhosis were more likely to expe-rience graft loss than those with biliary atresia. Children under-going transplant from a donor with a nonidentical blood type hada worse outcome, as did those transplanted before 2002. Youngdonors, less than 5 months of age, also had an increased riskfor graft loss. Warm ischemia time, included as a continuousvariable, was a predictor of graft loss, with each additionalminute of ischemia resulting in a decrement in survival.
The analyses for center-specific effects failed to dem-onstrate that center was a significant confounder in explainingthe differential survival of the various graft types. The dif-ferences between graft types observed using the standardanalysis remained significant in the robust-variance approachto account for center variations. The variance of the centerrandom effects in the frailty model was 0.084 (P � 0.06),which does not provide evidence for a center-specific effectin explaining our results.
DISCUSSIONLiver transplantation is considered to be the standard of
care for children and adults with end stage liver disease.1
However, the promise of transplantation is limited by theavailability of donor organs for transplant. Historically, thisshortage was most acute for pediatric recipients because ofthe need for size matching of donors and recipients. Toaddress this disparity, surgeons developed technical varianttransplant techniques (split, reduced, and live-donor) for thepediatric population.2 The literature suggests no difference intransplant survival for technical variants relative to wholeorgan transplantation in a number of pediatric series describ-ing the experience of high-volume centers.8–10 By contrast,reports of major cumulative series indicated improved out-come for whole organs versus the technical variant types,particularly reduced and split transplants.11 Although live-donor grafts in some series have demonstrated either equiv-alent or even a survival advantage over whole organ trans-plantation,12,13 with the possibility that this advantage may bemost apparent in those less than 2-years of age.14
The present study was an analysis of the outcome of2192 children undergoing liver transplantation at 1 of the 44participating centers of the SPLIT research group over an11-year period. Our univariate results demonstrated worseoverall graft survival for all of the technical variant tech-niques and worse patient survival for those undergoing splitand reduced liver transplantation with a trend to worsesurvival for those undergoing transplantation from a live-donor. However, on a multivariate analysis, with the com-posite outcome of graft loss (death or retransplantation), bothsplit and reduced graft types had a worse outcome relative towhole organ. Recipients of organs from live-donors did notdemonstrate this disadvantage. The other variables that pre-dicted graft loss were primary diagnosis, donor–recipientblood type match, donor age, year of transplant, and warm
ischemia. All of the technical variant transplant types werealso associated with an increased risk of complications bothat 30 days post-transplantation and in those who survived to24 months.
It is important to put the relative poorer outcome oftechnical variant techniques into perspective. At 1-year,whole organs had a 93% patient survival rate, whereas therate for reduced was 83.2%, split 87%, and live-donor 89%.Four-year survival was 89% whole, 79% reduced, 85% split,and 85% live-donor. Thus, although relative to a wholeorgan, reduced and split grafts have a slightly decreasedprobability of survival, the overall results for each of thetransplant types are excellent. The slight decrement in overallsurvival must be balanced with the fact that almost all ofthese children would have died without transplantation, par-ticularly when one considers the generally higher acuity ofpatients receiving technical variant grafts.
It must also be noted that using technical variant tech-niques significantly decrease the waiting list mortality.2,9 Inthis study, patients receiving a technical variant waited onaverage 2.3 months less than those who received a wholeliver. This highlights the fact that the relative decrease inpost-transplantation survival needs to be balanced with thegains in survival to transplant. Redding et al using Whiting-ton’s method to calculate an overall survival based on pre-transplant and post-transplant survival,15 demonstrated a sig-nificant advantage to live-donor over deceased-donor (87%vs. 70%) transplantation primarily due to enhanced survivalprior to transplant. Thus, although associated with slightdecrements in post-transplantation survival, because of the ex-cellent overall outcome and significant improvements in graftavailability and survival to transplant as a result of the technicalvariant techniques, the net effect of such techniques is of sig-nificant benefit to the pediatric patient with liver failure.
Despite the excellent overall results, it is still importantto note and understand the increased morbidity of technicalvariant procedures with the ultimate goal of developingstrategies to overcome these challenges. The perioperativemorbidity after pediatric liver transplantation typically in-cludes biliary, portal, and arterial complications, followed byintestinal perforation and bleeding.16 Biliary complications inour series included bile leaks and anastomotic strictures. All3 technical variant types had an increased incidence of bileleak at 30-days ranging from 12.0% for recipients of reducedgrafts to 15.7% for split recipients. The corresponding inci-dence in recipients of whole organ grafts was 3.7%. Recipi-ents of both reduced and live-donor grafts had an increasedincidence of stricture at 24-months post-transplantation. Mul-tiple hepatic ducts and damage to the delicate peribiliaryvasculature are said to increase the complication rate. Tech-nical maneuvers such as stentless microsurgical biliary re-construction and enteric biliary drainage are known to sig-nificantly lower the incidence of anastomotic strictures andbile leaks.17,18 Given the increased incidence of biliary com-plications among recipients of technical variant grafts, webelieve that potential improvement in the biliary morbiditycan be expected by future microsurgical advances. The im-portance of these advances is highlighted by the outcome at
Annals of Surgery • Volume 246, Number 2, August 2007 Pediatric Liver Transplantation
© 2007 Lippincott Williams & Wilkins 307

24-months post-transplantation. At this time point, over 20%of recipients of reduced grafts and 30% of live-donor recip-ients had biliary tract strictures (intrahepatic or anastomotic).These numbers must be interpreted in the context that all ofthe patients who were included in these analyses had survivedto 24 months, and thus they are successes that we strive for,and a significant long-term biliary complication in more than1 in 5 is concerning. Clearly, there is yet much that needs tobe done to improve the outcome for these patients.
The spectrum of vascular complications after pediatricliver transplant is related to both the venous and arterialsupply of the graft. Reconstructions of the portal venoussupply in the pediatric population varies from slight portalvein mismatches in size-matched donor to significant discrep-ancies in diameter and decreased length in live-donorgrafts.19 More reconstructions can be successfully performedusing interposition grafts; however, these are associated witha significant increase in complications.20,21 Such reconstruc-tions are more frequently employed in technical variant livertransplantation. We considered type of biliary and vascularreconstruction in our univariate analyses of graft loss; how-ever, these did not achieve statistical significance for consid-eration in the multivariate model.
The incidence of hepatic artery thrombosis has beenreported to be as high as 26% and is among the major causesfor graft loss.22,23 Very young age and small body mass areprobably the most significant risk factors, although thesefactors can be overcome with microvascular techniques.24,25
In this series, none of the technical variant techniques wereassociated with an increased risk of hepatic artery thrombo-sis, and at 30 days, the overall incidence of this complicationwas 7.5%. Although the nature of our data does not permitone to address the reasons for the low incidence of hepaticartery thrombosis, one can speculate that this may be due toan increase in the use of microvascular techniques for arterialreconstruction.
Portal venous thrombosis was a more common compli-cation among recipients of all technical variant grafts both at30 days and 24 months post-transplantation. The increasedrisk of portal venous thrombosis among live-donor recipientswas previously identified by Millis et al.20 However, webelieve that in the same way that microvascular techniqueshave resulted in a reduction in hepatic arterial complications,such techniques may play a role in future advances in portalreconstruction.
It is unclear why children who received technical vari-ant grafts had an increased risk of cardiac, pulmonary, andrespiratory complications, but it is important to note thatpatients tended to be younger and sicker at the time oftransplant. Although the differences in pretransplant clinicalstatus may explain these discrepancies in outcome, graft typewas an independent predictor of graft loss on multivariateanalysis, which controlled for baseline acuity. Therefore, onecannot fully account for the increased risk of morbidity andmortality following a technical variant procedure on the basisof differences in pretransplant acuity. A recent study foundthat the perioperative complications were independent riskfactors for survival.26 Thus, the detrimental impact of graft
type on survival may be related to the increased incidence ofimmediate perioperative complications experienced by recip-ients of technical variant grafts. Thus, surgical innovations,such as increased use of microsurgical reconstructive tech-niques, not only have the potential to improve immediateperioperative outcome but also survival.
Technical variant graft types were associated with anincreased need for blood transfusion. Although speculative, itis intriguing to consider that the increased risk of systemiccomplications around the time of transplant may be partiallyrelated to this. Perioperative transfusions are associated withan increased risk of infection and systemic complications inadult patients27 and previous reports have demonstrated thata high blood loss correlates with poor patient outcome afterliver transplantation.28 A recent report demonstrated thatperioperative normovolemic anemia, with a target hemoglo-bin concentration between 8 and 9 g/dL, was safe in pediatriclive-donor transplants.29 Such a strategy warrants furtherconsideration in a larger trial, and this may be achievable viaa multicenter network such as the SPLIT research group.
Age was not an independent predictor for graft loss onunivariate analyses, and was not included in the multivariateanalysis. This is in contrast to a previous report on a largeseries of pediatric liver transplant recipients.26 In secondaryanalyses, we included age for consideration in the multivar-iate model, as a multicategory variable, continuous variable,and dichotomous variable (� or �1 year). However, agenever achieved statistical significance for inclusion in ourfinal multivariate model. Age is closely associated with grafttype as well as primary disease, both of which were includedin the final model. Therefore, it is possible that age did notmeet inclusion in the multivariate model because of its tightrelationship to these variables. However, an alternate inter-pretation that may be drawn from these data is that the notionthat younger children have a worse outcome has to do withthe fact that younger children were more likely to receive atechnical variant graft. It may not have been possible, giventhe small number of patients with each type of technicalvariant graft in the previous report,26 to statistically examinethe impact of graft type. Thus, age was viewed to be theimportant predictor rather than graft type. A recipient’s age,size, and acuity are the primary features that guide the choiceof graft. Although it would be optimal to transplant onlywhole livers and minimize complications, the unfortunatecurrent limited availability of organs for transplantation pre-cludes this possibility.
This analysis based on data from a registry has anumber of limitations and biases, both known and unknown.First, participation in SPLIT is voluntary, and therefore maybe subject to bias. Second, it is not possible to perform 100%verification of accuracy and completeness of data submittedto the data-coordinating center. Site visits are conductedevery 2 years. Third, given that centers with a wide range ofexperience contribute data to SPLIT, discrepancies betweenthe outcome of a large series such as this and smaller singlecenter series may be related to center-specific effects. How-ever, we were not able to demonstrate any center-specificeffects in interpreting the impact of graft type on the proba-
Diamond et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins308

bility of graft loss. Despite the limitations afforded by regis-try data, our results are important both as they provide aninsight into the cumulative experience in managing childrenundergoing liver transplantation but also in that they may beused to generate hypotheses for future studies.
In conclusion, our analysis of the differential outcomesof various graft types in the SPLIT registry clearly demonstratesthat despite significant advances, there is a differential outcomefor recipients of split and reduced grafts. This is in contrast tosingle center series, and may be related to the enhanced statis-tical power of this large series. The challenge from a surgicalperspective is to continue to improve on the technical varianttechniques and as such ultimately improve outcome. Webelieve the fact that children who were transplanted after2002 had improved survival rates is evidence that technicalinnovations can improve outcome. As the SPLIT registrycontinues to accumulate data, we shall continue to activelytrack the outcome and advances in managing these challeng-ing and important patients.
ACKNOWLEDGMENTSThe SPLIT Research Group are: S. Dunn, J. Menendez,
L. Flynn (Alfred I Dupont Hospital for Children, Wilmington,DE); M. Jonas, L. Krawczuk, M. Christoff (Boston Children’sHospital, Boston, MA); R. Kane, E. Phillips, L. Ferrer (Car-dinal Glennon Children’s Hospital, St. Louis University, St.Louis, MO); T. Heffron, J. DePaolo, T. Pillen, L. Davis (Chil-dren’s Healthcare of Atlanta, Atlanta, GA); J. Bucuvalas,F. Ryckman, A. Hawkins, G. Arya (Children’s HospitalCincinnati, Cincinnati, OH); M. Narkewicz, R. Sokol, F.Karrer, C. Mark, K. Orban-Eller (Children’s Hospital Den-ver, University of Colorado School of Medicine, Denver,CO); E. Rand, K. Anderer (Children’s Hospital of Philadel-phia, Philadelphia, PA); G. Mazariegos, N. Chien, L. Seward(Children’s Hospital of Pittsburgh, Thomas E Starzl Trans-plantation Institute Pittsburgh, PA); P. Atkinson (Children’sHospital Western Ontario, London, ON, Canada); G. Telega,S. Lerrett (Children’s Hospital of Wisconsin, Milwaukee,WI); J. Roden, N. Mittal, L. Cutright (Children’s MedicalCenter of Dallas, Dallas, TX); E. Alonso, J. Lokar, S. Kelly,K. Neighbors (Children’s Memorial Medical Center, Trans-plant Center of Excellence, Chicago, IL); W. Andrews, J.Daniel, V. Fioravanti, A. Tendick (Children’s Mercy Hospi-tal, Kansas City, MO); D. Desai, S. Jarvis (Duke UniversityMedical Center, Durham, NC); A. Fecteau, V. Ng, M. DeAngelis, A. Benidir (Hospital for Sick Children Toronto,Toronto, ON, Canada); J. Tector, J. Lim, J. Molleston, J.Pearson (Indiana University Medical College, Indianapolis,IN); K. Schwarz, P. Colombani, M. Alford, M. Felix, R. Jurao(Johns Hopkins Hospital, Baltimore, MD); J. Eason, J. Es-hun, S. Powell (Le Bonheur Children’s Medical Center,Memphis, TN); D. Freese, J. Weckwerth, J. Greseth, L. Young(Mayo Medical School, Rochester, MN); R. Fisher, M. Akye-ampong (Medical College of Virginia, Richmond, VA); S.Emre, B. Shneider, N. Kerkar, S. Cuellar (Mount SinaiMedical Center, New York, NY); S. Lobritto, L. Smith, P.Harren, K. Maseda (New York Presbyterian Hospital, NewYork, NY); L. Book, M. O’Gorman, C. Kawai, L. Bruschke, J.
Kraus (Primary Children’s Hospital Medical Center, SaltLake City, UT); F. Alvarez, S. Martin, C. Viau (Sainte-JustineHospital, Montreal, QC, Canada); H. Soriano, K. Falkenstein(St. Christopher’s Hospital for Children, Philadelphia, PA);R. Shepherd, J. Lowell, M. Nadler (St. Louis Children’sHospital, St. Louis, MO); S. So, W. Berquest, M. Castillo, A.Bula (Stanford University Medical Center, Palo Alto, CA); S.Karpen, J. Mayo, J. Goss, D. Fishman, V. McLin, B. Carter,C. O’Mahony, T. Aloia, D. Garner (Texas Children’s Hospi-tal, Houston, TX); S. McDiarmid, S. Fiest (UCLA MedicalCenter, Los Angeles, CA); S. Gilmour, B. Dodd, N. Kneteman(University of Alberta, Edmonton, AB, Canada); J. Lavine, A.Khanna, R. Clawson (University of California San Diego,San Diego Medical Center, San Diego, CA); P. Rosenthal, D.Filipowski (University of California San Francisco, SanFrancisco, CA); J. Millis, P. Boone (University of Chicago,Chicago, IL); R. Gonzalez-Peralta, A. Hemming, M. Hodik,S. McCracken (University of Florida-Shands Children’s Hos-pital, Gainesville, FL); A. Tzakis, T. Kato, D. Weppler, L.Cooper, M. Gonzalez, A. Santiago (University of Miami,Jackson Memorial Hospital, Miami, FL); J. Lopez, J. Magee,V. Shieck (University of Michigan, Ann Arbor, MI); A.Humar, B. Durand, L. Studenski (University of Minnesota,Minneapolis, MN); A. Langnas, D. Antonson, J. Botha, W.Grant, D. Sudan, D. Andersen, B. Fleckten, K. Seipel (Uni-versity of Nebraska Med Center, Omaha, NE); J. Fair, S.Lichtman, K. Andreoni, J. Prinzhorn, V. Buchholz (Universityof North Carolina, Chapel Hill, NC); P. Abt, T. Shisler, C.Mack (University of Rochester, Strong Memorial Hospital,Rochester, NY); G. Halff, S. Wallace (University of Texas,HSC San Antonia, San Antonio, TX); S. Horslen, M. Young(University of Washington Seattle, Seattle, WA); M. Kalayoglu,A. D’Alessandro, N. Erickson, R. Judo, S. Knechtle, E. Spaith(University of Wisconsin, Madison, WI).
The Studies of Pediatric Liver Transplantation (SPLIT)research group thanks the following people at the datacoordinating center (EMMES Corporation): A. LindbladPhD, D. Brown, G. Fraser, N. Hornbeak, J. Mitchell, L.Covington, and N. Patel.
REFERENCES1. Abramson O, Rosenthal P. Current status of pediatric liver transplanta-
tion. 2000;4:533–552.2. Ghobrial RM, Farmer DG, Amersi F, et al. Advances in pediatric liver
and intestinal transplantation. Am J Surg. 2000;180:328–334.3. Bismuth H, Houssin D. Reduced-size orthotopic liver graft for liver
transplantation in children. Surgery. 1984;95:367–370.4. Pichlmayr R, Ringe B, Gubernatis G, et al. Transplantation einer
spenderbeber auf zwei empfanger (splitting-transplantation): eine neuemethode in der weiterentwicklung der lebersegment transplantation.Langenbecks Arch Chir. 1988;373:127–130.
5. Raia S, Nery JR, Mies S. Liver transplantation from live donors. Lancet.1988;2:497–503.
6. Strong RW, Lynch SV, Ong TN, et al. Successful liver transplantationfrom a living donor to her son. N Engl J Med. 1990;322:1505–1507.
7. Dunn SP, Haynes JH, Nicolette LA. Split liver transplantation benefitsthe recipient of the ‘leftover liver’. J Pediatr Surg. 1997;32:252–254.
8. Ghobrail RM, Yersiz H, Farmer DG, et al. Predictors of survival after invivo split liver transplantation: analysis of 110 consecutive patients. AnnSurg. 2000;232:312–323.
9. Reding R, de Ville de Goyet J, Delbeke I, et al. Pediatric liver trans-plantation with cadaveric or living-related donors: comparative results in90 elective recipients of primary grafts. J Pediatr. 1999;134:280–286.
Annals of Surgery • Volume 246, Number 2, August 2007 Pediatric Liver Transplantation
© 2007 Lippincott Williams & Wilkins 309

10. Sieders E, Peeters PMJG, Vergert EMT, et al. Analysis of survival andmorbidity after pediatric liver transplantation with full-size and technicalvariant grafts. Transplantation. 1999;68:540–545.
11. Burdelski MM, Rogiers X. What lessons have we learned in pediatricliver transplantation? J Hepatol. 2005;42:28–33.
12. Abt PL, Rapaport-Kelz R, Desai NM, et al. Survival among pediatricliver transplant recipients: impact of segmental grafts. Liver Transpl.2004;10:1287–1293.
13. Sindhi R, Rosendale J, Mundy D, et al. Impact of segmental grafts onpediatric liver transplantation—a review of the United Network forOrgan Sharing Scientific Registry data (1990–1996). J Pediatr Surg.1999;34:107–110.
14. Roberts JP, Hulbert-Shearon TE, Merion RM, et al. Influence of grafttype on outcomes after pediatric liver transplantation. Am J Transplant.2004;4:373–377.
15. Whitington PF. Living donor liver transplantation: ethical consider-ations. J Hepatol. 1996;24:625–627.
16. Boering DC, Kim JS, Mueller T, et al. One hundred thirty-two consec-utive pediatric liver transplants without hospital mortality: lessonslearned and outlook for the future. Ann Surg. 2004;240:1002–1012.
17. Cronin DC, Alonso EM, Piper JB, et al. Biliary complications in livingdonor liver transplantation. Transplant Proc. 1997;29:419–420.
18. Heffron TG, Pillen T, Welch D, et al. Biliary complications after pediatricliver transplantation revisited. Transplant Proc. 2003;35:1461–1462.
19. Saad S, Tanaka K, Inomata Y, et al. Portal vein reconstruction inpediatric liver transplantation from living donors. Ann Surg. 1998;227:275–281.
20. Millis JM, Seaman DS, Piper JB, et al. Portal vein thrombosis and stenosisin pediatric liver transplantation. Transplantation. 1996;62:748–754.
21. Marwan IK, Fawzy AT, Egawa H, et al. Innovative techniques for andresults of portal vein reconstruction in living-related liver transplanta-tion. Surgery. 1999;125:265–270.
22. Blumhardt G, Ringe B, Lauchart W, et al. Vascular problems in livertransplantation. Transplant Proc. 1987;19:2412.
23. Tan KC, Yandza T, de Hemptinne B, et al. Hepatic artery thrombosis inpediatric liver transplantation. J Pediatr Surg. 1988;23:927–930.
24. Millis JM, Cronin DC, Brady LM, et al. Primary living-donor livertransplantation at the University of Chicago: technical aspects of the first104 recipients. Ann surg. 2000;232:104–111.
25. Mori K, Nagata I, Yamagata S, et al. The introduction of microvascularsurgery to hepatic artery reconstruction in living-donor liver transplan-tation—its surgical advantages compared with conventional procedures.Transplantation. 1992;54:263–268.
26. Goss JA, Shackleton CR, McDiarmid SV, et al. Long-term results ofpediatric liver transplantation: an analysis of 569 transplants. Ann Surg.1998;228:411–420.
27. Taylor RW, Manganaro L, O’Brien J, et al. Impact of allogenic packedred blood cell transfusion on nosocomial infection rates in the criticallyill patient. Crit Care Med. 2002;30:2249–2254.
28. Sieders E, Peeters PMJG, Vergert EMT, et al. Graft loss after pediatricliver transplantation. Ann Surg. 2002;235:125–132.
29. Jawan B, de Villa V, Luk HN, et al. Perioperative normovolemic anemiais safe in pediatric living-donor liver transplantation. Transplantation.2004;77:1394–1398.
Diamond et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins310

