Conservative Christianity, Partnership, Hormones and Sex in ...
40
Conservative Christianity, Partnership, Hormones and Sex in Late Life. Aniruddha Das, Ph.D. 1,2 Stephanie Nairn, M.A. 1 1 Department of Sociology, McGill University, Montreal, Quebec, Canada. 2 To whom correspondence should be addressed at Department of Sociology, McGill University, Montreal, Quebec H3A 2T7, Canada. Correspondence and galley proofs: Aniruddha Das Assistant Professor, Department of Sociology McGill University Room 712, Leacock Building, 855 Sherbrooke Street West Montreal, Quebec H3A 2T7, Canada E-mail: [email protected] Tel.: 514-398-4582 Fax: 514-398-3403
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Conservative Christianity, Partnership, Hormones and Sex in ...
Conservative Christianity, Partnership, Hormones and Sex in Late Life. Aniruddha Das, Ph.D.1,2 Stephanie Nairn, M.A.1
1Department of Sociology, McGill University, Montreal, Quebec, Canada. 2To whom correspondence should be addressed at Department of Sociology, McGill University, Montreal, Quebec H3A 2T7, Canada. Correspondence and galley proofs: Aniruddha Das Assistant Professor, Department of Sociology McGill University Room 712, Leacock Building, 855 Sherbrooke Street West Montreal, Quebec H3A 2T7, Canada E-mail: [email protected] Tel.: 514-398-4582 Fax: 514-398-3403
2
ABSTRACT
Using nationally representative data from the 2005-2006 U.S. National Social Life, Health, and
Aging Project (NSHAP), this study queried relationship, sexual, and sex hormone patterns
among married evangelical women and men aged 57 to 85, relative to those in other religions.
Results suggested that despite potentially more unequal gender roles, evangelical older women
may have better marital quality—perhaps due to the recent transformation of their male
counterparts into authoritative-yet-supportive “soft patriarchs”. Correspondingly, these women—
especially those with greater subjective religiosity, or more support from a spouse—reported
consistently better sexual outcomes than their counterparts in other religions. In addition, they
also had lower estradiol—whether due to psychobiological effects of their better relationships, or
self-selection of those with differential hormone levels into particular partnership patterns. While
older men in these communities also experienced more satisfactory marriages, and had lower
androgens (testosterone, DHEA), their relational assets were less uniformly matched by better
sexual outcomes—perhaps reflecting a gender disparity in the linkage between these factors.
KEY WORDS: evangelicals; older adults; marital quality; sexual outcomes; sex hormones;
NSHAP.
3
INTRODUCTION
Recent studies suggest that despite patriarchal gender roles, marital quality may be higher
among conservative Christians (evangelicals) than other religious groups—partly due to more
supportive behavior from one’s spouse (Bartowski, 2001; Wilcox, 2004, 2006; Wilcox & Nock,
2006; Wilcox & Wolfinger, 2007, 2008; Wolfinger & Wilcox, 2008). This is particularly true
among women, whose happiness in the marriage seems more strongly affected than men’s by a
partner’s support and emotional availability (England & Farkas, 1986; Erickson, 1993; Maccoby,
1998; Nock, 2001; Sayer & Bianchi, 2000; Thompson & Walker, 1989; Wilkie, Ferree, &
Ratcliff, 1998). A separate literature links relationship satisfaction to greater sexual desire,
activity, and pleasure—with this association again potentially stronger among women than men
(Avis et al., 2005; Basson, 2008; Dennerstein, Dudley, & Burger, 2001; Dunn, Croft, & Hackett,
1999; Meston & Buss, 2007). This may be especially true at older ages, when intimacy and trust
can help in the maintenance of satisfactory sex in the presence of age-related frailties (Das,
Laumann, & Waite, 2012). Finally, recent biomedical studies indicate associations of these
partnership patterns with sex-hormone levels—suggesting unexplored differentials in the latter
across religious groups.
Despite these potential linkages, there have been few empirical and no nationally
representative analyses of relationship and especially sexual outcomes among evangelical older
adults. Using data from the 2005-2006 National Social Life, Health, and Aging Project
(NSHAP)—a national probability sample of U.S. adults aged 57 to 85—the present study begins
to fill these gaps. In addition to providing baseline data on a range of sexual, hormonal, and
partnership differentials among married evangelical women and men in late life, relative to those
4
in other religions, it examined variations in these patterns by subjective religiosity, and by a
partner’s support.
Christian Conservatism and Marital Quality
Two divergent perspectives emerge from the literature on Christian conservatism and
marital quality: a feminist theory approach assuming patriarchal gender roles among evangelicals,
and hence these women’s lower satisfaction in the relationship; and a neotraditional approach
predicting their greater marital happiness due to evangelical men’s decades-long and church-
promoted transformation into emotional available and supportive “soft patriarchs” (Wilcox, 2004,
p. 53).
Some scholars rooted in feminist theory have tended to assume that greater patriarchy
among conservative Christians lowers their marital quality, particularly among women
(Gallagher, 2003; McQuillan & Ferree, 1998; Wilcox, 2006). Consistent with this view, multiple
studies indicate a strong association between “traditional” gender roles in the household, and
more marital conflict as well as women’s greater relationship unhappiness (Blair & Johnson,
1992; Greenstein, 1996; Hochschild & Machung, 1989). Moreover, a substantial literature does
suggest gender inequality in evangelical marriages—as reflected in the Southern Baptist
Convention’s 1998 declaration that a wife should “submit herself graciously” to her husband’s
leadership (Niebuhr, 1998; Wilcox, 2006, p. 42). Empirical studies find particularly strong
support for traditional gender attitudes and inequality in household duties among conservative
Christian communities, and a strikingly high likelihood of these women to marry and bear
children early, and remain permanently outside the workforce (Bartkowski, 1999, 2001;
Bartkowski, Wilcox, & Ellison, 2000; Glass & Jacobs, 2005; Wilcox, 1998, 2006). Moreover,
these values and behaviors seem directly fostered by church-based activities and connections—
5
with evangelical institutions providing strong social, ideological, and political support for
conservative gender and family policies (Wilcox, 2006).
Despite these patterns, a cluster of recent studies—both qualitative and probability-
sample—suggests better marital quality among conservative Christians than other religious
groups, particularly for women (Wilcox, 2004, 2006; Wilcox & Wolfinger, 2007, 2008;
Wolfinger & Wilcox, 2008). In part, the mechanism seems to be more supportive behavior and
emotional availability by evangelical men—an especially crucial factor for women’s greater
satisfaction in the relationship (England & Farkas, 1986; Erickson, 1993; Maccoby, 1998; Nock,
2001; Sayer & Bianchi, 2000; Thompson & Walker, 1989; Wilkie et al., 1998). In turn, these
behaviors seem driven by a decades-long process of ideological and social change within
evangelical religious institutions (Hunter, 1987; Miller, 1997; Roof, 1993; Shibley, 1996; Wilcox,
1998). As Wilcox (2006) argues, concern over the degeneration of marriage and the family—
coupled with feminism raising women’s expectations of men even within conservative
communities—have led these churches to focus specifically on improving men’s family patterns.
Analysis of texts and self-help manuals promoted by evangelical groups, such as the Promise
Keepers, indicates that men are perceived as the “weak link” in families, and their emotional
unavailability and irresponsible behaviors as one reason behind divorces, frail families and (more
generally) a disintegration of America’s traditional social fabric (Hegstrom, 2004; McCartney,
Trent, & Smalley, 1992; Spalding, 1996; Wilcox 2004, 2006). Accordingly, through sermons,
church-based activities, and mass media, evangelical institutions have expended much effort in
encouraging men to prioritize their marriages, and give time and attention to their wives and
children (Bartkowski, 2001; Blanchard, Goyer, & Hodges, 2013; Hunter, 1987; Keller, 2011;
McCartney et al., 1992; Pinckney, 1997; Wilcox, 1998, 2006; Yerkovich & Yerkovich, 2008).
6
The focus seems especially to be on promoting men’s emotional openness and expressiveness, as
a means to nurturing deep and meaningful worldly connections mirroring the relationship
between Christ and the church (Hunter, 1987; Keller, 2011; Pinckney, 1997; Smalley & Smalley,
2010; Wilcox & Wolfinger, 2007; Wolfinger & Wilcox, 2008; Yerkovich & Yerkovich, 2008).
Correspondingly, demographic studies suggest that churchgoing evangelical husbands are more
involved and affectionate in their marriages than those with other religious affiliations, and their
wives report more happiness in the relationship (Wilcox & Wolfinger, 2007; Wolfinger &
Wilcox, 2008). Overall, this emerging literature indicates that these marriages may blend
traditional and unequal gender roles with unusually high levels of emotional intimacy as well as
support from the male partner—a relational style that has been termed “neotraditional” (Wilcox,
2006, p. 44). In addition, evangelical institutions and church-centered networks seem to strongly
emphasize “decency” in social roles—i.e., hard work, marital fidelity, avoidance of risky
behaviors such as drinking and drug abuse, and responsible parenting (Wilcox, 2006; Wilcox &
Wolfinger, 2008). Thus, these communities may have more stable life- and family-patterns,
experiencing lower rates of divorce and of domestic violence than any other major religious
group (Ellison, Bartkowski, & Anderson, 1999; Wilcox, 2006). These conjectures led to
Hypothesis 1 (Table 1).
Next, biomedical literature indicates that these religious-group variations in partnership
may also correspond with distinct (and unexplored) sex-hormone differentials. Among women,
for instance, a small set of convenience-sample studies indicates that lower estradiol may be
linked to fewer lifetime sex partners and more satisfaction in a current relationship (Durante &
Li, 2009). It remains unclear whether less estradiol leads women to select into these relationship
patterns—or whether psychobiological effects of current or past partnerships induce these
7
hormone levels. However, potential explanations include these women’s weaker receptivity to
mating signals, lower self- and other-rated attractiveness, and hence a diminished propensity
toward “opportunistic mating” or search for higher-quality mates (Buss & Shackelford, 2008;
Durante & Li, 2009; Roney & Simmons, 2008; Roney, Simmons, & Gray, 2011; Schmitt & Buss,
2001). Similarly, associations have been reported for both genders, and especially men, between
lower androgen levels and fewer current or lifetime partners (Alvergne, Faurie, & Raymond,
2009; Archer, 2006; Bogaert & Fisher, 1995; Gray, 2003; Peters, Simmons, & Rhodes, 2008;
Pollet, van der Meij, Cobey, & Buunk, 2011; van Anders, Hamilton, & Watson, 2007)—with
this diminished serial- or concurrent-polyamory arguably enhancing marital commitment and
quality. Among men, for instance, a large literature on the “challenge hypothesis” indicates that
both testosterone and DHEA may catalyse a trade-off between mating and parenting effort—
such that lower levels of these androgens may inhibit sexual promiscuity and promote
investments in one’s monogamous partner (Archer, 2006; Wingfield, Hegner, Dufty, & Ball,
1990). As with women’s estradiol, however, pathways are yet to be established. In contrast to the
challenge hypothesis, a rival “social modulation” model suggests an effect of relationship
patterns to hormones, such that long-term “exposure” to a stable and high-quality partnership
might lower one’s androgens (Archer, 2006; Pollet et al., 2011). Regardless of causal direction,
the evidence above suggests that if marital quality is indeed higher among evangelicals, these
men and women may also exhibit lower sex-hormone levels. Accordingly, Hypothesis 2 (Table
1) was included to examine hormonal differentials by religious category.
