
Serotherapy of B-Cell Neoplasms With Anti-B4Blocked Ricin: A Phase I Trial of Daily Bolus Infusion
11
1992 79: 576-585 Lambert and WA Blattler ML Grossbard, AS Freedman, J Ritz, F Coral, VS Goldmacher, L Eliseo, N Spector, K Dear, JM trial of daily bolus infusion Serotherapy of B-cell neoplasms with anti-B4-blocked ricin: a phase I http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requests Information about reproducing this article in parts or in its entirety may be found online at: http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprints Information about ordering reprints may be found online at: http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtml Information about subscriptions and ASH membership may be found online at: reserved. Copyright 2011 by The American Society of Hematology; all rights 900, Washington DC 20036. weekly by the American Society of Hematology, 2021 L St, NW, Suite Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published For personal use only. by guest on July 10, 2011. bloodjournal.hematologylibrary.org From
Transcript of Serotherapy of B-Cell Neoplasms With Anti-B4Blocked Ricin: A Phase I Trial of Daily Bolus Infusion
1992 79: 576-585
Lambert and WA BlattlerML Grossbard, AS Freedman, J Ritz, F Coral, VS Goldmacher, L Eliseo, N Spector, K Dear, JM trial of daily bolus infusionSerotherapy of B-cell neoplasms with anti-B4-blocked ricin: a phase I
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
reserved.Copyright 2011 by The American Society of Hematology; all rights900, Washington DC 20036.weekly by the American Society of Hematology, 2021 L St, NW, Suite Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published
For personal use only. by guest on July 10, 2011. bloodjournal.hematologylibrary.orgFrom

Serotherapy of B-Cell Neoplasms With Anti-B4-Blocked Ricin: A Phase I Trial of Daily Bolus Infusion
By Michael L. Grossbard, Arnold S. Freedman, Jerome Ritz, Felice Coral, Victor S. Goldmacher, Laura Eliseo, Neil Spector, Keith Dear, John M. Lambert, Walter A. Blattler, James A. Taylor, and Lee M. Nadler
Anti-B4-blocked Ricin (Anti-B4-bR) is an immunotoxin com- prised of the anti-B4 monoclonal antibody (MoAb) and the protein toxin “blocked ricin.” The anti44 MoAb is directed against the B-lineage-restricted CD19 antigen expressed on more than 95% of normal and neoplastic B cells. Blocked ricin is an altered ricin derivative that has its nonspecific binding eliminated by chemically blocking the galactose binding domains of the B chain. In vitro cytotoxicity studies demon- strate that the IC,, of Anti-B&bR is 2 x lo-’’ mol/L compared with 4 x lo-’’ mol/L for native ricin. A phase I dose escalation clinical trial was conducted in 25 patients with refractory B-cell malignancies. Anti-B4-bR was administered by daily I-hour bolus infusion for 5 consecutive days at doses ranging from 1 pg/kg/d t o 60 pg/kg/d. Serum levels above 1 nmol/L were achieved transiently in the majority of pa-
LTHOUGH INCREASED doses and new combina- A tions of cytotoxic therapy may result in enhanced tumor cell cytoreduction, progressive dose escalation of these agents is ultimately limited by their nonspecific end-organ toxicity. In contrast, monoclonal antibodies (Mo- Abs) directed against cell-surface antigens expressed on malignant cells have the capacity to specifically target therapy. Serotherapy with MoAbs may potentially trigger endogenous host cytotoxic mechanisms, and more impor- tantly, may provide non-cross-resistant mechanisms of tumor cell kill. To date, more than 100 patients with leukemias and lymphomas have been treated with unconju- gated MoAbs.’-‘2 Although sustained clinical responses associated with minimal systemic toxicity occasionally have been observed with several highly selected antibodies, most of these responses have been short-lived.
Because the overwhelming majority of MoAbs have had a limited capacity to mediate endogenous host effector mech- anisms, an alternative approach to therapy uses MoAbs as delivery vehicles for drugs, toxins, and radionuclides. A number of MoAb-toxin conjugates, known as immunotox- ins, have been constructed and have already proceeded through both preclinical and clinical toxicity studies.I3 In applying this concept, one approach has been to isolate and
From the Divisions of Tumor Immunology and Biostatistics, Dana-Farber Cancer Institute; the Departments of Medicine and Biostatistics, Haward Medical School, Boston; and ImmunoGen, Inc, Cambridge, MA.
Submitted July 25, 1991; accepted September 27, 1991. Supported by National Institute of Health Grants CA34183 and
CA55207. Address reprint requests to Michael L. Grossbard, MD, Division of
Tumor Immunology, Dana-Farber Cancer Institute, 44 Binney St, Boston, M A 021 15.
The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. section 1734 solely to indicate this fact. 0 1992 by The American Society of Hematology. 0006-4971 I921 7903-0004$3.OO/0
tients treated at the maximum tolerated dose of 50 pg/kg/d for 5 days for a total dose of 250 pg/kg. The dose-limiting toxicity was defined by transient, reversible grade 3 eleva- tions in hepatic transaminases, without impaired hepatic synthetic function. Minor toxicities included transient hy- poalbuminemia, thrombocytopenia, and fevers. Human anti- mouse antibody and human anti-ricin antibody were de- tected in nine patients. One complete response, two partial responses, and eight mixed or transient responses were observed. These results show the in vitro and in vivo cytotoxicity of Anti-BebR and indicate that this immuno- toxin can be administered as a daily bolus infusion for 5 days with tolerable, reversible toxicity. o 1992 by The American Society of Hematology.
conjugate the toxic A chain of ricin to MoAbs directed against differentiation antigens expressed on the surface of malignant cells.14 By isolating the toxic A chain of ricin from the B chain that mediates nonspecific binding of the toxin, it was hoped that the MoAb would carry the toxin specifically to the malignant cell surface and facilitate its internaliza- tion. A number of clinical trials exploring this approach identified tolerable and reversible nonspecific toxicities accompanying a limited number of durable response^.'^-^^ However, in separating the A chain of ricin from the B chain, not only is the nonspecific binding function deleted, but the B chain’s ability to enhance translocation of the A chain across the cell membrane has been removed.” There- fore, the selection of MoAbs for conjugation to ricin A chain is critical and the cytotoxicity of the immunotoxin is dependent on the degree to which the antigen-immuno- toxin complex is internalized.
An alternative method of avoiding nonspecific binding is to block or remove the binding domain of a toxin, hopefully preserving the enhancement of trans10cation.l~ To mini- mize nonspecificity but to retain cytotoxicity of a ricin-based immunotoxin, an altered toxin was produced by covalently blocking the two high-affinity nonspecific galactose binding sites with natural ligands.2” In an attempt to develop an immunotoxin to treat human B-cell malignancies, the anti-B4 antibody directed against. the CD19 antigen was selected because CD19 is: (1) expressed on 95% of normal and neoplastic B cells; (2) highly B-lineage restricted; (3) detected very early in B-cell ontogeny; and (4) not shed into the circulation.” The anti-B4 antibody was linked to blocked ricin thereby developing a novel immunotoxin, termed AntkB4-blocked Ricin (Anti-B4-bR). In vitro preclinical studies of this immunotoxin show that it is highly cytotoxic for B4 antigen positive cells and, more importantly, that this cytotoxicity is restricted to these cells. In this report, we describe a phase I clinical trial of Anti-B4-bR detailing pharmacokinetics, toxicity, and clinical response data in patients with relapsed B-cell leukemias and lymphomas receiving daily bolus infusions of Anti-BkbR for 5 consec- utive days.
576 Blood, Vol79, No 3 (February I ) , 1992: pp 576-585
For personal use only. by guest on July 10, 2011. bloodjournal.hematologylibrary.orgFrom

SEROTHERAPY WITH ANTI-B4-BLOCKED RICIN 577
MATERIALS AND METHODS
Anti-B4 MoAb
ously described.22,u Anti-B4 is an IgGl murine MoAb and was prepared as previ-
Blocked Ricin Native ricin was obtained from E-Y Laboratories (San Mateo,
CA). As described elsewhere, the ricin B chain was modified by covalent reaction with an activated glycopeptide to block binding sites while preserving toxic activity.*’ The glycopeptide ligand also contains a sulfhydryl groqp introduced with the reagent 2-iminothi- olane, which provides a reactive group for linking the blocked ricin to anti-B4 antibody.