ORIGINAL ARTICLES
CalprotectinA Novel Noninvasive Marker for Intestinal Allograft Monitoring
Debra Sudan, MD,* Luciano Vargas, MD,* Yimin Sun, MD,* Lisette Bok,† Gerard Dijkstra, MD,†and Alan Langnas, DO*
Objective: To identify a noninvasive screening test for intestinalallograft monitoring.Summary Background Data: Intestinal allograft rejection is diffi-cult to distinguish from other causes of diarrhea and can rapidly leadto severe exfoliation or death. Protocol biopsies are standard forallograft monitoring but may cause serious complications. No non-invasive test has shown clinical utility for monitoring of the intes-tinal allograft.Methods: Calprotectin levels (n � 68) were measured in this pilotstudy from ileostomy effluent in patients with histologic evidence ofacute rejection (n � 12), viral enteritis (n � 5), and nonspecificinflammation (n � 16) and compared with those with normalallograft histology (n � 35).Results: Median stool calprotectin levels from patients with rejec-tion were significantly higher than those from patients with viralenteritis or normal biopsies �198 mg/kg compared with 7 and 19mg/kg, respectively (P � 0.0002)�. Receiver operator characteristicssuggest the optimal cut-off level to distinguish rejection from otherdiagnoses is 92 mg/kg with specificity of 77% and sensitivity of83%. Although false-positive results occurred in 26% of patientswith normal biopsies and 30% with nonspecific changes, no treatedepisode of acute rejection was below the cutoff. In addition, in 2patients with serial levels, elevations in the calprotectin levelspreceded histologic changes by 6 to 18 days.Conclusions: Low stool calprotectin levels correlate well with a lowrisk for intestinal allograft rejection. If confirmed, biopsies may bereserved in the future for confirmation of rejection, eliminatingprotocol biopsies, and immunosuppressive changes could poten-tially be made before allograft injury.
(Ann Surg 2007;246: 311–315)
Intestinal transplantation has become standard therapy forpatients who suffer life-threatening complications from in-
testinal failure.1 One of the most common clinical presenta-tions after intestinal transplantation is diarrhea. The cause ofthe diarrhea may be rejection of the allograft, infectiousenteritis, or toxic reaction to medications or foods. A nonin-vasive test to differentiate these causes is not clinicallyavailable at this time.2 Serial endoscopic biopsy through atemporary ileostomy to obtain tissue for histology is thereforerequired. When mild rejection is treated promptly with addi-tional immunosuppression, it is usually easily controlled.Delay in the treatment by just hours to days may result inprogression from mild to severe exfoliative rejection, whichis associated with a substantial risk of graft loss (up to 93%)and mortality (50–70%).3–8 Protocol biopsies are thereforeroutinely performed weekly in the first 3 months after intes-tinal transplantation and whenever intestinal transplant recip-ients present with diarrhea. The histologic and endoscopicpatterns of intestinal allograft rejection and viral enteritisafter intestinal transplantation or in other immunocompro-mised patients have been reviewed elsewhere.9–12 Althoughhistology may or may not be definitive in patients withinfectious enteritis as the cause of diarrhea, exclusion ofrejection will prevent increasing immunosuppression in theseinstances, which could have devastating consequences.
The problems with protocol biopsy is that a temporaryileostomy is routinely performed in most patients to facilitateeasy endoscopic access, although it is not appealing to manypatients and family. In addition, endoscopy is an expensiveinvasive procedure that may require general anesthesia inchildren, and biopsy is associated with a risk for complica-tions, albeit low, such as bleeding and/or intestinal perfora-tion in 1% to 5% of intestinal transplant recipients.13,14 Inaddition, although histology remains the gold standard for thediagnosis of acute rejection, up to 30% of biopsies arenondiagnostic.11,15
Recent studies have examined the role of calprotectin inthe evaluation of gut inflammation and have found that it canaccurately distinguish active inflammatory bowel disease (animmune mediated bowel injury) from other causes of boweldysfunction.16–19 Calprotectin is a protein that has 2 subunits,each of which are part of the S100 family of proteins andcomprises approximately half of the cytosolic protein inneutrophils. Calprotectin has been isolated from activatedmacrophages, but does not appear to be present in lympho-
From the *Department of Transplant, University of Nebraska MedicalCenter, Omaha, NE; and †Department of Internal Medicine, UniversityMedical Center Groningen, Groningen, The Netherlands.
Supported by the Edna Ittner Grant from the Department of Pediatrics at theUniversity of Nebraska Medical Center.
Reprints: Debra Sudan, MD, University of Nebraska Medical Center, 983285Nebraska Medical Center, Omaha, NE 68198-3285. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0311DOI: 10.1097/SLA.0b013e3180f61af4
Annals of Surgery • Volume 246, Number 2, August 2007 311

cytes.20,21 Calprotectin can be secreted extracellularly in asoluble form, but is more commonly released as a result ofcell disruption or death.22–24 Mucosal epithelial cells havealso been shown to express calprotectin in their cytoplasmconstitutively. Therefore, increased shedding of epithelialcells could contribute to the increased levels found in stool.
Inflammatory bowel disease (IBD) monitoring is thearea with the most clinical experience in the use of stoolcalprotectin levels, reliably differentiating active IBD fromirritable bowel syndrome and correlating with disease activityin serial measurements.19,25,26 Calprotectin is a very stablecompound at room temperature and can be measured withinhours with a simple ELISA test, so that quick turn around ofresults could be used for clinical decision making, similar toallograft histology. With this background, we hypothesizedthat sampling for calprotectin levels in succus entericusobtained from the stomas of intestinal transplant recipientscould be used as a noninvasive screening test for allograftrejection.
METHODSThis study was performed at the University of Ne-
braska Medical Center with the Institutional Review Board(IRB) approval including the informed consent of intesti-nal transplant recipients or parents of recipients in accor-dance with ethical standards. Intestinal biopsy samples andstool were prospectively collected for the purpose ofidentifying noninvasive markers for the evaluation of theintestinal allografts. This is a pilot study of 68 stoolsamples collected from 20 patients, between July 2003 andJune 2004. All patients who were enrolled in the tissuebank during this time, underwent intestinal allograft bi-opsy, and had stool samples collected were included in thisstudy. Seventeen of the 20 patients were enrolled imme-diately after transplantation and 3 patients were enrolledwhen they returned for evaluation of complications 3 to 6years after transplantation. Eighteen of the patients werechildren (median age, 2; range, 1–13) and 2 were adults(ages 23 and 53 years, respectively). The median timebetween transplantation and stool collection was 2.5months (range, 0 – 65 months). All stool samples availablefrom the Intestinal Transplant Tissue Bank at the Univer-sity of Nebraska Medical Center that were collected at thetime of any abnormal histologic diagnosis were evaluatedfor this study, including 12 samples in 5 patients withacute rejection, 5 samples in 3 patients with viral enteritis,and 16 samples in 11 patients with nonspecific enteritis. Inaddition, a selection of 35 samples from 16 patients werechosen from those with normal allograft histology. Eachsample was considered independently, and calprotectinlevels were compared with the associated histology of thesimultaneous intestinal allograft biopsy. Histologic diag-nosis was made by examination of H&E staining of slidesprepared from fixed allograft biopsy specimens, using thestandard criteria developed by pathologists experienced inintestinal allograft histology.12 Fluid samples were ob-tained from the ileostomy within 24 hours of a therapeutic
or protocol biopsy and frozen at �80°C in 1.5-mL aliquotsuntil batch sample analysis.
Blinded specimens were used for duplicate measure-ment of calprotectin levels. Calprotectin was detected andquantified using CALPREST ELISA kit (NovaTec Immun-diagnostica, Germany) according to manufacturer’s instruc-tions. The optical density (OD) of the samples is measured at405 nm with a microtiter plate reader and then plotted as thelog value.
Data are presented as the median (range) unless other-wise stated. Comparisons of the median calprotectin levels ofeach of the 4 groups were made using the Kruskal–Wallis testand the Dunn’s multiple comparison post test. P � 0.05 wasconsidered significant. Receiver–operator curves were gen-erated to analyze the optimal cutoff levels. Graph Pad Prismsoftware was used to perform the statistical analysis.
RESULTSFigure 1 summarizes the distribution of the calprotectin
values in each of the 4 diagnostic groups. The median value(and 25th/75th quartile values) for calprotectin for each of the4 groups (acute rejection, viral enteritis, nonspecific enteritis,and normal) were 198 (103/251), 7 (6.25/35), 57 (17/106),and 19 (6.25/85) mg/L, respectively. Overall median valuesof these groups are significantly different (P � 0.0002), andpost-test evaluation reveals the differences to be between therejection and normal groups (P � 0.001) and the rejectionand viral enteritis groups (P � 0.01). Receiver–operatorcharacteristics suggest an optimal cutoff of 92 mg/L with77% specificity and 83% sensitivity in distinguishing rejec-tion from specimens without rejection (Fig. 2). The negativepredictive value of calprotectin for clinically relevant acuterejection was excellent. Only 1 patient in this pilot study witha calprotectin level below the optimal cutoff had histologicchanges consistent with rejection, and this patient was nottreated with any additional immunosuppression due to theabsence of symptoms and repeat biopsy 24 hours later re-vealing no evidence of rejection.
The positive predictive value for calprotectin appearsreasonable for a screening test. Seventy-six percent of pa-
FIGURE 1. Summary of median calprotectin levels (mg/L) in4 groups of patients based on allograft histology; acute re-jection (n � 12; 198 mg/L), normal (n � 35: 19 mg/L), viralenteritis (n � 5; 7 mg/L), and nonspecific enteritis (n � 16;57 mg/L).
Sudan et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins312

tients with normal biopsies, 100% with viral enteritis, and70% with nonspecific enteritis had calprotectin levels belowthe cutoff (Fig. 1). Patients with nonspecific enteritis onhistology were the most likely to have increased calprotectinlevels (median level � 57 mg/dL).
Of the 13 samples with high calprotectin levels withouthistologic signs of rejection (ie, normal or nonspecific enter-itis), 30% either preceded or followed histologic resolution ofan episode of acute rejection; 3 samples were obtained from2 different patients 1 week to 18 days before the histologicdiagnosis of acute rejection (Fig. 3) and one was from one ofthe same patients 1 week after treatment for acute rejection.Nine additional samples from 7 patients had high calprotectinlevels (�92 mg/dL), and the clinical situation of these pa-tients included severe pericarditis without diarrhea in 1 pa-tient, severe skin rash and diarrhea attributed to a drugreaction in 1 patient, 2 samples from 1 patient who wasclinically well, diarrhea of unclear etiology (in 2 patients;resolved without change in immunosuppression in 1 andresolved with elevation of baseline tacrolimus levels in 1), 1
patient in the first 10 days after transplant, and 1 sampleobtained several days after ostomy revision in 1 patient.
DISCUSSIONIn renal or liver allograft recipients, routine protocol
biopsies are not performed in most centers. Instead, screeningtests such as creatinine for recipients of renal allografts andliver function tests for recipients of liver allografts are usedfor clinical monitoring. A recent review of intestinal allograftmonitoring demonstrated that no such test is clinically avail-able for screening after intestinal transplantation.2 Althoughelevations in screening tests for renal and liver allograftsoften prompt a biopsy to confirm rejection before treatment,other causes for the elevations such as dehydration, biliaryleak, or drug toxicity may be the etiology of the abnormalvalues. Among the tests that have been previously investi-gated for allograft monitoring, citrulline has been the mostextensively studied. Although low citrulline levels reflectpoor intestinal function, they are routinely low after trans-plantation for the first month or two, which is the time ofhighest risk for the development of rejection.27,28 The mostconcerning aspect of citrulline as a potential screening test isthat once levels normalizes after transplantation, they do notbecome decreased/abnormal until substantial injury to thegraft has occurred.28 This suggests citrulline levels maycorrelate well with severe rejection episodes, but may not beuseful in identifying mild to moderate rejection episodeswhen they are still reversible. In addition, citrulline levelsvary with body surface area such that levels in children areroutinely below the normal established for adults even inthe presence of normal intestinal function.27 In light of thedemographics of intestinal transplantation with more than50% performed in children and the limitations noted,citrulline has not to date shown clinical utility.
The possible role of calprotectin in solid organ rejectionhas been suggested previously. In kidney and lung allografts,macrophages with increased membrane expression of thecalprotectin proteins appear in the allograft during acute
FIGURE 2. Receiver operating curve showing the optimalcutoff for calprotectin levels (92 mg/L) in predicting thepresence or absence of intestinal allograft rejection with77% specificity and 83% sensitivity.
FIGURE 3. Sequential calprotectin measurements in 3 patients with moderate or severe rejection on intestinal allograft histol-ogy (arrows indicate the time when the histologic diagnosis was made). Two of these patients showed elevations of calprotec-tin levels in 3 ostomy effluent samples obtained prior to identifiable changes in histology (signified by the *), ie, 150 mg/L (*)in patient 2 when allograft histology showed nonspecific enteritis and 1 week before the peak of 425 (2) measured at thetime moderate rejection was diagnosed; and 50 mg/L (*) in patient 3, who previously had undetectable levels, but increasedto 225 mg/L (2) at the time the histology revealed acute rejection.
Annals of Surgery • Volume 246, Number 2, August 2007 Calprotectin
© 2007 Lippincott Williams & Wilkins 313

rejection episodes.29–31 The specificity of the increased mem-brane expression of calprotectin for allograft rejection is notclear, since experiments using cultured alveolar macrophagealso show increased membrane expression after stimulationwith bacterial lipopolysaccharide.31 In the only publishedreport examining an intestinal transplant recipient, elevationsin serum calprotectin levels occurred simultaneous with orimmediately before 3 clinical episodes of rejection and didnot correspond to elevations of the patients white blood cellcount.32 The role of calprotectin levels in stool has not beenpreviously examined in any solid organ transplant recipient.
In this pilot study, we examined, in a blinded manner,representative ileostomy samples from 20 small bowel trans-plant recipients. The findings of this report suggest that lowcalprotectin levels (�92 mg/L) uniformly defined patientswithout acute rejection. In the only patient in this pilot studywith histologic evidence of acute rejection and a low calpro-tectin level, repeat biopsy was performed within 24 hours dueto the absence of diarrhea, and the histology of the repeatbiopsy was normal. This patient was correctly identified bythe calprotectin level. Although he was spared additionalimmunosuppression, he required repeat endoscopy and bi-opsy with the associated risks due to the initial histologysuggesting rejection.
Calprotectin levels in this study appear to be useful formonitoring intestinal allografts, similar in efficacy to creati-nine and liver function studies for monitoring of renal or liverallografts and similar to the gold standard, allograft histology(ie, 30% nondiagnostic). Here we found 24% of patients withnormal histology and 31% with nonspecific enteritis hadelevations above the threshold for calprotectin, whereas nopatient treated for rejection had a low level. A therapeuticbiopsy to confirm or exclude rejection reserved for the one-fourth of recipients with diarrhea and elevated stool calpro-tectin would be a tremendous decrease in biopsies comparedwith current practice and would lead to significant savings incosts, manpower, and potential risk.
Several areas require further investigation. As noted,the early postoperative period requires further examinationsince elevation of calprotectin levels in the absence of acuterejection was identified in 1 patient, likely the result ofpreservation injury and within days of ostomy revision in asecond patient. Of note, the immediate posttransplant eleva-tion above the cutoff level for calprotectin was brief and rapidnormalization in this patient within 2 weeks of intestinaltransplantation was observed in contrast to the studies ofplasma citrulline where normalization took on average 45days. Although the current data set for serial observations islimited and the results must be confirmed, this pilot study alsosuggests that calprotectin levels may be more sensitive thanhistology as a marker for immunologic activation in the earlyor prerejection time points. Serial monitoring with concurrentbiopsy is needed to determine how uniformly the increase incalprotectin levels occur before the histologic changes as seenin 2 patients in this study and depicted in Figure 3. Ifconfirmed, these findings suggest that monitoring of calpro-tectin levels may provide an opportunity to adjust immuno-suppression before allograft injury. Finally, this pilot study
did not find any elevations in calprotectin levels in patientswith defined viral infections, although the number of patientswas limited. Since this is the group of patients that are mostlikely to be harmed by an increase in immunosuppression, itis particularly useful that calprotectin levels were uniformlylow in this group. Further studies will need to include patientswith rotavirus, Norwalk virus, and Clostridium difficile colitisas these causes of infectious diarrhea were not represented inthis study.
There are some limitations to the interpretation of theresults of this study. First, this was a retrospective analysisof selected patient samples with known diagnosis, al-though the individuals performing the assays were blindedas to the source of the samples. A prospective study toexamine the risk of using calprotectin for screening as analternative to routine protocol biopsy is currently underway.This prospective study will include serial measurements in allenrolled patients and assess all episodes of viral enteritis toanswer many of the questions raised above.
In conclusion, calprotectin is a promising clinicalscreening test for intestinal allograft rejection. Low levels ofcalprotectin correlate extremely well with a low risk forallograft rejection and likely will allow for elimination ofprotocol biopsies in a large proportion of patients who areotherwise clinically well. If the clinical utility of this markeris confirmed in currently ongoing prospective validation stud-ies, future studies will be aimed at adjusting immunosuppres-sion at the time of increased immune activation and prior toallograft injury.
ACKNOWLEDGMENTSThe authors thank Bev Fleckten, BS, CCRC, Kris
Seipel, BS, CCRC, Sharon Kochanowicz, RN, APRN, andVicki Cox, RN, BSN, CCTN for their many and variedcontributions and their patience throughout the study and toTina Rackley for administrative support.
REFERENCES1. Kaufman SS, Atkinson JB, Bianchi A, et al. Indications for pediatric
intestinal transplantation: a position paper of the American Society ofTransplantation. Pediatr Transplant. 2001;5:80–87.
2. Sudan D. Small bowel transplantation: current status and new develop-ments in allograft monitoring. Curr Opin Organ Transplant. 2005;10:124–127.
3. Sudan DL, Chinnakotla S, Horslen S, et al. Basiliximab decreases theincidence of acute rejection after intestinal transplantation. TransplantProc. 2002;34:940–941.
4. Fishbein TM, Kaufman SS, Florman SS, et al. Isolated intestinal trans-plantation: proof of clinical efficacy. Transplantation. 2003;76:636–640.
5. Gaynor JJ, Kato T, Selvaggi G, et al. The importance of analyzing graftand patient survival by cause of failure: an example using pediatric smallintestine transplant data. Transplantation. 2006;81:1133–1140.
6. Ishii T, Mazariegos GV, Bueno J, Ohwada S, Reyes J. Exfoliativerejection after intestinal transplantation in children. Pediatr Transplant.2003;7:185–191.
7. Sudan DL, Kaufman S, Horslen S, Fox I, Shaw BW Jr, Langnas A.Incidence, timing, and histologic grade of acute rejection in small boweltransplant recipients. Transplant Proc. 2000;32:1199.
8. Grant D, Abu-Elmagd K, Reyes J, et al. 2003 report of the intestinetransplant registry: a new era has dawned. Ann Surg. 2005;241:607–613.
Sudan et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins314

