Thrombosis and bleeding in myeloproliferative disorders: identification of at-risk patients with...
8
Thrombosis and bleeding in myeloproliferative disorders: identification of at-risk patients with whole blood platelet aggregation studies A. MANOHARAN, R. G EMMELL , T. B RIGHTON, S. D UNKLEY, K. L OPEZ AND P. K YLE Department of Clinical Haematology, St George Hospital, Kogarah, New South Wales, Australia Received 9 November 1998; accepted for publication 16 February 1999 Summary. Seventy-five patients with chronic myelo- proliferative disorders were studied to investigate platelet function by simultaneous measurement of platelet aggrega- tion by the impedance method and ATP dense granule release using a whole blood platelet lumi-aggregometer, in an attempt to identify patients at risk for thrombosis and bleeding. Thirty-nine patients had at least one abnormal result indicating platelet hyperactivity (i.e. impedance or release with one agonist being above the reference range); 16 patients had platelet hypoactivity (i.e. at least one result was below the reference range), whilst 14 had co-existence of hyper- and hypoactivity. Six patients had normal results. 20/ 53 patients with platelet hyperactivity (alone or mixed) had a positive history of venous and/or arterial thrombosis; in comparison, only two of the other 22 patients had a positive history. During a median follow-up of 33 months, nine patients with and one patient without platelet hyperactivity respectively developed new thrombotic events before the addition of specific therapy. A total of 50 patients with and eight patients without platelet hyperactivity respectively received specific treatment including aspirin and/or cyto- toxic therapy. All but one elderly patient with platelet hyperactivity have remained free of new thrombotic events on specific therapy. Two of the 17 patients with platelet hypoactivity had major clinical bleeding. These observations highlight the need to test platelets for hyper- as well as hypo-function and suggest a useful role for routine whole blood platelet aggregation studies to identify the patients at risk for thrombosis or bleeding. Keywords: myeloproliferative disorders, platelet studies. Bleeding and thrombosis are common causes of morbidity and mortality in patients with myeloproliferative disorders (MPD): polycythaemia vera (PV), essential thrombo- cythaemia (ET), chronic granulocytic leukaemia (CGL) and idiopathic myelofibrosis (IMF) (Schafer, 1984). Thrombotic complications in patients with MPD may involve the arterial and/or the venous system. Most arterial thrombotic events tend to involve the cerebrovascular, peripheral vascular, coronary arterial or the microvascular systems (Michiels et al, 1985, 1993; Arboix et al, 1995; Schafer, 1996; Landolfi et al, 1997). Venous thrombosis occurs in 25–40% of patients and may involve large vessels such as the portal vein and inferior vena cava (Randi et al, 1991; Gruppo Italiano Studio Policitemia, 1995; Johnson et al, 1995). Age over 60 years, previous history of thrombosis, associated cardiovascular risk factors (e.g. smoking, hyperlipidaemia) and uncontrolled thrombocytosis have been identified as risk factors for thrombosis (Cortelazzo et al, 1995; Schafer, 1996; Landolfi et al, 1997). Neither the degree of thrombocytosis nor any specific platelet function abnormality has been shown to identify patients who are at risk for thrombotic complications. Further, injudicious use of aspirin and other non-steroidal anti-inflammatory agents has been recognized as a risk factor for bleeding (Schafer, 1996; Landolfi et al, 1997). Commonly reported bleeding manifestations in MPD include easy bruising, epistaxis and gingival bleeding. Major haemorrhages, mostly gastro- intestinal, are rare but have been reported in patients receiving high doses of aspirin (Tartaglia et al, 1986; Schafer, 1996; Landolfi et al, 1997). A very high platelet count (i.e. >1000 × 10 9 /l) has been correlated with a bleeding tendency (van Genderen & Michiels, 1994). As in the case of patients at risk for thrombosis, in-vitro platelet function studies have generally failed to identify patients who are at risk for bleeding (Schafer, 1996; Landolfi et al, 1997). British Journal of Haematology , 1999, 105, 618–625 618 q 1999 Blackwell Science Ltd Correspondence: Professor A. Manoharan, Department of Clinical Haematology, St George Hospital, Kogarah, NSW 2217, Australia.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Thrombosis and bleeding in myeloproliferative disorders: identification of at-risk patients with...

Thrombosis and bleeding in myeloproliferative disorders:identification of at-risk patients with whole bloodplatelet aggregation studies
A. MANOHARAN, R. GEMMELL, T. BRIGHTON, S. DUNKL EY, K. LOP EZ AND P. KYLE
Department of Clinical Haematology, St George Hospital, Kogarah, New South Wales, Australia
Received 9 November 1998; accepted for publication 16 February 1999
Summary. Seventy-five patients with chronic myelo-proliferative disorders were studied to investigate plateletfunction by simultaneous measurement of platelet aggrega-tion by the impedance method and ATP dense granulerelease using a whole blood platelet lumi-aggregometer, inan attempt to identify patients at risk for thrombosis andbleeding.
