Deep dermal burn injury results in scarless wound healing in the ovine fetus
Upload
independentCategory
view
0download
0
CLINICAL ISSUES
Risk factors for deep sternal wound infections after cardiac surgery in
Jordan
Ibtisam M Al-Zaru, Ali A Ammouri, Mousa A Al-Hassan and Anas A Amr
Aim. The purpose of this study was to assess rates of and risk factors for deep sternal wound infection after coronary artery
bypass grafting surgery.
Background. Deep sternal wound infection is one of the most devastating complications of cardiac surgery, resulting in multiple
operative and non-operative procedures and increased hospital costs.
Design. A retrospective design using an existing coronary artery surgery database of adults (n = 206) who had undergone
coronary artery bypass grafting surgeries between January 2004–January 2006 at a university affiliated hospital, northern
Jordan was used.
Method. Multiple logistic regression analyses were used to asses rates of and risk factors for deep sternal wound infection.
Results. Deep sternal wound infection incidence rate was 22% of the total sample. Risk factors of deep sternal wound infection
include: (1) diabetes (OR = 0Æ317, p = 0Æ048), (2) Obesity (OR = 0Æ275, p = 0Æ011), (3) duration of surgery (OR = 4Æ22,
p = 0Æ032) and (4) use of intraaortic balloon pump (OR = 0Æ033, p = 0Æ001).
Conclusion. The proposed model provides a preliminary indication of risk factors placing coronary artery bypass grafting
patients at risk of DSWI. Further investigations and testing of the model are needed.
Relevance to clinical practice. Determining patients who are at risk of developing deep sternal wound infection after cardiac
surgeries is the first step towards its prevention.
Key words: coronary artery bypass grafting, deep sternal wound infection, infection, Jordan, risk, wounds
Accepted for publication: 15 July 2009
Introduction
Coronary heart disease (CHD) remains the leading cause of
death in developing and developed countries (World Health
Organization 2006). In Jordan, 30,491 patients of coronary
artery diseases were reported in the year 2005 and they were
responsible for 38% of the main causes of mortality (Jordan
Ministry of Health [MOH] 2005, CDC 2006). Coronary
artery bypass grafting (CABG) was considered one of the
major surgical procedures used to alleviate symptoms of
CHD. In Jordan, the number of CABG surgeries has
dramatically increased since 1990; with 3000 cardiac surger-
ies annually (MOH 2005). Although CABG surgery has great
advantages of minimising morbidity and mortality, it poses a
great threat to life and future health (Borger et al. 1998,
Orenstein et al. 2005).
One of the major complications after CABG surgery is
deep sternal wound infection (DSWI) which is an infection of
the anterior mediastinal space involving muscle, bone and/or
mediastinum (Garner et al. 1988). The documented incidence
Authors: Ibtisam M Al-Zaru, PhD, RN, Assistant Professor, Faculty
of Nursing, Jordan University of Science & Technology, Irbid; Ali A
Ammouri, PhD, RN, MSN, Assistant Professor, School of Nursing,
Hashemite University, Zarqa; Mousa A Al-Hassan, PhD, RN,
Associate Professor, Faculty of Nursing, Jordan University of
Science & Technology, Irbid; Anas A Amr, RN, MSN, Registered
Nurse, King Abdullah University Hospital, Irbid, Jordan
Correspondence: Ali Ammouri, Assistant Professor, School of
Nursing, Hashemite University, PO Box 150459, Zarqa 13115,
Jordan. Telephone: 962 5 3903333 ext. 4621.
E-mail: [email protected], [email protected]
� 2010 Blackwell Publishing Ltd, Journal of Clinical Nursing, 19, 1873–1881 1873
doi: 10.1111/j.1365-2702.2010.03193.x

of DSWI varies from 0Æ6–3% (Vaska 1993, Borger et al.
1998, Baskett et al. 1999, Olsen et al. 2002). DSWI is one of
the most devastating complications of cardiac surgery,
resulting in multiple operative and non-operative procedures
and increased hospital costs with some patients requiring
hospitalisation as long as six months (Hollenbeak et al.
2000, Orenstein et al. 2005). The result of this complication
is a mortality of 8Æ6–47% (De Feo et al. 2001, Olsen et al.
2002). Therefore, understanding of risk factors of DSWI
post-CABG may provide information to alert nurses to
patients who are at risk and optimise the preoperative health
status of CABG patients.
Background
Many risk factors have been identified as independent predic-
tors for DSWI following CABG, which include preoperative
risk factors (e.g., age, gender, obesity, smoking,, chronic
obstructive pulmonary disease (COPD), hypertension, diabe-
tes mellitus and emergency cardiac surgery); intraoperative
risk factors [e.g., use of internal mammary arteries (IMA) and
long duration of surgery and cardiopulmonary bypass (CPB)
time] and postoperative risk factors (e.g., prolonged mechan-
ical ventilation, re-exploration for bleeding and haemody-
namically complicated postoperative course) (Troutman et al.
2001, Ku et al. 2005, Toumpoulis et al. 2005).
The sternal wound infection prediction model provided the
framework for this study (Hussey et al. 1998). This regres-
sion model identified preoperative, intraoperative and post-
operative patient characteristics considered as risk factors for
postoperative DSWI. Assessing relationships between presur-
gical patient characteristics and incidence of DSWI may be
important for early intervention and care-related decisions by
nurses as well as other health care providers, patients and
family members.
Preoperative risk factors
Many studies of DSWI following CABG surgery have
attempted to identify preoperative risk factors for infection.
