A dynamic prognostic model to predict survival in primary myelofibrosis: a study by the IWG-MRT...
18
doi:10.1182/blood-2007-11-121434 Prepublished online January 10, 2008; Enrica Morra and Mario Lazzarino Cecilia Del Curto, Daniela Pietra, Laura Vanelli, Paolo Bernasconi, Cristiana Pascutto, Mario Cazzola, Francesco Passamonti, Elisa Rumi, Marianna Caramella, Chiara Elena, Luca Arcaini, Emanuela Boveri, myelofibrosis A dynamic prognostic model to predict survival in post-polycythemia vera (4217 articles) Neoplasia (1739 articles) Free Research Articles (3722 articles) Clinical Trials and Observations Articles on similar topics can be found in the following Blood collections http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requests Information about reproducing this article in parts or in its entirety may be found online at: http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprints Information about ordering reprints may be found online at: http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtml Information about subscriptions and ASH membership may be found online at: digital object identifier (DOIs) and date of initial publication. the indexed by PubMed from initial publication. Citations to Advance online articles must include final publication). Advance online articles are citable and establish publication priority; they are appeared in the paper journal (edited, typeset versions may be posted when available prior to Advance online articles have been peer reviewed and accepted for publication but have not yet Copyright 2011 by The American Society of Hematology; all rights reserved. 20036. the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.org From
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of A dynamic prognostic model to predict survival in primary myelofibrosis: a study by the IWG-MRT...
doi:10.1182/blood-2007-11-121434Prepublished online January 10, 2008;
Enrica Morra and Mario LazzarinoCecilia Del Curto, Daniela Pietra, Laura Vanelli, Paolo Bernasconi, Cristiana Pascutto, Mario Cazzola, Francesco Passamonti, Elisa Rumi, Marianna Caramella, Chiara Elena, Luca Arcaini, Emanuela Boveri, myelofibrosisA dynamic prognostic model to predict survival in post-polycythemia vera
(4217 articles)Neoplasia � (1739 articles)Free Research Articles �
(3722 articles)Clinical Trials and Observations �Articles on similar topics can be found in the following Blood collections
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
digital object identifier (DOIs) and date of initial publication. theindexed by PubMed from initial publication. Citations to Advance online articles must include
final publication). Advance online articles are citable and establish publication priority; they areappeared in the paper journal (edited, typeset versions may be posted when available prior to Advance online articles have been peer reviewed and accepted for publication but have not yet
Copyright 2011 by The American Society of Hematology; all rights reserved.20036.the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom
A DYNAMIC PROGNOSTIC MODEL TO PREDICT SURVIVAL IN POST-
POLYCYTHEMIA VERA MYELOFIBROSIS.
Francesco Passamonti,1 Elisa Rumi,1 Marianna Caramella,2 Chiara Elena,1 Luca Arcaini,1
Emanuela Boveri,3 Cecilia Del Curto,1 Daniela Pietra,1 Laura Vanelli,1 Paolo Bernasconi,1
Cristiana Pascutto,1 Mario Cazzola,1 Enrica Morra,2 Mario Lazzarino1.
1Department of Hematology, Fondazione IRCCS Policlinico San Matteo, University of
Pavia, Italy; 2Department of Hematology, Ospedale Niguarda Ca’ Granda, Milan, Italy; 3
Department of Surgical Pathology, Fondazione IRCCS Policlinico San Matteo, University
of Pavia, Italy
Short title: Prognosis in post-PV MF
Correspondence: Francesco Passamonti, M.D., Department of Hematology, Fondazione
IRCCS Policlinico San Matteo, Viale Golgi 19, 27100 Pavia, Italy. E-mail:
Blood First Edition Paper, prepublished online January 10, 2008; DOI 10.1182/blood-2007-11-121434
Copyright © 2008 American Society of Hematology
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom

2
Abstract
Post-polycythemia vera myelofibrosis (post-PV MF) is a late evolution of PV. Within 647
patients with PV we found that leukocytosis (white blood cell count >15 x109/L) at
diagnosis is a risk factor for the evolution in post-PV MF. In a series of 68 patients who
developed post-PV MF median survival was 5.7 years. Hemoglobin level <10 g/dL at
diagnosis of post-PV MF was an independent risk factor for survival. The course of post-
PV MF, however, is a dynamic process that implies a progressive worsening of clinical
parameters. Using a multivariate Cox proportional hazard regression with time-dependent
covariates, we found that a dynamic score based on hemoglobin <10 g/dL, platelet count
<100 x109/L, and white blood cell count >30 x109/L is useful to predict survival at any time
from diagnosis of post-PV MF. The resulting hazard ratio of the score was 4.2 (95% CI:
2.4-7.7; P < .001), meaning a 4.2-fold worsening of survival for each risk factor acquired
during follow-up. In conclusion, leukocytosis at diagnosis of PV is a risk factor for evolution
in post-PV MF. A dynamic score based on hemoglobin level, platelet and white blood cell
count predicts survival at any time from diagnosis of post-PV MF.
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom

3
Introduction
Post-polycythemia vera myelofibrosis (post-PV MF) is a recently named condition,1 that
represents the natural evolution of patients with polycythemia vera (PV).2 The criteria
proposed for the diagnosis of post-PV MF1 set the time-point of evolution along the natural
history of the disease. Patients’ survival after transition to MF, as well as the prognostic
factors for survival, are not defined.