To summarize, the positive behavioral impact of constant church-promoted ideological
and social pressures may make evangelical men more emotionally expressive as well as reliable
spouses, potentially leading to happier and more committed marriages—variations that should be
8
especially consistent among those most religious in this group. Moreover, these partnership
patterns may also correspond with unexplored differentials in sex-hormone levels. In turn, a
growing literature supports a strong association between these relationship traits, and sexual
behaviors and satisfaction, along with gender differences in these connections.
Relationship Quality and Sex
As noted, a range of studies links happiness in the partnership to better sexual
outcomes—especially among women. Recent theoretical frameworks of the sexual response
cycle consistently indicate a role of emotional intimacy in women’s greater desire for and
satisfaction in sex. Thus, for instance, Basson’s “circular model” posits women’s subjective
desire, as well as arousal, as responsive rather than spontaneous or innate—with such
responsivity induced in large part by psychosocial aspects of the relationship (Basson, 2001,
2005, 2008; Basson et al., 2004; Giles & McCabe, 2009; Leiblum, 2001; McCabe et al., 2010).
Similarly, the “dual control” model proposed by Bancroft and colleagues (Bancroft et al., 2005;
Bancroft, Graham, Janssen, & Sanders, 2009; Bancroft & Janssen, 2000) suggests a role of
negative relationship features in inhibiting both women’s and men’s sexual response.
Empirically, multiple studies indicate that partnership problems are a major self-perceived cause
of women’s dysunctions (King, Holt, & Nazareth, 2007)—and associated with multiple sexual
problems among older men as well as women (Das et al., 2012; Laumann, Das, & Waite, 2008).
In contrast, positive feelings toward a current partner (generally, as well as during intercourse)
seem to avert sexual distress (Bancroft, Loftus, & Long, 2003), and among older women, may
alleviate dysfunction due to hormone loss (Dennerstein et al., 2001). More broadly, there is
growing evidence from cross-sectional as well as longitudinal studies that factors such as
emotional bonding, romance, and happiness in the relationship are key triggers for sexual desire,
9
responsivity, as well as satisfaction among both men and women at all ages (Avis et al., 2005;
Basson, 2008; Dennerstein et al., 2001; Dunn et al., 1999; Meston & Buss, 2007). This can be
particularly true in late life, when maintenance of satisfactory sex despite increasing frailty,
health problems, and dysfunctions—one’s own or a partner’s—may require more mutual
understanding and trust (Das et al., 2012). If so, older adults with higher marital quality—such as,
potentially, evangelical men and especially women—may also experience better sexual
outcomes than those in other religious groups. Hypothesis 3 (Table 1) reflects these arguments.
METHOD
Participants
Data were from the 2005-2006 U.S. National Social Life, Health, and Aging Project.
NSHAP is a nationally-representative probability sample of 1550 women and 1455 men aged 57
to 85 years, with an oversampling of Blacks, Hispanics, men, and those 75 to 85. The mean age
for both women and for men was 68 years. In-home interviews of household-dwelling adults in
these age ranges were conducted between July 2005 and March 2006, in both English and
Spanish. The survey had an unweighted response rate of 74.8% and a weighted response rate of
75.5% (Lindau et al., 2007; O’Muircheartaigh, Eckman, & Smith, 2009).
Procedure
In addition to self report, data included assessments of physical and sensory function,
height and weight, and salivary, blood, and vaginal mucosal samples—all collected at the time of
interview by non-medically trained interviewers. Most interviewers were experienced personnel
given further training in conducting interviews by NORC at the University of Chicago, and
remained with the project throughout the interview period. Participant consent was obtained
10
prior to interview. Institutional review boards at the Divison of the Social Sciences and NORC at
the University of Chicago approved data collection procedures (Smith et al., 2009).
Measures
Dependent variables
First, partner support was indexed by two separate ordinal variables, for being able to
rely on and open up to (one’s) partner—each running from 1 (hardly ever (or never)) to 3 (often).
Next, relationship satisfaction was a two-item standardized summary index, comprised of self-
reported happiness in, and emotional satisfaction with, the relationship. Cronbach’s alpha
(Cronbach, 1951) for the combination of these two Likert scales was 0.72. Sexual activity was
indexed by self-reported frequency of sex in the preceding year, and ranged from 0 (no sex last
year) to 5 (once a day or more). Sex and sexual activity were both defined as “any mutually
voluntary activity with another person that involves sexual contact, whether or not intercourse or
orgasm occurs” (Waite et al., 2009). Similarly, participants reported on whether they had a
physically pleasureable relationship, through an ordinal scale running from 0 (not at all) to 4
(extremely). Next, conservative sexual values were indicated by participants’ perceptions of
whether love was necessary for sex, and whether their religion shaped their sexual behavior—
each Likert item ranging from 1 (strongly disagree) to 4 (strongly agree). Associations of these
two indicators with the independent variables were examined separately. As noted, the outcomes
also included levels (in pg/mL) of three sex hormones—estradiol, testosterone, and DHEA—
derived from saliva samples taken during the biomeasure collection portion of the in-home
interview (Gavrilova & Lindau, 2009). Following previously validated protocols (Granger et al.,
2007), passive drool was used to collect whole unstimulated saliva, which was then frozen until
11
assay. Salivary enzyme immunoassays were conducted by Salimetrics Laboratories (State
College, PA), using commercially available kits.
Finally, for both genders, five sexual problems were queried. These included hypoactive
sexual desire (lack of interest in sex); anorgasmia (inability to achieve orgasm during
intercourse); experiencing pain during sex; anhedonia (lack of pleasure in sex); and anxiety
about performance. In addition, physiological arousal issues—trouble maintaining or achieving
an erection (men) and lubrication problems (women)—were also examined in exploratory
analysis. However, their associations with the independent religion variables failed to reach
significance net of controls, and were therefore dropped in the final models. Data on sexual
problems were collected in NSHAP through dichotomous response items, each asking the
participant about the presence of a sexual problem for “several months or more” over the
preceding 12 months (Laumann et al., 2008; Waite, Laumann, Das, & Schumm, 2009).
Participants were only asked these questions if they reported any partnered sex in the past year.
Those reporting a problem were also asked how much they were bothered by it, following the
recommendations of a consensus panel on women’s sexual dysfunctions (Basson et al., 2000).
However, inclusion of personal distress into definitions of sexual problems or dysfunctions has
been extensively critiqued (Laumann et al., 2008; Rosen & Laumann, 2003). Moreover, such a
strategy would have lowered cell sizes below analytic tractability. Therefore, following the 2004
recommendations of the International Consultation on Erectile Dysfunction (Lue et al., 2004),
this study only examined sexual problems per se. Finally, NSHAP women but not men reporting
sex in the preceding year were also asked how often they felt sexually aroused (“turned on”)
during intercourse, with response categories ranging ordinally from 0 (never) to 4 (always).
Independent variables
12
A single dichotomous measure indexed conservative Christian status, relative to all other
religions. Participants were first asked about their “current religious preference.” For those self-
reporting a Protestant affiliation, the specific denomination or branch was then queried.
Participants in a “Baptist” or “Methodist” denomination, who also attended religious services
weekly or more, were coded as conservative Christians, or evangelicals. (It is acknowledged that
U.S. evangelicalism subsumes a range of other churches. However, NSHAP response categories
precluded a more inclusive classification—leading to potential bias in the analyses). The latter
criterion was added to reflect literature indicating consistently better relationship (and hence,
arguably, sexual) outcomes only among evangelicals who attended church regularly (Wilcox,
2006)—perhaps due to greater exposure to ideological and social pressures from the
congregation.
To further explore the role of religious beliefs in conditioning these effects, this
dichotomous variable was cross-categorized by “strongly agreeing” with the statement that
religion shaped one’s sexual behavior—the NSHAP religiosity item most directly linked to sex.
This yielded dummy indicators for conservative Christian, religion guides sex less, and
conservative Christian, religion guides sex more, with other religion as the reference. Similarly,
variation in effects by partner support was examined by cross-categorizing Christian
conservatism with self-reports on being able to open up to as well as rely on one’s partner
“often”. Accordingly, dummy indicators were included for conservative Christian, low partner
support, and conservative Christian, high partner support, with the reference category remaining
the same.
Control variables
13
A participant’s age was entered linearly as a continuous variable in all analyses.
Education—proxying both greater knowledge or awareness of sexual issues, and socioeconomic
status—was an integer score ranging from 1 (less than high school) to 4 (a Bachelor’s degree or
more). Race or ethnicity was indexed through a set of dummy variables for Black and
Hispanic/other, with non-Hispanic White as the reference. Seventy-seven percent of women and
70% of men in the Hispanic/other category were non-Black Hispanics, with the remainder
comprised of American Indians or Alaskan natives, Asian or Pacific Islanders, and “other.” Next,
all analysis adjusted for diagnosed health conditions. NSHAP participants were asked about any
lifetime diagnoses of a range of medical conditions, of which nine—heart attack, arthritis, ulcers,
asthma, stroke, hypertension, diabetes, cancer, and (among men) enlarged prostate—were
combined into a single score based on the Charlson comorbidity index (Charlson, Pompei, Ales,
& McKenzie, 1987; Williams, Pham-Kanter, & Leitsch, 2009). An additional control was added
for current use of sex hormone supplements. NSHAP collected a complete log of currently used
medications during the in-home interview, by direct observation using a computer-based log.
The Multum® drug database, based on the hierarchical classifications of the American Hospital
Formulary Service, was used for coding drug names (Qato, Schumm, Johnson, Mihai, & Lindau,
2009). Finally, all models for sex hormones adjusted for two additional factors: saliva collection
time of day (in hourly units, on a 24-hour scale), and self-reported hours since last food/drink.