Thirty-nine patients had at least one abnormal resultindicating platelet hyperactivity (i.e. impedance or releasewith one agonist being above the reference range); 16patients had platelet hypoactivity (i.e. at least one result wasbelow the reference range), whilst 14 had co-existence ofhyper- and hypoactivity. Six patients had normal results. 20/53 patients with platelet hyperactivity (alone or mixed) hada positive history of venous and/or arterial thrombosis; incomparison, only two of the other 22 patients had a positive
history. During a median follow-up of 33 months, ninepatients with and one patient without platelet hyperactivityrespectively developed new thrombotic events before theaddition of specific therapy. A total of 50 patients with andeight patients without platelet hyperactivity respectivelyreceived specific treatment including aspirin and/or cyto-toxic therapy. All but one elderly patient with platelethyperactivity have remained free of new thrombotic eventson specific therapy. Two of the 17 patients with platelethypoactivity had major clinical bleeding.
These observations highlight the need to test platelets forhyper- as well as hypo-function and suggest a useful role forroutine whole blood platelet aggregation studies to identifythe patients at risk for thrombosis or bleeding.
Keywords: myeloproliferative disorders, platelet studies.
Bleeding and thrombosis are common causes of morbidityand mortality in patients with myeloproliferative disorders(MPD): polycythaemia vera (PV), essential thrombo-cythaemia (ET), chronic granulocytic leukaemia (CGL) andidiopathic myelofibrosis (IMF) (Schafer, 1984).
Thrombotic complications in patients with MPD mayinvolve the arterial and/or the venous system. Most arterialthrombotic events tend to involve the cerebrovascular,peripheral vascular, coronary arterial or the microvascularsystems (Michiels et al, 1985, 1993; Arboix et al, 1995;Schafer, 1996; Landolfi et al, 1997). Venous thrombosisoccurs in 25–40% of patients and may involve large vesselssuch as the portal vein and inferior vena cava (Randi et al,1991; Gruppo Italiano Studio Policitemia, 1995; Johnsonet al, 1995). Age over 60 years, previous history ofthrombosis, associated cardiovascular risk factors (e.g.
smoking, hyperlipidaemia) and uncontrolled thrombocytosishave been identified as risk factors for thrombosis (Cortelazzoet al, 1995; Schafer, 1996; Landolfi et al, 1997). Neither thedegree of thrombocytosis nor any specific platelet functionabnormality has been shown to identify patients who are atrisk for thrombotic complications. Further, injudicious use ofaspirin and other non-steroidal anti-inflammatory agentshas been recognized as a risk factor for bleeding (Schafer,1996; Landolfi et al, 1997). Commonly reported bleedingmanifestations in MPD include easy bruising, epistaxis andgingival bleeding. Major haemorrhages, mostly gastro-intestinal, are rare but have been reported in patientsreceiving high doses of aspirin (Tartaglia et al, 1986; Schafer,1996; Landolfi et al, 1997). A very high platelet count (i.e.>1000 × 109/l) has been correlated with a bleeding tendency(van Genderen & Michiels, 1994). As in the case of patientsat risk for thrombosis, in-vitro platelet function studies havegenerally failed to identify patients who are at risk forbleeding (Schafer, 1996; Landolfi et al, 1997).
British Journal of Haematology, 1999, 105, 618–625
618 q 1999 Blackwell Science Ltd
Correspondence: Professor A. Manoharan, Department of ClinicalHaematology, St George Hospital, Kogarah, NSW 2217, Australia.

619Thrombosis and Bleeding in MPD
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 618–625
The majority of previous studies have used conventionaloptical platelet aggregation performed on platelet-richplasma as described by Born & Hume (1967). Hyperaggreg-ability is not readily assessed by this method, and over-whelmingly these studies report hypoactive platelets andlittle clinical correlation. In this prospective study we haveinvestigated platelet function by simultaneous measurementof platelet aggregation and ATP dense granule release bywhole blood platelet lumi-aggregometry, in an attempt toidentify the patients at risk and, if possible, prevent majorbleeding and thrombotic events.
MATERIALS AND METHODS
Patients. 75 patients with various MPD from a singleinstitution (St George Hospital, Sydney) were entered intothe study from December 1993 (when whole blood plateletlumi-aggregometry became available) to November 1997.The diagnosis of MPD was made by standard criteria onfindings made by examination of their peripheral blood, bonemarrow and related laboratory investigations (Berlin, 1975;Laszlo, 1975; Berk et al, 1986). A diagnosis of PV was madeby demonstration of a true erythrocytosis by blood volumestudies and compatible blood and bone marrow findings asdescribed by the Polycythaemia Vera Study Group (Berk et al,1986). The diagnosis of CML was made by the demonstra-tion of Philadelphia chromosome positivity and compatiblehaematological findings in peripheral blood and bonemarrow. A diagnosis of ET was made with peripheralthrombocytosis, characteristic marrow features with stain-able marrow iron stores as described by Murphy et al (1997).A diagnosis of IMF was made by characteristic marrowfeatures (fibrosis and/or proliferation) with splenomegaly, acompatible blood film (leucoerythroblastic with teardroppoikilocytes), and the absence of other causes of myelo-fibrosis (Silverstein, 1983). Some patients were diagnosedwith an unclassifiable MPD. These patients had featurescompatible with MPD (persistent peripheral blood cytosiswithout an obvious cause, organomegaly, hypercellularmarrow with morphologic features of MPD) yet neitherfulfilled the above-described criteria for a particular MPD, ora relevant investigation (e.g. karyotype, blood volume study)was not obtained before therapy was commenced. Allpatients were reviewed (usually monthly) within theDepartment of Clinical Haematology. At each follow-upvisit a clinical history with specific reference to thromboticor bleeding symptoms, a physical examination and relevantpathology was performed. The treatment of individualpatients varied according to their type of MPD, andtheir treating Haematologist. Whole blood platelet lumi-aggregometry (WBPA) was performed at time of diagnosis ofMPD in 32 patients, and a mean of 39 months (range 2–224months) after diagnosis in 43 patients.
