
How safe is curettage of low-grade cartilaginous neoplasms diagnosed by imaging with or without...
8
1098 THE BONE & JOINT JOURNAL ONCOLOGY How safe is curettage of low-grade cartilaginous neoplasms diagnosed by imaging with or without pre-operative needle biopsy? M. T. Brown, P. D. Gikas, J. S. Bhamra, J. A. Skinner, W. J. S. Aston, R. C. Pollock, A. Saifuddin, T. W. R. Briggs From London Bone and Soft Tissue Sarcoma Service, Royal National Orthopaedic Hospital, Stanmore, United Kingdom M. T. Brown, MB BS, BSc (Hons), MRCS (Eng), Specialist Registrar P. D. Gikas, MB BS (Hons), FRCS, MD, Specialist Registrar J. S. Bhamra, MB BS, BSc (Hons), MRCS (Eng), Clinical Research Fellow J. A. Skinner, MB BS, FRCS (Eng), FRCS (Orth), Consultant Orthopaedic Surgeon W. J. S. Aston, BSc, MB BS (Ed), FRCS (Ed), FRCS (Tr&Orth), Consultant Orthopaedic Surgeon R. C. Pollock, BSc (Hons), MB BS, FRCS (Eng), FRCS (Tr&Orth), Consultant Orthopaedic Surgeon A. Saifuddin, MBChB, MRCP, FRCR, Consultant Radiologist T. W. R. Briggs, MD (Res), MCh (Orth), FRCS (Ed), Consultant Orthopaedic Surgeon Royal National Orthopaedic Hospital, London Bone and Soft Tissue Sarcoma Service, Brockley Hill, Stanmore, Middlesex, HA7 4LP, UK. Correspondence should be sent to Mr M. T. Brown; e-mail: [email protected] ©2014 The British Editorial Society of Bone & Joint Surgery doi:10.1302/0301-620X.96B8. 32056 $2.00 Bone Joint J 2014;96-B:1098–105. Received 27 March 2013; Accepted after revision 20 March 2014 The pre-operative differentiation between enchondroma, low-grade chondrosarcoma and high-grade chondrosarcoma remains a diagnostic challenge. We reviewed the accuracy and safety of the radiological grading of cartilaginous tumours through the assessment of, first, pre-operative radiological and post-operative histological agreement, and second the rate of recurrence in lesions confirmed as high-grade on histology. We performed a retrospective review of major long bone cartilaginous tumours managed by curettage as low grade between 2001 and 2012. A total of 53 patients with a mean age of 47.6 years (8 to 71) were included. There were 23 men and 30 women. The tumours involved the femur (n = 20), humerus (n = 18), tibia (n = 9), fibula (n = 3), radius (n = 2) and ulna (n = 1). Pre-operative diagnoses resulted from multidisciplinary consensus following radiological review alone for 35 tumours, or with the addition of pre-operative image guided needle biopsy for 18. The histologically confirmed diagnosis was enchondroma for two (3.7%), low-grade chondrosarcoma for 49 (92.6%) and high-grade chondrosarcoma for two (3.7%). Three patients with a low-grade tumour developed a local recurrence at a mean of 15 months (12 to 17) post-operatively. A single high-grade recurrence (grade II) was treated with tibial diaphyseal replacement. The overall recurrence rate was 7.5% at a mean follow-up of 4.7 years (1.2 to 12.3). Cartilaginous tumours identified as low-grade on pre-operative imaging with or without additional image-guided needle biopsy can safely be managed as low-grade without pre-operative histological diagnosis. A few tumours may demonstrate high-grade features histologically, but the rates of recurrence are not affected. Cite this article: Bone Joint J 2014; 96-B:1098–105. Chondrosarcomas represent a heterogeneous group of tumours ranging from indolent and low-grade to aggressive and high-grade with the ability to metastasise. 1,2 They are the sec- ond most common primary malignant bone tumour after osteosarcoma. Management requires a multidisciplinary approach, combin- ing clinical assessment, radiological investiga- tions and histological grading. Primary chondrosarcomas arise de novo and comprise more than 85% of all chondrosarco- mas. They are most commonly located in the pel- vis, followed by the proximal femur, proximal humerus, distal femur and ribs. 1-3 Secondary chondrosarcomas arise from benign cartilaginous neoplasms, such as enchondromas or osteochon- dromas. Presenting symptoms are highly variable and many patients are asymptomatic, the diag- nosis being made incidentally on plain radio- graphs, and particularly MRI for conditions such as meniscal or rotator cuff tears. 4 Pain is the most common presenting symp- tom for cartilaginous neoplasms, followed by local swelling. Pain is present in between 81% 5 and 95% 6 of chondrosarcomas, compared with 37% 7 to 79% 6,8 of enchondromas, but it is likely that a selection bias over-estimates the latter. The pain associated with a chondro- sarcoma is typically insidious, progressive, worse at night and of longer duration (months or years); however, these features cannot relia- bly differentiate a chondrosarcoma from an enchondroma. 9 A palpable mass accompanies 28% to 82% of chondrosarcomas. 9 Enchon- dromas affecting the small bones of the hands and feet are more likely to present with pain and swelling than those in long bones. Surgical management remains the mainstay of treatment, as chondrosarcomas are rela- tively resistant to radiotherapy and chemother- apy. 1,10 The assessment of a chondrosarcoma in a long bone requires the combined review of the radiological appearance and the histologi- cal grade, as neither has sufficient specificity alone to differentiate a grade I chondro- sarcoma from an enchondroma. 7,11,12 Chon- drosarcomas are graded histologically into three grades (I–III). However, the staging
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of How safe is curettage of low-grade cartilaginous neoplasms diagnosed by imaging with or without...

