Perspectives in Implementing Radiogenomics to Radiotherapy
8
Perspectives in Implementing Radiogenomics to Radiotherapy William Tyler Tran, RTT, BSc, MSc(c) a * and Carol Gillies, RTT, MSc, FCAMRT a,b a Odette Cancer Centre, Sunnybrook Health Sciences Centre b University of Toronto Received 21 July 2009; revised 17 March 2010; accepted 18 March 2010 ABSTRACT Genomics is the study of all nucleotide sequences, including struc- tural genes, regulatory sequences and noncoding DNA segments, in the chromosomes of an organism. Radiogenomics focuses on the underlying genetic causes of cellular responses to radiation and its applications to radiation oncology practice. The purpose of this review is to introduce the technology behind radiogenomics and discuss how it may impact radiotherapy practice for practi- tioners. A literature search was conducted on PubMed using the key words genomics, genes, pharmacogenomics, radiogenomics, dose painting and dose sculpting. A review of the literature shows much promise for future radiation oncology health care practices. Current findings from radiogenomics research require much work in translational research via rigorous testing, evaluation and valida- tion to corroborate data and research methodologies. This review consolidates the theoretical basis of radiogenomics research and discusses the considerations of genomics technology in the context of how it will impact radiotherapy practice. The promise of radiogenomics applications holds a future role in identifying tissue-specific radiation resistance and tolerance by identifying genes responsible for radiobiological response. RE ´ SUME ´ La ge ´nomique est l’e ´tude de toutes les se ´quences nucle ´otides, in- cluant les ge `nes de structure, les re ´gions re ´gulatrices et les segments d’ADN non code ´s et les chromosomes d’un organisme. La radioge ´- nomique met l’accent sur les causes ge ´ne ´tiques sous-jacentes des re ´- ponses cellulaires au rayonnement et leur application en radio- oncologie. Le but de cette e ´tude documentaire est de pre ´senter la technologie utilise ´e en radioge ´nomique et de voir comment cette technologie peut influencer la pratique de la radiothe ´rapie pour les praticiens. Une e ´tude documentaire a e ´te ´ mene ´e (en anglais) sur PubMed a ` partir des mots-cle ´s suivants : genomics, genes, pharmaco- genomics, radiogenomics, dose painting, dose sculpting. L’examen de la documentation montre que l’avenir est prometteur pour la pratique de la radio-oncologie. Il faudra beaucoup de travail de recherche translationnelle, par des essais rigoureux, des e ´valuations et des validations pour corroborer les donne ´es et les me ´thodologies des e ´tudes de radioge ´nomique actuelles. Cette e ´tude documentaire consolide la base the ´orique de la recherche en radioge ´nomique et aborde la question de la technologie de la radioge ´nomique dans le contexte des re ´percussions sur la pratique de la radiothe ´rapie. Les applications de radioge ´nomique promettent de jouer un ro ˆle futur dans l’identification de la re ´sistance et de la tole ´rance spe ´cifiques des tissus au rayonnement par l’identification de ge `nes responsables de la re ´ponse radiobiologique. Introduction Close attention was paid to scientific research conducted in the 1990s that involved the Human Genome Project. The project coordinated findings with respect to unraveling the unknowns of human gene sequences and their function. By identifying these genes, researchers proposed that it would lead to other discoveries that would have significant implica- tions toward the understanding of disease, human systems bi- ology and physiology. Futhermore, understanding the genes involved in malignant transformation may lead to improved diagnostics, predictive markers of treatment responses, gene expression profiles for revised tumour classification and clini- cal outcome, and the development of targeted therapeutics against select genes [1–5]. Ultimately, this gained knowledge would hold great promise to applications in medicine. In recent years, the study of the genome (termed genomics) has increased in popularity within the medical community, particularly as predictive tools in drug response, termed phar- macogenomics. The study of pharmacogenomics examines cor- relations between genotypic (gene trait) and phenotypic (physical trait) variability in drug response. In radiation on- cology, researchers are interested in understanding not drug response, but medical radiation response. Hence the term * Corresponding author: William Tyler Tran, 2075 Bayview Avenue, Toronto, Ontario, Canada, M4N 3M5. E-mail address: [email protected] (W.T. Tran). 1939-8654/$ - see front matter Ó 2010 Elsevier Inc. All rights reserved. doi: 10.1016/j.jmir.2010.03.005 Journal of Medical Imaging and Radiation Sciences 41 (2010) 79-86 Journal of Medical Imaging and Radiation Sciences Journal de l’imagerie médicale et des sciences de la radiation www.elsevier.com/locate/jmir
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Perspectives in Implementing Radiogenomics to Radiotherapy
Journal of Medical Imaging and Radiation Sciences
Journal of Medical Imaging and Radiation Sciences 41 (2010) 79-86
Journal de l’imagerie médicaleet des sciences de la radiation
www.elsevier.com/locate/jmir
Perspectives in Implementing Radiogenomics to Radiotherapy
William Tyler Tran, RTT, BSc, MSc(c)a* and Carol Gillies, RTT, MSc, FCAMRTa,b
a Odette Cancer Centre, Sunnybrook Health Sciences Centreb University of Toronto
Received 21 July 2009; revised 17 March 2010; accepted 18 March 2010
ABSTRACT
Genomics is the study of all nucleotide sequences, including struc-tural genes, regulatory sequences and noncoding DNA segments,in the chromosomes of an organism. Radiogenomics focuses on
the underlying genetic causes of cellular responses to radiationand its applications to radiation oncology practice. The purposeof this review is to introduce the technology behind radiogenomics
and discuss how it may impact radiotherapy practice for practi-tioners. A literature search was conducted on PubMed using thekey words genomics, genes, pharmacogenomics, radiogenomics,
dose painting and dose sculpting. A review of the literature showsmuch promise for future radiation oncology health care practices.Current findings from radiogenomics research require much workin translational research via rigorous testing, evaluation and valida-
tion to corroborate data and research methodologies. This reviewconsolidates the theoretical basis of radiogenomics research anddiscusses the considerations of genomics technology in the context
of how it will impact radiotherapy practice. The promise ofradiogenomics applications holds a future role in identifyingtissue-specific radiation resistance and tolerance by identifying
genes responsible for radiobiological response.
