Nonspecific and immune-specific up-regulation of cytokines in rabbit dermal tuberculous (BCG)...
11
Nonspecific and immune-specific up-regulation of cytokines in rabbit dermal tuberculous (BCG) lesions Katsunori Sugisaki,* Arthur M. Dannenberg, Jr.,* ²‡§ YasuharuAbe,* Junji Tsuruta,* Wei-Juin Su, ² Waheeda Said,* Lili Feng, Teizo Yoshimura, Paul J. Converse, ² and Phoebe Mounts ² Departments of *Environmental Health Sciences, ² Molecular Microbiology and Immunology, and ‡ Epidemiology, School of Hygiene and Public Health, and § Department of Pathology, School of Medicine, The Johns Hopkins University, Baltimore, Maryland Abstract: To our knowledge, this is the first se- quential study of cytokines in tissue sections of developing and healing tuberculous (BCG) lesions. In situ hybridization, immunohistochemical, and RT-PCR techniques were used. Cytokine mRNAs showed a biphasic pattern. The percentage of mononuclear cells (MN) containing IL-1b, TNF-a, MCP-1, and IL-8 mRNAs was highest in 1- to 3-day lesions, apparently because of the nonspecific in- flammatory response caused by the tubercle bacilli in the BCG vaccine. At 5 days, this percentage was significantly reduced. With IFN-g, the peak and trough were delayed by 2 days. By 9 days, the percentage of MN containing the mRNAs of all five cytokines had again increased and the rabbits had become tuberculin-positive. In general, MCP-1 and TNF-a proteins and the vascular adhesion mol- ecules, ICAM, VCAM, and perhaps ELAM, peaked at about 3 days. Many mononuclear cells surround- ing the central areas of solid and liquefied caseous necrosis contained chemokine IL-8 mRNA. IL-8 is known to attract PMN, and PMN were present nearby. In contrast, MN containing chemokine MCP-1 mRNA were present more peripherally in areas rich in macrophages and lymphocytes. The early nonspecific cytokine response seems to be an adjuvant effect of the mycobacteria in BCG vaccine in that it causes a rapid entry of macrophages, lymphocytes, granulocytes, and probably dendritic cells into local sites of antigen deposition. This effect should be considered in developing improved vaccines for the prevention of tuberculosis, be- cause BCG vaccines producing a strong early cyto- kine response should be more immunogenic than BCG vaccines with similar antigens producing a weak response. J. Leukoc. Biol. 63: 440–450; 1998. Key Words: IL-1b · TNF-a · MCP-1 · IL-8 (NAP-1) · IFN-g · ICAM-1 · ELAM-1 (E-selectin) · VCAM-1 INTRODUCTION This report describes sequential changes in mRNAs of five major cytokines: interleukin-1b (IL-1b), tumor necrosis factor a (TNF-a), monocyte chemoattractant protein-1 (MCP-1), inter- leukin-8 (IL-8), and interferon-g (IFN-g), as rabbit Bacille Calmette Gue ´rin (BCG) lesions developed and healed. IL-1b and TNF-a are primary cytokines that up-regulate the produc- tion of other cytokines [1–3]. These primary cytokines also up-regulate adhesion molecules in the microvasculature that enable the diapedesis of mononuclear cells (MN) and polymor- phonuclear neutrophils (PMN) into inflammatory sites [4–6]. MCP-1 is a C-C chemokine that attracts and activates MN, i.e., macrophages and lymphocytes [7–9]. IL-8 is a C-X-C chemo- kine that attracts and activates granulocytes, especially PMN [7, 9]. IFN-g is an induced cytokine produced by natural killer (NK) cells [10] and by antigen-specific Th1 lymphocytes as part of the cell-mediated immune response [11]. IFN-g activates macrophages to inhibit (or kill) tubercle bacilli [12–14]. Several investigators have evaluated the cytokines present at the sites of active tuberculosis in humans [reviewed in refs. 15–17]. In tuberculous pleuritis (a self-healing form of human tuberculosis), cytokine proteins and mRNAs were found in the Abbreviations: BCG, Bacille Calmette-Gue ´rin, the attenuated Mycobacte- rium bovis used worldwide as a vaccine for tuberculosis; ELAM-1, endothelial- leukocyte adhesion molecule 1 (E-selectin); ICAM-1, intercellular adhesion molecule 1, a member of the immunoglobulin supergene family; IFN-g, interferon-g; IL-1b, interleukin-1b; IL-8, interleukin-8 (same as NAP-1), a C-X-C chemokine; IP-10, IFN-g-inducible protein-10; MCP-1, monocyte chemoattractant (activating) protein 1, a C-C chemokine; MIP-1a, macrophage inflammatory protein 1a, a C-C chemokine; MIP-1b, macrophage inflammatory protein 1b, a C-C chemokine; NAP-1, neutrophil attractant/activating protein 1 (same as IL-8); PBMC, peripheral blood mononuclear cells; PBS, phosphate- buffered saline solution; PPD, purified protein derivative of Mycobacterium tuberculosis; RT-PCR, reverse transcription-polymerase chain reaction; TGF-b, transforming growth factor b; TNF-a, tumor necrosis factor a; VCAM-1, vascular cell adhesion molecule 1, a member of the immunoglobulin supergene family; MN, mononuclear cells; NK cells, natural killer cells. Correspondence: Arthur M. Dannenberg, Jr., M.D., Johns Hopkins School of Hygiene and Public Health, 615 N. Wolfe Street, Baltimore, MD 21205. Katsunori Sugisaki and Yasuharu Abe were on leave of absence from the Department of Internal Medicine, Oita Medical University, Oita, Japan. Junji Tsuruta was on leave of absence from the Institute for Medical Immunology, Kumamoto University School of Medicine, Kumamoto, Japan. Wei-Juin Su is on leave of absence from the Chest Department, Veterans General Hospital, Taipei, Taiwan. Lili Feng is from the Department of Immunology, Scripps Research Institute, La Jolla, CA. Teizo Yoshimura is from the Laboratory of Immunobiol- ogy, National Cancer Institute, Frederick, MD. Received September 15, 1997; revised December 22, 1997; accepted December 23, 1997. 440 Journal of Leukocyte Biology Volume 63, April 1998
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Nonspecific and immune-specific up-regulation of cytokines in rabbit dermal tuberculous (BCG)...

Nonspecific and immune-specific up-regulation of cytokinesin rabbit dermal tuberculous (BCG) lesions
Katsunori Sugisaki,* Arthur M. Dannenberg, Jr.,*†‡§ Yasuharu Abe,* Junji Tsuruta,* Wei-Juin Su,†
Waheeda Said,* Lili Feng, Teizo Yoshimura, Paul J. Converse,† and Phoebe Mounts†
Departments of *Environmental Health Sciences, †Molecular Microbiology and Immunology,and ‡Epidemiology, School of Hygiene and Public Health, and §Department of Pathology, School of Medicine,The Johns Hopkins University, Baltimore, Maryland
Abstract: To our knowledge, this is the first se-quential study of cytokines in tissue sections ofdeveloping and healing tuberculous (BCG) lesions.In situ hybridization, immunohistochemical, andRT-PCR techniques were used. Cytokine mRNAsshowed a biphasic pattern. The percentage ofmononuclear cells (MN) containing IL-1b, TNF-a,MCP-1, and IL-8 mRNAs was highest in 1- to 3-daylesions, apparently because of the nonspecific in-flammatory response caused by the tubercle bacilliin the BCG vaccine. At 5 days, this percentage wassignificantly reduced. With IFN-g, the peak andtrough were delayed by 2 days. By 9 days, thepercentage of MN containing the mRNAs of all fivecytokines had again increased and the rabbits hadbecome tuberculin-positive. In general, MCP-1 andTNF-a proteins and the vascular adhesion mol-ecules, ICAM, VCAM, and perhaps ELAM, peakedat about 3 days. Many mononuclear cells surround-ing the central areas of solid and liquefied caseousnecrosis contained chemokine IL-8 mRNA. IL-8 isknown to attract PMN, and PMN were presentnearby. In contrast, MN containing chemokineMCP-1 mRNA were present more peripherally inareas rich in macrophages and lymphocytes. Theearly nonspecific cytokine response seems to be anadjuvant effect of the mycobacteria in BCG vaccinein that it causes a rapid entry of macrophages,lymphocytes, granulocytes, and probably dendriticcells into local sites of antigen deposition. Thiseffect should be considered in developing improvedvaccines for the prevention of tuberculosis, be-cause BCG vaccines producing a strong early cyto-kine response should be more immunogenic thanBCG vaccines with similar antigens producing aweak response. J. Leukoc. Biol. 63: 440–450;1998.
