
Reconstruction of resected mandibles using a hydroxyapatite veterinary bone graft
6
609 Reconstruction of resected mandibles using a hydroxyapatite veterinary bone graft Wafaa I. Abdel-Fattah*, W.G. Osirist , Shamael S. MohamedS and M.R. Khalil’ *Ceramic Department, National Research Center, Egypt; ‘Biophysics Department, Faculty of Science, Cairo University, Giza, Egypt; ‘Faculty of Medicine, Alexandria University, Alexandria, Egypt; “Faculty of Dentistry, Alexandria University, Alexandria, Egypt A newly developed bone equivalent hydroxyapatite was derived from veterinary bone (VHAP). Sections of 1 cm of six rabbit mandibles were equally replaced by this VHAP graft. Radiological studies by X-ray were performed pre-operatively, immediately, and 1, 2 and 3 months post-operatively. The graft host-bone interface was examined periodically by scanning electron microscopy (SEM). Accompanying structural changes of the graft 3 months post-operatively were compared with the pre-operative findings by infra-red (IR) spectroscopic analysis. Complete union of the biomaterial to the host bone after 3 months was evidenced radiologically. SEM proved complete graft integration. This was accompanied by a decrease in optical density of the IR analysis of post-operative VHAP, indicating some leaching of the ions. Clinically, the graft was completely incorporated in the mandible without any complications. We discuss the use of VHAP in humans to reconstruct post-surgical mandibular defects. Keywords: Hydroxyapatite, bone-implant interface, mandibular grafting Received 5 April 1993; accepted 17 September 1993 Resection of a part of the mandible is required in many procedures of head and neck surgery, especially in tumours of the mandible and in the removal of a part of it following carcinoma invasion from the oral cavity and oropharynx’S ‘. It is also needed as a safety margin when there is a possibility of local spread or perineural spread via the inferior alveolar nerve3,4. Reconstruction of post-surgical mandibular defects is of paramount importance to restore the aesthetic state of the patient as well as to improve articulation and masticatory functions. During the last 3 decades, the material of choice for grafting alveolar clefts is autogenous particulate cancel- lous bone and marrow5,6, which is advantageously responsive to post-surgical functional demands, A significant morbidity is associated with autogenous grafting procedures; in addition, post-operative pain and the potential for cosmetic defects, seroma, haematomas, dehiscence and wound infection exist at virtually every donor site. In this connection iliac grafting has the additional risk of significant blood loss and neurosensory disturbance7-‘. Calcium phosphate bioceramics proved to be safe and effective for a variety of restorative and preserva- Correspondence to Dr W.I. Abdel-Fattah. tive clinical applications”. ll. The suitability of calcium phosphate ceramics for bone substitution is based on the fact that their elemental components are present in the bone naturally”. However, recent research indicates the presence of fragments of trical- cium phosphate occasionally localized in lymph nodes, a migration which is clinically undesirable13. Rapid rates of chemical dissolution in fl-tricalcium phosphate is a condition that can inhibit the regenera- tion of bone through the implant. De Grootr4 reported hydroxyapatite to be one of the most active ceramics with considerable promise as a hard tissue repair and/ or replacement material. Dense hydroxyapatite was reported to be non-reversible while porous hydroxyapa- tite is reversible. The following considerations might be included in the clinical criteria for an ideal bone graft and/or implant material: 1. It exists in unlimited supply without the need of secondary surgical site. 2. It does not exhibit antigenitic properties. 3. It facilitates revascularization. osteoinduction, osteo- genesis and osteoconduction within the defect and provides stability and support’5. The present article is part of a study to evaluate the repair of mandibular defects using porous hydroxyapa- c 1994 Butterworth-Heinemann Ltd 0142.9612/94/15609-06 Biomaterials 1994, Vol. 15 No. 8
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Reconstruction of resected mandibles using a hydroxyapatite veterinary bone graft

609
Reconstruction of resected mandibles using a hydroxyapatite veterinary bone graft
Wafaa I. Abdel-Fattah*, W.G. Osirist , Shamael S. MohamedS and M.R. Khalil’ *Ceramic Department, National Research Center, Egypt; ‘Biophysics Department, Faculty of Science, Cairo University, Giza, Egypt; ‘Faculty of Medicine, Alexandria University, Alexandria, Egypt; “Faculty of Dentistry, Alexandria University, Alexandria, Egypt
A newly developed bone equivalent hydroxyapatite was derived from veterinary bone (VHAP).
