Pediatric Musculoskeletal Infections - PedRad.org
93
Pediatric Musculoskeletal Infections Tal Laor, M.D. Cincinnati Children’s Hospital Medical Center University of Cincinnati College of Medicine SPR Pediatric MSK Imaging Austin, TX- Jan 2016 http://theodysseyonline.com/
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Pediatric Musculoskeletal Infections - PedRad.org

Pediatric Musculoskeletal Infections
Tal Laor, M.D.
Cincinnati Children’s Hospital Medical Center
University of Cincinnati College of Medicine
SPR Pediatric MSK Imaging Austin, TX- Jan 2016
http://theodysseyonline.com/
Osteomyelitis Initial Focus
• Usually hematogenous source – All age groups: S. aureus
•Panton-Valentine leukocidin (PVL genes)
– <4 mo: also enterobacter, grp A & B strep
– >4 mo - 4 years: Kingella kingae, H. flu
– Sickle cell: also Salmonella
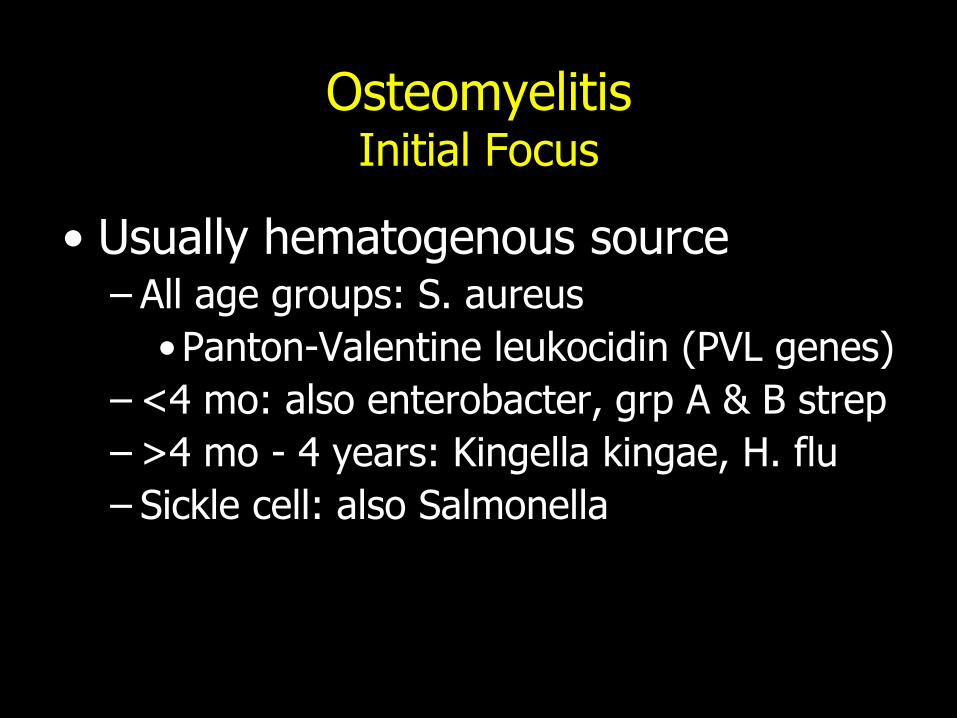
Metaphysis
• Increased vascularity
– Gd and 99mTc-MDP uptake
Subtracted image (+Gd)
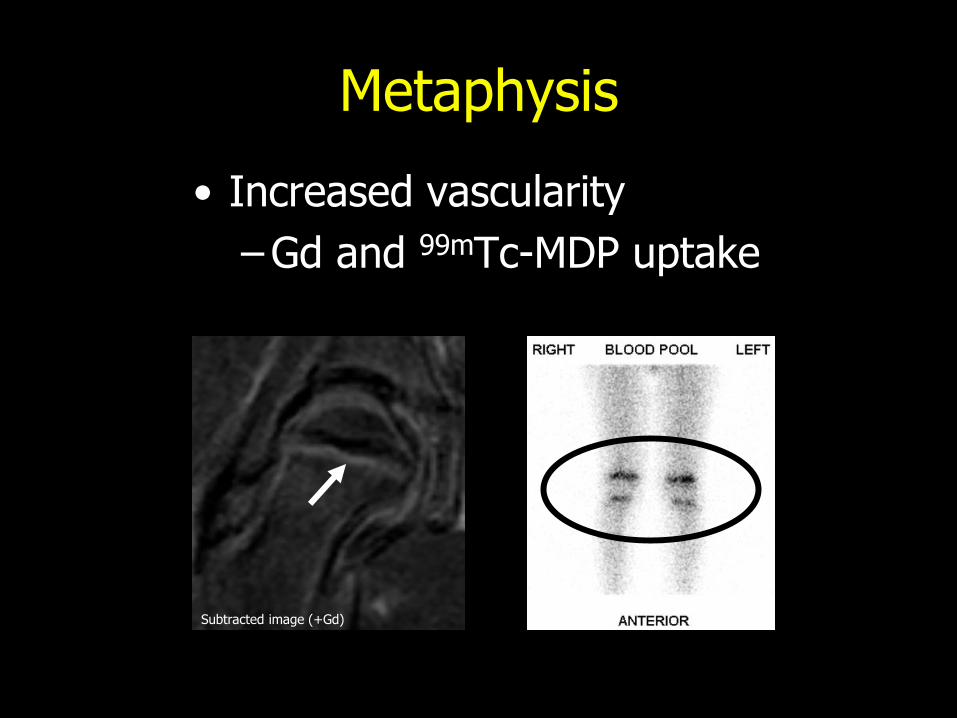
• Sluggish flow
• Decreased phagocytosis
* *
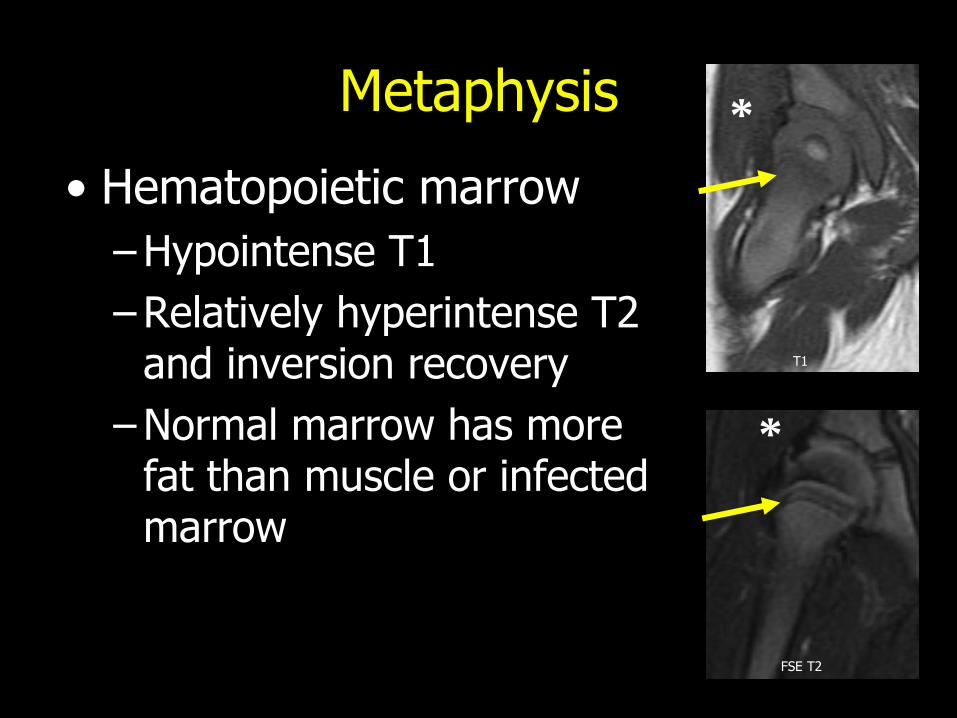
Metaphysis
• Hematopoietic marrow
– Hypointense T1
– Relatively hyperintense T2 and inversion recovery
– Normal marrow has more fat than muscle or infected marrow
T1
FSE T2
*
*

“Metaphyseal Equivalents”
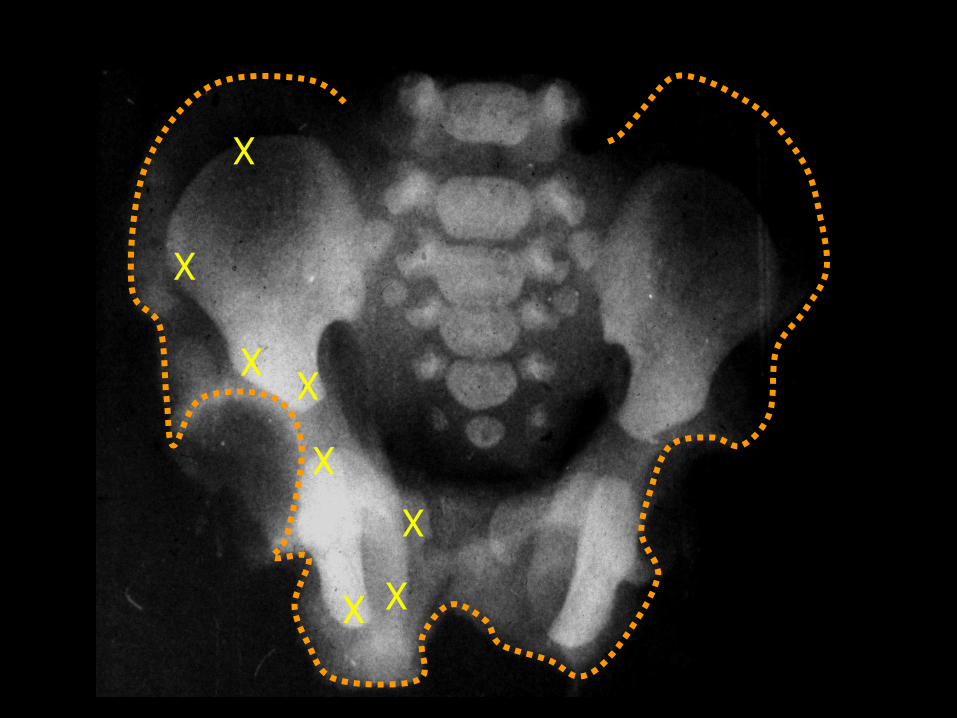
X
X
X
X
X
X
X
X