Statistical Analyses
All analyses were gender specific. Given the theoretical focus of the study, all models
were restricted to those currently married. After dropping 16 missing observations for
conservative Christianity, the maximum sample size for women was 724, and for men was 1,065.
Eighty-five percent (N = 112) of conservative Christian men, and 77% (N = 953) of those in
14
other religions, were married. Among women, the corresponding proportions were 61% (N = 95)
and 54% (N = 629), respectively, with those widowed comprising the bulk of the remainder in
each case. As the last section makes clear, dependent variables included continuous, ordinal, as
well as dichotomous measures. Accordingly, results are from OLS, ordinal logit, and logistic
regression models, respectively. To facilitate pattern-visualization, coefficients rather than odds
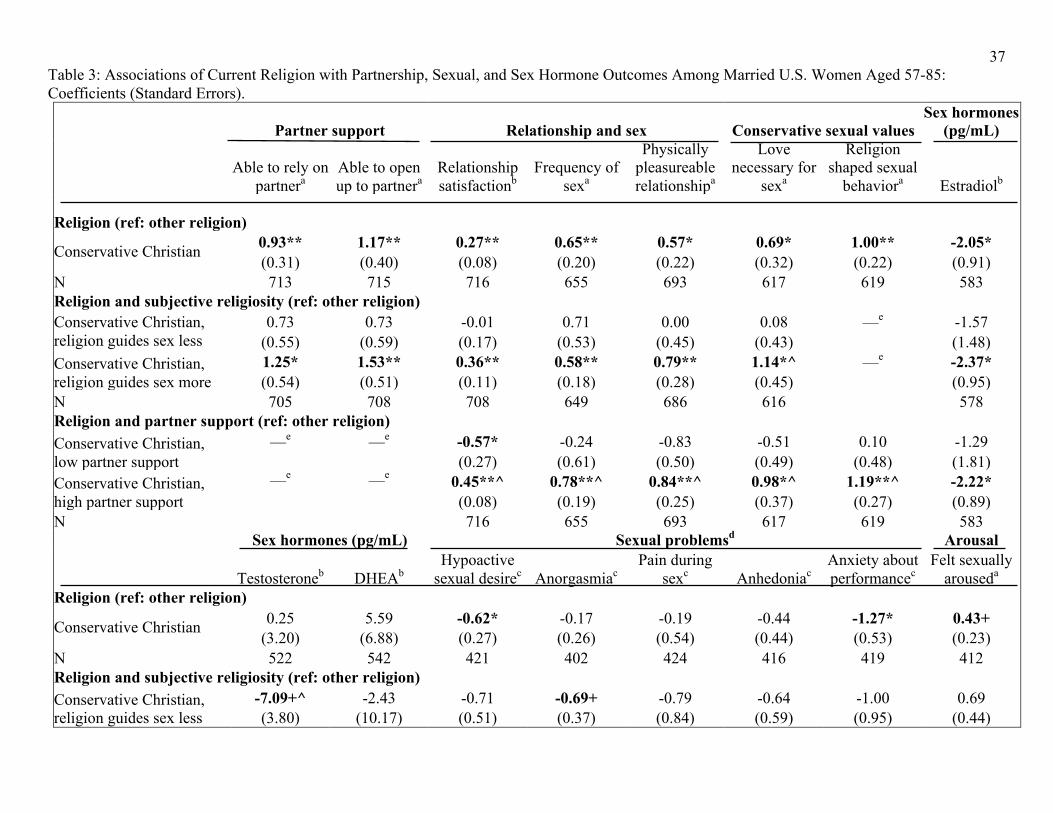
ratios are presented for categorical outcomes. Table 3 reports results for associations among
women of conservative Christianity with relationship and sexual outcomes, as well as sex
hormones—along with variations in these effects by subjective religiosity, and by partner
support. To further validate the coding of the independent variables—i.e., ensure that they
captured the social groups and processes of interest—two indicators of conservative sexual
values (religion shaping sexual behavior, and love being necessary for sex) were also included in
the dependent variables. Corresponding results for men are presented in Table 4.
All analyses were conducted with the STATA 12.0 statistical package (Stata Corp., 2011).
Results were weighted using svy methods for complex survey data, first using population weights
that adjusted for the intentional oversampling of Blacks and Hispanics, and also incorporated a
non-response adjustment based on age and urbanicity (O’Muircheartaigh et al., 2009). Standard
errors were adjusted for sample stratification (sampling strata independently) and clustering
(sampling individuals within each of 100 primary sampling units).
RESULTS
Table 2 presents summary statistics for all dependent and control variables used in the
analyses, stratified by conservative Christian status.
Women’s Outcomes
15
Both sexual and relationship factors were generally better among conservative Christian
women than those in other religious groups (Table 3). Consistent with prior literature, these
women had better partner support—being able to rely on (Coeff. = 0.93) and open up to (Coeff.
= 1.17) their spouses more—and, correspondingly, more relationship satisfaction (Coeff. =
0.27). Frequency of sex in the preceding year (Coeff. = 0.65), as well as physical pleasure in the
relationship (Coeff. = 0.57), was greater for conservative Christian women compared to other
religious groups. These women also had more conservative sexual values—more likely than
women in other religions to perceive love as necessary for sex (Coeff. = 0.69), and that religion
shaped their sexual behaviors (Coeff. = 1.00). Among those sexually active (with any intercourse
last year), evangelical women were also less likely to report hypoactive sexual desire (Coeff. = -
0.62) or performance anxiety (Coeff. = -1.27), and experienced more subjective arousal (Coeff. =
0.43). However, their estradiol levels were also lower (Coeff. = -2.05).
Next, associations were more uniformly positive for conservative Christians who
reported that religion guided their sex life more, relative to those in other religions. Thus, it was
only these evangelical women who reported greater partner support—being able to rely on
(Coeff. = 1.25) and open up to (Coeff. = 1.53) their spouse; higher relationship satisfaction
(Coeff. = 0.36); more frequent sex (Coeff. = 0.58) and physical pleasure (Coeff. = 0.79)—as well
as a higher likelihood of perceiving love to be necessary for sex (Coeff. = 1.14). Similarly,
among those sexually active, it was only these women who experienced less performance anxiety
(Coeff. = -1.25)—although they also had lower estradiol levels (Coeff. = -2.37). In contrast, no
examined outcome was more likely among evangelical women with lower subjective religiosity.
However, these women did have lower testosterone levels than those in other religions (Coeff. =
16
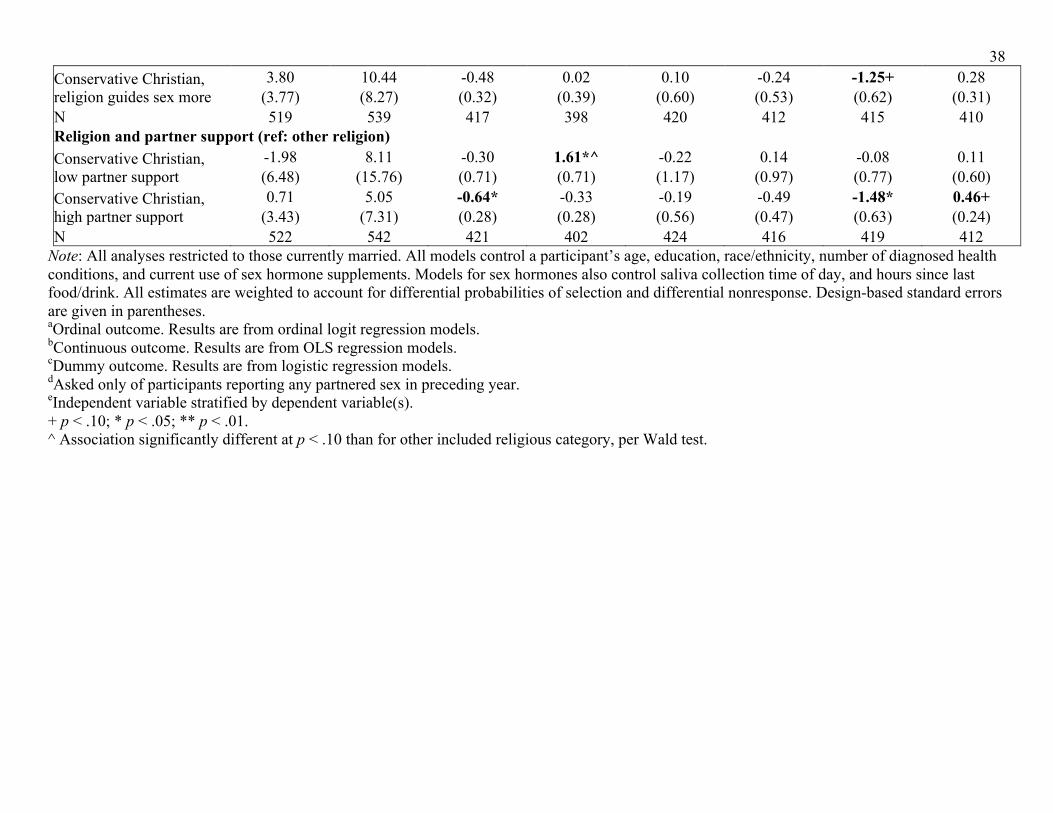
-7.09)—and, among those with intercourse in the past year, a lower likelihood of anorgasmia
(Coeff. = -0.69).
Finally, outcomes were also more uniformly positive among evangelical women with
than those without more partner support. Specifically, relative to women in other religious
groups, it was only the former who had more sex last year (Coeff. = 0.78), more physical
pleasure (Coeff. = 0.84) and higher relationship satisfaction (Coeff. = 0.45)—as well as a higher
likelihood of reporting that love was necessary for sex (Coeff. = 0.98), and that religion guided
their sexual behavior (Coeff. = 1.19). Similarly, among those sexually active, likelihood of
hypoactive sexual desire (Coeff. = -0.64) or performance anxiety (Coeff. = -1.48) were also
lower only among these women, and their subjective arousal higher (Coeff. = 0.46). Moreover, it
was also these women who had lower estradiol levels (Coeff. = -2.22). In contrast, none of the
outcomes were significantly better among evangelical women with low partner support than
those in the reference category. However, the former did report lower satisfaction in the
relationship (Coeff. = -0.57)—and among sexually active women, more anorgasmia (Coeff. =
1.61).
