
Deep dermal burn injury results in scarless wound healing in the ovine fetus
9
Deep dermal burn injury results in scarless wound healing in the ovine fetus JOHN F. FRASER, MBChB a ; LEILA CUTTLE, BSc a ; MARGIT KEMPF, BmedLSci a ; GAEL E. PHILLIPS, MBBS b ; PETER K. O’ROURKE, PhD c ; KELVIN CHOO, MBBS a ; MARK T. HAYES, PhD a ; ROY M. KIMBLE, MBChB a Early to mid-term fetuses heal cutaneous incisional wounds without scars; however, fetal response to burn injury has not been ascertained. We present a fetal model of thermal injury and subsequent analysis of fetal and lamb response to burn injury. A reproducible deep dermal burn injury was created in the fetus by application of water at 66 ˚C for 7seconds, and at 82 ˚C for 10 seconds to the lamb. Macroscopically, the area of fetal scald was undetectable from day 7 post injury, while all lamb scalds were readily identified and eventually healed with scarring. Using a five-point histopathology scoring system for alteration in tissue morphology, differences were detected between control and scalded skin at all stages in lamb postburn, but no difference was detected in the fetal model after day 7. There were also large differences in content of a-smooth muscle actin and transforming growth factor-b1 between control and scalded lamb and these differences were statistically significant at day 14 (P < 0.01). This novel model of fetal and lamb response to deep dermal injury indicates that the fetus heals a deep burn injury in a scarless fashion. Further elucidation of this specific fetal process of burn injury repair may lead to improved outcome for patients with burn injury. (WOUND REP REG 2005;13:189–197) Burn injury is well recognized as a major cause of mortality in the relatively fit and young population. There have been major advances in the treatment of patients with severe burn injury, such that the mortality associated with burns has dropped dramatically. In 1948, a child who sustained a 50% body surface area (BSA) burn would have a 50% risk of death (LD50). 1 By 1997, the same child would require a 98% BSA burn for the same mortality rate. 2 However, the improvements seen in the mortality figures are not reflected in the morbidity associated with postburn scarring. The constitutive growth rate of the child is more rapid than the formation of postburn scar tissue, resulting in contractures, particularly around joints. The effects of scar tissue in the child can be seen as a systemic disease affecting psychosocial development, osteo- penia, body temperature regulation (due to reduced efficiency of perspiration), and repeated operation for contracture release, as well as the discomfort asso- ciated with continued physiotherapy and occupational therapy. The cost to the community is significant, with >60% of the cost of treatment of a child’s burns being incurred after closure of the wound. 3 Treatment of burn scarring is limited to prolonged wearing of pressure garments, steroid injections which may be BoSA Bovine serum albumin BSA Body surface area DDBI Deep dermal burn injury H&E Hematoxylin and eosin aSMA a-smooth muscle actin TBS Tris-buffered saline solution TGF Transforming growth factor From the Royal Children’s Hospital Burns Research Group a , Royal Children’s Hospital, University of Queensland; Department of Paediatrics and Child Health b , Queensland Health Pathology Services, Royal Brisbane Hospital; and School of Population Health c , University of Queensland, Herston, Brisbane, Queensland, Australia. Manuscript received: June 8, 2004 Accepted in final form: September 24, 2004 Reprint requests: John F. Fraser, MBChB, Department of Paediatrics and Child Health, Royal Children’s Hospital, Herston Rd., Herston, Queensland, Australia, 4029. Fax: þ617 3365 5455; Email: [email protected]. Copyright # 2005 by the Wound Healing Society. ISSN: 1067-1927. 189
Transcript of Deep dermal burn injury results in scarless wound healing in the ovine fetus

Deep dermal burn injury results in scarless wound healingin the ovine fetus
JOHN F. FRASER, MBChBa; LEILA CUTTLE, BSca; MARGIT KEMPF, BmedLScia; GAEL E. PHILLIPS, MBBSb; PETERK. O’ROURKE, PhDc; KELVIN CHOO, MBBSa; MARK T. HAYES, PhDa; ROY M. KIMBLE, MBChBa
Early to mid-term fetuses heal cutaneous incisional wounds without scars; however, fetal response to burn injuryhas not been ascertained. We present a fetal model of thermal injury and subsequent analysis of fetal and lambresponse to burn injury. A reproducible deep dermal burn injury was created in the fetus by application of water at66 ˚C for 7 seconds, and at 82 ˚C for 10 seconds to the lamb. Macroscopically, the area of fetal scald wasundetectable from day 7 post injury, while all lamb scalds were readily identified and eventually healed withscarring. Using a five-point histopathology scoring system for alteration in tissue morphology, differences weredetected between control and scalded skin at all stages in lamb postburn, but no difference was detected in thefetal model after day 7. There were also large differences in content of a-smooth muscle actin and transforminggrowth factor-b1 between control and scalded lamb and these differences were statistically significant at day 14(P < 0.01). This novel model of fetal and lamb response to deep dermal injury indicates that the fetus heals a deepburn injury in a scarless fashion. Further elucidation of this specific fetal process of burn injury repair may lead toimproved outcome for patients with burn injury. (WOUND REP REG 2005;13:189–197)
Burn injury is well recognized as a major cause ofmortality in the relatively fit and young population.There have been major advances in the treatment ofpatients with severe burn injury, such that the mortalityassociated with burns has dropped dramatically. In1948, a child who sustained a 50% body surface area(BSA) burn would have a 50% risk of death (LD50).1 By1997, the same child would require a 98% BSA burn for
the same mortality rate.2 However, the improvementsseen in the mortality figures are not reflected in themorbidity associated with postburn scarring. Theconstitutive growth rate of the child is more rapidthan the formation of postburn scar tissue, resultingin contractures, particularly around joints. The effectsof scar tissue in the child can be seen as a systemicdisease affecting psychosocial development, osteo-penia, body temperature regulation (due to reducedefficiency of perspiration), and repeated operation forcontracture release, as well as the discomfort asso-ciated with continued physiotherapy and occupationaltherapy. The cost to the community is significant, with>60% of the cost of treatment of a child’s burns beingincurred after closure of the wound.3 Treatmentof burn scarring is limited to prolonged wearing ofpressure garments, steroid injections which may be
BoSA Bovine serum albumin
BSA Body surface area
DDBI Deep dermal burn injury
H&E Hematoxylin and eosin
aSMA a-smooth muscle actin
TBS Tris-buffered saline solution
TGF Transforming growth factor
From the Royal Children’s Hospital Burns ResearchGroupa, Royal Children’s Hospital, University ofQueensland; Department of Paediatrics andChild Healthb, Queensland Health PathologyServices, Royal Brisbane Hospital; and Schoolof Population Healthc, University of Queensland,Herston, Brisbane, Queensland, Australia.