Anti-BI4R Anti-BkbR was manufactured and supplied by ImmunoGen,
Inc (Cambridge, MA).Z4 Anti-B4 and blocked ricin were covalently bonded through the use of the linker molecule succinimidyl 4-(N-maleimidomethyl) cyclohexane carbovlate (SMCC) supplied by the Pierce Chemical Co (Rockford, IL). Anti-B4-bR was purified from the conjugate reaction mixture by affinity chromatog- raphy and gel filtration. Anti-B4-bR was formulated as a sterile injectable solution containing 100 kg/mL of Anti-B4-bR dissolved in phosphate-buffered saline, pH 7.3, with 1 mg/mL of human serum albumin (Immuno-US, Rochester, MI) added as a carrier. Anti-BkbR was stored at 2 to 8°C before administration. Four lots of Anti-B4-bR were used during this study (Lot nos. E001.288, E003.988, E01.1208A, E01.0410B). Anti-B4-Ricin A chain was prepared as previously described for use in cytotoxicity st~dies.’~
Cytotoxicity Assays Samples of immunotoxins were incubated with cells (Namalwa,
MOLT-4) at 37°C for 24 hours. The cells were then washed and placed into fresh medium for the determination of the surviving fraction of cells. This growth-back extrapolation assay has been extensively described by Goldmacher et al.*’
Peripheral Blood Cell Immunophenotyping Cell surface phenotypic analysis was performed on peripheral
blood mononuclear cells as previously described.*‘ Cells were examined for the expression of CD19, CD20, and CD2, using the B4, B1, and T11 MoAbs coupled to phycoerythrin (Coulter lmmunology, Hialeah, FL) at saturating binding concentrations. Isotype identical nonreactive mouse MoAbs coupled to phyco- erythrin were used as negative controls. Cell were then analyzed on an EPICS C (Coulter Electronics, Hialeah, FL) flow cytometer. The absolute numbers of B and T cells were calculated as previously described.”
Immunoperoxidase Staining Reactivity of both the anti-B4 MoAb and Anti-B4-bR was tested
against both lymphoid and nonlymphoid tissues. For tissue stain- ing, the anti-B4 concentration was 40 pg/mL and the optimal concentration of Anti-B4-bR was determined to be 10 kg/mL. lsotype identical MOPC-21 antibody was used as a control.
Patient Selection Patients were eligible for this study if they had non-T cell acute
lymphoblastic leukemia (ALL), B-cell chronic lymphocytic leuke- mia (CLL), or B-cell non-Hodgkin’s lymphoma (NHL) that had relapsed from conventional primary or salvage chemotherapy
regimens and demonstrated failure to respond to any regimens of known therapeutic benefit. Tumors were defined to be in resistant relapse if they failed to respond to standard salvage chemotherapy regimens with a 50% reduction in disease. Tumor cells from all patients were required to demonstrate reactivity with the anti-B4 or anti-B1 MoAb because it has previously been shown that tumor cells which express the B1 antigen also express the B4 antigen?2 Moreover, tumor cell reactivity with the anti-B4 antibody could only be determined in patients for whom fresh or frozen tissue was available for analysis. Patients were required to have an Eastern Cooperative Oncology Group (ECOG) performance status of 0 to 2, an expected survival of more than 2 months, and at least 3 weeks since any prior chemotherapy, radiation therapy, or major surgery. All patients were required to have a total bilirubin <2.0 mg/dL, SGOT < 90 IU, and creatinine < 2.0 mg/dL. At protocol entry, patients had a white blood cell count >3,000/mm3, hematocrit > 25%, platelets > 100,000/mm3. All patients were without clini- cally significant cardiac symptomatology and had ejection fractions greater than 40%. Patients had no clinically significant pulmonary symptomatology. All patients underwent lumbar punctures before therapy to rule out the presence of lymphomatous meningitis, which would preclude their enrollment on this protocol. All patients signed an informed consent form approved by the Institu- tional Review Board of the Dana-Farber Cancer Institute (DFCI).
Study Design Prestudy samples of blood, bone marrow, and lymph node were
obtained and analyzed for evidence of tissue involvement with tumor cells capable of binding anti-B4 or anti-B1. Documentation of all measurable disease before and after treatment was under- taken with computed tomographic (CT) scans, radioisotope scans including gallium scans and liver-spleen scans, and chest x-rays. In addition, bone marrow aspirates and biopsies were used to assess the extent of bone marrow involvement.
Eligible patients were admitted to the DFCI and received daily doses of Anti-BkbR administered as a 1-hour bolus infusion via a central venous line for 5 consecutive days. All patients received allopurinol 100 mg orally t.i.d. starting 48 hours before treatment. Patients were observed as inpatients for 24 hours after the final dose of immunotoxin. The study was designed to gradually escalate the administered dose of Anti-B4-bR until grade I11 National Cancer Institute Common Toxicity Criteria toxicity was reached. The dose limiting toxicity (DLT) was defined as the grade 111 toxicity that resulted in cessation of dose escalation. At least three patients underwent bolus infusion therapy at each dose. If there was no demonstrable grade I11 toxicity at a given dose level for all three patients, both during the infusion and 4 weeks thereafter, the next three patients were treated at the next dose level. Patients were eligible for retreatment at the same dose every 28 days if they continued to meet protocol eligibility requirements and failed to develop human anti-mouse antibody (HAMA) or human anti-ricin antibody (HARA).
Blood was drawn from each patient daily before immunotoxin infusion and samples were obtained for pharmacologic assessment and for the development of HAMA and HARA. Physical examina- tions were performed daily during therapy and side effects were elicited at that time. Patients were examined once each week in follow-up and side effects were elicited at these visits. Follow-up blood studies were obtained weekly for 4 weeks.
Pharmacology Samples were drawn for serum levels of Anti-BbbR just before
immunotoxin infusion, and at times 1, 1.5, 2, 2.5, 3, 4, 6, and 10 hours after completion of the infusion. Anti-B4-bR concentration
For personal use only. by guest on July 10, 2011. bloodjournal.hematologylibrary.orgFrom

578 GROSSBARD ET AL
in serum was determined by using two independent enzyme-linked immunosorbent assay (ELISA) methods. In addition, in patients treated at doses of Anti-B&bR >20 pg/kg/d, at the peak concentration the biologic activity of Anti-B&bR was assayed in a growth-back cytotoxicity assay and used to determine conjugate concentration by extrapolation from a standard cytotoxicity curve. All three measurements yielded similar results. The two ELISA assays were sandwich assays in which the Anti-B&bR conjugate was captured on plates coated with sheep anti-mouse IgG (Fc specific) and then assayed with either goat anti-mouse IgG conju- gated to alkaline phosphatase or rabbit anti-ricin Ig followed by goat anti-rabbit Ig Conjugated to alkaline phosphatase. A signal amplification method (Bethesda Research Laboratories, Gaithers- burg, MD) was used allowing the use of highly diluted serum samples and reducing the nonspecific background signals.
HAMA I U R A Detection HAMA and HARA were measured by established ELISA
techniques that take advantage of the multivalency of the Ig molecules. The antigens anti-B4 or blocked ricin were coated on plates to capture the specific human antiserum. Biotinylated antigen was then captured by the bound human antiserum and assayed with streptavidin conjugated to horseradish peroxidase. In both assays, the antigens were used in excess and the final signals recorded were directly proportional to the amount of absorbed specific human antibody. HAMA and HARA were considered positive if the patient’s value was greater than two standard deviations above the value for a negative control.
Response Criteria Response was assessed 4 weeks after each course of therapy. For
NHL, a complete response (CR) was defined as disappearance of all clinically evident disease and all disease noted by staging studies that persisted for a minimum of 4 weeks. For ALL and CLL, disappearance of all detectable leukemia cells from peripheral blood and bone marrow for a minimum of 4 weeks was considered a CR.
For NHL, a partial response (PR) was defined as a 50% decrease in the sum of the products of the perpendicular diameters of all measurable lesions lasting for a minimum of 4 weeks. No simulta- neous increase in the size of any other lesion or the appearance of any new lesion may occur. For ALL and CLL, a 50% decrease in the numbers of leukemia cells in peripheral blood and bone marrow is also necessary for a PR.
Stable disease was defined as no change in circulating tumor cells, bone marrow tumor cells, or lymph node masses.
