
Impedance analysis of Bi3.25La0.75Ti3O12 ferroelectric ceramic

Clin Chem Lab Med 2012;50(12):2093–2105 © 2012 by Walter de Gruyter • Berlin • Boston. DOI 10.1515/cclm-2012-0289
Review
The emerging role of biomarkers and bio-impedance in evaluating hydration status in patients with acute heart failure
Salvatore Di Somma 1, *, Silvia Navarin 1 , Stefania Giordano 1 , Francesco Spadini 1 , Giuseppe Lippi 2 , Gianfranco Cervellin 3 , Bryan V. Dieffenbach 4 and Alan S. Maisel 4
1 Department of Medical-Surgery Sciences and Translational Medicine , Post Graduate School of Emergency Medicine, Sapienza University, Sant ’ Andrea Hospital, Rome , Italy 2 Laboratory of Clinical Chemistry and Hematology , Academic Hospital Parma , Italy 3 Emergency Department , Academic Hospital of Parma, Parma , Italy 4 Division of Cardiology , University of California San Diego, San Diego Veterans Healthcare System, San Diego, CA , USA
Abstract
The quantitative and qualitative estimation of total body fl uid content has proven to be crucial for both diagnosis and prog-nosis assessment in patients with heart failure. The aim of this review is to summarize the current techniques for assess-ing body hydration status as well as the principal biomarkers associated with acute heart failure (AHF). Although clinical history, physical examination and classical imaging tech-niques (e.g., standard radiography and echocardiography) still represent the cornerstones, novel and promising tools, such as biomarkers and bio-electrical impedance are achiev-ing an emerging role in clinical practice for the assessment of total body fl uid content. In the acute setting, the leading advantages of these innovative methods over device are rep-resented by the much lower invasiveness and the reasonable costs, coupled with an easier and faster application. This arti-cle is mainly focused on AHF patients, not only because the overall prevalence of this disease is dramatically increasing worldwide, but also because it is well-known that their fl uid overload has a remarkable diagnostic and prognostic signifi -cance. It is thereby conceivable that the bio-electrical vector
analysis (BIVA) coupled with laboratory biomarkers might achieve much success in AHF patient management in the future, especially for assisting diagnosis, risk stratifi cation, and therapeutic decision-making.
Keywords: acute heart failure; bio-impedance; biomarkers; hydration status; total body water.
Introduction
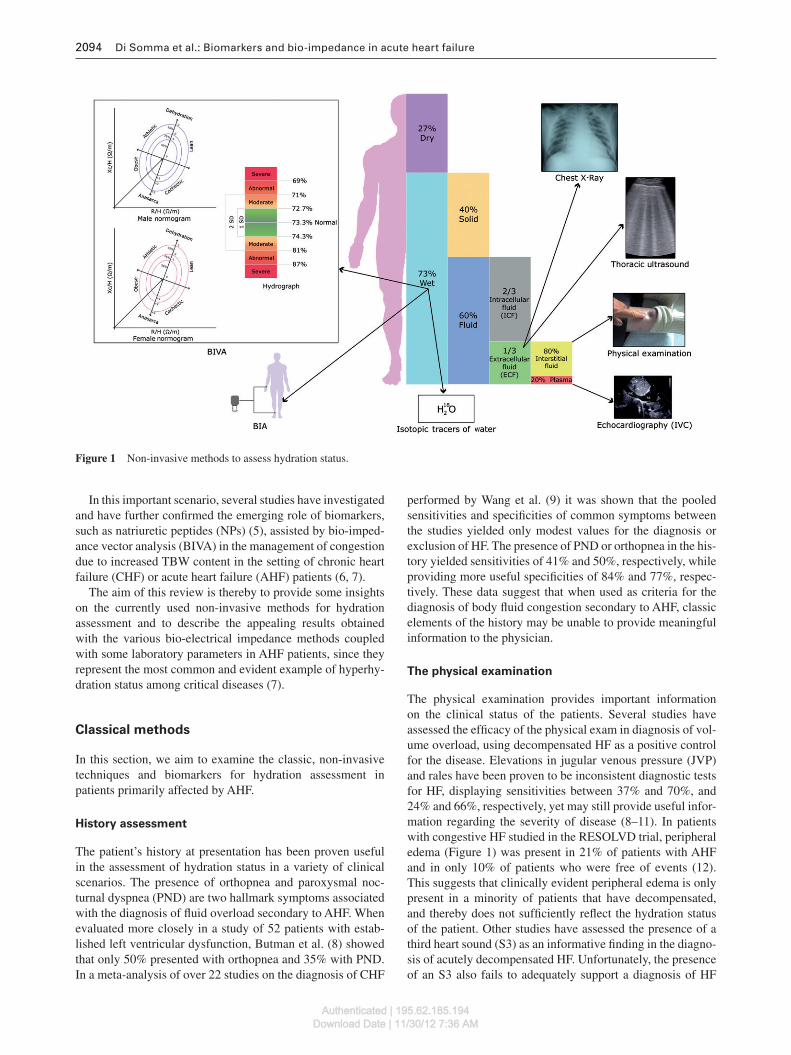
The total body water (TBW) in the healthy population is esti-mated to be approximately 60 % of the body weight, and is supposed to change during life because it is infl uenced by age, amount of fat tissues as well as hormonal homeostasis. Although there is a continuous shift of body fl uids through-out the cells, they are operatively divided into two compart-ments, intracellular and extracellular. The intracellular fl uid is defi ned as the water contained within the cell membranes and represents nearly two-thirds of TBW. The remaining one-third is the extracellular compartment that is further divided into interstitial fl uid and intravascular fl uid (1) (Figure 1 ). The TBW is constantly adjusted by some important homeostatic mechanisms including the balance between water intake and water loss through renal and gastrointestinal output, breathing and sweating (2) . The estimation of TBW content is impor-tant in the prognostic assessment of critically ill patients and should be considered a vital parameter coupled with blood pressure, heart and respiratory rates, oxygen saturation and temperature.
The accurate and fast assessment of total fl uid balance in critical patients, along with a standard and reliable means for its evaluation, has always been challenging for physicians working in the acute care setting. The current gold standard (i.e., isotope dilution) is not used in everyday clinical prac-tice and is even more diffi cult to apply when an emergency clinical decision is required (3) . Several approaches have been used to estimate the hydration status of patients, includ-ing history and physical examination, laboratory testing and imaging techniques (3) . The clinical experience has provided unquestionable evidence that fl uid overload refl ects the wors-ening of clinical conditions in a variety of severe disorders, such as heart failure (HF), chronic kidney diseases (CKD), and liver cirrhosis (4) . Moreover, the invasive catheterization of heart and great vessels only refl ects the circulating volume of total fl uid content and not the TBW.
*Corresponding author: Prof. Salvatore Di Somma, MD, PhD, Department of Medical-Surgery Sciences and Translational Medicine, Post Graduate School of Emergency Medicine, Sapienza University, Sant ’ Andrea Hospital, Via di Grottarossa,1035/1039 00189 Rome, ItalyPhone: + 39 6 33775581/ + 39 6 33775592, Fax: + 39 6 33775890, E-mail: [email protected] Received May 8, 2012; accepted July 22, 2012 ; previously published online September 19, 2012
Authenticated | 195.62.185.194Download Date | 11/30/12 7:36 AM
2094 Di Somma et al.: Biomarkers and bio-impedance in acute heart failure
In this important scenario, several studies have investigated and have further confi rmed the emerging role of biomarkers, such as natriuretic peptides (NPs) (5) , assisted by bio-imped-ance vector analysis (BIVA) in the management of congestion due to increased TBW content in the setting of chronic heart failure (CHF) or acute heart failure (AHF) patients (6, 7) .
The aim of this review is thereby to provide some insights on the currently used non-invasive methods for hydration assessment and to describe the appealing results obtained with the various bio-electrical impedance methods coupled with some laboratory parameters in AHF patients, since they represent the most common and evident example of hyperhy-dration status among critical diseases (7) .
Classical methods
In this section, we aim to examine the classic, non-invasive techniques and biomarkers for hydration assessment in patients primarily affected by AHF.
History assessment
The patient ’ s history at presentation has been proven useful in the assessment of hydration status in a variety of clinical scenarios. The presence of orthopnea and paroxysmal noc-turnal dyspnea (PND) are two hallmark symptoms associated with the diagnosis of fl uid overload secondary to AHF. When evaluated more closely in a study of 52 patients with estab-lished left ventricular dysfunction, Butman et al. (8) showed that only 50 % presented with orthopnea and 35 % with PND. In a meta-analysis of over 22 studies on the diagnosis of CHF
performed by Wang et al. (9) it was shown that the pooled sensitivities and specifi cities of common symptoms between the studies yielded only modest values for the diagnosis or exclusion of HF. The presence of PND or orthopnea in the his-tory yielded sensitivities of 41 % and 50 % , respectively, while providing more useful specifi cities of 84 % and 77 % , respec-tively. These data suggest that when used as criteria for the diagnosis of body fl uid congestion secondary to AHF, classic elements of the history may be unable to provide meaningful information to the physician.
