Effects of thyroid hormones on the heart
14
Clin Invest Arterioscl. 2014;26(6):296---309 www.elsevier.es/arterio REVIEW ARTICLE Effects of thyroid hormones on the heart Hernando Vargas-Uricoechea a,∗ , Anilsa Bonelo-Perdomo b , Carlos Hernán Sierra-Torres c a Division of Endocrinology and Metabolism, Internal Medicine Department, University of Cauca, Popayán-Cauca, Colombia b Division of Basic Immunology and Biomedical Sciences, University of Valle, Cali-Valle, Colombia c Division of Genetic and Molecular Epidemiology, University of Cauca, Popayán-Cauca, Colombia Received 14 June 2014; accepted 25 July 2014 Available online 22 October 2014 KEYWORDS Cardiovascular; Hyperthyroidism; Hypothyroidism; Subclinical dysfunction; Thyroid hormones; Heart; Atrial fibrillation; Thyrotoxicosis; Mortality Abstract Thyroid hormones have a significant impact on heart function, mediated by genomic and non-genomic effects. Consequently, thyroid hormone deficiencies, as well as excesses, are expected to result in profound changes in cardiac function regulation and cardiovascu- lar hemodynamics. Thyroid hormones upregulate the expression of the sarcoplasmic reticulum calcium-activated ATPase and downregulate the expression of phospholamban. Overall, hyper- thyroidism is characterized by an increase in resting heart rate, blood volume, stroke volume, myocardial contractility, and ejection fraction. The development of ‘‘high-output heart fail- ure’’ in hyperthyroidism may be due to ‘‘tachycardia-mediated cardiomyopathy’’. On the other hand, in a hypothyroid state, thyroid hormone deficiency results in lower heart rate and weaken- ing of myocardial contraction and relaxation, with prolonged systolic and early diastolic times. Cardiac preload is decreased due to impaired diastolic function. Cardiac afterload is increased, and chronotropic and inotropic functions are reduced. Subclinical thyroid dysfunction is rela- tively common in patients over 65 years of age. In general, subclinical hypothyroidism increases the risk of coronary heart disease (CHD) mortality and CHD events, but not of total mortality. The risk of CHD mortality and atrial fibrillation (but not other outcomes) in subclinical hyper- thyroidism is higher among patients with very low levels of thyrotropin. Finally, medications such as amiodarone may induce hypothyroidism (mediated by the Wolff---Chaikoff), as well as hyperthyroidism (mediated by the Jod---Basedow effect). In both instances, the underlying cause is the high concentration of iodine in this medication. © 2014 Sociedad Espa˜ nola de Arteriosclerosis. Published by Elsevier España, S.L.U. All rights reserved. Abbreviations: AIH, amiodarone-induced hypothyroidism; AIT, amiodarone-induced thyrotoxicosis; AF, atrial fibrillation; ANP, atrial natri- uretic peptide; CHD, coronary heart disease; T2, diiodothyronine; LV, left ventricular; RAAS, Renin---Angiotensin---Aldosterone system; rT3, reverse T3; SHyper, subclinical hyperthyroidism; SHypo, subclinical hypothyroidism; SCTD, subclinical thyroid dysfunction; TMC, tachycardia- mediated cardiomyopathy; TRs, thyroid hormone receptors; TREs, thyroid hormone response elements; TH, thyroid hormones; TSH, thyroid stimulating hormone; TRH, thyrotropin-releasing hormone; T4, thyroxine; T3, triiodothyronine. ∗ Corresponding author. E-mail address: [email protected] (H. Vargas-Uricoechea). http://dx.doi.org/10.1016/j.arteri.2014.07.003 0214-9168/© 2014 Sociedad Espa˜ nola de Arteriosclerosis. Published by Elsevier España, S.L.U. All rights reserved. Document downloaded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Transcript of Effects of thyroid hormones on the heart

C
R
E
H
a
b
c
RA
urms
h0
Document downloa
lin Invest Arterioscl. 2014;26(6):296---309
www.elsevier.es/arterio
EVIEW ARTICLE
ffects of thyroid hormones on the heart
ernando Vargas-Uricoecheaa,∗, Anilsa Bonelo-Perdomob, Carlos Hernán Sierra-Torresc
Division of Endocrinology and Metabolism, Internal Medicine Department, University of Cauca, Popayán-Cauca, ColombiaDivision of Basic Immunology and Biomedical Sciences, University of Valle, Cali-Valle, ColombiaDivision of Genetic and Molecular Epidemiology, University of Cauca, Popayán-Cauca, Colombia
eceived 14 June 2014; accepted 25 July 2014vailable online 22 October 2014
KEYWORDSCardiovascular;Hyperthyroidism;Hypothyroidism;Subclinicaldysfunction;Thyroid hormones;Heart;Atrial fibrillation;Thyrotoxicosis;Mortality
Abstract Thyroid hormones have a significant impact on heart function, mediated by genomicand non-genomic effects. Consequently, thyroid hormone deficiencies, as well as excesses,are expected to result in profound changes in cardiac function regulation and cardiovascu-lar hemodynamics. Thyroid hormones upregulate the expression of the sarcoplasmic reticulumcalcium-activated ATPase and downregulate the expression of phospholamban. Overall, hyper-thyroidism is characterized by an increase in resting heart rate, blood volume, stroke volume,myocardial contractility, and ejection fraction. The development of ‘‘high-output heart fail-ure’’ in hyperthyroidism may be due to ‘‘tachycardia-mediated cardiomyopathy’’. On the otherhand, in a hypothyroid state, thyroid hormone deficiency results in lower heart rate and weaken-ing of myocardial contraction and relaxation, with prolonged systolic and early diastolic times.Cardiac preload is decreased due to impaired diastolic function. Cardiac afterload is increased,and chronotropic and inotropic functions are reduced. Subclinical thyroid dysfunction is rela-tively common in patients over 65 years of age. In general, subclinical hypothyroidism increasesthe risk of coronary heart disease (CHD) mortality and CHD events, but not of total mortality.The risk of CHD mortality and atrial fibrillation (but not other outcomes) in subclinical hyper-thyroidism is higher among patients with very low levels of thyrotropin. Finally, medicationssuch as amiodarone may induce hypothyroidism (mediated by the Wolff---Chaikoff), as well ashyperthyroidism (mediated by the Jod---Basedow effect). In both instances, the underlying causeis the high concentration of iodine in this medication.
ded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
© 2014 Sociedad Espanola de Arteriosclerosis. Published by Elsevier España, S.L.U. All rightsreserved.
Abbreviations: AIH, amiodarone-induced hypothyroidism; AIT, amiodarone-induced thyrotoxicosis; AF, atrial fibrillation; ANP, atrial natri-retic peptide; CHD, coronary heart disease; T2, diiodothyronine; LV, left ventricular; RAAS, Renin---Angiotensin---Aldosterone system; rT3,everse T3; SHyper, subclinical hyperthyroidism; SHypo, subclinical hypothyroidism; SCTD, subclinical thyroid dysfunction; TMC, tachycardia-ediated cardiomyopathy; TRs, thyroid hormone receptors; TREs, thyroid hormone response elements; TH, thyroid hormones; TSH, thyroid
timulating hormone; TRH, thyrotropin-releasing hormone; T4, thyroxine; T3, triiodothyronine.∗ Corresponding author.
E-mail address: [email protected] (H. Vargas-Uricoechea).
ttp://dx.doi.org/10.1016/j.arteri.2014.07.003214-9168/© 2014 Sociedad Espanola de Arteriosclerosis. Published by Elsevier España, S.L.U. All rights reserved.

Effects of thyroid hormones 297
PALABRAS CLAVECardiovascular;Hipertiroidismo;Hipotiroidismo;Disfunción subclínica;Hormonas tiroideas;Corazón;Fibrilación auricular;Tirotoxicosis;Mortalidad
Efectos de las hormomas tiroideas en el corazón
Resumen Las Hormonas Tiroideas (HT) tienen un impacto significativo sobre la función car-diaca, el cual es mediado por efectos genómicos y no-genómicos. Como consecuencia, ladeficiencia y el exceso de las HT origina profundos cambios en la regulación de la funcióncardiaca y en algunos aspectos hemodinámicos y cardiovasculares. Las HT supra-regulan laexpresión de la ATPasa activada por calcio del retículo sarcoplasmático, e infra-regulan laexpresión de fosfolambán. En general, el hipertiroidismo se caracteriza por un incremento enla frecuencia cardiaca en reposo, del volumen sanguíneo, de la contractilidad miocárdica ydel volumen sistólico, entre otros. El desarrollo de ‘‘Falla cardiaca de alto gasto’’ en hiper-tiroidismo puede ser debido a ‘‘Cardiomiopatía mediada por taquicardia’’. Por otro lado; enel estado hipotiroideo, la deficiencia de HT origina bradicardia, debilidad en la contractilidady relajación miocárdica, con prolongación del tiempo sistólico y diastólico temprano. La dis-minución en la precarga se debe a las alteraciones en la función diastólica; la post-carga seincrementa, y las funciones cronotrópicas e inotrópicas están disminuidas. El hipotiroidismosubclínico incrementa el riesgo de mortalidad por Enfermedad Arterial Coronaria (EAC) y deeventos por EAC, pero no aumenta el riesgo de mortalidad total. El riesgo de mortalidad porEAC y de fibrilación auricular (pero no de otros resultados) en hipertiroidismo subclínico esmayor entre pacientes con niveles muy bajos de tirotropina. Finalmente, medicamentos comola amiodarona puede inducir hipotiroidismo (mediado por el efecto de Wolff-Chaikoff, ademásde hipertiroidismo (mediado por el efecto de Jod-Basedow. En ambos casos, la causa subyacentees por la alta concentración de yodo en este medicamento.© 2014 Sociedad Espanola de Arteriosclerosis. Publicado por Elsevier España, S.L.U. Todos losderechos reservados.