* Corresponding author: William Tyler Tran, 2075 Bayview Avenue,
Toronto, Ontario, Canada, M4N 3M5.
E-mail address: [email protected] (W.T. Tran).
1939-8654/$ - see front matter � 2010 Elsevier Inc. All rights reserved.
doi: 10.1016/j.jmir.2010.03.005
RESUME
La genomique est l’etude de toutes les sequences nucleotides, in-cluant les genes de structure, les regions regulatrices et les segmentsd’ADN non codes et les chromosomes d’un organisme. La radioge-
nomique met l’accent sur les causes genetiques sous-jacentes des re-ponses cellulaires au rayonnement et leur application en radio-oncologie. Le but de cette etude documentaire est de presenter la
technologie utilisee en radiogenomique et de voir comment cettetechnologie peut influencer la pratique de la radiotherapie pour lespraticiens. Une etude documentaire a ete menee (en anglais) sur
PubMed a partir des mots-cles suivants : genomics, genes, pharmaco-genomics, radiogenomics, dose painting, dose sculpting. L’examende la documentation montre que l’avenir est prometteur pour lapratique de la radio-oncologie. Il faudra beaucoup de travail de
recherche translationnelle, par des essais rigoureux, des evaluationset des validations pour corroborer les donnees et les methodologiesdes etudes de radiogenomique actuelles. Cette etude documentaire
consolide la base theorique de la recherche en radiogenomique etaborde la question de la technologie de la radiogenomique dans lecontexte des repercussions sur la pratique de la radiotherapie. Les
applications de radiogenomique promettent de jouer un role futurdans l’identification de la resistance et de la tolerance specifiquesdes tissus au rayonnement par l’identification de genes responsables
de la reponse radiobiologique.
Introduction
Close attention was paid to scientific research conducted inthe 1990s that involved the Human Genome Project. Theproject coordinated findings with respect to unraveling theunknowns of human gene sequences and their function. Byidentifying these genes, researchers proposed that it wouldlead to other discoveries that would have significant implica-tions toward the understanding of disease, human systems bi-ology and physiology. Futhermore, understanding the genes
involved in malignant transformation may lead to improveddiagnostics, predictive markers of treatment responses, geneexpression profiles for revised tumour classification and clini-cal outcome, and the development of targeted therapeuticsagainst select genes [1–5]. Ultimately, this gained knowledgewould hold great promise to applications in medicine.
In recent years, the study of the genome (termed genomics)has increased in popularity within the medical community,particularly as predictive tools in drug response, termed phar-macogenomics. The study of pharmacogenomics examines cor-relations between genotypic (gene trait) and phenotypic(physical trait) variability in drug response. In radiation on-cology, researchers are interested in understanding not drugresponse, but medical radiation response. Hence the term

Figure 1. 1) DNA (genes) translates to 2) mRNA, which in turn elicits 3) pro-
tein synthesis for 4) protein production modulating biological and phenotyp-
ical expression.
radiogenomics was coined to describe this branch of genomescience. Radiogenomics measures the relationship between ge-netic variations associated with radiation sensitivity and toxic-ity by using data from genome-wide association studies or bytracking candidate genes suspected of playing a role in radia-tion response.
The current standards of practice for dose prescription inradiation oncology are primarily based on assessing radiobio-logical effects with close consideration to anatomic location,histological type, tumor stage, potential regional nodal in-volvement and normal structures in the region [6]. The aimis to administer an optimal therapeutic ratio by achieving op-timal tumor control while minimizing the probability of nor-mal tissue toxicity. To optimize this ratio, current researchinterests are studying a variety of dosimetric approaches.Some of these approaches, including intensity-modulated ra-diation therapy (IMRT), show promise in reducing peripheraltissue toxicity in some sites [7,8]. Researchers are now lookingat a predictive tool to determine individual limits of radiationresistance and tolerance in both healthy and neoplastic cells.Ultimately, the appropriate radiotherapy regimens will enablepractitioners to use not only dosimetric advances, but also ge-netic knowledge to maximize the therapeutic ratio.
The implications of this technology on radiotherapy practicewill be enormous. It is envisioned that prognostic predictionmodels of cancer genomes will reveal how altered gene expressionprofiles result in resistance to treatment and disease progressionor relapse in the absence of cytotoxic therapy. In turn, this willallow for the enhancement of the therapeutic ratio for improvedtreatment outcomes and reduced treatment morbidity. This ar-ticle will introduce radiogenomics technology and discuss thescientific approach, its challenges and how this technology canbe integrated into current radiotherapy technologies.
Biological Reasoning in Radiogenomics
The underlying biology of our existence lies in our geneticsequence. Our genome is responsible for our physical traitsand physiological regulation. It is our biological blueprint(Figure 1).