9. Manez R, Kusne S, Green M, et al. Incidence and risk factors associatedwith the development of cytomegalovirus disease after intestinal trans-plantation. Transplantation. 1995;59:1010–1014.
10. Kakugawa Y, Kami M, Kozu T, et al. Endoscopic evaluation forcytomegalovirus enterocolitis after allogeneic haematopoietic stem celltransplantation. Gut. 2006;55:895–896.
11. Sudan DL, Kaufman SS, Shaw BW Jr, et al. Isolated intestinal trans-plantation for intestinal failure. Am J Gastroenterol. 2000;95:1506–1515.
12. Ruiz P, Bagni A, Brown R, et al. Histological criteria for the identifi-cation of acute cellular rejection in human small bowel allografts: resultsof the pathology workshop at the VIII International Small BowelTransplant Symposium. Transplant Proc. 2004;36:335–337.
13. Pignone M, Rich M, Teutsch SM, Berg AO, Lohr KN. Screening forcolorectal cancer in adults at average risk: a summary of the evidence forthe U. S. Preventive Services Task Force. Ann Intern Med. 2002;137:132–141.
14. Sigurdsson L, Reyes J, Putnam PE, et al. Endoscopies in pediatric smallintestinal transplant recipients: five years experience. Am J Gastroen-terol. 1998;93:207–211.
15. Wu T, Abu-Elmagd K, Bond G, Nalesnik MA, Randhawa P, DemetrisAJ. A schema for histologic grading of small intestine allograft acuterejection. Transplantation. 2003;75:1241–1248.
16. Roseth AG, Schmidt PN, Fagerhol MK. Correlation between faecalexcretion of indium-111-labelled granulocytes and calprotectin, a gran-ulocyte marker protein, in patients with inflammatory bowel disease.Scand J Gastroenterol. 1999;34:50–54.
17. Tibble JA, Sigthorsson G, Bridger S, Fagerhol MK, Bjarnason I. Surrogatemarkers of intestinal inflammation are predictive of relapse in patients withinflammatory bowel disease. Gastroenterology. 2000;119:15–22.
18. Poullis A, Foster R, Northfield TC, Mendall MA. Review article: faecalmarkers in the assessment of activity in inflammatory bowel disease.Aliment Pharmacol Ther. 2002;16:675–681.
19. Fagerhol MK. Calprotectin, a faecal marker of organic gastrointestinalabnormality. Lancet. 2000;356:1783–1784.
20. Striz I, Trebichavsky I. Calprotectin—a pleiotropic molecule in acuteand chronic inflammation. Physiol Res. 2004;53:245–253.
21. Yui S, Nakatani Y, Mikami M. Calprotectin (S100A8/S100A9), an
inflammatory protein complex from neutrophils with a broad apoptosis-inducing activity. Biol Pharm Bull. 2003;26:753–760.
22. Rammes A, Roth J, Goebeler M, Klempt M, Hartmann M, Sorg C.Myeloid-related protein (MRP) 8 and MRP14, calcium-binding proteinsof the S100 family, are secreted by activated monocytes via a novel,tubulin-dependent pathway. J Biol Chem. 1997;272:9496–9502.
23. Boussac M, Garin J. Calcium-dependent secretion in human neutrophils:a proteomic approach. Electrophoresis. 2000;21:665–672.
24. Voganatsi A, Panyutich A, Miyasaki KT, Murthy RK. Mechanism ofextracellular release of human neutrophil calprotectin complex. J LeukocBiol. 2001;70:130–134.
25. Wassell J, Dolwani S, Metzner M, Losty H, Hawthorne A. Faecalcalprotectin: a new marker for Crohn’s disease? Ann Clin Biochem.2004;41:230–232.
26. Li B, Hartono C, Ding R, et al. Noninvasive diagnosis of renal-allograftrejection by measurement of messenger RNA for perforin and granzymeB in urine. N Engl J Med. 2001;344:947–954.
27. Gondolesi GE, Kaufman SS, Sansaricq C, et al. Defining normal plasmacitrulline in intestinal transplant recipients. Am J Transplant. 2004;4:414–418.
28. Pappas PA, GT A, Gaynor JJ, et al. An analysis of the associationbetween serum citrulline and acute rejection among 26 recipients ofintestinal transplant. Am J Transplant. 2004;4:1124–1132.
29. Burkhardt K, Bosnecker A, Hillebrand G, et al. MRP8/14-positivemacrophages as early acute cellular rejection markers, and solubleMRP8/14 and increased expression of adhesion molecules followingrenal transplantation. Transplant Proc. 1995;27:890–891.
30. Goebeler M, Roth J, Burwinkel F, Vollmer E, Bocker W, Sorg C.Expression and complex formation of S100-like proteins MRP8 andMRP14 by macrophages during renal allograft rejection. Transplanta-tion. 1994;58:355–361.
31. Frachon I, Fattal-German M, Magnan A, et al. Emergence of inflam-matory alveolar macrophages during rejection or infection after lungtransplantation. Transplantation. 1994;57:1621–1628.
32. Ikemoto M, Tanaka T, Takai Y, Murayama H, Tanaka K, Fujita M. NewELISA system for myeloid-related protein complex (MRP8/14) and itsclinical significance as a sensitive marker for inflammatory responsesassociated with transplant rejection. Clin Chem. 2003;49:594–600.
Annals of Surgery • Volume 246, Number 2, August 2007 Calprotectin
© 2007 Lippincott Williams & Wilkins 315

ORIGINAL ARTICLES
Mediastinal Carcinosis Involving the Esophagus in BreastCancer: The “Breast-Esophagus” Syndrome
Report on 25 Cases and Guidelines for Diagnosis and Treatment
Sabrina Rampado, MD,† Alberto Ruol, MD, FACS,* Maria Guido, MD,‡Giovanni Zaninotto, MD, FACS,† Giorgio Battaglia, MD,* Mario Costantini, MD,†
Giuseppe Portale, MD,* Alessandra Amico, MD,† and Ermanno Ancona, MD, FACS*
Introduction: Breast metastases of mucosal/submucosal layers ofthe esophagus are extremely rare: esophageal involvement is usuallypart of a mediastinal carcinosis.Aim: We report the largest series to date of 25 cases of metastaticesophageal involvement from breast cancer, discussing both diag-nostic techniques and treatment options.Materials and Methods: Twenty-five female patients with a historyof breast cancer referred for secondary esophageal involvement(1980–2006) were studied.Results: All patients presented with worsening dysphagia. Twenty-four had undergone surgery for breast cancer a median of 10 yearsearlier: 1 had received chemoradiotherapy, and 17 had adjuvantradiotherapy/telecobalt therapy following breast surgery. Endo-scopic biopsy/cytology were negative for cancer in 17 of 19 patients;in 9 patients, the diagnosis was made with thoracoscopy/laparos-copy. Immunohistochemical staining was done in 10 patients (ERand/or PrR positive). Fifteen patients presented with distant meta-static involvement. Therapy was directed toward dysphagia relief,mostly with endoscopic dilations/prostheses. Complications (4 per-forations) occurred only in those 15 patients who had endoscopicdilations/prostheses. Fifteen patients had cytoreductive therapy.Nine of 25 patients are still alive. The median overall survival was7 months; 1-, 3-, and 5-year survival rates were 44%, 16%, and 8%,respectively.Conclusions: A “breast-esophagus” syndrome can be defined: it isoften diagnosed only after excluding other diseases or after relief ofdysphagia with adequate therapy. The presence of distant metastaseshelps the diagnosis of esophageal involvement from mediastinal carci-nosis, while diagnosis is a problem in case of mediastinal/pleuraldisease only: in this case, exploratory thoracoscopy is mandatory for afinal diagnosis. Given the high related risk of perforation from endo-
scopic procedures (dilations/prostheses), the treatments of choice arecurrently hormone therapy or chemotherapy/radiotherapy.
(Ann Surg 2007;246: 316–322)
Metastases from breast cancer often involve locoregionaland distant lymph nodes, lung, bone, liver, and brain.1
Metastatic involvement of the gastrointestinal tract is un-usual, but the frequency of esophageal and mediastinal me-tastases from breast cancer is probably underestimated. Ac-cording to Asch et al (autoptic study),2 their incidence rangesbetween 5% and 6% among women dying of advanced breastcancer, which would suggest a clinically silent esophagealinvolvement in a considerable number of patients.
Metastases to the inner (mucosal and submucosal) lay-ers of the esophageal wall are extremely rare3; indeed, esoph-ageal involvement is usually due to mediastinal carcinoma-tosis. Many such lesions develop several years after theprimary breast cancer has been treated and can be mistakenfor a second primary. Esophageal or mediastinal metastasesfrom breast cancer are usually asymptomatic,2,4 but a clinicalsyndrome may develop, with progressively worsening dys-phagia, after a long disease-free interval (up to 22 years4)since mastectomy. The corresponding peculiar radiologic andendoscopic picture is a concentric stricture of the esophaguscovered by normal mucosa due to the involvement of theesophageal wall from the outside inwards, usually in themiddle and lower thirds of the esophagus.
We report here on 25 cases of dysphagia due to esoph-ageal stricture in patients with metastatic breast cancer of theesophagus, discussing the difficulties encountered in identi-fying and staging these malignancies in the mediastinum andthe corresponding treatment options.
MATERIALS AND METHODSIn a series of 4198 cases of malignant esophageal
disease observed between 1980 and April 2006, 114 (2.7%)were metastases from nonesophageal primaries (thyroid,
From the *Istituto Oncologico Veneto (IOV-IRCCS), the †Department ofMedical and Surgical Sciences, Clinica Chirurgica III, and the ‡Depart-ment of Diagnostic Sciences and Special Therapies, Pathology Section,University of Padova School of Medicine, Padova, Italy.
Reprints: Alberto Ruol, MD, FACS, Department of Medical and SurgicalSciences, Clinica Chirurgica III, University of Padova School of Medicine,Via Giustiniani 2, 35128 Padova, Italy. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0316DOI: 10.1097/01.sla.0000263507.11053.26
Annals of Surgery • Volume 246, Number 2, August 2007316

lung, bronchi, lymphoma, colon, uterus, breast, and oralcavity).
The breast was the site of the primary tumor in 25patients (0.6%), with a median age of 58 years (interquartilerange �IQR�, 56–67 years). All but one had undergonesurgery for breast cancer a median of 10 years (IQR, 8–17years) before presenting with esophageal involvement. Sev-enteen of the 25 patients (68%) had been given postoperativeadjuvant radiotherapy or telecobalt therapy.
All patients were referred for worsening dysphagialasting a median 8 months (IQR, 5–12 months); 14 (56%)reported a weight loss greater than 10%; 3 (12.5%) haddysphonia.
Details on their previous treatments for breast cancerand clinicopathologic characteristics of their esophageal sec-ondaries are given in Table 1.
All cases were studied by means of barium swallow andupper endoscopy. Most patients also had computed tomogra-phy (CT) of the chest and abdomen. From 1995 onwards,endoscopic ultrasound was used selectively to better definethe extent of esophageal involvement. More recently, mini-mally invasive exploratory thoracoscopy has been used,where necessary, to facilitate the diagnosis.
The final diagnosis was based on the histologic assess-ment of biopsy samples, wherever possible. More recently,immunohistological staining has become available to detectestrogen receptor (ER), progesterone receptor (PgR), c-erb,and cytokeratin expressions.
Statistical AnalysisData are expressed as medians and IQRs. Proportions
were compared using the �2 or Fisher exact test. Continuousvariables were compared using the Mann-Whitney U test.Survival estimates were calculated by the Kaplan-Meiermethod and survival comparisons were performed using thelog-rank test. A P value below 0.05 was considered signifi-cant.
RESULTSBased on barium swallow studies (Fig. 1), the mid- (13
of 25, 52%) or lower third (7 of 25, 28%) of the esophaguswas usually affected (Table 2). The median length of theesophageal stricture was 5 cm (IQR, 3–6 cm). All but 1patient had endoscopy, which revealed the extrinsic esopha-geal wall involvement with an apparently normal mucosallayer. Endoscopic biopsy sampling or brush cytology was
TABLE 1. Details of Prior Breast Cancer Treatment
Patient No. Age (yr)Disease-FreeInterval (yr)
Type of Surgeryfor Breast
Cancer Adjuvant Therapy
1980–1990
1 52 9 Mastectomy No
2 56 9 Mastectomy No
3 46 8 Mastectomy Telecobalt therapy � chemotherapy
4 75 22 Mastectomy No
5 56 20 Mastectomy Telecobalt therapy
6 71 8 Mastectomy Radiotherapy
7 69 4 Mastectomy Telecobalt therapy
8 53 9 Mastectomy Radiotherapy � chemotherapy
9 67 10 Mastectomy Chemotherapy
10 58 16 Mastectomy Telecobalt therapy
11 45 4 Mastectomy No
1991–2006
12 65 17 Mastectomy Radiotherapy � chemotherapy
13 63 2 Quadrantectomy Radiotherapy � chemotherapy � hormone therapy
14 70 14 Mastectomy No
15 51 21 Mastectomy Chemotherapy � hormone therapy
16 58 9 Quadrantectomy Radiotherapy
17 56 1,5 None Radiotherapy � chemotherapy
18 87 11 Mastectomy Radiotherapy � hormone therapy
19 56 20 Mastectomy Hormonal therapy � radiotherapy
20 75 9 Quadrantectomy Radiotherapy � chemotherapy
21 53 14 Mastectomy Radiotherapy
22 58 10 Quadrantectomy Radiotherapy
23 64 17 Mastectomy Hormone therapy
24 56 17 Mastectomy Radiotherapy � chemotherapy � hormone therapy
25 62 3 Mastectomy Radiotherapy � chemotherapy � hormone therapy
Total 58 10 — —
Annals of Surgery • Volume 246, Number 2, August 2007 Breast-Esophagus Syndrome
© 2007 Lippincott Williams & Wilkins 317

done in all but 6 patients, which were negative for cancer in17 of 19 (89%). Endoscopic ultrasound was performed in 6patients, revealing thickening of the esophageal wall in 4 andperiesophageal lymphadenopathy in 2 (1 patient had both)(Fig. 2). CT scans of the chest and abdomen were performedin 14 patients and disclosed a circumferential thickening ofthe esophageal wall and/or mediastinal lymph node enlarge-ment (Fig. 3). One patient had a positron emission tomogra-phy scan, which showed an increased SUV (standardizeduptake value) in the paramediastinal region. Breast cancermarkers (MCA, Ca 15.3, Ca 125) were evaluated in 10 of 25cases (40%) and at least one was above normal limits in 5 of10 cases (50%). Nine cases were diagnosed after minimallyinvasive exploratory thoracoscopy (n � 5) or laparoscopy(n � 4). Immunohistochemical staining (Fig. 4) was done in10 patients and was positive for ER and/or PgR.
Fifteen patients (60%) also presented with other, non-mediastinal metastases involving: liver (3), lung and supra-clavicular and axillary lymph nodes (1), skin (4), bone (4),liver and bone (1), bone and supraclavicular lymph nodes (1),skin and bone (1). The tracheobronchial tree was also af-fected in 2 patients.
Treatment focused mainly on palliation of dysphagia(Table 3). During the initial period, up until 1990, thisconsisted (in 11 patients) of endoscopic dilation (4 cases),endoscopic positioning of a prosthesis (4 cases) feeding
FIGURE 1. Barium swallow showing concentric stricture inthe middle and distal thirds of the esophagus.
TABLE 2. Level of Esophageal Stricture
Level of Stricture % (No.)
Upper esophagus 20 (5/25)
Mid esophagus 52 (13/25)
Lower esophagus 28 (7/25)
FIGURE 2. CT scan of the chest: esophageal wall thickeningbelow the tracheal bifurcation.
FIGURE 3. Endoscopic ultrasound showing enlarged medias-tinal lymph nodes.
Rampado et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins318

gastrostomy (2 cases); 3 patients were given cytoreductivetherapy, which was the only treatment in 1 case. All thecomplications seen were endoscopic perforations (after dila-
tion in 2, after positioning a prosthesis in 1), which weretreated as follows: bipolar exclusion and cervical retrosternalesophagogastroplasty in the first patient, who died of respi-ratory insufficiency during the postoperative period; cervicaldrainage, gastrostomy and a prosthesis to exclude the fistulain the second; and conservative treatment in the third.
In the latter period, since 1990 (14 patients), treatmenthas consisted of: endoscopic dilation (3), endoscopic pros-thesis (3), gastrostomy (1), and Heller’s myotomy (1 patientwith instrumental and functional test suggestive of achalasia);11 patients were given cytoreductive therapy, which was theonly treatment in 6 cases. Complications included one endo-scopic perforation after positioning a prosthesis with a tra-cheoesophageal fistula, which was treated with a bipolarexclusion and subcutaneous gastroesophageal bypass.
Nine of the 11 patients treated before 1990 had distantmetastases (81.8%), as opposed to 6 of 14 (42.9%) treatedafter 1990 (P � not significant). Three patients (27.3%)presenting before 1990 were given cytoreductive therapy,versus 11 of 14 patients (78.6%) after 1990 (P � notsignificant).
Patients treated before 1990 survived a median 3months, while for those treated afterward the median survivalwas 17.5 months (P � not significant). Nine patients are stillalive, and 16 have died. The median survival for the wholeseries was 7 months (IQR, 1–26 months); the 1-, 3-, and5-year actuarial survival rates were 46%, 16%, and 8%,respectively.
Patients who were given cytoreductive therapy (chemo-radiotherapy and/or hormone therapy) survived a median 16months, as opposed to 4.5 months for those who were not(P � not significant).
Patients with mediastinal/pleural metastases alone sur-vived a median 19 months, while those with other remotemetastases survived 3 months (P � not significant).
DISCUSSIONMetastatic esophageal disease from previously treated
breast cancer has been estimated to account for 0.4% of allcases of symptomatic esophageal obstruction.5 The majorityof symptomatic cases of involvement of the outer layers ofthe esophageal wall (secondary to breast cancer) are due tomediastinal carcinosis, while metastases to the inner layers ofthe esophagus are extremely rare.6
Patients with metastatic breast carcinoma present clin-ically with dysphagia even several years after being treatedfor breast cancer: in our series, this interval was 10 years(median). Associated symptoms include weight loss, an-orexia, or dysphonia. In some cases, the clinical presentationmay mimic achalasia7 or nonspecific esophageal motilitydisorder.8 Metastatic lesions are most often found in themiddle or distal thirds of the esophagus, as confirmed in thisseries. Most patients are postmenopausal.3
The mechanism behind esophageal spread from breastcancer is controversial. We found an infiltration of the me-diastinal pleura with esophageal tissue involvement. Thespread of the disease is most likely lymphatic, through theintercostal vessels, to reach the internal mammary chain and
FIGURE 4. Immunohistochemistry: positive staining for ER(a), PgR (b), and c-erb (c).
Annals of Surgery • Volume 246, Number 2, August 2007 Breast-Esophagus Syndrome
© 2007 Lippincott Williams & Wilkins 319

the mediastinal lymph nodes, thus the intramural lymphaticsof the esophagus, with subsequent stenosis of the esophagus.The involvement of the intertracheobronchial lymph nodesand the lymphatic connections in the mediastinum wouldexplain why the middle third of the esophagus is the mostfrequent site of stenosis in these patients.10 That is why mostauthors use the expression “mediastinal localization” ratherthan “esophageal metastasis” to describe this condition.There are only a few reports of “true” esophageal metastasesfrom breast cancer.6 Breast cancer may also infiltrate intra-murally within the esophagus and disrupt its motility by
obliterating nerve plexuses as well as the normal esophagealarchitecture.3
It is a challenge to diagnose an esophageal stricture dueto esophageal involvement from breast cancer, and it isparticularly difficult to differentiate between primary esoph-ageal tumor, postactinic stenosis, peptic stricture, and medi-astinal carcinomatosis. In our experience, when patients werediagnosed as having an esophageal primary, they had alreadybeen suffering from dysphagia for about 3 months, whereaspatients with secondary esophageal cancer had been experi-encing this symptom for approximately 8 months (P �
TABLE 3. Clinicopathologic Characteristics, Treatment, and Survival
Patient No.Level ofStricture
Duration ofDysphagia
(mo)Other Sites of
Metastases
EndoscopicBiopsy/Brush
Cytology EUS TherapyStatus(mo)
1980–1990
1 Mid 12 Bone Positive No Prosthesis* Dead, 2
2 Mid-lower 6 Liver Negative No Laparoscopy, dilation, prosthesis,chemotherapy
Dead, 3
3 Upper-mid 5 No Negative No Dilation Dead, 19
4 Mid 6 Liver Negative No Dilation Dead, 1
5 Lower 3 Skin Negative No Chemotherapy Dead, 39
6 Upper 5 Bone Negative No Dilation† Dead, 12
7 Lower-cardia 2 Liver Negative No Laparoscopy, dilation‡ Dead, 1
8 Upper 14 Pulmonary,lymphnodes
NA No Gastrostomy Dead, 7
9 Mid 3 Liver, bone Negative No Dilation, prosthesis Dead, 2
10 Mid 7 No Negative No Dilation, prosthesis Dead, 19
11 Upper 2 Bone Negative No Gastrostomy, chemotherapy Dead, 1
1991–2006
12 Mid 14 No Negative No Dilation, hormone therapy Alive, 67
13 Mid 5 Bone, lymphnodes
NA Yes Hormone therapy, chemotherapy Dead, 16
14 Mid 8 No Negative Yes Thoracoscopy, radiotherapy,hormone therapy
Dead, 26
15 Mid 9 No Negative No Radiotherapy, hormone therapy Alive, 75
16 Lower 12 bone Negative Yes Thoracoscopy, dilation, prosthesis Dead, 34
17 Mid 1 Skin, bone Negative No Dilation Dead, 1.5
18 Upper 2 Skin Positive No Dilation, hormone therapy Dead, 3
19 Upper-mid 15 Skin Negative No Dilation, prosthesis,§ hormonetherapy
Alive, 40
20 Mid 11 No Negative Yes Thoracoscopy, hormone therapy Alive, 19
21 Cardia 24 No NA No Laparoscopy, gastrostomy,hormone therapy
Alive, 28
22 Mid-lower 10 No NA Yes Thoracoscopy, hormone therapy,chemotherapy
Alive, 1
23 Mid 8 No Negative No Thoracoscopy, hormone therapy,chemotherapy
Alive, 1
24 Upper 10 Skin NA No Prosthesis, chemotherapy Alive, 1
25 Cardia 24 No NA Yes Myotomy, hormone therapy Alive, 1
Total — 7.5 — — — — —
*Esophageal perforation managed conservatively.†Esophageal perforation treated with gastrostomy, cervical drainage, and stent placement to seal the perforation.‡Esophageal perforation treated with esophagectomy and retrosternal gastric pull-up.§Tracheoesophageal fistula managed with subcutaneous esophagogastric bypass.�Died of respiratory failure during the perioperative period.NA indicates not assessed; EUS, endoscopic ultrasound.
Rampado et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins320