Manuscript received: June 8, 2004Accepted in final form: September 24, 2004Reprint requests: John F. Fraser, MBChB, Department of
Paediatrics and Child Health, Royal Children’sHospital, Herston Rd., Herston, Queensland,Australia, 4029. Fax: þ617 3365 5455; Email:[email protected].
Copyright # 2005 by the Wound Healing Society.ISSN: 1067-1927.
189

associated with their own morbidity in the growingchild, and repeated grafting, which is associated withscarring itself. New treatments of scar therapy havebeen as yet inadequate.4
Research into the fetal response to the incisionalwound indicates that the fetus can heal this wound in ascarless fashion if the injury occurs in the early periodof gestation. The incisional wound heals in a well-described pattern with minimal tissue loss, and thus,even in the postnatal mammal, heals rapidly. Thedegree of tissue loss, pathophysiology, and vascularchanges associated with a burn wound, however, setsthe burn wound apart from an incisional wound. Thereis a much larger loss of tissue, and the injury repair isdetermined by both tissue depth and amount of tissuelost. The mechanism is also different. An incisionalwound is created, for example, by a sharp knife, andfollowing the injury the stimulus is ended. In a burnwound, however, the tissue destruction does not ceaseon the removal of the heat source. Cell injury occurs denovo, long after the removal of the heat source. Thecellular responses in burn wound healing also differ mark-edly from incisional wounds. Hence the burn wound isseen as a different entity from the incisional wound.
Epidermal and superficial dermal burn injuries,where the hair follicle and sweat gland are untouched,heal with migration of epithelial cells from the woundedges and from intact epidermal appendages. Wherethese appendages are numerous, this depth of burninjury results in almost no scar tissue formation.5 Adermal injury that breaches the reticular (deep) dermisuniversally causes scar tissue formation.6
The fibroblast is viewed as an engine of fibrosisand scar tissue formation.7 It is the major contributorto the quantity of collagen produced following a ther-mal injury and can change its phenotypic appearance inresponse to tissue injury or stress to include a contract-ile apparatus consisting of actin fibers.8 The resultantcell is the myofibroblast, and it is known to containactin and myosin as well as the expression of a-smoothmuscle actin (aSMA), the most reliable marker of themyofibroblast.9
The nascence and apoptosis of the myofibroblast,as well as the whole process of tissue responseto thermal injury and resulting scar formation aredetermined by a large number of growth factors andcytokines. The transforming growth factor (TGF)superfamily of cytokines has been shown to play animportant role in wound healing and is released bymany cells implicated in this process.10 TGF-b1 isknown to stimulate the transition of fibroblasts intocontractile myofibroblasts and may delay the apoptosisof these cells.11 It also acts, along with a variety offactors produced by the wound bed, to induce epithe-lial cell proliferation and migration.12 Fibroblasts cul-tured from hypertrophic scar produce more TGF-b1
than fibroblasts from normal scars,13 and serum fromrecovering burn patients has twice the level of TGF-b1than that of control patients.14 It is thus a key factor inmodulation of burn wound healing.
Burrington recognized more than 30 years ago that themammalian fetus has the ability to repair full-thicknessincisional wounds in a scarless fashion without inflamma-tion, and with restoration of perfect tissue architecture.15,16
However, excisional wounds and wounds caused by che-mical irritation heal with scarring, leading to the conclusionthat the fetus has the ability to scar, but can regenerateperfect tissue architecture in response to specific injurypatterns.17,18 There has been no study of the fetal responseto thermal injury.
We hypothesized that a mid-gestational fetus wouldheal a deep dermal burn injury in a scarless fashion,and a 1-month-old lamb would heal a similar injurywith scarring. To test our hypotheses, we developedmodels of deep dermal partial thickness injury in the80-day gestation (term¼ 150 days) Merino fetus and the1-month-old Merino lamb. Subsequently, having createdthis model of reproducible injury, we went on toconduct a study of the different healing modalities ofthese wounds.
MATERIALS AND METHODSThe two models were conducted concurrently onMerino sheep supplied by the University of Queenslandwith approval from the University of QueenslandAnimal Ethics Committee.
Fetal modelMerino ewes were super-ovulated with 500 IU Folligon(Intervet International, Boxmeer, The Netherlands) andtime mated. At 80 days fetal gestation, the ewes wereanesthetized using thiopentone (10–15 mg/kg) and intu-bated with a size 10 Portex endotracheal tube. Anesthe-sia was maintained with halothane in 100% oxygen andcontinuous pulse oximetry monitoring was usedthroughout the procedure.
