
Nanoscopic and Photonic Ultrastructural Characterization of Two Distinct Insulin Amyloid States
Upload
independentCategory
view
1download
0
Synaptic Differences in the PostmortemStriatum of Subjects With Schizophrenia:A Stereological Ultrastructural Analysis
ROSALINDA C. ROBERTS,* JOY K. ROCHE, AND ROBERT R. CONLEYMaryland Psychiatric Research Center, Department of Psychiatry, University of Maryland School of Medicine,
Baltimore, Maryland 21228
KEY WORDS ultrastructure; caudate; putamen; neuroleptics; basal ganglia
ABSTRACT The striatum processes motor, cognitive, and limbic function, all ofwhich are perturbed in schizophrenia. The present study examined the synapticorganization of the caudate and putamen in schizophrenia. Postmortem striatum wasobtained from 10 normal controls (NC) and 17 subjects with schizophrenia (SZ), pre-pared for electron microscopy, and analyzed using stereological principles. The den-sities of total synapses, asymmetric synapses (characteristic of excitatory inputs), andasymmetric axospinous synapses (characteristic of cortical input) were higher in thecaudate of the SZs vs. NCs. These changes were most profound in the off-drug SZcases and were also elevated in subjects on antipsychotic drugs (APDs). In comparisonto NCs, there were no significant differences in the putamen of the SZ cohort as awhole group; however, there were more asymmetric axospinous synapses in the off-drug subgroup. The increase in density of synapses in the SZs does not appear to becaused by antipsychotic medication and may represent failure of normal synapticpruning or abnormal sprouting. Higher density of cortical-type synapses in SZs vs.NCs may reflect adaptation of corticostriatal circuitry or hyperstimulation of striatalprojection neurons. The abnormal synaptic organization could have several importantand different downstream effects depending on the precise circuitry involved and maybe related to limbic or cognitive dysfunction in schizophrenia. Synapse 56:185–197,2005. ' 2005 Wiley-Liss, Inc.
INTRODUCTION
The mammalian striatum is a topographically organ-ized structure that interacts with other brain regionsto process motor, cognitive, and limbic circuitry(Alexander et al., 1990; Haber et al., 2000; McFarlandand Haber, 2002; Parent and Hazrati, 1995; Smith andParent, 1986), all of which are abnormal in schizophre-nia (Bunney and Bunney, 2000; Harrison, 1999;Powers, 1999). Most postmortem studies have focusedon the cortical regions that subserve these functions,even though there is abundant evidence for a role forthe striatum in cognitive and limbic function (Charpierand Deniau, 1997; Collinson et al., 2003; Cote et al.,1995; Gerfen, 1984; Hugdahl, 2000; Levesque andParent, 1998; Lieberman, 2000; White and Hiroi,1998). For example, damage to or neurodegeneration inthe caudate nucleus results in numerous deficits simi-lar to those present in schizophrenia, such as adecrease in executive function, impaired ability tomanipulate acquired knowledge, shorter attentionspan, memory impairment, and apathy (Bokura and
Robinson, 1997; Caplan et al., 1990; Hasselbalch et al.,1992; Mendez et al., 1989; Yanagisawa, 1996). The cau-date nucleus and anterior putamen receive inputs fromdorsolateral and other areas of prefrontal cortex, ante-rior cingulate cortex, and from motor and premotor cor-tex (Alexander et al., 1986; Chikama et al., 1997; Eblenand Graybiel, 1995; Goldman-Rakic, 1994; Goldman-Rakic and Selemon, 1986; Haber et al., 1995, 2000;Kunishio and Haber, 1994; Parent and Hazrati, 1995;Smith et al., 1998). Therefore, abnormalities in eitherthe caudate or putamen could be involved in the def-icits with working memory, limbic dysfunction (psycho-sis), and/or motor function, respectively, that arepresent in schizophrenia (Selemon, 2001; Selemon andGoldman-Rakic, 1999; Tamminga et al., 1992).
*Correspondence to: Dr. Rosalinda C. Roberts, Maryland PsychiatricResearch Center, P.O. Box 21247, Baltimore, MD 21228.E-mail: [email protected]
Received 19 November 2004; Accepted 10 February 2005
DOI 10.1002/syn.20144
Published online in Wiley InterScience (www.interscience.wiley.com).
' 2005 WILEY-LISS, INC.
SYNAPSE 56:185–197 (2005)

The striatum of subjects with schizophrenia showsseveral abnormalities that may play an important rolein the pathophysiology of schizophrenia (Harrison,1999; Powers, 1999). Numerous studies have shownthat striatal metabolic rate is compromised in peoplewith schizophrenia (Bartlett et al., 1991; Buchsbaumet al., 1987, 1992a,b; Cleghorn et al., 1992; DeLisiet al., 1985; Resnick et al., 1988). Several studieshave implicated neuroanatomical, neurochemical, andmitochondrial abnormalities in the striatum of sub-jects with schizophrenia (Ben-Shachar, 2002; Karryet al., 2004; Kleinman et al., 1985; Holt et al., 1999;Korpi et al., 1986; Kung and Roberts, 1999; Lahtiet al., 1998; Prince et al., 1999; Simpson et al., 1992).The striatum in schizophrenia displays augmentationof presynaptic dopamine function, suggesting an in-crease in dopamine synthesis capacity and an in-crease in presynaptic dopamine stores (Abi-Darghamet al., 1998, 2000; Breier et al., 1997; Dao-Castellanaet al., 1997; Hietala et al., 1994, 1995, 1999; Laruelleet al., 1996, 1999). In schizophrenic subjects, abnor-mally high activity in the caudate is positively corre-lated with formal thought disorder (Kircher et al.,2001; McGuire et al., 1998). Electron microscopicstudies of the striatum have shown smaller spinesand abnormalities in synaptic organization, mitochon-dria, and astrocytes (Kung and Roberts, 1999; Kunget al., 1998a,b; Roberts et al., 1996; Uranova, 1996;Uranova et al., 1996, 2001). Given the role of thestriatum in functions that are abnormal in schizo-phrenia and the evidence from in vivo and postmor-tem studies, it is likely that the caudate or putamenor both are involved in the disease.
In a previous study from our laboratory, synapticabnormalities were found in schizophrenic subjectsincluding a small increase in the density of axospi-nous synapses (Kung et al., 1998a). In animals, themajority of terminals forming this type of synapseoriginate from glutamatergic neurons in the cortex(Kemp and Powell, 1971a–c). In the human brain it isnot practical or possible to use the tract-tracingexperiments that are performed in animals to identifyconnectivity and the ultrastructural features of syn-apses found in particular pathways. However, byexamining the morphological characteristics of syn-apses, such as symmetry and postsynaptic targets, itis possible to gain insight as to the origin of the neu-rons forming the synapses, and whether the neuraltransmission is likely to be excitatory or inhibitory.We were interested in extending our previous studiesto include a stereological analysis of synaptic density.Our hypotheses are that there are abnormalities insynaptic organization in the striatum in schizophrenicsubjects and that antipsychotic drug treatment isprobably not responsible for these abnormalities. Thiswork has been published in preliminary form (Robertset al., 2001).
SUBJECTS AND METHODSSubjects
Postmortem human brain tissue was collected bythe Maryland Brain Collection (MBC) within 8 h ofdeath from 10 control cases and 17 cases with schizo-phrenia. The next of kin gave permission for the tis-sue to be collected and used by the MBC. None of thecases used in this study were known to be HIV orhepatitis B positive, or in comas, or on respiratorsprior to death. The control group (NC) was matchedto the group with schizophrenia (SZ) using age, post-mortem interval (PMI), gender, and race as criteria.
Information on the cases was determined fromautopsy reports, medical records, and family inter-views. Controls were defined as people without a life-time diagnosis of a serious mental illness other thanalcohol or substance abuse/dependence. Diagnoses ofschizophrenia, alcohol abuse/dependence, substanceabuse, or other mental illness were made indepen-dently by two research psychiatrists according toDSM-IV criteria using the SCID (Scheduled ClinicalInterview for the DSM-III-R) (Spitzer et al., 1992)and the Diagnosis Evaluation After Death (DEAD)(Salzman et al., 1983). Diagnoses and demographicsfor individual cases are presented in Table I. The Uni-versity of Maryland Institutional Review Board,which is a human ethics committee, approved all pro-cedures.