aTsaaprmpitsiRrTqfijcdThsaic
Document downloaded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Introduction
It is likely that all cells in the body are targets for thy-roid hormones (TH). Despite not being strictly necessaryfor life, TH have profound effects on many physiologic pro-cesses. Changes in thyroid status markedly influence cardiaccontractile and electrical activity; increased or reducedaction of TH on certain molecular pathways in the heart andvasculature causes relevant cardiovascular derangements.Receptors for TH are intracellular DNA-binding proteinsthat function as hormone-responsive transcription factors;TH enter cells through membrane transporter proteins.A number of plasma membrane transporters have beenidentified, some of which require ATP hydrolysis; onceinside the nucleus, the hormone binds to its receptor, andthe hormone-receptor complex interacts with specific DNAsequences in the promoter regions of responsive genes. Theeffect of DNA-binding of the hormone-receptor complex isto modulate gene expression, either by stimulating or inhib-iting transcription of specific genes. Cellular actions of THmay be initiated within the cell nucleus, at the plasma mem-brane, in cytoplasm and cytoskeleton, and in organelles;changes in gene expression caused by TH have a significanteffect on the contractile apparatus and the sarcoplasmicreticulum. Consequently, it is expected that TH excess ordeficit will be reflected in increased myocardial contractil-ity, heart rate, relaxation, arrhythmias and cardiac output
(in hyperthyroidism), and decreases in these parameters inhypothyroidism.Thyroid hormone nuclear receptors (TRs) mediate thebiological activities of T3 via transcriptional regulation,
vcfit
nd the genes that are transcriptionally regulated by3 are critical in the regulation of systolic and dia-tolic properties of the myocardium. T3 is the biologicallyctive thyroid hormone; it is mostly generated peripher-lly by 5′-monodeiodination of thyroxine (T4). TH have aro-angiogenic effect in adults and can stimulate arte-iolar growth in the normal heart as well as afteryocardial infarction. In presence of hyperthyroidism, thereload is increased; there is high cardiac output, withncreased heart rate, reduced peripheral vascular resis-ance and hyperdynamic circulation. The reduction inystemic vascular resistance is responsible for the decreasen renal perfusion pressure and for activation of theenin---Angiotensin---Aldosterone system (RAAS), with theesulting increase in sodium absorption and blood volume.he increased risk of cardiac mortality could be a conse-uence of the increased risk of arrhythmias, especially atrialbrillation (AF), and the risk of heart failure in these sub-ects. In presence of hypothyroidism, there are importanthanges in cardiac structure and function, with severityepending on the degree and the duration of TH deficiency.his state is characterized by low cardiac output, decreasedeart rate and stroke volume, reduction in systolic and dia-tolic functions; there is also a decline in cardiac preloadnd blood volume, as well as a drop in renal perfusion withmpaired free water clearance and hyponatremia. The lowardiac output is caused by bradycardia and a reduction in
entricular filling and cardiac contractility. Systemic vas-ular resistance may increase, and diastolic relaxation andlling are slow. An increase in cardiovascular risk and mor-ality has also been described.
2
Mc
TfrmtThbrdtttasctabThltrroTaapcattbpriitil
pabwtltwtao
moT
tetiicTetTf
wTohleilo
attap
emeapattp
ogTtts
htrT
aat
cfc
Document downloaded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
98
echanisms of TH action on theardiovascular system
H play a key role in energy homeostasis. The set pointor TH production and secretion by the thyroid gland isegulated by the hypothalamic thyrotropin-releasing hor-one (TRH), determining the equilibrium between serum
hyroid stimulating hormone (TSH) and TH concentrations.1,2
he major form of TH produced by the thyroid is the pro-ormone thyroxine (T4) which can be converted into theiologically active tri-iodothyronine (T3) mediated by theemoval of an iodide by deiodinases (the iodothyronineeiodinases constitute a family of selenoenzymes that selec-ively remove iodide from thyroxine and its derivatives,hus activating or inactivating these hormones which have aissue-specific distribution). All deiodinases are membrane-nchored proteins of 29---33 kDa that share substantialequence homology, catalytic properties and contain seleno-ysteine as the key residue within their catalytic centers;hey catalyze and sequentially remove stereo-specific iodinetoms from T4, generating active and inactive isomers ofoth T3 and diiodothyronine (T2). The deiodination of T4,3, and other iodothyronines is an integral component of THomeostasis.3,4 There are three deiodinases: Type 1 (D1),ocalized to the plasma membrane and expressed in liver,hyroid and kidney, it catalyzes removal of inner or outering iodine atoms in equimolar proportions to generate T3,everse T3 (rT3), or T2, depending on the substrate. Mostf the circulating T3 is derived from conversion of T4 to3 by the actions of D1. Type 2 (D2), which is consider-bly more efficient than D1, catalyzes only the removal ofn outer ring iodine atom from T4, generating the activeroduct T3. The major role of D2 is to control the intra-ellular T3 concentration, its availability to the nucleus,nd the saturation of the nuclear T3 receptor in targetissues; it is mainly active in brain, pituitary, and skele-al muscle. And Type 3 (D3), which is expressed in therain and other tissues; it irreversibly inactivates T3, orrevents activation of T4 by catalyzing removal of an innering iodine atom to generate T2 or rT3, respectively. Thus,nactivating D3 prevents TH access to specific tissues at crit-cal times and reduces TH receptors (TRs) saturation. Givenhese functions, D3 is considered the major physiologicalnactivator and terminator of TH action at the peripheralevel.5,6
TH signaling is a local phenomenon, with target cellslaying a major role through restricted expression of thectivating or inactivating deiodinases. This local role playedy the deiodinases in customizing TH signaling is the mainay in which TH exert its metabolic effects. Although the
hyroid gland produces predominantly T4, the primary bio-ogically active form of the hormone is T3, which bindso, and activates, the TRs. TRs homodimerize or interactith other nuclear receptors such as the retinoic X recep-
or and control essential functions in growth, developmentnd metabolism, and are important for normal functioningf almost all tissues.
TRs are transcription factors that bind to thyroid hor-one response elements (TREs) in the regulatory regions
f target genes. TRs are encoded by two genes, THRA andHRB, located on chromosomes 17 and 3, respectively.
oos
H. Vargas-Uricoechea et al.
T3, the active form of TH, exerts many of its actionshrough its TRs: TR�1, TR�2, TR�1, and TR�2. TRs, with thexception of TR�2, are expressed in all tissues and the pat-ern of expression varies in different types of tissues. TR�1s predominantly expressed in the myocardium and regulatesmportant genes related to cell differentiation and growth,ontractile function, pacemaker activity, and conduction.he three major TRs isoforms, TR�1, TR�1, and TR�2, arexpressed in a tissue-specific fashion and regulate a spec-rum of metabolic and developmental functions; moreover,Rs are members of the nuclear receptor superfamily andunction as T3-inducible transcription factors.7,8
The TRs are highly homologous transcription factorshich transduce signals of active forms of TH (especially3). Like other nuclear receptors, TRs bind TREs comprisedf degenerate repeats of the sequence AGGTCA, usually aseterodimers with retinoid X receptors (RXRs). From theseocations, the TRs recruit co-regulator complexes that influ-nce gene expression, and T3 modulates transcription bynducing conformational changes in the receptor C-terminaligand binding domain which, in turn, alters the complementf TR associated co-regulators.
The selective actions of TRs are influenced by local ligandvailability, by transport of TH into the cell by relatedransporters, by the relative expression and distribution ofhe TR isoforms and nuclear receptor co-repressors and co-ctivators; and, finally, by the sequence, arrangement, andromoter context of the TREs.
TH binds to serum transport proteins that help ensureven delivery of hormone to all tissues, cell type-specificembrane transporters, cytoplasmic interacting proteins,
nzymes that variously activate pro-hormones or inactivatective hormones, and the TRs themselves. TH interactingroteins regulate important steps that dictate hormonevailability for the intracellular receptor, so it is very impor-ant to understand structure activity relationships of TH inhe context of both the receptor and the proteins that com-rise the entire signaling system.
TH acts in large part by binding to nuclear TRs. Bindingf the T3 ligand to the TRs results, for a great majority ofenes, in their increased transcription. In the absence of the3 ligand, TRs can repress the expression of genes leadingo gene silencing. The communication between the TH andhe basal transcription machinery occurs through a complexet of co-activators and co-repressors.9,10
The ligand-activated TRs recruit co-activators, whichave a positive stimulatory interaction with the basicranscriptional machinery. In contrast, recruitment of TH-elated co-repressors leads to decreased transcription ofH-responsive genes.
The mediation of nuclear T3 receptor-based TH action is complex process which is influenced by TH concentrationnd the level and type of the TR alpha and beta isoforms;he configuration of the TREs also influences TH action.
The important role of interactions with co-repressors ando-activators, and the interactions with cell type-specificactors, lead to changes in the histone acetylation status ofhromatin.
Besides the well-characterized genomic action (nuclear)f TH, mediated by TRs, the non-genomic action of TH isften related to activation of signaling pathways. The clas-ical genomic actions of T3 are mediated by high-affinity
Effects of thyroid hormones 299
T3-T4
T3
T3
TR
Protein
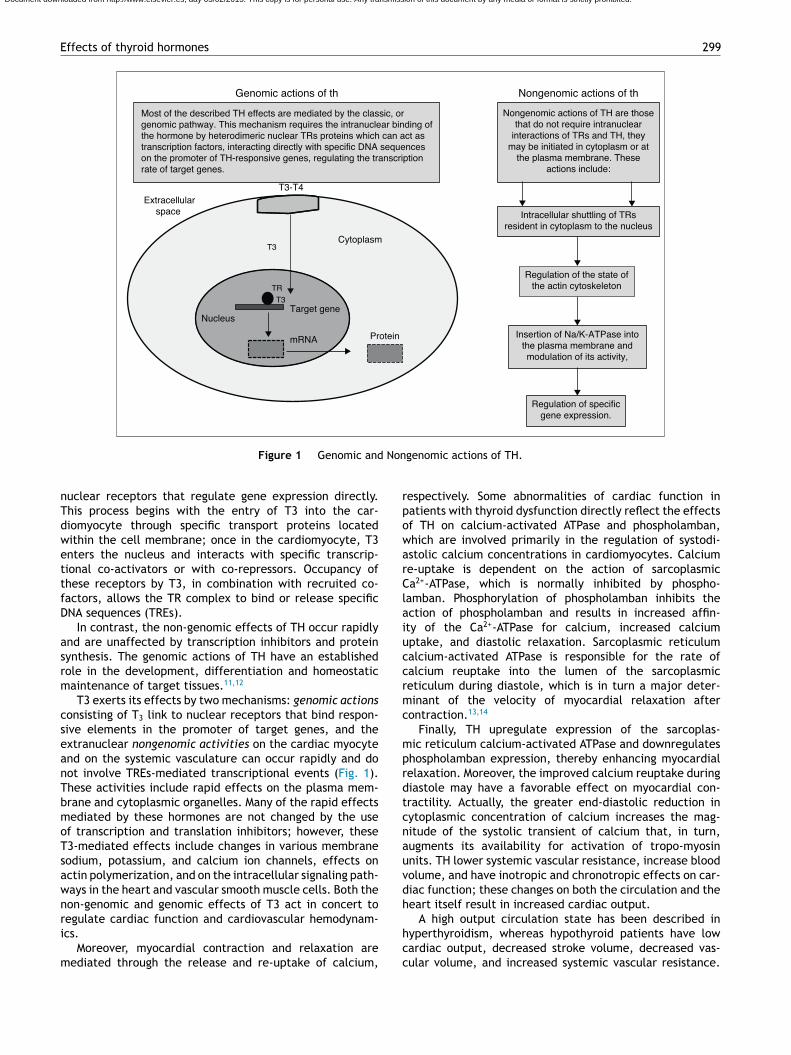
Genomic actions of th
Most of the described TH effects are mediated by the classic, orgenomic pathway. This mechanism requires the intranuclear binding ofthe hormone by heterodimeric nuclear TRs proteins which can act astranscription factors, interacting directly with specific DNA sequenceson the promoter of TH-responsive genes, regulating the transcriptionrate of target genes.