The ewe was placed in the supine position, theanterior abdomen was prepared by shaving, and thearea was swabbed with BetadineTM. Following thecreation of a paramedian skin incision, avoiding thesuperficial central abdominal vein, the uterus wasdelivered onto the operating field. A hysterotomywound was fashioned, and the head and upper trunk ofthe fetus was delivered to the sterile field to conservemaximal quantities of amniotic fluid. Polypropylene tubesof 15 ml volume with a 1.5 cm diameter were filled withsterile water and were heated in a hot water bath. Thetemperature of the water was measured using a digitalthermometer (N19-Q1436; Dick Smith Electronics, Regents
WOUND REPAIR AND REGENERATION190 FRASER ET AL. MARCH–APRIL 2005

Park, NSW, Australia, range �50 ˚C to 100 ˚C [ �0.5%]).Once the tubes had reached the chosen temperature theywere removed in a sterile manner from the water bath andquickly inverted onto the flank of the fetus, care beingtaken to avoid spillage. To identify the margin of the burnarea, the scalded areas were marked by tattooing withsterilized ink (Rotring, Hamburg, Germany) in a 27Gneedle. The fetus was then returned to the uterus, whichwas closed. After the laparotomy wound was sutured, theewe was awakened and returned to the sheep pen.
Lamb modelMerino lambs, conceived with assistance of super-ovulation as previously described, were born in ourresearch center and fed from both mother and standardgrass/grain feed ad libitum. At 28–30 days, the lambswere anesthetized with thiopentone (15 mg/kg) andintubated with a size 6.0 Portex endotracheal tube.Anesthesia was continued with halothane/100% oxygenmixture, and continuous pulse oximetry monitoringwas used throughout the procedure. The lamb wasshaved on a standard area of the lower abdomen, initi-ally with sheep clippers then with a razor, lukewarmwater, and shaving cream, until the skin was freeof wool. The wound area was then gently washedwith lukewarm water to remove any soap residue. Hotwater for scalding was prepared as previouslydescribed and applied in the same manner. Followingthe creation of scalds and tattooing of the wound mar-gin with ink, the wounds were covered with paraffingauze and MeloninTM soft cotton dressing (Smith andNephew, Mt. Waverley, Australia), to reduce directtrauma and soiling to of the burned area. The lambwas then awakened and returned to a pen.
Determination of correct burn parametersTo establish the optimal temperature and duration ofthermal injury, a total of three fetuses and six lambswere used with multiple scalds at varying temperatureson all animals. Scalds were created using the aforemen-tioned method. In the fetal model, an initial tempera-ture of 60 ˚C for 5 seconds, increasing in 2-secondincrements, was the starting point, as this temperatureis relevant in thermal injury in children.19 The tempera-ture was also increased in 2 ˚C increments up to amaximum of 72 ˚C. At 2 days post operation, the eweswere euthanized using pentobarbital sodium 200 mg/ml(20%), and the duplicate samples of the different tem-perature scalds were cut out within the wound borderand fixed in 10% buffered formalin. Tissues were thenblocked in paraffin and 4-mm sections were taken andstained with hematoxylin and eosin (H&E). These sec-tions were analyzed for depth of injury by a specialistfetal histopathologist, who was blinded to the tempera-tures used to create the injuries. A deep dermal burn
injury (DDBI) was defined as an injury causing celldeath into the reticular dermis, with subtotal necrosisof the hair follicle bulb.20 As the depth of the hairfollicle bulb varies in sheep, multiple fields of viewfrom the duplicate samples were assessed. A tempera-ture of 66 ˚C for 7 seconds was found to give a consist-ent depth of injury in the fetus, with damage to, but notcomplete necrosis of, the hair follicle bulb. Using thesame process, a temperature of 82 ˚C for 10 secondsconsistently created a deep dermal injury in the lambmodel.
Experimental protocol and analysisFollowing the development of these models, a total of15 fetuses and 15 lambs were scalded in the abovemanner, using water at 66 ˚C for 7 seconds and 82 ˚Cfor 10 seconds for the fetus and lamb, respectively. Theanimals were euthanized in a serial manner: threerandomly selected animals each on days 1, 7, 14, 21and 60. Discs of injured skin and control unburnt skin(contralateral flank) were obtained from each animal toallow for direct comparison, initially using light micro-scopy. Wounds were examined, photographed, andtissue was retrieved and stored for later analysis byimmunohistochemistry, proteomic analysis, RNAanalysis and electron microscopy. Macroscopically,there were no burn wound infections in the lambgroup, nor any sign of significant trauma.
Histopathological analysis of tissue repairTissue sections were fixed in 10% buffered formalinand blocked in paraffin. Sections of 4 mm thicknesswere stained with H&E. These sections were thenexamined in a blinded manner by the same histopathol-ogist who assisted in the creation of the model.Between three and four sections on each slide wereexamined. To determine whether the tissue was burnedor control, a scoring system was developed to enable amore objective assessment. A total of five markers ofinjury were observed: number of fibroblasts, alterationof interstitial tissue, epidermal thickness, number ofhair follicles, and alteration in papillary and reticulardermis. These markers were graded from 0 to 3, with0¼ normal and 3¼ severe abnormality For example:0¼ normal number of hair follicles and 3¼ veryfew hair follicles remaining; 0¼ normal number offibroblasts and 3¼much greater number of fibroblasts,etc. For each tissue section these scores were thenadded together to get a total score for each sample.To validate this novel scoring system, the same histo-pathologist scored the slides on two separate occa-sions, between 1 and 3 months apart. She was blindedto her previous scoring of the same slides. Onceall slides were assessed and scored on the second
WOUND REPAIR AND REGENERATIONVOL. 13, NO. 2 FRASER ET AL. 191

occasion, the scores in each category were comparedagainst those from the first assessment and a kappastatistic was determined to provide a measure ofconcordance between these scores. A kappa valuegreater than 0.4 is considered to show good concor-dance.21
Immunohistochemical analysis of scarringFour-micron paraffin sections of burn and control skinwere immunohistochemically analyzed for aSMA andTGF-b1. Slides were dewaxed, hydrated, and washedwith Tris-buffered saline solution (TBS). The TGF-b1slides then underwent an antigen retrieval step of 0.1%trypsin in phosphate buffered saline solution at 37 ˚Cfor 15 minutes. All slides had an endogenous peroxideremoval step (0.6% H2O2 in TBS, 10 minutes) followedby blocking in 4% powdered milk in TBS (aSMA) and/or1 : 10 goat normal serum in 1% bovine serum albumin(BoSA) in TBS (aSMA and TGF-b1) for 20 minutes. Theprimary antibodies used were: monoclonal mouse anti-aSMA (#A2547; Sigma Aldrich, St. Louis, MO) 1/400 in1% BoSA in TBS for 90 minutes, and rabbit anti-TGF-b1(#sc-146; Santa Cruz Biotechnology, Santa Cruz, CA) 1/40 in 1% BoSA in TBS overnight at 4 ˚C. The secondaryantibodies used were: goat anti-mouse-HRP (#P0447;DAKO, Carpinteria, CA) 1/100 for 60 minutes (foraSMA) and ‘‘Envision þ System/HRP, Rabbit’’ (#K4003;DAKO) neat for 60 minutes (for TGF-b1). Developmentwas with 3´-diamino benzidine (#2014; Zymed Labora-tories, South San Francisco, CA) for 2 minutes (aSMA)and 5 minutes (TGF-b1) followed by a counterstainwith hematoxylin. A negative control was used foreach protein that consisted of no primary antibody.