Progressive disease was defined by an increase in the size of lymph node masses or an increase in the number of leukemic cells in peripheral blood or bone marrow. If some masses increased and some decreased, the response was mixed, but still scored as progression. Transient responses were defined as those partial and complete responses which persisted for less than 28 days.
RESULTS
Zn vitro cytotoxicity ofAnti-BI4R. In vitro cytotoxicity of Anti-BbbR was determined by 24-hour exposure of Nam- alwa cells, a B4-positive Burkitt’s lymphoma line, to the immunotoxin. In vitro efficacy was determined using the growth back-extrapolation assay that assesses log cell kill. Table 1 shows the IC,, values derived when Namalwa cells are exposed to either ricin, ricin A chain, Anti-B4-Ricin-A chain, blocked ricin, or Anti-B4bR for a 24-hour incuba- tion period. The IC,, for native ricin is 4 X lo-’’ mol/L.
Table 1. In Viro Cytotoxicity Studies
Toxin
IC37 IC37 Toxin Toxin (mollL) + (mollL) 30 mmollL Lactose
24-h exposure to Namalwa cells Ricin 4 x 10-12 3 x 10-9 Ricin A chain 3 x 10-7 3 x 10-7 Anti-84-ricin A chain Blocked ricin 2 x 10-8 8 x 10-8 Anti-84-blocked ricin 2 x 10-11 2 x 10-11
2.5 x 10-7
24-h exposure to Molt-4 cells Anti-84-blocked ricin 1.5 x 10-9
When ricin A chain is tested against Namalwa cells, the IC,, is 5 logs higher, indicating the importance of the B chain. Conjugation of anti-B4 to ricin A chain produced an immunotoxin that is no more cytotoxic than ricin A chain itself. Unconjugated blocked ricin is 3.5 logs less toxic to Namalwa cells than native ricin, confirming that the block- ing process substantially reduces nonspecific cytotoxicity. Finally, by conjugating anti-B4 to blocked ricin, the result- ant immunotoxin is only five-fold less cytotoxic than ricin itself. The in vitro specificity of Anti-B4-bR cytotoxicity was demonstrated by performing similar cytotoxicity studies using the B4 antigen negative T-cell leukemia line, MOLT-4. Anti-B4-bR demonstrates 2 logs greater cytotoxicity on Namalwa cells than on the BCnegative cell line.
To alleviate the concern that cytotoxicity was due to residual unblocked ricin, the above cytotoxicity studies were repeated in the presence of 30 mmol/L lactose. By adding lactose to the incubation, the IC,, should increase if immunotoxin cytotoxicity is mediated by nonspecific bind- ing to cell surface galactose residues via the ricin B chain. While the IC,, for ricin increases 3 logs in the presence of lactose, the IC,, values for both blocked ricin and Anti- B4-bR remain unchanged. Lastly, the cytotoxicity of Anti- B4-bR could be entirely reversed by the addition of excess unconjugated antibody to the incubation, such that an IC,, could no longer be determined, demonstrating that cytotox- icity was mediated through the binding of Anti-BbbR to B4 antigen on the cell surface.
Zmmunoperoxidase staining. Anti434 MoAb and Anti- B 4 b R had an identical distribution when assessed by immunoperoxidase staining (M. Borowitz, Duke University School of Medicine, personal communication, June 1989). Anti-B4-bR reacted with all tissues that had lymphoid cells as a significant component, including lymph nodes, spleen, bone marrow, and thymus. Two lymphomas tested also showed strong reactivity with Anti-B4-bR. Anti-B4bR did not react with tissues of epithelial, mesenchymal, or neuro- ectodermal origin. Within the liver, there was no reactivity with hepatocytes, bile ducts, Kupffer cells, or endothelium. Likewise, there was no reactivity with myocardium, skeletal muscle, gastrointestinal tract, breast, lung, pancreas, or ovaries. Immunoperoxidase studies showed that the anti-B4 antibody binds to astrocytes in three of four specimens tested. However, a second anti-CD19 antibody, Leu 12, did not bind to astrocytes. In all tissues tested, staining with the control antibody, MOPC-21, was absent.
For personal use only. by guest on July 10, 2011. bloodjournal.hematologylibrary.orgFrom
SEROTHERAPY WITH ANTLB4-BLOCKED RICIN 579
Preclinical studies. In vivo preclinical studies in Swiss albino mice were undertaken using intravenous bolus infusions of Anti-BbbR administered over 60 seconds at dosages ranging from 50 pglkg to 2,000 pglkg. At doses below 500 pglkg, histopathologic examination showed minimal periportal inflammation in the liver, bone marrow hyperplasia, and germinal center necrosis in spleen and lymph nodes. Moreover, at these doses no lethality was observed. When doses of Anti-BbbR of 1,000 or 2,000 pg/kg were administered, all mice died within 3 days. Histopathologic studies in these animals demonstrated multifocal hepatocellular necrosis and hemorrhage as well as generalized bone marrow, lymph node, and splenic necrosis. Subsequently, Anti-B4-bR was administered for 5 consecutive days at doses of either 40 pg/kg/d (total dose 200 pglkg) or 200 Fg/kg/d (total dose 1,000 pglkg). No lethality was seen at the lower dose and 4 of 20 mice died at the higher dose. At 200 pglkgld, histopathologic changes included multifocal hepatocellular necrosis, bone marrow and lymphoid hyperplasia, acute tubular necrosis in the kidney, and moderate to severe alveolar edema.
Similar in vivo studies were undertaken in adult cynomol- gus monkeys using both single bolus infusions of Anti- B4-bR administered over 60 seconds and daily bolus infusions administered for 5 consecutive days. Single bolus doses ranged from 50 to 1,000 pg/kg. At doses of 200 pg/kg or less, no clinical toxicity was observed while histopatho- logic examination showed mild to moderate hepatocellular vacuolation, hyperplasia of lymphoid tissues, and myeloid and erythroid hyperplasia in the bone marrow. At 500 pglkg, the monkey developed symptoms of lethargy and inappetence, and had the additional pathologic finding of superficial hemorrhages in the pancreas, heart, lungs, and kidneys. The monkey treated at 1,000 pglkg died 5 days after therapy and had similar pathologic findings to the other monkeys. When Anti-B4-bR was administered to cynomolgus monkeys in five divided daily doses at 10 pg/kg/d for 5 days, minimal multifocal hepatic necrosis, mild bone marrow hyperplasia, diffuse lymphoid hyperpla- sia, and mild hyaline deposition in renal tubules were observed. At 100 pglkgld for 5 days, similar toxicity was observed, but the changes were more pronounced. Neither dose was associated with lethal toxicity.