0.001). At the time of admission, only 20% of cases (2 of 10)had a diagnosis of neoplastic mediastinitis, in 50% (5 of 10),it was esophageal stenosis not otherwise specified; in 20% (2of 10), it was esophageal carcinoma; and in 10% (1 of 10), itwas achalasia.
The presence of distant metastases makes it easier todiagnose esophageal involvement due to mediastinal carci-nosis, whereas patients presenting with a mediastinal and/orpleural diffusion alone pose considerable diagnostic difficul-ties. The distinction lies in establishing whether it is a case ofprimary esophageal cancer, a postactinic stenosis, or a me-tastasis to the mediastinum. In this subgroup of patients,minimally invasive exploratory thoracoscopy is mandatory toreach a definitive diagnosis, although in experienced hands,EUS-FNAB could be a valid alternative. In our experience of709 female patients with the cancer of the esophagus, 31(4.4%) had a positive history of breast cancer. Of these, 13(42%) had received radiotherapy. Thus, this value wouldsupport in part the hypothesis that women who have radio-therapy to the breast are at greater risk of developing esoph-ageal cancer.11
The diagnosis of esophageal involvement depends on aclinical history of breast cancer. Several imaging methodscan be helpful, ie, barium swallow, endoscopy, endosonog-raphy, CT scan. On the other hand, although the definitivediagnosis should be founded on a histologic assessment,endoscopic biopsies are usually negative for cancer.
EUS-guided FNAB is reported useful as a diagnosticalternative to exploratory surgery,12 enabling cytologic andhistopathologic specimens to be obtained from lymph nodesand mediastinal masses suspected of malignancy. In ourexperience, a histopathologic diagnosis demanded thoracos-copy and biopsy of the mediastinal periesophageal tissueand/or pleura in 5 cases and laparoscopy in 4. In a fewpatients, when biopsy samples were negative for cancer, anex adjuvantibus diagnosis was reached on the basis of dys-phagia relief after hormone therapy and/or chemotherapyand/or radiotherapy.
The histopathologic diagnosis is important to assess thepattern and degree of atypia and for evaluating ER and PRexpression.
By the time symptoms appear, the majority of patientsalready have distant metastases and the treatment is usuallyaimed to palliation of dysphagia. Endoscopic treatment seemsthe most logical but is not usually indicated because of thehigh risk of perforation. In our series, the perforation rateafter endoscopic treatment with dilations or prostheses was ashigh as 26.7% versus 4.4% (28 of 638) among patients withprimary esophageal cancer treated during the same period atour department (P � 0.004). More recently, expandablemetal stents have been found a safe and effective treatment ofesophageal obstruction caused by inoperable cancer.13 Ametastatic lesion in the esophagus with a short stenosis maybe a valid indication for stent placement, but extreme cautionis mandatory because the tissue is relatively inelastic andthere is a risk of severe complications. The safety of thisapproach needs to be confirmed in patients with esophagealstricture secondary to breast cancer. In our opinion, stent
placement can temporarily relieve the dysphagia symptomswith an acceptable risk (providing the procedure is handledby a center with plenty of experience), whereas repeatedendoscopic dilations are not to be recommended, since theyexpose the patient to a risk of perforation at every session.
Given the high incidence of multiple metastatic lesionsfrom breast cancer, surgical resection is not the treatment ofchoice as far as the esophagus is concerned, although thereare reports of successful palliative resection with subtotalesophagectomy and gastrointestinal tract reconstruction.14
Nowadays, most authors claim that hormone therapymay be effective in relieving dysphagia. Moreover, a disease-free survival as long as 5 years has been reported withhormone therapy.15,16 Other authors have suggested thatradiotherapy, with or without chemotherapy, should be thetreatment of choice, given the relatively low risk for thepatient and its effectiveness in relieving dysphagia.17 In ourexperience, the preferred treatment shifted with time fromendoscopic dilation or stent placement (with the related riskof severe complications, namely, esophageal perforation andtracheoesophageal fistula) toward hormone therapy or che-motherapy and/or radiotherapy, with improved survival ratefrom 4.5 to 16 months.
These data are confirmed by a recent report from theMayo Clinic,18 with 73 patients affected by gastrointestinalmetastases and peritoneal carcinosis from breast cancer. Mostof these patients were treated with systemic chemotherapy(59%) or hormonal therapy (56%). Chemotherapy and hor-monal therapy significantly affected survival (P � 0.02).Chemotherapy and hormonal therapy should be consideredthe initial treatment, when the diagnosis of mediastinal car-cinosis from breast cancer is made, given that they signifi-cantly affect survival. On the other hand, endoscopic place-ment of a stent should be reserved to those patients who donot have a significant improvement of dysphagia after treat-ment, or in case a tracheoesophageal fistula, although it rarelydevelops.
Given that mediastinal carcinosis from breast cancer isconsidered an advanced-stage disease in any case and espe-cially in patients with distant metastases at diagnosis, nutri-tional support with percutaneous endoscopic gastrostomy orsurgical gastrostomy/jejunostomy (even with minimally in-vasive techniques,19,20 whenever possible) should be guaran-teed to allow a decent quality of life.
CONCLUSIONEsophageal involvement from breast cancer is rare and
its diagnosis is often a clinical challenge. A “breast-esopha-gus” syndrome can be described based on history of breastcancer, worsening dysphagia, typical radiologic pattern, andnegative endoscopic biopsies with apparently normal esoph-ageal mucosa. The diagnostic process (Fig. 5) includes bar-ium swallow, endoscopy with endosonography, chest-abdo-men CT scans, and minimally invasive exploration, whennecessary. These diagnostic tools may be helpful, althoughsometimes the diagnosis can be reached after exclusion ofother diseases or after relieving dysphagia with ex adjuvan-tibus treatments. Finding a distant metastasis helps in diag-
Annals of Surgery • Volume 246, Number 2, August 2007 Breast-Esophagus Syndrome
© 2007 Lippincott Williams & Wilkins 321

nosing mediastinal carcinosis, but in patients without anysigns of distant spread an exploratory thoracoscopy or evenEUS-FNAB (both in experienced centers) is needed to estab-lish a definitive diagnosis. The current treatments of choiceare hormone therapy or chemotherapy and/or radiotherapy,which have replaced endoscopic dilation and stent placementdue to the high risk of complications related with the latter.
REFERENCES1. Wu CM, Hruban RH, Fishman EK. Breast carcinoma metastatic to the
esophagus. CT finding with pathologic correlation. Clin Imaging. 1998;22:343–345.
2. Asch MJ, Wiedel PD, Habif DV. Gastrointestinal metastases fromcarcinoma of the breast: autopsy study and 18 cases requiring operativeintervention. Arch Surg. 1968;96:840–843.
3. Boccardo F, Merlano M, Cannobbio L, et al. Esophageal involvement inbreast cancer: report of six cases. Tumori. 1982;68:149–153.
4. Graham WP 3rd. Gastro-intestinal metastases from carcinoma of thebreast. Ann Surg. 1964;159:477–480.
5. Toreson WE. Secondary carcinoma of the esophagus as a cause ofdysphagia. Arch Pathol. 1944;38:82–84.
6. Sunada F, Yamamoto H, Kita H, et al. A case of esophageal stricture dueto metastatic breast cancer diagnosed by endoscopic mucosal resection.Jpn J Clin Oncol. 2005;35:483–486.
7. Herrera JL. Esophageal metastases from breast carcinoma presenting asachalasia. Am J Med Sci. 1992;303:321–323.
8. Isaacs P, MacGillvray N, Springett N. Late recurrence of breast cancerpresenting with esophageal dysmotility. J Clin Gastroenterol. 1989;11:588–590.
9. Lortat-Jacob JL, Fekete F, Garcia Moran M. Dysplagie et cancer du sein.Ann Chir. 1964;18:975–985.
10. Sanborn EB, Beattie ER Jr, Slaughter DP. Secondary neoplasm of themediastinum. J Thoracic Surg. 1957;35:678–682.
11. Salminen E, Pukkala E, Kiel K, et al. Impact of radiotherapy in the riskof esophageal cancer as subsequent primary cancer after breast cancer.Int J Radiat Oncol Biol Phys. 2006;65:699–704.
12. Sobel JM, Lai R, Mallery S, et al. The utility of EUS-guided FNA in thediagnosis of metastatic breast cancer to the esophagus and the medias-tinum. Gastrointest Endosc. 2005;61:416–420.
13. De Palma GD, Di Matteo E, Romano G, et al. Plastic prosthesis versusexpandable metal stents for palliation of inoperable esophageal thoraciccarcinoma: a controlled prospective study. Gastointest Endosc. 1996;43:478–482.
14. Koike M, Akiyama S, Kodera Y, et al. Breast carcinoma metastasis tothe esophagus: report of two cases. Hepatogastroenterology. 2005;52:1116–1118.
15. Shimada Y, Imamura M, Tobe T. Successful esophagectomy for meta-static carcinoma of the esophagus from breast cancer: a case report. JpnJ Surg. 1989;19:82–85.
16. Erman M, Karaoglu A, Oksuzoglu B, et al. Solitary esophageal metas-tasis of breast cancer after 11 years: a case report. Med Oncol. 2002;19:171–175.
17. Atkins JP. Metastatic carcinoma to the esophagus: endoscopic consid-erations with special reference to carcinoma of the breast. Ann OtolRhinol Laryngol. 1966;75:356–367.
18. McLemore EC, Pockaj BA, Reynolds C, et al. Breast cancer: presenta-tion and intervention in women with gastrointestinal metastasis andcarcinomatosis. Ann Surg Oncol. 2005;12:886–894.
19. Murayama KM, Johnson TJ, Thompson JS. Laparoscopic gastrostomyand jejunostomy are safe and effective for obtaining enteral access.Am J Surg. 1996;172:591–594.
20. Denzer U, Mergener K, Kanzler S, et al. Mini-laparoscopically guidedpercutaneous gastrostomy and jejunostomy. Gastrointest Endosc. 2003;58:434–438.
FIGURE 5. Flow chart for diagnosis and treatment. EGD,esophagogastroduodenoscopy; CT, computed tomography;EUS, endoscopic ultrasound; PET, positron emission tomog-raphy; FNAB, fine needle aspiration biopsy.
Rampado et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins322

ORIGINAL ARTICLES
Predictors and Outcome of Gastrointestinal Complicationsin Patients Undergoing Cardiac Surgery
Farzan Filsoufi, MD, Parwis B. Rahmanian, MD, Javier G. Castillo, MD, Corey Scurlock, MD,Peter E. Legnani, MD, and David H. Adams, MD
Objective: To determine the incidence and independent predictorsof gastrointestinal complications (GICs) following cardiac surgery.Summary Background Data: Gastrointestinal ischemia and hem-orrhage represent a rare but devastating complication followingheart surgery. The profile of patients referred for cardiac surgery haschanged during the last decade, questioning the validity of previ-ously reported incidence and risk factors.Methods: We retrospectively analyzed prospectively collected datafrom 4819 patients undergoing cardiac surgery between 1998 and2004. Patients with GICs were compared with the entire patientpopulation. Study endpoints were mortality, postoperative morbid-ities, and long-term survival.Results: GICs occurred in 51 (1.1%) patients. Etiologies wereintestinal ischemia (n � 30; 59%) and hemorrhage (n � 21; 41%).The incidence decreased during the study period (1998–2001: 1.3%,2002–2004: 0.7%; P � 0.04). The incidence per type of procedurewas as follows: coronary artery bypass grafting (CABG)/valve(2.4%), aortic surgery (1.7%), valve surgery (1.0%), and CABG(0.5%; P � 0.001). Multivariate analysis revealed age (odds ratio�OR� � 2.1), myocardial infarction (OR � 2.5), CHF (OR � 2.4),hemodynamic instability (OR � 2.8), cardiopulmonary bypass time�120 minutes (OR � 6.2), peripheral vascular disease (OR � 2.2),renal (OR � 3.2), and hepatic failure (OR � 10.8) as independentpredictors of GICs. The overall hospital mortality among patientswith GICs was 33%. Long-term survival was significantly decreasedin patients with GICs compared with the control group.Conclusions: Gastrointestinal complications following cardiac sur-gery remain rare with an incidence �1% in a contemporary series.The key to a lower incidence of GICs lies in systematic applicationof preventive measures and new advances in intraoperative manage-ment. Identification of independent risk factors would facilitate thedetermination of patients who would benefit from additional peri-operative monitoring. Future resources should therefore be redi-rected to mitigate GICs in high-risk patients.
(Ann Surg 2007;246: 323–329)
The incidence of gastrointestinal complications (GICs) af-ter cardiac surgery varies between 0.3% and 3%.1–4
Although they occur infrequently, GI events are seriouscomplications that carry high mortality and morbidity rates.Previous reports on the incidence and risk factors for thiscomplication have focused on patients undergoing coronaryartery bypass grafting (CABG) or large cohorts of cardiacsurgery patients with predominantly CABG procedures.2,5
During the last few years, with the broader application ofpercutaneous transluminal coronary angioplasty (PTCA), thepopulation of patients referred for cardiac surgery has signif-icantly changed. Currently, a majority of patients in tertiarycenters is referred for more complex procedures includingcombined valve/CABG, multiple valve and aortic procedures.
In addition, during the last decade, significant advanceshave also been made in the perioperative management ofpatients undergoing cardiac surgery, which could have im-pacted the incidence of GICs. These changes have raised thequestion of the validity of previously reported incidence andrisk factors for the occurrence of this complication. In thisstudy, we sought to determine the incidence, independent riskfactors, and outcome following GICs in a heterogeneouscohort of cardiac surgery patients in a recent era.
PATIENTS AND METHODS
Study PopulationWe retrospectively analyzed a series of 4986 consecu-
tive patients undergoing cardiac surgery at the Mount SinaiMedical Center between January 1998 and December 2004.Patients undergoing cardiac transplantation or assist deviceimplantation (n � 167) were excluded from this study.
The protocol was approved by our local institutionalreview board and compliant to the Health Insurance Porta-bility and Accountability Act regulations and the ethicalguidelines of the 1975 declaration of Helsinki. The approvalincluded a waiver of informed consent.
Data Collection and Outcome AnalysisClinical variables were prospectively entered into the
New York State Department of Health (NYSDH, State Car-diac Advisory Committee) data registry (www.health.state.ny.us). The NYSDH data registry represents a mandatory ver-ified peer-reviewed data collection system including all adultcardiac surgery procedures in the state of New York and recordsand analyzes data in a strictly supervised and widely reported
From the Department of Cardiothoracic Surgery, Mount Sinai School ofMedicine, New York, NY.
Reprints: Farzan Filsoufi, MD, Department of Cardiothoracic Surgery,Mount Sinai School of Medicine, 1190 Fifth Avenue, Box 1028, NewYork, NY 10029. E-mail: [email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0323DOI: 10.1097/SLA.0b013e3180603010
Annals of Surgery • Volume 246, Number 2, August 2007 323

fashion. Patient demographics and risk factors, operative infor-mation, and postoperative outcome data were retrospectivelyanalyzed. Additional information was obtained from patientcharts when necessary. Follow-up survival information wasobtained by cross matching patient’s social security number withthe web-based social security death index (ssdi.rootsweb.com).When a patient was not registered as being dead, he wasconsidered alive. Table 1 summarizes preoperative variablesincluded in this study and their definition as indicated.
In addition, the logistic EuroSCORE was used for riskstratification.6 The EuroSCORE is a risk stratification systembased on multiple preoperative risk factors to predict opera-tive mortality. Patients were divided into 4 subgroups deter-mined by their predicted mortality as follows: low risk (3%),moderate risk (3%–9%), high risk (9%–25%), and very highrisk (�25%).
The main outcome parameter of this study is the oc-currence of postoperative GICs. This complication was de-fined in accordance to the NYSDH data registry: any post-operative episode of vomiting blood, gross blood in the stool,perforation or necrosis of the stomach or intestine that re-quired an invasive diagnostic or therapeutic intervention,such as gastroscopy, colonoscopy, or laparotomy. Other GI-related morbidities such as cholecystitis, pancreatitis, or par-alytic ileus were not included in the analysis. The medicalrecords, operative notes, radiographs, and autopsy reports ofall patients with GICs were reviewed thoroughly when ap-plicable. Patients without GICs served as the control group.
Further outcome measures for this study included hospitalmortality, major postoperative complications (respiratory fail-ure, renal failure, deep sternal wound infection, bleeding requir-ing reoperation, unplanned reoperation, stroke), length of hos-pital stay, and late survival. Hospital mortality was defined asdeath following the procedure before patients discharge regard-less of the duration of hospitalization. Patients who died afterdischarge from hospital but within 30 days following the pro-cedure were also considered as hospital deaths. Respiratoryfailure was defined as prolonged ventilator therapy (�72 hours)or need for reintubation or tracheostomy. Renal failure wasdefined as creatinine �2.5 mg/dL for more than 7 postoperativedays or the need for dialysis. Stroke was defined as a newpermanent neurologic event occurring perioperatively or post-operatively.
Intraoperative and Postoperative ManagementAll procedures were performed using standard anes-
thetic and surgical techniques adapted to the individual pro-cedures. A small skin incision and a full or partial sternotomywere performed in all patients. Epi-aortic scanning of theascending aorta was done to rule out ascending aortic athero-sclerotic disease prior to cannulation (since January 2002).After systemic heparinization, cardiopulmonary bypass(CPB) was instituted between the ascending aorta and eitherthe right atrium using a two-stage cannula or both venaecavae. Cardioplegia using high potassium cold blood wasadministered in an antegrade and/ or retrograde fashion formyocardial protection. In patients undergoing valve surgery,further myocardial protection was obtained with mild tomoderate systemic cooling (28°C to 30°C). Procedures in-volving the aortic arch were performed in deep hypothermiccirculatory arrest. After the completion of CPB, protaminewas given based on the heparin level. Following surgery, allpatients were transferred to the intensive care unit. Patientswere weaned from ventilator when hemodynamic stabilitywas achieved, no postoperative bleeding occurred, and ade-quate consciousness was obtained. Stable patients were trans-ferred to the regular ward and discharged home or to a
TABLE 1. Variables Included in Present Study
Variables
Age
Gender
Preop. variables
Weight (kg)
Height (cm)
Body mass index (kg/m2)
Diabetes mellitus requiring medication
Hypertension
Preop. renal failure (creatinine �2.5 mg/dL or dialysis)
Prior cerebrovascular accident
Peripheral vascular disease
Chronic lung disease (COPD)
Hepatic failure (liver disease and bilirubin �2 mg/dL and albumin�3.5 g/dL)
Prior myocardial infarction
Prior heart operation
Congestive heart failure (NYHA class III and IV)
Active endocarditis
Ejection fraction (%)
Urgent operation (requiring operation during current hospitalization)
Emergent operation (refractory unrelenting cardiac compromiserequiring emergency operation )
Unstable (patient requires pharmacologic or mechanical support tomaintain blood pressure or output)
Cardiogenic shock (acute hypotension or low cardiac index despitesupport)
Preop. intra-aortic balloon pump
Intraop. variables
Type of procedure (isolated CABG, isolated valve, valve/CABG, aorticprocedures)
Cardiopulmonary bypass time (CPB time)
Cross clamp time
Use of internal mammary artery
Postop. variables
Hospital mortality (death during same admission or within 30 d aftersurgery when discharged)
Renal failure (Creatinine �2.5 mg/dL more than 7 days or dialysis)
Respiratory failure (prolonged ventilator therapy ��72 hours�,reintubation, or tracheostomy)
Stroke (new permanent neurological event)
Postop. myocardial infarction
Bleeding requiring reoperation
Deep sternal wound infection
Unplanned reoperation
Gastrointestinal complication
Length of hospital stay
Filsoufi et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins324