The physical examination
The physical examination provides important information on the clinical status of the patients. Several studies have assessed the effi cacy of the physical exam in diagnosis of vol-ume overload, using decompensated HF as a positive control for the disease. Elevations in jugular venous pressure (JVP) and rales have been proven to be inconsistent diagnostic tests for HF, displaying sensitivities between 37 % and 70 % , and 24 % and 66 % , respectively, yet may still provide useful infor-mation regarding the severity of disease (8 – 11) . In patients with congestive HF studied in the RESOLVD trial, peripheral edema (Figure 1) was present in 21 % of patients with AHF and in only 10 % of patients who were free of events (12) . This suggests that clinically evident peripheral edema is only present in a minority of patients that have decompensated, and thereby does not suffi ciently refl ect the hydration status of the patient. Other studies have assessed the presence of a third heart sound (S3) as an informative fi nding in the diagno-sis of acutely decompensated HF. Unfortunately, the presence of an S3 also fails to adequately support a diagnosis of HF
Figure 1 Non-invasive methods to assess hydration status.
Authenticated | 195.62.185.194Download Date | 11/30/12 7:36 AM

Di Somma et al.: Biomarkers and bio-impedance in acute heart failure 2095
and fl uid overload, with prevalence between 36 % and 55 % in decompensated patients (9 – 12) . Overall, the reliability of the physical exam in detecting volume overload is questionable (9, 13) . Stevenson et al. (14) showed that the evaluation of all volume overload characteristics by means of the presence of a positive physical exam (including evidence of JVD, rales and/or edema) had a rather limited sensitivity (i.e., 58 % ) in patients with diagnosed HF and volume overload (PCWP > 22 mm Hg).
Standard radiography
Chest radiography is also frequently used to identify the pre-sence of volume overload in the acutely ill patient (Figure 1). Gao et al. (15) recently showed that chest radiography can be a useful tool for identifying elevated intravascular volumes in peritoneal dialysis patients before treatment, by using the cardiothoracic ratio and the vascular pedicle width. However, chest radiography lacks accuracy in the diagnosis of decom-pensated HF. In a study analyzing hospitalization rates in 86,376 HF patients from the Acute Decompensated Heart Failure Registry (ADHERE), it was found that the frequency of patient admission with a negative chest radiography was greater than that of patients with a positive chest radiography, 23.3 % vs. 13.0 % (16) . Although radiography is performed on many patients presenting to the ED with decompensated HF, it is still unclear whether the test would provide correct and appropriate diagnostic information. An important chest radio-graphy parameter is, however, the vascular pedicle width, since its evaluation shows a statistically signifi cant difference (p < 0.0004) in AHF patients as compared with healthy con-trols (6) .
Echocardiography
The European Society of Cardiology (ESC) (17) and the American College of Cardiology/American Heart Association (ACC/AHA) guidelines (18) clearly state that echocardio-graphy represents “ the single most useful diagnostic test in the evaluation of patients with HF ” . Echocardiography is a non-invasive surrogate which can provide hemodynamic data, such as stroke volume and cardiac output. The estima-tion of pulmonary artery pressure requires the presence of tricuspid valve regurgitation for mean and diastolic pres-sure as well as an accurate estimate of right atrial pressure and thus of circulatory volume content. Echocardiography also evaluates the diastolic function, and its dysfunction is classifi ed according to severity. Mild diastolic dysfunction is characterized by a decrease in early diastolic fl ow velo-city (E wave) and a greater reliance on atrial contraction (A wave) to fi ll the left ventricle (E/A < 1). Moderate diastolic dysfunction presents as increasing left atrial pressure at the onset of diastole and increases in early diastolic fl ow velocity to a level near that of normal fi lling (E/A 1 to 1.5). Severe diastolic dysfunction occurs when left atrial pressure is fur-ther elevated, so that early diastolic fl ow is very rapid and left atrial and left ventricle pressures equalize quickly during early diastole (E/A > 2). According to the American Society
of Echocardiography (ASE) guidelines, the ejection fraction (EF) measured with the 2D method is considered abnormal if < 55 % (18) . An important part of echocardiography is the evaluation of Inferior Vena Cava (IVC), because it is con-sidered as a surrogate circulatory volume (Figure 1). The use of IVC sonography has increased markedly as a method for determining volume status, especially with the advent of por-table, handheld ultrasound devices. The assessment is based on the measurement of the changes in vena cava diameter with inspiration and expiration, with the maximum IVC diameter occurring with increases in thoracic pressure during expira-tion. In a study of 35 CKD patients before and after hemodi-alysis, the IVC diameter decreased in parallel with reductions of blood volume after hemodialysis (19) . A similar study on blood donors before and after donation of 450 mL of blood also showed changes in IVC diameter measurements after volume removal. Mean changes in diameter ranged from 17.4 to 11.9 mm on expiration (p < 0.0001), and from 13.3 to 8.13 mm on inspiration (p < 0.0001) (20) . These fi ndings demon-strate an effective role for IVC sonography in the detection of mild changes in volume state. It is noteworthy, however, that echocardiographic assessment is of great utility in the evalua-tion of vascular fl uid content in patients with AHF, but cannot provide reliable information on TBW content.
Thoracic ultrasound
Thoracic ultrasound (TUS) is a relatively new imaging tech-nique used for identifying interstitial and/or alveolar edema in volume overloaded patients, especially those with CHF (Figure 1). TUS depends on the identifi cation of sonographic artifact called “ B-lines ” or lung comets. These fi ndings were fi rst described in 1997 by Lichtenstein and colleagues (21) . Liteplo et al. (22) found similar results in a study of 100 patients in the Emergency Thoracic Ultrasound in the Differentiation of the Etiology of Shortness of Breath Study (ETUDES), where it was shown that a positive TUS displayed a likelihood ratio for the diagnosis of CHF of 3.88 (99 % CI 1.55 – 9.73), whereas a negative TUS had a negative likeli-hood ratio of 0.5 (99 % CI 0.30 – 0.82). These results suggest that TUS alone is effective for diagnosing volume overload secondary to CHF in patients presenting to the ED with short-ness of breath.
Isotopic tracers of water – the gold standard for
TBW measurement
Isotopic tracers of water represent the “ gold standard ” for TBW measurement (23, 24) . These radioisotope assays uti-lize structural similarity between radioisotope (D 2 O, 3 H 2 O, H 2
18 O) and water to estimate the TBW after suffi cient time for balance. After equilibration, samples are collected and radioisotopes are measured by mass spectrometry. TBW esti-mation can then be accurately performed based on the atom percentage of the radioisotope compared with water in the sample (25) . Although the test is very effective for assessing the fl uid volume in a patient with abnormal homeostasis, it
Authenticated | 195.62.185.194Download Date | 11/30/12 7:36 AM

2096 Di Somma et al.: Biomarkers and bio-impedance in acute heart failure
is unfortunately impractical given the time (often more than 6 h) required for equilibration (26, 27) . Therefore, accurate, and even more importantly, practical measures of hydration status are still necessary for the evaluation of patients in a timely manner.
Laboratory biomarkers
The Biomarkers Defi nitions Working Group of the National Institute of Health (NIH) has reliably defi ned a biological marker, better known as “ biomarker ” , as a “ … characteris-tic that is objectively measured and evaluated as an indica-tor of normal biologic processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention ” (28) . According to this defi nition, biomarkers are now used in a kaleidoscope of clinical conditions in the ED, including diag-nosis (29) and prognostic assessment (30) of acute myocardial infarction, diagnosis of acute renal injury (31) , acute pancrea-titis (32) , pre-eclampsia (33) , stroke (34) , CHF assessment (35) and AHF (Table 1 ).
Serum blood indices are commonly used for assessment of hydration status abnormalities in AHF patients. Changes in serum sodium concentrations and their associations with dis-eases including abnormal fl uid homeostasis are accurate tools for assessing hydration status. Decreased serum osmolarity is a common fi nding in patients with CHF. In these patients, the heart becomes unable to pump blood forward effectively, thus leading to activation of neurohormonal mechanisms that result in increased serum renin activity and downstream aldosterone secretion (36) . The resultant effect is that these patients develop hyponatremia secondary to unequal and pathologic retention of water compared to salt. Hyponatremia can also be used as a metric for disease status. A study of 66 chronic CHF patients with hyponatremia showed that those with neurohormonal hyperactivation required more diuretic (i.e, furosemide) than those without the electrolyte abnorma-lity in order to recompensate (37) . Severe hyponatremia is also associated with worse prognosis in HF patients, and this parameter is currently included in the guidelines as an indica-tor of high mortality outcome for these patients (38) .