Key Words: IL-1b · TNF-a · MCP-1 · IL-8 (NAP-1) · IFN-g ·ICAM-1 · ELAM-1 (E-selectin) · VCAM-1
INTRODUCTION
This report describes sequential changes in mRNAs of fivemajor cytokines: interleukin-1b (IL-1b), tumor necrosis factor a
(TNF-a), monocyte chemoattractant protein-1 (MCP-1), inter-leukin-8 (IL-8), and interferon-g (IFN-g), as rabbit BacilleCalmette Guerin (BCG) lesions developed and healed. IL-1band TNF-a are primary cytokines that up-regulate the produc-tion of other cytokines [1–3]. These primary cytokines alsoup-regulate adhesion molecules in the microvasculature thatenable the diapedesis of mononuclear cells (MN) and polymor-phonuclear neutrophils (PMN) into inflammatory sites [4–6].MCP-1 is a C-C chemokine that attracts and activates MN, i.e.,macrophages and lymphocytes [7–9]. IL-8 is a C-X-C chemo-kine that attracts and activates granulocytes, especially PMN[7, 9]. IFN-g is an induced cytokine produced by natural killer(NK) cells [10] and by antigen-specific Th1 lymphocytes as partof the cell-mediated immune response [11]. IFN-g activatesmacrophages to inhibit (or kill) tubercle bacilli [12–14].
Several investigators have evaluated the cytokines present atthe sites of active tuberculosis in humans [reviewed in refs.15–17]. In tuberculous pleuritis (a self-healing form of humantuberculosis), cytokine proteins and mRNAs were found in the
Abbreviations: BCG, Bacille Calmette-Guerin, the attenuated Mycobacte-rium bovis used worldwide as a vaccine for tuberculosis; ELAM-1, endothelial-leukocyte adhesion molecule 1 (E-selectin); ICAM-1, intercellular adhesionmolecule 1, a member of the immunoglobulin supergene family; IFN-g,interferon-g; IL-1b, interleukin-1b; IL-8, interleukin-8 (same as NAP-1), aC-X-C chemokine; IP-10, IFN-g-inducible protein-10; MCP-1, monocytechemoattractant (activating) protein 1, a C-C chemokine; MIP-1a, macrophageinflammatory protein 1a, a C-C chemokine; MIP-1b, macrophage inflammatoryprotein 1b, a C-C chemokine; NAP-1, neutrophil attractant/activating protein 1(same as IL-8); PBMC, peripheral blood mononuclear cells; PBS, phosphate-buffered saline solution; PPD, purified protein derivative of Mycobacteriumtuberculosis; RT-PCR, reverse transcription-polymerase chain reaction; TGF-b,transforming growth factor b; TNF-a, tumor necrosis factor a; VCAM-1,vascular cell adhesion molecule 1, a member of the immunoglobulin supergenefamily; MN, mononuclear cells; NK cells, natural killer cells.
Correspondence: Arthur M. Dannenberg, Jr., M.D., Johns Hopkins School ofHygiene and Public Health, 615 N. Wolfe Street, Baltimore, MD 21205.
Katsunori Sugisaki and Yasuharu Abe were on leave of absence from theDepartment of Internal Medicine, Oita Medical University, Oita, Japan. JunjiTsuruta was on leave of absence from the Institute for Medical Immunology,Kumamoto University School of Medicine, Kumamoto, Japan. Wei-Juin Su is onleave of absence from the Chest Department, Veterans General Hospital, Taipei,Taiwan. Lili Feng is from the Department of Immunology, Scripps ResearchInstitute, La Jolla, CA. Teizo Yoshimura is from the Laboratory of Immunobiol-ogy, National Cancer Institute, Frederick, MD.
Received September 15, 1997; revised December 22, 1997; acceptedDecember 23, 1997.
440 Journal of Leukocyte Biology Volume 63, April 1998

pleural exudates and/or in pleural tissue biopsies. The cyto-kines present were TNF [18], IFN-g [18, 19], IL-10 [19], IL-12[20], and others. In tuberculous granulomas within humanlungs, IL-1 protein [21] and transforming growth factor b
(TGF-b) [22] were present. None of these studies evaluatedchanges in cytokine mRNA or protein as the lesions progressedand regressed.
Other investigators evaluated the cytokines in peripheralblood mononuclear cells (PBMC) from tuberculous patients.With the reverse transcription-polymerase chain reaction (RT-PCR) technique, IL-1, IL-8, and TNF-a mRNAs were found inPBMC of these patients, but not in PBMC from healthytuberculin-negative people [23]. The PBMC of patients withsevere tuberculosis also contained IFN-g mRNA [23]. Whencultured 24 h in the presence of tubercle bacilli, the PBMC oftuberculous patients showed suppressed IFN-g protein andmRNA compared to healthy tuberculin-positive people [24].More TGF-b, an immunosuppressive cytokine, was producedby (and found in) the blood monocytes of patients withtuberculosis than by (or in) the blood monocytes of healthytuberculin-positive controls [17, 22, 25]. Although analyses ofhuman PBMC should be prognostically useful, they do notalways reflect the situation in the tuberculous lesions them-selves. For example, in hosts with poor resistance, an increasein suppressive cytokines may reflect (and be the cause of) theprogression of the local disease. On the other hand, in hostswith good resistance an increase in such suppressors mayreflect the regression or control of the local disease becausefurther expansion of the immune forces is no longer needed andmay even be detrimental.
The cytokines participating in mouse tuberculosis have beenreviewed [26, 27]. In C57BL/6 mice, lungs (infected by aerosol)with each of three strains of M. tuberculosis contained themRNAs of IL-1b, TNF-a, IL-2, and IFN-g, and the chemo-kines MCP-1, MIP-1a, MIP-2, and IP-10 [28]. RT-PCRmethodology was used. In general (in mice), the largest amountsof these mRNAs (compared to the amounts of a housekeepinggene) were present at 60 and 80 days after infection.
In the livers of mice infected intravenously with virulent M.tuberculosis (Erdman), IL-12 mRNA and IFN-g mRNA in-creased as the infection progressed [29]. In the spleens of miceinfected intravenously with M. avium, IFN-g mRNA peaked atabout 30 days [30]. In none of these mouse studies, however,were the cytokines or their mRNAs actually analyzed in tissuesections of the tuberculous lesions.
The studies reported herein were undertaken to evaluatedirectly (by in situ hybridization techniques) the number anddistribution of cells containing cytokine mRNAs within devel-oping and healing BCG lesions in rabbits. We also evaluatedseveral vascular adhesion molecules that control the infiltrationof leukocytes into these lesions.
The rabbit model was chosen because tuberculous lesions ofboth rabbits and humans show a large amount of caseousnecrosis and, among the commonly used laboratory animals,only rabbits (like humans) have lesions that readily liquefy andform cavities [31–33]. In rabbits BCG vaccine produces typicaltuberculous lesions with caseous centers that soon liquefy.
MATERIALS AND METHODS
Vaccination of rabbits with BCG and removalof the resulting lesions
New Zealand White rabbits (2.3–3.0 kg) were injected intradermally inmultiple sites; each site received about 5 3 106 Tice BCG [4]. The resultinglesions were measured with calipers, as described previously [34]. Briefly, theproduct of length and width and pinched double thickness (in mm), multipliedby a factor of 0.52, provided the volume of the lesion in cubic millimeters. Afteran intramuscular injection of 0.3–0.4 mL of ketamine hydrochloride (100mg/mL), two lesions were surgically removed at various times. On the last day ofeach experiment, the rabbits were killed with a 2.5-to 3.0-mL intravenousinjection of pentobarbital (65 mg/mL) and the remaining lesions were removedimmediately thereafter.
Tuberculin tests
A 1:30 dilution of 43 Old Tuberculin (0.1 mL/site; Lederle Laboratories,American Cyanamid Co., Pearl River, NY) was injected intradermally and thevolume of the resulting reaction was measured with calipers 2 days later [34].