Post-PV MF is a delayed event in the course of PV. No risk factors for this condition have
been identified so far. In patients with PV, the 15-year risk of evolution to myelofibrosis is
estimated at 6% and the incidence is 5.1 x1000 person-years.3 A similar figure is reported
in young patients with PV.4 Patients with post-PV MF have a high rate of detection of the
JAK2 (V617F) mutation ranging from 91%5 to 100%.6 Concerning the JAK2 (V617F)
mutation burden, patients with post-PV MF have the highest proportion of mutant alleles
within patients with chronic myeloproliferative disorders (CMD).6 An abnormal stem cell
trafficking has been reported in patients with post-PV MF.7-9 JAK2 (V617F) may activate
circulating granulocytes playing a role in the constitutive mobilization of CD34+ cells into
peripheral blood. This phenomenon is particularly evident in patients with PV and post-PV
MF.6
Current treatments for patients with post-PV MF do not affect survival and are considered
palliative.10 Allogeneic hematopoietic stem-cell transplantation is the only curative
treatment for post-PV MF. Only few patients, however, have been treated with fully
ablative11 or reduced-intensity conditioning allogeneic transplantation.12 Clinical trials on
JAK2 inhibitors are still under way.13
Within a cohort of 647 patients with PV, 68 developed post-PV MF according to the criteria
of the International Working Group on Myelofibrosis Research and Treatment (IWG-
MRT).1 The aim of this study is to define survival of patients with post-PV MF and to
identify prognostic factors for survival. We developed a dynamic prognostic model useful
to predict survival at any time from diagnosis.
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom

4
Patients, materials, and methods
Patients
Within 76 consecutive patients previously diagnosed as post-PV MF, systematic revision
of clinical and histopathologic records identified 68 patients fitting diagnostic criteria for
post-PV MF established by the IWG-MRT.1 Patients were followed from 1982 to 2007 at
the Division of Hematology of the Fondazione Policlinico San Matteo, University of Pavia,
and at the Division of Hematology of the Niguarda Ca’ Granda Hospital, Milan, Italy.
Patients of the two Institutions were well matched with regard to baseline demographic
and disease characteristics. The diagnosis of PV and of primary myelofibrosis (PMF) was
made in accordance with the criteria in use at the time of first observation.14-16 The study
was approved by the institutional ethics committee of Pavia, and the procedures followed
were in accordance with the Helsinki Declaration of 1975, as revised in 2000. Samples for
molecular analysis were obtained after patient provided written informed consent.
JAK2 (V617F) mutational analysis
Granulocytes were obtained from the neutrophil fraction by osmotic lysis of red cells.
Genomic DNA was obtained by using the Puregene Blood DNA isolation kit (Gentra
Systems, Minneapolis, MN). A quantitative real-time polymerase chain reaction-based
allelic discrimination assay was used to detect the V617F mutation of JAK2 gene.17
Flow cytometric analysis of circulating CD34+ cells
Circulating CD34+ cells were enumerated by flow cytometry using a single-platform assay
as previously described,18 following the cell-gating guidelines recommended by the
International Society for Hematotherapy and Graft Engineering (ISHAGE)19 and the
subsequent modifications of the European Working Group of Clinical Cell Analysis
(EWGCCA).20 Daily instrument quality control, including fluorescence standardization,
linearity assessment, and spectral compensation were performed to ensure identical
operation from day to day.
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom

5
Statistical analysis
The cumulative probability of survival was estimated using the Kaplan-Meier method.
Comparison between survival curves was performed using the Gehan-Wilcoxon test.
Survival analysis was performed using Cox models with time-dependent covariates to
assess the effect of the variables of interest on overall survival (OS). Cox regression
models were also applied to carry out multivariate survival analyses. Standardized
mortality ratios (SMR) were calculated to compare the patients’ mortality with the mortality
of the general population in Italy. The Italian mortality rates by age, sex, and calendar year
were provided by the Istituto Nazionale di Statistica (ISTAT). Statistical analyses were
performed using Microsoft Excel 2000 (Redmond, Washington), Statistica 7.1 (Stat-Soft
Inc., Tulsa, Oklahoma), and Stata 9.2 (StataCorp, College Station, Texas).
Results
Disease information prior to post-PV MF
A total of 647 patients with PV were evaluated at the two Institutions between 1970 and
2007. The median interval between the diagnosis of PV and that of post-PV MF was 13
years (range, 2.4-29.6 years). We found that the longer the follow-up of patients with PV,
the higher the risk of developing post-PV MF (P < 0.001). During PV, myelosuppressive
agents were given to 65 (96%) of 68 patients who developed post-PV MF and to 501
(86.4%) of 579 patients who did not, while the remaining patients received phlebotomy
alone. The rate of patients receiving myelosuppression was significantly higher among
those who developed post-PV MF (P = 0.01). On the other hand, patients receiving
myelosuppression had a significantly longer follow-up than those treated with phlebotomy
alone (7.1 years and 2.9 years, respectively; P < 0.001).
To investigate potential risk factors of transformation in post-PV MF present at diagnosis of
PV, we evaluated the clinical features at diagnosis in the whole cohort of patients (n= 647).