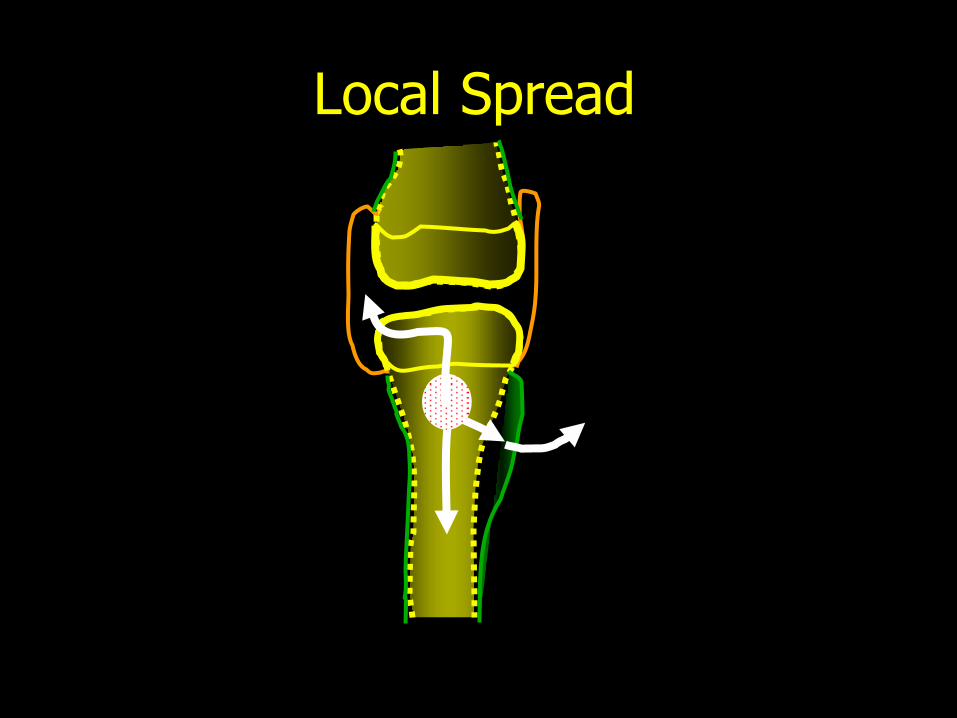
Medullary extension
Subperiosteal and soft tissue extension
Epiphyseal and articular extension
Local Spread
Local Spread
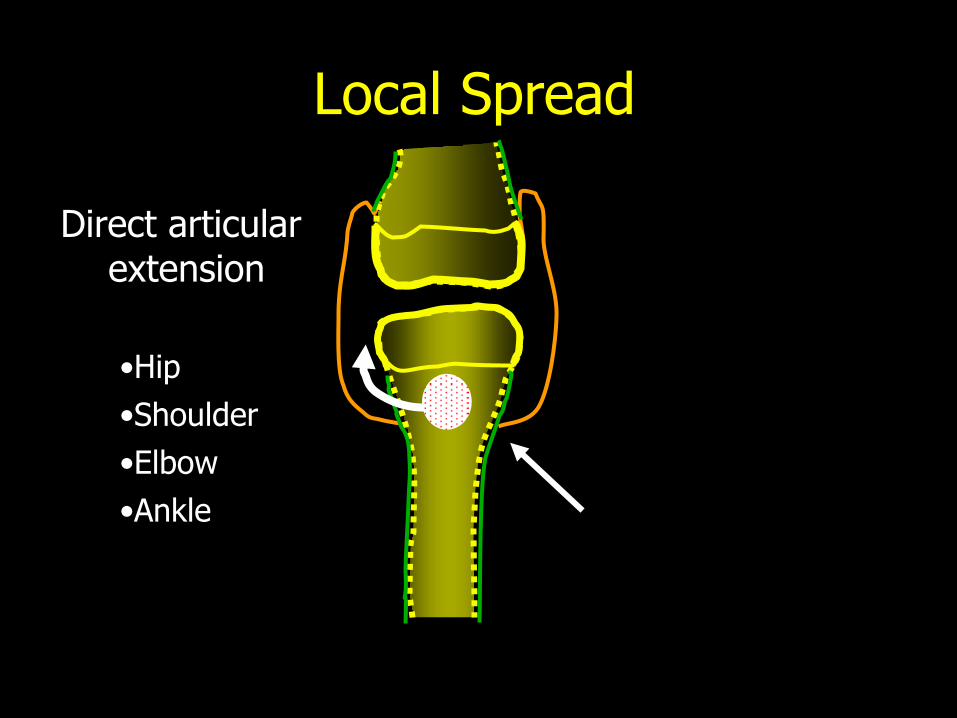
Direct articular
extension
Local Spread
•Hip
•Shoulder
•Elbow
•Ankle

