Pediatric - IAP Kerala
40
1 November 2018 Companion A Publication of Indian Academy of Pediatrics, Kerala State Branch Editor’s Page (3) Message from National Secretary (4) State President’s Message (5) Secretary’s Message (6) ORS preparations (7) Birth Defects Surveillance (12) Rheumatic Pneumonia (14) Journal S nippets (17) Obesity (18) Moments of Glory (19) Refresh ur Radiology (20) Pediatric Photo Quiz (21) Snaps from Branches (22) Wilson’s D isease (23) Answers (24) Pedi-Crossword (38) Vol. 14 Issue 2 Kochi November 2018 Pediatric
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Pediatric - IAP Kerala

1 November 2018
CompanionA Publication of Indian Academy of Pediatrics, Kerala State Branch
Editor’s Page (3)
Message from National Secretary (4)
State President’s Message (5)
Secretary’s Message (6)
ORS preparations (7)
Birth Defects Surveillance (12)
Rheumatic Pneumonia (14)
Journal Snippets (17)
Obesity (18)
Moments of Glory (19)
Refresh ur Radiology (20)
Pediatric Photo Quiz (21)
Snaps from Branches (22)
Wilson’s Disease (23)
Answers (24)
Pedi-Crossword (38)
Vol. 14 Issue 2 Kochi November 2018Pediatric

2 Pediatric Companion

3 November 2018
Editor’s Page
design & production : pixel studio, cochin @ 98460 38143
Dear IAPians,
Year 2018 is about to be over, and what a year!!
This year will be inscribed in golden letters in the history of IAP Kerala. Kunhu sir and Riaz have taken us into another world. A world full of academics, enjoyment, and reunion!
We have achieved 100% of our goals. The President’s Action Plan, VIBGYOR, was a great success, showing our unity, academic excellence and administrative capability.
We are blessed to have Dr Remesh Kumar as our Honorary secretary General. Many of the national programs like united airways and all about fever had come to our own state and we could experience the flavor and taste of great academic feast, sitting in our own small state.
PEDICON Kerala is being organized at Manjeri, within a couple of weeks. We express best of luck to the organizing team. We are also heading towards the national PEDICON at Mumbai. We express our best wishes to IAP national office bearers and the organizing committee for making this event the greatest ever academic program conducted under IAP banner.
Regards,
Dr. M. VijayakumarAddl. Professor, Dept. of PediatricsGovt. Medical College, CalicutMob : 94470 71637Email : [email protected]
President : Dr. Mohammed KunjuVice President : Dr. M. Narayanansecretary : Dr. I. RiazTreasurer : Dr. Johny sebastianJoint secretary : Dr. D. Balachandar Imm. Past President : Dr. M.N. VenkiteswaranPresident Elect : Dr. M.K. santhosh
I A P S tAt e O f f I c e b e A r e r S 2 0 1 8Vice President Elect : Dr. P.R. JayakumarEditor : Dr. M. VijayakumarWebsite Editor : Dr. shibu KizhaketharaNational EB Members : Dr. Jayaraman T.P., Dr. O. Jose Dr. shimmy PouloseWomen’s Wing Co-ordinator : Dr. Prameela Jogi
P e D I At r I c c O M PA N I O N O f f I c e b e A r e r S 2 0 1 8
Dr. Ananda Kesavan T.M. Dr. Babu Francis C.A.Dr. sr. Betty JoseDr. Geeta GovindrajDr. Gireesh s.Dr. Jayakrishnan M.P.Dr. Jayakumar C.Dr. Jayakumar P.R.
Dr. JayasreeDr. Mohammed KunjuDr. Mohandas NairDr. Muhammed M.T.P.Dr. Narayanan M.Dr. Naushad K.Dr. Pisharody P.N.N.Dr. Remesh Kumar R.
Dr. T.V. RaviDr. santhosh M.K.Dr. silvan Mathews GeorgeDr. suresh Kumar E.K.Dr. Tonny MampillyDr. Venkiteswaran M.N.Dr. Zulfikar Ahmed
Advisory BoArd EditoriAl BoArdProf Dr MKC NairProf Dr TU sukumaranProf Dr Kurien ThomasDr shaji Thomas JohnDr Abraham K PaulDr s. s. KamathProf Dr PsN MenonProf Dr sushama BaiProf Dr Parvathy VKProf Dr Lalitha Kailas,Prof Dr Riyaz ADr. P.M.C. Nair
Cover photograph by Rajesh Kuttiadan

4 Pediatric Companion
M E S S A G E F R O M N A T I O N A L S E C R E T A R Y
Dear senior Academicians & Friends in IAP Kerala,
The academy year 2018 is almost through. We at IAP Kerala had a most fruitful year with an array of academic and community oriented activities happening across the state in this period. Almost the entire branch office bearers were on their toes trying to keep pace with the splash of activities unleashed by the Team of Dr Mohammed Kunju & Dr. Riaz. And equal to the task were the supporting OB Team of 2018.
The VIBGYOR, the icon theme for the year, was taken up by our members in a truly fanatic manner. The year also saw a number of innovative activities from IAP Kerala on a joint footing with the state Government. And the media visibility by the members, branches as well as the state was equally laudable.
The Central IAP too had its ratings move up in a mega scale in the current academy year. The vibrant team led by the ever charismatic President Dr santosh T soans was able to convert the aspirations of the entire IAP fraternity into a reality. Apart from the umpteen number of academic programs which covered almost every branch in IAP map, the year set a new bench mark on the social front. We were able to get directly involved in pursuing a number of social measures. Child Advocacy also gained a quantum leap in this period especially in the fight against child abuse and interventions for suicide prevention.
Friends, the IAP Family growth has recently been bound more on emotional terms than academics . This second Family away from home is sure to provide us a better emotional quality driving the positive energy amongst us. Let’s keep this together to maximise our efforts to strengthen the child care system in this country.
Warmth, affection and mutual respect is the key to our success in IAP Kerala. Let us make it a dream unit wherein the budding pediatricians of our state must be most enthused to get involved to have a happy academic and social life.
It is time to voice kudos to the outgoing Team led by Dr Mohameed Kunju, Dr Riaz, Dr Narayanan, Dr. Balachandran and Dr. Jhony sebastian for driving IAP Kerala in a momentous fashion for the past one year. We all are sure the new Team of Dr santosh M.K., Dr. Balachandran, Dr. Jayakumar P.R, Dr. Johny and Dr . Krishnamohan is certain to take IAP Kerala to much more heights in the upcoming Academy Year.
Hearty Congratulations to our Editor, Dr. M. Vijayakumar who has shown unparalleled passion and commitment to nurture our flagship journal in an exemplary manner.
Loving regards,
Jai IAP ! Jai Hind !
Remesh Kumar R.

5 November 2018
P R E S I D E N T ’ S M E S S A G E
Dear IAP brothers and sisters,One more issue of companion. Good gong. Happy to know that there is good acceptance even from outside Kerala. It is with great pleasure and satisfaction that I am signing off as the President of IAP Kerala 2018. It was an eventful year with a multitude of activities and complete involvement of all IAP members of Kerala. It was very much heartening to note that the presidential action plan was taken up by great enthusiasm which has no parallel in the history of IAP. With God Almighty‘s help the presidential action plan could be christened as Vibgyor and the program was kicked off by the short film on epilepsy. The film was aptly titled as Mazhavillu and had depicted how beautiful colours of joy had spread through the life of a little girl. The viewership of more than 1.5 lakhs is a record by itself. From the word “go” the activities of last year was in a great tempo. Immediately after the historic elections the first EB was a great get together with more than hundred members participating. The flagship programme of Vibgyor, “victory over learning disorder” has literally shaken Kerala by unprecedented participation of the members. I must thank all the dear IAP members who had taken classes in both BRC and teachers training programs. Through “improving the knowledge” program, asthma and respiratory awareness programme was done along with the knowledge dissemination about epilepsy. The respiratory symposium itself was again a unique event. simultaneously 12 centres witnessed live CME programme along with an uninterrupted video broadcasting of one major talk by nationally acclaimed speaker. Another big success was the “Battling the disability” program. Formation of downs syndrome support group and autism support program was a great success. “Go for the green” - taking up the youngsters causes was also a grand success. Dissemination of pulse oximetry program and preventive cardiology program was highly appreciated by all. “Overcoming the ordeal” of hypothyroidism and growth retardation was taken up enthusiastically by the endocrine group . Finally “recipe” program was again a huge success were the recipe for self was taken up in a very big manner by the formation of fitness club in various branches, and organisation of badminton and football matches . Culmination of recipe that is the prescription for self during the Manjeri Pedicon by the array of sports activities tells the sustainability of the Vibgyor action plan.
To crown the presidential action plan weeks and Day celebrations, subchapter conferences, national president’s action plans, periodic monthly meetings, member’s individual activities all took place in an uninterrupted manner. All subchapters were competing each other to make the state, annual conferences a huge success. It’s the time to thank all the IAP members from Parassala to Kasaragod. All the EB Members who painstakingly participated in all the executive board meetings has to be specially applauded. special thanks are due to Dr Venkateswaran , immediate past President for all the support and guidance given to me. It’s Dr Riaz state secretary who master minded the year long IAP activities. Indebtedness to Riaz cannot be expressed in words. Vice President Dr Narayan, Treasurer dr Johny sebastian, and joint secretary Dr Balachandar were in their active might. Dr Remesh Kumar was a staunch supporter of Kerala IAP’s activities inspite of his national commitment.Past presidents, all HODs and veteran Pediatricians all has to be specially thanked for their never ending concern for nurturing the mother organization. stewardship of IAP is going to be handed over to an able team headed by Dr M K santhosh. Dr Vijayaumar , the editor is doing a commendable work by bringing out the issues of companion very regularly.I am happy that Manjeri Pedicon is also organised in par with the gold standards of Kerala IAP. The organising committee headed by Dr K K Joshi, is to be complimented profusely for their year-long preparation and selfless dedication in making the pedicon 2018 a memorable event. Let me say good bye to the president ship of 2018 with happy note. Let’s all come together under the umbrella of IAP and keep the unity for years to come. Once again thanking each and every one of you for making everything happen.
Jai IAP - Jai Hind !
Prof. Dr P.A.M. Kunju President, Indian Academy of Pediatrics Kerala 2018DEAN Faculty of Medicine Kerala UniversityProf and Head Dept of Ped Neuro, Medical College Trivandrum

6 Pediatric Companion
S E C R E T A R Y ’ S M E S S A G E
Respected Teachers, seniors and dear friends,
I bring you warm wishes from the State IAP Office!
We are in the last phase of IAP activities during the year. VIBGYOR- the unique action plan rolled out by our dear President, Dr PA Mohammed Kunju has proved to be a grand success by itself. All the branches from Kasaragode to Thiruvananthapuram, small and large, have taken each component of the program to greater heights. starting off with the LD awareness classes (V- Victory to all) to thousands of school teachers all over the state and all set to end with the grand IAP sports Meet, (R- recipe for self) VIBGYOR was one of the greatest ever action plans taken up by IAP, was truly an inclusive one covering all important aspects of child care as well as self-care. I take this opportunity to thank all the branch office bearers and the torch bearers of the component programs from my heart for the excellent execution.
We can be proud that IAP Kerala is currently the most important stakeholder in every programme for children in our state. We are currently a part of the state Immunisation Technical Advisory Group as well as the Infant Mortality Committee. It`s a matter of great pride in almost all districts during the days and week celebrations the district administration as well as the NHM invited our office bearers for jointly organising the sessions. In the national level we are witnessing great changes with Dr R Remeshkumar as our HsG and the excellent CIAP modules prepared by the trio- Dr santhosh soans, Dr Digant shastri and Dr Remeshkumar- are running house full in our state during the last months of the IAP year. We are expecting more much modules for our branches in the next year too. We are always thankful to our exemplary leaders like Dr MKC Nair, Dr T U sukumaran and Dr sachidananda Kammath for their visionary steps which made our dear Academy stand tall among other professional organisations.
I wish all the very best to the new team led by Dr santhosh MK, Dr Balachander D and wish 2019 be a greater year for our dear IAP.
Before I stop I wish to express my profuse thanks to my dear presidents, MNV sir and Kunju sir for guiding me properly, Vijayakumar sir for keeping our journal stand tall always, and the team, Dr Balachandran, Dr Johnny, Dr Parameswaran and Dr Narayanan for being with me through thick and thin over the last two years. Once again I thank my patrons, teachers and friends for the affection and trust bestowed upon me.
Yours sincerely,
Dr. Riaz I.

7 November 2018
dr Kaleem Ahammed, dr Jasir K. (DNB registrars)
dr sajana t.M., dr Kishore suseelan (Specialists in Pediatrics)
Aster Medcity, Kochi
Commercial ORS preparations : A brief analysis
introductionAccording to WHO (World Health Organi-
sation), diarrhoea is the second leading cause of under-five mortality in developing countries, killing at least 525, 000 under five children every year (1). In low-income countries, children under three years old experience on average three episodes of diarrhoea every year. Each episode deprives the child of the nutrition necessary for growth. As a result, diarrhoea is a major cause of malnutrition, and malnourished children are more likely to fall ill from diarrhoea.
Children with diarrhoea are at risk of dying due to dehydration, and early and appropriate fluid replacement is a main intervention to prevent death. Yet few children with diarrhoea in developing countries receive appropriate treatment with oral rehydration therapy and continued feeding. According to UNICEF Global database data (2012) only 34% children with diarrhoea in developing countries have access to ORs (2).
MethodIn the occasion of ORs week 2018, we
collected commercial ORs preparations from 10 different pharmacies in and around Kochi city. We approached pharmacists with generic prescription of ORs and collected both ORs sachets and Ready-to-drink packs. Composition of different brands printed on their label were collected and tabulated.
Composition
All the brands of ORs sachets that we collected were compliant to the new WHO ORs formulation with total osmolality of 245mOsm/l (Table 1). On the other hand, most of ready to drink preparations were non-compliant to WHO formula (Table 2). Majority of these contained lower sodium content and a large amount of
added sugar. It is contrary to basic therapeutic principle of 1:1 molar concentration of sodium and glucose in ORT. WHO recommends that glucose content should be at least equal that of sodium but should not exceed 111 mmol/l. Higher glucose content is in fact thought to increase the incidence of osmotic diarrhoea (3). Many of them contain additional electrolytes like Magnesium, calcium and nutrients like Vitamin C and Taurine. These may have unknown effect in children with diarrhea. For these reasons, one of the ready-to- drink brand bears a warning label – “Not recommended for treatment of diarrhea”; although it is being marketed as ORs.
FlavouringMost of the branded ORs sachets were
flavoured. Although there is theoretical advantage for flavoured ORS in term of better acceptability, the WHO/CDD Programme study on acceptability in Philippines showed neither advantage or disadvantage for flavoured ORS when compared to standard ORs. (4) For this reason and with aim of making ORs available at low price in health system, UNICEF and WHO recommend that governments should use ORs composition that contains only the four basic ingredients. Because of difficulties in controlling the amount of ORs solution consumed per kg of body weight and per day, it is almost impossible to determine whether the consumed doses of colouring and/or flavouring agents are within the safe limits. Although not documented, it also seems that certain flavouring agents can cause allergies and other side effects, particularly in infants and small children.