Changes in hematocrit may also be effective measures of hydration status, especially elevations with decreased blood volume. Although postural variations can affect the hemato-crit value, changes in hematocrit are expected in the context of net water gain or loss (39) . However, mild to moderate decreases in the water volume are not easily detected by blood indices (40) .
Uric acid levels > 9.8 mg/dL ( > 585 μ mol/L) have been asso-ciated with a worse outcome in HF patients. Hyperuricemia refl ects increased activity of the xanthine oxidase pathway that causes oxidative stress and impair nitric oxide (NO) pro-duction, thus worsening cardiovascular condition (41) .
The accuracy of brain natriuretic peptide (BNP) in the diagnosis, monitoring, and prognostic stratifi cation of AHF has been unquestionably established in a variety of interna-tional trials (42, 43) . BNP is the active hormone, composed of 32 amino acids, while N-Terminal pro-brain natriuretic peptide (NT-Pro BNP) is the inactive form, composed of 76
amino acids. They are both produced by the heart in response to volume and pressure overload, and their increase is propor-tional to systolic and diastolic dysfunction. In patients with acute dyspnea the cut-off value for BNP (1-32) are tradition-ally established at < 100 pg/mL (NT-Pro BNP < 400 pg/mL) to rule out HF, and > 400 pg/mL (NT-Pro BNP > 2000 pg/mL) to confi rm HF. Values between 100 and 400 pg/mL (between 400 and 2000 pg/mL for NT-Pro BNP) are considered in the so-called “ grey zone ” , and require further scrutiny (42) . Limitations in using these NPs emerge in certain conditions including renal dysfunction, obesity and atrial fi brillation. Pro-B-type natriuretic peptide 1-108 (proBNP 1-108) is the 108-amino acid prohormone that is cleaved to the 32-amino acids, biologically active brain natriuretic peptide (BNP 1-32), also known as B-type natriuretic peptide, and to the 76-amino acids, biologically inactive N-terminal pro-B-type natriuretic peptide (NTproBNP1-76). Recently, it has been shown that ProBNP (1-108) circulates in the majority of healthy humans in the general population and is a sensitive and specifi c bio-marker for the detection of systolic dysfunction. The proBNP (1-108) to NT-proBNP (1-76) ratio may provide insights into altered proBNP (1-108) processing during HF progression, providing important new insights into the biology of the BNP system (44, 45) .
The application of NPs in everyday practice carries, how-ever, undisputed advantages for improving the clinical man-agement of patients with AHF, in that they are useful aids for stratifying the risk in the ED, predicting death and rehospitali-zation, and guiding therapy (46, 47) .
The role of mid-region pro-atrial natriuretic peptide (MR-proANP) has also been investigated. In the diagnosis of AHF a cut-off of 120 pmol/L has been proven to be as accurate as BNP (1-32) (negligible accuracy difference of 0.9 % ). MR-proANP is considered particularly useful not only in obese and intermediate BNP (1-32) levels patients (48) but also in patients with impaired renal function as compared with BNP (1-32) and NT-ProBNP (1-76) (49) .
Recently, in addition to NPs, other interesting and prom-ising biomarkers have proven useful in the management of AHF, and a multimarker panel approach has been suggested to detect different causes of acute dyspnea (50) .
Latest results from the biomarkers in acute heart failure (BACH) trial support the role of several innovative biomark-ers, such as procalcitonin (PCT). PCT has been investigated for the diagnosis of pneumonia in patients with AHF. Elevated PCT ( > 0.21 ng/mL) is associated with a worse outcome when antibiotic therapy is not established (p = 0.046), while a low PCT value (i.e., < 0.05 ng/mL) is associated with a better out-come if not treated with antibiotics (p = 0.049) (51) .
Another interesting result from the 15-center BACH trial defi nes the mid-region pro-adrenomedullin (MR-proADM), the precursor of the hypotensive adrenomedullin, an accurate 14-day mortality predictor. This is also confi rmed by the area under the curve (AUC) in receiver operating characteristics (ROC) curve of MR-proADM (0.742) which is higher than that of BNP (0.484) and NT-proBNP (0.586) (52) . Another promising biomarker is copeptin, the C-terminal part of the vasopressin pro-hormone. It is an independent predictor for
Authenticated | 195.62.185.194Download Date | 11/30/12 7:36 AM

Di Somma et al.: Biomarkers and bio-impedance in acute heart failure 2097
Table 1 Summary of the main utility biomarkers in HF.
Biomarkers Diagnosis and physiopathology Adverse prognosis
Serum sodium (n.v.: 136 – 145 mmol/L) AHF- RAA activation
< 120 mmol/L
Serum creatinine (n.v.: 0.5 – 1.5 mg/dL) Cardiorenal syndrome
> 150 μ mol/L > 1.5 mg/dL
Serum uric acid (n.v.: m 3.2 – 8.1 mg/100 mL; 2.2 – 7.1 mg/100 mL) AHF- oxidative stress
> 9.8 mg/dL
NPs (blood and serum): • BNP • NT-proBNP • MR-proANP
v.n.: HF cut-off: < 100 pg/mL; > 400 pg/mL < 400 pg/mL; > 2000 pg/mL < 120 pmol/L; > 120 pmol/L AHF: left ventricle volume and pressure overload (heart muscle stretching)
> 1000 pg/mL > 5000 pg/mL –
ST2 (serum) (n.v.: 1.75 – 34.3 U/mL) AHF-overload
> 10 ng/mL
PCT (serum) (cut-off: 0.05 ng/mL) Infection in AHF
0.05 – 0.5 ng/mL local infection 0.5 – 2 ng/mL systemic infection 2 – 10 ng/mL SIRS – sepsis > 10 ng/mL sepsis
NGAL (serum and urine) (cut-off: 150 ng/mL serum a ; 130 ng/mL urine a ) Cardiorenal syndrome
> 100 ng/mL a
Copeptin (serum) (median 3.7 pmol/L a ) AHF-vascular alterations
> 54.2 pmol/L a
MR-proADM (serum) AHF-vascular alterations > 2.15 nmol/L a ADMA (serum) AHF-oxidative stress a
a Different trials use different cut-off. ADMA, asymmetric dimethylarginine; AHF, acute heart failure; BNP, brain natriuretic peptide; MR-proADM, mid-region pro-adrenomedulin; MR-proANP, mid-region pro-atrial natriuretic peptide; NGAL, neutrophil gelatinase-associated lipocalin; NT-proBNP, N-terminal pro-brain natriuretic peptide; PCT, procalcitonin; RAA, renine-angiotensin-aldosterone.
short-term (30 days) mortality, especially in patients with AHF (p < 0.0001). The prognostic value of copeptin ( > 54.2 pmol/L) has been evaluated alone and in association with NT-proBNP and BNP, and their AUC were 0.83, 0.76 and 0.63, respectively (53) . Finally, a subanalysis of the BACH trial confi rmed that MR-proADM and copeptin in combina-tion have the best 14-day mortality prediction (AUC = 0.818), compared with all other markers (52) .
A new and still not adequately investigated biomarker is soluble ST2, which is involved in cardiac remodelling and overload (54) . An increase in ST2 above 10 ng/mL is consid-ered a predictor of mortality in patients with AHF (p < 0.001) (55) .
Due to the known, complex and multifaceted interplay between heart and kidneys, AHF is often complicated by acute kidney injury (AKI) in critical patients. This circum-stance defi nes a high mortality condition, called cardiorenal syndrome (56) . Classically, an increase of serum creatinine ( > 150 μ mol/L) (16) is used to defi ne renal injury, but it is only marginally associated with the outcome (AUC of 0.57) (57) . Neutrophil gelatinase-associated lipocalin (NGAL) is a new biomarker that might help risk stratifi cation in AHF patients. Although not absolutely specifi c for AKI (it is also produced and released by neutrophils) (58) , it is still an early marker of AKI. A discharge value of NGAL > 100 ng/mL, combined with BNP values or even measured alone, has been proven to be a powerful predictor of 30-day adverse outcomes (57) . Finally, a preliminary study has shown that increased plasma
levels of asymmetric dimethylarginine (ADMA) are strong and independent predictor of short- and long-term mortality in AHF patients (NYHA Class III/IV) with reduced EF (59) .