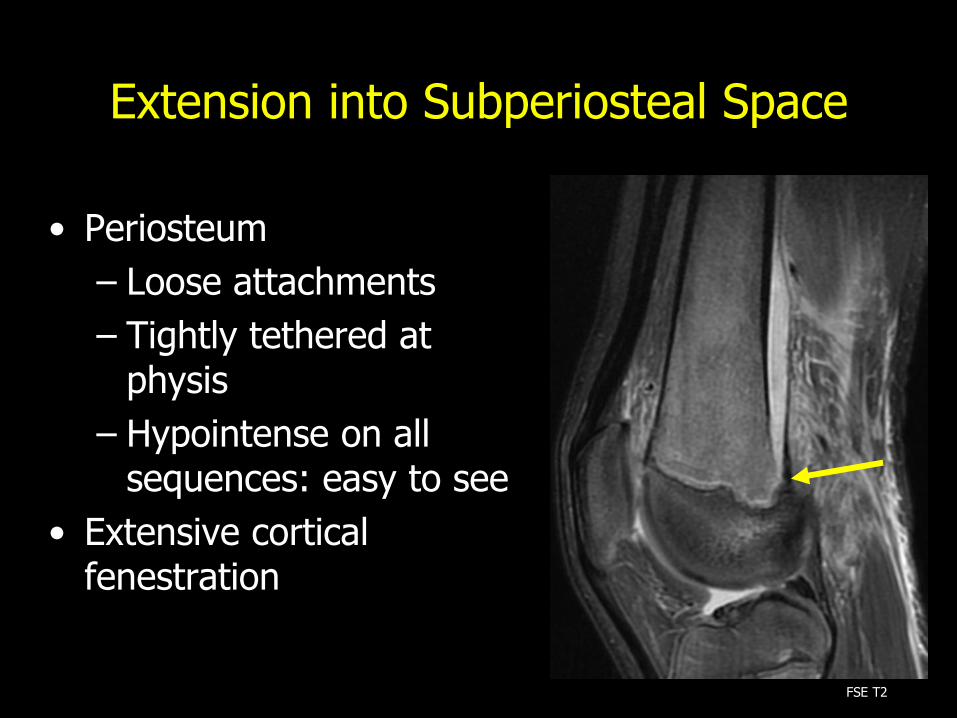
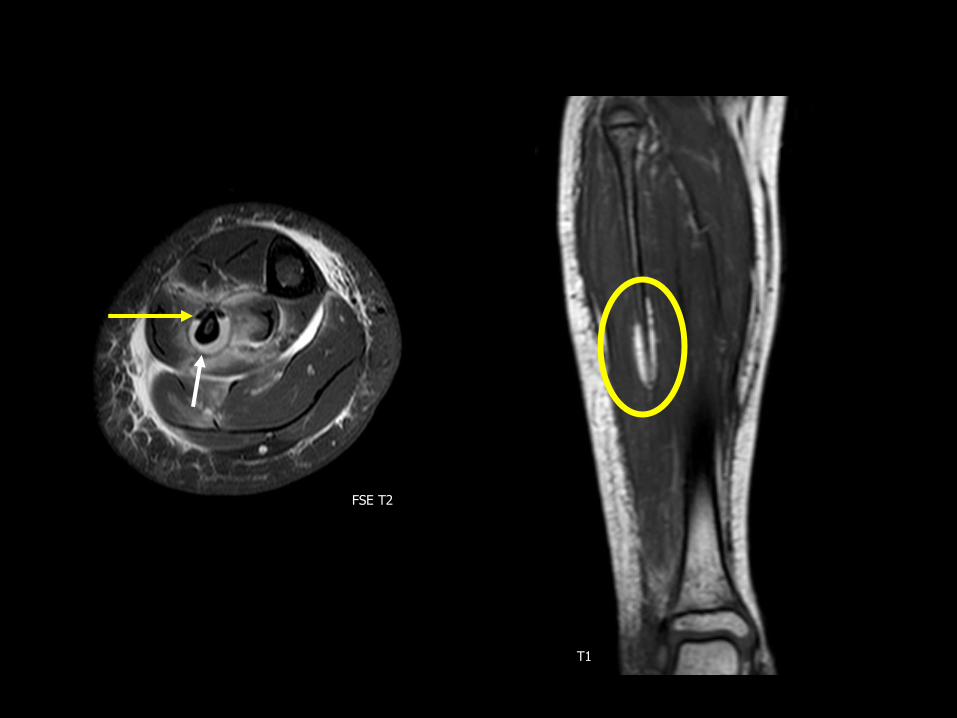
Extension into Subperiosteal Space
• Periosteum
– Loose attachments
– Tightly tethered at physis
– Hypointense on all sequences: easy to see
• Extensive cortical fenestration
FSE T2
• Periosteum
– Loose attachments
– Tightly tethered at physis
– Hypointense on all sequences: easy to see
• Extensive cortical fenestration
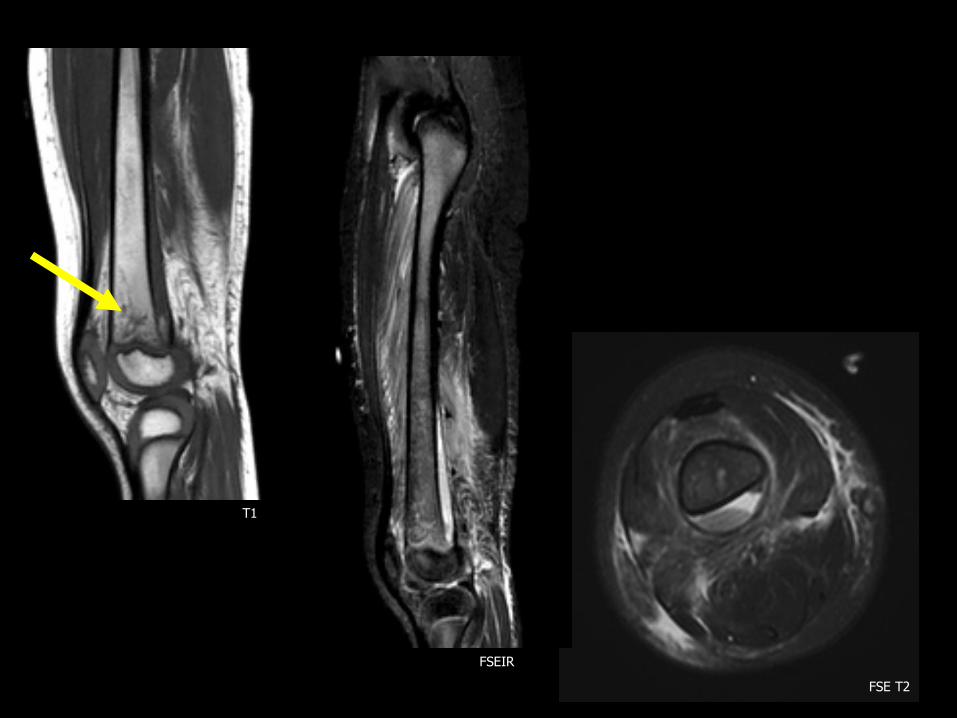
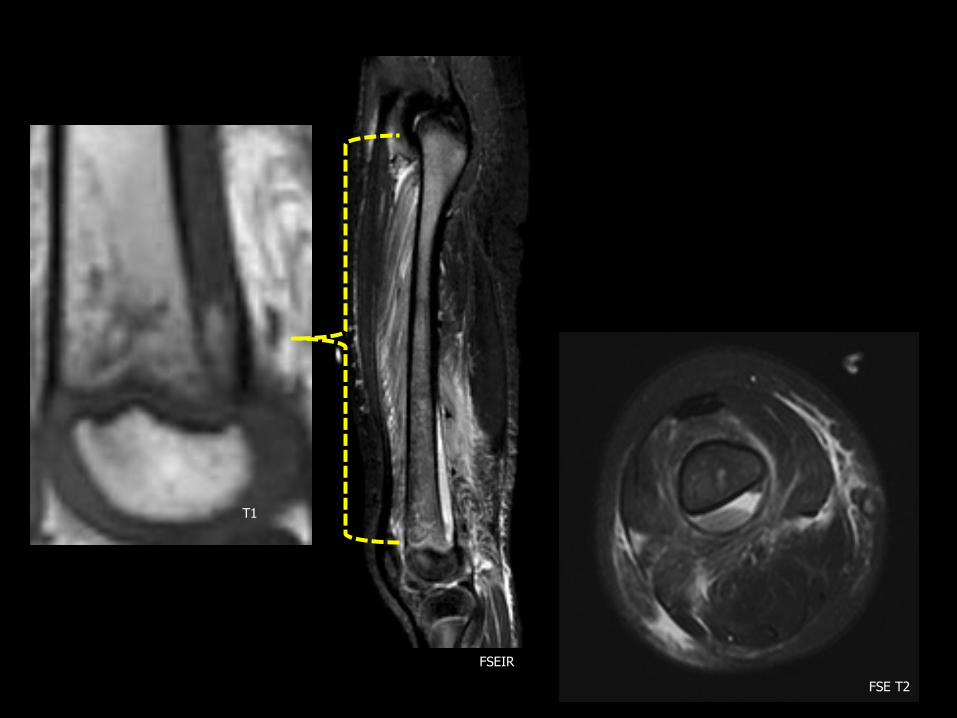
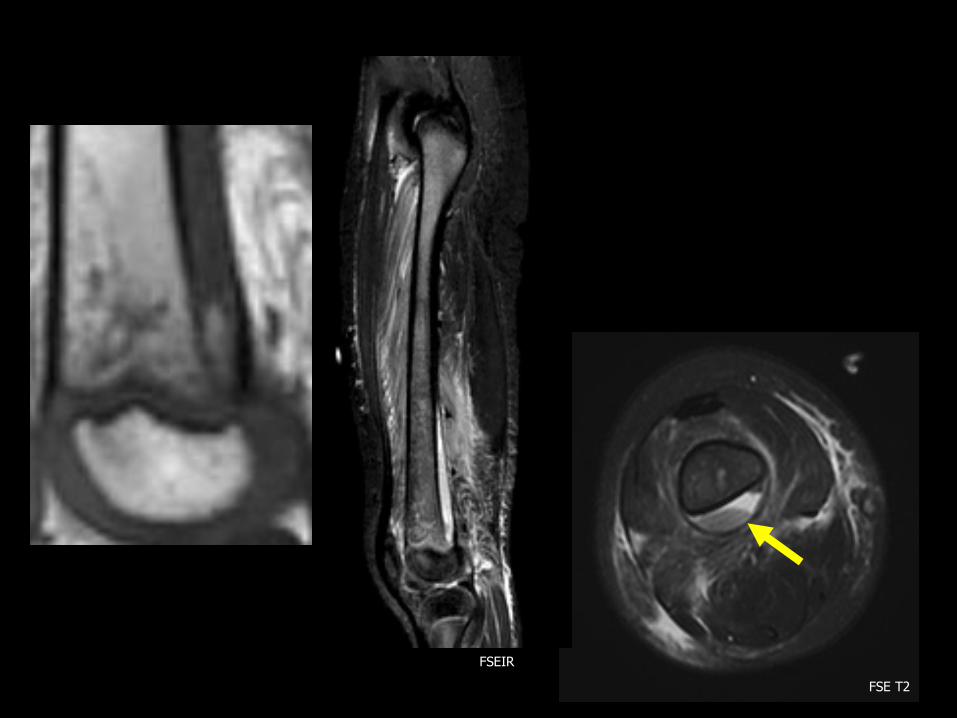
Extension into Subperiosteal Space
FSE T2

medullary space
periosteum
cortex

2-year old 15-year old
T1 + Gd T1 + Gd

FSE T2


T1 + Gd
FSE T2
T1
FSEIR

FSE T2
T1
FSEIR

FSE T2
T1
FSEIR

FSE T2
T1
FSEIR
FSE T2
T1
FSEIR
FSE T2
T1
FSEIR

Persistent Fat Signal
• In bone, subperiosteal space
• Increased intramedullary pressure leads to septic necrosis, lipocyte death, release of free fatty globules
• Acellular marrow spaces
T1
Davies AM, Eur Radiol (2005). 15:2194
FSE T2
T1

