Proton Radiotherapy for Pediatric Ewing’s Sarcoma: Initial Clinical Outcomes
7
CLINICAL INVESTIGATION Pediatric Cancer PROTON RADIOTHERAPY FOR PEDIATRIC EWING’S SARCOMA: INITIAL CLINICAL OUTCOMES BARBARA ROMBI, M.D.,* THOMAS F. DELANEY , M.D., y SHANNON M. MACDONALD, M.D., y MARY S. HUANG, M.D., z DAVID H. EBB, M.D., z NORBERT J. LIEBSCH, M.D., PH.D., y KEVIN A. RASKIN, M.D., x BEOW Y. YEAP , M.D., k KAREN J. MARCUS, M.D., { NANCY J. T ARBELL, M.D., y AND TORUNN I. YOCK, M.D., M.C.H. y *ATreP (Provincial Agency for Proton Therapy), Trento, Italy; Departments of y Radiation Oncology, z Pediatric Hematology and Oncology, x Orthopaedic Surgery, and k Medicine, Massachusetts General Hospital–Harvard Medical School, Boston, MA; and { Division of Radiation Oncology, Children’s Hospital Boston, MA Purpose: Proton radiotherapy (PT) has been prescribed similarly to photon radiotherapy to achieve comparable disease control rates at comparable doses. The chief advantage of protons in this setting is to reduce acute and late toxicities by decreasing the amount of normal tissue irradiated. We report the preliminary clinical outcomes in- cluding late effects on our pediatric Ewing’s sarcoma patients treated with PT at the Francis H. Burr Proton Ther- apy Center at Massachusetts General Hospital (Boston, MA). Methods and Materials: This was a retrospective review of the medical records of 30 children with Ewing’s sar- coma who were treated with PT between April 2003 and April 2009. Results: A total of 14 male and 16 female patients with tumors in several anatomic sites were treated with PT at a median age of 10 years. The median dose was 54 Gy (relative biological effectiveness) with a median follow- up of 38.4 months. The 3-year actuarial rates of event-free survival, local control, and overall survival were 60%, 86%, and 89%, respectively. PT was acutely well tolerated, with mostly mild-to-moderate skin reactions. At the time of writing, the only serious late effects have been four hematologic malignancies, which are known risks of topoisomerase and anthracyline exposure. Conclusions: Proton radiotherapy was well tolerated, with few adverse events. Longer follow-up is needed to more fully assess tumor control and late effects, but the preliminary results are encouraging. Ó 2012 Elsevier Inc. Proton radiation, Ewing’s sarcoma. INTRODUCTION Currently 60% to 70% of patients with localized Ewing’s sarcoma survive more than 5 years (1–4). Because Ewing’s sarcoma is highly responsive to radiation therapy, and it often occurs in bones not easily resected, radiotherapy is a mainstay of treatment and is used in approximately 60% of Ewing’s sarcoma patients (5–11). Radiation is used in the postoperative setting for patients with close or positive resection margins and sometimes in the setting of a poor or slow clinical response to neoadjuvant chemotherapy (12–16). Radiation is typically used instead of surgery for children with unresectable tumors or in cases in which surgery would result in too great morbidity. However, definitive radiotherapy causes side effects as a result of the nontumor tissues irradiated in the process. Proton radiotherapy (PT) can be prescribed similarly to photon radiotherapy to achieve comparable disease control rates at comparable doses. The chief advantage of protons in this setting is to spare acute and late toxicities by decreas- ing the amount of normal tissue receiving radiation. The ab- sence of an exit dose beyond the Bragg peak results in approximately 50% to 60% reduction in integral dose (17). In this study, we report early clinical outcomes in children and adolescents with Ewing’s sarcoma who were treated Reprint requests to: Torunn I. Yock, M.D. M.C.H., Department of Radiation Oncology, Massachusetts General Hospital, 100 Blossom Street, Cox Building 341, Boston, MA 02114; Tel: (617) 726-7559; Fax: (617) 726-3603; E-mail: [email protected] Presented in part in oral form at PTCOG (Particle Therapy Co- Operative Group) 48, September 28 - October 3, 2009, Heidelberg, Germany. Supported in part by the Federal Share of program income earned by Massachusetts General Hospital on National Institutes of Health Grant #C06 CA059267, Proton Therapy Research and Treatment Center. Conflict of interest: none. Acknowledgments—We acknowledge Judith Adams, C.M.D., for her work on the figures. Received June 29, 2010, and in revised form March 17, 2011. Accepted for publication March 23, 2011. 1142 Int. J. Radiation Oncology Biol. Phys., Vol. 82, No. 3, pp. 1142–1148, 2012 Copyright Ó 2012 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/$ - see front matter doi:10.1016/j.ijrobp.2011.03.038
-
Upload
hms-harvard -
Category
Documents
-
view
0 -
download
0