Preparation of tissues for histological evaluation
The BCG lesions (and tuberculin reactions) were removed, bisected on the frontto rear axis, and placed in cold (4°C) 4% paraformaldehyde in 0.1 M sodiumphosphate buffer (pH 7.2) made with diethylpyrocarbonate (DEPC)-treateddistilled deionized water [35]. After 4–5 h on a shaker at 4°C, the specimenswere transferred to 20% sucrose in phosphate-buffered saline (PBS) [sodiumphosphate buffer (0.01 M, pH 7.2) in NaCl (0.15 M) in DEPC-treated water],and then shaken at 4°C overnight. The next morning they were transferred to a20% sucrose-5% glycerol solution in the same PBS and shaken at 4°C foranother 2 h.
For the in situ hybridization procedures, the specimens were placed inTissue-Tek O.C.T. embedding compound (Miles, Inc., Elkart, IN) in plasticboats and quick-frozen in an isopentane slush created by immersing a beaker ofisopentane in liquid nitrogen. After the frozen specimens were removed and theisopentane had evaporated from their surfaces, they were wrapped in Parafilm(American National Can Co., Greenwich, CT) and stored in a 280°C freezeruntil used for sectioning in a cryostat.
For the immunohistochemical procedures [4], the tissue specimens were notfixed in parformaldehyde, but were immediately frozen in O.C.T. embeddingcompound and stored as described above.
For careful histological study, some of the specimens were embedded at 4°Cin glycol methacrylate (Immunobed, Polysciences, Inc., Warrington, PA). Someof the specimens were also immediately frozen in O.C.T., without paraformalde-hyde fixation, in order to demonstrate (by immunohistochemical techniques)TNF-a and MCP-1 proteins and the vascular adhesion molecules, ICAM-1,ELAM-1, and VCAM-1.
In situ hybridization procedure
This procedure is essentially that of Gillitzer et al. [36, 37] with the slightmodifications described prevously [3]. The in situ hybridizations for cytokinemRNAs were performed with 35S-antisense RNA probes (complementary tocellular mRNA). Duplicate tissue sections were hybridized with 35S-sense RNAprobes (homologous to cellular mRNA). These 35S-sense RNA probes did notlabel the cells evaluated in the experiments reported here.
For autoradiography, slides were dipped into Kodak NTB-2 emulsion(diluted with equal parts of 600 mM ammonium acetate) and exposed at 4°C for7–21 days. The slides were then developed and counterstained with Giemsa ormethyl green.
Preparation and sources of 35S-antisenseand 35S-sense IL-1b, TNF-a, MCP-1, and IL-8(NAP-1) RNAs for in situ hybridization35S-antisense and 35S-sense RNA probes were made, as previously described[3], from plasmids containing cDNA inserts of rabbit IL-1b, MCP-1, IL-8, andTNF-a. The T3/T7 Riboprobe Synthesis System (Promega Corp., Madison, WI)
Sugisaki et al. Cytokines in tuberculous lesions 441

with 35S-UTP supplied by Dupont-New England Nuclear Products (Boston,MA) was used.
Recombinant Okayama plasmids containing cDNA for rabbit IL-1b wereprovided by Masaru Yoshinaga (First Department of Pathology, KumamotoUniversity, Kumamoto, Japan) [38, 39].
Recombinant Bluescript plasmids containing cDNA for rabbit MCP-1 andrabbit IL-8 were produced in the laboratory of Teizo Yoshimura at the NationalCancer Institute in Frederick, MD [40].
A recombinant Bluescript plasmid containing cDNA for rabbit TNF-a wasproduced (also in this National Cancer Institute laboratory) from a cDNAlibrary obtained from Concavalin A-stimulated rabbit spleen cells [unpub-lished work]. The sequences were identical to those published by Ito et al. [41,42].
TNF-a cDNA insert was shortened as follows to enable us to make effective35S-antisense and 35S-sense RNA probes: the TNF-a plasmid was cut withHind III just outside the TNF-a insert and then cut with Nco I. The Nco I cutsTNF-a at 153 nucleotides distal to its termination codon [42]. The shortened4-kb plasmid containing the remaining TNF-a coding sequences was gelpurified using the Geneclean Kit (Bio-101, Inc., Vista, CA). Because this linearplasmid (produced by Nco I and Hind III) does not have ends suitable forcircularization, an adapter was synthesized as two oligonucleotides that weresubsequently annealed to each other:
. . . .58CATGGGGGA380 0 0 0 0
38CCCCTTCGA58. . . .
The annealed adapter was ligated into the 4-kb plasmid, which then circular-ized and was able to transform Escherichia coli (maximal efficiency STBL-2-competent E. coli with low recombination activity, supplied by Life Technolo-gies, Inc., Gaithersburg, MD). This transformation proved successful in all ofthe 12 colonies that were cultured and then screened after extraction andpurification of the shortened TNF-a plasmids (now designated pWTA) withPERFECTprep Plasmid DNA Kit (5 PRIME = 3 PRIME, Inc., Boulder, CO).For in vitro transcription, the shortened TNF-a cDNA plasmid (pWTA) was (1)linearized with Nco I and transcribed from the T7 promoter to generate theantisense probe, and (2) linearized with EcoR I and transcribed from the T3promoter to generate the sense probe.
RT-PCR
Because we were unable to demonstrate IFN-g in tissue sections of BCG lesionsby in situ hybridization, we used the more sensitive (semi-quantitative)RT-PCR procedure. Half of each BCG lesion was minced in a sterile Petri dish(placed on cracked ice), transferred to an Eppendorf tube containing 600 µL ofRNA Stat-60 from Teltest, Inc. (Friendswood, TX) to inhibit RNases, immersedfor approximately 10 s in liquid nitrogen, transferred to dry ice, and stored at
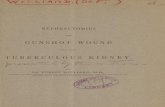
Fig. 1. (A) Size of BCG lesions in rabbits at various times after receiving eightintradermal injections of about 5 3 106 BCG on each flank. Note the biphasicnature of the curve (see text). Lesions from day 0–5 came from the same fourrabbits and the paired t test was used. Lesions from day 9–37 came from otherrabbits, and the unpaired t test was used. Means and standard errors are shown,along with the statistical significance between points: *P , 0.05 and ***P ,
0.01. The rabbits had significant dermal tuberculin reactions from 9 days on:2, 0 to 100 mm3; 1,100 to 200 mm3; 11, 200 to 400 mm3; and 111, greaterthan 400 mm3. (B) Mononuclear cells (MN) and PMN per square millimeter oftissue section in BCG lesions at various times during their development andhealing. PMN accumulate around the caseous necrotic areas of the BCGlesions. Note that even though the number of MN per square millimeterremained high during healing (at 37 days), the volume of the BCG lesions wasdiminished (see panel A). (C) The number of bacilli in the central area of BCGlesions of various ages, visualized by acid-fast staining with carbol fuchsin. Asthe lesions progressed, a shift occurred from bacilli located intracellularly(mostly in intact and necrotic macrophages) to bacilli located extracellularly inareas of (liquefied) caseous necrosis. By 23 days, the number of bacilli wasgreatly reduced.
442 Journal of Leukocyte Biology Volume 63, April 1998

280°C. RNA was isolated (with minor modifications) according to theinstructions provided with the RNA Stat-60.
The RT-PCR were performed according to the directions in the Perkin ElmerGeneAmp RNA PCR kit from Roche Molecular Systems, Inc. (Branchburg, NJ).The forward and reverse DNA primers were derived from the sequence of rabbitIFN-g provided by Buffer Fennie at Genentech, Inc. (South San Francisco, CA).For a reference standard, forward and reverse DNA primers of the housekeep-ing gene for glyceraldehyde-3-phosphate dehydrogenase (GAPDH; provided byDiane E. Griffin, Johns Hopkins School of Hygiene [43]) were used (instead ofthe IFN-g primers) with duplicate master mixes.
Aliquots of each DNA sample of IFN-g and GAPDH (amplified by PCR)were placed on 0.8% agarose gels, electrophoresed, and stained with ethidiumbromide [35]. NIH Image software Version 1.52 (Wayne S. Rasband, NationalInstitutes of Health, Bethesda, MD) was used to capture and quantify thenumber of pixels of each band.