Parameters taken into account were: age, hemoglobin level, platelet count, white blood cell
count, spleen size, (all considered as continuous numerical variables), leukocytosis (white
blood cell count >15 x109/L), calendar year at diagnosis and institutional location.
Univariate survival analysis showed that white blood cell count as numerical variable (P
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom

6
<0.001) and white blood cell count >15 x109/L (P =0.002) were significant risk factors for
transformation in post-PV MF.
Clinical features at diagnosis of post-PV MF
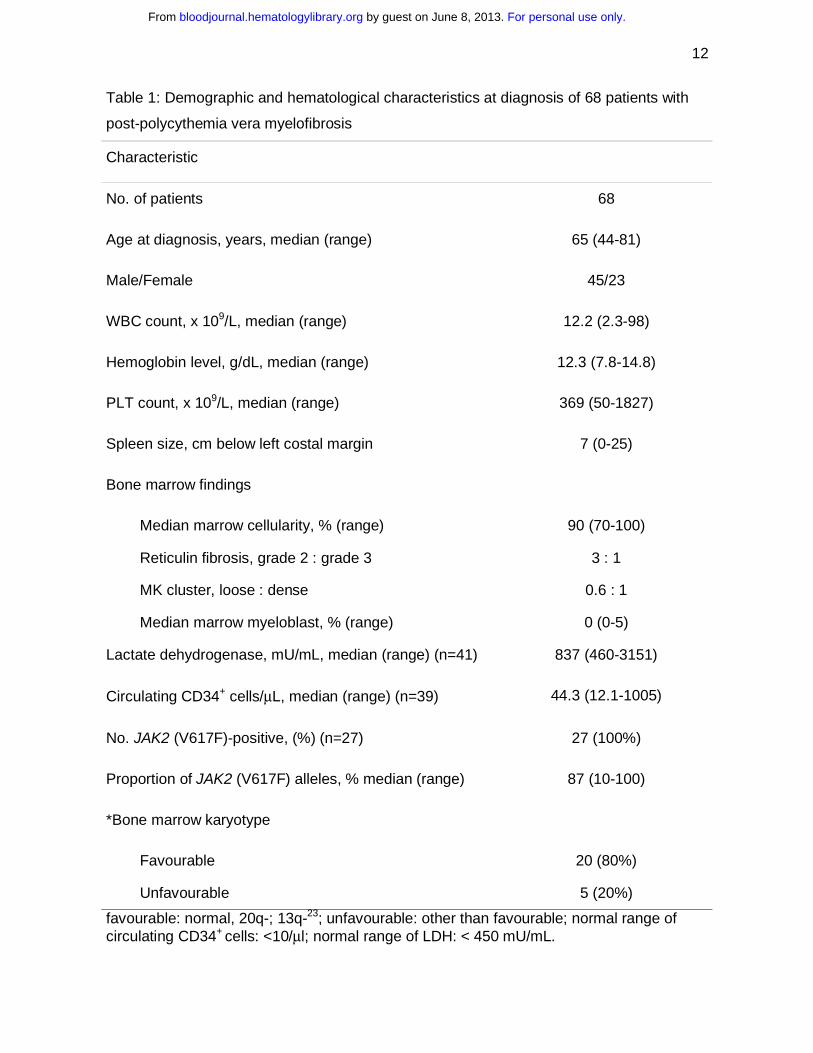
Table 1 summarizes clinical and hematological data at diagnosis of 68 patients with post-
PV MF. IWG-MRT criteria and patients’ distribution per single criterion are outlined in
Table 2. Regarding spleen, one patient underwent splenectomy before diagnosis of post-
PV MF. Another patient with no spleen enlargement at diagnosis of post-PV MF showed
anemia and leuko-erythroblastic peripheral picture in addition to required criteria. Among
47 patients studied for the JAK2 (V617F) mutation at different intervals from diagnosis, all
carried the mutation. Within 27 patients evaluated at diagnosis, 21 (78%) had more than
50% mutant alleles. In all patients, the number of circulating CD34+ cells and serum lactate
dehydrogenase (LDH) level exceeded the upper reference value (10 cells /µL for CD34+
cells and 450 mU/mL for LDH).
Disease complications and outcome
Patients with post-PV MF were observed for 181 person-years of follow-up after diagnosis
and received palliative treatments. During follow-up, the incidence of thrombosis was 42
x1000 person-years (95% CI: 19-93.5): three patients had deep venous thrombosis, two
had stroke and one myocardial infarction. Two patients had splenic infarction. The
incidence of leukemia was 50 x1000 person-years (95% CI: 26-115) and the 3-year
leukemia-free survival was 82%. Univariate analysis performed on clinical parameters at
diagnosis of post-PV MF identified as significant risk factors for leukemia the low platelet
count (P = .041) and the high circulating CD34+ cell count (P = .016). In a multivariate Cox
proportional hazard regression, only circulating CD34+ cell count retained a significant
impact on leukemia-free survival (P = .036).