Bio-impedance analysis (BIA)
Bio-electrical impedance is the term used to describe the response of a living organism to an externally applied elec-tric current by surface electrodes. It measures the opposition to the fl ow of electric current throughout the tissues. Electric current is administered by surface electrodes that need high current (800 μA) and high voltage to decrease the instabil-ity related to cutaneous impedance (10,000 Ω /cm 2 ) (60) . This impedance value, termed electrical impedance (Z), consists of two components, resistance (R) and reactance (Xc). In terms of impedance, the human body can be schematically consid-ered as a system composed of several different conductors in parallel, each of which opposes the passage of an alternating current, which passes through two pathways: extracellular tis-sue and intracellular membranes. Since extracellular (ECW) and intracellular water (ICW) compartments contain ions, they are electrically conductive. Thus, estimations of fl uid volume can be based on their impedance to electrical fl ow as cell membranes may act as capacitors. The resistivity of ECW ionic composition is close to that of saline, but the ICW ionic composition depends on the type of cell and, as a result, resistivity cannot be measured directly. For technical reasons,
Authenticated | 195.62.185.194Download Date | 11/30/12 7:36 AM

2098 Di Somma et al.: Biomarkers and bio-impedance in acute heart failure
impedance meters using surface electrodes are limited to a frequency range of 5 – 1000 kHz, and the ECW and the TBW) resistance must be calculated by extrapolation as proposed by the Cole-Cole model (61) .
In bio-impedance analysis (BIA) the angular component of the polar coordinate representation, called the phase angle (PA), is assessed. The principle of measurement is based upon the fact that the condensers in the alternating current circuit lead to a time delay Δ t: the current maxi-mum is in advance of the voltage maximum. PA represents the measurement of this time delay between the periodic signals of current and voltage, which vary sinusoidally at the same frequency. It is calculated from resistance and reactance according to the formula: PA = arc-tangent reac-tance/resistance × 180 ° / π . The PA might be an indicator of cell membrane integrity as well as distribution of ICW and ECW, and it can also be used to assess total cell mass (62) . Cox multivariate models have also been used to estab-lish that PA may be considered a signifi cant and indepen-dent predictor of mortality in patients with liver cirrhosis (p < 0.01) (63) .
However, it is important to consider that impedance mea-surements are rooted in an approximation of the human body as a sum of fi ve interconnected cylinders (limbs and trunk). This approximation is calculated from the length and perim-eters of the limbs and the trunk through a dimensionless shape factor (Kb) in the resistance – volume relationship for a single cylinder. A value of 4.3 for Kb has been established from statistical anatomical measurements in adults (64) . It is also noteworthy that there are several factors impacting BIA including height, weight, position of the body and limbs, intense physical activity before BIA measurements, infection, dermatological conditions, ambient temperature and non-ad-herence of electrodes (65 – 68) .
In 1871, Thomasset et al. (69) performed the initial study assessing the electrical properties of tissues to measure imped-ance using two frequencies of 1 kHz and 100 kHz through two subcutaneously inserted needles. Using the Cole-Cole model, he could then estimate the ECW and TBW volumes. Since then, tetra-polar BIA has been widely investigated in medical research as a tool for assessing body composition. Its use has gradually expanded from estimation of body composition in healthy individuals to embrace the assessment of fl uid vol-ume and distribution in various patient populations.
Single-frequency whole-body BIA (SF-WBIA) and bio-
electrical impedance spectroscopy (BIS)
The whole-body BIA (WBIA) uses four surface electrodes, two placed on the wrist and two on the ankle, at the distal metacarpals and metatarsals, respectively, with the subject supine. A low-level alternating current is administered at either single (50 kHz) or multiple frequencies (e.g., 1, 5, 50, 200, 500 and 2000 kHz), and then whole-body Z, R and Xc are measured. These variables are adjusted for height and then combined with various physical and demographic vari-ables (body weight, age, gender, etc), into regression models to predict volume status.
In 1983, Nyboer et al. (70) used the four-surface electrode WBIA technique, initially presented by Hoffer in 1969, to assess body composition in 144 subjects. A signifi cant cor-relation was observed between body fat mass (r = 0.860), TBW (r = 0.947) and lean body weight (r = 0.934) with the whole-body impedance and the hydrostatic weighing, which is another method for measuring the body mass density. It is based on Archimedes ’ principle and is performed during forced exhalation with residual lung volume (70) . By 1986, the WBIA was accurately described and validated by Kushner (71) , for assessing TBW by BIA and deuterium-isotope dilu-tion in 58 subjects. He found a signifi cant correlation (r = 0.99) between BIA, weight and deuterium-dilution space.
In 1990, BIS was introduced by Xitron as a new method to measure both ECW and ICW volumes using Hanai ’ s mix-ture conductivity theory for concentrated disperse systems in evaluating dielectric dispersion due to interfacial polarization (72, 73) .
The BIS device, which is able to assess TBW and differen-tiate between ECW and ICW (TBW-ICW), uses low and high frequencies of 5 kHz – 2 MHz and extrapolates resistance val-ues of extracellular and intracellular fl uids, respectively, with the Cole-Cole model. From these resistance values, extra- and intra-cellular resistivities are derived with the Hanai model.
There is now consolidated evidence that the whole-body technique, as compared with reference methods, can lead to inaccurate assessment of body composition in some circum-stances. In 54 patients with end stage renal disease, TBW measurements derived by deuterium dilution and WBIA showed no signifi cant difference (mean difference = – 1.221 L, p = 0.12) between the two methods in estimating fl uid status. Unfortunately, WBIA lacked consistency across all patient populations and signifi cantly overestimated fl uid status in obese patients (mean = – 6.789 L, p = 0.001) (74) . In 2003, Sun et al. developed a gender-specifi c, age- and race-combined equation with the use of a multi-component model including densitometry, isotope dilution and dual-X-ray absorptiometry (DXA). A sample of 1829 patients aged from 12 to 94 years old were studied and their body composition was assessed by SF-WBIA. The fi nal equation, validated by prediction of sum of squares (PRESS) statistics, showed the utility of WBIA in epidemiologic studies (75) .
Segmental BIA (SBIA)
Segmental BIA (SBIA) has been developed as a practical alternative to WBIA. It is a four-electrode bio-impedance device with contact (tactile) electrodes that measure imped-ance in the upper (arm-to-arm) or the lower (leg-to-leg) body of a standing subject (76 – 79) . The main assumptions of this measurement technique are that conductor volume is equally distributed in the upper and lower body, segmental imped-ance values are proportional to whole-body impedance and whole-body resistance can be derived by the sum of segmen-tal resistances (80, 81) . Interestingly, the segmental imped-ance technique may be used for personal monitoring of body composition because it does not require the presence of an operator. Another type of segmental bio-electrical impedance
Authenticated | 195.62.185.194Download Date | 11/30/12 7:36 AM

Di Somma et al.: Biomarkers and bio-impedance in acute heart failure 2099
uses eight electrodes, four of which are placed in the handles of the machine (in contact with the thumbs and palms) and the other four in the foot scale pads, in contact with the balls of feet and heels. These machines operate at either single or multiple frequencies while the subject stands. A recent study on 112 AHF patients used a segmental multi-frequency bio-electrical analysis to estimate the 6-month prognostic value of pre-discharge edema index, a derived surrogate for hydration status, and established that an edema index > 0.390 (i.e., the cut-off value) represents a signifi cant HF-related predictor of re-hospitalization (p = 0.04) (82) .
WBIA vs. SBIA
The clinical application of segmental BIA was assessed for determining fl uid accumulation in 30 patients undergoing abdominal surgery. ECW distribution changes ( Δ ECW) were monitored preoperatively (before the induction of anesthesia) and postoperatively (after recovery from anesthesia). The Δ ECW was estimated by the multi-frequency whole-body device and as a sum of fi ve body segments. The most sig-nifi cant resistance decrease was found in the trunk where the fl uid composition contributes minimally to the whole body resistance. It was thus concluded that segmental multi-fre-quency bio-electrical impedance analysis provides Δ ECW assessment better then the whole-body technique in patients with non-homogeneous fl uid distribution (83) . Although BIA cannot be considered as an individual reference tool, newer studies have warranted its broader application in combination with other techniques.
Bio-electrical impedance vector analysis (BIVA)
BIVA can be considered an integrated component of BIA measurement, and is a simple and quick method for assessing fl uid status and body cell mass (84) . It can also be used as a quality control measure for correct analysis of BIA results (85) .
BIVA is a non-invasive technique to estimate body com-position by bio-electrical impedance measurements, R, Xc and Z (86, 87) . All biological structures have a specifi c resis-tance, defi ned as the strength of opposition by a tissue to the electric current fl ow (7) . Fat-free tissues and fl uids are good conductors because they offer a low resistance to the electric current fl ow, while bone and fat tissues are bad conductors because they are electrically resistant. Therefore, the resis-tance is inversely related with the TBW, thus representing an indirect measure of the amount of body fl uid. The measured reactance is dependent upon the presence of inductors and/or electrolytic capacitors. Since all cell membranes act like a small capacitor, reactance can be considered as an indirect measure of cell membrane activity and integrity, and is pro-portional to body mass (66, 88) .