1098 THE BONE & JOINT JOURNAL
ONCOLOGY
How safe is curettage of low-grade cartilaginous neoplasms diagnosed by imaging with or without pre-operative needle biopsy?
M. T. Brown,P. D. Gikas,J. S. Bhamra,J. A. Skinner,W. J. S. Aston,R. C. Pollock,A. Saifuddin,T. W. R. Briggs
From London Bone and Soft Tissue Sarcoma Service, Royal National Orthopaedic Hospital, Stanmore, United Kingdom
M. T. Brown, MB BS, BSc (Hons), MRCS (Eng), Specialist Registrar P. D. Gikas, MB BS (Hons), FRCS, MD, Specialist Registrar J. S. Bhamra, MB BS, BSc (Hons), MRCS (Eng), Clinical Research Fellow J. A. Skinner, MB BS, FRCS (Eng), FRCS (Orth), Consultant Orthopaedic Surgeon W. J. S. Aston, BSc, MB BS (Ed), FRCS (Ed), FRCS (Tr&Orth), Consultant Orthopaedic Surgeon R. C. Pollock, BSc (Hons), MB BS, FRCS (Eng), FRCS (Tr&Orth), Consultant Orthopaedic Surgeon A. Saifuddin, MBChB, MRCP, FRCR, Consultant Radiologist T. W. R. Briggs, MD (Res), MCh (Orth), FRCS (Ed), Consultant Orthopaedic SurgeonRoyal National Orthopaedic Hospital, London Bone and Soft Tissue Sarcoma Service, Brockley Hill, Stanmore, Middlesex, HA7 4LP, UK.
Correspondence should be sent to Mr M. T. Brown; e-mail: [email protected]
©2014 The British Editorial Society of Bone & Joint Surgerydoi:10.1302/0301-620X.96B8. 32056 $2.00
Bone Joint J 2014;96-B:1098–105. Received 27 March 2013; Accepted after revision 20 March 2014
The pre-operative differentiation between enchondroma, low-grade chondrosarcoma and high-grade chondrosarcoma remains a diagnostic challenge. We reviewed the accuracy and safety of the radiological grading of cartilaginous tumours through the assessment of, first, pre-operative radiological and post-operative histological agreement, and second the rate of recurrence in lesions confirmed as high-grade on histology. We performed a retrospective review of major long bone cartilaginous tumours managed by curettage as low grade between 2001 and 2012. A total of 53 patients with a mean age of 47.6 years (8 to 71) were included. There were 23 men and 30 women. The tumours involved the femur (n = 20), humerus (n = 18), tibia (n = 9), fibula (n = 3), radius (n = 2) and ulna (n = 1). Pre-operative diagnoses resulted from multidisciplinary consensus following radiological review alone for 35 tumours, or with the addition of pre-operative image guided needle biopsy for 18. The histologically confirmed diagnosis was enchondroma for two (3.7%), low-grade chondrosarcoma for 49 (92.6%) and high-grade chondrosarcoma for two (3.7%). Three patients with a low-grade tumour developed a local recurrence at a mean of 15 months (12 to 17) post-operatively. A single high-grade recurrence (grade II) was treated with tibial diaphyseal replacement. The overall recurrence rate was 7.5% at a mean follow-up of 4.7 years (1.2 to 12.3). Cartilaginous tumours identified as low-grade on pre-operative imaging with or without additional image-guided needle biopsy can safely be managed as low-grade without pre-operative histological diagnosis. A few tumours may demonstrate high-grade features histologically, but the rates of recurrence are not affected.
Cite this article: Bone Joint J 2014; 96-B:1098–105.
Chondrosarcomas represent a heterogeneousgroup of tumours ranging from indolent andlow-grade to aggressive and high-grade withthe ability to metastasise.1,2 They are the sec-ond most common primary malignant bonetumour after osteosarcoma. Managementrequires a multidisciplinary approach, combin-ing clinical assessment, radiological investiga-tions and histological grading.
Primary chondrosarcomas arise de novo andcomprise more than 85% of all chondrosarco-mas. They are most commonly located in the pel-vis, followed by the proximal femur, proximalhumerus, distal femur and ribs.1-3 Secondarychondrosarcomas arise from benign cartilaginousneoplasms, such as enchondromas or osteochon-dromas. Presenting symptoms are highly variableand many patients are asymptomatic, the diag-nosis being made incidentally on plain radio-graphs, and particularly MRI for conditions suchas meniscal or rotator cuff tears.4
Pain is the most common presenting symp-tom for cartilaginous neoplasms, followed bylocal swelling. Pain is present in between 81%5
and 95%6 of chondrosarcomas, comparedwith 37%7 to 79%6,8 of enchondromas, but itis likely that a selection bias over-estimates thelatter. The pain associated with a chondro-sarcoma is typically insidious, progressive,worse at night and of longer duration (monthsor years); however, these features cannot relia-bly differentiate a chondrosarcoma from anenchondroma.9 A palpable mass accompanies28% to 82% of chondrosarcomas.9 Enchon-dromas affecting the small bones of the handsand feet are more likely to present with painand swelling than those in long bones.