The SZs were divided into subgroups based on theirantipsychotic drug (APD) status within the last6 months of life. Seven cases were on atypical APDs,seven cases were on typical APDs. Two cases were offAPDs, and in one case this information was not able tobe determined. The absence of an APD in the toxicologyreport was not taken as conclusive evidence that theperson was not on their medication because of the shorthalf-life of APD drugs. The cases off-APD medicationwere off APD for at least 6 months.
Tissue processing
Coronal blocks (1 cm thick) of the striatum wereimmersed in a cold solution of 4% paraformaldehydeand 1% glutaraldehyde in 0.1 M phosphate buffer,pH 7.2–7.4, (PB). Samples were taken from the head ofthe caudate and anterior putamen. Samples from theputamen were available for 15 out of the 17 SZ cases.The tissue was cut with a Vibratome (at a thickness of40 mm) and the sections were collected into cold PB. Thetissue from the cases in this study were used in paststudies described in our previous publications (Kunget al., 1998a,b; Roberts and Knickman, 2002; Robertset al., 2001). Tissue samples ~0.5 � 1.0 cm in size wereexcised from the caudate and putamen and were flat-embedded using standard techniques. Pieces of the cau-date and putamen were embedded in two separate vials,in case of breakage during the embedding process.
186 R.C. ROBERTS ET AL.

Briefly, the sections were rinsed in PB (3 � 10 min),immersed in 1% osmium tetroxide for 1 h, stained enbloc with 1% uranyl acetate for 2 h, dehydrated in alco-hol, embedded in resin, and heated at 608C for 72 h.Samples were randomly chosen from both dorsal andventral regions within the caudate and putamen, cutout, and mounted on Beem capsules (SPI Supplies, WestChester, PS). The blocks were then thin-sectioned at athickness of 90 nm. The mean number of sections ineach ribbon was 14 6 3.3 serial sections. An average of210 mm3 was analyzed per case per caudate or putamen.
The pH of a sample of cerebellum was determinedfrom several of the cases according to the techniquesof Harrison et al. (1995) and Johnston et al. (1997). Asample piece of tissue (a 1.5–2.0 cm chunk) was dis-sected from the frozen brain with a bone saw. The tis-sue was homogenized for ~1 min so as not to raisethe temperature of the sample, then the pH probefrom Omni’s PCR Tissue Homogenizing Kit wasinserted to measure the pH.
Data collection and analysis
Quantitative analysis was performed from the cau-date and putamen. The analysis of synaptic organiza-tion was performed with the experimenter blinded tothe diagnosis. Three-dimensional reconstruction simi-
lar to the technique described by Geinisman et al.(1996) was utilized rather than counting profiles thatappear in a single disector (present in one section butnot in the lookup section). The 3D reconstruction tech-nique, in which synapse identification is more accurate,was used to determine the synaptic density of all syn-apses combined and of various subsets of synapses, asdescribed previously (Roberts and Knickman, 2002). Ineach section montages or three photomicrographs weretaken at 10,000� which formed an area of ~100 mm2.All synapses appearing in the first montage in the se-ries and all synapses that crossed the exclusion lines(top or right borders of the counting frame) in any ofthe series were excluded. Any new synapses thatappeared in subsequent montages, that met criteria,were numbered and followed throughout their extentin each of the montages in which they appeared. Eachindividual synapse appeared in at least one section, butusually several, and could be accurately identified as totype. The criteria for identifying a synapse were paral-lel pre- and postsynaptic membranes with a discern-able synaptic cleft, a postsynaptic density, and three ormore synaptic vesicles at the synapse in the presynap-tic terminal. Synapses were identified as asymmetricaxospinous (AS), asymmetric axodendritic (AD), sym-metric axospinous (SS), symmetric axodendritic (SD),all asymmetric synapses (Asym, AS þ AD), or all
TABLE I. Characteristics of individual postmortem subjects
Case # DSM-IV PMI ARG Cause of death Antipsychotic drugsToxicological findings(at time of death)
Controls1 3 79AM ASCVD none none2 3 48AM MVA none none3 * 4 36CM MVA none alcohol4 6 47CM ASCVD none none5 7 32CF Cardiac arrhythmia none none6 8 43AF ASCVD none none7 * 5 37CF ASCVD none alcohol, THC8 * 6 21CM MVA none alcohol9 5 68AM ASCVD none none10 * 8 43AF Liver cirrhosis none alcohol
Subjects with schizophrenia11 CUT 7 32CM Multiple injuries (jump) Clozapine Clozapine12 CUT 5 52CF Aspirated food Risperidone Diphenhydramine13 CUT 6 45CM Drug intoxication Risperidone Olanzapine, Fluoxetine,
Nortriptyline14 CUT 3 58AF ASCVD Off at time of death None15 Paranoid 3 37CM Polydipsia Fluphenazine Sertraline16 Paranoid 6 60AF Pulmonary thrombosis Loxapine Loxapine17 Paranoid** 8 43CF Seizure, drug intoxication Clozapine Carbamazepine18 Paranoid 8 47CM ASCVD Risperidone None19 CUT 4 43AM Seizure Thioridizine Thioridizine20 Paranoid 5 60AM Amyloidosis Olanzapine Olanzapine21 NOS 3 33AF Drug intoxication Off at time of death Trazodone22 CUT 7 67AM ASCVD Not able to determine Neg for Clonazapam23 CUT 3 71CM ASCVD Chlorpromazine Trifluoperazine24 CUT 3 59AF ASCVD Chlorpromazine Dextromethorphan25 Paranoid 6 45AM Hanging Olanzapine Olanzapine26 NOS 5 48AF Hanging Haloperidol None27 CUT 5 53CM MI Perphenazine Carbamazepine
Demographic, psychiatric, and other information is shown for each individual case. PMI, postmortem interval (hours); ARG, age (years), race, gender; A, African-American; C, Caucasian; M, male; F, female; ASCVD, atherosclerotic cardiovascular disease; MVA, motor vehicle accident; MI, myocardial infarction; THC, tetra-hydrocannabinol; *alcohol abuse/dependence; **polysubstance abuse; CUT, chronic undifferentiated type. The cases on risperidone were treated with doses thatfell in the atypical APD range. The toxicology report reflects substances found in the blood or urine. The absence of an APD in the toxicology report was not takenas conclusive evidence that the person was not on their medication because of the short half-life of APD drugs. Cases 14 and 21 were off APD medication for atleast 6 months. The putamen was not available for cases 25 and 26. The pH of representative EM samples in 6.65 6 0.12.
187STRIATAL SYNAPSES IN SCHIZOPHRENIA
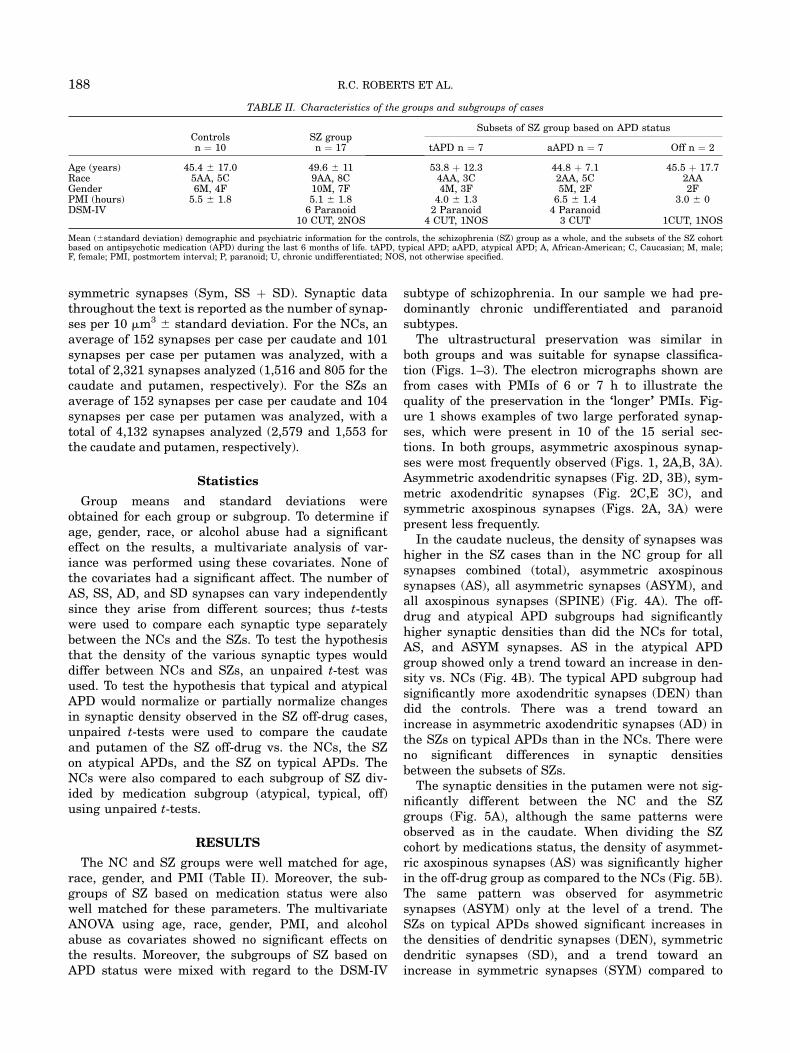
symmetric synapses (Sym, SS þ SD). Synaptic datathroughout the text is reported as the number of synap-ses per 10 mm3 6 standard deviation. For the NCs, anaverage of 152 synapses per case per caudate and 101synapses per case per putamen was analyzed, with atotal of 2,321 synapses analyzed (1,516 and 805 for thecaudate and putamen, respectively). For the SZs anaverage of 152 synapses per case per caudate and 104synapses per case per putamen was analyzed, with atotal of 4,132 synapses analyzed (2,579 and 1,553 forthe caudate and putamen, respectively).