Transcript of Proton Radiotherapy for Pediatric Ewing’s Sarcoma: Initial Clinical Outcomes

Int. J. Radiation Oncology Biol. Phys., Vol. 82, No. 3, pp. 1142–1148, 2012Copyright � 2012 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/$ - see front matter
jrobp.2011.03.038
doi:10.1016/j.iCLINICAL INVESTIGATION Pediatric Cancer
PROTON RADIOTHERAPY FOR PEDIATRIC EWING’S SARCOMA: INITIALCLINICAL OUTCOMES
BARBARA ROMBI, M.D.,* THOMAS F. DELANEY, M.D.,y SHANNON M. MACDONALD, M.D.,y
MARY S. HUANG, M.D.,z DAVID H. EBB, M.D.,z NORBERT J. LIEBSCH, M.D., PH.D.,y
KEVIN A. RASKIN, M.D.,x BEOW Y. YEAP, M.D.,k KAREN J. MARCUS, M.D.,{ NANCY J. TARBELL, M.D.,y
AND TORUNN I. YOCK, M.D., M.C.H.y
*ATreP (Provincial Agency for Proton Therapy), Trento, Italy; Departments of yRadiation Oncology, zPediatric Hematology andOncology, xOrthopaedic Surgery, and kMedicine, Massachusetts General Hospital–Harvard Medical School, Boston, MA; and
{Division of Radiation Oncology, Children’s Hospital Boston, MA
Reprinof RadiaBlossom(617) 726Present
OperativeGermany.Suppor
by Massa
Purpose: Proton radiotherapy (PT) has been prescribed similarly to photon radiotherapy to achieve comparabledisease control rates at comparable doses. The chief advantage of protons in this setting is to reduce acute and latetoxicities by decreasing the amount of normal tissue irradiated. We report the preliminary clinical outcomes in-cluding late effects on our pediatric Ewing’s sarcoma patients treated with PTat the Francis H. Burr Proton Ther-apy Center at Massachusetts General Hospital (Boston, MA).Methods and Materials: This was a retrospective review of the medical records of 30 children with Ewing’s sar-coma who were treated with PT between April 2003 and April 2009.Results: A total of 14 male and 16 female patients with tumors in several anatomic sites were treated with PT ata median age of 10 years. The median dose was 54 Gy (relative biological effectiveness) with a median follow-up of 38.4 months. The 3-year actuarial rates of event-free survival, local control, and overall survival were60%, 86%, and 89%, respectively. PT was acutely well tolerated, with mostly mild-to-moderate skin reactions.At the time of writing, the only serious late effects have been four hematologic malignancies, which are known risksof topoisomerase and anthracyline exposure.Conclusions: Proton radiotherapy was well tolerated, with few adverse events. Longer follow-up is needed to morefully assess tumor control and late effects, but the preliminary results are encouraging. � 2012 Elsevier Inc.
Proton radiation, Ewing’s sarcoma.
INTRODUCTION
Currently 60% to 70% of patients with localized Ewing’ssarcoma survive more than 5 years (1–4). Because Ewing’ssarcoma is highly responsive to radiation therapy, and itoften occurs in bones not easily resected, radiotherapy isa mainstay of treatment and is used in approximately 60%of Ewing’s sarcoma patients (5–11). Radiation is used inthe postoperative setting for patients with close or positiveresection margins and sometimes in the setting of a pooror slow clinical response to neoadjuvant chemotherapy(12–16). Radiation is typically used instead of surgery forchildren with unresectable tumors or in cases in which
t requests to: Torunn I. Yock, M.D. M.C.H., Departmenttion Oncology, Massachusetts General Hospital, 100Street, Cox Building 341, Boston, MA 02114; Tel:-7559; Fax: (617) 726-3603; E-mail: [email protected] in part in oral form at PTCOG (Particle Therapy Co-Group) 48, September 28 - October 3, 2009, Heidelberg,
ted in part by the Federal Share of program income earnedchusetts General Hospital on National Institutes of Health
1142
surgery would result in too great morbidity. However,definitive radiotherapy causes side effects as a result of thenontumor tissues irradiated in the process.
Proton radiotherapy (PT) can be prescribed similarly tophoton radiotherapy to achieve comparable disease controlrates at comparable doses. The chief advantage of protonsin this setting is to spare acute and late toxicities by decreas-ing the amount of normal tissue receiving radiation. The ab-sence of an exit dose beyond the Bragg peak results inapproximately 50% to 60% reduction in integral dose (17).In this study, we report early clinical outcomes in childrenand adolescents with Ewing’s sarcoma who were treated
Grant #C06 CA059267, Proton Therapy Research and TreatmentCenter.Conflict of interest: none.
Acknowledgments—We acknowledge Judith Adams, C.M.D., forher work on the figures.Received June 29, 2010, and in revised form March 17, 2011.
Accepted for publication March 23, 2011.

Proton radiation for Ewing’s sarcoma d B. ROMBI et al. 1143
with passively scattered three-dimensional (3D) conformalPT at Massachusetts General Hospital (Boston, MA).