Some risk factors emerge from several studies and are well
documented that include advanced age, male gender, female
gender, obesity, diabetes, COPD, current smoking and urgent
CABG procedure (Borger et al. 1998, Vuorisalo et al. 1998,
McConkey et al. 1999, Sofer et al. 1999, Thomas et al. 1999,
Orhan et al. 2004). Diabetes mellitus has been proven to be
the most independent risk factor for DSWI following open
heart procedures (Swenne 2006). It increases the incidence of
infection up to fivefold over the normal population (Toum-
poulis et al. 2005).
Obesity is often considered to be a significant risk factor
and an independent predictor for the development of post-
operative DSWI (Zacharias & Habib 1996, Cayci et al.
2008). DSWI occurs twice as frequently in obese individuals
and nearly threefold in those who are severely obese
(Birkmeyer et al. 1998). Also, COPD was found to be an
independent risk factor associated with the development of
DSWI. Patients with COPD have greater colonisation of
bacteria that may lead to prolonged ventilator time after
surgery; patients on the ventilator longer than 48 hours had a
9Æ5-fold greater chance of developing deep sternal wound
infection (Baskett et al. 1999, Khan et al. 2000).
Intraoperative risk factors
Researchers found that the incidence of deep sternal wound
infection increased with the use of a single IMA and increased
further with the use of bilateral IMA on patients with
diabetes (De Paulis et al. 2005). In addition, harvesting of a
unilateral IMA caused a decrease in the blood supply to the
chest area, increased duration of surgery and increased
bleeding postoperatively (Sethi et al. 1991, Carrier et al.
1992).
Higher infection rates have been associated with surgical
time longer than four hours; the risk of developing a DSWI
increased 1Æ47-fold for every hour the operation continued
(Kirkland et al. 1999). Extended time on cardiopulmonary
bypass (CPB) is also linked to higher infection rates. The
consequences of CPB increase the likelihood of patients’ need
for blood products, having an extended time on the ventila-
tor, or requiring inotropic support, also increase the risk of
postoperative infection. (Borger et al. 1998, Jaffe & Samm-
uels 1999).
Postoperative risk factors
Patients having postoperative courses complicated by cardiac
arrest with cardiopulmonary resuscitation, bleeding requiring
re-exploration and poor haemodynamics requiring inotropic
support are at increased risk of developing DSWI (Borger
et al. 1998, Khan et al. 2000). Cardiopulmonary resuscita-
tion places the sternum at risk of fracture or dehiscence and
the body diverts blood to vital organs only (Vaska 1993). In
addition, patients requiring re-exploration for bleeding
within the first postoperative days had a 3Æ5- fold higher risk
of a DSWI (Khan et al. 2000). Furthermore, re-exploration
also carries a high likelihood of blood transfusions, inotropic
support, increased length of stay in intensive care unit (ICU)
and ‘ventilation’ time (Milano et al. 1995, Borger et al. 1998,
Baskett et al. 1999). Postoperative length of stay in ICU,
IM Al-Zaru et al.
1874 � 2010 Blackwell Publishing Ltd, Journal of Clinical Nursing, 19, 1873–1881

mechanical ventilator and blood transfusion were found to
have significant effects on development of DSWI (Vaska
1993, Guler et al. 2001, Chelemer et al. 2002, Ku et al.
2005).
Despite the well documented information about risk
factors of DSWI post-cardiac surgery, the literature is lacking
studies that investigated risk factors of DSWI post-CABG
surgery in Jordan. Determining patients who are at risk of
developing DSWI after cardiac surgeries is the first step
towards its prevention. Therefore, the purpose of this study
was to assess prevalence of and risk factors for DSWI after
CABG surgery at a university hospital in northern Jordan.
The objectives of the study were (1) to assess prevalence of
DSWI post-CABG surgeries; (2) to assess risk factors and
their association with DSWI; and (3) to determine predictors
of DSWI post-CABG surgery in Jordan.
Methods
Design
A correlational, retrospective design using an existing coro-
nary artery surgery data base was used to assess prevalence of
and risk factors for DSWI after CABG surgery at a university
hospital in northern Jordan.
Sample and setting
All patients who had undergone CABG surgeries between
January 2005–January 2007 were potential participants in
the current study. Patients were included in this study if they:
(1) had undergone CABG surgery, (2) were between
35–75 years old, (3) were mentally competent and (4) had a
complete medical record. Patients were excluded if they had
any concurrent surgery (e.g., valve replacement, congenital
heart surgery, or carotid endarterectomy) and their surgery
did not require intraoperative cardiopulmonary bypass. The
final sample that met the inclusion criteria was comprised
of 206 subjects.
The study was conducted at a university affiliated hospital,
which is a teaching hospital that offers clinical training for
medical, nursing and other health related specialties and is
located within the campus of a public university. It has a 633
beds capacity with medical, surgical, orthopaedic, emer-
gency, psychiatric, intensive care units, coronary care unit,
catheterisation lab and open heart surgery department. Also,
the hospital is a referral hospital that provides specialised
health care for patients referred from military, governmental
and private hospitals in the northern area of Jordan.
Patients undergoing cardiac surgery are usually admitted a
few days before the surgical procedure for completion of
physical and laboratory examination. Patients with CABG
surgeries usually stay two days in the cardiac intensive care
unit (which has a capacity of four beds and 12 registered
nurses working in the unit) and then if they are stable, are
transferred to the intermediate unit (which has a capacity of
24 beds and 18 registered nurses working in the unit).