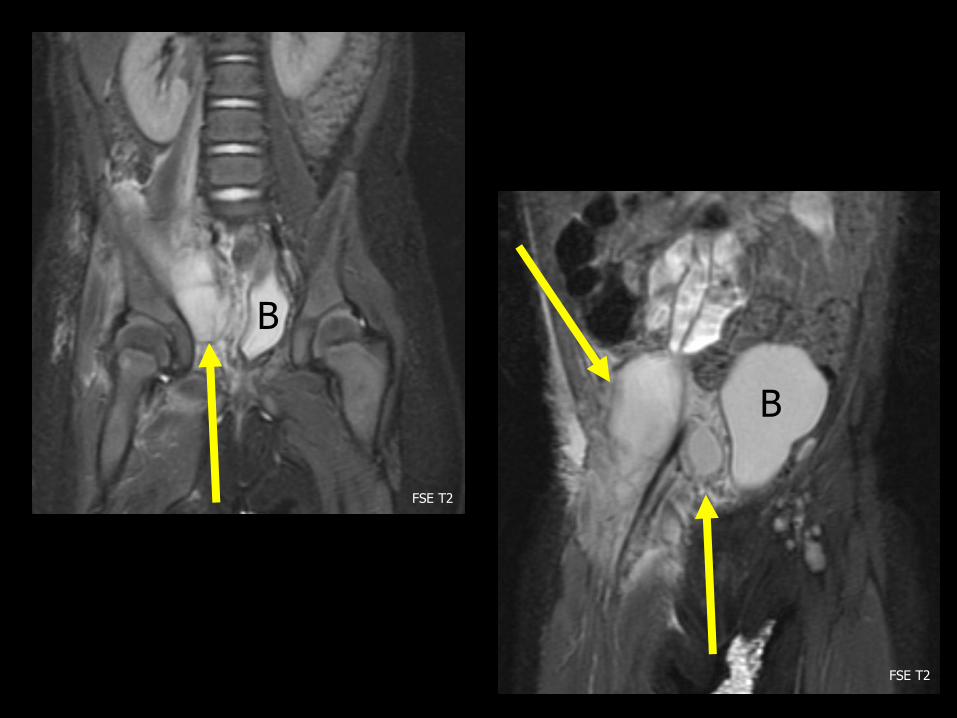
Extension into the Soft Tissues
• In > 50% of osteomyelitis
• Particularly common in the pelvis
T1 + Gd
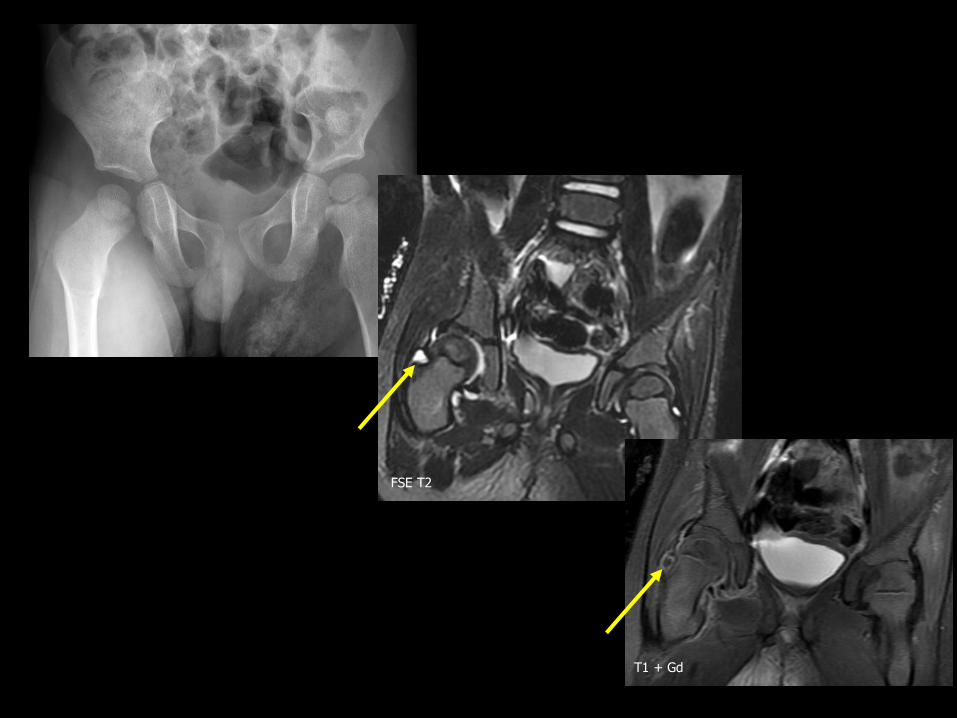
Pelvic Osteomyelitis
• Metaphyseal equivalents in >90%
• Soft tissue abnormalities in 80%
• Variable presentation depends on spread
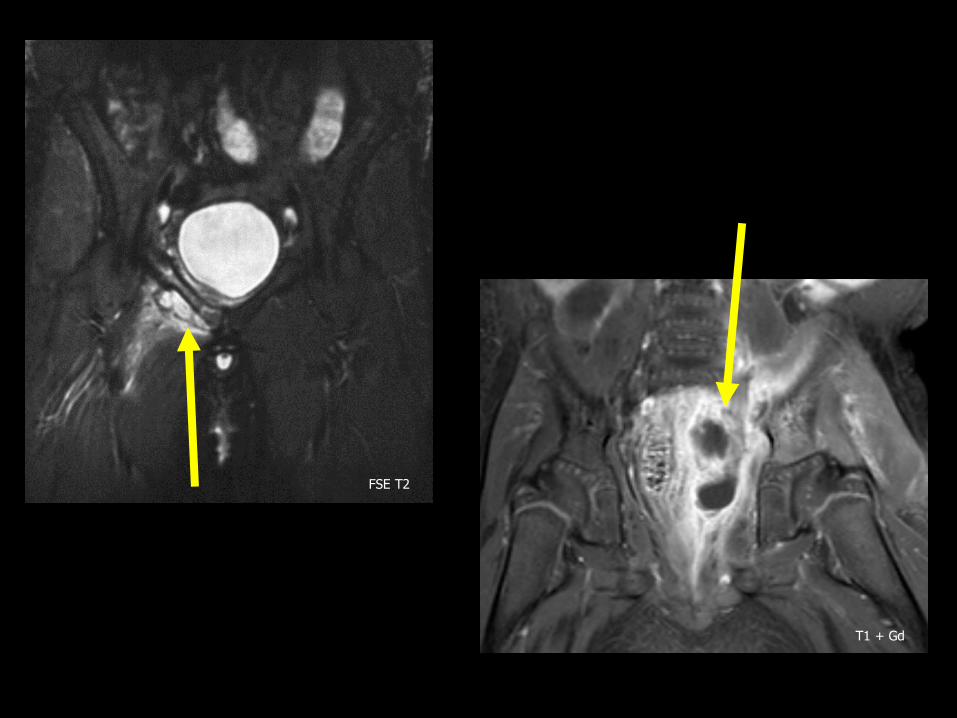
T1 + Gd
FSE T2

B
B
FSE T2
FSE T2

T1 + Gd
T1 + Gd
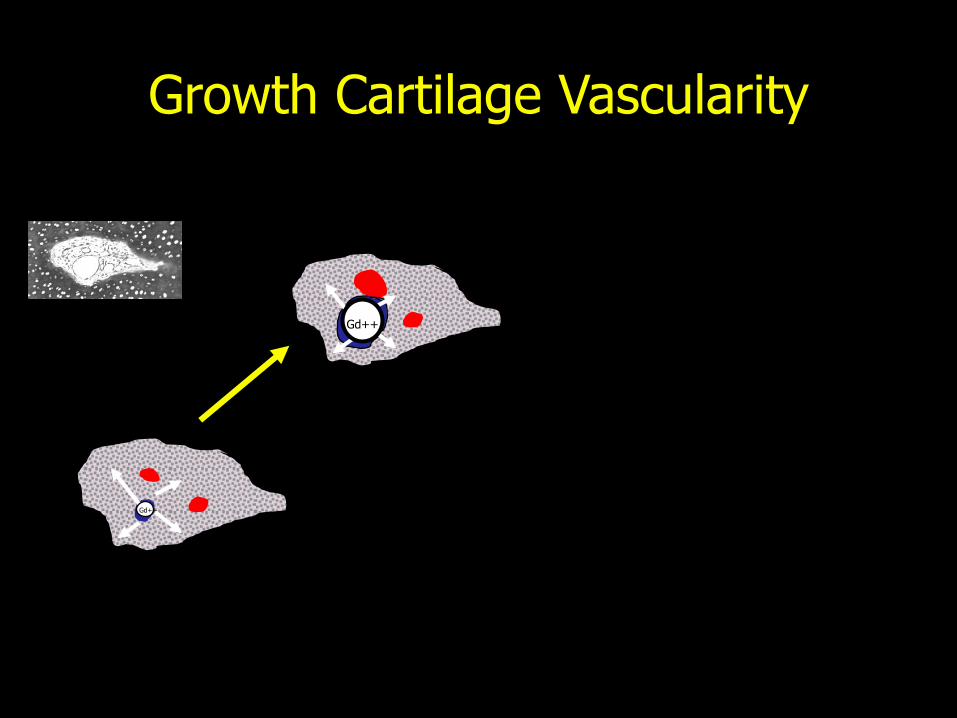
• Patterns of epiphyseal-metaphyseal vascularity:
– Infant: communication
– Child/adolescent: physis is a relative barrier
– Adult: continuity
Extension into the Physis and Epiphysis
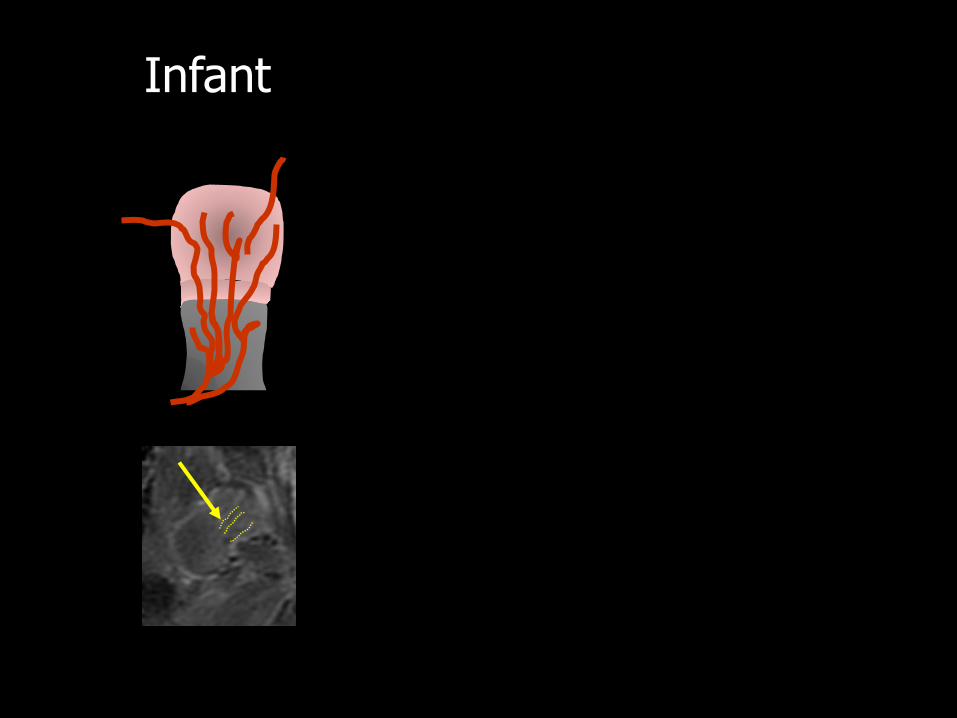
Infant
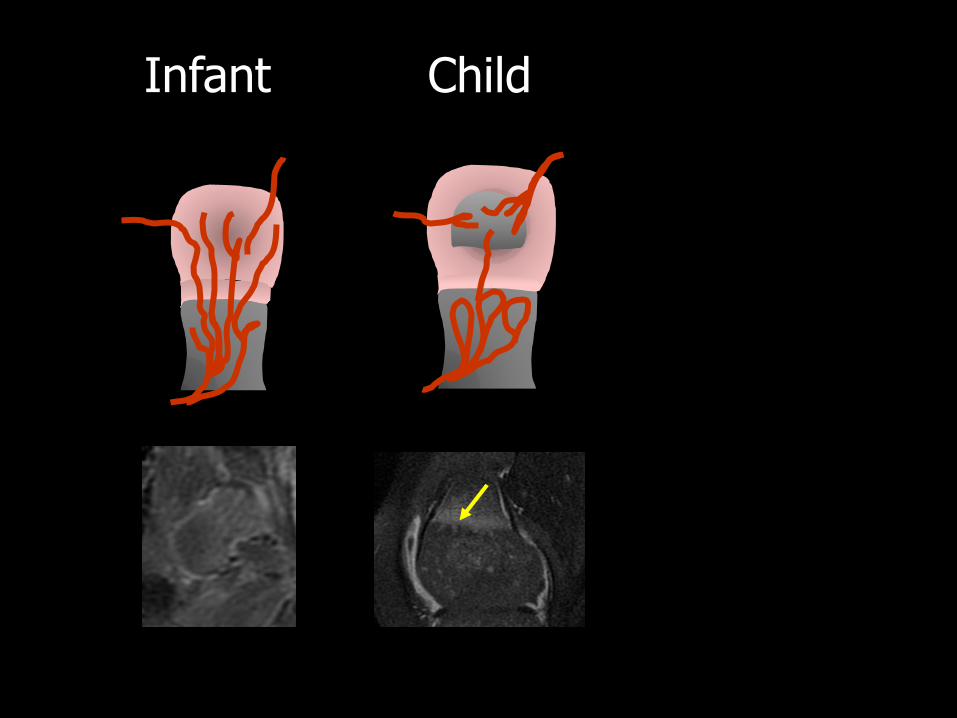
Infant Child