To enable an objective and quantitative scoringsystem, slides were then visualized using a NikonEP600 microscope (Kanagawa, Japan) fitted with aSpot RT slider cooled CCD camera (Diagnostic Instru-ments, Inc., Sterling Heights, MI) and captured directlyas digital images. Up to five fields were captured fromeach slide, and all slides were photographed on thesame day to avoid any variability associated with thelight source. Image morphometry was analyzed usingImagePro Plus� image analysis software (Version4.1.29, Media Cybernetics, Silver Spring, MD), whichcan automatically calculate the area (square microns)of stained protein (brown) in each of the sections. TheTGF-b1 was mainly prevalent in the epidermis, so onlythe protein within the epidermal border was counted.Alpha-SMA is present in blood vessels and the erector
pili muscle associated with hair follicles, as well as inmyofibroblasts. To ensure only interstitial aSMA wasincluded, counting was performed inside 50-mm-squareboxes positioned within the interstitial area (avoidingepidermis, hair follicles, and blood vessels). The aver-
age of 12 of these boxes was used for each field, withup to five fields viewed per slide.
Statistical analysisData for fetuses and lambs were analyzed separately byanalysis of variance using hierarchical models to parti-tion variability according to different levels of replica-tion and sampling. At the highest level, differenceswere tested against variability between replicate ani-mals. At the next level, differences between burn andcontrol treatments and the interaction of this compar-ison with days were tested against the residual vari-ation from the split plot design at the tissue level.These steps were all that were required for analysis oflight microscopy. In the immunohistochemical assess-ment sampling variability was estimated from the dif-ferences between the five fields for each tissue sample.In the case of aSMA, variation between the 12 boxes foreach field was used to estimate the subsampling vari-ation. Variance components were estimated by equatingexpected mean squares with estimated mean squares ateach level of the hierarchical model. These variancecomponents were then used in sensitivity analysesto assess the impact of the changes in the numberof animals, tissue samples, field, and boxes on thevariance of the population mean.
RESULTSThere was a 100% survival rate for both fetus and lamb.We found a temperature of 66 ˚C for 7 seconds createda deep dermal burn injury in the fetus and 82 ˚C for 10seconds created the same wound in the lamb.
Macroscopic analysis of scalded tissueAt fetal postmortem, the wound was visible as a hyper-emic circle at day 1 (and day 2 during the creation of themodel), but by day 7 and subsequently thereafter theblack ink tattoo was the only method of identifying thescalded area (Figure 1). On several fetuses at day 14 and21, there was a well-circumscribed area of soft exudateoverlying the scald area. This fell away on gentle lavagewith normal saline to reveal uninjured skin beneath. Thescald area was covered by wool at day 60.
On postmortem of the lambs, the areas of scaldwere easily identified at all time points. Eschar wasevident up to day 21 post injury, and absent by day 60.After removal of the eschar, palpable elevated contrac-ture was evident in the center of the scalded area. Dueto the regeneration of wool and relatively small size ofthe injury, it was occasionally difficult to identify thescald at day 60. We did not attempt to shave the wooloff, as this may have induced further tissue trauma.
WOUND REPAIR AND REGENERATION192 FRASER ET AL. MARCH–APRIL 2005

Histopathological analysis of scarringThe histopathologist’s composite score for all sampleswere compared against each other (intra observercorrelation), using kappa measurement of agreement,which provides a coefficient of agreement for nominalscales.21 The kappa value in the fetal samples was 0.53(standard error 0.049), which was lower than that forthe lambs, at 0.742 (standard error 0.042).21
The composite scores for the five markers of injuryof fetus and lamb in triplicate samples were comparedat each time point for burn and control skin (Figure 2).The largest difference between fetus and lamb wasseen in the number of fibroblasts, followed by changesin the dermis, with the smallest difference being
changes in epidermis. However, there were changes inall categories. Epidermal changes were prominent inthe earlier stages post injury, but had resolved in thelater stages, explaining the relatively low differences inepidermal scoring between fetus and lamb. In all sam-ples of lamb tissue, there was a statistically significantdifference in scores between burnt and control samplesat all time periods, indicating that the histopathologistcould determine differences between control andscalded lamb tissue. In the fetus, there was a statistic-ally significant difference between burn and controlscores at day 1, but no statistically significant differ-ence following that. Thus, the injury created on thelamb was histopathologically detectable throughoutthe study period but was histopathologically undetect-able after day 1 in the fetus.
Immunohistochemical analysis of scarringAlpha-SMA staining was localized to blood vessels, erec-
tor pili muscle, and myofibroblasts in the interstitium(Figure 3). The amount of aSMA was calculated and theresults were expressed as average � standard error ofthe mean (Figure 4). Thermal injury resulted in no sig-nificant differences in quantity of aSMA in the fetalmodel at any stage post injury, nor were there any sig-nificant differences in content of aSMA between controlsamples of fetal and lamb skin. However, there weresignificant differences in aSMA content of the burnt andcontrol lamb at all stages other than day 60.