rehabilitation facility when appropriate. Intraoperative vari-ables used in this study are reported in Table 1.
Ulcer ProphylaxisPatients undergoing cardiac surgery at our institution
routinely received H2-blockers as ulcer prophylaxis. Patientswith a history of GI bleeding were treated with proton pumpinhibitors instead.
Statistical AnalysesNormally distributed continuous variables are pre-
sented as mean � SD and otherwise as median � interquar-tile range (IQR). Categorical variables are shown as thepercentage of the sample. A P value �0.05 was consideredstatistically significant for all used tests.
To identify preoperative and perioperative factors as-sociated with the occurrence of GICs, data were explored bycontingency table analyses to look for evidence that somevalues should be grouped and for evidence of linear trend incontinuous variables. �2 test, Fisher exact test, and Cochran-Armitage test for trend were used to identify factors thatsignificantly influenced the risk of GICs when considered oneat a time. These factors were then entered in a stepwiselogistic regression analysis to identify a set of independentvariables associated with postoperative GICs. The odds ratio(OR), corresponding 95% confidence interval (CI), and the Pvalue are reported for each independent factor. Similar anal-yses were undertaken to identify independent factors predict-ing hospital mortality in patients suffering from postoperativeGI complications. Long-term survival was analyzed usingKaplan–Meier survival curves. Differences in patient charac-teristics were controlled by Cox proportional hazard analysis.The statistical analysis was performed using SPSS for Win-dows, version 14.0 (SPSS Inc., Chicago, IL) and SAS version9.1.3 (SAS Institute Inc., Cary, NC).
RESULTSA total of 4819 adult patients were included in this
study. The mean age was 63 � 14 years, 52% (n � 2497) ofpatients were older than 65 years, and 64% (n � 3084) ofpatients were male. Preoperative risk factors included hyper-tension (n � 3226, 67%), diabetes mellitus (n � 1278, 26%),PVD (n � 534, 11%), COPD (n � 334, 7%), and renal failure(n � 240, 5%). Congestive heart failure was present in 980patients (20%). The mean ejection fraction was 45.5% �15.2%. Eleven percent (n � 569) of patients had a history ofat least one previous cardiac operation. Patient demographicsand the distribution of preoperative risk factors are summa-rized in Table 2.
Forty-nine percent (n � 2374) of patients underwentisolated CABG (conventional CABG, n � 2002, 84%; off-pump CABG, n � 372, 16%), 21% (n � 1001) had a singleor multiple valve procedures, 14% (n � 678) of patientsunderwent combined valve and CABG procedures, and 16%(n � 766) underwent surgery involving the ascending aorta orthe aortic arch. During the study period, a total of 2328patient underwent isolated CABG procedures.
Fifty one patients (1.1%) suffered from postoperativeGICs. The majority of these patients presented with intestinal
ischemia (n � 30 of 51, 59%). The clinical manifestationsincluded necrosis of the small intestine in 16 patients andnecrosis of the colon/rectum in 14 patients. Clinical symp-toms in patients with ischemic GICs were predominatelyabdominal distension (n � 20, 67%) and abdominal pain(n � 5, 17%). In addition, elevation of serum lactate wasconsistently observed in the majority of patients (n � 19,63%). Abdominal CT scan was available in 12 patients andshowed abnormalities suggestive of ischemic bowel diseasein 8 (67%) patients (dilated small bowel loops, n � 8, wallthickening, n � 4, extraluminal air, n � 3, pneumatosis, n �1). The remaining 21 patients (41%) presented with upper orlower gastrointestinal hemorrhage. The clinical manifesta-tions in this subgroup were as follows: esophageal varicosebleeding (2 patients), erosive gastritis/gastric ulcer (12 pa-tients), duodenal ulcer (2 patients), and colorectal bleeding (5patients). In patients with hemorrhagic complications, he-matemesis (n � 12, 57%) and decreased hematocrit level
TABLE 2. Univariate Analysis of Patient Demographics,Preoperative Risk Factors, and Operative Data
Control Group(n � 4768)
GIC Group(n � 51) P
Mean age (yr) 63.4 � 13.8 69.0 � 10.6 0.040
Age �65 yr 2350 (49.3) 35 (68.6) 0.004
Male gender 3013 (63.2) 29 (56.9) 0.215
CHF 930 (19.5) 25 (49.0) �0.001
EF �30 829 (17.4) 19 (37.3) 0.001
Previous MI 524 (11.0) 14 (27.5) 0.001
Previous cardiac operation 542 (11.4) 12 (23.5) 0.011
Hemodynamic instability 141 (3.0) 8 (15.7) �0.001
Preop. IABP 155 (3.8) 2 (4.1) 0.560
Renal failure 231 (4.8) 11 (21.6) �0.001
PVD 516 (10.8) 14 (27.5) 0.001
Hepatic failure 29 (0.6) 3 (5.9) 0.004
Endocarditis 103 (2.2) 5 (9.8) 0.005
Previous CVA 346 (7.3) 9 (17.6) 0.011
Hypertension 3184 (66.8) 40 (78.4) 0.050
Diabetes mellitus 1262 (26.5) 18 (35.3) 0.106
COPD 328 (6.9) 6 (11.8) 0.139
Op. procedures 0.001
Isolated CABG 2362 (49.5) 12 (23.5) �0.001
Single and multiplevalves
991 (20.8) 10 (19.6) 0.500
Combined CABG �valves
662 (13.9) 16 (31.4) 0.001
Aortic procedures 753 (15.8) 13 (25.5) 0.051
CPB time �120 min 2998 (62.9) 47 (92.2) �0.001
Mean EuroSCORE 9.4 � 11.6 23.9 � 17.9 �0.001
Low (�3%) 1441 30.2 1 2.0 �0.001
Moderate (3–�9%) 1879 39.4 9 17.6 0.001
High (9–�25%) 1022 21.4 18 35.3 0.017
Very high (�25%) 426 8.9 23 45.1 �0.001
Values are mean � SD or as no. (%).CHF indicates congestive heart failure; EF, ejection fraction; MI, myocardial
infarction; IABP, intra-aortic balloon pump; PVD, peripheral vascular disease; CVA,cerebrovascular accident; COPD, chronic obstructive pulmonary disease; CABG, cor-onary artery bypass grafting; CPB, cardiopulmonary bypass.
Annals of Surgery • Volume 246, Number 2, August 2007 Gastrointestinal Complications After Cardiac Surgery
© 2007 Lippincott Williams & Wilkins 325

(n � 17, 81%) despite administration of red blood cells werethe most common indicators. The diagnosis was confirmed inall patients with upper or lower gastrointestinal endoscopy.We observed a significant decrease of GICs during the studyperiod: from 1.3% between 1998 and 2001 to 0.7% between2002 and 2004 (P � 0.044).
The rate of GICs was different when the patient popu-lation was stratified by procedures: isolated CABG (n � 12,0.5%), single or multiple valve surgery (n � 10, 1.0%),combined CABG and valve procedures (n � 16, 2.4%), andaortic surgery (n � 13, 1.7%) (P � 0.001). The incidence ofgastrointestinal complications in the conventional and off-pump CABG groups were 10 (0.5%) and 2 (0.5%), respec-tively (P � not significant). When patients were stratifiedaccording to EuroSCORE, we observed an increasing rate ofGICs with increased predicted mortality: low risk (n � 2,0.1%), moderate risk (n � 8, 0.4%), high risk (n � 17, 2%),and very high (n � 24, 5%) (P � 0.001).
Predictors of Gastrointestinal ComplicationsIn univariate analysis, patients with GICs were more
likely to present preoperative risk factors including age �65years, severe impaired left ventricular function, history ofmyocardial infarction, CHF, hemodynamic instability on ad-mission, need for intra-aortic balloon pump, previous cardiacprocedure, CPB time �120 minutes, previous CVA, PVD,hepatic failure, preoperative renal failure, endocarditis, andEuroSCORE (Table 2). Stepwise multivariate logistic regres-sion analysis revealed age over 65 years (odds ratio �OR� �2.1, P � 0.023), previous myocardial infarction (OR � 2.5,P � 0.006), CHF (OR � 2.4, P � 0.005), hemodynamicinstability (OR � 2.8, P � 0.010), CPB time �120 minutes(OR � 6.2, P � 0.001), PVD (OR � 2.2, P � 0.001), renalfailure (OR � 3.2, P � 0.003), and hepatic failure (OR �10.8, P � 0.001) as independent predictors for the occurrenceof GICs after cardiac surgery (Table 3).
Outcome of Patients With GastrointestinalComplications
The treatment strategies varied according to the etiol-ogy of GICs. Sixteen of 30 patients with ischemic GICsunderwent surgery. The procedures performed included small
bowel resection (n � 6) and hemicolectomy/ colectomy (n �10). Fourteen patients with ischemic GICs were not explored.The majority of these patients had a delayed diagnosis andwere considered too critically ill to undergo an invasiveprocedure. All 21 patients with GI hemorrhage were treatedwith transfusion and proton pump inhibitors. In addition, 15patients (71%) required additional endoscopic treatment, in-cluding clip placement, thermocoagulation, or epinephrinesclerotherapy. Finally, surgery was performed in 3 patients(14%). One of these 3 patients underwent gastrectomy forintractable upper GI bleeding, whereas 2 patients had ahemicolectomy for lower GI bleeding.
The overall hospital mortality among patients withGICs was 33% (n � 17) compared with a mortality rate of4.3% (n � 204) in patients without postoperative GICs (P �0.001). In the subgroup of patients presenting with bowelnecrosis, the mortality rate was 47% (n � 14 of 30). Themortality rate among patients with GICs undergoing surgerywas 25% (n � 4 of 16). In patients with ischemic event notundergoing surgery, the mortality rate was 71% (n � 10 of14). Among patients with hemorrhagic GICs, the mortalityrate was 14% (3 of 21).
Patients with GICs were more likely to present othermajor postoperative complications, including stroke, myocar-dial infarction, sternal wound infection, reoperation for bleed-ing, renal failure, and respiratory failure (Table 4). Themedian length of hospital stay was significantly increased inpatients with GICs compared with the control group (7 days,IQR 5–11 days vs. 32 days, IQR 14–73 days, P � 0.001).
Follow-up DataFollow-up was completed for 4591 patients (98%). The
mean follow-up time was 4.2 � 2.3 years. Long-term sur-vival of discharged patients was significantly decreased inpatients with GICs compared with patients without this com-plication. One-year and 5-year survival rates were 69% � 8%and 59% � 9% for patients with GICs and 94% � 1% and82% � 1%, respectively, for the population without compli-cation (P � 0.001). Figure 1 shows Kaplan–Meier survivalcurves.
DISCUSSIONThis study was conducted to analyze retrospectively the
incidence, independent risk factors for the occurrence ofTABLE 3. Independent Predictors of the Development ofGIC Following Cardiac Surgery (Multiple Logistic RegressionAnalysis)
Odds Ratio 95% CI P
PVD 2.2 1.4–3.3 0.000
CPB time �120 min 6.2 2.2–17.3 0.001
Hepatic failure 10.8 2.6–45.8 0.001
Renal failure 3.2 1.5–6.9 0.003
Congestive heart failure 2.4 1.3–4.4 0.005
Myocardial infarction 2.5 1.3–4.8 0.006
Hemodynamic instability 2.8 1.3–6.1 0.010
Age �65 yr 2.1 1.1–3.8 0.023
PVD indicates peripheral vascular disease; CPB, cardiopulmonary bypass; CI,confidence interval.
TABLE 4. Mortality and Morbidities
ControlGroup
GICGroup
Pn % n %
In-hospital mortality 204 4.2 17 33.3 �0.001
Respiratory failure 376 7.8 35 68.6 �0.001
Postop. CVA 112 2.3 8 15.7 �0.001
Sternal wound infection 75 1.6 7 13.7 �0.001
Renal failure 68 1.4 6 11.8 �0.001
Reoperation for bleeding 104 2.2 5 9.8 0.006
Postop. MI 31 0.6 3 5.9 0.005
CVA indicates cerebrovascular accident; MI, myocardial infarction.
Filsoufi et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins326

GICs, and early and late survival following this condition ina large cohort of patients undergoing cardiac surgery withina recent period. In our study, using a precise definition ofGICs based on the NYSDH data registry, the incidence of thiscomplication was 1.1% (n � 51). The majority of patients(59%, n � 31) had ischemic bowel disease, while 41% (n �21) had GI hemorrhage. The overall hospital mortality was33% (47% in the ischemic group and 14% in patients withgastrointestinal hemorrhage). We were able to identify 8independent predictors for the occurrence of GICs, includingage over 65 years, previous myocardial infarction, CHF,hemodynamic instability, PVD, renal failure, hepatic failure,and CPB time �120 minutes. Long-term survival of patientswith GICs was significantly reduced to patients without thiscomplication.
GICs following open heart procedures represent a rarebut serious event. The incidence of GI complications in theliterature varies between 0.3% and 3%. This variation mightbe explained by an inconsistency in defining GICs in differentstudies. Mangi et al analyzed 8709 patients undergoing car-diac surgery and reported an incidence as low as 0.5%.2
These authors only reported patients with GICs, which re-quired a general surgical consult. Using this definition, theyonly included the “sickest” patients presenting with advancedGICs, particularly ischemic bowel disease. Consequently,patients with GICs controlled by medical or endoscopictreatment without surgical consult were not reported in theirseries. In contrast, one of the highest rates of GICs wasreported by Christenson et al.3 These authors used a broaddefinition of GICs, including acute cholecystitis, pancreatitis,and medically treated GI bleeding and reported an incidenceof 2.9% in a series of 3493 patients. Despite differences indefining this postoperative complication, the 2 most commonetiologies of GICs reported by most clinical series are isch-emic bowel disease and GI hemorrhage.2,4,5 Based on thesefindings, the NYSDH Data Registry requires the report ofthese 2 major events in patients undergoing cardiac surgery.
According to this precise definition, the incidence of GICswas 1.1% in our series, which is at the lower end of thereported range in the literature.
Another interesting finding of our study is that we wereable to demonstrate a significant decrease in the incidence ofthis complication during the study period (from 1998 to 2001,1.3%; and from 2002 to 2004, 0.7%, P � 0.04). Thisreduction was notified in the incidence of both, ischemic andmore markedly of hemorrhagic GICs. Our study design doesnot allow us to determine the precise explanation for thisfinding; however, we think that the key to a lower incidenceof GICs lies in systematic application of preventing measuresand new advances in intraoperative management of patientsundergoing cardiac surgery. The decrease in the incidence ofhemorrhagic GICs during the recent era is probably related toa better patient selection preoperatively with the routineworkup of patients with a history of GI hemorrhage andpeptic ulcer. In addition, improved perioperative ulcer pro-phylaxis with the systematic use of H2-blockers or protonpump inhibitors might have contributed in decreasing theincidence of this condition. The decrease in the incidence ofischemic GICs might be explained by implementation of newintraoperative measurements, which were introduced in ourpractice since 2002. These measurements include routineepi-aortic ultrasonography to detect any atherosclerotic le-sions2,7 prior to aortic manipulation and cannulation. Thesurgical strategy is then determined according to the presenceor absence of calcification in the ascending aorta and itsextent. The resulting reduced rate of plaque disruption andperipheral embolization due to aortic cannulation might havecontributed in decreasing the incidence of GI ischemicevents.7,8 Another important measurement is the use of axil-lary artery instead of femoral artery as an inflow for arterialcannulation in patients undergoing complex aortic surgery inthe setting of ascending aortic/arch dissections or aneu-rysms.9 This technique preserves antegrade arterial perfusionduring CPB and avoids retrograde perfusion, which carriesthe risk of complications such as retrograde atheroembolismor organ malperfusion.10 Maintenance of higher perfusionpressures (�70 mm Hg) in all patients, particularly thosewith atherosclerotic risk factors,11 and an adequate hemato-crit on CPB12 may have also played a role in avoidingabdominal organ hypoperfusion.
Our data indicate that ischemic bowel disease remainsthe main etiology of GICs. Previous studies from the 1990sreported gastrointestinal hemorrhage as the most frequentetiology of GICs.1,4 In 1995, in a series of 1831 patients,Spotnitz et al4 reported an incidence of 2% GICs followingcardiac surgery. In their series, 46% had upper or lower GIbleeding and only 5% suffered from bowel necrosis.4 Incontrast, in a more recent study, Mangi et al reported mes-enteric ischemia as the dominant etiology of GICs. In theirstudy, 67% patients with GICs had an intestinal ischemia.2 Inour series, ischemic GICs occurred in 59% (n � 30 of 51) ofpatients confirming the finding of the Mangi et al study. Thechanges in the profile of patients undergoing cardiac surgerymay be a potential explanation for the increasing incidence ofischemic GI events. Today cardiac surgical patients are older,
FIGURE 1. Kaplan–Meier survival curves showing long-termsurvival of discharged patients. GICs, gastrointestinal compli-cations.
Annals of Surgery • Volume 246, Number 2, August 2007 Gastrointestinal Complications After Cardiac Surgery
© 2007 Lippincott Williams & Wilkins 327