Sample collection. Venous blood was collected under lighttourniquet through 19 gauge needles into vacutainers (BectonDickinson). A 3 ml di-potassium EDTA (1·5 mg/ml) samplewas collected first followed by three 4·5 ml tri-sodium citrate(0·109 M) vacutainers. The collection was performed early inthe morning following a light breakfast. All subjects were
required to have not ingested aspirin or other non-steroidalanti-inflammatory agents for at least 10 d, no garlic orchinese food for 2 d, and no alcohol for 24 h. Any othermedication was noted and checked for effect on plateletfunction. Automated cell counts were performed on theEDTA sample tube (CellDyne, Abbott Australia), and thecitrate tubes were used for whole blood platelet lumi-aggregometry studies. Testing on all samples was completedwithin 2 h of collection.
Whole blood platelet lumi-aggregometry (WBPA). Plateletaggregation (measured as the increase in impedance)and release were simultaneously measured using a wholeblood platelet lumi-aggregometer (Model 560, ChronologCorporation, Haverton, Pa., U.S.A.) according to themanufacturer’s instructions. The citrate tubes were thor-oughly mixed by gentle inversion before dispensing 450 ml ofcitrated whole blood into seven cuvettes each containing450 ml of normal saline (Baxter 0·9% Sodium ChlorideSolution for Irrigation) and a disposable siliconized stir bar,and 900 ml of citrated whole blood into an eighth cuvettecontaining only a disposable siliconized stir bar. The tubeswere immediately capped, identified by marking pencil, andwarmed at 378C in the incubation wells. After a minimum of2 min, 100 ml luciferase (Chronolume, Haem Pty Ltd,Melbourne, Australia) was added to the first two cuvetteswhich were immediately placed in the aggregometry wellsand stirred for 2 min. After 2 min a standard amount of ATP(2 nM) was added to the first cuvette and the luminescencecalibrated. To the second cuvette 1 U/ml thrombin wasadded and the luminescence measured over 6 min. Simulta-neous measurements of release and impedance were thenperformed on the next four cuvettes. In each case thecuvettes were warmed and stirred for a minimum of 2 min.The impedance electrodes were placed into the cuvettes andcalibration checked. After agonist addition, the impedanceand luminescence were measured over 6 min. The agonistsused were (in sequence) 5 mM/ml ADP, 2 mg/ml collagen,0·5 mM/ml arachidonic acid and 1 mg/ml ristocetin. Allagonists were obtained from Chronolog Corporation (HaemPty Ltd, Melbourne, Australia). Finally, spontaneous aggre-gation was assessed on the last two cuvettes as previouslydescribed (Balduini et al, 1988). Each cuvette was placed inthe aggregometry wells and stirred for 15 min. Spontaneousplatelet aggregation (SPA) was present if the impedanceincreased by more that 1 Ohm over the 15 min.
Forty-nine normal volunteers (33 females) aged from 24and 79 years (mean 49 years) with a median platelet countof 243 × 109/l (112–347) were studied to establish areference range (Table I). The reference interval representsthe mean 62 standard deviations after logarithmic trans-formation. Normal volunteers met our criteria of no aspirin(or similar drugs) for 10 d and no garlic or alcohol for 2 dprior to collection. The method was found to be reproducibleby comparison of WBPA results on healthy individualsperformed on multiple occasions. Many factors are known toinfluence impedance and release as assesed by WBPA,including haematocrit, platelet count, and diluting solutions(Bertolino et al, 1993). As there are no published informa-tion reports on the reference interval for WBPA obtained at

platelet counts outside normal levels, we performed dilutionstudies on blood obtained from healthy volunteers (whilemaintaining the haemoglobin and haematocrit) and foundour reference range was compatible with platelet counts aslow as 80 × 109/l. While the effect of platelet counts above450 × 109/l upon WBPA has not been systematicallyassessed, we found no correlation between any individualimpedance or release result over platelet counts between 80and 450 × 109/l. Additionally, dilution studies of fivepatients with apparent reactive thrombocytosis or post-splenectomy thrombocytosis (platelet counts between 800and 1000 × 109/l), did not demonstrate appreciably differentimpedance or release results. The median platelet count forall patients in this study was 559 × 109/l, and only fivepatients underwent WBPA at platelet counts >1000 × 109/l.No consistent relationship between platelet count and SPAhas been found; further, we found, as have others (Barbuiet al, 1973; Wu, 1978; Raman et al, 1989) that SPA
disappears upon dilution in some patients with reactivethrombocytosis and MPD.
Platelets were considered to be hyperactive if at leastone result (i.e. impedance or release with one agonist) wasabove the reference range, and hypoactive if at least oneresult (i.e. impedance or release with one agonist) was belowthe reference range. Mixed hypo- and hyperactive plateletswere considered present when at least one result (i.e.impedance or release) was below and above the referencerange respectively. Spontaneous platelet aggregation wasconsidered separately, i.e. independent of platelet hyper- orhypoactivity.
RESULTS
Seventy-five patients with MPD were entered into the study(Table II). 20 patients were diagnosed with PV, 30 with ET,six with CML, 11 with MF, and eight with an unclassifiedMPD. The median age of the total group of patients was72 years (range 25–95); there were 43 females and 32males. Platelet counts at the time of WBPA were normal(150–450 × 109/l) in 19, increased in 50, and reduced in sixpatients (27, 28, 81, 81, 108 and 148 × 109/l).