Statistics
Group means and standard deviations wereobtained for each group or subgroup. To determine ifage, gender, race, or alcohol abuse had a significanteffect on the results, a multivariate analysis of var-iance was performed using these covariates. None ofthe covariates had a significant affect. The number ofAS, SS, AD, and SD synapses can vary independentlysince they arise from different sources; thus t-testswere used to compare each synaptic type separatelybetween the NCs and the SZs. To test the hypothesisthat the density of the various synaptic types woulddiffer between NCs and SZs, an unpaired t-test wasused. To test the hypothesis that typical and atypicalAPD would normalize or partially normalize changesin synaptic density observed in the SZ off-drug cases,unpaired t-tests were used to compare the caudateand putamen of the SZ off-drug vs. the NCs, the SZon atypical APDs, and the SZ on typical APDs. TheNCs were also compared to each subgroup of SZ div-ided by medication subgroup (atypical, typical, off)using unpaired t-tests.
RESULTS
The NC and SZ groups were well matched for age,race, gender, and PMI (Table II). Moreover, the sub-groups of SZ based on medication status were alsowell matched for these parameters. The multivariateANOVA using age, race, gender, PMI, and alcoholabuse as covariates showed no significant effects onthe results. Moreover, the subgroups of SZ based onAPD status were mixed with regard to the DSM-IV
subtype of schizophrenia. In our sample we had pre-dominantly chronic undifferentiated and paranoidsubtypes.
The ultrastructural preservation was similar inboth groups and was suitable for synapse classifica-tion (Figs. 1–3). The electron micrographs shown arefrom cases with PMIs of 6 or 7 h to illustrate thequality of the preservation in the ‘‘longer’’ PMIs. Fig-ure 1 shows examples of two large perforated synap-ses, which were present in 10 of the 15 serial sec-tions. In both groups, asymmetric axospinous synap-ses were most frequently observed (Figs. 1, 2A,B, 3A).Asymmetric axodendritic synapses (Fig. 2D, 3B), sym-metric axodendritic synapses (Fig. 2C,E 3C), andsymmetric axospinous synapses (Figs. 2A, 3A) werepresent less frequently.
In the caudate nucleus, the density of synapses washigher in the SZ cases than in the NC group for allsynapses combined (total), asymmetric axospinoussynapses (AS), all asymmetric synapses (ASYM), andall axospinous synapses (SPINE) (Fig. 4A). The off-drug and atypical APD subgroups had significantlyhigher synaptic densities than did the NCs for total,AS, and ASYM synapses. AS in the atypical APDgroup showed only a trend toward an increase in den-sity vs. NCs (Fig. 4B). The typical APD subgroup hadsignificantly more axodendritic synapses (DEN) thandid the controls. There was a trend toward anincrease in asymmetric axodendritic synapses (AD) inthe SZs on typical APDs than in the NCs. There wereno significant differences in synaptic densitiesbetween the subsets of SZs.
The synaptic densities in the putamen were not sig-nificantly different between the NC and the SZgroups (Fig. 5A), although the same patterns wereobserved as in the caudate. When dividing the SZcohort by medications status, the density of asymmet-ric axospinous synapses (AS) was significantly higherin the off-drug group as compared to the NCs (Fig. 5B).The same pattern was observed for asymmetricsynapses (ASYM) only at the level of a trend. TheSZs on typical APDs showed significant increases inthe densities of dendritic synapses (DEN), symmetricdendritic synapses (SD), and a trend toward anincrease in symmetric synapses (SYM) compared to
TABLE II. Characteristics of the groups and subgroups of cases
Controlsn ¼ 10
SZ groupn ¼ 17
Subsets of SZ group based on APD status
tAPD n ¼ 7 aAPD n ¼ 7 Off n ¼ 2
Age (years) 45.4 6 17.0 49.6 6 11 53.8 þ 12.3 44.8 þ 7.1 45.5 þ 17.7Race 5AA, 5C 9AA, 8C 4AA, 3C 2AA, 5C 2AAGender 6M, 4F 10M, 7F 4M, 3F 5M, 2F 2FPMI (hours) 5.5 6 1.8 5.1 6 1.8 4.0 6 1.3 6.5 6 1.4 3.0 6 0DSM-IV 6 Paranoid 2 Paranoid 4 Paranoid
10 CUT, 2NOS 4 CUT, 1NOS 3 CUT 1CUT, 1NOS
Mean (6standard deviation) demographic and psychiatric information for the controls, the schizophrenia (SZ) group as a whole, and the subsets of the SZ cohortbased on antipsychotic medication (APD) during the last 6 months of life. tAPD, typical APD; aAPD, atypical APD; A, African-American; C, Caucasian; M, male;F, female; PMI, postmortem interval; P, paranoid; U, chronic undifferentiated; NOS, not otherwise specified.
188 R.C. ROBERTS ET AL.

the SZs on atypical APDs. In addition, the density ofasymmetric axodendritic synapses (AD) was higher inthe SZs on typical APDs than the NCs.
DISCUSSION
The main results of the present study show altera-tions in synaptic organization in the striatum of sub-jects with schizophrenia (SZ) compared to that of con-trols (NCs). In comparison to NCs, the density of syn-apses was higher in the caudate in the cohort of SZcases as a combined group (n ¼ 17) for all synapsescombined due to a significant increase in asymmetricaxospinous (AS) synaptic density. In the putamen, thedensity of AS synapses was higher than that of NCsin the off-drug subset of SZ cases, but not the groupof SZ as a whole (n ¼ 15). When subdividing the SZgroup by medication status, the alterations in totalsynaptic density and that of AS synapses did notappear to be caused by APD medication. Since thesubgroups of SZ divided by APD status were com-prised of a mixture of paranoid and undifferentiatedcases, the results presented here are most likely notconfounded by heterogeneity of symptoms in the sub-groups of SZ. Although our results showed certain
changes in less frequent synaptic types, such as axo-dendritic synapses, these findings should be regardedas preliminary due to the low overall frequency oftheir numbers.
The present study shows several alterations in syn-aptic circuitry in the SZ group, but without a compar-ison psychiatric group the possibility that the resultsare found in other psychiatric illnesses, such as bipo-lar subjects, cannot be excluded. In fact, in our pre-vious study (Kung et al., 1998a), AS synapses wereincreased in density in comparison to the NC in asmall psychiatric comparison group. The rarity of tis-sue usable for electron microscopy, and the long time-frame required to collect it, make the timely inclusionof all desirable control groups unrealistic. A studyincluding other psychiatric groups is certainly animportant follow-up to the present study to helpdetermine the specificity to schizophrenia of thechanges we observed in the present study.
Results found in SZs may be obscured or caused byAPD treatment, rather than being related to thepathophysiology of the disease. For example, volumechanges in the striatum have been observed in SZpatients and, for the most part, have been attributedto APD effects (Chakos et al., 1994; Gunduz et al.,
Fig. 1. A,B: Two electron micrographs, three sections (270 nm)apart, through the same region of the caudate nucleus from case 25,a hanging suicide victim with a 6-h PMI. These micrographs illus-trate that the ultrastructural preservation is quite adequate todetermine synapse morphology even in this case that suffered a cer-tain amount of asphyxia due to the cause of death and had a
‘‘longer’’ PMI. Two spines (s1 and s2) receive asymmetric axospinous(AS) synapses (arrows) from different axon terminals (at1 and at2).The arrows indicate the active zones in each synapse; note that thepostsynaptic densities of both synapses are perforated. a, myeli-nated axon; m, mitochondrion. Scale bars ¼ 1.0 mm.