TGF-b1 staining was localized mainly in the epider-mis with some staining in developing hair follicles
LambFetus
Day 21
Day 14
Day 7
FIGURE 3. Representative photographs of the fetal and lambflank at 7, 14, and 21 days after burn (66 ˚C for 7 seconds and82 ˚C for 10 seconds, respectively). Arrows indicate the locationof the burn circles (diameter 1.5 cm).
100 µm
FIGURE 1. Representative photomicrograph of fetal skin at 2days post injury following application of heated water at 66 ˚Cfor 7 seconds. The epidermis has necrosed and fallen off, andthere is subtotal necrosis in a number of the hair follicles (H&Estaining).
100 µm
FIGURE 2. Representative photomicrograph of lamb skin at 2days post injury following application of heated water at 82 ˚Cfor 10 seconds. In comparison to the fetal skin, the moreadherent epidermis is still present but all epidermal nuclei aredead. As in the fetal skin, there is subtotal necrosis in a numberof the hair follicles (H&E staining).
WOUND REPAIR AND REGENERATIONVOL. 13, NO. 2 FRASER ET AL. 193
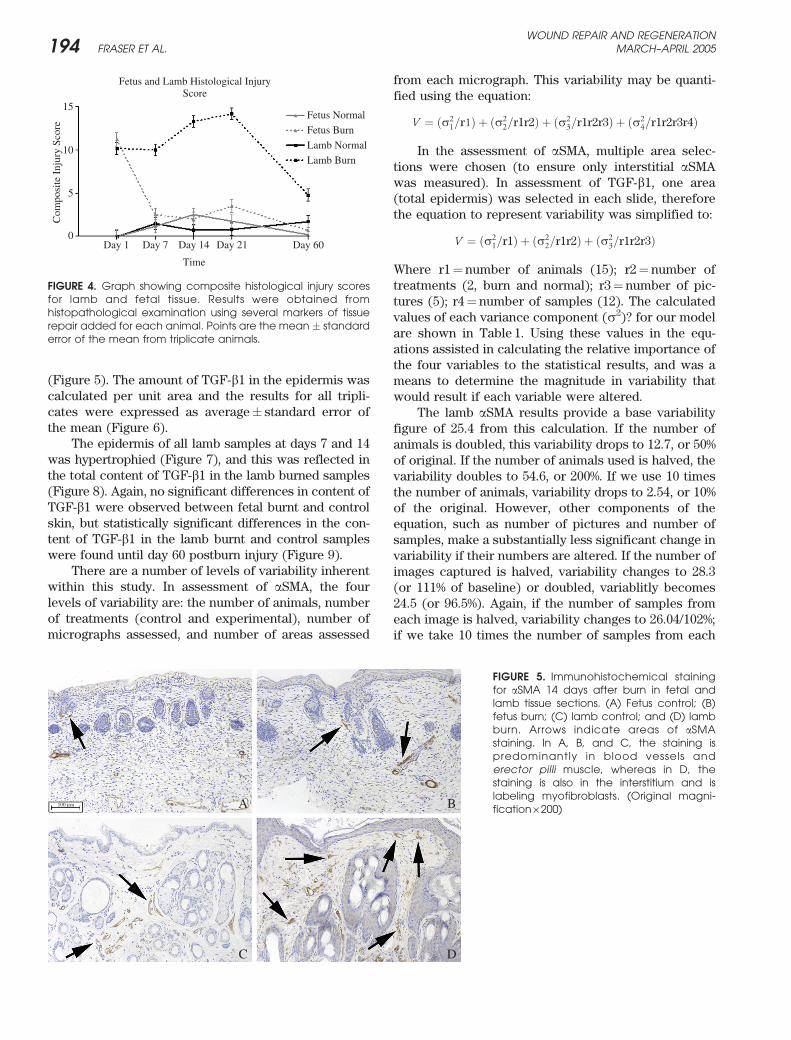
(Figure 5). The amount of TGF-b1 in the epidermis wascalculated per unit area and the results for all tripli-cates were expressed as average� standard error ofthe mean (Figure 6).
The epidermis of all lamb samples at days 7 and 14was hypertrophied (Figure 7), and this was reflected inthe total content of TGF-b1 in the lamb burned samples(Figure 8). Again, no significant differences in content ofTGF-b1 were observed between fetal burnt and controlskin, but statistically significant differences in the con-tent of TGF-b1 in the lamb burnt and control sampleswere found until day 60 postburn injury (Figure 9).
There are a number of levels of variability inherentwithin this study. In assessment of aSMA, the fourlevels of variability are: the number of animals, numberof treatments (control and experimental), number ofmicrographs assessed, and number of areas assessed
from each micrograph. This variability may be quanti-fied using the equation:
V ¼ ðs21=r1Þ þ ðs2
2=r1r2Þ þ ðs23=r1r2r3Þ þ ðs2
4=r1r2r3r4Þ
In the assessment of aSMA, multiple area selec-tions were chosen (to ensure only interstitial aSMAwas measured). In assessment of TGF-b1, one area(total epidermis) was selected in each slide, thereforethe equation to represent variability was simplified to:
V ¼ ðs21=r1Þ þ ðs2
2=r1r2Þ þ ðs23=r1r2r3Þ
Where r1¼ number of animals (15); r2¼ number oftreatments (2, burn and normal); r3¼ number of pic-tures (5); r4¼ number of samples (12). The calculatedvalues of each variance component (s2)? for our modelare shown in Table 1. Using these values in the equ-ations assisted in calculating the relative importance ofthe four variables to the statistical results, and was ameans to determine the magnitude in variability thatwould result if each variable were altered.