Surgical management remains the mainstayof treatment, as chondrosarcomas are rela-tively resistant to radiotherapy and chemother-apy.1,10 The assessment of a chondrosarcomain a long bone requires the combined review ofthe radiological appearance and the histologi-cal grade, as neither has sufficient specificityalone to differentiate a grade I chondro-sarcoma from an enchondroma.7,11,12 Chon-drosarcomas are graded histologically intothree grades (I–III). However, the staging

HOW SAFE IS CURETTAGE OF LOW-GRADE CARTILAGINOUS NEOPLASMS 1099
VOL. 96-B, No. 8, AUGUST 2014
system most often used is the Musculoskeletal TumourSociety (MSTS) system,13 which classifies them as eitherlow (MSTS stage I) or high grade (MSTS stage II). MSTSstage III tumours can be any grade with metastases. Severalstudies have reported the safety of intralesional curettage forthe treatment of low-grade chondrosarcomas (Table I),14-18
whereas for high-grade lesions resection is required.19,20
Grades I and III chondrosarcomas are regarded as low- andhigh-grade, respectively; however, grade II lesions are lessclearly defined as they may display both low- and high-grade features. After demonstrating similarities of outcomebetween grade I and II lesions, Reith, Horodyski andScarborough21 considered grade II to be low grade. In accord-ance with other authors, we classify grade II chondrosarcomasas high-grade.19,20
Differentiation between enchondroma and sequential his-tological grades on pre-operative imaging alone is compli-cated by interobserver variability, with the greatestdisagreement between enchondroma and low-gradechondrosarcoma.11,12 A reliable radiological technique fordifferentiating between low- and high-grade chondrosarco-mas has not been identified, although the MRI features ofdedifferentiated chondrosarcoma have been described.22
Pre-operative histological diagnosis provided by image-guided needle biopsy can accurately differentiate low- fromhigh-grade lesions.23 However, it is painful, expensive, andrisks seeding the tumour.24 Furthermore, the possibility ofmissing areas of high-grade tumour in a predominantlylow-grade lesion remains.
Recently, Berber et al25 reported their experience of themanagement of low-grade appendicular chondrosarcomas,which were diagnosed on imaging alone without pre-operative needle biopsy and treated with primary curettage;this was found to be a safe form of treatment. However,their study population involved patients with a pathologi-cally proven low-grade chondrosarcoma, followed byreview of the imaging to see which were diagnosed as lowgrade based on radiology. This methodology would not,therefore, include patients with a histological diagnosis ofhigh-grade chondrosarcoma who may have been treatedsurgically as low grade based on imaging features.
In this study we aimed to determine the prevalence ofareas of high-grade chondrosarcoma in a study population
treated surgically as low-grade chondrosarcoma on MRIcriteria alone, or MRI combined with image-guided needlebiopsy, and to determine whether this finding has anyimpact on the rate of local recurrence following curettage.
Patients and MethodsWe retrospectively reviewed cartilaginous neoplasms man-aged as low-grade chondrosarcomas with intralesionalcurettage between 2001 and 2012. Patients were identifiedfrom the pathology database of a supraregional sarcomaunit. All patients with central chondrosarcoma, irrespec-tive of grade that had been treated with primary curettagewere included in the study. The diagnosis was made pre-operatively by a multidisciplinary team, either after radio-logical review alone or with the addition of the results of animage-guided needle biopsy. Clinical information wastaken from patient notes, in addition to radiology and his-tological records. In line with similar studies, only longbone cartilaginous neoplasms were reviewed. Small bonechondral lesions are more likely to be enchondromas,which do not require surgery. The study had ethicalapproval.
The radiological grade was ascribed by a single consult-ant radiologist (AS) with seven years’ experience of imagingbone tumours at the start of the study. No grading system ispublished for the MRI diagnosis of chondrosarcoma, andthe suggested grade was based on experience using dataavailable in the literature. The MRI features consideredtypical for a low-grade chondral tumour (enchondroma orgrade I chondrosarcoma) were26 (1) a lobular intramedul-lary lesion with intermediate T1W signal intensity (SI),increased T2W/STIR SI with or without punctate areas ofsignal void corresponding to cartilaginous matrix mineral-isation and mild endosteal scalloping (Fig. 1); and (2) theabsence of oedema around the tumour, cortical expansion,periostitis, cortical destruction and soft-tissue extension.The latter features are considered to be suspicious for a high-grade chondrosarcoma, and all such lesions would undergopre-operative image-guided needle biopsy (Table II).26 Wecategorise endosteal scalloping as mild (involving < 1/3 corti-cal thickness), moderate (1/3 to 2/3) or severe (> 2/3).
The histological grading was based on the light micros-copy features according to the World Health Organization
Table I. Summary of studies dealing with the outcome of the management of low-grade chondral tumours
Study Total patients Treatments (number of cases)Mean follow-up in years (range)
Local recurrence number Metastasis number
Hanna et al (2009)14 39 Curettage and cementation 5.1 (3 to 8.7) 2 0Leerapun et al (2007)15 70 Curettage (13) 8.5 (0.2 to 22.8) 1 1 (same patient)
Wide resection (54) 1 2Marginal excision (3) 0 0
Donati et al (2010)16 31 Curettage (15) 13 (5.5 to 24.7) 2 0Resection (16) 0 0
Souna et al (2010)17 15 Curettage with cryotherapy (15) 8 (5 to 11) 2 0Mohler et al (2010)18 46 Curettage with cryotherapy (46) 3.9 (1.5 to 11.2) 2 0

1100 M. T. BROWN, P. D. GIKAS, J. S. BHAMRA, J. A. SKINNER, W. J. S. ASTON, R. C. POLLOCK, A. SAIFUDDIN, T. W. R. BRIGGS
THE BONE & JOINT JOURNAL
criteria (Table III).1 High cellularity, the presence of hostbone encasement, open chromatin, mucoid matrix qualityand an age > 45 years favour chondrosarcoma over enchon-droma.1 Where the biopsy showed a mixed grade, the highergrade was taken as the final grading. Bone scintigraphy mayreveal increased radionuclide uptake in long-bone chondro-sarcoma compared with enchondroma;27 however, thisimaging modality cannot reliably differentiate between low-grade chondrosarcoma and enchondroma. Confirmed high-grade chondrosarcomas at our unit are routinely imagedwith whole-body technetium (99mTc-MDP) bone scintigra-phy (Draximage, Diagnostic Imaging Ltd, Québec, Canada)and thoracic CT for the purposes of staging. The presence ofbone metastases in the absence of pulmonary metastases isextremely rare (and even rarer at presentation),28 and we donot use bone scintigraphy for the initial staging of chondro-sarcomas, irrespective of grade. This differs from its earlyroutine use in the assessment of patients with osteosarcomaand Ewing’s sarcoma in our unit.