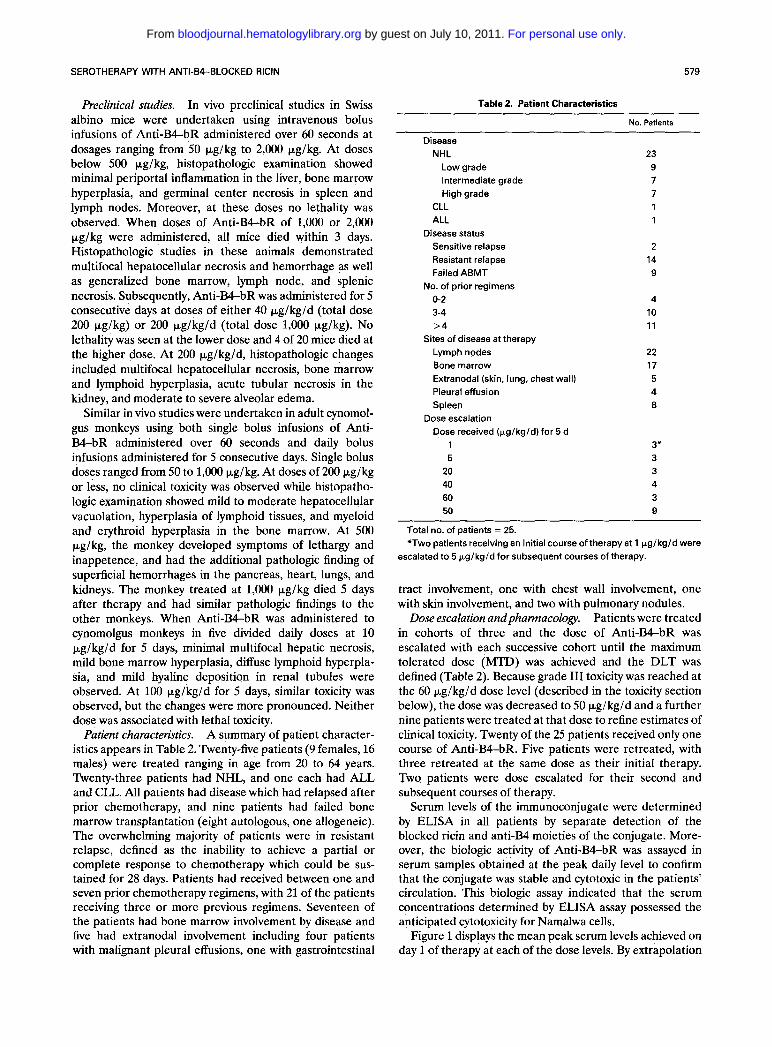
A summary of patient character- istics appears in Table 2. Twenty-five patients (9 females, 16 males) were treated ranging in age from 20 to 64 years. Twenty-three patients had NHL, and one each had ALL and CLL. All patients had disease which had relapsed after prior chemotherapy, and nine patients had failed bone marrow transplantation (eight autologous, one allogeneic). The overwhelming majority of patients were in resistant relapse, defined as the inability to achieve a partial or complete response to chemotherapy which could be sus- tained for 28 days. Patients had received between one and seven prior chemotherapy regimens, with 21 of the patients receiving three or more previous regimens. Seventeen of the patients had bone marrow involvement by disease and five had extranodal involvement including four patients with malignant pleural effusions, one with gastrointestinal
Patient charactektics.
Table 2. Patient Characteristics
No. Patients
Disease NHL
Low grade Intermediate grade High grade
CLL ALL
Sensitive relapse Resistant relapse Failed ABMT
No. of prior regimens 0-2 3-4 >4
Lymph nodes Bone marrow Extranodal (skin, lung, chest wall) Pleural effusion Spleen
Dose received (bg/kg/d) for 5 d
Disease status
Sites of disease at therapy
Dose escalation
1 5
20 40 60 50
23 9 7 7 1 1
2 14 9
4 10 11
22 17 5 4 8
3* 3 3 4 3 9
Total no. of patients = 25. *Two patients receiving an initial course of therapy at 1 pg/kg/d were
escalated to 5 bg/kg/d for subsequent courses of therapy.
tract involvement, one with chest wall involvement, one with skin involvement, and two with pulmonary nodules.
Patients were treated in cohorts of three and the dose of Anti-BbbR was escalated with each successive cohort until the maximum tolerated dose (MTD) was achieved and the DLT was defined (Table 2). Because grade I11 toxicity was reached at the 60 pg/kg/d dose level (described in the toxicity section below), the dose was decreased to 50 pg/kg/d and a further nine patients were treated at that dose to refine estimates of clinical toxicity. Twenty of the 25 patients received only one course of Anti-B4-bR. Five patients were retreated, with three retreated at the same dose as their initial therapy. Two patients were dose escalated for their second and subsequent courses of therapy.
Serum levels of the immunoconjugate were determined by ELISA in all patients by separate detection of the blocked ricin and anti-B4 moieties of the conjugate. More- over, the biologic activity of Anti-B4-bR was assayed in serum samples obtained at the peak daily level to confirm that the conjugate was stable and cytotoxic in the patients’ circulation. This biologic assay indicated that the serum concentrations determined by ELISA assay possessed the anticipated cytotoxicity for Namalwa cells.
Figure 1 displays the mean peak serum levels achieved on day 1 of therapy at each of the dose levels. By extrapolation
Dose escalation andphamzacology.
For personal use only. by guest on July 10, 2011. bloodjournal.hematologylibrary.orgFrom

580 GROSSBARD ET AL
O 1 lh 5 20 40 50
ll-l 60
Fig 1. Day 1 mean peak serum levels (nmol/L) of Anti-B4-bR as dose was escalated from 1 pg/ kg/d to 60 pg/kg/d. Levels reflect the mean peak level as derived from all patients treated at a given dose level. Serum levels on subsequent days of therapy were not signifi- cantly different from the day 1 levels. Error bars indicate standard error.
from in vitro studies, serum levels above 0.5 nmol/L would be predicted to kill up to 3 logs of cells after a 24-hour exposure to AntLB4-bR. The peak level was achieved between 1 and 2 hours after bolus administration of Anti-B4-bR. Although the peak serum levels on subse- quent days of therapy are not depicted, they did not vary significantly from the day 1 levels. As seen in Fig 1, at dosages below 20 kgIkg/d for 5 days, peak daily serum levels were below 0.5 nmol/L. At higher bolus doses of Anti-B4-bR, peak daily serum levels above 2 nmol/L were achieved. As the bolus dose was increased, the day 1 serum level generally increased despite substantial differences in the patients with respect to tumor type and tumor bulk.
Figure 2 depicts the mean serum levels achieved at various time points on day 1 of therapy in the nine patients treated at the MTD of 50 kg/kg/d. The peak serum level was achieved within 1 to 2 hours after the infusion, but
E
u, 5
3 1 T
0 2 4 6 a 10 Time (his)
Fig 2. Pharmacokinetics of A n t i - W R administration In nine patients treated at the MTD of 50 pg/kg/d. The figure depicts day 1 mean serum levels (nmol/L) of A n t i - W R over 10 hours. A similar pattern of serum levels was obtained on subsequent days of therapy and at other dose levels. Error bars indicate standard error.
decreased to levels below 0.5 nmol/L within 4 hours after the end of the infusion in six of the nine patients. A similar pattern of Anti-BkbR serum levels was achieved at all dose levels, although lower peak levels were achieved at the lower doses and the level decreased below 0.5 nmol/L in under 4 hours.
Toxicity Anti-BbbR administration was well
tolerated and patients developed few systemic symptoms. Table 3 summarizes the observed toxicities. Clinically significant toxicities were limited to hepatic toxicity and occasional hematologic toxicity, and these will be discussed in detail below. Five patients developed fevers greater than 101°F in association with therapy, but other systemic reactions including fatigue, malaise, and nausea were absent at doses below the MTD. There were no myalgias or musculoskeletal pain, nor was there evidence of rhabdomy- olysis. There were no allergic manifestations of immuno- toxin administration, including anaphylaxis, rash, or im- mune complex formation. Patients showed no evidence of cardiac toxicity on serial electrocardiograms or radionu- clide ventriculograms. Pulmonary function remained un- changed on serial pulmonary function testing. Further, there was no nephrotoxicity, proteinuria, or change in creatinine clearance after therapy.
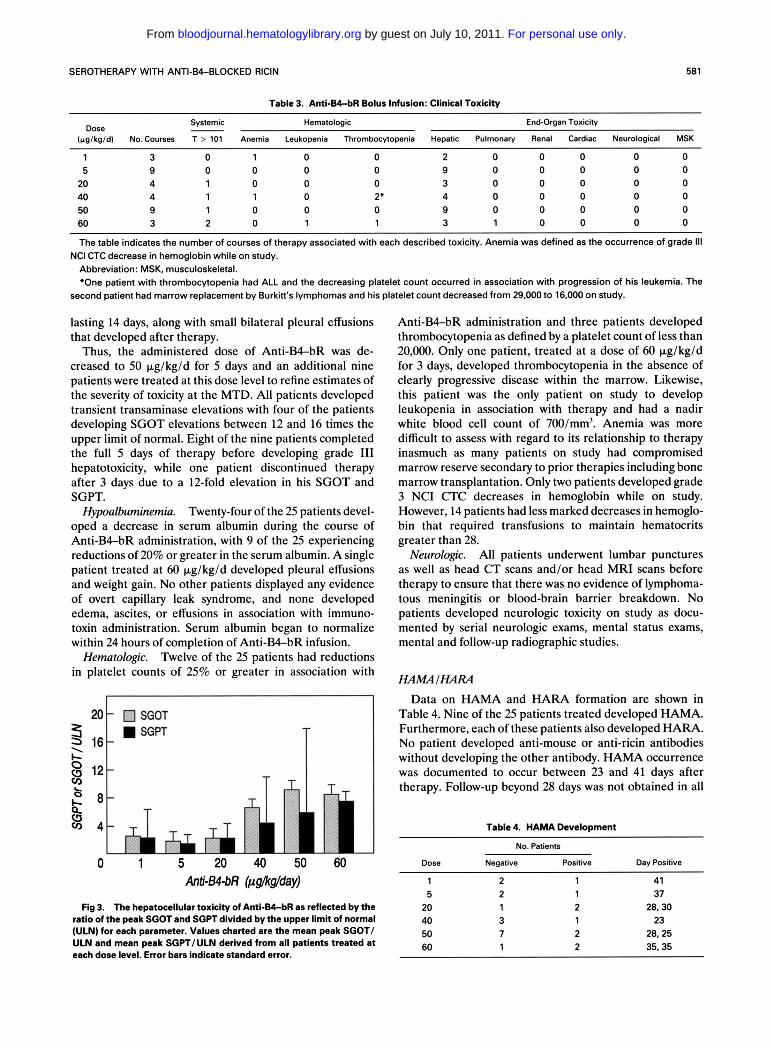
The major toxicity observed was tran- sient elevation of hepatic transaminases that began within 24 to 48 hours after the start of the bolus infusions, peaked within 48 hours of administration of the final dose, and generally resolved within 7 days after the final dose. Although hepatic transaminase were elevated in most patients on this trial, other parameters of hepatic function including prothrombin time, partial thromboplastin time, alkaline phosphatase, or bilirubin remained unchanged.