Representative examples of hyperactive, hypoactive andco-existing hyper- and hypoactive WBPA are demonstratedin Figs 1, 2 and 3 respectively. A total of 39 patients hadabnormal laboratory result(s) indicating platelet hyper-aggregability; 14 had evidence of hyper- as well ashypoaggregability, 16 had platelet hypoaggregability, andsix had normal results. 20/53 patients (36%) with eitherplatelet hyperactivity or co-existing hyper- and hypoactivityhad a positive history of venous and/or arterial thrombosis.
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 618–625
620 A. Manoharan et al
Table II. Clinical data of patients with myeloproliferative disease.
Myeloproliferative Chronicdisorders Polycythaemia Essential Idiopathic myelocyticunclassified vera thrombocythaemia myelofibrosis leukaemia Total
No. patients 8 20 30 11 6 75Females/males 4/4 10/10 20/10 6/5 3/3 43/32Median age (yr) (range) 70 (65–95) 76 (54–84) 71 (25–88) 74 (31–84) 67 (52–78) 72 (25–95)Median platelet count 545 (81–717) 386 (81–683) 644 (108–2452) 244 (27–1172) 693 (174–981) 559 (27–2452)×109/l (range)
Spontaneous platelet aggregation (SPA)Detected at diagnosis 0/4 2/10 10/14 0/2 0/2 12/32Overall 1/6 9/20 17/30 2/10 1/6 30/72
Whole blood platelet lumi-aggregometry (WBPA performed at diagnosis)Hypoactive 1 7 (3) 0 7 (1) 1 16 (5)Normal 0 2 (1) 3 (2) 0 0 5 (3)Mixed hypo- and hyperactive 4 (2) 5 (2) 3 1 (1) 1 (1) 14 (6)Hyperactive 3 (2) 6 (4) 24 (11) 3 4 (1) 40 (18)
Clinical events at diagnosis (in follow-up)Erythromelalgia 1 3 (1) 5 (1) 0 0 8 (2)Arterial 2 3 (2) 3 (1) 1 (1) (1) 10 (5)Venous 1 5 2 (3) 1 (3) 1 10 (6)Total events 4 11 (3) 10 (5) 2 (4) 1 (1) 28 (13)
Table I. Reference interval for impedance and release bywhole blood lumi-aggregometry (mean 6 2 SD).
Impedance ReleaseAgonist (Ohms) (in nM ATP)
Collagen (2 mg/ml) 15–50 0·4–2·0AA (0·5 mM) 16–44 0·5–2·0ADP (5 mM) 10–32 0·2–2·0Ristocetin (1 mg/ml) 5·0–34 –Thrombin (1 U/ml) – 0·5–2·0

621Thrombosis and Bleeding in MPD
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 618–625
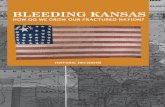
Fig 1. A representative study of hyperactive platelets. Whole blood impedance and release was simultaneously measured using a whole bloodplatelet lumi-aggregometer (see text for details). In this diagram 0·5 mM/ml of arachidonic acid (channels 1 and 2) or 2 mg/ml of collagen(channels 3 and 4) were added to one of two cuvettes containing whole blood. The horizontal divisions represent time, with each horizontaldivision equivalent to 60 s. Impedance (channels 1 and 3) and release (channels 2 and 4) were measured by the extent of deflection from baselinein the vertical axis. Impedance was measured in Ohm (20 Ohm is equivalent to three vertical divisions) and Release was measured in nM ATP(each vertical division is equivalent to 10% release with 2 nM ATP equivalent to 43%). The results (see Amplitude) were as follows: arachidonicacid 53 Ohm and 0·88 nM; collagen 55 Ohm and 0·69 nM.
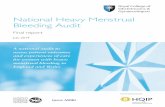
Fig 2. A representative study of hypoactive platelets. Whole blood impedance and release was simultaneously measured using a whole bloodplatelet lumi-aggregometer (see text for details). In this diagram 0·5 mM/ml of archidonic acid (channels 1 and 2) or 2 mg/ml of collagen(channels 3 and 4) were added to one of two cuvettes containing whole blood. The horizontal divisions represent time, with each horizontaldivision equivalent to 60 s. Impedance (channels 1 and 3) and release (channels 2 and 4) were measured by the extent of deflection from baselinein the vertical axis. Impedance was measured in Ohm (20 Ohm is equivalent to three vertical divisions) and Release was measured in nM ATP(each vertical division is equivalent to 10% release with 2 nM ATP equivalent to 53%). The results (see Amplitude) were as follows: arachidonicacid 9 Ohm and 0·22 nM; collagen 17 Ohm and 0·0 nM.

The clinical events included erythromelalgia (eight), tran-sient cerebral ischaemic attacks (five), deep venous throm-bosis (three), pulmonary embolism (four), superficial venousthrombophlebitis (one), portal vein thrombosis (one), andlower limb arterial ischaemia (two). Three of these patientshad more than one event. In contrast, among the 16 patientswith hypoactive platelets two patients have had thromboticevents (one with erythromelalgia and one with stroke,erythromelalgia and pulmonary embolism). The six patientswith normal results had no history of clinical events. A pasthistory of thrombotic events was significantly associatedwith platelet hyperactivity (OR 6·1, 95% CI 1·3–28·7,P ¼ 0·023).