The lamb aSMA results provide a base variabilityfigure of 25.4 from this calculation. If the number ofanimals is doubled, this variability drops to 12.7, or 50%of original. If the number of animals used is halved, thevariability doubles to 54.6, or 200%. If we use 10 timesthe number of animals, variability drops to 2.54, or 10%of the original. However, other components of theequation, such as number of pictures and number ofsamples, make a substantially less significant change invariability if their numbers are altered. If the number ofimages captured is halved, variability changes to 28.3(or 111% of baseline) or doubled, variablitly becomes24.5 (or 96.5%). Again, if the number of samples fromeach image is halved, variability changes to 26.04/102%;if we take 10 times the number of samples from each
Fetus Normal
Fetus Burn
Lamb Normal
Lamb Burn
Day 1 Day 7 Day 14 Day 21 Day 60
Time
0
10
5
15
Com
posi
te I
njur
y Sc
ore
Fetus and Lamb Histological InjuryScore
FIGURE 4. Graph showing composite histological injury scoresfor lamb and fetal tissue. Results were obtained fromhistopathological examination using several markers of tissuerepair added for each animal. Points are the mean � standarderror of the mean from triplicate animals.
A B
C D
100 µm
FIGURE 5. Immunohistochemical stainingfor aSMA 14 days after burn in fetal andlamb tissue sections. (A) Fetus control; (B)fetus burn; (C) lamb control; and (D) lambburn. Arrows indicate areas of aSMAstaining. In A, B, and C, the staining ispredominantly in blood vessels anderector pilli muscle, whereas in D, thestaining is also in the interstitium and islabeling myofibroblasts. (Original magni-fication·200)
WOUND REPAIR AND REGENERATION194 FRASER ET AL. MARCH–APRIL 2005

image, variability changes to 24.99/98%. Use of thisequation determined from our model allows us tomodify and optimize efficiency in future studies.
DISCUSSIONIt has long been recognized that the fetus heals anincisional wound in a scarless fashion. However, thepathophysiology of the thermal injury and its repair isso far removed from an incisional wound that it wouldbe imprudent to assume the two injuries heal in asimilar fashion. This novel model provides the firstproof that the fetus heals a DDBI in a scarless fashionand the lamb heals a similar wound with scarring.Although the temperatures and duration of injuryrequired to create the injuries in the fetus and lambare different (67 ˚C for 7 seconds and 82 ˚C for 10 sec-onds, respectively), the histological injuries and depth
of burn are similar. This relationship is equivalent tothat seen in human children and adults, first describedby Moritz and Henriques, and is the result of differ-ences in skin thickness and tensile strength.19 The tem-peratures required to inflict a DDBI are much higher inour study than those reported in that previous work,which was unsupported by histopathological assess-ment.
This model provides a vehicle to compare the heal-ing mechanisms of the ovine fetus and lamb inresponse to DDBI. The macroscopic, histological, andimmunohistochemical analysis all support the hypoth-esis that the fetus heals a deep dermal burn injury in ascarless fashion while the lamb heals with scarring.The validated histological scoring system, which exam-ined five parameters recognized to be integral in woundrepair, confirmed the initial macroscopic observationthat evidence of scar formation was not present in thefetus from day 7 postburn, but was present in the lambthroughout all time points examined. The statisticallysignificant differences seen in assessment of burntfetus vs. control at day 1 were as a result of the recentthermal damage and tissue necrosis, and not of tissuerepair.
The immunohistochemical analysis indicates thatthe healing response occurring in this model is consist-ent with current knowledge of the fetal wound healingprocess. Thermal damage to skin is known to result inthe infiltration of fibroblasts and inflammatory cells.22
TGF-b1 induces the conversion of these fibroblasts tomyofibroblasts23 and is known to lead to the synthesisof aSMA and type I collagen by the myofibroblast.23
This results in myofibroblast-conducted contraction ofthe wound as well as formation of the extracellularmatrix. The content of aSMA (and hence the numberof myofibroblasts) in skin has been shown to correlate
Day 1 Day 7 Day 14 Day 21 Day 60
Time
0
80
60
40
20
100
120A
vera
ge α
SM
A(s
quar
e m
icro
ns)
Fetus and Lamb αSMA
Fetus NormalFetus BurnLamb NormalLamb Burn
FIGURE 6. Graph showing semiquantitative analysis ofimmunohistochemistry for aSMA in lamb and fetal tissue. Resultswere obtained from digitally captured images analyzed usingImage Pro Plus (Media Cybernetics v 4.1.29). Points are the mean� standard error of the mean from triplicate animals.
A B
C D
200 µm
FIGURE 7. Immunohistochemical stainingfor TGF-b1 14 days after burn in lamb andfetal tissue sections. (A) Fetus control; (B)fetus burn; (C) lamb control; and (D) lambburn. Arrows indicate areas of TGF-b1staining. The staining is predominantly inthe epidermis, with some in developing hairfollicles. The hypertrophied epidermis in Dshows massive overexpression of TGF-b1.(Original magnification· 100)
WOUND REPAIR AND REGENERATIONVOL. 13, NO. 2 FRASER ET AL. 195

with the degree of contracture seen in skin conditionssuch as contracture and hypertrophic scar tissue for-mation.24 It has been hypothesized that fetal woundsmay heal scarlessly due to the lack of or underdevelop-ment of fetal myofibroblasts.25,26 In this study, there isevidence of myofibroblastic activity in the fetal model,but it is considerably less than that seen in the lamb.There also appears to be a gestational age-relatedincrease in aSMA in the fetus. This is consistent withwork done by others showing that an increase in gesta-tional age correlates with an increase in aSMA expressionand scar-producing capacity.26 In the lamb, the level ofaSMA dissipates quickly after day 14. The disappearanceof myofibroblasts by apoptosis following wound closure iswell established and the reduction in aSMA level seen inthis model may be due to this.27 The temporal relationshipbetween TGF-b1 and aSMA, with the increase in TGF-b1occurring at a similar time to the increase of aSMA, sug-gests a role for TGF-b1 in stimulating the production ofmyofibroblasts and further validates this model.