Applying the above criteria we identified a total of 53patients managed with primary curettage for a chondro-
sarcoma, which was predicted to be low grade purely onMRI features in 35, or on MRI and image-guided needlebiopsy in 18. There were 23 men and 30 women, with amean age of 47.6 years (8 to 71). The lesions occurred mostcommonly in the femur (n = 20), followed by the humerus(n = 16), tibia (n = 9), fibula (n = 3), radius (n = 2) and ulna(n = 1) (Table IV).
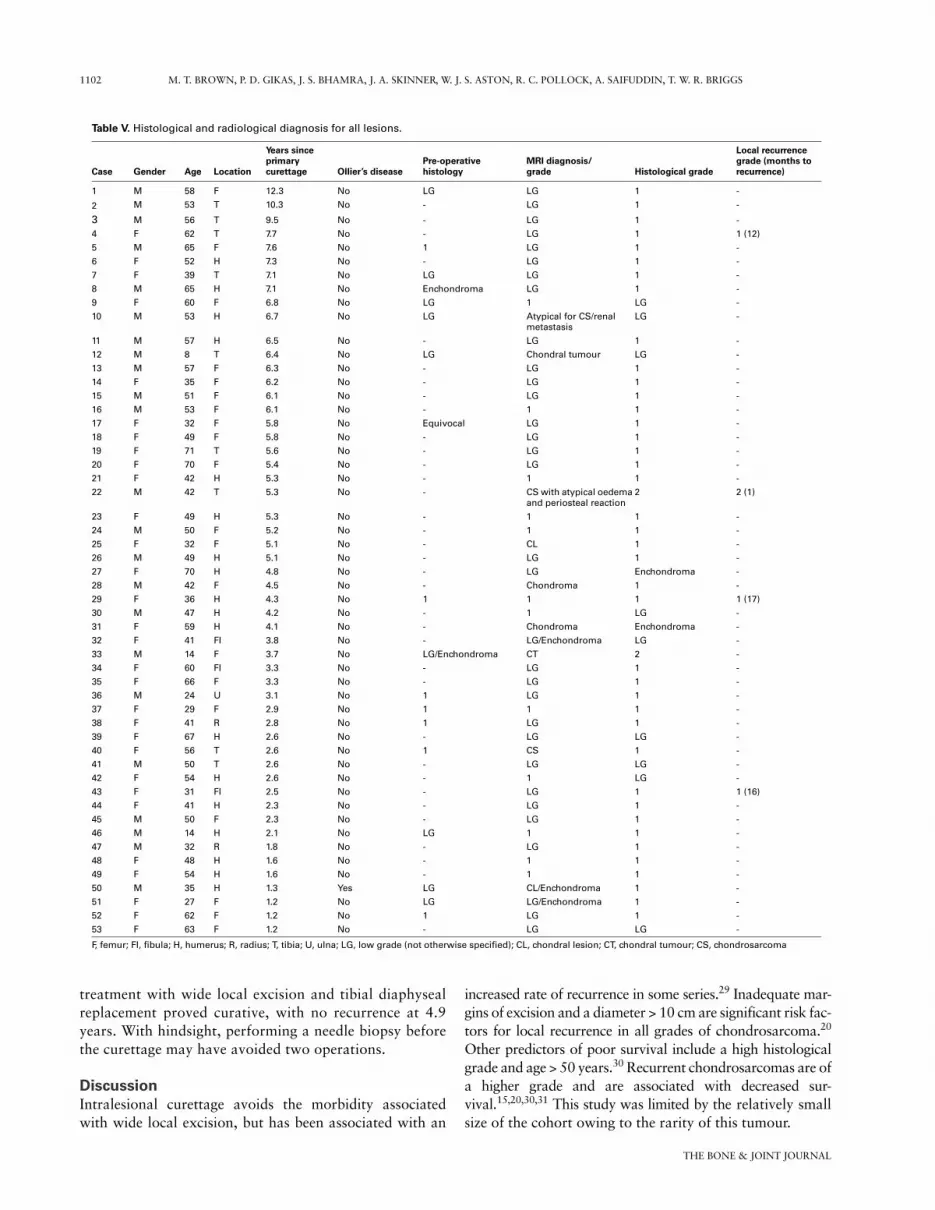
ResultsA diagnosis of chondrosarcoma was confirmed histologi-cally in 51 and enchondroma in two patients (Table V). Allthe chondrosarcomas were primary except for one second-ary grade I chondrosarcoma, which occurred in a patientwith Ollier’s disease. Both enchondromas occurred in theproximal humerus. A total of 49 chondrosarcomas werefound to be low grade and two were high grade, includingone that was a mixed grade I and II lesion and one that wasgrade II. No grade III chondrosarcomas were seen.