METHODS AND MATERIALS
Patients and proceduresA total of 30 children with Ewing’s sarcoma have been treated at
the Francis H. Burr Proton Therapy Center at Massachusetts Gen-eral Hospital between April 2003 and April 2009. All patientsreceived chemotherapy based on the AEWS (A-Ewing Sarcoma)0031 and POG (Pediatric Oncology Group) 9354 protocol followedby proton irradiation, with or without surgery. Computed tomogra-phy (CT) treatment planning was used in conjunction with addi-tional diagnostic studies to assist in defining target volumes.Imaging included CT images at diagnosis, magnetic resonance im-aging (MRI), positron emission tomography (PETor PET/CT), andbone scans. Each patient was immobilized with customized immo-bilization device based on the tumor site to be irradiated.All patients were treated with passively scattered proton radia-
tion with treatment plans generated with XiO planning software(CMS Inc., St Louis, MO). The Francis H. Burr Proton TherapyCenter provides a rotational gantry system and maximum protonbeam energy of 231 MeV. The proton dose was prescribed in Gy(relative biological effectiveness [RBE]), using the RBE value of1.1 (18, 19). PT was delivered to an initial clinical target volume
Table 1. Patient ch
Patient ID Disease site treated SexAgeat PT
1 Lumbar spine and paraspinal M 17.92 Pelvic mass, left ileum F 11.63 Pelvic mass, left iliopsoas muscle M 16.64 Thoraco-lumbo-sacral spine and paraspinal F 2.65 Cervico-thoracic and paraspinal F 3.56 Parieto-occipital bone F 4.87 Thoracic paraspinal region M 4.38 Base of skull with intracranial extension M 6.59 Left chest wall F 9.2
10 Upper lung, neck and paraspinal F 3.711 Base of skull F 7.412 Left orbit, nasal cavity and maxillary sinus F 15.413 Thoraco-lumbar and paraspinal F 15.214 Base of tongue F 1.815 Ethmoid sinus invading orbit M 17.716 Thoracic spine and paraspinal F 11.817 Thoraco-lumbar spine F 3.118 Lumbar spine F 13.019 Thoraco-lumbar spine M 10.120 Occipital region M 2.321 Temporal bone M 11.822 Pelvic mass, ischium M 10.123 Lumbo-sacral spine/pelvis M 4.224 Medial right orbit M 14.825 Thoracic spine and paraspinal, recurrent* F 16.126 CNS metastasis, recurrent* F 14.527 Pelvis F 9.728 Lumbo-sacral spinal and paraspinal, recurrent* M 21.029 Lumbar spine M 11.530 Base of skull, sphenoid body and wing M 9.8
Abbreviations: ID= identification; PT= Proton therapy; STR= subtotalsection; Bx: biopsy; CTV1= clinical target volume 1; CTV2= CTV= clinicmale; F= female; CNS = central nervous system.* Patients had been treated with surgery and/or PT to the primary lesi
(CTV1) defined as any visible bony or soft tissue tumor and anytumor edema seen on preoperative and prechemotherapy MRI/CT/PET scans plus a 1-to 2 cm anatomically constrained margin.The boost clinical target volume (CTV2) was typically defined asthe original bony extent of disease plus the post-chemotherapysoft tissue disease and 1- to 2 cm anatomically constrained margin.The prescribed dose to the CTV1 was between 30.6 and 55.8 Gy(RBE) given in 1.8 Gy (RBE) daily fractions. CTV2 was treatedto a total dose between 45 and 59.4 Gy (RBE), depending on theclinical characteristics of the disease. The planning target volumein proton therapy is taken into account differently from that withphoton therapy, and accommodations are made in the planning pro-cess. Proximal and distal range uncertainties are directly taken intoaccount in the choice of range and modulation of the spread-outBragg peak, and uncertainties in patient positioning are directlytranslated into increased aperture margin (35 mm) and rangecompensator smearing (5 mm) to provide the desired target volumecoverage.The daily setup of a patient was confirmed using diagnostic
quality orthogonal radiographs which were compared with theplanning CT’s digitally reconstructed radiographs. Shifts of assmall as 1 mm were made in 6 degrees of freedom (df; x, y, zplanes and pitch, roll, and yaw) with computer assistance andconfirmatory pretreatment radiographs. When necessary, chil-dren were treated under anesthesia (typically age 5 years andyounger).
aracteristics
Surgery type(STR, NGTR, GTR, Bx only)
CTV1Gy (RBE)
CTV2Gy (RBE)
Total doseGy (RBE)
STR 45.0 45.0Bx only 45.0 12.6 57.6Bx only 45.0 10.8 55.8STR 45.0 45.0STR 43.2 12.6 55.8GTR 45.0 45.0Bx only 43.2 9.6 52.8Bx only 45.0 10.8 55.8Bx only 50.4 50.4NGTR 30.6 19.8 50.4STR 54.0 54.0STR 45.0 14.4 59.4Bx only 45.0 45.0Bx only 39.6 16.2 55.8Bx only 45.0 10.8 55.8Bx only 46.8 46.8NGTR 45.0 45.0GTR 50.4 5.4 55.8Bx only 43.2 7.2 50.4Bx only 55.8 55.8Bx only 50.4 5.4 55.8Bx only 45.0 10.8 55.8Bx only 45.0 5.4 50.4STR 54.0 54.0Bx only 45.0 5.4 50.4STR 51.0 5.4 56.4Bx only 45.0 10.8 55.8STR 45.0 5.4 50.4STR 45.0 5.4 50.4Bx only 50.0 8 58.0
resection; NGTR= near gross total resection; GTR= gross total re-al target volume 2; Gy (RBE)= Gray Radiobiologic Equivalent; M=
on; PT was delivered to the site of recurrence.