8 Pediatric Companion
table 1 - Comparison of few commercial ors sachets available in the marketSl
No
Bran
d
Man
ufac
-tu
red
/ M
ar-
kete
d by
Sodi
um
(mm
ol/L
)
Pota
ssiu
m
(mm
ol/L
)
Chlo
ride
(m
mol
/L)
Citr
ate
(mm
ol/L
)
Dext
rose
(m
mol
/L)
Tota
l Osm
(m
mOs
m)
Adde
d su
gar
Addi
tives
Flav
our
ClaimPrice per 200ml of ORS (in Rupees)
1 Electral ® FDC 75 20 65 10 75 245 - - - Based on WHO formula 4.13
2 ORS Alkem 75 20 65 10 75 245 - - OrangeWHO recommended reduced osmolarity
formula3.20
3 ORS Intas 75 20 65 10 75 245 - Orange WHO recommended formula 3.0
4 ORS Powder Unicure 75 20 65 10 75 245 - - -
Kerala Govt.
Supply
5 Prolyte ® Cipla 75 20 65 10 75 245 - - Orange WHO recommended
formula 3.13
6 Rexlyte ® Elder 75 20 65 10 75 245 - - Orange WHO recommended
ORS formula 3.15
table 2 - Composition of few ready to drink ors packs available in the market.
Sl N
o
Bran
d
Man
ufac
-tu
red
/ M
arke
ted
by
Sodi
um
(mm
ol/L
)
Pota
ssiu
m
(mm
ol/L
)
Chlo
ride
(m
mol
/L)
Citr
ate
(mm
ol/L
)
Dext
rose
(m
mol
/L)
Tota
l Osm
(m
mOs
m)
Added sugar Additives Fla-
vour ClaimPrice per 200ml of ORS (in Rupees)
1 Electral ® FDC 75 20 65 10 75 245 - - Apple
Meets WHO recommended ORS
composition22.48
2 Electro + ®
Amrutan-jan 50 20 40 - 75 - 8g/
100ml Vit. C Apple
ORS with added glucose and
electrolytes. Not recommended for treatment of diar-
rhoea
35
3 Electrobi-on Sip ® Merk 50 20 40 - - - 6.8g/
100ml Vit. C Apple Refreshing electro-lyte drink 33
4 Electro-sip ® Ipca 50 20 40 - 75 - 6.8g/
100ml
Vit. C, Zinc, Taurine,
Magnesium, Calcium
OrangeNon-carbonated water based fla-
voured drink37
5 Elecxir ®
Halewood Laborato-
ries75 20 65 10 75 245 - Apple As per revised
WHO formula 25.49
6 Olyte ® Aristo 75 20 65 10 75 245 - Orange WHO recommend-ed formula 27.99
7 ORS Cipla 75 20 65 10 75 245 - - Lemon WHO recommend-ed formula 27
8 ORSL ® Johnson & Johnson 60 20 50 - - - 1g/
100ml Vitamin C AppleScientifically formu-lated to effectively
rehydrate and restore fluid and electrolytes.
35
9 Rebalanz QRS ® Dr Reddy’s 50 20 40 - - - 6.8g/
100mlApple juice
concentrate, Vitamin C
Apple Ready to serve fruit beverage 30
10 Walyte ® Wallace 50 20 40 - 75 - 6.8g/
100mlMagnesium,
Calcium Apple Electrolyte energy drink 35

9 November 2018
Packaging and labellingThe commercial ORs sachets comes with
attractive labels highlighting the added flavour. Most of them does not to comply to the guidelines for labels of ORs (The sample label recommended by UNICEF and WHO is shown in figure 1)(5). Many of the ready-to-drink preparations do not clearly display the concentration of each content and the total osmolality of the solution. This makes difficult for health care workers to verify that the product complies with WHO formula.
Although many sachets clearly displayed the directions of use, method of preparation, storage and administration, some of the sachets lacked it.
The ready to drink ORs is being marketed in attracted tetrapak® packing which is appealing to children. As it is ready to drink, it is much easier for care givers, as well.
PricingORs sachets were found to be much cheaper
when compared to their ready to drink counter parts. On average, ORs sachets costed Rs 3.32 per 200ml sachet, ready to drink preparations costed Rs 34.49 per 200ml pack.
ConclusionORs has been considered the magical solution
to prevent diarrheal deaths in children. Although
widely marketed through government and private pharmaceuticals, awareness about the use of ORs is still lacking in developing countries like India. On analysis ORs sachets and ready to drink preparations, ORs sachets were compliant to WHO formula and were much cheaper. Whereas, many ready to drink preparations high glucose content with low sodium and had additives which had unknown effects in treatment of children with diarrhoea.
rEFErEnCE1. Diarrhoeal disease Key facts scope of diarrhoeal dis-
ease. 2018;(May 2017):1–5. 2. Unicef. Pneumonia and diarrhoea Tackling the deadli-
est diseases for the world’s poorest children [Internet]. United Nations Children’s Fund. 2012. 1-86 p. Avail-able from: http://www.unicef.org/eapro/Pneumo-nia_and_Diarrhoea_Report_2012.pdf
3. GW M. High sugar worse than high sodium in oral rehydration solutions. Acta Paediatr scand 1983 Mar;72(2)161-6 [Internet]. Available from: https://www.ncbi.nlm.nih.gov/pubmed/6340410
4. saniel MC, Zimicki s, Carlos CC, Maria AC, Balis AC MC. Acceptability of rice-based and flavoured glucose-based oral rehydration solutions: a randomized con-trolled trial. J Diarrhoeal Dis Res. 1997;Jun;15(2):
5. N. Bachewar, V. Thawani KG. Are ORs brands in India using the name of WHO judiciously ? Indian J Phar-macol. 2006;38(6):439–41.
Fig. 1 - UniCEF/WHo recommended label on ors packets.

10 Pediatric Companion
Birth Defects SurveillanceIndia lacks a national birth defects survei-
llance. Data on the prevalence of congenital anomalies are available mostly from hospital-based, cross-sectional studies.
First cohort study from India establishes that the congenital anomaly rates were high, affecting one in forty four births in the cohort. The prevalence of congenital anomalies was identical to the stillbirth prevalence in the cohort, highlighting their public health importance.
The Global Burden of Disease study 2013 identified congenital anomalies among the top ten causes of mortality in children less than five years of age.
It’s a leading cause of death in children in this age group in the high-income countries, they are not considered to be significant public health problems in low- and middle-income countries.
(LMIC) due to – 1. low in prevalence -. their proportionate contribution to mortality is significantly lower as compared to other perinatal causes, infections (sepsis, pneumonia and diarrhea) and malnutrition, and 2. their management is resource intensive – lack of public health services for birth defects, including congenital anomalies.
This is changing esp in urban areas – infections are on the decrease and management of intrapartum related complications, premature births, low birth weight babies, and infections are contributing to an increasing contribution of congenital anomalies to neonatal deaths
indiAIndian people are living in the midst of
risk factors for birth defects, e.g., universality of marriage, high fertility, large number of unplanned pregnancies, poor coverage of antenatal care, poor maternal nutritional status, high consanguineous marriages rate, and high carrier rate for hemoglobinopathies.
Birth defects can be defined as structural or functional abnormalities, including metabolic disorders, which are present from birth.
India - In 2010, congenital anomalies were estimated to be the fifth largest cause of neonatal deaths in India after preterm births (34.7%), intrapartum complications (19.6%), pneumonia (16.3%) and neonatal sepsis (15%) - contribute to 60 699 neonatal deaths in India in 2013, which accounted for the highest global burden of neonatal mortality due to congenital anomalies
Congenital heart defects (CHDs) were the most prevalent anomalies (65.86 per 10 000 births), with atrial septal defects (43.91 per 10 000 births) and ventricular septal defects (27.44 per 10 000 births) being the most commonly presenting heart defects. Two-thirds of the CHDs were detected post birth at mean age 4.5 ± 2 days.
Malformations of the musculoskeletal system (49.40 per 10 000 births) were primarily contributed by talipes equinovarus (32.93 per 10 000 births).
Urinary system anomalies (38.42 per 10 000 births) included congenital hydronephrosis (16.47 per 10 000 births) and polycystic kidney disease (10.98 per 10 000 births).
The most frequent nervous system anomalies were neural tube defects (NTDs, 27.44 per 10 000 births).
Anomalies of the digestive system, genital organs and respiratory system were less frequently encountered (21.95 per 10 000 births, 16.47 per 10 000 births and 10.98 per 10 000 births respectively).
Minor anomaly affected live births; of which the most frequently presenting anomalies were unilateral undescended testicle and single umbilical artery.
dr. Jeeson C. UnniEditor-in-chief, IAP Drug Formulary Asso. Sr. Consultant in Paediatrics
Aster Medcity, Kochi

11 November 2018
Health service implicationsAnomalies identified as typically requiring
surgery included severe CHDs, orofacial cleft, diaphragmatic hernia, duodenal atresia and tracheoesophageal fistula.
Pediatric surgery services for congenital anomalies have to be included as a component of newborn care.
Utilization of sonography services for the detection of fetal anomalies - one fifth of severely affected births were avoided through prenatal detection and subsequent pregnancy termination.
Although termination of pregnancy due to detection of a fetal anomaly is legally permissible in India, there are currently no government guidelines on the incorporation of sonography as a routine investigation in antenatal care.
Furthermore, a need for counseling prior to and after the ultrasound examination was observed, as women underwent this investigation with little preparation in case of detection of an anomaly. It was noted that upon detection of an anomaly, and when there was no option to terminate the pregnancy, women were left to carry the pregnancy to term, with no psychosocial support to help them address or prepare for the impending birth.
Need for guidelines for the use of sonography during pregnancy, including appropriate pre- and post-test counseling, accompanied by widespread dissemination of knowledge among women about the utility of sonography in the detection of congenital anomalies.
Need for a linkage between pediatric services and care for children with special needs. There are currently no rehabilitative services for children with disabilities, and as such there is no opportunity for referral of children with special needs for rehabilitative care
Psychosocial support service for parents was urgently required.
2. important lessons for birth defects surveillance in India 1. limitations of using hospital based registry data for estimation of
prevalence rates; 2. need to implement standard case definitions - congenital anomalies may be contributing to two key public health indicators - low birth weight and prematurity
Birth defect policyEstablish surveillance for birth defects.
surveillance data will permit the description of the epidemiology and public health impact of congenital anomalies, and anticipate the health care needs for birth defects in urban and rural India
Census of infants with special needs, in order to provide support for childhood disability and children with chronic medical needs
Thoroughly examine infants prior to discharge, and implementation of low cost measures such as pulse oximetry to ensure that most babies with CHD are detected at the earliest
Package of services for birth defects needs to be established. An integral part of the service package would be the provision of counseling and psychosocial support, in order to address the distress associated with an affected birth, and to limit out-of-pocket expenditure on multiple medical advices.
Rashtriya Bal swasthya Karyakram, the national early screening and diagnosis programme for children in India, has in place some services to address a few of these concerns
Prevention of congenital anomaliesLow education levels, widespread health
promotion messages emphasizing preconception care to prevent birth defects should be a key step in any birth defects prevention programme.
Upto 40% of NTDs can be prevented with preconception folic acid supplementation - the intervention would reduce about 30,000 affected births in India, considering complete compliance.
Population based strategies such as iodization, double fortification of salt, flour fortification with multivitamins, folic acid supplementation, periconceptional care, carrier screening and prenatal screening are some of proven strategies for control of birth defects.

12 Pediatric Companion
Off Label Medications in PediatricsDespite having pediatric specific formularies
and guidelines for drug use in pediatric therapeutics, off-label drug use remains an important public health issue for infants, children, and adolescents, because an overwhelming number of drugs still have no information in the labeling for use in pediatrics. It presents an even larger and more complex issue in preterm and full-term neonates, infants and in children younger than 2 years, and children with chronic and/or rare diseases. The purpose of off-label use is to benefit the individual patient. Practitioners use their professional judgment to determine these uses. As such, the term “off-label” does not imply an improper, illegal, contraindicated, or investigational use. Therapeutic decision-making must always rely on the best available evidence and the importance of the benefit for the individual patient.
The term “off-label” use refers to use of a drug that is not included in the package insert for that drug or a drug that is not mentioned for a particular, age, route of administration, duration or is not mentioned at all in the IAP Drug Formulary. It is acceptable to use drugs off label and to publish results related to off-label use, but it is not acceptable to receive remuneration from the sponsor for these uses.
The absence of labeling for a specific age group or for a specific disorder does not necessarily mean that the drug’s use is improper for that age or disorder. Rather, it only means that there is not enough evidence based studies to support its use for that specific age group or a specific disorder. In contrast to the absence of pediatric-specific information on some medications, other drug labels contain statements such as “the safety and efficacy in pediatric patients have not been established,” and explicit evidence-based warnings and contraindications are included on the label where indicated. Understanding the
distinction between the lack of approval for a particular use or dosing regimen in the former case versus explicit warnings or contraindications against use in the latter is essential for the pediatric practitioner.
In addition, when considering best practices for therapeutic decision-making, it is essential to understand that the various standard guidelines and IAP Drug Formulary does not regulate the use of drugs as they pertain to the practice of medicine.
therapeutic decision-MakingTherapeutic decision-making should always
be guided by the best available evidence and the importance of the benefit for the individual patient. Practitioners are in agreement regarding the importance of practicing evidence-based medicine. However, for the pediatric population, gold standard clinical trials are often not available, so practitioners must rely on either less definitive information, such as expert opinion for the age group that they are treating, or use evidence from a different population to guide practice. There are now many resources available to help assess the quality of evidence-based medicine, including but not restricted to articles in peer-reviewed journals.
At times, there may be little or no published information to guide therapy. This situation is especially true when treating rare diseases or sparse populations such as neonates. In such situations, the practicing physician can play an important role in adding to therapeutic information by publishing his or her experience with off-label uses of drugs. These reports can serve as the basis of more formal efficacy and
dr. Jeeson C. UnniEditor-in-chief, IAP Drug Formulary Asso. Sr. Consultant in Paediatrics
Aster Medcity, Kochi

13 November 2018
safety studies and can serve as a therapeutic decision-making resource for other physicians. The practicing physician also has a responsibility to report adverse events to the IAP CO or the IAP Drug Formulary.
Non-availability of suitable formulations of various pediatric medications in strengths required for this population also result in off label prescriptions being used in pediatrics.
In most situations, off-label use of medications is neither experimentation nor research. The administration of an approved drug for a use that is not approved is not considered research and does not warrant special consent or review if it is deemed to be in the individual patient’s best interest.
In general, if existing evidence supports the use of a drug for a specific indication in a particular patient, the usual informed-consent conversations should be conducted, including anticipated risks, benefits, and alternatives. If the off-label use is based on sound medical evidence, no additional informed consent beyond that routinely used in therapeutic decision-making is needed. However, if the off-label use is experimental, then the patient (or parent) should be informed of its experimental status. In addition, particular risk-benefit ratios presented by the unproven therapies must be carefully considered and disclosed, and standard of care practices should be reviewed. When use of a drug is truly investigational, drug use should be performed in conjunction with a well-designed clinical trial whenever possible. This is especially true when the physician proposes to treat a group of patients rather than a single individual. Patients and/or their legal guardians should be specifically informed that the proposed therapy is investigational, and their consent to proceed despite the risks of investigational therapy should be carefully documented. Whether institutional review, consultation, or written consent are required for a given intervention depends on
the degree of risk or departure from standard practices and the extent to which research, rather than individual patient care, is involved.
Pediatricians may be concerned that the off-label use of an approved drug may invite a variety of legal actions. To conform to accepted professional standards, the off-label use of a drug should be done in good faith, in the best interest of the patient, and without fraudulent intent. A practitioner may be accountable for the negligent use of any drug in a civil action, regardless of whether the IAP Drug Formulary has approved the use of that drug. Labeling is not intended to preclude the practitioner from using his or her best medical judgment in the interest of patients or to impose liability for off-label use. Indeed, the practice of medicine will more than likely require a practitioner to use drugs off label to provide the most appropriate treatment of a patient. However, because the use of drugs in an off-label capacity can increase the liability risk for a practitioner should an adverse event or poor outcome ensue, it is essential that practitioners document the decision-making process to use a drug off label in the patient’s medical record.
drug-related Problems in ChildrenThese include heterogeneous nature of
pediatric population, lack of standard dosage, inability to swallow solid dosage forms, off-label and unlicensed drug use, less acceptance of bitter oral formulations, stability and safety of excipients, needle phobias, calculation errors by prescribers, pharmacists or nurses, poor adherence, lack of available dosage forms and concentrations which necessitate additional calculations and manipulations of commercially available dosage forms or preparation of extemporaneous formulations, lack of familiarity between adult and pediatric guidelines, confusion between adult and pediatric preparations, limited published information, administration errors and use of inappropriate measuring devices.