Infant Child Adolescent


FSE T2

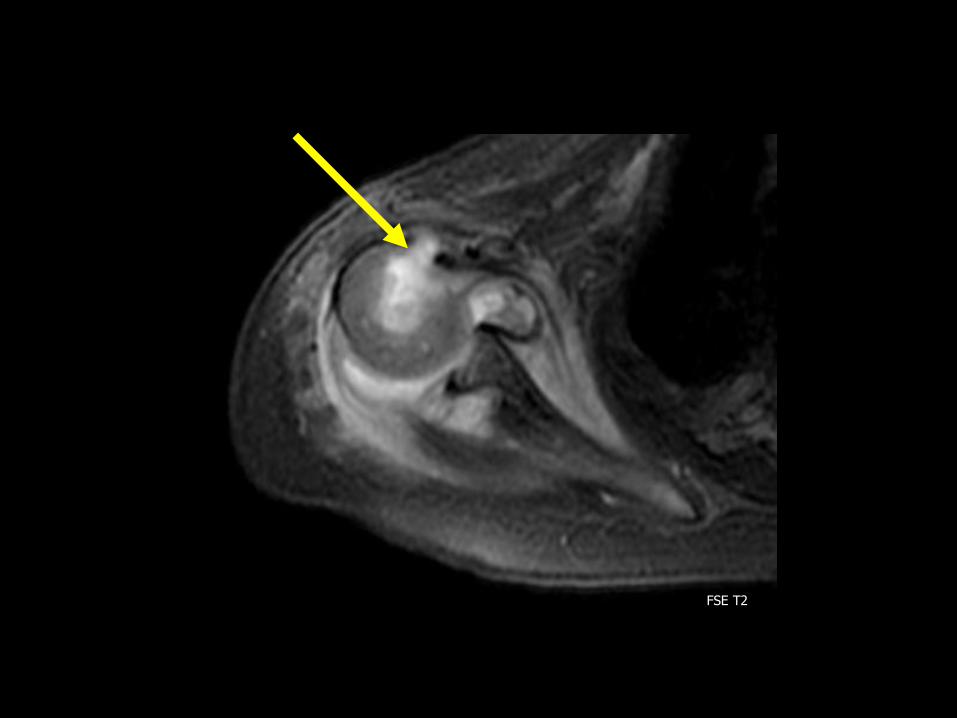
Extension into the Physis and Epiphysis
• Frequent in neonates
• Abnormal signal intensity and lack of enhancement of cartilage
• “Chondro-osteomyelitis” or “chondritis”


FSE T2
FSE T2
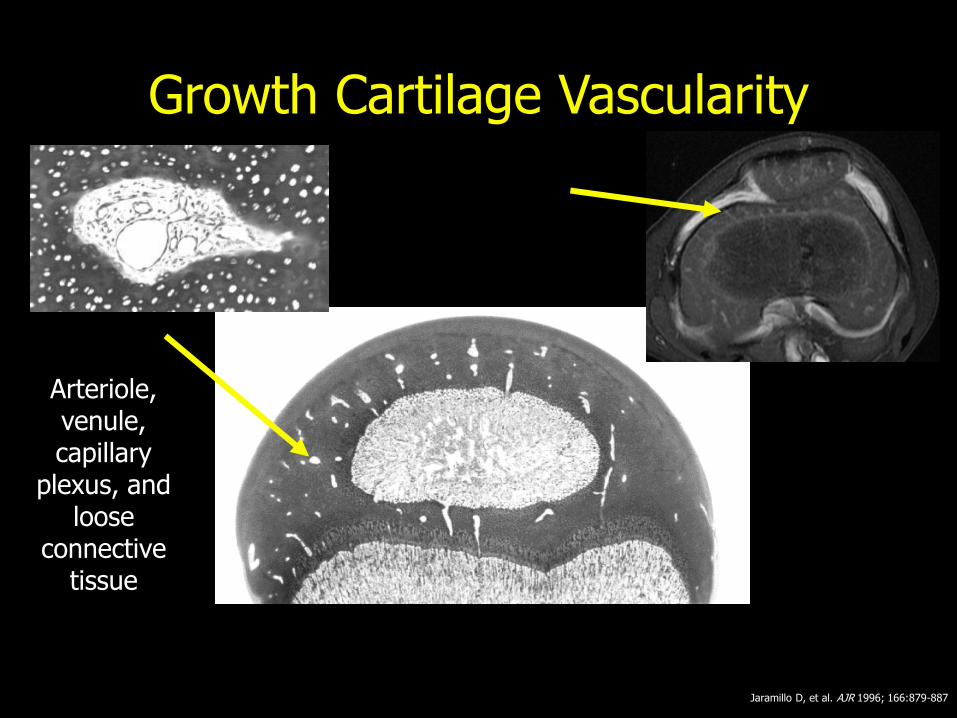
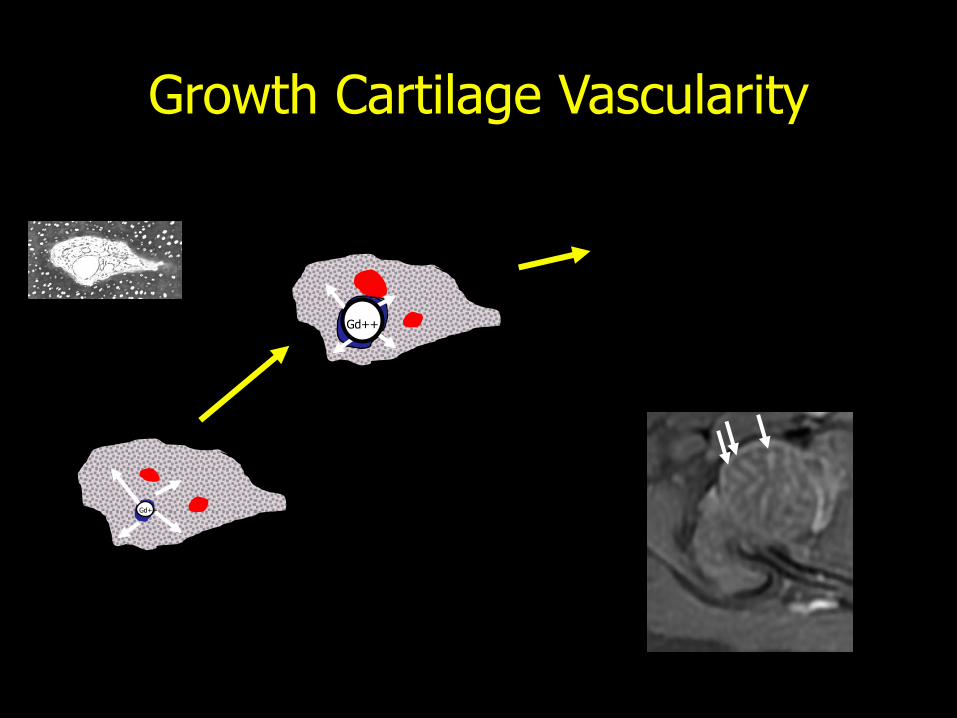
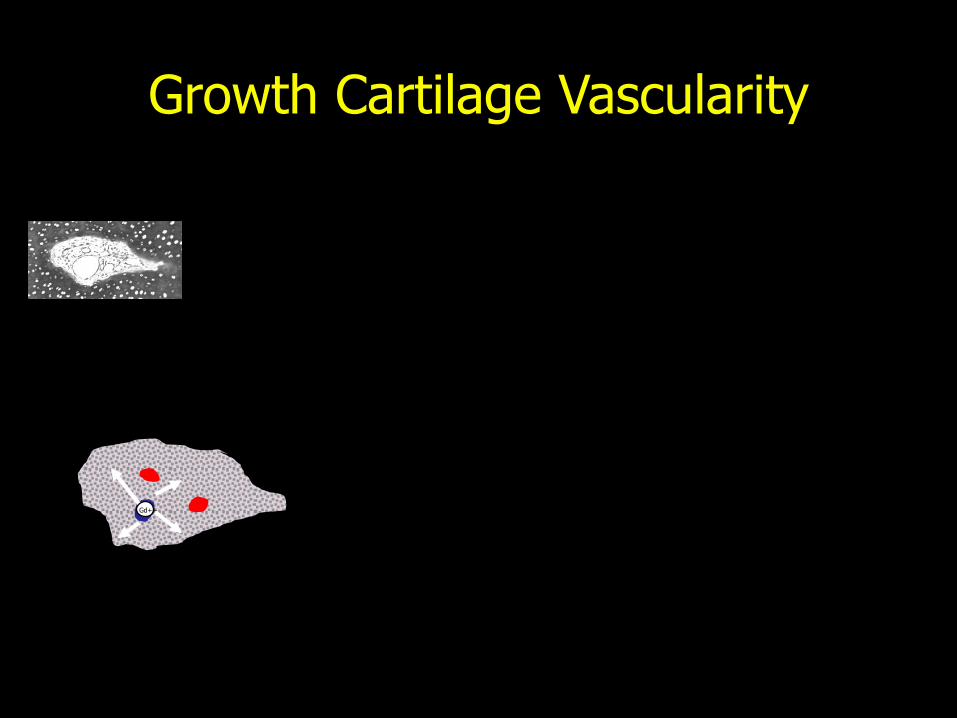
Growth Cartilage Vascularity
Jaramillo D, et al. AJR 1996; 166:879-887
Arteriole, venule, capillary
plexus, and loose
connective tissue

