A phase 2 trial of combination therapy with thalidomide, arsenic trioxide, dexamethasone, and...
9
A Phase 2 Trial of Combination Therapy With Thalidomide, Arsenic Trioxide, Dexamethasone, and Ascorbic Acid (TADA) in Patients With Overlap Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) or Primary Myelofibrosis (PMF) Nelli Bejanyan, MD 1 ; Ramon V. Tiu, MD 1,2 ; Azra Raza, MD 3 ; Ania Jankowska, PhD 2 ; Matt Kalaycio, MD 1 ; Anjali Advani, MD 1,2 ; Josephine Chan, PhD 1 ; Yogen Saunthararajah, MD 1,2 ; Lindsey Mooney, BS 1 ; Jaroslaw P. Maciejewski, MD, PhD 1,2 ; and Mikkael A. Sekeres, MD, MS 1,2 BACKGROUND. Primary myelofibrosis (PMF) and overlap myelodysplastic/myeloproliferative neoplasms (MDS/MPN) are clonal hema- topoietic disorders that share similar clinical features and molecular abnormalities, such as the Janus kinase 2 (JAK2) valine to phe- nylalanine mutation at codon 617 (V617F) and the tet methylcytosine dioxygenase 2 (TET2) mutation. There are limited therapeutic options available for these diseases, and single agents have only modest efficacy. In this phase 2 study, the authors combined multi- ple active agents (thalidomide, arsenic trioxide, dexamethasone, and ascorbic acid [TADA]) to treat patients with these disorders. METHODS. This multicenter trial was conducted from January 2005 to July 2007. The primary endpoint was to evaluate the efficacy of TADA therapy. Patients received the combination for one 12-week cycle followed by maintenance thalidomide for an additional 3 months. Response was assessed using International Working Group criteria. RESULTS. Among 28 enrolled patients, the median age was 66.5 years; 15 patients had MDS/MPN-unclassifiable, 8 patients had chronic myelomonocytic leukemia type 1, and 5 patients had PMF. Approximately 60% of the patients had normal cytogenetics. The JAK2V617F mutation was detected in 5 of 14 tested patients, and TET2 mutations were detected in 2 of 8 tested patients. Almost half of the patients had splenomegaly. With a median on-study follow-up of 5.7 months, 21 patients (75%) completed the entire 12-week course of therapy, and 6 patients (29%) responded to TADA. With a median extended follow-up of 24.1 months for 15 evaluable patients, the median progression-free survival was 14.4 months, and the median overall survival was 21.4 months. CONCLUSIONS. The TADA regimen yielded clinical responses in patients with PMF and MDS/MPN. To the authors’ knowledge, this study represents the first trial targeting this patient population. The results indicated that it is reasonable to incorporate multiple novel agents in the treatment of these rare diseases. Cancer 2012;118:3968-76. V C 2011 American Cancer Society . KEYWORDS: thalidomide, arsenic trioxide, dexamethasone, and ascorbic acid, myelodysplastic/myeloproliferative neoplasms, primary myelofibrosis, myelofibrosis, trial. INTRODUCTION Primary myelofibrosis (PMF) and overlap myelodysplastic syndromes/myeloproliferative neoplasms (MDS/MPN) are clonal disorders of hematopoietic stem cell origin associated with a variable clinical course. On the basis of the 2008 World Health Organization (WHO) classification of myeloid and lymphoid neoplasms, MDS/MPN encompasses chronic my- elomonocytic leukemia (CMML)-1 and CMML-2; atypical chronic myeloid leukemia, breakpoint cluster region—v-abl Abelson murine leukemia viral oncogene homolog 1 (BCR/ABL1)-negative (atypical chronic myeloid leukemia [aCML]); juvenile myelomonocytic leukemia (JMML); and MDS/MPN-unclassifiable (MDS/MPN-u), which includes refractory anemia with ring sideroblasts and thrombocytosis (RARS-T) as a provisional entity. 1 These overlap syndromes have pathobiologic and clinical evidence of both MDS and MPN, characterized by bone marrow hypercellularity, various myeloid lineage dysplastic and proliferative features, ineffective hematopoiesis, and frequent association with hepatosplenomegaly. PMF is a myeloproliferative neoplasm that often presents with upfront bone marrow fibrosis, dysplastic megakaryo- cytes, extramedullary hematopoiesis, and elevated leukocyte and platelet counts. Patients with PMF and overlap MDS/ MPN frequently develop progressive cytopenias and may evolve into acute myeloid leukemia. The development of DOI: 10.1002/cncr.26741, Received: August 30, 2011; Revised: October 16, 2011; Accepted: October 25, 2011, Published online December 16, 2011 in Wiley Online Library (wileyonlinelibrary.com) Corresponding author: Mikkael A. Sekeres, MD, MS, Director, Leukemia Program, Associate Professor of Medicine, Department of Hematologic Oncology and Blood Disorders, Cleveland Clinic Taussig Cancer Institute, Desk R35, 9500 Euclid Avenue, Cleveland, OH 44195; Fax: (216) 636-0636; [email protected] 1 Leukemia Program, Department of Hematologic Oncology and Blood Disorders, Cleveland Clinic Taussig Cancer Institute, Cleveland, Ohio; 2 Department of Trans- lational Hematology and Oncology, Cleveland Clinic Taussig Cancer Institute, Cleveland, Ohio; 3 Columbia University, New York, New York Presented in part at the 49th Annual Meeting of the American Society of Hematology; December 8-11, 2007; Atlanta, Georgia. 3968 Cancer August 15, 2012 Original Article
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of A phase 2 trial of combination therapy with thalidomide, arsenic trioxide, dexamethasone, and...