Patients stay four to five days in the intermediate unit before
they are discharged home. Annually, around 257 CABG
surgeries are performed at the hospital by four surgeons (King
Abdullah University Hospital 2005). Cases that are diag-
nosed with DSWI during occasional period of stay or
re-admitted for the same reason are treated in the interme-
diate care unit until recovery.
Instrument
The Sternal Wound Infection Prediction Scale (SWIPS)
developed by Hussey et al. (1998) was used to assess risk
factors for DSWI after CABG surgery. The SWIPS was
developed to provide a quick and easy way of assessing
individuals who are at risk of developing DSWI (Hussey
et al. 1998). The tool assesses 21 risk factors in the
preoperative, intraoperative and postoperative phases, with
each factor having a weight of 1–9. A score of 27 or greater
indicates that the patient is at risk of developing DSWI.
Initial data collected retrospectively indicated that the SWIPS
is able to accurately predict patients who will develop a
sternal wound infection with 72% accuracy (Hussey et al.
1998). Troutman et al. (2001) reported sufficient validity
and reliability of the SWIPS with a sensitivity of 60Æ7% (the
percentage of patients with infection predicted to have
infection) and specificity of 75Æ9% (the percentage of
patients without infection predicted not to have infection).
For the purpose of this paper, SWIPS was used only to
identify risk factors for DSWI and total scores were not
calculated; all risk factors were dichotomously scored. In this
study, a special case of alpha coefficient (KR20) was
calculated for the competing demands scale because data
were dichotomously scored; it was 0Æ79. Demographic
characteristics of the subjects were collected by an instru-
ment that was developed by the researchers that include age,
gender, marital status, weight, height and body mass index,
date of operation, length of stay in ICU preoperative and
type of organisms isolated.
Data collection
The study survey and protocol were reviewed and approved
by the Institutional Review Boards at a governmental
university and at a university hospital. Sample selection was
Clinical issues Deep sternal wound infections
� 2010 Blackwell Publishing Ltd, Journal of Clinical Nursing, 19, 1873–1881 1875
derived from the coronary artery surgery data base at the
Medical Records Department (MRD). The researchers col-
lected the data by reviewing all medical records of eligible
patients to complete the Sternal Wound Infection Prediction
Scale (SWIPS). The patient information was entered and
confidentially maintained within the MRD.
A DSWI was defined according to the guidelines of the
CDC ‘as an infection of the anterior mediastinal space
involving muscle, bone and/or mediastinum’ (Garner et al.
1988, p. 129). Diagnosis of DSWI required at least one of the
following criteria: (1) an organism isolated from culture of
mediastinal tissue or fluid; (2) evidence of mediastinitis seen
during surgery; and (3) presence of chest pain, sternal
instability, or fever (>38 �C) and purulent discharge from
the mediastinum area (during 30- days postoperation time)
(King et al. 2002).
Potential risk factors for DSWI were classified into three
groups according to stages (preoperative, intraoperative and
postoperative). Preoperative potential risk factors included
demographic factors (age, gender and smoking), medical
history factors (diabetes, hypertension and COPD) and
physical parameters (ejection fraction, impaired immunity
response (abnormal white blood cells count), emergency
cardiac surgery and obesity body mass index [(BMI) ‡ 30]
(Table 1). Intraoperative potential risk factors included
duration of surgery, use of an intraaortic balloon pump
(IABP), use of an IMA and total cardiopulmonary bypass
time (Table 2). Postoperative potential risk factors included
blood transfusion, inotropic support (dopamine-dobutamine
and other medication such as epinephrine, nor-epinephrine,
amiodarone and neo-synephrine), mechanical ventilation
(number of hours postoperative), cardiopulmonary resusci-
tation (CPR), length of stay in ICU after cardiac surgery and
re-exploration for bleeding (Table 3).
Data analysis
The creation of data analysis files were completed and
managed by the researchers. The data were entered into SPSSSPSS
(Version 12) computer software. Data were organised by
subject’s identification number and no identifiers were used.
All data were analysed at alpha level of 0Æ05.
To meet objective number one, descriptive statistics were
used to describe study variables. Categorical data were
recorded and were reported as frequencies and percentages.
Continuous variables were analysed reporting means and
standard deviation. To meet objective number two, risk
factors for DSWI were assessed using t-test analysis used for
continuous variables and the chi-square test for categorical
variables. In addition, we conducted Fisher’s exact test
whenever the chi-square expected value of at least one cell
was less than five (Tables 1 and 3).
To develop a model to predict risks for DSWI that meet
objective number three, the association among the indepen-
dent variables and the dichotomous dependent variable
(DSWI) was tested using stepwise multiple logistic regres-
sion analysis with a generalised logit link function. The odds
ratio from the model indicated the association of interest.