Nongenomic actions of TH are thosethat do not require intranuclear
interactions of TRs and TH, theymay be initiated in cytoplasm or at
the plasma membrane. Theseactions include:
Intracellular shuttling of TRsresident in cytoplasm to the nucleus
Regulation of specificgene expression.
Cytoplasm
Extracellularspace
Target geneNucleus
mRNA
Nongenomic actions of th
Insertion of Na/K-ATPase intothe plasma membrane andmodulation of its activity,
Regulation of the state ofthe actin cytoskeleton
Non
rpowarClaiuccrmc
mprdtcnauvdh
Document downloaded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Figure 1 Genomic and
nuclear receptors that regulate gene expression directly.This process begins with the entry of T3 into the car-diomyocyte through specific transport proteins locatedwithin the cell membrane; once in the cardiomyocyte, T3enters the nucleus and interacts with specific transcrip-tional co-activators or with co-repressors. Occupancy ofthese receptors by T3, in combination with recruited co-factors, allows the TR complex to bind or release specificDNA sequences (TREs).
In contrast, the non-genomic effects of TH occur rapidlyand are unaffected by transcription inhibitors and proteinsynthesis. The genomic actions of TH have an establishedrole in the development, differentiation and homeostaticmaintenance of target tissues.11,12
T3 exerts its effects by two mechanisms: genomic actionsconsisting of T3 link to nuclear receptors that bind respon-sive elements in the promoter of target genes, and theextranuclear nongenomic activities on the cardiac myocyteand on the systemic vasculature can occur rapidly and donot involve TREs-mediated transcriptional events (Fig. 1).These activities include rapid effects on the plasma mem-brane and cytoplasmic organelles. Many of the rapid effectsmediated by these hormones are not changed by the useof transcription and translation inhibitors; however, theseT3-mediated effects include changes in various membranesodium, potassium, and calcium ion channels, effects onactin polymerization, and on the intracellular signaling path-ways in the heart and vascular smooth muscle cells. Both thenon-genomic and genomic effects of T3 act in concert to
regulate cardiac function and cardiovascular hemodynam-ics.Moreover, myocardial contraction and relaxation aremediated through the release and re-uptake of calcium,
hcc
genomic actions of TH.
espectively. Some abnormalities of cardiac function inatients with thyroid dysfunction directly reflect the effectsf TH on calcium-activated ATPase and phospholamban,hich are involved primarily in the regulation of systodi-stolic calcium concentrations in cardiomyocytes. Calciume-uptake is dependent on the action of sarcoplasmica2+-ATPase, which is normally inhibited by phospho-
amban. Phosphorylation of phospholamban inhibits thection of phospholamban and results in increased affin-ty of the Ca2+-ATPase for calcium, increased calciumptake, and diastolic relaxation. Sarcoplasmic reticulumalcium-activated ATPase is responsible for the rate ofalcium reuptake into the lumen of the sarcoplasmiceticulum during diastole, which is in turn a major deter-inant of the velocity of myocardial relaxation after
ontraction.13,14
Finally, TH upregulate expression of the sarcoplas-ic reticulum calcium-activated ATPase and downregulateshospholamban expression, thereby enhancing myocardialelaxation. Moreover, the improved calcium reuptake duringiastole may have a favorable effect on myocardial con-ractility. Actually, the greater end-diastolic reduction inytoplasmic concentration of calcium increases the mag-itude of the systolic transient of calcium that, in turn,ugments its availability for activation of tropo-myosinnits. TH lower systemic vascular resistance, increase bloodolume, and have inotropic and chronotropic effects on car-iac function; these changes on both the circulation and theeart itself result in increased cardiac output.
A high output circulation state has been described inyperthyroidism, whereas hypothyroid patients have lowardiac output, decreased stroke volume, decreased vas-ular volume, and increased systemic vascular resistance.

300 H. Vargas-Uricoechea et al.
Table 1 Cardiac and hemodynamic consequences of hyperthyroidism.
Reduction of the systemic vascular resistance Increase in cardiac outputDecrease in renal perfusion Increase in heart rateDecrease in diastolic arterial pressure Increase in pulse amplitudeDecrease in afterload Increase in stroke volumeImprovement in diastolic relaxation Increase in PNA secretionPeripheral vasodilatation Increase in blood volumeTachyarrhythmias Increase in preloadAlteration of cardiomyofibril contractility Increase in renal blood flowConcentric cardiac hypertrophy Increase in systolic arterial pressurePremature trial heart beats Increase in myocardial contractilityLow interatrial difference of action potential duration Increase in LV systolic functionReduced functional cardiac reserve and physical load tolerance Increase of end-diastolic left ventricular volumePulmonary hypertension Increase of number of �1-adrenoreceptorsDelay in intraventricular conduction Increased risk of total mortalityProlongation in intra-atrial conduction Increased risk of cardiovascular disease
Tuhcpcctban
icmfcrccees
A
Document downloaded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Increase in sympathetic tone
hese alterations in cardiac function mediated by TH dependltimately on the regulation of target genes within theeart and on indirect effects resulting from hemodynamichanges. Moreover, TH play an important role in bloodressure (BP) control but may exert other effects on theardiovascular system; both hypo and hyperthyroidism mayause cardiovascular dysfunction, increase the response ofissues to the action of the sympathetic system, and this maye a mechanism by which they regulate BP. However, TH canlso activate the RAAS without involving the sympatheticervous system.
A number of cardiovascular changes have been describedn thyroid dysfunction, and the right treatment for theondition has shown to be of great benefit. The heart is aajor target for TH action, and thyroid dysfunction has pro-
ound effects on the heart and cardiovascular system, i.e.,hanges in cardiac gene expression in the contractile appa-atus, the sarcoplasmic reticulum, and the outer myocyticell membrane. The positive inotropic, dromotropic, andhronotropic heart rates are also increased by TH, and theseffects are associated with greater sensitivity of adren-rgic and cardiac receptors, as well as increased myosinynthesis.15,16
. In the hyperthyroid state, TH modulate every com-ponent of the cardiovascular system necessary fornormal cardiovascular development and function. ExcessTH have pronounced cardiovascular manifestations(Table 1). Overall, hyperthyroidism is characterized byan increase in resting heart rate (at least half thepatients with hyperthyroidism have sinus tachycardiaexceeding 100 beats/min) blood volume, stroke volume,myocardial contractility and ejection fraction, and animprovement in diastolic relaxation. An increase in THlevel induces resting tachycardia, palpitations are oneof the most-common symptoms associated with overthyperthyroidism, and about 20% of hyperthyroid patients
overall have AF. Since symptoms of hyperthyroidism areoften non-specific and develop slowly, the latter maybe the first clinical manifestation of thyroid dysfunc-tion; and this arrhythmia increases the risk of blood clotIncreased risk for heart failure events
formation inside the heart, with embolism and strokeif there is clot dislodgment.17,18 The AF is usually per-sistent rather than paroxysmal, and is more probablein older patients --- perhaps reflecting a reduction inthe threshold for this arrhythmia with age. Pulse pres-sure is widened, cardiac output and sympathetic toneare increased, and a hyperkinetic apex beat and a loudfirst heart sound are described; in addition, an accen-tuated pulmonic component of the second sound canbe noticed frequently. The increase in chronotropismand batmotropism is probably caused by imbalancedsympathovagal tone due to a relative rather than anabsolute adrenergic overdrive. Alterations in the pulseand heart sounds are common, as is also the case withthe Means---Lerman ‘‘scratch’’ (mid-systolic and end-tidal murmur heard at the left upper sternal borderthought to occur from rubbing of the pericardium againstthe pleura, which may sound like a pericardial frictionrub as seen in pericarditis). Left ventricular (LV) systolicfunction is consistently increased at rest and the rateof LV chamber relaxation and LV filling is increased.19,20
Additionally, systolic arterial pressure is increased anddiastolic arterial pressure is decreased, so that pulsepressure is particularly wider and mean arterial pres-sure is usually decreased, with a remarkable increasein cardiac output and a notable reduction in periph-eral vascular resistance. However, hyperthyroidism hasonly minor effects on mean arterial blood pressure,because of increases in systolic pressure --- caused byincreased stroke volume --- and decreases in diastolicpressure due to peripheral vasodilatation. The periph-eral vascular effects result from a TH-mediated decreasein systemic peripheral resistance, induced by dilatingarterioles and by increased metabolic rate in peripheraltissues. As a rule, the total peripheral vascular resis-tance decreases in thyrotoxicosis, and these alterationsmay be mediated by changes in non-thyroid hormones
21,22
which affect the vasculature. Even though in thyro-toxicosis plasma catecholamines are unchanged or low,the �-adrenergic receptor density is altered in a time-and tissue-dependent manner, raising tissue sensitivity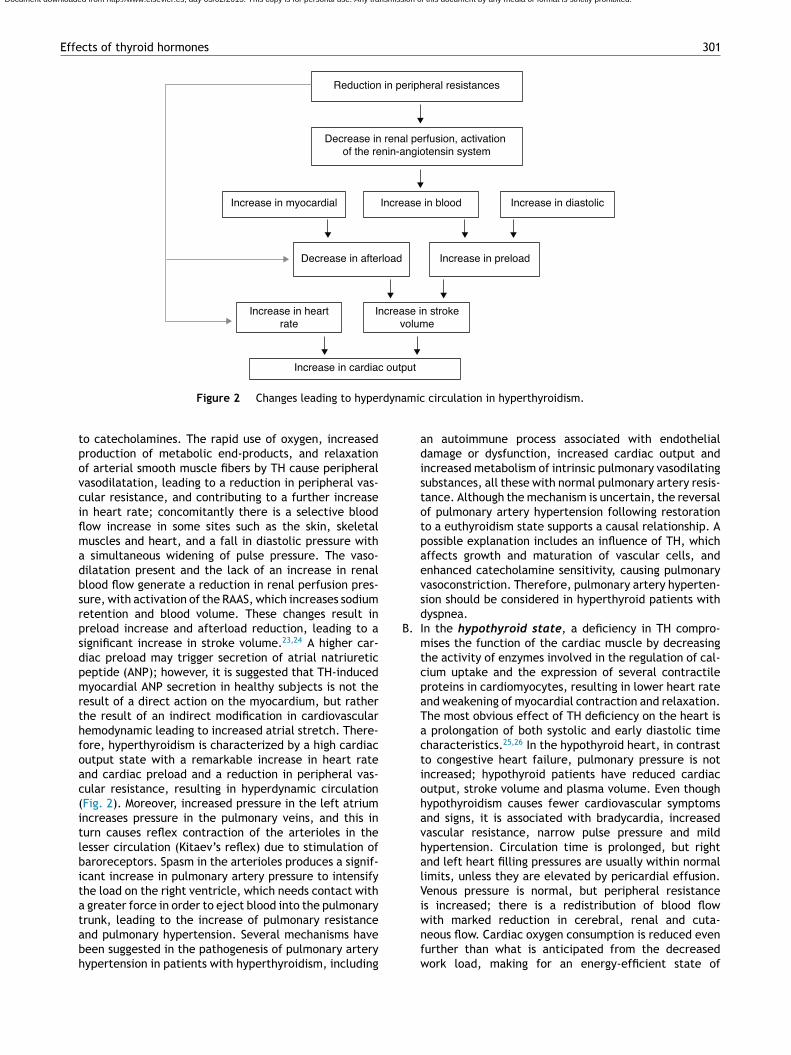
Effects of thyroid hormones 301
Reduction in peripheral resistances
Decrease in renal perfusion, activation of the renin-angiotensin system
Increase in myocardial Increase in blood Increase in diastolic
Decrease in afterload Increase in preload
Increase in heartrate
Increase in strokevolume
Increase in cardiac output
dyna
B
Document downloaded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Figure 2 Changes leading to hyper