A Phase 2 Trial of Combination Therapy With Thalidomide,
Arsenic Trioxide, Dexamethasone, and Ascorbic Acid (TADA) in
Patients With Overlap Myelodysplastic/Myeloproliferative
Neoplasms (MDS/MPN) or Primary Myelofibrosis (PMF)
Nelli Bejanyan, MD1; Ramon V. Tiu, MD1,2; Azra Raza, MD3; Ania Jankowska, PhD2; Matt Kalaycio, MD1;
Anjali Advani, MD1,2; Josephine Chan, PhD1; Yogen Saunthararajah, MD1,2; Lindsey Mooney, BS1;
Jaroslaw P. Maciejewski, MD, PhD1,2; and Mikkael A. Sekeres, MD, MS1,2
BACKGROUND. Primary myelofibrosis (PMF) and overlap myelodysplastic/myeloproliferative neoplasms (MDS/MPN) are clonal hema-
topoietic disorders that share similar clinical features and molecular abnormalities, such as the Janus kinase 2 (JAK2) valine to phe-
nylalanine mutation at codon 617 (V617F) and the tet methylcytosine dioxygenase 2 (TET2) mutation. There are limited therapeutic
options available for these diseases, and single agents have only modest efficacy. In this phase 2 study, the authors combined multi-
ple active agents (thalidomide, arsenic trioxide, dexamethasone, and ascorbic acid [TADA]) to treat patients with these disorders.
METHODS. This multicenter trial was conducted from January 2005 to July 2007. The primary endpoint was to evaluate the efficacy
of TADA therapy. Patients received the combination for one 12-week cycle followed by maintenance thalidomide for an additional 3
months. Response was assessed using International Working Group criteria. RESULTS. Among 28 enrolled patients, the median age
was 66.5 years; 15 patients had MDS/MPN-unclassifiable, 8 patients had chronic myelomonocytic leukemia type 1, and 5 patients had
PMF. Approximately 60% of the patients had normal cytogenetics. The JAK2V617F mutation was detected in 5 of 14 tested patients,
and TET2 mutations were detected in 2 of 8 tested patients. Almost half of the patients had splenomegaly. With a median on-study
follow-up of 5.7 months, 21 patients (75%) completed the entire 12-week course of therapy, and 6 patients (29%) responded to TADA.
With a median extended follow-up of 24.1 months for 15 evaluable patients, the median progression-free survival was 14.4 months,
and the median overall survival was 21.4 months. CONCLUSIONS. The TADA regimen yielded clinical responses in patients with PMF
and MDS/MPN. To the authors’ knowledge, this study represents the first trial targeting this patient population. The results indicated
that it is reasonable to incorporate multiple novel agents in the treatment of these rare diseases. Cancer 2012;118:3968-76. VC 2011American Cancer Society.
KEYWORDS: thalidomide, arsenic trioxide, dexamethasone, and ascorbic acid, myelodysplastic/myeloproliferative neoplasms,
primary myelofibrosis, myelofibrosis, trial.
INTRODUCTIONPrimary myelofibrosis (PMF) and overlap myelodysplastic syndromes/myeloproliferative neoplasms (MDS/MPN) areclonal disorders of hematopoietic stem cell origin associated with a variable clinical course. On the basis of the 2008WorldHealth Organization (WHO) classification of myeloid and lymphoid neoplasms, MDS/MPN encompasses chronic my-elomonocytic leukemia (CMML)-1 and CMML-2; atypical chronic myeloid leukemia, breakpoint cluster region—v-ablAbelson murine leukemia viral oncogene homolog 1 (BCR/ABL1)-negative (atypical chronic myeloid leukemia[aCML]); juvenile myelomonocytic leukemia (JMML); and MDS/MPN-unclassifiable (MDS/MPN-u), which includesrefractory anemia with ring sideroblasts and thrombocytosis (RARS-T) as a provisional entity.1 These overlap syndromeshave pathobiologic and clinical evidence of both MDS and MPN, characterized by bone marrow hypercellularity, variousmyeloid lineage dysplastic and proliferative features, ineffective hematopoiesis, and frequent association withhepatosplenomegaly.
PMF is a myeloproliferative neoplasm that often presents with upfront bone marrow fibrosis, dysplastic megakaryo-cytes, extramedullary hematopoiesis, and elevated leukocyte and platelet counts. Patients with PMF and overlap MDS/MPN frequently develop progressive cytopenias and may evolve into acute myeloid leukemia. The development of
DOI: 10.1002/cncr.26741, Received: August 30, 2011; Revised: October 16, 2011; Accepted: October 25, 2011, Published online December 16, 2011 in Wiley
Online Library (wileyonlinelibrary.com)
Corresponding author: Mikkael A. Sekeres, MD, MS, Director, Leukemia Program, Associate Professor of Medicine, Department of Hematologic Oncology and
Blood Disorders, Cleveland Clinic Taussig Cancer Institute, Desk R35, 9500 Euclid Avenue, Cleveland, OH 44195; Fax: (216) 636-0636; [email protected]
1Leukemia Program, Department of Hematologic Oncology and Blood Disorders, Cleveland Clinic Taussig Cancer Institute, Cleveland, Ohio; 2Department of Trans-
lational Hematology and Oncology, Cleveland Clinic Taussig Cancer Institute, Cleveland, Ohio; 3Columbia University, New York, New York
Presented in part at the 49th Annual Meeting of the American Society of Hematology; December 8-11, 2007; Atlanta, Georgia.