As there were 21 potential risk factors (see Tables 1–3), to
avoid multicollinearity among the explanatory variables, we
performed collinearity diagnostic by assessing the value of
variance-inflation factor (VIF); variables that has VIF
greater than 10 were excluded from the model analysis
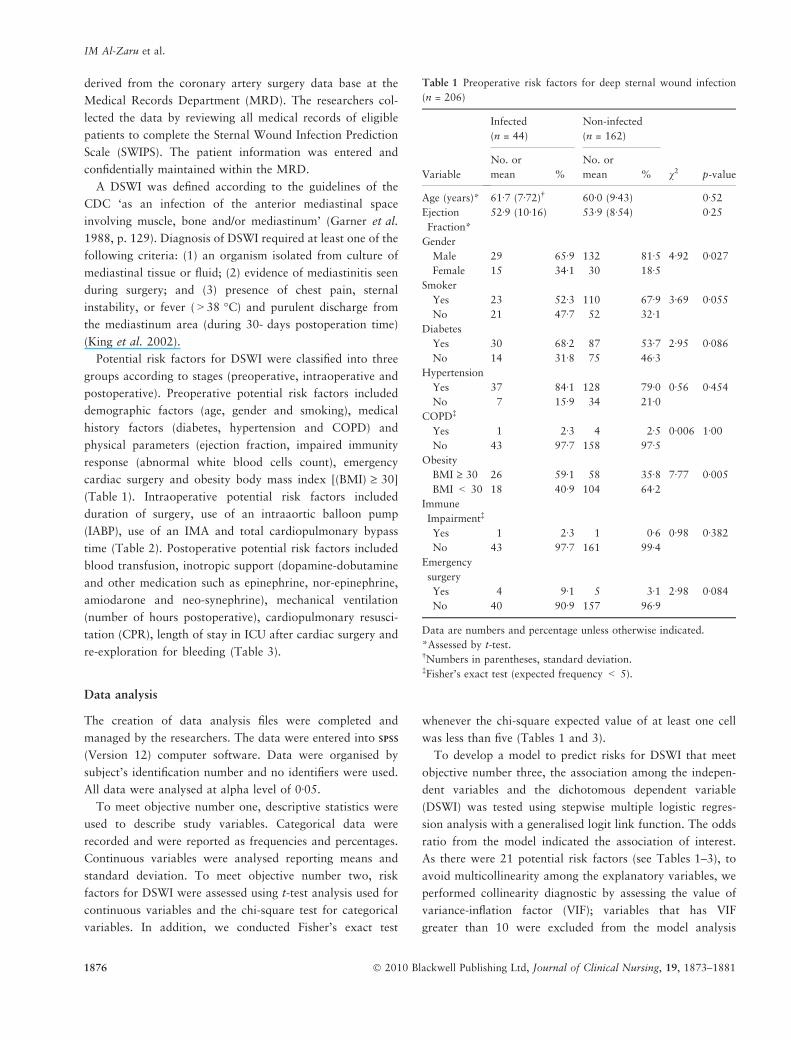
Table 1 Preoperative risk factors for deep sternal wound infection
(n = 206)
Variable
Infected
(n = 44)
Non-infected
(n = 162)
v2 p-value
No. or
mean %
No. or
mean %
Age (years)* 61Æ7 (7Æ72)� 60Æ0 (9Æ43) 0Æ52
Ejection
Fraction*
52Æ9 (10Æ16) 53Æ9 (8Æ54) 0Æ25
Gender
Male 29 65Æ9 132 81Æ5 4Æ92 0Æ027
Female 15 34Æ1 30 18Æ5Smoker
Yes 23 52Æ3 110 67Æ9 3Æ69 0Æ055
No 21 47Æ7 52 32Æ1Diabetes
Yes 30 68Æ2 87 53Æ7 2Æ95 0Æ086
No 14 31Æ8 75 46Æ3Hypertension
Yes 37 84Æ1 128 79Æ0 0Æ56 0Æ454
No 7 15Æ9 34 21Æ0COPD�
Yes 1 2Æ3 4 2Æ5 0Æ006 1Æ00
No 43 97Æ7 158 97Æ5Obesity
BMI ‡ 30 26 59Æ1 58 35Æ8 7Æ77 0Æ005
BMI < 30 18 40Æ9 104 64Æ2Immune
Impairment�
Yes 1 2Æ3 1 0Æ6 0Æ98 0Æ382
No 43 97Æ7 161 99Æ4Emergency
surgery
Yes 4 9Æ1 5 3Æ1 2Æ98 0Æ084
No 40 90Æ9 157 96Æ9
Data are numbers and percentage unless otherwise indicated.
*Assessed by t-test.�Numbers in parentheses, standard deviation.�Fisher’s exact test (expected frequency < 5).
IM Al-Zaru et al.
1876 � 2010 Blackwell Publishing Ltd, Journal of Clinical Nursing, 19, 1873–1881

(Schroeder 1990). All variables were included in the
analysis.
Results
Objective one
Two hundred and six patients with CABG surgeries met the
inclusion criteria and composed the study sample. Of the 206
patients, 161 (78Æ2%) were males and 45 (21Æ8%) were
females. Patients’ ages ranged from 35–75 years with a mean
age of 60Æ3 years (SD 9Æ1). Data revealed that all the subjects
were married, none of them had stayed pre-operatively in the
ICU and only two subjects (1%) had impaired immune
response (See Table 2–4). Approximately 21Æ6% (n = 44)
from total sample developed DSWI, and coagulase-negative
staphylococcus (COAG) bacteria occupied the majority of
infected participants (54Æ5%).
Objective two
Preoperative risk factors
Chi-square analysis indicated that the percentage of males
who had DSWI was significantly higher than the percentage
of females who had DSWI (66Æ9 vs. 34Æ1, v2 = 4Æ92, df = 1,
p = 0Æ027). Also, there was a significant difference in obesity
between DSWI patients and non-infected subjects (v2 = 7Æ77,
df = 1, p = 0Æ005). The percentages of subjects with BMI
‡ 30 were 59Æ1 for DSWI and 35Æ8 for non-infected. How-
ever, there were no significant differences in age, ejection
fraction, smoking, diabetes, hypertension, COPD, immune
response and emergency surgery between DSWI patients and
non-infected subjects (Table 1).