The BIVA technique was developed at the University of Padua (Italy) (7) . The machine uses an alternating current fl ux of 800 μ A and an operating frequency of 50 kHz. The results are visualized in two ways, as a vector or as a BIVA-
derived hydration percentage. The fi rst method includes a direct impedance plot which measures R and Xc, as a bi-vari-ate vector in a normogram (85) . Reference values adjusted for age, body mass index (BMI), and gender are plotted as so-called tolerance ellipses in the same coordinate system. Three tolerance ellipses are distinguished, corresponding to the 50th, 75th and 95th vector percentile of the healthy refer-ence population (86) . The major axis of this ellipse indexes hydration status and the minor axis refl ects tissue mass. The second method involves a scale called the Hydrograph (or Hydrogram), which expresses the state of hydration as a percentage. This value is calculated by an independently determined equation that uses the two components of BIVA, R and Xc. A normal value is 73.3 % with tolerance between 72.7 % and 74.3 % , corresponding to the 50th percentile (7) (Figure 1).
Regarding interpretation of values, the length of Z vector is inversely related to fl uid volume, whereas the PA offers insight into the relative distribution of fl uids. A fundamen-tal outcome of several studies is the delineation of the 75 % tolerance ellipse as the indicator of the boundary of normal tissue hydration. Vectors outside the upper pole of the 75 % ellipse indicate dehydration, whereas others outside the 75 % confi dence ellipse of the lower pole are characteristic of fl uid overload or overhydration. Thus, short vectors with a small PA are associated with edema, whereas longer ones with an increased PA indicate dehydration (86, 89, 90) . Moreover, vectors above or below the minor axis (meaning upper-left or lower right half of ellipses) are associated with more or less cell mass in soft tissue, respectively, with extremes along the minor axis. As previously discussed, the normal BIVA-derived hydration values for the hydrograph are comprised between 72.7 % and 74.3 % , values above or below such rela-tive thresholds indicate a state of hyperhydration (wet) and dehydration (dry) (91) . These two classes can be further sub-divided into mild, moderate or severe volume abnormalities (92) .
The BIVA technique is very handy and can be used at the bedside, with the patient supine with inferior limbs at 45 ° and superior limbs abducted at 30 ° to avoid skin contacts with the trunk (66) . Four skin electrodes are applied, two on the wrist and two on the ipsilateral ankle. A minimal inter-electrode distance of 5 cm has been recommended to prevent interac-tion between electrodes. The subject is laid recumbent on a non-conductive surface. Free fl uid in thorax and abdomen (lung congestion, pleural effusion, ascites, urine, food) does not affect the impedance values measured by this technique (6) .
Despite being relatively new, BIVA is becoming recog-nized as a superior method for TBW content assessment (93) . Clinical studies have been carried out in hospitalized patients with severe renal diseases to assess the utility of BIVA in assessing volume status. Studies involving uremic patients, compared to healthy controls, showed signifi cantly shorter vectors with smaller PAs. As discussed above, shorter vectors (low impedance) are associated with hyperhydration. These vectors then lengthened after dialysis, showing the ability of BIVA to detect signifi cant changes of fl uid status after
Authenticated | 195.62.185.194Download Date | 11/30/12 7:36 AM

2100 Di Somma et al.: Biomarkers and bio-impedance in acute heart failure
dialysis. Changes in the volume of fl uid removed signifi cantly correlated with changes in vector components (p < 0.001 in men, p = 0.03 in women). Vectors of unstable (e.g., adverse outcomes) compared to stable hemodialysis patients were sig-nifi cantly different. It was also found that vectors of unstable patients were longer with smaller PAs, and these differences persisted after hemodialysis (89) . Similar fi ndings were found in patients treated with peritoneal dialysis, before and after fl uid removal (86) .
New application fi elds are emerging in critical care. In intensive care unit patients, the central venous pressure (CVP) was correlated with impedance measured by BIVA. CVP values are signifi cantly and inversely correlated with indi-vidual impedance vector components (r 2 = 0.28 and 0.27 with resistance and reactance, respectively), and with both vector components together (r 2 = 0.31). Specifi cally, CVP values > 12 mm Hg were associated with shorter impedance vectors (out-side the lower pole of the 75 % reference ellipse) in 93 % of patients, thus indicating fl uid overload. Conversely, CVP val-ues < 3 mm Hg were associated with long impedance vectors (outside the upper pole of the 75 % reference ellipse) in only 10 % of patients, indicating tissue dehydration. The progres-sive increase of CVP values was associated with shorter and down-sloping impedance vectors on the R-Xc graph (94) .
The role of BIVA coupled with TUS has shown its effec-tiveness in discriminating cardiac and non-cardiac acute dyspnea patients presenting in ED (69 % sensitivity, 79 % specifi city) (95) .
Future directions in managing AHF patients
using biomarkers plus BIVA
The BIVA evaluation is an appealing perspective when applied in patients in the acute setting with congestive HF because of specifi c fl uid overload. A study by Di Somma et al. (6) , shows that BIVA data in decompensated AHF patients at admission to the ED are statistically different as compared with controls (p < 0.0007). AHF patients had a signifi cantly higher value of hydration status (77 ± 4) as compared with controls (73 ± 2). Sequential BIVA measurements in AHF patients showed reduc-tion of congestion due to diuretic treatment. A signifi cant corre-lation with events (death or re-hospitalization) at 3 months was also observed in patients with average hydration values > 80 % . It was also demonstrated that combined use of BIVA and BNP may improve the management of AHF patients in ED when compared to BNP alone, thus allowing a faster and much more accurate triage. BIVA helped distinguish cardiogenic dysp-nea from non-cardiogenic causes and – in combination with BNP – was also useful for management of AHF patients, since both measures were helpful to guide emergency physician ’ s decisions about diuretic therapy (e.g., preventing overuse).
Valle et al. (91) found that the combination of BNP and BIVA measurements could prevent unnecessary aggressive diuretic therapy, thereby reducing the level of renal compli-cations. BIVA-BNP guided management during hospitaliza-tion for HF was associated with lower events after discharge, independent of other prognostic variables (91) .
The evaluation of total body fl uid has a great utility also in patients with cardiorenal syndrome, and its use in combina-tion with other parameters (e.g., in a multimarker approach) has been proposed as a new model of management of ED patients with cardiorenal syndrome (96) .
According to the large number of studies available in the scientifi c literature, the role of impedance is becoming more and more predominant for the assessment of hydration sta-tus. Characteristics, such as quick and simple use, non-inva-siveness and low cost would make this device appealing and potentially useful in a kaleidoscope of medical fi elds. BIVA seems to be more accurate and more reliable when compared with other impedance techniques (Figure 1). Further tri-als with larger patient populations are obviously needed to express a defi nitive consensus on the clinical effectiveness of BIVA, as well as for identifying those clinical settings where it can be more advantageous.
The use of BIVA in guiding the treatment of various disease states has not been adequately studied. It would be interesting to standardize BIVA employment in AHF patients, in combi-nation with biomarkers, to guide a proper and correct diuretic therapy. Preliminary data from studies that have monitored the variations of BIVA values in volume overloaded patients has already shown its utility in guiding diuretic treatment, but more clinical evidence is necessary to create BIVA/diuretic guidelines. Another promising application is related to the emerging role of ultrafi ltration in unloading CHF patients that do not benefi t from diuretic therapy. Regular use of BIVA plus NPs might assist physicians to decide the amount of water to remove, thus avoiding harmful consequences. Due to its quick and easy use, BIVA should also be tested for its effi cacy in primary care setting as a means for monitoring congested patients. This application could help primary care physicians in the management of these patients, since exacerbations may be detected sooner, avoiding severe worsening that may require hospitalization.
BIVA alone is probably not the defi nitive answer to all challenging questions about hydration status, but it seems to be a useful and promising device for everyday use, especially when coupled with biomarker measurement, because it is accurate, non-invasive, cheap and easy to use in combination with other techniques.
Confl ict of interest statement
Authors ’ confl ict of interest disclosure: The authors stated that there are no confl icts of interest regarding the publication of this article. Research funding: None declared. Employment or leadership: None declared. Honorarium: None declared.
References
1. Di Somma S, Lukaski HC, Codognotto M, Peacock WF, Fiorini F, Aspromonte N, et al. Consensus paper on the use of BIVA (bio-electrical impedance vector analisis) in medicine for the manage-ment of body hydration. Emerg Care J 2011;4:6 – 14.
Authenticated | 195.62.185.194Download Date | 11/30/12 7:36 AM

Di Somma et al.: Biomarkers and bio-impedance in acute heart failure 2101
2. Verbalis JG. Disorders of body water homeostasis. Best Pract Res Clin Endocrinol Metab 2003;17:472 – 503.
3. Peacock FW, Karina M, Soto MS. Current technique of fl uid sta-tus assessment. Congest Heart Fail 2010;16:45 – 51.
4. Di Somma S, Gori CS, Grandi T, Risicato M, Salvatori E. Fluid assessment and management in emergency department. Contrib Nephrol 2010;164:227 – 36.