3968 Cancer August 15, 2012
Original Article

cytopenia, particularly anemia, is recognized as an adverseprognostic feature in several prognostic scoring systems ofPMF (Lille, Mayo, Dynamic International PrognosticScoring System [DIPSS], and DIPSS-Plus classifications)and CMML (M. D. Anderson classification).2-5 Multiplenew molecular abnormalities that play an important rolein the pathogenesis of myeloproliferative and myelodys-plastic disorders have been identified within the past dec-ade, including the Janus kinase 2 (JAK2) valine tophenylalanine mutation at codon 617 (V617F) mutation,which is identified in 40% to 65% patients with of PMFand in 26% to 60% of patients with MDS/MPN.6-10 Thetet methylcytosine dioxygenase 2 (TET2) mutation is thesecond most prevalent molecular abnormality, seen in17% of PMF cases and 22%-58% of MDS/MPN.9,11-13
Additional molecular abnormalities known to be associ-ated with MPN and MDS/MPN include myeloprolifera-tive virus oncogene (MPL), additional sex combs like 1(ASXL1), isocitrate dehydrogenase 1 and 2 (IDH1/IDH2), Cas-Br-M (murine) ecotropic retroviral trans-forming sequence (CBL), enhancer of zeste homolog 2(EZH2), lymphocyte-specific adapter protein Lnk (LNK),and IKAROS family zinc finger 1 (IKZF1).9,13-19
Despite advances in understanding the underlyinggenetic alterations in PMF andMDS/MPN, patients withthese diseases continue to face limited treatment options,and no current clinical trials specifically target patientswith overlap MDS/MPN. Allogeneic stem cell transplan-tation is the only potential curative modality, yet mostpatients are not suitable candidates. Alternatives are usedeither to treat symptoms or to attempt to treat the disease,largely by cross-applying therapeutic principles fromMDS therapies: response rates, however, usually are<20% to 25% and are of short duration.20-39 Thalido-mide and its successor lenalidomide are antiangiogenesisagents with cytokine-modulating activity that have beenused in combination with steroids in PMF patients andproduce response rates from 40% to 50%.23,24 Arsenic tri-oxide (ATO), which works through apoptotic and prodif-ferentiating mechanisms, inhibits the production ofvascular endothelial growth factor40,41 and has been usedas a single agent and in combination with gemtuzumabozogamicin in patients with MDS, producing responserates from 20% to 30%.38
For the current study, we investigated the efficacy of4-agent combination therapy with thalidomide, ATO,dexamethasone, and ascorbic acid (AA) (TADA) inpatients with PMF and overlap MDS/MPN. This combi-nation was chosen to target mechanisms of disease devel-opment for both MDS and MPN, because it is believed
that patients with overlap MDS/MPN have disease char-acteristics of both disorders. AA depletes intracellular glu-tathione, thereby enhancing the activity of ATO.42-44
MATERIALS AND METHODS
Patients and Setting
Patients aged �18 years who had a diagnosis of MDS/MPN or PMF, an Eastern Cooperative Oncology Groupperformance status of 0 to 2, and no previous thalidomideor ATO therapy were enrolled from January 2005 to July2007. Before patients were enrolled, all diagnoses ofMDS/MPN (including MDS/MPD-u and CMML-1and CMML-2) and PMF were confirmed by bone mar-row analysis at 1 of the 3 participating institutions (Cleve-land Clinic, University Hospitals in Cleveland, orUniversity of Massachusetts) based on 2001 WHO path-ologic classification.45 Negative BCR/ABL testing wasrequired for study enrollment in patients with a diagnosisof MPN. On the basis of the 2002 M. D. Andersen prog-nostic scoring system for CMML, our study patients withCMML (n¼ 8) were distributed in the following risk cat-egories: low risk, 5 patients; intermediate-1 risk, 2patients; and intermediate-2 risk, 1 patient.5 In addition,the prognostic grouping of PMF patients (n¼ 5) was asfollows: based on the Lille classification, there were 2 low-risk patients, 2 intermediate-risk patients, and 1 high-riskpatient; based on the Mayo classification, there were 2low-risk patients, 1 intermediate-risk patient, and 2 high-risk patients; and, based on the DIPSS classification, therewas 1 low-risk patient, 2 intermediate-1-risk patients, and2 intermediate-2-risk patients.4 Patients had to have a lifeexpectancy of at least 3 months, a platelet count>10,000/mm3, and normal organ function.
All patients who participated in this study providedwritten informed consent. In addition, the majority ofpatients treated at Cleveland Clinic provided consent forblood and bone marrow aspirate draw for correlative mo-lecular analyses. This study was registered with Clinical-Trials.gov as National Clinical Trial NCT00274820.
Study Design
This was a single-arm, open-label, multicenter, phase 2study and was approved by the institutional review ofboards at the study centers where patients were enrolled.Enrollment occurred from January, 2005 through July,2007. The primary endpoint of the study was to evaluateresponse to the TADA combination, as defined below.Secondary endpoints included safety and diseasetransformation.
TADA in MDS/Bejanyan et al
Cancer August 15, 2012 3969

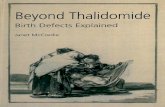
Patients received oral thalidomide 50 mg daily for2 weeks, then 100 mg daily, ATO based on the phase 2European Union MDS regimen31 (0.25 mg/kg intrave-nously on days 1-5 of week 1 then twice weekly duringweeks 2-12), oral dexamethasone 4 mg daily for 5 daysevery 4 weeks, and oral AA 1000 mg 2 to 3 hoursbefore each ATO infusion over a 12-week cycle. (Fig.1) Thalidomide maintenance was continued for anadditional 3 months in responding patients as tolerated.Patients received no growth factors during the study.Study protocol required bone marrow evaluation andspleen size assessment at baseline and after week 12 toassess for treatment response. To monitor for ATO car-diac toxicity, a 12-lead electrocardiogram was obtainedat baseline and weekly thereafter to assess QTc interval.The serum potassium level was kept �4.0 mEq/dL, andthe magnesium level was kept at >1.8 mg/dL with elec-trolyte supplementation as needed at the time of eachelectrocardiogram screening. Laboratory evaluations andstudy visits occurred weekly for the first 4 weeks thenevery 4 weeks thereafter for each cycle. Adverse eventswere assessed using National Cancer Institute CommonTerminology Criteria version 3.0. If grade 2 or 3 treat-ment-related adverse events occurred, then the next doseof the drug was delayed for up to 4 weeks until symp-tom improvement. Adverse events that persisted for >4weeks resulted in patient withdrawal from study, as diddisease progression. Patients were followed for at least 4
weeks after discontinuation of the study drugs or studycompletion.
Statistics and Efficacy Assessment
Because the TADA regimen had never been tested beforethis study, interim toxicity assessment was performed afterenrollment of the first 6 patients with the intention to dis-continue the study if 2 or more patients experienced grade�2 nonhematologic toxicity. Patients who received anyamount of study drug were included in the efficacy analy-sis. Survival and follow-up were calculated from the timeof study enrollment and were complete for all patientsthrough the completion of maintenance thalidomide andthrough May, 2011 for 15 patients. The overall responserate (ORR) was defined as achieving complete remission(CR), partial remission (PR), and/or clinical improve-ment based on 2006 International Working Group(IWG) criteria for PMF for all study participants; in addi-tion, CR, PR, and/or hematologic improvement (HI)were defined based on 2006 IWG response criteria forMDS in patients with overlap MDS/MPN, because thereare no specific response criteria to address this diagnosticentity.46,47 Disease progression also was assessed based on2006 criteria for PMF in all study participants and basedon 2006 IWG response criteria for MDS in patients withoverlapMDS/MPN. Baseline characteristics are presentedas medians with ranges, and the Kaplan-Meier method
Figure 1. The thalidomide (Thal), arsenic trioxide (ATO), dexamethasone (Dex), and ascorbic acid (AA) regimen (TADA) isillustrated.