The mean follow-up after curettage was 4.7 years(1.2 to 12.3), with 26 patients (49%) followed-up formore than five years, including 18 diagnosed on MRI
Fig. 1a
Figure 1a – Typical MRI features of a low-grade chondral tumour. Coronal T1W SE image showing a lobularintermediate signal intensity lesion (arrows) with areas of punctate signal void consistent with matrix mineral-isation. Figure 1b – Axial STIR image shows the lesion (arrows) to be hyperintense. Note the absence of any per-ilesional oedema.
Fig. 1b
Table II. MRI features considered typical for low- and high-grade chondral tumours26
Low-grade features (diagnosis requires absence of all high-grade features below)
I Lobular intramedullary lesion with intermediate T1W signal intensity (SI)II Increased T2W/STIR SI with/without punctate areas of signal voidIII Mild endosteal scalloping (< 1/3 cortical thickness)
High-grade featuresI Peritumoural oedemaII Cortical expansionIII PeriostitisIV Cortical destructionV Soft-tissue extension

HOW SAFE IS CURETTAGE OF LOW-GRADE CARTILAGINOUS NEOPLASMS 1101
VOL. 96-B, No. 8, AUGUST 2014
alone and eight on MRI and biopsy. Those with follow-upfor five years included the earliest case of low-grade recur-rence (7.7 years’ follow-up), and a single high-grade recur-rence (5.3 years’ follow-up) (see Case 2 below).
Local recurrence was seen in three low-grade patients.The mean time to recurrence was 15 months (12 to 17).Two of these recurred once and were treated with repeatcurettage. The third recurred twice, initially at one year andagain at two years, and both were treated with furthercurettage with no subsequent recurrence for five years. Theoverall rate of recurrence was 7.5%.
The two high-grade tumours were located in the proxi-mal femur and tibia, respectively.Illustrative cases: case 1. A femoral chondrocarsoma wasdiagnosed in a 14-year-old boy with bilateral Perthes’ dis-ease and Stickler syndrome who had undergone a rightvarus femoral osteotomy. Routine biplanar imaging identi-fied a lytic lesion (Fig. 2a). However, the MRI report was of acartilaginous neoplasm (3.3 × 2.3 × 1.9 cm) (Figs. 2b and 2c).The diagnosis following image-guided biopsy was of a low-grade lesion, consistent with enchondroma. Internal fixa-tion was performed to reduce the risk of fracture of thefemoral neck, and this was combined with intralesionalcurettage. Histology demonstrated a grade I chondrosar-
coma with areas of grade II. No metastases were identifiedon thoracic CT and radionuclide bone scans. After multi-disciplinary discussion and consultation with the patient,regular surveillance was favoured over resection. Surveil-lance continues with no recurrence 3.7 years after surgery.Illustrative cases: case 2. A grade II tibial chondrosarcomawas complicated by recurrence one month after curettage.The 42-year-old man had originally presented with a four-month history of pain and swelling in the proximal lefttibia. Radiographs had shown a mildly expansile, well-defined lytic lesion with a mild solid periosteal reaction,endosteal scalloping and punctate mineralisation(Fig. 3a). MRI scans revealed features consistent with alow-grade chondrosarcoma with reactive perilesionalmedullary oedema (Figs 3b and 3c). Although this featurewas considered atypical, needle biopsy was not per-formed. The lesion, which was presumed to be a low-grade chondrosarcoma after multidisciplinary consensus,was treated by curettage with the addition of bonecement. The histological diagnosis was of a grade IIchondrosarcoma with no evidence of dedifferentiation.Biplanar radiography four weeks post-operatively showedsome periosteal reaction and a possible breach of the lat-eral cortex. MRI confirmed local recurrence (Fig. 4) and
Table III. World Health Organization light microscopic histological grading criteriafor primary central chondrosarcoma (excluding hand and foot)1
Grade I
I Moderate cellularityI Hyperchromatic, plump nuclei of uniform sizeIII Occasional binucleated cells
Grade II (including grade I appearances)IV Mitoses are absentI Increased cellularityII Increased nuclear atypia (size and shape), hyperchromasia and nuclear sizeIII Mitoses can be found
Grade III (including grade I and II appearances)I Increased cellularity, pleomorphism and atypiaII Mitoses easily detected
Table IV. Summary of location and grade of chondrosarcomas and enchondromas
Location Incidence Low-grade High-grade
Chondrosarcoma Femur 20 19 1Humerus 16 16 0Tibia 9 8 1Radius 2 2 0Fibula 3 3 0Ulna 1 1 0
Enchondroma Humerus 2 N/A N/ATotal 53 49 2
1102 M. T. BROWN, P. D. GIKAS, J. S. BHAMRA, J. A. SKINNER, W. J. S. ASTON, R. C. POLLOCK, A. SAIFUDDIN, T. W. R. BRIGGS
THE BONE & JOINT JOURNAL
treatment with wide local excision and tibial diaphysealreplacement proved curative, with no recurrence at 4.9years. With hindsight, performing a needle biopsy beforethe curettage may have avoided two operations.
DiscussionIntralesional curettage avoids the morbidity associatedwith wide local excision, but has been associated with an
increased rate of recurrence in some series.29 Inadequate mar-gins of excision and a diameter > 10 cm are significant risk fac-tors for local recurrence in all grades of chondrosarcoma.20
Other predictors of poor survival include a high histologicalgrade and age > 50 years.30 Recurrent chondrosarcomas are ofa higher grade and are associated with decreased sur-vival.15,20,30,31 This study was limited by the relatively smallsize of the cohort owing to the rarity of this tumour.