5. Clerico A, Vittorini S, Passino C. Measurement of the pro-hormone of brain type natriuretic peptide (proBNP): method-ological considerations and pathophysiological relevance. Clin Chem Lab Med 2011;49:1949 – 54.
6. Di Somma S, De Berardinis B, Bongiovanni C, Marino R, Ferri E, Alfei B. Use of BNP and bioimpedance to drive therapy in heart failure patients. Congest Heart Fail 2010;(Suppl 1):S56 – 61.
7. Marino R, Magrini L, Ferri E, Gagliano G, Di Somma S. B-Type natriuretic peptide and non-invasive haemodynamics and hydra-tion assessment in the management of patients with acute heart failure in emergency department. High Blood Press Cardiovasc Prev 2010;17:219 – 25.
8. Butman SM, Ewy GA, Standen JR, Kern KB, Hahn E. Bedside cardiovasculer examination in patients with severe chronic heart failure: importance of rest or inducible jugular venous distention. J Am Coll Cardiol 1993;22:968 – 74.
9. Wang CS, Fitzgerald JM, Shulzer M, Mak E, Ayas NT. Does this dyspneic patient in the emergency department have congestive heart failure ? J Am Med Assoc 2005;294:1944 – 56.
10. Chakko S, Woska D, Martinez H, De Marchena E, Futterman L, Kessler KM, et al. Clinical, radiographic, and haemodynamic correlations in chronic congestive heart failure. Am J Med 1991;90:353 – 9.
11. Drazner MH, Rame JE, Stevenson LW, Dries DL. Prognostic importance ef elevated jugular venous pressure and a third heart sound in patients with heart failure. N Engl J Med 2001;345:574 – 81.
12. Tsuyuki RT, McKelvie RS, Arnold JM, Avezum AJ, Barretto AC, Carvalho AC, et al. Acute precipitants of congestive heart failure exacerbations. Arch Intern Med 2001;161:2337 – 42.
13. Marantz PR, Kaplan MC, Alderman MH. Clinical diagnosis of congestive heart failure in patients with acute dyspnea. Chest 1990;97:776 – 81.
14. Stevenson LW, Perloff JK. The limited reliability of physical sign for estimating hemodynamics in chronic heart failure. J Am Med Assoc 1989;261:884 – 8.
15. Gao N, Kwan BC, Chow KM, Chung KY, Leung CB, Li PK, et al. Measurements on the routine chest radiograph as prognos-tic markers in Chinese peritoneal dialysis patients. Clin Nephrol 2011;76:16 – 22.
16. Collins SP, Lindsell CJ, Storrow AB, Abraham WT. Prevalence of negative chest radiography results in the emergency depart-ment patient with decompensated heart failure. Ann Emerg Med 2006;47:13 – 8.
17. Dickstein K, Choen-Solal A, Philippatos G, McMurray J, Ponikowski P, Poole-Wilson PA. ESC guidelines for the diagno-sis and treatment of acute and chronic heart failure 2008. Eur J Heart Fail 2008;10:933 – 89.
18. Kirkpatrick JN, Vannan MA, Narula J, Lang RM. Echocardi-graphy in heart failure: applications, utility and new horizons. J Am Coll Cardiol 2007;50:381 – 96.
19. Katzarski KS, Nisell J, Randmaa I, Danielsson A, Freyschuss U, Bergstr ö m J. A critical evaluation of ultrasound measurement of inferior vena cava diameter in assessing dry weight in normoten-sive and hypertensive hemodialysis patients. Am J Kidney Dis 1997;30:459 – 65.
20. Lyon M, Blaivas M, Brannam L. Sonographic measurement of inferior vena cava as a marker of blood loss. Am J Emerg Med 2005;23:45 – 50.
21. Lichtenstein D, M é zi è re G, Biderman P, Gepner A, Barr é O. The comet tail artifact. An ultrasound sign of alveolar-interstitial syn-drome. Am J Respir Crit Care Med 1997;156:1640 – 6.
22. Liteplo AS, Marill KA, Villen T, Miller RM, Murray AF, Croft PE, et al. Emergency thoracic ultrasound in the differentiaion of the etiology of shortness of breath (ETUDES): sonographic B-lines and N-terminal Pro-brain-type natriuretic peptide in diagnosing congestive heart failure. Acad Emerg Med 2009;16:201 – 10.
23. Ritz P. Bioelectrical impedance analysis estimation of water com-partments in elderly disease patients: the source study. J Gerontol A Biol Sci Med Sci 2001;56:M344 – 8.
24. Cheuvront S. Hydration assessment of athletes. Sports Sci Exchange 2005;18.
25. Schoeller DA, van Santen E, Peterson DW, Dietz W, Jaspan J, Klein PD. Total body water measurement in humans with 18O and 2H labeled water. Am J Clin Nutr 1980;33:2686 – 93.
26. Armstrong LE. Assessing hydration status: the elusive gold stan-dard. J Am Coll Nutr 2007;26:575S – 84S.
27. Colley RC, Byrne NM, Hills AP. Implications of the variability in time to isotopic equilibrium in the deuterium dilution tech-nique. Eur J Clin Nutr 2007;61:1250 – 5.
28. Biomarkers-Defi nitions-Working-Group. Biomarkers and surro-gate endpoints: preferred defi nitions and conceptual framework. Clin Pharmacol Ther 2001;69:89 – 95.
29. Christ M, Bertsch T, Popp S, Bahrmann P, Heppner HJ, M ü ller C. High-sensitivity troponin assays in the evaluation of patients with acute chest pain in the emergency department. Clin Chem Lab Med 2011;49:1955 – 63.
30. Lippi G, Plebani M, Di Somma S, Monzani V, Tubaro M, Volpe M. Considerations for early acute myocardial infarction rule-out for emergency department chest pain patients: the case of copep-tin. Clin Chem Lab Med 2012;50:243 – 53.
31. Soni SS, Pophale R, Ronco C. New biomarkers for acute renal injury. Clin Chem Lab Med 2011;49:1257 – 63.
32. Lippi G, Valentino M, Cervellin G. Laboratory diagnosis of acute pancreatitis: in search of the Holy Grail. Crit Rev Clin Lab Sci 2012;49:18 – 31.
33. Can M, Sancar E, Harma M, Guven B, Mungan G, Acikgoz S. Infl ammatory markers in preeclamptic patients. Clin Chem Lab Med 2011;49:1469 – 72.
34. Cho SY, Park TS, Lee HJ, Lee WI, Suh JT. Functional assay or antigen test for protein C and protein S in ischemic stroke: which shows the greatest change ? Clin Chem Lab Med 2011;49:1919 – 20.
35. Jungbauer C, Riedlinger J, Buchner S, Birner C, Resch M, Lubnow M. High-sensitive troponin T in chronic heart failure correlates with severity of symptoms, left ventricular dysfunction and prognosis independently from N-terminal pro-B-type natri-natriuretic peptide. Clin Chem Lab Med 2011;49:1899 – 906.
36. Lilly LS, Dzau VJ, Williams GH, Rydstedt L, Hollenberg NK. Hyponatremia in congestive heart failure: implication for neurohumoral activation and responses to orthostasis. J Clin Endocrinol Metab 1984;59:924 – 30.
37. Mettauer B, Rouleau JL, Bichet D, Juneau C, Kortas C, Barjon JN, et al. Sodium and water excretion abnomalities in congestive heart failure. Ann Intern Med 1986;105:161 – 7.
38. Packer M, Lee WH, Kessler PD, Gottlieb SS, Bernstein JL, Kukin ML. Role of neurohormonal mechanisms in determining survival in patients with severe chronic heart failure. Circulation 1987;75:IV80 – 92.
Authenticated | 195.62.185.194Download Date | 11/30/12 7:36 AM

2102 Di Somma et al.: Biomarkers and bio-impedance in acute heart failure
39. Harrison MH. Effects of thermal stress and exercise on blood volume in humans. Physiol Rev 1985;65:149 – 209.
40. Armstrong LE, Soto JA, Hacker FT, Casa DJ, Kavouras SA, Maresh CM. Urinary indices during dehydration, exercise and rehydration. Int J Sport Nutr 1998;8:345 – 55.
41. Hare JM, Johnson RJ. Uric acid predicts clinical outcomes in heart failure. Circulation 2003;107:1951 – 3.
42. Maisel AS, Nakao K, Ponikowski P, Peacock WF, Yoshimura M, Suzuki T, et al. Japanese-Western consensus meeting on bio-markers. Int Heart J 2011;53:253 – 65.
43. Brunetti M, Pregno S, Sch ü nemann H, Plebani M, Trenti T. Economic evidence in decision-making process in laboratory medicine. Clin Chem Lab Med 2011;49:617 – 21.