Table 2 Intraoperative risk factors for deep sternal wound infection
(n = 206)
Variable
Infected
(n = 44)
Non-
infected
(n = 162)
v2 p-valueNo. % No. %
Duration of surgery
£4 hours 35 79Æ5 147 90Æ7 4Æ21 0Æ04
>4 hours 9 20Æ5 15 9Æ3IABP*
Yes 17 38Æ6 3 1Æ9 53Æ41 0Æ000
No 27 61Æ4 159 98Æ1CPB time
£2 hours 8 18Æ2 44 27Æ2 1Æ47 0Æ223
>2 hours 36 81Æ8 118 72Æ8IMA
Yes 36 81Æ8 140 86Æ4 0Æ58 0Æ443
No 8 18Æ2 22 13Æ6
IABP, intraaortic balloon pump; CPB, cardiopulmonary bypass;
IMA, internal mammary arteries.*Fisher’s exact test (expected frequency < 5).
Table 3 Postoperative risk factors for deep sternal wound infection
(n = 206)
Variable
Infected
(n = 44)
Non-infected
(n = 162)
v2 p-value
No. or
mean
% No. or
mean
%
Mechanical
ventilation*
13Æ2(9Æ62)�
11Æ8(8Æ23)
0Æ56
Blood transfusion�
Yes 44 100 147 90Æ7 4Æ39 0Æ044
No 0 0 15 9Æ3Dopamine-dobutamine
Yes 32 72Æ7 47 29Æ0 27Æ96 0Æ001
No 12 27Æ3 115 71Æ0Other medication
Yes 15 34Æ1 18 11Æ1 13Æ58 0Æ001
No 29 65Æ9 144 88Æ9CPR�
Yes 3 6Æ8 0Æ0 0Æ0 11Æ21 0Æ009
No 41 93Æ2 162 100
Stay in ICU
£3 days 20 45Æ5 125 77Æ2 16Æ68 0Æ001
>3 days 24 54Æ5 37 22Æ8Re-exploration
Yes 16 36Æ4 18 8Æ0 22Æ97 0Æ001
No 28 63Æ6 149 92Æ0
Data are numbers and percentage unless otherwise indicated.
Other medication, epinephrine, nor-epinephrine, amiodarone, &
neo-synephrine; CPR, cardiopulmonary resuscitation; ICU, intensive
care unit.
*Assessed by t-test.�Numbers in parentheses, standard deviation.�Fisher’s exact test (expected frequency < 5).
Table 4 Final fitted logistic regression model for risk factors for deep
sternal wound infection (n = 206)
Variable Beta estimate p-value OR 95% CI
Intercept 25Æ11 0Æ000
Diabetes �1Æ149 0Æ048 0Æ317 0Æ099–0Æ933
Obesity
(BMI ‡ 30)
�1Æ252 0Æ011 0Æ275 0Æ102–0Æ742
Duration of
surgery
(>4 hours)
1Æ440 0Æ032 4Æ220 1Æ136–15Æ677
IABP �3Æ404 0Æ000 0Æ033 0Æ005–0Æ204
All 21 variables were entered in the model.
OR, odds ratio; CI, confidence interval; IABP, intraaortic balloon
pump.
Clinical issues Deep sternal wound infections
� 2010 Blackwell Publishing Ltd, Journal of Clinical Nursing, 19, 1873–1881 1877

Intraoperative risk factors
Chi-square analysis indicated that the duration of surgery
(v2 = 4Æ21, df = 1, p = 0Æ04) and use of IABP (v2 = 53Æ41,
df = 1, p < 0Æ001) showed significant associations with
infection incidences. DSWI patients were more likely than
non-infected patients to have longer duration of surgery
and more use of IABP (See Table 2). The percentage of
patients with DSWI who experienced a duration of surgery
more than four hours was higher than the percentage of
non-infected patients who experienced a duration of sur-
gery more than four hours (20Æ5 vs. 9Æ3). The percentage
of patients with DSWI who had used IABP was higher
than the percentage of non-infected patients who had used
IABP (38Æ6 vs. 1Æ9). However, there were no significant
differences in use of an IMA and cardiopulmonary bypass
time.
Postoperative risk factors
Chi-square analysis indicated that blood transfusion
(v2 =4Æ39, df = 1, p = 0Æ044), dopamine-dobutamine use
(v2 = 27Æ96, df = 1, p = 0Æ001), other medication use (v2 =
13Æ58, df = 1, p < 0Æ001), CPR (v2 = 11Æ21, df = 1,
p = 0Æ009), stay in ICU (v2 = 16Æ68, df = 1, p = 0Æ001) and
re-exploration (v2 = 22Æ97, df = 1, p = 0Æ001) showed sig-
nificant differences among DSWI patients and non-infected
patients (See Table 3). However, there was no significant
difference in mechanical ventilation mean time between
DSWI patient and non-infected patients.