Table V. Histological and radiological diagnosis for all lesions.
Case Gender Age Location
Years since primarycurettage Ollier’s disease
Pre-operative histology
MRI diagnosis/grade Histological grade
Local recurrence grade (months to recurrence)
1 M 58 F 12.3 No LG LG 1 -
2 M 53 T 10.3 No - LG 1 -
3 M 56 T 9.5 No - LG 1 -
4 F 62 T 7.7 No - LG 1 1 (12)
5 M 65 F 7.6 No 1 LG 1 -
6 F 52 H 7.3 No - LG 1 -
7 F 39 T 7.1 No LG LG 1 -
8 M 65 H 7.1 No Enchondroma LG 1 -
9 F 60 F 6.8 No LG 1 LG -
10 M 53 H 6.7 No LG Atypical for CS/renal metastasis
LG -
11 M 57 H 6.5 No - LG 1 -
12 M 8 T 6.4 No LG Chondral tumour LG -
13 M 57 F 6.3 No - LG 1 -
14 F 35 F 6.2 No - LG 1 -
15 M 51 F 6.1 No - LG 1 -
16 M 53 F 6.1 No - 1 1 -
17 F 32 F 5.8 No Equivocal LG 1 -
18 F 49 F 5.8 No - LG 1 -
19 F 71 T 5.6 No - LG 1 -
20 F 70 F 5.4 No - LG 1 -
21 F 42 H 5.3 No - 1 1 -
22 M 42 T 5.3 No - CS with atypical oedema and periosteal reaction
2 2 (1)
23 F 49 H 5.3 No - 1 1 -
24 M 50 F 5.2 No - 1 1 -
25 F 32 F 5.1 No - CL 1 -
26 M 49 H 5.1 No - LG 1 -
27 F 70 H 4.8 No - LG Enchondroma -
28 M 42 F 4.5 No - Chondroma 1 -
29 F 36 H 4.3 No 1 1 1 1 (17)
30 M 47 H 4.2 No - 1 LG -
31 F 59 H 4.1 No - Chondroma Enchondroma -
32 F 41 FI 3.8 No - LG/Enchondroma LG -
33 M 14 F 3.7 No LG/Enchondroma CT 2 -
34 F 60 FI 3.3 No - LG 1 -
35 F 66 F 3.3 No - LG 1 -
36 M 24 U 3.1 No 1 LG 1 -
37 F 29 F 2.9 No 1 1 1 -
38 F 41 R 2.8 No 1 LG 1 -
39 F 67 H 2.6 No - LG LG -
40 F 56 T 2.6 No 1 CS 1 -
41 M 50 T 2.6 No - LG LG -
42 F 54 H 2.6 No - 1 LG -
43 F 31 FI 2.5 No - LG 1 1 (16)
44 F 41 H 2.3 No - LG 1 -
45 M 50 F 2.3 No - LG 1 -
46 M 14 H 2.1 No LG 1 1 -
47 M 32 R 1.8 No - LG 1 -
48 F 48 H 1.6 No - 1 1 -
49 F 54 H 1.6 No - 1 1 -
50 M 35 H 1.3 Yes LG CL/Enchondroma 1 -
51 F 27 F 1.2 No LG LG/Enchondroma 1 -
52 F 62 F 1.2 No 1 LG 1 -
53 F 63 F 1.2 No - LG LG -
F, femur; FI, fibula; H, humerus; R, radius; T, tibia; U, ulna; LG, low grade (not otherwise specified); CL, chondral lesion; CT, chondral tumour; CS, chondrosarcoma

HOW SAFE IS CURETTAGE OF LOW-GRADE CARTILAGINOUS NEOPLASMS 1103
VOL. 96-B, No. 8, AUGUST 2014
Hanna et al14 reported a series of 39 low-grade chondro-sarcomas that were treated by curettage and cementation,with local recurrence in two patients (5%) and no metasta-ses at a mean follow-up of 5.1 years (3 to 8.7) (Table I).Clinical review using the MSTS score showed good func-tional outcomes with a mean score of 94% (79% to100%). Leerapun et al15 demonstrated no difference inoverall disease-free survival and the incidence of localrecurrence or metastasis between patients with grade I pri-mary chondrosarcoma treated with either curettage or wideen bloc resection. Donati et al16 reported two recurrences in15 patients who had been managed with intralesional resec-tion, and no recurrences in 16 patients managed with wideresection at a mean follow-up of 157 months (66 to 296).Souna et al17 reported no local recurrence or metastasis in
15 patients with grade I intramedullary chondrosarcoma ofa long bone managed with curettage and cryotherapy aftera mean follow-up of more than five years. Mohler et al18
used curettage with cryotherapy in the treatment of 46grade I chondrosarcomas and reported a recurrence in twopatients (4.3%) at a mean follow-up of 47 months (18 to132). The evidence for the efficacy of curettage of low-grade lesions is further supported by a recent systematicreview and meta-analysis by Hickey et al32 which comparedcurettage with wide resection of grade I chondrosarcomasand, from a relatively small sample size of 190 tumours,concluded that neither treatment has an increased risk oflocal recurrence or metastasis.
The role of needle biopsy in the pre-operative assessmentof appendicular chondral tumours has previously been
Fig. 2a
Case 1. Figure 2a – Anteroposterior radiograph of the left hip showing a lobular lytic lesion (arrows) in the left femoral neck. Figure 2b – CoronalT1W SE MR image, and c) axial STIR image showing a lesion (arrows) with features that would be consistent with a low-grade chondral tumour.