Men’s Outcomes
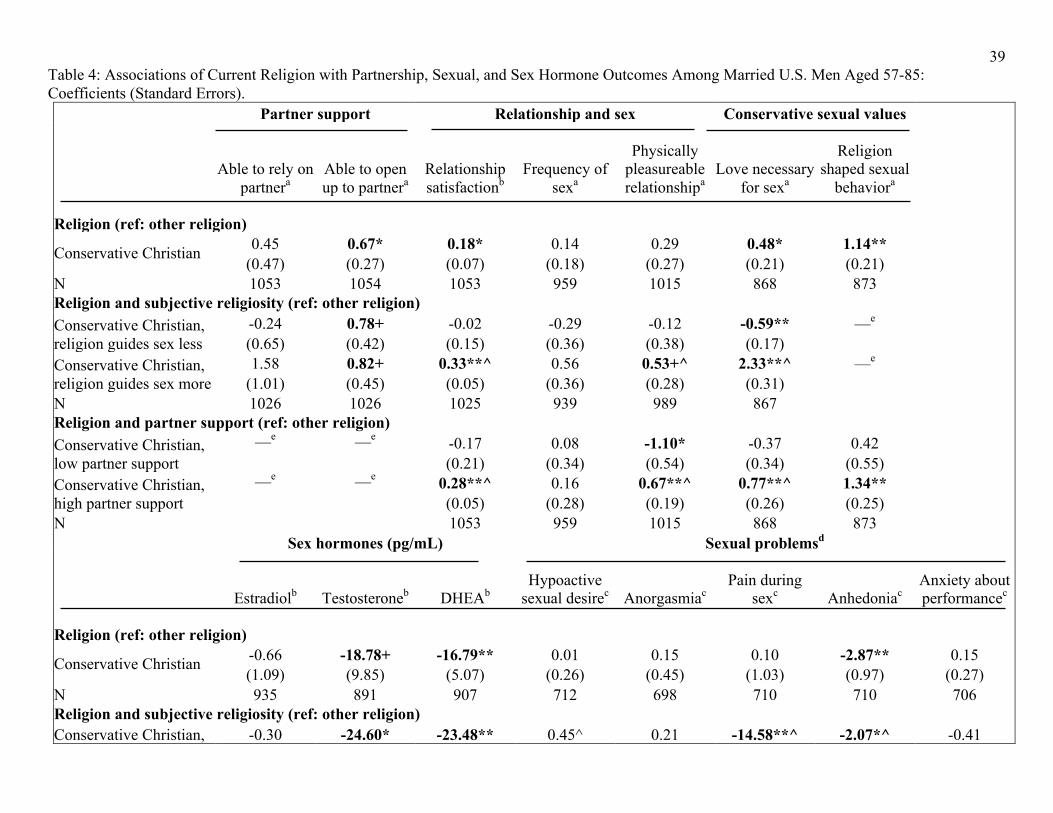
Men’s differentials (Table 4) seemed somewhat less uniform than women’s. As with their
female counterparts, married evangelical men did have generally better relationship features than
those in other religions. These included more partner support—i.e., being able to open up to
one’s spouse (Coeff. = 0.67)—and higher relationship satisfaction (Coeff. = 0.18). Similarly,
these men were also more conservative in their values—more likely to believe that love was
necessary for sex (Coeff. = 0.48), and that religion guided their sexual behaviors (Coeff. = 1.14).
Overall, however, evangelical men’s relational and attitudinal patterns seemed less consistently
17
matched than women’s by better sexual outcomes—with these men no more likely to report
frequent sex or physical pleasure in the relationship than those in other religions. Among those
sexually active, they did experience less anhedonia (Coeff. = -2.87). Moreover, as with women’s
estradiol, these men also had lower androgen levels—both testosterone (Coeff. = -18.78) and its
precursor, DHEA (Coeff. = -16.79).
With regard to subjective religiosity, relationship satisfaction (Coeff. = 0.33) was higher
only among evangelical men who reported that religion guided their sex life more, relative to
those in other religions. Moreover, only these men reported more physical pleasure in the
partnership (Coeff. = 0.53)—and that love was necessary for sex (Coeff. = 2.33). Partner support
(opening up to a partner), in contrast, was better among evangelical men with higher (Coeff. =
0.82) as well as lower (Coeff. = 0.78) subjective religiosity. Also, among sexually active men, it
was only this latter group that reported less pain during sex (Coeff. = -14.58)—with anhedonia
lower among more (Coeff. = -14.53) as well as less (Coeff. = -2.07) religious evangelical men.
Moreover, it was also only the latter who had lower androgen levels—both testosterone (Coeff. =
-24.60) and DHEA (Coeff. = -23.48)—than men in other religions.
Finally, again consistent with women’s patterns, evangelical men’s outcomes were
somewhat stratified by more partner support—with relational satisfaction (Coeff. = 0.28) and
physical pleasure (Coeff. = 0.67) higher only for those with this asset. Similarly, it was these
men who had more conservative sexual values—more likely to report that love was necessary for
sex (Coeff. = 0.77) and that their religion guided their sexual behaviors (Coeff. = 1.34). In
contrast, evangelical men with low partner support also reported less physical pleasure in the
relationship (Coeff. = -1.10) than those in other religions—and, among men with intercourse in
the past year, more hypoactive sexual desire (Coeff. = 0.71). Sexual peformance anxiety,
18
however, was also lower in this group (Coeff. = -0.71). The same was true of pain during sex
(Coeff. = -15.72), while anhedonia was lower among sexually active evangelical men with more
(Coeff. = -2.51) as well as less (Coeff. = -14.57) partner support. Finally, androgen levels did not
seem to vary by this factor. Associations with testosterone failed to reach significance, while
DHEA was lower among conservative Christian men with less (Coeff. = -19.39) as well as more
support from their partner (Coeff. = -16.22).
Supplementary Analysis: Employment, Education
Logistic regression models—controlling a participant’s age, education and race—tested whether
gender roles were more unequal among conservative Christians. The two dichotomous dependent
variables in these analyses were self-reported current employment (whether full- or part-time),
and any college education (whether a vocational certificate, an associate’s degree, or a Bachelors
or higher formal degree). In the results, married evangelical women reported significantly less
current employment, relative to both women in other religions (Coeff. = -0.64) and to their male
counterparts (Coeff. = -0.93). Among married evangelicals, moreover, women were strikingly
less likely than men to have had any college education (Coeff. = -0.71).
Supplementary Analysis: Lifetime Sexual Partners
A final set of ordinal logit regression models—adjusting for the same factors as Tables 3 and 4—
was used to examine life-course partnering patterns, as indicated by one’s self-reported lifetime
number of opposite-gender sexual partners. In the results, both conservative Christian women
(Coeff. = -0.47) and men (Coeff. = -0.86) reported significantly fewer partners.
DISCUSSION
An emerging literature suggests that despite patriarchal gender roles, marital quality may
perhaps be higher among conservative Christian (evangelical) older adults—particularly for
19
women, and those more religious—than their counterparts in other religions (Hypothesis 1, Table
1). In turn, this potential differential led to two further conjectures—lower sex-hormone levels
among married evangelicals, especially those with more partner support (Hypothesis 2), and their
better sexual outcomes than those in other religious groups (Hypothesis 3). Accordingly, data
from a nationally representative probability sample of older U.S. adults were used to query
relational, sexual, and hormone patterns among married evangelicals, relative to their
counterparts in other religions; variations in these outcomes by their subjective religiosity; and
by partner support. Women’s results (Table 3) were generally consistent with better sexual
outcomes and lower estradiol among conservative Christians—especially those more religious or
with greater support from a spouse. In contrast, while married men’s relational differentials were
also per expectations (Table 4), their sexual and hormonal (androgen) patterns seemed less
uniform than among women—reflecting perhaps a looser linkage between these sets of factors.
To recall, it was noted that extant literature on Christian conservatism and marital quality
yields contradictory predictions, with some feminist theory perspectives assuming more
relationship dissatisfaction among evangelical women due to traditional ideologies—and a newer
wave of qualitative as well as probability-sample studies suggesting both genders’ greater marital
happiness in this group, due to evangelical men’s recent shift to a neotraditional role combining
patriarchy with more emotional availability and support (Hypothesis 1, Table 1). Results (Tables
3, 4) were generally consistent with the latter conjecture. As reported, supplementary analysis
did support unequal gender roles among evangelicals, with married women in this community
reporting significantly less current employment than those in other religions, as well as their
male counterparts. Similarly, among married evangelicals, women were strikingly less likely
than men to have had any college education. Despite these differentials, not only did these
20
women receive more support from their partner—and, correspondingly, reported more
satisfaction with the relationship than their counterparts in other religions—but these outcomes
were uniformly positive only among evangelical women with higher subjective religiosity (Table
3). Similarly, likelihood of being able to open up to a partner, and (hence) relationship happiness,
were also higher among evangelical men—with the latter outcome better only among those more
religious (Table 4).
Next, it was argued that these partnership differentials may also correspond to unexplored
hormonal variations. Specifically, biomedical literature links lower sex-hormone levels
(women’s estradiol, men’s androgens) with greater commitment to and investments in one’s
monogamous partnership—whether due to hormonal effects on these relational outcomes, or
psychobiological effects of current or past partnerships on hormone levels. Accordingly, it was
speculated that religious groups with systematically better partnership quality, such as
evangelicals, may also exhibit lower average levels of these endogenous reproductive steroids
(Hypothesis 2, Table 1). As conjectured, androgen (testosterone, DHEA) levels were
significantly lower among conservative Christian men (Table 4), and estradiol among their
female counterparts (Table 3), than those in other religions. Moreover, in stratified analyses,
estradiol was lower only among evangelical women reporting a greater role of religion in their
sex lives, and those more able to open up to and rely on their spouse (Table 3). Men’s stratified
results, however, were less consistent with expectations, with both androgens lower only among
less religious evangelical men, and DHEA lower among those with more as well as less partner
support (Table 4).