To identify IFN-g DNA, a 35S-labeled probe was prepared [35] from aplasmid (also supplied by Buffer Fennie at Genentech) that contained thecoding sequence for rabbit IFN-g. The known and unknown IFN-g DNAs wereelectrophoresed on agarose gels and blotted onto nylon membranes [35]. Theresulting blots clearly confirmed that IFN-g DNA was produced by the PCRamplification.
Acid fast stain for tubercle bacilli
The tubercle bacilli in the fixed-frozen tissue sections were stained with carbolfuchsin by the Ziehl-Neelsen method as described prevously [44]. Briefly, thesections were heated with carbol fuchsin at 70°C for 10 min, washed,decolorized with acid-alcohol for 20 s, and counterstained with acid methyleneblue.
Preparation of rabbit recombinant MCP-1 proteinand an antibody to it
The rabbit MCP-1 cDNA [40], without the sequence of its signal peptide, wasamplified (with the appropriate primers) by 10 PCR cycles (1) to obtain thecorrect reading frame, and (2) to incorporate the appropriate restriction enzymesites for subcloning into the expression vector, pMal-c, obtained from NewEngland Biolabs, Inc. (Beverly, MA). E. coli TB1 cells (transformed by the newrecombinant plasmid) were grown in 100 mL of Super medium (25 g tryptone,15 g yeast extract, 5 g NaCl per liter) at 37°C to OD600 5 0.400. The chemicalinducer IPTG was added until 0.3 mM was reached and the induced TB1 cellswere grown for an additional 2–3 h. The TB1 cells were then pelleted and lysedaccording to the instructions provided by the manufacturer (New EnglandBiolabs). The cell lysate was diluted, and the MCP-1 protein bound to its carrier(a maltose-binding protein) was purified by means of an amylose resin column.The purified carrier/MCP-1 complex was dialyzed and then cleaved by FactorXa at a concentration of 1 U per 200 µg protein for 6 h. The now freemaltose-binding carrier was removed by a second passage through an amyloseresin column. Guinea pigs were then immunized with the now isolated MCP-1protein in complete Freund’s adjuvant, and their serum (containing polyclonalantibodies to MCP-1) was used in a 1:200 dilution for the immunohistochemicalprocedures described below.
Immunohistochemical procedures
These procedures have been previously described in detail [4]. Briefly, theyemployed a primary antibody, a biotinylated secondary antibody to the IgG1fraction of the primary antibody, and a diaminobenzidine-peroxidase colorreaction produced with the ABC kit, i.e., the avidin-biotin-peroxidase complex(Vector Laboratories, Inc., Burlingame, CA).
Guinea-pig anti-rabbit MCP-1 was produced as described above. Goatanti-rabbit TNF-a polyclonal antibody (IgG fraction) was purchased fromPharMingen (San Diego, CA) and used at 5 µg protein/mL. The secondaryantibodies were biotinylated goat anti-guinea-pig IgG and biotinylated rabbitanti-goat IgG, respectively. Our controls had the primary antibodies replaced bywhole serum from normal guinea pigs for MCP-1, and IgG from normal goats forTNF-a. No colored reaction product was produced in these controls.
Monoclonal antibodies to the adhesion molecules ELAM-1, ICAM-1, andVCAM-1 were obtained, and the immunohistochemical reactions were per-formed in a similar manner [see ref. 4 for details]. Dr. Barry A. Wolitsky [45],Department of Inflammation/Autoimmune Diseases, Hoffmann-LaRoche, Inc.
(Nutley, NJ) supplied the primary antibody (IgG) to ELAM (mouse anti-rabbitE-selectin mAb14G2). It was used in 1:1000 dilution. Dr. Myron I. Cybulsky[46, 47], Brigham and Women’s Hospital, Harvard Medical School, Boston, MA(present address: Department of Pathology, The Toronto Hospital, University ofToronto, Ontario, Canada) supplied the primary antibodies to ICAM (Rb2/3)and VCAM (Rb1/9). Both were IgG1 immunoglobulins produced by an NS-1hybridoma in tissue culture medium RPMI 1640 containing 10% normal horseserum. They were used in 1:150 and 1:8 dilutions, respectively.
For quantitation, the total microvasculature in representative areas wasstained with a monoclonal antibody to Von Willebrand factor [4]. Then, with theprobe of an image analyzer, the stained areas were outlined (not including thevessel lumens). These stained areas were then summed to provide the total areaof microvasculature in square millimeters. A similar procedure was used forvessels stained for each adhesion molecule. The percentage of the totalmicrovasculature that was stained for each type of adhesion molecule was thenreadily calculated. Details of this process have been presented previously [4].
Glycol methacrylate (GMA) tissue sections
GMA-embedded tissue sections (cut at 1–2 µm) have a clarity and resolutionapproaching those seen with very low power electron microscopy. We used suchsections whenever accurate cell identification was required [48]. However, wecould not get satisfactory in situ hybridization of the rabbit cytokine mRNAs inpilot experiments with either GMA-embedded or paraffin-embedded tissuesections.
Counting 35S-labeled cells in tissue sectionsof BCG lesions
In Giemsa-stained fixed-frozen BCG tissue sections, labeled and unlabeled MN(mainly macrophages and lymphocytes, with some swollen fibroblasts) werecounted microscopically with a 340 objective lens and a 1.0-cm2 ocular grid.In sites that were densely infiltrated with MN, five representative grid areaswere selected, and the percentage of 35S-labeled MN in the total MN populationat the site was calculated. The number of labeled and unlabeled MN in thesedensely infiltrated areas ranged from 300 to 900 per grid area (16 grid areastotal 1.00 mm2). Tuberculosis is a locally controlled disease, i.e., the hostarrests the disease locally at the sites where bacilli are present [49]. Presentingour results as a percentage of MN labeled for cytokine mRNA (or for cytokineprotein) in the densely cell-infiltrated areas of the BCG lesions therefore seemsto be a most pertinent way to assess the in vivo contribution of the cytokinesevaluated.
For each cytokine, mononuclear cells were labeled only with the antisense35S-RNA probes and not with the sense 35S-RNA probes. The cells wereconsidered to be labeled when the number of silver grains was three or moretimes that of the background.
RESULTS and INTERPRETATIONS
Size and characteristics of the BCG lesions
The BCG lesions reached peak size in 2–3 weeks and werealmost healed at 5–7 weeks (Fig. 1A). Variations in size amongthe lesions were often due to the time of ulceration and thequantity of necrotic material discharged from the liquefiedcenters. The rabbits were slightly tuberculin-positive 9 daysafter the injection of BCG and strongly tuberculin-positive from14 days on (Fig. 1A).
At 3 and 5 days, the transsected lesions showed small foci ofnecrosis on gross examination. Between 9 and 23 days, most ofthese necrotic foci had fused to form a large central necroticfocus, which sooner or later liquefied and discharged some ofits contents by rupturing through the epidermis. At 37 days, thelesions were almost healed. The ulcer was usually epithelial-ized, little or no necrotic contents remained inside, and the cellinfiltrate was greatly reduced.
Sugisaki et al. Cytokines in tuberculous lesions 443

The lesions that had discharged most of their liquefiednecrotic contents seemed to heal the fastest. [We intentionallyselected such healing lesions for our 37-day evaluations.]
Histopathology
At 1 and 3 days, the BCG lesions showed scattered areas ofintact and fragmented leukocytes among the collagen fibers. At9, 23, and 37 days, few if any collagen fibers were present in thenecrotic areas and in the adjoining areas densely infiltratedwith cells. (Both granulocytes and macrophages contain collage-nases.) The peripheral areas of BCG lesions were not includedin our quantitative evaluations. Such peripheral areas con-tained more dispersed cells, as well as more collagen fibers,including newly formed collagen as the lesions healed.
The cell infiltrate was mainly composed of mononuclear cells(mostly macrophages and lymphocytes; Fig. 1B). These cellsrapidly infiltrated the areas containing the bacilli and remainedthroughout the healing process (Fig. 1B). PMN were present inthe initial infiltrate and near the caseous and liquefied areas ofthe older lesions. In 23-day lesions, epithelioid cells werecommon in the tuberculous granulation tissue surrounding thecaseous/liquefied center. (Epithelioid cells are macrophagesthat have ingested and digested tubercle bacilli [33].) Eosino-phils were rare, but plasma cells were common at 23 days. Theresemblance of dermal BCG lesions to lesions in the lungproduced by the inhalation of virulent bovine-type tuberclebacilli [31] was particularly striking, except that BCG lesionssoon healed, whereas virulent lesions often progressed. In eachcase, caseation, liquefaction, ulceration or cavity formation,and encapsulation by fibrous tissue occurred. The cell composi-tion of the lesions produced by virulent and attenuated bacilliwas nearly identical.