Original Article
3970 Cancer August 15, 2012

was used to estimate progression-free survival (PFS) andoverall survival (OS).
RESULTS
Baseline Characteristics
Twenty-eight patients were enrolled on the study, and 21of those patients (75%) completed the full 12-week cycleof therapy. The remaining patients (n¼ 7) did not com-plete therapy for the following reasons: patient choice andwithdrawal of consent (n¼ 3; 11%), nonhematologicadverse events (n¼ 2; 7%), thrombocytopenia (n¼ 1;4%) and no response (n¼ 1; 4%). Baseline characteristicsof all patients are presented in Table 1. The median agewas 66.5 years (range, 49-82 years). Fifteen patients(54%) had a diagnosis of MDS/MPN-u, 8 patients (29%)had a diagnosis of CMML-1, and 5 patients (18%) had adiagnosis of PMF. Almost half (46%) presented with ei-ther palpable or radiographically evident splenomegaly.Fifteen patients (54%) had received previous therapy fortheir disease; most (n¼ 9; 60%) had received erythropoie-sis-stimulating agents, 2 (13%) had received azacitidine,and 1 (7%) had received an investigational therapy. Othertherapies included prednisone (13%), anagrelide (13%),and hydroxyurea (7%). The results of cytogenetic analysiswere available for 25 patients (89%). A normal karyotypewas detected in 13 patients (57%) with MDS/MPN andin 3 patients (60%) with PMF. Complex cytogeneticswere observed in 2 patients (7%), both of whom hadMDS/MPN. There were no patients with isolated dele-tion 5q, deletion 20q, or deletion 7 chromosomal abnor-malities. Five patients were positive for the JAK2V617Fmutation of 14 patients who were tested (36%). TET2mutational status was assessed later in 8 patients withMDS/MPN patients who had peripheral blood samplesavailable, 2 of whom were positive (25%). Neither ofthese 2 patients had concomitant JAK2V617F mutations.Therapy was initiated either for significant cytopenias(61%) or for disease-related symptoms (39%).
Adverse Events and Patient-ReportedSymptoms
The interim toxicity analysis based on the first 6 enrolledpatients indicated that the combination regimen was safefor study continuation. Adverse events in most patientswere mild (grade 1) to moderate (grade 2) (Table 2).Seven patients (25%) experienced grade �3 hematologictoxicities, including thrombocytopenia (n¼ 3; 11%),neutropenia (n¼ 3; 11%), and leukocytosis (n¼ 1; 4%).Fatigue was the most common nonhematologic toxicityand was observed in 82% of patients; only 8 patients
Table 1. Patient Characteristics
Baseline Characteristic No. of Patients (%)
Median age, y 66.5
Primary diagnosisMDS/MPN-u 15 (54)
CMML-1 8 (29)
PMF 5 (18)
Splenomegaly 13 (46)
Laboratory valuesLactate dehydrogenase, U/L
Normal, 100-200
Median [range] 300 [137-903]
Leukocyte count, K/lLNormal, 3.7-11.0
Median [range] 12.1 [0.9-70.5]
Hemoglobin value, g/dL
Normal, 12-17
Median [range] 10.3 [6.4-13.4]
Platelet count, K/lLNormal, 150-400
Median [range] 126.5 [15-792]
Circulating peripheral blast count, %
Normal limits 0
Median [range] 0 [0-5]
Cytogenetics for MDS/MPNNormal 13 (57)
122p 1 (4)
19 1 (4)
18 2 (9)
2Y 1 (4)
212p 1 (4)
Complex: ‡3 abnormalities 2 (9)
Unknown: no growth 2 (9)
Cytogenetics for PMFNormal 3 (60)
16 1 (20)
Unknown: no growth 1 (20)
Mutational statusJAK2 V617F, n5 14 tested 5 (36)
MDS/MPN 2
PMF 3
TET2, n5 8 tested 2 (25)
MDS/MPN 2
PMF ND
Prior therapies, n¼15Erythropoietin-stimulating agents 9 (60)
5-Azacytidine 2 (13)
Hydroxyurea 1 (7)
Anagrelide 2 (13)
Prednisone 2 (13)
Investigational 1 (7)
Reason for initiating therapyAnemia 8 (29)
Thrombocytopenia 9 (32)
Disease-related symptoms 11 (39)
Abbreviations: CMML-1, chronic myelomonocytic leukemia type 1; JAK2
V617F, Janus kinase valine to phenylalanine mutation at codon 617; MDS,
myelodysplastic syndrome; MPN, myeloproliferative neoplasm; MPN-u,
unclassifiable myeloproliferative neoplasm; ND, not done; PMF, primary
myelofibrosis; TET2, tet methylcytosine dioxygenase 2.
TADA in MDS/Bejanyan et al
Cancer August 15, 2012 3971

(29%) experienced grade�3 symptoms. Additional com-mon nonhematologic grade 3/4 adverse events includeddyspnea (18%) and infections (14%). Approximatelytwo-thirds of the patients developed neuropathy,although most of these episodes were only mild to moder-ate in severity, and all resolved. Similarly, approximately60% of study patients experienced grade 1/2 lowerextremity swelling, which was managed successfully withdiuretics. Episodes of grade 3/4 fluid overload, includingcardiac tamponade and pleural effusions, developed in 1patient and 2 patients, respectively. Two of the studypatients had grade 1/2 QTc prolongation; however, inboth patients, these electrocardiographic abnormalitieswere clinically insignificant. No thrombotic episodes wereobserved.