Finally, it was conjectured that if marital quality and support from a partner are indeed
higher among conservative Christians than other religious groups, this might induce better sexual
21
outcomes among the former (Hypothesis 3, Table 1). Moreover, this differential may be
especially strong among women, whose sexual desire and satisfaction have been consistently
linked in the literature to emotional intimacy in the relationship. As reported above, separate
analysis indicated that evangelical women as well as men had significantly fewer opposite-
gender lifetime sexual partners. Despite these life-course patterns, married evangelical women
reported more current sex and greater physical pleasure than women in other religions—and,
among those with recent intercourse, fewer problems with sexual desire or performance anxiety,
as well as more subjective arousal (Table 3)—consistent with positive sexual effects of their
better relationships. (Eighty percent of these women—compared to only 65% of their
counterparts in other religions—had had sex in the preceding year. Additionally, as noted,
women’s lubrication problems—along with men’s erectile difficulties—were also queried in
exploratory analysis, with both outcomes dropped in the final models due to a lack of significant
associations with the religion predictors.) Moreover, as with the estradiol results above, these
differentials seemed stratified by subjective religiosity, with only evangelical women reporting a
greater role of religion in their sex lives having more intercourse and physical pleasure, as well
as less performance anxiety. In contrast, conservative Christian men’s better relationships were
not as uniformly matched by positive sexual outcomes (Table 4)—reflecting perhaps a somewhat
looser linkage between their sexual and partnership factors than among women. Despite their
lower androgens, however, those in this group with intercourse in the past year (81%, compared
to 75% of men in other religions) did report less anhedonia. In addition, among married
evangelicals, only men with higher subjective religiosity reported more physical pleasure in the
relationship. Unexpectedly, however, it was their less religious counterparts who reported fewer
22
problems with pain during sex. Men’s anhedonia, on the other hand, was less frequent among
evangelicals with as well as without these attitudes.
As with religiosity, stratification by partner support also yielded sexual differentials
generally consistent with expectations (Hypothesis 3, Table 1)—with both women’s (Table 3)
and men’s (Table 4) results indicating more uniformly positive outcomes among evangelicals
more able to open up to and rely on a spouse. Specifically, it was evangelical women with more
such support who reported more sex, more physical pleasure, and greater relationship
satisfaction—and, among those with intercourse in the past year, fewer problems with sexual
desire or performance anxiety, as well as more subjective arousal. In contrast, sexually active
evangelical women with low support from a spouse also reported more anorgasmia. Men’s
patterns seemed similarly although less uniformly stratified, with only evangelical men with
greater partner support reporting higher relationship satisfaction as well as physical pleasure.
Those less able to rely on or open up to their spouse, in contrast, also reported less physical
pleasure and (among those with recent intercourse) more hypoactive sexual desire than men in
other religions. Contrary to expectations, however, they also had fewer problems with pain
during sex—while anhedonia was less likely among evangelical men with or without partner
support.
Overall, then, findings from this nationally-representative study suggested that despite
facing greater patriarchy, evangelical older women may experience better marital quality than
those in other religions—perhaps due to the decades-long church-promoted transformation of
their male counterparts into authoritative-yet-supportive “soft patriarchs” (Wilcox, 2004, p. 53).
Moreover, these psychosocial assets also seemed to induce positive sexual effects, with
conservative Christian women—especially those more religious, and/or with more partner
23
support—reporting consistently better sexual outcomes and fewer problems with intercourse.
These linkages held despite their lower estradiol levels. While the influence of this hormone on
women’s sexual behavior and motivation remains debated, some small-sample analyses do
suggest such linkages (Dennerstein, Randolph, Taffe, Dudley, & Burger, 2002; Pitkin & Rees,
2008; Wylie et al., 2010). If so, findings from the present study suggest that the positive sexual
effects of evangelical women’s better relationships may outweigh potentially negative influences
of their lower estradiol. While men in this group also appeared to experience more satisfactory
partnerships, their sexual patterns were less consistent—perhaps reflecting a gender differential
in the linkage between these two sets of factors.
Limitations
There were several limitations to this study. Most importantly, given the cross-sectional
data, temporal order and causal direction could not be demonstrated—for instance, between
partner support and sexual outcomes. Additionally, the NSHAP data contained no information
about a spouse’s religious affiliations, attitudes, or behaviors. Hence, inferences about
evangelical partners providing more support had to be based on a participant’s own ratings. More
generally, other than salivary hormone levels, all analyses were based on self-reports, which
provided no direct evidence of sexual or relational patterns—making participants’ differential
sensitivity to the same factors a potential problem. Cell sizes were small for many of the
models—such as differentials by subjective religiosity and partner support among evangelicals;
and sexual problems, queried only for the subsample with recent intercourse—although, that
multiple associations reached significance despite this low power testifies to their strength. The
present study should thus be seen as a broad analysis that establishes baseline linkages and lays
the groundwork for deeper examination.
24
Summary
Data from a nationally representative probability sample suggested that consistent with
previous studies on younger age groups, evangelical men and especially women in late life had
more support from a partner and (hence) better marital quality than their counterparts in other
religions. In keeping with a sparse recent literature, they also had lower sex hormone levels—
whether because psychobiological aspects of their better relationships had lowered their
hormones, or because those with more of these endogenous reproductive steroids had selected
into less “traditional” partnership trajectories and worse current marriages. Moreover, at least
among women, evangelicals’ better marriages also seemed to induce positive sexual effects, with
these women reporting consistently better sexual outcomes than those in other religions—
especially when they had more spousal support and/or greater subjective religiosity. Men’s
relationship differentials were less uniformly matched by their sexual patterns, reflecting perhaps
a somewhat looser linkage between these sets of factors than among women.
25
REFERENCES
Alvergne, A., Faurie, C., & Raymond, M. (2009). Variation in testosterone levels and male
reproductive effort: Insight from a polygynous human population. Hormones and
Behavior, 56, 491-497.
Archer, J. (2006). Testosterone and human aggression: An evaluation of the challenge
hypothesis. Neuroscience and Biobehavioral Reviews, 30, 319-345.
Avis, N. E., Zhao, X., Johannes, C. B., Ory, M., Brockwell, S., & Greendale, G. A. (2005).
Correlates of sexual function among multi-ethnic middle-aged women: Results from the
Study of Women's Health Across the Nation (SWAN). Menopause, 12, 385-398.
Bancroft, J., Herbenick, D., Barnes, T., Hallam-Jones, R., Wylie, K., Janssen, E., et al. (2005).
The relevance of the dual control model to male sexual dysfunction: The Kinsey
Institute/BASRT collaborative project. Sexual and Relationship Therapy, 20, 13-30.
Bancroft, J., Graham, C. A., Janssen, E., & Sanders, S. A. (2009). The Dual Control model:
Current status and future directions. Journal of Sex Research, 46, 121-142.
Bancroft, J., & Janssen, E. (2000). The dual control model of male sexual response: A theoretical
approach to centrally mediated erectile dysfunction. Neuroscience and Biobehavioral
Reviews, 24, 571-579.
Bancroft, J., Loftus, J., & Long, J. S. (2003). Distress about sex: A national survey of women in
heterosexual relationships. Archives of Sexual Behavior, 32, 193-208.
Bartkowski, J. P. (1999). One step forward, one step back: “Progressive traditionalism” and the
negotiation of domestic labor in evangelical families. Gender Issues, 17, 37-61.
Bartkowski, J. P. (2001). Remaking the godly marriage: Gender negotiation in evangelical
families. New Brunswick, N. J.: Rutgers University Press.
26
Bartkowski, J. P., Wilcox, W. B., & Ellison, C. G. (2000). Charting the paradoxes of evangelical
family life: Gender and parenting in conservative Protestant households. Family Ministry,
14, 9-21.
Basson, R., Berman, J., Burnett, A., Derogatis, L., Ferguson, D., Fourcroy, J., et al. (2000).
Report of the international consensus development conference on female sexual
dysfunction: Definitions and classifications. Journal of Urology, 163, 888-893.
Basson, R. (2001). Human sex-response cycles. Journal of Sex and Marital Therapy, 27, 33-43.
Basson, R. (2005). Women's sexual dysfunction: Revised and expanded definitions. CMAJ, 172,
1327-1333.
Basson, R. (2008). Women's sexual function and dysfunction: Current uncertainties, future
directions. International Journal of Impotence Research, 20, 466-478.
Basson, R., Althof, S., Davis, S., Fugl-Meyer, K., Goldstein, I., Leiblum, S., et al. (2004).
Summary of the recommendations on sexual dysfunctions in women. Journal of Sexual
Medicine, 1, 24-34.
Blair, S. L., & Johnson, M. P. (1992). Wives' perceptions of the fairness of the division of
household labor: The intersection of housework and ideology. Journal of Marriage and
the Family, 54, 570-581.
Blanchard, K., Goyer, T., & Hodges, P. (2013). Lead your family like Jesus: Powerful parenting
principles from the creator of families. Carol Stream, IL: Tyndale House.
Bogaert, A. F., & Fisher, W. A. (1995). Predictors of university men's number of sexual partners.
Journal of Sex Research, 32, 119-130.
Buss, D. M., & Shackelford, T. K. (2008). Attractive women want it all: Good genes, economic
investment, parenting proclivities, and emotional commitment. Evolutionary Psychology,
27
6, 134-136.
Charlson, M. E., Pompei, P., Ales, K. L., & McKenzie, C. R. (1987). A new method of
classifying prognostic comorbidity in longitudinal studies: Development and validation.
Journal of Chronic Diseases, 40, 373-383.
Cronbach, L. J. (1951). Coefficient alpha and the internal structure of tests. Psychometrika, 16,
297-334.
Das, A., Laumann, E. O., & Waite, L. J. (2012). Sexual expression over the life course: Results
from three landmark surveys. In J. DeLamater & L. Carpenter (Eds.), Sex for life: From
virginity to viagra, how sexuality changes throughout our lives (pp. 236-259). New York:
New York University Press.
Dennerstein, L., Dudley, E., & Burger, H. (2001). Are changes in sexual functioning during
midlife due to aging or menopause? Fertility and Sterility, 76, 456-460.
Dennerstein, L., Randolph, J., Taffe, J., Dudley, E., & Burger, H. (2002). Hormones, mood,
sexuality, and the menopausal transition. Fertility and Sterility, 77, S42-S48.
Dunn, K. M., Croft, P. R., & Hackett, G. I. (1999). Association of sexual problems with social,
psychological, and physical problems in men and women: A cross sectional population
survey. Journal of Epidemiology and Community Health, 53, 144-148.
Durante, K. M., & Li, N. P. (2009). Oestradiol level and opportunistic mating in women.
Biology Letters, 5, 179-182.
Ellison, C. G., Bartkowski, J. P., & Anderson, K. L. (1999). Are there religious variations in
domestic violence? Journal of Family Issues, 20, 87-113.
England, P., & Farkas, G. (1986). Households, employment and gender. Hawthorne, N.Y.:
Aldine de Gruyter.
28
Erickson, R. J. (1993). Reconceptualizing family work: The effect of emotion work on
perceptions of marital quality. Journal of Marriage and the Family, 55, 888-900.