Fig. 2cFig. 2b
Fig. 3a
Case 2. Figure 3a - Anteroposterior radiograph of the left tibia showing a lobular lytic lesion (arrows) in the proximal tibial diaphysis withmatrix mineralisation and mild solid periosteal response. Figure 3b - Coronal T1W SE MR image and c) axial STIR image showing a lesionwith features that would be consistent with a chondral tumour. However, the presence of perilesional oedema-like marrow signal (arrows)is an atypical finding for a low-grade tumour.
Fig. 3cFig. 3b

1104 M. T. BROWN, P. D. GIKAS, J. S. BHAMRA, J. A. SKINNER, W. J. S. ASTON, R. C. POLLOCK, A. SAIFUDDIN, T. W. R. BRIGGS
THE BONE & JOINT JOURNAL
investigated. We recently reported an 89.5% rate of accuracywhen grading chondrosarcomas and a 93.6% rate of accu-racy when distinguishing low- from high-grade tumoursusing image-guided needle biopsy.23 Berber et al25 reportedthe safety of curettage in the treatment of enchondroma orlow-grade chondrosarcoma diagnosed with pre-operativeimaging only, without biopsy (n = 53). In our study mostpatients (n = 35, 66%) were treated surgically, based purelyon the MRI features. Patients who underwent pre-operativeneedle biopsy (n = 18) were mostly those in the early years ofthe study, when there was less experience and confidence inmaking the diagnosis purely on MRI appearances, or if therewere unusual features such as atypical location (e.g. the fem-oral condyle). Few authors have evaluated the value ofpositron emission tomography (PET) to differentiateenchondroma from chondrosarcoma and predict out-come, but Brenner, Conrad and Eary33 supported its use.We do not currently use PET for this purpose.
This study provides further evidence for the safety of thisapproach as long as strict criteria are adhered to in the MRIdiagnosis of a low-grade chondral tumour, emphasising theimportance of a multidisciplinary approach. The low riskof local recurrence and metastatic disease allows a moreconservative surgical approach for low-grade tumours,with curettage providing an effective treatment that permitspreservation of the limb and decreased morbidity. As aresult of these findings, biopsy is only performed in our unitif chondral lesions demonstrate atypical or inconclusivefeatures on MRI. Curettage of low-grade tumours whenrelying on pre-operative radiology with or without addi-tional needle biopsy will result in only a small proportiondemonstrating high-grade features on histology. Only twohigh-grade chondrosarcomas were identified. The first washighly atypical, being a femoral neck lesion in a 14-year-old
boy identified incidentally during the management ofPerthes’ disease. Owing to the unclear nature of the lesion,pre-operative needle biopsy was undertaken, yielding adiagnosis of low-grade chondrosarcoma. The curettedspecimen revealed small areas of grade II tumour in a lesionthat was predominantly grade I, and the patient remainswell following curettage alone. The second patient with agrade II chondrosarcoma should ideally have undergonepre-operative needle biopsy because of the presence of reac-tive perilesional medullary oedema. The diagnosis of agrade II lesion would have been made and the patienttreated primarily with resection and diaphyseal replace-ment.
We conclude that cartilaginous tumours which are diag-nosed as low-grade on MRI alone or with the addition ofimage-guided needle biopsy can be safely managed withintralesional curettage. Furthermore, the finding of high-grade areas histologically is rare, and may not affect theoverall rate of local recurrence.
No benefits in any form have been received or will be received from a commer-cial party related directly or indirectly to the subject of this article.
This article was primary edited by J. Scott and first proof edited by G. Scott.
References1. Fletcher CDM, Bridge JA, Hogendoorn P, Mertens F. WHO Classification of
Tumours of Soft Tissue and Bone, Fourth Edition. Lyon: IARC Press, 2013.2. Gelderblom H, Hogendoorn PC, Dijkstra SD, et al. The clinical approach towards
chondrosarcoma. Oncologist 2008;13:320–329.3. Pring ME, Weber KL, Unni KK, Sim FH. Chondrosarcoma of the pelvis. A review of
sixty-four cases. J Bone Joint Surg [Am] 2001;83-A:1630–1642.4. Kransdorf MJ, Peterson JJ, Bancroft LW. MR imaging of the knee: incidental
osseous lesions. Magn Reson Imaging Clin N Am 2007;15:13–24.5. Björnsson J, McLeod RA, Unni KK, Ilstrup DM, Pritchard DJ. Primary chondro-
sarcoma of long bones and limb girdles. Cancer 1998;83:2105–2119.6. Murphey MD, Flemming DJ, Boyea SR, et al. Enchondroma versus chondrosar-
coma in the appendicular skeleton: differentiating features. Radiographics1998;18:1213–1237.
7. Geirnaerdt MJ, Hermans J, Bloem JL, et al. Usefulness of radiography in differ-entiating enchondroma from central grade 1 chondrosarcoma. AJR Am J Roentgenol1997;169:1097–1104.
8. Potter BK, Freedman BA, Lehman RA Jr, et al. Solitary epiphyseal enchondro-mas. J Bone Joint Surg [Am] 2005;87-A:1551–1560.
9. Murphey MD, Walker EA, Wilson AJ, et al. From the archives of the AFIP: imag-ing of primary chondrosarcoma: radiologic-pathologic correlation. Radiographics2003;23:1245–1278.