Survival (months)0 12 24 36 48 60 72 84
0%
20%
40%
60%
80%
100%
3y EFS 60%
3y OS 89 %
1144 I. J. Radiation Oncology d Biology d Physics Volume 82, Number 3, 2012
Statistical analysisWe classified all patients who experienced disease progression or
second malignant neoplasm or who died as having experienced anevent. Event-free survival (EFS) was defined as the time frominitiation of PT until the first occurrence of an event or last patientcontact, at which time the patient was censored. Each event was fur-ther classified as local recurrence, systemic recurrence, local andsystemic recurrence, death, or second malignant neoplasm. Patientswith disease progression that had any local component were con-sidered to have experienced a local failure (LF). Disease-specificsurvival (DSS) was defined similarly to EFS, excluding secondmalignant neoplasm as an event.The outcome measures were overall survival (OS), EFS, DSS,
and local control (LC) defined from the initiation of PT. The ratesof OS, EFS, DSS, and LC were calculated by the method of KaplanandMeier (20) using SAS 9.1 (SAS Institute, Cary, NC). The cumu-lative incidence of second malignancies was estimated by consider-ing death as a competing risk using Gray’s method and the cmprskpackage in R version 2.6.2 (R Foundation for Statistical Comput-ing). The 95% confidence interval (95% CI) for cumulativeincidence was constructed based on a log–log transformation.
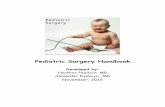
Fig. 1. Overall survival and event-free survival curves.
Ethical considerationsInstitutional review board approval for this study was obtained,
and complete anonymity of names and medical record numberswas maintained in accordance with the institution’s requirements.
RESULTS
All patients 21 years of age or younger with Ewing’s sar-coma who were treated at the Francis H. Burr Proton Ther-apy Center between April 2003 and April 2009 wereincluded in this study. Patient and treatment characteristicsare listed in Table 1. A total of 30 children (14 male and16 female) received PT at a median age of 10 years (range,1.8–21 years). The distribution of location of the tumors inthis population was unusual compared with other publishedaccounts, presumably because of the referral bias for tumorsnear critical normal structures and the enhanced ability of PTto spare these tissues. The tumors were located in the pelvis(four), trunk (15 tumors, 14 of which were vertebral body orsacrum), head-and-neck region (four), and base of skull orcranium (seven). There were no extremity lesions. The ma-jority of the patients (48%) were between 10 and 17 yearsold, with 42% younger than 10 years.
Overall, the median total prescribed dose was 54 Gy(range, 45–59.4) delivered at 1.8 Gy (RBE) per fraction.Nineteen patients received post-surgical PT to a mediandose of 50.4 Gy (RBE; range, 45–59.4). Two patients weregiven <20% of the dose with photon radiotherapy to improveskin sparing for the shallow tumors.Most of the patients witha vertebral body tumor had a laminectomy or other decom-pressive procedure with partial removal of epidural tumor toalleviate compression of the spinal cord. Gross tumor wasusually left behind in this setting. Prescribed doses for thesevertebral body tumors ranged from 45 to 57.6 Gy (RBE; me-dian, 55.8), limiting the spinal cord to 45 Gy (RBE) or less.
Three patients were given PT as salvage after a late (>4years) isolated local failure in 1 patient and distant failure
in 2 patients. The first salvage patient was treated with sur-gery and PT to 50.4 Gy for a local failure 4 years after hehad received photon radiation to a dose of 45 Gy for a lum-bar–sacral paraspinal mass involving the L4 vertebral body.The second salvage patient was treated with surgery, che-motherapy, and PT to CSI (Cranio-Spinal Irradiation) (18Gy) and had a field boost (56.4 Gy) for a brain metastasis6 years after her primary treatment. The third salvage pa-tient was treated for locally recurrent chest wall diseasepreviously treated with surgery and chemotherapy 7 yearsearlier.
Disease statusAt a median follow-up of 38.4 months (range, 17.4
months to 7.4 years), 21 patients (70%) have remainedfree of disease; specifically, 20 patients after initial PTand 1 patient after salvage PT. The 3-year EFS and OSare 60% and 89%, respectively (Fig. 1). Excluding thesalvage patients, the 3-year EFS and OS are 63% and88%. The 3-year DSS is 68%. Five patients (17%) werealive with disease at the last analysis: 2 with a local fail-ure, 1 patient with recurrence in a distant site only, and 2patients with combined local and distant recurrence ofdisease. The 3-year LC for all 30 patients is 86%. Exclud-ing the 3 salvage patients (n = 27), the 3-year LC is 88%.Four patients (13%) have died, 3 of disease progressionand 1 patient of acute myeloid leukemia (AML). Four pa-tients have developed secondary malignancies, 3 patientsAML, and 1 patient myelodysplastic syndrome (MDS).As of the time of writing, no secondary solid tumorshave been observed.
Acute effects of treatmentProton radiotherapy was acutely well tolerated. All pa-
tients sustained a skin reaction as a result of PT. Sixteen

Proton radiation for Ewing’s sarcoma d B. ROMBI et al. 1145
patients developed Grade 1 skin reactions (erythema with orwithout dry desquamation); 9 patients Grade 2 skin reactions(bright eythema or patchy moist desquamation), and 5 pa-tients Grade 3 skin reactions (confluent moist desquama-tion). One patient with a base-of-tongue Ewing’s sarcomadeveloped hoarseness, swelling, and a confluent mucositisin the radiation portal, which required hospitalization. An-other patient with orbital primary lesion developed Grade2 kerato-conjunctivitis. Eighteen patients complained ofGrade 1 fatigue (mild over baseline), 2 patents Grade 2(moderate, difficulty performing the activities of daily living[ADL] and 1 patient Grade 3 fatigue (severe, interfering withADL).