Scientists in this century started investigating the benefitsof understanding the genome’s mechanistic properties andhow it might transform health care delivery. In pharmacoge-nomics, drug responses are studied in relation to one’s geneticresponse trademark. This is accomplished mainly by examin-ing pharmacokinetic absorption, distribution, metabolismand excretion. Each of these processes has genes that are re-sponsible for physiological drug response. These responsesrange from drug efficacy to adverse drug reactions. In radio-genomics, ionizing radiation is not administered as are phar-macological drugs. Therefore, absorption, distribution,metabolism and excretion events are not relevant. Eventsthat do occur during radiotherapy administration that mea-sure efficacy and toxicity are described by classical radiobio-logical theory: repair, reassortment, repopulation andreoxygenation. These radiobiological events are products ofunderlying genetic factors that occur when ionizing radiation
80 W.T. Tran and C. Gillies/Journal of Medical Imag
is applied to the human system. In fact, gene products can beseen as nature’s own radiosensitizers and radioprotectors(Table 1).
Radiogenomics research aims to identify genes thatbecome upregulated or downregulated during radiation expo-sure and gene sequences that can act as predictive indicationsof radiotherapy response. Identification of these genes and se-quences includes those that play a role in cellular regulation,mitotic cycling, stress response, apoptosis and intracellularsignaling [10]. Cellular responses to radiation are not an oc-currence of one gene product, but a collaboration of manygene products that culminate in a mediated response [10].
Gene Identification and Technology
The human genome is composed of approximately 3 bil-lion base pairs and up to 25,000 genes [9,10]. These genesand their variants have an important role in the onset andidentification of disease and are also suspected in modulatedradiobiological response phenotypes. Genetic variants can oc-cur in a variety of ways that are not limited to truncations, de-letions or scrambling. In fact, gene variants commonly occuras single nucleotide polymorphisms (SNPs). SNPs are DNAsequence variations that occur when a single nucleotide (A,T, C, or G) in the genome sequence is altered. SNPs comprise90% of naturally occurring sequence variation in the humangenome. When found in certain genes, SNPs can act as bio-logical markers to understanding biological response to ioniz-ing radiation [10]. It is important to stress that SNPsoccurring in a gene do not definitively indicate a functionalor phenotypical modulation. Rather, SNPs may give probabi-listic indications as to how a gene may be expressed in radia-tion toxicity phenotypes.
Gene Expression Profiling
The success of radiotherapy in eradicating a tumor de-pends principally on the total radiation dose given. However,
ing and Radiation Sciences 41 (2010) 79-86
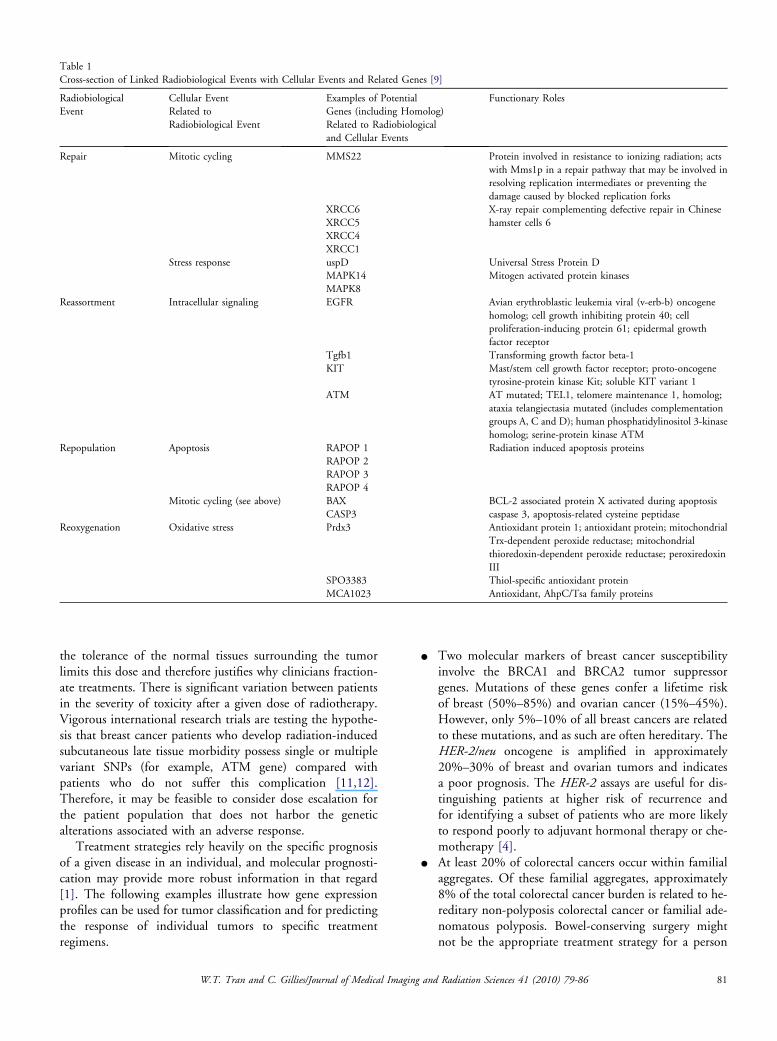
Table 1
Cross-section of Linked Radiobiological Events with Cellular Events and Related Genes [9]
Radiobiological
Event
Cellular Event
Related to
Radiobiological Event
Examples of Potential
Genes (including Homolog)
Related to Radiobiological
and Cellular Events
Functionary Roles
Repair Mitotic cycling MMS22 Protein involved in resistance to ionizing radiation; acts
with Mms1p in a repair pathway that may be involved in
resolving replication intermediates or preventing the
damage caused by blocked replication forks
XRCC6
XRCC5
XRCC4
XRCC1
X-ray repair complementing defective repair in Chinese
hamster cells 6
Stress response uspD
MAPK14
MAPK8
Universal Stress Protein D
Mitogen activated protein kinases
Reassortment Intracellular signaling EGFR Avian erythroblastic leukemia viral (v-erb-b) oncogene
homolog; cell growth inhibiting protein 40; cell
proliferation-inducing protein 61; epidermal growth
factor receptor
Tgfb1 Transforming growth factor beta-1
KIT Mast/stem cell growth factor receptor; proto-oncogene
tyrosine-protein kinase Kit; soluble KIT variant 1
ATM AT mutated; TEL1, telomere maintenance 1, homolog;
ataxia telangiectasia mutated (includes complementation
groups A, C and D); human phosphatidylinositol 3-kinase
homolog; serine-protein kinase ATM
Repopulation Apoptosis RAPOP 1
RAPOP 2
RAPOP 3
RAPOP 4
Radiation induced apoptosis proteins
Mitotic cycling (see above) BAX BCL-2 associated protein X activated during apoptosis
CASP3 caspase 3, apoptosis-related cysteine peptidase