189STRIATAL SYNAPSES IN SCHIZOPHRENIA

2002; Gur et al., 1998; Keshavan et al., 1994, 1998;Scheepers et al., 2001; Shihabuddin et al., 1998).Neuroleptic naıve SZs at first break have smaller ornormal striatal volumes in comparison to NCs (Gun-duz et al., 2002; Keshavan et al., 1998; Shihabuddinet al., 1998). Typical APD treatment appears to mod-estly increase caudate size (<10%) (Chakos et al.,
1994), while the atypical APD clozapine has beenreported either to reduce caudate size (Scheeperset al., 2001) or to have no effect (Gur et al., 1998).The possibility that our synaptic density findings arean artifact of APD-induced volume changes isunlikely for several reasons. An increased volume ofthe caudate and putamen in SZs together with an
Fig. 2. Examples of different types of striatal synapses fromcontrols. A: A spine (s) emerges from a dendrite (den) and receivestwo synapses. One axon terminal (at) forms an asymmetric axospi-nous (AS) synapse (arrow) with the head of the spine, while a smallaxon terminal (indicated by at and arrow) forms a symmetric axo-spinous (SS) synapse (black and white arrow) with the spine neck.Case 4. B: A spine (s) receives a perforated asymmetric axospinous
(AS) synapse (arrows); the asterisk marks the perforation in thepostsynaptic density. Case 5. C: An axon terminal (at) forms a sym-metric axodendritic (SD) synapse (black and white arrow) with adendrite. Case 5. D: Two axon terminals (at) form asymmetric axo-dendritic (AD) synapses (arrows) with a large dendrite (den). Thesynapse at the top has a perforated postsynaptic density (*). Mito-chondria are indicated (m). Scale bars ¼ 0.5 mm.
190 R.C. ROBERTS ET AL.

increased density of some types of synapses wouldamplify, not negate, our present findings. If anything,our density measurements may underrepresent thetotal synapse number in the entire striatum of sub-
jects with schizophrenia. Moreover, typical vs. atypi-cal APD have different effects on caudate volume(Gur et al., 1998), but most synaptic density increasesare equivalent between cases on typical vs. atypical
Fig. 3. Examples of different types of striatal synapses from theSZ group. A: A spine (s1) with a short neck emerges (curved arrow)from a dendrite (den). An axon terminal (at1) forms an asymmetricaxospinous (AS) synapse (arrow) with spine 1. An adjacent spine(s2) receives two synapses, an asymmetric axospinous (AS) synapse(arrow) from an axon terminal (at2) and a symmetric axospinous
(SS) synapse (black and white arrow) from a different axon terminal(at3) sparsely filled with synaptic vesicles. B: A dendrite (den)receives an asymmetric axodendritic (AD) synapse (arrow). C: Adendrite (den) receives symmetric axodendritic (SD) synapse (blackand white arrows, * at perforation in the postsynaptic density).Mitochondria are indicated (m). Scale bars ¼ 0.5 mm.
191STRIATAL SYNAPSES IN SCHIZOPHRENIA

APDs. Also, if volume changes were responsible forour synaptic findings, then it would be expected thatall synapses would show a similar direction and mag-nitude of change, and this is not the case.
The cellular component that is responsible for thechanges in volume of the SZ striatum is not known,but probably is not due to an increase in synapticdensity. In the present study, all but two individualsin the SZ group were treated with APD medicationsprior to death, which is a limitation of the study. Thehighest density of all synapses combined wasobserved in the subjects off-drug, followed by thosesubjects treated with APDs. This suggests that APDs
do not increase overall striatal synaptic density or thedensity of asymmetric axospinous synapses (whichconstitute the vast majority of synapses). This conclu-sion, which must be interpreted with caution due tothe small size of the group off APDs, is validated byanimal work. For example, chronic treatment withhaloperidol, a typical APD, produces decreases inoverall synaptic density and AS density in the stria-tum (Meshul et al., 1996; Roberts and Lapidus, 2003;Roberts et al., 1995a), while the atypical APD, olanza-pine, produces no changes in synaptic density (Rob-erts, 2001). It is noteworthy to point out that thecases off APDs were APD-free for at least 6 months.
Fig. 4. Graphs comparing the synaptic organization in the cau-date nucleus in (A) controls vs. the subjects with schizophrenic (SZ),and (B) the caudate in the controls and the SZ subgroups based onAPD medication. Note that the number of SZ cases in A is 17,whereas in B it is 16 because information on APD status in one casewas not able to be determined. Bars are the mean values per caseper 10 mm3; error bars represent standard deviation. TOTAL ¼ all
synapses combined; AS ¼ asymmetric axospinous; AD ¼ asymmetricaxodendritic; SS ¼ symmetric axospinous; SD ¼ symmetric axoden-dritic; ASYM ¼ all asymmetric synapses (AS þ AD); SYM ¼ allsymmetric synapses (SS þ SD); SPINE ¼ all axospinous synapses(AS þ SS); DEN ¼ all axodendritic synapses (AD þ SD). Results oft-tests are indicated: *P < 0.05; **P < 0.025; t, P < 0.075.
192 R.C. ROBERTS ET AL.

That time frame of withdrawal from medication issufficient to return APD-induced increases in dopa-mine receptors to normal levels in humans (Nyberget al., 1997). Also, in rats treated chronically withhaloperidol, after a withdrawn period of 1 month syn-aptic density returned to normal (Roberts et al.,1995a). Therefore, our cases, which were off APDs forat least 6 months, probably retained minimal or noeffects of the medication. The increase in asymmetricaxodendritic synapses in the putamen and axoden-dritic synapses in the caudate may be caused by typi-cal APD, as the density of these synapses was lowerin controls than in the subgroup of SZ on typicalAPD.
The increase in density of axospinous synapsesobserved in the present study is consistent with ourprevious study using a smaller cohort of SZ cases andusing simple profile counts rather than stereology(Kung et al., 1998a). Our results confirm those ofUranova et al. (1996), who also reported an increasein density of axospinous synapses in the caudate ofSZs and interpreted this to be a reflection of aberrantsprouting in the schizophrenic brain. While the aver-age size of axon terminals appears similar in SZs ascompared to NCs (Kung et al., 1998a), and most ofthe terminals we observed were normal in appear-ance, other investigators have reported that some ter-minals are swollen or degenerated (Uranova et al.,
Fig. 5. Graphs comparing the synaptic organization in the puta-men of (A) controls vs. the subjects with schizophrenic (SZ), and (B)the putamen in the controls and the SZ subgroups based on APDmedication. Note that the number of SZ cases in A is 15, whereas inB it is 14 because for one of the cases information on APD status
was not able to be determined. Bars are the mean values per caseper 10 mm3; error bars represent standard deviation. Results of thet-tests are indicated: *P < 0.05, **P < 0.025; t, P < 0.07. See Figure4 for abbreviations.
193STRIATAL SYNAPSES IN SCHIZOPHRENIA

1996). However, the proportion of terminals whichshowed pathology was not reported (Uranova et al.,1996), and it is therefore difficult to weigh the poten-tial impact of inactive or pathological axon terminalsand synapses with other data.
Synaptic density changes were observed in the SZsin several subtypes of synapses, implicating multiplesources of inputs. As in other species (Chung et al.,1977; Hassler et al., 1978; Pasik et al., 1976; Robertset al., 1995a,b), the majority of synapses present inthe human striatum form asymmetric synapses(Roberts and Knickman, 2002; Roberts et al., 1996),characteristic of excitatory synaptic transmission. Thesource of the vast majority of striatal asymmetric syn-apses is from the cortex (Dube et al., 1988; Hassleret al., 1978), but additional inputs arise from the thala-mus (Chung et al., 1977; Kemp and Powell, 1971a–c;Sadikot et al., 1992a,b; Smith et al., 1994), the raphe(LaVoie and Parent, 1990), and the amygdala (Kitaand Kitai, 1990). Thus, since the subtype of synapsewhich increased most in density in SZ was AS synap-ses, the corticostriatal pathway is certainly implicated(Dube et al., 1988; Hassler et al., 1978). Dendriticsynapses, particularly of the asymmetric type, werealso elevated in density in the SZ group, implicatingthe thalamus, raphe, and/or amygdala. Symmetricsynapses, typical of inhibitory transmission (DiFiglia,1987; DiFiglia and Aronin, 1982; Kitai et al., 1979;Ribak et al., 1979; Wilson and Groves, 1980; Pickelet al., 1981; Somogyi et al., 1981; Freund et al., 1984;Kubota et al., 1987a,b) showed few changes in densityin the SZs. The differences in density of asymmetricaxodendritic and symmetric synapses appeared to bedue to APD effects. The differential response of thesesynaptic types is intriguing, but may not be part ofthe disease process.