Notwithstanding the small number of patients in this
study, no other clinical or laboratory factors (includingplatelet count) were associated wih platelet hyperactivity orpast history of thrombotic events. The analysis of agonist(each chosen because of its conventional use in plateletaggregometry for nearly 30 years) impedance or releaserevealed a very heterogenous mix of abnormalities. Only sixof the 75 patients had completely normal WBPA studies. Wedid not find any particular pattern of impedance or release,nor a correlation between the impedance and the releasestudy results (Table III).
Patients were followed for a median of 33 months (range4–264 months) from diagnosis. During this period anadditional nine patients, all with platelet hyperactivity,developed thrombotic events. Transient cerebral ischaemiadeveloped in five, all of whom received anticoagulanttherapy. One patient developed stroke (saggital sinusthrombosis) and concurrent pulmonary embolism andcommenced oral anticoagulant therapy. One patientdeveloped erythromelalgia and commenced aspirin. Twoadditional patients (one ET, one IMF) ceased aspirin forsurgical procedures and developed post-operative pulmonaryembolism. In comparison, no patients with normal plateletfunction and only one patient with platelet hypoactivitydeveloped new thrombotic events (simultaneous retinal veinthrombosis and pulmonary embolism treated with oralanticoagulation). However, statistical analysis failed to showa significant relationship between platelet hyperactivityand thrombotic events during follow-up (OR 1·09, 95% CI
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 618–625
622 A. Manoharan et al
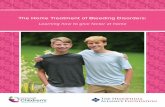
Fig 3. A representative study of mixed hypo- and hyperactive platelets. Whole blood impedance and release was simultaneously measured using awhole blood platelet lumi-aggregometer (see text for details). In this diagram 0·5 mM/ml of archidonic acid (channels 1 and 2) or 2 mg/ml ofcollagen (channels 3 and 4) were added to one of two cuvettes containing whole blood. The horizontal divisions represent time, with eachhorizontal division equivalent to 60 s. Impedance (channels 1 and 3) and release (channels 2 and 4) were measured by the extent of deflectionfrom baseline in the vertical axis. Impedance was measured in Ohm (20 Ohm is equivalent to three vertical divisions) and release was measuredby nM ATP (each vertical divison is equivalent to 10% release with 2 nM ATP equivalent to 35%). The results (see Amplitude) were as follows:arachidonic acid 9 Ohm and 1·8 nM; collagen 59 Ohm and 0·22 nM.
Table III. Impedance versus release results.
Reduced Normal IncreasedADP release ADP release ADP release
Impedance results (n ¼ 20) (n ¼ 51) (n ¼ 4)
Reduced 6 2 0Normal 6 8 1Increased 6 41 3Mixed hypo/hyperactive 2 0 0for impedance only

623Thrombosis and Bleeding in MPD
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 618–625
0·51–36·2, P ¼ 0·18). Odds ratio 1·09, 95% CI 0·51–36·2,P ¼ 0·18.
Fifty of the 53 patients with laboratory evidence of platelethyperactivity (with or without a positive history of thrombosis)were given specific therapy comprising aspirin (100 mg/d oron alternate days) alone (23) or with chemotherapy (13);aspirin with anticoagulant therapy (two); chemotherapyalone (eight); and oral anticoagulant therapy with orwithout chemotherapy (five). Intermittent hydroxyurea(Manoharan, 1991) was the most commonly used form ofchemotherapy. Three patients did not receive any specifictherapy including aspirin because of physician preference(two) or easy bruising (one). During the follow-up periodranging from 4 to 156 months (median 33 months), onlyone patient experienced clinical thrombosis. An 80-year-oldfemale with CGL experienced recurrent transient cerebralischaemic attacks despite aspirin and chemotherapy. Onepatient on aspirin and oral anticoagulant therapy developediron deficiency anaemia related to ulcerative oesaphagitisbut no other patients on aspirin manifested clinical bleedingduring this period. Eight of the 22 patients with normal orhypoactive platelets received specific therapy includingaspirin alone (four), aspirin with chemotherapy (two), orchemotherapy alone (two). No patient in this groupdeveloped new thrombotic events during a median follow-up of 55 months (range 13–264). Two patients with platelethypoactivity have suffered clinically significant haemor-rhage including spontaneous intracranial haemorrhage(one) and muscle haematoma requiring transfusion follow-ing a fall (one); neither was on aspirin therapy at the time ofbleeding.
Spontaneous platelet aggregation (SPA) was seen in 40%of the patients tested (9/20 PRV, 17/30 ET, 2/10 IMF, 1/6CML, 1/6 MPD unclassified). We found no statisticalcorrelation between SPA and any other clinical or laboratoryfactor, including WBPA results. SPA occurred in 3/13, 2/5,3/13 and 23/41 patients with hypoaggregable, normal,mixed hypo- and hyperactive and hyperactive platelets byWBPA, respectively. SPA was found in 14/30 (47%) patientswith and 16/42 (38%) without a positive history of venousand/or arterial thrombosis. Although the median plateletcount was higher in the group of patients with SPA (632 v532 × 109/l), no significant difference in platelet count wasseen between these groups.