present with significant preoperative comorbidities includingatherosclerotic diseases and require more complex and pro-longed cardiac procedures. The presence of these factorspotentially increases the risk of abdominal organ hypoperfu-sion and thromboembolic events, which represent the 2 mainpathophysiologic mechanisms of ischemic GICs. This expla-nation is further corroborated by a clear identification ofindependent risk factors for the occurrence of this complica-tion using multivariate analysis. Only a few studies haveperformed this type of statistical analysis and were able tofind the influence of age,1,5,13 NYHA class,1,5 postoperativevascular complications,5 postoperative low cardiac outputsyndrome,13 need for IABP support,2 and inconsistently CPBtime1,5 as predictors for the occurrence of GICs followingcardiac surgery. Our study revealed 8 independent factorsassociated with this complication, demonstrating the differentpathophysiologic mechanisms involved, namely, hypoperfu-sion and thromboembolic events. Age over 65 years, previousmyocardial infarction, PVD, and renal failure reflect a highincidence of atherosclerotic burden increasing the risk ofthromboembolic events following cardiac surgery. Other riskfactors, such as CHF, hemodynamic instability, and CPBtime �120 minutes reflect the risk for perioperative andpostoperative hypoperfusion due to low cardiac output ordecreased systemic blood pressure.
Most of our patients with GICs presented with morethan one complication. This is in accordance with otherpublished data.5,14 Recht et al reported a significantly in-creased rate of neurologic, pulmonary, renal, and infectiouscomplications in patients with GICs, but were not able toidentify a cause-relationship between different organ dys-functions and GI events.14 Similarly, our study was notdesigned to clarify the association between the occurrence ofthis complication and other major morbidities following car-diac surgery.
Despite the fact that we were able to show the reductionin the incidence of this complication during the recent years,the associated mortality, particularly of intestinal ischemiaremains high.2,5 Most patients with bleeding complicationsare diagnosed early and can be treated medically or endo-scopically with a relatively low mortality. In contrast, inpatients with intestinal ischemia diagnosis is often delayeddue to masked symptoms and the surgical therapy is per-formed often as a salvage operation resulting in a highmortality. Therefore, in patients with high risk for this com-plication careful postoperative examination is recommendedto establish early diagnosis and surgical therapy when thiscomplication occurs.
Reports on long-term survival in patients with GICsremain scarce. In our study, 1-year and 5-year survival indischarged patients with GICs were 68% � 8% and 59% �9%, respectively, compared with 94% � 1% and 82% � 1%in patients without this complication. This is similar to theresults reported by Andersson et al, which have shown a1-year survival rate of 50% in patients with GICs.5 Ourobservation of a decreased survival in these patients evenafter hospital discharge might be based on the possibility thatGICs may be a marker of predisposition to death rather than
a direct cause. This assumption is supported by our findingthat the incidence of GI events following cardiac surgery iscorrelated to the predicted mortality by EuroSCORE. Thisimplies that at least some patients who die after a GI eventwere independently disposed to perioperative and postoper-ative death regardless of the GICs. However, we were notable to determine the exact causes of death in patients whodied during follow-up.
LimitationsThis study retrospectively analyzed prospectively col-
lected data and has therefore certain limitations. Databasesmay underreport events and risk factors. However, theNYSDH periodically visits participating center for validationand there has not been any question of the quality of our data,or underreporting of adverse events in our center. Anotherproblem all databases face is that of incomplete data. Riskmodels can only adjust for data that has been collected. Ourstudy did not examine some previously reported risk factorsfor the occurrence of GICs such as heparin-induced throm-bocytopenia, atrial fibrillation, and transfusion require-ments.2,15
CONCLUSIONGastrointestinal complications, particularly ischemic
GICs, remain a rare but life-threatening event followingcardiac surgery. The systematic application of measurementssuch as epi-aortic scanning, avoidance of retrograde perfu-sion by the use of axillary artery instead of femoral arterycannulation, and the preservation of a high perfusion pressureduring CPB have probably contributed in the decrease of theincidence of this complication in recent years. Identificationof independent risk factors would facilitate the determinationof patients who would benefit from additional workup prior toundergoing cardiac surgery. In addition, these patients wouldbenefit from close surveillance for early diagnosis, whichshould lead to an aggressive treatment approach. Futureresources should therefore be redirected to mitigate GICs inhigh-risk patients.
ACKNOWLEDGMENTSThe authors thank Carol A. Bodian, DrPH, Department
of Biomathematical Sciences, Mount Sinai School of Medi-cine, New York, NY, for expert statistical support.
REFERENCES1. Zacharias A, Schwann TA, Parenteau GL, et al. Predictors of gastrointes-
tinal complications in cardiac surgery. Tex Heart Inst J. 2000;27:93–99.2. Mangi AA, Christison-Lagay ER, Torchiana DF, et al. Gastrointestinal
complications in patients undergoing heart operation: an analysis of8709 consecutive cardiac surgical patients. Ann Surg. 2005;241:895–901; discussion 901–904.
3. Christenson JT, Schmuziger M, Maurice J, et al. Postoperative visceralhypotension the common cause for gastrointestinal complications aftercardiac surgery. Thorac Cardiovasc Surg. 1994;42:152–157.
4. Spotnitz WD, Sanders RP, Hanks JB, et al. General surgical complica-tions can be predicted after cardiopulmonary bypass. Ann Surg. 1995;221:489–496; discussion 496–497.
5. Andersson B, Nilsson J, Brandt J, et al. Gastrointestinal complicationsafter cardiac surgery. Br J Surg. 2005;92:326–333.
6. Nashef SA, Roques F, Michel P, et al. European system for cardiac
Filsoufi et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins328

operative risk evaluation (EuroSCORE). Eur J Cardiothorac Surg.1999;16:9–13.
7. Wareing TH, Davila-Roman VG, Daily BB, et al. Strategy for thereduction of stroke incidence in cardiac surgical patients. Ann ThoracSurg. 1993;55:1400–1407; discussion 1407–1408.
8. Sharony R, Grossi EA, Saunders PC, et al. Propensity case-matched anal-ysis of off-pump coronary artery bypass grafting in patients with atheroma-tous aortic disease. J Thorac Cardiovasc Surg. 2004;127:406–413.
9. Hedayati N, Sherwood JT, Schomisch SJ, et al. Axillary artery cannu-lation for cardiopulmonary bypass reduces cerebral microemboli. J Tho-rac Cardiovasc Surg. 2004;128:386–390.
10. Watanabe K, Fukuda I, Osaka M, et al. Axillary artery and transapicalaortic cannulation as an alternative to femoral artery cannulation. EurJ Cardiothorac Surg. 2003;23:842––843.
11. Gold JP, Charlson ME, Williams-Russo P, et al. Improvement ofoutcomes after coronary artery bypass: a randomized trial comparing
intraoperative high versus low mean arterial pressure. J Thorac Cardio-vasc Surg. 1995;110:1302–1311; discussion 1311–1314.
12. DeFoe GR, Ross CS, Olmstead EM, et al. Lowest hematocrit on bypassand adverse outcomes associated with coronary artery bypass grafting:Northern New England Cardiovascular Disease Study Group. Ann Tho-rac Surg. 2001;71:769–776.
13. Yoshida K, Matsumoto M, Sugita T, et al. Gastrointestinal complica-tions in patients undergoing coronary artery bypass grafting. Ann ThoracCardiovasc Surg. 2005;11:25–28.
14. Recht MH, Smith JM, Woods SE, et al. Predictors and outcomes ofgastrointestinal complications in patients undergoing coronary arterybypass graft surgery: a prospective, nested case-control study. J Am CollSurg. 2004;198:742–747.
15. Ghosh S, Roberts N, Firmin RK, et al. Risk factors for intestinalischaemia in cardiac surgical patients. Eur J Cardiothorac Surg. 2002;21:411–416.
Annals of Surgery • Volume 246, Number 2, August 2007 Gastrointestinal Complications After Cardiac Surgery
© 2007 Lippincott Williams & Wilkins 329

ORIGINAL ARTICLES
Treatment of Palmar HyperhidrosisT4 Level Compared With T3 and T2
Yu-Tang Chang, MD,* Hsien-Pin Li, MD,* Jui-Ying Lee, MD,* Pei-Jung Lin, MD,†Chien-Chih Lin, MD,*‡ Eing-Long Kao, MD,*‡ Shah-Hwa Chou, MD,*‡ and Meei-Feng Huang, RN*
Objective: The aim of this study was to compare the outcomes of 3different levels of sympathectomy.Summary Background Data: Most surgeons still perform T2 orT2–3 sympathectomy for palmar hyperhidrosis, but both these treat-ments can cause severe side effects. Some recent articles haveadvocated T4 sympathectomy and obtained satisfactory results.Methods: Between January 2000 and August 2004, 234 records ofpatients treated for palmar hyperhidrosis were retrospectively re-viewed. Of them, 86 patients were treated with endoscopic thoracicsympathectomy of T2 (ETS2), 78 patients with ETS3, and 70 patientswith ETS4. Follow-up data were collected using a telephone ques-tionnaire with a scoring system. Multiple linear regressions wereused to model markers for degree of satisfaction and severity ofcompensatory sweating (CS), including descriptive data, level ofsympathectomy, clinical outcomes, and postoperative complications.Results: Mean follow-up was 47.1 � 17.2 months. All 3 levels ofsympathectomy could have achieved comparable improvement ofpalmar hyperhidrosis (P � 0.162). However, 88.5% of the patientsnoticed CS. Patients with ETS4 presented the lowest incidence of CS(P � 0.030), had the least severity of CS (� � �1.537, P � 0.002),and felt the least palmar overdryness (P � 0.001). None expressedregret for the procedure in the ETS4 group (P � 0.022). Being obesedid not increase the incidence of CS, but the severity of CS wasdirectly related to body mass index (� � 0.917, P � 0.001). Thepatients would be more satisfied if the severity of CS was minimal(� � �0.185, P � 0.002). The degree of satisfaction may decreasewith time (� � �0.025, P � 0.003) and was lower when their palmswere overdry (� � �1.463, P � 0.001).Conclusions: Different from the current procedure of T2 or T3
sympathectomy for palmar hyperhidrosis, T4 sympathectomy wouldbe a better and more effective procedure with minimal long-termcomplications.
(Ann Surg 2007;246: 330–336)
Endoscopic thoracic sympathectomy (ETS) has beenwidely accepted as a safer and more effective procedure
for the treatment of palmar hyperhidrosis with higher successrates. However, the flagrant side effect mostly influencing thequality of life is the presence of compensatory sweating (CS).To reduce the incidence of severe compensatory symptoms,several authors limited the extent of resections for hyperhi-drosis to a single level,1–4 whereas Lin and Telaranta intro-duced the classification of sympathetic disorder according tosegmental distribution of sympathetic innervations.5 Accord-ing to the classification, interruption of T2 ganglion mayameliorate facial blushing and vibration disorder, T3 ganglionfor facial sweating and blushing, T4 for palmar sweating, andT5 for axillary sweating (bromidrosis). Previously, we alsopublished the importance of classification in sympatheticsurgery and offered a proposed mechanism for CS.6
As per most reports from 2005,7–9 most surgeons haveperformed T2 or T2–3 sympathectomy for palmar hyperhidro-sis. Recently, several authors treated palmar hyperhidrosisfollowing the modified Lin-Telaranta classification and ob-tained very good results.1,6,10–12 However, published detailsof any comparative method concerning long-term outcome ofT2, T3, and T4 sympathectomy are still lacking. In the presentstudy, we have analyzed the long-term follow-up of palmarhyperhidrosis treated by the 3 different levels of sympathec-tomy and we have also evaluated which level of ganglioninterrupted is the best for palmar hyperhidrosis.
PATIENTS AND METHODSThis was a retrospective review at a single medical
center between January 2000 and August 2004 by the samesurgical team. During the 5-year period, 158 men and 176women were treated for palmar hyperhidrosis. This studyincluded some patients mentioned in previous articles.6,10
Mean age at operation of hyperhidrosis was 22.9 � 7.7 yearsand mean body mass index (BMI) was 21.1 � 3.2 kg/m2. Onehundred and fifty patients were treated by ETS of T2 (ETS2),92 patients by ETS3, and 92 patients by ETS4. The differentprocedures performed were based on the changes in practiceinspiration from the reports in other centers.3–5,12 Indeed,most patients in group ETS2 were operated on earlier in theperiod and most patients in groups ETS3 and ETS4 underwentsurgery later in the period.
From the *Department of Surgery, Kaohsiung Medical University Hospital;†Department of Neurology, E-Da Hospital and I-Shou University; and‡Department of Surgery, Faculty of Medical School, College of Medi-cine, Kaohsiung Medical University, Kaohsiung, Taiwan.
Reprints: Shah-Hwa Chou, MD, Division of Thoracic Surgery, Departmentof Surgery, Kaohsiung Medical University Hospital, Kaohsiung MedicalUniversity,100 Tzyou 1st Road, Kaohsiung 80708, Taiwan. E-mail:[email protected].
Copyright © 2007 by Lippincott Williams & WilkinsISSN: 0003-4932/07/24602-0330DOI: 10.1097/SLA.0b013e3180caa466
Annals of Surgery • Volume 246, Number 2, August 2007330

Surgical TechniqueThe surgical technique of ETS was performed as pre-
viously described.7,10 Under general anesthesia with singlelumen tracheal intubation, the patient’s arms were extendedslightly upward and the axillae were exposed. Either two5-mm ports or a single-port approach was used. For theformer method, 1 port at the axilla and 1 at the midaxillaryline at the level of the nipple were inserted. For the lattermethod, a 10-mm port was inserted at the third intercostalspace over the midaxillary line. Because the first rib wasusually difficult to visualize through thoracoscopy (Karl StorzGmbH & Co, Tuttlingen, Germany), the second, third, fourth,and fifth ribs were identified according to the anatomiclandmark of the first rib covered by an area of bright yellowfat at the costovertebral junction. At the level where thesympathetic chain crossed the ribs, the parietal pleura wasopened with the diathermic hook. The upper and lower endsof the intended ganglion were completely coagulated bysimple diathermy at the head of the upper and lower ribs, forexample: the fourth and fifth ribs for T4 ganglion. After beingseparated from the surrounding tissue, the sympathetic chainwas gently cauterized and transected completely but theganglion was left in position without removal by manipula-tion. The lung was routinely inflated after the procedure tomake sure that it was well-expanded. No stitches were re-quired for the 5-mm port, whereas 1 or 2 stitches were necessaryfor the 10-mm port. The same procedure was performed on thecontralateral side. Postoperative chest radiography was per-formed routinely.
Data CollectionFirst, case patients were analyzed for their descriptive
variables (age at operation, gender, BMI, and family history)by reviewing the medical charts. Second, at least 1 outpatientclinic was visited routinely within 1 week and the patientimmediate postoperative outcomes were recorded accordingto the medical files. Third, follow-up data (at least 20 monthsfrom the time of surgery) were collected using a standardizedtelephone questionnaire. The visual analog scale (VAS)graded between 0 (none at all) and 10 (worst possible symp-toms and clothes needing to be changed frequently) was usedto represent the sweating pattern. Patient satisfaction aftersympathectomy was also assessed from VAS 0 (extremedissatisfaction) to 10 (excellent satisfaction). The score ofpalmar sweating before sympathectomy was recorded in sum
A (rest and emotional response) (min: 0; max: 20). The scoreof palmar sweating after sympathectomy was also recorded insum B (0–20). The change of sweating pattern before andafter sympathectomy was recorded in sum (A � B). Subjec-tive outcomes included recurrence of palmar hyperhidrosis,presence of gustatory sweating, presence of CS, regions ofCS, severity of CS, palmar overdryness after sympathectomy,and regret after sympathectomy. This questionnaire allowedthe research team to obtain an accurate pattern of postoper-ative sweating and follow-up data.
Statistical AnalysisBefore beginning our analysis, the available literature
was reviewed to identify factors thought to be important inCS and patient’s satisfaction. Student t tests and �2 tests wereused to compare continuous and categorical descriptive vari-ables respectively between enrolled and nonenrolled patients.The differences in enrolled patients were compared across the3 groups of various surgical interventions using analysis ofvariance (ANOVA) for continuous variables and �2 tests forcategorical variables. Further analysis with Scheffe post hoctest was planned when the ANOVA showed that there was astatistical difference between groups. Univariate and multi-variate linear regression analyses were used to examine therelationships between the subjective clinical outcomes anddegree of satisfaction. Linear regression analyses were alsoused to examine the risk factors of severity of CS among thepatients. Using the binary coding, the relationships betweenCS and 3 different levels of sympathectomy were also eval-uated in the linear regression. Potential confounders such aspatient age, gender, BMI, duration of follow-up, and postop-erative outcomes were adjusted in all multivariate analyses.Results were expressed as a mean with standard deviation oreffect and 95% confidence interval where appropriate. A Pvalue of less than 0.05 denoted statistical significance. SPSSfor Windows version 12.0 was used for all statistics.
RESULTS
Descriptive DataResponse rate for the telephone questionnaire was
67.1% (Table 1). The data for 90 patients were not collected.Of these, 68 of them had incorrect phone numbers and 16patients had gone abroad. Six patients who received ETS2refused the telephone interview by reason of recurrence in 3,
TABLE 1. Descriptive Variables in Enrolled Patients
Enrolled Patients (N) ETS2 (86) ETS3 (78) ETS4 (70) P
Age (yr) 20.4 � 4.4* 25.9 � 9.2 23.9 � 8.5 �0.001
Gender (male/N) 0.48 0.41 0.57 0.145
Sum A 14.8 � 3.9 14.6 � 3.6 14.3 � 3.9 0.713
BMI (kg/m2) 20.8 � 2.8 22.0 � 3.7* 20.7 � 2.6 0.013
Follow-up (mo) 60.9 � 15.3† 35.6 � 13.5† 43.1 � 10.3† �0.001
*Significant difference from the 2 other groups.†Significant difference between groups.ETS indicates endoscopic thoracic sympathectomy; sum A, the score of palmar sweating before sympathec-
tomy; BMI, body mass index.
Annals of Surgery • Volume 246, Number 2, August 2007 T4 Sympathectomy for Palmar Hyperhidrosis
© 2007 Lippincott Williams & Wilkins 331

severe CS in 2, and left brachial plexopathy in 1. Of the 244patients, data in 10 patients were incomplete and records of234 patients were enrolled. A comparison of the 234 com-plete follow-up patients with those who were not includedshowed no significant differences in age, gender, and BMI(P � 0.654, 0.430, and 0.217).
Of 234 participating patients, 112 of them (47.9%)were students. A family history was elicited in 113 of 234patients (48.3%). The mean age of enrolled patients was22.3 � 7.2 years and mean BMI was 20.9 � 3.4 kg/m2.Before operation, 26 patients (11.1%) had once tried top-ical antiperspirants as treatment but this did not producesatisfactory results. There were 86 patients of ETS2, 78patients of ETS3, and 70 patients of ETS4 enrolled. Genderand the score of palmar sweating before sympathectomy(sum A) among 3 enrolled groups were comparable (P �0.145 and 0.713). The average age (P � 0.001) and thebody configurations (P � 0.430) of the patients weresimilar clinically, though there were statistically signifi-cant differences among the 3 groups. Mean follow-up was47.1 � 17.2 months.
Short-term OutcomeDuring operation, no patient died or developed Horner
syndrome, no procedures were converted to thoracotomy, andadhesions were found in 3 patients (1.3%). Two hundred andtwenty patients (94.0%) could be discharged within 24 hoursafter the operation. Immediate complications were usuallymild and requiring at most a day or 2 of prolonged hospitalstay. Seventy-six patients (32.5%) had subcutaneous emphy-sema and 33 patients (14.1%) had pneumothorax on fol-low-up x-ray. All of the pneumothorax cases were residual(not because of lung injury) and most of them were generallyreabsorbed spontaneously and needed no further treatment.However, 6 patients (2.6%) required chest tube drainage. Theother complications included 8 patients (3.4%) with pulmo-nary atelectasis, 7 patients (3.0%) with intercostal pain, 2patients (0.9%) with pleural effusions, and 1 patient (0.4%)with hemothorax.
Long-term Follow-upThe length of mean follow-up in ETS2 was 60.9 � 15.3
months, in ETS3 35.6 � 13.5 months, and in ETS4 43.1 �
TABLE 2. Clinical Feature of the Patients With Long-term Follow-up
ETS2 (86) ETS3 (78) ETS4 (70) P
Sum B 2.3 � 3.0* 1.1 � 2.0* 2.1 � 3.1 0.012
Sum (A � B) 12.6 � 5.1 13.5 � 3.8 12.2 � 4.2 0.162
CS (%) 92 92 80† 0.030
Severity of CS 6.3 � 2.8 6.3 � 2.9 3.9 � 2.6† �0.001
Regions of CS 2.1 � 1.3* 2.1 � 1.2 1.6 � 1.2* 0.015
Recurrence (%) 25.6* 7.7* 22.9 0.008
Gustatory sweating (%) 5.8* 23.1* 11.4 0.004
Palmar overdryness (%) 36.0 39.7 8.6† �0.001
Regret after sympathectomy (%) 9.3* 3.8 0* 0.022
Degree of satisfaction 6.3 � 2.5† 7.8 � 1.8 7.9 � 1.8 �0.001
*Significant difference between groups.†Significant difference from the 2 other groups.ETS indicates endoscopic thoracic sympathectomy; sum B, the score of palmar sweating after sympathectomy;
sum (A � B), the difference of palmar sweating before and after operation; CS, compensatory sweating.
FIGURE 1. The schematic drawing showing T4 sympathec-tomy was performed by simple diathermic severance of thesympathetic trunk.
Chang et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins332