Sections of 1 cm of six rabbit mandibles were equally replaced by this VHAP graft. Radiological
studies by X-ray were performed pre-operatively, immediately, and 1, 2 and 3 months post-operatively.
The graft host-bone interface was examined periodically by scanning electron microscopy (SEM).
Accompanying structural changes of the graft 3 months post-operatively were compared with the
pre-operative findings by infra-red (IR) spectroscopic analysis. Complete union of the biomaterial to
the host bone after 3 months was evidenced radiologically. SEM proved complete graft integration.
This was accompanied by a decrease in optical density of the IR analysis of post-operative VHAP,
indicating some leaching of the ions. Clinically, the graft was completely incorporated in the mandible
without any complications. We discuss the use of VHAP in humans to reconstruct post-surgical
mandibular defects.
Keywords: Hydroxyapatite, bone-implant interface, mandibular grafting
Received 5 April 1993; accepted 17 September 1993
Resection of a part of the mandible is required in many procedures of head and neck surgery, especially in tumours of the mandible and in the removal of a part of it following carcinoma invasion from the oral cavity and oropharynx’S ‘. It is also needed as a safety margin when there is a possibility of local spread or perineural spread via the inferior alveolar nerve3,4. Reconstruction of post-surgical mandibular defects is of paramount importance to restore the aesthetic state of the patient as well as to improve articulation and masticatory functions.
During the last 3 decades, the material of choice for grafting alveolar clefts is autogenous particulate cancel- lous bone and marrow5,6, which is advantageously responsive to post-surgical functional demands, A significant morbidity is associated with autogenous grafting procedures; in addition, post-operative pain and the potential for cosmetic defects, seroma, haematomas, dehiscence and wound infection exist at virtually every donor site. In this connection iliac grafting has the additional risk of significant blood loss and neurosensory disturbance7-‘.
Calcium phosphate bioceramics proved to be safe and effective for a variety of restorative and preserva-
Correspondence to Dr W.I. Abdel-Fattah.
tive clinical applications”. ll. The suitability of calcium phosphate ceramics for bone substitution is based on the fact that their elemental components are present in the bone naturally”. However, recent research indicates the presence of fragments of trical- cium phosphate occasionally localized in lymph nodes, a migration which is clinically undesirable13. Rapid rates of chemical dissolution in fl-tricalcium phosphate is a condition that can inhibit the regenera- tion of bone through the implant. De Grootr4 reported hydroxyapatite to be one of the most active ceramics with considerable promise as a hard tissue repair and/ or replacement material. Dense hydroxyapatite was reported to be non-reversible while porous hydroxyapa- tite is reversible.
The following considerations might be included in the clinical criteria for an ideal bone graft and/or implant material:
1. It exists in unlimited supply without the need of secondary surgical site.
2. It does not exhibit antigenitic properties. 3. It facilitates revascularization. osteoinduction, osteo-
genesis and osteoconduction within the defect and provides stability and support’5.
The present article is part of a study to evaluate the repair of mandibular defects using porous hydroxyapa-
c 1994 Butterworth-Heinemann Ltd 0142.9612/94/15609-06
Biomaterials 1994, Vol. 15 No. 8

610 mandible reconstruction using VHAP: W.i. A~de/-~~ff~~ et al.
tite of veterinary origin (VHAP), after being chemically and thermelly treated to extract the antigenicity of its organic constituents.
~TER~LS AND ~HODS
~ydrQxyaFat~ta ~reparatiu~
The veterinary bone was crushed and boiled for several hours in a solution of sodium carbonate to extract the organic material. The bone fragments were thermally treated by heating up to 600°C in an electrically heated furnace16. X-ray dif~a~tion patterns proved the structure to be that of hydroxyapatito ~~~g~re 11 using a Cu K, target and a Philips X-Ray ~if~~ctometer (type ~~6~~~~).