Repeat WBPA studies were performed in 22 patients. Threeof the four patients with initial hypoactivity remainedhypoactive, but one patient with PRV became hyperactiveand was commenced on aspirin although asymptomatic. Ofthe five patients initially normal by WBPA, one remainednormal; one developed a mixed picture, two became hypoac-tive, and one patient with ET became hyperactive with SPAand was commenced on aspirin despite being asymptomatic.13 patients with hyperactive platelets were retested. 12 weretested while on aspirin and five, five and two were hypoactive,mixed hypo- and hyperactive, and persistently hyperactiverespectively. The one patient not receiving aspirin remainedunchanged. Of 15 patients with SPA who were retested onaspirin all but one had normalized. The median time betweenretesting was 10·3 months (range 2·8–27·3).
DISCUSSION
Our clinical experience from this study suggests that wholeblood platelet lumi-aggregometry studies are useful inpatients with MPD. We found a high prevalence of in-vitroplatelet hyperactivity in patients with a previous history ofthrombosis. Using WBPA, we identified a group of patientswith hyperactive platelets most of whom were then treatedwith antiplatelet therapy, oral anticoagulation and/orchemotherapy. Only one of 53 patients treated in thismanner suffered clinical thrombosis after a median of 33months follow-up. The rarity of thrombotic events in patientswith normal or hypoactive platelets also validates theusefulness of whole blood platelet aggregation studies inMPD. With this insight, it seems appropriate to initiate activetherapeutic measures, including low-dose aspirin, in patientswith hyperactive platelets even in the absence of clinicallyevident thrombotic events. The indiscriminate usage of anti-platelet medications in MPD is potentially hazardous andcannot be recommended. In a prospective randomized studyby the Polycythaemia Vera Study Group, aspirin (300 mg/d)and persantin (75 mg t.i.d.) did not prevent thromboticcomplications and resulted in excessive haemorrhage(Tartaglia et al, 1986). Some patients experience unusualprolongations of the skin bleeding time or significant clinicalhaemorrhage only after aspirin has been commenced(Adams et al, 1974; Kessler et al, 1982).
There are a number of published observations thatimplicate platelet hyperactivity with thrombotic events inpatients with MPD. Platelet hyperactivity was demonstratedin a small cohort of patients by perfusing whole blood overde-endothelialized artery segments (Sacher et al, 1981).The highest platelet reactivity was found in patientswith thrombotic events. Increased plasma levels of beta-thromboglobulin and platelet factor 4, consistent withexcessive platelet activation in vivo, have often been foundin patients with MPD and on occasions correlated withthrombotic events (Boughton et al, 1978; Wehmeier et al,1990). Vreeken & Van Aken (1971) reported a relationshipbetween thrombotic erythromelalgia and spontaneousplatelet aggregation in platelet-rich plasma (PRP). Prestonet al (1974) described six thrombocythaemic patients whopresented with digital ischaemia and had enhanced aggre-gation to collagen and ADP on PRP aggregometry and 4/5tested also had spontaneous aggregation. Dramatic relief ofpain was seen in all cases within 6 h of ingestion ofaspirin, and the platelet hyperactivity were reversed. Wu(1978) also described a relationship between platelethyperactivity and thrombosis in a cohort of 28 patientswith MPD and 11 patients with reactive thrombosis.Thrombosis was seen in seven patients with MPD and fivehad spontaneous aggregation with otherwise normalaggregometry. Two patients had haemorrhage, neither ofwhom had SPA and one had hypoactive platelets byaggregation. 19 patients without thrombosis or bleedingdid not have SPA, and only one patient with reactivethrombocytosis had SPA. Fabris et al (1981) also found acorrelation between platelet hyperactivity and thrombosis,and platelet hypoactivity and haemorrhage in their study of

38 patients with primary thrombocythaemia. Van Genderenet al (1995) prospectively demonstrated a shortened meanplatelet survival time in patients with thrombocythaemiacomplicated by erythromelalgia, with a normalization ofsymptoms and platelet survival with aspirin. More recentstudies (Michiels et al, 1996; van Genderen & Michiels,1997) confirmed the efficacy of aspirin in controllingmicrovascular symptoms. Rinder et al (1998) correlatedthe risk of thrombosis with increased platelet turnover inprimary and secondary thrombocytosis. Our results and theabove-mentioned studies document the therapeutic efficacyof aspirin in preventing further thrombotic events in patientswith platelet hyperactivity. Additionally, Nurden et al (1996)documented platelet hyperaggregability due to plateletactivation using specific monoclonal antibodies and flowcytometry in a patient with recurrent major venousthrombosis who was successfully treated with long-termticlopidine.
The majority of previous studies, using conventionaloptical platelet aggregometry, have however been unable todemonstrate a correlation between in vitro assessment ofplatelet function and clinical events (both thrombosis andhaemorrhage) in patients with MPD. The general lack ofcorrelation between in-vitro platelet function studies and thespecific haemostatic complication in patients with MPD hasbeen variably attributed to (i) multiple and contradictoryplatelet abnormalities in the same patient; (ii) change ofplatelet function during the course of the disease (i.e. de novo)or as a result of treatment; and (iii) pathogenic mechanism(s)involving non-platelet sources (e.g. leucocytes) or otheraspects of haemostasis such as clot fragility (Schafer, 1984;Baker & Manoharan, 1988; Castaman et al, 1995; Landolfiet al, 1997). Balduini et al (1988, 1991) have performeddirect comparisons between conventional optical PRPplatelet aggregometry and WBPA in 120 patients withMPD. In an initial study of 18 patients with IMF,WBPA studies showed 22%, 22% and 55% of the patientsto be hypoactive, normal or hyperactive. Conventionalaggregometry demonstrated 33% of the patients to behypoactive and 66% were normal (Balduini et al, 1988). Inthe latter publication, these disparate results were confirmedand suggested that conventional PRP aggregometry wasinadequate for in vitro assessment of platelet function inpatients with MPD (Balduini et al, 1991). No correlation betweenWBPA and thrombotic or haemorrhagic complications weremade in these studies.