Gallagher, S. (2003). Evangelical identity and gendered family life. Piscataway, N.J.: Rutgers
University Press.
Gavrilova, N., Lindau, S. T. (2009). Salivary sex hormone measurement in a national,
population-based study of older adults. Journals of Gerontology-Series B Psychological
Sciences and Social Sciences, 64, i94-i105.
Giles, K. R., & McCabe, M. P. (2009). Conceptualizing women's sexual function: Linear vs.
circular models of sexual response. Journal of Sexual Medicine, 6, 2761-2771.
Glass, J., & Jacobs, J. (2005). Childhood religious conservatism and adult attainment among
black and white women. Social Forces, 84, 555-579.
Granger, D. A., Kivlighan, K. T., Fortunato, C., Harmon, A. G., Hibel, L. C., Schwartz, et al.
(2007). Integration of salivary biomarkers into developmental and behaviorally-oriented
research: Problems and solutions for collecting specimens. Physiology and Behavior, 92,
583-590.
Gray, P. B. (2003). Marriage, parenting, and testosterone variation among Kenyan Swahili men.
American Journal of Physical Anthropology, 122, 279-286.
Greenstein, T. N. (1996). Gender ideology and perceptions of the fairness of the division of
household labor: Effects on marital quality. Social Forces, 74, 1029-1042.
Hegstrom, P. (2004). Angry men and the women who love them: Breaking the cycle of physical
and emotional abuse. Kansas City, KS: Beacon Hill Press.
Hochschild, A., & Machung, A. (1989). The second shift: Working parents and the revolution at
home. New York: Viking.
29
Hunter, J. D. (1987). Evangelicalism: The coming generation. Chicago, IL: University of
Chicago Press.
Keller, T. (2011). The meaning of marriage: Facing the complexities of commitment with the
wisdom of God. New York: Dutton Adult.
King, M., Holt, V., & Nazareth, I. (2007). Women's views of their sexual difficulties:
Agreement and disagreement with clinical diagnoses. Archives of Sexual Behavior, 36,
281-288.
Laumann, E. O., Das, A., & Waite, L. J. (2008). Sexual dysfunction among older adults:
Prevalence and risk factors from a nationally representative U.S. probability sample of
men and women 57-85 years of age. Journal of Sexual Medicine, 5, 2300-2311.
Leiblum, S. (2001). Critical overview of the new consensus classifications and definitions of
female sexual dysfunction. Journal of Sex and Marital Therapy, 27, 159-169.
Lindau, S. T., Schumm, L. P., Laumann, E. O., Levinson, W., O'Muircheartaigh, C. A., & Waite,
L. J. (2007). A study of sexuality and health among older adults in the United States.
New England Journal of Medicine, 357, 762-774.
Lue, T., Basson, R., Rosen, R., Guiliano, F., Khoury, S., & Montorsi, F. (2004). Sexual medicine:
Sexual dysfunction in men and women. Paris: Health Publications.
Maccoby, E. E. (1998). The two sexes: Growing up apart, coming together. Cambridge, MA:
Harvard University Press.
McCabe, M., Althof, S. E., Assalian, P., Chevret-Measson, M., Leiblum, S. R., Simonelli, C., et
al. (2010). Psychological and interpersonal dimensions of sexual function and
dysfunction. Journal of Sexual Medicine, 7, 327-336.
McCartney, B., Trent, J. T., & Smalley, G. (1992). What makes a man?: Twelve promises that
30
will change your life! Colorado Springs, CO: Navpress Publishing Group.
McQuillan, J., & Ferree, M. M. (1998). The importance of variation among men and the
benefits of feminism for families. In A Booth and A. Crouter (Eds.), Men in families:
When do they get involved? What difference does it make? (pp. 213-225). Hillsdale, N.J.:
Lawrence Erlbaum.
Meston, C. M., & Buss, D. M. (2007). Why humans have sex. Archives of Sexual Behavior, 36,
477-507.
Miller, D. E. (1997). Reinventing American Protestantism: Christianity in the new millennium.
Berkeley, CA: University of California Press.
Niebuhr, G. (1998). Southern Baptists declare wife should ‘submit' to her husband. New York
Times, June 10, 1998.
Nock, S. L. (2001). The marriages of equally dependent spouses. Journal of Family Issues, 22,
755-775.
O'Muircheartaigh, C., Eckman, S., & Smith, S. (2009). Statistical design and estimation for the
National Social Life, Health, and Aging Project. Journals of Gerontology-Series B
Psychological Sciences and Social Sciences, 64, i12-i19.
Peters, M., Simmons, L. W., & Rhodes, G. (2008). Testosterone is associated with mating
success but not attractiveness or masculinity in human males. Animal Behaviour, 76,
297-303.
Pinckney, C. What is Christian marriage? (sermon) Community Bible Church:
Williamstown, MA, 1997. Downloaded from: http://tcpiii.tripod.com/marriage2.htm
Pitkin, J., & Rees, M. (2008). Urogenital atrophy. Menopause International, 14, 136-137.
Pollet, T. V., der Meij, L. V., Cobey, K. D., & Buunk, A. P. (2011). Testosterone levels and
31
their associations with lifetime number of opposite sex partners and remarriage in a large
sample of American elderly men and women. Hormones and Behavior, 60, 72-77.
Qato, D. M., Schumm, L. P., Johnson, M., Mihai, A., & Lindau, S. T. (2009). Medication data
collection and coding in a home-based survey of older adults. Journals of Gerontology-
Series B Psychological Sciences and Social Sciences, 64, i86-i93.
Roney, J. R., & Simmons, Z. L. (2008). Women's estradiol predicts preference for facial cues of
men's testosterone. Hormones and Behavior, 53, 14-19.
Roney, J. R., Simmons, Z. L., & Gray, P. B. (2011). Changes in estradiol predict within-women
shifts in attraction to facial cues of men's testosterone. Psychoneuroendocrinology, 36,
742-749.
Roof, W. C. (1993). A generation of seekers: The spiritual journeys of the Baby Boom
generation. New York: Harper Collins.
Rosen, R. C., & Laumann, E. O. (2003). The prevalence of sexual problems in women: How
valid are comparisons across studies? Archives of sexual behavior, 32, 209-211.
Sayer, L. C., & Bianchi, S. M. (2000). Women's economic independence and the probability of
divorce. Journal of Family Issues, 21, 906-943.
Schmitt, D. P., & Buss, D. M. (2001). Human mate poaching: Tactics and temptations for
infiltrating existing mateships. Journal of Personality and Social Psychology, 80, 894-
917.
Shibley, M. A. (1996). Resurgent evangelicalism in the United States: Mapping cultural change
since 1970. Columbia, SC: University of South Carolina Press.
Smith, S., Jaszczak, A., Graber, J., Lundeen, K., Leitsch, S., Wargo, E., et al. (2009). Instrument
development, study design implementation, and survey conduct for the National Social
32
Life, Health, and Aging Project. Journals of Gerontology-Series B Psychological
Sciences and Social Sciences, 64, i20-i29.
Spalding, J. D. (1996). Bonding in the bleachers: A visit to the Promise Keepers. The Christian
Century, 113, 260-265.
Stata Corp. (2011). STATA Release 12.0. College Station, TX: Stata Press.
Thompson, L., & Walker, A. J. (1989). Gender in families: Women and men in marriage, work,
and parenthood. Journal of Marriage and the Family, 51, 845-871.
van Anders, S. M., Hamilton, L. D., & Watson, N. V. (2007). Multiple partners are associated
with higher testosterone in North American men and women. Hormones and Behavior,
51, 454-459.
Waite, L. J., Laumann, E. O., Das, A., & Schumm, L. P. (2009). Sexuality: Measures of
partnerships, practices, attitudes, and problems in the National Social Life, Health, and
Aging Study. Journals of Gerontology-Series B Psychological Sciences and Social
Sciences, 64, i56-i66.
Wilcox, W. B. (1998). Conservative protestant childrearing: Authoritarian or authoritative?
American Sociological Review, 63, 796-809.
Wilcox, W. B. (2004). Soft patriarchs, new men: How Christianity shapes fathers and husbands.
Chicago, IL: University of Chicago Press.
Wilcox, W. B. (2006). Religion and the domestication of men. Contexts, 5, 42-46.
Wilcox, W. B, & Nock, S. L. (2006). What's love got to do with it? Equality, equity, commitment
and women's marital quality. Social Forces, 84, 1321-1345.
Wilcox, W. B., & Wolfinger, N. H. (2007). Then comes marriage? Religion, race, and marriage
in urban America. Social Science Research, 36, 569-589.
33
Wilcox, W. B., & Wolfinger, N. H. (2008). Living and loving “decent”: Religion and
relationship quality among urban parents. Social Science Research, 37, 828-843.
Wilkie, J. R., Ferree, M. M., & Ratcliff, K. S. (1998). Gender and fairness: Marital satisfaction in
two-earner couples. Journal of Marriage and Family, 60, 577-594.
Williams, S. R., Pham-Kanter, G., & Leitsch, S. A. (2009). Measures of chronic conditions and
diseases associated with aging in the National Social Life, Health, and Aging Project.
Journals of Gerontology-Series B Psychological Sciences and Social Sciences, 64, i67-
i75.
Wingfield, J. C., Hegner, R. E., Dufty Jr, A. M., & Ball, G. F. (1990). The “challenge
hypothesis”: theoretical implications for patterns of testosterone secretion, mating
systems, and breeding strategies. American Naturalist, 136, 829-846.
Wolfinger, N. H., & Wilcox, W. B. (2008). Happily ever after? Religion, marital status, gender
and relationship quality in urban families. Social Forces, 86, 1311-1337.
Wylie, K., Rees, M., Hackett, G., Anderson, R., Bouloux, P.-M., Cust, M., et al. (2010).
Androgens, health and sexuality in women and men. Human Fertility, 13, 277-297.
Yerkovich, M., & Yerkovich, K. (2008). How we love: A revolutionary approach to deeper
connections in marriage. Colorado Springs, CO: WaterBrook Press.

34
Table 1: Summary of hypotheses. Relative to those in other religious groups, conservative Christian older adults—particularly women, and those with greater subjective religiosity—will experience:
1. better marital quality, as indicated by greater support from a partner and more relationship satisfaction; and, especially when they have such support:
2. lower sex hormone levels; and 3. better sexual outcomes as well as a lower likelihood of sexual problems.