14 Pediatric Companion
Rheumatic Pneumonia : A forgotten complication of Rheumatic Fever
introductionRheumatic Fever (RF) and Rheumatic
Heart Disease (RHD) remain significant causes of cardiovascular diseases in the world today. Even though there is a decrease in the incidence of acute RF and RHD in developed countries during the past five decades, they remain as major public health problems in developing countries. Rheumatic fever in this century appears to be largely a disease of crowding and poverty.
ARF has extremely variable manifestations and remains a clinical syndrome for which no specific diagnostic test exists. Rheumatic pneumonia (RP) is a well-described, poorly understood, rare manifestation of rheumatic fever that is generally fatal. RP has been reported for more than a century and it has been traditionally associated with a high mortality rate (1). We are presenting a case of RP, to increase awareness of such a forgotten entity, in order to determine optimal management.
Case reportAn 8 year old boy presented to emergency
department with severe respiratory distress. On taking a detailed history, his complaints started about 8 days back with fever. Fever was of high grade intermittent type and was not associated with rashes, vomiting, loose stools, seizure or pain during micturition. For initial 2 days of fever he had sore throat which relieved on its own. Child developed cough 5 days back which was productive in nature, and was progressive. For the last 2 days he was having chest pain and breathlessness. It was a central chest pain associated with breathlessness even at rest. Child preferred sitting up than lying down even at night.
On repeated questioning, mother gives a past history of fever with sore throat 6 weeks back and
later, joint pain. Joint pain was noted first in the knee and later spread to ankle after knee pain got relieved. It was typically migratory type and disappeared with treatment from primary health centre. No history of tuberculosis or contact with tuberculosis. Fully immunized. His growth and development were normal.
At admission, child was conscious, sick looking with severe respiratory distress having tachypnoea and retractions. Pallor present, no cyanosis/clubbing/ edema. PR-130/min, regular, high volume collapsing type, all peripheral pulses well palpable. BP-98/30 in right upper limb, 150/40 in right lower limb. RR-52/min, temp-100.5degree F, spO2-96% in room air. Dancing carotids, Quincke’s sign and Traube’s sign were present. On cardiovascular examination : JVP raised to 4cm, precordium was hyperdynamic. Apex in left 6th Intercostal space in the anterior axillary line. Grade I LPsH was present. s1 masked, s2 loud, s3 present. A high pitched pan-systolic murmur Grade IV/VI intensity best heard in LLsB, and a low pitched early diastolic murmur Grade III intensity heard in 3rd left sternal border. Respiratory system was normal with bilateral vesicular breath sound. GIT: 4 cm soft tender liver with no spleen/ascites. Nervous system exam-normal.
On investigation: Hb – 7.9gm%, TC-10100cells/mm, EsR-120mm/1sthr, RFT, LFT, s.electrolytes-normal. CRP-positive, AsO-negative. Peripheral smear showed normocytic normochromic anaemia. X-ray chest: lung fields showed air bronchogram and significant
dr. t.M. AnandaKesavan dr. Aijo Joy
Dept of Pediatrics Govt. Medical College, Thrissur

15 November 2018
cardiomegaly. ECG: sinus rhythm, HR-130/min, right axis deviation(+100degree). Echo-mild LV dysfunction, LV dilated, moderate MR, severe AR, mild TR with mild PAH.No pericardial effusion. Child was advised complete bed rest, propped up position with oxygen. With a possibility of rheumatic fever activation, he was put on Tab. Prednisolone, Inj. CP, Inj. Frusemide and blood transfusion.
While admitted in the hospital, child was persistently having severe tachypnea with respiratory distress and he always preferred a sitting up and leaning forward position. Because of increased apprehension and restlessness he was given Inj Morphine. Later Milrinone infusion was added on day 2 of admission suspecting intractable cardiac failure (even though there was no oedema or basal crepitation). On next 2days, there was a little improvement in his breathlessness.
On day 5, child became more dyspnoeic with a RR of 78/min. On auscultation air entry was reduced on right lower lung zones and tubular bronchial breathing on right interscapular and infrascapular area. All other lung areas are with good air entry with no creptations. Xray chest was taken and it showed right sided consolidation (fig 1). With this new finding we added Inj Vancomycin also. On day 6 of admission child collapsed and succumbed to death. since parents were not willing, we could not perform his postmortem.
In view of his past history and present admission with clinical features like extreme breathlessness, local chest findings and absence of pedal oedema and basal crepitations, we made a diagnosis rheumatic pneumonia.
discussionRP is a rare clinical entity first described as
long ago as 1845, by Latham. He described it as “but the heart is not the only vital organ liable to suffer inflammation in acute rheumatism. The
lungs may suffer also. And the diseases which result are bronchitis, pneumonia, pleurisy.” (1) In 136 cases of acute rheumatism, he observed pneumonia in 18 and noted a graver outcome in those cases. He further made the observation that pneumonia was much more common in patients with carditis than in those with the articular manifestation alone. RP was described as an entity by such prominent clinicians as Walshe(2), Cheadle(3) and Garrod(4) in the second half of the nineteenth century.
Rheumatic pneumonitis occurs in the course of acute severe rheumatic fever, usually associated with active carditis, and aggravates the clinical picture. severe dyspnea and tachypnea, toxicity and a worsening course are the hallmarks of this process. Massive consolidation of the lung without rales is the rule; roentgenologically, the picture often resembles pulmonary edema so that clinical differentiation may be almost impossible. The diagnosis is suggested through observation in a patient with active rheumatic carditis of an unremitting, diffuse pulmonary consolidation, marked tachypnea, and unresponsiveness to steroid and antibiotic therapy usually terminating in death
Cheadle described six instances of pneumonia during an outbreak of ARF involving 26 cases and described hyperpnea and fever as its manifestations(3). 1926, Rabinowitz’(5) reported a specific rheumatic pneumonia even though he failed to find Aschoff bodies in histologic sections. He observed that the pulmonary lesions could not be explained on the basis of heart failure or compression of the lung by serous effusions because these factors were not present in all his cases of rheumatic pneumonia. Many studies indicate a greater acceptance of rheumatic pneumonitis as a specific manifestation and not simply an intercurrent complication of severe rheumatic fever(6-8).
In our case at no time were there signs of congestive heart failure or venous congestion. In

16 Pediatric Companion
this case of ARF with carditis a severe, fulminant pneumonia of extensive proportions caused death at a time when cardiac failure was not apparent. Intense dyspnea and striking tachypnea were the outstanding features. Treatment directed at amelioration of cardiac failure and ARF were ineffective.
Even though necropsy confirmation is lacking in this case, rheumatic pneumonitis appears as a possibility. RP possesses no pathognomonic clinical features, this diagnosis and its differentiation from bacterial and viral processes remain speculative. This unusual complications, such as RP, are a challenging diagnosis for clinicians without experience of this illness(9).
so the association of pulmonary consolidation, tachypnea, the resistance to steroid therapy and the fatal outcome in a patient with known active rheumatic carditis. support of our diagnosis of RP.
rEFErEnCEs1. Latham, P. M.: Lectures on subjects Connectedwith
Clinical Medicine Comprising Disease ofthe Heart. London, Longman, Brown, Greenand Longman, 1845, Vol. 1, Lecture 9, p. 159.
2. Valshe, W. H.: Practical Treatise on the Diseasesof the Lungs. London, James Walton,1871, p. 375.
3. Cheadle, W. B.: On an outbreak of rheumaticpneumo-nia. Lancet 1: 861, 1888.
4. Garrod, A. E.: A Treatise on Rheumatism. London,C. Griffin & Co., 1890, p. 107.
5. Rabinowitz, M. A.: Rheumatic pneumonia. J.A.M.A. 87: 142, 1926Path. 21: 741, 1945.
6. scott, R. F., Thomas, W. A.; Kissane,J. M.: Rheumatic pneumonitis: Pathologic features.J. Pediat. 54: 60, 1959.
7. Lees, A. W.: Acute polyarthritis with pulmonarycon-solidation and pleural effusion. Brit. M. J.1: 246, 1962.
8. spencer, H.: Pathology of the Lung. Oxford.Pergamon Press, 1962, Chapter 18, p. 566.
9. Burgert sJ, Classen DC, Burke JP, Veasy LG. Rheumatic pneumonia: reappearance of a previously recognized complication of acute rheumatic fever. Clin Infect Dis 1995;21:1020–2
Fig 1 : Xray showing pneumonia on right side

17 November 2018
dr. Gireesh s.Associate Professor
Dept. of PediatricsGovt. Medical College, Kozhikode
J O u R N A L S N I P P E T S1. What is the longterm neuro
developmental outcome of caffeine therapy on ELBW infants?
Mürner-Lavanchy IM et al. Caffeine for Apnea of Prematurity (CAP) Trial Group. Pediatrics. 2018;141(5) Epub 2018 Apr 11.
What they did: Thirteen academic hospitals in Canada, Australia, Great Britain, and sweden participated in this part of the 11-year follow-up of the double-blind, randomized, placebo-controlled trial. Measures of general intelligence, attention, executive function, visuomotor integration and perception, and behaviour were obtained in up to 870 children. The effects of caffeine therapy were assessed by using regression models.
What they found: Neurobehavioral outcomes were generally similar for both the caffeine and placebo group. The caffeine group performed better than the placebo group in fine motor coordination (mean difference [MD]= 2.9; 95% confidence interval [CI]: 0.7 to 5.1; P = .01), visuomotor integration (MD = 1.8; 95% CI: 0.0 to 3.7; P<.05), visual perception (MD = 2.0; 95% CI: 0.3 to 3.8; P = .02), and visuospatial organization (MD = 1.2; 95% CI: 0.4 to 2.0; P = .003).
Conclusions: Neonatal caffeine therapy for apnea of prematurity improved visuomotor, visuoperceptual, and visuospatial abilities at age 11 years. General intelligence, attention, and behaviour were not adversely affected by caffeine, which highlights the long-term safety of caffeine therapy for apnea of prematurity in very low birth weight neonates.
2. Is there any role for oral administration of honey or sucralfate after button battery(BB) ingestion in children?
Anfang RR, Jatana KR, Linn RL, Rhoades K, Fry J, Jacobs IN Laryngoscope. 2018
What they did: Apple juice, orange juice, pure honey, pure maple syrup, and sucralfate were screened using a 3 V lithium (3 V-CR2032) BB on cadaveric porcine esophagus. The most promising in vitro options were tested against a saline control in live American Yorkshire piglets with anode-facing placement of the BB on the posterior wall of the proximal esophagus for 60 minutes. BB voltage and tissue pH were measured before battery placement and after removal. The 10 mL irrigations occurred every 10 minutes from t = 5 minutes. Gross and histologic assessment was performed on the esophagus of piglets euthanized7 ± 0.5 days following BB exposure.
What they found: Honey and sucralfate demonstrated to a significant degree the most protective effects in vitro and in vivo. Both neutralized the tissue pH increase and created more localized and superficial injuries; observed in vivo was a decrease in both full-thickness injury (i.e., shallower depths of necrotic and granulation tissue) and outward extension of injury in the deep muscle beyond surface ulcer margins (P < .05).
Conclusions: In the crucial period between BB ingestion and endoscopic removal, early and frequent ingestion of honey in the household setting and sucralfate in the clinical setting has the potential to reduce injury severity and improve patient outcomes.