In an earlier study from this institution (Baker &Manoharan, 1988) we reported co-existence of hyper- andhypoactive platelets in some patients with MPD, and achange of platelet function during the course of the diseasein some others, with platelet hypo-function being the onlyconstant abnormality over time. In the present study, inwhich a simpler yet more sophisticated method of investiga-tion has been used, we observed co-existence of hyper- andhypoactivity in 14/75 patients. A change of platelet functionwas also found in occasional patients. These observationshighlight the need to test platelets for hyper- as well ashypo-function, and to repeat the studies from time to time(e.g. 2–3 years), especially in patients with normal or
hyper-function. Although none of the patients receivingaspirin therapy in the present study developed bleeding,should it occur, it would be prudent to stop the drug andrepeat the studies to rule out the possibility of a change inplatelet function.
In conclusion, we continue to use WBPA to selectpatients for antiplatelet therapy. Patients with hyperactiveplatelets receive low-dose aspirin therapy as part of theirtreatment. Patients with normal or hypoactive plateletsreceive low-dose aspirin only if otherwise clinically indicated.Continuing prospective experience with this approach seemswarranted.
REFERENCES
Adams, T., Schutz, L. & Goldberg, L. (1974) Platelet functionabnormalities in the myeloproliferative disorders. ScandinavianJournal of Haematology, 13, 215–224.
Arboix, A., Besses, C., Acin, P., Massons, J.B., Florensa, L.,Oliveres, M. & Sans-Sabrafen, J. (1995) Ischemic stroke as firstmanifestation of essential thrombocythemia: report of six cases.Stroke, 26, 1463–1466.
Baker, R.I. & Manoharan, A. (1988) Platelet function in myelo-proliferative disorders: characterization and sequential studiesshow multiple platelet abnormalities, and change with time.European Journal of Haematology, 40, 267–272.
Balduini, C.L., Bertolino, G., Gamba, G., Barosi, G., Sinigaglia, F.,Noris, P., Bisio, A. & Ascari, E. (1988) Platelet aggregation inplatelet rich plasma and whole blood in 18 patients affected byidiopathic myelofibrosis. European Journal of Haematology, 41,267–272.
Balduini, C.L., Bertolino, G., Noris, P. & Piletta, G.C. (1991) Plateletaggregation in platelet-rich plasma and whole blood in 120patients with myeloproliferative disorders. American Journal ofClinical Pathology, 95, 82–86.
Barbui, T., Battista, R. & Dini, E. (1973) Spontaneous plateletaggregation in myeloproliferative disorders: a preliminary study.Acta Haematologica, 50, 25–29.
Berk, P.D., Goldberg, J.D., Donovan, P.B., Fruchtman, S.M.,Berlin, N.I. & Wasserman, L.R. (1986) Therapeutic recommenda-tions in polycythemia vera based on Polycythemia Vera StudyGroup protocols. Seminars in Hematology, 23, 132–143.
Berlin, N.I. (1975) Diagnosis and classification of the polycythemias.Seminars in Hematology, 12, 339–351.
Bertolino, G., Noris, P. & Balduini, C.L. (1993) Effect of differentsample preparation methods on the results of the impedancetechnique in the study of platelet hyper- and hypo-function inwhole blood. Thrombosis Research, 71, 89–94.
Born, G.V. & Hume, M. (1967) Effects of the numbers and sizes ofplatelet aggregates on the optical density of plasma. Nature, 215,1027–1029.
Boughton, B.J., Allington, M.J. & King, A. (1978) Platelet andplasma beta thromboglobulin in myeloproliferative syndromesand secondary thrombocytosis. British Journal of Haematology, 40,125–132.
Castaman, G., Lattuada, A., Ruggeri, M., Tosetto, A., Mannucci, P.M.& Rodeghiero, F. (1995) Platelet von Willebrand factor abnorm-alities in myeloproliferative syndromes. American Journal ofHematology, 49, 289–293.
Cortelazzo, S., Finazzi, G., Ruggeri, M., Vestri, O., Galli, M.,Rodeghiero, F. & Barbui, T. (1995) Hydroxyurea for patientswith essential thrombocythemia and a high risk of thrombosis.New England Journal of Medicine, 332, 1132–1136.
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 618–625
624 A. Manoharan et al

625Thrombosis and Bleeding in MPD
q 1999 Blackwell Science Ltd, British Journal of Haematology 105: 618–625
Fabris, F., Randi, M., Sbrojavacca, R., Casonato, A. & Girolami, A.(1981) The possible value of platelet aggregation studies inpatients with increased platelet number. Blut, 43, 279–285.
Gruppo Italiano Studio Policitemia (1995) Polycythemia vera: thenatural history of 1213 patients followed for 20 years. Annals ofInternal Medicine, 123, 656–664.
Johnson, M., Gernsheimer, T. & Johansen, K. (1995) Essentialthrombocytosis: underemphasized cause of large-vessel thrombo-sis. Journal of Vascular Surgery, 22, 443–449.