Reoxygenation Oxidative stress Prdx3 Antioxidant protein 1; antioxidant protein; mitochondrial
Trx-dependent peroxide reductase; mitochondrial
thioredoxin-dependent peroxide reductase; peroxiredoxin
III
SPO3383 Thiol-specific antioxidant protein
MCA1023 Antioxidant, AhpC/Tsa family proteins
the tolerance of the normal tissues surrounding the tumorlimits this dose and therefore justifies why clinicians fraction-ate treatments. There is significant variation between patientsin the severity of toxicity after a given dose of radiotherapy.Vigorous international research trials are testing the hypothe-sis that breast cancer patients who develop radiation-inducedsubcutaneous late tissue morbidity possess single or multiplevariant SNPs (for example, ATM gene) compared withpatients who do not suffer this complication [11,12].Therefore, it may be feasible to consider dose escalation forthe patient population that does not harbor the geneticalterations associated with an adverse response.
Treatment strategies rely heavily on the specific prognosisof a given disease in an individual, and molecular prognosti-cation may provide more robust information in that regard[1]. The following examples illustrate how gene expressionprofiles can be used for tumor classification and for predictingthe response of individual tumors to specific treatmentregimens.
W.T. Tran and C. Gillies/Journal of Medical Imag
C Two molecular markers of breast cancer susceptibilityinvolve the BRCA1 and BRCA2 tumor suppressorgenes. Mutations of these genes confer a lifetime riskof breast (50%–85%) and ovarian cancer (15%–45%).However, only 5%–10% of all breast cancers are relatedto these mutations, and as such are often hereditary. TheHER-2/neu oncogene is amplified in approximately20%–30% of breast and ovarian tumors and indicatesa poor prognosis. The HER-2 assays are useful for dis-tinguishing patients at higher risk of recurrence andfor identifying a subset of patients who are more likelyto respond poorly to adjuvant hormonal therapy or che-motherapy [4].
C At least 20% of colorectal cancers occur within familialaggregates. Of these familial aggregates, approximately8% of the total colorectal cancer burden is related to he-reditary non-polyposis colorectal cancer or familial ade-nomatous polyposis. Bowel-conserving surgery mightnot be the appropriate treatment strategy for a person
ing and Radiation Sciences 41 (2010) 79-86 81

with non-polyposis colorectal cancer or familial adeno-matous polyposis who has an increased likelihood ofsubsequent colon malignancies than for an individualwithout a genetic predisposition. High-dose radiationtherapy with concurrent chemotherapy might be themost appropriate therapeutic intervention.
In these two examples, treatment interventions would beindividually tailored according to the patients’ gene expressionprofiles.
Current Studies in Radiogenomics
Radiogenomics research is underway through a variety ofscientific venues. Some of these studies include: GENEPI,RAPPER, GENEPAR and RADGENOMICS and are con-ducted in most of the industrialized world. Translational re-search is imperative to analyze sort, and integrate data intopractical uses. For example, the study Radiogenomics: Assess-ment of Polymorphisms for Predicting the Effects of Radio-therapy (RAPPER) aims to extract DNA from the bloodsamples of 2,200 patients with breast, prostate, gynecologicalor rectal cancers who undergo/underwent curative radiother-apy. RAPPER is designed to explore associations betweenSNPs and radiotherapy toxicity. The objective of this geno-typing study is to provide a means of identifying radiosensi-tive patients and lead to a greater individualization ofradiation dose prescription to optimize tumor control whilereducing variability in normal tissue radiation response andtoxicity. The integration of genetic profiling into radiotherapypractice would allow an increase in tumor dose for radiation-tolerant patients, increasing their probability of localrecurrence-free survival.
Current radiogenomic studies are summarized in Table 2.
Imaging Technologies and Radiogenomics
Although traditional radiographic imaging is a routine partof radiotherapy practice and is very useful in patient position-ing during treatment, it has little use in delineating variationsin tissue phenotypes and limitations in tracking tumor re-sponses during treatment. Studies using other imaging modal-ities with specific gene expression patterns may contributeto the diagnosis, prognosis and potential gene expression–associated treatment responses of various forms of cancer(Table 3).