Objective three
Generalised logit model
Statistics suggested that the model fit the data well
(Chi-square = 87Æ57, p < 0Æ001; Goodness of fit = 5Æ738,
p = 0Æ677). A probability (p) value >0Æ05 for Hosmer and
Lemeshow goodness of fit and the deviance residual
measures indicate that the model fits the data well. The
final model derived from the entire sample (N = 206) was
composed of the following variables: (1) diabetes (OR = 0
Æ317, p = 0Æ048), (2) Obesity (OR = 0Æ275, p = 0Æ011), (3)
duration of surgery (OR = 4Æ22, p = 0Æ032) and (4) use of
IABP (OR = 0Æ033, p < 0Æ001) (Table 4). Diabetic patients
had 31% higher risk of DSWI than non-diabetic patient;
patients with BMI ‡ 30 had 27 per cent higher risk of
DSWI than patients with BMI £ 30; compared with
patients with duration of surgery £4 hours, patients who
had duration of surgery >4 hours had 4Æ2 times the
risk of DSWI; and patients who used IABP post-surgery
had 3 per cent higher risk of DSWI than patients who did
not.
Discussion
The aim of this study was to assess prevalence of and risk
factors for DSWI after CABG surgery at a public university
hospital, northern Jordan. Identifying risk factors for devel-
oping DSWI is important and amenable to early presurgical
intervention by nurses and other health team professionals.
The final model identified diabetes, obesity, duration of
surgery and use of IABP as predictors of DSWI after CABG
surgery.
Twenty-two per cent of the sampled patients reported
significantly high prevalence of DSWI post-CABG surgery.
This result was higher than the globally reported incidence
rate (1–3%) (Borger et al. 1998, Baskett et al. 1999, Olsen
et al. 2002).
Data revealed that COAG accounted for up to 54Æ5% of
DSWI which is congruent with what the literature reported
(Antunes et al. 1997, Catarina et al. 2000). COAG were a
normal flora occupying the patient’s own skin and the
surgical team’s nose, arms and foreheads (Catarina et al.
2000). Skin preparation (clipping instead of shaving) and
applying strict universal precaution such as wearing gloves,
head cap, face mask and gown is necessary to prevent
microbes’ spread. Also, adherence to aseptic technique and
using separate instruments for each surgical site is a must
(Catarina et al. 2000).
Chi-square analysis indicated that CABG patients with
DSWI were males, obese, had long surgery duration, used
IABP and had postoperative courses complicated by CPR,
bleeding requiring re-exploration and blood transfusion and
poor haemodynamics requiring inotropic medication sup-
port that resulted in an increased length of stay in ICU
postoperatively. All these factors placed CABG patient at
risk of having DSWI. These results are consistent with the
findings of previous studies (Borger et al. 1998, Khan et al.
2000).
The final model was constructed from 21 risk factors using
stepwise multiple logistic regression analysis with a general-
ised logit link function for the dichotomous dependent
variable. Four variables emerged as risk factors for DSWI,
two preoperative parameters related to patient history or
physical characteristics (diabetes and obesity), one intraop-
erative parameter related to duration of surgery and one
postoperative parameter related to use of IABP were risk
factors for DSWI. The results of this study support findings
from previous reports that diabetes (Toumpoulis et al. 2005,
Swenne 2006), obesity (BMI ‡ 30) (Borger et al. 1998,
McConkey et al. 1999, Cayci et al. 2008), long surgery
duration (Kirkland et al. 1999) and the use of IABP (Borger
et al. 1998) are predictors of DSWI.
IM Al-Zaru et al.
1878 � 2010 Blackwell Publishing Ltd, Journal of Clinical Nursing, 19, 1873–1881

Previous studies explained that the effects of diabetes on
the vasculature may predispose individuals to infection and
may impede the ability to treat the infection because of poor
blood supply to the infected area and the inability of
antibiotics to reach the site, in addition to impairment of
the white blood cells’ ability to phagocytose and effectively
kill bacteria (Zerr et al. 1997). Furnary et al. (1999) sug-
gested that a continuous intravenous insulin infusion pre and
postoperatively reduced the incidence of DSWI.
Patients with obesity have more adipose tissue in the chest
area that is poorly perfused, which limits oxygen delivery.
Furthermore, the extra weight caused by adipose tissue puts
additional strain on the incision, which may further reduce
blood supply (Vaska 1993). Obese individuals are also at risk
for sternal wound dehiscence and sternal wire breakage
(Shaffer & Corish 1998). Planned cardiac surgery prepara-
tion must take into consideration controlling patients’ weight
with strategies that are suitable for the health status of the
patient and availability of time.
Duration of surgery was found to be a risk factor for
DSWI. The longer the duration of surgery the more environ-
mental exposure and therefore a higher infection rate was
expected. Factors related to duration of surgery included
patient disease severity, urgency of surgery, surgical proce-
dure, surgical team and operating room The study findings
suggest that the operating room environment (e.g., temper-
ature, humidity and airflow), urgency of surgery, surgical
procedure and surgical team should be examined for other
risk factors for DSWI.
Use of IABP was found to be a risk factor for DSWI. The
IABP is a circulatory support device. Patients who need an
IABP are those suspected of having severe left ventricular
dysfunction or congestive heart failure. While one can
reasonably assume that the most severely ill patient – who
required IABP- also experienced prolong surgery duration,
prolonged mechanical ventilation, complicated postoperative
course haemodynamically, use of inotropic support and
prolonged stay in ICU, it is unclear which factors are
contributing to the relation between use of IABP and
development of DSWI. The study findings suggested that
patient clinical status should be examined further in associ-
ation with DSWI.
Limitations of the study
The results of our study should be interpreted by taking
into account some limitations. The retrospective nature of
this study precluded the ability to infer causal relationships
between the statistically significant risk factors and DSWI.