In the caudate in the SZ group, there were moretotal synapses, particularly of the corticostriatal type,than in the NC group. Synaptic density may be simi-lar between the NC and the SZ early in development,and the divergence in density may be due to a lack ofnormal synaptic pruning in schizophrenia. Alterna-tively, the increased synaptic density in schizophreniamay be due to abnormal sprouting, as suggested byUranova et al. (1996). Ultrastructural comparisons ofsynaptic number across developmental ages wouldaid in interpreting our data. Unfortunately, no suchstudies have been reported in human. Few striatalaxospinous synapses are present prenatally in eitheranimals or humans (Brand and Rakic, 1984; Robertsand Kung, 1999; Sharpe and Tepper, 1998; Uryuet al., 1999). Developmental studies in rodents showthat striatal asymmetric axospinous synapsesincrease in density from birth to postnatal day 21(Sharpe and Tepper, 1998; Uryu et al., 1999). There-after, synaptic density either remains stable ordeclines, depending on the subregion of the striatum
(Uryu et al., 1999). If synaptic number decreases incontrol brains due to normal pruning processes, thiswould suggest that the increase in synaptic density inschizophrenia might be due to a failure of normalpruning processes. If, however, synaptic number nor-mally stays the same or increases during develop-ment, then the increase in synaptic density in schizo-phrenia may be due to abnormal sprouting.
The increased density of cortical-type synapses inthe striatum in schizophrenia may be an APD drugeffect (unlikely, as discussed above), a primary lesion,or a compensatory sequela of abnormal circuitry else-where in the cortico-basal ganglia-thalamic-corticalloop (Alexander et al., 1986, 1990). The prefrontal cor-tex in schizophrenia shows strong evidence for fewersynaptic connections, including reduced volume ofneuropil (Selemon and Goldman-Rakic, 1999; Sele-mon et al., 2001), fewer dendritic spines (Glantz andLewis, 2000), and a probable increase of inhibitorytone on the axon initial segments of layer III pyrami-dal neurons (Woo et al., 1998; Pierri et al., 1999).Moreover, thalamic neurons in the medial dorsalnucleus, which send excitatory projections to layer IIIneurons, are reduced in number (Pakkenberg, 1990;Young et al., 2000). Also, there is reduced density ofdopaminergic inputs in the cortex (Akil et al., 1999).Taken together, the cortical neurons in the prefrontalcortex of schizophrenic subjects suffer from reducedexcitatory thalamic inputs, fewer spines that are therecipient of excitatory inputs, and a probable increasein inhibitory tone on the axon initial segments. Inspite of the complicated abnormalities in both excita-tory and inhibitory neurotransmission in the prefron-tal cortex, the cortex apparently manages to makemore synapses in the striatum. Thus, increased num-bers of cortical synapses may be a compensatoryresponse to the hypothesized overall diminished corti-cal output discussed by Lewis et al. (1999). Anotherinterpretation is that striatal spiny neurons areactually overexcited in schizophrenia. This latter sce-nario could have several different downstream effects,depending on which population of medium spiny neu-rons is affected. Since there are several circuitsthrough the caudate and putamen that might beabnormal in schizophrenia, further studies are neces-sary to identify where these changes occur. In addi-tion, the striatum is topographically organized (Haberet al., 2000), and abnormalities in particular regionscould be related to different functional deficits. Forexample, if synaptic pathology at the level of the cau-date and/or putamen is involved in psychosis or cogni-tion, one would expect to find aberrations in the ven-tral or central regions of the striatum, respectively.Abnormalities in either the direct or indirect pathwaywould differentially affect specific downstream con-nections and have different functional consequences.Striatal patches and matrix process different types of
194 R.C. ROBERTS ET AL.

information (Gerfen, 1984, 1989; Langer and Gray-biel, 1989), and can be identified with several neuro-chemical markers (Gerfen et al., 1985; Graybiel andRagsdale, 1978; Holt et al., 1997; Presna et al., 1999).Follow-up studies analyzing the synaptic organizationin dorsal vs. ventral striatal regions, in the striosomalcompartments, on neurons in the direct vs. indirectpathways, and in other basal ganglia nuclei will benecessary to begin to elucidate the functional impactof the findings of the present study. Such studies areunder way in our laboratory.
ACKNOWLEDGMENTS
The authors thank the members of the MarylandBrain Collection: Dr. Carol Tamminga for diagnoses,Terri U’Prichard for permissions and interviews, Dr.Sami Daoud for dissections, and Drs. David Fowlerand Jack Titus (Office of the Chief Medical Examiner)for support and cooperation. We also thank SharonStilling for help with preparing the manuscript.
REFERENCES
Abi-Dargham A, Gil R, Krystal J, Baldwin R, Seibyl J, Bowers M,van Dyck CH, Charney DS, Innis RB, Laruelle M. 1998. Increasedstriatal dopamine transmission in schizophrenia: confirmation ina second cohort. Am J Psychiatry 155:761–767.
Abi-Dargham A, Rodenhiser J, Printz D, Zea-Ponce Y, Gil R, KegelesLS. 2000. Increased baseline occupancy of D2 receptors by dopa-mine in schizophrenia. Proc Natl Acad Sci USA 97:8104–8109.
Akil M, Pierri JN, Whitehead RE, Edgar CL, Mohila C, SampsonAR, Lewis DA. 1999. Lamina-specific alterations in the dopamineinnervation of the prefrontal cortex in schizophrenic subjects. AmJ Psychiatry 156:1580–1589.
Alexander GE, DeLong MR, Strick PL. 1986. Parallel organizationof functionally segregated circuits linking basal ganglia and cor-tex. Annu Rev Neurosci 9:357–381.
Alexander GE, Crutcher MD, DeLong MR. 1990. Basal ganglia-tha-lamocortical circuits: parallel substrates for motor, oculomotor,‘‘prefrontal’’ and ‘‘limbic’’ functions. Prog Brain Res 85:119–146.
Bartlett EJ, Wolkin A, Brodie JD, Laska EM, Wolf AP, Sanfil M.1991. Importance of pharmacologic control in PET studies: effectsof thiothixene and haloperidol on cerebral glucose utilization inchronic schizophrenia. Psychiatry Res 40:115–124.
Ben-Shachar D. 2002. Mitochondrial dysfunction in schizophrenia: apossible linkage to dopamine. J Neurochem 83:1241–1251.
Bokura H, Robinson RG. 1997. Long-term cognitive impairmentassociated with caudate stroke. Stroke 28:970–975.
Brand S, Rakic P. 1984. Cytodifferentiation and synaptogenesis inthe neostriatum of fetal and neonatal rhesus monkeys. AnatEmbryol 169:21–34.
Breier A, Su TP, Saunders R, Carson RE, Kolachana BS, de BartolomeisA, Weinberger DR, Weisenfeld N, Malhotra AK, Eckelman WC,Pickar D. 1997. Schizophrenia is associated with elevated amphet-amine-induced synaptic dopamine concentrations: evidence from anovel positron emission tomography method. Proc Natl Acad SciUSA 94:2569–2574.
Buchsbaum MS, Wu JC, DeLisi LE, Holcomb HH, Hazlett E,Cooper-Langston K, Kessler R. 1987. Positron emission tomogra-phy studies of basal ganglia and somatosensory cortex neurolepticdrug effects: differences between normal controls and schizo-phrenic patients. Biol Psychiatry 22:479–494.
Buchsbaum MS, Haier RJ, Potkin SG, Nuechterlein K, Bracha HS,Katz M, Lohr J, Wu J, Lottenberg S, Jerabek PA, Trenary M,Tafalla R, Reynolds C, Bunney W. 1992a. Frontostriatal disorderof cerebral metabolism in never-medicated schizophrenics. ArchGen Psychiatry 49:935–942.