Table 2
Summary of Radiogenomics Studies and Data Targets
Study Sites Data Colle
GENE-PARE [10] Breast, prostate, head and neck Genes stud
GENEPI [13] Breast, prostate, head and neck,
rectum
Collaborat
RAPPER [14] Breast, prostate, gynecological 50 candida
and cytoki
RADGENOMICS [15] Breast, cervix, prostate, head
and neck
DNA repa
programm
82 W.T. Tran and C. Gillies/Journal of Medical Imag
Fluorodeoxyglucose (FDG)-positron emission tomography(PET) as a functional imaging tool serves to produce a volu-metric map of radiobiological factors in tumor and healthytissue. It is used for diagnosis, staging and monitoring cancertreatment in Hodgkin disease, non-Hodgkin lymphoma andlung cancer; in searching for tumor metastases; and for recur-rence by accurately measuring glucose metabolism. The indi-cations that might prompt a PET scan include new orsuggestive symptoms, equivocal or suspicious findings on clin-ical examination and equivocal or abnormal radiographic re-sults. FDG-PET is useful in the tracking of cellular changesand activities such as glucose metabolism, cell division andhypoxia [17]. Metabolic activities can be indicators of cellularfunction and therefore can be used as interpretative data ingene expression. FDG-PET would be a useful tool in alliancewith radiogenomics studies to track the predicted outcome oftumor response, inherently by taking advantage of its capabil-ity to delineate the extent of disease and therefore offers bothdiagnostic and staging capabilities in one approach [17].
Hypoxia
A considerable amount of research has focused on tumorhypoxia in treatment outcomes, with particular interest inthe genes regulating hypoxic events in vivo. Several imagingtechniques designed for measuring tissue and tumor oxygen-ation are emerging, that is, blood oxygen level-dependentmagnetic resonance (MR), flow and oxygen-dependent MR,PET and dynamic enhanced MR imaging.
Glioblastoma multiforme is the most common and lethalprimary adult brain tumor. MR imaging with its ability to ex-tract structural, compositional, physiological and functionalinformation can capture multidimensional in vivo portraitsof glioblastoma multiforme. A study conducted by Diehn etal. [18] identified an ‘‘infiltrative imaging phenotype’’ amongglioblastoma multiforme patients with hypoxia phenotypes ashaving a greater tendency toward multiple tumor foci and sig-nificantly shorter survival. They found that correlation of con-trast enhancement with hypoxia-associated gene signatureslikely reflects the presence of dysfunctional vasculature in hyp-oxic regions of tumors. They surmised that this radiopheno-type could potentially be used as an imaging biomarker forselecting patients for antiangiogenic therapy. Prospectivestudies are also being done in the assessment of hypoxia-associated markers in head and neck and esophageal cancers.In essence, identifying gene variants and the genes responsible
ction Approach
ied: ATM, TGFB1, XRCC1, XRCC3, SOD2, and hHR21
ive network with tissue data bank
te genes examined; DNA damage response, cell cycle checkpoint control,
nes
ir genes, cell cycle genes, oncogenes, tumor suppressor genes, genes for
ed cell death, genes for signal transduction, and genes for oxidative processes
ing and Radiation Sciences 41 (2010) 79-86

Table 3
Imaging Modalities, Adapted from Stone et al, 2000 [16]
Imaging Modality Can Provide Information and be Used for:
Anatomical imaging Mainstay of diagnosis and treatment planning
Physiologic imaging Determine macroscopic blood flow (angiography,
MRI)
Blood volume or permeability (dynamic CT or MRI,
PET)
Tissue structure (diffusion-weighted MRI, MT-
weighted MRI)
Traditional ‘‘X-rays’’ Little definition of soft tissues
CT Additional soft-tissue definition
MRI and MRS Tumor volume, cerebral blood flow and volume,
vessel permeability, tissue water diffusion, blood
oxygenation, pH, and cellular metabolites
Functional imaging Tissue states (for example, fibrosis), activity of proteins
(eg, activation of TGFB), and about specific cell
events (for example, inflammation)
SPECT and PET Glucose metabolism, cell proliferation, angiogenesis,
cerebral blood flow, capillary permeability, hypoxia,
drug delivery and reporter gene expression
MRI, magnetic resonance imaging; CT, computed tomography; PET,
positron emission tomography; MT, magnetization transfer; MRS, mag-
netic resonance spectroscopy; TGFB, transforming growth factor beta;
SPECT, single photon emission computed tomography.
Figure 2. Dosimetrists will plan around areas of high radioresistance and areas
of lower radioresistance. The surrounding tissue will be dosed according to
their predicted radiation tolerances; a concept commonly known as ‘‘dose
painting.’’ The different lines within the anatomical structures represent dif-
ferent regions of predicted radiation response.
for hypoxia can enhance the disease profile portrait when cou-pled with radiogenomics data [19].
These imaging advances alongside clinical laboratory datawill give practitioners an improved perspective for treatmentplanning approaches to the target volumes.
Devising Dose Sculpting Models Based on Biological Data: AProstate Example
Dose sculpting refers to creating multiple subtargetvolumes within one larger target volume using three-dimensional planning techniques such as IMRT. The ratio-nale behind dose sculpting is that different regions withinthe Gross Tumour Volume (GTV) can have varying degreesof radioresponsiveness and may benefit from creating doseconstraints to these multiple regions of interest. An exampleis given in a prostate model (Figure 2). The initial dosimetricplan would entail a non-uniform dose pattern to multiplesubregions dependent on their predicted radiation responseprofiles and could be modified as the patient progressesthrough treatment [20]. This can potentially be achievedthrough imaging (for example, PET, MR), and the histolog-ical data attained from these imaging modalities could be usedto selectively obtain tissue biopsies from regions of interestwithin the prostate itself. These multiple regions would revealgenetic expression profiles that would allow the clinician tothen decide on how he or she would contour and constrainthe dose to these targeted areas. Therefore, these approachesmay soon have applications for the prediction and trackingof individual patient treatment response and judicial selectionof molecular targeting based on specific tumor cell signaling[20].