Four patients complained of mild nausea and 1 patient ofmoderate nausea attributed to the PT. Five patients hadGrade 1 anorexia (loss of appetite without alteration in eat-ing habits), and 9 patients had Grade 2 anorexia (oral intakealtered without significant weight loss or malnutrition)during PT treatment.
Functional outcome and late sequelaeScolioses/kyphoses developed in 5 patients (3 mild, 1
moderate, and 1 severe). All patients who developed spinedeformities had vertebral body primary tumors and lami-nectomies before PT. One patient treated definitively fora pelvic primary tumor had a mild limb length discrepancyrequiring no intervention. PT-induced skin changes (mildhyperpigmentation or teleangiectasias) were observed in6 patients. One patient treated to the paranasal sinuseshas teleangectasias of the nasal cavity, causing occasional(but mild) nosebleeds. Two patients had partial permanentalopecia in the cranial treated area. Two patients treated fortumors involving orbital adnexa developed late effects, 1patient with canalicular stenosis, epiphora, and left lid par-alytic lagophthalmos after treatment (surgery and PT),which has required placement of a gold weight into the up-per lid of the affected left eye, and the second patient witha chronic corneal ulcer. Two patients have developed endo-crine deficiencies after treatment to the hypothalamic pitu-itary axis for their cranial/base of skull primaries.Unilateral high frequency hearing loss has occurred in 1patient who received the full prescription dose of 55.8Gy (RBE) to one cochlea.
Secondary malignanciesFour patients developed secondary malignancies, 3 pa-
tients with AML and 1 patient withMDS. The hematologicalmalignancies are known risks of etoposide and doxorubicinexposure, and all patients received relatively high cumula-tive doses of etoposide chemotherapy depending on the pro-tocol used. Three patients were treated with chemotherapyregimens based on COG (Children’s Oncology Group)AEWS0031 protocol, and 1 patient as per POG protocol9354. The median interval between diagnosis and secondmalignancy was 27 months (range, 17–35 months). The 2-year cumulative incidence of second malignancy was 7%
(95% CI, 1–19%) and the 3-year cumulative incidence was15% (95% CI, 5–32%).
DISCUSSION
The clinical outcome of patients with Ewing’s sarcomahas improved considerably over the past several decades.This is largely due to multimodality therapy and improve-ments in systemic therapies as well as surgical andradiation therapy techniques. Current chemotherapeuticregimens using alkylating agents and topoisomerase IIinhibitors have improved both local and distant control ofdisease (1). In addition, the use of diagnostic imaging in-cluding MRI, PET, and CT have permitted better delinea-tion of disease and have enabled radiation oncologists tomore precisely target tumor volumes and avoid healthytissues.
PT provides a means to further improve radiation dose de-livery by better localizing the dose to the target and minimiz-ing dose to the surrounding normal structures (19). With PT,for a given beam there is no exit dose to normal tissues thusdecreasing the amount of normal tissue irradiated (Fig. 2). Inaddition, depending on the depth and thickness of a tumor,there may also be decreased entrance dose to the normal tis-sues the beam traverses before depositing the spread-outBragg peak in the target volume (21–23). Numerousdosimetric studies on a variety of pediatric and adulttumors have shown that PT is generally superiordosimetrically to other external beam photon techniqueincluding intensity-modulated radiation therapy (24–27).Our series represents the first and largest clinical series ofpediatric patients with Ewing’s sarcoma treated with PT.The treatment was very well tolerated with minimal acutetoxicity. The excellent LC and OS rates reported heredemonstrate that PT provides comparable local controlwith more favorable dose distributions that seem to betranslating into a more favorable morbidity profile.However, there are relatively few late-effect data in Ewing’ssarcoma patients in the literature for direct comparison, withonly four papers documenting subsequent side effects fromradiation therapy (28–31).
Dunst et al. report that, in patients treated on a multi-institutional Ewing’s sarcoma study (CESS 86) with 60 Gyor more, 9% developed Grade 3 to 4 complications (28).Two Ewing’s sarcoma patients developed chronic proctitisafter pelvic irradiation (1 patient had received 15% higherthen recommended dose and required a colostomy), and 2patients developed pathological fractures. The type of frac-tionation did not influence the frequency of complications.Higher fracture risk (20%) after subsequent radiation ther-apy has been documented by Fuchs et al. in 8 of 41 patientswho received a mean radiation dose of 55 Gy on the femur/ulna bones (29). These authors also described 13 patientswho developed radiation-related complications, includingtwo major wound complications, three pulmonary fibroses,two second malignancies, one neuropathy, one limb leg dis-crepancy, and one femoral head necrosis. Paulino et al.

Fig. 2. Proton dosimetry in a patient with Ewing’s sarcoma of the base of skull, pelvis, and vertebral body.