Figure 3 depicts the degree of SCOT and SGPT eleva- tions observed at the different dose levels. This is reflected as the ratio of the peak SCOT and SGPT divided by the upper limit of normal value for those parameters. The extent of transaminase elevation increased as the adminis- tered dose increased and defined the DLT.
The MTD was exceeded at 60 kg/kg/d. Three patients were treated at this dose level. The first patient completed all 5 days of therapy without significant hepatotoxicity, but died of sepsis 2 weeks after completing therapy. The second patient receiving 60 p,g/kg/d developed an SCOT elevation to 10 times the upper limit of normal and a SGPT elevation to 11 times normal on day 4 of therapy. The NCI CTC criteria define grade 111 hepatotoxicity as an elevation of SCOT and SGPT between 5 and 20 times normal, so this degree of transaminase elevation defined the DLT and established the MTD. This patient also exhibited nausea, malaise, inappetence, and low-grade fever from day 2 through day 8. By day 14, the SCOT had returned to normal range, and by day 28 the SGPT had normalized. The third patient treated at 60 pg/kg/d received just 3 days of therapy because the SCOT increased to 13.5 times normal on day 3 although the SGPT was only 8 times normal. This patient also developed thrombocytopenia and leukopenia, both
Overall toxicity.
Hepatotoxicity.
For personal use only. by guest on July 10, 2011. bloodjournal.hematologylibrary.orgFrom
SEROTHERAPY WITH ANTI-64-BLOCKED RICIN 581
Table 3. A n t i - W R Bolus Infusion: Clinical Toxicity
Systemic Hematologic End-Organ Toxicity Dose
1 3 0 1 0 0 2 0 0 0 0 0 5 9 0 0 0 0 9 0 0 0 0 0
20 4 1 0 0 0 3 0 0 0 0 0 40 4 1 1 0 2' 4 0 0 0 0 0 50 9 1 0 0 0 9 0 0 0 0 0 60 3 2 0 1 1 3 1 0 0 0 0
The table indicates the number of courses of therapy associated with each described toxicity. Anemia was defined as the occurrence of grade 111
Abbreviation: MSK, musculoskeletal. 'One patient with thrombocytopenia had ALL and the decreasing platelet count occurred in association with progression of his leukemia. The
(pgglkgld) No. Courses T > 101 Anemia Leukopenia Thrombocytopenia Hepatic Pulmonav Renal Cardiac Neurological MSK
NCI CTC decrease in hemoglobin while on study.
second patient had marrow replacement by Burkitt's lymphomas and his platelet count decreased from 29,000 to 16,000 on study.
lasting 14 days, along with small bilateral pleural effusions that developed after therapy.
Thus, the administered dose of Anti-B4-bR was de- creased to 50 p.g/kg/d for 5 days and an additional nine patients were treated at this dose level to refine estimates of the severity of toxicity at the MTD. All patients developed transient transaminase elevations with four of the patients developing SGOT elevations between 12 and 16 times the upper limit of normal. Eight of the nine patients completed the full 5 days of therapy before developing grade I11 hepatotoxicity, while one patient discontinued therapy after 3 days due to a 12-fold elevation in his SGOT and SGPT.
Twenty-four of the 25 patients devel- oped a decrease in serum albumin during the course of Anti-B4-bR administration, with 9 of the 25 experiencing reductions of 20% or greater in the serum albumin. A single patient treated at 60 p.g/kg/d developed pleural effusions and weight gain. No other patients displayed any evidence of overt capillary leak syndrome, and none developed edema, ascites, or effusions in association with immuno- toxin administration. Serum albumin began to normalize within 24 hours of completion of Anti-BbbR infusion.
Twelve of the 25 patients had reductions in platelet counts of 25% or greater in association with
Hypoalbuminemia.
Hematologic.
' 8 - k s? 4 -
0 1 5 20 40 Anti-WbR (.uslkglday)
Fig 3. The hepatocellular toxicity of A n t i - W R as reflected by the ratio of the peak SGOT and SGPT divided by the upper limit of normal (ULN) for each parameter. Values charted are the mean peak SGOT/ ULN and mean peak SGPT/ULN derived from all patients treated at each dose level. Error bars indicate standard error.
Anti-B4-bR administration and three patients developed thrombocytopenia as defined by a platelet count of less than 20,000. Only one patient, treated at a dose of 60 pg/kg/d for 3 days, developed thrombocytopenia in the absence of clearly progressive disease within the marrow. Likewise, this patient was the only patient on study to develop leukopenia in association with therapy and had a nadir white blood cell count of 700/mm3. Anemia was more difficult to assess with regard to its relationship to therapy inasmuch as many patients on study had compromised marrow reserve secondary to prior therapies including bone marrow transplantation. Only two patients developed grade 3 NCI CTC decreases in hemoglobin while on study. However, 14 patients had less marked decreases in hemoglo- bin that required transfusions to maintain hematocrits greater than 28.
Neurologic. All patients underwent lumbar punctures as well as head CT scans and/or head MRI scans before therapy to ensure that there was no evidence of lymphoma- tous meningitis or blood-brain barrier breakdown. No patients developed neurologic toxicity on study as docu- mented by serial neurologic exams, mental status exams, mental and follow-up radiographic studies.
HAMIHAM Data on HAMA and HARA formation are shown in
Table 4. Nine of the 25 patients treated developed HAMA. Furthermore, each of these patients also developed HARA. No patient developed anti-mouse or anti-ricin antibodies without developing the other antibody. HAMA occurrence was documented to occur between 23 and 41 days after therapy. Follow-up beyond 28 days was not obtained in all
Table 4. HAMA Development
No. Patients
Dose Negative Positive Day Positive
1 2 1 41 5 2 1 37
20 1 2 28,30 40 3 1 23 50 7 2 28,25 60 1 2 35,35
For personal use only. by guest on July 10, 2011. bloodjournal.hematologylibrary.orgFrom
patients, so some patients might have developed HAMAI HARA at later time points.
Five patients received repeat courses of therapy, with four patients receiving two courses of therapy and one patient receiving four courses of therapy. Only a single patient receiving more than one course of therapy ulti- mately developed HAMA after a second course. No patient was retreated after developing HAMA. There were no allergic manifestations associated with HAMAIHARA for- mation. HAMA formation was not related to dose level or disease type.