to catecholamines. The rapid use of oxygen, increasedproduction of metabolic end-products, and relaxationof arterial smooth muscle fibers by TH cause peripheralvasodilatation, leading to a reduction in peripheral vas-cular resistance, and contributing to a further increasein heart rate; concomitantly there is a selective bloodflow increase in some sites such as the skin, skeletalmuscles and heart, and a fall in diastolic pressure witha simultaneous widening of pulse pressure. The vaso-dilatation present and the lack of an increase in renalblood flow generate a reduction in renal perfusion pres-sure, with activation of the RAAS, which increases sodiumretention and blood volume. These changes result inpreload increase and afterload reduction, leading to asignificant increase in stroke volume.23,24 A higher car-diac preload may trigger secretion of atrial natriureticpeptide (ANP); however, it is suggested that TH-inducedmyocardial ANP secretion in healthy subjects is not theresult of a direct action on the myocardium, but ratherthe result of an indirect modification in cardiovascularhemodynamic leading to increased atrial stretch. There-fore, hyperthyroidism is characterized by a high cardiacoutput state with a remarkable increase in heart rateand cardiac preload and a reduction in peripheral vas-cular resistance, resulting in hyperdynamic circulation(Fig. 2). Moreover, increased pressure in the left atriumincreases pressure in the pulmonary veins, and this inturn causes reflex contraction of the arterioles in thelesser circulation (Kitaev’s reflex) due to stimulation ofbaroreceptors. Spasm in the arterioles produces a signif-icant increase in pulmonary artery pressure to intensifythe load on the right ventricle, which needs contact witha greater force in order to eject blood into the pulmonary
trunk, leading to the increase of pulmonary resistanceand pulmonary hypertension. Several mechanisms havebeen suggested in the pathogenesis of pulmonary arteryhypertension in patients with hyperthyroidism, includingmic circulation in hyperthyroidism.
an autoimmune process associated with endothelialdamage or dysfunction, increased cardiac output andincreased metabolism of intrinsic pulmonary vasodilatingsubstances, all these with normal pulmonary artery resis-tance. Although the mechanism is uncertain, the reversalof pulmonary artery hypertension following restorationto a euthyroidism state supports a causal relationship. Apossible explanation includes an influence of TH, whichaffects growth and maturation of vascular cells, andenhanced catecholamine sensitivity, causing pulmonaryvasoconstriction. Therefore, pulmonary artery hyperten-sion should be considered in hyperthyroid patients withdyspnea.
. In the hypothyroid state, a deficiency in TH compro-mises the function of the cardiac muscle by decreasingthe activity of enzymes involved in the regulation of cal-cium uptake and the expression of several contractileproteins in cardiomyocytes, resulting in lower heart rateand weakening of myocardial contraction and relaxation.The most obvious effect of TH deficiency on the heart isa prolongation of both systolic and early diastolic timecharacteristics.25,26 In the hypothyroid heart, in contrastto congestive heart failure, pulmonary pressure is notincreased; hypothyroid patients have reduced cardiacoutput, stroke volume and plasma volume. Even thoughhypothyroidism causes fewer cardiovascular symptomsand signs, it is associated with bradycardia, increasedvascular resistance, narrow pulse pressure and mildhypertension. Circulation time is prolonged, but rightand left heart filling pressures are usually within normallimits, unless they are elevated by pericardial effusion.Venous pressure is normal, but peripheral resistanceis increased; there is a redistribution of blood flow
with marked reduction in cerebral, renal and cuta-neous flow. Cardiac oxygen consumption is reduced evenfurther than what is anticipated from the decreasedwork load, making for an energy-efficient state of
302 H. Vargas-Uricoechea et al.
Table 2 Cardiovascular and hemodynamic changes in a hypothyroid state.
Narrow pulse pressure Decrease in stroke volumeIncrease in diastolic arterial pressure Decrease in preloadAtrioventricular blocks Decrease in blood volumePeripheral vasoconstriction Decrease in cardiac outputVentricular tachyarrhythmias, because of bradycardia and
hypothermiaReduction in exercise tolerance
Pericarditis Reduction in myocardial contractilityPericardial tamponade BradycardiaNegative chronotropic and inotropic state Increased risk for all-cause mortality and
Cardiovascular disease deathProlongation of the QT interval Increased risk for heart failure eventsImpaired Left Ventricular systolic synchronization Increase in peripheral vascular resistancesProlongation of the isovolumetric relaxation time Decrease in LV systolic functionFlattened or inverted T waves Right bundle branch blockIncrease in the QT dispersion Increase in arterial stiffness
Document downloaded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Decreased amplitude of p wave
cardiac contraction. However, congestive heart failurehas been described in severely hypothyroid patientswithout underlying heart disease. Measurements of iso-volumetric relaxation time reveal a prolongation ofthis interval.27,28 In addition, there is prolongation ofthe pre-ejection period and an increased pre-ejectionperiod to LV ejection time ratio (Table 2). Myocar-dial work efficiency is lower in normal subjects thanother sick persons. Angina pectoris, diastolic hyper-tension, atrioventricular blocks, and pericarditis aremajor cardiovascular complications in a hypothyroidstate. Diastolic dysfunction both at rest and on exer-tion is the most uniformly found cardiac abnormalityin patients with hypothyroidism; LV diastolic functionis altered, with a slowed myocardial relaxation andimpaired early ventricular filling. This is frequentlyassociated with a fluctuating impairment in LV systolicfunction even at a very early stage. LV asynchrony isdefined as deterioration of the simultaneous contrac-tion of corresponding cardiac segments; as a result,delayed activation of some ventricular segments leadsto uncoordinated contraction. LV asynchrony may affectdiastolic and systolic functions, exercise capacity, prog-nosis, quality of life, and symptoms of heart failure,worsening the heart failure. LV systolic function ismarginally subnormal, with slightly lower ejection frac-tion and stroke volume values.29,30 Preload is reduced,with a subnormal cardiac output. High cholesterol lev-els are an additional risk for the development ofatherosclerosis. Alterations in the pulse and peripheralvasoconstriction may be observed, such as prolonga-tion of the QRS complex and the QT interval (theQT interval reflects traditional electrocardiographicparameter of the duration of ventricular repolariza-tion) with an increased risk of developing ventriculartachyarrhythmias. QT dispersion is the inter-lead vari-ability of the QT interval on surface electrocardiogram,
reflecting regional variations in myocardial repolariza-tion. Increased QT dispersion has been linked to theoccurrence of malignant ventricular arrhythmias andsudden cardiac death; clinical observations show thatLeft ventricular posterior wall thickness
ventricular arrhythmias and sudden death are uncom-mon in hypothyroidism, despite the marked prolongationof the QT interval. However, increased QT dispersionin hypothyroidism may facilitate ventricular arrhythmiaswith hypokalemia, hypomagnesemia, long QT syndrome,and sudden cardiac death.
Other findings are: incomplete or complete right bun-dle branch block, decreased p wave amplitude, diffuseflattening or inversion of T waves together with a gen-eralized low voltage of all the complexes. The T wave isdome-shaped and partially obliterates the ST segment(‘‘the mosque sign’’). Isolated myxedema may causeheart failure, pericardial effusion (PE) and pericardialtamponade (PT), especially in subjects with profoundT4 deprivation; PE in hypothyroidism is common and themechanisms of myxedematous PE are increased perme-ability of capillaries with subsequent leakage of proteinrich fluid into the interstitial space, impaired lymphaticdrainage, and salt and water retention; nevertheless, aneffusion which causes cardiac tamponade is rarely seen.PT in hypothyroid patients with PE is attributed to theslow accumulation of fluid and the remarkable compli-ance of the pericardium.
The heart in overt myxedema is often flabby, andgrossly dilated. Classic findings of overt myxedema are:cardiac enlargement, dilatation, significant bradycardia,weak arterial pulses, hypotension, distant heart sounds,low EKG voltage, non-pitting edema and evidence of con-gestive heart failure.
There is a relationship between hypothyroidism andcoronary artery disease, either because of the pres-ence of a negative chronotropic and inotropic state orthe presence of hypercholesterolemia and hypertension,with an increased risk of atherogenesis; but otherwise,thyroid hormones are powerful regulators of vascula-ture in the adult myocardium; therefore, a low free T3state would inhibit neovascularization in cardiac tissue
after acute myocardial infarction, which would accel-erate cardiac pathologic remodeling and heart failure,leading to short-term and long-term adverse cardiacevents.31,32
hidOfmh>dpdmoboccacc
ooissb
drt(mrotension, and diastolic dysfunction. It is not known whethercardiomyopathy in hyperthyroidism is secondary to directtoxic effects of excess thyroid hormone, whether it resultsfrom the hyperdynamic or high-output stress caused by the
TH excess(hyperthyroidism)
Document downloaded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Effects of thyroid hormones
Special considerations
Heart failure in hyperthyroidism
Besides its metabolic and thermoregulatory tissue effects,TH regulate cardiac performance by acting on the heartand vascular system. Hyperthyroid patients can manifestfindings of congestive heart failure in the absence of priorcardiac injury. Diastolic and systolic functions are clearlymodified by TH; ventricular contractile function is alsoaltered by changes in the hemodynamic pattern, secondaryto TH effects on peripheral vascular tone. TH equilibriumpreserves positive ventricular---arterial coupling, leadingto an adequate balance for cardiac work. Hemodynamicalterations due to hyperthyroidism decrease myocardialcontractile reserve and do not allow further increases inejection fraction and cardiac output on exertion, prob-ably because of the inability to reduce the already lowperipheral vascular resistance, while constriction of venousvessels increases. The resulting decrease in peripheral vas-cular resistance activates the RAAS, leading to retention ofsodium and fluid.33,34
The forced increase in preload and total blood volumeincreases cardiac work and stimulates the development ofmyocardial hypertrophy. However, the increase in preloadand blood volume leads to a rise in ventricular filling pres-sure, and to a moderate degree of pulmonary and peripheralcongestion. Cardiac output is augmented by a higher heartrate and increased stroke volume, facilitating the returnof blood to the heart. These changes result in increasedmean circulatory filling pressure, which promotes retro-grade blood flow to the right atrium. However, TH alsoincrease erythropoiesis, and the net effect is an increasein total blood volume and stroke volume.