The median survival of patients with post-PV MF was 5.7 years. The standardized
mortality ratio (SMR) was 6.5 (95% CI: 4.2-10.1), indicating a significantly higher mortality
for patients with post-PV MF in comparison with the general Italian population matched for
age, sex, and calendar year (P < .001). We compared the survival of patients with post-PV
MF (mortality: 11.1 per 100 person-years) with the survival of 291 patients with PMF
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom

7
(mortality: 10.1 per 100 person-years). Gehan-Wilcoxon test showed that survival of
patients with post-PV MF was not significantly different from that of patients with PMF (P =
.32). Also after adjustment for white blood cell count, hemoglobin level, platelet count,
spleen size and age in a multivariate Cox proportional hazard regression model, there was
no difference in survival between the two conditions.
Finally, to evaluate whether transformation to myelofibrosis affects the overall survival of
patients with PV, a Cox proportional hazard regression model with transformation to
myelofibrosis as time-dependent covariate was applied to the whole series of PV patients.
We found that survival of patients with PV was significantly worsened after progression to
post-PV MF (HR= 2.17; 95% CI: 1.27-3.72; P = .005). This finding retained statistical
significance also after adjustment for age, white blood cell count, hemoglobin level, platelet
count, spleen size in a multivariate Cox proportional hazard regression model.
Prognostic factors at diagnosis of post-PV MF
The parameters we evaluated at diagnosis of post-PV MF to investigate potential
predictors of survival were: age, hemoglobin level, platelet count, white blood cell count,
spleen size, year-duration of PV, serum lactate dehydrogenase level, granulocyte JAK2-
V617F mutation burden, circulating CD34+ cells (all considered as continuous numerical
variables), hemoglobin value <10 g/dL,21 white blood cell count <4 x109/L,21 white blood
cell count >30 x109/L,21 platelet count <100 x109/L,22 karyotype23 (according to the
categorization in use for PMF). Univariate survival analysis showed that hemoglobin value
<10 g/dL (P < .001) and circulating CD34+ cell count (P = .009) were significant risk factors
for survival. Multivariate Cox regression model including the parameters available in all
patients at diagnosis of post-PV MF (hemoglobin value, white blood cell count, platelet
count, spleen size, age) indicated that only hemoglobin <10 g/dL was an independent risk
factor for survival (P < .001). Using this hemoglobin level as cut-off, patients could be
stratified into two risk categories with significantly different survival: 6.6 years for those
with hemoglobin value ≥10 g/dL and 1.9 years for those with hemoglobin value <10 g/dL
(P = .0001).
Time-dependent analysis of prognostic factors
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom
8
Sixty-four patients with post-PV MF had longitudinal blood cell count measurements at
regular intervals from diagnosis. We studied this cohort of patients to assess whether
variation of hematological parameters during follow-up may further help in predicting
survival at any time from diagnosis. The acquisition of the following parameters was
studied: hemoglobin level <10 g/dL,21 platelet count <100 x109/L,22 white blood cell count
<4 x109/L or >30 x109/L.21 Modification of therapy was not involved in the acquisition of
risk factors. During follow-up of post-PV MF, hemoglobin level dropped below 10 g/dL in
17 (26%) patients, platelet count below 100 x109/L in 23 (36%), white blood cell count
below 4 x109/L in 7 (11%) and above 30 x109/L in 14 (22%).
As a first step, we evaluated univariate survival analysis with Cox regression models using
hemoglobin value <10 g/dL, platelet count <100 x109/L, white blood cell count <4 x109/L
and white blood cell count >30 x109/L as time-dependent covariates. The HRs were 5.8
(95% CI: 2.2-15.2; P < 0.001) for hemoglobin, 4.5 (95% CI: 1.67-12, P =.003) for platelets,
8.2 (95% CI: 3-22; P <.001) for white blood cells >30 x109/L, while white blood cells <4
x109/L did not significantly affect survival (P = .115). After adjustment for age in a
multivariate Cox proportional hazard regression with time-dependent covariates,
hemoglobin value <10 g/dL, platelet count <100 x109/L and white blood cell count >30
x109/L retained statistical significance on survival.
So, we defined a dynamic scoring system based on these three independent risk factors.
As the 95% CIs of the three HRs did not differ, we assigned the same weight (presence =
1; absence = 0) to the three factors. As a consequence, the resulting score can be easily
calculated by simply counting the number of risk factors acquired at any time during follow-
up. The lower risk group includes patients who never acquire risk factors during follow-up
(i.e. hemoglobin ≥10 g/dL, platelets ≥100 x109/L and white blood cells <30 x109/L).