Peripheral Blood Immunophenotyping Quantitative studies of B cells and T cells were per-
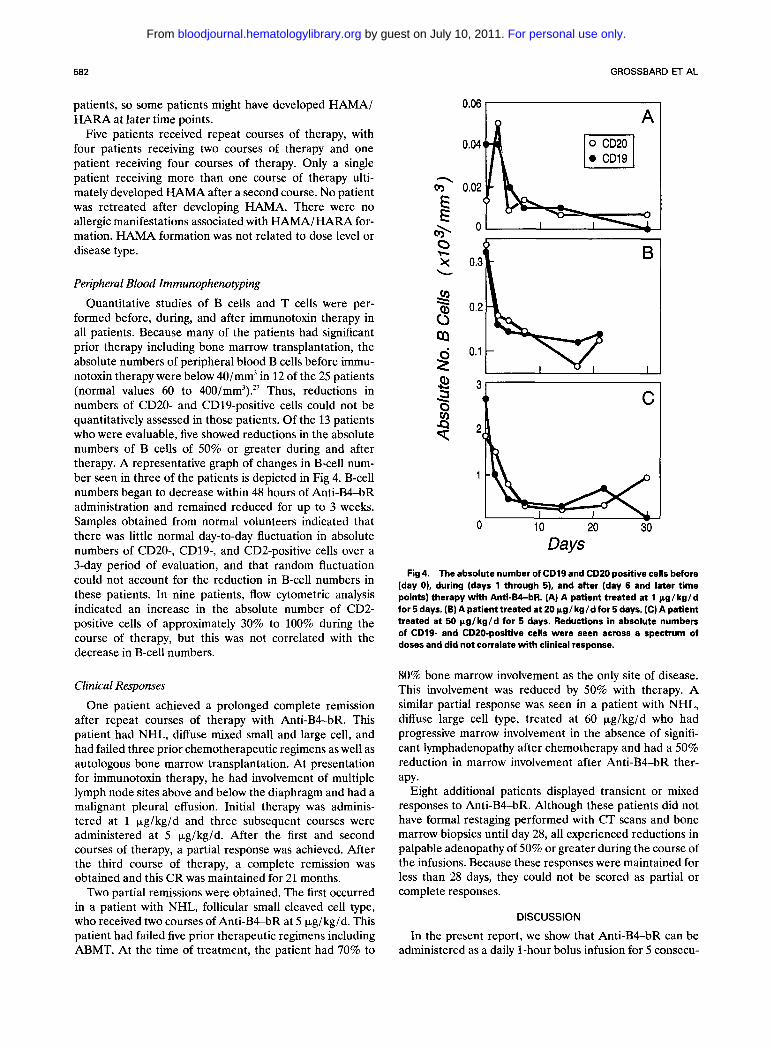
formed before, during, and after immunotoxin therapy in all patients. Because many of the patients had significant prior therapy including bone marrow transplantation, the absolute numbers of peripheral blood B cells before immu- notoxin therapy were below 40/mm3 in 12 of the 25 patients (normal values 60 to 400/mm3).” Thus, reductions in numbers of CD20- and CD19-positive cells could not be quantitatively assessed in those patients. Of the 13 patients who were evaluable, five showed reductions in the absolute numbers of B cells of 50% or greater during and after therapy. A representative graph of changes in B-cell num- ber seen in three of the patients is depicted in Fig 4. B-cell numbers began to decrease within 48 hours of Anti-B4-bR administration and remained reduced for up to 3 weeks. Samples obtained from normal volunteers indicated that there was little normal day-to-day fluctuation in absolute numbers of CD20-, CD19-, and CD2-positive cells over a 3-day period of evaluation, and that random fluctuation could not account for the reduction in B-cell numbers in these patients. In nine patients, flow cytometric analysis indicated an increase in the absolute number of CD2- positive cells of approximately 30% to 100% during the course of therapy, but this was not correlated with the decrease in B-cell numbers.
Clinical Responses One patient achieved a prolonged complete remission
after repeat courses of therapy with Anti-B4-bR. This patient had NHL, diffuse mixed small and large cell, and had failed three prior chemotherapeutic regimens as well as autologous bone marrow transplantation. At presentation for immunotoxin therapy, he had involvement of multiple lymph node sites above and below the diaphragm and had a malignant pleural effusion. Initial therapy was adminis- tered at 1 pg/kg/d and three subsequent courses were administered at 5 pglkgld. After the first and second courses of therapy, a partial response was achieved. After the third course of therapy, a complete remission was obtained and this CR was maintained for 21 months.
Two partial remissions were obtained. The first occurred in a patient with NHL, follicular small cleaved cell type, who received two courses of Anti-B&bR at 5 pglkgld. This patient had failed five prior therapeutic regimens including ABMT. At the time of treatment, the patient had 70% to
GROSSBARD
0.06 I I
0.04 h A
3 C
ET AL
Days Fig 4. The absolute number of CD19 and CD20 positive cells before
(day 0). during (days 1 through 5). and after (day 6 and later time points) therapy with Anti-B&bR. (A) A patient treated at 1 pg/kg/d for 5 days. (B) A patient treated at 20 pg/ kg/d for 5 days. (C) A patient treated at 50 Kglkgld for 5 days. Reductions in absolute numbers of CD19- and CD2O-positive cells were seen across a spectrum of doses and did not correlate with clinical response.
80% bone marrow involvement as the only site of disease. This involvement was reduced by 50% with therapy. A similar partial response was seen in a patient with NHL, diffuse large cell type, treated at 60 pg/kg/d who had progressive marrow involvement in the absence of signifi- cant lymphadenopathy after chemotherapy and had a 50% reduction in marrow involvement after Anti-B4-bR ther- apy.
Eight additional patients displayed transient or mixed responses to Anti-B4-bR. Although these patients did not have formal restaging performed with CT scans and bone marrow biopsies until day 28, all experienced reductions in palpable adenopathy of 50% or greater during the course of the infusions. Because these responses were maintained for less than 28 days, they could not be scored as partial or complete responses.
DISCUSSION
In the present report, we show that Anti-B&bR can be administered as a daily 1-hour bolus infusion for 5 consecu-
For personal use only. by guest on July 10, 2011. bloodjournal.hematologylibrary.orgFrom

SEROTHERAPY WITH ANTI-B&BLOCKED RICIN 583
tive days with tolerable, reversible toxicity. Using this administration schedule, therapeutic serum levels of Anti- B4-bR as determined from in vitro cytotoxicity studies were transiently obtained at doses greater than 20 pg/kg/d. The MTD was reached at 50 pglkgld for 5 days and the dose-limiting toxicity was defined by transient grade 3 elevations of SGOT and SGPT without impairment of hepatic synthetic function. Other systemic toxicities, with the exception of low-grade fever and thrombocytopenia, occurred rarely in patients treated at doses below the MTD. Although this phase I dose escalation trial was undertaken with the intent of defining both the DLT and MTD, several clinically significant responses were observed including one CR, two PRs, and eight transient responses. This study demonstrates the safety of administration of Anti-B4-bR by daily bolus infusion for 5 days; however, conclusions regarding efficacy must be tempered by both the refractory nature of the diseases treated and the failure to achieve sustained serum levels of the immunotoxin. Nevertheless, the presence of one complete and two partial responses was noteworthy.
In vitro studies confirm the cytotoxicity, efficacy, and specificity of Anti-B&bR. Indeed, the in vitro efficacy of Anti-BkbR is comparable with that of ricin itself. In vitro studies show that concentrations of Anti-B4-bR greater than 0.5 nmol/L can kill greater than 3 logs of Namalwa cells after a 24-hour exposure. By contrast, an Anti-B4- Ricin A chain immunoconjugate was no more cytotoxic than ricin A chain alone. This may reflect the importance of the B chain in toxin function. However, other investigators have developed equally potent anti-CD19-Ricin A chain conjugates using alternative antibodies, suggesting that the targeted epitope may also be critical in determining cyto- toxic efficiency.’’
Pharmacokinetic studies in this trial indicate that bolus administration of Anti-B4-bR results in peak serum levels within 1 to 2 hours. Furthermore, at the MTD, peak serum levels greater than 2 nmol/L were routinely achieved, albeit transiently. Thus, daily bolus infusions of Anti-B4-bR failed to yield sustained therapeutic serum levels compara- ble with the levels required to induce cytotoxicity in vitro.
The maximum tolerated dose of Anti-B4-bR as adminis- tered in this trial was 50 Fg/kg/d for 5 days or a total dose 250 pg/kg. Two of three patients receiving doses at 60 pg/kg/d were unable to complete the 5-day course of infusions due to hepatotoxicity and one patient at that dose developed evidence of capillary leak syndrome, with the development of pleural effusions. Although hypoalbumine- mia and modest reductions in platelets occurred frequently, neither of these toxicities limited dose escalation. The absence of significant pulmonary, cardiac, neurologic, and renal toxicity was striking given the extensive prior chemo- therapy received by most patients that could have caused sub-clinical damage to end organs and predisposed patients to toxicity.