The transcriptional effects lead to increased contractilitythrough effects on the release and uptake of sarcoplasmicreticular calcium and phosphorylation of phospholamban.The non-transcriptional effects are induced by the effectof TH on various ion channels.35,36 All these cardiac effects,along with low peripheral vascular resistance and increasein total blood volume, lead to a high cardiac outputstate (often called ‘‘high-output heart failure’’). However,
‘‘heart failure’’ is not really the appropriate term becausecardiac output is increased, although congestive circula-tion is present (Table 3). The tachycardia observed inTable 3 Characteristics that define ‘‘high-output heartfailure’’ in hyperthyroidism.
Persistent tachycardia Decrease in peripheralvascular resistance
Increase in cardiac preload Increase in ventricularfilling pressure
Increase in pulmonaryarterial pressure
Increase in total bloodvolume
Absence of underlying heartdisease
Increase in activity of thesympatho-adrenal systemand increase in cardiactissue responsiveness tocatecholamines
303
yperthyroidism appears to be due to a combination ofncreased rate of diastolic depolarization and decreaseduration of the action potential in the sinoatrial nodal cells.n the other hand, the development of ‘‘high-output heart
ailure’’ in hyperthyroidism may be due to ‘‘tachycardia-ediated cardiomyopathy’’ (TMC). A high cardiac output
as been described as being 8 L/min or a cardiac index3.9 L/min/m2. TMC is defined as secondary ventricularysfunction due to chronic tachycardia, which is fully orartially recoverable after heart rate normalization. Theiagnosis should be suspected in patients with compro-ised ventricular function in the course of a ventricular
r supraventricular tachycardia. The diagnosis can onlye established with the recovery of ventricular functionnce the tachycardia and the thyrotoxic state are underontrol.37,38 While TMC usually presents with significantardiac enlargement, reduced ventricular wall thickness,nd impaired ventricular contraction similar to dilatedardiomyopathy, the cardiac abnormalities normalize withontrol of the tachyarrhythmia and heart failure.
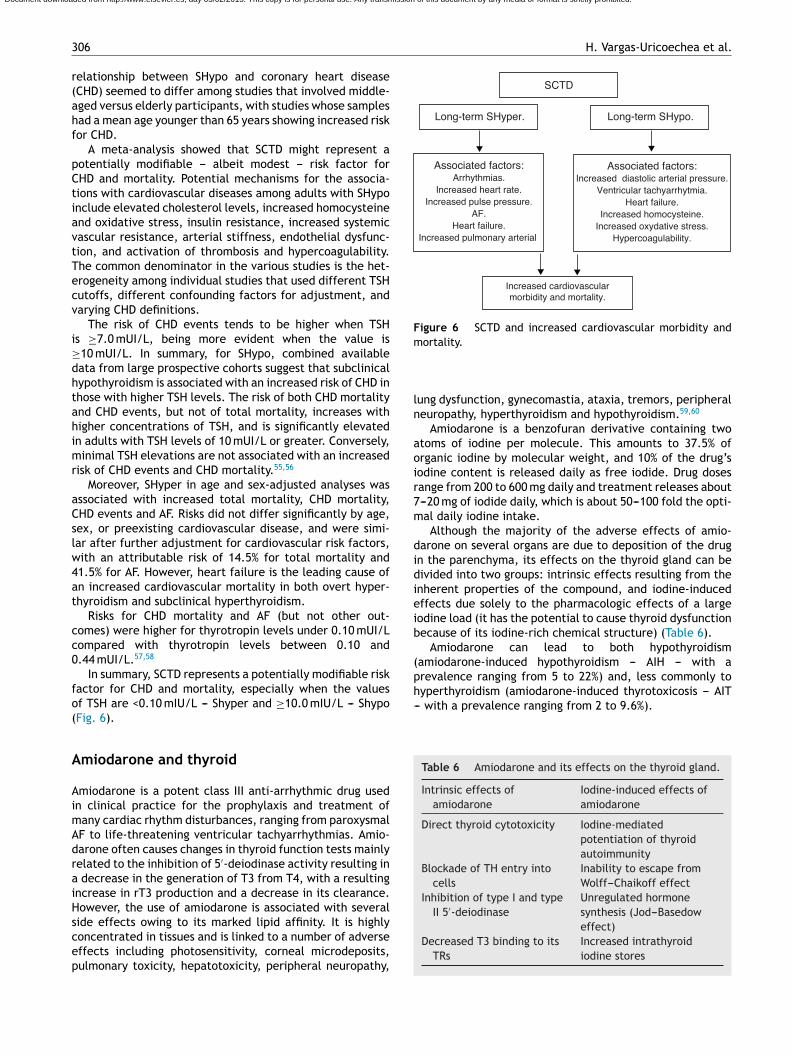
Actually, it has been proposed that cardiovascular effectsf hyperthyroidism, i.e., tachycardia, increased cardiacutput, systolic hypertension, and myocardial contractil-ty are the result, not only of increased activity of theympatho-adrenal system, but also of increased cardiac tis-ue responsiveness to catecholamines, with upregulation ofeta adrenergic receptors (Figs. 3 and 5).
The term ‘‘thyrotoxic cardiomyopathy’’ defines myocar-ial damage caused by the toxic effects of abundant TH,esulting in altered energy production by myocytes (oxida-ive phosphorylation, glycolysis), intracellular metabolismprotein synthesis) and myofibril contractile function. Theain manifestations are left ventricular hypertrophy, heart
hythm disturbances --- usually, atrial fibrillation --- dilationf the heart chambers and heart failure, pulmonary hyper-
Decreased systemic vascular resistance
Decreased effective arterial filling volume
Increased renal sodium reabsorption and blood
Increased cardiac inotropyand chronotropy
Increased cardiac output
Figure 3 Increase in cardiac output mediated by TH excess.
304
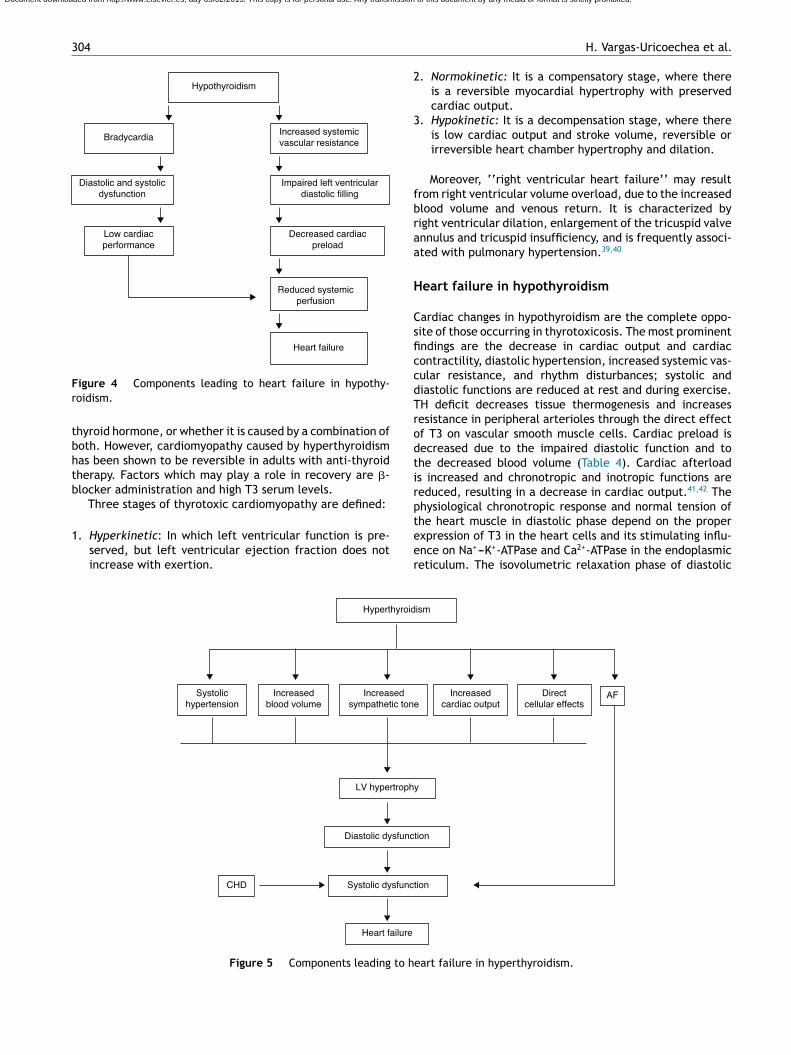
Hypothyroidism
BradycardiaIncreased systemicvascular resistance
Diastolic and systolicdysfunction
Impaired left ventriculardiastolic filling
Low cardiacperformance
Decreased cardiacpreload
Reduced systemicperfusion
Heart failure
Fr
tbhtb
1
2
3
fbraa
H
CsficcdTrodtirp
Document downloaded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
igure 4 Components leading to heart failure in hypothy-oidism.
hyroid hormone, or whether it is caused by a combination ofoth. However, cardiomyopathy caused by hyperthyroidismas been shown to be reversible in adults with anti-thyroidherapy. Factors which may play a role in recovery are �-locker administration and high T3 serum levels.
Three stages of thyrotoxic cardiomyopathy are defined:
. Hyperkinetic: In which left ventricular function is pre-served, but left ventricular ejection fraction does notincrease with exertion.
teer
Heart failure
Systolic dysfunc
Diastolic dysfunc
LV hypertroph
CHD
Increasedsympathetic ton
Increasedblood volume
Systolichypertension
Hyperthyroid
Figure 5 Components leading to h
H. Vargas-Uricoechea et al.
. Normokinetic: It is a compensatory stage, where thereis a reversible myocardial hypertrophy with preservedcardiac output.