18 Pediatric Companion
Obesity : Some Thoughts1. The prevalence of adolescent obesity in
the UsA has increased from 4.6% to 19.6% within 45 years, 1963 to 2008. As genetic changes only occur over thousands of years, this increase has to be due to environmental factors. They are the plentiful availability of low-cost energy-dense junk food and a sedentary lifestyle caused by TV, the internet and the mobile phone.
2. ‘Matter can neither be created nor destroyed.’ A person can gain 1 kg weight only if he consumes 7300 calories more than his body uses up. He should not compare his intake to that of another: the obese tend to walk more slowly, are less likely to use the stairs, and more likely to use a car or bike for short distances.
3. Obese people (unconsciously) underestimate their food intake. They may eat from larger and deeper plates that hold twice as much rice as standard plates. (Eating from a smaller plate is an effective aid in weight reduction).
4. “Obesity runs in our family genes.” But even the slim spouse has gained weight, indicating that the home meals are rich in oil and sugar.
5. An obese individual frequently asserted that his breakfast consisted of a cup of tea, a plate of rice for lunch and 1-2 chapattis for dinner. This was true. However he neglected to mention that every morning he had a packet of chips along with tea while reading the newspaper, snacked heavily while watching sports on TV every night, and routinely had dessert after lunch and dinner.
6. “I eat very little rice, I drink tea ‘without’ and I avoid oily food.” Wheat is as fattening as rice. 1 spoon of sugar has only 20 calories. It is the total caloric intake, not the quality, that determines weight.
7. “I drink plenty of water, that is why I’m so fat.” Water is zero-calorie. Obese persons develop larger stomachs, and tend to drink larger quantities of water.
8. “I don’t have breakfast”. Routinely skipping a meal consistently results in weight gain: the
body rebels, and the person unconsciously consumes more at lunch and dinner, and snacks too.
9. “A eats less than B, yet weighs 10 kg more than him.” Obesity is a bank account. Two men of the same age and height lead identical lives, yet 5 years later A weighs more -- because A initially weighed 15 kg more.
10. An extra 100 calories per day = 36500 cals/yr = 5 kg weight gain annually. One vada, idli or puri provides 70-80 calories, a veg puff 166 calories, and 100 ml of payasam adds 312 calories.
11. The good news is that a modest reduction in calories will result in significant weight loss over a year without causing hunger, and without the rebound weight gain that occurs in aggressive diets. Aim for 20% caloric reduction at every meal: avoid snacks, avoid dessert, and maximize vegetable and fruit intake (except plantains).
12. The beer belly is for real: 340 ml of beer or 45 ml of whiskey equals 70-100 calories. Alcohol has no proteins, vitamins or minerals, and actually reduces serum levels of Vitamin A and some B vitamins.
13. “I walk for 30 minutes daily.” This uses up 100-150 calories. Exercise increases HDL-cholesterol, builds muscles, and reduces atherotic plaque, but weight reduction is modest.
14. Mothers gain weight due to weaning. They optimistically take too much in the plate, and use their stomachs as waste bins for the leftover food.
15. Adolescents are always hungry. Let them eat plenty, as they need to grow upwards; restrict them only when they start growing forwards.
dr newton luiz
Dhanya Mission Hospital
Potta, Trichur

19 November 2018 19 november 2018
M o m e n t s o f G l o r y
Pediatric Cardiology conference@Cochin Neuropedicon inauguration@Kannur
IAP Team with Health Minister for containment of Nipah Out break
PEDCRITICON inaugurated by Dr Santhosh Soans, National President
NEPHROCON inauguration by Dr P. A. Muhammed Kunju, President IAP Kerala
on 9th Sept. 2018.
Dr P. A. Muhammed Kunju, IAP State President felicitated by Kasaragod IAP
Central IAP Action Plan STRIDE Workshop conducted at Kochi on 16th Sept. 2018
Special General Body Meeting of Central IAP @ IMA House, Kochi

20 Pediatric Companion20 Pediatric Companion
R E F R E S H u R R A D I O L O G Y dr.t.M. Ananda KesavanDept of Pediatrics
Govt. Medical College, Thrissur
Fig 1 : Xray taken for fever and cough of 3 days duration
Fig 3 : Newborn with vomiting and abdominal distention. Dysmorphic facies and simian crease
Fig 5 : Bow leg and protruded abdomen (complete diagnosis)
Fig 6 : 14 days old baby crying while mother tried to hold the baby
Fig 4 : Acute onset of cough
Fig 2 : X ray of sibling (otherwise asymptomatic)
(Answers on Page 24

21 November 2018
(Answers on Page 24
21 november 2018
P E D I A T R I C P H O T O q u I z dr. sankar v.H. Addl. Professor, Geneticist
SAT, Trivandrum
QUiz - 1
n Characteristic features and identify the syndrome.
QUiz - 3n Identify the
dysmorhic features.
n What is the diagnosis.
QUiz - 5n Identify the
characteristic abnormality
n Identify the syndrome
QUiz - 7
n Identify the hand abnormality.n Mention two conditions where this finding will be
characteristic feature.
QUiz - 9
n 3 month old child admitted with features of CCF.
n Identify the abnormality.
QUiz - 10
n Identify the abnormality.n Mention two conditions where this
finding will be characteristic.
QUiz - 6n Identify the characteristic
hand abnormality.
QUiz - 8n Identify the vertebral
abnormality.n Name a condition.
QUiz - 4n Identify the
abnormality.
n Most probable diagnosis.
n What is the cranial abnormality.
QUiz - 2n Identify the
charecterstic facial features.
n Most probable syndrome.

22 Pediatric Companion22 Pediatric Companion
Felicitation of Pediatricians at Kannur
New Born Week Inauguration - Prof K.C. Rajagopal at Kozhikode
Autism day celebration at District Autism Center, Alappuzha
IAP State Football Match Winners, Calicut Dare Devils
MKC Nair Oration by Dr Shaji Thomas John during
Adolescon at IMCH, Kozhikode
Breastfeeding Week Celebrations @ Thrissur
Medicolegal CME at Kozhikode
Children’s Day Celebration at IMCH Kozhikode
S n a p s f r o m B r a n c h e s
Dr Sebastian Lukos (IAP Kottayam) at St.Thomas HSS Pala on World Diabetes Day
National Nutrition Week - at Govt. Medical College, Kalamassery
GROWTH CME on Oct. 28th - inagurated by Dr P A M Kunju
Dr S Omana, HOD Pediatrics inagurating the Children’s day celebrations at ICH Kottayam
IAP Malapuram : Children’s Day Celebrations
CME on Neurodevelopmental Disorders at Aster Medcity, Kochi

23 November 2018
Wilson’s Disease - The Master MasqueradorThere are two distinct disorders of copper
transport: Menkes kinky hair disease, an X-linked defect of copper transport at the intestinal level and Wilson’s disease (WD), an autosomal recessive disorder of copper overload at the hepatic level.
WD is a rare disease characterized by toxic accumulation of copper in liver, brain, cornea, skeletal system and other tissues. It is an important cause of chronic liver disease and fulminant hepatitis in children. It is an unpardonable mistake on the part of any doctor, especially a pediatrician , to miss the diagnosis of WD as it is very well treatable and almost curabl, if diagnosed and treated on time.
synonyMs• Hepatolenticular degeneration• Westphal pseudosclerosis• Westphal Strumpell disease• Wilson-Konovalov disease
GEnEtiCsThe real prevalence of WD is still debated. The
widely cited prevalence figure of 1:30,00 is actually prior to the discovery of the Gene of WD, ATP7B, and hence may not be very accurate now. Mass screening for WD in East Asian populations, based on ceruloplasmin, has suggested a significantly higher frequency, ranging from 1:500 to 1:3000.
Although Wilson correctly recorded the familial nature of the disease, it was Hall who demonstrated its inheritance in the year 1921, later shown to be autosomal recessive.
The abnormal gene for WD is on the long arm of chromosome 13, hence WD may be referred to as the ‘unlucky disease’. Using multipoint linkage techniques, the abnormal gene was localized more specifically to chromosome 13 at q14-q21. With subsequent linkage and fluorescent in situ hybridization studies, the disease locus was refined to a genomic region flanked proximally by the DNA marker, D13 s31, and distally by D13 s59.
In 1993, the gene responsible for Menkes disease (MNK) was identified and found to be similar to the WD gene. The WD gene, ATP7B, and the MNK gene, ATP7A, encode copper transporting P-type ATPase
The Menkes protein is expressed in all tissues except the liver; the WD product is expressed mainly in the liver and also in kidney, brain and placenta. The WD gene is arranged in 21 exons and spans over 80 kb of genomic sequence. WD results mainly from missense mutations or small deletions.
The ATP7B gene encodes a transmembrane copper-transporting ATPase, expressed on the hepatocyte canalicular membrane. More than 520
mutations in ATP7B gene have been reported in the Human Genome Mutation Database , but not all mutations cause the disease. The overwhelming majority of patients are compound heterozygotes containing different mutations on each ATP7B allele.
table 1. Genes and Wd
Gene Chromosome numberWilson’s diseaseCeruloplasmin
Metallothionein
13q3q16
PAtHoGEnEsisCopper is an essential dietary nutrient which
is present in most of dietary products. It is an important co-factor for many proteins. It facilitates electron transfer reactions and is essential for mitochondrial respiration, melanin biosynthesis, dopamine metabolism, iron homeostasis, antioxidant defense, connective tissue formation, and peptide amidation. However, it can be potentially toxic to the cells as it leads to the formation of hydroxyl radicals, which are the most potent of all free radicals, by the Fenton reaction.
It is very difficult to make a biochemical diagnosis of WD in neonatal period as serum ceruloplasmin is very low, and also in the first 3-4 months of life, as the serum ceruloplasmin level and liver copper are normally elevated during this time. There may be a control gene responsible for fetal copper metabolism. From birth onwards, 10-20 mg of copper accumulates every year. It usually takes 6-15 years before a child becomes symptomatic due to copper accumulation. In siblings, there may be considerable differences regarding clinical and laboratory findings. Hence, there may be exogenous or endogenous factors which modify the genetically determined process or alter the gene expression within the families involved.
Copper MetabolismThe average intake of copper in breast-fed babies
is 50 μg/kg/day and in older children and adults is 1 mg/day. Of this, 50% is unabsorbed and passed in the stools and 30% is lost through the skin. Copper absorption occurs in the small intestine, primarily the duodenum, by ATP7A. It is interesting that copper is
dr. A. riyaz Pediatric Gastroenterologist
Professor & Head of PediatricsKannur Medical College

24 Pediatric Companion
one of the few nutrients that can be absorbed from the stomach also, though to s smaller extent. The remaining 20% is absorbed into enterocytes by metallothionein, which is a 10 kDa cytosolic, cysteine-rich protein. Copper is then exported from the enterocyte to the portal blood by the Menkes protein. Absence of this protein causes accumulation of copper within the enterocytes, failure of absorption and systemic copper deficiency. As there is no enterohepatic circulation for copper, copper excreted into bile is not reabsorbed.
In the portal blood, copper is carried loosely bound to:• Albumin• Amino acids, especially histidine• Transcuprein, an unidentified high molecular
weight globulinCopper is rapidly taken up by the hepatocytes
and used as a co-factor for copper-dependent intracellular enzymes like cytochrome oxidase and superoxide dismutase.
Copper absorption is inhibited by zinc which is the rationale for zinc therapy in WD.
liver CopperThe hepatocyte protects itself against copper
toxicity by the following mechanisms:• Controlling the uptake of copper• Chaperoning copper to its various intracellular
destinations• Binding free cytoplasmic copper (by glutathione
and metallothionein)• Actively transporting copper out of liver (by
Wilson’s disease protein).Copper is transported to the hepatocyte at the
basolateral membrane, from the portal blood. The
newly arriving copper is transported to various intracellular locations by three specific copper-chaperone proteins.
Any unbound cytoplasmic copper is bound to glutathione or metallothionein, and excess copper is sequestered in lysosomes.
In a child with WD, hepatic damage begins as this storage capacity is exceeded, by about 3 years of age.
Hah 1, along with ATP7B gene product (WDP), transports six copper molecules to the Golgi body, where it binds to apoceruloplasmin, (the ceruloplasmin without copper) to form ceruloplasmin (copper containing ceruloplasmin is also called holoceruloplasmin). This is then transported out of the hepatocytes to reach various tissues for their metabolic activities. Part of copper is bound to lysosomes and excreted into bile.
In WD, copper cannot enter Golgi body due to the absence of WDP, and hence it cannot bind to apoceruloplasmin. Copper in its unbound form cannot be utilized by the tissues or be excreted in the bile. Hence, copper accumulates initially in the cytosol bound to metallothionein and subsequently in the lysosomes. Increased liver copper content along with hepatocellular damage leads to the release of copper into the blood stream, where it binds to albumin or small peptides. This leads to an increase in free serum copper concentrations (non-ceruloplasmin bound copper). However, total serum copper may not be elevated because of the reduced concentration of ceruloplasmin.
About 95% of serum copper is bound to ceruloplasmin. The serum ceruloplasmin level is usually low in WD, not because copper levels affect the synthesis of apoceruloplasmin (ceruloplasmin without copper) but because the half-life of apoceruloplasmin
.1) Synophriz, cornelia délange syndrome2) Mandibulo facial dysostosis, lateral eyelid
coloboma, Trecher Collins syndrome3) Cleating, hypertelorism, amniotic band
syndrome 4) Syndactyly-mitten hand, Apert syndrome,
craniosynostosis5) Polydactyly, nail hypoplasia, multiple
frenulum, ellis van creveld syndrome6) Split hand malformation, ectrodactyly7) Short 4&5 metacarpals, Turner syndrome,
pseudohypoparathyroidism8) Hemivertebrae, spondylothoracic dysplasia,9) Vein of Galen malformation10) Intracranialcalcifications,congenital
toxoplasmosis, Aicardi Goutier syndrome
PHoto QUiz - AnsWErs (PAGE 21).Fig 1 : Eventration of diaphragm. It was
asymptomatic in this child (Accidental finding)
Fig 2 : Absence of clavicle(Cleidocranial dysostosis)
Fig 3 : Annular pancrease in Down syndrome baby(“Double bubble” sign)
Fig 4 : Right Lower lobe Collapse(Foreign body aspiration)
Fig 5 : Rickets (with greenstick fracture)
Fig 6 : Fracture right clavicle (with callus formation)
rEFrEsH Ur rAdioloGy (PAGE 20) AnsWErs
25 November 2018
decreases from 4-5 days to 4-5 hours in the absence of copper.
PAtHoPHysioloGy of WdThe toxicity of copper is due to:
• Its binding to SH group of cysteine, which is converted into an irreversible form by oxidation
• Formation of free radicals like hydroxyl radicals by the Fenton reaction, resulting in lipid peroxidation which in turn is responsible for functional and structural disturbances of bio membranes.
• A reduction in vitamin E levels, aggravating lipid peroxidation.
PAtHoloGyThe earl iest changes include glycogen
deposition in the nuclei of periportal hepatocytes and microvesicular fatty infiltration. Early in the course of WD, hepatocellular copper is bound mainly to metallothionein and is distributed diffusely in the cytoplasm of hepatocytes. Therefore, histochemical stains for copper are negative.
As the disease progresses, the copper content exceeds the storage capacity of metallothionein and copper is deposited in lysosomes. Lysosomal aggregates of copper can be detected by special staining techniques for copper or copper-binding protein such as rubeanic acid or orcein, respectively. In the cirrhotic liver, some areas may have no stainable copper at all. If the clinical presentation mimics autoimmune hepatitis, a liver biopsy specimen may reveal classic histologic features such as interface hepatitis, severe inflammation or Mallory (Mallory-Denk) bodies.
If untreated, this evolves into macronodular cirrhosis or progresses rapidly into fulminant hepatitis. Interestingly, the risk of hepatocellular carcinoma (HCC) is extremely low, unlike hemochromatosis, as copper may be protective in man against development of HCC.
The initial changes are:• Microvesicular fatty infiltration of hepatocytes• Glycogen-containing vacuoles in the nuclei• Kupffer cell hypertrophy.Later Changes:• Hepatocellular necrosis• Large hepatocytes with multiple nuclei• Mallory Denk hyaline bodies• Fibrosis• Interface hepatitis • Macronodular cirrhosis.
deiss’s staging of WdThis is a valuable staging system that explains
many of the confusing findings in WD.
stage iThis begins at birth and there is a progressive
accumulation of copper in the cytosol of the hepatocytes. The process continues until all hepatic binding sites for copper are saturated. The patient is asymptomatic at this stage and it is seen before 5 years of age.
stage iiIn this stage, liver is saturated with copper and
is redistributed from the cytosol of hepatocytes to the lysosomes and copper is released from the liver into serum. If this release occurs gradually, the patient is asymptomatic but if rapid, hepatocellular necrosis develops and the patient develops hepatic or neurologic manifestations. In addition, rapid release of copper into the blood may result in hemolytic anemia.
stage iiiCopper continues to be stored in the lysosomes,
and varying degrees of fibrosis or cirrhosis may occur. At this stage, accumulation of copper also occurs in brain, cornea, kidney or skeleton. Patients may remain asymptomatic for years if the deposition of copper in liver and brain develops slowly.
stage ivHere, copper accumulation occurs rapidly and
hepatic and neurologic symptoms become apparent in a short time.
stage vThis occurs when treatment is begun and patient
recovers; or the patient dies from hepatic failure or irreversible brain damage.
CliniCAl FEAtUrEsAge of onsetAlthough the failure to excrete biliary copper
is present from birth, symptoms of WD generally do not develop until about three years of age, and rarely become evident before age of five. However, if mutations have completely knocked out gene function, the child may become symptomatic even by 2-3 years when pediatricians usually do not consider the possibility of WD. At the same time, if mutations are milder, the patient may present for the first time with hepatic manifestations or neurologic or psychiatric symptoms even as late as 70 years of age.
The age of onset of WD is earlier in Indian children compared to Western children. This may be because the average intake of copper in India ranges from 5-7 mg/day which is higher compared to Western countries (0.34-1.1 mg/day) . The practice of cooking food in copper/copper alloy pots may be contributory.
Unfortunately, symptoms at any age are frequently non-specific. Children with WD present with liver disease, whereas neuropsychiatric symptoms are more common after the age of 18 years
Hepatic manifestationsThe hepatic manifestations of WD may be of
almost any variety:

26 Pediatric Companion
• Acute hepatitis• Fulminant hepatic failure• Chronic hepatitis• Asymptomatic hepatomegaly• Serendipitous finding of abnormal LFT• Variceal hemorrhage from unsuspected portal
hypertension• Signs of decompensated chronic liver disease.
Acute HepatitisMany patients present with acute hepatitis that
is commonly misdiagnosed as viral hepatitis. Here, the patient appears to recover initially but later develops progressive liver disease or neurological manifestations.
Fulminant HepatitisWD is responsible for 5% of FHF worldwide.
This is characterized by progressive jaundice, ascites and hepatic and renal failure usually in a child or young person. Hepatocellular necrosis occurs due to accumulation of copper. Virtually all patients will already be cirrhotic. Acute intravascular hemolysis may be due to the destruction of erythrocytes by a sudden flux of copper from the necrotic hepatocytes. KF ring may be absent.
Urinary and serum copper levels will be very high. serum ceruloplasmin is usually low. However, it may be normal or even raised as it is an acute phase reactant. serum transaminases and sAP are inappropriately low for fulminant viral hepatitis. A low sAP to bilirubin ratio, although not diagnostic, is suggestive of fulminant WD.
It may be extremely difficult to distinguish fulminant WD from other causes of fulminant hepatitis. Any child or adolescent with fulminant hepatitis should be considered to have WD until proven otherwise. The presence of hemolysis is a point in favour of WD.
Diagnosis of Fulminant Wilsonian HepatitisThe following clues may help to suspect fulminant
WD:• History of consanguinity.• Absence of other known causes of fulminant
hepatitis like hepatitis B/A, drugs etc.• History of death of siblings/ close family members
due to undiagnosed liver disease.• History of neuropsychiatric illness in the family.• Disproportionate increase in serum bilirubin
(>15mg/dL) and relatively low transaminases.• AST: ALT more than 4• Very low serum alkaline phosphatase• Berman’s ratio: S. alkaline phosphatase(IU/L) to
bilirubin (mg/dl) ratio of less than 2. However, this ratio may not be useful in children as the
alkaline phosphatase levels are usually high in growing children.
• Evidence of hemolysis in the peripheral smear.• Low ceruloplasmin levels and/or high
transaminase levels in siblings/parents• Siblings or parents with high urine copper and
serum free copper Chronic liver disease
10–30% of patients present with features of chronic hepatitis and cirrhosis characterized by polyarthralgia, edema, ascites, clubbing, gynecomastia, spider angiomas, splenomegaly, ascites and portal hypertension. The disease can exist without any neurologic manifestations. In some, the cirrhosis is well compensated. Liver biopsy with measurement of hepatic copper may be necessary for diagnosis.
All young patients with chronic liver disease showing slurring of speech, hemolysis, and early ascites and with a family history of cirrhosis should be screened for WD. WD may also present as acute liver failure with an associated Coombs-negative hemolytic anemia and acute renal failure. some patients have transient episodes of jaundice due to hemolysis. Low grade hemolysis may be associated with WD when liver disease is not clinically evident.
Fatty liverFatty liver is commonly seen in WD, and the
patients can be misdiagnosed as having non-alcoholic steatohepatitis (NAsH). Hence, WD should be ruled out in all patients with a diagnosis of NAsH.
neuropsychiatric ManifestationsNeuropsychiatric manifestations are typically
seen in late teens or early twenties though it may rarely be seen in children as young as 6 years also. Subtle findings may appear in children much earlier in life, including changes in behavior, deterioration in schoolwork or inability to perform activities requiring good hand-eye coordination. Handwriting may deteriorate, and cramped small handwriting as in Parkinson’s disease (micrographia) may develop.
Other common findings include tremor, lack of motor coordination, drooling, dysarthria, dystonia and spasticity. The characteristic tremor in WD which is coarse and irregular is called “ wing beating tremor”. severe pseudobulbar palsy may result in transfer dysphagia which may pose a risk of aspiration pneumonia. Dysautonomia may be present. Migraine headaches and insomnia have been reported; however, seizures are infrequent. A soft whispery voice (hypophonia) is another early feature of neurological involvement.
Along with behavioral changes, other psychiatric manifestations include depression, anxiety and even frank psychosis. Many children with neurological or psychiatric manifestations may have cirrhosis also but many of them do not have evidence of liver disease.

27 November 2018
nEUroloGiCAl & PsyCHiAtriC MAniFEstAtions oF Wd
Box 1 neurological & Psychiatric
mani festations of Wd
neurological manifestations• Movement disorders ( wing-beating tremor,
involuntary movements) Micrographia• Drooling, dysarthriaHypophonia• Rigid dystonia• Pseudobulbar palsy• Dysautonomia• Migraine • Insomnia• SeizuresPsychiatric manifestations• Depression• Neurotic behaviour• Personality changes• Psychosis
The sensory system is virtually spared and intelligence is not affected. Most of the patients with neuropsychiatric manifestations have asymptomatic hepatosplenomegaly and/or biochemical evidence of liver disease and histological changes on liver biopsy.
ophthalmologic ManifestationsKayser-Fleischer ring (KFr)
Copper is actually distributed throughout the cornea but fluid streaming favors accumulation near the limbus. KF rings, seen in the Descemet’s layer of cornea, first appear in the superior aspect of the cornea ((10 to 2 O’clock position), followed by the inferior aspect (5 to 7 O’clock position); the medial and lateral portions of the ring then subsequently fill in to complete the ring. Because of this pattern of ring evolution, it is important to lift the eyelid during the examination so that incomplete ring formation is not overlooked. It is seen in virtually 100% of patients with neurological manifestations. However, it is seen in only about 50% of patients with hepatic disease and 10% of asymptomatic patients with WD.
It is about 1–3 mm in width, greenish yellow or brown in colour and located at the periphery of cornea. It is visible on direct inspection only when iris pigmentation is light and copper deposition is heavy.
It consists of electron dense granules containing copper-sulphur complexes. Although excess copper is distributed throughout the cornea, copper-sulphur complexes are seen only in the Descemet’s membrane. In the early stages it can be seen only by slit-lamp examination. Later, it can be seen by naked eye examination also. A complete KF ring indicates long-
standing disease and severe copper overload. KF rings range in color from golden to brown or
green, but more unusual colors– ruby red, bright green, ultramarine blue – have also been described. Because of its color, it can be easily identified in patients with blue eyes, but it may be very difficult or even impossible to visualize in brown-eyed persons without slit-lamp examination. In other words, it is easy to detect in Caucasians and difficult in our patients. The rings begin to form in the periphery of the cornea and then spread centrally toward the pupil. However, in some patients there may be a clear area between the ring and the limbus.
It should be stressed that KF ring is not pathognomonic of WD, as it can be seen in any condition causing chronic cholestasis including biliary atresia. However, in such cases, the rings are incomplete and can be seen only by slit lamp examination
KF-like rings may be seen in some non-hepatic conditions also. Prolonged use of estrogen-based oral contraceptive pills in adolescent girls may elevate serum copper levels and this may result in copper deposition and ring formation in Descemet’s membrane. However, this is seen within the mid-periphery rather than the outer edges of the cornea.
Rarely, similar rings may be seen in diseases associated with very high gammaglobulin levels like chronic lymphocytic leukemia in which copper deposition is central, rather than in the periphery of cornea. The central corneal copper deposition in such patients may affect vision, unlike in WD. Fleischer’s ring, seen in keratoconus due to hemosiderin deposition in basal epithelial cells, appears as a greenish or brownish ring in the peripheral cornea that may be mistaken for KF rings.
In rare persons with incidental detection of KF rings, WD should be excluded.
Sunflower (sunburst) CataractThis results from anterior capsular deposition
of copper and has a sunflower or sunburst-like appearance, consisting of a central powder-like disc with radiating petal-like spokes.
It is a characteristic lesion of WD, the only other condition in which it is seen being chalcosis (copper foreign body in the eye). Interestingly, it does not affect vision. It was described by siemerling and Oloff in 1922, and is rarer than KF ring.
Both KF rings and sun flower cataracts will gradually disappear with effective medical treatment by 3 years, or following liver transplantation, though the rate of disappearance may not correlate with resolution of clinical symptoms. As copper is removed from the cornea it leaves a pitted silver appearance which can be seen by slit lamp. This finding is one of the earliest signs of effective decoppering.
The reappearance of either of either KF ring or sunflower cataract in a medically treated patient in

28 Pediatric Companion
whom these had previously disappeared suggests noncompliance with therapy.
dermatologic FindingsCopper is essential for the activity of the enzyme
tyrosine hydroxylase (tyrosinase). As body copper is very high in WD, the activity of this enzyme is increased. It is a key enzyme for melanin synthesis and aids conversion of tyrosine to DOPA and melanin. Hence melanin synthesis is increased in WD and this gives a dark complexion to patients with advanced WD.
Blue lunulae of nails, pretibial hyperpig mentation and acanthosis nigricans may also be seen.
skeletal ManifestationsA peculiar manifestation of WD in India is the
‘osseomuscular’ type with genu valgum, suggestive of resistant rickets. The other features include osteomalacia, osteochondritis and recurrent fractures. Involvement of the large joints is seen due to the accumulation of copper in the synovium.
renal ManifestationsCopper is deposited in the proximal renal tubular
cells. Hence, it causes proximal tubular dysfunction characterized by aminoaciduria, glycosuria, renal tubular acidosis, impaired phosphate reabsorption or a full blown Fanconi syndrome and decreased glomerular filtration rate.
It may also cause nephrolithiasis secondary to distal renal tubular acidosis.
Hematologic ManifestationsIn any child with unexplained Coombs negative
hemolytic anemia, WD should be ruled out. Hemolysis is due to the sudden release of copper from the liver into the blood stream.
Cardiac manifestationsCopper deposition in the heart can lead to
cardiomyopathy or cardiac arrhythmias. sudden death in WD has been attributed to cardiac involvement but is rare.
Endocrine manifestationsHypoparathyroidism has been attributed to
infiltration of the parathyroid gland by copper. Amenorrhoea and testicular problems appear to result from Wilson disease itself, not from cirrhosis. Infertility or repeated spontaneous abortion may be a sign of WD.
MiscellaneousPancreatitis and rhabdomyolysis of skeletal
muscles may be seen. diFFErEntiAl diAGnosis
WD should be considered in the differential diagnosis of any young patient with:• Unexplained liver disease• Concomitant liver and neuropsychiatric illness• Fulminant hepatic failure
• Unexplained Coombs -negative hemolytic anemia• Unexplained elevation of transaminases
Acute viral hepatitis, chronic liver disease due to hepatitis B, hepatitis C, autoimmune hepatitis, metabolic liver diseases like galactosemia, hereditary fructose intolerance, alpha-1-antitrypsin deficiency, fulminant hepatic failure of various causes and non alcoholic steatohepatitis should be excluded in all children with suspected WD. If a child with suspected viral hepatitis does not improve in the first 2 weeks, the possibility of an underlying WD should always be considered. A positive HBsAg result should not prevent further investigation for the presence of WD as both may coexist.
Autoimmune hepatitis All children with apparent autoimmune hepatitis
who do not respond rapidly to steroids must be carefully re-evaluated for WD. At times, a patient with WD may improve with a brief course of steroids along with specific treatment for WD.
It should also be remembered that rarely a patient may have both WD and autoimmune hepatitis together.
Fulminant hepatic failure (FHF)some children with WD may present as fulminant
FHF. Hence, WD should always be excluded in any child above the age of 3 years with FHF.
non-alcoholic steatohepatitis (nAsH)Hepatic steatosis is common in WD and hence it
may be mistaken for NAsH. However, hepatic steatosis in WD is not as severe as in NAsH. Nevertheless, occasional patients with WD closely resemble NAsH or may have both diseases.
diAGnosisIf WD is not recognized and treated adequately,
the progression of hepatic and neurologic damage can be very rapid resulting even in FHF. Therefore, the prompt detection of this condition is vital. It can be diagnosed only if the clinician has a high index of suspicion, just like the classic Alfred Hitchcock thriller sUsPICION starring Cary Grant and Joan Fontain. In general, it should be excluded in any patient with unexplained liver disease.
The classic triad of WD consists of:• Hepatic disease• Neurological disease• KF ring.
Because at present, de novo genetic diagnosis is expensive and not universally available (and sometimes inconclusive), a combination of careful clinical history, family history, physical examination and laboratory investigations will usually help in clinching the diagnosis.
No single test is diagnostic of WD, but the presence of any two of the following is sufficient for the diagnosis:

29 November 2018
• Low serum ceruloplasmin • KF ring• Hepatic copper > 250 µg/g dry liver tissue.• 24-hour urinary copper >100 µg
Unexplained Coombs negative hemolytic anemia and biochemical evidence of hepatitis are useful supportive parameters.
serum Ceruloplasmin Ceruloplasmin is a 132-kd blue colored alpha
globulin synthesized by hepatocytes and secreted into the circulation. Its gene is on chromosome 3. It carries 90% of copper in the blood, with each molecule of ceruloplasmin binding up to six copper atoms tightly so that the copper is not readily exchangeable . The remaining 10% of plasma copper is carried by albumin but the binding is less tight compared to ceruloplasmin.
serum ceruloplasmin is decreased by 50% of lower normal value in 90% of patients with WD. However, low levels may also be seen in: • Normal neonates- it is very low at birth, resembling
that seen in WD. It increases to 30-50 mg/dL in the first years of life.
• Kwashiorkor- as ceruloplasmin is a plasma protein just like albumin
• Disorders that cause marked renal or enteric protein loss, such as nephrotic syndrome or protein-losing enteropathy.
• Fulminant hepatitis• End-stage liver disease of any cause with
associated poor synthetic function • Rare diseases like Menkes disease and hereditary
aceruloplasminemia • Any condition causing copper deficiency like
total parenteral nutrition with inadequate copper inclusion , malabsorption following gastric bypass surgery and excessive zinc administration
• 10% of heterozygotes for WD.Ceruloplasmin which is bound to copper is
referred to as holoceruloplasmin , and it represents
most of circulating ceruloplasmin. Ceruloplasmin that is not bound to copper is called apoceruloplasmin.
The genetic mutations causing WD impair the hepatic incorporation of copper into apoceruloplasmin. The six copper atoms present in holoceruloplasmin make it stable unlike apoceruloplasmin.
Besides, the half life of apoceruloplasmin is lower than that of holoceruloplasmin. These 2 factors are responsible for the lower level of serum ceruloplasmin seen in WD.
Ceruloplasmin is normal or even high in 10% of WD with active liver involvement and also in hepatitis and malignancies. This is because it is an acute phase reactant and hence its synthesis is increased if the child has an associated inflammation or tissue injury. In WD, as the inflammation abates, the serum ceruloplasmin level decreases to the low level typically seen in this condition. Ceruloplasmin is estrogen sensitive and hence it is also elevated in any condition with increased estrogen levels, like estrogen therapy and pregnancy.
Normal values for serum ceruloplasmin vary by age. They are very low during neonatal period and up to first six months, then peak in early childhood (30 to 50 mg/dl ), finally reaching the adult range (20 to 35 mg/dl ).
An extremely low serum ceruloplasmin level (<5 mg/dl) should be taken as a strong evidence for the diagnosis of WD. If it is modestly subnormal, further evaluation is necessary. However, it should always be remembered that a normal serum ceruloplasmin level does not exclude the diagnosis of WD.
An important drawback is that ceruloplasmin levels assessed by radial immunodiffusion assays used in most laboratories may overestimate it, thus missing the diagnosis. Ceruloplasmin is only a good screening test which cannot be solely relied on to confirm the diagnosis. (Table 2)
serum copperIn WD, the serum total copper level is usually low
in proportion to the reduction in serum ceruloplasmin, in spite of the copper overload. However, it may be
table 2 Biochemical parameters of Wd
Parameter Normal Wilson’s disease Ceruloplasmin 24-hour-urine copper
before penicillamine 24 hour urine copper
after penicillamine S Serum total copper Serum free copper Liver copper
> 20mg/dL <40 µg
Up to 20 times the basal level
80–120µg/dl 8 –12 µg/dl < 55 µg/g of dry liver tissue
< 20mg/dL> 100 µg
Very high- ranges from 40-10,000 µgLow/normal/high>25 µg/dl>250 µg/g of dry liver tissue
Serum uric acid and phosphate concentrations may be low in patients with untreated WD , reflecting renal tubular dysfunction.

30 Pediatric Companion
low, normal or high in WD . The author’s experience is its estimation in suspected WD does not help in the diagnosis.
Measurement of serum total copper levels actually includes both ceruloplasmin-bound and nonceruloplasmin-bound copper (free copper). Determination of the serum free copper concentration is useful in the diagnosis of WD. However, the drawback is that the test depends on the adequacy of the methods for measuring both serum copper and ceruloplasmin. Besides, the sensitivity and specificity of free copper for diagnosing WD have not been well-established.
serum free copper level is usually determined indirectly from the serum total copper and serum ceruloplasmin concentrations . Each mg of ceruloplasmin contains approximately 3.15 µg of copper. Thus, free copper can be calculated by the following equation:
Free copper (µg/dL) = serum total copper (µg/dL) – (3.15 x serum ceruloplasmin [mg/dL]).
It can be calculated directly with atomic absorption, which is not freely available in our country.
When the serum ceruloplasmin is low, we expect the serum copper also to be low (as we are measuring the ceruloplasmin-bound copper) . If the serum ceruloplasmin is low, and the serum copper is high or normal, it indicates that the serum free copper is high.
The normal serum free copper level is usually 8 –12 µg/dl. In children with untreated WD, it is typically above 20 to 25 µg/dL. It may be 10 times higher in patients with fulminant hepatic failure due to WD with intravascular hemolysis.
Children with WD who are on regular medication, a free copper level of <5 µg/dL indicates systemic copper depletion, and that the child is compliant with treatment.
relative exchangeable copper (rEC)In free copper, what is measured is not actually
“free” copper, because copper in the plasma compartment is always loosely bound to albumin and various amino acids, and hence the notion of “exchangeable copper” has been suggested.
REC is a recently described method for estimation of free copper. It focuses on copper that can be mobilized from proteins and peptides apart from ceruloplasmin using the chelating agent EDTA- ethylenediamine tetra acetic acid. This is called exchangeable copper. This exchangeable copper can be analyzed further and normalized by the total serum copper, giving rise to the term “relative exchangeable copper.” REC may be useful diagnostically and for treatment monitoring as it gives direct measurement instead of estimates.
However, it is not yet available commercially. Further studies are necessary to include this test in the routine diagnostic approach of WD.
24-hour urine copper estimation Urinary copper excretion is useful for the
diagnosis of WD and for monitoring therapy. It actually reflects the free copper concentration in plasma.
Normal values for urinary copper excretion vary in different laboratories but are in the range of ≤30 to 40 µg/day. WD is typically associated with 24-hour urinary copper excretion of >100 µg , although lower values may be seen in 25% of asymptomatic patients with confirmed disease . Values >40 µg/24 hours are suggestive of WD, and these children require further evaluation to confirm the diagnosis.
It should be realized that urine copper excretion may be high in children with other forms of chronic liver disease and also those who are heterozygotes for WD. However, in them the levels are usually below 100 µg/24 hours.
MethodThe 24-hour collection is begun at the usual time
the patient awakens. The first void is discarded and the exact time is noted. All urine passed subsequently is collected, with the last void timed to finish the collection at exactly the same time the next morning. The time of the final urine specimen should not vary by more than 5 or 10 minutes from the time of starting the collection the previous morning.
It is possible to determine whether the urine collection was for a full 24-hour period by measuring total urinary creatinine excretion (normal, 10–20 mg/kg/ 24 hr).Values significantly above or below this suggest over- and under-collection, respectively, which may affect the accuracy of the result.
False-positive results of a 24-hour urine copper excretion (i.e.>100 μg/24hr) may be seen if:• The patient is receiving any type of copper
chelation therapy • The collection is contaminated by exogenous
copper• The patient has chronic hepatitis, cholestatic
cirrhosis, or nephrotic syndromeRenal failure is a contraindication for this test.
spot urine collections which are highly variable are not reliable for making a diagnosis of WD.
There are some precautions to be taken for this highly informative test. It is important to avoid Copper contamination of the urine collection bottles. Wide-necked bottles with copper-free disposable polyethylene liners should be used. The bottles should be rinsed with distilled water; tap water should be avoided as it may contain copper. Before analysis, 30 ml of hydrochloric acid may be added to the urine to prevent precipitation of copper hydroxide, which occurs when the urine is alkaline resulting in false low urinary copper content. This is not necessary if urine pH is neutral or acidic.

31 November 2018
Penicillamine challenge testUrinary copper excretion may be increased
in several liver diseases apart from WD. Hence, penicillamine challenge test is used to increase sensitivity and specificity of 24 hour urine copper in WD. Penicillamine greatly increases urinary copper excretion in WD, but to a lesser extent only in other forms of liver disease.
The child, regardless of his weight, is given 500 mg of penicillamine just before the beginning of the 24-hour urine collection and another 500 mg after 12 hours. Urinary copper excretion greater than 40 µg/24 hours is suggestive of WD; it may even go up to 1000 µg/24 hours.
drawbacks• Unreliable to exclude WD in asymptomatic
siblings• Cannot differentiate heterozygous carriers from
affected homozygotes• Some studies have shown that it may be high in
children with virus A hepatitis • Not standardized in adults.
Fortunately, it has been standardized in children, in whom it can be used as an adjunctive test.
liver CopperLiver copper can be estimated by neutron
activation analysis or atomic absorption spectrometry, which are very expensive and not freely available.
It is important to collect liver biopsy samples without extraneous copper contamination. However, usually ordinary disposable liver biopsy needles can be used. The sample must be at least 1 cm in length. In the early stages of WD, when copper is distributed diffusely in the liver cell cytoplasm, this measurement may clearly indicate hepatic copper overload. However, in later stages, the measurement of hepatic copper is less reliable because copper is distributed unequally in the liver.
The normal total copper in the body is 50–150 mg and hepatic copper content is <55 µg /g of dry liver tissue. In WD, the hepatic copper content is usually more than 250 µg /g of dry liver tissue. It may even reach 3000 μg/g. WD can be excluded if the hepatic copper concentration is <55 µg/g dry liver tissue in untreated patients. However, if it is between 50 -250 µg /g , and the liver histology shows evidence of active liver disease, molecular genetic testing for ATP7B mutations is indicated to establish the diagnosis.
Histochemical evaluation with special stains like rhodamine, rubeanic acid or Timm’s silver sulphide detects only the lysosomal copper deposition, revealing focal copper stores in less than 10% of patients. Orcein may show a characteristic granular pattern in 50% of patients with WD. A negative biochemical stain for copper on a liver biopsy never rules out WD. These stains are invariably positive in cholestatic disorders like biliary atresia, prolonged extrahepatic biliary
obstruction and sclerosing cholangitis. However, these may be easily distinguished clinically and hence usually do not cause diagnostic confusion. With advanced liver disease, hepatic copper decreases as this copper is distributed to other tissues. At this stage, copper is distributed heterogeneously in the liver, and it may or may not be present in nodules. Due to these limitations, histochemical staining of copper should not be relied upon to diagnose WD.
Besides, biopsy may not be possible in a child with severe liver dysfunction. Transjugular liver biopsy may be performed if a significant coagulopathy is present.
Features of HemolysisWD should be ruled out in any child with
unexplained Coombs-negative hemolytic anemia and biochemical evidence of hepatitis.
Uric Acidserum uric acid may be decreased at presentation
with symptomatic hepatic or neurological disease because of associated renal tubular dysfunction (Fanconi syndrome).
imagingCranial CT scanning may show changes, including
increased density and ventricular enlargement, before neurological changes appear. MRI is more sensitive which may show hyperintensity on T2 MR imaging in the region of the basal ganglia. ‘Face of giant panda’ is the typical MRI finding of brain in neuro-WD due to hypodensity of the superior colliculi and hyperdensity of the medial substantia nigra and tegmentum. (Note: “Eye of tiger appearance” in MRI is seen in Hallervorden spatz disease). Dilatation of the third ventricle, and focal lesions in the thalamus, putamen and pallidum may also be seen.
Molecular Genetic testingThere are two types of molecular diagnosis for
WD—mutational analysis and haplotype analysis (linkage analysis) of the ATP7B gene.
Mutational analysisMore than 520 mutations in the ATP7B gene
have been identified by single strand conformation polymorphism analysis or by sequencing of each of the 21 exons. Hence, diagnosis of WD by DNA mutational analysis is very difficult unless a proband mutation is known. Most patients are compound heterozygotes. This makes it even more difficult to diagnose as we usually do not consider the possibility of WD at this age.
If a patient has a severe gene defect that has abolished the gene product, he could become symptomatic very early in life. Most patients are compound heterozygotes, carrying two different mutations for the gene.
It is now possible to confirm the diagnosis of WD by direct identification of mutations. The spectrum of manifestations of WD is actually wider than was

32 Pediatric Companion
recognized previously. There is still no confirmatory biochemical test. sometimes, even a combination of all tests prove inadequate for a diagnosis. For example, KF rings, thought to be pathognomonic of neuro- WD may not be present always. similarly, serum ceruloplasmin may be normal in a major proportion of patients with hepatic presentation. Due to the high cost and complexity, molecular testing cannot be readily used as a screening test for WD. However, if it is difficult to establish the diagnosis by clinical and biochemical tests, molecular testing will be extremely useful.
Haplotype analysisHaplotype analysis (analysis of the alleles of
microsatellite markers surrounding ATP7B) is an important strategy for cloning the abnormal gene in WD. This technique helps to diagnose siblings of WD patients (as affected, heterozygote or normal) when the mutation(s) cannot be identified in the affected proband.
Recently developed techniques permit sequencing of the entire ATP7B gene and thus are suitable for primary genetic diagnosis. However, these molecular techniques are expensive, not universally available, and can be interpreted only by expert geneticists.
radiocopper loading test (rlt) Very rarely, in a patient with suspected WD, all
biochemical tests may be normal, KF rings are absent and liver biopsy is contraindicated. In such patients, RLT may be very useful.
2 mg of cupric acetate containing 0.5 mCi of Cu-64 is given orally after an 8-hour fast in 100–150 mL of fruit juice . and the serum radioactivity is measured serially at 1, 2, 4, 24 and 48 hours. In normal people and patients with non-Wilsonian liver disease, the radiocopper rises at 1 and 2 hours as copper is absorbed into the bloodstream bound to albumin. It then falls with a secondary rise at 24 or 48 hours as the non-ceruloplasmin bound copper is incorporated into the newly synthesized ceruloplasmin in the liver and released into the circulation.
In WD, the initial rise of radiocopper at 1–2 hours occurs as copper is absorbed into the bloodstream. However, radiocopper is not incorporated into ceruloplasmin, even if ceruloplasmin levels are normal. Hence the secondary rise at 24 hours will be absent.
Although this test has been performed occasionally in the past , it is now rarely used because of the difficulty in obtaining the isotope.
Modified Calicut Scoring System for diagnosis of Wd
Most of the sophisticated investigations mentioned above are available only in very few centres in our country. Hence the diagnosis of WD will be very difficult for pediatrician s working in the periphery. We have therefore evolved a simple scoring system that may help in the diagnosis of WD (Table).
table 3 diagnosis of Wd (ideal)
KF ring Sunflower cataractLow ceruloplasmin High urine copperHigh liver copper Radiocopper studiesMutational analysis Haplotype analysis
Table 4 Modified Calicut score
Features PointsConsanguinity Sibling death due to liver diseaseLow ceruloplasmin Low ceruloplasmin & high SGPT i n siblings and parentsKF ringHigh urine copperSunflower cataractTotal
2233
33420
If the score is less than 3, WD is unlikely, and the patient should be investigated for other causes of liver disease. If the score is 4–8, WD is probable and the patient should be re-evaluated for WD. If the score is above 8, WD is definite. This helps to assess the severity of patients presenting with hepatic decompensation.
detection of symptom-free HomozygotesAll siblings of the patient should be screened.
A homozygote is suggested by hepatomegaly, splenomegaly, vascular spiders, and a slight elevation of transaminases. KF rings may or may not be seen. serum ceruloplasmin will be reduced. Liver biopsy with copper analysis is confirmatory.
There may be some difficulty in differentiating the homozygote from the heterozygote. If the two mutations of the index case are known, these can be tested in the siblings. If mutations cannot be detected in the Wilson’s disease gene, haplotype analysis comparing the affected patient with siblings should be done. Homozygotes must be treated even if symptom-free. Heterozygotes do not require treatment.
Ceruloplasmin in pregnancyCeruloplasmin levels increase gradually during
pregnancy, reaching the maximum at term. Hence, in a pregnant patient with WD, serum ceruloplasmin may be in the normal range (greater than 20 mg/dl). Thus, a diagnosis of WD may be difficult in pregnancy.
trEAtMEntThe aim of therapy is to decrease copper absorption
and accumulation in the liver and central nervous system. This indicates the need for lifelong medical therapy in all patients with WD.
dietary Management: see Box• Dietary copper intake should be restricted to
<1 mg/day. If possible, the copper content of