10.3 months. The patients with ETS3 had the least degree ofpostoperative sweating in their hands (sum B) (P � 0.012),though the differences of palmar sweating before and afteroperations were comparable among the 3 groups �sum (A �B)� (P � 0.162) (Table 2). Up to 88.5% of the patients mightnotice CS in previously less affected regions of the body.There were usually multiple regions of CS, but group ETS4had less areas involved (P � 0.015). The most commonregion of CS was the back, occurring in 56.3% of ETS2, 75%of ETS3, and 42.9% of ETS4 (Fig. 2). Compared with theback, CS affected less frequently the anterior aspect of thebody and the lower legs. Group ETS4 also had lower inci-dence and lesser severity of CS when compared with theother 2 groups (P � 0.030, and �0.001). Patients (13.2%)may notice increased sweating while smelling or eating spicyfood (gustatory sweating). Of those patients with recurrenceof palmar hyperhidrosis, 22 patients (25.6%) were in group
ETS2, 6 patients (7.7%) in group ETS3, and 16 patients(22.9%) in group ETS4. Sixty-nine patients (29.5%) com-plained about overdryness of their palms, especially groupsETS2 and ETS3 (P � 0.001). Most patients were satisfiedwith the results of surgery, especially in groups ETS3 andETS4 (P � 0.001). Eleven patients (4.7%) regretted thesurgical procedure, especially in group ETS2 (P � 0.022). Nopatient expressed regret in group ETS4.
The results of factors influencing the extent of CS areshown in Table 3. In the univariate analysis, the extent ofCS was directly related to the BMI and regions of CS,while being independent of age, gender, presence of gus-tatory sweating, positive family history, and duration offollow-up. In the multivariate analysis, the severity of CSwas still significantly directly related to the BMI andregions of CS in total patients (� � 0.132, P � 0.021 and� � 0.917, P � 0.001). Group ETS4 presented with a lesserextent of CS than group ETS2 in both univariate and multivariateanalysis (� � �2.409, P � 0.001 and � � �1.537, P � 0.002).The patients with ETS3 were found to have a greater extent ofCS than the patients with ETS2 in univariate analysis (� �1.113, P � 0.007), but this was not significant after additionaladjustment (� � 0.325, P � 0.533).
The results of factors influencing postoperative satis-faction are shown in Table 4. In the univariate analysis, thedegree of satisfaction was directly related to age and thedifference of palmar sweating before and after operation �sum(A � B)�, but was inversely related to the regions of CS, theseverity of CS, the score of palmar sweating after sympathec-tomy (sum B), the duration of follow-up, palmar overdryness,and recurrence of palmar hyperhidrosis. Patient satisfactionwas independent of gender, BMI, presence of gustatorysweating, presence of CS, and positive family history. In themultivariate analysis, the degree of satisfaction in patientswas significantly inversely related to the severity of CS, thescore of palmar sweating after sympathectomy (Sum B),duration of follow-up, and palmar overdryness (� � �0.185,P � 0.002; � � �0.159, P � 0.011; � � �0.025, P � 0.003and � � �1.463, P � 0.001), whereas age, regions of CS, thedifference of palmar sweating before and after operation �sum
FIGURE 2. Regions of compensatory sweating of the 3groups.
TABLE 3. Factors Influencing the Extent of CS Estimated by Univariate and MultivariateLinear Regression
Univariate Regression Multivariate Regression
Effect (95% CI) P Effect (95% CI) P
Age �0.03 (�0.052–0.046) 0.907 �0.016 (�0.060–0.029) 0.495
Gender �0.532 (�1.304–0.239) 0.175 �0.267 (�0.983–0.449) 0.463
BMI 0.137 (0.015–0.260) 0.028 0.132 (0.020–0.244) 0.021
Gustatory sweating 0.862 (�0.275–1.999) 0.137 0.619 (�0.430–0.668) 0.246
Regions of CS 1.083 (0.086–1.360) �0.001 0.917 (0.643–1.190) �0.001
FH 0.574 (�0.198–.345) 0.144 0.247 (�0.447–0.941) 0.484
Duration of Follow-up 0.016 (�0.006–0.038) 0.160 0.018 (�0.008–0.043) 0.174
ETS3 1.113 (0.304–�1.921) 0.007 0.325 (�0.699–1.349) 0.533
ETS4 �2.409 (�3.195–�1.622) �0.001 �1.537 (�2.487–�0.586) 0.002
BMI indicates body mass index; CS, compensatory sweating; FH, family history; ETS, endoscopic thoracic sympathectomy.
Annals of Surgery • Volume 246, Number 2, August 2007 T4 Sympathectomy for Palmar Hyperhidrosis
© 2007 Lippincott Williams & Wilkins 333

(A � B)�, and recurrence were not significant after additionaladjustment (P � 0.382, 0.371, 0.691, and 0.169).
DISCUSSIONETS is currently recognized as the best method of
treatment for palmar hyperhidrosis. However, it is difficult tosay whether the operation is successful or not,11 being totallybased on the patient’s subjective feelings.13 To date, there are2 quality-of-life instruments that examine the physical andpsychologic condition of patients after ETS.1,13 We consid-ered that telephone visits might fail or be incomplete if thequestions asked were excessively long or complex. In thepresent series, these patients were followed up by a simplifiedtelephone questionnaire with VAS under the following is-sues: degree of palmar sweating before and after operation,severity of CS, degree of satisfaction, and regret after opera-tion. Because 84 patients never received the questionnaire be-cause they had emigrated, the actual response rate may becalculated as 93.6%. According to the visiting results, both ETS3and ETS4 could provide comparable satisfaction and were sig-nificantly different from what ETS2 provided (P � 0.001).
In the present study, different levels of sympathectomyall brought about good effects in reducing palmar hyperhi-drosis �sum (A � B), P � 0.162�. However, a large discrep-ancy of satisfaction was noted among patients, and postop-erative complications nearly accounted for all the disparity insatisfaction. The multivariate logistic regression showed thatthe most important variable influencing satisfaction after theoperation was the presence of palmar overdryness (� ��1.463, P � 0.001) (Table 4) and the most importantvariable associated with the severity of CS was the number ofregions of CS (� � 0.917, P � 0.001) (Table 3). In Table 2,the patients with ETS4 had the lowest incidence of CS, theleast regions of CS and their palms were simultaneously theleast suffering from overdryness (P � 0.030, 0.015, and�0.001). None of the patients with ETS4 regretted having the
operation. Compared with ETS3, it seemed that ETS4 forpalmar hyperhidrosis was a more effective approach, whichcould minimize postoperative complications, including pal-mar overdryness, presence of CS, and regions of CS.
Generally, the more sympathetic segments excised, thegreater the incidence of severe compensatory symptoms.2,14
Several authors limited the extent of resections for hyperhi-drosis to a single level to reduce the incidence of severecompensatory symptoms.1–4 However, the correlation be-tween the level of the sympathetic trunk interrupted andseverity of CS was reported (Fig. 1).2,15 Inclusion of the T2lesion results in significantly more severe CS than otherlevels not having T2 removed.2,16 In the present series,different degrees of CS were found after different level ofsympathectomy (P � 0.001). Compared with ETS2, theseverity of CS was directly related to ETS3 (� � 0.325, P �0.533) and significantly inversely related to ETS4 (� ��1.537, P � 0.002) in the multivariate analyses.
Compensatory sweating seems to be a permanent sideeffect and occurred in 88.5% of our patients and the detaileddistribution is shown in Figure 2. The distributions of thepreferential location among the 3 groups were comparable,and back and lower extremities were the common regions.When compared with groups ETS2 and ETS3, group ETS4had less areas involved (P � 0.015). However, the highestincidence in the back and the lowest in the buttock werepresented in group ETS3. Perhaps we should have asked ourpatients more clearly whether their CS occurred in the upper,middle, or lower back. Besides, patients may confuse the area“lower back” or “buttock.” In general, several authors havedescribed that the most common region was the posterioraspect of the trunk.17,18 The authors believe that postopera-tive sweating is “reflex sweating” instead of CS because thepositive feedback mechanism (reflex sweating) of the auto-nomic nervous system is induced by blocked negative feed-back signal (sympathectomy).6 T2 interruption stops negative
TABLE 4. Factors Influencing Postoperative Satisfaction Estimated by Univariate andMultivariate Linear Regression
Univariate Regression Multivariate Regression
Effect (95% CI) P Effect (95% CI) P
Age 0.053 (0.017–0.088) 0.004 0.015 (�0.019–0.049) 0.382
Gender 0.117 (�0.455–0.688) 0.688 0.006 (�0.533–0.544) 0.983
BMI 0.076 (�0.015–0.167) 0.101 0.057 (�0.030–0.144) 0.198
Gustatory sweating 0.141 (�0.702–0.984) 0.742 0.018 (�0.794–0.830) 0.964
Presence of CS �0.842 (�1.730–0.046) 0.063 0.342 (�0.839–1.523) 0.569
Regions of CS �0.241 (�0.468–�0.014) 0.037 �0.120 (�0.384–0.144) 0.371
Severity of CS �0.204 (�0.295–�0.112) �0.001 �0.185 (�0.301–�0.069) 0.002
FH 0.048 (�0.524–0.620) 0.868 0.359 (�0.177–0.895) 0.188
Sum B �0.175 (�0.276–�0.074) 0.001 �0.159 (�0.281–�0.036) 0.011
Sum (A � B) 0.067 (0.003–0.130) 0.040 0.014 (�0.054– 0.082) 0.691
Duration of follow-up �0.038 (�0.054–�0.023) �0.001 �0.025 (�0.042–�0.009) 0.003
Palmar overdryness �1.268 (�1.873–�0.663) �0.001 �1.463 (�2.048–�0.878) �0.001
Recurrence �1.021 (�1.740–�0.302) 0.006 �0.550 (�1.337–0.236) 0.169
BMI indicates body mass index; CS, compensatory sweating; FH, family history; sum B, the score of palmar sweating aftersympathectomy; sum (A � B), the difference of palmar sweating before and after operation.
Chang et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins334

feedback signals from T2 and below and provides the stron-gest positive feedback signal. T3 interruption preserves somenegative feedback signals (from T2) whereas T4 interruptionpreserves more (from T2 and T3). Therefore, the positivefeedback signals are much weaker in T4 interruption than inT2 interruption. The severest form of CS was observed morefrequently in the T2 group than in the T3 group.15,16,19 Thedetailed mechanism of reflex sweating has been described inour previous publication.6
Patient satisfaction would not be affected by the pres-ence of CS or a lot of regions of CS (P � 0.569 and 0.371).The above results illustrated that these patients all have acertain cognition regarding CS, which seems inevitable.However, the degree of satisfaction would drop if the degreeof CS was too serious (� � �0.185, P � 0.002). Panhoferet al1 also reported that the quality of life in patients whodeveloped severe CS was worse than before surgery. There-fore, those patients should be excluded from surgery if riskfactors could be identified for the development of CS. Be-cause the triggering factors of hyperhidrosis are emotion andanxiety rather than a hot environment,20 obesity was not arisk factor of presence of CS (BMI �24 vs. �24 kg/m2; oddsratio 2.28; 95% confidence interval (CI), 0.52–10.14; P �0.276). However, CS was actually more serious in obeseindividuals (� � 0.132, P � 0.021) although no statisticallysignificant association was found between BMI and the de-gree of satisfaction (P � 0.198). The same results weredescribed by de Campos et al.19 That is to say, when facinga broader-in-stature patient who seeks surgery for palmarperspiration, the surgeon must inform him/her that the degreeof CS after operation might be more serious than that of theaverage person.
Thirty-six percent of patients with ETS2 felt overdry-ness in their hands whereas only 8.6% of the patients withETS4 felt the same (P � 0.001). In the multivariate analysis,the degree of satisfaction may be significantly lower whentheir palms were quite dry (� � �1.463, P � 0.001). On thecontrary, group ETS4 usually had satisfyingly mildly moistrather than fissured palms. We believe that the nerves tosweat glands of the hands center on the upper part of thesympathetic trunk although the routes may originate fromT2 to T10. That is to say, the more uppermost the ganglioninterrupted, the drier the palms present. Much drier handsshould be observed in the T2 group than those of the T3
group theoretically. However, the least degree of postop-erative palmar sweating was presented in group ETS3.Because the incidence of recurrence may increase withtime no matter which level was transected,8,21 the differ-ences in the follow-up period among the 3 groups inter-fered in the analysis of the outcomes. The shortest durationof follow-up in group ETS3 accounted for the preponder-ance of the least degree of palmar sweating and the lowestrecurrence after sympathectomy.
We did not specifically ask our patients whether theirCS had improved during long-term follow-up, but their sat-isfaction decayed gradually with time (� � �0.025, P �0.003). Patient satisfaction is not only related to the result(reduction of palmar sweating), but also to patient tolerance
to complications (recurrence, palmar overdryness, and CS).Once the euphoria over improvement in their hyperhidrosisdissipates, the patient’s unsatisfied perception about postop-erative side effects will be amplified.
Several authors have described greater prevalence ofpalmar hyperhidrosis among women than men,1,2,8,13,17 andthe present study showed a balance between men and women.However, the conclusion of the present series is still appro-priate for the general population because the outcome factorssuch as the severity of CS and degree of satisfaction wereunrelated to gender in the multivariate analyses (P � 0.463and 0.983). Other predictive factors such as age, familyhistory, and presence of gustatory sweating were also studied;no relationships to the severity of CS and degree of satisfac-tion were found. Considering the limitations of a retrospec-tive study such as ours, we strongly advocate the organizationof a randomized prospective trial and quality-of-life protocolson this topic because ETS4 was a viable option in our presentseries and past studies.1,6,10–12
CONCLUSIONSWe consider that T4 level is now the level most
indicated for treating palmar hyperhidrosis. When com-pared with ETS2 and ETS3, ETS4 serves the purpose insolving excessive palmar sweating. Furthermore, ETS4reduces the occurrence and severity of CS, provides mildlymoist rather than fissured palms, minimizes regret after theoperation, and results in general satisfaction about qualityof life. Meanwhile, palmar overdryness was an importantfactor that affects the degree of satisfaction after sympa-thectomy. There was no association between obesity andpresence of CS; however, obese individuals who arescheduled for sympathectomy should be informed of thelikelihood of increased severity of CS. Patient satisfactionmight decrease gradually as time goes on no matter whichlevel of sympathetic ganglion was transected.
ACKNOWLEDGMENTSThe authors thank the Statistical Analysis Laboratory,
Department of Clinical Research, Kaohsiung Medical Uni-versity Hospital for their help.
REFERENCES1. Panhofer P, Zacherl J, Jakesz R, et al. Improved quality of life after
sympathetic block for upper limb hyperhidrosis. Br J Surg. 2006;93:582–586.
2. Dewey TM, Herbert MA, Hill SL, et al. One-year follow-up afterthoracoscopic sympathectomy for hyperhidrosis: outcomes and conse-quences. Ann Thorac Surg. 2006;81:1227–1232.
3. Yoon SH, Rim DC. The selective T3 sympathicotomy in patients withessential palmar hyperhidrosis. Acta Neurochir (Wien). 2003;145:467–471.
4. Yoon DH, Ha Y, Park YG, et al. Thoracoscopic limited T-3 sympathi-cotomy for primary hyperhidrosis: prevention for compensatory hyper-hidrosis. J Neurosurg. 2003;99(1 suppl):39–43.
5. Lin CC, Telaranta T. Lin-Telaranta classification: the importance ofdifferent procedures for different indications in sympathetic surgery.Ann Chir Gynaecol. 2001;90:161–166.
6. Chou SH, Kao EL, Lin CC, et al. The importance of classification insympathetic surgery and a proposed mechanism for compensatory hyper-hidrosis: experience with 464 cases. Surg Endosc. 2006;20:1749–1753.
Annals of Surgery • Volume 246, Number 2, August 2007 T4 Sympathectomy for Palmar Hyperhidrosis
© 2007 Lippincott Williams & Wilkins 335

7. Arnold WS, Daniel TM. Thoracoscopic sympathectomy. In: ShieldsTW, LoCicero J III, Ponn RB, et al, eds. General Thoracic Surgery.Philadelphia: Lippincott Williams and Wilkins; 2005;698–702.
8. Chiou TS, Chen SC. Intermediate-term results of endoscopic transaxil-lary T2 sympathectomy for primary palmar hyperhidrosis. Br J Surg.1999;86:45–47.
9. Chou SH, Lee SH, Kao EL. Thoracic endoscopic T2–T3 sympathectomyin palmar hyperhidrosis: experience of 112 cases. Surg Today. 1993;23:105–107.
10. Chou SH, Kao EL, Li HP, et al. T4 sympathectomy for palmar hyper-hidrosis: an effective approach that simultaneously minimizes compen-satory hyperhidrosis. Kaohsiung J Med Sci. 2005;21:310–313.
11. Neumayer C, Zacherl J, Holak G, et al. Limited endoscopic thoracicsympathetic block for hyperhidrosis of the upper limb: reduction ofcompensatory sweating by clipping T4. Surg Endosc. 2004;18:152–156.
12. Choi BC, Lee YC, Sim SB. Treatment of palmar hyperhidrosis byendoscopic clipping of the upper part of the T4 sympathetic ganglion.Preliminary results. Clin Auton Res. 2003;13:S48–S51.
13. de Campos JR, Kauffman P, Werebe Ede C, et al. Quality of life, beforeand after thoracic sympathectomy: report on 378 operated patients. AnnThorac Surg. 2003;76:886–891.
14. Licht PB, Pilegaard HK. Gustatory side effects after thoracoscopicsympathectomy. Ann Thorac Surg. 2006;81:1043–1047.
15. Reisfeld R. Sympathectomy for hyperhidrosis: should we place theclamps at T2–T3 or T3–T4? Clin Auton Res. 2006;16:384–389.
16. Yazbek G, Wolosker N, de Campos JR, et al. Palmar hyperhidrosis—which is the best level of denervation using video-assisted thoraco-scopic sympathectomy: T2 or T3 ganglion? J Vasc Surg. 2005;42:281–285.
17. Dumont P, Denoyer A, Robin P. Long-term results of thoracoscopicsympathectomy for hyperhidrosis. Ann Thorac Surg. 2004;78:1801–1807.
18. Adar R, Kurchin A, Zweig A, et al. Palmar hyperhidrosis and its surgicaltreatment: a report of 100 cases. Ann Surg. 1977;186:34–41.
19. de Campos JR, Wolosker N, Takeda FR, et al. The body mass index andlevel of resection: predictive factors for compensatory sweating aftersympathectomy. Clin Auton Res. 2005;15:116–120.
20. Vetrugno R, Liguori R, Cortelli P, et al. Sympathetic skin response—basic mechanisms and clinical applications. Clin Auton Res. 2006;13:256–270.
21. Reisfeld R, Nguyen R, Pnini A. Endoscopic thoracic sympathectomy forhyperhidrosis: experience with both cauterization and clamping meth-ods. Surg Laparosc Endosc Percutan Tech. 2002;12:255–267.
Chang et al Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins336

BOOK REVIEWS
Multiorgan Resections forCancer, Advanced SurgicalTechniques
Marco P. Merlini and Ronald F.Martin; New York, Thieme VerlagPublishing, 196 pages (US $190)
Multiorgan Resection for Cancer, Ad-vanced Surgical Techniques covers animpressive array of surgical oncologyprocedures at the extremes of cura-tive surgery. The operative procedures(technical steps) are presented in alogical stepwise fashion. Tumor biol-ogy, extent of disease (local and met-astatic), and signs of unresectabilityare addressed. The indications andcontraindications, and surgical pitfallsare addressed for each surgical inter-vention. Each topic is logically andsystematically approached: preopera-tive evaluation, surgical positioning,operative technique complications andresults.
This text is written for a surgicalaudience with special interest in ab-dominal oncology. Surgeons in train-ing (residents and fellows) and prac-ticing surgeons will find the texthelpful. Each chapter provides lessonslearned from experience with a spe-cific emphasis on anatomy and tech-nique. The editors have compiled an
extensive list of surgical topics, whichinclude upper and lower gastrointesti-nal tracts, pelvic, retroperitoneal, andperitoneal diseases. Color illustrationsare numerous but vary in educationalvalue and quality.
This is not a standard “how to”book and should be read with some cau-tion. Some topics addressed are clearlycontroversial and unproven. Some proce-dures are best performed by experiencedteams at high-volume hospitals. The bestaspect of this text is its ability to present abalanced view of heroic surgical tech-niques with the natural history of the dis-ease or tumor biology.
Neal Wilkinson, MDIowa City, IA
Current Therapy in Colonand Rectal Surgery, 2nd ed.
Victor W. Fazio, James M. Church,and Conor P. Delaney; St. Louis,Mosby, Inc., 612 pages (US $160)
This authoritative textbook is a majorrevision of the first edition (published in1990) and includes the many contribu-tions made in the field of colorectalsurgery during the past 2 decades. Over100 nationally and internationally rec-ognized experts authored the 95 chap-ters using a clear and consistent format
that packages even the most complextopics into reader-friendly, logical mod-ules. The detailed management algo-rithms and quality illustrations through-out the book greatly augment the text.Although not exhaustive in its breadth,the text more than adequately coversall of the clinical topics relevant to thefield today.
Colorectal surgeons and generalsurgeons will find that Current Therapydelivers material in a concise and artic-ulate fashion without sacrificing content.The focus on the practical aspects of thefield of colorectal surgery distinguishesthis book from other recent colorectaltexts. This may be best illustrated by thesection dedicated to complications andother miscellaneous topics, which manyreaders will find invaluable.
Current Therapy provides a refresh-ing, comprehensive (yet not overwhelm-ing) practical guide to the management ofcolorectal surgery patients that many prac-ticing surgeons will appreciate and finduseful on a daily basis. In addition, sur-geons at any point in their training willfind this text most helpful in terms of itsscope, readability, and focus on the clini-cal management of the spectrum of colo-rectal diseases.
Daniel L. Feingold, MDNew York, New York
Annals of Surgery • Volume 246, Number 2, August 2007 337