. Hypokinetic: It is a decompensation stage, where thereis low cardiac output and stroke volume, reversible orirreversible heart chamber hypertrophy and dilation.
Moreover, ‘‘right ventricular heart failure’’ may resultrom right ventricular volume overload, due to the increasedlood volume and venous return. It is characterized byight ventricular dilation, enlargement of the tricuspid valvennulus and tricuspid insufficiency, and is frequently associ-ted with pulmonary hypertension.39,40
eart failure in hypothyroidism
ardiac changes in hypothyroidism are the complete oppo-ite of those occurring in thyrotoxicosis. The most prominentndings are the decrease in cardiac output and cardiacontractility, diastolic hypertension, increased systemic vas-ular resistance, and rhythm disturbances; systolic andiastolic functions are reduced at rest and during exercise.H deficit decreases tissue thermogenesis and increasesesistance in peripheral arterioles through the direct effectf T3 on vascular smooth muscle cells. Cardiac preload isecreased due to the impaired diastolic function and tohe decreased blood volume (Table 4). Cardiac afterloads increased and chronotropic and inotropic functions areeduced, resulting in a decrease in cardiac output.41,42 Thehysiological chronotropic response and normal tension of
he heart muscle in diastolic phase depend on the properxpression of T3 in the heart cells and its stimulating influ-nce on Na+---K+-ATPase and Ca2+-ATPase in the endoplasmiceticulum. The isovolumetric relaxation phase of diastoliction
tion
y
AFDirectcellular effects
Increasedcardiac outpute
ism
eart failure in hyperthyroidism.

Effects of thyroid hormones 305
Table 4 Components leading to heart failure inhypothyroidism.
Bradycardia Impaired systolic functionDecreased cardiac preload Impaired diastolic functionIncreased systemic vascular
resistanceImpaired left ventriculardiastolic filling
Increase in left ventricular Pericardial effusion
Table 5 Risk factors for AF in patients withhyperthyroidism.
Classic factors Novel factors
Age >60 years ObesityIschemic heart disease Chronic kidney diseaseCongestive heart failure ProteinuriaMale sex Elevated transaminase
concentrationsCardiac valve disease Elevated sensitive C reactive
proteinTSH levels <0.1 mIU/L Serum free T4 concentration
Female sex
ifct
wrrhtmhr(sdt
rlA
dcp
Sc
AsparT((ea
Document downloaded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
mass
function slows down, just like the contraction velocity dur-ing systole, and there is chamber dilatation and impairedmyocardial blood flow (Fig. 4).
Dilated cardiomyopathy (DCM) is a heart muscle disorderdefined by the presence of a dilated and poorly functioningleft ventricle in the absence of abnormal loading condi-tions (hypertension, valve disease) or ischemic heart diseasesufficient to cause global systolic impairment; in hypothy-roidism, although cardiac output is reduced, heart failureis relatively rare because there is a lower oxygen demandin the periphery. The improvement of the cardiac func-tion after hormonal treatment is an important argument infavor of the implication of hypothyroidism in the genesis ofDCM.43,44
Atrial fibrillation and thyroid
AF is the most common cardiac complication of hyperthy-roidism, occurring in an estimated 10% to 25% of overtlyhyperthyroid patients; in comparison 0.4% of the generalpopulation has AF, representing an independent risk factorfor cardiovascular events.
Prevalence increases with age; so much so that 25% ofhyperthyroid patients older than 60 years had AF comparedto 5% in patients less than 60 years of age, indicating thatage is a major factor in the onset of AF.
The propensity to develop AF may be due to the short-ened refractory period of atrial cells and a greater delay inthe rectifier potassium current increases between the rightatrium and the left atrium, creating a substrate for AF.45,46
Furthermore, TH potentiate the effect of the adrener-gic system on the heart, and while catecholamine levelsare either normal or decreased in hyperthyroidism, cate-cholamine action occurs through increased tissue sensitivitydue to upregulated transcription of beta-adrenergic recep-tors and differences in autonomic innervations betweenatria and ventricles. It is also possible that the sensitivityof atrial or ventricular myocardial cells to TH is different.
Generally, the onset of AF occurs with premature com-plexes originating from the pulmonary veins, and thepersistence of AF requires re-entry; premature complexesoccur secondary to automaticity or triggered activity. Hyper-thyroidism is associated with reduced vagal activity andreduced heart rate variability; the rapid and irregularheartbeat produced by AF increases the risk of blood clotformation inside the heart.47,48
These clots may eventually become dislodged, causingembolism. Moreover, TH have various effects on coagula-tion, TH excess is associated with coagulation abnormalities,such as shortened activated partial thromboplastin time,
i
lb
Cardiac frequency>80 beats/min
ncreased fibrinogen levels, and increased factor VIII andactor X activity in patients in sinus rhythm with thyrotoxi-osis; even so, the best evidence-based study did not find arend toward increased embolic risk.
AF alters atrial electrical and structural properties in aay that promotes its own maintenance; this increases the
isk of recurrence and may alter the response to antiar-hythmic drugs. The risk factors for AF in patients withyperthyroidism are similar to those in the general popula-ion (age, ischemic heart disease, congestive heart failure,ale sex and valvular heart disease). However, other factors
ave been associated with the presence of AF in hyperthy-oidism (Table 5) including obesity, chronic kidney diseasewhich is a powerful predictor of new-onset AF in hyperten-ive patients, independently of LV hypertrophy and left atrialilatation), proteinuria, female sex, serum free T4 concen-ration, and elevated transaminase concentrations.49,50
Moreover, it has been suggested that high sensitive Ceactive protein, an indicator of inflammation, free T4, andeft atrial diameter are associated with the development ofF in patients with hyperthyroidism.
Moreover, hypothyroidism is associated with bradycardia,ecreased variability in heart rate, and has been asso-iated with a lower risk of AF compared with euthyroidatients.51,52
ubclinical thyroid dysfunction (SCTD) andardiovascular disease and mortality
lthough it is recognized that patients with SCTD may haveubtle symptoms of thyroid dysfunction, the definition isurely a biochemical one: SCTD is defined as serum free T4nd total or free T3 levels within their respective referenceanges in the presence of abnormal serum TSH levels. SerumSH is undetectable or low in subclinical hyperthyroidismSHyper), and it is increased in subclinical hypothyroidismSHypo). It is a common finding in the growing population oflderly patients, occurring in 10---15% among those aged 65nd older.53,54
Controversy persists about whether screening and treat-
ng subclinical thyroid dysfunction is warranted.SHypo has been associated with elevated cholesterolevels and increased risk for atherosclerosis. SHyper haseen associated with cardiovascular and total mortality. The
3 H. Vargas-Uricoechea et al.
r(ahf
pCtiavtTecv
i≥dhtahimr
aCslw4at
cc0
fo(
A
AimAdraiHscep
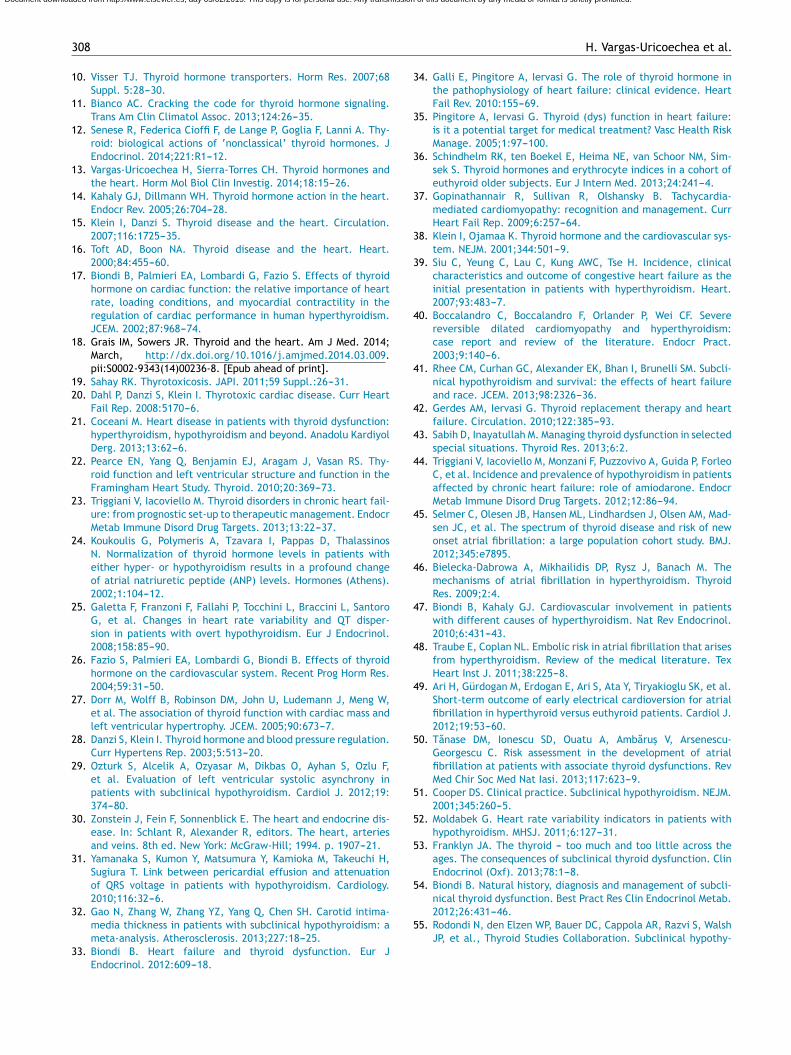
SCTD
Long‐term�SHyper.
Associated�factors:Arrhythmias.
Increased�heart�rate.Increased�pulse�pressure.
AF.Heart�failure.
Increased�pulmonary�arterial�
Long‐term�SHypo.
Associated�factors:Increased��diastolic�arterial�pressure.
Ventricular�tachyarrhytmia.Heart�failure.
Increased�homocysteine.Increased�oxydative�stress.
Hypercoagulability.
Increased�cardiovascularmorbidity�and�mortality.
Figure 6 SCTD and increased cardiovascular morbidity andm
ln
aoir7m
didieib
(phyperthyroidism (amiodarone-induced thyrotoxicosis --- AIT--- with a prevalence ranging from 2 to 9.6%).
Table 6 Amiodarone and its effects on the thyroid gland.
Intrinsic effects ofamiodarone
Iodine-induced effects ofamiodarone
Direct thyroid cytotoxicity Iodine-mediatedpotentiation of thyroidautoimmunity
Blockade of TH entry intocells
Inability to escape fromWolff---Chaikoff effect
Inhibition of type I and typeII 5′-deiodinase
Unregulated hormonesynthesis (Jod---Basedow
Document downloaded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
06
elationship between SHypo and coronary heart diseaseCHD) seemed to differ among studies that involved middle-ged versus elderly participants, with studies whose samplesad a mean age younger than 65 years showing increased riskor CHD.