44. Macheret F, Boerrigter G, McKie P. Pro-B-type natriuretic pep-tide 1-108 circulates in the general community. Plasma determi-nants and detection of left ventricular dysfunction. J Am Coll Cardiol 2011;57:1386 – 95.
45. Emdin M, Passino C, Clerico A. Natriuretic peptide assays revisited. Do we need pro-B-type natriuretic peptide ? J Am Coll Cardiol 2011;57:1396 – 8.
46. Daniels LB, Maisel AS. Natriuretic peptides. J Am Coll Cardiol 2007;18;50:2357 – 68.
47. Maisel A, Mueller C, Adams K Jr, Anker SD, Aspromonte N, Cleland JG, et al. State of the art: using natriuretic peptide levels in clinical practice. Eur J Heart Fail 2008;10:824 – 9.
48. Maisel A, Mueller C, Nowak R, Peacock WF, Landsberg JW, Ponikowski P, et al. Mid-region pro-hormone markers for diag-nosis and prognosis in acute dyspnea: results from the BACH (biomarkers in acute heart failure) trial. J Am Coll Cardiol 2010;55:2062 – 76.
49. Daniels LB, Clopton P, Potocki M, Mueller C, McCors J, Richhards M, et al. Infl uence of age, race, sex, and body mass index on interpretation of midregional pro atrial natriuretic peptide for the diagnosis of acute heart failure: results from the BACH multinational study. Eur J Heart Fail 2010;14:22 – 31.
50. Gori CS, Magrini L, Travaglino F, Di Somma S. Role of bio-markers in patients with dyspnea. Eur Rev Med Pharmacol Sci 2011;15:229 – 40.
51. Maisel AS, Neath SX, Landsberg J, Mueller C, Nowak RM, Peacock WF, et al. Use of procalcitonin for the diagnosis of pneumonia in patients with a chief complaint of dyspnoea: results from the BACH (biomarkers in acute heart failure) trial. Eur J Heart Fail 2012;14:278 – 86.
52. Peacock WF, Nowak R, Christenson R, Di Somma S, Neath SX, Hartmann O, et al. Short-term mortality risk in emergency depart-ment acute heart failure. Acad Emerg Med 2011;18:947 – 58.
53. Potocki M, Breidthardt T, Mueller A, Reichlin T, Socrates T, Arenja N, et al. Copeptin and risk stratifi cation in patients with acute dyspnea. Crit Care 2010;14:R213.
54. Alsous SJ, Richards AM, Troughton R, Than M. ST2 as diagnos-tic and prognostic utility for all cause mortality and heart failure patients presenting to emergency department with chest pain. J Cardiac Fail 2012;18:304 – 10.
55. Pascual-Figal DA, Manzano-Fern á ndez S, Boronat M, Casas T, Garrido IP, Bonaque JC, et al. Soluble ST2, high-sensitivity troponin T- and N-terminal pro-B-type natriuretic peptide: com-plementary role for risk stratifi cation in acutely decompensated heart failure. Eur J Heart Fail 2011;13:718 – 25.
56. Cruz DN, Fard A, Clementi A, Ronco C, Maisel A. Role of bio-markers in the diagnosis and management of cardio-renal syn-dromes. Semin Nephrol 2012;32:79 – 92.
57. Maisel AS, Mueller C, Fitzgerald R, Brikhan R, Hiestand BC, Iqbal N, et al. Prognostic utility of plasma neutrophil gelati-naseassociated lipocalin in patients with acute heart failure: The
NGAL evaluation along with B-type natriuretic peptide in acutely decompensated heart failure (GALLANT) trial. Eur J Heart Fail 2011;13:846 – 51.
58. Lippi G, Cervellin G. Neutrophil gelatinase-associated lipocalin: a more specifi c assay is needed for diagnosing renal injury. Clin Chim Acta 2012;413:1160 – 1.
59. Zairis MN, Patsourakos NG, Tsiaousis GZ, Theodossis-Georgilas A, Melidonis A, Makrygiannis SS, et al. Plasma asymmetric dim-ethylarginine and mortality in patients with acute decompensa-tion of chronic heart failure. Heart 2012;98:860 – 4.
60. Kyle UG, Bosaeus I, De Lorenzo AD, Deurenberg P, Elia M, G ó mez JM, et al. Bioelectrical impedance analysis part I: review of principles and methods. Clin Nutr 2004;23:1226 – 43.
61. Cole KS. Membranes, ions and impulses: a chapter of classi-cal biophysics. Berkeley, CA: University of California Press, 1972:1.
62. Barbosa-Silva MC, Barros AJ, Wang J, Heymsfi eld SB, Pierson RN. Bioelectrical impedance analysis: population ref-erence values for phase angle by age and sex. Am J Clin Nutr 2005;82:49 – 52.
63. Selberg O, Selberg D. Norms and correlates of bioimped-ance phase angle in healthy human subjects, hospitalized patients, and patients with liver cirrhosis. Eur J Appl Physiol 2002;86:509 – 16.
64. Van Loan MD, Withers PO, Matthie JR, Mayclin PL. Use of bio-impedance spectroscopy to determine extracellular fl uid, intrac-ellular fl uid, total body water and fat-free mass. Basic Life Sci 1993;60:67 – 70.
65. Matthie R. Bioimpedence measurements of human body com-position: critical analysis and outlook. Expert Rev Med Devices 2008;5:239 – 61.
66. Kushner RF. Bioelectrical impedance analysis: a review of prin-ciples and applications. J Am Coll Nutr 1992;11:119 – 209.
67. Dehghar M, Merchant AT. Is bioelectrical impedance accurate for use in large epidemiological studies ? Nutr J 2008;7:26.
68. Buchholz AC, Bartok C, Shoeller DA. The validity of bioelectri-cal impedance models in clinical populations. Nutr Clin Pract 2004;19:433 – 46.
69. Thomasset A. Bio-electrical properties of tissue impedance mea-surements. Lyon Med 1963;209:1325 – 52.
70. Nyboer J, Liedtke RJ, Reid KA, Gessert WA. Nontraumatic electrical detection of total body water and density in man. Med Jadertina 1983;15:381 – 4.
71. Kushner RF, Schoeller DA. Estimation of total body water by bio-electrical impedance analysis. Am J Clin Nutr 1986;44:417 – 24.
72. Matthie JR, Withers PO, Van Loan MD, Mayclin PL. Develop-ment of commercial complex bio-impedance spectroscopic system for determining intracellular and extracellular water vol-umes. Proceedings of the 8th international conference on electri-cal bio-impedance 1992;203 – 5.
73. Hanai T. Electrical properties of emulsions. In: Sherman PH, edi-tor. Emulsion Science. London: Academic, 1968:354 – 477.
74. Cooper BA, Aslani A, Ryan M. Comparing different methods of assessing body composition in end-stage renal failure. Kidney Int 2000;58:408 – 16.
75. Sun SS, Chumlea WC, Heymsfi eld SB, Lukaski HC, Schoeller D, Friedl K, et al. Development of bioelectrical impedance pre-diction equations for body composition with the use of a multi-component model for use in epidemiologic surveys. Am J Clin Nutr 2003;77:331 – 40.
76. Nunez C, Gallagher D, Grammes J, Baumgartner RN, Ross R, Wang Z, et al. Bioimpedance analysis: potential for measur-ing lower limb skeletal muscle mass. J Parenter Enteral Nutr 1999;23:96 – 103.
Authenticated | 195.62.185.194Download Date | 11/30/12 7:36 AM

Di Somma et al.: Biomarkers and bio-impedance in acute heart failure 2103
77. Utter AC, Nieman DC, Ward AG, Butterworth DE. Use of the leg-to-leg bioelectrical impedance method in assessing body-compo-sition change in obese women. Am J Clin Nutr 1999;69:603 – 7.
78. Mitayani M, Kanehisa H, Fukunaga T. Validity of bioelectrical impedance and ultrasonographic methods for estimating muscle volume of the upper arm. Eur J Appl Physiol 2000;82:391 – 6.
79. Biggs J, Cha K, Horch K. Electrical resistivity of the upper arm and leg yields good estimates of whole body fat. Physiol Meas 2001;22:365 – 76.
80. Baumgartner RN, Chumlea WC, Roche AF. Estimation of body composition from bioelectric impedance of body segment. Am J Clin Nutr 1989;50:221 – 6.
81. Lukaski HC, Scheltinga MR. Improved sensitivity of tetrapo-lar bioelectrical impedance estimates of fl uid change and fat-free mass with proximal placements of electrodes. Age Nutr 1994;5:123 – 9.
82. Liu MH, Wang CH, Huang YY, Tung TH, Lee CM, Yang NI, et al. Edema index-guided disease management improves 6-month outcomes of patients with acute heart failure. Int Heart J 2012;53:11 – 7.