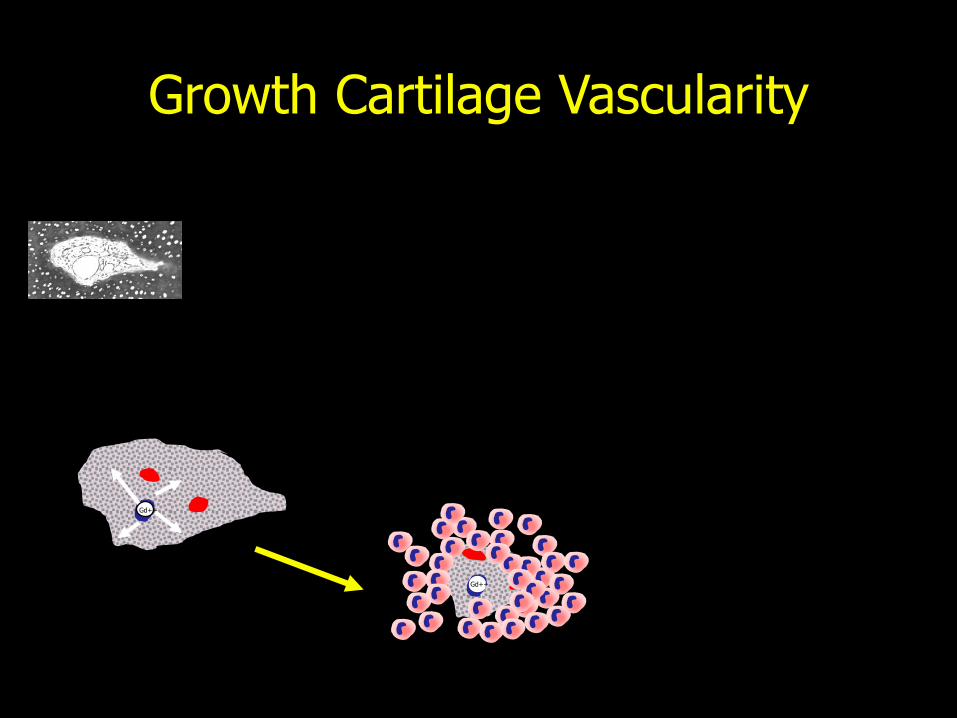
Growth Cartilage Vascularity
Gd++
Growth Cartilage Vascularity
Gd++
Gd++
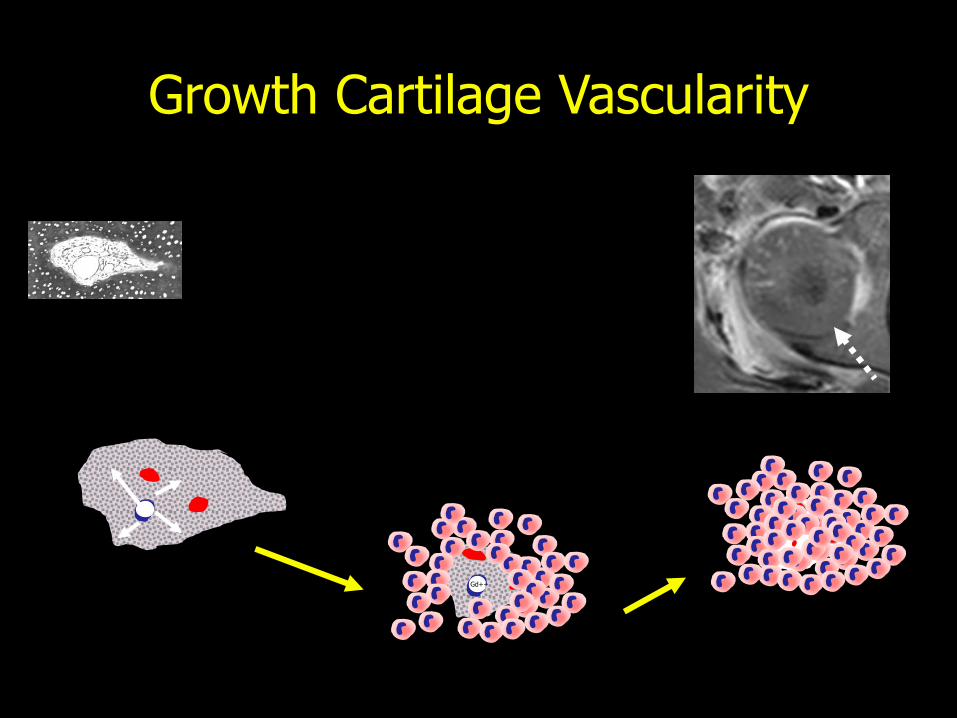
Growth Cartilage Vascularity
Gd++
Gd++
Growth Cartilage Vascularity
Gd++
Growth Cartilage Vascularity
Gd++
Gd++
Growth Cartilage Vascularity
Gd++

Growth Cartilage Vascularity
Gd++

10-month old girl with foot pain

FSE T2 T1 + Gd

FSE T2 T1 + Gd

after treatment
T1 + Gd

T1 + Gd

T1 + Gd

Extension into a Joint
• Epiphyseal osteomyelitis

FSE T2
Extension into a Joint
• Intracapsular location of metaphysis
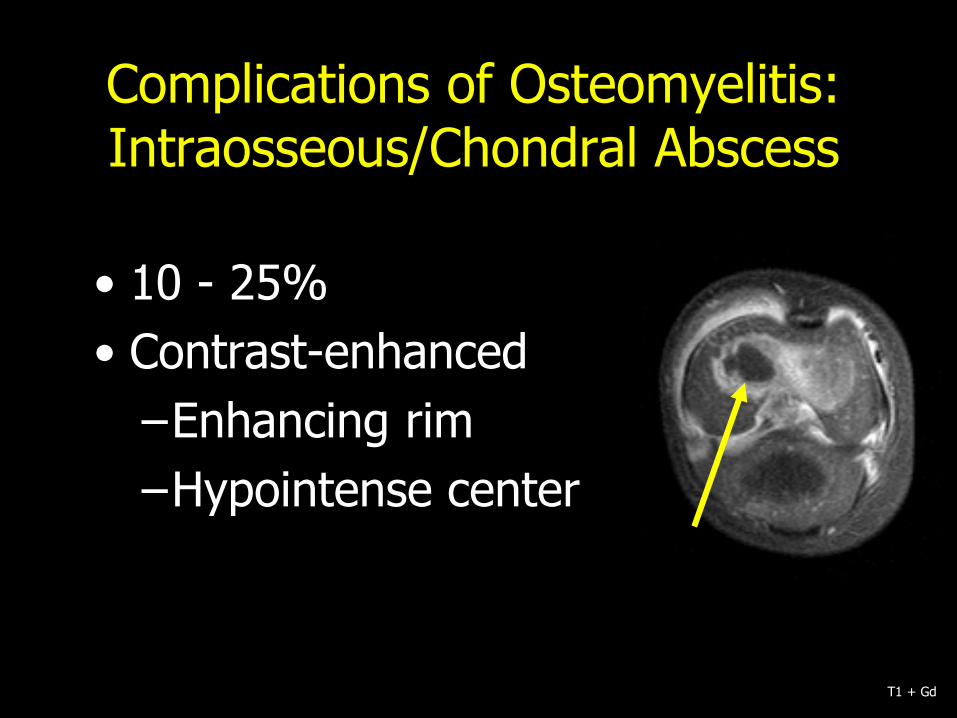
Complications of Osteomyelitis: Intraosseous/Chondral Abscess
• 10 - 25%
• Contrast-enhanced
–Enhancing rim
–Hypointense center
T1 + Gd


FSE T2 T1 + Gd
• Infection accounts for 10-15% of growth arrest
• Mechanisms:
– Direct destruction (metaphyseal focus)
– Ischemia (e.g. meningococcemia)
Complications of Osteomyelitis: Growth Arrest
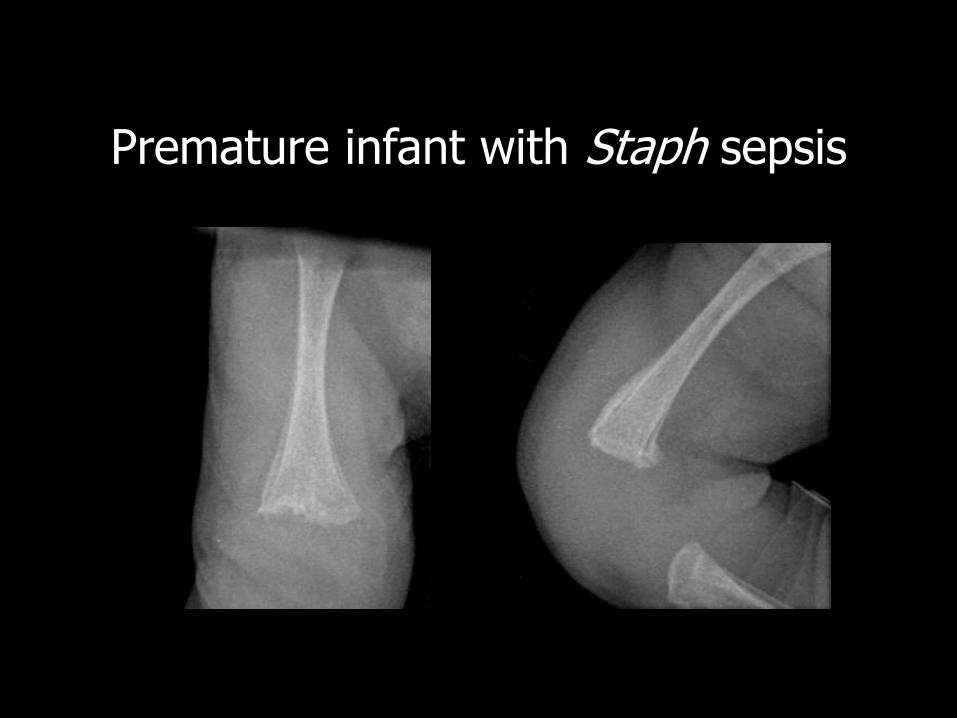
Premature infant with Staph sepsis