1146 I. J. Radiation Oncology d Biology d Physics Volume 82, Number 3, 2012
describe treatment-and tumor-related late effects in a retro-spective analysis of 40 patients with Ewing’s sarcoma local-ized in the extremity (48%), pelvis (25%), spine/trunk (22%)and head and neck (5%). Late effects occurred in 10 of 19patients who survived at least 5 years after radiation therapyand included 6 patients with muscular atrophy, 4 patientswith limb length discrepancy, 3 patients with decreasedrange of motion in joints, 2 patients with scoliosis, and 2 pa-tients with fractures, 1 with ovarian failure, and 2 with sec-ondary malignancies (30).
Indelicato et al. observed multiple late complications di-rectly related to RT in patients who had received definitiveRT to an entire bone or pelvic region for their Ewing’s tumor.These complications included hemorrhagic cystitis, 2 pe-ripheral neuropathies, osteoradionecrosis of the hip, necro-tizing fasciitis of the elbow, and 2 osteosarcomas arising inthe radiation field (31).
Although it is too early to extensively evaluate long-termtoxicity, we have seen relatively few late complications at-tributed to nontarget radiation dose to date. In particular,some bone growth abnormalities are mostly attributable tosurgery (i.e., kyphoses in patients with laminectomies).Some neuro-endocrine hormonal deficits were noted in
patients treated for tumors in cranium, high-frequency hear-ing loss in 1 patient and Grade 2 chronic corneal erosion in 1patient. Most of the late effects described here result from ra-diation dose to structures in close contiguity to the target andwould have definitely resulted with PTas well, and could notbe spared with protons without underdosing the target vol-ume. Notably absent are late effects to the bowel, bladder,heart, or lung from the incidental dose to these structuresif photons had been used for the patients treated for vertebralbody or sacral Ewing’s sarcoma. Also, with 11 lesions in thehead-and-neck area or cranium, there have been remarkablyfew neuroendocrine late effects.
Our cohort of patients has had no second solid tumors todate. However, there is an unusually high cumulative inci-dence (15% at 3 years) of secondary hematologic malig-nancy, including 3 patients with AML and 1 patient withMDS. The risk of secondary tumor after standard treatmentsfor Ewing’s sarcoma has been previously reported; it rangesfrom 1% to more than 20%, depending on the type and cu-mulative dose of chemotherapy, as well as type and doseof radiation therapy and duration of follow-up (32–36).These rates include both solid and hematologicmalignancies. Our study did not show any solid secondary

Proton radiation for Ewing’s sarcoma d B. ROMBI et al. 1147
tumors, the actuarial rate of AML/MDS at 3 year was 15%.Although most studies show overall rates of 2% to 2.5% ofsecondary AML/MDS (1, 37), recent data from St. JudeChildren’s Research Hospital reveal that rates may behigher than initially reported. Navid et al. report a 6.4%cumulative incidence of secondary hematologicalmalignancies in their Ewing’s cohort, occurring in thepatients treated on recent protocols that have includeddoxorubicin, etoposide, ifosfamide, cyclophosphomide, aswell as G-CSF (38). Rodriguez-Galindo et al. report evenhigher cumulative incidence of secondary AML/MDS at 4years 7.9%, for the group of patients who received more in-tensive chemotherapy that included large doses of alkyla-tors, topoisomerase II inhibitors, and G-CSF factors basedon the EW (Ewing Sarcoma) 92 protocol, whereas in theEW87 group treated with less intensive doses of chemother-apy, the cumulative incidence is 0% (39). Bhatia et al. reporta cumulative incidence of MDS/AML of 11% at 5 years inthe patients with metastatic disease treated with high-intensity therapy on (Intergroup Ewing’s trial) INT-0091,which included higher doses of doxorubicin, cyclophospha-mide, and ifosfamide. It is unclear whether our increasedrate of secondary leukemias is a true reflection of the riskfor patients treated with aggressive regimens that includea topoisomerase II inhibitior or is instead a chance occur-rence in a relatively small series (36). Although multiplestudies have shown that radiation therapy in the setting ofknown leukemogenic therapies does not significantly in-crease the risk of second leukemias (36, 40), certainlyradiation alone and with alkylating agents raises the risk ofsecondary solid tumors (41–43).
Our relatively high cumulative incidence of secondaryleukemia in this PT cohort raises the question of whetherPT may somehow increase the risk of secondary leukemia.
Although long-term follow-up data seem to show a de-creased risk of second malignancy in a PT cohort, this studydid not specifically look at the risk of secondary leukemiasafter treatment (44). Because this is the only elevated rate ina PT cohort, it is reasonable to continue to treat patientswith Ewing’s sarcoma with PT but to be cognizant in thefuture and monitor rates of secondary leukemias as wellas solid tumors. There is another possible explanation:Tumor in proximity to bone marrow may cause a local en-vironment of tumor-related cytokines that predisposes tosecondary leukemia in the setting of certain chemother-apies. The PT cohort is made up exclusively of axiallylocated tumors that are in close proximity to bone marrow,and this may account for the increased rates observed. Aretrospective look at the secondary cases enrolled in coop-erative group studies should help to delineate whether loca-tion of tumor predisposes to secondary leukemias. Themost likely explanation is that this is a statistical aberrationin a small cohort, but this will need to be evaluated furtherin future studies.