Conversely, higher risk categories include patients with one, two, or three risk factors,
respectively. To assess the impact on survival of this dynamic scoring system, we
analyzed the score as a continuous time-dependent covariate in a Cox survival regression
model, obtaining a HR of 4.2 (95% CI: 2.4-7.7; P < .001). This implies a 4.2-fold increase
of risk when the patient acquires one risk factor at any time from the diagnosis of post-PV
MF. The time-dependent prognostic model retained statistical significance after adjustment
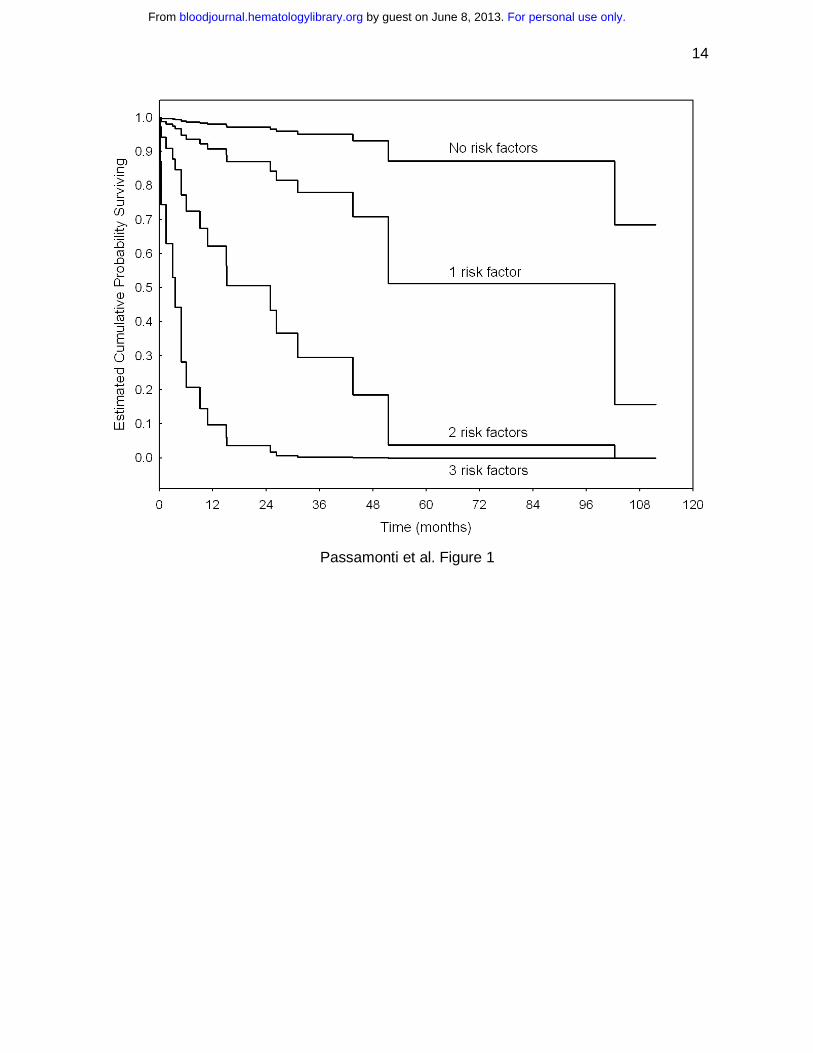
for age (HR: 6.7, 95% CI: 3-14.7; P < .001). Figure 1 exemplifies the impact of this
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom
9
dynamic prognostic model on survival, showing the estimated survival curves for the
resulting four risk groups according to the Cox time-dependent model.
Discussion
In this study we evaluated 68 patients who developed post-PV MF within a cohort of 647
patients with PV. Diagnosis of post-PV MF is based on distinctive criteria, recently
proposed by the IWG-MRT.1 These criteria combine histopathological (bone marrow
fibrosis), clinical (splenomegaly, constitutional symptoms), and hematological findings
(anemia, leukoerythroblastic peripheral blood picture).
In this series of 647 patients with PV, the analysis of risk factors that may predict
transformation to post-PV MF showed that the presence of leukocytosis (white blood cell
count > 15 x109/L) at diagnosis of PV significantly correlates with post-PV MF occurrence.
A correlation between leukocytosis and risk of acute leukemia has been recently reported
in patients with PV.24 These data indicate that PV patients with leukocytosis are at higher
risk of disease evolution. This suggests that within PV patients those with leukocytosis are
the most appropriate candidates for clinical trials with JAK2 inhibitors.
A not yet defined issue in the natural history of PV concerns whether the development of
post-PV MF has adverse prognostic implication on survival.2 Using a Cox proportional
hazard regression model, with transformation to post-PV MF as time-dependent covariate,
our data indicates a worsening of overall survival of patients with PV after fibrotic
transformation.
Studying the 68 patients of this series who developed post-PV MF, we found that all
patients with available JAK2 (V617F) status carried the mutation with a high mutational
burden. In fact, 78% of patients at diagnosis of post-PV MF had more than 50% mutant
alleles, as previously reported.6 In PMF, the rate of homozygosity for JAK2 (V617F) has
been recently reported to be 28%.25 Constitutive mobilization of CD34+ cells into peripheral
blood represents a frequent phenomenon in post-PV MF7,18and all patients tested in this
study had high circulating CD34+ cell count. Serum LDH measurement has been recently
introduced in the proposed revision of WHO criteria for CMD as additional criterion to
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom
10
diagnose PMF.1 All patients in this series with post-PV MF had high levels of serum LDH,
highlighting the clinical utility of this parameter in these patients.
Regarding disease complications of patients with post-PV MF, this study shows that
thrombosis remains a relatively frequent complication in PV patients also after transition to
myelofibrosis. Leukemia occurs with an incidence of 50 x1000 person-years and
circulating CD34+ cell count at diagnosis of post-PV MF may predict leukemia-free
survival. The frequency of leukemic transformation in patients with post-PV MF seems
higher than that reported in patients with PMF.26
In this study, the median survival of patients with post-PV MF was 5.7 years, slightly lower
than that reported in a study including patients with post-PV and post-essential
thrombocythemia MF.23 To better stratify patients, we studied potential risk factors for
survival at diagnosis of post-PV MF. Using a multivariate Cox proportional hazard
regression, we found that an hemoglobin level <10 g/dL is an independent risk factor for
survival. In fact, patients with hemoglobin value ≥10 g/dL had a median survival of 6.6
years, while those with hemoglobin value <10 g/dL had a median survival of 1.9 years.