The observed hepatocellular toxicity was likely due to clearance of the immunotoxin by the reticuloendothelial system, especially the liver, and probably was not attribut- able either to nonspecific antibody binding or the presence
of free blocked ricin. Indeed, immunoperoxidase staining failed to indicate binding of either the anti-B4 antibody or Anti-BkbR to hepatic tissue. Likewise, no free blocked ricin was detectable in the patients’ serum, so there was no evidence of dissociation of the immunoconjugate in serum. Moreover, this hepatotoxicity is not unique to Anti-B4-bR and has been reported with the recombinant fusion protein DAB,, interleukin-2 (IL-2) where the MTD also was defined by transient grade 3 elevations of SGOT and SGPT.29 In DAB4,,IL-2, the receptor binding domain of diphtheria toxin has been replaced by human IL-2. Like ricin, native diphtheria toxin is a two-chain toxin which includes a toxic A chain that functions by inhibiting protein synthesis. Thus, hepatotoxicity may result from hepatic uptake of the toxic moiety in both Anti-B4-bR and the diphtheria toxin fusion protein.
Several of the patients receiving Anti-BkbR developed both decreases in platelet counts and anemia while on therapy. Reductions in platelets likely were due to en- hanced platelet clearance by the reticuloendothelial sys- tem, although direct marrow toxicity cannot be entirely excluded. Likewise, mild anemia could be attributable to the phlebotomy of 250 to 350 cm3 of blood necessitated by the ancillary studies on this trial or could be due to a direct effect of the immunotoxin on the bone marrow.
The side effect profile of Anti-BkbR compares favorably with that observed in other clinical trials of ricin-based immuno toxin^.'^^"^^^-^^ Previous clinical trials using ricin-A chain immunotoxins have reported similar nonspecific toxic- ities including fever, malaise, and anorexia. Moreover, transient elevations of hepatic transaminases have been observed during therapy with other ricin-based immunotox- ins (administered at similar dosages), although they did not define the MTD.I6,’’ In contrast, capillary leak syndromes characterized by hypoalbuminemia, peripheral edema, weight gain, and effusions have been a prominent feature in patients treated with other ricin-based immunotoxins and have defined the MTD and DLT in the majority of clinical trials using these agents. While hypoalbuminemia often occurred in patients treated with Anti-BbbR, capillary leak syndrome occurred in only a single patient who was treated at a dose above the MTD. Less frequently, the MTD of other ricin A chain immunotoxins has been defined by rhabdomyolysis and renal dysfunction, neither of which occurred in this This discrepancy in side effects at the MTD may be attributable to the decreased nonspecific uptake of the Anti-BbbR by the endothelium and a concomitant reduction in endothelial damage. If higher serum levels of Anti-B4-bR had been maintained over a longer period of time, it is possible that we might have observed enhanced nonspecific toxicity including capillary leak syndromes.
Two major problems limit the efficacy of Anti-B4-bR when it is administered by daily bolus infusion. First, the development of a human immune response to both the murine MoAb and the blocked ricin toxin occurred fre- quently. In some prior therapeutic trials using murine MoAbs, the development of HAMA has proven to be a limiting factor in delivering repeat courses of therapy.,,’ In
For personal use only. by guest on July 10, 2011. bloodjournal.hematologylibrary.orgFrom

584 GROSSBARD ET AL
the case of ricin-based immunotoxins, the ricin moiety itself is antigenic and patients can also form antiricin antibodies. After HAMA or HARA develops, future courses of ther- apy with the immunotoxin might be ineffective due to rapid clearance of the immunotoxin from the blood stream. Alternatively, these antibodies might be directed against sites on the immunotoxin that do not block cytotoxicity and therefore might not abrogate immunotoxin effectiveness so that repeat courses of therapy could be admini~tered.3~ Moreover, the potential exists for the deposition of immune complexes formed between the immunotoxin and antibod- ies against it. The patients treated on this trial were felt to be significantly immunocompromised given their underly- ing diseases and prior therapy, including BMT. Neverthe- less, 9 of the 25 patients developed HAMA and HARA. Although this rate of antibody formation is lower than that previously reported for patients with solid tumors treated with ricin A chain immunotoxins, it is above the rate reported for patients with leukemias and lymphomas who have undergone immunotoxin therapy.'7.'8,33336 HAMA and HARA were noted to occur between 23 and 41 days after the completion of the infusion, which is 14 to 21 days later than generally observed with other immunotoxins. Despite the reduction that occurred in the absolute numbers of both malignant and normal B cells in several patients, concomi- tant clinically significant suppression of B-cell function as reflected by either an increased rate of infections or an
inability to produce HAMA/HARA was not observed in this study. It remains possible that a different mode of immunotoxin administration such as prolonged continuous infusion may provide a more lasting depression of B-cell numbers and function thereby further limiting HAMA and HARA development.
The second major limitation of this trial was that thera- peutic serum levels were only transiently maintained. In vitro cytotoxicity studies indicate that the log cell kill of Namalwa cells at a specific concentration of Anti-B4-bR is significantly enhanced by prolonging the time of exposure. Also, prolonged continuous infusion may increase the cytotoxicity of Anti-B4-bR for normal B cells and impair the development of human immune response to its adminis- tration. Based on these in vitro observations, we are currently conducting a dose escalation trial in which Anti- B4-bR is administered to patients with relapsed leukemias and lymphomas by 7-day constant intravenous infusion.
ACKNOWLEDGMENT
We gratefully acknowledge the advice and encouragement provided by Drs Stuart Schlossman and Baruj Benacerraf. Debo- rah Vaz was instrumental in organizing the trial and in coordinat- ing data management. We thank Jeanne Kinsella, NP, for assis- tance in data management. Lee M. Nadler and Jerome Ritz are consultants to ImmunoGen, Inc.