How radiogenomics technology could be used is explainedin the following example:
W.T. Tran and C. Gillies/Journal of Medical Imag
When Patient X initially visits the health care practitioner’soffice for symptom assessment, the clinician will pursue a se-ries of diagnostic tests that can include routine blood work,special serum analysis, urinalysis or radiograph to elucidatethe nature and origin of the symptoms. The test results willbe used to determine the most appropriate treatment ap-proach. Often the histopathology is the key component inthe diagnostic workup because it will determine what treat-ment approaches will be best suited for the patient. Tumor,nodal involvement and metastatic prevalence will remain anessential diagnostic tool with special attention to the geneticand cellular behaviors of disease that can be acquired by radio-genomics testing. This test would involve prostate tissuebiopsy to obtain information regarding disease prevalenceand radiotoxic susceptibility to the subregions of the prostate.Other regions of interest such as the bladder, small bowel,seminal vesicles, femoral heads and rectum will be assessed us-ing radiogenomics biomarkers that can be found in bloodsamples. The patient will receive an individualized treatmentprescription that is, multivariable at differential treatment lo-cations (for example, dependent on patient physiology andanatomy, the location of the cancer within the lobes of theprostate, the radiosensitivity of adjacent tissues/organs andareas of hypoxia, Gleason scoring). This individualized treat-ment regimen will extend to changes to the fractionationscheme. Future implications to fractionation will be chal-lenged to reflect the predicted response and tolerance accord-ing to cellular repair, reoxygenation, repopulation andreassortment processes that occur between fractions. The pre-scription will therefore attempt to achieve a maximum attain-able therapeutic ratio with consideration given to dosetolerances of the surrounding tissue and differential radiationresponse regions within the tumor itself. This approach willreplace the traditional ‘‘cookie-cutter’’ dose regimens. Under-standing the molecular pathways of cellular injury and tissuefibrosis will modify the severity of acute and chronic radiationinjuries and will benefit the patient by reducing acute side ef-fects that can be predicted before the treatment is delivered. In
ing and Radiation Sciences 41 (2010) 79-86 83

return, health care providers such as radiation therapists, radi-ation oncologists and nurses can customize their patient edu-cation and management decisions based on this information.The radiation planning and delivery method will exploitIMRT approaches, but will also require the clinician to con-tour around multiple subregions of the prostate according tothe harmonized data obtained from histopathology, imagingmodalities and radiogenomics data.
IMRT offers an excellent planning approach because doseconstraints can be created to reflect the desired or predictedoutcomes found in both advanced imaging techniques andlaboratory genetic data. Dose sculpting using IMRT will be-come an established norm in radiation treatment deliverywhere this volumetric map will further exploit inhomoge-neous dose distributions adapted to tumor heterogeneity(that is, desired dose and dose constraints).
Phenotype identification through laboratory and imagingdata will play an important role in determining radiotherapyregimens. However, these predictive factors do not definitivelytranslate into prognostic factors for patients [21]. The conceptof radiogenomics allows for increased approaches in predict-ing patient response, but does not eliminate careful attentionto reactions during the patient’s treatment. There are manyfactors that contribute to treatment response such as dosime-try, the patient’s lifestyle and if other treatments are givenadjuvantly.
Opportunities and Challenges in Radiogenomics Research
The final step of moving toward radiogenomics applica-tions in a clinical setting lies in translational research. Ques-tions about implementing cost effective ways to translatethis technology into everyday clinical practice and the use ofgenetic information are all considerations being undertaken.
Research has to be conducted to assess the efficacy of theseapproaches and whether the assays used in the research labo-ratory can be applied in the clinical settings. Policy makerswill have to examine educational reform to train professionalsand develop the correct physical infrastructure to house andattain samples, results and information channels for patients.It will also be necessary to adequately equalize research prac-tices and, therefore, research results across all studies.
A reporting and analyses documentation strategy to trackpatient progress, reactions and any discrepancies in treatmentdelivery warrants attention. Translational research will dependon the concise understanding of treatment parameters thatlead to scientific results. Therefore, clinical trials must incor-porate all aspects of data that are not limited to the data col-lection of radiogenomic profiles of the patient.
One of the biggest challenges in radiogenomics research isaccessibility of information. To make this technology feasible,scientists across all studies will have to pool their data to strat-ify radiation response gene panels. Tissue specificity, histolog-ical type, sampling data and providing enough statistical dataare all factors that warrant validation, cross-referencing andtranslational analysis. For example, translational analysiswould be important for cross-referencing gene panels with
84 W.T. Tran and C. Gillies/Journal of Medical Imag
radiotoxicity grading. The difficulty lies in how to quantifyand define radiotoxicity, because many practitioners have dif-ferent interpretations and use different grading systems to de-scribe how the patient has reacted to treatment. Therefore,translational research is needed to quantify early and late ad-verse reactions in radiation oncology. Suggestions for a com-mon measure may be through well-established gradingsystems such as Late Effects Normal Tissue-Subjective,Objective, Management, Analytic (LENT-SOMA) [16],Common Toxicity Criteria or Radiation Therapy OncologyGroup (RTOG) Acute Radiation Morbidity Scoring Criteria.Whichever format is chosen, it must be standardized and eas-ily facilitate comparison between studies and allow analysis byother researchers.