The cut-off of 10 g/dL for hemoglobin is also considered useful in the risk stratification of
patients with PMF.21-23,27-29 Another common behaviour between patients with post-PV MF
and those with PMF is survival, that we found similar in the two conditions. Regarding the
adverse impact of unfavourable karyotype on survival reported in a prior study,23 we did
not find a significant correlation in our series of patients with post-PV MF. This may
probably reflect the small number of patients with unfavourable karyotype or the different
patient population.
The course of post-PV MF is a dynamic process during which progressive deterioration of
clinical parameters occurs. This may imply the acquisition of additional risk factors. In fact,
hemoglobin and platelets progressively tend to decrease, while leukocytes tend either to
increase or to decrease. On this ground, we developed a time-dependent scoring system
that can be used to predict survival at any time after diagnosis. According to this model,
patients are classified into a risk group at diagnosis and remain in the same group until the
acquisition of new risk factors. At this time-point patients enter a higher risk category. We
provide evidence that a dynamic scoring system based on hemoglobin <10 g/dL, platelet
count <100 x109/L and white blood cell count >30 x109/L is useful to predict survival at any
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom
11
time from diagnosis. In fact, the score predicts a 4.2-fold worsening of survival for each
risk factor acquired at any time during follow-up of post-PV MF. The survival curves
resulting from this dynamic model have to be interpreted differently from traditional survival
curves. In fact, the survival curves of the dynamic model represent an estimated survival
as long as the patient remains in the same risk group. A more accurate prediction of
survival has potential clinical implications, as these patients are JAK2 mutated and may be
candidates to clinical trials with JAK2-inhibitors.
In conclusion, this study demonstrates that patients with PV showing a white blood cell
count >15 x109/L at diagnosis have higher risk of developing post-PV MF. When patients
with PV develop post-PV MF, a dynamic prognostic model based on hemoglobin level,
platelet count, and white blood cell count may predict survival at any time after diagnosis.
Acknowledgments. This study was supported by grants from Fondazione Cariplo, Milan,
Italy; Associazione Italiana per la Ricerca sul Cancro (AIRC), Milan, Italy; Fondazione
Ferrata Storti, Pavia, Italy; Fondazione IRCCS Policlinico San Matteo, Pavia, Italy; Ministry
of University and Research, Rome, Italy.
Contributions. F.P. and M.L conceived the study, collected, analyzed, interpreted data,
wrote the paper; E.M. and M.C. analyzed and interpreted data; E.R. collected and
analyzed data; M.C., C.E., L.A., C.D. collected clinical data; E.B: performed bone marrow
evaluation; D.P. performed JAK2 mutation analysis; L.V. performed CD34+ cell count; P.B.
performed cytogenetic analysis; C.P. did statistical analyses.
The authors have no potential conflict of interest to disclose
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom
12
Table 1: Demographic and hematological characteristics at diagnosis of 68 patients with
post-polycythemia vera myelofibrosis
Characteristic
No. of patients 68
Age at diagnosis, years, median (range) 65 (44-81)
Male/Female 45/23
WBC count, x 109/L, median (range) 12.2 (2.3-98)
Hemoglobin level, g/dL, median (range) 12.3 (7.8-14.8)
PLT count, x 109/L, median (range) 369 (50-1827)
Spleen size, cm below left costal margin 7 (0-25)
Bone marrow findings
Median marrow cellularity, % (range) 90 (70-100)
Reticulin fibrosis, grade 2 : grade 3 3 : 1
MK cluster, loose : dense 0.6 : 1
Median marrow myeloblast, % (range) 0 (0-5)
Lactate dehydrogenase, mU/mL, median (range) (n=41) 837 (460-3151)
Circulating CD34+ cells/µL, median (range) (n=39) 44.3 (12.1-1005)
No. JAK2 (V617F)-positive, (%) (n=27) 27 (100%)
Proportion of JAK2 (V617F) alleles, % median (range) 87 (10-100)
*Bone marrow karyotype
Favourable 20 (80%)
Unfavourable 5 (20%)
favourable: normal, 20q-; 13q-23; unfavourable: other than favourable; normal range of circulating CD34+ cells: <10/µl; normal range of LDH: < 450 mU/mL.