A meta-analysis showed that SCTD might represent aotentially modifiable --- albeit modest --- risk factor forHD and mortality. Potential mechanisms for the associa-ions with cardiovascular diseases among adults with SHyponclude elevated cholesterol levels, increased homocysteinend oxidative stress, insulin resistance, increased systemicascular resistance, arterial stiffness, endothelial dysfunc-ion, and activation of thrombosis and hypercoagulability.he common denominator in the various studies is the het-rogeneity among individual studies that used different TSHutoffs, different confounding factors for adjustment, andarying CHD definitions.
The risk of CHD events tends to be higher when TSHs ≥7.0 mUI/L, being more evident when the value is10 mUI/L. In summary, for SHypo, combined availableata from large prospective cohorts suggest that subclinicalypothyroidism is associated with an increased risk of CHD inhose with higher TSH levels. The risk of both CHD mortalitynd CHD events, but not of total mortality, increases withigher concentrations of TSH, and is significantly elevatedn adults with TSH levels of 10 mUI/L or greater. Conversely,inimal TSH elevations are not associated with an increased
isk of CHD events and CHD mortality.55,56
Moreover, SHyper in age and sex-adjusted analyses wasssociated with increased total mortality, CHD mortality,HD events and AF. Risks did not differ significantly by age,ex, or preexisting cardiovascular disease, and were simi-ar after further adjustment for cardiovascular risk factors,ith an attributable risk of 14.5% for total mortality and1.5% for AF. However, heart failure is the leading cause ofn increased cardiovascular mortality in both overt hyper-hyroidism and subclinical hyperthyroidism.
Risks for CHD mortality and AF (but not other out-omes) were higher for thyrotropin levels under 0.10 mUI/Lompared with thyrotropin levels between 0.10 and.44 mUI/L.57,58
In summary, SCTD represents a potentially modifiable riskactor for CHD and mortality, especially when the valuesf TSH are <0.10 mIU/L --- Shyper and ≥10.0 mIU/L --- ShypoFig. 6).
miodarone and thyroid
miodarone is a potent class III anti-arrhythmic drug usedn clinical practice for the prophylaxis and treatment ofany cardiac rhythm disturbances, ranging from paroxysmalF to life-threatening ventricular tachyarrhythmias. Amio-arone often causes changes in thyroid function tests mainlyelated to the inhibition of 5′-deiodinase activity resulting in
decrease in the generation of T3 from T4, with a resultingncrease in rT3 production and a decrease in its clearance.owever, the use of amiodarone is associated with several
ide effects owing to its marked lipid affinity. It is highlyoncentrated in tissues and is linked to a number of adverseffects including photosensitivity, corneal microdeposits,ulmonary toxicity, hepatotoxicity, peripheral neuropathy,ortality.
ung dysfunction, gynecomastia, ataxia, tremors, peripheraleuropathy, hyperthyroidism and hypothyroidism.59,60
Amiodarone is a benzofuran derivative containing twotoms of iodine per molecule. This amounts to 37.5% ofrganic iodine by molecular weight, and 10% of the drug’sodine content is released daily as free iodide. Drug dosesange from 200 to 600 mg daily and treatment releases about---20 mg of iodide daily, which is about 50---100 fold the opti-al daily iodine intake.Although the majority of the adverse effects of amio-
arone on several organs are due to deposition of the drugn the parenchyma, its effects on the thyroid gland can beivided into two groups: intrinsic effects resulting from thenherent properties of the compound, and iodine-inducedffects due solely to the pharmacologic effects of a largeodine load (it has the potential to cause thyroid dysfunctionecause of its iodine-rich chemical structure) (Table 6).
Amiodarone can lead to both hypothyroidismamiodarone-induced hypothyroidism --- AIH --- with arevalence ranging from 5 to 22%) and, less commonly to
effect)Decreased T3 binding to its
TRsIncreased intrathyroidiodine stores

C
Td
pcOottd
R
Pqt
Ce
Dap
C
Tc
R
Document downloaded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Effects of thyroid hormones
AIT appears to occur more frequently in geographicalareas with low iodine intake, whereas AIH is more fre-quent in iodine-sufficient areas. In contrast to AIT, AIH isslightly more frequent in females (probably due to underly-ing Hashimoto’s thyroiditis).
The most likely pathogenic mechanism is that the thy-roid gland is unable to escape from the acute Wolff---Chaikoffeffect after an iodine load and to resume normal thyroid hor-mone synthesis. The large amount of iodide released duringthe metabolism of amiodarone leads to an adaptive block-age of further thyroidal iodide uptake and TH biosynthesis(Wolff---Chaikoff effect). Although it can be apparent withinthe first two weeks of treatment, further exposure to iodineleads to normal resumption of TH synthesis. This escape phe-nomenon from the Wolff---Chaikoff effect helps protect theindividual from developing hypothyroidism.61,62
The pharmacological concentrations of iodide associatedwith amiodarone treatment lead to a protective inhibition ofthyroidal T4 and T3 synthesis and release by thyroid withinthe first two weeks of treatment. After 3 months of amio-darone administration, a steady state is reached, with somehormonal changes persisting indefinitely. Total and free T4and rT3 remain at the upper end of normal or slightly ele-vated, and serum T3 levels remain in the low normal range.In contrast, serum TSH levels return to normal after 12weeks of therapy.
The cause for TSH normalization is presumed to be anincrease in the T4 production rate, possibly as a result ofincreased intrathyroidal iodine stores and escape from theWolff---Chaikoff effect.63
Two main mechanisms can lead to AIT: iodine-inducedhyperthyroidism (type 1 AIT, a form of Jod---Basedow effect,which is identical to that seen in patients with endemiciodine deficient goiter who are given iodide replacement);or destructive thyroiditis with destruction of thyroid fol-licles resulting in a thyroiditis with excess release of T3and T4 (type 2 AIT), caused by amiodarone itself and itshigh iodine content. Type 1 AIT occurs in subjects with anabnormal thyroid (goiter or latent autoimmune disease),with the iodine load triggering autonomous thyroid hormoneproduction.
Type 2 develops in subjects who have an apparently nor-mal gland and may reflect TH release due to direct cytotoxiceffects of the drug on thyrocytes. The nature of destructivethyroiditis is that of a self-limiting disease. AIT may developearly during amiodarone treatment or even several monthsafter drug withdrawal. This is because of amiodarone andits metabolites --- mainly desethylamiodarone.64,65
Dronedarone is a new anti-arrhythmic drug, which wasdesigned to maintain the potent antiarrhythmic and rate-controlling effects of amiodarone while reducing its toxiceffects. Dronedarone is a non-iodinated benzofuran deriva-tive of amiodarone in which the iodine moieties, observedwith amiodarone, are substituted with a methyosulfon-amide group. However, dronedarone is less lipophilic thanamiodarone, with a much shorter half-life (24 h) thanamiodarone (several weeks); it is also extensively metab-olized primarily by the cytochrome P450 3A4 system
and excreted in the bile with minimal renal excretion.Dronedarone does not appear to cause any of the thyroid,pulmonary and neurological adverse effects observed withamiodarone.66---68307
onclusions
hyroid dysfunction causes remarkable cardiovascularerangements.
TH has numerous effects on the cardiovascular system inhysiological conditions which are mediated mainly by intra-ellular receptors, but also through non-genomic pathways.n the basis of the understanding of the cellular mechanismsf TH action on the cardiovascular system, it is possibleo explain the mechanism of cardiac output, cardiac con-ractility, blood pressure, vascular resistance, and rhythmisturbances that result from thyroid dysfunction.
esponsabilidades éticas
rotección de personas y animales. Los autores declaranue para esta investigación no se han realizado experimen-os en seres humanos ni en animales.
onfidencialidad de los datos. Los autores declaran que enste artículo no aparecen datos de pacientes.
erecho a la privacidad y consentimiento informado. Losutores declaran que en este artículo no aparecen datos deacientes.
onflict of interest
he authors declare that there is no conflict of interest thatould bias the impartiality of this review.
eferences
1. Chiamolera MI, Wondisford FE. Minireview: thyrotropin-releasing hormone and the thyroid hormone feedback mech-anism. Endocrinology. 2009;150:1091---6.
2. Zhang J, Lazar MA. The mechanism of action of thyroid hor-mones. Annu Rev Physiol. 2000;62:439---66.
3. Bianco AC, Salvatore D, Gereben B, Berry MJ, Larsen PR.Biochemistry, cellular and molecular biology, and physiologi-cal roles of the iodothyronine selenodeiodinases. Endocr Rev.2002;23:38---89.
4. Orozco A, Valverde RC, Olvera A, García G. Iodothyronine deiod-inases: a functional and evolutionary perspective. J Endocrinol.2012;215:207---19.
5. Dentice M, Marsili A, Zavacki AM, Reed Larsen P, Salvatore D. Thedeiodinases and the control of intracellular thyroid hormonesignaling during cellular differentiation. Biochim Biophys Acta.2013;1830:3937---45.
6. Maia AL, Goemann IM, Souza Meyer EL, Wajner SM. Deiodi-nases: the balance of thyroid hormone Type 1 iodothyroninedeiodinase in human physiology and disease. J Endocrinol.2011;209:283---97.
7. Lin JZ, Sieglaff DH, Yuan C, Su J, Arumanayagam AS, FirouzbakhtS, et al. Gene specific actions of thyroid hormone receptor sub-types. PLOS ONE. 2013;8:e52407.
8. Flamant F, Gauthier K. Thyroid hormone receptors: the chal-lenge of elucidating isotype-specific functions and cell-specific
response. Biochim Biophys Acta. 2013;1830:3900---7.9. Astapova I, Hollenberg AN. The in vivo role of nuclear receptorcorepressors in thyroid hormone action. Biochim Biophys Acta.2013;1830:3876---81.
3
1
1
1
1
1
1
1
1
1
12
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
Document downloaded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
08
0. Visser TJ. Thyroid hormone transporters. Horm Res. 2007;68Suppl. 5:28---30.
1. Bianco AC. Cracking the code for thyroid hormone signaling.Trans Am Clin Climatol Assoc. 2013;124:26---35.
2. Senese R, Federica Cioffi F, de Lange P, Goglia F, Lanni A. Thy-roid: biological actions of ‘nonclassical’ thyroid hormones. JEndocrinol. 2014;221:R1---12.