Surgical pmcedure
1. Six healthv rabbits of known breed (Flanderf, 3-4 months of age and 1.5-2 kg in weight, were the subject of this study. Ketamine hydrochloride (Ketalar) intramuscular anaesthesia at a dose of 10mlfkg body weight was used to anaes~etize the animals. The mandible was exposed by reflecting a mucoper- iosteaf flap from the gingival margin extending from the ascending ramps up to the canine region without injury to the teeth. Osteotomy of a square piece af full thickness of mandible bone (1 x 1 cm) was performed using bone cutting forceps. A sterile (VHAP) block was shaped to fit into the created defect to repair and replace the excised bone. The soft tissues were approxi- mated and the mu~oper~oste~m was sutured over the implant using 000 catgut sutures. A pre- operatively prepared splint was then fixed by circumferential wires for 3 weeks. The animals’ mandibles were not im~~~bilized. They were killed after 1.5 and 3 months (three rabbits each time).
Radiographic evaluation
Occlusal X-ray exposures were used to evaluate the progress of healing of the repaired resected mandibles. Films were recorded for each rabbit pre-operatively, immediately, and 1, 2 and 3 months F~st”operatively.
Scan&g electrun microscopy @EM]
The host bone and the grafted area were obtained from animals killed 1.5 and 3 months post-o method advocated by White and Shors’ P
eratively. The was followed.
In&a-red spectral analysis
Samples of the biomaterial (VHAP) were evaluated pre- and 3 months post-operatively to evaluate consecutive structural changes, Measurements were carried out in the range of ~%@-600cm-’ using a Beckman Infra-red Spectrophotometer (Type 4220), The KBr disc technique was used in this study. For the sake of comparison the IR spectrum of cancellous bone was also included.
RESULTS
The X-ray diffraction (XRD) analysis (F’igure 2) of the prepared VHAP revealed the structure of typical h}7dr~xyapatite with no other detectable phases.
Clinically, all wouads healed uneventfully by first interactions. All animals continued to gain weight. After 3 months, it was not possible to differentiate the VHAP implant from the host bone by clinical examina- tion as normal contours were achieved.
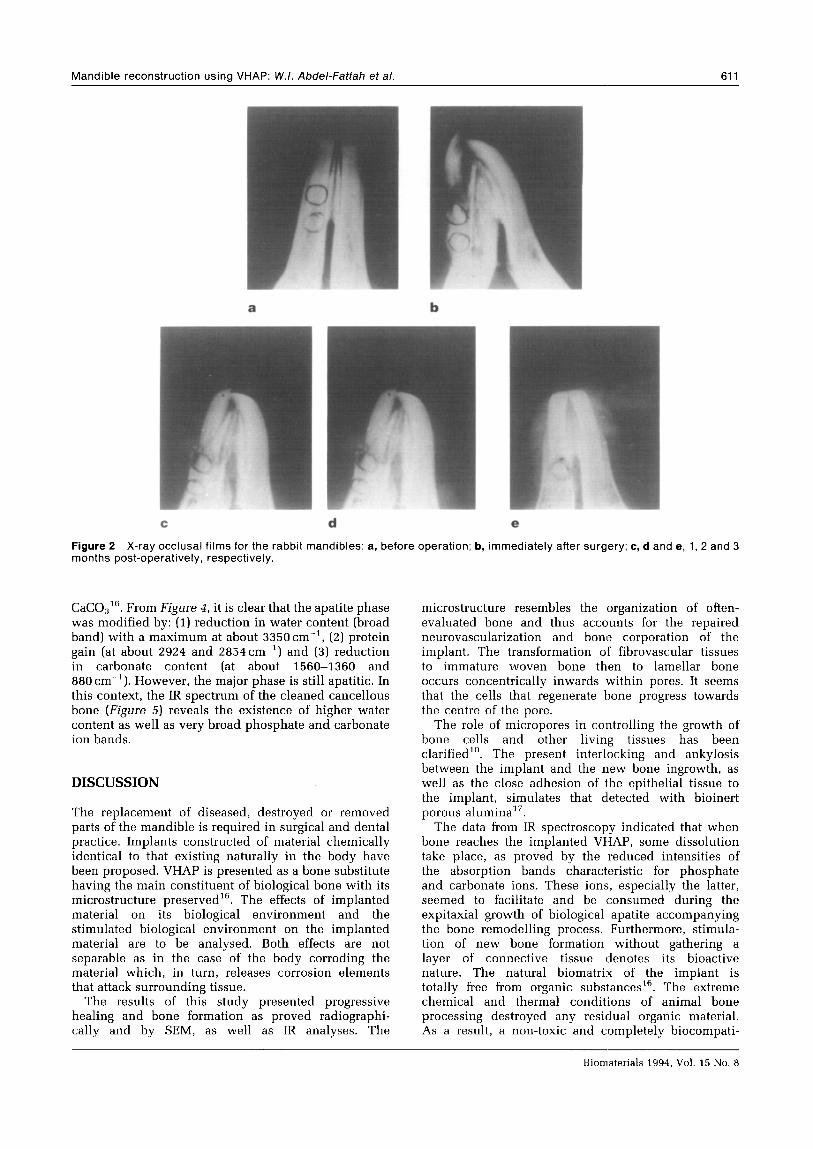
The mandibles of the rabbits before surgery are shown in Figure ~a. Figure 2b shows the bone defect of 1 x 1 cm with the implant in position separated completely from the host bone. The 2 month post- operation film shows that the implant is still separated from the host bone (Figure ZC), although the start of assembly and orientation of the implant can be observed. Two months post-operatively (Figore Ed), the implant is well oriented in its site and greatly approximates the host bone. There is some degree of demarcation between the graft and the surrounding bone, Three months p~s~~~peratively, the implant (Fjgure 2e) is Gompletely fused to the bone and could not be defined from it due to its complete integrations