Treatment Efficacy
The median follow-up on the study was 5.7 months(range, 3.3-9.0 months). According to IWGmyelofibrosiscriteria, 6 patients (21%) responded to TADA therapy: 1patient achieved PR (4%), and the remaining patients(18%) had clinical improvement. Responses wereobserved only among patients who completed the full 12-week cycle of therapy (Table 3). The patient who achievedPR had CMML-1 and also had evidence of a bone mar-row response, with interval improvement of bone marrowfibrosis from 4þ at baseline to 2þ at 12 weeks of therapy.Regression of splenomegaly was observed in 2 patientswith overlap MDS/MPN; no spleen size reduction wasobserved in any of the patients with PMF. One of 5patients with PMF (20%) responded to therapy withimprovement of anemia. When modified IWG-MDS cri-teria were applied to patients with MDS/MPN, 2achieved HI-erythroid responses, and 1 achieved a plateletresponse (ORR, 20%). (Table 3) All 5 patients who hadthe JAK2V617F mutation continued to have stable dis-ease throughout the study period. One of the 2 patientswith a TET2 mutation achieved HI, and the other had
Table 2. Adverse Events (n¼28)
Event No. of Patients (%)
Patients WithAny Events
Patients WithGrade 3/4 Events
Hematologic adverse eventsAnemia 1 (3.6) 0 (0)
Thrombocytopenia 3 (10.7) 3 (10.7)
Neutropenia 4 (14.3) 3 (10.7)
Leukocytosis 1 (3.6) 1 (3.6)
Nonhematologic adverse eventsCardiovascular
Atrial fibrillation 1 (3.6) 0 (0)
QTC prolongation 2 (7.1) 0 (0)
Tachycardia 2 (7.1) 1 (2.5)
Cardiac tamponade 1 (3.6) 0 (0)
Cardiogenic edema 17 (60.7) 0 (0)
Hypertension 2 (7.1) 0 (0)
Hypotension 4 (1.3) 2 (7.1)
Respiratory
Cough 10 (35.7) 0 (0)
Dyspnea 16 (57.1) 5 (17.9)
Hypoxia 1 (3.6) 1 (3.6)
Pneumonitis 7 (25) 2 (7.1)
Pleural effusion 2 (7.1) 2 (7.1)
Gastrointestinal
Anorexia 6 (21.4) 0 (0)
Dry mouth 1 (3.6) 0 (0)
Dyspepsia 10 (35.7) 0 (0)
Nausea 8 (28.6) 0 (0)
Vomiting 3 (10.7) 1 (3.6)
Diarrhea/constipation 12 (46.4) 0 (0)
Transaminitis 5 (17.9) 0 (0)
Genitourinary and fluid/electrolyte
Renal failure 2 (7.1) 2 (7.1)
Dehydration 1 (3.6) 0 (0)
Hypomagnesaemia 1 (3.6) 0 (0)
Urination problem 2 (7.1) 0 (0)
Sexual dysfunction 2 (7.1) 0 (0)
Neurologic
Neuropathy 18 (64.3) 2 (7.1)
Anxiety/confusion 5 (17.1) 0 (0)
Dizziness 7 (25) 0 (0)
Headache 7 (25) 0 (0)
Hearing problems 2 (7.1) 0 (0)
Visual problems 6 (21.4) 0 (0)
Sleep disturbances 3 (10.7) 1 (3.6)
Infection/fever
Fever without infection 6 (21.4) 0 (0)
Infection 11 (39.3) 4 (14.3)
Dermatologic
Rash 13 (46.4) 1 (3.6)
Pruritus 2 (7.1) 0 (0)
Pigmentation changes 4 (14.3) 0 (0)
Alopecia 3 (10.7) 0 (0)
Musculoskeletal
Myalgia 6 (21.4) 1 (3.6)
Bone pain 5 (17.9) 1 (3.6)
Bleeding
Epistaxis 1 (3.6) 0 (0)
Brusing 5 (17.9) 2 (7.1)
(Continued)
Table 2. Adverse Events (n¼28) (Continued)
Event No. of Patients (%)
Patients WithAny Events
Patients WithGrade 3/4 Events
Constitutional/other
Fatigue 23 (82.1) 8 (28.6)
Rigors/chills 4 (14.3) 1 (3.6)
Night sweats 2 (7.1) 0 (0)
Lymphadenopathy 1 (3.6) 0 (0)
Splenomegaly 6 (21.4) 0 (0)
Weight changes 5 (17.9) 0 (0)
Original Article
3972 Cancer August 15, 2012

stable disease. There were no instances of acute leukemiatransformation or death throughout the study.
Extended Follow-Up Results
Extended follow-up data were available for 15 patents.The median extended follow-up was 24.1 months (range,5.2-75.8 months) for all evaluable patients, the medianPFS was 14.4 months (n¼ 14), and the median OS was21.4 months (n¼ 15). Disease progression with transfor-mation to acute myeloid leukemia was observed in 2patients, including 1 with CMML-1 and 1 with MDS/MPN-u. Both of these patients presented with myeloidsarcoma, the first at 6 months of follow-up and the secondat 20 months of follow-up. Only 2 of 15 patients com-pleted the full 6-month course of therapy with the 12-week cycle of TADA followed by maintenance thalido-mide. One of these patients, who remained alive at thetime of this report, had PMF with the JAK2V617F muta-tion and continued with stable disease at 52 months offollow-up. The second patient who completed therapyhad CMML-1 and achieved a PR with TADA. He died ofsuicide at 23 months of follow-up, at which point he wasstill in remission. At the time this report was in prepara-tion, 4 of 15 evaluable patients remained alive. In addition
to the aforementioned patient who had duplication ofchromosome 6, 3 other patients had normal karyotypes.Two of those patients had CMML-1 and had stable dis-ease on TADA. One of them carried a TET2 mutationand underwent an allogeneic stem cell transplantation at 5months of follow-up, and the second patient continued tobe transfusion-independent despite receiving no furthertherapy after the completion of TADA. The fourthpatient, who underwent previous renal transplantation,had MDS/MPN-u and did not respond to TADAtherapy.
DISCUSSIONPMF and overlap MDS/MPN remain considerable thera-peutic challenges, because current treatment options areonly modestly successful without durable responses.There are no drugs approved by the US Food and DrugAdministration specifically for MPNs, whereas the hypo-methyating agents (azacitidine and decitabine) includeCMML on their label based on limited overlap patientsenrolled on pivotal trials. Thus, these patients representan unmet therapeutic medical need, and only retrospec-tive, subgroup data support treatment approaches.