33 November 2018
the drinking water should be estimated and if it exceeds 0.1 mg/L, it may be necessary to decopper the water.
• Copper-rich food like meat , fish including dried fish and shellfish, liver, kidney, chocolates, nuts, dried beans, green chillies, mushrooms, legumes, unprocessed wheat, cocoa products, potato crisps, rye flour, oat flakes, milk products, cheese, pineapple and mineral water should be avoided.
• Vegetarian food, from which copper cannot be easily mobilized, is therefore recommended.
• Copper and brass vessels should not be used for cooking.
Box 2: diEt in Wd
Group-1 Food High in Copper Content- Should be Avoided• Meat Like Lamb, Chicken, Duck• Organ Meat Including Liver, Heart, Kidney, Brain• Fish- Salmon, Squid, Shellfish Like Shrimp, Lobster,
Clams, Crab• Soya Protein• Nuts And Oil Seeds• Vegetables: Mushroom, Beetroot, Onion Stalk, Dried
Beans, Soybeans, Baked Beans, Dried Peas, Lentil, Green Leafy Vegetables, Green Chillies, Spinach, And Mustard Greens.
• Cereals: Barley, Whole Wheat Products, Corn, Jowar, Ragi, Bajra
• All Spices • Dried Fruits, Raisins, Dates, Prunes• Bournvita, Horlicks, Milo Etc• Chocolates, Cocoa, Chocolate Milk, Soya Milk• Multiple Minerals With Copper• Mineral WaterGroup 2 Moderate Copper Content- May Be Taken As
Permitted• All Other Fish• Peanut Butter• Vegetables- White Radish, Spinach, Broccoli,
Asparagus, Tomato, Potato, Green Peas• Fruits- Orange, Papaya, Seethaphal, Pear, Green Grapes,
Ketchup,Group-111- Low Copper- Can Be Taken Safely• Rice • Eggs• All Dairy Products• Butter, Cream, Mayonnaise• Refined Flour, Bread, Pasta• Most Fruits And Vegetables Except Those Listed In
Group II• Coffee, Tea• Dhal Can Be Used Weekly Once/Twice
Pharmacologic therapyWD was uniformly fatal until treatments were
developed half a century ago. It was one of the first liver diseases for which effective pharmacologic treatment was identified.
Conventional medical therapies are based on either copper chelators like d-penicillamine, trientine and tetrathiomolybdate, or zinc. Chelators mobilize intracellular copper into the circulation which is then
excreted in the urine. Zinc decreases copper content mainly by reducing intestinal absorption.
initial therapyThe aim is to reduce copper to subtoxic levels
which usually takes about 6 months. Maintenance therapy
The aim is to maintain a negative copper balance so as to prevent copper accumulation and toxicity. D-penicillamine, trientine and zinc are used for this.
D-Penicillamine (β- β- dimethylcysteine)D-Penicillamine, introduced by Walshe in 1956, is
the cornerstone of therapy. It is a sulfhydryl-containing metabolite of penicillin.
D-penicillamine is thought to ‘detoxify’ the liver copper by the following mechanisms:• It inhibits the accumulation of copper in
hepatocellular lysosomes and solubilizes copper for mobilization from these particles, but not from cytoplasmic metallothionein
• Induction of metallothionein in liver favoring lysosomal sequestration (like zinc)
• Augmenting the thiol pool, binding copper in other nontoxic complexes
• A direct anti-inflammatory action • Reduction of hepatic fibrosis by impairing
collagen cross-linking. Thus, unbound or “toxic” copper will not be
available to injure the liver and CNs.Dose: 20 mg/kg/day, one hour before or two
hours after meals as it is best absorbed in the absence of food. If D-penicillamine is taken with food, its absorption is decreased almost by 50%. The maximum dose should not exceed 1 g/day (unless justified by the clinical status of the patient). Pyridoxine should also be given in the dose of 25 mg/day.
Usually, significant clinical improvement is seen within weeks of starting treatment. Generally, symptoms subside first, followed by the disappearance or fading of the KF ring. Liver function tests show improvement within several months and hepatic copper content decreases subsequently. However, if there is no improvement, the dose may be increased to 1.5–2 g/day.
In neuro WD, there may be initial worsening of symptoms following D-penicillamine. This may be because of the release of large amounts of copper from the liver that gets deposited in the brain. starting with a small dose and then increasing it gradually could avoid this. Another option is to replace it with trientine or zinc.
Adverse Effects Initially, a mixture of D and L isomers was used
and hence adverse effects were more. D-penicillamine is much less toxic, but still causes significant side effects in 5–10% of patients. Urticaria, agranulocytosis, aplastic anemia and lymphadenopathy may be seen.

34 Pediatric Companion
It may rarely cause sLE, Goodpasture syndrome and nephrotic syndrome. Dermatological toxicities reported include progeric changes in the skin , elastosis perforans serpingosa and pemphigus or pemphigoid lesions, lichen planus, aphthous stomatitis and cutis laxa.
For treatment of these reactions, penicillamine may be temporarily discontinued until the lesions resolve and 2 or 3 days before restarting therapy, prednisolone may be started in the dose of 0.5mg/kg/day. Penicillamine is then reintroduced at a lower dose and increased gradually. When the final dose is reached and tolerated, prednisolone may be stopped.
In the event of serious unremitting side effects, penicillamine should be substituted by trientine.
During the first 2 months of D-penicillamine treatment, white cell and platelet counts are done twice weekly, then monthly up to 6 months and thereafter less frequently. Proteinuria should also be looked for. The serum ceruloplasmin may decrease after initiation of treatment with D-penicillamine and it may then remain low. When the patient responds to treatment, liver regains synthetic activity and hence serum ceruloplasmin may increase. Hence, repeated estimation of ceruloplasmin will not be useful in the follow up of these patients.
Response to treatment is monitored by measuring urine copper while on treatment. This is highest immediately after starting treatment and may even exceed 1000 µg per day at that time. With maintenance treatment, urinary copper excretion should be around 200-500 µg/day. If urine copper excretion is <200 µg/day, it indicates either non-adherence to therapy or over treatment and excess copper removal. In those with non-adherence to therapy, free copper is elevated. serum free copper becomes normal with effective treatment.trientine (triethylene tetramine dihydrochloride)
Trientine was introduced in 1969 by Walshe as a second-line drug in children who do not tolerate penicillamine. It was approved by the FDA in 1985.
It has a polyamine-like structure chemically distinct from penicillamine. It lacks sulfhydryl groups and copper is chelated by forming a stable complex with the four constituent nitrogen in a planar ring. It increases renal excretion of copper like penicillamine. It has a lower cupriuretic effect than D-penicillamine but is clinically effective. The incidence of neurological worsening after beginning treatment is much less compared to penicillamine. It is an effective initial therapy even for patients presenting with decompensated WD.
Early toxicity includes bone marrow suppression and proteinuria. It may later cause sLE, Goodpasture syndrome, sideroblastic anemia, nephrotoxicity and skin and mucosal lesions. Patients are monitored by 24- hour urine copper and other lab tests as in penicillamine.
As trientine also chelates iron, co-administration of trientine and iron should be avoided as the complex with iron is toxic.
The main drawback is that it is extremely expensive compared to D-penicillamine.
Dose: 20 mg/kg, 1 hour before or 2 hours after food.
zincZinc was introduced in the treatment of WD by
schouwink from Holland in 1961. It is an attractive drug as it is more physiological than D-penicillamine and trientine, is less toxic and very cheap.
Zinc induces metallothionein synthesis in the enterocytes and hence copper is trapped in them. Thus, it prevents copper from entering the portal circulation which is then lost in the stool as enterocytes are shed in normal turnover.
Zinc also induces synthesis of copper binding metallothionein in the hepatocytes, thereby reducing the damaging effects of free copper in liver.
Additionally, zinc may interfere with lipid peroxidation and enhance the availability of glutathione. Body secretions like saliva, gastric juice, bile, pancreatic juice and succus entericcus contain about 1 mg copper. As this copper is also not absorbed and is lost in stools, tissue copper can also be decreased.
In patient presenting with neurologic or psychiatric signs, zinc may have a role as a first line therapy as it does not cause neurological deterioration. As it is not teratogenic unlike D-penicillamine and trientine, it is the recommended therapy during pregnancy. some advocate zinc only for maintenance treatment, but it can be used as first-line therapy, for asymptomatic or presymptomatic patients.
Effect of therapy and compliance can be monitored by 24-hour urine zinc (should be >2 mg) and urine copper levels (should be <125 µg). This can be done 6 monthly initially and then annually. The urine copper level is a good reflection of the body’s excess load of easily mobilizable copper. It will increase if control is not adequate. A decrease in urine zinc is an early signal that the patient’s compliance is not optimal.
After initial treatment with D-penicillamine, zinc alone can be used for maintenance therapy. If both D-penicillamine and zinc are used, they should be given at different times. The rationale for combined therapy is that both drugs act in different ways and there may be an additive effect. It may help to produce an optimum response without using toxic levels of penicillamine.
Thus, zinc is a very useful drug for patients with WD . Negligible toxicity compared to penicillamine and trientine ia a major advantage. Besides, it is very cheap compared to the other drugs. One month course of zinc costs only about Rs 200-250, compared to Rs 1500-1800 for penicillamine and Rs 10,000 – 12,000 for trientine.

35 November 2018
doseChildren: Elemental zinc 25 mg thrice a day
between meals.Adolescents and adults: 50 mg thrice daily Zinc should be taken with water or juice.
However, if it causes gastritis, it can be taken with meals. It should not be taken at the same time as iron or calcium supplements.
In countries where penicillamine, trientine, and zinc acetate are not available or cannot be afforded, zinc salts such as the gluconate or sulfate provide an alternative treatment option.
Ammonium tetrathiomolybdate (AtM)This drug has an interesting history. sheep are
very susceptible to copper poisoning, but this is less likely to occur on molybdenum-supplemented feeds. This effect is due to the formation of ammonium tetrathiomolybdate in the gut.
ATM is a powerful copper chelator and became an effective drug for bovine copper poisoning. It was introduced by Brewer in patients with neuro WD who develop worsening of neurological symptoms following penicillamine therapy.
Unlike the other drugs used for WD, this relatively new drug, after absorption from the gut, forms a tripartite inert complex with copper and protein both in the gut and blood rendering the complex non absorbable and non toxic, so that the cells cannot take up copper. It has a higher affinity for copper than metallothionein. Given with food, it can also form complexes with dietary copper throughout the gut which are excreted in the stools.
It is especially effective in acute neurological disease as it does not exacerbate neurologic manifestations, unlike D-penicillamine. It may rarely cause anemia, bone marrow depression and hepatitis.
Dose: 30 mg twice daily.However, it is still not available commercially.
(Table 5)
MonitorinG oF PAtiEntsThe key to long term success of pharmacotherapy
for WD is strict adherence to the use of medications. This is important to ensure compliance with therapy, to confirm clinical and biochemical improvement and to identify complications early.• History and clinical examination to detect any
changes in the symptoms and signs of liver or neurologic disease.
• Pill counts.• Complete blood count and urine analysis as well
as physical and neurological examinations should be performed regularly, at least twice annually
• Screening for biochemical evidence of hepatic dysfunction by estimation of transaminases and INR.
• Periodic slit-lamp examination to see if the KF ring is disappearing; or it has reappeared after therapy
• Response to treatment monitored by measuring 24- hour urinary copper excretion which should be around 200-500 µg per day. It is more difficult to interpret changes in urine copper because renal excretion reflects the effect of the drug as well as body loading with copper. The ideal way of monitoring anti-copper effects of trientine and penicillamine is by following 24-hour free serum copper.
• Measurement of urinary copper or zinc excretion. 24 hour urinary copper excretion in patients on zinc therapy is not significantly elevated because zinc acts by preventing copper absorption from gut. However, a rise in urinary copper excretion to above 150 to 250 μg/24 hours may indicate noncompliance or inadequate treatment. If so, they are likely to be accompanied by an increase in the serum free copper level. Urinary and plasma levels of zinc may also be used to monitor compliance with zinc therapy.
table 5: Expense of Wd therapy
DrugMonthly
expense in RsDose Side effects Monitoring
Penicillamine
Trientine
Zinc
Tetrathio-molybdate
1500-1800
10,000-12,0000
200-250
Not available freely
20mg/kg in 2-3 DD-do-
25mg TID30 mg BD
BM depression; SLE; ne-phrotic syndromeBM depression; SLE; Goodpasture syndromeGastritisBM depression; hepatitis
24 h urinary copper, serum free copper-do-
24 h urinary copper; serum free copper ;24 h urine zinc level