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom
13
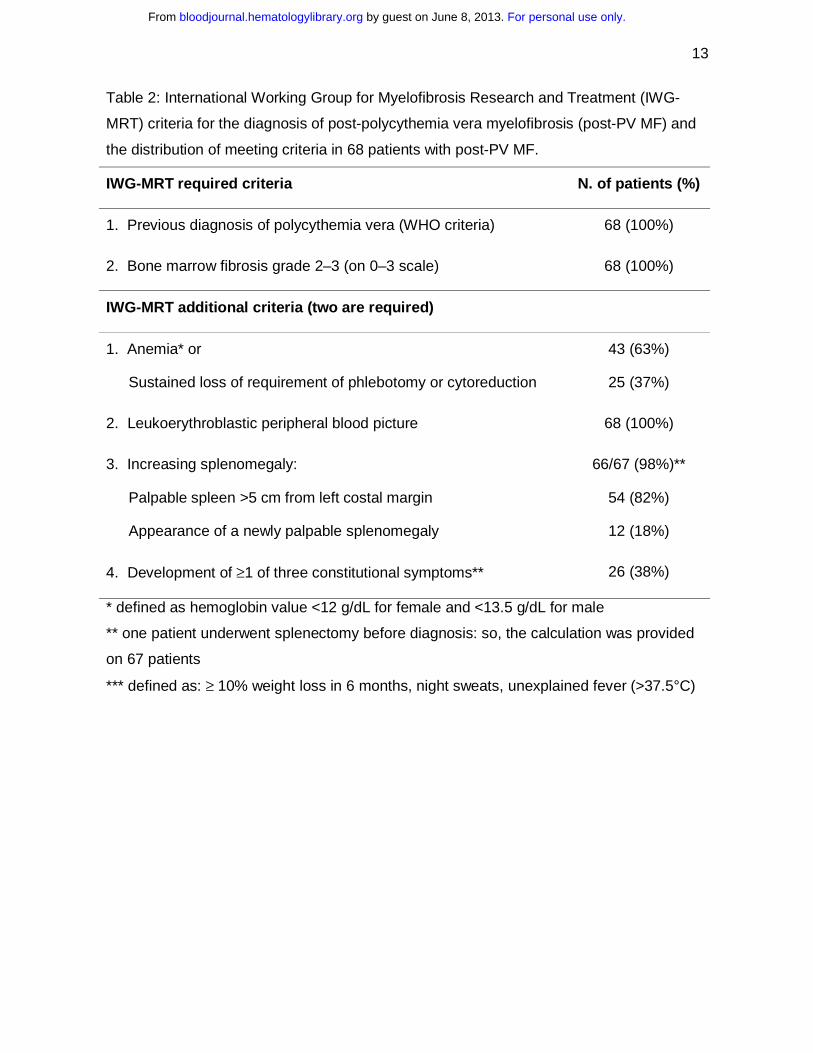
Table 2: International Working Group for Myelofibrosis Research and Treatment (IWG-
MRT) criteria for the diagnosis of post-polycythemia vera myelofibrosis (post-PV MF) and
the distribution of meeting criteria in 68 patients with post-PV MF.
IWG-MRT required criteria N. of patients (%)
1. Previous diagnosis of polycythemia vera (WHO criteria) 68 (100%)
2. Bone marrow fibrosis grade 2–3 (on 0–3 scale) 68 (100%)
IWG-MRT additional criteria (two are required)
1. Anemia* or
Sustained loss of requirement of phlebotomy or cytoreduction
43 (63%)
25 (37%)
2. Leukoerythroblastic peripheral blood picture 68 (100%)
3. Increasing splenomegaly:
Palpable spleen >5 cm from left costal margin
Appearance of a newly palpable splenomegaly
66/67 (98%)**
54 (82%)
12 (18%)
4. Development of ≥1 of three constitutional symptoms** 26 (38%)
* defined as hemoglobin value <12 g/dL for female and <13.5 g/dL for male
** one patient underwent splenectomy before diagnosis: so, the calculation was provided
on 67 patients
*** defined as: ≥ 10% weight loss in 6 months, night sweats, unexplained fever (>37.5°C)
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom
14
Passamonti et al. Figure 1
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom

15
Legend to Figure
Figure 1. Time-dependent survival estimation in post-polycythemia vera
myelofibrosis.
Survival curves estimated from the Cox proportional-hazard regression with time-
dependent covariates. According to the model, each patient is initially assigned to a risk
group and followed in that group as long as no changes in risk factors take place. The
patient is reassigned to another risk group whenever further risk factors are acquired. So,
each patient may contribute with some observation time to the estimate of survival in
different risk groups. Therefore, the upper curve includes patients who did not acquire any
risk factors during the whole follow-up (i.e. hemoglobin level ≥10 g/dL, platelet count ≥100
x109/L, white blood cell count <30 x109/L). The other curves include patients who acquired
one, two, or three factors during follow-up.