Number of bacilli
Acid-fast bacilli were always more numerous where there wasnecrosis. At 1 and 3 days, many bacilli were present in bothintact macrophages (and PMN) and in the necrotic cells (Fig.1C). At 5 and 9 days, the number of bacilli found in intact cellswas much reduced but many bacilli remained in the necroticfoci, which were fusing and liquefying (Fig. 1C and Fig. 2). At23 days, very few bacilli could be found in intact tissues, andthe number of bacilli in the caseous necrotic center was greatlyreduced (Fig. 1C).
Tuberculin reactions
The rabbits were tuberculin-negative at 3 days after infection,but at 9 days they were distinctly tuberculin-positive (Fig. 1A).At 14–23 days, tuberculin sensitivity reached a peak thatsubsequently was only slightly reduced as the BCG lesionshealed [34, 50]. The rabbits became skin-test-positive totuberculin and developed distinct liquefied/caseous centers atthe same time.
Cytokine mRNAs in BCG lesions: identifiedin mononuclear cells by in situ hybridizationThe biphasic pattern
In tissue sections of the BCG lesions, IL-1b, TNF-a, MCP-1,and IL-8 (NAP-1) mRNAs were visualized by in situ hybridiza-
tion with 35S-antisense RNA probes and autoradiography. Thepercentage of mononuclear cells labeled for these cytokinemRNAs showed a biphasic pattern as the lesions developed(Fig. 3); there was a large initial peak at 1–3 days, followed bya trough at 5 days, and then another rise (see Discussion). Theinitial pronounced up-regulation of MCP-1 mRNA suggeststhat this mononuclear-cell-attracting chemokine played animportant role in the initial mononuclear cell infiltration.
The distribution of labeled cells
At 3 days, all of the mononuclear cells labeled for four cytokinemRNAs were located in the exudate between the collagenfibers. However, from 5 days on, after distinct areas of necrosiswere clearly established, the mononuclear cells labeled foreach of the four cytokine mRNAs had their own distributionpatterns. (1) Cells containing IL-1b and IL-8 mRNAs werefound near the necrotic centers and sometimes even withinsuch centers (Fig. 4). Therefore, IL-1b and IL-8 were probablyinvolved in the recruitment of the PMN that accumulated nearthe caseous centers. (2) Mononuclear cells containing TNF-amRNAs were more widely distributed than those containingIL-1b and IL-8 mRNAs, and were most numerous among theinfiltrating cells of 3-day BCG. (3) The majority of the
Fig. 2. Liquefied caseous center of a 5-day dermal BCG lesion stained fortubercle bacilli. Many bacilli appear as clumps within macrophages. Otherbacilli are located extracellularly in the liquefied debris. All darkly stainedparticles are bacilli. Because this is necrotic material, the macrophages are notdistinctly recognizable in the photograph but their rounded outline and size(arrows) clearly identify their cell type. Fixed-frozen tissue section stained bycarbol fuchsin and counterstained with methylene blue. 31000.
444 Journal of Leukocyte Biology Volume 63, April 1998

mononuclear cells containing MCP-1 mRNA were found in theouter third of the areas densely infiltrated with cells. Theselabeled mononuclear cells were closely associated with themicrovasculature, a propitious location for cells producingchemoattractants. Cells containing MCP-1 mRNA were alsopresent more peripherally in the highly vascularized areaslocated between the hair follicles.
Cell types containing MCP-1, IL-1b, IL-8,and TNF-a mRNAs
In the BCG lesions, MCP-1 mRNA was frequently found inmononuclear cells, occasionally in vascular endothelial cells,but never in PMN. IL-1b and IL-8 mRNAs were found mainlyin mononuclear cells and occasionally in PMN. TNF-a mRNAwas found only in mononuclear cells.
In healing (37-day) lesions, large mononuclear cells wereoften labeled for MCP-1 mRNA, but the mature epithelioid
cells in such lesions were not labeled for MCP-1 mRNA, nor forIL-1b, TNF-a, and IL-8 mRNAs. The keratinocytes of theepidermis and hair follicles were occasionally labeled for IL-8mRNA but not for the other three cytokines.
Immunohistochemical studiesfor cytokine proteins
BCG lesions of various ages were stained by immunohistochemi-cal techniques for MCP-1 and TNF-a proteins (Table 1). Thepercentage of cells containing the proteins of these twocytokines was highest at 1, 3, and 5 days and reduced at 9 days.No decrease occurred in the percentage of mononuclear cellsstaining positively for these cytokine proteins at 5 days, eventhough the percentage of mononuclear cells containing themRNAs was decreased at this time (see Fig. 3). We have noconclusive explanation for the discrepancy between cytokinemRNAs and cytokine proteins at 5 days. Perhaps, once formed,
Fig. 3. These four graphs show the percentage of total mononuclear cells that were labeled for cytokine mRNA in BCG lesions at various times during theirdevelopment and regression. Note the biphasic pattern of the cytokine mRNAs. The means (with their standard errors) of (usually) five rabbits are shown. For moredetails, see Counting 35S-labeled cells in Materials and Methods. The P values between the peaks and the troughs are *P , 0.05, **P , 0.02, and *** P , 0.01.During healing, the P values between the second peak and the lowest (healing) point that followed it are for IL-1b, TNF-a, MCP-1, and IL-8: P , 0.02, P , 0.05,P , 0.06, and P , 0.02, respectively. All P values between the troughs and second peaks were , 0.12, which is suggestive but not statistically significant.
Sugisaki et al. Cytokines in tuberculous lesions 445

the cytokine proteins became attached to receptors on the MNthat they helped recruit. If so, then both donor and recipientcells would be labeled histochemically.
The cells stained for MCP-1 protein were mainly largemacrophages (Fig. 5), but some microvessel endothelial cellswere also stained at 23 and 37 days. MCP-1 protein wasdetected in more mononuclear cells than was TNF-a protein.Only macrophages were stained for TNF-a proteins.
In tissue sections of BCG lesions, the mononuclear cellsstaining positively for MCP-1 and TNF-a proteins showed thesame distribution pattern as the mononuclear cells containingMCP-1 and TNF-a mRNAs (see above), i.e., MCP-1 protein-containing MN were more frequent in the outer third of areas
densely infiltrated with cells. This finding further supports theconclusion that cells containing cytokine mRNA were activelyproducing cytokine protein.
Vascular ICAM-1, ELAM-1, and VCAM-1 in 3-dayBCG lesions
Vascular adhesion molecules (which enable the diapedesis ofleukocytes) are known to be up-regulated in all inflammatoryreactions [5, 6], including those produced in rabbits by BCG[4]. This up-regulation is triggered by the primary cytokinesIL-1b and TNF-a [1, 3, 51, 52], as well as the chemokines [9].Because the number of cells containing IL-1b, TNF-a, MCP-1,and IL-8 mRNAs was two to five times higher in 1- to 3-dayBCG lesions than in older BCG lesions (Fig. 3), we wonderedwhether the number of microvessels up-regulated for adhesionmolecules was also highest at this time.
To answer this question, we evaluated (by immunohistochemi-cal techniques) the vascular adhesion molecules, ICAM-1,ELAM-1, and VCAM-1 in 3-day BCG lesions, a time notreported in our previous communication on this subject [4]. Wefound that the microvasculature area immunostained for ICAM-1and VCAM-1 in 3-day BCG lesions averaged about 60%greater than the microvasculature area stained for ICAM-1 andVCAM-1 in 9-day lesions (Fig. 6). The microvascular areastained for ELAM-1, however, was not greater at 3 days than at9 days. The early up-regulation of cytokines and vascularadhesion molecules suggests that both were involved in theinitial emigration of large numbers of mononuclear cells fromthe bloodstream into the BCG lesions.