LETTERS TO THE EDITOR
Hormone ReceptorStatus as a Prognostic
Factor in Breast CancerPatients With HepaticMetastases Treated by
Liver Resection
To the Editor:
We read with great interest the arti-cle by Adam et al1 regarding liver
resection for patients with hepatic me-tastases from breast cancer. Authorsfound that failure to respond to preoper-ative chemotherapy, a R2 resection, andthe absence of repeat hepatectomy wereindependently associated with poorersurvival. However, they did not mentionhormone receptor status of the patients,which might have an effect on the sur-vival rate. In their analysis, estrogen(ER) positive and progesterone (PR)positive patients had a longer survivalthan ER negative and PR negative pa-tients (median survival, 50 and 87 monthsfor ER and PR positive patients, respec-tively, and 27 and 29 months for ER andPR negative patients, respectively). Al-though these results were not implicatinghormone receptor status as an independentvariable, there is a trend for hormone re-ceptor patients to have a longer survival.Moreover, Elias et al2 in their study eval-uated 54 breast cancer patients with livermetastases as the sole site of metastaticdisease (except for bone metastases in 3patients) who underwent hepatectomy.They showed that the only factor influenc-ing survival in both the univariate andmultivariate analyses was the hormone re-ceptor status (P � 0.03), and the relativerisk of death was found to be increased by3.5-fold when hormone receptor was neg-ative. Given the information above, hor-mone receptor status of breast cancer pa-tients with hepatic metastases may also beconsidered for the selection of patientswho are candidates for liver resection.
Tugrul Purnak, MDDepartment of Internal Medicine
Hacettepe University Faculty of MedicineAnkara, Turkey
Kadri Altundag, MDDepartment of Medical Oncology
Hacettepe University Faculty of MedicineAnkara, Turkey
REFERENCES1. Adam R, Aloia T, Krissat J, et al. Is liver
resection justified for patients with hepatic me-tastases from breast cancer? Ann Surg. 2006;244:897–908.
2. Elias D, Maisonnette F, Druet-Cabanac M, etal. An attempt to clarify indications for hep-atectomy for liver metastases from breastcancer. Am J Surg. 2003;185:158 –164.
Reply:
We appreciate Dr. Purnak’s and Dr.Altundag’s comments regarding
our recent publication in the Annals ofSurgery. The authors correctly note thathormone receptor status is an importantprognostic indicator in patients with lo-calized breast cancer, that our statisticalanalysis showed a trend toward a sur-vival advantage in receptor positive pa-tients undergoing resection of hepaticmetastases, and that Elias et al found astrong association between hormone re-ceptor status and survival after hepaticresection of breast cancer liver metasta-ses. The statistical strength differencesfor this variable between our study andDr. Elias’ study may be due to differ-ences in the number of patients analyzed(54 vs. 85 patients) and differences inpatient selection/characteristics.
On the basis of our analysis, how-ever, we would disagree that patient se-lection for hepatic resection of breastcancer liver metastases should be basedsolely on the hormone receptor status.Although this factor should be used tocounsel patients regarding the postoper-ative prognosis and need for postopera-tive systemic therapy and close surveil-lance, if a breast cancer patient hasresectable intrahepatic disease, con-trolled extrahepatic disease, and a favor-able response to preoperative systemictherapy, we would strongly advocate forsurgical therapy regardless of hormonereceptor status.
In summary, we would agree toconsider hormonal receptor status as afavorable prognostic factor when posi-tive but not as a contraindication to liversurgery when negative.
Rene Adam, MD, PhDThomas Aloia, MDPaul Brousse Hospital
Villejuif, [email protected]
Impact of LaparoscopicResection for Colorectal
Cancer on OperativeOutcomes and Survival
To the Editor:
I would like to congratulate Dr. Lawand colleagues for their recent study
reporting their experience with laparo-scopic colectomies.1 This study is justone of their many fine contributions tothe field of colorectal surgery. Two mainconclusions can be drawn from theirstudy, ie, laparoscopic colectomy resultsin shorter postoperative convalescenceand more controversially, laparoscopy isassociated with improved short-term sur-vival compared with open surgery.
The findings of Law et al thatlaparoscopically treated patients whohave significantly earlier return ofbowel function, earlier resumption ofdiet, and shorter hospitalization aresupported by several randomized con-trolled trials (RCTs)2–4 and hence seemirrefutable. However, one must still re-main cautious when interpreting these re-sults because it is important to note thatnone of these studies were double-blinded.Hence, biases resulting from patient andsurgeon attitudes and practices remain.The influence of laparoscopic surgery onimproved outcomes in unblinded patientsmay be akin to the “placebo” effect,whereby patients are more motivated afterwhat they perceive as having undergone amore minor “key hole” surgery. Un-blinded surgeons may also contribute tothe improved postoperative outcomes be-cause surgeons may adopt more aggres-sive attitudes towards early feeding anddischarge after laparoscopy. This bias isevident in Table 3 of the study,1 wherebyit can be observed that although the min-imum time to pass first flatus or first bowelmotion was 0 days in the open group, theminimum time to first fluid or solid intakewas 1 and 2 days, respectively. Con-
Annals of Surgery • Volume 246, Number 2, August 2007338

versely in the laparoscopic group, al-though the minimum time to pass firstflatus or first bowel motion was 1 day, theminimum time to first fluid or solid intakewas 0 days. The authors also observed thatthere was a trend towards a shorter post-operative convalescence over the 2 timeperiods in patients undergoing open sur-gery, which provides indirect evidencethat the managing surgeons’ attitudes andpractices can have an important influenceon postoperative outcome.
The second conclusion drawn bythe authors was that laparoscopy wasassociated with an improved 3-yearoverall survival compared with opensurgery. This result, although compati-ble with the results from the RCT byLacy et al,4 is not supported by the otherRCTs,2,3 and the explanation for this isunclear. Although the authors suggestedthat favorable immunologic factors mayexplain the difference, several other rea-sons may account for their observations.First, selection bias is likely to be amajor source of bias in their nonran-domized study. Although not statisti-cally significant, it can be observed thatpatients in the laparoscopic group hadsmaller tumors, lower stage, and lowerAmerican Association of Anaesthetists(ASA) score status, compared with pa-tients in the open group. These factors asa whole are likely to contribute to theimproved short-term survival in the lapa-roscopic group. Furthermore, the higherpostoperative mortality observed in theopen group is another potential contribut-ing factor to the decreased 3-year surviv-als observed in the open group. Wereoperative deaths censored or included asevents in their calculation of actuarialsurvivals?
Finally, the duration of follow-upof patients is an important factor whenpredicting survivals via the Kaplan–Meier method. The observed improvedsurvival in the laparoscopic group couldbe secondary to the shorter follow-up inthis group compared with that in theopen group. Although the analysis wasconfined to the period between June 2000and December 2004, it is possible thatmost of the laparoscopic cases were per-formed in the latter part of the study com-pared with the open group, and hence hada shorter follow-up. Thus, it is important
for us to know the mean and medianfollow-up times of the laparoscopic versusthe open group, which was not reported inthe study. From my observation of thesurvival curves in the study (Figs. 1–4),1 itwould certainly seem that patients inthe laparoscopic group had shorter fol-low-up. For example in Figure 4, thelatest time for an “event” (death in thiscase) to occur in the survival curvewas 36 months in the laparoscopicgroup and no “event” occurred afterthis. Contrastingly in the open group,multiple “events” occurred between 36and 48 months suggesting that patientsin this group had longer follow-up.
Brian K. P. Goh, MBBS,MRCS, MMed
Department of SurgerySingapore General Hospital
REFERENCES1. Law WL, Lee YM, Choi HK, Seto CL, Ho JW.
Impact of laparoscopic resection for colorectalcancer on operative outcomes and survival.Ann Surg. 2007;245:1–7.
2. Nelson H, Sargent DJ, COST Study Group. Acomparison laparoscopic assisted and open co-lectomy for colon cancer. N Engl J Med. 2004;350:2050–2059.
3. Guilloi PJ, Quirke P, Thorpe H, et al. Short-termendpoints of conventional versus laparoscopi-cally-assisted surgery in patients with colorectalcancer (MRC CLASSICC trial): multicentre, ran-domised controlled trial. Lancet. 2005;365:1718–1726.
4. Lacy AM, Garcia-Valdecasas JC, Delgado S,et al. Laparoscopy-assisted colectomy versusopen colectomy for treatment of non-metastaticcolon cancer: a randomised trial. Lancet. 2002;359:2224–2229.
Reply:
We appreciate Dr. Goh’s interest inour article1 and his concern re-
garding our interpretation of the resultswas well considered. We reported theresults and the impact of adopting lapa-roscopic colectomy in patients withcolorectal malignancy in a high volumecenter over a 9-year period. We foundthat laparoscopic resection was associ-ated with better short-term outcomes interms of shorter duration of ileus, earlierresumption of feeding, and shorter hos-pital stay. Admittedly, the study was nota randomized trial and standardizedperioperative care was not implementedduring the study period. Biases in the
postoperative management were un-avoidable. However, in the second pe-riod of the study, the postoperativemanagement, both in the open and lapa-roscopic groups, aimed at early feedingand early mobilization. The resumptionof diet was based on the clinical judg-ment of the surgeons and was not de-layed until the passage of flatus or bowelmovement. The minimum time to startdiet for patients in the open group onday 1 would just demonstrate that thegeneral wellbeing of the patients did notallow them to tolerate oral diet intake inday 0. The demonstration of improve-ment in short-term outcomes was actu-ally compatible with the results of mostof the published randomized controlledtrials,2,3 in which the perioperative man-agement was also based on the sur-geons’ judgment and was not in theform of a standardized recovery pro-gram. Recent studies showed improvedshort-term outcome with the applicationof enhanced recovery program in bothopen and laparoscopic colectomy.4–6
Published results from randomized stud-ies, which compared laparoscopic withopen with standardized postoperative,were not conclusive. Basse et al did notshow any difference between laparo-scopic and open resection in patientswith the enhanced recovery program,7
whereas King et al showed improvedshort-term outcome in patients who un-derwent laparoscopic surgery.8 How-ever, in both studies, the number ofpatients was small. Large-scale random-ized trials to compare the surgical ap-proaches with a standardized postopera-tive program are certainly necessary toavoid the bias of the surgeons in thepostoperative management.
Concerning Dr. Goh’s commentson our results on survival, we would liketo clarify that in the analysis of survival,patients who died in the postoperativeperiod (30 days) were excluded. Thestage, size, and the ASA status were notstatistically significant when the 2groups were compared. In the analysisof survival, we also stratified accordingto the stage and the results were shownin Figures 2–4 in the article. The bettersurvival in stage III patients (althoughnot statistically significant) was compat-ible with Lacy et al’s results.3 Actually,better survival in patients with node pos-
Annals of Surgery • Volume 246, Number 2, August 2007 Letters to the Editor
© 2007 Lippincott Williams & Wilkins 339

itive disease was also shown in the studyby Capussotti et al.9 Concerning the me-dian follow-up of the 2 groups of pa-tients, in contrary to what Dr. Gohthought, the median follow-up periodfor the laparoscopic group is actuallylonger than that for open surgery. Wecompared the 2 groups of patients withKaplan–Meier method and log-rank test,which is the recommended method forcomparison of survival in patients withdifferent duration of follow-up.
Wai Lun LAW, MS, FRCS (Edin.),FACS
Department of SurgeryUniversity of Hong Kong Medical Centre
Queen Mary HospitalHong Kong
REFERENCES1. Law WL, Lee YM, Choi HK, et al. Impact of
laparoscopic resection for colorectal cancer onoperative outcomes and survival. Ann Surg.2007;245:1–7.
2. The Clinical Outcomes of Surgical TherapyStudy Group. A comparison of laparoscopi-cally assisted and open colectomy for coloncancer. N Engl J Med. 2004;350:2050–2059.
3. Lacy AM, Garcia-Valdecasas JC, Delgado S, etal. Laparoscopy-assisted colectomy versusopen colectomy for treatment of non-metastaticcolon cancer: a randomised trial. Lancet. 2002;359:2224–2229.
4. Basse L, Hjort JD, Billesbolle P, et al. Aclinical pathway to accelerate recovery aftercolonic resection. Ann Surg. 2000;232:51–57.
5. Delaney CP, Zutshi M, Senagore AJ, et al.Prospective, randomized, controlled trial be-tween a pathway of controlled rehabilitationwith early ambulation and diet and traditionalpostoperative care after laparotomy and intes-tinal resection. Dis Colon Rectum. 2003;46:851–859.
6. Raue W, Haase O, Junghans T, et al.‘Fast-track’ multimodal rehabilitation programimproves outcome after laparoscopic sigmoid-ectomy: a controlled prospective evaluation.Surg Endosc. 2004;18:1463–1468.
7. Basse L, Jakobsen DH, Bardram L, et al.Functional recovery after open versus laparo-scopic colonic resection: a randomized, blindedstudy. Ann Surg. 2005;241:416–423.
8. King PM, Blazeby JM, Ewings P, et al.Randomized clinical trial comparing laparo-scopic and open surgery for colorectal cancerwithin an enhanced recovery programme.Br J Surg. 2006;93:300–308.
9. Capussotti L, Massucco P, Muratore A, et al.Laparoscopy as a prognostic factor in curativeresection for node positive colorectal cancer:results for a single-institution nonrandomizedprospective trial. Surg Endosc. 2004;18:1130–1135.
Steatosis as a RiskFactor in Liver Surgery
To the Editor:
We read with interest the article byVetelainen et al entitled “Steato-
sis as a Risk Factor in Liver Surgery”in the January 2007 issue of Annals ofSurgery.1 We agree with the authorsthat the full impact of hepatic steatosison outcomes after liver surgery is onlybeginning to be understood. However,recent data have clearly delineated asubset of patients in whom steatosismay be most relevant—those with ste-atohepatitis, who are at increased riskfor liver failure and death after majorliver resection.
Slow progress in understandingthe impact of steatosis on outcomes aftermajor liver surgery may be related inpart to a failure to distinguish betweensteatohepatitis and uncomplicated ste-atosis (without significant inflammationand other changes). Although it is in-creasingly clear that uncomplicated ste-atosis may be associated with morebleeding during parenchymal transec-tion2 and more posthepatectomy compli-cations, including infections,3 steatosishas not been associated with a signifi-cant increase in mortality.4 In contrast,however, several authors have recentlyshown that patients with steatohepatitismay be at higher risk for liver failureand death after major hepatectomy.5,6
A clear understanding of the dif-ference between steatosis and steato-hepatitis was recently provided in a sim-ple, objective pathologic grading systemfor steatohepatitis proposed by Kleineret al for the Nonalcoholic Steatohepati-tis Clinical Research Network.7 The“Kleiner score” provides a reproduciblemeans of evaluating liver specimens fornonalcoholic fatty liver disease and isbased on 3 simple, objective factorsscored on standard hematoxylin and eo-sin-stained liver parenchyma: percent-age parenchymal involvement by steato-sis, degree of lobular inflammation, anddegree of ballooning of hepatocytes.
An important element of this scor-ing system is that disease can be classi-fied as severe steatohepatitis even ifthere is only a minor degree of steatosis.Furthermore, the score is clinically rel-
evant. We recently analyzed outcomeafter hepatectomy for colorectal livermetastases in 406 patients whose re-sected liver parenchyma was subjectedto systematic pathologic analysis.6 Wedemonstrated that patients with steato-hepatitis (Kleiner score �4) had a sig-nificantly higher 90-day posthepatec-tomy mortality rate than did patientswho did not have steatohepatitis (14.7%vs. 1.6%; odds ratio 10.5; P � 0.001).Whether the risk associated with steato-hepatitis relates to failure of the steato-hepatitic liver to regenerate after hepa-tectomy is unclear, but Vetelainen et al’sobservation that adenosine triphosphate(ATP) storage is impaired in patientswith obesity-related steatohepatitis mayprovide a basis for this hypothesis.
Among the spectrum of drug-in-duced hepatic injuries, steatohepatitis is adistinct subtype. The study from our groupalso analyzed the pathologic changes inthe nontumorous liver associated withspecific chemotherapy regimens.6 No spe-cific chemotherapy regimen was associ-ated with steatosis when steatohepatitiswas excluded. However, treatment withirinotecan was associated with the devel-opment of steatohepatitis whereas treat-ment with other agents (5-fluorouracilalone or oxaliplatin) was not. Further-more, oxaliplatin was associated withsinusoidal injury, not steatosis or steato-hepatitis, and resection in patients withsinusoidal injury was not associated withan increase in mortality—a finding subse-quently confirmed by others.8
Uncomplicated steatosis is a com-mon finding in resected liver paren-chyma but appears not to be associatedwith a major risk of death after hepatec-tomy. In contrast, steatohepatitis is as-sociated with an increased risk of liverfailure and death after hepatectomy.Further understanding of the influenceof various histopathologic liver changeson outcome after hepatectomy will re-quire careful evaluation of the liver us-ing standardized pathologic assessment.Collective reference to liver injuries as“steatosis” or “chemotherapy related”must be viewed as an oversimplificationof a complex spectrum of injuries thatincludes simple steatosis, steatohepati-tis, sinusoidal injury, and combinationsof these and other injuries, particularly
Letters to the Editor Annals of Surgery • Volume 246, Number 2, August 2007
© 2007 Lippincott Williams & Wilkins340

in light of data indicating agent-specificinjuries that portend different outcomes.
Eddie K. Abdalla, MDJean-Nicolas Vauthey, MD
Department of Surgical OncologyThe University of Texas M. D. Anderson
Cancer CenterHouston, Texas
REFERENCES1. Vetelainen R, van Vliet A, Gouma DJ, van
Gulik TM. Steatosis as a risk factor in liversurgery. Ann Surg. 2007;245:20–30.
2. Behrns KE, Tsiotos GG, DeSouza NF, et al.Hepatic steatosis as a potential risk factor formajor hepatic resection. J Gastrointest Surg.1998;2:292–298.
3. Belghiti J, Hiramatsu K, Benoist S, et al. Sevenhundred forty-seven hepatectomies in the1990s: an update to evaluate the actual riskof liver resection. J Am Coll Surg. 2000;191:38–46.
4. Kooby DA, Fong Y, Suriawinata A, et al. Impactof steatosis on perioperative outcome followinghepatic resection. J Gastrointest Surg. 2003;7:1034–1044.
5. Fernandez FG, Ritter J, Goodwin JW, et al.Effect of steatohepatitis associated with irino-tecan or oxaliplatin pretreatment on resectabil-ity of hepatic colorectal metastases. J Am CollSurg. 2005;200:845–853.
6. Vauthey JN, Pawlik TM, Ribero D, et al.
Chemotherapy regimen predicts steatohepatitisand an increase in 90-day mortality after sur-gery for hepatic colorectal metastases. J ClinOncol. 2006;24:2065–2072.
7. Kleiner DE, Brunt EM, Van Natta M, et al.Design and validation of a histological scoringsystem for nonalcoholic fatty liver disease.Hepatology. 2005;41:1313–1321.
8. Aloia T, Sebagh M, Plasse M, et al. Liverhistology and surgical outcomes after preoper-ative chemotherapy with fluorouracil plus ox-aliplatin in colorectal cancer liver metastases.J Clin Oncol. 2006;24:4983–4990.
Reply:
We thank Dr. Abdalla and Dr. Vau-they for their interesting com-
ments. The spectrum of liver injury as-sociated with nonalcoholic fatty livers isindeed complex and requires more de-tailed discussion. The “Kleiner score” isan important step forward in classifyingsteatohepatitis, which is unequivocallyassociated with an increased risk of post-hepatectomy liver failure. Althoughsteatotis per se has not been identified asa major risk factor for mortality afterliver resection, it was an independentpredictor of postoperative complicationsin several studies.1 Also, in a model ofmild steatosis in the rat, we showedincreased hepatocellular damage and
impaired functional recovery after 70%liver resection.2 These findings suggestthat steatosis, even in the absence of in-flammatory and fibrotic changes, poten-tially gives rise to parenchymal injury inthe regenerating liver, which is likely dueto mitochondrial dysfunction. We still be-lieve, therefore, that caution is justifiedwhen assessing patients with uncompli-cated steatosis for major liver resection.Our understanding of the risks of liversteatosis is rapidly evolving, and we ap-preciate the important contributions of Dr.Abdalla and Dr. Vauthey in this field.
Thomas M. van Gulik, MDReeta Vetelaınen, MDAcademic Medical Center
Amsterdam, The [email protected]
REFERENCES1. McCormack L, Petrowsky H, Jochum W, et al.
Hepatic steatosis is a risk factor for postopera-tive complications after major hepatectomy: amatched case-control study. Ann Surg. 2007;245(6):923–930.
2. Vetelainen R, Bennink RJ, van Vliet AK,et al. Mild steatosis impairs functional recov-ery after liver resection in an experimentalmodel. Br J Surg. 2007 May 11; �Epub aheadof print�.
Annals of Surgery • Volume 246, Number 2, August 2007 Letters to the Editor
© 2007 Lippincott Williams & Wilkins 341




