Table 3. Treatment Responsea
Patient Group IWG MDS ResponseCriteria
IWG Myelofibrosis Response Criteria
Response No. ofPatients (%)
Response No. ofPatients (%)
All patients, N¼ 28
ORR 6 (21.4)
PR 1 (3.6)
Clinical improvement: Hb, spleen 5 (17.9)
SD 14 (50)
MDS/MPN, N¼ 23
ORR 3 (13) ORR 5 (21.7)
HI-erythroid 2 (8.7) PR 1 (4.3)
HI-platelets 1 (4.3) Clinical improvement: Hb, spleen 4 (17.4)
SD 11 (47.8) SD 10 (43.5)
PMF, N¼ 5
ORR 1 (20)
PR 0 (0)
Clinical improvement: Hb 1 (20)
SD 4 (80)
Patients who completed at least one 12-wk cycle of therapy, N¼ 21b
ORRc 3 (17.6) ORR 6 (28.6)
HI-erythroid 2 (11.8) PR 1 (4.8)
HI-platelets 1 (5.9) Clinical improvement: Hb, spleen 5 (23.8)
SD 11 (64.7) SD 11 (52.4)
Abbreviations: Hb, hemoglobin; HI, hematologic improvement; IWG, International Working Group; MDS, myelodysplastic
syndrome; MPN, myeloproliferative neoplasm; ORR, overall response rate; PMF, primary myelofibrosis; PR, partial
response; SD, stable disease.aNo patient developed leukemic transformation or disease progression during thalidomide, arsenic trioxide, dexametha-
sone, and ascorbic acid (TADA) therapy.b Seventeen patients with MDS/MPN and 4 patients with PMF completed 1 cycle of therapy.c Responses according to IWG MDS response criteria were calculated only for patients with MDS/MPN.
TADA in MDS/Bejanyan et al
Cancer August 15, 2012 3973

The drugs included in the TADA combination,both independently and in limited combinations, havedemonstrated activity in both MPN and MDS. Whenused as monotherapies, higher drug doses usually arerequired to produce a clinical effect, even in previouslyuntreated or lower risk patients.32,35,36,48,49 Unfortu-nately, higher doses often cause intolerable medicationside effects, requiring discontinuation of effective thera-pies.23,48 Therefore, combining several effective agents atlower doses has become a common approach to overcomedose-limiting toxicities, particularly when those drugshave nonoverlapping mechanisms of action.
This study demonstrated that the TADA regimen issafe and tolerable enough that 75% of largely previouslytreated patients could complete an intensive 12-weektherapeutic course. The regimen also was moderatelyeffective and was comparable to recently reported, long-term follow-up data on 50 patients with PMF from theMayo Clinic27 in which IWG myelofibrosis response cri-teria were applied retrospectively to assess the response tothalidomide-prednisone alone or in combination witheither cyclophosphamide or etanercept. The reportedgrade 3/4 hematologic and neurologic toxicities werecomparable to those observed in our study. In anotherstudy, ATO in combination with low-dose thalidomideresulted in clinical responses in 25% of 28 patients withlower risk and higher risk MDS and CMML.37 Overall,the nonhematologic adverse events, again, were compara-ble to TADA, with fatigue, fluid retention, and dyspneaobserved in approximately 50% of patients followed byinfections (29%) and neuropathy (21%). In contrast toTADA therapy, hematologic toxicities, such as neutrope-nia and thrombocytopenia, were twice as common. Thali-domide produces favorable responses selectively amongpatients with erythroid linage MDS.34
The steroid component of TADA may be responsi-ble for the lower rates of neutropenia and thrombocytope-nia in our study. In 1 report, when prednisone wascombined with thalidomide, several patients with baselinethrombocytopenia experienced platelet count recovery inaddition to a hemoglobin response.22 The addition ofdexamethasone to ATO and thalidomide in our study didnot seem to adversely affect the toxicity profile of theTADA regimen and, thus, could be considered in combi-nations as tolerated to improve hematologic responses.More novel combinations with lenalidomide and predni-sone demonstrated responses in approximately 33% ofpatients with PMF.25 However, this effect was compro-mised by significant myelosuppression, with rates of grade3/4 neutropenia and anemia of 58% and 42%, respec-
tively. Another study that used single-agent lenalidomidefor PMF reported grade 3/4 neutropenia in approximately33% of enrolled patients.24 Comparing these results withthe rates of hematologic toxicity observed using theTADA regimen, neutropenia and thrombocytopenia ofany grade were observed in only 14% and 11% ofpatients, respectively. Only 1 patient in our study had todiscontinue the therapy because of hematologic toxicity,which was an episode of thrombocytopenia. Nonhemato-logic adverse effects were tolerable, and only 2 patientsrequired study withdrawal. Fatigue and fluid retentionwere the most common side effects, although they weremild to moderate in most patients.
Similar to our observation of responses observedpreferentially in patients who received a longer treatmentcourse, other studies have reported the achievement ofgreater hematologic responses in patients who received atleast 3 months of continuous therapy.34,50 Therefore, toachieve maximal effects and possibly durable responses totherapy, it is essential to find an optimal regimen withacceptable toxicity profile.
No major clinical differences were observed betweenresponders and nonresponders in our TADA study. Morethan half of the TADA participants had received therapiesfor their diseases before enrollment on this study. Thetreatment results did not differ significantly betweenuntreated and previously treated individuals, emphasizingthe benefit of combination therapy at any stage of disease.With the current availability of newer agents, such ashypomethylators, immunomodulatory derivatives, andJAK2 inhibitors, further opportunities will emerge fornew combination therapies, some of which already havedemonstrated promising clinical efficacy.28,30,38 Onenext, obvious step would be to substitute lenalidomide orpomolidomide for thalidomide in the current studydesign.
In conclusion, TADA appears to be relatively welltolerated and yields clinical responses in patients withPMF and MDS/MPD. The identification of novel pre-dictive biomarkers, such as cytokine profiles and 5-hydroxymethylcytosine levels, may help identify patientswho are more likely to respond to this regimen. It is possi-ble to design a tolerable combination regimen and toassess responses specifically for patients with overlapMDS/MPN, an orphan disease group in whom therapeu-tic options are limited.
FUNDING SOURCESThis investigation was supported in part by CephalonCorporation.
Original Article
3974 Cancer August 15, 2012

CONFLICT OF INTEREST DISCLOSURESThe authors made no disclosures.