IFN-g mRNA in BCG lesions identified byRT-PCR (a semiquantitative technique)
In BCG lesions, the ratio of IFN-g mRNA to the housekeepingGAPDH mRNA was highest at 5 days, was decreased at 7 days,and was increased again at 9 days (Fig. 7). The 9-day level wasmaintained at 23 days when the BCG lesions were at theirmaximum size (Fig. 1A). Thus, similar to the mRNA levels ofthe four cytokines represented in Figure 3, the IFN-g mRNAsshowed a biphasic pattern. However, the time sequence of theIFN-g mRNAs shown in Figure 7 (obtained by RT-PCR of BCGlesion homogenates) cannot be compared to that in Figure 3(obtained by in situ hybridization of BCG tissue sections)because of the completely different methodologies used.
We were not able to detect sufficient RNA in normal skin todetermine the exact IFN-g/GAPDH mRNA ratios. Given thevery low or absent levels of the other four cytokines in normalskin (see Fig. 3), we assumed for Figure 7 that IFN-g mRNAwas also very low or absent.
DISCUSSION
Comparisons among the five cytokines evaluated
With in situ hybridization, the antisense RNA probes for onetype of cytokine do not necessarily hybridize with the sameaffinity as do antisense probes for another type of cytokine.Therefore, in Figure 3, the percentages of mononuclear cellscontaining IL-1b, TNF-a, MCP-1, and IL-8 mRNAs cannot be
Fig. 4. A 16-day dermal BCG lesion in situ hybridized for IL-8 mRNA. At theborder of the liquefied caseous center (lower part of photograph) is a group ofcells labeled for IL-8. They were identified as large macrophages by carefulfocusing of the microscope. One of the labeled cells is also present in theliquefied debris (upper part of photograph). Note the numerous PMN present.(The chemokine IL-8 is known to attract PMN.) Fixed-frozen tissue sectionhybridized with antisense IL-8 35S-RNA, autoradiographed and counterstainedwith Giemsa. 3480.
TABLE 1. Percentage of Mononuclear Cells Stained for MCP-1and TNF-a Proteins
Age of BCG lesions, days
1 3 5 9 23 37
MCP-1 protein 111 111 111 11 6 1TNF-a protein 1 11 11 6 2 2
Symbols: 2, 0–0.5%; 6, 0.5–1%; 1, 1–2%; 11, 2–5%, 111, .5%.
446 Journal of Leukocyte Biology Volume 63, April 1998

compared nor can they be compared with lesion IFN-g mRNAmeasured by RT-PCR.
We were, however, able to compare the changes in the mRNAlevels of each cytokine as the BCG lesions developed andhealed (Fig. 8). With all five cytokines, the highest levels ofmRNA seemed to occur early. Subsequently, the mRNAsdecreased, but during the immune phase the number of MNcontaining IFN-g and IL-8 mRNAs seemed to remain higher(relative to the early peak) than the number containing IL-1b,TNF-a, and MCP-1 mRNAs. The IFN-g of the immune phase(produced mainly by Th1 lymphocytes [11]) is known toenhance the microbicidal functions of macrophages [12–14].IL-8 is a major PMN chemoattractant and activator. PMN areknown to accumulate around areas of necrosis and in areas ofbacterial invasion [5]. The number of MN containing IL-8seemed to decrease at 37 days, when tissue necrosis was muchreduced and the ulcer was becoming epithelialized.
Total cytokine-producing MN
The question arises as to whether the changes in the percentageof MN labeled for cytokine mRNA reflect the total number ofsuch cytokine-producing MN in the BCG lesions. This questionreally has two parts. The first is the total number of cytokine-
Fig. 6. Percent of microvasculature in BCG lesions stained immunohistochemi-cally for the adhesion molecules, ICAM-1, ELAM-1, and VCAM-1. Note thatICAM and VCAM peaked early, suggesting that these adhesion moleculesenabled the initial cell infiltration. Means (and their standard errors) from fiverabbits are shown: *P , 0.05; **P , 0.02; ***P , 0.01 between points. (SeeMaterials and Methods.)
Fig. 5. (A) An unfixed-frozen tissue section of a 3-day dermal BCG lesion stained immunohistochemically for MCP-1 protein. In the partly necrotic exudatebetween the remaining collagen fibers are large positively stained mononuclear cells. (MCP-1 protein was not easily demonstrated in later lesions that containedreduced levels of MCP-1 mRNA.) Anti-rabbit MCP-1 polyclonal antibody, biotinylated anti-guinea pig IgG, and the Vector avidin-biotin-peroxidase procedure,counterstained with Giemsa is shown. 3250. (B) A 3-day dermal BCG lesion embedded in glycol methacrylate and stained with Giemsa. This photograph shows someof the histological detail that is absent in frozen sections. In the center and upper half are large MN similar to those stained histochemically in panel A. (Thedifferences in size between the large MN in panels A and B are probably due to local diffusion of the MCP-1 protein.) In the lower half are PMN, which are common in3-day BCG lesions. 3560.
Sugisaki et al. Cytokines in tuberculous lesions 447

producing cells in the entire lesion, which is roughly propor-tional to the lesion size. The lesions markedly increase in sizefor 14 days, and after 23 days they decrease in size as they heal(Fig. 1A). Because these changes in lesion size are so great,they reflect both the total number of MN and the total number ofMN labeled for cytokines.
The second part of the question is the total number ofcytokine-producing cells in the dense areas of the lesions. Thecontrol of tuberculous lesions is local, in fact microlocal [53]. Inother words, the tubercle bacillus is destroyed (or inhibited) inareas where it resides in the tissues, and cytokines only activatemacrophages in these areas [53], which are the dense areas thatwe counted in tissue sections of the lesions. The total numbersof unlabeled and labeled MN per square millimeter in suchareas can be derived from Figures 1B and 3, respectively. Thetotal number of MN containing IL-1b, TNF-a, and MCP-1mRNA showed a pattern similar to the percentage of these cellsrepresented in Figure 3. The total MN containing IL-8 mRNAlikewise showed a similar pattern, but with IL-8 the totalnumber of these cells at 23 days approached that in the 3-daypeak, probably because the extensive necrosis at 23 days is astimulus for IL-8 production.
Although Figure 1B does not show data at 5 days, there is noreason to believe that the number of MN in the dense areasdecreased between 3 and 9 days. In fact, our impression (fromstudying the tissue sections) is that the dense areas becamemore compact as the edema at 1 and 3 days subsided. Figure1A gives the volume of the BCG lesions in cubic millimeters.This volume reflects both the edema (in the first 3 days) and thecell infiltration. It confirms that there was less edema at 5 daysbecause the size of the lesion actually declined at 5 days.
A continuous infiltration of new cells occurred as the BCGlesions grew to peak size at 14 days (Fig. 1A). The decline inpercentage of MN labeled for cytokine mRNA at 5 days is
Fig. 7. Changes in IFN-g mRNA in rabbit BCG lesions, relative to those ofglyceraldehyde-3-phosphate dehydrogenase (GAPDH) mRNA (see text).GAPDH mRNA level per cell is known to remain rather constant without widefluctuations, as cells up- and down-regulate their various activities. The means(and their standard errors) from three rabbits are shown. ***P , 0.01 by thepaired t test.
Fig. 8. A diagrammaticsummary of our findings.IFN-g mRNA up-regula-tion lagged behind theup-regulation of the otherfour cytokine mRNAs.IFN-g peaked at 5 days,had a trough at 7 days,and remained at two-thirds peak levels at 9and 23 days when localacquired cell-mediatedimmunity developed andthen peaked.
448 Journal of Leukocyte Biology Volume 63, April 1998

readily explained by the infiltration of unlabeled MN. After thisdecline, the percentage of labeled MN was maintained, presum-ably by the developing immune response. Between 5 and 14days the size of the BCG lesions was increasing rapidly becauseof cell infiltration (without edema; Fig. 1A). This rapid growthshows that new MN were continuously recruited into the site.The percentage of MN containing cytokine mRNA changedrelatively little between 9 and 23 days (Fig. 3). Therefore, eithermany newly recruited MN up-regulated their cytokine mRNAsor the cytokine-producing MN already in the lesions dividedand their progeny retained their cytokine mRNAs.
In short, the most pronounced cytokine production (per mm2)in the dense areas of BCG lesions was early and nonspecific.Then, as cell-mediated immunity developed and becameestablished, local cytokine production seemed to be maintainedat rather constant (but lower) levels. The volume of each entireBCG lesion increased between 5 and 14 days due to cellinfiltration, and this volume decreased between 23 and 37 daysdue to the healing process (see Fig. 1A). Therefore the totalnumber of cytokine-producing cells in intact BCG lesions wasincreasing and decreasing at these respective times.