Another challenge is insight into identifying other factorsinvolved in gene response. Patients receiving radiation treat-ments will have to be followed vigilantly with respect tointerventions or concurrent therapies (that is, chemotherapy,antioxidant or alternative medicine regimens) and whether so-cioeconomic status or lifestyle increased symptoms of radia-tion toxicity. Radiation treatments must be welldocumented by practitioners to ensure that consistent treat-ment is administered to patients. Practitioners must ensure ac-curate record keeping of deviations in radiation treatment andmanagement of treatment side effects, etc.
Because future implications of radiogenomics informationwill result in refined treatment margins, practitioners will havean increased duty to take necessary measures for volume tar-geting. Site-specific protocols may include mandatory imageguidance to optimize site localization [22]. Because treatmentprescriptions will potentially change from using traditional ra-diobiological fractionation schemes, it is imperative that prac-tice standards reflect the growing demand for more stringentpatient immobilization techniques, image guidance tech-niques and quality assurance in therapy workup (such asdose and treatment volume verification). In the radiogenom-ics era, standardized treatments will be very different and in-dividualization will be the key process from patient to patient.Practitioners will be required to scrutinize each plan toa greater degree to verify treatment site, dose and fractionationregimes, treatment approach and biological response totreatment.
Ethical and Medical Risks to the Patient with the Conduct ofRadiogenomics Testing
Genome-wide association studies are demonstrating rela-tionships between novel gene variants/chromosomal loci andcommon diseases and their phenotypes. Using microarrayanalyses, researchers examine interpersonal differences in in-herited genetic variability and compare the prevalence of thegene variants among patient controls with a given disease.Knowing the lucrative nature of these studies and the publics’desire to know his or her levels of risk for specific conditions,there is an emergence of commercially available personalizedgenome services or gene profiles. Ethical review of
ing and Radiation Sciences 41 (2010) 79-86

information and confidentiality will have to be closely scruti-nized to resolve any potential impacts to the patient.
Before there can be widespread integration of genomic in-formation into clinical practice, practitioners must be aware oflegal, ethical and social implications. The conduct of radioge-nomic research, testing and its implementation is intimatelyassociated with the health care practitioner/patient relation-ship. Also, these technologies may raise questions regardingdiscrimination from employment practices, allocation ofhealth care resources, insurance practices, equitable access togenomic technologies and changes to scopes of practice. Al-though the authors of this article are not medical ethicists,it is noteworthy to include these important considerationswhen implementing radiogenomics technology into clinicalpractice.
Radiogenomic testing for clinical application is subject torigorous evaluation. First is the test’s analytic ability (to accu-rately and reliably measure the genotype of interest). Second isclinical validity (the ability of the test to detect or predict theassociated disorder. Components include the test’s sensitivity,specificity and positive and negative predictive value). Last isthe test’s clinical utility (the balance of its associated risks andbenefits if it were introduced into clinical practice) [23]. Theuse of this information must be explained to the patient un-dergoing radiogenomics testing.
Informed consent will be an important step in allowingdifferent practitioners access to genetic test results and pro-files. Informed consent acknowledges patients’ rights tomake autonomous decisions about their personal values/be-liefs about the genetic information and to make voluntary de-cisions that reflect their health care after adequate disclosureof the specific elements of the genetic-related test, researchor procedure in question. Because radiogenomics technologyhas not been implicated in the treatment process, it is difficultto assess the potential health risks that are involved in the test-ing procedure. Though the risks involved in attaining bloodsamples and tissue biopsies are mainly risks in sterilizationand infection control, these risks are minimal in the industri-alized world. A notable risk to the management of one’shealth (and not a risk to health per se) would be the decisionsthat are made from the genetic data obtained. As the publicseeks safe, credible and reliable radiogenomic testing and in-formation through different venues, it will require profes-sional assistance and counseling to help make sense of thepossible social, psychological, physiological and economic im-plications of the results. It is important to assess patients’ un-derstanding of their risk of illness, reason(s) for wantinggenetic testing and possible outcomes so that they can makeinformed, knowledgeable health care-related decisions.Therefore, radiogenomics technology will have a significantimpact on policy making to ensure that informed consentwill reflect the initial intentions of sample collection. It is a so-cietal concern involving radiogenomic testing because an indi-vidual’s DNA sample collected for other purposes may beused for additional research and testing without the patient’sinformed consent. After testing is complete, there may be fear
W.T. Tran and C. Gillies/Journal of Medical Imag
or misconception that if an individual does not meet definedinclusion criteria, he or she will be denied ‘‘optimal’’ treat-ment or offered treatment perceived as ‘‘inferior.’’
Beneficence will obligate practitioners to do no harm totheir patients and to maximize the possible benefits and min-imize the possible harms of genetic information and testing[24]. Genetic information obtained from family history andradiogenomic testing may reveal information about the healthrisks of the individual patient and of other family memberswho may not be aware of the health concern. Screening familymembers for mutations may be appropriate in hereditarycases, but the appropriateness of screening in asymptomaticpatients depends on test sensitivity, specificity and feasibilitybased on both cost and access [1]. An ethical dilemma arisingfor health care providers is whether they have a moral obliga-tion to inform family members of their potential health risksversus that of respect for the patient’s confidentiality.
Conclusion
Before radiogenomics technology approaches can be im-plemented with confidence, there is much to consider. Nodoubt, this technology holds phenomenal potential in chang-ing health care policy and radiation treatment approaches. Be-cause the scientific community is undergoing rigorous reviewand experimentation, radiation practitioners may be unsureabout how this technology will be implemented, though theideas discussed in this article give some perspectives as tohow the authors foresee this change. Radiogenomics aims tooptimize the therapeutic ratio by looking at genetic factorsthat dictate radioresistance and radiosensitivity. Radiogenom-ics technology can be combined with existing technologies toenhance treatment outcome through predictive and adaptivetesting in radiotherapy. New data will complement classicalradiobiology and give greater insight to how we can optimizemedical sciences in radiation oncology.