Scanning electron microscapic examinaiion [Figure 3af illustrates the incomplete line of demarcation between the host bone (Hb) and the implant bone (Ib) after 1.5 months post-operation. Partial healing and soft tissue integration, which are clearer in Figure 3b, are noted, Complete integration between the host bone and implant bone is clearly noticed 3 months post- operatively, with pores starting to be filled with soft tissue simulating the Harvesian system of natural bone (Figure 3~). Complete lining of pores by tissue and implant is seen to be fully integrated in the bone (Figure 3d). F‘b I rous tissue is recognized invading the implant through the pores in some other areas (Figure 3tZ).
The IR spectral analysis of the bone p~st~gr~~ing (II) exhibits lower intensity compared with that of its original state (1) in the IR regions characteristic for carbonate and phosphate groups (F&ure 4) This indicates the partial resorption of these ions by the host bone. The presence of carbonate ions is not surprising as it was reported that bono contains
Wydroxyapatite phase
I f t
40 35 30 28*/nin (Cu Kaj
Figure 1 X-ray diffraction analysis of the prepared VHAP (Cu K, target).
Biomateriafs 1994, Vol. 15 No. 8
Mandible reconstruction using VHAP: W.I. Abdel-Fattah et al. 611
b
d e
Figure 2 X-ray occlusal films for the rabbit mandibles: a, before operation; b, immediately after surgery; c, d and e, 1, 2 and 3 months post-operatively, respectively.
CaC03”. From Figure 4, it is clear that the apatite phase was modified by: (1) reduction in water content (broad band) with a maximum at about 3350cm-‘, (2) protein gain (at about 2924 and 2854cm-‘) and (3) reduction in carbonate content (at about 1560-1360 and 880 cm-‘). However, the major phase is still apatitic. In this context, the IR spectrum of the cleaned cancellous bone (Figure 5) reveals the existence of higher water content as well as very broad phosphate and carbonate ion bands.
DISCUSSION
The replacement of diseased, destroyed or removed parts of the mandible is required in surgical and dental practice. Implants constructed of material chemically identical to that existing naturally in the body have been proposed. VHAP is presented as a bone substitute having the main constituent of biological bone with its microstructure preserved16. The effects of implanted material on its biological environment and the stimulated biological environment on the implanted material are to be analysed. Both effects are not separable as in the case of the body corroding the material which, in turn, releases corrosion elements that attack surrounding tissue.