2 years later

FSE T2 FSE PD


FSE T2
T1 + Gd
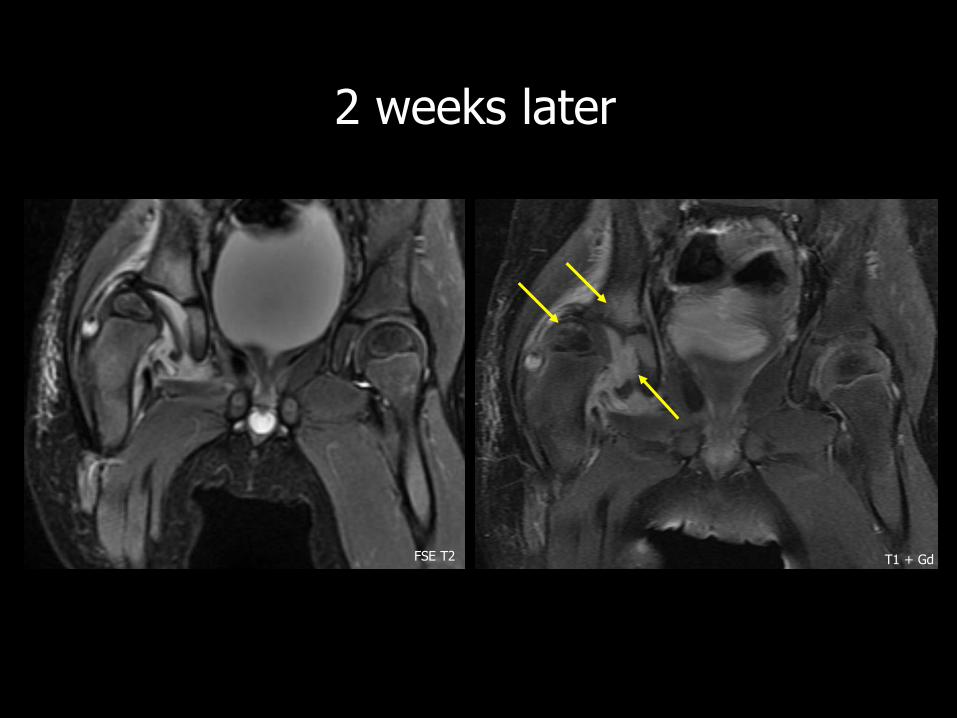
2 weeks later
FSE T2 T1 + Gd

1 year later
FSE T2

Considerations
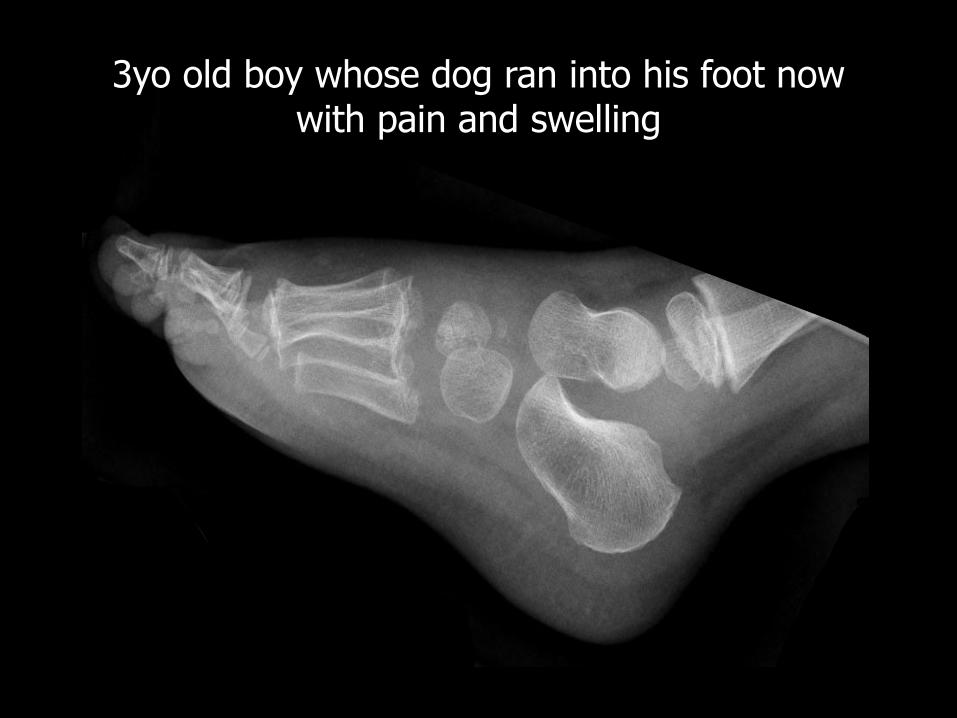
3yo old boy whose dog ran into his foot now with pain and swelling

6 weeks later, cast off, unable to bear weight

FSE T2 T1 + Gd

three weeks after the fall
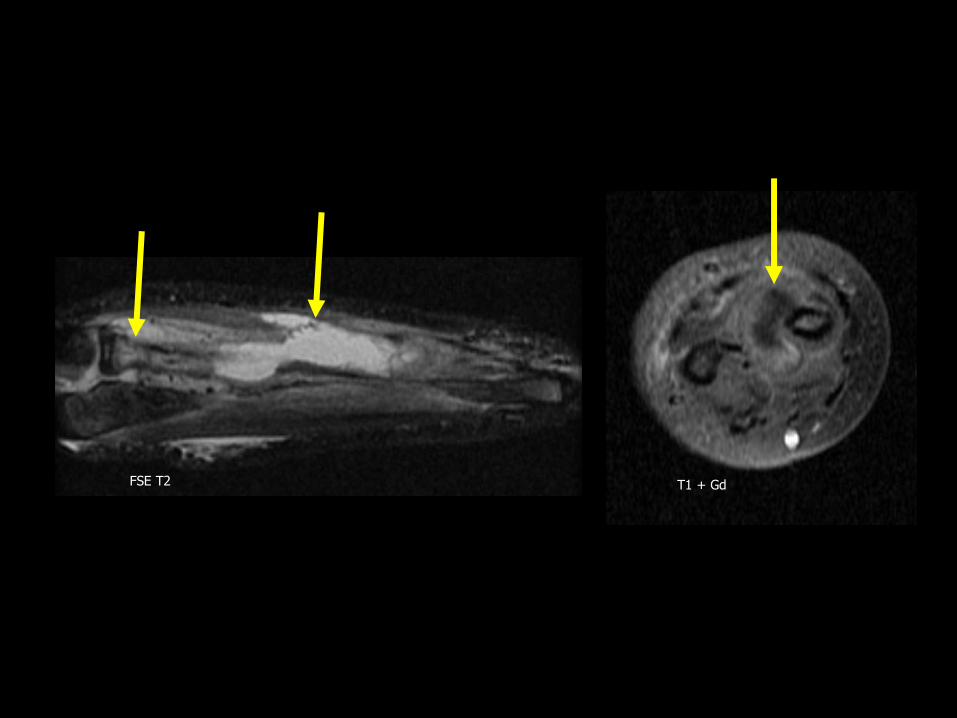
FSE T2 T1 + Gd