CONCLUSION
In summary, we provide evidence of good early clinicaloutcomes using PT for patients with Ewing’s sarcoma. Pro-ton radiotherapy is well tolerated, with few acute affects andlow rates of late side effects. The physical properties of pro-tons reduce irradiation of healthy tissue without decreasingtarget coverage or compromising disease control. Althoughthe follow-up is short, failures are typically seen within 2years, and these early disease outcomes are comparablewith those in the literature. Longer follow-up time is neededto more fully assess tumor control and late effects oftreatment.
REFERENCES
1. Grier HE, Krailo MD, Tarbell NJ, et al. Addition of ifosfamideand etoposide to standard chemotherapy for Ewing’s sarcomaand primitive neuroectodermal tumor of bone. N Engl J Med2003;348:694–701.
2. Marina NM, Pappo AS, Parham DM, et al. Chemotherapydose-intensification for pediatric patients with Ewing’s familyof tumors and desmoplastic small round-cell tumors: A feasi-bility study at St. Jude Children’s Research Hospital. J ClinOncol 1999;17:180–190.
3. Cotterill SJ, Ahrens S, Paulussen M, et al. Prognostic factors inEwing’s tumor of bone: Analysis of 975 patients from the Eu-ropean Intergroup Cooperative Ewing’s Sarcoma Study Group.J Clin Oncol 2000;18:3108–3114.
4. Bacci G, Mercuri M, Longhi A, et al. Neoadjuvant chemo-therapy for Ewing’s tumour of bone: Recent experience atthe Rizzoli Orthopaedic Institute. Eur J Cancer 2002;38:2243–2251.
5. Bacci G, Picci P, Cherlinzoni F, et al. Localized Ewing’s sar-coma of bone: Ten years experience at the Istituto OrtopedicoRizzoli in 124 cases treated with multimodal therapy. Eur JCancer Clin Oncol 1985;21:163–173.
6. Bacci G, Toni A, Avella M, et al. Long-term results in 144localized Ewing’s sarcoma patients treated with combinedtherapy. Cancer 1989;63:1477–1486.
7. Wilkins RM, Pritchard DJ, Burgert EO Jr., et al. Ewing’s sar-coma of bone. Experiences with 140 patients. Cancer 1986;58:2551–2555.
8. Burgert EO Jr., Unni KK. The role of radiation therapy in themanagement of nonmetastatic Ewing’s sarcoma of bone.Report of the Intergroup Ewing’s sarcoma study. Int J RadiatOncol Biol Phys 1981;7:141–145.
9. J€urgens H, Bier V, Dunst J, et al. The German Society of Pedi-atric Oncology Cooperative Ewing Sarcoma Studies CESS 81/86: Report after 6 1/2 years. Klin Padiatr 1988;200:243–252.
10. Dunst J, Sauer R, Burgers JM, et al. Radiotherapy in Ewing sar-coma: Current results of the German Society of Pediatric On-cology studies CESS 81 and CESS 86. Klin Padiatr 1988;200:261–266.
11. Jurgens H, Exner U, Gardner H, et al. Multidisciplinary treat-ment of primary Ewing’s sarcoma of bone. A 6-year experienceof a European cooperative trial. Cancer 1988;61:23–32.
12. Craft AW, Cotterill SJ, Bullimore JA, et al. Long-term resultsfrom the first UKCCSG Ewing’s Tumour Study (ET1). UnitedKingdom Children’s Cancer Study Group (UKCCSG) and theMedical Research Council Bone SarcomaWorking Party. Eur JCancer 1997;33:1061–1069.
13. Donaldson SS, Torrey M, Link MP, et al. A multidisciplinarystudy investigating radiotherapy in Ewing’s sarcoma: End

1148 I. J. Radiation Oncology d Biology d Physics Volume 82, Number 3, 2012
results of POG #8346. Pediatric Oncology Group. Int J RadiatOncol Biol Phys 1998;42:125–135.
14. Shankar AG, Pinkerton CR, Atra A, Ashley S, et al. Localtherapy and other factors influencing site of relapse in patientswith localised Ewing’s sarcoma. United Kingdom Children’sCancer Study Group (UKCCSG). Eur J Cancer 1999;35:1698–1704.
15. Elomaa I, Blomqvist CP, Saeter G, et al. Five-year results inEwing’s sarcoma. The Scandinavian Sarcoma Group experi-ence with the SSG IX protocol. Eur J Cancer 2000;36:875–880.
16. Schuck A, Ahrens S, PaulussenM, et al. Local therapy in local-ized Ewing tumors: Results of 1058 patients treated in theCESS 81, CESS 86, and EICESS 92 trials. Int J Radiat OncolBiol Phys 2003;55:168–177.
17. Isacsson U, Hagberg H, Johansson KA, et al. Potential advan-tages of protons over conventional radiation beams for paraspi-nal tumours. Radiother Oncol 1997;45:63–70.
18. Paganetti H, Niemierko A, Ancukiewicz M, et al. Relativebiological effectiveness (RBE) values for proton beam therapy.Int J Radiat Oncol Biol Phys 2002;53:407–421.
19. ICRU ( International Commission on Radiation Units andMea-surements) Report 78. Prescribing, recording, and reportingproton-beam therapy. J ICRU 2007;7:21–28.
20. Kalbfleisch J, Prentice R. The statistical analysis of failure timedata. New York, NY: Wiley; 1980.
21. DeLaney TF. Clinical proton radiation therapy research at theFrancis H. Burr Proton Therapy Center. Technol Cancer ResTreat 2007;6:61–66.