REFERENCES1. Vardiman JW, Brunning RD, Arber DA, et al. Introduction and
overview of the classification of the myeloid neoplasms. In: Swer-dlow SH, Campo E, Harris NL, et al. eds. WHO Classification ofTumours of Haematopoietic and Lymphoid Tissues. Lyon, France:IARC Press; 2008:18-30.
2. Dingli D, Schwager SM, Mesa RA, Li CY, Dewald GW, Tefferi A.Presence of unfavorable cytogenetic abnormalities is the strongestpredictor of poor survival in secondary myelofibrosis. Cancer. 2006;106:1985-1989.
3. Gangat N, Caramazza D, Vaidya R, et al. DIPSS plus: a refinedDynamic International Prognostic Scoring System for primary myelo-fibrosis that incorporates prognostic information from karyotype, pla-telet count, and transfusion status. J Clin Oncol. 2011;29:392-397.
4. Passamonti F, Cervantes F, Vannucchi AM, et al. A dynamic prog-nostic model to predict survival in primary myelofibrosis: a studyby the IWG-MRT (International Working Group for Myeloproli-ferative Neoplasms Research and Treatment). Blood. 2010;115:1703-1708.
5. Onida F, Kantarjian HM, Smith TL, et al. Prognostic factors andscoring systems in chronic myelomonocytic leukemia: a retrospectiveanalysis of 213 patients. Blood. 2002;99:840-849.
6. James C, Ugo V, Le Couedic JP, et al. A unique clonal JAK2 muta-tion leading to constitutive signalling causes polycythaemia vera.Nature. 2005;434:1144-1148.
7. Kralovics R, Passamonati F, Buser AS, et al. A gain-of-functionmutation of JAK2 in myeloproliferative disorders. N Engl J Med.2005;352:1779-1790.
8. Tefferi A, Lasho TL, Patnaik MM, et al. JAK2 germline geneticvariation affects disease susceptibility in primary myelofibrosisregardless of V617F mutational status: nullizygosity for the JAK246/1 haplotype is associated with inferior survival. Leukemia. 2010;24:105-109.
9. Szpurka H, Jankowska AM, Makishima H, et al. Spectrum ofmutations in RARS-T patients includes TET2 and ASXL1 muta-tions. Leuk Res. 2010;34:969-973.
10. Gurevich I, Luthra R, Konoplev SN, Yin CC, Medeiros LJ, Lin P.Refractory anemia with ring sideroblasts associated with markedthrombocytosis: a mixed group exhibiting a spectrum of morpho-logic findings. Am J Clin Pathol. 2011;135:398-403.
11. Jankowska AM, Szpurka H, Tiu RV, et al. Loss of heterozygosity4q24 and TET2 mutations associated with myelodysplastic/myelo-proliferative neoplasms. Blood. 2009;113:6403-6410.
12. Delhommeau F, Dupont S, Della Valle V, et al. Mutation inTET2 in myeloid cancers. N Engl J Med. 2009;360:2289-2301.
13. Tefferi A. Novel mutations and their functional and clinical rele-vance in myeloproliferative neoplasms: JAK2, MPL, TET2, ASXL1,CBL, IDH and IKZF1. Leukemia. 2010;24:1128-1138.
14. Makishima H, Rataul M, Gondek LP, et al. FISH and SNP-A kar-yotyping in myelodysplastic syndromes: improving cytogeneticdetection of del(5q), monosomy 7, del(7q), trisomy 8 and del(20q).Leuk Res. 2010;34:447-453.
15. Sugimoto Y, Muramatsu H, Makishima H, et al. Spectrum of mo-lecular defects in juvenile myelomonocytic leukaemia includesASXL1 mutations. Br J Haematol. 2010;150:83-87.
16. Pardanani A, Lasho TL, Finke CM, Mai M, McClure RF, TefferiA. IDH1 and IDH2 mutation analysis in chronic-and blast-phasemyeloproliferative neoplasms. Leukemia. 2010;24:1146-1151.
17. Grand FH, Hidalgo-Curtis CE, Ernst T, et al. Frequent CBL muta-tions associated with 11q acquired uniparental disomy in myelopro-liferative neoplasms. Blood. 2009;113:6182-6192.
18. Oh ST, Simonds EF, Jones C, et al. Novel mutations in the inhibi-tory adaptor protein LNK drive JAK-STAT signaling in patientswith myeloproliferative neoplasms. Blood. 2010;116:988-992.
19. Abdel-Wahab O, Pardanani A, Patel LJ, et al. Concomitant analysisof EZH2 and ASXL1 mutations in myelofibrosis, chronic myelo-
monocytic leukemia and blast-phase myeloproliferative neoplasms[abstract]. Blood. 2010;116:3070.
20. Besa EC, Nowell PC, Geller NL, Gardner FH. Analysis of theandrogen response of 23 patients with agnogenic myeloid metapla-sia: the value of chromosomal studies in predicting response andsurvival. Cancer. 1982;49:308-313.
21. Cervantes F, Alvarez-Larran A, Domingo A, Arellano-Rodrigo E,Montserrat E. Efficacy and tolerability of danazol as a treatment forthe anaemia of myelofibrosis with myeloid metaplasia: long-termresults in 30 patients. Br J Haematol. 2005;129:771-775.
22. Mesa RA, Steensma DP, Pardanani A, et al. A phase 2 trial of com-bination low-dose thalidomide and prednisone for the treatment ofmyelofibrosis with myeloid metaplasia. Blood. 2003;101:2534-2541.
23. Thomas DA, Giles LFJ, Albitar M, et al. Thalidomide therapyfor myelofibrosis with myeloid metaplasia. Cancer. 2006;106:1974-1984.
24. Tefferi A, Cortes J, Verstovesk S, et al. Lenalidomide therapy inmyelofibrosis with myeloid metaplasia. Blood. 2006;108:1158-1164.
25. Quintas-Cardama A, Kantarjian HM, Manshouri T, et al. Lenalido-mide plus prednisone results in durable clinical, histopathologic,and molecular responses in patients with myelofibrosis. J ClinOncol. 2009;27:4760-4766.