Therefore, future testing of the proposed model with
prospective longitudinal data will increase understanding
of the most effective predictive model to prevent DSWI
after CABG surgery in Jordan. Small sample size and
convenience sampling and may not be truly representative
of Jordanian CABG patients, thus limiting the generalis-
ability of findings. Important factors that may contribute to
infection include those related to environment, operating
room, surgical and health team and postoperative care
were not included in this study. Further studies might focus
on the relationship between these factors and development
of DSWI.
Conclusion
Assessing presurgical risk factors for DSWI in patients who
will undergo CABG may be important for early intervention
and care-related decisions by nurses as well as other health
care providers, patients and family members. We studied
infection prevalence and risk factors for DSWI post-CABG
at a governmental university hospital in northern Jordan.
High prevalence of DSWI was reported from the sampled
patients. The final model indicated that diabetes, obesity,
duration of surgery and use of IABP were risk factors for
DSWI. Controlling these factors may help in controlling
DSWI after CABG surgery. This explanatory model requires
further development and validation prior to implementation.
Relevance to clinical practice
DSWI is one of the major complications after CABG surgery
DSWI, resulting in multiple operative and non-operative
procedures and increased hospital costs. Identifying risk
factors for developing DSWI is important and amenable to
early presurgical intervention by nurses and other health team
professionals.
Contributions
Study design: IA, AA, MA; data collection and analysis: IA,
AA, MA and manuscript preparation: AA, IA, MA, A Am.
Conflict of interest
The authors declare that they have no conflict of interests.
References
Antunes PE, Bernardo JE, Egue¢ nio L, De Olivera JF & Antunes MJ
(1997) Mediastinitis after aorto-coronary bypass surgery. Euro-
pean Journal of Cardiothoracic Surgery 12, 443–449.
Clinical issues Deep sternal wound infections
� 2010 Blackwell Publishing Ltd, Journal of Clinical Nursing, 19, 1873–1881 1879

Baskett RJ, Macdougall CE & Ross DB (1999) Is mediastinits a
preventable complication? A 10 years review. Annals of Thoracic
Surgery 67, 462–465.
Birkmeyer N, Charlesworth DC, Hernandez F, Leavitt BJ, Marrin
CA, Morton JR, Olmstead EM & O’Connor GT (1998) Obesity
and risk of adverse outcome associated with coronary artery by-
pass surgery. Circulation 97, 1689–1694.
Borger MA, Rao V, Weisel RD, Ivanovs J, Cohen G, Scully HE &
David TE (1998) Deep Sternal wound infection: risk factors and
outcomes. Annals of Thoracic Surgery 65, 1050–1056.
Carrier M, Gregoire J, Tronc F, Cartier R, Leclerc Y & Pelletier LC
(1992) Effect of internal mammary artery dissection on sternal
vascularization. Annals of Thoracic Surgery 53, 115–119.
Catarina YB, Eva M & Ulrika R (2000) Spread of Coagulase-
Negative Staphylococci during cardiac operations in a modern
operating room. Annals of Thoracic Surgery 69, 1110–1115.
Cayci C, Russo M, Cheema F, Martens T, Ozcan V, Argenziano M,
Oz MC & Ascherman J (2008) Risk analysis of deep sternal wound
infections and their impact on long-term survival: a propensity
analysis. Annals of Plastic Surgery 61, 294–301.
CDC (2006) Assessing risk factors for chronic disease – Jordan.
Morbidity and Mortality Weekly Report 55, 653–655.
Chelemer SB, Prato BS, Cox PM, O’Connor GT & Morton JR (2002)
Association of bacterial infection and red blood cell transfusion
after coronary artery bypass surgery. Annals of Thoracic Surgery
73, 138–142.
De Feo M, Renzulli A, Ismeno G, Gregorio R, Della Corte A, Utili R
& Cotrufo M (2001) Variables predicting adverse outcome in
patients with deep sternal wound infection. Annals of Thoracic
Surgery 71, 324–331.
De Paulis R, De Notaris S, Scaffa R, Nardella S, Zeitani J,
Del Giudice C, De Peppo AP, Tomai F & Chiariello L (2005)
The effect of bilateral internal thoracic artery harvesting on
superficial and deep sternal wound infection. Journal of Thoracic
and Cardiovascular Surgery 129, 536–543.
Furnary AP, Zerr KJ, Grunkemeier GL & Starr A (1999) Continuous
intravenous insulin infusion reduces the incidence of deep sternal
wound infection in diabetic patients after cardiac procedures.
Annals of Thoracic Surgery 67, 352–362.
Garner JS, Jarvis WR & Emori TG (1988) Center for disease control
and prevention: definitions for nosocomial infections. American
Journal of Infection Control 16, 128–140.
Guler M, Kirali K & Toker ME (2001) Different CABG methods in
patients with chronic obstructive pulmonary disease. Annals of
Thoracic Surgery 71, 152–157.
Hollenbeak CS, Murphy DM & Koening S (2000) The clinical
and economic impact of deep chest surgical site infection following
coronary artery bypass graft surgery. Chest 118, 397–402.
Hussey LC, Leeper B & Hynan LS (1998) Development of the sternal
wound infection prediction scale. Heart and Lung 27, 326–336.
Jaffe RA & Sammuels SI (1999) Anesthesiologist’s Manual of
Surgical Procedures, 2nd edn. Philadelphia, Lippincott Williams &
Wilkins.
Jordan Ministry of Health (2005) Health Indicators. Available at:
http://www.moh.gov.jo/head-page.htm (accessed February 2005).