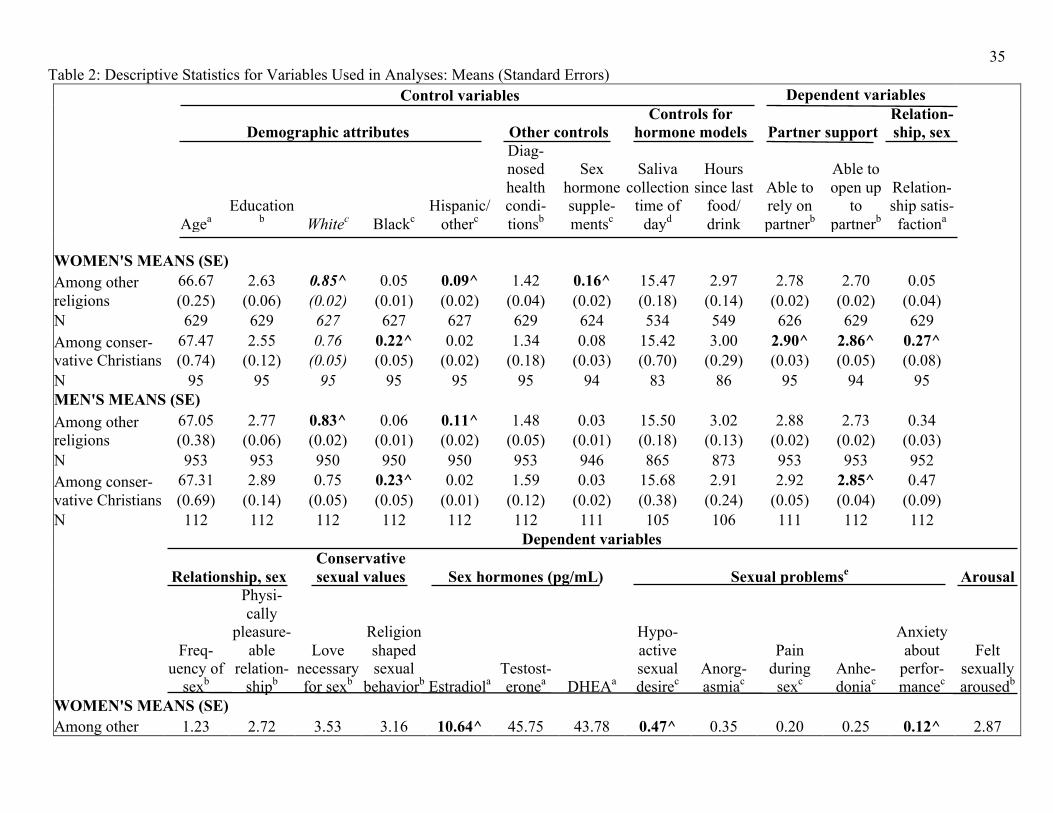
35 Table 2: Descriptive Statistics for Variables Used in Analyses: Means (Standard Errors) Control variables Dependent variables
Demographic attributes Other controls Controls for
hormone models
Partner support Relation-ship, sex
Agea Education
b Whitec Blackc Hispanic/
otherc
Diag-nosed health condi-tionsb
Sex hormone supple-mentsc
Saliva
collection time of
dayd
Hours since last
food/ drink
Able to rely on partnerb
Able to open up
to partnerb
Relation-ship satis-factiona
WOMEN'S MEANS (SE)
Among other religions
66.67 2.63 0.85^ 0.05 0.09^ 1.42 0.16^ 15.47 2.97 2.78 2.70 0.05 (0.25) (0.06) (0.02) (0.01) (0.02) (0.04) (0.02) (0.18) (0.14) (0.02) (0.02) (0.04)
N 629 629 627 627 627 629 624 534 549 626 629 629 Among conser-vative Christians
67.47 2.55 0.76 0.22^ 0.02 1.34 0.08 15.42 3.00 2.90^ 2.86^ 0.27^ (0.74) (0.12) (0.05) (0.05) (0.02) (0.18) (0.03) (0.70) (0.29) (0.03) (0.05) (0.08)
N 95 95 95 95 95 95 94 83 86 95 94 95 MEN'S MEANS (SE) Among other religions
67.05 2.77 0.83^ 0.06 0.11^ 1.48 0.03 15.50 3.02 2.88 2.73 0.34 (0.38) (0.06) (0.02) (0.01) (0.02) (0.05) (0.01) (0.18) (0.13) (0.02) (0.02) (0.03)
N 953 953 950 950 950 953 946 865 873 953 953 952 Among conser-vative Christians
67.31 2.89 0.75 0.23^ 0.02 1.59 0.03 15.68 2.91 2.92 2.85^ 0.47 (0.69) (0.14) (0.05) (0.05) (0.01) (0.12) (0.02) (0.38) (0.24) (0.05) (0.04) (0.09)
N 112 112 112 112 112 112 111 105 106 111 112 112
Dependent variables
Relationship, sex Conservative sexual values
Sex hormones (pg/mL)
Sexual problemse Arousal
Freq-uency of
sexb
Physi-cally
pleasure-able
relation-shipb
Love necessary for sexb
Religion shaped sexual
behaviorb
Estradiola Testost-eronea DHEAa
Hypo-active sexual desirec
Anorg-asmiac
Pain during sexc
Anhe-doniac
Anxiety about
perfor-mancec
Felt sexually arousedb
WOMEN'S MEANS (SE) Among other 1.23 2.72 3.53 3.16 10.64^ 45.75 43.78 0.47^ 0.35 0.20 0.25 0.12^ 2.87
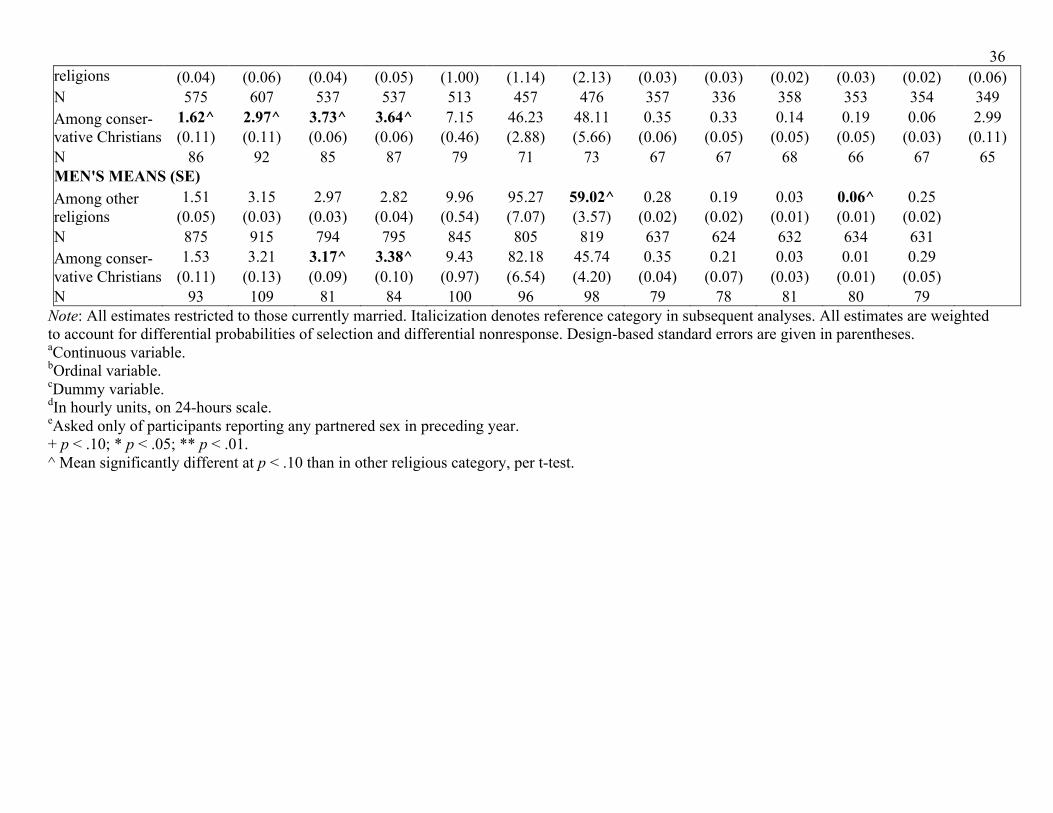
36 religions (0.04) (0.06) (0.04) (0.05) (1.00) (1.14) (2.13) (0.03) (0.03) (0.02) (0.03) (0.02) (0.06) N 575 607 537 537 513 457 476 357 336 358 353 354 349 Among conser-vative Christians
1.62^ 2.97^ 3.73^ 3.64^ 7.15 46.23 48.11 0.35 0.33 0.14 0.19 0.06 2.99 (0.11) (0.11) (0.06) (0.06) (0.46) (2.88) (5.66) (0.06) (0.05) (0.05) (0.05) (0.03) (0.11)
N 86 92 85 87 79 71 73 67 67 68 66 67 65 MEN'S MEANS (SE) Among other religions
1.51 3.15 2.97 2.82 9.96 95.27 59.02^ 0.28 0.19 0.03 0.06^ 0.25 (0.05) (0.03) (0.03) (0.04) (0.54) (7.07) (3.57) (0.02) (0.02) (0.01) (0.01) (0.02)
N 875 915 794 795 845 805 819 637 624 632 634 631 Among conser-vative Christians
1.53 3.21 3.17^ 3.38^ 9.43 82.18 45.74 0.35 0.21 0.03 0.01 0.29 (0.11) (0.13) (0.09) (0.10) (0.97) (6.54) (4.20) (0.04) (0.07) (0.03) (0.01) (0.05)
N 93 109 81 84 100 96 98 79 78 81 80 79 Note: All estimates restricted to those currently married. Italicization denotes reference category in subsequent analyses. All estimates are weighted to account for differential probabilities of selection and differential nonresponse. Design-based standard errors are given in parentheses. aContinuous variable. bOrdinal variable. cDummy variable. dIn hourly units, on 24-hours scale. eAsked only of participants reporting any partnered sex in preceding year. + p < .10; * p < .05; ** p < .01. ^ Mean significantly different at p < .10 than in other religious category, per t-test.
37 Table 3: Associations of Current Religion with Partnership, Sexual, and Sex Hormone Outcomes Among Married U.S. Women Aged 57-85: Coefficients (Standard Errors).