26. Mesa RA, Yao X, Cripe LD, et al. Lenalidomide and prednisonefor myelofibrosis: Eastern Cooperative Oncology Group (ECOG)phase 2 trial E4903. Blood. 2010;116:4436-4438.
27. Thapaliya P, Tefferi A, Pardanani A, et al. International WorkingGroup for Myelofibrosis Research and Treatment response assess-ment and long-term follow-up of 50 myelofibrosis patients treatedwith thalidomide-prednisone based regimens. Am J Hematol. 2011;86:96-98.
28. Iastrebner M, Jang JH, Nucifora E, et al. Decitabine in myelodys-plastic syndromes and chronic myelomonocytic leukemia: Argenti-nian/South Korean multi-institutional clinical experience. LeukLymphoma. 2010;51:2250-2257.
29. Costa R, Abdulhaq H, Haq B, et al. Activity of azacitidine inchronic myelomonocytic leukemia. Cancer. 2011;117:2690-2696.
30. Scott BL, Ramakrishnan A, Storer B, et al. Prolonged responses inpatients with MDS and CMML treated with azacitidine and etaner-cept. Br J Haematol. 2010;148:944-947.
31. Vey N, Bosly A, Guerci A, et al. Arsenic trioxide in patients withmyelodysplastic syndromes: a phase II multicenter study. J ClinOncol. 2006;24:2465-2471.
32. Raza A, Meyer P, Dutt D, et al. Thalidomide produces transfusionindependence in long-standing refractory anemias of patients withmyelodysplastic syndromes. Blood. 2001;98:958-965.
33. Musto P, Falcone A, Sanpaolo G, Bisceglia M, Matera R, CarellaAM. Thalidomide abolishes transfusion-dependence in selectedpatients with myelodysplastic syndromes. Haematologica. 2002;87:884-886.
34. Musto P. Thalidomide therapy in adult patients with myelodysplas-tic syndrome: a North Central Cancer Treatment Group phase IItrial. Cancer. 2007;109:1211-1212; author reply 1212.
35. Strupp C, Germing U, Aivado M, Misgeld E, Haas R, GattermannN. Thalidomide for the treatment of patients with myelodysplasticsyndromes. Leukemia. 2002;16:1-6.
36. Moreno-Aspitia A, Colon-Otero G, Hoering A, et al. Thalidomidetherapy in adult patients with myelodysplastic syndrome. A NorthCentral Cancer Treatment Group phase II trial. Cancer. 2006;107:767-772.
37. Raza A, Buonamici S, Lisak L, et al. Arsenic trioxide and thalido-mide combination produces multi-lineage hematological responsesin myelodysplastic syndromes patients, particularly in those withhigh pretherapy EVI1 expression. Leuk Res. 2004;28:791-803.
38. Sekeres MA, Maciejewski JP, Erba HP, et al. A phase 2 study ofcombination therapy with arsenic trioxide and gemtuzumab ozoga-micin in patients with myelodysplastic syndromes or secondaryacute myeloid leukemia. Cancer. 2011;117:1253-1261.
39. List A, Shiller G, Mason J, Douer D, Ellison R. Trisenox (arsenictrioxide) in patients with myelodysplastic syndromes (MDS): pre-liminary findings in a phase II clinical study [abstract]. Blood.2003;102:422a.
TADA in MDS/Bejanyan et al
Cancer August 15, 2012 3975

40. Chen GQ, Shi ZG, Tang W, et al. Use of arsenic trioxide (As2O3)in the treatment of acute promyelocytic leukemia (APL): I. As2O3exerts dose-dependent dual effects on APL cells. Blood. 1997;89:3345-3353.
41. Chen GQ, Zhu J, Shi XG, et al. In vitro studies on cellular andmolecular mechanisms of arsenic trioxide (As2O3) in the treatmentof acute promyelocytic leukemia: As2O3 induces NB4 cell apoptosiswith downregulation of Bcl-2 expression and modulation of PML-RAR alpha/PML proteins. Blood. 1996;88:1052-1061.
42. Grad JM, Bahlis NJ, Reis I, Oshiro MM, Dalton WS, Boise LH.Ascorbic acid enhances arsenic trioxide-induced cytotoxicity in mul-tiple myeloma cells. Blood. 2001;98:805-813.
43. Dai J, Weinberg RS, Wasman S, Jing Y. Malignant cells can be sen-sitized to undergo growth inhibition and apoptosis by arsenic triox-ide through modulation of the glutathione redox system. Blood.1999;93:268-277.
44. Bahlis NJ, McCafferty-Grad J, Jordan-McMurry I, et al. Feasibilityand correlates of arsenic trioxide combined with ascorbic acid-medi-ated depletion of intracellular glutathione for the treatment ofrelapsed/refractory multiple myeloma. Clin Cancer Res. 2002;8:3658-3668.
45. Jaffe ES, Harris NL, Stein H, Vardiman JW, eds. World HealthOrganization Classification of Tumors of Hematopoietic andLymphoid Tissues. Lyon, France: IARC Press; 2001.
46. Cheson BD, Greenberg PL, Bennett JM, et al. Clinical applicationand proposal for modification of the International Working Group(IWG) response criteria in myelodysplasia. Blood. 2006;108:419-425.
47. Tefferi A, Barosi G, Mesa RA, et al. IWG for Myelofibrosis Researchand Treatment (IWG-MRT). International Working Group (IWG)consensus criteria for treatment response in myelofibrosis with mye-loid metaplasia, for the IWG for Myelofibrosis Research and Treat-ment (IWG-MRT). Blood. 2006;108:1497-1503.
48. Bouscary D, Legros L, Tulliez M, et al. for the Groupe Francais desMyelodysplasies (GFM). A nonrandomised dose-escalating phase IIstudy of thalidomide for the treatment of patients with low-risk mye-lodysplastic syndromes: the Thal-SMD-2000 trial of the GroupeFrancais des Myelodysplasies. Br J Haematol. 2005;131:609-618.
49. Bowen D, MacIlwaine L, Cavanaugh J, et al. Thalidomide therapyfor low-risk myelodysplasia. Leuk Res. 2005;29:235-236.
50. Jabbour E, Thomas D, Kantarjian H, et al. Comparison of thalido-mide and lenalidomide as therapy for myelofibrosis. Blood. 2011;118:899-902.
Original Article
3976 Cancer August 15, 2012