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom
16
References
1. Barosi G, Mesa RA, Thiele J, et al. Proposed criteria for the diagnosis of post-polycythemia vera and post-essential thrombocythemia myelofibrosis: a consensus statement from the international working group for myelofibrosis research and treatment. Leukemia. 2007. 2. Spivak JL. Polycythemia vera: myths, mechanisms, and management. Blood. 2002;100:4272-4290. 3. Passamonti F, Rumi E, Pungolino E, et al. Life expectancy and prognostic factors for survival in patients with polycythemia vera and essential thrombocythemia. Am J Med. 2004;117:755-761. 4. Passamonti F, Malabarba L, Orlandi E, et al. Polycythemia vera in young patients: a study on the long-term risk of thrombosis, myelofibrosis and leukemia. Haematologica. 2003;88:13-18. 5. Tefferi A, Lasho TL, Schwager SM, et al. The JAK2(V617F) tyrosine kinase mutation in myelofibrosis with myeloid metaplasia: lineage specificity and clinical correlates. Br J Haematol. 2005;131:320-328. 6. Passamonti F, Rumi E, Pietra D, et al. Relation between JAK2 (V617F) mutation status, granulocyte activation, and constitutive mobilization of CD34+ cells into peripheral blood in myeloproliferative disorders. Blood. 2006;107:3676-3682. 7. Barosi G, Viarengo G, Pecci A, et al. Diagnostic and clinical relevance of the number of circulating CD34(+) cells in myelofibrosis with myeloid metaplasia. Blood. 2001;98:3249-3255. 8. Arora B, Sirhan S, Hoyer JD, Mesa RA, Tefferi A. Peripheral blood CD34 count in myelofibrosis with myeloid metaplasia: a prospective evaluation of prognostic value in 94 patients. Br J Haematol. 2005;128:42-48. 9. Popat U, Frost A, Liu E, et al. High levels of circulating CD34 cells, dacrocytes, clonal hematopoiesis, and JAK2 mutation differentiate myelofibrosis with myeloid metaplasia from secondary myelofibrosis associated with pulmonary hypertension. Blood. 2006;107:3486-3488. 10. Tefferi A. Myelofibrosis with myeloid metaplasia. N Engl J Med. 2000;342:1255-1265. 11. Deeg HJ, Gooley TA, Flowers ME, et al. Allogeneic hematopoietic stem cell transplantation for myelofibrosis. Blood. 2003;102:3912-3918. 12. Rondelli D, Barosi G, Bacigalupo A, et al. Allogeneic hematopoietic stem-cell transplantation with reduced-intensity conditioning in intermediate- or high-risk patients with myelofibrosis with myeloid metaplasia. Blood. 2005;105:4115-4119. 13. Pardanani A. JAK2 inhibitor therapy in myeloproliferative disorders: rationale, preclinical studies and ongoing clinical trials. Leukemia. 2007. 14. Berk PD, Goldberg JD, Donovan PB, Fruchtman SM, Berlin NI, Wasserman LR. Therapeutic recommendations in polycythemia vera based on Polycythemia Vera Study Group protocols. Semin Hematol. 1986;23:132-143. 15. Vardiman JW, Harris NL, Brunning RD. The World Health Organization (WHO) classification of the myeloid neoplasms. Blood. 2002;100:2292-2302. 16. Barosi G, Ambrosetti A, Finelli C, et al. The Italian Consensus Conference on Diagnostic Criteria for Myelofibrosis with Myeloid Metaplasia. Br J Haematol. 1999;104:730-737. 17. Rumi E, Passamonti F, Pietra D, et al. JAK2 (V617F) as an acquired somatic mutation and a secondary genetic event associated with disease progression in familial myeloproliferative disorders. Cancer. 2006.
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom
17
18. Passamonti F, Vanelli L, Malabarba L, et al. Clinical utility of the absolute number of circulating CD34-positive cells in patients with chronic myeloproliferative disorders. Haematologica. 2003;88:1123-1129. 19. Keeney M, Chin-Yee I, Weir K, Popma J, Nayar R, Sutherland DR. Single platform flow cytometric absolute CD34+ cell counts based on the ISHAGE guidelines. International Society of Hematotherapy and Graft Engineering. Cytometry. 1998;34:61-70. 20. Brando B, Barnett D, Janossy G, et al. Cytofluorometric methods for assessing absolute numbers of cell subsets in blood. European Working Group on Clinical Cell Analysis. Cytometry. 2000;42:327-346. 21. Dupriez B, Morel P, Demory JL, et al. Prognostic factors in agnogenic myeloid metaplasia: a report on 195 cases with a new scoring system. Blood. 1996;88:1013-1018. 22. Dingli D, Schwager SM, Mesa RA, Li CY, Tefferi A. Prognosis in transplant-eligible patients with agnogenic myeloid metaplasia: a simple CBC-based scoring system. Cancer. 2006;106:623-630. 23. Dingli D, Schwager SM, Mesa RA, Li CY, Dewald GW, Tefferi A. Presence of unfavorable cytogenetic abnormalities is the strongest predictor of poor survival in secondary myelofibrosis. Cancer. 2006;106:1985-1989. 24. Gangat N, Strand J, Li CY, Wu W, Pardanani A, Tefferi A. Leucocytosis in polycythaemia vera predicts both inferior survival and leukaemic transformation. Br J Haematol. 2007;138:354-358. 25. Barosi G, Bergamaschi G, Marchetti M, et al. JAK2 V617F mutational status predicts progression to large splenomegaly and leukemic transformation in primary myelofibrosis. Blood. 2007;110:4030-4036. 26. Mesa RA, Li CY, Ketterling RP, Schroeder GS, Knudson RA, Tefferi A. Leukemic transformation in myelofibrosis with myeloid metaplasia: a single-institution experience with 91 cases. Blood. 2005;105:973-977. 27. Reilly JT, Snowden JA, Spearing RL, et al. Cytogenetic abnormalities and their prognostic significance in idiopathic myelofibrosis: a study of 106 cases. Br J Haematol. 1997;98:96-102. 28. Cervantes F, Pereira A, Esteve J, et al. Identification of 'short-lived' and 'long-lived' patients at presentation of idiopathic myelofibrosis. Br J Haematol. 1997;97:635-640. 29. Visani G, Finelli C, Castelli U, et al. Myelofibrosis with myeloid metaplasia: clinical and haematological parameters predicting survival in a series of 133 patients. Br J Haematol. 1990;75:4-9.
For personal use only. by guest on June 8, 2013. bloodjournal.hematologylibrary.orgFrom