83. Tatara T, Tsuzaki K. Segmental bioelectrical impedance analysis improves the prediction for extracellular water volume changes during abdominal surgery. Crit Care Med 1998;26:470 – 6.
84. Walter-Kroger A, Kroker A, Mattiucci-Guehlke M, Glaab T. A practical guide to bioelectrical impedence analysis using the example of chronic obstructing pulmonary disease. Nutr J 2011;10:35.
85. Bosy-Westphal A, Danielzyck S, Dorhofer RP, Piccoli A, Muller MJ. Pattern of bioelectrical impedance vector distribution by body mass index and age: implication for body-composition analysis. Am J Clin Nutr 2005;82:60 – 8.
86. Piccoli A. Bioeletric impedance vector distribution in perito-neal dialysis patient with different hydration status. Kidney Int 2004;65:1050 – 63.
87. Lukasky HC, Johnson PE, Bolonchuk WW. Assesment of fat-free mass using bioelectrical impedance measurements of human body. Am J Clin Nutr 1985;41:810 – 7.
88. Talluri T, Lietdke RJ, Evangelisti A, Talluri J, Maggia G. Fat-free mass qualitative assessment with bioelectrical impedance analy-sis (BIA). Ann N Y Acad Sci 1999;20:873 – 94.
89. Piccoli A. Identifi cation of operational clues to dry weight pre-scription in hemodialysis using bioimpedance vector analysis. Kidney Int 1998;53:1036 – 43.
90. Bozzetto S, Piccoli A, Montini G. Bioelectrical impedence vec-tor analysis to evaluate relative hydration status. Pediatr Nephrol 2010;25:329 – 34.
91. Valle R, Aspromonte N, Milani L, Peacock FW, Maisel AS, Santini M, et al. Optimizing fl uid management in patient with acute decompensated heart failure (ADHF): the emerging role of combined measurement of body hydration status and brain natri-uretic peptide (BNP) levels. Heart Fail Rev 2011;16:519 – 29.
92. Piccoli A, Rossi B, Pilon L, Bucciante G. A new method for mon-itoring body fl uid variation by bioimpedence analysis: the R/Xc graph. Kidney Int 1994;46:534 – 9.
93. Tuy T, Peacok F. Noninvasive volume assessment in the emer-gency department: a look at B-type natriuretic peptide and bioimpedence vector analysis. Contrib Nephrol 2011;171:187 – 93.
94. Piccoli A, Pittoni G, Facco E. Relationship between central venous pressure and bioimpedance vector analysis in critically ill patients. Crit Care Med 2000;28:132 – 7.
95. Piccoli A, Codognotto M, Chanchi V, Vettore G, Zaninotto M, Plebani M, et al. Differentation of cardiac and non cardiac dys-pnea using bio-electrical impedance vector analysis. J Card Fail 2012;18:226 – 32.
96. Di Somma S, Gori CS, Salvatori E. How to manage cardio-renal syndrome in the emergency room. Contrib Nephrol 2010;165:93 – 100.
Prof. Salvatore Di Somma (07/06/1953) graduated in Medicine cum laude (Univer-sity of Naples, 1978) and postgraduated cum laude both in Internal Medicine and in Cardiology (University of Naples, 1983 and 1987). He began his university career at the Department of Clinical and Experimental Medicine and as Assistant Professor –
Emergency Medicine and Cardioangiology – at the University Federico II of Naples (1978 – 2001). He was research fellow in cardiology at the University of Pavia (1989 – 1992) and was Assistant Professor in the Cardiovascular Research Institute of the Department of Medicine, New York Medical College, USA (1994 – 1996). Now Prof. Di Somma is Associate Professor of Medicine and Chairman of the Postgraduate School of Emergency Medicine, II Medical School, La Sapienza University of Rome. He is the Director of Emergency Medicine in Sant ’ Andrea Hospital, Rome. Prof. Di Somma is author to more than 400 papers in the fi eld of Cardiology and Emergency Medicine. He is the director of an international cooperation team and reviewer for international medical journals.
Silvia Navarin born on (01/08/1987) was born in Rome and graduated from Liceo Classico E. Montale also in Rome (100/100). She graduated from the Second School of Medicine, La Sapienza, University of Rome. She has been a member of the Italian Red Cross since 2006 as a fi rst aid instructor, ambu-lance operator, and she was the Italian Red Cross delegate for the international cooperation work between Italy and Bosnia
Herzegovina (2008) and also at the international meeting in Solferino (2009). She has been involved in medical practise and research programs in the Emergency Department of Sant ’ Andrea Hospital in Rome since 2009. She participated in a professional exchange program of the International Federation of Medical Students ’ Association at the Department of Emergency Medicine in the University Clinical Centre Ljubljana in 2010. She won a 3 months international scholarship at the University of California, San Diego and took part in a research project for her graduation thesis in the Veterans Affair San Diego Healthcare System.
Authenticated | 195.62.185.194Download Date | 11/30/12 7:36 AM

2104 Di Somma et al.: Biomarkers and bio-impedance in acute heart failure
Stefania Giordano (23/07/1987) was born in Rome. She graduated from Liceo Classico-Linguistico Gaio Valerio Catullo in 2006, and she also gradu-ated in the second School of Medicine at La Sapienza University of Rome. She has been involved in medi-cal practise and research programs at the Emergency Department of Sant ’ Andrea
Hospital in Rome since 2008. In 2011 she received a cer-tifi cate of “ Echography in the emergency department ” . She won a 3 months international scholarship at the University of California, San Diego where she took part in a research project for her graduation thesis at the Veterans Affairs San Diego Healthcare System.
Francesco Spadini (07/01/1976) was born in Rome. He graduated from Liceo Scientifi co Statale Louis Pasteur in 1994. From 1994 to 1997 he worked at the Physics Department at La Sapienza Rome University. From 1997 to 2005 he worked in the IT industry. He is cur-rently studying at the Second School of Medicine at La
Sapienza Rome University, where he is also collaborating on various research projects.
Prof. Giuseppe Lippi is the Director of the Clinical Chemistry and Hematology Laboratory of the Academic Hospital of Parma and Associate Professor of Clinical Biochemistry and Molecular Biology. He has a degree in Medicine and a specialization in Clinical Biochemistry and Laboratory Medicine. He currently serves as Associate Editor of
Clinical Chemistry and Laboratory Medicine and Seminars in Thrombosis of Hemostasis. He is also chairman of the sci-entifi c division of the Italian Society of Clinical Biochemistry and Molecular Biology (SIBioC), and member of the board of the European Association of Clinical Chemistry (EFCC).
Prof. Lippi is author of more than 750 publications on inter-national journals indexed in PubMed and Thomson, and in more than 90 % of them as main or senior author. His main area of research includes preanalytical variability, analytical and clinical validation of novel biomarkers, metabolism of lipoproteins and relevant assay methods, diagnosis and man-agement of disorders of hemostasis.
Prof. Cervellin Gianfranco (30/06/1955) graduated in Medicine in 1980. He com-pleted his postgratuate stud-ies in Geriatrics in 1984 and in Cardiology in 1988 at the University of Parma, Italy). He has been the Director of Emergency Medicine in Azienda Ospedaliero, University of Parma, Italy since October 2005. In April
2006 he became the Professor of Emergency Medicine at the University of Parma, Italy. He is author of approximately100 publications (66 available on PubMed), and some book chapters.
Bryan Dieffenbach is cur-rently a medical student at the University of California, San Diego (UCSD) School of Medicine. Prior to medi-cal school, he completed a Master of Science degree at UCSD studying the innate immune response in rheu-matoid arthritis. As an under-graduate, he graduated with honors from UCSD with a degree in Biochemistry and Cell Biology. He was also the captain of the UCSD Men ’ s Track and Field Team.
Authenticated | 195.62.185.194Download Date | 11/30/12 7:36 AM

Di Somma et al.: Biomarkers and bio-impedance in acute heart failure 2105
Dr. Alan Maisel attended University of Michigan Medical School and com-pleted his cardiology training at the University of California, San Diego. He is currently Professor of Medicine at the University and Director of the Coronary Care Unit and the Heart Failure Program at the affi liated Veterans Affairs Medical Center. He is con-sidered one of the world ’ s experts on cardiac biomark-
ers, and is given credit for ushering in the use of BNP levels in clinical practice around the world. He has over 300 articles in print and a large clinical and basic science laboratory. Dr. Maisel is also a fi xture at the medical school, where he has won countless teaching awards from medical students as well as interns and residents. His yearly San Diego Biomarker meeting is considered the most prestigious of its kind. He is currently an Associate Editor of the Journal of American College of Cardiology.
Authenticated | 195.62.185.194Download Date | 11/30/12 7:36 AM
Copyright © 2022 FDOKUMEN




