22. MacDonald SM, DeLaney TF, Loeffler JS. Proton beam irradi-ation. Cancer Invest 2006;24:199–208.
23. Levin WP, Kooy H, Loeffler, et al. Proton beam therapy. Br JCancer 2005;8:849–854.
24. Yock T, Schneider R, Friedmann A, et al. Proton radiotherapyfor orbital rhabdomyosarcoma: Clinical outcome and a dosi-metric comparison with photons. Int J Radiat Oncol BiolPhys 2005;63:1161–1168.
25. St Clair WH, Adams JA, Bues M, et al. Advantage of protonscompared with conventional X-ray or IMRT in the treatment ofa pediatric patient with medulloblastoma. Int J Radiat OncolBiol Phys 2004;58:727–734.
26. Kozak KR, Adams J, Krejcarek SJ, et al. A dosimetric compar-ison of proton and intensity-modulated photon radiotherapy forpediatric parameningeal rhabdomyosarcomas. Int J Radiat On-col Biol Phys 2009;74:179–186.
27. MacDonald SM, Safai S, TrofimovA, et al. Proton radiotherapyfor childhood ependymoma: Initial clinical outcomes and dosecomparisons. Int J Radiat Oncol Biol Phys 2008;71:979–986.
28. Dunst J, J€urgens H, Sauer R, et al. Radiation therapy in Ewing’ssarcoma: An update of the CESS 86 trial. Int J Radiat OncolBiol Phys 1995;32:919–930.
29. Fuchs B, Valenzuela RG, Inwards C, et al. Complications inlong-term survivors of Ewing sarcoma. Cancer 2003;98:2687–2692.
30. Paulino AC, Nguyen TX, Mai WY. An analysis of primary sitecontrol and late effects according to local control modality in
non-metastatic Ewing sarcoma. Pediatr Blood Cancer 2007;48:423–429.
31. Indelicato DJ, Keole SR, Shahlaee AH, et al. Definitive radio-therapy for ewing tumors of extremities and pelvis: Long-termdisease control, limb function, and treatment toxicity. Int JRadiat Oncol Biol Phys 2008;72:871–877.
32. Kuttesch JF Jr., Wexler LH, Marcus RB, et al. Second ma-lignancies after Ewing’s sarcoma: Radiation dose-dependency of secondary sarcomas. J Clin Oncol 1996;14:2818–2825.
33. Strong LC, Herson J, Osborne BM, et al. Risk of radiation-related subsequent malignant tumors in survivors of Ewing’ssarcoma. J Natl Cancer Inst 1979;62:1401–1406.
34. Bacci G, Longhi A, Barbieri E, et al. Second malignancy in597 patients with ewing sarcoma of bone treated at a singleinstitution with adjuvant and neoadjuvant chemotherapy be-tween 1972 and 1999. J Pediatr Hematol Oncol 2005;27:517–520.
35. McLean TW, Hertel C, Young ML, et al. Late events in pe-diatric patients with Ewing sarcoma/primitive neuroectoder-mal tumor of bone: The Dana-Farber Cancer Institute/Children’s Hospital experience. J Pediatr Hematol Oncol1999;21:486–493.
36. Bhatia S, Krailo MD, Chen Z, et al. Therapy-related myelodys-plasia and acute myeloid leukemia after Ewing sarcoma andprimitive neuroectodermal tumor of bone: A report from theChildren’s Oncology Group. Blood 2007;109:46–51.
37. Granowetter L, Womer R, Devidas M, et al. Dose-intensifiedcompared with standard chemotherapy for nonmetastatic Ew-ing sarcoma family of tumors: A Children’s Oncology GroupStudy. J Clin Oncol 2009;27:2536–2541.
38. Navid F, Billups C, Liu T, et al. Second cancers in patients withthe Ewing sarcoma family of tumours. Eur J Cancer 2008;44:983–991.
39. Rodriguez-Galindo C, Poquette CA, Marina NM, et al. Hema-tologic abnormalities and acute myeloid leukemia in childrenand adolescents administered intensified chemotherapy forthe Ewing sarcoma family of tumors. J Pediatr Hematol Oncol2000;22:321–329.
40. Pui CH, Ribeiro RC, Hancock ML, et al. Acute myeloid leuke-mia in children treated with epipodophyllotoxins for acute lym-phoblastic leukemia. N Engl J Med 1991;325:1682–1687.
41. Meadows AT, Friedman DL, Neglia JP, et al. Second neo-plasms in survivors of childhood cancer: Findings from theChildhood Cancer Survivor Study cohort. J Clin Oncol 2009;27:2356–2362.
42. Blatt J, Olshan A, Gula MJ, et al. Second malignancies in very-long-term survivors of childhood cancer. Am J Med 1992;93:57–60.
43. Tucker MA, Coleman CN, Cox RS, et al. Risk of second can-cers after treatment for Hodgkin’s disease. N Engl J Med 1988;318:76–81.
44. Chung C, Keating N, Yock T, et al. Comparative analysis ofsecond malignancy risk in patients treated with proton therapyversus conventional photon therapy. Int J Radiat Oncol BiolPhys 2008;72:S8.




