Implications
The intradermal injection of BCG apparently initiates an earlypronounced nonspecific cytokine response both in the residentcells and in the mononuclear cells that soon infiltrate the sitebecause their IL-1b, TNF-a, MCP-1, and IL-8 mRNAs wereup-regulated at 3 days. These cytokines, and the accompanyingup-regulation of vascular adhesion molecules, probably playedimportant roles in the accumulation of macrophages andlymphocytes at the local site of infection. A similar nonspecificresponse would probably occur in the draining lymph nodes.
Lurie showed that acquired resistance to tuberculosis wassuperimposed on, and determined by, the native (genetic)resistance of his inbred rabbit strains [33, 50, 54]. The earlytuberculous lesions (and probably their draining lymph nodes)of Lurie’s resistant rabbits contained greater numbers ofmononuclear cells than did lesions of his susceptible rabbits.Such large numbers of local lymphocytes and macrophagescontributed to the high levels of acquired immunity to tubercu-losis that his resistant rabbits developed. By analogy, a vaccinethat recruited a large number of macrophages, lymphocytes,and dendritic cells into local sites where the antigens aredeposited would be a more effective immunological stimulusthan a vaccine that recruited a small number of these cells.
Therefore, the most effective tuberculosis vaccines would notonly contain the most appropriate mycobacterial antigens butalso contain mycobacterial adjuvants that recruit the largestnumber of infiltrating cells. Both properties should be consid-ered in developing better vaccines for tuberculosis than ourcurrently available strains of BCG.
ACKNOWLEDGMENTS
This work was supported primarily by grants AI-27165 andAI-35195 from the National Institute of Allergy and InfectiousDiseases; and partly by grants ES-03819 for the Johns Hopkins
Environmental Health Sciences Center from the NationalInstitute of Environmental Health Sciences, Research TrianglePark, North Carolina, and HL-10342 from the National Heart,Lung and Blood Institute.
We appreciate the technical assistance of Rena Ashworthand Lita P. Fay during various parts of these studies, and theeditorial assistance of Ilse M. Harrop. Timothy H. Phelps, of theJohns Hopkins Department of Art as Applied to Medicine drewFigure 8.
In conducting research using animals, the investigatorsadhere to the Guide for the Care and Use of Laboratory Animals,prepared by the Committee on Care and Use of LaboratoryAnimals of the Institute of Laboratory Animal Resources,National Research Council (NIH Publication No. 86-23, Re-vised 1985).
REFERENCES
1. Kupper, T. S. (1990) Immune and inflammatory processes in cutaneoustissues: Mechanisms and speculations. J. Clin. Invest. 86, 1783–1789.
2. Luger, T. A., Schwarz, T. (1995) The role of cytokines and neuroendocrinehormones in cutaneous immunity and inflammation. Allergy 50, 292–302.
3. Tsuruta, J., Sugisaki, K., Dannenberg, A. M., Jr., Yoshimura, T., Abe, Y.,Mounts, P. (1996) The cytokines NAP-1 (IL-8), MCP-1, IL-1b and GRO inrabbit inflammatory skin lesions produced by the chemical irritant sulfurmustard. Inflammation 20, 293–318.
4. Abe, Y., Sugisaki, K., Dannenberg, A. M., Jr. (1996) Rabbit vascularendothelial adhesion molecules: ELAM-1 is most elevated in acuteinflammation, whereas VCAM-1 and ICAM-1 predominate in chronicinflammation. J. Leukoc. Biol. 60, 692–703.
5. Majno, G., Joris, I. (1996) The leukocyte’s call to action: Five steps tophagocytosis. In Cells, Tissues, and Disease: Principles of General Pathol-ogy. Cambridge, MA: Blackwell Scientific, 385–413.
6. Norris, P., Poston, R. N., Thomas, D. S., Thornhill, M., Hawk, J., Haskard,D. O. (1991) The expression of endothelial leukocyte adhesion molecule-1(ELAM-1), intercellular adhesion molecule-1 (ICAM-1), and vascular celladhesion molecule-1 (VCAM-1) in experimental cutaneous inflammation:A comparison of ultraviolet B erythema and delayed hypersensitivity. J.Invest. Dermatol. 96, 763–770.
7. Bacon, K. B., Schall, T. J. (1996) Chemokines as mediators of allergicinflammation. Int. Arch. Allergy Immunol. 109, 97–109.
8. Carr, M. W., Roth, S. J., Luther, E., Rose, S. S., Springer, T. A. (1994)Monocyte chemoattractant protein 1 acts as a T-lymphocyte chemoat-tractant. Proc. Natl. Acad. Sci. USA 91, 3652–3656.
9. Zack, O. M., Ben-Baruch, A., Oppenheim, J. J. (1996) Chemokines:Progress toward identifying molecular targets for therapeutic agents. TrendsBiotech. 14, 46–51.
10. Scott, P., Trinchieri, G. (1995) The role of natural killer cells inhost-parasite interactions. Curr. Op. Immunol. 7, 34–40.
11. Mosmann, T. R., Sad, S. (1996) The expanding universe of T-cell subsets:Th1, Th2 and more. Immunol. Today 17, 138–146.
12. Flynn, J. L., Chan, J., Triebold, K. J., Dalton, D. K., Stewart, T. A., Bloom,B. R. (1993) An essential role for interferon-g in resistance to Mycobacte-rium tuberculosis infection. J. Exp. Med. 178, 2249–2254.
13. Murray, H. W. (1988) Interferon-gamma, the activated macrophage, andhost defense against microbial challenge. Ann. Int. Med. 108, 595–608.
14. Orme, I. M., Miller, E. S., Roberts, A. D., Furney, S. K., Griffin, J. P.,Dobos, K. M., Chi, D., Rivoire, B., Brennan, P. J. (1992) T lymphocytesmediating protection and cellular cytolysis during the course of Mycobacte-rium tuberculosis infection. Evidence for different kinetics and recognitionof a wide spectrum of protein antigens. J. Immunol. 148, 189–196.
15. Barnes, P. F., Modlin, R. L. (1996) Human cellular immune responses toMycobacterium tuberculosis. In Tuberculosis (T. M. Shinnick, ed.) Berlin:Springer, 197–219.
16. Barnes, P. F., Modlin, R. L., Ellner, J. J. (1994) T-cell responses andcytokines. In Tuberculosis: Pathogenesis, Protection and Control (B. R.Bloom, ed.) Washington, DC: The American Society for Microbiology,417–435.
17. Wallis, R. S., Ellner, J. J. (1994) Cytokines and tuberculosis. (A review) J.Leukoc. Biol. 55, 676–681.
Sugisaki et al. Cytokines in tuberculous lesions 449

18. Barnes, P. F., Fong, S-J., Brennan, P. J., Twomey, P. E., Mazumder, A.,Modlin, R. L. (1990) Local production of tumor necrosis factor and IFN-gin tuberculous pleuritis. J. Immunol. 145, 149–154.
19. Barnes, P. F., Lu, S., Abrams, J. S., Wang, E., Yamamura, M., Modlin, R. L.(1993) Cytokine production at the site of disease in human tuberculosis.Infect. Immun. 61, 3482–3489.
20. Zhang, M., Gately, M. K., Wang, E., Gong, J., Wolf, S. F., Lu, S., Modlin,R. L., Barnes, P. F. (1994) Interleukin-12 at the site of disease intuberculosis. J. Clin. Invest. 93, 1733–1739.
21. Chensue, S. W., Warmington, K. S., Berger, A. E., Tracey, D. E. (1992)Immunohistochemical demonstration of interleukin-1 receptor antagonistprotein and interleukin-1 in human lymphoid tissue and granulomas. Am.J. Pathol. 140, 269–275.
22. Toossi, Z., Gogate, P., Shiratsuchi, H., Young, T., Ellner, J. J. (1995)Enhanced production of TGF-b by blood monocytes from patients withactive tuberculosis and presence of TGF-b in tuberculous granulomatouslung lesions. J. Immunol. 154, 465–473.