With the increase of TGF-b1 seen in the lamb, therewas a parallel increase in epidermal area. There was
significant epidermal hyperplasia at days 7 and 14, withthe area of lamb burn epidermis increasing to 3.9 timesthe size of the control at day 14. This corresponded toan increase of TGF-b1 expression, with the amount ofTGF-b1 approximately 3.5 times that of the control atday 14. Application of TGF-b1 to fetal wounds has beenshown to lead to fibrosis and scar formation,28 and it isinteresting that the significant increase in TGF-b1 seenhere in the lamb is not seen in the nonscarring fetus.When antibodies to TGF-b1 and -b2 were administeredto healing wounds, there was found to be a significantreduction in scarring.29 Recent work by others suggeststhat overexpression of TGF-b1 may inhibit apoptosisof the myofibroblast. This would result in an exagger-ated contraction of the wound, together with over-production of collagen and granulation tissue.30 Themassive increase in production of TGF-b1 by the lambkeratinocytes in this model shows the active role ofthese cells not only in reepithelialization, but also inscar maturation.31
Immunohistochemical results can be examined in asemiquantitative, rather than a qualitative manner,using the image analysis method employed here. Com-puter-assisted image analysis has proven superior tovisual estimates of immunostaining, allowing for amuch more objective assessment and less variation.32
A thorough statistical analysis of the results obtainedby this method allowed us to determine the variabilityinherent in the model and, based on this, to predict howaltering some of the parameters may improve theexperimental outcome and reduce the variability inthe results. Here, the variability within the image cap-ture and analysis method was only 3.2–7.5% of the varia-bility between animal replicates (data not shown). Anumber of other predictions can be made using thecalculation formula (in results section) to determinethe effect of using more animals, pictures, and fieldsof view in the analysis. Based on these predictions, wehave determined that we can afford to halve the amountof sampling taken within each picture when measuringaSMA levels. This will enhance the efficiency and speedof our experiments in the future, and similar statisticalanalysis is recommended to others developing compar-able models.
Day 1 Day 7 Day 14 Day 21 Day 60
Time
Fetus and Lamb TGFβ1
120000
90000
60000
30000
0
Am
ount
of
TG
Fβ1
(squ
are
mic
rons
)
Fetus NormalFetus BurnLamb NormalLamb Burn
FIGURE 8. Graph showing semiquantitative analysis ofimmunohistochemistry for TGF-b1 in lamb and fetal epidermis.Results were obtained from digitally captured images analyzedusing Image Pro Plus (Media Cybernetics v 4.1.29). Points arethe mean � standard error of the mean from triplicate animals.
Day 1 Day 7 Day 14Day 21 Day 60Time
Fetus and Lamb Epidermal Area
150000
200000
250000
300000
100000
50000
0
Epi
derm
al A
rea
(squ
are
mic
rons
)
Fetus NormalFetus BurnLamb NormalLamb Burn
FIGURE 9. Graph showing semiquantitative analysis of theepidermal area, showing massive hypertrophy of lambepidermis at burn days 7 and 14. Results were obtained fromthe digitally captured images for TGF-b1 and analyzed usingImage Pro Plus (Media Cybernetics v 4.1.29). Points are themean � standard error of the mean from triplicate animals.
Table 1. Compilation of the variance component (s2) valuesfor each level of replication and sampling in our model, afterpartitioning variability in a hierarchical manner.
s1 s2 s3 s4
Lamb. aSMA 332 43.82 202.1 994.26. TGFb1 63.68 67.4 430.6
Fetus. aSMA 40.56 14.68 7.16 132.19. TGFb1 44.17 124.9 31.33
* There are no s42 values for TGF-b1 as total epidermis was assessed, rather than
taking discrete areas.
WOUND REPAIR AND REGENERATION196 FRASER ET AL. MARCH–APRIL 2005

The environments in which the fetal and lambwounds healed were very different. The fetus is bathedin a sterile amniotic fluid and protected from directtissue trauma, whereas the lamb is not. Previous datahas supported the theory that it is the fetal tissue per seand not the fetal environment that induces a scarlesswound, as the fetal opossum heals an incisional woundin a scarless fashion, despite spending the majority ofits development in the extra-amniotic maternal pouch.33
Hence, we believe that while the warm, growth factor-filled amniotic fluid may be beneficial, it is not an essen-tial contributor to the scarless wound. As previous studieshave shown, it is likely that there is something intrinsic tothe fetal skin itself that enables the skin to heal scarlessly.Elucidation of this factor or factors would be of immeas-urable benefit to the thousands of children and adultswho suffer from burn injuries each year. The develop-ment and further study of this model of scarless fetalwound healing may allow us to achieve that.
REFERENCES1. Bull JP, Fischer AJ. A study of mortality in a burns unit; a revised
estimate. Ann Surg 1954;139:269–74.
2. Wolf SE, Rose JK, Desai MH, Mileski JP, Barrow RE, Herndon DN.
Mortality determinants in massive pediatric burns. An analysis of 103
children with > or ¼ 80% TBSA burns (> or ¼ 70% full-thickness).
Ann Surg 1997;225:554–65; discussion 565–9.
3. American Burn Association. Outcomes measurement in pediatric
burn care: an agenda for research: executive summary and final
report. J Burn Care Rehabil 2003;24:269–74.
4. Greenfield E, Jordan B. Advances in burn wound care. Crit Care
Nurs Clin North Am 1996;8:203–15.
5. Zawacki BE. The natural history of reversible burn injury. Surg
Gynecol Obstet 1974;139:867–72.
6. Williams WG. Pathophysiology of the burn wound. In: Herndon D,
editor. Total burn care. London: W.B. Saunders, 2002:514–22.
7. Lorenz HP, Lin RY, Longaker MT, Whitby DJ, Adzick NS. The fetal
fibroblast: the effector cell of scarless fetal skin repair. Plast
Reconstr Surg 1995;96:1251–9; discussion 1260–1.