REFERENCES 1. Nadler LM, Stashenko P, Hardy R, Kaplan WD, Button LN,
Kufe DW, Antman KH, Schlossman SF Serotherapy of a patient with a monoclonal antibody directed against a human lymphoma- associated antigen. Cancer Res 403147,1980
2. Ritz J, Pesando JM, Sallan SE, Clawell LA, Notis-McConarty J, Rosenthal P, Schlossman SF Serotherapy of acute lymphoblastic leukemia with monoclonal antibody. Blood 58:141,1981
3. Ball ED, Bernier GM, Cornwell GG 111, McIntyre OR, O'Donnell JF, Fanger MW: Monoclonal antibodies to myeloid differentiation antigen: In vivo studies of three patients with acute myelogenous leukemia. Blood 62:1203,1983
4. Miller R, Oseroff AR, Stratte PT, Levy R: Monoclonal antibody therapeutic trials in seven patients with T-cell lymphoma. Blood 62:988,1983
5. Dillman RO, Shawler DL, Dillman JB, Royston I: Therapy of chronic lymphocytic leukemia and cutaneous T-cell lymphoma with T-101 monoclonal antibody. J Clin Oncol2:881,1984
6. Foon KA, Schroff RW, Bunn PA, Mayer D, Abrams PG, Fer M, Ochs J, Bottino GC, Sherwin SA, Carlo DJ, Herberman RB, Oldham R K Effects of monoclonal antibody therapy in patients with chronic lymphocytic leukemia. Blood 64:1085,1984
7. Meeker TC, Lowder J, Maloney DG, Miller R, Thielemans K, Warnke R, Levy R: A clinical trial of anti-idiotype therapy for B-cell malignancy. Blood 65:1349,1985
8. Hale G, Dyer MJS, Clark MR, Phillips JM, Marcus R, Riechmann L, Winter G, Waldmann H: Remission induction in non-Hodgkin lymphoma with reshaped human monoclonal anti- body CAMPATH-1H. Lancet 2:1394,1988
9. Waldmann TA, Goldman CK, Bongiovanni KF, Sharrow SO, Davey MP, Cease KB, Greenberg SJ, Longo DL: Therapy of patients with human T-cell lymphotrophic virus I-induced adult T-cell leukemia with anti-Tac, a monoclonal antibody to the receptor for interleukin-2. Blood 72:1805,1988
10. Dyer MJS, Hale G, Hayhoe FGJ, Waldman H: Effects of CAMPATH-1 antibodies in vivo in patients with lymphoid malig- nancies: Influence of antibody isotype. Blood 73:1431,1989
11. Scheinberg DA, Straus DJ, Yeh SD, Divgi C, Garin-Chesa P, Graham M, Pentlow K, Coit D, Oettgen HF, Old U: A Phase I toxicity, pharmacology, and dosimetry trial of monoclonal antibody OKB7 in patients with non-Hodgkin's lymphoma: Effects of tumor burden and antigen expression. J Clin Oncol8:792,1990
12. Scheinberg DA, Lovett D, Divgi CR, Graham MC, Berman E, Pentlow K, Feirt N, Finn RD, Clarkson BD, Gee TS, Larson SM, Oettgen H, Old LJ: A phase I trial of monoclonal antibody M195 in acute myelogenous leukemia: Specific bone marrow targeting and internalization of radionuclide. J Clin Oncol 9:478, 1991
13. FitzGerald D, Pastan I: Targeted toxin therapy for the treatment of cancer. J Natl Cancer Inst 81:1455,1989
14. Vitetta ES, Fulton RJ, May RD, Till M, Uhr JW: Redesign- ing nature's poisons to create anti-tumor reagents. Science 238: 1098,1987
15. Spitler LE, Mischak R, Scannon P: Therapy of metastatic malignant melanoma using Xomazyme Mel, a murine monoclonal anti-melanoma ricin A chain immunotoxin. Int J Rad Appl Instrum [B] 16:625,1989
16. Spitler LE, del Rio M, Khentigan A, Wedel NI, Brophy NA, Miller LL, Harkonen WS, Rosendorf LL, Lee HM, Mischak RP, Kawahata RP, Stoudemire JB, Fradkin LB, Bautista EE, Scannon PJ: Therapy of patients with malignant melanoma using a mono- clonal antimelanoma antibody-ricin A chain immunotoxin. Cancer Res 47:1717,1987
17. Byers VS, Rodvien R, Grant K, Durrant LG, Hudson KH, Baldwin RW, Scannon PJ: Phase I study of monoclonal antibody- ricin A chain immunotoxin XomaZyme-791 in patients with meta- static colon cancer. Cancer Res 49:6153,1989
For personal use only. by guest on July 10, 2011. bloodjournal.hematologylibrary.orgFrom
SEROTHERAPY WITH ANTI-B&BLOCKED RICIN 585
18. Hertler AA, Schlossman DM, Borowitz MJ, Blythman HE, Casellas P, Frankel AE: An anti-CD5 immunotoxin for chronic lymphocytic leukemia: Enhancement of cytotoxicity with human serum albumin-monensin. Int J Cancer 43215,1989
19. Youle RJ, Neville DM Jr: Kinetics of protein synthesis inactivation by ricin-anti Thy 1.1 monoclonal antibody hybrids. J Biol Chem 257:1598,1982
20. Lambert JM, McIntyre G, Gauthier MN, Zullo D, Rao V, Steeves RM, Goldmacher VS, Blattler WA: The galactose-binding sites of the cytotoxic lectin ricin can be chemically blocked in high yield with reactive ligands prepared by chemical modification of glycopeptides containing triantennaly N-linked oligosaccharides. Biochemistry 30:3234,1991
21. Anderson KC, Slaughenhoupt B, Bates MP, Pinkus G, O’Hara C, Schlossman SF, Nadler LM: Expression of human B-cell associated antigens on leukemias and lymphomas: A model of human B cell differentiation. Blood 63:1424,1984
22. Nadler LM, Anderson KC, Marti G, Bates MP, Park E, Daley JF, Schlossman SF: B4, a human B lymphocyte-associated antigen expressed on normal, mitogen-activated, and malignant B lymphocytes. J Immunol131:244,1983
23. Goldmacher VS, Scott CF, Lambert JM, McIntyre GD, Blattler WA, Collinson AR, Stewart JK, Chong LD, Cook S, Slayter HS, Beaumont E, Watkins S: Cytotoxicity of gelonin and its conjugates with antibodies is determined by the extent of their endocytosis. J Cell Physiol 141:222,1989
24. Lambert JM, Goldmacher VS, Collinson AR, Nadler LM, Blattler W A An immunotoxin prepared with blocked ricin: A natural plant toxin adapted for therapeutic use. Cancer Res 1991 (in press)
25. Goldmacher VS, Anderson J, Blattler WA, Lambert JM, Senter PD: Antibody-complement-mediated cytotoxicity is en- hanced by ribosome-inactivating proteins. J Immunol 135:3648, 1985
26. Anderson KC, Ritz J, Takvorian T, Coral F, Daley H, Gorgone BC, Freedman AS, Canellos GP, Schlossman SF, Nadler LM: Hematologic engraftment and immune reconstitution post- transplantation with anti-B1 autologous bone marrow. Blood 69597,1987
27. Pedrazzini A, Freedman AS, Andersen J, Heflin L, Ander- son K, Takvorian T, Canellos GP, Whitman J, Coral F, Ritz J, Nadler LM: Anti-B-cell monoclonal antibody-purged autologous bone marrow transplantation for B-cell non-Hodgkin’s lymphoma: Phenotypic reconstitution and B-cell function. Blood 74:2203,1989
28. Ghetie MA, May RD, Till M, Uhr JW, Ghetie V, Knowles PP, Relf M, Brown A, Wallace PM, Janossy G, Amlot P, Vitetta ES, Thorpe P: Evaluation of ricin A chain-containing immunotox- ins directed against CD19 and CD22 antigens on normal and malignant human B-cells as potential reagents for in vivo therapy. Cancer Res 48:2610,1988
29. LeMaistre CF, Von Hoff D, Meneghetti C, Adkins D, Rosenblum M, Reuben J, Deisseroth A, Parker K, Shaw J, Woodworth T: DAB,, IL-2 is effective therapy for some patients with IL-2 receptor expressing malignancies. Proc ASCO 10:280, 1991
30. Gould BJ, Borowitz MJ, Groves ES, Carter PW, Anthony D, Weiner LM, Frankel AE: Phase I study of an anti-breast cancer immunotoxin by continuous infusion: Report of a targeted toxic effect not predicted by animal studies. J Natl Cancer Inst 81:775, 1989
31. Weiner LM, O’Dwyer J, Kitson J, Comis RL, Frankel AE, Bauer RJ, Konrad MS, Groves ES: Phase I evaluation of an anti-breast carcinoma monoclonal antibody 260F9-recombinant ricin A chain immunoconjugate. Cancer Res 49:4062, 1989
32. Byers VS, Henslee PJ, Kernan NA, Blazar BR, Gingrich R, Phillips GL, LeMaistre CF, Gilliland G, Antin JH, Martin P, Tutscha PJ, Trown P, Ackerman SK, O’Reilly RJ, Scannon PJ: Use of an anti-pan T-lymphocyte ricin A chain immunotoxin in steroid- resistant acute graft-versus-host disease. Blood 75:1426,1990
33. Stone M, Amlot P, Fay J, Till M, Ghetie M, Collins R, Tong A, May R, Newman J, Clark P, Thorpe P, Uhr J, Vitetta E: Immunotoxin therapy of B cell lymphoma. Blood 76:374a, 1990 (abstr)
34. LeMaistre F, Deisseroth A, Fogel B, Meneghetti C, Ma J, Anderson M, Saria E, Lomen P, Byers V: Phase I trial of H65-RTA in patients with chronic lymphocytic leukemia. Blood 76:295a, 1990 (abstr)
35. LeMaistre CF, Rosen S, Frankel A, Kornfeld S, Saria E, Meneghetti C, Drajesk J, Fishwild D, Scannon P, Byers V Phase I trial of H65-RTA immunoconjugate in patients with T-cell lym- phoma. Blood 78:1173,1991
36. Oratz R, Speyer JL, Wernz JC, Hochster H, Meyers M, Mischak R, Spitler LE: Antimelanoma monoclonal antibody-ricin A chain immunoconjugate (XMMME-001-RTA) plus cyclophos- phamide in the treatment of metastatic malignant melanoma: Results of a phase I1 trial. J Bio Resp Mod 9:345,1990
For personal use only. by guest on July 10, 2011. bloodjournal.hematologylibrary.orgFrom



