The results of this study presented progressive healing and bone formation as proved radiographi- tally and by SEM, as well as IR analyses. The
microstructure resembles the organization of often- evaluated bone and thus accounts for the repaired neurovascularization and bone corporation of the implant. The transformation of fibrovascular tissues to immature woven bone then to lamellar bone occurs concentrically inwards within pores. It seems that the cells that regenerate bone progress towards the centre of the pore.
The role of micropores in controlling the growth of bone cells and other living tissues has been clarified’“. The present interlocking and ankylosis between the implant and the new bone ingrowth, as well as the close adhesion of the epithelial tissue to the implant, simulates that detected with bioinert porous alumina17.
The data from IR spectroscopy indicated that when bone reaches the implanted VHAP, some dissolution take place, as proved by the reduced intensities of the absorption bands characteristic for phosphate and carbonate ions. These ions, especially the latter, seemed to facilitate and be consumed during the expitaxial growth of biological apatite accompanying the bone remodelling process. Furthermore, stimula- tion of new bone formation without gathering a layer of connective tissue denotes its bioactive nature. The natural biomatrix of the implant is totally free from organic substanceslfi. The extreme chemical and thermal conditions of animal bone processing destroyed any residual organic material. As a result, a non-toxic and completely biocompati-
Biomaterials 1994, Vol. 15 No. 8

612 Mandible reconstruction using VHAP: W.I. Abdel-Fattah et a/.
Figure 3 Scanning electron micrographs of the mandible of rabbit: a and b, 1.5 months post-operatively; c, d and e, 3.0 months post-operatively. lb, implanted bone; Hb, host bone.
ble material is obtained. In this connection, the IR spectroscopic analysis successfully proved bone proliferation as some peaks of protein were accompa- nied by some release of carbonate and phosphate to host tissue. Several authors’s~‘g denoted the role of the carbonate ions of apatite against rapid leaching before new bone formation after grafting in osseous and non-osseous sites - a case which, although qualitative, is not easily detected by radiography and SEM.
CONCLUSIONS
The VHAP can be classified as a bioactive biomater- ial having its natural porosity preserved, which enhances the large number of ingrowth cells that guarantee close adhesion and prevent infection from the implant, and therefore presents favourable biocompatibility. The present material solves many problems associated with porous implants. The degree of interconnectivity which occurs naturally in the veterinary bone eliminates the problem of narrowed and dead-ended pathways that may prevent fibrovas- cular tissue and bone to fully penetrate the implant.
The present VHAP has another advantage of being easily and readily shaped by the surgeon, facilitating exact contouring of the implant. Precise placement is enhanced and bulk displacement is prevented.
Biomaterials 1994, Vol. 15 No. 8

Mandible reconstruction using VHAP: W.I. Abdel-Fattah et al. 613
Wavelength (urn) 602.53.0 f 7 a 9 10 11 12 131415 1 I I I I III m
‘$ - __’
1560-1360cm -1 f24T-goo ,,-l/-aaO cm-'
-.m____--’
I I I I I I 4000 3600 3200 2800 1600 1400 1200 1000 800 650
Wavenumber -1
[cm 1
Figure 4 IR spectral analysis of VHAP before and after 3 months grafting: ---, pre-operatively; -, post-operatively.
1200-900 cm -1
OCCO 4000
Wavenumber (cm -1 )
Figure 5 IR spectral analysis of cancellous bone before thermal treatment.
Porous implants of veterinary origin (VHAP) proved to be well-integrated in bones and, therefore, they can be used in the restoration of mandibular defects created by surgery for cancer, intraoral cancer regions, excisions of mandible for safety margins, alveolar carcinoma and mandibular tumours. The IR spectroscopy technique should complement other techniques to assess bone formation and/or resorption.
REFERENCES
1 Hoopes JE. The forehead flap in intraoral reconstruc- tion. In: Anderson R, Hoopes JE, eds. Symposium of Malignancy of the Head and Neck. St Louis: CV Mosby, 1975; 1: 193-195.