Kessler, C.M., Klein, H.G. & Havlik, R.J. (1982) Uncontrolledthrombocytosis in chronic myeloproliferative disorders. BritishJournal of Haematology, 50, 157–167.
Landolfi, R., Marchioli, R. & Patrono, C. (1997) Mechanismsof bleeding and thrombosis in myeloproliferative disorders.Thrombosis and Haemostasis, 78, 617–621.
Laszlo, J. (1975) Myeloproliferative disorders (MPD): myelofibrosis,myelosclerosis, extramedullary hematopoiesis, undifferentiatedMPD, and hemorrhagic thrombocythemia. Seminars in Hematol-ogy, 12, 409–432.
Manoharan, A. (1991) Management of myelofibrosis with inter-mittent hydroxyurea. British Journal of Haematology, 77, 252–254.
Michiels, J.J., Abels, J., Steketee, J., van Vliet, H.H. & Vuzevski, V.D.(1985) Erythromelalgia caused by platelet-mediated arteriolarinflammation and thrombosis in thrombocythemia. Annals ofInternal Medicine, 102, 466–471.
Michiels, J.J., Koudstaal, P.J., Mulder, A.H. & van Vliet, H.H. (1993)Transient neurologic and ocular manifestations in primarythrombocythemia. Neurology, 43, 1107–1110.
Michiels, J.J., van Genderen, P.J., Lindemans, J. & van Vliet, H.H.(1996) Erythromelalgic, thrombotic and hemorrhagic manifesta-tions in 50 cases of thrombocythemia. Leukemia and Lymphoma,22, (Suppl. 1), 47–56.
Murphy, S., Peterson, P., Iland, H. & Laszlo, J. (1997) Experience ofthe Polycythemia Vera Study Group with essential thrombocythemia:a final report on diagnostic criteria, survival, and leukemictransition by treatment. Seminars in Hematology, 34, 29–39.
Nurden, P., Bihour, C., Smith, M., Raymond, J.M. & Nurden, A.T.(1996) Platelet activation and thrombosis: studies in a patientwith essential thrombocythemia. American Journal of Hematology,51, 79–84.
Preston, F.E., Emmanuel, I.G., Winfield, D.A. & Malia, R.G. (1974)Essential thrombocythaemia and peripheral gangrene. BritishMedical Journal, iii, 548–552.
Raman, B.K., Van Slyck, E.J., Riddle, J., Sawdyk, M.A., Abraham, J.P.& Saeed, S.M. (1989) Platelet function and structure in
myeloproliferative disease, myelodysplastic syndrome, and sec-ondary thrombocytosis. American Journal of Clinical Pathology, 91,647–655.
Randi, M.L., Stocco, F., Rossi, C., Tison, T. & Girolami, A. (1991)Thrombosis and hemorrhage in thrombocytosis: evaluation ofa large cohort of patients (357 cases). Journal of Medicine, 22,213–223.
Rinder, H.M., Schuster, J.E., Rinder, C.S., Wang, C., Schweidler, H.J. &Smith, B.R. (1998) Correlation of thrombosis with increasedplatelet turnover in thrombocytosis. Blood, 91, 1288–1294.
Sacher, R.A., Jacobson, R.J. & McGill, M. (1981) Functional andmorphological studies of platelet reactivity with vessel wallsubendothelium in chronic myeloproliferative disease. BritishJournal of Haematology, 49, 43–52.
Schafer, A.I. (1984) Bleeding and thrombosis in the myeloprolifera-tive disorders. Blood, 64, 1–12.
Schafer, A.I. (1996) Management of thrombocythemia. CurrentOpinion in Hematology, 3, 341–346.
Silverstein, M.N. (1983) Agnogenic myeloid metaplasia. Hematology(ed. by W. J. Williams, E. Beutler, A. J. Erslev and M. A. Lichtman),p. 214. McGraw-Hill, New York.
Tartaglia, A.P., Goldberg, J.D., Berk, P.D. & Wasserman, L.R. (1986)Adverse effects of antiaggregating platelet therapy in the treatment ofpolycythemia vera. Seminars in Hematology, 23, 172–176.
van Genderen, P.J. & Michiels, J.J. (1994) Erythromelalgic, thrombo-tic and haemorrhagic manifestations of thrombocythaemia.Presse Medicale, 23, 73–77.
van Genderen, P.J. & Michiels, J.J. (1997) Erythromelalgia: apathognomonic microvascular thrombotic complication in essen-tial thrombocythemia and polycythemia vera. Seminars inThrombosis and Hemostasis, 23, 357–363.
van Genderen, P.J., Michiels, J.J., van Strik, R., Lindemans, J. &van Vliet, H.H. (1995) Platelet consumption in thrombocythemiacomplicated by erythromelalgia: reversal by aspirin. Thrombosisand Haemostasis, 73, 210–214.
Vreeken, J. & van Aken, W.G. (1971) Spontaneous aggregation ofblood platelets as a cause of idiopothic thrombosis and recurrentpainful toes and fingers. Lancet, ii, 1395–1397.
Wehmeier, A., Fricke, S., Scharf, R.E. & Schneider, W. (1990) Aprospective study of haemostatic parameters in relation to theclinical course of myeloproliferative disorders. European Journal ofHaematology, 45, 191–197.
Wu, K.K. (1978) Platelet hyperaggregability and thrombosis inpatients with thrombocythemia. Annals of Internal Medicine, 88,7–11.