Buchsbaum MS, Potkin SG, Siegel Jr BV, Lohr J, Katz M,Gottschalk LA, Gulasekaram B, Marshall JF, Lottenberg S, TengCY, Abel L, Plon L, Bunney Jr WE. 1992b. Striatal metabolic rateand clinical response to neuroleptics in schizophrenia. Arch GenPsychiatry 49:966–974.
Bunney WE, Bunney BG. 2000. Evidence for a compromised dorso-lateral prefrontal cortical parallel circuit in schizophrenia. BrainRes Rev 31:138–146.
Caplan LR, Schmahmann JD, Kase CS, Feldmann E, Baquis G,Greenberg JP, Gorelick PB, Helgason C, Hier DB. 1990. Caudateinfarcts. Arch Neurol 47:133–143.
Chakos MH, Lieberman JA, Bilder RM, Borenstein M, Lerner G,Bogerts B, Wu H, Kinon B, Ashtari M. 1994. Increase in caudatenuclei volumes of first-episode schizophrenic patients taking anti-psychotic drugs. Am J Psychiatry 151:1430–1436.
Charpier S, Deniau JM. 1997. In vivo activity-dependent plasticityat cortico-striatal connections: evidence for physiological long-term potentiation. Proc Natl Acad Sci U S A 94:7036–7040.
Chikama M, McFarland N, Amaral DG, Haber SN. 1997. Insularcortical projections to functional regions of the striatum correlatewith cortical cytoarchitectonic organization in the primate. J Neu-rosci 17:9686–9705.
Chung JW, Hassler R, Wagner A. 1977. Degeneration of two of ninetypes of synapses in the putamen after center median coagulationin the cat. Exp Brain Res 28:345–361.
Cleghorn JM, Franco S, Szechtman B, Kaplan RD, Szechtman H,Brown GM, Nahmias C, Garnett ES. 1992. Toward a brain map ofauditory hallucinations. Am J Psychiatry 149:1062–1069.
Collinson SL, Mackay CE, James AC, Quested DJ, Phillips T, Rob-erts N, Crow TJ. 2003. Brain volume, asymmetry and intellectualimpairment in relation to sex in early-onset schizophrenia. Br JPsychiatry 183:114–120.
Cote PY, Levitt P, Parent A. 1995. Distribution of limbic system-associated membrane protein immunoreactivity in primate basalganglia. Neuroscience 69:71–81.
Dao-Castellana M-H, Paillere-Martinot M-L, Hantraye P, Attar-LevyD, Remy P, Crouzel C, Artiges E, Feline A, Syrota A, Martinot JL.1997. Presynaptic dopaminergic function in the striatum of schiz-ophrenic patients. Schizophr Res 23:167–174.
DeLisi LE, Holcomb HH, Cohen RM, Pickar D, Carpenter W, Mori-hisa JM, King AC, Kessler R, Buchsbaum MS. 1985. Positronemission tomography in schizophrenic patients with and withoutneuroleptic medication. J Cereb Blood Flow Metab 5:201–206.
DiFiglia M. 1987. Synaptic organization of cholinergic neurons inthe monkey neostriatum. J Comp Neurol 255:245–258.
DiFiglia M, Aronin N. 1982. Ultrastructural features of immuno-reactive somatostatin neurons in the rat caudate nucleus. J Neu-rosci 2:1267–1274.
Dube L, Smith AD, Bolam JP. 1988. Identification of synaptic termi-nals of thalamic or cortical origin in contact with distinctmedium-size spiny neurons in the rat neostriatum. J Comp Neu-rol 267:455–471.
Eblen F, Graybiel AM. 1995. Highly restricted origin of prefrontalcortical inputs to striosomes in the macaque monkey. J Neurosci15:5999–6013.
Freund TF, Powell JF, Smith AD. 1984. Tyrosine hydroxylase-immu-noreactive boutons in synaptic contact with identified striatonig-ral neurons, with particular reference to dendritic spines. Neuro-science 13:1189–1215.
Geinisman Y, Gundersen HJG, Van Der Zee E, West MJ. 1996.Unbiased stereological estimation of the total number of synapsesin a brain region. J Neurocytol 25:805–819.
Gerfen CR. 1984. The neostriatal mosaic: compartmentalization ofcorticostriatal input and striatonigral output systems. Nature311:461–464.
Gerfen CR. 1989. The neostriatal mosaic: striatal patch-matrix organ-ization is related to cortical lamination. Science 246:385–388.
Gerfen CR, Baimbridge KG, Miller JJ. 1985. The neostriatal mosaic:Compartmental distribution of calcium-binding protein and par-valbumin in the basal ganglia of the rat and monkey. Proc NatlAcad Sci U S A 82:8780–8784.
Glantz LA, Lewis DA. 2000. Decreased dendritic spine density onprefrontal cortical pyramidal neurons in schizophrenia. Arch GenPsychiatry 57:65–73.
Graybiel AM, Ragsdale Jr CW. 1978. Histochemically distinct compart-ments in the striatum of human,monkey and cat demonstrated by ace-thycholinesterase staining. Proc Natl Acad Sci USA 75:5723–5726.
Goldman-Rakic PS. 1994. Working memory dysfunction in schizo-phrenia. J Neuropsychiatry Clin Neurosci 6:348–357.
Goldman-Rakic PS, Selemon LD. 1986. Topography of corticostriatalprojections in nonhuman primates and implications for functionalparcellation of the neostriatum. In: Jones EG, Peters A, editors.Cerebral cortex. New York: Plenum Press. p 447–466.
Gunduz H, Wu H, Ashtari M, Bogerts B, Crandall D, Robinson DG,Alvir J, Lieberman J, Kane J, Bilder R. 2002. Basal ganglia vol-umes in first-episode schizophrenia and healthy comparison sub-jects. Biol Psychiatry 51:801–808.
195STRIATAL SYNAPSES IN SCHIZOPHRENIA

Gur RE, Maany V, Mozley PD, Swanson C, Bilker W, Gur RC. 1998.Subcortical MRI volumes in neuroleptic-naıve and treatedpatients with schizophrenia. Am J Psychiatry 155:1711–1717.
Haber SN, Kunishio K, Mizobuchi M, Lynd-Balta E. 1995. The orbi-tal and medial prefrontal circuit through the primate basal gan-glia. J Neurosci 15:4851–4867.
Haber SN, Fudge JL, McFarland NR. 2000. Striatonigrostriatalpathways in primates form an ascending spiral from the shell tothe dorsolateral striatum. J Neurosci 20:2369–2382.
Harrison PJ. 1999. The neuropathology of schizophrenia: a criticalreview of the data and their interpretation. Brain 122:593–624.
Harrison PJ, Health PR, Eastwood SL, Burnet PWJ, McDonald BPearson RCA. 1995. The relative importance of premortem acido-sis and postmortem interval for human brain gene expressionstudies: sellective mRNA vulnerability and comparison with theirencoded proteins. Neurosci Lett 200:151–154.
Hasselbalch SG, Oberg G, Sorensen SA, Andersen AR, Waldemar G,Schmidt JF, Fenger K, Paulson OB. 1992. Reduced regional cere-bral blood flow in Huntington’s disease studied by SPECT. J Neu-rol Neurosurg Psychiatry 55:1018–1023.
Hassler R, Chung JW, Rinne U, Wagner A. 1978. Selective degener-ation of two out of the nine types of synapses in cat caudatenucleus after cortical lesions. Exp Brain Res 31:67–80.
Hietala J, Syvalahti E, Vuorio K, Nagren K, Lehikoinen P, Ruotsa-lainen U, Rakkolainen V, Lehtinen V, Wegelius U. 1994. StriatalD2 dopamine receptor characteristics in neuroleptic-naıve schizo-phrenic patients studied with positron emission tomography. ArchGen Psychiatry 51:116–123.
Hietala J, Syvalahti E, Vuorio K, Rakkolainen V, Bergman J, Haapar-anta M, Solin O, Kuoppamaki M, Kirvela O, Ruotsalainen V, Salo-kangas RKR. 1995. Presynaptic dopamine function in striatum ofneuroleptic-naive schizophrenic patients. Lancet 346:1130–1131.
Hietala J, Syvalahti E, Wilkman H, Vuorio K, Rakkolainen V, Berg-man J, Haaparanta M, Solin O, Kuoppamaki M, Eronen E, Ruot-salainen V, Salakangas RK. 1999. Depressive symptoms and pre-synaptic dopamine function in neuroleptic-naıve schizophrenia.Schizophr Res 35:41–50.