10. Eriksson AI, Schiller A, Mankin HJ. The management of chondrosarcoma of bone.Clin Orthop Relat Res 1980;153:44–66.
11. Skeletal Lesions Interobserver Correlation among Expert Diagnosticians(SLICED) Study Group. Reliability of histopathologic and radiologic grading of car-tilaginous neoplasms in long bones. J Bone Joint Surg [Am] 2007;89-A:2113–2123.
12. Eefting D, Schrage YM, Geirnaerdt MJ, et al. Assessment of interobserver vari-ability and histologic parameters to improve reliability in classification and grading ofcentral cartilaginous tumors. Am J Surg Pathol 2009;33:50–57.
13. Enneking WF. A system of staging musculoskeletal neoplasms. Clin Orthop RelatRes 1986;204:9–24.
14. Hanna SA, Whittingham-Jones P, Sewell MD, et al. Outcome of intralesionalcurettage for low-grade chondrosarcoma of long bones. Eur J Surg Oncol2009;35:1343–1347.
15. Leerapun T, Hugate RR, Inwards CY, Scully SP, Sim FH. Surgical managementof conventional grade I chondrosarcoma of long bones. Clin Orthop Relat Res2007;463:166–172.
16. Donati D, Colangeli S, Colangeli M, Di Bella C, Bertoni F. Surgical treatment ofgrade I central chondrosarcoma. Clin Orthop Relat Res 2010;468:581–589.
17. Souna BS, Belot N, Duval H, Langlais F, Thomazeau H. No recurrences inselected patients after curettage with cryotherapy for grade I chondrosarcomas. ClinOrthop Relat Res 2010;468:1956–1962.
Fig. 4
Case 2. Coronal T1W SE MR imagetwo months after primary curettage,showing a local recurrence (arrow)distal to the cement.

HOW SAFE IS CURETTAGE OF LOW-GRADE CARTILAGINOUS NEOPLASMS 1105
VOL. 96-B, No. 8, AUGUST 2014
18. Mohler DG, Chiu R, McCall DA, Avedian RS. Curettage and cryosurgery for low-grade cartilage tumors is associated with low recurrence and high function. ClinOrthop Relat Res 2010;468:2765–2773.
19. Lee FY, Mankin HJ, Fondren G, et al. Chondrosarcoma of bone: an assessment ofoutcome. J Bone Joint Surg [Am] 1999;81-A:326–338.
20. Fiorenza F, Abudu A, Grimer RJ, et al. Risk factors for survival and local control inchondrosarcoma of bone. J Bone Joint Surg [Br] 2002;84-B:93–99.
21. Reith JD, Horodyski MB, Scarborough MT. Grade 2 chondrosarcoma: stage I orstage II tumor? Clin Orthop Relat Res 2003;415:45–51.
22. MacSweeney F, Darby A, Saifuddin A. Dedifferentiated chondrosarcoma of theappendicular skeleton: MRI-pathological correlation. Skeletal Radiol 2003;32:671–678.
23. Jennings R, Riley N, Rose B, et al. An evaluation of the diagnostic accuracy of thegrade of preoperative biopsy compared to surgical excision in chondrosarcoma of thelong bones. Int J Surg Oncol 2010;2010:270195.
24. Mankin HJ, Lange TA, Spanier SS. The hazards of biopsy in patients with malig-nant primary bone and soft-tissue tumors. J Bone Joint Surg [Am] 1982;64-A:1121–1127.
25. Berber O, Datta G, Sabharwal S, et al. The safety of direct primary excision oflow-grade chondral lesions based on radiological diagnosis alone. Acta Orthop Belg2012;78:254–262.
26. Douis H, Saifuddin A. The imaging of cartilaginous bone tumours. II. Chondrosar-coma. Skeletal Radiol 2013;42:611–626.
27. Murphey MD, Walker EA, Wilson AJ, et al. From the archives of the AFIP: imag-ing of primary chondrosarcoma: radiologic-pathologic correlation. Radiographics2003;23:1245–1278.
28. Douis H, James SL, Grimer RJ, Davies MA. Is bone scintigraphy necessary in theinitial surgical staging of chondrosarcoma of bone? Skeletal Radiol 2012;41:429–436.
29. Ozaki T, Lindner N, Hillmann A, et al. Influence of intralesional surgery on treat-ment outcome of chondrosarcoma. Cancer 1996;77:1292–1297.
30. Söderström M, Ekfors TO, Böhling TO, et al. No improvement in the overall sur-vival of 194 patients with chondrosarcoma in Finland in 1971-1990. Acta OrthopScand 2003;74:344–350.
31. Schwab JH, Wenger D, Unni K, Sim FH. Does local recurrence impact survival inlow-grade chondrosarcoma of the long bones? Clin Orthop Relat Res 2007;462:175–180.
32. Hickey M, Farrokhyar F, Deheshi B, Turcotte R, Ghert M. A systematic reviewand meta-analysis of intralesional versus wide resection for intramedullary grade Ichondrosarcoma of the extremities. Ann Surg Oncol 2011;18:1705–1709.
33. Brenner W, Conrad EU, Eary JF. FDG PET imaging for grading and prediction of out-come in chondrosarcoma patients. Eur J Nucl Med Mol Imaging 2004;31:189–195.














![Accuracy of distinguishing between dysembryoplastic neuroepithelial tumors and other epileptogenic brain neoplasms with [11C]methionine PET](https://static.fdokumen.com/doc/165x107/63360da5cd4bf2402c0b568c/accuracy-of-distinguishing-between-dysembryoplastic-neuroepithelial-tumors-and-other.jpg)