T1
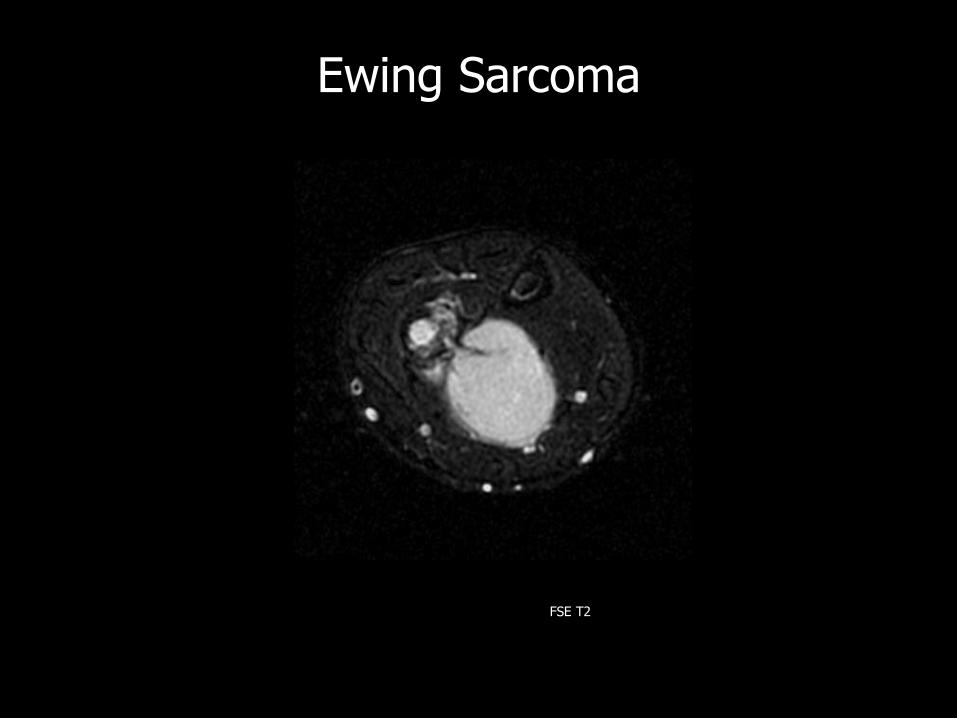
Ewing Sarcoma
FSE T2

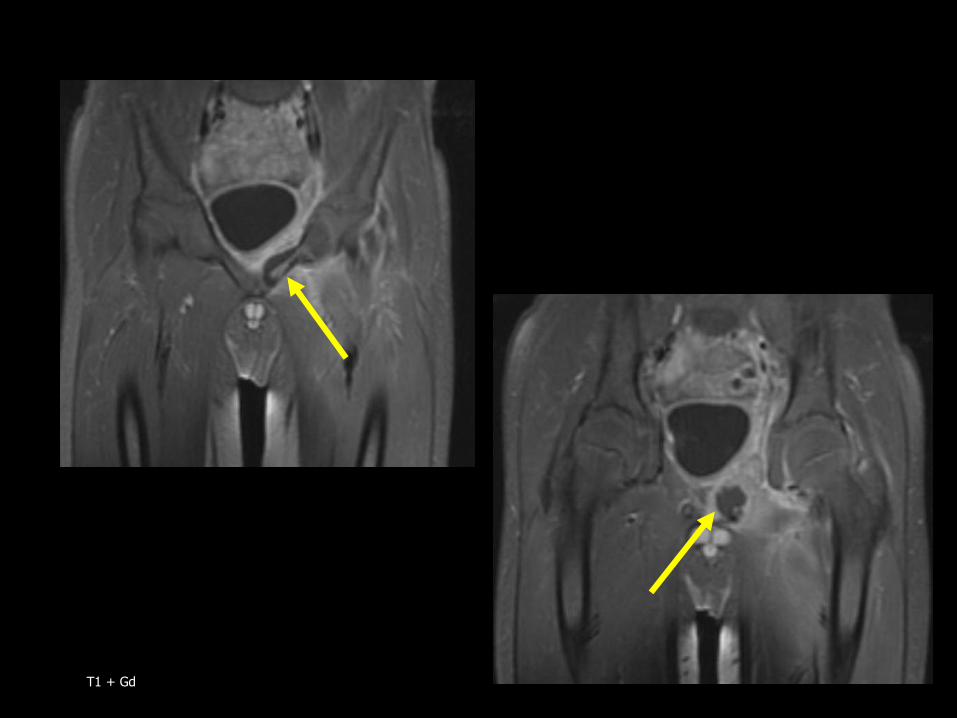
T1 + Gd

T1 + Gd

FSE T2
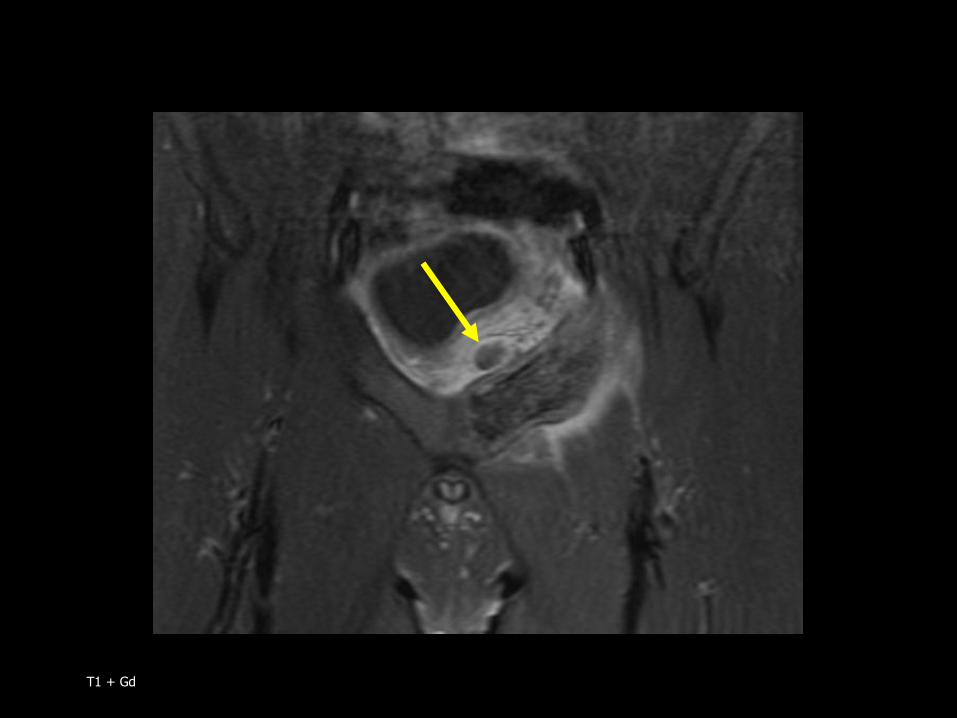
T1 + Gd
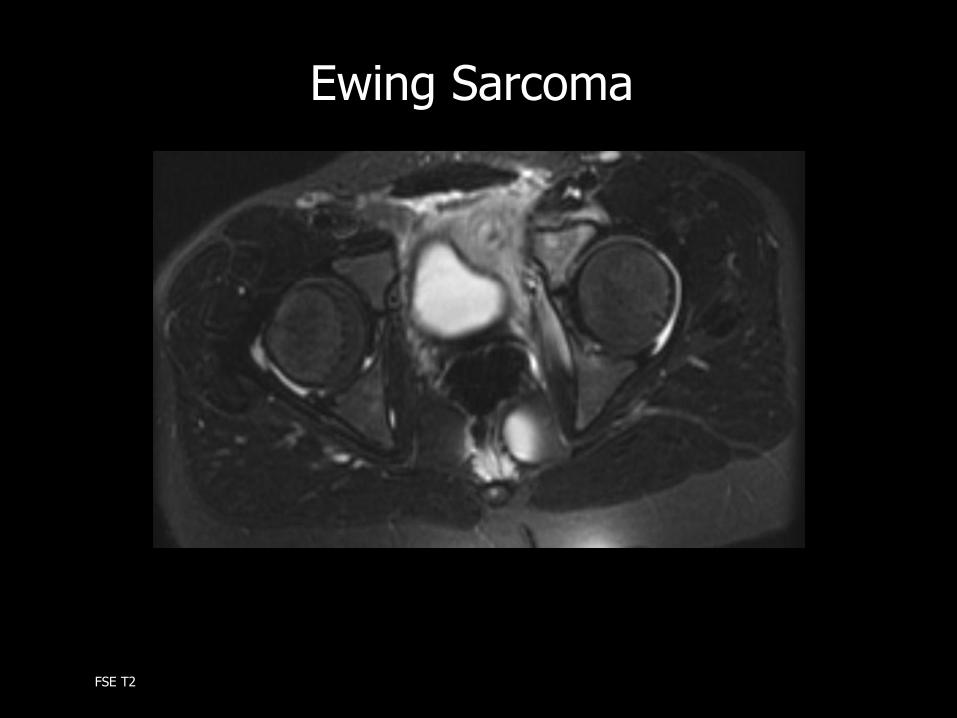
Ewing Sarcoma
FSE T2

3 yo girl with swollen knee

FSE T2

Juvenile Idiopathic Arthritis
T1 + Gd
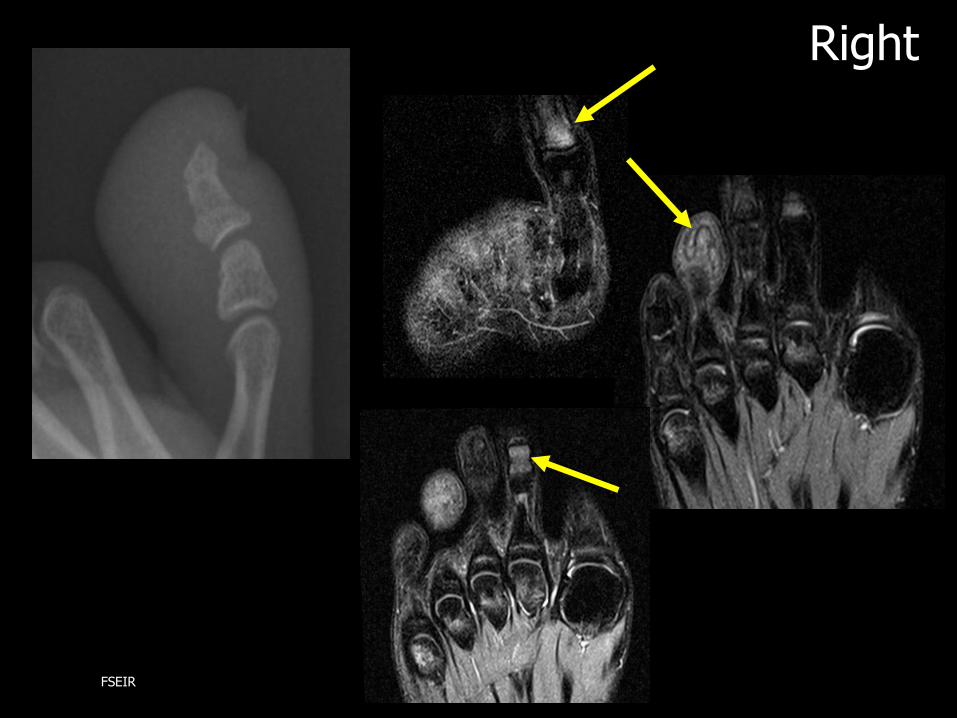
Right
FSEIR

Left
FSEIR