36 Pediatric Companion
AntioXidAnt tHErAPyThe use of antioxidants as adjunctive therapy
in WD has not been fully explored. Copper induces oxidative damage to the hepatocytes and α-tocopherol levels may be low during copper overload. Hence, it has been proposed that α-tocopherol in the dose of 400-1200 IU/day may be given in divided doses with meals in symptomatic patients with WD.
MAnAGEMEnt oF tHE PrEGnAnt AdolEsCEnt
This is important in pediatrics as we are now treating adolescents also.
Copper status should be optimized before contemplating pregnancy. Patients require more frequent monitoring during pregnancy. Even though penicillamine does have teratogenic potential, benefits of continuing treatment far outweigh risks of sudden withdrawal of treatment, which may precipitate fulminant hepatic failure. Zinc can be continued at the same dose, but the dose of D-Penicillamine and trientine may be reduced by 25–50%.
D-Penicillamine may impair wound healing after caesarean section or episiotomy. This is another indication for reducing the dose of D-penicillamine toward the latter weeks of pregnancy for better wound healing.
ContrACEPtion in WdThe physician should advise only spermicidal,
barrier methods. Intrauterine devices like copper-T which contain copper should not be used. If contraceptive pills are used, progesterone only preparations are advisable as estrogens may interfere with biliary copper excretion. They may also cause diagnostic confusion by increasing ceruloplasmin levels.
novEl tHErAPiEs• As the current treatment available cannot cure
WD gene defect, novel strategies are essential which may help to correct ATP7B mutants.
• There are studies on enhancing the mutant ATP7B protein expression with residual copper export activity.
• Some other therapies tested in animal models include hepatocyte transplantation, lentiviral gene transfer or adenovirus-mediated transfer
• Gene Therapy-here, a normal allele of the WD gene is introduced into the hepatocytes of a patient who is homozygous for WD. This is under experimental stage at present.
livEr trAnsPlAntAtionThe role of orthotopic liver transplantation is well
established in patients with fulminant liver failure caused by WD as it corrects the underlying hepatic metabolic defects of WD. In addition, patients with end-stage liver disease caused by WD should also be considered for LT . Long-term survival is excellent following LT and the liver lesion does not recur following transplant because of the presence of ATP7B
in the donor liver. The outcome of children with severe neurologic
or psychiatric manifestations of WD is poor after LT; besides, these patients may not adhere to the strict medical regimens after LT. Hence, LT should be reserved for patients with severe, decompensated liver disease that is unresponsive to therapy, or with fulminant hepatic failure.
Live-donor LT, even from a heterozygous family member, yields adequately functioning grafts. However, if the donor is a sibling of the patient, mutational analysis of his or her ATP7B gene is essential to exclude presymptomatic WD.
After successful LT , all laboratory parameters improve. LT is a causal therapy which confirms that the primary metabolic defect of WD is located in the liver. This means that anti-copper drugs and copper restricted food are not required anymore following transplantation.
ProGnosisUntreated WD is progressive and fatal. The
greatest danger is that the patient remains undiagnosed and dies untreated. The prognosis of patients with WD who comply with pharmacotherapy is excellent, even if cirrhosis or chronic hepatitis is present at the time of diagnosis. Patients with neurologic or psychiatric symptoms of WD may continue to recover for months to years after the initiation of treatment. In some patients with neurologic or hepatic disease, symptoms or biochemical abnormalities persist but stabilize with treatment.
At present, the best way to determine whether and to what extent a patient’s disease is reversible is to await the response to treatment. In chronic hepatitis, response to treatment can be poor. Jaundice, ascites, high serum bilirubin and transaminases and prolonged prothrombin time are ominous signs. Liver transplantation may be life-saving in such patients. Unlike hemochromatosis, hepatocellular carcinoma is uncommon.
GEnEtiC CoUnsElinGRisk to family members:A. Risk to the parents of a probandThe parents of a patient with WD are obligate
heterozygotes . They may have low serum ceruloplasmin, borderline normal urinary copper, and elevated urine copper on D-penicillamine challenge. There may also be mild elevation of liver copper (100–250 µ g/g of dry liver tissue). Clinical disease is not known to occur in carriers.
B. Risk to the siblings of a proband• 25% will have WD.• 50% will be unaffected carriers.• 25% will be normal.
C. Risk to the offsprings of a proband The offsprings of an affected individual are
obligate carriers.

37 November 2018
MAnAGEMEnt oF siBlinGs oF WdThe siblings of a child with WD have a 25% chance
of being affected. Hence they should have a thorough clinical examination, LFT, slit-lamp examination for KF rings, serum ceruloplasmin and 24-hour urine copper. If these are normal, WD is unlikely.
If any one of these is abnormal, a liver biopsy should be done for histology, electron microscopy and quantitative hepatic copper content.This screening should be done initially at 3–5 years of age and repeated at 15 years of age. The results are unreliable, if done before 3 years of age.
sUrGEry in WdAs penicillamine inhibits collagen cross linking,
it may interfere with wound healing. Hence, the dose of penicillamine should be reduced but not stopped, for 10-14 days after surgery.
nEWBorn sCrEEninGMeasurement of ceruloplasmin in Guthrie dried-
blood spots or urine samples from newborns may promote detection of individuals affected with WD but further refinement of methodology involving immunologic measurement of ceruloplasmin is required before wide-scale implementation can be advised.
MEdniK syndromeThis is a recently reported rare multisystem
disorder of copper metabolism with features of both Menkes kinky hair disease and Wilson’s disease. (Mental retardation,Enteropathy, Deafness, Neuropathy, Ichthyosis, Keratoderma) . It is due to mutations in the AP1s1 gene, which encodes an adaptor protein necessary for intracellular trafficking of copper pump proteins ATP7A (Menkes disease) and ATP7B (Wilson’s disease).
This rare disease with a unique picture and copper overload of liver, is treatable by zinc acetate .
sUMMAry
• WD is one of the few treatable metabolic liver diseases.• WD should be considered in any individual between the
ages of 3 and 55 years with liver disease of uncertain cause. Age alone should not be the basis for eliminating a diagnosis of WD.
• Diagnosis of WD remains challenging, involving clinical, laboratory, histological and molecular tools.
• WD must be excluded in any patient with unexplained liver disease along with neurological or neuropsychiatric abnormalities.
• WD should be excluded in any patient with unexplained Coombs negative hemolytic anemia.
• In a patient with suspected WD, KF rings should be sought by slit-lamp examination by an experienced ophthalmologist. The absence of KF ring does not exclude the diagnosis of WD, even in patients with predominant neurological disease.
• An extremely low serum ceruloplasmin level (<5 mg/dl) is highly suggestive of WD. subnormal levels suggest further evaluation is necessary. Normal ceruloplasmin level does not exclude the diagnosis of WD.
• Increased transaminases may be the only abnormality found in early course of WD
• Basal 24-hour urinary copper should be done in all patients with suspected WD. It is typically >100 μg in symptomatic patients, but >40 μg may also indicate WD and requires further investigation.
• If basal urinary copper excretion is <100 μg/24 hours, penicillamine challenge studies may be required.
MorE on tHis toPiC1. Pilankatta R, Lewis D, Inesi G. Involvement of protein
kinase D in expression and trafficking of ATP7B (copper ATPase). J Biol Chem. 2011;286(9):7389–96. 2.
2. Bhave s, Bavdekar A, Pandit A: Paediatric Wilson’s disease in India. Paediatrics Today. Vol 3 No 1, 2000.
3. Heinz Weiss K, Thurik F, Gotthardt DN, et al: Efficacy and safety of oral chelators in treatment of patients with Wilson disease, Clin Gastroenterol Hepatol 11:1028–1035, 2013.
4. Pandit A, Bavdekar A, Bhave s: Wilson’s disease. Ind J Pediatr, 2002; 69:785–791.
5. schilsky ML, Tavill As: Wilson’s disease. In schiff ER, sorrell M, Maddrey W (Eds): schiff’s Diseases of the Liver, 10th ed. Philadelphia, Lippincott Williams & Wilkins, 2007, pp 1023-1040.
6. Roberts EA: Wilson’s disease. In Dooley Js, Lok AsF, Burroughs AK, Heathcote EJ (eds): sherlock’s diseases of the liver and biliary system, 12th ed. Blackwell Publishing Ltd, 2012
7. Coffey AJ, Durkie M, Haque s, et al. A genetic study of Wilson disease in the United Kingdom Brain 2013;136:1476
8. Riyaz A.: Wilson disease. In Pediatric Gastroenterology and Hepatology.Ed A. Riyaz. 3rd ed. Paras Publishers,2008
9. Ala A, Walker AP, Ashkan K, Dooley Js, schilsky ML. Wilson’s disease. Lancet. Feb 3 2007; 369(9559):397-408.
10. Merle U, schaefer M, Ferenci P, stremmel W. Clinical presentation, diagnosis and long-term outcome of Wilson’s disease: a cohort study. Gut. Jan 2007; 56(1): 115-20.
11. sinha s, Taly AB. Withdrawal of penicillamine from zinc sulphate-penicillamine maintenance therapy in Wilson’s disease: promising, safe and cheap. J Neurol sci. Jan 15 2008; 264(1-2):129-32.
12. Chakraborty PP, Mandal sK, Bandyopadhyay D, Bandyopadhyay R, Chowdhury sR. Recurrent limb weakness as initial presentation of Wilson’s disease. Indian J Gastroenterol. 2007; 26(1):36-8
13. Korman JD, Volenberg I, Balko J et al. screening for Wilson Disease in acute liver failure: a comparison of currently available diagnostic tests. Hepatology 2008; 48: 1167 – 1174
14. Linn FH, Houwen RH, van Hattum J, van der Kleij s, van Erpecum KJ. Long -term exclusive zinc monotherapy in symptomatic Wilson disease: experience in 17 patients. Hepatology 2009; 50:1442–52.
15. Nazer H. Ede RJ, Mowat AP et al. Wilson’s disease, clinical presentation and use +of prognostic index. Gut 1986; 27:1377-81
16. Beihardt s, Leiss W, stattermayer AF, et al. Long-term outcomes of patients with Wilson disease in a large Austrian cohort. Clin Gastroenterol Hepatol. 2014;12:683
17. Krishnakumar P, Riyaz A. Wilson disease presenting as depressive disorder. Ind Pediatr. 2005;42;182
18. EAsL Clinical Practice Guidelines: Wilson’s disease. J Hepatol. 2012;56(3):671–85.
19. schilsky ML. Long-term outcome for Wilson disease: Clin Gastroenterol Hepatol. 2014;12:690–1
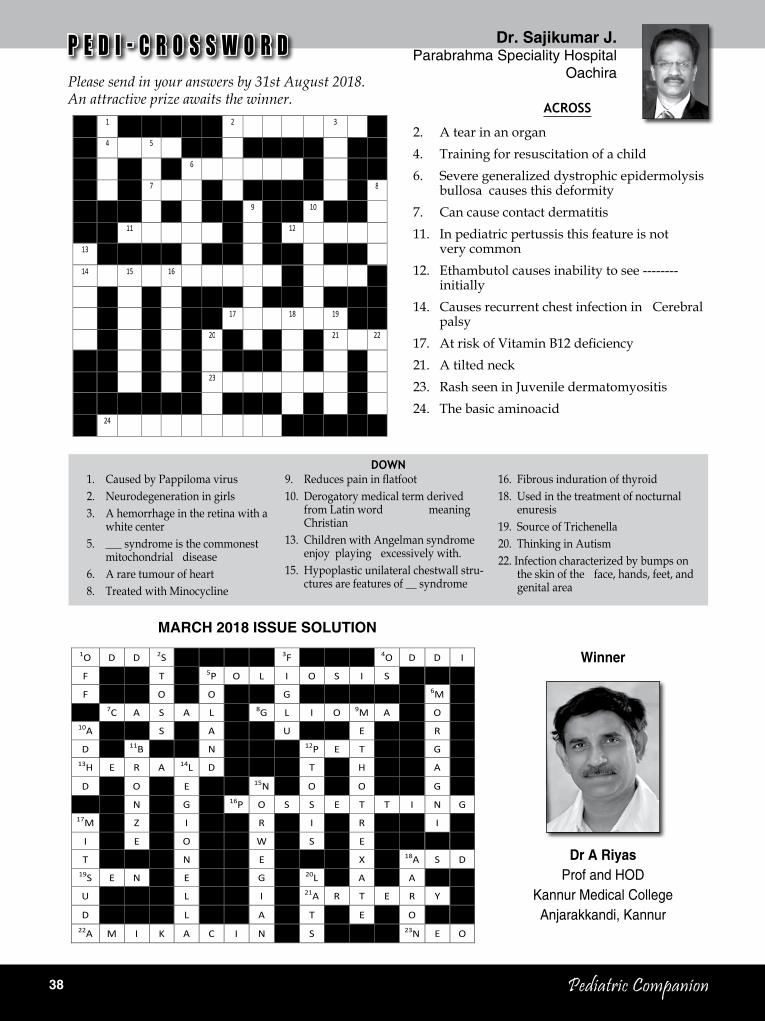
38 Pediatric Companion
PEDICROSSWORD
1 2 3 4 5 6 7 8 9 10 11 12
13 14 15 16 17 18 19 20 21 22 23 24
ACROSS 2. A tear in an organ 4. Training for resuscitation of a child 6. Severe generalized dystrophic epidermolysis bullosa causes this deformity 7. Can cause contact dermatitis 11. In pediatric pertussis this feature is not very common 12. Ethambutol causes inability to see -------- initially 14. Causes recurrent chest infection in Cerebral palsy 17. At risk of Vitamin B12 deficiency 21. A tilted neck 23. Rash seen in Juvenile dermatomyositis 24. The basic aminoacid
DOWN 1. Caused by Pappiloma virus 2. Neurodegeneration in girls 3. A hemorrhage in the retina with a white center 5. ---------- syndrome is the commonest mitochondrial disease 6. A rare tumour of heart 8. Treated with Minocycline 9. Reduces pain in flatfoot 10. Derogatory medical term derived from Latin word meaning Christian 13. Children with Angelman syndrome enjoy playing excessively with. 15. Hypoplastic unilateral chestwall structures are features of ----- syndrome 16. Fibrous induration of thyroid 18. Used in the treatment of nocturnal enuresis 19. Source of Trichenella 20. Thinking in Autism 22. Infection characterized by bumps on the skin of the face, hands, feet, and genital area
Please send in your answers to the editor by _____. An attractive prize awaits the winner.
Dr. Sajikumar. J Parabrahma Specialty Hospital
Oachira
dr. sajikumar J.Parabrahma Speciality Hospital
Oachira
1. Caused by Pappiloma virus2. Neurodegeneration in girls3. A hemorrhage in the retina with a
white center5. ___ syndrome is the commonest
mitochondrial disease6. A rare tumour of heart8. Treated with Minocycline
9. Reduces pain in flatfoot10. Derogatory medical term derived
from Latin word meaning Christian
13. Children with Angelman syndrome enjoy playing excessively with.
15. Hypoplastic unilateral chestwall stru-ctu res are features of __ syndrome
Down
MArCH 2018 issUE solUtion
16. Fibrous induration of thyroid18. Used in the treatment of nocturnal
enuresis 19. source of Trichenella20. Thinking in Autism22. Infection characterized by bumps on
the skin of the face, hands, feet, and genital area
P E D I - C R O S S W O R DPlease send in your answers by 31st August 2018. An attractive prize awaits the winner.
Across
2. A tear in an organ4. Training for resuscitation of a child6. severe generalized dystrophic epidermolysis
bullosa causes this deformity7. Can cause contact dermatitis11. In pediatric pertussis this feature is not
very common12. Ethambutol causes inability to see --------
initially14. Causes recurrent chest infection in Cerebral
palsy17. At risk of Vitamin B12 deficiency21. A tilted neck23. Rash seen in Juvenile dermatomyositis24. The basic aminoacid
Winner
dr A riyas Prof and HOD
Kannur Medical College Anjarakkandi, Kannur
1O D D 2S 3F 4O D D I
F T 5P O L I O S I S
F O O G 6M
7C A S A L 8G L I O 9M A O 10A S A U E R
D 11B N 12P E T G 13H E R A 14L D T H A
D O E 15N O O G
N G 16P O S S E T T I N G 17M Z I R I R I
I E O W S E
T N E X 18A S D 19S E N E G 20L A A
U L I 21A R T E R Y
D L A T E O 22A M I K A C I N S 23N E O

39 November 2018

40 Pediatric Companion
rni regn. no. KErEnG/2006/18758Pediatric Companion november 2018 rs.20.00
Owned, Printed, Published and Edited by Dr. M. Narayanan, ‘Sarovaram’ Mamangalam, Palarivattom P.O., Kochi 682 025, Kerala and printed at Geo Printshop, Kochi for G.K. Printers, Azad Road, Kaloor, Kochi-17, Published at Kochi. Design : Pixel Studio, Cochin-28