8. Gabbiani G. The myofibroblast in wound healing and fibrocon-
tractive diseases. J Pathol 2003;200:500–3.
9. Dugina V, Fontao L, Chaponnier C, Vasiliev J, Gabbiani G. Focal
adhesion features during myofibroblastic differentiation are
controlled by intracellular and extracellular factors. J Cell Sci
2001;114:3285–96.
10. Roberts A. Transforming growth factor B. In: Clark, RAF, editor.
The molecular and cell biology of wound repair, 2nd edn. New
York: Plenum Press, 1996:275–308.
11. Arora PD, McCulloch CA. The deletion of transforming
growth factor-beta-induced myofibroblasts depends on growth
conditions and actin organization. Am J Pathol 1999;155:2087–99.
12. Greenhalgh DG, Wound healing. In: Herndon D, editor. Total burn
care. London: W.B. Saunders, 2002:523–35.
13. Wang R, Ghahary A, Shen Q, Scott PG, Roy K, Tredget EE.
Hypertrophic scar tissues and fibroblasts produce more
transforming growth factor-beta1 mRNA and protein than normal
skin and cells. Wound Rep Reg 2000;8:128–37.
14. Tredget EE, Shankowsky HA, Pannu R, Nedelec B, Iwashina T,
Ghahary A, Taerum TV, Scott PG. Transforming growth factor-
beta in thermally injured patients with hypertrophic scars: effects
of interferon alpha-2b. Plast Reconstr Surg 1998;102:1317–28; dis-
cussion 1329–30.
15. Adzick NS, Harrison MR, Glick PL, Beckstead JH, Villa RL,
Scheuenstuhl H, Goodson WH, 3rd. Comparison of fetal, newborn,
and adult wound healing by histologic, enzyme-histochemical,
and hydroxyproline determinations. J Pediatr Surg 1985;20:315–9.
16. Burrington JD. Wound healing in the fetal lamb. J Pediatr Surg
1971;6:523–8.
17. Longaker MT, Whitby DJ, Jennings RW, Duncan BW, Ferguson MW,
Harrison MR, Adzick NS. Fetal diaphragmatic wounds heal with
scar formation. J Surg Res 1991;50:375–85.
18. Kumta S, Ritz M, Hurley JV, Crowe D, Romeo R, O’Brien BM.
Acute inflammation in foetal and adult sheep: the response to
subcutaneous injection of turpentine and carrageenan. Br J Plast
Surg 1994;47:360–8.
19. Moritz A, Henriques F. Studies in thermal injury II. The relative
importance of time and surface temperature in the causation of
cutaneous burns. Am J Pathol 1947;23:695–720.
20. Shakespeare PG. Standards and quality in burn treatment. Burns
2001;27:791–2.
21. Cohen J. A co-efficient of agreement for nominal scales. Educ
Psychol Meas 1960;20:37–46.
22. Diegelmann RF, Cohen IK, Kaplan AM. The role of macrophages
in wound repair: a review. Plast Reconstr Surg 1981;68:107–13.
23. Desmouliere A, Geinoz A, Gabbiani F, Gabbiani G. Transforming
growth factor-beta 1 induces alpha-smooth muscle actin expres-
sion in granulation tissue myofibroblasts and in quiescent and
growing cultured fibroblasts. J Cell Biol 1993;122:103–11.
24. Igarashi A, Nashiro K, Kikuchi K, Sato S, Ihn H, Fujimoto M,
Grotendorst GR, Takahara K. Connective tissue growth factor
gene expression in tissue sections from localized scleroderma,
keloid, and other fibrotic skin disorders. J Invest Dermatol
1996;106:729–33.
25. Estes JM, Vande Berg JS, Adzick NS, MacGillivray TE, Desmouliere A,
Gabbiani G. Phenotypic and functional features of myofibroblasts
in sheep fetal wounds. Differentiation 1994;56:173–81.
26. Cass DL, Sylvester KG, Yang EY, Crombleholme TM, Adzick NS.
Myofibroblast persistence in fetal sheep wounds is associated with
scar formation. J Pediatr Surg 1997;32:1017–21; discussion 1021–2.
27. Desmouliere A, Redard M, Darby I, Gabbiani G. Apoptosis med-
iates the decrease in cellularity during the transition between
granulation tissue and scar. Am J Pathol 1995;146:56–66.
28. Lanning DA, Nwomeh BC, Montante SJ, Yager DR, Diegelmann RF,
Haynes JH. TGF-beta1 alters the healing of cutaneous fetal
excisional wounds. J Pediatr Surg 1999;34:695–700.
29. Shah M, Foreman DM, Ferguson MW. Control of scarring in adult
wounds by neutralising antibody to transforming growth factor
beta. Lancet 1992;339 (8787):213–4.
30. Zhang HY, Phan SH. Inhibition of myofibroblast apoptosis by
transforming growth factor beta (1). Am J Respir Cell Mol Biol
1999;21:658–65.
31. Hakvoort T, Altun V, van Zuijlen PP, de Boer WI, van
Schadewij WA, van der Kwast TH. Transforming growth factor-
beta (1)-beta (2)-beta (3), basic fibroblast growth factor and
vascular endothelial growth factor expression in keratinocytes
of burn scars. Eur Cytokine Netw 2000;11:233–9.
32. Seidal T, Balaton AJ, Battifora H. Interpretation and quantifica-
tion of immunostains. Am J Surg Pathol 2001;25:1204–7.
33. Armstrong JR, Ferguson MW. Ontogeny of the skin and the
transition from scar-free to scarring phenotype during wound
healing in the pouch young of a marsupial, Monodelphis domes-
tica. Dev Biol 1995;169:242–60.
WOUND REPAIR AND REGENERATIONVOL. 13, NO. 2 FRASER ET AL. 197




