Holt DJ, Graybiel AM, Saper CB. 1997. Neurochemical architectureof the human striatum. J Comp Neurol 34:1–25.
Holt DJ, Herman MM, Hyde TM, Kleinman JE, Sinton CM, Ger-man DC, Hersh LB, Graybiel AM, Saper CB. 1999. Evidence for adeficit in cholinergic interneurons in the striatum in schizophre-nia. Neuroscience 94:21–31.
Hugdahl K. 2000. Lateralization of cognitive processes in the brain.Acta Psychol (Amst) 105:211–235.
Johnston NL, Cerevnak J, Shore AD, Torrey EF, Yolken RH, StanleyNeuropathology Consortium. 1997. Multivariate analysis of RNAlevels from postmortem human brains as measured by threemethods of RT-PCR. J Neurosci Methods 77:83–92.
Karry R, Klein E, Shachar DB. 2004. Mitochondrial complex I sub-units expression is altered in schizophrenia: a postmortem study.Biol Psychiatry 55:676–684.
Kemp JM, Powell TPS. 1971a. The structure of the caudate nucleusof the cat: light and electron microscopy. Philos Trans R Soc Lond(Biol) 262:383–401.
Kemp JM, Powell TPS. 1971b. The site of termination of afferentfibres in the caudate nucleus. Philos Trans R Soc Lond (Biol)262:413–427.
Kemp JM, Powell TPS. 1971c. The termination of fibres from thecerebral cortex and thalamus upon dendritic spines in the caudatenucleus: a study with the Golgi method. Philos Trans R Soc Lond(Biol) 262:429–439.
Keshavan MS, Bagwell WW, Haas GL, Sweeney JA, Schooler NR,Pettegrew JW. 1994. Changes in caudate volume with neuroleptictreatment [Letter]. Lancet 344:1434.
Keshavan MS, Rosenberg D, Sweeney JA, Pettegrew JW. 1998.Decreased caudate volume in neuroleptic-naıve psychotic patients.Am J Psychiatry 155:774–778.
Kircher TTJ, Liddle PF, Brammer MJ, Williams SCR, Murray RM,McGuire PK. 2001. Neural correlates of formal thought disorderin schizophrenia. Arch Gen Psychiatry 58:769–774.
Kita H, Kitai ST. 1990. Amygdaloid projections to the frontal cortexand the striatum in the rat. J Comp Neurol 298:40–49.
Kitai ST, Preston RJ, Bishop GA, Kocsis JD. 1979. Striatal projec-tion neurons: morphological and electrophysiological studies.In: Poirier LJ, Sourkes TL, Bedard PJ, editors. Advances in neu-rology. New York: Raven Press. p 45–51.
Kleinman JE, Hong J, Iadarola M, Govoni S, Gillin CJ. 1985. Neu-ropeptides in human brain — postmortem studies. Prog Neuro-psychopharmacol Biol Psychiatry 9:91–95.
Korpi ER, Kleinman JE, Goodman SI, Phillips I, DeLisi LE,Linnoila M, Wyatt RJ. 1986. Serotonin and 5-hydroxyindoleacetic
acid in brains of suicide victims. Comparison in chronic schizo-phrenic patients with suicide as cause of death. Arch Gen Psy-chiatry 43:594–600.
Kubota Y, Inagaki S, Kito S, Wu J-Y. 1987a. Dopaminergic axonsdirectly make synapses with GABA neurons in the rat neostria-tum. Brain Res 406:147–156.
Kubota Y, Ingaki S, Shimada S, Kito S, Eckenstein F, Tohyama M.1987b. Neostriatal cholinergic neurons receive direct synapticinputs from dopaminergic axons. Brain Res 413:179–184.
Kung L, Roberts RC. 1999. Mitochondrial pathology in human schiz-ophrenic striatum: a postmortem ultrastructural study. Synapse31:67–75.
Kung L, Conley R, Chute DJ, Smialek J, Roberts RC. 1998a. Synap-tic changes in the striatum of schizophrenic cases: a controlledpostmortem ultrastructural study. Synapse 28:125–139.
Kung L, Force M, Chute DJ, Roberts RC. 1998b. Immunocytochemi-cal localization of tyrosine hydroxylase in the human striatum: apostmortem ultrastructural study. J Comp Neurol 390:52–62.
Kunishio K, Haber SN. 1994. Primate cingulostriatal projection:limbic striatal versus sensorimotor striatal input. J Comp Neurol350:337–356.
Lahti RA, Cochrane EV, Roberts RC, Tamminga CA. 1998. [3H]-Neu-rotensin receptor densities in human postmortem tissue obtainedfrom normal and schizophrenic persons. An autoradiographicstudy. J Neural Transm 105:507–516.
Langer LF, Graybiel AM. 1989. Distinct nigrostriatal projection sys-tems innervate striosomes and matrix in the primate striatum.Brain Res 498:344–350.
Laruelle M, Abi-Dargham A, van Dyck CH, Gil R, De Souza CD,Erdos J, McCance E, Rosenblatt W, Fingado C, Zoghbi SS, Bald-win RM, Seibyl JP, Krystal JH, Charney DS, Innis RB. 1996. Sin-gle photon emission computerized tomography imaging of amphet-amine-induced dopamine release in drug free schizophrenic sub-jects. Proc Natl Acad Sci USA 93:9235–9240.
Laruelle M, Abi-Dargham A, Gil R, Kegeles L, Innis R. 1999.Increased dopamine transmission in schizophrenia: relationshipto illness phases. Biol Psychiatry 46:56–72.
LaVoie B, Parent A. 1990. Immunohistochemical study of the seroto-ninergic innervation of the basal ganglia in the squirrel monkey.J Comp Neurol 299:1–16.
Levesque M, Parent A. 1998. Axonal arborization of corticostriataland corticothalamic fibers arising from prelimbic cortex in the rat.Cereb Cortex 8:602–613.
Lewis DA, Pierri JN, Volk DW, Melchitzky DS, Woo T-UW. 1999.Altered GABA neurotransmission and prefrontal cortical dysfunc-tion in schizophrenia. Biol Psychiatry 46:616–626.
Lieberman MD. 2000. Intuition: a social cognitive neuroscienceapproach. Psychol Bull 126:109–137.
McFarland NR, Haber SN. 2002. Thalamic relay nuclei of the basalganglia form both reciprocal and nonreciprocal cortical connec-tions, linking multiple frontal cortical areas. J Neurosci 22:8117–8132.
McGuire PK, Quested DJ, Spence SA, Murray RM, Frith CD, LiddlePF. 1998. Pathophysiology of ‘‘positive’’ thought disorder in schizo-phrenia. Br J Psychiatry 173:231–235.
Mendez MF, Adams NL, Lewandowski KS. 1989. Neurobehavioralchanges associated with caudate lesions. Neurology 39:349–354.
Meshul CK, Andreassen OA, Allen C, Jorgensen HA. 1996. Correla-tion of vacuous chewing movements with morphological changesin rats following 1-year treatment with haloperidol. Psychophar-macology 125:238–247.
Nyberg S, Farde L, Halldin C. 1997. Delayed normalization of cen-tral D2 dopamine receptor availability after discontinuation ofhaloperidol decanoate. Preliminary findings. Arch Gen Psychiatry54:953–958.
Pakkenberg B. 1990. Pronounced reduction of total neuron numberin mediodorsal thalamic nucleus and nucleus accumbens in schiz-ophrenics. Arch Gen Psychiatry 47:1023–1028.
Parent A, Hazrati L-N. 1995. Functional anatomy of the basal gan-glia. I. The cortico-basal ganglia-thalamo-cortical loop. Brain ResRev 20:91–127.
Pasik P, Pasik T, DiFiglia M. 1976. Quantitative aspects of neuronalorganization in the neostriatum of the macaque monkey. In: YahrMD, editor. The basal ganglia. Research Publications of the Asso-ciation for Research in Nervous and Mental Disease. New York:Raven Press. p 57–90.
Pickel VM, Beckley SC, Joh TH, Reis DJ. 1981. Ultrastructuralimmunocytochemical localization of tyrosine hydroxylase in theneostriatum. Brain Res 225:373–385.