2 De Santo LW, Wicker JH, Deswek. Mandibular osteot- omy and lingual flaps in patients with cancer of the tonsil and tongue base. Arch Otolaryngol 1975; 101: 652.
3 Mardelson BC, Hadgkinson DJ, Woods E. Cancer of the oral cavity. Surg Clin N Am 1977; 57: 285.
4 Flynon MB, Moor C. Marginal resection in the manage- ment of squamous cancer of the floor of the mouth. Am J Surg 1974; 128: 490.
5
6
7
8
9
10
11
12
13
14 15
Boyne PJ, Sands NR. Secondary bone grafting of residual alveolar and palatal clefts. J Oral Surg 1972; 30: 87. Hall HD, Posmick JC. Early results of secondary bone grafts in 106 alveolar clefts. J Oral Maxillofac Surg 1983; 41: 289. Cowley SP, Anderson LD. Hernias through donor sites for iliac bone grafts. J Bone Joint Surg 1983; 65-A: 1023. Cocklin J. Autogenous bone grafting-complications at the donor sites. JBone Joint Surg 1971; 53-B: 153. Laure SWS, Kabau LB, Mulliken, et al. Donor site morbidity after harvesting rib and iliac bone. Plast Reconst Surg 1984; 73: 933. Marx RE, Miller RI, Ehler WJ et al. A comparison of particulate allogenic and particulate autogenous bone grafts into maxillary alveolar clefts in dogs. J Oral Maxillofac Surg 1984; 42: 3. De Groot K. Bioceramics consisting of calcium phosphate salts. Biomaterials 1980; 1: 47. Lavernia C, Schoenung JM. Calcium phosphate ceramics as bone substitutes. Am Ceram Sot Bull 1991; 70: 95. White E, Shors EC. Biomaterial aspects of interpore- porous hydroxyapatite. Dent Clin N Am 1986; 30: 49. De Groot K. Interceram, No. 4238-41, 1987. Cobb CM, Eick SD, Barker BF, Moshy EL, Hiatt WR. Restoration of mandibular continuity defects using
Biornaterials 1994. Vol. 15 No. 8

614 Mandible reconstruction using VHAP: W.I. Abdel-Faftah et al.
combinations of hydroxyapatite and autogenous bone: microscopic observations. J Oval Maxillofac Surg 1990; 48: 268.
16 Abdel-Fattah WI, Selim MM. Thermal behaviour of both chemically precipitated and biological hydroxyapatites. Ceramica Acta 1991; 4: 65.
17 Kawalara H. Bioceramics Symp, Keel, 1978. 18 Heughebaert M, Le Geros RZ, Oineste M, Ouilhem A,
Bone1 0. Physicochemical characterization of deposits associated with HA ceramics implanted in nonosseous sites. J Biomed Mater Res Appl Biomaterials 1988; 22: 257.
19 Daculsi G, Le Geros RZ, Heughebaert M, Barbieux I. Formation of carbonate-apatite crystals after implanta- tion of calcium phosphate ceramics. Calc Tissue Int 1990; 46: 20.
Second International Symposium on Computer Methods in
Biomechanics and Biomedical Engineering
21-24 September 1994
Marriott Hotel, Swansea, Wales, UK
The objective of the symposium, the second in the series, is to focus on the progress and rapid advances being made in computer modelling applied to biomedical engineering problems and also to bring together leading researchers, scientists and clinicians working in this area. The format of the Symposium will follow a pattern of invited lectures which will be presented by distinguished contributors and these will be complemented by presentations from the Symposium participants.
Primary inkrest will be placed on prosthesis design and response, joint and bone mechanics and hard/sofi tissue analysis. Material modelling, analysis of biological mechanisms, computer implementation and experimental verification will also be reviewed. Particular consideration will be given to new and recent advances associated with these areas of research.
For further information please contact: John Middleton, Centre for Biomechanics and Biomedical Engineering, Engineering Building, University College Swansea, Singleton Park, Swansea SA2
Biomaterials 1994, Vol. 15 No. 8




