3. Vargas-Uricoechea H, Sierra-Torres CH. Thyroid hormones andthe heart. Horm Mol Biol Clin Investig. 2014;18:15---26.
4. Kahaly GJ, Dillmann WH. Thyroid hormone action in the heart.Endocr Rev. 2005;26:704---28.
5. Klein I, Danzi S. Thyroid disease and the heart. Circulation.2007;116:1725---35.
6. Toft AD, Boon NA. Thyroid disease and the heart. Heart.2000;84:455---60.
7. Biondi B, Palmieri EA, Lombardi G, Fazio S. Effects of thyroidhormone on cardiac function: the relative importance of heartrate, loading conditions, and myocardial contractility in theregulation of cardiac performance in human hyperthyroidism.JCEM. 2002;87:968---74.
8. Grais IM, Sowers JR. Thyroid and the heart. Am J Med. 2014;March, http://dx.doi.org/10.1016/j.amjmed.2014.03.009.pii:S0002-9343(14)00236-8. [Epub ahead of print].
9. Sahay RK. Thyrotoxicosis. JAPI. 2011;59 Suppl.:26---31.0. Dahl P, Danzi S, Klein I. Thyrotoxic cardiac disease. Curr Heart
Fail Rep. 2008:5170---6.1. Coceani M. Heart disease in patients with thyroid dysfunction:
hyperthyroidism, hypothyroidism and beyond. Anadolu KardiyolDerg. 2013;13:62---6.
2. Pearce EN, Yang Q, Benjamin EJ, Aragam J, Vasan RS. Thy-roid function and left ventricular structure and function in theFramingham Heart Study. Thyroid. 2010;20:369---73.
3. Triggiani V, Iacoviello M. Thyroid disorders in chronic heart fail-ure: from prognostic set-up to therapeutic management. EndocrMetab Immune Disord Drug Targets. 2013;13:22---37.
4. Koukoulis G, Polymeris A, Tzavara I, Pappas D, ThalassinosN. Normalization of thyroid hormone levels in patients witheither hyper- or hypothyroidism results in a profound changeof atrial natriuretic peptide (ANP) levels. Hormones (Athens).2002;1:104---12.
5. Galetta F, Franzoni F, Fallahi P, Tocchini L, Braccini L, SantoroG, et al. Changes in heart rate variability and QT disper-sion in patients with overt hypothyroidism. Eur J Endocrinol.2008;158:85---90.
6. Fazio S, Palmieri EA, Lombardi G, Biondi B. Effects of thyroidhormone on the cardiovascular system. Recent Prog Horm Res.2004;59:31---50.
7. Dorr M, Wolff B, Robinson DM, John U, Ludemann J, Meng W,et al. The association of thyroid function with cardiac mass andleft ventricular hypertrophy. JCEM. 2005;90:673---7.
8. Danzi S, Klein I. Thyroid hormone and blood pressure regulation.Curr Hypertens Rep. 2003;5:513---20.
9. Ozturk S, Alcelik A, Ozyasar M, Dikbas O, Ayhan S, Ozlu F,et al. Evaluation of left ventricular systolic asynchrony inpatients with subclinical hypothyroidism. Cardiol J. 2012;19:374---80.
0. Zonstein J, Fein F, Sonnenblick E. The heart and endocrine dis-ease. In: Schlant R, Alexander R, editors. The heart, arteriesand veins. 8th ed. New York: McGraw-Hill; 1994. p. 1907---21.
1. Yamanaka S, Kumon Y, Matsumura Y, Kamioka M, Takeuchi H,Sugiura T. Link between pericardial effusion and attenuationof QRS voltage in patients with hypothyroidism. Cardiology.2010;116:32---6.
2. Gao N, Zhang W, Zhang YZ, Yang Q, Chen SH. Carotid intima-
media thickness in patients with subclinical hypothyroidism: ameta-analysis. Atherosclerosis. 2013;227:18---25.3. Biondi B. Heart failure and thyroid dysfunction. Eur JEndocrinol. 2012:609---18.
5
H. Vargas-Uricoechea et al.
4. Galli E, Pingitore A, Iervasi G. The role of thyroid hormone inthe pathophysiology of heart failure: clinical evidence. HeartFail Rev. 2010:155---69.
5. Pingitore A, Iervasi G. Thyroid (dys) function in heart failure:is it a potential target for medical treatment? Vasc Health RiskManage. 2005;1:97---100.
6. Schindhelm RK, ten Boekel E, Heima NE, van Schoor NM, Sim-sek S. Thyroid hormones and erythrocyte indices in a cohort ofeuthyroid older subjects. Eur J Intern Med. 2013;24:241---4.
7. Gopinathannair R, Sullivan R, Olshansky B. Tachycardia-mediated cardiomyopathy: recognition and management. CurrHeart Fail Rep. 2009;6:257---64.
8. Klein I, Ojamaa K. Thyroid hormone and the cardiovascular sys-tem. NEJM. 2001;344:501---9.
9. Siu C, Yeung C, Lau C, Kung AWC, Tse H. Incidence, clinicalcharacteristics and outcome of congestive heart failure as theinitial presentation in patients with hyperthyroidism. Heart.2007;93:483---7.
0. Boccalandro C, Boccalandro F, Orlander P, Wei CF. Severereversible dilated cardiomyopathy and hyperthyroidism:case report and review of the literature. Endocr Pract.2003;9:140---6.
1. Rhee CM, Curhan GC, Alexander EK, Bhan I, Brunelli SM. Subcli-nical hypothyroidism and survival: the effects of heart failureand race. JCEM. 2013;98:2326---36.
2. Gerdes AM, Iervasi G. Thyroid replacement therapy and heartfailure. Circulation. 2010;122:385---93.
3. Sabih D, Inayatullah M. Managing thyroid dysfunction in selectedspecial situations. Thyroid Res. 2013;6:2.
4. Triggiani V, Iacoviello M, Monzani F, Puzzovivo A, Guida P, ForleoC, et al. Incidence and prevalence of hypothyroidism in patientsaffected by chronic heart failure: role of amiodarone. EndocrMetab Immune Disord Drug Targets. 2012;12:86---94.
5. Selmer C, Olesen JB, Hansen ML, Lindhardsen J, Olsen AM, Mad-sen JC, et al. The spectrum of thyroid disease and risk of newonset atrial fibrillation: a large population cohort study. BMJ.2012;345:e7895.
6. Bielecka-Dabrowa A, Mikhailidis DP, Rysz J, Banach M. Themechanisms of atrial fibrillation in hyperthyroidism. ThyroidRes. 2009;2:4.
7. Biondi B, Kahaly GJ. Cardiovascular involvement in patientswith different causes of hyperthyroidism. Nat Rev Endocrinol.2010;6:431---43.
8. Traube E, Coplan NL. Embolic risk in atrial fibrillation that arisesfrom hyperthyroidism. Review of the medical literature. TexHeart Inst J. 2011;38:225---8.
9. Ari H, Gürdogan M, Erdogan E, Ari S, Ata Y, Tiryakioglu SK, et al.Short-term outcome of early electrical cardioversion for atrialfibrillation in hyperthyroid versus euthyroid patients. Cardiol J.2012;19:53---60.
0. Tanase DM, Ionescu SD, Ouatu A, Ambarus V, Arsenescu-Georgescu C. Risk assessment in the development of atrialfibrillation at patients with associate thyroid dysfunctions. RevMed Chir Soc Med Nat Iasi. 2013;117:623---9.
1. Cooper DS. Clinical practice. Subclinical hypothyroidism. NEJM.2001;345:260---5.
2. Moldabek G. Heart rate variability indicators in patients withhypothyroidism. MHSJ. 2011;6:127---31.
3. Franklyn JA. The thyroid --- too much and too little across theages. The consequences of subclinical thyroid dysfunction. ClinEndocrinol (Oxf). 2013;78:1---8.
4. Biondi B. Natural history, diagnosis and management of subcli-nical thyroid dysfunction. Best Pract Res Clin Endocrinol Metab.2012;26:431---46.
5. Rodondi N, den Elzen WP, Bauer DC, Cappola AR, Razvi S, WalshJP, et al., Thyroid Studies Collaboration. Subclinical hypothy-
6
6
6
6
6
fibrillation or flutter. NEJM. 2007;357:987---99.68. Christiansen CB, Torp-Pedersen C, Køber L. Efficacy and safety
Document downloaded from http://www.elsevier.es, day 05/02/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Effects of thyroid hormones
roidism and the risk of coronary heart disease and mortality.JAMA. 2010;304:1365---74.
56. Rodondi N, Bauer DC. Subclinical hypothyroidism and cardiovas-cular risk: how to end the controversy. JCEM. 2013;98:2267---9.
57. Collet TH, Gussekloo J, Bauer DC, den Elzen WP, Cappola AR,Balmer P, et al., Thyroid Studies Collaboration. Subclinicalhyperthyroidism and the risk of coronary heart disease and mor-tality. Arch Intern Med. 2012;172:799---809.
58. Gencer B, Collet TH, Virgini V, Auer R, Rodondi N. Subclini-cal thyroid dysfunction and cardiovascular outcomes amongprospective cohort studies. Endocr Metab Immune Disord DrugTargets. 2013;13:4---12.
59. Bogazzi F, Tomisti L, Bartalena L, ghini-Lombardi F, Martino E.Amiodarone and the thyroid: a 2012 update. J Endocrinol Invest.2012;35:340---8.
60. Cohen-Lehman J, Dahl P, Danzi S, Klein I. Effects of amio-darone therapy on thyroid function. Nat Rev Endocrinol. 2010;6:34---41.
61. Padmanabhan H. Amiodarone and thyroid dysfunction. SouthMed J. 2010;103:922---30.
62. Leung AM, Braverman LE. Iodine-induced thyroid dysfunction.Curr Opin Endocrinol Diabetes Obes. 2012;19:414---9.
309
3. Eskes SA, Wiersinga WM. Amiodarone and thyroid. Best PractRes Clin Endocrinol Metab. 2009;23:735---51.
4. Bogazzi F, Bartalena L, Martino E. Approach to the patient withamiodarone induced thyrotoxicosis. J Clin Endocrinol Metab.2010;95:2529---35.
5. Palermo-Garófalo C, Martínez JH, Silva F, González E, Torres O,Figueroa J, et al. The cardiology and endocrinology connectionbetween amiodarone and thyrotoxicosis: case report and reviewof the literature. Bol Asoc Med P R. 2013;105:47---53.
6. Le Heuzey JY, De Ferrari GM, Radzik D, Santini M, Zhu J, DavyJM. A short-term, randomized, double-blind, parallel-groupstudy to evaluate the efficacy and safety of dronedarone ver-sus amiodarone in patients with persistent atrial fibrillation: theDIONYSOS study. J Cardiovasc Electrophysiol. 2010;21:597---605.
7. Singh BN, Connolly SJ, Crijns HJ, Roy D, Kowey PR, Capucci A,et al. Dronedarone for maintenance of sinus rhythm in atrial
of dronedarone: a review of randomized trials. Expert Opin DrugSaf. 2010;9:189---99.