Pierri JN, Chaudry AS, Woo TU, Lewis DA. 1999. Alterations inchandelier neuron axon terminals in the prefrontal cortex ofschizophrenic subjects. Am J Psychiatry 156:1709–1719.
196 R.C. ROBERTS ET AL.
Powers RE. 1999. The neuropathology of schizophrenia. J Neuropa-thol Exp Neurol 58:679–690.
Presna L, Gimenenz-Amaya JM, Parent A. 1999. Chemical hetero-geneity of the striosomal compartment in the human striatum. JComp Neurol 413:603–618.
Prince JA, Blennow K, Gottfries CG, Karlsson I, Oreland L. 1999.Mitochondrial function is differentially altered in the basal gan-glia of chronic schizophrenics. Neuropsychopharmacology 21:372–379.
Resnick SM, Gur RE, Alavi A, Gur RC, Reivich M. 1988. Positronemission tomography and subcortical glucose metabolism in schiz-ophrenia. Psychiatry Res 24:1–11.
Ribak CE, Vaughn JE, Roberts E. 1979. The GABA neurons andtheir axon terminals in rat corpus striatum as demonstrated byGAD immunocytochemistry. J Comp Neurol 187:261–284.
Roberts RC. 2001. The effect of chronic olanzapine treatment onstriatal synaptic organization. Synapse 39:8–15.
Roberts RC, Knickman J. 2002. The ultrastructural organization ofthe patch matrix compartments in the human striatum. J CompNeurol 452:128–138.
Roberts RC, Kung L. 1999. The processing and use of postmortemhuman brain tissue for electron microscopy. In: Dean B, KleinmanJ, Hyde TM, editors. Using CNS tissue in psychiatric research: apractical guide. New York: Harwood Academic. p 7:127–140.
Roberts RC, Lapidus B. 2003. Ultrastructural correlates of haloperi-dol-induced oral dyskinesias in rats: a study of unlabeled andenkephalin-labeled striatal terminals. J Neural Transm 110:961–975.
Roberts RC, Gaither LA, Gao X-M, Kashyap SM, Tamminga CA.1995a. Ultrastructural correlates of haloperidol-induced oral dys-kinesias in rat striatum. Synapse 20:234–243.
Roberts RC, McCarthy KE, Du F, Ottersen OP, Okuno E, SchwarczR. 1995b. 3Hydroxyanthranilic acid oxygenase-containing astro-cytic processes surround glutamate-containing axon terminals inthe rat striatum. J Neurosci 15:1150–1161.
Roberts RC, Gaither LA, Peretti FJ, Lapidus B, Chute DJ. 1996.Synaptic organization of the human striatum: a postmortemultrastructural study. J Comp Neurol 374:523–534.
Roberts RC, Knickman JK, Conley R. 2001. Synaptic organization ofthe patch matrix compartments in postmortem striatum from peo-ple with schizophrenia and controls. Soc Neurosci Abstr 27:894.
Sadikot AF, Parent A, Francois C. 1992a. Efferent connections ofthe centromedian and parafascicular thalamic nuclei in the squir-rel monkey: A PHA-L study of subcortical projections. J CompNeurol 315:137–159.
Sadikot AF, Parent A, Smith Y, Bolam JP. 1992b. Efferent connec-tions of the centromedian and parafascicular thalamic nuclei inthe squirrel monkey: a light and electron microscopic study of thethalamostriatal projection in relation to striatal heterogeneity.J Comp Neurol 320:228–242.
Salzman S, Endicott J, Clayton P, Winokur G. 1983. Diagnosticevaluation after death (DEAD). Rockville, MD: National Instituteof Mental Health, Neuroscience Research Branch.
Scheepers FE, de Wied CC, Hulshoff Pol HE, van de Flier W,van der Linden JA, Kahn RS. 2001. The effect of clozapine on cau-date nucleus volume in schizophrenic patients previously treatedwith typical antipsychotics. Neuropsychopharmacology 24:47–54.
Selemon LD. 2001. Regionally diverse cortical pathology in schizo-phrenia: Clues to the etiology of the disease. Schizophr Bull 27:349–377.
Selemon LD, Goldman-Rakic PS. 1999. The reduced neuropilhypothesis: A circuit based model of schizophrenia. Biol Psychia-try 45:17–25.
Sharpe NA, Tepper JM. 1998. Postnatal development of excitatorysynaptic input to the rat neostriatum: an electron microscopicstudy. Neuroscience 84:1163–1175.
Shihabuddin L, Buchsbaum MS, Hazlett EA, Haznedar MM,Harvey PD, Newman A, Schnur DB, Spiegel-Cohen J, Wei T, MachacJ, Knesaurek K, Vallabhajosula S, Biren MA, Ciaravolo TM,Luu-Hsia C. 1998. Dorsal striatal size, shape, and metabolic rate innever-medicated and previously medicated schizophrenics perform-ing a verbal learning task. Arch Gen Psychiatry 55:235–243.
Simpson MD, Slater P, Royston MC, Deakin JF. 1992. Regionallyselective deficits in uptake sites for glutamate and gamma-amino-butyric acid in the basal ganglia in schizophrenia. Psychiatry Res42:273–282.
Smith Y, Parent A. 1986. Differential connections of caudate nucleusand putamen in the squirrel monkey (Saimiri sciureus). Neuro-science 18:347–371.
Smith Y, Bennett BD, Bolam JP, Parent A, Sadikot AF. 1994. Syn-aptic relationships between dopaminergic afferents and cortical orthalamic input in the sensorimotor territory of the striatum inmonkey. J Comp Neurol 344:1–19.
Smith Y, Bevan MD, Shink E, Bolam JP. 1998. Microcircuitry of thedirect and indirect pathways of the basal ganglia. Neuroscience86:353–387.
Somogyi P, Bolam JP, Smith AD. 1981. Monosynaptic cortical inputand local axon collaterals of identified striatonigral neurons. Alight and electron microscopic study using the Golgi-peroxidasetransport-degeneration procedure. J Comp Neurol 195:567–584.
Spitzer RL, Williams JB, Gibbon M, First MB. 1992. The structuredclinical interview for DSM-III-R (SCID). I. History, rationale, anddescription. Arch Gen Psychiatry 49:624–629.
Tamminga CA, Thaker GK, Buchanan R, Kirkpatrick B, Alphs LD,Chase TN, Carpenter WT. 1992. Limbic system abnormalitiesidentified in schizophrenia using positron emission tomographywith fluorodeoxyglucose and neocortical alterations with deficitsyndrome. Arch Gen Psychiatry 49:522–30.
Uranova NA. 1996. Brain synaptic plasticity in schizophrenia. VestnRoss Akad Med Nauk 4:23–29.
Uranova NA, Casanova MF, DeVaughn NM, Orlovskaya DD, Deni-sov DV. 1996. Ultrastructural alterations of synaptic contacts andastrocytes in postmortem caudate nucleus of schizophrenicpatients. Schizophr Res 22:81–83.
Uranova N, Orlovskaya D, Vikhreva O, Zimina I, Kolomeets N,Vostrikov V, Rachmanova V. 2001. Electron microscopy of oligo-dendroglia in severe mental illness. Brain Res Bull 55:597–610.
Uryu K, Butler AK, Chesselet M-F. 1999. Synaptogenesis and ultra-structural localization of the polysialylated neural cell adhesionmolecule in the developing striatum. J Comp Neurol 405:216–232.
White NM, Hiroi N. 1998. Preferential localization of self-stimula-tion sites in striosomes/patches in the rat striatum. Proc NatlAcad Sci U S A 95:6486–6491.
Wilson CJ, Groves PM. 1980. Fine structure and synaptic connec-tions of the common spiny neuron of the rat neostriatum: a studyemploying intracellular injection of horseradish peroxidase. JComp Neurol 194:599–615.
Woo T-U, Whitehead RE, Melchitzky DS, Lewis DA. 1998. A sub-class of prefrontal gamma-aminobutyric acid axon terminals areselectively altered in schizophrenia. Proc Natl Acad Sci USA95:5341–5346.
Yanagisawa N. 1996. Historical review of research on functions ofbasal ganglia. Eur Neurol 36(Suppl 1):2–8.
Young KA, Manaye KF, Liang C, Hicks PB, German DC. 2000.Reduced number of mediodorsal and anterior thalamic neurons inschizophrenia. Biol Psychiatry 47:944–953.
197STRIATAL SYNAPSES IN SCHIZOPHRENIA
Copyright © 2022 FDOKUMEN




