23. Schauf, V., Rom, W. N., Smith, K. A., Sampaio, E. P., Meyn, P. A.,Tramontana, J. M., Cohn, Z. A., Kaplan, G. (1993) Cytokine gene activationand modified responsiveness to interleukin-2 in the blood of tuberculosispatients. J. Infect. Dis. 168, 1056–1059.
24. Zhang, M., Lin, Y., Iyer, D. V., Gong, J., Abrams, J. S., Barnes, P. F. (1995)T-cell cytokine responses in human infection with Mycobacterium tubercu-losis. Infect. Immun. 63, 3231–3234.
25. Ellner, J. J. (1997) Regulation of the human immune response duringtuberculosis. J. Lab. Clin. Med. 130, 469–475.
26. Orme, I. M. (1996) Immune responses in animal models. In Tuberculosis(T. M. Shinnick, ed.) Berlin: Springer, 181–196.
27. Orme, I. M., Collins, F. M. (1994) Mouse model of tuberculosis. InTuberculosis: Pathogenesis, Protection and Control (B. R. Bloom, ed.)Washington, DC: The American Society for Microbiology, 113–134.
28. Rhoades, E. R., Cooper, A. M., Orme, I. M. (1995) Chemokine response inmice infected with Mycobacterium tuberculosis. Infect. Immun. 63, 3871–3877.
29. Cooper, A. M., Roberts, A. D., Rhoades, E. R., Callahan, J. E., Getzy,D. M., Orme, I. M. (1995) The role of interleukin-12 in acquired immunityto Mycobacterium tuberculosis infection. Immunol. 84, 423–432.
30. Appelberg, R., Castro, A. G., Pedrosa, J., Silva, R. A., Orme, I. M.,Minoprio, P. (1994) Role of gamma interferon and tumor necrosis factoralpha during T-cell-independent and -dependent phases of Mycobacteriumavium infection. Infect. Immun. 62, 3962–3971.
31. Converse, P. J., Dannenberg, A. M., Jr., Estep, J. E., Sugisaki, K., Abe, Y.,Schofield, B. H., Pitt, M. L. M. (1996) Cavitary tuberculosis produced inrabbits by aerosolized virulent tubercle bacilli. Infect. Immun. 64,4776–4787.
32. Dannenberg, A. M., Jr., Rook, G. A. W. (1994) Pathogenesis of pulmonarytuberculosis: an interplay of tissue-damaging and macrophage-activatingimmune responses—dual mechanisms that control bacillary multiplica-tion. In Tuberculosis: Pathogenesis, Protection and Control (B. R. Bloom,ed.) Washington, DC: The American Society for Microbiology, 459–483.
33. Lurie, M. B. (1964) Resistance to Tuberculosis: Experimental Studies inNative and Acquired Defense Mechanisms. Cambridge, MA: HarvardUniversity Press.
34. Dannenberg, A. M., Jr., Ando, M., Shima, K. (1972) Macrophage accumu-lation, division, maturation, and digestive and microbicidal capacities intuberculous lesions. III. The turnover of macrophages and its relation totheir activation and antimicrobial immunity in primary BCG lesions andthose of reinfection. J. Immunol. 109, 1109–1121.
35. Sambrook, J., Fritsch, E. F., Maniatis, T. (1989) Molecular Cloning: ALaboratory Manual, 2nd ed. Cold Spring Harbor, NY: Cold Spring HarborLaboratory.
36. Gillitzer, R., Berger, R., Mielke, V., Muller, C., Wolff, K., Stingl, G. (1991)Upper keratinocytes of psoriatic skin lesions express high levels ofNAP-1/IL-8 mRNA in situ. J. Invest. Dermatol. 97, 73–79.
37. Gillitzer, R., Wolff, K., Tong, D., Muller, C., Yoshimura, T., Hartmann,A. A., Stingl, G., Berger, R. (1993) MCP-1 mRNA expression in basalkeratinocytes of psoriatic lesions. J. Invest. Dermatol. 101, 127–131.
38. Matsukawa, A., Ohkawara, S., Maeda, T., Takagi, K., Yoshinaga, M. (1993)Production of IL-1 and IL-1 receptor antagonist and the pathologicalsignificance of lipopolysaccharide-induced arthritis in rabbits. Clin. Exp.Immunol. 93, 206–211.
39. Mori, S., Goto, F., Goto, K., Ohkawara, S., Maeda, S., Shimada, K.,Yoshinaga, M. (1988) Cloning and sequence analysis of a cDNA forlymphocyte proliferation potentiating factor of rabbit polymorphonuclearleukocytes: Identification as rabbit interleukin 1 (beta). Biochem. Biophys.Res. Commun. 150, 1237–1243.
40. Yoshimura, T., Yuhki, N. (1991) Neutrophil attractant/activation protein-1and monocyte chemoattractant protein-1 in rabbit: cDNA cloning and theirexpression in spleen cells. J. Immunol. 146, 3483–3488.
41. Ito, H., Shirai, T., Yamamoto, S., Akira, M., Kawahara, S., Todd, C. W.,Wallace, R. B. (1986) Molecular cloning of the gene encoding rabbit tumornecrosis factor. DNA 5, 157–165.
42. Ito, H., Yamamoto, S., Kuroda, S., Sakamoto, H., Kajihara, J., Kiyota, T.,Hayashi, H., Kato, M., Seko, M. (1986) Molecular cloning and expressionin Escherichia coli of the cDNA coding for rabbit tumor necrosis factor.DNA 5, 149–156.
43. Wesselingh, S. L., Levine, B., Fox, R. J., Choi, S., Griffin, D. E. (1994)Intracerebral cytokine mRNA expression during fatal and nonfatal alphavi-rus encephalitis suggests a predominant type-2 T cell response. J.Immunol. 152, 1289–1297.
44. Bartholomew, J. W. (1981) Stains for microorganisms in sections. InStaining Procedures, 4th ed. (G. Clark, ed.) Baltimore, MD: Williams &Wilkins, 441–473.
45. Olofsson, A. M., Arfors, K-E, Ramezani, L., Wolitzky, B. A., Butcher, E. C.,Von Andrian, U. H. (1994) E-selectin mediates leukocyte rolling ininterleukin-1-treated rabbit mesentery venules. Blood 84, 2749–2758.
46. Cybulsky, M. I., Gimbrone, M. A., Jr. (1991) Endothelial expression of amononuclear leukocyte adhesion molecule during atherogenesis. Science251, 788–791.
47. Richardson, M., Hadcock, S. J., DeReske, M., Cybulsky, M. I. (1994)Increased expression in vivo of VCAM-1 and E-selectin by the aorticendothelium of normolipemic and hyperlipemic diabetic rabbits. Arterio-scler. Thromb. 14, 760–769.
48. Vogt, R. F., Jr., Hynes, N. A., Dannenberg, A. M., Jr., Castracane, S., Weiss,L. (1983) Improved techniques using Giemsa-stained glycol methacrylatetissue sections to quantitate basophils and other leukocytes in inflamma-tory skin lesions. Stain Technol. 58, 193–205.
49. Dannenberg, A. M., Jr. (1968) Cellular hypersensitivity and cellularimmunity in the pathogenesis of tuberculosis: Specificity, systemic andlocal nature, and associated macrophage enzymes. Bacteriol. Rev. 32,85–102.
50. Lurie, M. B., Zappasodi, P., Cardona-Lynch, E., Dannenberg, A. M., Jr.(1952) The response to the intracutaneous inoculation of BCG as an indexof native resistance to tuberculosis. J. Immunol. 68, 369–387.
51. Bevilacqua, M. P., Nelson, R. M. (1993) Selectins. J. Clin. Invest. 91,379–387.
52. McEver, R. P. (1994) Selectins. Curr. Op. Immunol. 6, 75–84.53. Suga, M., Dannenberg, A. M., Jr., Higuchi, S. (1980) Macrophage
functional heterogeneity in vivo: Macrolocal and microlocal macrophageactivation, identified by double-staining tissue sections of BCG granulo-mas for pairs of enzymes. Am. J. Pathol. 99, 305–324.
54. Lurie, M. B., Zappasodi, P., Tickner, C. (1955) On the nature of geneticresistance to tuberculosis in the light of the host-parasite relationships innatively resistant and susceptible rabbits. Am. Rev. Tuberc. Pulm. Dis. 72,297–329.
450 Journal of Leukocyte Biology Volume 63, April 1998