References
[1] Ansell, S. M., Ackerman, M. J., Black, J. L., Roberts, L. R., &
Tefferi, A. (2003). Primer on medical genomics, part VI: genomics
and molecular genetics in clinical practice. Mayo Foundation for Med-
ical Education and Research. Mayo Clinical Proc. 78, 307–317.
[2] Williams, PD, Lee, JK, & Theodorescu, D. (2009). Genomancy:
predicting tumour response to cancer therapy based on the oracle of
genetics. Curr Oncol. 16, 56–58.
[3] Nuyten, D. S. A., & van de Vijver, M. J. (2008). Using microarray
analysis as a prognostic and predictive tool in oncology: focus on breast
cancer and normal tissue toxicity. Semin Radiat Oncol. 18, 105–114.
[4] Ren S, Liu S, Howell Jr P, Xi Y, Enkemann SA, Ju J, Riker AI. The im-
pact of genomics in understanding human melanomaprogression and
metastasis, 2008. http://www.medscape.com/viewarticle/578549.
[5] Anundson, S. A., Bittner, M., & Fornance, A. J. Jr. (2003). Functional
genomics as a window on radiation stress signalling. Oncogene. 22,
5828–5833.
[6] Chao, K., Perez, C., & Brad, L. (2002). Radiation Oncology Management
Decisions, (2nd ed.). Philadelphia: Lippincott Williams and Wilkins.
[7] Chao, K. (2002). Protection of salivary function by intensity modulated
radiation therapy in patients with head and neck cancer. Semin Radiat
Oncol. 12, 20–25.
ing and Radiation Sciences 41 (2010) 79-86 85

[8] Zelefsky, M., Fuks, Z., & Happersett, L., et al. (2000). Clinical experi-
ence with intensity modulated radiation therapy (IMRT) in prostate pa-
tients. Radiother Oncol. 55, 241–249.
[9] National Institute of Health: Gene Database. Available online at: http://
www.ncbi.nlm.nih.gov/sites/entrez
[10] West, C., Elliott, R., & Burnett, N. (2007). The genomics revolution
and radiotherapy. Clin Oncol. 19, 470–480.
[11] Ho, A., Atencio, D., & Peters, S., et al. (2006). Genetic predictors of
adverse radiotherapy effects: the GENE-PARE project. Int J Radiat On-
col Biol Phys. 65, 646–655.
[12] Andreassen, C. N., Alsner, J., & Overgaard, J. (2002). Does variability
in normal tissue reactions after radiotherapy have a genetic basis–where
and how to look for it? Radiother Oncol. Vol. 64(2), 131–140.
[13] Baumann, M., Holscher, T., & Begg, A. (2003). Towards genetic pre-
diction of radiation responses: ESTRO’S GENEPI project. Radiother
Oncol. 69, 121–125.
[14] Burnet, N., Elliott, R., & Dunning, A., et al. (2006). Radiosensitivity,
radiogenomics and RAPPER. Clin Oncol. 18, 525–528.
[15] Iwakawa, M., Imai, T., Harada, Y., & Ban, S., et al. (2002). Radgenom-
ics Project. Nippon Igaku Hoshasen Gakkai Zasshi. 62, 484–489.
[16] Stone HB, McBride WH, Coleman CN. Meeting report: modifying
normal tissue damage postirradiation report of a workshop sponsored
by the Radiation Research Program, National Cancer Institute, Be-
thesda, MD, September 6–8, 2000, Radiation Research 157, 204–223
Radiation Research Society.
86 W.T. Tran and C. Gillies/Journal of Medical Imag
[17] Avril, N., & Weber, W. (2005). Monitoring response to treatment in
patients utilizing PET. Radiol Clin N Am. 43, 189–204.
[18] Diehn, M., Nardini, C., Wang, D. S., McGovern, S., Jayaraman, M., &
Liang, Y., et al. (2008). Identification of noninvasive imaging surrogates
for brain tumor gene-expression modules. Natl Acad Sci U S A. 105,
5213–5218.
[19] Coleman, C. N. (2003). Linking radiation oncology and imaging
through molecular biology (or now that therapy and diagnosis have sep-
arated, it’s time to get together again!). 2002 RSNA Annual Oration in
Radiation Oncology. Radiology. 228, 29–35.
[20] Ling, C. L., Humm, J., & Larson, S. T., et al. (2000). Towards multi-
dimensional radiotherapy (MD-CRT) biological imaging and biological
conformality. Int J Oncol Biol Phys. 47, 551–560.
[21] Bentzen, S. (2008). From cellular to high throughput predictive assays
in radiation oncology: challenges and opportunities. Sem Radiat Oncol.
18, 75–88.
[22] Tran, W. T. (2009). Practical considerations in cone beam and ultra-
sound in prostate localization: a review of the literature. J Med Imaging
Radiat Sci. 40, 3–8.
[23] Hunter, D. J., Khoury, M. J., & Drazen, J. M. (2008). Letting the ge-
nome out of the bottle – will we get our wish? New Engl J Med. 358,
105–107.
[24] Ulrich, C. M., Wallen, G. R., & Grady, C. (2008). Ethics and genetics:
what should every advanced practice nurse know? Clin Scholars Rev J
Doct Nurs Pract. 1, 69–71.
ing and Radiation Sciences 41 (2010) 79-86