Partner support Relationship and sex Conservative sexual values Sex hormones
(pg/mL)
Able to rely on
partnera Able to open up to partnera
Relationship satisfactionb
Frequency of sexa
Physically pleasureable relationshipa
Love necessary for
sexa
Religion shaped sexual
behaviora
Estradiolb
Religion (ref: other religion)
Conservative Christian 0.93** 1.17** 0.27** 0.65** 0.57* 0.69* 1.00** -2.05* (0.31) (0.40) (0.08) (0.20) (0.22) (0.32) (0.22) (0.91)
N 713 715 716 655 693 617 619 583 Religion and subjective religiosity (ref: other religion) Conservative Christian, religion guides sex less
0.73 0.73 -0.01 0.71 0.00 0.08 —e -1.57 (0.55) (0.59) (0.17) (0.53) (0.45) (0.43)
(1.48)
Conservative Christian, religion guides sex more
1.25* 1.53** 0.36** 0.58** 0.79** 1.14*^ —e -2.37* (0.54) (0.51) (0.11) (0.18) (0.28) (0.45)
(0.95)
N 705 708 708 649 686 616
578 Religion and partner support (ref: other religion) Conservative Christian, low partner support
—e —e -0.57* -0.24 -0.83 -0.51 0.10 -1.29
(0.27) (0.61) (0.50) (0.49) (0.48) (1.81)
Conservative Christian, high partner support
—e —e 0.45**^ 0.78**^ 0.84**^ 0.98*^ 1.19**^ -2.22*
(0.08) (0.19) (0.25) (0.37) (0.27) (0.89)
N
716 655 693 617 619 583
Sex hormones (pg/mL) Sexual problemsd Arousal
Testosteroneb DHEAb Hypoactive
sexual desirec Anorgasmiac Pain during
sexc Anhedoniac Anxiety about performancec
Felt sexually arouseda
Religion (ref: other religion)
Conservative Christian 0.25 5.59 -0.62* -0.17 -0.19 -0.44 -1.27* 0.43+ (3.20) (6.88) (0.27) (0.26) (0.54) (0.44) (0.53) (0.23)
N 522 542 421 402 424 416 419 412 Religion and subjective religiosity (ref: other religion) Conservative Christian, religion guides sex less
-7.09+^ -2.43 -0.71 -0.69+ -0.79 -0.64 -1.00 0.69 (3.80) (10.17) (0.51) (0.37) (0.84) (0.59) (0.95) (0.44)
38 Conservative Christian, religion guides sex more
3.80 10.44 -0.48 0.02 0.10 -0.24 -1.25+ 0.28 (3.77) (8.27) (0.32) (0.39) (0.60) (0.53) (0.62) (0.31)
N 519 539 417 398 420 412 415 410 Religion and partner support (ref: other religion) Conservative Christian, low partner support
-1.98 8.11 -0.30 1.61*^ -0.22 0.14 -0.08 0.11 (6.48) (15.76) (0.71) (0.71) (1.17) (0.97) (0.77) (0.60)
Conservative Christian, high partner support
0.71 5.05 -0.64* -0.33 -0.19 -0.49 -1.48* 0.46+ (3.43) (7.31) (0.28) (0.28) (0.56) (0.47) (0.63) (0.24)
N 522 542 421 402 424 416 419 412 Note: All analyses restricted to those currently married. All models control a participant’s age, education, race/ethnicity, number of diagnosed health conditions, and current use of sex hormone supplements. Models for sex hormones also control saliva collection time of day, and hours since last food/drink. All estimates are weighted to account for differential probabilities of selection and differential nonresponse. Design-based standard errors are given in parentheses. aOrdinal outcome. Results are from ordinal logit regression models. bContinuous outcome. Results are from OLS regression models. cDummy outcome. Results are from logistic regression models. dAsked only of participants reporting any partnered sex in preceding year. eIndependent variable stratified by dependent variable(s). + p < .10; * p < .05; ** p < .01. ^ Association significantly different at p < .10 than for other included religious category, per Wald test.
39 Table 4: Associations of Current Religion with Partnership, Sexual, and Sex Hormone Outcomes Among Married U.S. Men Aged 57-85: Coefficients (Standard Errors). Partner support Relationship and sex Conservative sexual values
Able to rely on partnera
Able to open up to partnera
Relationship satisfactionb
Frequency of sexa
Physically
pleasureable relationshipa
Love necessary for sexa
Religion shaped sexual
behaviora
Religion (ref: other religion)
Conservative Christian 0.45 0.67* 0.18* 0.14 0.29 0.48* 1.14** (0.47) (0.27) (0.07) (0.18) (0.27) (0.21) (0.21) N 1053 1054 1053 959 1015 868 873
Religion and subjective religiosity (ref: other religion) Conservative Christian, religion guides sex less
-0.24 0.78+ -0.02 -0.29 -0.12 -0.59** —e (0.65) (0.42) (0.15) (0.36) (0.38) (0.17)
Conservative Christian, religion guides sex more
1.58 0.82+ 0.33**^ 0.56 0.53+^ 2.33**^ —e (1.01) (0.45) (0.05) (0.36) (0.28) (0.31)
N 1026 1026 1025 939 989 867 Religion and partner support (ref: other religion)
Conservative Christian, low partner support
—e —e -0.17 0.08 -1.10* -0.37 0.42
(0.21) (0.34) (0.54) (0.34) (0.55)
Conservative Christian, high partner support
—e —e 0.28**^ 0.16 0.67**^ 0.77**^ 1.34**
(0.05) (0.28) (0.19) (0.26) (0.25)
N
1053 959 1015 868 873
Sex hormones (pg/mL) Sexual problemsd
Estradiolb Testosteroneb DHEAb
Hypoactive
sexual desirec Anorgasmiac Pain during
sexc Anhedoniac Anxiety about performancec
Religion (ref: other religion)
Conservative Christian -0.66 -18.78+ -16.79** 0.01 0.15 0.10 -2.87** 0.15 (1.09) (9.85) (5.07) (0.26) (0.45) (1.03) (0.97) (0.27)
N 935 891 907 712 698 710 710 706 Religion and subjective religiosity (ref: other religion) Conservative Christian, -0.30 -24.60* -23.48** 0.45^ 0.21 -14.58**^ -2.07*^ -0.41
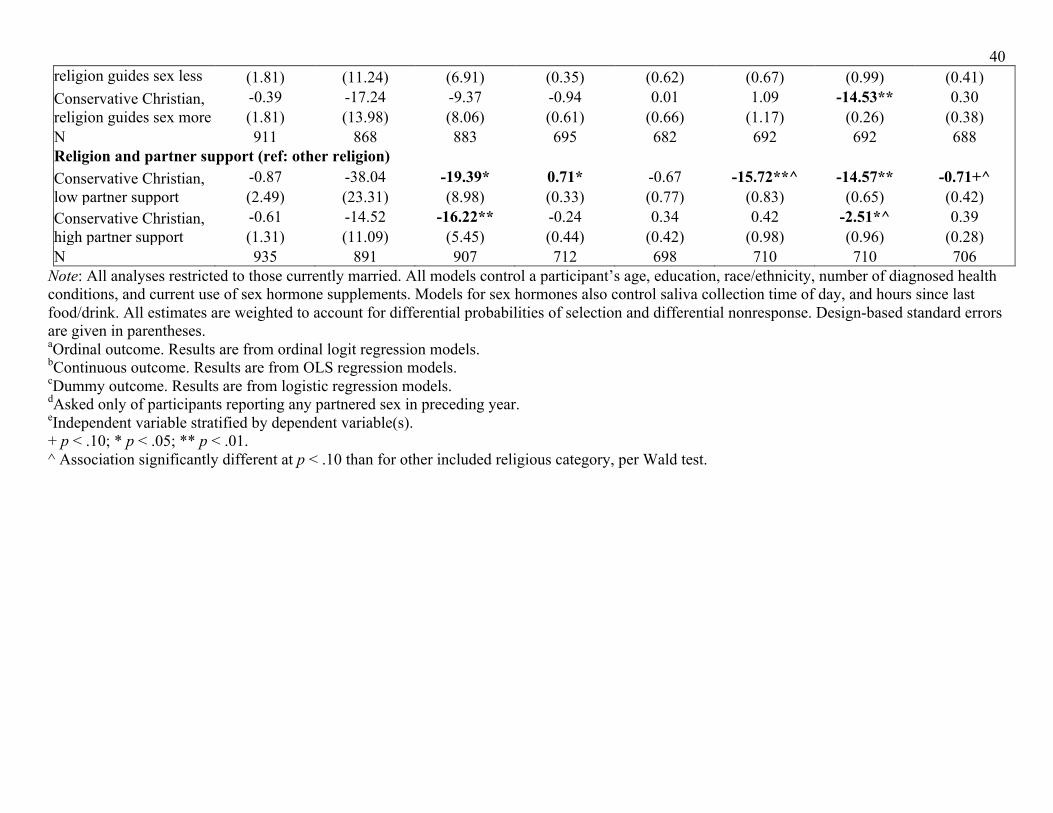
40 religion guides sex less (1.81) (11.24) (6.91) (0.35) (0.62) (0.67) (0.99) (0.41) Conservative Christian, religion guides sex more
-0.39 -17.24 -9.37 -0.94 0.01 1.09 -14.53** 0.30 (1.81) (13.98) (8.06) (0.61) (0.66) (1.17) (0.26) (0.38)
N 911 868 883 695 682 692 692 688 Religion and partner support (ref: other religion) Conservative Christian, low partner support
-0.87 -38.04 -19.39* 0.71* -0.67 -15.72**^ -14.57** -0.71+^ (2.49) (23.31) (8.98) (0.33) (0.77) (0.83) (0.65) (0.42)
Conservative Christian, high partner support
-0.61 -14.52 -16.22** -0.24 0.34 0.42 -2.51*^ 0.39 (1.31) (11.09) (5.45) (0.44) (0.42) (0.98) (0.96) (0.28)
N 935 891 907 712 698 710 710 706 Note: All analyses restricted to those currently married. All models control a participant’s age, education, race/ethnicity, number of diagnosed health conditions, and current use of sex hormone supplements. Models for sex hormones also control saliva collection time of day, and hours since last food/drink. All estimates are weighted to account for differential probabilities of selection and differential nonresponse. Design-based standard errors are given in parentheses. aOrdinal outcome. Results are from ordinal logit regression models. bContinuous outcome. Results are from OLS regression models. cDummy outcome. Results are from logistic regression models. dAsked only of participants reporting any partnered sex in preceding year. eIndependent variable stratified by dependent variable(s). + p < .10; * p < .05; ** p < .01. ^ Association significantly different at p < .10 than for other included religious category, per Wald test.