Khan J, Magnetti S, Davis E & Zhang J (2000) Late outcomes of
open heart surgery in patients 70 years and older. Annals of
Thoracic Surgery 69, 165–170.
King Abdullah University Hospital (2005) King Abdullah University
Hospital Statistical Report 2005. Irbid, Jordan.
King RB, Rozanski A, Blumenthal JA & Kaplan J (2002) Impact
of psychological factors on the pathogenesis of cardiovascu-
lar disease and implications for therapy. Circulation 99, 2192–
2217.
Kirkland KB, Briggs JP, Trivette SL, Wilkinson WE & Sexton DJ
(1999) The impact of surgical-site infections in the 1990s:
attributable mortality, excess length of hospitalization and extra
costs. Infection Control and Hospital Epidemiology 20, 725–
730.
Ku C, Ku S, Yin J & Lee A (2005) Risk Factors for sternal and leg
surgical site infections after cardiac surgery in Taiwan. American
Journal of Epidemiology 161, 661–671.
McConkey SJ, L¢Ecuyer PB, Murphy DM, Leet TL, Sundt TM &
Fraser VJ (1999) Results of a comprehensive infection control
program for reducing surgical-site infections in coronary artery
bypass surgery. Infection control and hospital epidemiology 20,
533–538.
Milano CA, Kesler K, Archibald N, Sexton DJ & Jones RH (1995)
Mediastinitis after coronary artery bypass surgery: risk factors and
long-term survival. Circulation 92, 2245–2251.
Olsen MA, Lock-Buckley P, Hopkins D, Polish LB, Sundt TM &
Fraser VJ (2002) The risk factors for deep and superficial chest
surgical-site infections after coronary artery bypass graft surgery
are different. Journal of Thoracic and Cardiovascular Surgery 124,
136–145.
Orenstein A, Kachel F, Zuloff-Shani A, Paz Y, Sarig O, Haik J,
Smolinsky AK, Mohr R, Shinar E & Danon D (2005) Treatment of
deep sternal wound infections post-open heart surgery by appli-
cation of activated macrophage suspension. Wound Repair and
Regeneration 13, 237–242.
Orhan G, Bicer Y, Aka SA, Sargin M, Simsek S, Senay S, Aykac Z
& Eren EE (2004) Coronary artery bypass graft operations
safely in obese patients. European Journal of Cardio-thoracic
Surgery 25, 212–217.
Schroeder MA (1990) Diagnosing and dealing with multicollinearity.
Western Journal of Nursing Research 12, 175–187.
Sethi GK, Copeland JG, Moritz T, Henderson W, Zadina K &
Goldman S (1991) Comparison of postoperative complications
between saphenous vein and IMA grafts to left anterior descending
coronary arteries. Annals Thoracic Surgery 51, 733–738.
Shaffer RB & Corish C (1998) Cardiac surgery and women. Journal
of Cardiovascular Nursing 12, 14–31.
Sofer D, Gurevitch J, Shapira I, Paz Y, Matsa M, Kramer A & Mohr
R (1999) Sternal wound infections in patients after coronary artery
bypass grafting using bilateral skeletonized internal mammary
arteries. Annals of Surgery 229, 585–590.
SPSS Base (2002) Version 12 for Windows User’s Guide. SPSS,
Chicago.
Swenne CL (2006). Wound infection following coronary artery by-
pass graft surgery: risk factors and the experiences of patients.
Unpublished doctoral dissertation. Acta Universitatis Upsaliensis
Uppsala.
Thomas TA, Taylor SM, Crane MM, Cornett WR, Langan EM,
Snyder BA & Cull DL (1999) An analysis of limb-threatening
lower extremity wound complications after 1090 consecutive
coronary artery bypass procedures. Vascular Medicine 4, 83–88.
IM Al-Zaru et al.
1880 � 2010 Blackwell Publishing Ltd, Journal of Clinical Nursing, 19, 1873–1881

Toumpoulis IK, Anagnostopoulos CE, DeRose J & Swistel DJ (2005)
The impact of deep sternal wound infection on long-term survival
after coronary artery bypass grafting. Chest 127, 464–471.
Troutman S, Hussey LC, Hynan L & Lucisano K (2001) Sternal
wound infection prediction scale: a test of the reliability and
validity. Nursing and Health Sciences 3, 1–8.
Vaska PL (1993) Sternal wound infections. AACN Clinical Issues in
Critical Care Nursing 4, 475–483.
Vuorisalo S, Haukipuro K, Pokela R & Syrjala H (1998) Risk fea-
tures for surgical-site infections in coronary artery bypass surgery.
Infection Control and Hospital Epidemiology 19, 240–247.
WHO (2006) Cardiovascular Disease: Prevention and Control.
Available at: http://www.who.int/dietphysicalactivity/publications/
facts/cvd/en/ (accessed February 2006).
Zacharias A & Habib RH (1996) Factors predisposing to median
sternotomy complications: deep vs. superficial infection. Chest
110, 1173–1178.
Zerr KJ, Furnary AP, Grunkemeier GL, Bookin S, Kanhere V & Starr
A (1997) Glucose control lowers the risk of wound infection in
diabetics after open heart surgery. Annals of Thoracic Surgery
63, 356–361.
Clinical issues Deep sternal wound infections
� 2010 Blackwell Publishing Ltd, Journal of Clinical Nursing, 19, 1873–1881 1881

This document is a scanned copy of a printed document. No warranty is given about the accuracy of the copy.
Users should refer to the original published version of the material.
Copyright © 2022 FDOKUMEN